Submitted:
21 June 2023
Posted:
22 June 2023
You are already at the latest version
Abstract
Hemianopia poses significant challenges and requires effective rehabilitation strategies. Traditional visual restoration methods have focused on low-level vision therapies in controlled environments. This paper proposes the integration of natural and ecologically valid environments, e.g., virtual reality (VR), three-dimensional (3D) settings, and cognitive interactions for visual rehabilitation. We review various studies that employed common practices in laboratory or controlled settings. We also discuss the disadvantages of traditional techniques and advocate for a comprehensive and ecological framework in visual rehabilitation. Instead of correcting visual inputs, we emphasize training the visual system to adapt and restore functionality in real-world contexts. By combining real-world environments and higher-level vision approaches, we can enhance visual recovery, improve daily functioning, and restore the quality of life for individuals with visual field defects. Moreover, we stress the importance of incorporating natural environments, VR, 3D settings, and cognitive interactions to maximize the effectiveness of visual rehabilitation and empower patients to regain their visual abilities in real-world scenarios. Continued research and development in this field are crucial to refine and expand the application of these innovative techniques, ultimately enhancing the lives of individuals affected by visual field defects.
Keywords:
Hemianopia
; Real-world conditions
; Visual rehabilitation
; Visual field defects
1. Introduction
Human beings are well-known as visual animals. Our visual system, which is a complex and extraordinary computational system, supports many of our impressions, understanding, and behavior [1]. It allows us to recognize, distinguish, and adjust our movements and behavior. Vision is not a spontaneous framework of neural coding and responses; instead, it relies on earlier learned rules about the structure of the environment around us, making our visual experience complex and unique [2]. The vital role of our visual system in our lives becomes apparent through the vast amount of information it provides about the world. It enables us to recognize objects, faces, shapes, patterns, and spatial awareness, including finding addresses. Moreover, vision contributes to learning and education, emotional processing by providing emotional stimuli, and ultimately, our survival, emphasizing its critical importance to us.
The significance of vision in our lives can be attributed to its "informativeness." When processing stimuli from different sensory channels, individuals rely on the most precise or accurate modality for the task they are engaged in or preparing for [3,4,5].To illustrate this, let us consider the situation of crossing the street. While one could focus solely on hearing and paying attention to the sound of approaching cars, the preferred and trusted method is inspecting the surroundings by looking left and right. This reliance on vision is due to its perceived precision and accuracy, as it provides a more reliable assessment of the presence or absence of cars. Therefore, individuals turn their heads to visually confirm the absence of approaching vehicles before crossing the street [6,7].
With a single gaze, we can take in an enormous amount of information, and our foveal acuity allows us to focus on intricate details of what we perceive. Additionally, vision enables us to calibrate and coordinate movements in space, such as locomotion and hand gestures, owing to its superior spatial resolution compared to other senses. Spatial cognition and object identification are primarily facilitated by vision, making it the primary sensory modality in these processes [4,8,9]
The dominance of vision can also be attributed to the potential "weakness" of the visual system. Posner et al. (1976) hypothesized that humans have a strong tendency to actively attend to visual events to compensate for the relatively poor alerting properties of the visual system compared to the auditory or tactile systems[10]. This hypothesis suggests that under conditions of high arousal, both animals and humans are more likely to switch their attention toward the auditory modality to react more rapidly to potential threats [10,11]
However, the visual system is susceptible to damage, deficits, and disorders. This section will explore the visual field and its defects, specifically visual field defects (VFDs). It will involve describing the anatomy of the visual system and discussing VFDs, which refer to the condition where vision is lost in specific visual field sectors.
Starting from when reflections, object signals, or light enter our eyes, the optic nerves extend to the optic chiasm, a midline cross-point. Through the help of the temporal hemiretina, the optic tract processes input data to higher levels, leading to meaningful and interpretable information. Each eye receives and processes half of the visual field (hemifield). The nasal hemiretina ensures the processing of information from both hemifields, projecting it to the visual cortex of the contralateral hemisphere [12]. Figure 1 shows how the two eyes collectively produce the entire visual field.
Indeed, each hemifield spans from peripheral points to the central field, resulting in two equal regions where both eyes contribute to viewing each hemifield. Combining the nasal retina from one eye and the temporal retina from the other eye collaboratively presents the entire visual field. Figure 2 provides a simplified representation of this process, visually depicting how the input from each eye converges to form a unified visual field.
Visual deficits can arise from various factors, including underlying medical conditions, injuries, or age-related changes. Common visual deficits include myopia (nearsightedness) [13], hyperopia (farsightedness) [14], presbyopia (age-related difficulty in focusing on close objects) [15], astigmatism (distorted vision due to irregularly shaped cornea) [14], and color vision deficiencies, such as red-green color blindness [16], and hemianopia [5]. Due to the specific anatomy of the visual system, lesions occurring at different locations along the visual pathway led to distinct consequences in visual processing. Therefore, understanding the topography of these lesions and their effects is crucial.
Figure 3 illustrates different sites within the visual system and the corresponding cases of hemianopia. It demonstrates that deficits presented in both eyes can either be entirely monocular or affect different parts of the visual field in each eye.
A typical deficit that involves the loss of vision is hemianopia, which refers to the loss of vision in half of the visual field, either on the left or right side. Hemianopia typically occurs due to damage to the visual pathways in the brain, often caused by strokes, traumatic brain injuries, or tumors[3,5]. When the primary visual cortex or optic radiation is affected, it disrupts the transmission of visual information from the eyes to the brain, resulting in the loss of vision in one-half of the visual field. In this case, this visual defect is called homonymous hemianopia (HH) [17].
Between 52% and 70% of hemianopia patients experience severe neuropsychological and psychological consequences, including cognitive deficits, memory loss, academic performance deficits, neglect, disturbances in daily life, and attention deficits [18]. The functional impairment caused by hemianopia poses a constant challenge in healthcare research due to its multifaceted effects on daily activities and social connectedness. One significant consequence of limited visual acuity resulting from reduced visual fields caused by hemianopia is decreased quality-of-life outcomes [19]. In addition to restricted social engagement opportunities, independent driving becomes nearly impossible due to compromised peripheral visual functions, a common issue among these patients. Moreover, providing adequate care for individuals with this condition presents significant challenges for caregivers and close relatives.
Vision loss and visual deficits have always been intriguing topics in rehabilitation science. Researchers from various disciplines, including neuroscience, neuropsychology, neurology, and engineering, are interested in finding new rehabilitative approaches to improve visual deficits. After a brain injury, individuals with visual field disorders constitute one of the largest groups who suffer from the consequences [1,20]. Although it is evident that after clinical situations such as traumatic brain injuries, one cannot always fully recover from the pre-injury visual state [21], scientists have persistently taken on the challenge of attempting the seemingly impossible. Stroke-induced hemianopia, for instance, is believed to resolve spontaneously over time, but after six months, the deficits are considered permanent [22]; medication may assist in restoring sight in tumors-related cases, though patients with hemianopia often experience permanent vision loss.
Recent scientific advancements and research on mammals and humans have shed new light on the subject [22,23,24,25,26]. Compelling evidence for plasticity within the primary visual cortex indicates the potential for visual improvements following a period of visual deprivation. Additionally, studies have demonstrated that repeated sensory practice stimulates long-term perceptual learning [27], utilizing experience-dependent plasticity. Consequently, the theory of using training methods to improve visual impairments has gained wide acceptance, leading to further research.
The visual field constraint of hemianopia has recently garnered significant attention in extensive research, particularly regarding treatment options for affected patients. However, despite these findings and their implications for patient care, access to visual rehabilitation services through primary healthcare providers remains limited [8,22,25].
Rehabilitation for hemianopia is a complex and sometimes challenging process. Before discussing the available treatments, it is important to define and discuss key aspects of rehabilitation in cases of visual field loss. Rehabilitation [28] is a process aimed at helping individuals with injuries achieve a better or optimal level of physical, social, and practical functioning related to their specific problem. The primary goal of rehabilitation is to reduce the impairment experienced by affected individuals. In the context of vision, rehabilitation involves attempting to modify the mechanisms and functions of the brain and visual system through systematic experiments and practices to restore some or all lost visual functionality [28].
Among the possible rehabilitative approaches for patients with visual field loss and hemianopia, neurological rehabilitation encompasses various forms, such as prism glasses [29] and surgical methods, which are beyond the scope of this review. On the other hand, neuropsychological rehabilitation has gained considerable interest in recent years and has seen significant growth. The success of psychological approaches in rehabilitating language [30], memory [31], and attention [32] have prompted researchers to explore applying these methods to patients with vision loss. While there are many intriguing results from rehabilitation studies, there are still numerous questions and areas of uncertainty that need to be addressed by scientists to improve the quality of life for patients and potentially restore vision.
As mentioned earlier, brain plasticity plays a crucial role in vision research [33], as the human brain is a complex and adaptable organ capable of rewiring and adjusting its connections to maximize survival and functionality. Restitutive approaches and compensatory approaches are two popular approaches in the field of vision rehabilitation [34]. Restitutive approaches aim to improve or restore visual function through targeted exercises, activities, or interventions. These include vision therapy, sensory substitution devices, low vision rehabilitation, and perceptual training [8,34,35]. Vision therapy, also known as orthoptics or vision training, involves a series of eye exercises and activities to enhance specific visual skills [36]. Sensory substitution devices utilize technology to substitute impaired or missing sensory inputs with alternative sensory information [37]. Low vision rehabilitation focuses on maximizing remaining vision through aids and strategies [38]. Perceptual training aims to improve visual processing and interpretation skills through exercises targeting specific aspects of visual perception [39].
