
Submitted:
20 June 2023
Posted:
21 June 2023
You are already at the latest version
Abstract
Gut microbiota is a complex and dynamic ecosystem that influences various aspects of human health. Unfortunately, there is a lack of literature highlighting the importance of gut microbiome especially in diabetes management. This paper performs bibliometric analysis to establish the rising interest of researchers in this area and the importance of gut microbiota in diabetes management. Subsequently, the study performs a narrative review to provide an overview of the gut microbiota consisting of bacteria, archaea, fungi, and viruses, and its diversity, composition, and variation among individuals. The paper further discusses the role of the gut microbiota in different diseases, including Clostridium difficile infection, behavioral disorders, cancer, obesity, diabetes, atherosclerosis, and inflammatory bowel disease, among others. It emphasizes the link between gut dysbiosis (imbalanced gut microbiota) and the development of chronic metabolic disorders. Additionally, the paper discusses the factor negatively impacting the gut microbiota. The paper concludes by explaining the mechanistic abnormalities that link dysbiosis to type 2 diabetes, including changes in short-chain fatty acid production, amino acid metabolism, bile acid regulation, and the production of specific bacterial products. Thus, the paper highlights the importance of understanding gut microbiota and related mechanisms for developing therapeutic interventions targeting the gut microbiota.
Keywords:
Gut Microbiota
; Dysbiosis
; Endocrine
; Diabetes
; Therapeutic
1. Introduction
The human body is a multifaceted walking environment. It includes around 40 trillion bacteria, which have 10 times more genes than a human cell, however, this ratio has subsequently been recalculated as 1.3:1[1]. The development of human gut bacteria predates humans by 10,000 years. Every creature on the planet has a unique gut microbiota and microbiome. There is interindividual variance in addition to topographic variation. Only 1% - 0.1% of bacteria can be cultivated in the laboratory. Direct investigation of gut microbiota reveals a far higher variety than cultivated isolates from stool samples. Many culture-independent technologies are now available, making gut microbiota fingerprinting a reality [2]. There is increased interest in academic discourse about gut microbiota and its role in diabetes management. While the importance of the gut microbiome in diabetes management is becoming increasingly evident, more studies are needed to uncover the specific mechanisms and develop targeted interventions, such as probiotics, prebiotics, and personalized dietary approaches, to optimize gut health and improve diabetes outcomes. Unfortunately, the awareness about the importance of gut microbiome in physicians is dismal and this paper addresses this issue by providing a primer on the topic and suggesting future agenda for the research. With this background, the objectives of this research paper are two prongs to perform a bibliometric analysis of the randomized controlled trials on the topic and provide a narrative review of the importance of the gut microbiome in diabetes management. The remaining papers are structured as follows. The next section discusses the material and methods followed by results and discussion. The paper concludes with key findings and suggestions about future directions for research.
2. Materials and Methods
For the first objective of the research bibliometric analysis was performed on the data collected from the PubMed database using the keyword “Gut Microbiota in Diabetes”. The inclusion criteria included clinical trials for which full text was available. The paper published in languages other than English language were excluded from the study. The tool used for the bibliometric analysis is VOSviewer [3]. A widely used open-source software tool for constructing and visualizing bibliometric networks. For the second research objective, this study utilizes a narrative review. A narrative review is an approach to summarizing existing research on a particular subject. To accomplish this objective, it amasses evidence from different resources and critically evaluates it with the intent of identifying prominent patterns and tendencies. Contrary to systemic reviews, which adhere strictly to methods, narrative reviews utilize description as their primary means for organizing data. The goal of such an arrangement is to make results more easily understandable and coherently presented [4].
3. Results & Discussion
This section lists the results of the study in two subsections.
3.1. Bibliometric Analysis on Gut Microbiome in Diabetes
The results of the bibliometric analysis suggest that there is increased interest in the researcher on the topic of Gut Microbiota in Diabetes. The trend of papers based on clinical trials published and indexed in PubMed is depicted in Figure 1.
The search using inclusion and exclusion criteria gave 164 listings which were extracted and saved in PubMed format. A map was created using bibliometric data extracted using VOSviewer. The cooccurrence analysis was performed using the author's keywords using the full counting method. The minimum number of cooccurrences of a keyword was set as five. As a result, out of a total of 243 keywords, 23 met this threshold. The result of the analysis is depicted in Figure 2.
The results suggest that Gut Microbiota is strongly associated with Obesity, Type 2 Diabetes, Insulin Resistance and Metabolic Syndrome. Out of a total of 1561 authors involved in the study 19 were repeated more than three times. The co-occurrence analysis of these authors is listed in Figure 3 for more information.
3.2. A Primer on Gut Microbiome in Diabetes
This section summarizes existing research on the topic of Gut Microbiome in Diabetes. The section is divided into eight subsections to improve the readability and for the reader.
3.2.1. Introduction of Gut Microbiome
Bacteria, Archaea, and Eucarya are the three kinds of life on Earth based on the small subunit Ribonucleic acid (RNA). Bacteria, Archea, and fungi, as well as prokaryotic and eukaryotic viruses, live in the human stomach [5]. The creature lives in an environment with a complicated antagonistic or symbiotic connection. RNA sequencing and short-gun sequencing of microbial gene extracts, together with a study of diverse metabolomes, can provide insight into the function of microbiota in health and illness. The colon's anaerobic environment promotes dense and diverse bacteria capable of fermenting complex carbohydrates [6]. The complex carbohydrates are either used by these microbiotas as an energy source or can be fermented to give rise to short-chain Fatty acids (SCFA) such as butyrate, Acetate, and Propionate [7], Figure 4.
3.2.2. Role of Microbiota in Healthy Individuals
The gut microbiota matures during the first five years of human life. Early life events are very important in terms of the type of gut microbiota and will harbor it for the rest of her life. Furthermore, these microbiota shows resilience to any external modification after these primitive five years of life [8]. Thus, early life events such as a type of microbiota in meconium, vaginal delivery, breast milk microbiota, antibiotic therapy in pregnancy & early life (before 5 years), cessation of breastfeeding (not type of solid food), and type of food habit in the family, significantly affect the gut microbiota. Although there can be an external environment that influences the maturation of gut microbiota in the form of transmission from other family members and the hospital environment, it is the maternal strain that selects the type of gut microbiota going to colonize inside the fetal gut.
The Gut microbiota along with its metabolite (metabolome) performs a variety of normal physiological functions and causes many pathophysiological abnormalities in different diseases. The important function of gut microbiota in disease & health are as follows: (1) Immunomodulation (2) Regulation of stem cell proliferation (3) Vascularization (4) Neurohormonal signaling of gut (5) Gut-Brain axis regulation (6) Host and bacterial energy production. (beta-oxidation) (7) Regulation of bone density (8) Epigenetic modification in host gene (Histone Acylation & unfolding) (9) Synthesis of vitamins, steroids, and neurotransmitters (10) Metabolism of Branch chain Amino Acids (BCAA), Carbohydrates, Fatty Acid & Proteins, Bile salts, Drugs, and Xenobiotics [5].
Similarly, the role of gut microbiota in different diseases and their therapy are ensuing (1) C-deficil infection (2) Behavioral disorders like Anxiety and Autism spectrum disorders (3) Cancer (4) Obesity (5) Type 2 and Type 1 Diabetes (6) Atherosclerosis (7) Diabetes Kidney disease (8) Non-alcoholic Liver Disease (9) Allergic Airway Disease (10) Inflammatory Bowel Disease, and (11) irritable bowel syndrome [5].
