
Submitted:
15 June 2023
Posted:
16 June 2023
You are already at the latest version
Abstract
Emerging organic contaminants (EOCs) of anthropogenic origins are ubiquitous in environmental compartments, including aquatic systems. Thus, EOCs have attracted considerable research and public attention due to their potential human and ecological health risks. However, compared to other aquatic environments such as wastewater systems, comprehensive reviews focussing on the occurrence and human health risks of EOCs in drinking water systems are still lacking. Therefore, to address this knowledge gap, the current review posits that drinking water systems harbour a cocktail of toxic EOCs, which pose public health risks via multiple exposure routes. In the present review, global evidence is examined to track EOCs along the source-pathway-receptor-impact-mitigation (SPRIM) continuum. Evidence shows that, various groups of EOCs, including pharmaceuticals and personal care products, solvents, plasticizers, endocrine disrupting compounds, gasoline additives, per- and polyfluoroalkyl substances (PFAS), food colourants, artificial sweeteners, and musks and fragrances, have been detected in drinking water systems. The anthropogenic sources of EOCs detected in drinking water systems, including wastewater systems and industrial emissions, are summarized. Further, the behaviour and fate of EOCs in the drinking water systems, including removal processes are discussed. Once in drinking water systems, human exposure to EOCs may occur via ingestion of contaminated drinking water and cooked foods, and possibly dermal contact and inhalation. The high-risk environments, and risk factors and behaviours predisposing humans to EOC exposure are discussed. Evidence on the human health risks of the various EOCs and a critique of the data are presented. Notably, besides inferential data, quantitative epidemiological evidence directly relating the occurrence of EOCs in drinking water systems to specific adverse human health outcomes is still scarce. Lastly, future research directions, including the need for quantitative public health risk assessment, and the application of emerging detection tools are discussed.
Keywords:
Human exposure
; high-risk environments
; human health hazards
; personal care products
; pharmaceuticals
; per- and polyfluoroalkyl substances
; risk factors
1. Introduction
Emerging organic contaminants (EOCs) is a diverse group comprising of various classes, including pharmaceuticals and personal care products (PPCPs), solvents, plasticizers, endocrine-disrupting compounds, gasoline additives, food colourants, artificial sweeteners, per- and polyfluoroalkyl substances (PFAS), and musks and fragrances [1]. EOCs are extensively used in industrial and household chemicals, personal care products, the food industry, and pharmaceuticals for animal and human healthcare [2]. Because they potentially pose public health risks, EOCs have received considerable research and public attention mainly in developed countries and to a relatively smaller degree, in low-income countries (LICs) [3,4,5,6].
To date, a large body of evidence exists on EOCs in various environmental systems, including soils, aquatic systems, biota, and atmosphere [1,3,4,5,6,7]. However, compared to other aquatic compartments, studies on aquatic environments, particularly wastewater systems, still dominate the literature on EOCs. For example, there are several research articles and reviews on the occurrence, behaviour, and fate of EOCs in wastewater [8,9,10]. Others have also investigated the ecological risks posed by EOCs in surface aquatic systems and marine bio-assay organisms [2,11,12].
EOCs in drinking water systems (DWS) have also received some research attention from as early as the 2000s, and several studies have detected various classes of EOCs in drinking water systems [3,13,14,15]. In the context of the present review, drinking water systems include: (1) surface water and groundwater serving as drinking water sources, (2) drinking water treatment systems, (3) drinking water storage and distribution systems, (4) untreated or treated water at the point of use, including tap water, and (5) bottled natural, mineral or treated water. To date, several studies have reported EOCs in drinking water systems (DWS) in a number of countries [3,13,14]. For instance, 49 different EOCs and their metabolites were detected in a DWTP at a total concentration in the range of 1600–4200 ng/L was recorded [16]. Tap water analysed in different housing topologies in Malaysia had bisphenol A of approximately 66.40 ng/L (high-rise housing), sulfamethoxazole, and caffeine [17]. The existence of neonicotinoids in drinking water sources has been reported in Hangzhou China [18]. The identified neonicotinoids include immidacloprid, acetamiprid, and clothianidin with concentrations of 11.9, 17.6, and 7.6 ngL-1 respectively. However, DWTPs have been shown to remove about 50% of surface water-derived neonicotinoids.
However, compared to data on wastewater systems, the corresponding original studies and reviews focusing on DWS are still relatively limited. The limited research on EOCs in DWS could be attributed to the previously held notion that the occurrence and health risks of EOCs in these aquatic systems could be low relative to that of wastewater systems. Yet drinking water represents one of the most direct human exposure and intake routes for EOCs. Recent evidence showing that drinking water systems also harbour diverse classes of emerging contaminants of anthropogenic origins [3,13,14] points to the need for comprehensive research on the topic.
Despite increasing evidence showing EOCs in DWS, comprehensive reviews on their occurrence, behaviour, fate and human health risks are still scanty relative to those on wastewater environments. To address this knowledge gap, the current review posits that drinking water systems harbour a cocktail of toxic EOCs, which pose human health risks via multiple exposure routes. In the present review, global evidence is examined to track EOCs along the source-pathway-receptor-impact-mitigation (SPRIM) continuum [1,19]. As pointed out in earlier papers, unlike reviews focusing on a few aspects such as occurrence and fate, the application of the SPRIM continuum framework enables the identification of well-studied as well as under-studied aspects of EOCs in the drinking water systems [1]. In this regard, the SPRIM continuum framework provides a comprehensive review of EOCs in drinking water systems.
This review seeks to: (1) present a summary of the occurrence, sources, behaviour, fate and removal processes of EOCs in drinking water treatment systems, (2) discuss human exposure routes, and high-risk settings and factors predisposing humans to EOC in drinking water systems, (3) discuss and critique the evidence on human health risks of EOCs, and (4) propose future research directions, including key knowledge gaps. The point sources, occurrences, and distribution of EOCs among drinking water sources are summarized in Figure 1.
2. Materials and Methods
The current study used a hybrid approach that included quantitative and qualitative methodologies. Using a Boolean search approach, literature from English language scholarly databases that include Google Scholar, ScienceDirect, Web of Science, and Scopus was searched and retrieved. In this case, the Boolean search strategies restricted and extended the search by combining search strings with search operators and modifiers including NOT, AND, and OR. This particular method allowed for the retrieval of the majority of literature relevant to the study objectives, although it may have omitted additional publications published in languages other than English. The individual articles were then subjected to a preliminary qualitative screening and evaluation based on the study objectives. Nevertheless, there was limited evidence of contamination of drinking by emerging contaminants before 2000, therefore subsequent searches were restricted to the period 2000 to 2023.
A brief overview of the Boolean search approach and representative strings of search phrases applied in this current study are summarized here. Specifically, the search strings included the following; (i) ‘emerging organic contaminants AND/OR drinking water systems’, (ii) ‘emerging organic contaminants AND/OR drinking water’, (iii) ‘emerging organic contaminants AND/OR occurrence in drinking water’, (iv) emerging organic contaminants AND/OR fate in drinking water’, (v) emerging organic contaminants AND/OR behaviour in drinking water’, (vi)‘emerging organic contaminants in drinking water AND/OR human exposure’, (vii) emerging organic contaminants in drinking water AND/OR human exposure pathway’, and (viii) Emerging organic contaminants AND/OR human health risks’.
Following the preliminary screening and analysis, relevant publications on the occurrence and public health risks emanating from drinking water-derived emerging organic contaminants were retained for further examination. The remaining publications were thoroughly reviewed, and the major findings were summarized in Tables 1 - 5. A completely systematic quantitative review employing bibliometric and meta-analysis methodologies was beyond the scope of the current.
3. Occurrence of Emerging Organic Contaminants in Drinking Water Systems
EOCs have been reported in several DWS, including groundwater, surface waters, water treatment systems, and water samples at the point of consumption (e.g., tap water) (Table 1, Table 2 and Table 3). The EOCs in DWS originate from many environmental sources, such as wastewater treatment plants (WWTPs), industrial sources, and on-site sanitation systems such as pit latrines and septic tanks (Figure 1). Because inputs often exceed the rates of their transformation and removal, EOC concentrations may persist or pseudo-persist in aquatic environments, including DWS. In this section, a comprehensive overview of the occurrence and fate of various EOCs in drinking water systems is given.
The occurrence of EOCs in DWS has been reported globally (Table 1). Whereas a considerable body of literature exists in developed countries [20,21], there are limited studies in LICs like those in Africa. However, challenges concerning water scarcity are frequently worse than in more developed countries. For instance, only a small number of open-access publications exist that describe the occurrence of EOCs in DWS in Africa, and these publications are only available for seven of the possible 54 countries in Africa, which is low. The few studies that have been conducted, however, have shown that there is a serious problem with EOCs in drinking water sources in Africa and other LICs (Table 1). Among other factors, the lack of highly sensitive and sophisticated analytical equipment necessary for such studies may be the cause of the limited data on the occurrence of EOCs in DWS in Africa and other LICs [22]. The equipment is also expensive and requires specialists to operate and maintain, which is a barrier to their availability in many LICs [23]. Some studies on emerging contaminants in groundwater sources in Africa were conducted by research groups from outside Africa. For example, in a study by Sorensen et al. [24], samples from Zambia were freighted to the UK for analysis by the UK Environment Agency National Laboratory Services.
Another reason for the lack of data representation on EOCs in DWS in LICs could be poor data management. In general, most African countries lack a national water quality database. Only detailed periodic surveys of specific water bodies conducted by specialist programs or donor-sponsored projects provide a reliable source of primary data [25]. The majority of the studies cited in Africa were reported by individuals or research teams in educational and research institutions. Similar to the scenario for the occurrence of EOCs in DWS, the dearth of data is much more severe with regard to ecological and public health risks [26]. Several studies have speculated on the reasons for this, and they all reflect weak research systems in LICs [4,8,26,27]. In subsequent sections, data on the various EOCs detected in DWS are presented.
3.1. Pharmaceuticals
When pharmaceutical compounds are released into the environment; they may end up in DWS (Table 1). Various classes of pharmaceutical compounds detected in DWS; include antibiotics [20; 21], analgesics [28], psychiatric drugs [29], stimulants [30], antidepressants [31], anticonvulsants, diuretics [32], and many others. In comparison to other classes of pharmaceutical compounds; several studies have shown that antibiotics are frequently detected in drinking water systems [20,21,33,34]. For example; erythromycin; roxithromycin; ciprofloxacin; ofloxacin; sulfadiazine; sulfamethoxazole; and oxytetracycline were detected in Chinese drinking water sources at frequencies of 20–100% and concentrations of <118.60 ng/L [21]. In a another study, ciprofloxacin (8.69 ng/L) and sulfamethoxazole (0.90 ng/L) were detected in both river water and tap water in Malaysia [34]. A related study in Hungary detected 19 pharmaceutical compounds in tap water with mean concentrations exceeding 30 ng L−1 [35]. With a mean concentration of 8.9 ng L−1, carbamazepine was the most frequently detected. Notably, the presence of pharmaceutical compounds in tap water indicates that the ineffectiveness of the water treatment methods. The removal of pharmaceutical compounds is important as some are linked to significant toxicological hazards, and pose public health risks [36]. Therefore, to safeguard public health, the development of innovative water treatment technologies capable of removing pharmaceutical compounds and other ECs should be a priority.
The detection of analgesics in DWS almost follows the trend of antibiotics (Table 1). Several studies reported the presence of analgesics (e.g., ibuprofen, dexamethasone, diclofenac, and naproxen) in DWS [21,34,37]. Ibuprofen, for instance, was detected in 60% of Colombia's raw water reservoirs [38]. Most importantly, the drug was still present, albeit at low concentrations (40 ng/L), in treated water, demonstrating that the EOCs cannot all be removed by the existing conventional treatment methods. In other studies, ibuprofen was detected in groundwater in Pakistan at a concentration of 154 ng/L [28], while diclofenac was detected in Germany river water at concentrations of up to 15 µg/L. Although the concentrations may seem too low to have any pharmacological effects on humans, chronic exposure could pose potential risks [39]. Moreover, pharmaceutical compounds may even have adverse effects at low concentrations, because they are designed to have therapeutic effects even at low concentrations.
Antibiotics, painkillers, stimulants, antidepressants, anti-hypertensives, hormones, and PPCP metabolites have also been reported in aquatic systems [40,41]. Other antibiotics such as ciprofloxacin, ampicillin, nalidixic acid, sulfamethoxazole, streptomycin, tetracycline, erythromycin, chloramphenicol, dihydrostreptomycin, kanamycin, apramycin, and tylosin, have been detected in DWS [40,42,43]. However, their concentrations in water vary with time and location. For example, antibiotics in the range of 0.21-25.6 μg/L were detected along the Umgeni River in South Africa [42]. A related study reported the occurrence of antibiotics in surface waters in Fez-Morocco with amoxicillin, erythromycin, sulfamethoxazole, tetracycline, ciprofloxacin, oxolinic acid, trimethoprim having concentrations in the range of 0.0019–4.107 μg/L [44]. Furthermore, higher concentrations (3.4–18.4 μg/L) were detected in Tunisian groundwater [43], indicating that they can contaminate drinking water sources. Besides occurring in drinking water sources, antibiotics have been detected in bottled and sachet water [45], posing threats to human health.
