Submitted:
29 June 2023
Posted:
03 July 2023
You are already at the latest version
Abstract
Gastric cancer is among the top 5 causes of cancer-related death worldwide. Preoperative chemotherapy has been established as an option in patients with locally advanced gastric cancer. However, chemotherapy yields variable results, owing to the cellular and molecular heterogeneity of this disease. Identifying patients who did or did not respond to preoperative therapy can allow clinicians to alter treatment modalities and provide important information related to prognostication. Pathologic response to preoperative therapies, called Tumor Response Grade (TRG), has been evaluated to quantify treatment response. Multiple systems for TRG have been established. However, literature has demonstrated inconsistent results for TGR systems and prognosis, possibly due to variability in interpretation of tumor response between systems and interobserver variability. Radiographic response to preoperative therapies using RECIST 1.1 criteria and endoscopically-assessed tumor response have demonstrated association with survival; however their use in gastric cancer remains challenging given the inability to accurately and consistently identify and measure the tumor, especially in the setting of neoadjuvant therapy where treatment-related changes can obscure the gastric wall layers. This review is focused on summarizing the available literature related to evaluating TRG in gastric cancer, as well as providing a brief overview on the use of radiographic and endoscopic methods to assess response to preoperative therapies. Lastly, we outline future directions regarding the use of a universal TRG system to guide care and assist with prognosis.
Keywords:
tumor response grade (TRG)
; gastric cancer
; RECIST
; tumor regression score
1. Introduction
Gastric cancer is the 5th most common cancer worldwide and 4th most common cause of cancer-related death, with over 1 million new cases and nearly 800 thousand deaths reported in 2020 (GLOBOCAN, 2020) [1]. Neoadjuvant therapies, including chemotherapy, chemoradiation and immunotherapy, are part of the treatment armamentarium for gastric cancer. Retrospective studies demonstrate that neoadjuvant therapy is associated with improvement in survival, particularly for more advanced stages [2]. Preoperative therapies for select patients can provide a plethora of advantages compared to adjuvant treatments. They allow for possible downstaging, decreasing the size of the primary tumor, reducing the extent of lymph node involvement, treating micrometastatic disease, and subsequently improving survival by increasing the chances of complete resection and cure. Additionally, preoperative systemic therapy ensures the delivery of systemic therapy in patients while therapy in the adjuvant setting may be hindered due to post-operative complications. Selecting the optimal preoperative treatment option depends on multiple factors, such as histology, tumor stage, gene expression status, patient comorbidities, performance status and toxicity profile of each therapeutic agent. Assessing response to preoperative chemotherapy can provide information regarding prognostication and help clinicians guide treatment in this patient population [3, 4].
2. Gastric Cancer and Preoperative Therapies
Patients with gastric adenocarcinoma clinical T2 stage (invasion of the muscularis propria) or higher, irrespective of nodal status, are candidates for either upfront surgery, neoadjuvant chemoradiation, or perioperative chemotherapy. Upon completion of any preoperative systemic therapy, patients are restaged and then undergo surgical resection, if their disease remains resectable [3]. The Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial from the UK showed that patients with resectable clinical >stage II (M0) disease treated with perioperative chemotherapy (three cycles pre- and three cycles post-operatively of epirubicin, cisplatin and 5FU [ECF]) had an improved 5 year survival rate of 36% versus 23% in the surgery-only group [5]. The FNCLCC/FFCD phase 3 trial from France showed similar results to the MAGIC trial, with patients who were treated with cisplatin-5FU followed by surgery having a 5-year survival rate of 38% compared to 24% in the surgery-only group [6]. In 2019, the results of a phase 2/3 trial from Germany showed that patients with >T2 and/or N-positive disease who received fluorouracil plus leucovorin, oxaliplatin and docetaxel (FLOT), had improved median overall survival (OS) to 50 months compared to 35 months in patients who received ECF/epirubicin–cisplatin–capecitabine (ECX) [7]. Those trials established the benefit of pre-operative chemotherapy in patients with locally advanced gastric cancer. However, given the heterogeneity of gastric cancer and the variable response to preoperative therapies, it is crucial to accurately identify those patients who respond to neoadjuvant chemotherapy and thus benefit from it, and those patients who do not respond, allowing for reassessment of their treatment options.