While these restitutive approaches have their merits, they often do not directly address brain reorganization or the establishment of new connections. They may only be suitable for some due to their cost and availability. In contrast, compensatory approaches meet these criteria; therefore, when restitutive approaches are not available, compensatory approaches are recommended. Compensatory approaches can also be helpful when used in combination with restorative training. Along with expanding the visual field, these approaches can enhance visual exploration within the blind field. By optimizing eye movements and attentional strategies, compensatory techniques can help individuals improve their ability to navigate and perceive objects in the blind field [34,40,41,42].
To understand the effectiveness of various practices for patients with hemianopia, a review of scientific literature from 2000 to 2023 was conducted. The search focused on major scientific databases, employing selection criteria to ensure the relevance and quality of the studies included in the review. The primary interest was in psychophysical interventions such as visual search, audio training, visual training, and eye-movement training while excluding clinical approaches like lenses or brain stimulation techniques.
2. Method
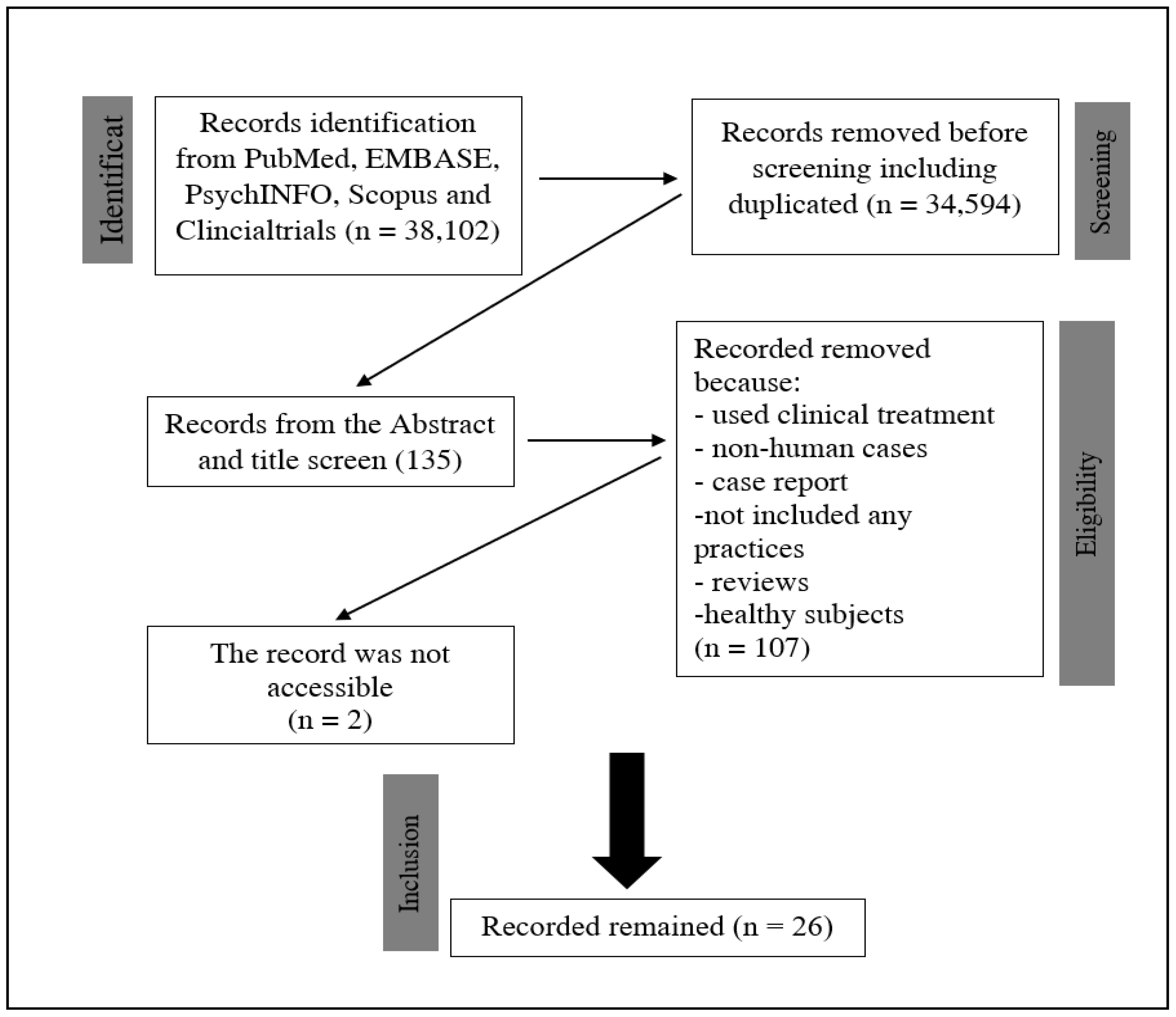
Following a comprehensive search and selection procedure, a total of 26 papers that met our predefined criteria were identified. Our search encompassed studies focusing on hemianopia and its treatments, utilizing databases such as PubMed, EMBASE, PsychINFO, Scopus, and Clinical trials. The PRISMA protocol was followed throughout to ensure transparency and rigor. The findings from our research endeavor are depicted in Figure 4, providing a visual representation of the outcomes obtained.
These studies have explored various interventions targeting individuals with hemianopia, yielding valuable insights into their efficacy—the comprehensive review and profound understanding of the current landscape of non-clinical interventions for hemianopia.
3. Results
Julkunen et al. [43] and Bolognini et al. [44] employed computer-based designs and sensory stimulations as training techniques. Their findings demonstrated notable improvements in static and kinetic perimetry, with significant differences between baseline and training sessions. Additionally, Bolognini et al. reported significant post hoc comparisons. Building upon these studies, Poggel et al. [35] implemented Visual Restoration Training (VRT), observing an expansion in the visual field size accompanied by enhancements in certain cognitive factors. Similarly, Leo et al. [45] conducted experiments involving visual and auditory stimulation, leading to reduced localization error and superior improvements in the blind field compared to the intact hemifield.
Incorporating Visual Control Training followed by audio-Visual Training, Passamonti et al. [46] discovered a substantial increase in visual detection and perceptual sensitivity in one of the cases relative to the others. They also noted improved accuracy in the triangle test among subjects and advancements in visual exploration and reading capabilities. Simultaneously, Nelles et al. [47] integrated eye movement training with physical and occupational therapies, although they reported a stable visual field defect with no discernible differences in the size of visual field defects following the training. Keller and Lefin-Rank [48] engaged patients in audio-visual exploration and separate audio-visual or visual stimulation training. Their results indicated significant improvements in detected targets, reading time, search time, saccade amplitude, and daily activities. Patients exhibited a 46% increase in the detection rate of target stimuli, with the audio-visual group demonstrating greater overall improvement across all outcome variables.
Continuing the trajectory, Hayes et al. [49] and Lewald et al. [50] conducted studies utilizing NVT vision rehabilitation and audio-visual training, respectively. Hayes et al. observed improvements in target missing and quality of life, while no significant change in the visual field was noted. Conversely, Lewald et al. found an increase in visual detection and hemifield alongside visual space compression on the intact side compared to the anodic side. Bahnemann et al. [51] employed a fixed-base driving simulator to assess reaction time and speed in detecting hazardous parameters. They also employed a reading text application under various settings to evaluate and enhance reading abilities. Over time, improvements were observed in patients' reading time and visual field, although no significant change in right hemifield vision was detected.
In subsequent years, Ten Brink et al. [52], Dundon et al. [53], and Tinelli et al. [54]delved into unimodal auditory, visual, and multisensory and cross-modal audio-visual training, respectively. Their results highlighted improvements in saccade performance across the entire visual field, attentional allocation in daily activities, visual exploration in the blind field, and an enhanced quality of life scale. sahraie et al. [55] employed NeuroEyeCoach™ and observed improved reaction times for cancellation tasks, reduced visual search times, and positive scanning outcomes. Similarly, Grasso et al. [56] conducted unisensory and multi-audio-visual sensory training, which led to improved visual search in audio-visual scenarios, enhanced fixation, oculomotor performance, and increased accuracy.
Subsequent works by Tinelli et al. [57], Rowe et al. [58], and Ivanov et al. [59] incorporated a combination of visual and acoustic stimuli, Fresnel prisms, visual search training, and standard care. These studies revealed significant improvements in visual detection rates within the affected hemifield, eye movement enhancement, and improved visual function. Furthermore, improvements in reading abilities, reading speed, visual function, search times, saccade amplitudes, and reduced number of saccades to locate targets were observed.
Additional investigations by Smaakjær et al. [60], Pineda-Ortíz et al. [61], Casco et al. [62], and Svaerke et al. [63] encompassed open-label examinations utilizing vision therapies, Visual Neurorehabilitation Therapy (NRT), and computer-based cognitive rehabilitation (CBCR). These studies demonstrated significant improvements in visual performance, enlargement of the visual field, ocular movements, reading abilities, and visuospatial symptoms post-stroke.
Three non-mutually exclusive hypotheses have been proposed regarding the expansion of the visual field in individuals with posterior cortical brain lesions. The first hypothesis suggests that neurons near the lesion can increase or shift their receptive fields to respond to stimuli in the transition zone. The second hypothesis postulates that islands of spared neurons within the damaged visual cortex can reorganize their connectivity, augmenting their response strength. Lastly, the third hypothesis proposes that residual vision can be achieved through alternative pathways directly projecting to higher visual areas, such as the lateral geniculate nucleus to the middle temporal area.