3.2.3. Pathophysiological Alteration in Gut Microbiome and Metabolomes
The diversity of gut microbiota is decreasing with industrialization and modern sanitization practices. The abundance of Bacteroides, Prevotella, Deselfovibrio, Lactobacillus, and Oxylobacter species are decreasing subsequently. The decrease in the diversity of microbiota as well as the type of abnormal gut microbiota has been associated with an increase in chronic metabolic illnesses like obesity, dyslipidemia, metabolic syndrome, insulin resistance, and type 2 diabetes [9]. The critical factors contributing to the decline in gut diversity are (1) Industrialization/ urbanization (2) Stander hygiene practice (3) Use of antibiotics before & during pregnancy and narrow-spectrum antibiotics in adults (4) Mode of delivery caesarian section vs normal delivery (5) Selection of vegetarian or non-vegetarian diet, fiber intake, and fermented food consumption, and (6) Exercise [10].
Furthermore, individuals with total colostomy are at a greater risk of type 2 diabetes than an individual with an intact colon. There is evidence using rat models that gut permeability is increased in rats with total colectomy. Gut dysbiosis is associated with obesity, dyslipidemia, metabolic syndrome, and insulin resistance. Apart from dysbiosis, the metabolites produced by these microbiotas are also important in the pathogenesis of these chronic metabolic disorders. For example, butyrate-producing bacteria decrease type 2 diabetes [11]. Furthermore, the branch chain amino acid (BCAA) production is also increased in patients with type 2 diabetes. However, at present, it is not clear whether these metabolic alterations are having causal association with type 2 diabetes, or they are the result of hyperglycemia [12].
3.2.4. Mechanistic Abnormality Linking Dysbiosis to Type 2 Diabetes
This section discusses the pathogenetic abnormalities of gut microbiota in diabetes.
- Increase Famicutis/Bacteroides ratio leading to an abnormality in short-chain fatty acid (SCFA)production e.g.: Butyrates, Acetate, Propionates, and Succinates (Figure 5) The dietary fiber is fermented into SCFA by gut microbiota to produce either beneficial or deleterious effects. These short-chain fatty acids, mainly butyrate, are responsible for providing energy to host approximately 10-15% by beta-oxidation. The higher concentration of butyrate also inhibits stem cell proliferation by Histone deacetylase (HDAC) inhibition and stimulates these cells to produce anti-inflammatory cytokines. Furthermore, their role is very crucial in regulating healthy and deep crypts and villi in the intestine and they also regulate the blood vessel density in crypts and villi. Butyrate is also important in maintaining the antimicrobial and anti-inflammatory effects in the intestine. The butyrate decreases pro-inflammatory cytokine (IL1 beta, IL-18 &TNF alfa) and anti-inflammatory cytokine (IL-10, TGF-beta) [13]. Apart from this it also modifies immunity by regulating the gene expression in macrophages by HDAC inhibition. The butyrate also acts on surface receptors like G protein-coupled receptors (GPR) 41 & GPR 43 to release Glucagon-like Peptide-1(GLP-1) and NPPY (N-terminal dipeptide sequence )apart from IL-18. The butyrate also corrects adiposity by inhibition of Histone Deacetylase (HDAC) leading to unbinding of the histone protein complex of DNA. Butyrates also improve gut integrity in goblet cells by binding to Amuc-100 surface receptors leading to an increase in TLR-2. Furthermore, butyrate can also stimulate the Pancreatic Polypeptide YY (PPYY) legends in colonocytes. In summary, we can infer that SCFA has both deleterious and protective effects on metabolic health and local immunity in the intestine [14].
- 2.
- Abnormal Tryptophan and other amino acid metabolites like branch chain amino acids (BCAA, Indol & Indol derivatives): The amino acid can also be degraded by specific bacteria to produce different metabolites which have an impact on metabolic health. The tryptophan is converted into imidazole propionate which activates mTORC1(Rapamycin complex) to cause insulin resistance at the level of muscle liver and adipose tissue. Furthermore, the bacteria also degrade different proteins into branch-chain amino acids (BCAA) which leads to insulin resistance (by mTORC1) and mitochondrial dysfunction. However, amino-acid derivatives like Indol/ Indol derivatives have a protective effect on metabolic health by reducing glucose intolerance and insulin resistance [15].
- 3.
- Primary and Secondary bile acids have a role in regulating host metabolism, Figure 6. They act by binding to the Farnesoid X receptor (FXR) which is a nuclear receptor and the Takeda G protein-coupled receptor-5 (TGR-5). Both FXR and TGR-5 regulate the GLP-1 and NPYY secretion regulating host metabolism. The binding affinity of secondary bile acid is increased after deconjugation, dehydrogenation, and dihydroxylation by gut microbiota and gut microbiota diversity is an important regulator of the secondary bile acid pool. Apart from the above-mentioned receptors vitamin D receptor (VDR), Sphingosine 1 phosphate receptor 2 (S1PR2) and pregnane X receptor (PXR) also play an important role in metabolic regulation by these bile acids. Other important metabolites which are produced from bile acids are Thyro-lithocholic acid and 6 c hydro-bile acid which are important regulators of thermogenesis. Deoxycholic acid, which is a secondary bile acid causes insulin resistance and hepatic steatosis by the FXR receptor. In summary, the FXR receptor is associated with both positive as well as negative effects on metabolism while the TGR-5 receptor has a predominantly positive effect. Furthermore, the bile acid also affects the type of microbiota and microbiota modifies the type and pool of bile acids, hence they have reciprocal relations [16].
- 4.
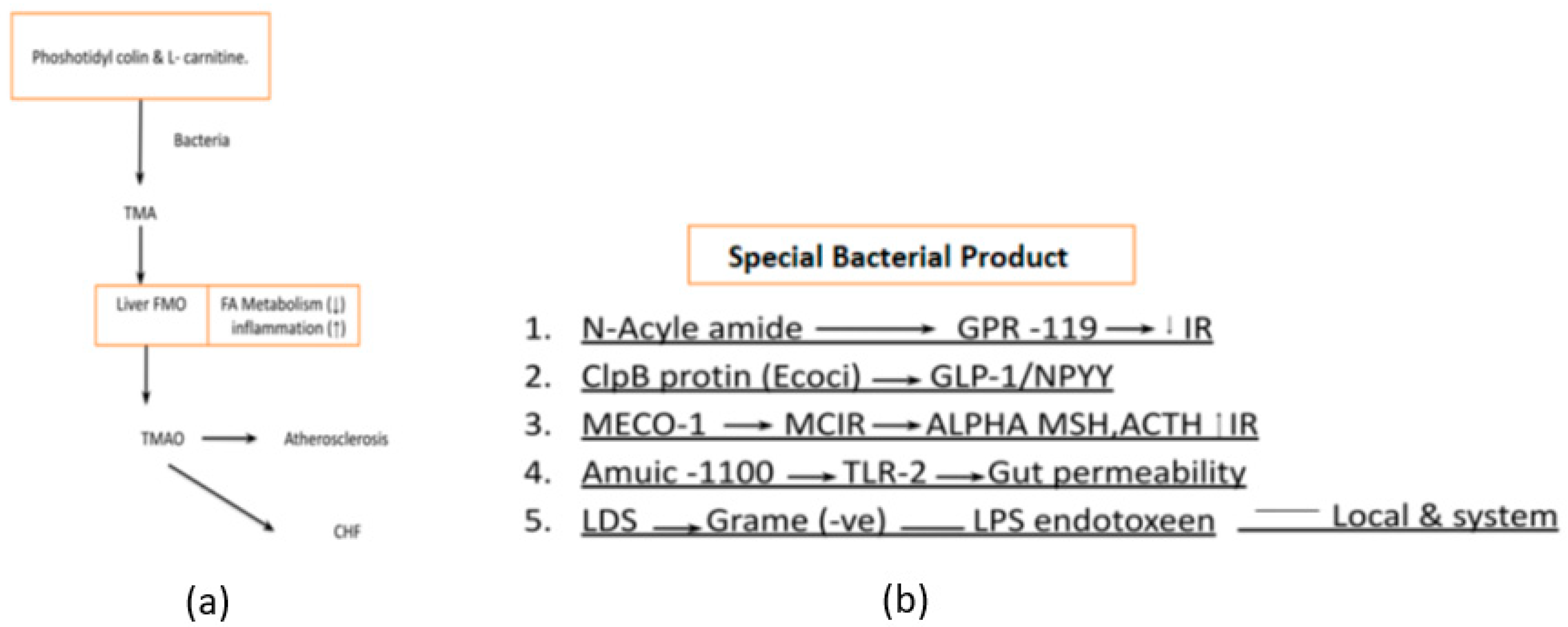
- Phosphatidylcholine and L-carnitine-derived metabolites like trimethylamine (TMA) which are later transformed into trimethylamine-N-oxide (TMAO) by the liver are the main culprits of atherosclerosis and heart failure [17] Figure 7a. Bacterial products have diverse functions and are studied for their roles in various research fields, including immunology, microbiology, and infectious diseases They play significant roles in bacterial physiology, host-microbe interactions, and disease pathogenesis. Specific bacterial products like Lipopolysaccharide (LPS), ClpB protein, MECO-1(Mitochondrial Etiology and Cognitive Function-1), etc. are critical in the management of diabetes [18] Figure 7b.