3. Gastric Cancer Staging and Tumor Response Grade
The 8th edition of the AJCC cancer staging manual, published in 2018, introduced an updated staging system for gastric cancer [8]. Due to the lack of a validated clinical staging system (cTNM) for gastric cancer in prior editions, the pathologic staging system (pTNM) was used instead by treating physicians in the pre-surgical setting without complete surgical pathology information. However, this created confusion and lacked accurate prognostication. The new AJCC staging system filled this gap by introducing a clinical staging system [9]. Additionally, a new post-neoadjuvant TNM system was introduced (labeled as ypTNM) which takes into consideration the use of neoadjuvant therapies and pathologic response. Stage is based on identification of the deepest focus of residual viable cancer cells within the gastric wall for ypT-stage, and the presence of malignant cells in regional lymph nodes for the ypN-stage. Kim et al. analyzed approximately 9000 patients with clinical stage 1-4 gastric cancer who underwent neoadjuvant therapy followed by resection. In their study, post-neoadjuvant stage (ypStage) was able to more accurately predict survival compared to clinical staging. Patients who were downstaged post-operatively had a statistically significant improvement in OS. For example, patients with clinical stage 3 disease who were downstaged to pathologic stage 1 or 2 had 5-year OS rates of 54.6% and 33.1% compared to 19.1% if stage remained the same [10].
According to the 6th edition of the Japanese Gastric Cancer Treatment Guidelines published in July 2021, tumor response to chemotherapy should be evaluated by the Japanese Classification of Gastric Carcinoma or the Response Evaluation Criteria in Solid Tumors (RECIST) [11]. RECIST 1.1 has become the gold standard for the assessment of treatment response in solid tumors [12]. It provides a set of rules and radiographic criteria that need to be met in order to characterize response to treatment as complete response, partial response, progressive disease, and stable disease. Another way to assess tumor response to treatment is by assessing tumor response grade (TRG). Tumor response grade or tumor regression score, defined as a measurable histologic response of tumor cells to neoadjuvant therapy, has been used a prognostic marker in several malignancies, including breast [13], pancreatic [14], and colorectal carcinoma [15, 16]. Complete response, or 100% treatment response, refers to a lack of viable tumor cells and the presence of fibrosis or fibroinflammation within the lesion. No response, or 0% treatment response, indicates a lack of any type of evident treatment effect. Incomplete response refers to the presence of residual cancer cells along with some degree of treatment effect [17]. While RECIST can provide valuable information in the pre-operative setting, TRG can only be measured in the post-operative setting, as it requires histopathologic examination of the resected surgical specimen.
4. Tumor Response Grading Systems
TRG is a histopathological grading system that evaluates the degree of response of tumor cells to preoperative therapy. Many different grading systems have been developed to document TRG, such as those by Becker et al. [18], Mandard et al. [19], Ryan et al. [20] and Japanese Gastric Cancer Association (JGCA) [11, 21] (table 1). Each TRG uses a different scaling system and interpretation guidelines, rendering difficult the direct comparison of results between different systems.