Notably, developed countries reported the majority of the findings, while limited research has been conducted in low-income countries, including Africa (Table 1). One study in Nigeria revealed considerable concentrations of amoxicillin, acetaminophen, nicotine, ibuprofen, and codeine in drinking bottled water, groundwater (wells and boreholes), and surface waters . More significantly, all the waters contained amoxicillin in the range of 1614, 238 - 358 ng/L. Similarly, ribavirin and famciclovir, which are antiretroviral drugs, were at 0.042 ng/mL and 0.055 ng/mL, respectively in South African drinking water [46]. Compared to other African countries, South Africa has a relatively larger number of studies on EOCs in DWS [46,47]. This may be due to the fact that South Africa is an upper-middle-income economy, which has research funding resources and relatively advanced research infrastructure to undertake such studies. The paucity of funding for such studies and the absence of advanced analytical facilities to detect such contaminants at a large scale may be the reason for the few investigations on the detection of pharmaceuticals in DWS in most LICs.

Table 1.
Pharmaceuticals as emerging organic contaminants in drinking water systems.
| Country | EOCs | Drinking Water System | Key results and Remarks | References |
|---|---|---|---|---|
| China | Antibiotics (trimethoprim, sulfadimidine, sulfadiazine, sulfamethoxazole, sulfachloropyridazine, norfloxacin, ciprofloxacin and enrofloxacin) | Groundwater | Antibiotics (0.44 -45.40 ng/L), at detection rates from 1.23%-95.06%. Contaminated groundwater with mixes of pharmaceuticals can act as potential drivers of antibiotic resistance in human beings | [20] |
| Zambia | Caffeine | Groundwater (shallow wells and boreholes) | Caffeine was detected in both shallow wells and borehole water at concentrations less than 0.17ng/L. The findings could not pose any risk but continuous exposure to the contaminant even at low concentrations is a cause for concern | [24] |
| China | Sulfamethoxazole | Tap water | The highest concentrations of 0.69 ng/L were detected. Detection frequencies ranged between 20–100% of sampled water. Water treatment methods failed to remove the EOCs. Long term exposure through ingestion is a concern for antibiotic resistance | [21] |
| China | Erythromycin, roxithromycin, ciprofloxacin, ofloxacin, sulfadiazine, sulfamethoxazole, oxytetracycline, ibuprofen, and naproxen. | Drinking water sources | All 9 pharmaceuticals were detected with frequencies of 20–100% and concentrations of <LOQ–118.60 ng/L. Long-term ingestion and exposure to the compounds raises concerns about antibiotic resistance. | [48] |
| Malaysia | Dexamethasone, Primidone, Propranolol, Ciprofloxacin, Sulfamethoxazole, Diclofenac | Tap water and river water | Pharmaceuticals were detected in both river water and tap water. Dexamethasone (2.11ng/L), Primidone (2.99 ng/L), Propranolol (0.69 ng/L), Ciprofloxacin (8.69 ng/L), Sulfamethoxazole (0.90 ng/L), and Diclofenac (21.39 ng/L) detected in tap water. | [34] |
| Nigeria | Amoxicillin, acetaminophen, nicotine, ibuprofen, and codeine | Surface waters, groundwater samples (wells and boreholes) and drinking bottled water samples | Amoxicillin: 238, 358, and 1614 ng/L in groundwater, drinking water, and surface water. Detection frequencies for acetaminophen, codeine, ibuprofen, and nicotine exceeded 70%. Chronic exposure to these drug mixtures warrants more inquiry into the potential health consequences of such inadvertent exposure. | [45] |
| South Africa | Ibuprofen, caffeine, paracetamol, efavirenz, paraxanthine | Influent water, WWTP effluent water | The pharmaceuticals present in influent and effluent, with concentrations ranging from < ILOQ-14.2 μg L−1 and < ILOQ - 2.45 μg L−1, respectively. The maximum concentrations recorded in the effluent water including river water samples were for ibuprofen, (4.14 μg L−), caffeine (2.98 μg L−1), paraxanthine (1.22 μg L−1), and efavirenz (0.58 μg L−1). These findings show that the contaminants were not completely removed by the conventional water treatment methods. | [47] |
| South Africa | Antibiotics, antipyretics, atenolol, bezafibrate, and caffeine | river water | All the pharmaceuticals were present in discharged treated water (river water) with concentrations of most drugs below 10 μg/L. | [49] |
| South Africa | Naproxen, ibuprofen | treated effluent water | The compounds were detected with average concentrations in the treated effluent ranging from 10.7 - 24.6 µgl.-1 | [50] |
| South Africa | Antiretroviral drugs (ribavirin, famciclovir) | influent water, treated drinking Water | Both drugs were found in both influent water and treated drinking water. The concentrations of ribavirin and famciclovir in influent water were 19.60 ng/mL and 19.00 ng/mL, respectively. In treated water it was 0.042 ng/mL and 0.055 ng/mL, respectively. | [46] |
| China | Different pharmaceuticals (e.g., antibiotics, angiotensin ii receptor blockers, diuretics, anticonvulsants) | tap water | Detection frequencies exceeded 80%. 4-acetaminopyrine (48.16 ng/L), florfenicol (84.56 ng/L), hydrochlorothiazide (33.13 ng/L), irbesartan (38.35 ng/L), primidone (32.85 ng/L, thiamphenicol (101.54 ng/L), and valsartan (66.84 ng/L), | [32] |
| Czech Republic | Ibuprofen, carbamazepine, naproxen, and diclofenac | WWTP effluent | Detection frequency: ibuprofen > carbamazepine > naproxen > diclofenac. Concentrations: 0.5-20.7 ng/L. Sampling points were at public water systems that serve 50.5% of the Czech population, and this could pose health risks to over half of the population. | [37] |
| Germany | Diclofenac | river water samples | Detected in 10 out of 27 water samples in concentrations of up to 15 μg/L. The concentrations are very low not to cause pharmacological effects in man but continuous exposure could have some potential risks. | [39] |
| Germany | Clofibric acid, Ibuprofen, Gemfibrocil, Fenoprofen, Indomethacin, Ketoprofen and Sarkosin-N-(phenylsulfonyl) (SPS) ng/L | pond and river water samples | At least one of the compounds was detected in 25 of 27 water samples in ng/L. The most frequently detected substance was SPS. Most are excreted after oral intake and were mostly found in rivers with direct connection to sewage plants. | [39] |
| Malaysia | Ciprofloxacin and amoxicillin | drinking water | Ciprofloxacin was found at the greatest quantity (0.667 ng/L), whereas amoxicillin was found at the lowest (0.001 ng/L). The long exposure through consumption of such water has potential risks | [33] |
| Hungary | Pharmaceutically active compounds (PhACs) | tap water | 19 PhACs were detected in tap water samples with a total mean concentration exceeding 30 ng L−1 only at 5 sites. The frequently detected PhAC, carbamazepine (54 % of the samples) had 8.9 ng L−1 as the mean concentration. Travel distance between drinking water wells decreased the PhAC concentrations. | [35] |
| Brazil | Pharmaceutically active compounds | surface and drinking water samples | Trace concentrations detected. Betamethasone, fluconazole, and prednisone, were most frequent, and had the greatest concentrations. Some PhACs were linked to significant toxicological hazards; as a result, such water consumption could be harmful to people's health. | [36] |
| China | Ibuprofen | tap water | The highest concentrations of 1.28 ng/L were detected. Detection frequencies ranged between 20–100% of sampled water. | [21] |
| Pakistan | Ibuprofen | ground water | Detected at 154 ng/L. Domestic wastewater discharge, hospital waste, and animal husbandry have all been identified as major sources of groundwater contamination. | [28] |
| Colombia | Ibuprofen | water reservoirs | Ibuprofen was detected in almost 60% of the reservoir water samples. The analgesic was still present in the treated water from the reservoir but at low doses (40 ng/L). Conventional treatment methods cannot remove all the EOCs. | [38] |
| China | Psychiatric pharmaceuticals (carbamazepine, diazepam, oxazepam, lorazepam, and alprazolam) | River water; treated water | Oxazepam, diazepam, lorazepam, and carbamazepine were at ng L−1 -75.5 ng L−1 in river water. Alprazolam (2.3 ng L−1), diazepam (0.5–3.2 ng L−1), and carbamazepine (0.8–2.5 ng L−1) were detected in treated water. | [29] |
| Brazil | Caffeine | drinking water | Caffeine concentrations in drinking water ranged from 1.8 ng L− 1 to 2.0 μg L− 1, while source water concentrations were at 40 ng L− 1 - 19 μg L− 1. Since caffeine is a substance with anthropogenic origins, its presence in treated water shows that domestic sewage was present in the source water. | [30] |
| Poland | Antidepressants (citalopram, mianserin, sertraline, moclobemid and venlafaxine) | tap water | citalopram (≤1.5 ng/L), moclobemid (≤0.3 ng/L), sertraline (<3.1 ng/L), mianserin (≤0.9 ng/L), and venlafaxine (≤1.9 ng/L). Their presence in tap water demonstrates an insufficient removal in the drinking water treatment facility and this could have long-term consequences, since pharmaceutical pollutants can synergize. | [31] |
| United Kingdom | Pharmaceutical of abuse (Fluoxetine, methamphetamine, ketamine) | drinking water | Concentration was between 0.14 and 2.81 ng/L. Since the presence of these pharmaceuticals has an impact on public health, identifying them is crucial when examining water quality. | [51] |
| Uganda | Various pharmaceuticals | surface water, and groundwater samples | Detected in water samples with concentrations similar to previous documented studies in SA. | [52] |
| Uganda | Ampicillin and benzylpenicillin | shallow groundwater | Both antibiotics were detected although at low concentrations to cause direct harm to human health. However, chronic exposure could lead to a proliferation of antibiotic resistance genes. | [53] |
| Kenya | pharmaceutically active compounds (PhACs) | groundwater wells | Fourteen PhACs were detected. Anti(retro)virals, were more prevalent PhACs, with nevirapine concentrations ≤700 ng/L. | [54] |
| Zimbabwe | Topiramate, thiabendazole-13C6, p-hydroxynobenzphetamine-2TFA, 4-imadazolidinone, and 5-(phenylmrthyl)-2-thioxo | river water and sediment | Topiramate was detected in river water, whilst the other drugs were found in the river sediment. The concentration of pharmaceuticals especially in sediments was at 0.01 to 0.29 mol/µl. | [55] |
3.2. Personal Care Products
Several studies have documented the existence of various personal care products in DWS, particularly in middle or high-income countries (Table 2). For example, triclosan and bisphenol A at concentrations of 9.74 ng/L and 66.40 ng/L, respectively were detected in tap water in Malaysia [34]. Another study conducted in China detected propylparaben, bisphenol A, and dicyclohexylamine in tap water with frequencies over 80% and concentrations of 47.50 ng/L, 31.51 ng/L, and 42.33 ng/L, respectively [32]. In addition to tap water, personal care products have also been reported in other DWS (Table 1). For instance, benzophenone and methyl paraben were reported in treated water and in reservoirs for drinking water treatment facilities [38]. However, both pollutants occurred in treated water at low concentrations (40 ng/L). Similar to other EOCs, data on personal care products in DWS is extremely scarce in LICs. Nonetheless, the few studies concur with those conducted in developed countries. For instance, a study in South Africa reported triclosan in treated effluent water. Triclosan was found with an average concentration of 10.7 to 24.6 gL-1 [50]. More significantly, the outcomes of the studies on personal care products (Table 1) demonstrate that the pollutants could not be entirely removed using conventional water treatment techniques commonly used in LICs. The occurrence of such EOCs in DWS raises concerns about potential human health risks.
Table 2.
Personal care products, musks and fragrances, and ultraviolet or sunscreening agents or blockers/filters detected in drinking water systems.
Table 2.