For a comprehensive overview of the studies mentioned above, refer to Table 1, which provides detailed information.
| # | Ref | Y | number of patients | subject description | Technique | Parameters | Environment | Outcome/s |
| 1 | [64] | 2003 | 5 patients | chronic stroke patients | computer-based design | not mentioned | static and kinetic perimetry improvement | |
| 2 | [2] | 2005 | 8 patients | PT's with chronic visual field defects participated in the study | sensory stimulations were used | three stimuli were presented: unimodal visual, unimodal auditory, and crossmodally visuo-auditory.presenting a visual target in different spatial positions within 120 trials and some targets without visual stimulihemianopia hemifield was more intensively stimulated than the intact hemifield | Laboratory setting | the difference between the baseline and each training session was significantSignificant post-hoc comparisons were reported |
| 3 | [65] | 2008 | 19 patients | subjects with damage to the retina or optic nerve disorders | VRT | not mentioned | visual field size is increased; also some cognitive factors were improvedvisual field size increased, | |
| 4 | [45] | 2008 | 12 patients | hemianopia with more than 2 months after diagnosis or incident | visual and auditory stimulation, unimodal auditory condition, unimodal visual catch-trial, and cross-modal condition | Laboratory setting | decrease localization error, improvement in the blind field was better than intact hemifield, | |
| 5 | [66] | 2009 | 12 patients and 12 control subjects | patients with chronic visual field deficits due to a postchiasmatic lesion | Control Visual Training and, subsequently, Audio-Visual Training. | Audio-Visual Training comprised systematic audio-visual stimulation of the intact and affected visual fields for 4 h daily over 2 weeks | Laboratory setting | Visual detection and perceptual sensitivity significantly increased in one of the cases compared to the other.The accuracy significantly improved in the triangle test between subjects. Compared to S1, the daily life activities were significantly reduced. A significant reduction in the length of the scan bathimprovement in ocular exploration characterized by fewer fixations and refixations, quicker and larger saccades, and reduced scan path lengthReading was improved |
| 6 | [67] | 2009 | 8 as the main and 12 control group | All patients had complete or nearly complete hemianopia | eye movement training and physical and occupational therapies | two daily training sessions of 30 min each for a total of 4 weeksAll patients also received 90 min daily of complementary physical and occupational therapy to facilitate the transfer of compensatory visual strategies into ADL functions | clinical-lab settings | stable visual field defectNo differences in the size of visual field defects were found after the training. |
| 7 | [68] | 2010 | 20 patients | patients with either left- or right-sided visualfield deficits | audio-visual exploration training | visual and acousticstimuli, 48 red light-emitting diodes (LEDs), and piezoelectricloudspeakers were positioned in 3 rows at different angles, and the same apparatus for visual exploration training | in a dimly illuminated room | significant improvements after audio-visual training for the number of detected targets in the visual exploration test, reading time, search time, amplitude and number of saccades in the EOG, and total score on the questionnaire of activities of daily living.the detection rate of target stimuli improved by about 46% in patients |
| 8 | [69] | 2010 | 20 patients | left or right visual field deficits after a stroke | Patients were randomly assigned to separate groups performing either audio-visual or visual stimulation training (20 sessions, each lasting 30 minutes). | lab settings / clinical environment | compensatory eye movement training, greater improvement for all outcome variables for the audio-visual group | |
| 9 | [70] | 2012 | 13 patients | patients with hemianopia | NVT vision rehabilitation over a 3-month intervention | laboratory setting | Target improvements were missing improvement in their quality of life, but the visual field was not improved significantly. | |
| 10 | [71] | 2012 | 10 patients | chronically 5 months after the first stroke | audio-visual training | controlled environment | increasing visual detection, increasing hemifield in visual detection | |
| 11 | [72] | 2013 | 10 patients and 10 control | chronically 6 months after lesion or diagnosis | audio-visual stimuli, including acoustic stimuli with visual target | controlled environment | visual space is compressed on the intact side compared to the anopic side | |
| 12 | [73] | 2015 | 14 patients | homonymous hemianopia | a fixed-base driving simulator by testing RT and speed while detecting a hazardous parameter | lab with simulator | The low-performance group missed more hazardous objects than the high-performance group, but there were no changes in the HP and control groups. Reaction times in the blind hemifield (patients) and right hemifield (healthy controls) differed significantly between the groups. Healthy controls reacted significantly faster in the right hemifield than either the HP. | |
| 13 | [73] | 2015 | 33 patients | reading text application | using a reading text application in different settings to evaluate their reading and improve it | Home-based training | reading right showed improvement in time. Improvement in the visual field of patients over time.no significant change in right hemifield vision | |
| 14 | [74] | 2015 | 8 patients | at least 26 months after the lesion | unimodal auditory, bimodal coincident spatially and temporally, bimodal disparate | lab settings | saccade improvement in patients in the intact field, | |
| 15 | [75] | 2015 | 8 patients | hemianopia with minimum 3 months after the lesion | visual and multisensory training | controlled environment | daily improvement of attentional allocation and visual exploration in the blind field improves the quality of life scale. | |
| 16 | [76] | 2015 | 3 patients | chronically 1 or more than one year after the lesion | unimodal visual, unimodal auditory, cross-modal audio-visual training | controlled environment | ||
| 17 | [77] | 2016 | 32 patients | either left or right homonymous hemianopia | NeuroEyeCoach™ | lab settings | improvement of time (RT) for cancellation task, decreased time in visual search, positive outcome in scanning | |
| 18 | 2016 | 24 patients | either left or right homonymous hemianopia | Home-based training | ||||
| 19 | [78] | 2016 | 10 patients | more than 3 months after diagnosis or lesion | unisensory training, multi-Audio-visual sensory training, unisensory Audio training | controlled environment | visual search improvement in audio-visual search, improving fixation and oculomotor performance, increased accuracy | |
| 20 | [79] | 2017 | 3 patients | the first subject after 3 months of stroke, the second subject was with HH on the right side, the third subject with partial left HH | visual and acoustic stimuli, audio-visual stimulation | a plastic arch-shaped device fixed horizontally on the table surface, two horizontal rows of visual stimuli (LEDs) for a total length of 192 cm, height of 32 cm, and thickness of 1.2 cm in which the instrument covered 180 Degrees as the entire visual field. Training includes 12 visual stimuli (24 LEDs) with a diameter of 0.5 and 12 acoustic stimuli | Laboratory setting | significant improvement in visual detection rates in the affected hemifield in both the Fixed-Eyes Condition, improved eye-movement pre and post-conditional, and improved visual detection in hemifield. The percentage of responses to audio-visual stimuli in the hemianopia hemifield improved |
| 21 | [80] | 2017 | 87 patients | stable hemianopia patients | Fresnel prisms, 30—visual search training, and 30—standard care | not mentioned | change in visual field area; improving reading abilities in both speed and accuracy;Visual function improved at 26 weeks in the visual search training arm compared to other interventions. | |
| 22 | [81] | 2018 | 22 patients – Kids | different reasons such as perinatal ischemia, tumor, stroke, hemispherectomy, hemiatrophy | computer-based visual search training (VST) for children | trained at home for 15 minutes twice/day, 5 days/week, for 6 weeks. | Home-based training | search times (STs) decreased significantly during the training and all search performance tests. This improvement persisted 6 weeks after the end of the training. Saccade amplitudes increased, the total number of saccades to find the target decreased, and the proportional number of saccades to the non-seeing side increased. During free viewing, saccades were equally distributed to both sides before and after training |
| 23 | [82] | 2018 | 24 patients | adult stroke patients | efficacy open-label investigation using vision therapies techniques | one lesson a week for 12 weeks carried out by an optometrist and a vision therapist. Between lessons, patients were to train at home for a minimum of 15-20 min daily. | Laboratory setting | Significant improvements in visual performance were measured for all test parameters from the baseline to the evaluation after the last lesson of vision training. Tracing test results improved, reading speed in words increased, peripheral awareness of visual markers improved |
| 24 | [83] | 2018 | 1 patient | visual area seizure | Visual neurorehabilitation therapy (NRT) | administered for 3 hours each week | Laboratory setting | ocular movements improved, visual search became more organized, the reading reached a level without mistakes, with rhythm and goog intonation |
| 25 | [84] | 2018 | 10 patients | Trained in detecting low contrast Gabor patches randomly presented in the blind field, which refers to regions of 0 dB sensitivity, and along the hemianopia boundary between absolute (0 dB) and partial blindness (>0 dB) | Laboratory setting | NRT led to significant visual field enlargement (≈5 deg), and the restored area acquired new visual functions such as small letter recognition and perception of moving shapes; for some patients, NRT also improved detection, either aware or not, of high contrast flickering grating and recognition of geometrical shapes entirely presented within the blind field. | ||
| 26 | [85] | 2019 | 14 patients | patient with a history of stroke | computer-based cognitive rehabilitation (CBCR) | visuospatial neglect or homonymous hemianopia in the subacute phase of the following stroke | Hospital- no natural ecology | CBCR improved visuospatial symptoms after a stroke |
The main focus of the practices we have examined is how to apply this training to real-life situations and the daily activities of our participants. Studies have addressed this issue, emphasizing the need to extend the assessment of training effectiveness to patients' everyday lives. As indicated in the tables of reviews and references to these practices, 25 out of 26 practices mentioned are based on clinical and laboratory settings. This lack of connection to the real environment often results in participants not utilizing their compensatory aids.
Most of the papers we mentioned show improvements in reading, target identification, object detection in noisy environments, and reaction times. However, enhancing full cognitive interaction, including multi-domain reactions, is crucial. Kerkhoff and colleagues (1994) demonstrated that combining compensatory search training with real-life exercises, such as locating objects at home, yields more naturalistic improvements in search performance than in laboratory settings. This is because a broader visual field enhances visual search abilities. Methods like prisms are less effective than other approaches because they correct the input to the visual system rather than train it. A study by [58] comparing prism glasses, visual search, and standard care in hemianopia patients showed that prism glasses are neither superior nor inferior to other cases. It is important to note and include this in our review when discussing real-world contexts. However, prisms are not designed to train the visual system to improve its function but to compensate for eye muscle weakness, align the eyes, and help maintain comfortable vision.