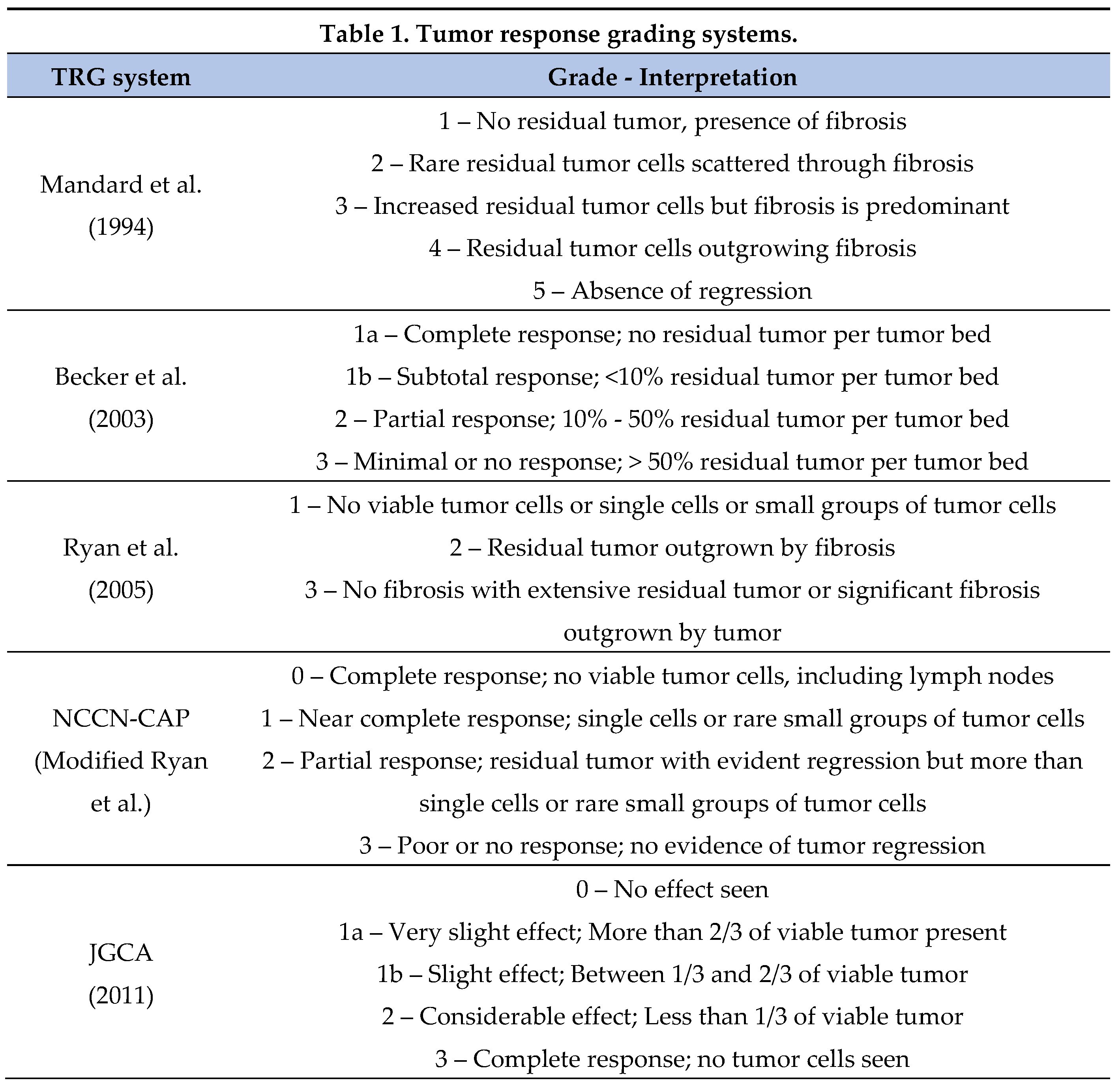
Assessing TRG can be challenging, and it can produce variable results between pathologists. The National Comprehensive Cancer Network (NCCN) recommends using the grading system currently used by the College of American Pathologists (CAP), a modification of the system developed by Ryan et al. [3, 20, 22]. The modification made to the Ryan et al. system is defining two separate grades for complete (no residual tumor) and near complete response (single cells or rare small groups of tumor cells) as TRG 0 and TRG 1 respectively. NCCN additionally specifies that TRG 0 is reserved for patients with complete response of the primary tumor, including lymph nodes. [3] The CAP Protocol for reporting gastric carcinomas suggests use of this modified system (Table 1, Figure 1), given its good interobserver reproducibility. However, use of other systems for assessment of treatment response, including estimation of response as the percentage of the gross lesion comprised of viable tumor cells in relation to fibrosis, is not precluded by the Protocol [3, 20, 22, 23].