Personal care products, musks and fragrances, and ultraviolet or sunscreening agents or blockers/filters detected in drinking water systems.
| Country | EOCs | Drinking Water System | Key Results and Remarks | References. |
|---|---|---|---|---|
| Personal care products | ||||
| Brazil | Triclosan and bisphenol A | drinking water, source water | Bisphenol A and Triclosan detected in at least one sample. | [30] |
| Brazil | Methylparaben | drinking water, surface water | Detected at concentrations ranging from 15 up to 840 ng L-1 in surface waters. In tap water methylparaben was at 17 ng L-1. The treatment significantly reduced the concentration but still, chronic exposure to tap water may have potential risks. | [56] |
| Colombia | Methyl paraben, benzophenone | reservoirs for drinking water treatment plants, treated water samples | Both compounds detected in raw. Both compounds were still present in the samples although at low concentrations (<40 ng/L) in treated water. This shows they persisted after treatment. | [38] |
| South Africa | Triclosan | treated effluent water | The compound was detected with an average concentration ranging from 10.7 - 24.6 µgl.-1. The compound was not completely removed during the wastewater treatment processes. | [50] |
| Malaysia | Triclosan and Bisphenol A | drinking water supply system (tap water) | Bisphenol A (66.40 ng/L) and triclosan (9.74ng/L) in tap water. These findings show that the conventional water treatment methods were not effective in removing all the contaminants. | [34] |
| China | Propylparaben, bisphenol A, dicyclohexylamine, | tap water | Detection frequencies were over 80% and concentrations of 47.50 ng/L, 31.51 ng/L, and 42.33 ng/L, respectively. | [32] |
| Kenya | Methylparaben and other PCPs | groundwater wells | Five PCPs detected. Methylparaben was the predominant at ≤10 μg/L. | [54] |
| Musks and fragrances | ||||
| USA | tonalide (AHTN) galaxolide (HHCB) |
bottled water, tap water, WWTP, surface water |
All the contaminants detected in the water samples, AHTN (490 ng/L) and HHCB (82 ng/L). | [57] |
| USA | tonalide (AHTN) galaxolide (HHCB) |
river water | HHCB (1 - 20 ng L−1), AHTN (0.5 -10 ng L−1). Both contaminants showed weak estrogenic activity in human cells. |
[58] |
| Serbia |
HHCB | drinking water | The highest concentration of 90 ng/L was found in drinking | [59] |
| China | celestolide (ADBI), phantolide (AHMI), AHTN, traseolide (ATII), HHCB |
tap water | All the contaminants were found to range in concentration from 0.3– 2.1 ng/L. The EOCs can bioaccumulate and have eco-toxicological effects on specific organisms, as well as cause endocrine disruption in humans. | [60] |
| China | AHTN, HHCB |
river water | HHCB (18.7ng/L) and AHTN (11.7 ng/L) were found in the water samples. | [60] |
| Portugal | Cashmeran, ADBI, HHCB, Musk Ketone, Musk xylene, AHMI, AHTN, ATII | drinking water | All chemicals detected in the range of ng/L–μg/L. Exposure to some of the contaminants is linked to diseases such as cancer, cognitive disorders in children, asthma, amyotrophic lateral sclerosis, and infertility. | [61] |
| Germany | HHCB, AHTN, HHCB-lactone |
surface water | About 60 ng L−1 (HHCB), 10 ng L−1 (AHTN) and 20–30 ng L−1 (HHCB-lactone) were found as typical riverine concentrations. | [62] |
| France | Tonalide (AHTN) | tap water, water reservoirs, borehole water |
Less than 1ng/L of the pollutant was detected in the water samples. | [63] |
| Ultraviolet (UV) or sunscreening agents or UV blockers/filters | ||||
| Spain | UV filters: 2-ethylhexyl 4-(dimethylamino) benzoate (OD-PABA), benzophenone-3 (BP3), 2-ethylhexyl 4-methoxycinnamate (EHMC), octocrylene (OC), and 3-(4-methylbenzylidene) camphor (4MBC) | tap water, clean waters | All UV filters were detected in all water samples. There were low detection limits for clean waters (0.02 - 8.42 ng/L). Maximum concentrations were detected in tap water: BP3 (290 ng/L), 4MBC (35 ng/L), OD-PABA (110 ng/L), EHMC (260 ng/L), and OC (170 ng/L). | [64] |
| Spain | UV filters | groundwater | 20- 55 ng/L. | [65] |
| Spain | UV filter benzophenone-4 (BP-4) | surface water, drinking water | The compound was detected in the 20–200 ng L−1 range. The findings show that the contaminant was not removed by conventional methods. | [66] |
| Brazil | UV filters: octocrylene (OC), ethylhexyl salicylate (ES), (benzophenone-3 (BP-3), and ethylhexyl methoxycinnamate (EHMC) | raw water, drinking water (treated and chlorinated water) | All compounds were detected, but only BP-3 (18-115 ng L−1) and EHMC (55 to 101 ng L−1) were quantifiable. | [67] |
| Zambia | Homosalate, Octocrylene |
Groundwater (shallow wells and borehole water) | The compounds were found at low concentrations, Homosalate (0.05ng/L) and Octocrylene (0.04ng/L). Chronic exposure to such waters especially through ingestion might pose potential health risks. | [24] |
Table 3.
Plasticizers, surfactants, flame retardants, endocrine disrupting chemicals, per- and polyfluoroalkyl substances, artificial food sweeteners, food colorants or dyes, and gasoline additives in drinking water systems.
Table 3.
Plasticizers, surfactants, flame retardants, endocrine disrupting chemicals, per- and polyfluoroalkyl substances, artificial food sweeteners, food colorants or dyes, and gasoline additives in drinking water systems.
| Country | EOCs | Drinking Water System | Key Results and Remarks | References |
|---|---|---|---|---|
| Plasticizers | ||||
| Pakistan | Different types of plasticizers | drinking water | 30 types of plasticizers detected in drinking water. Hence, there is a need for regular monitoring of water quality. | [68] |
| Malaysia | 4-octylphenol | drinking water supply system | 0.44 ng/L detected in tap water. | [34] |
| Spain | Bis(2-ethylhexyl) adipate and phthalate esters | tap water, commercial mineral water, river water | The compounds were detected and their limits of detection were between 0.006 and 0.17 μg l−1. | [69] |
| Mexico | Phthalic acid esters | bottled water | PAEs detected in bottled water. The dominant pollutant was dibutyl phthalate at 20.5-82.8 μg L−1. 0.7 < LOD < 2.4 μg L−1. |
[70] |
| Jordan | Phthalates (dibutyl-, di-2-ethylhexyl- and di-n-octyl-phthalate) | bottled water | The water was contaminated with dibutyl-, di-2-ethylhexyl- and di-n-octyl-phthalate, with total phthalate concentrations between 8.1 and 19.8 µg/L. Increasing the storage temperature of the bottled water increased the content of leached phthalates in the water (total concentration of 23–29.2 µg/L). | [71] |
| Saudi Arabia | Dialkyl phthalates | PET bottled water samples | The six phthalates at concentrations between 6.3 and 112.2 ng mL−1 were detected. The highest level was observed for di-n-butyl phthalate, followed by DEHP, DiBP, DMP, DEP and DiPP. LOD of detection was in the range between 0.3 and 2.6 ng mL−1. Phthalate residues leach from PET bottles into water and prolonged consumption of such waters is a public health concern | [72] |
| India | Phthalate esters | PET bottled water | Phthalate esters in bottled water, 0.03< LOD < 0.08 nmol L−1. Consumption of PET bottle-stored water or drinks is a cause for concern since PEs tends to exhibit endocrine disruption. | [73] |
| India | Bisphenol A | plastic-bottled water and household water tanks | LOD = 0.46 pg/mL and LOQ = 1.52 pg/mL. Bisphenol A traces detected in plastic-bottled water with concentrations ranging from 60-90 pg/mL. In plastic water tanks it was nondetectable-12 pg/mL. Consumption of bottled and storing water in plastic tanks may have a bad impact on humans since they can also interfere with reproductive systems. | [74] |
| South Africa | Total plasticizers | bottled water, drinking water treatment plants | Total plasticizers in the water. The frequent detection of these substances in drinking water calls for additional research into their environmental and public health impacts. | [75] |
| Kenya | Plasticizers | surface water (Lake Victoria) | Plasticizers were found in the surface water systems with concentrations of up to 6.5 μg L−1. The pollutant revealed high chronic and acute risk for toxicity in crustaceans, and the same can be true in humans. | [76] |
| Zambia | 1,6-Dioxacyclododecane-7,12-dione, Bis (4-chlorophenyl) sulfone, bis(2-ethylhexyl) phthalate, Bisphenol A, Cyclohexanone, Diisobutyl phthalate , Diethyl phthalate, Dimethyl phthalate, N-butyl Benzenesulfonamide, Triphenyl phosphate, |
groundwater (shallow wells and boreholes) | The contaminants were detected in both water systems at 0.03 - 34 ng/L. The findings indicate that the contaminants are capable of leaching from the various sources into the ground water drinking sources | [24] |
| Surfactants | ||||
| South Africa | 4-nonylphenol (NP) | water samples from boreholes, shallow wells and surface water | NP in water samples. The presence of NP in water samples might pose ecotoxicological risks to aquatic life as well as communities. | [77] |
| Brazil | linear alkylbenzene sulfonate (LAS) and its metabolite, sulfophenyl carboxylates | drinking and surface waters | The LAS concentrations in river water ranged between 14 and 155 μg l−1 and the levels of their metabolic intermediates were found from 1.2 to 14 μg l−1. LAS levels detected in the drinking water ranged between 1.6 and 3.3 μg l−1. The self-purification capacity of the water was demonstrated by the degradation of LAS in river water but still it was present even in drinking water. | [78] |
| Philippines | alkylbenzenesulfonates (ABS) and linear alkylbenzenesulfonates (LAS) | water source (freshwater lake) | Concentrations of ABS (1.1–75 and 1–66 μg L−1) and LAS (1.2–73 and 2.2–102 μg L−1) were detected in the tributaries. | [79] |
| Spain | non-ionic surfactants, linear alkylbenzene sulfonates (LASs) and alkyl ethoxysulfates (AESs) | wastewater treatment plants (WWTPs), drinking-water treatment plants (DWTPs) | Non-ionic surfactants were detected in raw waters (0.2 -100 μg L−1) , effluents (0.1 to 5 μg L−1). LASs and AESs found in all waters. Up to 32,000 μg L−1 of AESs and 3900 μg L−1 of LASs in WWTP feed; up to 114 μg L−1 of AESs and 25 μg L−1 of LASs in DWTPs. Thus conventional treatment processes are inadequate. |
[80] |
| Flame retardants | ||||
| China | Organophosphorus flame retardants (OPFRs) | water sources, DWTPs, tap water | OPFRs were detected at 9.25 - 224.74 ng/L. A reduction in concentration was noted in treated water. Residuals and the potential risk of OPFRs is concerning. | [81] |
| Korea | OPFRs | tap water, purified water, and bottled water | Predominant OPFRs detected were tris(2-chloroethyl) phosphate, tris(2-butoxyethyl) phosphate, and tris(2-chloroethyl) phosphate. | [82] |
| China | OPFRs | tap water | tap water (85.1 ng/L - 325 ng/L), and triphenyl phosphate (TPP), tris(2-butoxyethyl) phosphate (TBEP), and tris(2-chloroisopropyl) phosphate (TCPP) were predominant. | [83] |
| Spain | OPFRs | influent waters | Detected in influent waters at levels of 0.32–0.03 μg L−1. Efficient technologies should be developed to remove the compounds during water treatment. | [84] |
| South Africa | Brominated flame retardants (BFRs) | river water | Both BFRs were detected in Jukskei River water. | [85] |
| Pakistan | OPFRs, dechlorane plus (DP), polybrominated diphenylethers (PBDEs), and novel brominated flame retardants (NBFRs) | potable water in industrial and rural zones | FRs were detected with concentrations of OPFRs (71.05 ng/L), PBDEs (0.82 pg/L), NBFRs (1.39 pg/L) and DP (0.29 pg/L) in both zones. However, consumers of the water were found to be at low risk of FRs exposure through potable water consumption. | [86] |
| Endocrine disrupting chemicals (EDCs) | ||||
| Malaysia | Hormones, diethylstilbestrol |
river water and tap water | The drinking water supply system was observed to contain testosterone, progesterone, estrone, 17α-ethynylestradiol, and 17β-estradiol, with respective concentrations in the tap water of 2.52ng/L, 0.92 ng/L, 3.42 ng/L, 6.34 ng/L, and 11.68 ng/L. | [34] |
| South Africa | dichlorophenol (DCP), bisphenol A (BPA), 17β-oestradiol (E2) octylphenol (OP) |
freshwater, wastewater and treated effluents | Detected in concentrations of 0.127 and 0.261 μg/L for DCP. BPA present in all samples at 1.684 μ/L - 1.468 μg/L. E1 and E2 were detected in most samples at 0.135 μg/L - 1.06 μg/L, and OP at 1.683 μg/L. | [48] |
| Nigeria | 2,4-dinitrophenol, 2-nitrophenol, bisphenol A, 2,4-ichlorophenol, nonylphenol, 2,4,6-trichlorophenol | shallow ground water sources | 2-nitrophenol (0.0077ppm), 2,4- dinitrophenol (0.0554 ppm), 2,4-dichlorophenol (0.0111 ppm). |
[87] |
| Nigeria | bisphenol A (BPA), 4-nonylphenol (NP), and 4-tert-octylphenol (OP) | surface water (River) | BPA (1.20 - 63.64 μg/L), NP (< 0.20 - 2.15 μg/L) and OP (< 0.10 - 0.68 μg/L) were all detected in river water. | [88] |