- 5.
- Bacterial by-products also play an important role in regulating host metabolism. N acyl-amide & N acyl-serinol are two important products that act on G protein-coupled receptor (GPCR) to improve glucose tolerance. Apart from this E Coli also produces ClpB protein which stimulates alfa-MSH (α-melanotropin), GLP-1, and NPY to decrease food intake. Furthermore, the patients with anorexia nervosa, the ClpB protein level is markedly increased as compared to normal individuals. MECO-1 is another bacterial product that has a resemblance to alfa-MSH and ACTH (Adrenocorticotropic Hormone) which increase anti-inflammatory activity locally to suppress anti-inflammatory cytokines. The last but most important bacterial lysis product of gram-negative bacteria is LPS (Lipopolysaccharide), which acts as a pro-inflammatory cytokine stimulator not only this but in the presence of increased gut permeability, it also leads to bacterial endotoxemia. This induces a chronic inflammatory state which eventually leads to obesity and diabetes [19].
- 6.
- Alterations in innate immunity, such as TLR5 receptor deficiency-mediated changes in gut microbiota and inflammasome-mediated TLR4 and TLR9 agonists, have been implicated in the context of diabetes. The interplay between innate immunity, gut microbiota, and diabetes is a complex and active area of research. Disruptions in the immune system, such as TLR5 receptor deficiency and inflammasome activation, can influence the composition of the gut microbiota and trigger inflammatory responses that may contribute to diabetes pathogenesis [20].
3.2.5. Therapeutic Alteration of Gut Microbiota and Diabetes Management
Gut microbiota-based therapy can be divided into two main groups, Frist is untargeted therapy and the second is targeted therapy. Alteration of gut microbiota is a promising therapeutic approach for various diseases, including inflammatory bowel disease (IBD), heart failure, COVID-19, and autism spectrum disorder (ASD). However, there is insufficient data and confusion regarding the core microbiome associated with these diseases and the hidden mechanisms of gut microbiota alteration. The gut microbiota is a new promising therapeutic target for the prevention and treatment of IBD, and there is a need to explore gut microbiota-based treatment approaches further. Regulating the gut microbiota has shown promising prospects in curing various diseases, including diabetes, cancer, and so on, by using three major intervention principles: targeting, prebiotic/probiotic/symbiotic, antibiotics, fecal microbiota transplantation, and gene editing tools for individual species of gut bacteria or entire bacterial communities. Although more research may be needed to fully understand the underlying mechanisms of gut microbiota alterations and their therapeutic potential, current literature has demonstrated perturbations in the gut microbiota in various diseases.
3.2.6. Interaction between Drugs Used in Diabetes and Gut Microbiota
There is growing evidence to suggest that there is a bidirectional interaction between drugs used in diabetes and gut microbiota. A recent study has shown that an individual's gut flora makeup affects metabolism and glucose homeostasis, and the connection between gut bacteria and glycemic agents has become a focus of research. Anti-diabetes drugs affect the gut microbiota, and the gut microbiota influences the effectiveness of diabetic treatments [21]. The interaction between gut microbiota and antidiabetic drugs is complex and bidirectional. The composition and function of gut microbiota can be affected by antidiabetic drugs, while gut microbiota can influence an individual's response to a specific drug by altering the drug's bioactivity, bioavailability, or metabolism. Studies have shown that various anti-diabetic drugs, including metformin, α-glucosidase inhibitors, GLP, and acarbose, can affect the composition and function of gut microbiota. Additionally, the interaction between gut microbiota and herbal medicines has also been investigated in the context of type 2 diabetes treatment [22].
Recent research suggests that the gut microbiota and diabetes medicines are linked. The composition of gut flora has been shown to alter metabolism and glucose homeostasis. While anti-diabetes drugs modify the gut microbiota, the gut microbiota also influences the effectiveness of diabetic treatments. Changes in the gut microbiota are effective in increasing the effectiveness of anti-diabetic medications. For example, a study using dapagliflozin, a kind of SGLT2(Sodium-Glucose Cotransporter 2) inhibitor, on type 2 diabetic mice showed that dapagliflozin improved vascular function and altered gut microbiota. Furthermore, antidiabetic agents modify the gut flora and thereby alter gastrointestinal and plasma metabolite profiles, further improving metabolic health. The understanding of bi-directional drug-microbiome interactions and how they influence the clinical outcomes of antidiabetic drugs can pave the way to developing next-generation strategies to ameliorate diabetes. The composition of gut flora has been shown to alter metabolism and glucose homeostasis. The relationship between gut microbiota and glycemic agents is considerably less understood and is an emerging topic of research [23].
3.2.7. Future of Gut Microbiota Therapeutic and Research Directions
The future of gut microbiota-related treatment is promising, and it is expected to play a significant role in preventive and therapeutic medicine. The extraordinary progress in gut microbiota research has clarified the essential roles of the gut microbial community in governing the fundamental processes of human physiology and pathophysiology. Manipulating the gut microbiota has emerged as an evolving need in medicine, due to the important involvement of gut microbiota in the pathogenesis of many diseases. However, there are still many unsolved questions in this area, and developing new therapeutic strategies to manipulate the gut microbiota has become a huge challenge. The following are some of the unsolved questions in this area:
- 1.
- What is the optimal composition of the gut microbiota for human health?
The optimal composition of the gut microbiota for human health is not fully understood, and it may vary depending on several factors, including age, environment, diet, and diseases. However, some general characteristics of healthy gut microbiota have been identified [24]:
- The dominant gut microbial phyla are Firmicutes, Bacteroidetes
- Actinobacteria, Proteobacteria, Fusobacteria, and Verrucomicrobia, with the two phyla Firmicutes and Bacteroidetes representing 90% of gut microbiota.