A study assessing interobserver reproducibility of different TRG systems, measured the kappa (κ) statistic (with higher κ score indicating higher reproducibility), and found that the TRG systems by Mandard, Becker and JGCA have κ scores of 0.44, 0.52 and 0.28 respectively[24]. Ryan et al. compared a 3-point and 5-point TRG system in 60 patients with locally advanced rectal cancer who underwent neoadjuvant therapy and calculated κ scores of 0.84 and 0.64 respectively [20]. As TRG can only be evaluated only after surgical resection, its role in clinical practice remains ambiguous.
5. Tumor Response Grade Prognostication
Several studies have demonstrated an association of TRG with OS. In 1999, Lowy et al. published the results of 3 randomized controlled trials that investigated neoadjuvant treatment of patients with gastric cancer. In their study, they analyzed 83 patients with >T2, M0 gastric cancer who received preoperative chemotherapy followed by resection. Sixty-one patients underwent R0 resection, with 16 of them having pathologic response; 3 patients had complete histologic response, 10 had partial response (defined as <10% of viable tumor cells) and 3 with minor response (10-50% viable tumor cells). In their multivariate analysis, tumor response to chemotherapy was the only factor associated with overall survival, with a relative risk of 0.44 [25]. In a study published by Becker et al. in 2003, 36 patients with locally advanced gastric cancer (LAGC) received neoadjuvant etoposide, doxorubicin and cisplatin followed by resection. No patients had complete histologic response to therapy. Only four patients had <10% of residual disease, whereas 23 patients had >50% residual tumor. Univariate analysis demonstrated a statistically significant association of tumor regression with survival [18]. In another study published in 2011, the investigators evaluated TRG scores in 480 patients with LAGC who received neoadjuvant platinum-based chemotherapy. The study showed 21.2% of patients had complete (3.3%) or subtotal tumor regression (defined as <10% residual cancer, 17.9%), whereas 25.2% had partial tumor regression (10-50% residual cancer). Multivariate analysis revealed that tumor regression and post-operative lymph node status were factors associated with survival. Patients with complete/subtotal tumor regression had a mean survival of 128.6 months versus 61.9 months for partial tumor regression [26]. In another study by Xie et al. published in 2021, 249 patients with >T2 and/or N1 disease underwent oxaliplatin-based (69%) or non-oxaliplatin-based neoadjuvant therapy. Using the CAP TRG system, patients with TRG 0-1 had 3-year and 5-year survival rates of 85.2% and 74.5% respectively, compared to 56.1% and 44.1% in patients with TRG of 2. Patients with TRG 3 had significantly worse survival rates with 3-year and 5-year rates of 28.2% and 23.0% respectively. Multivariate analysis showed that TRG and margin status were factors associated with survival whereas TRG was the only factor associated with recurrence-free survival [27]. Sinnamon et al. evaluated 117 patients with clinical T2+ and/or N+ gastric cancer who underwent preoperative chemotherapy followed by resection. Amongst the most commonly used chemotherapy regimens, forty-one percent of patients received ECF/ECX, 26% received folinic acid, fluorouracil and oxaliplatin (FOLFOX), and 11.1% received FLOT. Using the CAP TRG, the majority of patients were found to have no response to treatment (TRG 3, 58%). TRG 1 and TRG 2 were found in 15% and 21% respectively, whereas complete response (TRG 0) was only found in 5.1% of the cohort. Increasing TRG score showed a statistically significant association with OS (HR 1.49, p = 0.026). Specifically, patients with TRG 0, 1, 2 and 3 had survival rates of 86.9, 74.5, 51.5 and 27 months respectively. No association between TRG and choice of chemotherapeutic regimen was observed. Post-therapy pathologic lymph node status was also associated with survival (HR 1.93, p = 0.026) [28]. This improvement in survival highlights the impact of tumor response to neoadjuvant therapy among “responders” and “non responders”.