| Morocco | nonylphenol, 2-phenylphenol, 4-tert-octylphenol, 4-phenylphenol, estrone, 17β-estradiol, triclosan, and bisphenol A |
River water | All the EDCs detected at 2.5 - 351 ng/L in all samples | [89] |
| USA | carbamazepine, iodinated contrast media, -blockers, antibiotics | Waste water, Tap water |
All the pollutants detected. The occurrence of the compounds especially in tap water shows that the traditional water treatment methods used failed to completely remove all the contaminants. | [90] |
| South Africa | bisphenol A, nonylphenol, di(2-ethylhexyl) adipate, dibutyl phthalate, di(2-ethylhexyl) phthalate, diisononylphthalate, 17β-estradiol, estrone, and ethynylestradiol | municipal drinking water | EDCs detected at distribution point water samples with EEq values ranging from 0.002 - 0.114 ng/L. | [91] |
| South Africa | Estradiol | influent water, WWTP effluent water (river water) | The compound was detected in both influent and effluent water (river water). The maximum concentrations recorded in river water samples was 2.45 μg L−1. | [47] |
| South Africa | bisphenol-A (BPA), estradiol | drinking bottled water | Estrogenic activity of the bottled water samples was detected at 20 °C and 40 °C. Equivalents of estradiol (0.001- 0.003 ng/L) and BPA (0.9 ng/L - 10.06 ng/L) were found. However, the concentrations of drugs posed an acceptable risk for a lifetime of exposure. | [92] |
| Mexico | ethylbenzene, 2-chlorophenol | groundwater, surface water | The concentration of the compounds ranged from ng/L to 140 mg/L. | [93] |
| France | carbamazepine, iodinated contrast media, -blockers, antibiotics diethylstilbestrol |
tap water | Concentrations in the ng/L range were detected. Exposure to such waters via consumption is associated with abnormalities in the structure and function of reproductive organs. | [94] |
| China | Lindane, heptachlor epoxide | ground water, surface water, tap water | Both compounds detected in concentration ranging from 0.17–860 ng/L and 0.11–10 ng/L. The compounds can bioaccumulate and magnify along the food chain with a huge impact on top predator species, including humans. |
[95,96] |
| United Kingdom | Nonylphenol Estrone (E1), and Estradiol (E2) |
municipal wastewater |
The EDCs were detected in concentrations of nonylphenol (1.2–2.7ng/L), E1 (15–220ng/L), and E2 (7–88ng/L). The EDCs cause feminization in fish in sewage treatment as they can mimic estrogenic even to non-target species. The same can impact humans. | [97] |
| Germany | Nonylphenol Estrone (E1) Estradiol (E2) |
drinking water, surface water |
Significant amounts of nonylphenol (8 ng/L), E1 (0.4 ng/L) and E2 (0.3 ng/L). An increase in vitellogenin levels, as well as the number of eggs produced by Pimephales promelas was observed. The same impact can affect humans through the ingestion of contaminated water. |
[98] |
| Zimbabwe | oestrogenic and androgenic chemicals | dam water (Umguza and Khami) | the contaminants were detected in both dam waters and were expressed as 17β-oestradiol equivalent (EEq), with concentrations as high as 237 ng l–1. | [99] |
| Tanzania | endocrine disrupting estrogens (ethinylestradiol, estrone and estradiol) | dam and river water | The presence of estrogens in the waters was revealed, with levels ranging from non-detectable levels to 16.97 ng/L. The detected concentrations, as reported in previous literature, were not significant enough to cause adverse health effects to humans. | [100] |
| Per- and polyfluoroalkyl substances | ||||
| China | PFAS | water source, DWTPs, and tap water | Concentrations: 13.4 ng/L - 17.6 ng/L. This highlights that PFAS are present in the treatment train and effective removal technologies should be employed. | [52] |
| Sweden | PFAS | ground water aquifer, surface water, drinking water. | PFAS detected in all water samples. For example, in surface water PFAS concentration reached 15 ng L−1 while ranged between 1 ng L−1 and 8 ng L−1 in drinking water. Water treatment reduced the concentration of PFAS. | [101] |
| USA | PFAS (e.g., Perfluorohexanoic acid (PFHxA), perfluorooctanoic acid (PFOA), and perfluoroheptanoic acid (PFHpA)) | drinking water | 14 PFAS were detected in drinking water. For example, maximum concentrations of 268 ng/L for PFHxA, 213 ng/L for PFOA, and 75.7 ng/L for PFHpA were recorded. PFOA, perfluorodecanoic acid, and PFHpA were each detected in at least one drinking water sample at concentrations > 20 ng/L. | [102] |
| USA | Perfluorooctanoic acid (PFOA), Perfluorooctane sulfonic acid (PFOS), Perfluorobutanoic acid, and Perfluorononanoic acid |
groundwater, surface water. and tap water | The contaminants were detected in all the water samples in a concentration ranging from 5–174 ng/L. PFAS can disrupt the female reproductive system by altering menstrual cycle, hormone secretion, and fertility. | [103,104] |
| China | Perfluorocarboxylic acids and Perfluorosulfonic acids | tap water | PFAS in the concentration ranged between 4.10 and 17.6 ng/L were detected in the water samples. | [32,52] |
| South Africa | Perfluorosulfonic acids, perfluorocarboxylic, Perfluoro-n-decane sulfonic acid, perfluoro-n-heptyl sulfonate |
surface water | The contaminants were detected in the range 0.14–89.04 ng/g. Single or mixtures of PFAS causes female reproductive tract dysfunction and disease. |
[105] |
| Uganda | perfluorohexanesulfonate (PFHxS), perfluorooctanoate (PFOA) |
drinking water reservoir (Lake Victoria). | PFOA and PFHxS were detected in the drinking water reservoir | [106] |
| Ethiopia | PFAS | surface water (river, lake) | Found at concentrations ranging from 0.073- 5.6 ng /L. | [107] |
| Ghana | perfluoroalkyl carboxylic acids, perfluoroalkane sulphonic acids |
river water, tap water | Both contaminants were found at concentrations between 281 and 398 ng/L in river water and between 197 and 200 ng/L in tap water. | [108] |
| Gasoline additives | ||||
| Italy, Belgium, and Luxembourg |
ethyl-tert-butylether (ETBE), methyl-tert-butylether (MTBE) | surface water, ground water, and tap water |
All the contaminants were detected in all the drinking water samples with concentration ranging from 10 - 100 ng/L. ETBE and MTBE are recalcitrant to treatment and their exposure via ingestion is very high, hence its risks may be also high. | [3] |
| USA | MTBE | groundwater, municipal drinking water supplies, private wells, and reservoirs. |
The pollutant was detected at concentrations ranging from 0.2 to 20 μg/L. Its complete removal requires more time, complicated and expensive treatment technologies. | [109] |
| Dutch | MTBE, methyl-tert-amyleter (TAME), and ETBE |
Groundwater and surface water | MTBE concentrations below 0.1 μg/L were detected. | [110] |
| Artificial food sweeteners | ||||
| USA | Sucralose | drinking water treatment plants | Sucralose detected in finished water samples. | [111] |
| Germany | Cyclamate, Acesulfame, saccharin, sucralose |
wastewater treatment plant | Detected in influents of the sewage treatment plants i.e., 190 μg/L for cyclamate, 40 μg/L for acesulfame and saccharin, and less than 1 μg/L for sucralose. | [112] |
| Switzerland | Acesulfame | surface water, ground water, and tap water |
Detected in influent and effluent (12−46 μg/L). The contaminant was not removed during treatment. Persistent concentrations in surface water samples, whilst groundwater concentrations of up to 4.7 μg/L. |
[113] |
| Switzerland | acesulfame, saccharin, cyclamate and sucralose. | surface water, tap water. | Saccharin and cyclamate were present in raw water for treatment but absent in tap water. Acesulfame ≤ 0.76 μg L−1 in tap water. | [114] |
| Switzerland | aspartame, acesulfame (ACE), neohesperidine dihydrochalcone, saccharin (SAC), neotame, cyclamate (CYC), and sucralose (SUC) | surface water, groundwater, and drinking water | The contaminants were detected in all water samples. ACE ≤ 7 μg/L and SUC ≤ 2.4 μg/L were detected in tap water. | [115] |
| Canada | Acesulfame, saccharin |
groundwater, |
All pollutants were detected but acesulfame was μg/L scale. | [116] |
| Food colourants or dyes | ||||
| Poland | Crystal violet, methyl violet 2 B, rhodamine B |
water reservoirs | Detected in the following concentrations: methyl violet 2 B (0.0571 μg/L), crystal violet (0.0122–0.0209 μg/L), rhodamine B (0.0594 μg/L). |
[117] |
| Poland | crystal violet, rhodamine B, and methyl violet | water reservoirs | Concentrations: 0.017 - 0.0043 μg/L. The contaminants have carcinogenetic, mutagenic and teratogenic properties. | [117] |
| Brazil | C.I. Disperse Blue 373, C.I. Disperse Orange 37 and Disperse Violet 93 | treated industrial effluent, raw river water, treated river water | The dyes were detected in concentrations ranging from 1.65 - 316ng/L. Water treatment processes failed to completely remove the dyes. |
[118] |
3.3. Plasticizers
Numerous studies have reported the presence of plasticizers in DWS, especially bottled water (Table 3) [70,71,72,74]. An example is a study in Saudi Arabia, which detected dialkyl phthalates (e.g., dimethyl phthalate, diethyl phthalate, diisopropyl phthalate, diisobutyl phthalate, di-n-butyl phthalate and di-ethylhexyl phthalate) in bottled water, at concentrations in the range of 6.3- 112.2 ng mL−1, and dibutyl, di-n-octyl-phthalate, and di-2-ethylhexyl were at a total phthalate concentration ranging from 8.1 to 19.8 g/L [71,72]. Despite the limited studies, LICs have also reported plasticizers in bottled water, indicating that this is not just a concern in developed countries. For instance, total plasticizers were measured and detected in bottled water in South Africa [75]. Interestingly, the majority of phthalate residues are believed to leach from plastic bottles into drinking water. This is because leached phthalates were shown to be present in higher concentrations in bottled water with longer storage times and warmer temperatures than samples with shorter storage times and lower temperatures [71,72]. Besides plasticizers originating from plastic bottles, evidence also shows that plasticizers occur in DWS without any connection to plastic bottles or storage containers (Table 3). For example, in studies not involving bottled water, a variety of plasticizers have been detected in DWS [34,68,69]. Plasticizer concentrations of up to 6.5 g L-1 were reported in surface water systems in Kenya [76]. Additionally, tap water and river water in Spain contained bis(2-ethylhexyl) adipate and six phthalate esters [69]. Although several studies linked plasticizers to possible human health risks following chronic exposure via consumption of contaminated water (Table 4), more studies are needed to determine how they affect human health.
3.4. Surfactants
The presence of various surfactants in DWS has been reported in several studies (Table 3). For example, in Brazil, linear alkylbenzene sulfonate (LAS) and its degradation by-product sulfophenyl carboxylates (SPC) were detected in drinking (1.6 - 3.3 μg L−1) and surface waters (14 and 155 μg L−1). Although the self-purification capacity of river water was demonstrated by the degradation of LAS, it persisted in drinking water. Another study conducted in Spain reported the presence of LAS, alkyl ethoxysulfates, and non-ionic surfactants in drinking water and wastewater treatment plants. Furthermore, investigations done in LICs found surfactants in DWS. For instance, 4-nonylphenol was found in shallow wells, surface water, and boreholes in South Africa [77]. Prolonged exposure to such contaminated water could cause adverse human health effects (Table 4). Further research should, therefore prioritize developing low-cost water treatment technologies that can eliminate or reduce such contaminants in DWS to safe concentrations.
3.5. Flame Retardants
Evidence on the occurrence of flame retardants (FRs) in DWS is presented in Table 3. Dechlorane plus (0.29 pg/L), novel brominated flame retardants (1.39 pg/L), polybrominated diphenylethers (0.82 pg/L), and organophosphate flame retardants (71.05 ng/L) were detected in potable water in Pakistan [86]. However, the concentrations were reported to be low risk following exposure to FRs through water consumption. Chronic exposure may, nevertheless, pose potential public health risks. In another study, organophosphate flame retardant residues were detected in drinking water sources, drinking water treatment plants, and tap water at concentrations in the range of 9.25 to 224.74 ng/L [81]. Flame retardants were also reported in drinking water systems in LICs, even though the studies were sparse compared to developed countries. For instance, polybrominated diphenyl ethers, polybrominated biphenyls, and brominated flame retardants have all been found in the Jukskei River water in South Africa [85].