- The relative abundance of Firmicutes and Bacteroidetes in the gut microbiota has been associated with health and disease markers, with a higher ratio of Firmicutes to Bacteroidetes being associated with obesity and metabolic disorders.
- The relative abundance of Firmicutes and Bacteroidetes in the gut microbiota has been associated with health and disease markers, with a higher ratio of Firmicutes to Bacteroidetes being associated with obesity and metabolic disorders.
- A healthy gut microbiota is capable of fermenting non-digestible substrates like dietary fibers and endogenous intestinal mucus, producing short-chain fatty acids that provide energy for the host and have anti-inflammatory and immunomodulatory effects.
- The composition of the gut microbiota can be influenced by diet, with a high intake of fiber, fruits, and vegetables being associated with more diverse and beneficial gut microbiota.
- 2.
- How do different factors, such as diet, antibiotics, and probiotics, affect the gut microbiota?
Different factors can affect the composition of the gut microbiota, including [25]:
- A high-fiber diet, particularly one that includes fruits and vegetables, can promote diverse and beneficial gut microbiota. On the other hand, a diet high in fat and sugar can lead to less diverse and less beneficial gut microbiota.
- Antibiotic use can disrupt the gut microbiota by reducing species diversity, altering metabolic activity, and promoting the growth of antibiotic-resistant bacteria.
- Probiotics are live microorganisms that can provide health benefits when consumed in adequate amounts. Probiotics can help to restore the balance of the gut microbiota and promote health.
- The gut microbiota changes with age, with a decrease in diversity and stability in older adults.
- Environmental factors, such as exposure to pollutants and toxins, can affect the gut microbiota.
- Some medications, such as proton pump inhibitors and non-steroidal anti-inflammatory drugs, can alter the gut microbiota.
- 3.
- How can we manipulate the gut microbiota to prevent or treat specific diseases?
Manipulating the gut microbiota can be a promising approach to prevent or treat specific diseases. Some of the strategies to manipulate the gut microbiota include [26]:
- Prebiotics are non-digestible food ingredients that selectively stimulate the growth and activity of beneficial bacteria in the gut. Prebiotics can be found in foods such as whole grains, fruits, and vegetables.
- Probiotics are live microorganisms that can provide health benefits when consumed in adequate amounts. Probiotics can help to restore the balance of the gut microbiota and promote health. Probiotics can be found in foods such as yogurt, kefir, and sauerkraut, or taken as supplements.
- Fecal microbiota transplantation involves the transfer of fecal material from a healthy donor to a recipient with a disrupted gut microbiota. FMT ( Fecal Microbiota Transplantation) is effective in treating recurrent Clostridioides difficile infections and may have the potential in treating other diseases associated with gut dysbiosis.
- Antibiotics can be used to selectively target harmful bacteria in the gut microbiota. However, antibiotics can also disrupt the balance of the gut microbiota and promote the growth of antibiotic-resistant bacteria.
- A healthy diet that is high in fiber and low in fat and sugar can promote diverse and beneficial gut microbiota. On the other hand, a diet high in fat and sugar can lead to less diverse and less beneficial gut microbiota.
- Prophylactic probiotics are used to prevent the development of diseases associated with gut dysbiosis. Prophylactic probiotics can be used in high-risk populations, such as premature infants and patients undergoing chemotherapy.
- 4.
- What are the long-term effects of manipulating the gut microbiota?
The long-term effects of manipulating the gut microbiota are not fully understood and require further research. However, some studies suggest that manipulating the gut microbiota can have differential and long-lasting effects depending on the specific intervention and the target spectrum of the intervention. Some potential long-term effects of manipulating the gut microbiota include [27]:
- Manipulating the gut microbiota with prebiotics, probiotics, or fecal transplants can improve digestive health and alleviate symptoms of functional gastrointestinal disorders.
- Manipulating the gut microbiota has been suggested as a potential strategy to prevent or treat various diseases, including metabolic disorders, inflammatory bowel disease, and Clostridioides difficile infection.
- The gut microbiota plays a crucial role in the development and regulation of the immune system. Manipulating the gut microbiota can alter immune function and potentially affect susceptibility to infections and autoimmune diseases.
- The gut microbiota is involved in the metabolism of nutrients and can affect energy balance and glucose metabolism. Manipulating the gut microbiota can potentially affect metabolism and contribute to the prevention or treatment of metabolic disorders.
- 5.
- How can we ensure the safety and efficacy of gut microbiota-related treatments?
Ensuring the safety and efficacy of gut microbiota-related treatments is crucial to their successful clinical application. Here are some strategies to ensure the safety and efficacy of gut microbiota-related treatments [28]:
- Preclinical studies can help to evaluate the safety and efficacy of gut microbiota-related treatments before they are tested in humans. Preclinical studies can include animal studies, in vitro studies, and computational modeling.
- Clinical trials are necessary to evaluate the safety and efficacy of gut microbiota-related treatments in humans. Clinical trials can include randomized controlled trials, open-label trials, and observational studies.
- The composition of gut flora is known to impact metabolism and glucose homeostasis. The relationship between gut microbiota and glycemic agents is considerably less well understood and is becoming a prominent topic of research.
- Adverse effects of gut microbiota-related treatments should be monitored closely to ensure patient safety. Adverse effects can include gastrointestinal symptoms, allergic reactions, and antibiotic resistance.
- Combining precision medicine and gut microbiota can improve drug efficacy and reduce drug toxicity. This approach involves identifying the gut microbiota composition of individual patients and tailoring treatments accordingly.
3.2.8. Challenges Associated with Gut Microbiota Therapies and Ethical Considerations
There are many hurdles when it comes to developing gut microbiota-based treatments for illnesses. These obstacles include figuring out ways to ensure the safety and effectiveness of such remedies while determining proper dosage levels and scheduling medications. Additional concerns involve pinpointing the central microbiome connected to specific afflictions and their underlying causes. Furthermore, understanding how gut microbiota interacts with additional elements like nutrition, lifestyle, and hereditary components is vital. Finally, creating techniques for administering treatments straight to the gut microbiota is necessary. However, despite these difficulties, recent research indicates great promise for utilizing gut microbiota-centered cures for numerous sicknesses, ranging from IBD (Inflammatory Bowel Disease) and cardiovascular disease to COVID-19 and ASD (autism spectrum disorder) [29].
When it comes to running clinical trials involving microbiome-based treatments, various ethical issues require careful consideration. For instance, researchers may face challenges when balancing the potential risks and benefits of the treatment for trial participants. Additionally, ensuring fair and equitable access to therapy for everyone who qualifies can be difficult. Another important concern involves sharing critical information with research participants, including any relevant medical findings discovered through microbiome testing [30]. The confidentiality of the microbiome data collected during the trial also needs to be protected. Moreover, obtaining informed consent from trial participants requires clearly explaining the potential risks and benefits associated with the microbiome-based therapy and its accompanying data collection processes. Researchers must also consider the impact on individual identity if changes occur to their microbiome composition. To address these ethical issues successfully, scientists and Institutional Review Boards (IRBs) need to cooperate in developing comprehensive analysis plans, transparent consent forms, and microbiome data management strategies that put the health and autonomy of research subjects first, while promoting meaningful scientific progress [31].