While the studies above show an association of TRG with OS, other studies challenge this. In 2007, Mansour et al. analyzed the histologic response of 168 patients with gastric adenocarcinoma who underwent neoadjuvant chemotherapy followed by resection. Even though the chemotherapeutic regimens varied among the cohort, the majority of patients (68%) received cisplatin-based chemotherapy. Eighteen patients (11%) had no evidence of histologic response and only 2 patients had complete response. The majority of patients had <20% histologic response, and 23% had a response >50%. In univariate analysis, histologic response >50% was associated with 3-year disease-specific survival of 69% versus 44% in patients with <50% response. In multivariate analysis, however, lymph node involvement and perineural or vascular invasion were found to be associated with disease-specific survival, but the effect of histologic response (scored as above or below 50%) was not significant. Of note, Cisplatin-based chemotherapy regimens were 3-times more likely to produce histologic response >50% [23]. In 2016, Smyth et al. evaluated the association of TRG and OS in patients who were enrolled in the MAGIC trial. Univariate analysis demonstrated an association between TRG scores and lymph node involvement on OS. However, multivariate analysis showed that lymph node involvement, and not tumor regression, was predictive of survival [5, 29].
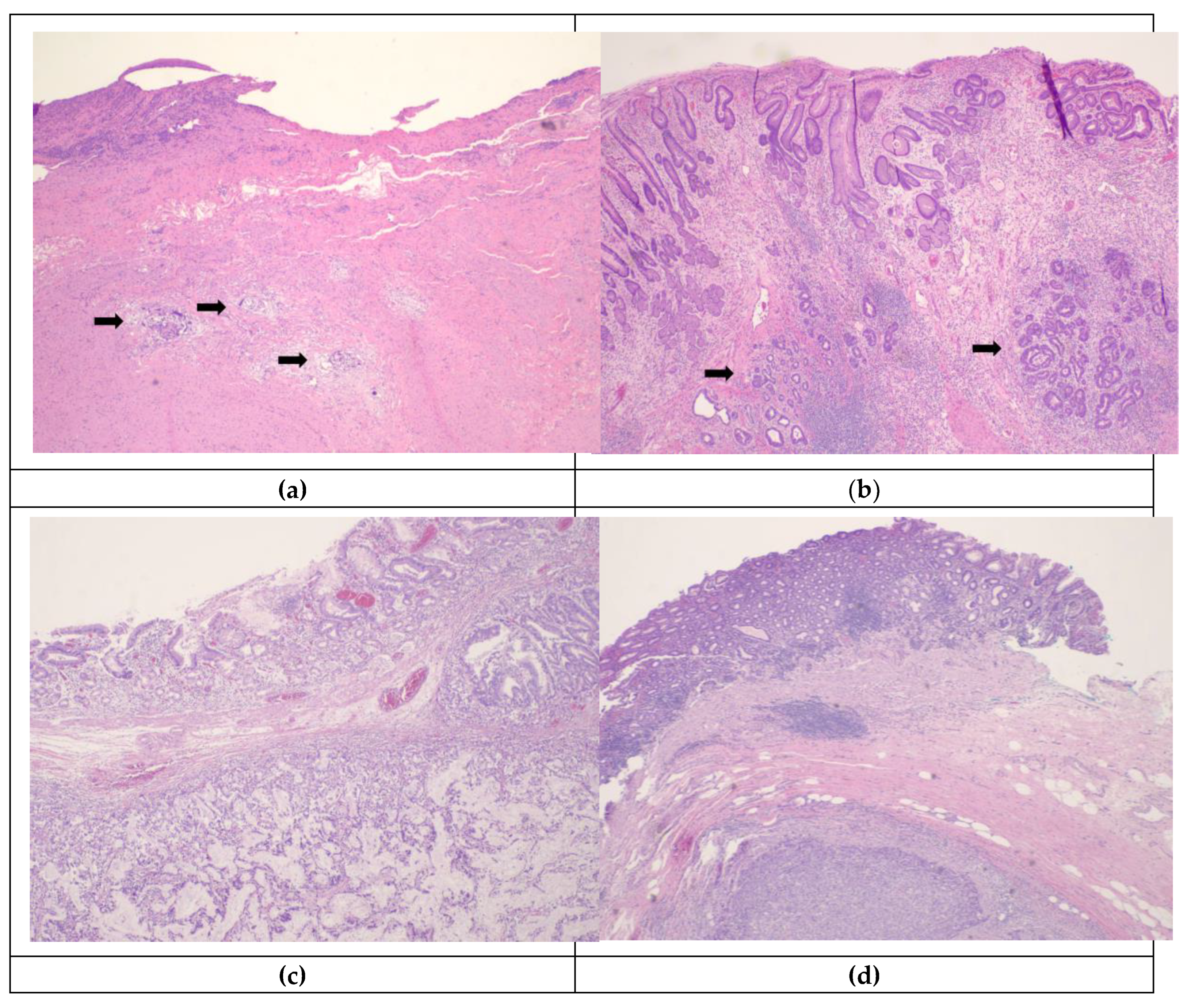
Figure 1.