Research by [29] using prism glasses on 23 participants demonstrated that two-thirds of the patients showed improvement of approximately 22 degrees in both the upper and lower quadrants. This suggests that utilizing an apparatus that includes a natural environment is beneficial. However, a remaining question is whether the same results would persist if the users stopped using the glasses. To date, there is no research on this topic. The primary goal of restoration therapies should be to achieve permanent improvement in the visual search rather than relying on temporary or device-based solutions. Despite various techniques and practices, no "standard" strategy for restoring visual loss exists. This lack of a standardized approach is mainly due to the initial belief that visual deficits are mostly permanent and irreversible.
None of the reviewed practices are based on ecological and high-level vision therapies. Instead, they primarily focus on low-level vision therapies. While some Virtual Reality practices in the early 1990s were marketed for vision improvement and restoration, subsequent findings revealed that the benefits outweighed by cost and outcome measures. As demonstrated and described in the results table, current research heavily relies on laboratory experiments to treat hemianopia cases. To provide a more realistic and improved opportunity, there should be an increase in cases involving 3D environments (either the real world or 3D or VR).
A study by [86] indicated that a group of hemianopia patients who performed well in a simulator environment did not perform as well in other tests, including lab settings. This confirms that while positive outcomes are observed in laboratory experiments, these improvements are not guaranteed in the natural world, and there is a possibility of lower performance. The study also revealed that patients have fewer opportunities for exploration in a realistic environment than healthy participants. This emphasizes the importance of a more authentic environment for better results and increased exploration opportunities, rather than relying on screens or controlled environments like labs or rooms. Notably, they mentioned that "the LP group was unaware of its poor performance," suggesting that while positive changes may be observed in laboratory settings, comparing them to a natural environment may not provide accurate results and could lead to misleading conclusions.
The real environment is inherently more complex and requires higher visual processing than laboratory settings, which primarily focus on low and mid-level visual systems. Therefore, it is crucial to practice in a way that necessitates additional adaptation of visual exploratory behavior. Implementing VR, 3D, or real environments can provide a much closer approximation of reality than detecting lights in a dimly lit room.
In the naturalistic simulation setting, patients with hemianopia demonstrate high performance characterized by adapted visual exploratory behavior, including increased amplitude and peak velocity of saccades, wider distribution of horizontal eye movements, and a shift of overall saccade distribution into the blind field [73]. This aspect has been explored in tasks involving free viewing, as seen in studies such as [87].
During tasks, patients with hemianopia, for example, encounter difficulties in target-object identification when presented with non-target situations, exhibiting repeated saccades and fixations on the same object. This leads to longer search times and unsystematic scan paths [88,89]. Their fixations predominantly dwell in their intact hemifield, and their saccades need to be more regular, accurate, and smaller to enable rapid and organized scanning. Consequently, they may overlook objects or relevant parts of a scene in their blind hemifield. These consequences are more evident in an environment with natural objects like a street than a monitor screen, which imposes a higher cognitive load. Given the controllability of the environment, practicing in real-world scenarios can promote more systematic exploration. Patients can adapt themselves to the natural world through such training. In a laboratory environment with a screen, the number of cognitive elements involved in the practice is much smaller than the active cognitive domains engaged in a natural or VR environment. Several studies and theories, such as [75,85,90,91], have discussed this matter, suggesting that visual blindness affects other domains, leading them to adopt compensatory visual search strategies in the seeing hemifield.
Head movement is another significant factor to consider in comparison to lab settings. Studies like [92] have shown that successful visual search is associated with head movements. For instance, providing patients with more opportunities to explore can improve their visual exploratory abilities in driving experiments or street walks. In most laboratory experiments, except for eye-tracking fixation, participants are engaged in tasks with minimal head movements. A study conducted by [93] comparing explorative saccade and flicker training demonstrated that explorative saccade training specifically improves saccadic behavior, natural search, and scene exploration in the blind field. Flicker-stimulation training, on the other hand, does not enhance saccadic behavior or visual fields. In a randomized controlled trial, the findings revealed significant benefits of compensatory exploration training, including subjective improvements in mastering daily activities.
A study utilizing fMRI data by [94] indicates that eye movement training induces plasticity in different brain regions by activating areas such as Brodmann 17 and 18. Their data reveals that healthy participants did not exhibit significant changes in these areas, highlighting the importance of eye movements. Most laboratory settings where patients with hemianopia undergo training involve fixation, a fixed head position, and minimal eye movements across different regions. By implementing broader training approaches involving VR, 3D, or real environments, we can activate these areas more effectively, facilitating patients' recovery in different brain regions and promoting increased cognitive activation.
Statistical studies in the natural sciences demonstrate that object boundaries often consist of visual elements that are nearby, continuous across intersections, or form smooth contours. Our visual system attempts to predict the typical features of an object in a natural scene. Based on geometric segmentation and cognitive influences, certain elements within the same context can be interpreted as either background or recognized objects.
Priming a stimulus can enhance the perception of the stimulus and the environment when executed correctly. Thus, combining cognitive features with natural scenes and adapting geometrical characteristics can improve neural coding in the visual system. This process can involve transient activity during specific modulations, subsequently influencing decision-making or contributing to long-term memory formation. For instance, consider practicing visual exploration with a hemianopia patient performing a task involving recognizing a traffic light at an intersection. Combining audio-visual cues, such as associating sounds with colors or lights, or vice versa, associating colors with sounds, can create an exploratory factor. In both cases, fostering long-term memory formation can be beneficial, as vision somewhat relies on memory.
It is worth noting that most current research primarily focuses on the lowest level of vision, encompassing local contrast, movement, and orientation. However, the real world extends beyond these fundamental aspects and incorporates high-level vision, including object recognition. When a scene and its shapes are presented to our vision, object recognition allows us to match objects with our memories and associate them with meaning. Therefore, vision is crucial in guiding body movement to elicit appropriate responses and actions. As previously mentioned, although retrieving vision from this foundational level is necessary, neglecting the broader scope of the scene, which involves high-level vision, can result in the loss of memories, dissociation of details, and difficulties after vision loss.
In cases of vision loss, most neural activities in the affected areas cease and do not occur. Each point in the visual field undergoes processing in multiple levels of channels that extract and analyze different aspects of visual input. Since many current strategies are based on experimental designs such as psychopy and psych toolbox, they often involve simple backgrounds and limited experiments. Consequently, these approaches fail to activate high-level visual systems, weakening neural activities in those areas. By incorporating wider training applications, including VR, 3D, or real environments, we can more effectively activate these areas, aiding patients in recovering different brain functions and promoting increased cognitive activation.
3. Conclusion
In conclusion, this study has examined the challenges and potential in rehabilitating visual field defects, particularly hemianopia. We have discussed the limitations of conventional approaches focusing primarily on low-level vision therapies conducted in laboratory or clinical settings. While these approaches have shown positive outcomes in specific visual skills, they often fail to address the complexities of real-world environments and higher-level vision processes.
During our analysis, we deliberately chose to exclude the works of Huxling et al. This decision was based on their consistent avoidance of using the term "hemianopia" and instead referring to it as "cortical blindness." However, it is important to acknowledge that Huxling et al. have significantly contributed to the field. Their extensive studies on training techniques in hemianopia, as demonstrated in their works [24,26,95,96,97,98,99,100], offer valuable insights and potential avenues for further investigation into hemianopia, despite their differing terminology.
A growing body of research emphasizes the integration of natural and ecologically valid environments in visual rehabilitation to overcome these limitations. Several studies in this review have demonstrated the benefits of utilizing virtual reality (VR), three-dimensional (3D) settings, or real-world scenarios to enhance visual recovery.
For instance, Kerkhoff and colleagues (1994) conducted a study in which patients with hemianopia performed a search task in a real home environment. They found that training in a naturalistic setting resulted in more natural improvements in search performance compared to a laboratory setting. This suggests that widening the field of exploration and practicing in environments that resemble real-life situations can lead to more effective rehabilitation outcomes.
Furthermore, studies have shown that incorporating audio-visual associations and priming stimuli can enhance visual perception and facilitate memory integration. For example, associating auditory cues with a traffic light can create an exploratory factor that links sound with color or light, enabling patients to better perceive and respond to real-world stimuli. This approach, which engages both low-level and high-level visual processes, promotes comprehensive and enduring improvements in visual function.
Moreover, research has demonstrated that VR and 3D environments can stimulate neural plasticity in different brain regions. Studies by Tinelli et al. (2017) and Rowe et al. (2017) have shown that visual training in immersive environments significantly improves visual detection, eye movements, and visuospatial symptoms. These findings underscore the potential of incorporating ecologically valid environments to activate and reorganize neural circuits associated with visual processing.
While the current research landscape provides valuable insights into the benefits of real-world and higher-level vision approaches, it is crucial to establish a standardized strategy for visual loss restoration. Nevertheless, the evidence suggests that adopting a comprehensive and ecological approach to visual rehabilitation can enhance visual recovery, improve daily functioning, and restore the quality of life for individuals with visual field defects.
In conclusion, integrating natural and ecologically valid environments, VR, 3D settings, and cognitive interactions into visual rehabilitation shows great promise in improving the outcomes of patients with visual field defects. By acknowledging the limitations of traditional approaches and embracing a holistic and adaptive framework, we can empower individuals to regain their visual abilities, successfully navigate real-world environments, and reintegrate into society. Continued research and development in this field are essential to refine further and expand the effectiveness of visual rehabilitation techniques, ultimately enhancing the lives of individuals affected by visual field defects.
Author Contributions
Conceptualization, MAK, and LB. Writing—original draft preparation, MAK; writing—review and editing, LB, EA; All authors have read and agreed to the published version of the manuscript.
Funding
This project has received funding from the European Union's Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No 101034319 and from the European Union – NextGenerationEU.
Conflicts of Interest
The authors declare no conflict of interest.