4. Conclusions
This paper is an attempt to highlight the importance of gut microbiota in human health and especially the management of diabetes. Firstly, the paper provides a bibliometric analysis of the paper indexed in PubMed. Then provides a primer on the use of gut microbiome in diabetes using a narrative review of the existing literature. The implication of this study is four prongs. Firstly, the study shows that there has been rising interest in gut microbiota among researchers and this research needs to be translated into clinical practice. Secondly, the cooccurrence analysis of extracted data shows that Gut Microbiota is strongly associated with Obesity, Type 2 Diabetes, Insulin Resistance and Metabolic Syndrome. Thirdly, the study provides the use of gut microbiome in diabetes management. Finally, the paper concluded with future research directions and possible challenges in conducting those. The finding of the paper is useful for physicians, diabetologists, dieticians, clinical researchers, and health policymakers.
Author Contributions
AM conceptualized the manuscript and was involved in the overall planning and development of the research project. PM was responsible for data collection, including the acquisition and organization of relevant research data. VM took charge of data analysis, employing tools to derive meaningful insights from the collected data. VM was involved in manuscript preparation, including the writing, and editing of sections related to data analysis and results. All authors reviewed and approved the final version of the manuscript, ensuring its scientific accuracy and integrity.
Funding
This research received no external funding.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable
Data Availability Statement
Data used in the study for bibliometric analysis can be downloaded from PubMed. The corresponding author can provide data on request.
Acknowledgments
Infrastructural support provided by Panacea Institute of Interdisciplinary Research and Education, Varanasi, India is greatly appreciated. We also thank reviewers and editors for their input and suggestions in making this manuscript publishable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ramires LC, Santos GS, Ramires RP, da Fonseca LF, Jeyaraman M, Muthu S, Lana AV, Azzini G, Smith CS, Lana JF. The Association between Gut Microbiota and Osteoarthritis: Does the Disease Begin in the Gut? International Journal of Molecular Sciences. 2022, 27;23(3):1494. [CrossRef]
- Andoh A. Physiological role of gut microbiota for maintaining human health. Digestion. 1960;93(3):176-81. [CrossRef]
- Van Eck NJ, Waltman L. VOSviewer manual. Manual for VOSviewer version. 2011.
- Baumeister RF, Leary MR. Writing narrative literature reviews. Review of general psychology. 1997 ;1(3):311-20.
- Lloyd-Price J, Abu-Ali G, Huttenhower C. The healthy human microbiome. Genome medicine. 2016;8(1):1-1. [CrossRef]
- Bashir A, Miskeen AY, Bhat A, Fazili KM, Ganai BA. Fusobacterium nucleatum. European Journal of Cancer Prevention. 2015;24(5):373-85.
- Reiss A, Jacobi M, Rusch K, Andreas S. Association of dietary type with fecal microbiota and short chain fatty acids in vegans and omnivores. J. Int. Soc. Microbiota. 2016; 1:1-9.
- Stokholm J, Blaser MJ, Thorsen J, Rasmussen MA, Waage J, Vinding RK, Schoos AM, Kunøe A, Fink NR, Chawes BL, Bønnelykke K. Maturation of the gut microbiome and risk of asthma in childhood. Nature communications. 2018 ;9(1):141. [CrossRef]
- Sonnenburg ED, Sonnenburg JL. The ancestral and industrialized gut microbiota and implications for human health. Nature Reviews Microbiology. 2019;17(6):383-90. [CrossRef]
- Tobin CA, Hill C, Shkoporov AN. Factors Affecting Variation of the Human Gut Phageome. Annual Review of Microbiology. 2023;77. [CrossRef]
- Levine A, Boneh RS, Wine E. Evolving role of diet in the pathogenesis and treatment of inflammatory bowel diseases. Gut. 2018 ;67(9):1726-38. [CrossRef]
- Siddik MA, Shin AC. Recent progress on branched-chain amino acids in obesity, diabetes, and beyond. Endocrinology and Metabolism. 2019;34(3):234-46.
- Salvi PS, Cowles RA. Butyrate, and the intestinal epithelium: modulation of proliferation and inflammation in homeostasis and disease. Cells. 2021;10(7):1775. [CrossRef]
- Gasaly N, Hermoso MA, Gotteland M. Butyrate, and the fine-tuning of colonic homeostasis: implication for inflammatory bowel diseases. International Journal of Molecular Sciences. 2021;22(6):3061. [CrossRef]
- Yang W, Cong Y. Gut microbiota-derived metabolites in the regulation of host immune responses and immune-related inflammatory diseases. Cellular & molecular immunology. 2021;18(4):866-77. [CrossRef]
- Pushpass RA, Alzoufairi S, Jackson KG, Lovegrove JA. Circulating bile acids as a link between the gut microbiota and cardiovascular health: Impact of prebiotics, probiotics, and polyphenol-rich foods. Nutrition Research Reviews. 2021:1-20. [CrossRef]
- Rajakovich LJ, Fu B, Bollenbach M, Balskus EP. Elucidation of an anaerobic pathway for metabolism of l-carnitine–derived γ-butyrobetaine to trimethylamine in human gut bacteria. Proceedings of the National Academy of Sciences. 2021;118(32): e2101498118. [CrossRef]
- Kobyliak N, Conte C, Cammarota G, Haley AP, Styriak I, Gaspar L, Fusek J, Rodrigo L, Kruzliak P. Probiotics in prevention and treatment of obesity: a critical view. Nutrition & metabolism. 2016;13(1):1-3. [CrossRef]
- Fan Y, Pedersen O. Gut microbiota in human metabolic health and disease. Nature Reviews Microbiology. 2021;(1):55-71. [CrossRef]
- Twycross J, Aickelin U. Towards a conceptual framework for innate immunity. In Artificial Immune Systems: 4th International Conference, ICARIS 2005, Banff, Alberta, Canada, August 14-17, 2005. Proceedings 4 2005 (pp. 112-125). Springer Berlin Heidelberg.
- Wu H, Esteve E, Tremaroli V, Khan MT, Caesar R, Mannerås-Holm L, Ståhlman M, Olsson LM, Serino M, Planas-Fèlix M, Xifra G. Metformin alters the gut microbiome of individuals with treatment-naive type 2 diabetes, contributing to the therapeutic effects of the drug. Nature medicine. 2017 ;23(7):850-8. [CrossRef]
- Kant R, Chandra L, Verma V, Nain P, Bello D, Patel S, Ala S, Chandra R. Gut microbiota interactions with anti-diabetic medications and pathogenesis of type 2 diabetes mellitus. World Journal of Methodology. 2022;12(4):246. [CrossRef]
- Khan I, Ullah N, Zha L, Bai Y, Khan A, Zhao T, Che T, Zhang C. Alteration of gut microbiota in inflammatory bowel disease (IBD): cause or consequence? IBD treatment targeting the gut microbiome. Pathogens. 2019 ;8(3):126. [CrossRef]
- Liang D, Leung RK, Guan W, Au WW. Involvement of gut microbiome in human health and disease: a brief overview, knowledge gaps, and research opportunities. Gut pathogens. 2018;10(1):1-9. [CrossRef]
- Chen J, He X, Huang J. Diet effects in gut microbiome and obesity. Journal of food science. 2014;79(4): R442-51. [CrossRef]
- Yamashita T, Emoto T, Sasaki N, Hirata KI. Gut microbiota and coronary artery disease. International heart journal. 2016;57(6):663-71. [CrossRef]
- Scott KP, Jean-Michel A, Midtvedt T, van Hemert S. Manipulating the gut microbiota to maintain health and treat disease. Microbial ecology in health and disease. 2015;26(1):25877. [CrossRef]
- Wong SH, Yu J. Gut microbiota in colorectal cancer: mechanisms of action and clinical applications. Nature Reviews Gastroenterology & Hepatology. 2019;16(11):690-704. [CrossRef]
- Zhang X, Cai X, Zheng X. Gut microbiome-oriented therapy for metabolic diseases: challenges and opportunities towards clinical translation. Trends in Pharmacological Sciences. 2021;42(12):984-7. [CrossRef]
- Ma Y, Liu J, Rhodes C, Nie Y, Zhang F. Ethical issues in fecal microbiota transplantation in practice. The American Journal of Bioethics. 2017 ;17(5):34-45. [CrossRef]
- Zhang F, Zhang T, Zhu H, Borody TJ. Evolution of fecal microbiota transplantation in methodology and ethical issues. Current opinion in pharmacology. 2019 ;49:11-6. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions, and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. |
Figure 1.