Histologic Tumor Regression Grades assigned using schema in the CAP Protocol: (a) Rare small groups of carcinoma cells (→) are present within a fibrotic tumor bed in an esophagogastrectomy specimen, corresponding to TRG 1; (b) residual foci of adenocarcinoma ( →) persist in a gastrectomy that showed evident treatment effect in the form of ulcer, necrosis, inflammation, and calcifications, consistent with TRG 2; (c),(d) extensive residual tumor is readily apparent, with no evidence of tumor regression, corresponding to TRG 3.
Figure 1.
Histologic Tumor Regression Grades assigned using schema in the CAP Protocol: (a) Rare small groups of carcinoma cells (→) are present within a fibrotic tumor bed in an esophagogastrectomy specimen, corresponding to TRG 1; (b) residual foci of adenocarcinoma ( →) persist in a gastrectomy that showed evident treatment effect in the form of ulcer, necrosis, inflammation, and calcifications, consistent with TRG 2; (c),(d) extensive residual tumor is readily apparent, with no evidence of tumor regression, corresponding to TRG 3.
6. Radiographic and Endoscopic Response to Chemotherapy and Prognostication
As mentioned earlier, response of solid tumors to chemotherapy can be evaluated in the preoperative setting according to RECIST 1.1 criteria, by measuring the size of a “measurable” lesion. Gastric cancer patients with radiographic response to neoadjuvant therapy have been shown to have improved disease-free and OS compared to non-responders [30, 31]. However, the location and volume of a gastric malignancy cannot be reliably and consistently identified and measured on computed tomography, rendering the use of RECIST criteria for primary gastric lesions challenging. For this reason, alternate measurable lesions are pursued (lymph nodes, liver metastasis) [12]. Additionally, radiographic assessment can underestimate tumor response to chemotherapy, as it cannot distinguish chemotherapy-induced inflammatory response and fibrosis from remaining tumor [30]. Chemotherapy-related changes result in distortion of the layers of the gastric wall, which in turn causes evaluation of tumor response with endoscopic ultrasound (EUS) to correlate poorly with histologic response seen on surgical specimens [32]. In 1999, Ajani et al. evaluated the accuracy of presurgical EUS and laparoscopy staging in patients with LAGC. In their study, 13 patients with LAGC underwent staging with EUS after completion of neoadjuvant therapy and before surgical intervention. EUS was able to accurately predict pathologic staging in only 3 out of 13 patients (13%), whereas 8 patients were understaged [33]. In another study, 40 patients with LAGC received neoadjuvant therapy and were restaged with EUS and CT before undergoing gastrectomy. EUS was found to be 47% and 39% accurate in correctly determining the pathologic T and N stage respectively, whereas computed tomography was 57% and 37% accurate. EUS downstaging of T and/or N status was significantly associated with OS (HR 0.12 ,95% CI 0.01-0.91 p=0.04), whereas CT downstaging did not reach statistical significance [34].
7. Future Directions
Undoubtedly, response to preoperative chemotherapy is associated with a favorable tumor biology and indicates tumor chemosensitivity. Conversely, nonresponse to chemotherapy points to a biologically aggressive and chemotherapy resistant tumor. Correctly identifying the group of patients in whom chemotherapy does not have an effect in the neoadjuvant setting will allow for potential alteration of the chemotherapeutic regimen and provide a “second chance” for disease control and ultimately, cure. Randomized controlled trials are needed to better understand the value of radiographic and histologic assessment of tumor response in prognostication and disease management. Future studies will need to focus on identifying the ideal preoperative methods and biomarkers that can accurately predict and assess tumor response. Additionally, while many TRG systems solely assess response of the primary tumor to neoadjuvant therapies, tumor response of metastatic lymph nodes will also need to be investigated further as a possible prognostic factor. A widely accepted post-treatment histologic grading system is needed, as it can be a valuable tool in comparing study results and treatment responses in the future. Advances in radiomics and genomics will improve clinical decision making in gastric cancer treatment and advance patient care.