3.6. Endocrine Disrupting Chemicals
Endocrine disrupting chemicals (EDCs) are pervasive in the aquatic environment, and have been reported in several DWS (Table 3). In Malaysia, drinking water supply systems (e.g., river water and tap water) were reported to contain testosterone (2.52 ng/L), progesterone (0.92 ng/L), estrone (3.42 ng/L), 17β-estradiol (6.34 ng/L), and 17α-ethynylestradiol (11.68 ng/L), with higher concentrations in the tap water [34]. In another study in Mexico, ethylbenzene, 2-chlorophenol, ethylbenzene, 2-chlorophenol was detected in groundwater and surface water samples [93]. Notably, the occurrence of EDCs in DWS in LICs (especially in Africa) was comparable to that in developed countries. For example, several studies reported the occurrence of EDCs in drinking water systems in Africa [47,87,88,91]. A study conducted in South Africa reported the occurrence of bisphenol A and estradiol in drinking bottled water by determining the estrogenic activity of water at different temperatures [21]. The results of the study showed the estrogenic activity of the bottled water samples was at 20 oC and 40 oC and equivalents of estradiol and bisphenol A were 0.001- 0.003 ng/L and 0.9 ng/L - 10.06 ng/L, respectively. A similar study was conducted in Morocco where 4-phenylphenol, nonylphenol, 4-tert-octylphenol, 2-phenylphenol, triclosan, 17β-estradiol, estrone, and bisphenol A were detected in river water at concentrations in the range of 2.5 - 351 ng/L [89]. However, the occurrence of the EDCs especially in tap water and bottled water shows that the treatment methods were not effective in removing the contaminants. This is suggestive of potential human exposure and associated health risks (Table 4).
3.7. Gasoline Additives
Surface water, tap water, groundwater, municipal drinking water supplies, private wells, and reservoirs have been reported to contain gasoline additives (Table 1). The detected gasoline additives include methyl-tert-butylether (MTBE), ethyl-tert-butylether (ETBE), and methyl-tert-amylether (TAME), with concentrations in the range of 10 to 100 ng/L in drinking water, and 0.2 to 20 g/L in the groundwater and surface water (Table 1). Both ETBE and MTBE are difficult to remove during drinking water treatment. In another study, MTBE concentrations in surface water, tap water, and ground water were reported to range between 10 and 100 ng/L in Italy, Belgium, and Luxembourg [3]. Although some gasoline additive compounds such as MTBE are currently thought to be non-toxic to humans, they are undesirable in principle, and must be removed from drinking water [119]. This is because studies on animals have reported potential health risks, while some gasoline additives have known human health effects (Table 2).
3.8. Per- and Poly-Fluoroalkyl Substances
Per- and polyfluoroalkyl substances (PFAS) are a relativey new group of EOCs which is frequently detected in DWS (Table 3). For example, in the USA the occurrence of PFAS (e.g., perfluorohexanoic acid, perfluorooctanoic acid, and perfluoroheptanoic acid) with concentrations ranging from 75.7 ng/L to 268 ng/L, was reported in drinking water [102]. PFAS were also reported in studies conducted in LICs [108], and this shows that the problem is worldwide. Specifically, the presence of perfluoroalkane sulphonic acids and perfluoroalkyl carboxylic acids in river water and tap water was reported in Ghana [108]. Furthermore, perfluorohexanesulfonate and perfluorooctanoate were found in the drinking water reservoir of Lake Victoria in Uganda . However, compared to other groups of EOCs, data on PFAS in DWS is still limited in both developed countries and LICs. Given their widespread use in industrial and household products, further research is needed to determine their occurrence in various DWS.
3.9. Artificial food Sweeteners
Artificial food sweeteners have been found in DWS (Table 3). For example, acesulfame, aspartame, cyclamate, neotame, neohesperidine dihydrochalcone, saccharin, and sucralose were found in groundwater, drinking water, and surface water in Switzerland [115]. Notably, acesulfame and saccharin had concentrations of up to 7 and 2.4 μg/L in tap water, respectively. Other studies conducted in Switzerland and Canada also reported the presence of artificial food sweeteners in surface water, groundwater, and tap water [114,116]. Artificial sweeteners are resistant to wastewater treatment processes, thus, they tend to occur frequently in DWS [120]. However, the potential human health effects of artificial sweeteners are still unknown [121]. This calls for further research to understand the public health risks posed by exposure to artificial food sweeteners.
3.10. Food colourants or Dyes
A number of previous studies have reported the contamination of water reservoirs such as lakes, dams, ponds, and rivers, with food colourants and dyes (Table 1). For example, methyl violet 2 B (0.0571 μg/L), crystal violet (0.0122-0.0209 μg/L), rhodamine B (0.0594 μg/L) were reported in surface water [122]. In another study, the concentrations of C.I. Disperse Blue 373, C.I. Disperse Orange 37, and Disperse Violet 93 in industrial effluent raw water and tap water ranged from 1.65 ng/L to 316 ng/L [118]. Furthermore, a study conducted in Poland detected crystal violet, rhodamine B, and methyl violet in water reservoirs, with concentrations in the range of 0.017 - 0.0043 μg/L [122].
3.11. Ultraviolet or Sunscreening Agents or UV Blockers
The occurrence of ultraviolet (UV) blockers in DWS is documented in several studies (Table 2). These contaminants are exceedingly difficult to remove using the existing conventional water treatment technologies, as shown by their occurrence in drinking water [64,66]. For instance, tap water and ‘clean waters’ (tap water treated through ion-exchange resins, well water, and mineral bottled water) were found to be contaminated with 2-ethylhexyl-4-(dimethylamino) benzoate, benzophenone-3, 3-(4-methylbenzylidene) camphor, 2-ethylhexyl-4-methoxycinnamate, and octocrylene [50]. In another study, UV filters were detected in raw water and drinking water . Furthermore, even groundwater and surface water may also contain UV filters. For example, detected UV filters in groundwater with concentrations ranging from 20 to 55 ng/L [65].
3.12. Musks and Fragrance
The occurrence of musk and fragrances in different DWS is presented in Table 2. Tonalide and galaxolide were detected in surface water as well as in treated water (bottled water, tap water) in the USA at concentrations of 0.5 -10 ng L−1 and 1 - 20 ng L−1, respectively [57,58,123]. Similarly, celestolide, phantolide, traseolide, galaxolide and tonalide were detected in tap water samples in China, with concentrations in the range of 0.3–2.1 ng/L [60]. Like other EOCs, musks and fragrances are not completely removed by conventiona drinking water treatment methods. Thus, human exposure to musks and fragrances via consumption of contaminated drinking water may lead to range of potential health risks (Table 4).
3.12. Disinfection by-Products
The disinfection of drinking water during treatment can result in the generation of disinfection-by-products such as haloacetic acids. These occur widely in DWS that rely on chlorination or chloramination for the final disinfection of drinking water [124,125,126,127]. Disinfection by-products are carcinogenic, and their occurrence and human health risks could be more pronounced in LICs where chlorination is commonly used for drinking water disinfection.
Apart from haloacetic acids, the transformation of organic pollutants by disinfection processes has significantly produced disinfection by-products that have been associated with drinking water pollution. In one study, disinfectant by-products, C (C4H6ClN3) and Y (C4H6ClN5) were detected in significantly high concentrations in Chinese urban tap water. These disinfectant by-products were derived from the chlorination of metformin-contaminated water [128]. The degradation of emerging contaminants to form transformation products in drinking water during treatment was reported in several studies. In one study, benzotriazoles were transformed into benzotriazoles degradation products (BTTPs) in urban aquifers. The main BTTPs were 4-dimethyl-2H-benzotriazole and 2-methyl-2H-benzotriazole from the transformation of 1H-benzotriazole and 4-methyl-1H-benzotriazole (4-MeBT) respectively. The temporary storage of benzotriazoles in sediments with a reduced hydraulic conductivity is presumably believed to have increased the transformation of benzotriazoles processes through transformation processes such as tautomerization and methylation [129]. Because a number of earlier reviews focusing on the topic exist [124,125,126], a detailed discussion on disinfection by-products is outside the scope of this review. However, their removal in DWS is briefly discussed among other EOCs.
4. Behaviour and Fate
The fate of EOCs in drinking water systems is dependent on the chemical and physical properties of the EOCs, and the aqueous media transporting them [130]. EOCs in DWTPs can undergo; (1) (bio)accumulation in microorganisms, (2) biodegradation, (3) photodegradation, (4) chemical degradation and transformation, and (5) physical removal. Most of these fate processes occur in drinking water treatment plants (DWTPs) based on; (1) physical contaminant removal (e.g., precipitation, sedimentation, filtration, and adsorption), (2) chemical transformation/disinfection (e.g., ozonation, chlorination, and ultraviolet irradiation), and (3) biological treatment (e.g., activated sludge) [32]. EOCs present several challenges in DWTPs as their removal has been limited in conventional treatment systems [131]. However, recalcitrant EOCs have been significantly removed by advanced techniques like membrane filtration, advanced oxidation processes, and biological processes [132].
Although DWTPs reduce the concentration of EOCs in water, EOCs may persist in drinking water after treatment. For example, nonylphenol, carbamazepine, perfluorooctanesulfonic, caffeine, and perfluorooctanoic were detected in treated drinking water at 7.90–53.62 ng/L, ≤1.20 ng/L, ≤12.66, ng/L, 12.47–66.33 ng/L, and ≤6.27 ng/L, respectively [133]. Thus, the removal of emerging contaminants in DWTPs is incomplete [134]. EOCs are normally degraded and reduced in DWTPs. For instance, in a study in Germany, sand filtration, and flocculation, were not efficient in eliminating carbamezapine, clofribric, and diclofenac [135]. Notably, clofribric was highly stable at considerably high ozone dosage, and a adsorption by granular activated carbon was low. Overall, the removal of nonylphenolic compounds along the treatment train was settling, flocculation, and sand filtration (7%), ozonation (85%), granular activated carbon filtration (73%), and chlorination (43%). Furthermore, coagulation techniques applied in DW plants through the use of aluminium based reagents reportedly eliminate about 20% and 75% of the precursors of haloacetic acids [136]. Besides coagulation, ion exchange has been reported as an efficient haloacetic acid precursor removal, with 50% to 70% removal efficiencies [137]. The removal of EOCs such as haloacetic acids has been improved by a combination of both coagulation and ion exchange techniques [126]. The use of granular activated carbon after chlorination reduces halogenated nitrogenous disinfection by-products (e.g. haloacetic acids) through adsorption [138]. Overall, UV, reverse osmosis systems process, and ion-exchange resins have been applied and showed significant removal of PFAS.
Notably, the methods applied in drinking water treatment such as flocculation and coagulation have shown low efficiency in the removal of PFAS such as perfluorooctanoic acid (PFOA) and perfluorooctysulfonic acid (PFOS). For example, concentrations in the μg/L range are reduced by only between 10 and 30% [103]. However, the application of other methods such as filtration in the presence of granular activated carbon reduced PFOS and PFOA in drinking water by up to 90% [139,140]. The removal of bisphenol A in the conventional drinking water treatment processes was reported to be between 76 and 99% (Arnold et al., 2013). Additionally, adsorbents such as poly-coated magnetic iron oxide nanoparticles are critical in the removal of nonylphenol. Approximately 67% was removed from drinking water through adsorption involving poly-coated magnetic iron oxide nanoparticles [141]. Apart from physical techniques such as microfiltration, coagulation and flocculation, ultrafiltration, sand filtration, and adsorption, the removal of some EOCs may be facilitated by specific microbial species. Notably, specific microorganisms can biotransform EOCs such as hormones and pharmaceuticals, and increase their degradation in DWTPs [142,143].
Due to their persistence, EOCs in DWS can (bio)accumulate in microorganisms during storage and transportation. This is because their biodegradation, photodegradation, and chemical degradation generally occur at significantly low rates [142]. Reduced degradation implies their natural removal from drinking water systems is limited [144]. Notably, there is limited research on the natural (bio)degradation of EOCs, including pharmaceuticals, and hormones. In a few exceptions where results of such studies are documented, they are limited to laboratory studies, which may not represent actual DWS. Thus, the implementation of data from these laboratory-based studies could be problematic due to lack of detailed understanding of removal processes operating in real DWS.
Furthermore, EOCs have been reported to accumulate in sediments during transportation. In this regard, a previous study detected 1289.8 ng/g tripentyl phosphate in sediments Wu et al. [145]. The concentration of EOCs in drinking water sources such as rivers may decrease through natural filtration during water transportation to DWTPs. River bank filtration of EOCs may reduce the abundance of EOCs in the filtrate. Thus, a significant difference between EOCs in bank filtrate (lower concentration) and water (higher concentration) of the Danube River was reported.