Trend of Research Interest on Gut Microbiota in Diabetes Source: Author’s Compilation.
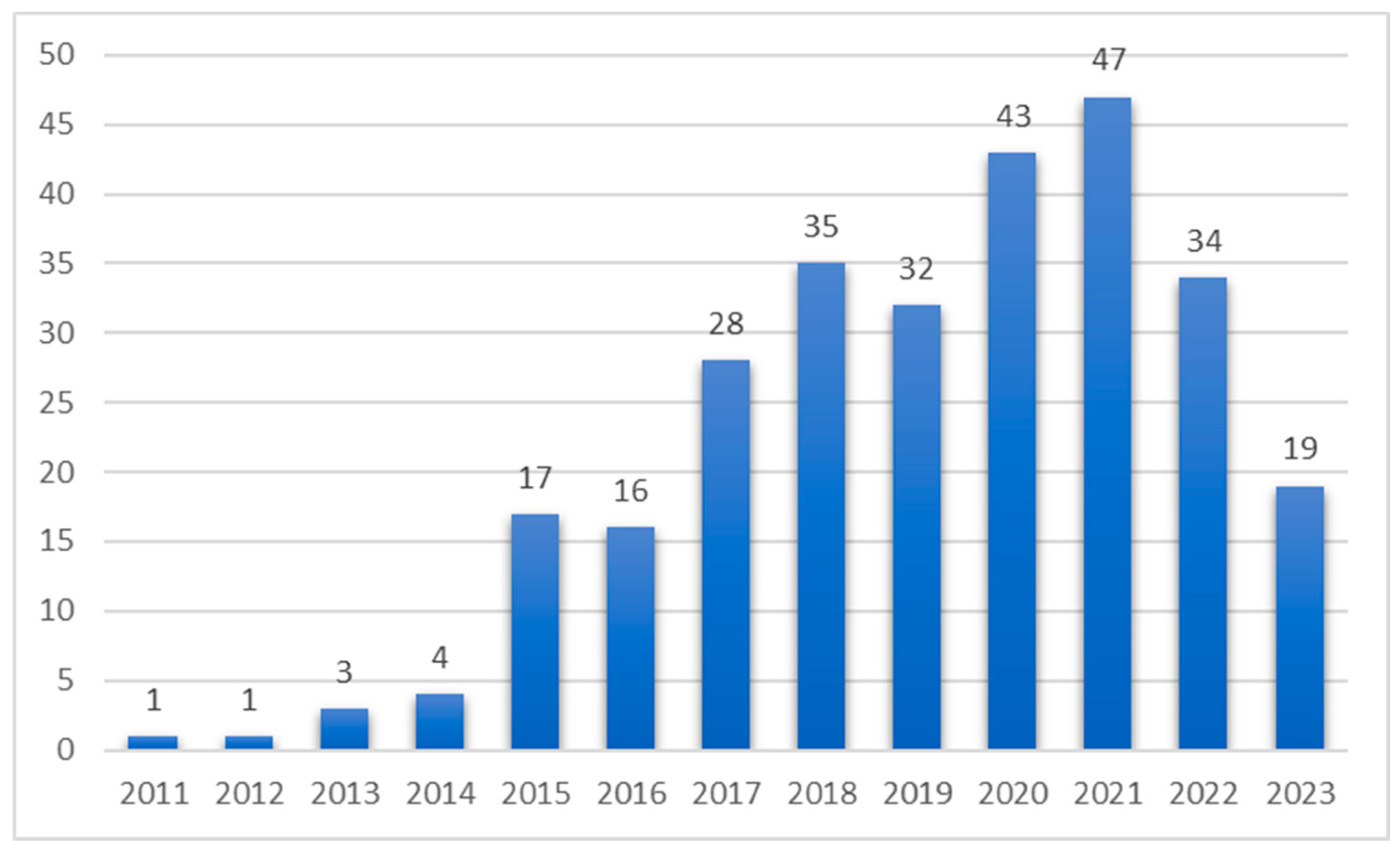
Figure 2.
Cooccurrence Analysis of Keywords Used in the Extracted Data Source: Author’s Compilation based on VOSviewer Output.
Figure 2.
Cooccurrence Analysis of Keywords Used in the Extracted Data Source: Author’s Compilation based on VOSviewer Output.

Figure 3.
Coauthorship Analysis of Authors Involved in the Extracted Data Source: Author’s Compilation based on VOSviewer Output.
Figure 3.
Coauthorship Analysis of Authors Involved in the Extracted Data Source: Author’s Compilation based on VOSviewer Output.
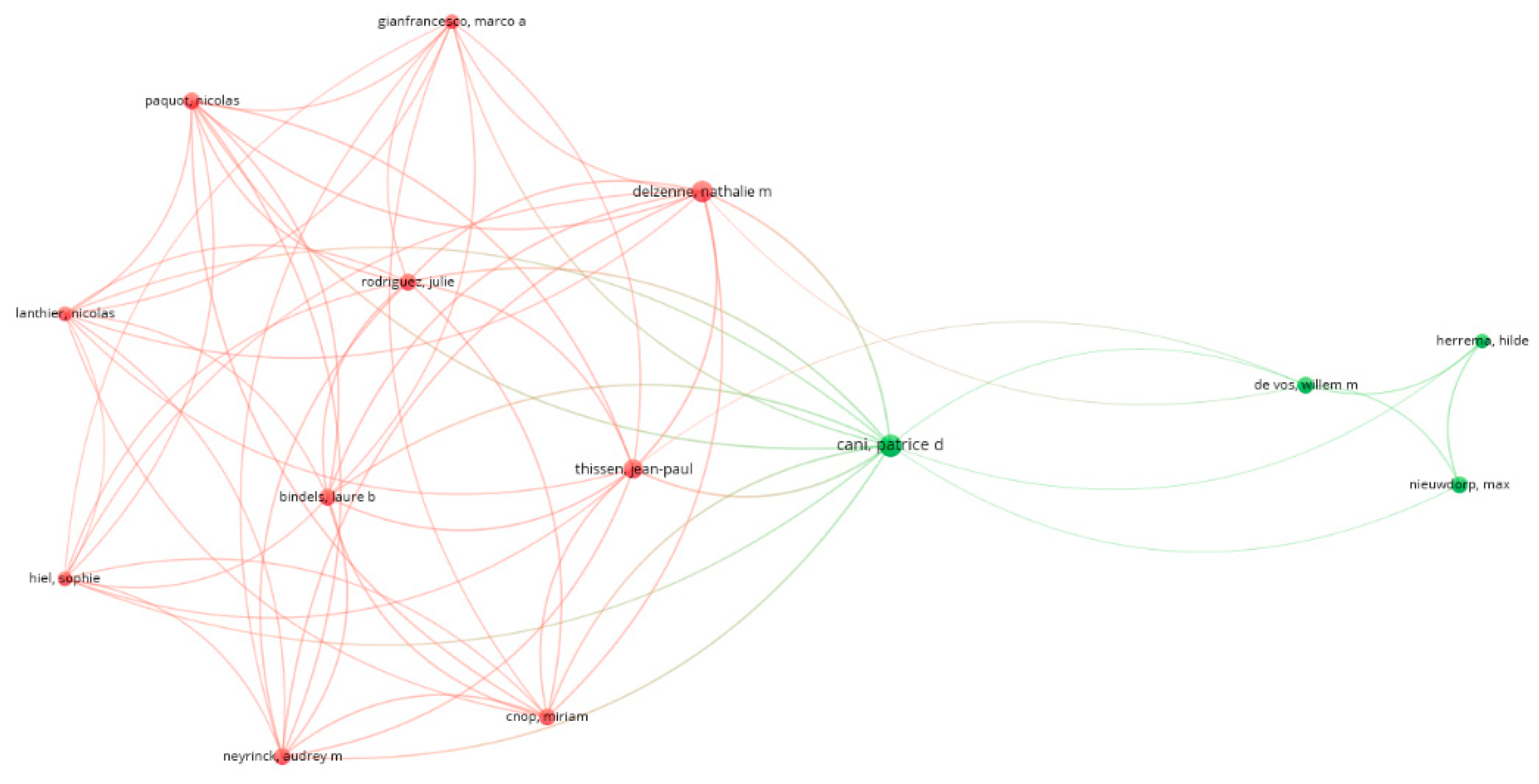
Figure 4.