8. Conclusions
There is evidence that tumor response grade following neoadjuvant therapy for gastric cancer is associated with survival. Although multiple grading systems exist, there is need for a single, unified, and widely accepted grading system that would allow for direct comparison of TRG results between studies. This would allow clinicians to provide complete counseling and supply their patients with more accurate prognostication.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jacques Ferlay, M.C., Isabelle Soerjomataram, Donald M. Parkin, Marion Piñeros, Ariana Znaor, Freddie Bray. Global Cancer Observatory: Cancer Today. Lyon: International Agency for Research on Cancer. 2020 [cited 2023 February 23]; Available from: https://gco.iarc.fr/today/home.
- Ramos-Santillan, V., et al., The order of surgery and chemotherapy matters: Multimodality therapy and stage-specific differences in survival in gastric cancer. J Surg Oncol, 2023. 127(1): p. 56-65. [CrossRef]
- National Comprehensive Cancer Network.. Gastric Cancer (Version 1.2023). 2023 April 11, 2023]; Available from: https://www.nccn.org/professionals/physician_gls/pdf/gastric.pdf.
- Petrillo, A. and E.C. Smyth, Multimodality treatment for localized gastric cancer: state of the art and new insights. Curr Opin Oncol, 2020. 32(4): p. 347-355. [CrossRef]
- Cunningham, D., et al., Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med, 2006. 355(1): p. 11-20. [CrossRef]
- Ychou, M., et al., Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol, 2011. 29(13): p. 1715-21. [CrossRef]
- Al-Batran, S.E., et al., Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet, 2019. 393(10184): p. 1948-1957. [CrossRef]
- Ajani JA, In H., Sano T, Gaspar LE, Erasmus JJ, Tang LH, Washington MK, Gerdes H, Wittekind CW, Mansfield PF, Rimmer C, Hofetetter WL, Kelson D. Stomach. In: Amin, M.B., Edge, S.B., Greene, F.L., et al. (Eds.) AJCC Cancer Staging Manual. 8th Ed. New York: Springer; 2017: 203-220.
- In, H., et al., The newly proposed clinical and post-neoadjuvant treatment staging classifications for gastric adenocarcinoma for the American Joint Committee on Cancer (AJCC) staging. Gastric Cancer, 2018. 21(1): p. 1-9. [CrossRef]
- Kim, G., et al., Providing Reliable Prognosis to Patients with Gastric Cancer in the Era of Neoadjuvant Therapies: Comparison of AJCC Staging Schemata. J Gastric Cancer, 2020. 20(4): p. 385-394. [CrossRef]
- Japanese Gastric Cancer, A., Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition). Gastric Cancer, 2023. 26(1): p. 1-25.
- Eisenhauer, E.A., et al., New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer, 2009. 45(2): p. 228-47. [CrossRef]
- Chung, Y.R., et al., Prognostic implications of regression of metastatic axillary lymph nodes after neoadjuvant chemotherapy in patients with breast cancer. Sci Rep, 2021. 11(1): p. 12128. [CrossRef]
- Ahn, S., et al., Four-Tier Pathologic Tumor Regression Grading System Predicts the Clinical Outcome in Patients Who Undergo Surgical Resection for Locally Advanced Pancreatic Cancer after Neoadjuvant Chemotherapy. Gut Liver, 2022. 16(1): p. 129-137. [CrossRef]
- Peng, Y.F., et al., Tumor regression grades: potential outcome predictor of locally advanced rectal adenocarcinoma after preoperative radiotherapy. World J Gastroenterol, 2015. 21(6): p. 1851-6. [CrossRef]
- Li, J.Y., et al., Survival landscape of different tumor regression grades and pathologic complete response in rectal cancer after neoadjuvant therapy based on reconstructed individual patient data. BMC Cancer, 2021. 21(1): p. 1214. [CrossRef]
- Amin MB, E.S., Greene F, Byrd DR, Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR, et al. (Eds.), AJCC Cancer Staging Manual. 8th ed. 2017: Springer International Publishing: American Joint Commission on Cancer.