Photodegradation as well as chemical and biological degradation transform specific EOCs into by-products that can be more toxic than the original EOCs [146]. For instance, incomplete oxidation of acyclovir leads to the generation of more ecotoxic by-products such as carboxy-acyclovir and N-(4-carbamoyl-2-imino-5-oxoimidazolidin)-formamido-N-methoxyacetic acid [146]). Although disinfection of EOCs often results in their removal in drinking water during treatment, it can also result in the emergence of toxic EOCs such as haloacetic acids [147].
Among the removal techniques for EOCs in DWTPs, transformation through oxidation with granular activated carbon filters and chlorine dioxide was the most suitable method. Membrane techniques have been widely investigated. For instance, in an electrodialysis reversal facility system, about 18 out of 49 compounds were quantifiable indicating removals of approximately 65% to 90% for the overall DWTP process [148]. Application of techniques such as reverse osmosis reduced the concentration of bisphenol A by up to 98% in drinking water. Other removal methods include biodegradation and volatilization [149,150]. Chlorination and de-chlorination of drinking water affect the fate of the EOCs [151]. Personal care products are likely to be removed through sorption and transformed into carbon dioxide and water in DWTPs. This may be linked to the fate of these personal care products in WWTPs where they are metabolised to water and CO2, and removed by sorption on sludge .
It has been shown that the concentrations of haloacetic acids and other EOCs in DWTPs can be eliminated by modification of disinfection and hydrolysis techniques, degradation of haloacetic acids post-formation, and the removing the precursor EOCs before disinfection. Advanced methodssuch as O3/H2O2/UV have resulted in a reduction (70%-90%) of haloacetic acids by up to through oxidation in the presence of non-selective and highly reactive species generated in the water treatment process [136]. A combination of ozonation and reverse osmosis processes removed up to 100% of meprobamate, estradiol, triclosan, trimethoprim, and naproxen [30]. Consistent with these findings, 98% of bisphenol A was removed in a short period (20 min) when a photo-Fenton process was applied to drinking water. It has been shown that the efficiency of removal of disinfection by-products can be enhanced by replacing chlorination with chloramination or through the use of hydrogen peroxide, UV, potassium permanganate, and ozone [124,152]. Alternatively, chlorination has been coupled with other techniques such as granular activated carbon filtration (biological active/inactive) to improve removal of disinfection by-products [138].
Generally, DWTP processes such as chlorination and chloroamination contribute to the transformation of EOCs. For instance, the hydrolysis of bisphenol diglycidyl ethers and bisphenol A at pH 7.6 to 9.1 was faster in the presence of free chlorine and was temperature dependent. Additionally, the hydrolysis process had a half-life ranging from 11 to 4.5 days at temperatures 15 ºC to 25ºC at pH 5-9. In one drinking water treatment plant, 76% of bisphenol A was removed through a processes involving ferric chloride coagulation, sorption with granular activated carbon, disinfection with sodium hypochlorite, and secondary disinfection [123]. EOCs such as nonylphenol have been removed (50% to 90%) from drinking water using granular activated carbon [153]. Generally, conventional DWTPs (including ozonation), and electrochemical treatments, have been reported to remove nonylphenol by 30% and 70%, respectively.
In one study, granular activated, disinfection with chlorine and ultraviolet radiation, ozonation, and disinfection were applied to drinking water. The removal efficiencies were between 5.3 and 99% for EOCs including PAHs, personal care products, steroids, and hormones [154]. However, ozonation was efficient in degrading polar pharmaceuticals such as carbamezapine (>90%), diclofenac (>90%), and bezafibrate (50%). An investigation on the behaviour of nonylphenolic (acidic and neutral), nonylphenolic chlorinated, and brominated derivatives in a DWTPin Barcelona, Spain observed that nonylphenolic compounds were significantly reduced by transformation processes before chlorination [134,155]. The concentration of short-ethoxychain nonylphenolic compounds and nonylphenolic compounds was reduced by 25-35%, and up to 90%, respectively, and the elimination factor for nonylphenolic compounds was 96-99%.
There is inadequate data on the fate and behaviour of EOCs when bio-sand filtration is applied to treat drinking water. However, there is evidence that sedimentation and bio-sand filtration can substantially remove EOCs through adsorption [156]. Biosand filtration has significantly reduced pharmaceuticals including antibiotics in drinking water [157,158]. The efficacy of bio-sand filtration was demonstrated in laboratory-based experiments, where 4.2% and 92% of sulfamethoxazole and trimethoprim were removed from water [157,158]. Nevertheless, further research is required under typical DWTP operating conditions in LICs. Data on water treatment processes that are efficient in removing EOCs is key in choosing technologies to safeguard public health. Besides, due to the use of rudimentary water treatment techniques, the removal of EOCs in DWS in LICs still poses significant challenges. This calls for further research to develop low-cost methods with capacity to remove EOCs in DWS.
5. Human Exposure Risks
5.1. Risk Factors and Behaviours
The occurrence of EOCs in DWS is a significant concern, as drinking water is a potential route of human exposure to pollutants [45,159,160]. Although EOCs exist at trace concentrations in drinking water, they biomagnify up the food chain and bioaccumulate in the human body, and are thus, highly toxic [160]. Although some studies have reported a low likelihood of EOCs causing any serious human health risks, there are significant uncertainties in such assessments [161], and there is growing evidence of increasing threats from such contaminants. Several studies investigated exposure risks to individual EOCs, but there is no conclusive information on the effects of long-term and low-level exposure to a cocktail of EOCs and their metabolites on human health [45,160]. The interactions of these contaminants may have unprecedented toxic effects on human health.
In some cities and countries (e.g., Windhoek in Namibia, Singapore, Orange County in California in the USA, Australia), treated wastewater is recycled into drinking water [162,163]. Given the diversity of EOCs and their incomplete removal in drinking water systems, health concerns have been raised about recycled drinking water. Thus, strict monitoring for a wide range of EOCs should conducted regularly to safeguard public health in such settings.
Human exposure to EOCs is through various routes, behaviours, and concentrations that may vary considerably over space and time [45,159]. Exposure pathways include drinking contaminated water, ingesting food prepared with contaminated water, and even dermal exposure during daily activities such as showers, bathing, or cleaning [164]. Groundwater is a valuable source of drinking water because it is thought to be less contaminated. Many people use groundwater directly for drinking purposes around the world, with approximately 40% of Americans relying on it [161,165]. However, groundwater is also prone to EOC contamination and could pose a human health threat. For example, discharges from wastewater treatment systems, landfills, aquacultural practices, industry, hospitals, and veterinary clinics might contaminate groundwater [40,161,165]. Furthermore, groundwater is linked to other sources, for example surface water, that are highly prone to pollution.
Antibiotics in water systems are a significant source of concern because they can lead to the development of antibiotic-resistant bacterial (ARB) strains. A previous study detected extremely high concentrations of amoxicillin (87-272.150 ng/L) in drinking water systems, which is linked to the development of ARB, posing a challenge in disease management [45]. In a study, the exposure risks and hazard quotients (HQ) of antibiotics commonly found in drinking water ranged from 10-9 to 2.5 [166]. Doxycycline had the highest HQ, exceeding the risk threshold (HQ=1). All the other antibiotics studied had HQs below the risk threshold, indicating a low likelihood of causing health risks. Risks of pharmaceutical mixtures were higher (HQ ranging from 10−2 to 2.6) than any individual [166]. Despite the increase in HQ values, the hazard index (HI) fell below those that can cause lifetime health risks. However, the compounds undergo biotransformation within the drinking water system producing metabolites. Research on the impacts of exposure to these metabolites is scarce, but they could be more toxic than the parent compounds. Furthermore, most pharmaceuticals persist within the environment leading to bioconcentration in surface water and groundwater [167].
Personal care products have been detected in drinking water systems. The four main classes of PCPs are phthalates, parabens, triclosan, and fragrances [168]. These compounds are the main ingredients in cosmetics and detergents, including toothpaste, soap, shampoo, deodorant, and mouthwash [40,169]. Most of these chemicals have endocrine-disrupting properties, which reportedly cause diseases such as diabetes, obesity, autism, neurological disorders, infertility, and some cancers in humans [168]. In addition, antibacterial compounds such as triclosan and musk fragrances have been detected in drinking water systems. Although studies have shown that these compounds occur in trace concentrations in drinking water, they can persist within the environment [170]. Once ingested, they are attracted to fat and are resistant to removal from the body, resulting in their accumulation in fatty tissues [168].
Endocrine disrupting chemicals include estrogen, progesterone, androgen, ethinylestradiol, bisphenol A, bisphenol-A and polychlorinated biphenylphthalate esters (PAEs) [171]. The EDCs, for example, bisphenol-A and PAEs can simulate hormones within the body of an organism or interfere with their physiological processes. Thus, they have been associated with infertility, diabetes, obesity, neurological diseases, and aberrant growth patterns [172]. Besides, the disrupted endocrine system causes acute to chronic diseases, including immune effects, behavioural changes, reproductive abnormalities, metabolic syndromes, epigenetic deregulation, and disrupted foetal development and growth [159]. Phthalates of higher molecular weight, for example, di (2-ethylhexyl) phthalate, di- n-butyl phthalate, and di-n-octyl phthalate, are mutagenic and can affect the liver, and excretory and reproductive systems [172].
A study conducted in Jabalpur City, India, detected phthalate esters in surface water, overhead water, and drinking water at concentrations in the ranges of 3927.89–7553.94 µg/L, 3.02–1527.29 µg/L, and 1.86–1438.20 µg/L, respectively, during winter [172]. However, EOC concentrations in summer were significantly higher, implying that human exposure risks may vary with seasons. With regards to human health risk, estimated hazard quotients associated with PAEs and bisphenol A exposures show that only di (2-ethylhexyl) phthalate (DEHP) has a higher (> 1.0) HQ and HQ-AA irrespective of the season. Exposure to DEHP is therefore associated with an increased risk for human health. Other studies, however, reported contrasting results, with two separate studies in Iran reporting HQs of less than 1 for DEHP [172]. This may suggest that exposure to PAEs and BPA does not result in adverse human health impacts. Nevertheless, further studies are required to ascertain the risks associated with these EOCs.
Besides seasonal variation, human exposure risk can also be affected by the life stages and health circumstances of individuals. A comparison of daily exposure risks to EDCs among adults, infants, and children revealed that children and infants are more susceptible to EDCs exposure due to the uptake of more water based on body weight [159]. With regards to bisphenol A, the observed daily intake in infants (1340 ng/day) was nearly tenfold that for adults (148 ng/day). Adults above 65 years, pregnant women, and lactating mothers undergo physiological changes that demand higher water uptake, making them more vulnerable to EDC exposure risks. Human exposures to EDCs, such as phthalates, can reduce fertility by prematurely activating primordial follicles and altering levels of sex-steroid hormones [173]. In females, prenatal exposure to EDCs and other chemicals has been associated with several adverse pregnancy outcomes, including miscarriage, preeclampsia, intrauterine growth restriction, poor weight gain during fetal development, and preterm delivery, have been reported [174]. In males, exposure to EDC in early life causes conditions such as hypospadias, congenital cryptorchidism, poor semen quality, testicular dysgenesis syndrome, and testicular germ cell cancer.
Human exposure to fluorinated compounds, such as PFAs, PFOAs, and PFOs, through drinking water causes similar health outcomes to phthalates. These compounds are concerning owing to their high mobility, persistence, and toxic potential [45]. Concentrations of PFOS ranging from 0.1 to 51 ng/L were detected in potable water in Japan [175], while a study in America detected PFOA concentrations of 26 and 27 ng/L, and PFOS concentrations of 57 and 63 ng/L in tap water [154]. The occurrence of these compounds in drinking water is associated with increased tumours, endocrine disruption, impaired neuro-development, and adverse reproductive outcomes in humans [173]. Evidence from an epidemiological study in Mid-Ohio valley showed that exposure to PFOA through drinking contaminated water for one year caused ulcerative colitis, testicular and kidney cancers, thyroid disease, high cholesterol, liver damage, pregnancy-induced hypertension, and decreased birth weight [176]. Despite studies linking the presence of these compounds to various diseases and conditions, there are insufficient epidemiological and toxicology studies to fully understand their human exposure risks.
Studies have shown that DWS are contaminated with various forms of EOCs, and the contamination levels vary with location and time. Concentrations of EOCs in drinking water systems depend on factors such as the source of water (groundwater or surface water), properties of the pollutant (persistence, mobility, accumulative, bio-magnification, etc), location, and seasonality. Although exposure to EOCs has been linked to adverse effects on human health, the epidemiological and toxicological data available is inconclusive, and most studies focused on individual contaminants. Most contaminant levels detected in drinking water systems fall below exposure risk thresholds. However, exposure to a cocktail of contaminants can adversely affect human health. Therefore, there is a need for more epidemiological and toxicological research to elucidate the potential adverse effects of inevitable exposure to EOCs.