Use of Diversified Microbiota in Fermentation of Complex Carbohydrates Source: Author’s Compilation. Note: IR: Ionizing radiation, FABP-4: Fatty Acid-Binding Protein 4, TLR-2: Toll-like receptor 2, LPS: Lipopolysaccharide, SCFA: Short-Chain Fatty Acids, HIF: Hypoxia-Inducible Factor and IL-1B: Interleukin-1 Beta.
Figure 4.
Use of Diversified Microbiota in Fermentation of Complex Carbohydrates Source: Author’s Compilation. Note: IR: Ionizing radiation, FABP-4: Fatty Acid-Binding Protein 4, TLR-2: Toll-like receptor 2, LPS: Lipopolysaccharide, SCFA: Short-Chain Fatty Acids, HIF: Hypoxia-Inducible Factor and IL-1B: Interleukin-1 Beta.
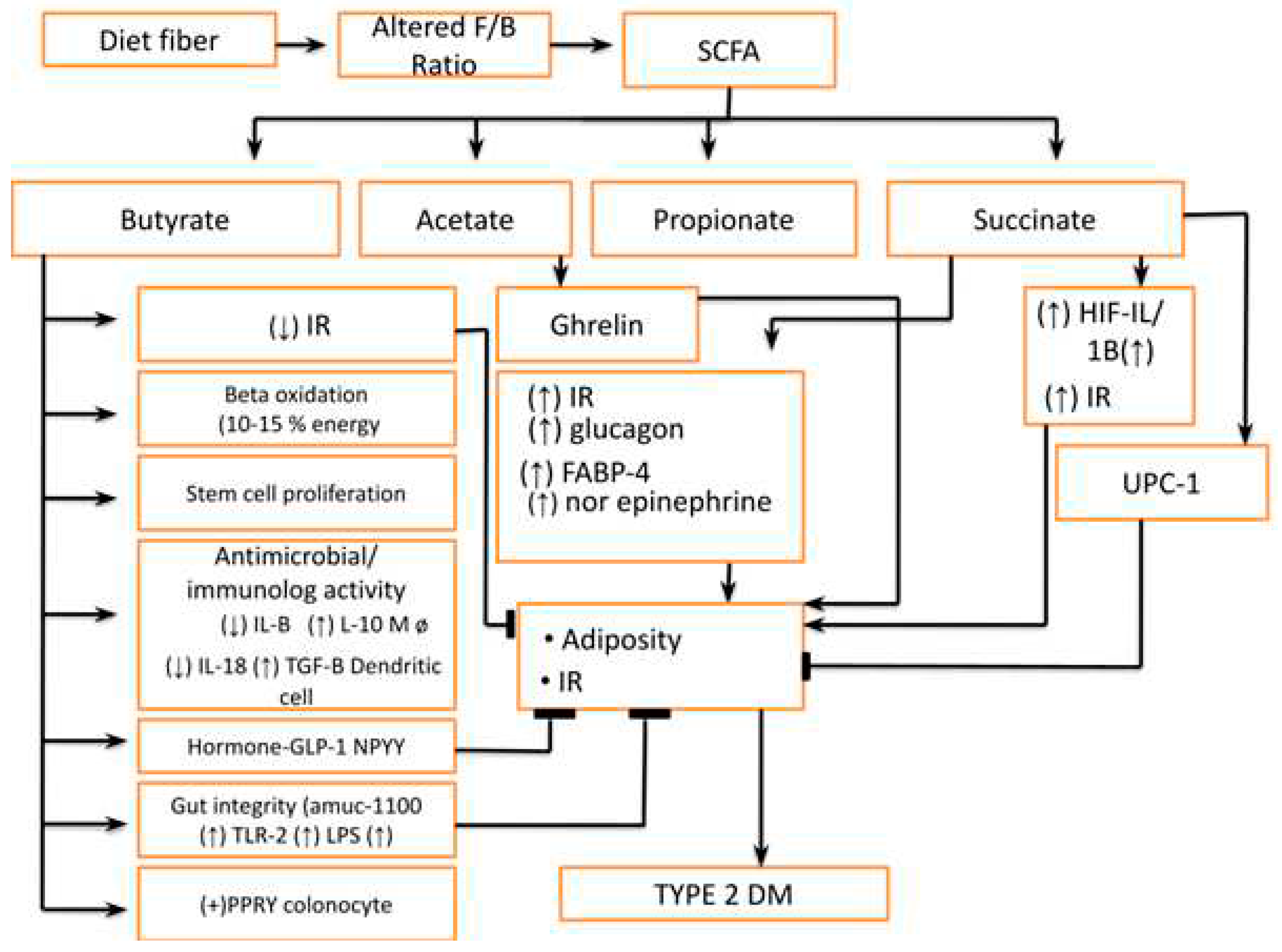
Figure 5.
Mechanism for Abnormality in SCFA Production Source: Author’s Compilation.