- Becker, K., et al., Histomorphology and grading of regression in gastric carcinoma treated with neoadjuvant chemotherapy. Cancer, 2003. 98(7): p. 1521-30. [CrossRef]
- Mandard, A.M., et al., Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer, 1994. 73(11): p. 2680-6. [CrossRef]
- Ryan, R., et al., Pathological response following long-course neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Histopathology, 2005. 47(2): p. 141-6. [CrossRef]
- Japanese Gastric Cancer, A., Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer, 2011. 14(2): p. 101-12. [CrossRef]
- Lawrence J. Burgart, M.W.V.C., MD*; Dhanpat Jain, MD Protocol for the Examination of Specimens From Patients With Carcinoma of the Stomach. 2022.
- Mansour, J.C., et al., Does graded histologic response after neoadjuvant chemotherapy predict survival for completely resected gastric cancer? Ann Surg Oncol, 2007. 14(12): p. 3412-8. [CrossRef]
- West, C.M., A. Naveed A. Hayes S. Formela L. Welch I. West C. M. Pritchard S., Assessment of Histopathological Response in Gastric and Gastro-Oesophageal Junction Adenocarcinoma following Neoadjuvant Chemotherapy: Which Scoring System to Use? Pathology. Pathology, 2012.
- Lowy, A.M., et al., Response to neoadjuvant chemotherapy best predicts survival after curative resection of gastric cancer. Ann Surg, 1999. 229(3): p. 303-8. [CrossRef]
- Becker, K., et al., Significance of histopathological tumor regression after neoadjuvant chemotherapy in gastric adenocarcinomas: a summary of 480 cases. Ann Surg, 2011. 253(5): p. 934-9. [CrossRef]
- Xie, J.W., et al., Prognostic Value of Tumor Regression Grading in Patients Treated With Neoadjuvant Chemotherapy Plus Surgery for Gastric Cancer. Front Oncol, 2021. 11: p. 587856. [CrossRef]
- Sinnamon, A.J., et al., Tumor Regression Grade and Overall Survival following Gastrectomy with Preoperative Therapy for Gastric Cancer. Ann Surg Oncol, 2023. 30(6): p. 3580-3589. [CrossRef]
- Smyth, E.C., et al., Effect of Pathologic Tumor Response and Nodal Status on Survival in the Medical Research Council Adjuvant Gastric Infusional Chemotherapy Trial. J Clin Oncol, 2016. 34(23): p. 2721-7. [CrossRef]
- Achilli, P., et al., Tumor response evaluation after neoadjuvant chemotherapy in locally advanced gastric adenocarcinoma: a prospective, multi-center cohort study. J Gastrointest Oncol, 2017. 8(6): p. 1018-1025. [CrossRef]
- Ott, K., et al., Neoadjuvant chemotherapy with cisplatin, 5-FU, and leucovorin (PLF) in locally advanced gastric cancer: a prospective phase II study. Gastric Cancer, 2003. 6(3): p. 159-67. [CrossRef]
- Kelsen, D., et al., Neoadjuvant therapy of high-risk gastric cancer: a phase II trial of preoperative FAMTX and postoperative intraperitoneal fluorouracil-cisplatin plus intravenous fluorouracil. J Clin Oncol, 1996. 14(6): p. 1818-28. [CrossRef]
- Ajani, J.A., et al., Enhanced staging and all chemotherapy preoperatively in patients with potentially resectable gastric carcinoma. J Clin Oncol, 1999. 17(8): p. 2403-11. [CrossRef]
- Park, S.R., et al., Endoscopic ultrasound and computed tomography in restaging and predicting prognosis after neoadjuvant chemotherapy in patients with locally advanced gastric cancer. Cancer, 2008. 112(11): p. 2368-76. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