References
- F. Criado-Boado et al., “Coevolution of visual behaviour, the material world and social complexity, depicted by the eye-tracking of archaeological objects in humans,” Sci. Rep., vol. 9, no. 1, Art. no. 1, Mar. 2019. [CrossRef]
- “Hemianopia, spatial neglect, and their multisensory rehabilitation - ScienceDirect”. 17 May. Available online: https://www.sciencedirect.com/science/article/pii/B978012812492500019X?via%3Dihub (accessed on 17 May 2023).
- S. Kedar, “Pediatric homonymous hemianopia.,” J. AAPOS Off. Publ. Am. Assoc. Pediatr. Ophthalmol. Strabismus, 2006.
- X. Zhang, S. Kedar, M. J. Lynn, N. J. Newman, and V. Biousse, “Natural history of homonymous hemianopia,” Neurology, vol. 66, no. 6, pp. 901–905, Mar. 2006. [CrossRef]
- X. Zhang, S. X. Zhang, S. Kedar, M. J. Lynn, N. J. Newman, and V. Biousse, “Natural history of homonymous hemianopia,” Neurology, vol. 66, no. 6, pp. 901–905, Mar. 2006. [Google Scholar] [CrossRef]
- R. B. Welch and D. H. Warren, “Immediate perceptual response to intersensory discrepancy.,” Psychol. Bull., vol. 88, no. 3, p. 638, 1980.
- M. O. Ernst and H. H. Bülthoff, “Merging the senses into a robust percept,” Trends Cogn. Sci., vol. 8, no. 4, pp. 162–169, 2004.
- L. M. Pambakian and C. Kennard, “Can visual function be restored in patients with homonymous hemianopia?,” Br. J. Ophthalmol., vol. 81, no. 4, pp. 324–328, Apr. 1997. [CrossRef]
- B. A. Sabel and E. Kasten, “Restoration of vision by training of residual functions,” Curr. Opin. Ophthalmol., vol. 11, no. 6, pp. 430–436, Dec. 2000. [CrossRef]
- M. I. Posner, M. J. Nissen, and R. M. Klein, “Visual dominance: an information-processing account of its origins and significance.,” Psychol. Rev., vol. 83, no. 2, p. 157, 1976.
- M. Mather and M. R. Sutherland, “Arousal-biased competition in perception and memory,” Perspect. Psychol. Sci. J. Assoc. Psychol. Sci., vol. 6, no. 2, pp. 114–133, Mar. 2011. [CrossRef]
- M. Gupta, A. C. Ireland, and B. Bordoni, “Neuroanatomy, Visual Pathway,” in StatPearls, Treasure Island (FL): StatPearls Publishing, 2023. Accessed: Jun. 19, 2023. [Online]. Available: http://www.ncbi.nlm.nih.gov/books/NBK553189/.
- J. B. Jonas, R. A. Jonas, M. M. Bikbov, Y. X. Wang, and S. Panda-Jonas, “Myopia: Histology, clinical features, and potential implications for the etiology of axial elongation,” Prog. Retin. Eye Res., p. 101156, Dec. 2022. [CrossRef]
- E. Harb, “Hyperopia☆,” in Reference Module in Neuroscience and Biobehavioral Psychology, Elsevier, 2017. [CrossRef]
- H. Al-khersan, H. W. Flynn, and J. H. Townsend, “Retinal Detachments Associated With Topical Pilocarpine Use for Presbyopia,” Am. J. Ophthalmol., vol. 242, pp. 52–55, Oct. 2022. [CrossRef]
- T. F. Tan et al., “Colour vision restrictions for driving: an evidence-based perspective on regulations in ASEAN countries compared to other countries,” Lancet Reg. Health - Southeast Asia, p. 100171, Mar. 2023. [CrossRef]
- K. W. Svaerke, K. V. Omkvist, I. B. Havsteen, and H. K. Christensen, “Computer-Based Cognitive Rehabilitation in Patients with Visuospatial Neglect or Homonymous Hemianopia after Stroke,” J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc., vol. 28, no. 11, p. 104356, Nov. 2019. [CrossRef]
- G. A. de Haan, J. Heutink, B. J. M. Melis-Dankers, O. Tucha, and W. H. Brouwer, “Spontaneous recovery and treatment effects in patients with homonymous visual field defects: a meta-analysis of existing literature in terms of the ICF framework,” Surv. Ophthalmol., vol. 59, no. 1, pp. 77–96, Jan. 2014. [CrossRef]
- C. S. Chen et al., “Vision-related quality of life in patients with complete homonymous hemianopia post stroke,” Top. Stroke Rehabil., vol. 16, no. 6, pp. 445–453, 2009. [CrossRef]
- M. Berthold-Lindstedt, J. Johansson, J. Ygge, and K. Borg, “How to assess visual function in acquired brain injury—Asking is not enough,” Brain Behav., vol. 11, no. 2, p. e01958, Nov. 2020. [CrossRef]
- L. de Munter, S. Polinder, R. J. M. Havermans, E. W. Steyerberg, and M. A. C. de Jongh, “Original research: Prognostic factors for recovery of health status after injury: a prospective multicentre cohort study,” BMJ Open, vol. 11, no. 1, 2021. [CrossRef]
- C. Perez and S. Chokron, “Rehabilitation of homonymous hemianopia: insight into blindsight,” Front. Integr. Neurosci., vol. 8, p. 82, 2014. [CrossRef]
- A. Sahraie, C. T. Trevethan, M. J. MacLeod, A. D. Murray, J. A. Olson, and L. Weiskrantz, “Increased sensitivity after repeated stimulation of residual spatial channels in blindsight,” Proc. Natl. Acad. Sci. U. S. A., vol. 103, no. 40, pp. 14971–14976, Oct. 2006. [CrossRef]
- K. R. Huxlin, “Perceptual plasticity in damaged adult visual systems,” Vision Res., vol. 48, no. 20, pp. 2154–2166, Sep. 2008. [CrossRef]
- S. Ajina, K. Jünemann, A. Sahraie, and H. Bridge, “Increased Visual Sensitivity and Occipital Activity in Patients With Hemianopia Following Vision Rehabilitation,” J. Neurosci., vol. 41, no. 28, pp. 5994–6005, Jul. 2021. [CrossRef]
- M. R. Cavanaugh and K. R. Huxlin, “Visual discrimination training improves Humphrey perimetry in chronic cortically induced blindness,” Neurology, vol. 88, no. 19, pp. 1856–1864, May 2017. [CrossRef]
- B. A. Wright, A. T. Sabin, Y. Zhang, N. Marrone, and M. B. Fitzgerald, “Enhancing Perceptual Learning by Combining Practice with Periods of Additional Sensory Stimulation,” J. Neurosci., vol. 30, no. 38, pp. 12868–12877, Sep. 2010. [CrossRef]
- S. Trauzettel-Klosinski, “Current Methods of Visual Rehabilitation,” Dtsch. Ärztebl. Int., vol. 108, no. 51–52, p. 871, Dec. 2011. [CrossRef]
- R. Giorgi, “Clinical and Laboratory Evaluation of Peripheral Prism Glasses for Hemianopia,” Optom. Vis. Sci., 2009.
- M. Pikhart, B. Klimova, A. Cierniak-Emerych, and S. Dziuba, “Psychosocial Rehabilitation Through Intervention by Second Language Acquisition in Older Adults,” J. Psycholinguist. Res., vol. 50, no. 5, pp. 1181–1196, Oct. 2021. [CrossRef]
- Y. Gopi, E. Wilding, and C. R. Madan, “Memory rehabilitation: restorative, specific knowledge acquisition, compensatory, and holistic approaches,” Cogn. Process., vol. 23, no. 4, pp. 537–557, Nov. 2022. [CrossRef]
- N. W. Park and J. L. Ingles, “Effectiveness of attention rehabilitation after an acquired brain injury: A meta-analysis,” Neuropsychology, vol. 15, pp. 199–210, 2001. [CrossRef]
- M. Rosa, M. F. Silva, S. Ferreira, J. Murta, and M. Castelo-Branco, “Plasticity in the Human Visual Cortex: An Ophthalmology-Based Perspective. BioMed Res. Int. 2013, 2013, 568354. [CrossRef]
- G. Kerkhoff, “Restorative and compensatory therapy approaches in cerebral blindness - a review,” Restor. Neurol. Neurosci., vol. 15, no. 2–3, pp. 255–271, 1999.
- D. A. Poggel, I. Mueller, E. Kasten, and B. A. Sabel, “Multifactorial predictors and outcome variables of vision restoration training in patients with post-geniculate visual field loss,” Restor. Neurol. Neurosci., vol. 26, no. 4–5, pp. 321–339, Jan. 2008.
- M. Scheiman et al., “A randomized clinical trial of vision therapy/orthoptics versus pencil pushups for the treatment of convergence insufficiency in young adults,” Optom. Vis. Sci., vol. 82, no. 7, pp. 583–593, 2005. [CrossRef]
- C. Jicol et al., “Efficiency of Sensory Substitution Devices Alone and in Combination With Self-Motion for Spatial Navigation in Sighted and Visually Impaired,” Front. Psychol., vol. 11, 2020, Accessed: Jun. 19, 2023. [Online]. Available: https://www.frontiersin.org/articles/10.3389/fpsyg.2020.01443.