5.2. High-risk Environments
To protect human and ecological health, it is important to assess and ascertain high-risk environments as well as groups most vulnerable to EOCs. The vulnerability of these groups is dependent on the occurrence and distribution of EOCs in aquatic environments. It is therefore paramount to relate risk factors to locations that expose groups of people to these contaminants. A high global mortality rate (>1 per 105) is attributed to unsafe drinking water, sanitation, and hygiene (WHO, 2019) with African countries and other low- and middle-income countries having rates of >0.1 %. This shows the disease burden and mortality due to water contaminants, including EOCs, which are attributed to several risk factors some [77]. Proximity to human activity, industrial and agricultural wastewater sources increase the occurrence of EOCs and exposes not only communities in the vicinity, but also end users of drinking water and aquatic foods [177,178,179]. Furthermore, the efficiency of treatment of the wastewater determines concentrations of EOCs and ultimately their public health risks. Consequently, poorly managed wastewater treatment facilities may release EOCs into drinking water sources.
Some old municipalities in the USA have combined sewer system outfalls, while other areas have on-site wastewater systems situated in highly forested areas that are not served by municipal waste water treatment plants [177]. As such, communities in these areas are exposed to the highest risk, especially if they lack advanced drinking water treatment systems. Another factor increasing risk is spacio-temporal fluctuations of EOCs in surface water that result from seasonal hydroclimatic patterns. Such patterns dilute and mobilize contaminants from diffuse as well as point sources [10]. A few studies confirm that EOCs from wastewater treatment facilities, such as metformin and sulfamethoxazole, with consistent loading to aquatic systems depict dilution dynamics [180]. This is because wastewater effluents are moderated throughout high-flow seasons, but may increase during low-flow or drought periods. Apart from these, pharmaceuticals such as acetaminophen, caffeine, and sulfamethoxazole, are commonly associated with wastewater treatment plants. These were found ubiquitous across seasons and in water from all source types, but highest concentrations were recorded in cold seasons, corresponding to high consumer use and lower environmental attenuation rates [77].
A previous study on drinking water sources in the Susquehanna River Basin in America showed that reservoirs had lower EOC occurrences than riverine sources due to higher forested land use and increased residence times for natural attenuation in reservoir source sites [177]. The results of this study also revealed that naproxen and ofloxacin posed a high risk in fish Daphnia and algae in riverine and reservoir sources. In addition, the exposure route determines the severity of the effects of EOCs since acetaminophen and sulfamethoxazole posed a lower risk (RQ<0.01) through fish consumption rather than through drinking water. Demographical factors influence the use of pharmaceutical and personal care products by consumers, thus, impacting release into DWS and the resulting human exposure risks [177]. Poor agricultural activities are one overlooked factor that increases the risk to EOCs. Such practices include improper application of manure, biosolids, and pesticides, which may increase release of EOCs into DWS.
High human exposure to EOCs in DWS correlates with risk severity. Regardless of the exposure routes, EOCs may have potential additive and synergistic effects on human health from mixtures of EOCs originating from multiple exposure routes [177,181]. Risks also differ due to the varying sensitivity of populations, including various age groups, and underlying health conditions [181]. Additionally, EOCs reaching drinking water from agricultural sources (e.g. thiamethoxan) exhibit accretion responses with elevated concentrations during higher flow conditions as the dominant transport pathway is surface runoff [182]. Caffeine and acetaminophen are generally removed fairly well through conventional wastewater treatment. However, they exhibit elevated or sustained concentration during high-flow events [177]. This suggests that they have other potential sources of EOCs in shallow lateral flow (e.g., septic tanks leach field), surface runoff from biosolids-embedded fields, and desorption from streamed sediments, among others.
Hot-spots for EOCs constitute high-risk factors. For example, areas with high concentrations of drugs excreted or disposed of in domestic sewer systems and landfill leachate, and effluents from hospitals and runoff from aquaculture and animal husbandry activities [183]. Household waste may also contribute to EOCs, particularly pharmaceuticals, in wastewater through the disposal of expired medicines into sinks and drains [184]. The EOCs subsequently contaminate drinking water sources through inadequate wastewater treatment and sewage leakage into the rivers. For instance, in Japan, pharmaceuticals such as ibuprofen, carbamazepine, crotamiton, and mefenamic acid and PCP were detected in rivers, illustrating a positive correlation between river flux and the occurrence of EOCs [185]. EOCs can contaminate groundwater through sewer and septic leakages [186]. In Taiwan, it was observed that concentrations of pharmaceuticals at water sites were highest (37.5%) for hospital effluents, followed by animal husbandry effluents and pharmaceutical manufacturing facilities, while minimum concentrations (<1%) were detected in aquaculture effluents [186]. This confirms that EOCs find their way to drinking water from effluents from diverse avenues. To further demonstrate this connectivity, data from this study correlated with data on the consumption of pharmaceuticals in Taiwan, suggesting human contamination as the source.
Pharmaceuticals occurring in municipal effluents, wastewater treatment facilities, and freshwater fluctuate probably due to natural attenuation from photolysis, biotransformation, sorption, dispersion, and volatilization or a combination of these [187,188]. Owing to their non-volatile nature, EOCs persist in drinking water systems because natural attenuation by the various removal mechanisms is low. Natural attenuation only relies on sorption, biological, chemical, and photo transformation and dilution [177,188]. Several studies and literature previously focused on the fate of EOCs in sediments, surface water, wastewater treatment facilities, effluent streams, and groundwater systems.
A few studies have been conducted to assess emerging organic contaminants and their associated eco-toxicological effects in LICs. Literature survey shows that most studies have been carried out in China and developed countries, with only a few or no studies in other parts of the world [189,190]. Particularly, the research effort in Africa is still very limited, with a few countries involved in investigations on EOCs. For example, with regards to pharmaceutical compounds and their derivatives, only five countries, namely South Africa, Kenya, Cote d’Ivoire, Tunisia, Zambia , and Zimbabwe, out of 54 have collected data on the occurrence of EOCs in drinking water systems [24,191]. One study carried out in South Africa detected polychlorinated biphenyls, bisphenol A, and acetaminophen in 90% of effluent from wastewater treatment facilities at concentrations of up to 200 µg/L [191]. Another study in South African estuaries reported the presence of EOCs including polychlorinated biphenyls (PCBs) and PFASs in water [192]. The average concentration of pesticides in water and suspended particles were 0.16 µg/L and 18.6 µg/kg for endosulfan, 0.45 µg/L, and 19.6 µg/kg for chlorpyrifos, and 0.15 µg/L and 34 µg/kg for prothiofos, which exceeded the US EPA guidelines for drinking water.
Challenges of EOCs are common globally but are exaggerated in Africa by socio-economic complications that culminate in poor sanitation [191]. Africa’s urban population is expected to reach 2 billion by 2030, exceeding the capacity to supply adequate infrastructure for securing safe drinking water, waste disposal services, and sanitation. In addition, the population increase in Africa is linked to the increased production, consumption, and disposal of a wide range of synthetic organic compounds [24]. This has exacerbated the challenges of wastewater and water management [193]. The installed conventional wastewater treatment facilities cannot remove the emerging contaminants, as they were not designed for such pollutants and hence their release into the receiving aquatic environment. For instance, the activated sludge-based technology, and even more advanced wastewater treatment technologies such as the membrane bioreactor processes, are not able to remove most of the EOCs in urban wastewaters [191]. A previous study conducted in South Africa to assess the occurrence and quantity of several EOCs in WWTP effluents confirmed the presence EOCs in 90% of the samples [191]. Non-steroidal anti-inflammatory drugs such as ibuprofen, ketoprofen, diclofenac and naproxen have also been detected in African effluents from wastewater treatment facilities in South Africa, Tunisia and Nigeria at concentrations around 410 µg/L [191].
The majority of groundwater systems in LICs in Africa have dissolution channels and fissures causing accelerated transport of water [194]. EOCs and naturally occurring hazardous compounds in soil, also find their way to aquifers due to groundwater recharge rate, aquifer type and depth, and land use that affects runoff. In Zimbabwe, Cameroon, Nigeria and Guinea, mining activities have been reported to mobilize EOCs to both ground and surface water [194]. Additionally, karst systems in LICs of Africa are prone to pollution from unconfined waste, particularly in systems that are in contact with bedrock outcrops and open water surfaces [194]. Karst aquifers are therefore the most vulnerable groundwater systems to anthropogenic pollution from EOCs, where half of detected compounds exceeded concentrations of 100 mg/L [189,194]. Water quality data, as well as hydrogeological evidence of management of groundwater resources, are scarce in sub-Saharan countries despite water quality being a critical challenge. Data obtained in studies in Europe and the USA cannot be directly applied elsewhere as the karst types differ significantly in age and degree of karstification as well as the EOCs studied.
Informal settlements are common in LICs due to socio-economic challenges, resulting in poor sanitation, a scenario well documented in Lusaka Zambia. Furthermore, it is estimated that 70% of African urban populations are not connected to centralized wastewater treatment systems, hence untreated or partially treated effluent is released into surface waters or the soil [24]. Communities is such areas rely on water sources such as wells, rivers, and lagoons. In Lagos Nigeria, EDCs at concentrations around 2.5 µg/L were detected in lagoons [195]. As a result of the higher density of contaminant sources, exposure risks are also likely to be significant [24]. In the case of Lusaka, water and sanitation authorities had difficulties keeping up with sanitation services, and they sought intervention from investors and non-governmental organizations [194]. This initiative has seen an improvement through the introduction of community involvement and updating of physical infrastructure that includes wastewater treatment facilities.
Another challenge facing LICs is lack of appropriate technologies for the detection of the EOCs. Policy formulation on EOCs depends on the availability of data. However, LICs lag behind in terms of technologies for data collection. Ultra-sensitive analytical techniques are required for the quantitation of most EOCs in the aquatic environment [196]. Besides, the skills for data collection and interpretation could be limited, while the cost of monitoring the EOCs could be prohibitively high.
5.3. Human Exposure Pathways
EOCs are introduced into DWS via a number of point and non-point sources, and the receptors are including environment, biota, and humans [30]. The environment as a receptor involves water, soil, and air, while biota includes soil, marine, and aquatic organisms. The former has been thoroughly investigated, while specific receptors within an organism at the cellular, process, and system levels as well as in the human body are not well studied [197]. At the organism level, receptors of EOCs include organs, systems (e.g., respiratory, endocrine, enzyme), biomolecules, biochemical processes, and specific target cell receptors.
The pathways through which humans are exposed to EOCs in water include primarily drinking, then inhalation, and dermal pathways. Studies show they pose severe public health risks in communities that depend on contaminated water sources [178]. PFOA and PFOs are the most thoroughly studied EOCs that have been detected in, and are associated with, surface water and drinking water. These have found their way to human organs and tissues, for instance, serum and breast milk . Other exposure pathways such as dermal absorption and inhalation of volatile EOCs lightly contribute to human exposure [198]. When inhaled, EOCs enter and irritate the nasal cavity, air passages, and lungs [199]. They become deposited in the airways or absorbed by the lungs into the bloodstream. Blood then carries these substances to the rest of the organs.
Dermal exposure to EOCs happens when the contaminants come in contact with the skin, for instance in the shower or while swimming. Although inhalation is considered the greatest exposure route for volatile EOCs, the skin can also absorb the contaminant in vapour form. However, there is inadequate evidence confirming significant correlations between EOCs and a number of health conditions. A small number of sites have been identified on the human body as suspected targets, especially the bladder. Colorectal tumours and bladder tumours have been associated with disinfectant by-products found in drinking water and have been correlated with drinking water habits [199].
The receptors for PFOAs are the most studied revealing its ligand nature, activating peroxisome proliferator-activated receptor α (PRARα) . PFOAs increase the incidence of hepatocellular adenoma, and the peroxisomal mass and fatty acid β-oxidation, and expansion of the smooth endoplasmic reticulum. Generally, PFOAs have high bioaccumulation potential, hence their occurrence in human tissues [200]. In the kidneys and lungs, perfluoro-butanoic acid was the most frequently detected compound. In the liver and brain, perfluorohexanoic acid showed maximum levels, while the concentration of perfluorooctanoic acid was highest in bone (about 20.9 ng/g). Lung tissues had the highest PFA concentration, while perfluorooctanoic acid and perfluorooctane sulfonic acid were predominant in the bone and liver, respectively [197]. Due to their polar and hydrophobic nature, EOCs containing fluorine have an affinity for proteins, and thus, have been detected in breast milk, human serum, and cord blood [201]. Of all EOCs, halogenated compounds such as polychlorinated dibenzo-p-dioxins, and dibenzofurans, and PFAs tend to bioaccumulate and so persist, and can be detected in urine [202]. Some studies, however, suggest that only one-fifth of the total body clearance is renal, implying the urinary system is not the sole route of elimination of EOCs. The elimination half-life of PFOA in humans was estimated at 3.5 years, while and that of PFOs was about 4.8 years [203]. In drinking water, EOCs have a half-life value in the range of 2.3-3.3 years. The difference in chain lengths of the organic contaminants also determines the accumulation and distribution in different tissues. A study on Tarragona community members in Spain confirmed a varying distribution of a wide range of EOCs that include PFOA, PFOS, and PFAs [203]. Evidence has shown that PFOA is mostly reported high in the liver, breast milk, and blood and less in the thyroid.