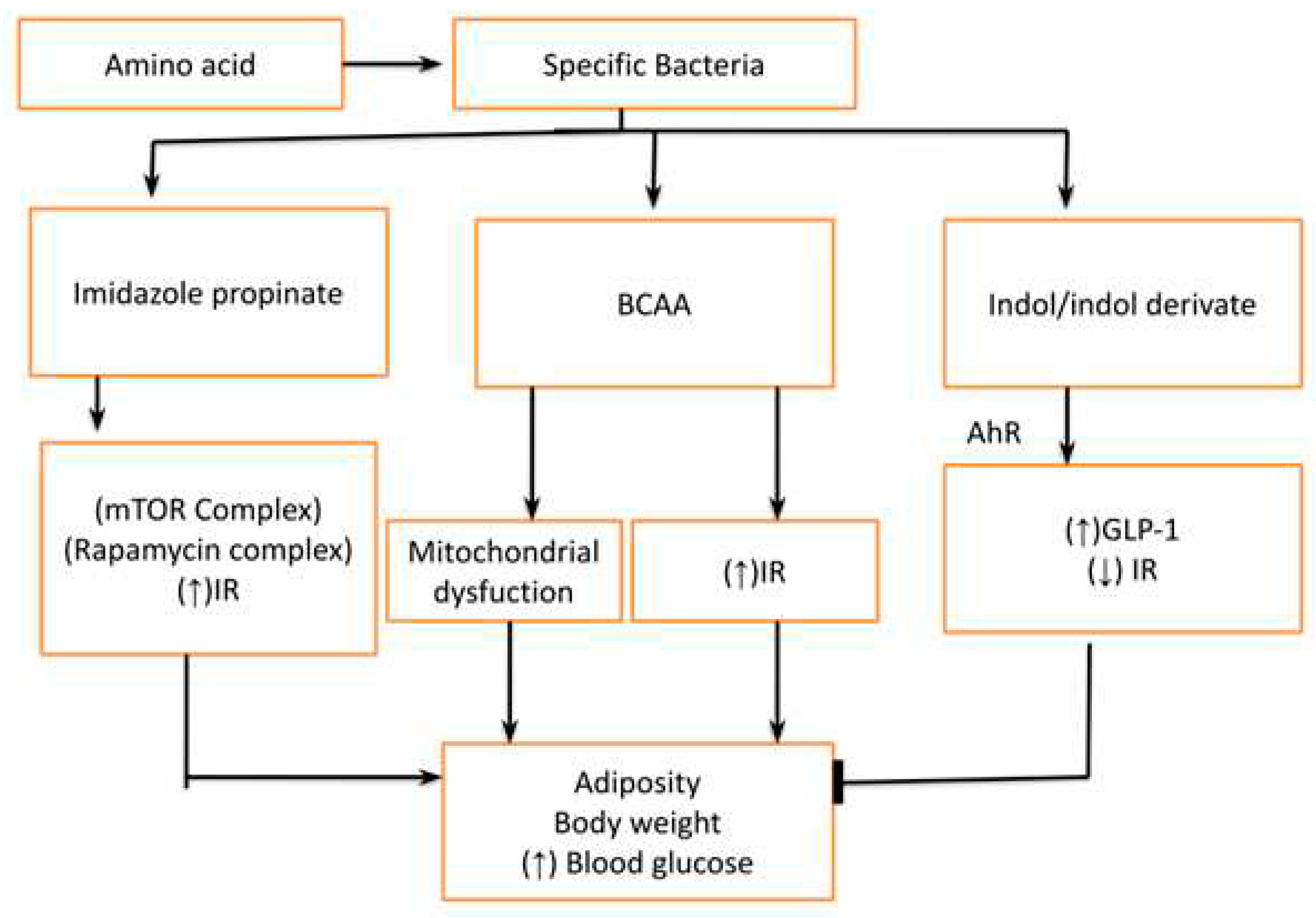
Figure 6.
Primary and Secondary Bile Acids have a role in regulating host Metabolism. Source: Author’s Compilation.
Figure 6.
Primary and Secondary Bile Acids have a role in regulating host Metabolism. Source: Author’s Compilation.
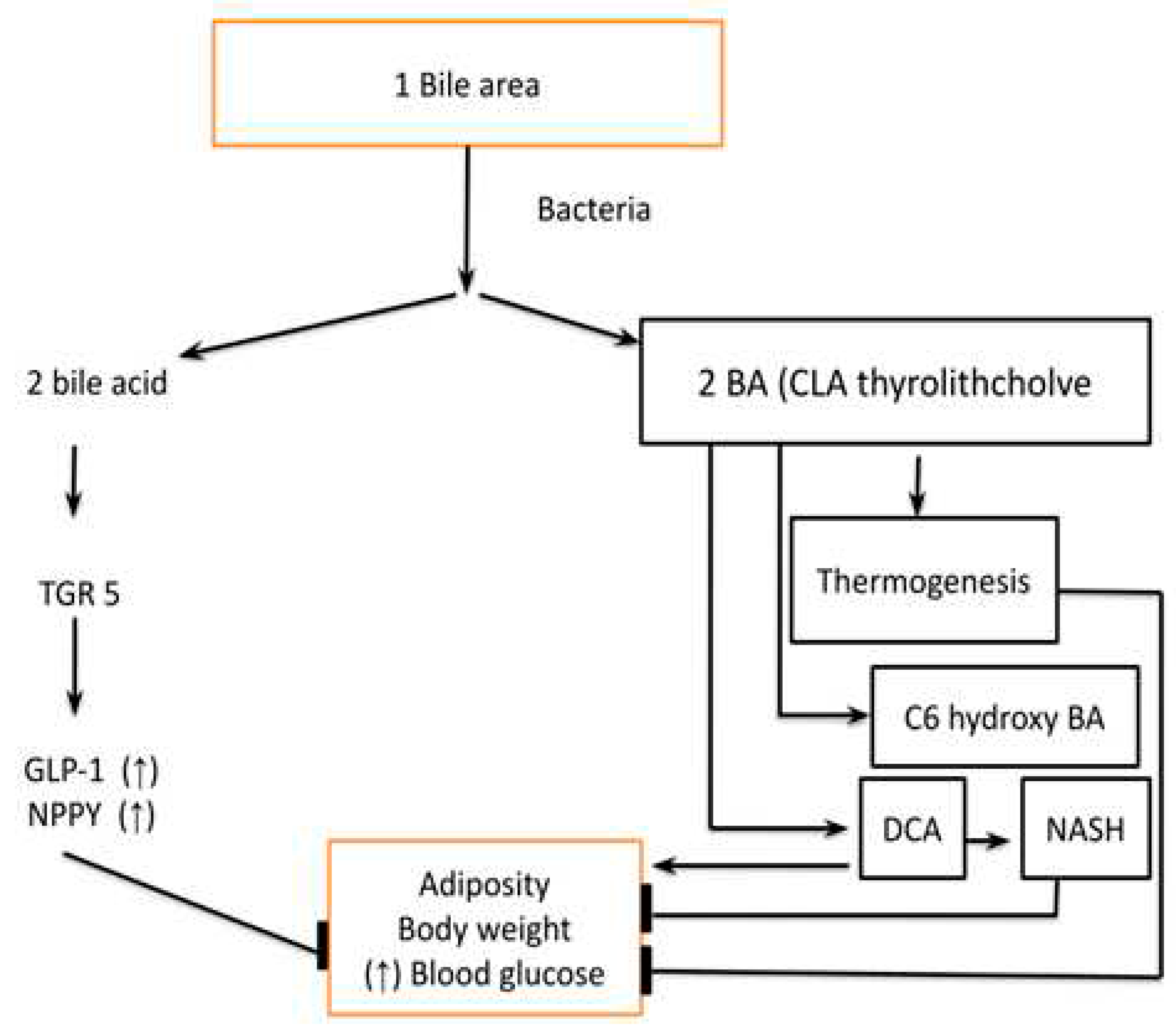
Figure 7.
(a) Phosphatidylcholine and L-carnitine-derived Metabolites, 7(b) Critical Bacterial Products in Management of Diabetes. Source: Author’s Compilation
Figure 7.
(a) Phosphatidylcholine and L-carnitine-derived Metabolites, 7(b) Critical Bacterial Products in Management of Diabetes. Source: Author’s Compilation
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