- R. M. van Nispen et al., “Low vision rehabilitation for better quality of life in visually impaired adults,” Cochrane Database Syst. Rev., vol. 2020, no. 1, p. CD006543, Jan. 2020. [CrossRef]
- D. J. Norton, R. K. McBain, D. Ongur, and Y. Chen, “Perceptual training strongly improves visual motion perception in schizophrenia,” Brain Cogn., vol. 77, no. 2, pp. 248–256, Nov. 2011. [CrossRef]
- G. Kerkhoff, U. Münßinger, E. Haaf, G. Eberle-Strauss, and E. Stögerer, “Rehabilitation of homonymous scotomata in patients with postgeniculate damage of the visual system: saccadic compensation training,” Restor. Neurol. Neurosci., vol. 4, no. 4, pp. 245–254, Jan. 1992. [CrossRef]
- S. Trauzettel-Klosinski, “[Rehabilitation of lesions in the visual pathways],” Klin. Monatsbl. Augenheilkd., vol. 226, no. 11, pp. 897–907, Nov. 2009. [CrossRef]
- S. Trauzettel-Klosinski, “Rehabilitative techniques,” Handb. Clin. Neurol., vol. 102, pp. 263–278, 2011. [CrossRef]
- L. Julkunen, O. Tenovuo, S. Jääskeläinen, and H. Hämäläinen, “Rehabilitation of chronic post-stroke visual field defect with computer-assisted training: a clinical and neurophysiological study,” Restor. Neurol. Neurosci., vol. 21, no. 1–2, pp. 19–28, 2003.
- N. Bolognini, F. Rasi, M. Coccia, and E. Làdavas, “Visual search improvement in hemianopic patients after audio-visual stimulation,” Brain, vol. 128, no. 12, pp. 2830–2842, Dec. 2005. [CrossRef]
- F. Leo, N. Bolognini, C. Passamonti, B. E. Stein, and E. Làdavas, “Cross-modal localization in hemianopia: new insights on multisensory integration,” Brain, vol. 131, no. 3, pp. 855–865, Mar. 2008. [CrossRef]
- C. Passamonti, C. Bertini, and E. Làdavas, “Audio-visual stimulation improves oculomotor patterns in patients with hemianopia,” Neuropsychologia, vol. 47, no. 2, pp. 546–555, Jan. 2009. [CrossRef]
- G. Nelles et al., “Eye-movement training-induced plasticity in patients with post-stroke hemianopia,” J. Neurol., vol. 256, no. 5, pp. 726–733, May 2009. [CrossRef]
- I. Keller and G. Lefin-Rank, “Improvement of visual search after audiovisual exploration training in hemianopic patients,” Neurorehabil. Neural Repair, vol. 24, no. 7, pp. 666–673, Sep. 2010. [CrossRef]
- A. Hayes, C. S. Chen, G. Clarke, and A. Thompson, “Functional improvements following the use of the NVT Vision Rehabilitation program for patients with hemianopia following stroke,” NeuroRehabilitation, vol. 31, no. 1, pp. 19–30, 2012,. [CrossRef]
- J. Lewald, M. Tegenthoff, S. Peters, and M. Hausmann, “Passive Auditory Stimulation Improves Vision in Hemianopia,” PLOS ONE, vol. 7, no. 5, p. e31603, May 2012. [CrossRef]
- M. Bahnemann et al., “Compensatory eye and head movements of patients with homonymous hemianopia in the naturalistic setting of a driving simulation,” J. Neurol., vol. 262, no. 2, pp. 316–325, Feb. 2015. [CrossRef]
- F. T. Brink, T. C. W. Nijboer, D. P. Bergsma, J. J. S. Barton, and S. V. der Stigchel, “Lack of Multisensory Integration in Hemianopia: No Influence of Visual Stimuli on Aurally Guided Saccades to the Blind Hemifield,” PLOS ONE, vol. 10, no. 4, p. e0122054, Apr. 2015. [CrossRef]
- N. M. Dundon, E. Làdavas, M. E. Maier, and C. Bertini, “Multisensory stimulation in hemianopic patients boosts orienting responses to the hemianopic field and reduces attentional resources to the intact field,” Restor. Neurol. Neurosci., vol. 33, no. 4, pp. 405–419, 2015. [CrossRef]
- F. Tinelli, G. Purpura, and G. Cioni, “Audio-Visual Stimulation Improves Visual Search Abilities in Hemianopia due to Childhood Acquired Brain Lesions,” Multisensory Res., vol. 28, no. 1–2, pp. 153–171, Jan. 2015. [CrossRef]
- A. Sahraie, N. Smania, and J. Zihl, “Use of NeuroEyeCoachTM to Improve Eye Movement Efficacy in Patients with Homonymous Visual Field Loss,” BioMed Res. Int., vol. 2016, p. e5186461, Sep. 2016. [CrossRef]
- P. A. Grasso, E. Làdavas, and C. Bertini, “Compensatory Recovery after Multisensory Stimulation in Hemianopic Patients: Behavioral and Neurophysiological Components,” Front. Syst. Neurosci., vol. 10, p. 45, May 2016. [CrossRef]
- F. Tinelli, G. Cioni, and G. Purpura, “Development and Implementation of a New Telerehabilitation System for Audiovisual Stimulation Training in Hemianopia,” Front. Neurol., vol. 8, 2017, Accessed: Jun. 20, 2023. [Online]. Available: https://www.frontiersin.org/articles/10.3389/fneur.2017.00621.
- F. J. Rowe et al., “A pilot randomized controlled trial comparing effectiveness of prism glasses, visual search training and standard care in hemianopia,” Acta Neurol. Scand., vol. 136, no. 4, pp. 310–321, Oct. 2017. [CrossRef]
- V. Ivanov et al., “Effects of visual search training in children with hemianopia,” PLoS ONE, vol. 13, no. 7, p. e0197285, Jul. 2018. [CrossRef]
- P. Smaakjær, S. T. Tødten, and R. S. Rasmussen, “Therapist-assisted vision therapy improves outcome for stroke patients with homonymous hemianopia alone or combined with oculomotor dysfunction,” Neurol. Res., vol. 40, no. 9, pp. 752–757, Sep. 2018. [CrossRef]
- M. Pineda-Ortíz, G. Pacheco-López, M. Rubio-Osornio, C. Rubio, and J. Valadez-Rodríguez, “Neurorehabilitation of saccadic ocular movement in a patient with a homonymous hemianopia postgeniculate caused by an arteriovenous malformation,” Medicine (Baltimore), vol. 97, no. 11, p. e9890, Mar. 2018. [CrossRef]
- C. Casco, M. Barollo, G. Contemori, and L. Battaglini, “Neural Restoration Training improves visual functions and expands visual field of patients with homonymous visual field defects,” Restor. Neurol. Neurosci., vol. 36, no. 2, pp. 275–291, 2018. [CrossRef]
- W. Svaerke, K. V. Omkvist, I. B. Havsteen, and H. K. Christensen, “Computer-Based Cognitive Rehabilitation in Patients with Visuospatial Neglect or Homonymous Hemianopia after Stroke,” J. Stroke Cerebrovasc. Dis., vol. 28, no. 11, Nov. 2019. [CrossRef]
- L. Julkunen, O. Tenovuo, S. Jääskeläinen, and H. Hämäläinen, “Rehabilitation of chronic post-stroke visual field defect with computer-assisted training,” Restor. Neurol. Neurosci., vol. 21, no. 1–2, pp. 19–28, Jan. 2003.
- D. A. Poggel, E. M. Mueller-Oehring, E. Kasten, U. Bunzenthal, and B. A. Sabel, “The topography of training-induced visual field recovery: Perimetric maps and subjective representations,” Vis. Cogn., vol. 16, no. 8, pp. 1059–1077, Nov. 2008. [CrossRef]
- C. Passamonti, I. Frissen, and E. Làdavas, “Visual recalibration of auditory spatial perception: two separate neural circuits for perceptual learning. Eur. J. Neurosci. 2009, 30, 1141–1150. [CrossRef] [PubMed]
- G. Nelles et al., “Eye-movement training-induced plasticity in patients with post-stroke hemianopia,” J. Neurol., vol. 256, no. 5, pp. 726–733, May 2009. [CrossRef]
- I. Keller and G. Lefin-Rank, “Improvement of Visual Search After Audiovisual Exploration Training in Hemianopic Patients,” Neurorehabil. Neural Repair, vol. 24, no. 7, pp. 666–673, Sep. 2010. [CrossRef]
- I. Keller and G. Lefin-Rank, “Repair,” 2010.
- M. Crotty, M. van den Berg, A. Hayes, C. Chen, K. Lange, and S. George, “Hemianopia after stroke: A randomized controlled trial of the effectiveness of a standardised versus an individualized rehabilitation program, on scanning ability whilst walking1,” NeuroRehabilitation, vol. 43, no. 2, pp. 201–209, 2018. [CrossRef]
- J. Lewald, M. Tegenthoff, S. Peters, and M. Hausmann, “Passive Auditory Stimulation Improves Vision in Hemianopia,” PLOS ONE, vol. 7, no. 5, p. e31603, May 2012. [CrossRef]
- J. Lewald, R. W. Kentridge, S. Peters, M. Tegenthoff, C. A. Heywood, and M. Hausmann, “Auditory-visual localization in hemianopia.,” Neuropsychology, vol. 27, no. 5, p. 573, 2013.
- M. Bahnemann et al., “Compensatory eye and head movements of patients with homonymous hemianopia in the naturalistic setting of a driving simulation,” J. Neurol., vol. 262, no. 2, pp. 316–325, Feb. 2015. [CrossRef]
- F. T. Brink, T. C. W. Nijboer, D. P. Bergsma, J. J. S. Barton, and S. V. der Stigchel, “Lack of Multisensory Integration in Hemianopia: No Influence of Visual Stimuli on Aurally Guided Saccades to the Blind Hemifield,” PLOS ONE, vol. 10, no. 4, p. e0122054, Apr. 2015. [CrossRef]
- M. Dundon, E. Làdavas, M. E. Maier, and C. Bertini, “Multisensory stimulation in hemianopic patients boosts orienting responses to the hemianopic field and reduces attentional resources to the intact field,” Restor. Neurol. Neurosci., vol. 33, no. 4, pp. 405–419, 2015. 2015. [CrossRef]
- F. Tinelli, G. Purpura, and G. Cioni, “Audio-Visual Stimulation Improves Visual Search Abilities in Hemianopia due to Childhood Acquired Brain Lesions,” Multisensory Res., vol. 28, no. 1–2, pp. 153–171, Jan. 2015. [CrossRef]
- Sahraie, N. Smania, and J. Zihl, “Use of NeuroEyeCoachTM to Improve Eye Movement Efficacy in Patients with Homonymous Visual Field Loss. BioMed Res. Int. 2016, 2016, 5186461. [CrossRef]
- P. A. Grasso, E. Làdavas, and C. Bertini, “Compensatory Recovery after Multisensory Stimulation in Hemianopic Patients: Behavioral and Neurophysiological Components,” Front. Syst. Neurosci., vol. 10, 2016, Accessed: Jun. 20, 2023. [Online]. Available: https://www.frontiersin.org/articles/10.3389/fnsys.2016.00045.
- F. Tinelli, G. Cioni, and G. Purpura, “Development and Implementation of a New Telerehabilitation System for Audiovisual Stimulation Training in Hemianopia,” Front. Neurol., vol. 8, 2017, Accessed: May 24, 2023. [Online]. Available: https://www.frontiersin.org/articles/10.3389/fneur.2017.00621. 24 May.
- F. J. Rowe et al., “A pilot randomized controlled trial comparing effectiveness of prism glasses, visual search training and standard care in hemianopia,” Acta Neurol. Scand., vol. 136, no. 4, pp. 310–321, Oct. 2017. [CrossRef]
- V. Ivanov et al., “Effects of visual search training in children with hemianopia. PloS One 2018, 13, e0197285. [CrossRef] [PubMed]
- P. Smaakjær, S. T. Tødten, and R. S. Rasmussen, “Therapist-assisted vision therapy improves outcome for stroke patients with homonymous hemianopia alone or combined with oculomotor dysfunction,” Neurol. Res., vol. 40, no. 9, pp. 752–757, Sep. 2018. [CrossRef]
- M. Pineda-Ortíz, G. Pacheco-López, M. Rubio-Osornio, C. Rubio, and J. Valadez-Rodríguez, “Neurorehabilitation of saccadic ocular movement in a patient with a homonymous hemianopia postgeniculate caused by an arteriovenous malformation: A Case Report,” Medicine (Baltimore), vol. 97, no. 11, p. e9890, Mar. 2018. [CrossRef]
- C. Casco, M. Barollo, G. Contemori, and L. Battaglini, “Neural Restoration Training improves visual functions and expands visual field of patients with homonymous visual field defects,” Restor. Neurol. Neurosci., vol. 36, no. 2, pp. 275–291, 2018. [CrossRef]
- W. Svaerke, K. V. Omkvist, I. B. Havsteen, and H. K. Christensen, “Computer-Based Cognitive Rehabilitation in Patients with Visuospatial Neglect or Homonymous Hemianopia after Stroke,” J. Stroke Cerebrovasc. Dis., vol. 28, no. 11, p. 104356, Nov. 2019. [CrossRef]
- J. Hamel, A. Kraft, S. Ohl, S. De Beukelaer, H. J. Audebert, and S. A. Brandt, “Driving Simulation in the Clinic: Testing Visual Exploratory Behavior in Daily Life Activities in Patients with Visual Field Defects,” J. Vis. Exp. JoVE, no. 67, p. 4427, Sep. 2012. [CrossRef]
- J. Lanyon and J. J. S. Barton, “Visual Search and Line Bisection in Hemianopia: Computational Modelling of Cortical Compensatory Mechanisms and Comparison with Hemineglect,” PLoS ONE, vol. 8, no. 2, p. e54919, Feb. 2013. [CrossRef]
- S. Schuett, R. W. Kentridge, J. Zihl, and C. A. Heywood, “Are hemianopic reading and visual exploration impairments visually elicited? New insights from eye movements in simulated hemianopia,” Neuropsychologia, vol. 47, no. 3, pp. 733–746, Feb. 2009. [CrossRef]
- L. M. Pambakian, D. S. Wooding, N. Patel, A. B. Morland, C. Kennard, and S. K. Mannan, “Scanning the visual world: a study of patients with homonymous hemianopia,” J. Neurol. Neurosurg. Psychiatry, vol. 69, no. 6, pp. 751–759, Dec. 2000. [CrossRef]
- E. L. SAIONZ, A. BUSZA, and K. R. HUXLIN, “Rehabilitation of visual perception in cortical blindness,” Handb. Clin. Neurol., vol. 184, pp. 357–373, 2022. [CrossRef]
- B. R. Bocanegra and R. Zeelenberg, “Dissociating emotion-induced blindness and hypervision,” Emot. Wash. DC, vol. 9, no. 6, pp. 865–873, Dec. 2009. [CrossRef]
- M. Wood et al., “Hemianopic and Quadrantanopic Field Loss, Eye and Head Movements, and Driving,” Invest. Ophthalmol. Vis. Sci., vol. 52, no. 3, pp. 1220–1225, Mar. 2011. [CrossRef]
- T. Roth, A. N. Sokolov, A. Messias, P. Roth, M. Weller, and S. Trauzettel-Klosinski, “Comparing explorative saccade and flicker training in hemianopia: A randomized controlled study,” Neurology, vol. 72, no. 4, pp. 324–331, Jan. 2009. [CrossRef]
- S. Bock and I. Fine, “Anatomical and functional plasticity in early blind individuals and the mixture of experts architecture,” Front. Hum. Neurosci., vol. 8, p. 971, Dec. 2014. [CrossRef]
- S. Kwon, B. K. Fahrenthold, M. R. Cavanaugh, K. R. Huxlin, and J. F. Mitchell, “Perceptual restoration fails to recover unconscious processing for smooth eye movements after occipital stroke,” eLife, vol. 11, p. e67573, Jun. 2022. [CrossRef]
- R. Huxlin and T. Pasternak, “Training-induced Recovery of Visual Motion Perception after Extrastriate Cortical Damage in the Adult Cat,” Cereb. Cortex, vol. 14, no. 1, pp. 81–90, 2004. [CrossRef]
- R. Huxlin, J. M. Williams, and T. Price, “A neurochemical signature of visual recovery after extrastriate cortical damage in the adult cat,” J. Comp. Neurol., vol. 508, no. 1, pp. 45–61, 2008. [CrossRef]
- R. Huxlin et al., “Perceptual Relearning of Complex Visual Motion after V1 Damage in Humans,” J. Neurosci., vol. 29, no. 13, pp. 3981–3991, Apr. 2009. [CrossRef]
- A. Barbot et al., “Changes in perilesional V1 underlie training-induced recovery in cortically-blind patients.” bioRxiv, p. 2020.02.28.970285, Mar. 21, 2020. [CrossRef]
- A. Das and K. R. Huxlin, “New approaches to visual rehabilitation for cortical blindness: outcomes and putative mechanisms,” Neurosci. Rev. J. Bringing Neurobiol. Neurol. Psychiatry, vol. 16, no. 4, pp. 374–387, Aug. 2010. [CrossRef]
Figure 1.
Role of two eyes in the visual field. 'Full Visual Field' by Casey Henley is licensed under a Creative Commons Attribution Non-Commercial Share-Alike (CC BY-NC-SA) 4.0 International License.
Figure 1.
Role of two eyes in the visual field. 'Full Visual Field' by Casey Henley is licensed under a Creative Commons Attribution Non-Commercial Share-Alike (CC BY-NC-SA) 4.0 International License.
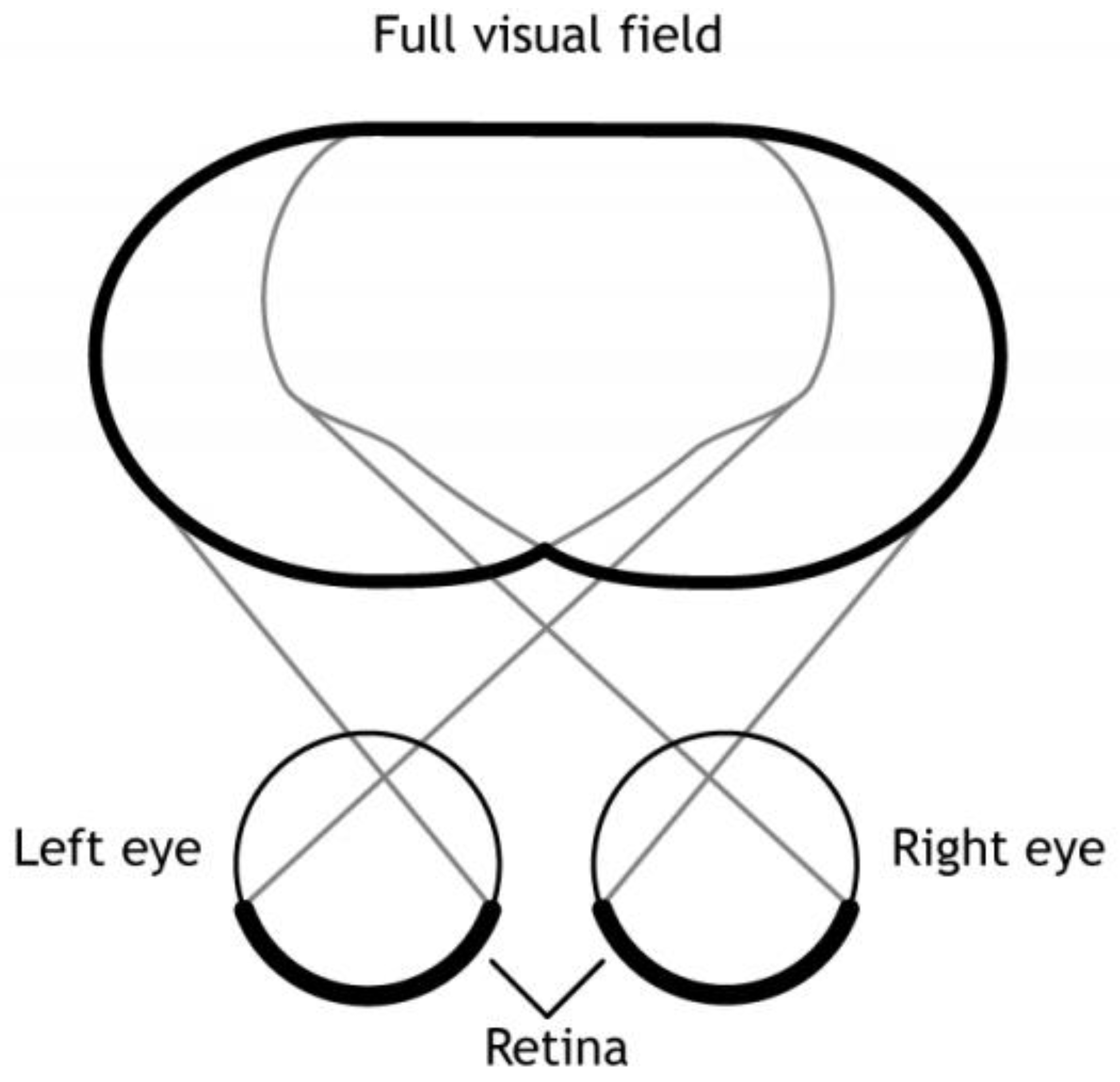
Figure 2.
'Visual Hemifields' by Casey Henley is licensed under a Creative Commons Attribution Non-Commercial Share-Alike (CC BY-NC-SA) 4.0 International License.
Figure 2.
'Visual Hemifields' by Casey Henley is licensed under a Creative Commons Attribution Non-Commercial Share-Alike (CC BY-NC-SA) 4.0 International License.
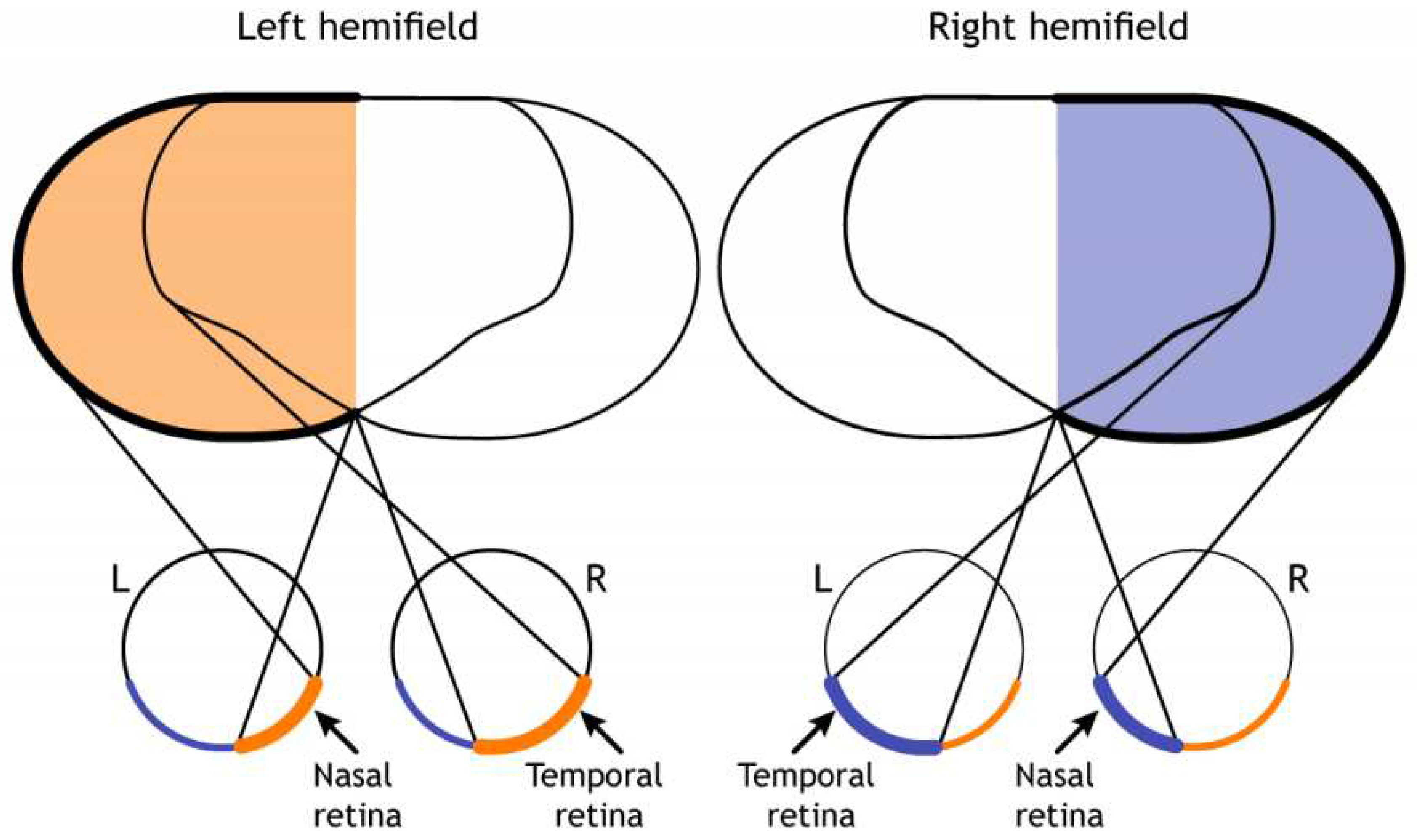
Figure 3.
Schematic of different pathways damages and results in visual deficits.
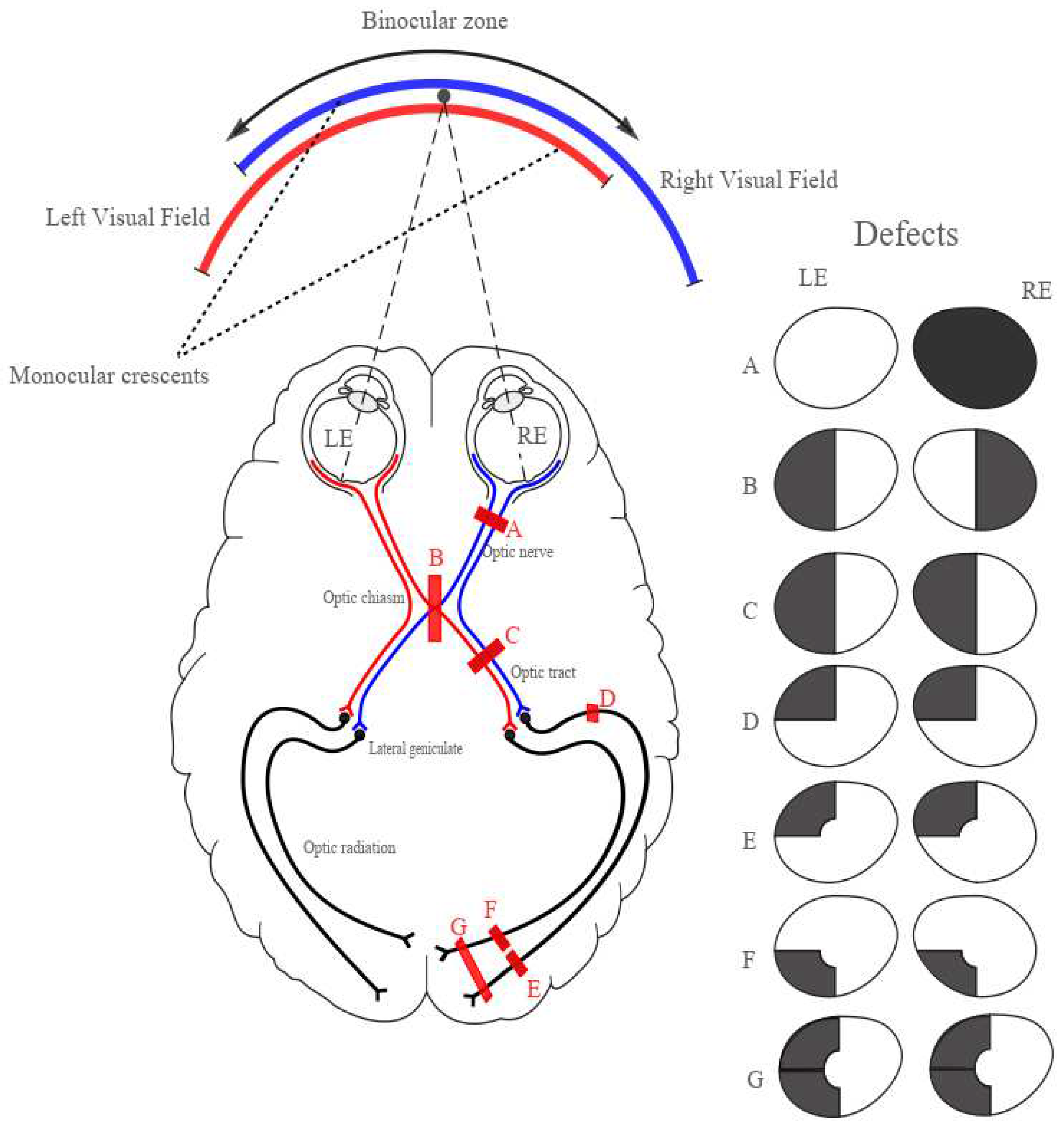
Figure 4.
Schematic of the literature search and article selection.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