Other receptors of EOCs are the homeostatic, metabolic, immune, and hormonal systems. PFCs affect glucose homeostasis, confirming their residence in the system. High PFNA levels in serum are associated with hyperglycemia and a higher B-cell activity [204]. A previous study showed an association between uric acid and PFCs, showing that PFOA serum concentrations are significantly related to a higher rate of hyperuricemia, a potential risk factor for hypertension and cardiovascular diseases [205]. Such is evidence of the deposit and persistence of the fluoro- compounds in the urinary system and serum.
There is overwhelming evidence on the adverse effects of EOCs in the human body. Human exposure to potential hormonal disruptors and PFCs might decrease fertility [206]. PFOs were reported to decrease women’s capacity to lactate, while perfluoroalkyl acids compromised testicular function and semen quality in males [207,208]. The prevalence of thyroid diseases such as papillary carcinoma and follicular carcinoma were shown to be directly linked to the concentration of PFCs in serum and tissue [209]. PFOs and PFOAs induce the increase of serum thyroxine while decreasing triiodothyronine uptake in humans. In a study performed on adolescents and children, PFOA was substantially associated with increased total lipid and low-density lipoprotein cholesterol, while PFOs were related to elevated total lipid, and lipoprotein cholesterol [210]. There also is evidence that PFOA and PFOs induce gene modifications during the metabolism of lipids in humans.
The bioaccumulation of EOCs in humans has been extensively studied using model animal. Suitable model organisms for screening sediment toxicity and assessing bioaccumulation are benthic fauna such as earthworms. For instance, Lumbriculus variegalusis intensively used in bioaccumulation studies they can burrow into sediments and tolerate highly contaminated areas [211]. Another worm species, L. variegalus, degraded and metabolized fipronil in sediments containing extremely high total organic carbon (39% w/w) spiked with pp’- dichlorodiphenyldichloethylene, dieldrin, fipronil, and triclosan [211]. The results showed that the concentrations of fipronil in tissue reached a peak after 2 days, and showed a 70% decrease in sediment. Many pharmaceutical compounds contain bioactive components with chronic effects on non-target biota. A bioconcentration factor of 113 was reported in goldfish upon exposure to high concentrations of pharmaceuticals and personal care products for 14 days [212]. The chronic effect could lead to gene mutation and a decline in fish populations [213]. Since humans are frequently exposed to a cock-tail of physico-chemically varied compounds rather than single contaminants, deciphering the severity of health consequences becomes complex.
Rodent models have also been used in studying the potential carcinogenicity of PFOs and PFOAs. One study demonstrated that EOCs cause pancreatic adenocarcinoma, benign liver adenomas, and Leydig cell adenomas [213]. In a lifetime feeding study, male rats suffered from hepatocellular adenomas after being fed on PFOA for 2 years [188]. Besides rodents, aquatic organisms such as Daphnia and molluscs are commonly used model organisms in EOC articulation [177,214].
Over 98% of the US population has been reported to have PFAS in serum [215]. Results suggested an association between exposure to PFOA and kidney cancer, although it remained unclear whether PFOA or other PFAS are renal carcinogens or if they influence the risk of renal cell carcinoma at concentrations observed in the general population. A range of EOCs were detected in a study on the urine of adolescents were screened to detect and identify new emerging contaminants [216]. The identified EOCs and their metabolites were recommended as candidate biomarkers of exposure in future studies. Going forward, more comprehensive studies that use human models are recommended as they give in-depth statistics that can help curb the effects of emerging organic contaminants.
6. Human Health Risks
The concentrations of some EOCs might have exceeded the minimal concentration that can pose human health hazards (Table 2 and Table 3). In addition, the concentrations varied with the type of EOC and season. Several EOCs were detected at low concentrations (Table 2), however, their recommended limits are still not sufficiently studied and determined. Some antibiotics have been reported at very low concentrations, indicating a low risk of microbes’ resistance selection and posing a moderate risk to aquatic biota and humans. However, some compounds might have exceeded their ecotoxicity concentration limits. Notably, the EOCs may be close to or exceed recommended limits in drinking water; thus, the risk they pose to public health must be quantified. Some studies also show that contaminants such as metal cations might interact with pharmaceutical compounds administered to humans and animals, or released into the environment causing greater public health risk [217]. For example, a previous study reported an interaction between bisphosphonates and mineral water containing high concentrations (80 mg/L) of calcium and magnesium reduce the absorption of risedronate in rats [217]. Consequently, such waters are not recommended when taking risedronate.
6.1. Evidence of Human Health Risks
Most EOCs have been suggested as environmental risky substances based on their human health risks. Acute and chronic toxic effects of EOCs on model animals and humans have been demonstrated in toxicology studies (Table 4).
Table 4.
Human health risks of Emerging Organic Contaminants in Humans.
| Type of EOC | Organism | Concentrations | Major Findings and Remarks | References |
|---|---|---|---|---|
| 1. Pharmaceuticals | ||||
| sulfonamides | humans | 20.06 μg/L- 1281.50 μg/L | Human health risk for age groups less than 12 months was reported. | [218] |
| Chloramphenicol, ciprofloxacin, sulfapyridine, doxycycline, enrofloxacin, florfenicol, levofloxacin, metronidazole, norfloxacin, sulfamethoxazole | humans | 0.5 -21.4 ng/L | Resistance election. | [219] |
| estrogen and sulfapyridine | Human | 0.09 - 304 ng/L | -Resistance selection. | [220] |
| Ciprofloxacin | Human | -Ciprofloxacin resistance. | [221] | |
| Bromate, perchlorate and chlorate | Human | -A potential cancer risk. | [222] | |
| fluoroquinolones, β-lactams, macrolides, phenicols, sulfonamides, tetracyclines | Human | concentrations at 0.0064 ng/mL -0.0089 ng/mL | -Accumulations in the body and detected in the urine. | [223] |
| 30 common antibiotics | Humans | 226.8~498.1ng/L | - The non-carcinogenic risk of different groups of people was reported. | [224] |
| 2. Personal care products | ||||
| Cyclic siloxanes D4(octamethylcyclotetrasiloxane) and D5 (decamethylcyclopentasiloxane) (personal care products) | Humans | -Affects the liver and also induces liver cell enzymes. -Primary target organ for D5 exposure by inhalation is the lung. |
[225] | |
| Nitro Musk (personal care products) | Humans | 5-10mmol/litre in surrounding media | Competitive binding capability to estrogen receptors. | [226] |
| Fragrances (personal care products) | Human | Facial dermatitis. | [227] | |
| Glycol ether (personal care products) | Human | Motile sperm count and infertility. | [228] | |
| Glycol ether metabolites (personal care products) | Human | Negative impact on the neurodevelopment of infants and children. | [229] | |
| Insect repellents (personal care products) | Human | Cause vomiting. | [230] | |
| Butylparaben & propylparaben (Personal care products) Parabens |
Human | Adverse birth outcomes decreased gestational age birth weight & body length of neonates. | [231] | |
| Methylparaben & propylparaben (personal care products) Parabens | Human | Increases gestational age. | [232] | |
| 3. Plasticizers | ||||
| plasticizers | Humans | 13.42–265.48 ng/L | -potential cancer risk. | [198] |
| Polyethylene terephthalate bottles | 0.046 and 0.71 μg/L | - Carcinogenic risk of 2.8 × 10−7. | [233] | |
| Plasticizers | Humans | Bio accumulation in the blood plasma and urine | [234] | |
| 4. Surfactants | ||||
| Alkyl sulfates (AS), linear alkylbenzene sulfonates (LAS), alcohol ethoxylates (AE), alkyl phenol ethoxylates (APE), alcohol ethoxy sulfates (AES), alpha olefin sulfonates (AOS) and secondary alkane sulfonates (SAS) | adult vertebrates | 1 to 20 mg/L. | -Acute toxic effects in adult vertebrates. -Acute oral toxicity to occur at doses of 650 to > 25,000 mg/kg. -No evidence for carcinogenic, mutagenic. |
[235] |
| 5. Flame retardants | ||||
| OPFRs | humans | 85.1 ng/L -325 ng/L, | - OPFRs in drinking water did not pose a major health concern for adults and children. | [83] |
| Polybrominated diphenyl ethers (PBDEs) | Humans | -Rapidly bioaccumulating-doubling every two to five years. | [236] | |
| Organophosphate flame retardants (OPFRs) | humans | median: 48.7 ng/L | estimated daily OPFRs intake was less than the oral reference dose values. | [82] |
| triphenyl phosphate, tris(1,3-dichloropropyl) phosphate | humans | 1.1 ng/mL and 1.2 ng/mL |
- endocrine-disrupting, reproductive toxins, carcinogens, neurotoxins -Flame retardants were detected in all urine samples, suggesting bio- accumulation. |
[237] |
| Organophosphate esters (OPEs) | humans | 13.42–265.48 ng/L | -potential cancer risk (>1.00E-6), no non-carcinogenic effects (<1). -Total OPEs in advanced DWTPs were much lower than those in conventional DWTPs. Relative to conventional DWTPs, advanced DWTPs removed approx. 65.6% and 36.5% of the carcinogenic risk and non-carcinogenic risk of OPEs, respectively. |
[32] |
| Flame retardants (FRs) | humans | Upto 71.05 ng/L | -The estimated daily intake (EDI) for all FRs was higher in children than adults. Both children and adults were at low risk (HQ < 1) | [86] |
| Organophosphate flame retardants (OPFRs) | humans | EDI through drinking water was ≤9.65 ng/kg body weight/day. | [238] | |
| 6 Endocrine disrupting chemicals | ||||
| Bisphenol A (BPA) | human | 0.4 to 25.5 μg/L | -Caused oocyte aneuploidy and reduced production of oestradiol decreased ovarian response including decreased peak oestradiol levels, decreased number of oocytes retrieved decreased pregnancy rates. |
[239] |
| BPA | human | <LOD to 65.3 μg/L. | -Unexplained infertility was present in 29% of the subjects decrease in peak oestradiol. |
[240] |
| 7. Gasoline additives | ||||
| MTBE | humans | 8 μM MTBE | -Insulin formed a molten globule -like structure. This shows MTBE promotes protein oxidation and the production of reactive oxygen species. | [241] |
| 8. Per- and Polyfluoroalkyl Substances (PFAS) | ||||
| Perfluorooctanoate (PFOA) and perfluorooctane sulfonate (PFOS) | Human (human liver HepaRG cell line) | concentrations of 40−50 ng/L | -No significant alterations in its activity were observed. | [242] |
| 9. Artificial food sweeteners | ||||
| Artificial sweeteners | human | 0.5-25 ng/L | -ASWs in groundwater did not appear to pose human a health risk. | [2] |
| Artificial sweeteners | human | Upto 21 µg/L | -Bio- accumulation detected in human waste. | [243] |
| 10. Food colourants or dyes | ||||
| tartrazine | human | 1 - 50 mg | -Irritable and restless and had sleep disturbance. | [244] |
| 11. Ultraviolet sunscreening agents or UV blockers/filters | ||||
| Benzophenone-3 (BP-3) | humans, rats | -Decline in male birth weight and decreased gestational age in humans. -Decrease in epididymal sperm density and a prolonged oestrous cycle for females were observed in rats. |
[245] | |
| Benzophenone-3 | human breast epithelial cells, | 1μM -5μM BP-3 |
-DNA damage in epithelial cells. | [246] |
| UV-B filter octylmethoxycinnamate (OMC) | human | 1, 10, and 50 μmol/L | -A decrease in vasorelaxation of human umbilical arteries was revealed. Possibility of OMC acting as an inductor of pregnancy hypertensive disorders. | [247] |
| 2-hydroxy-4-methoxybenzophenone; 4-methylbenzylidene camphor; 2-ethylhexyl 4-methoxycinnamate; and butyl-methoxydibenzoylmethane, | human macrophages | -mRNA expression of cytokines up-regulated. UV filters may alter the immune system functions of humans and may lead to the development of asthma or allergic diseases. | [248] | |
Table 5.
Human health risks of emerging organic contaminants on animal bioassay species.
| Type of EOC | Organism | Concentrations | Major Findings and Remarks | References |
|---|---|---|---|---|
| Personal care products | ||||
| Cyclic siloxanes D4(octamethylcyclotetrasiloxane) and D5 (decamethylcyclopentasiloxane) (personal care products) | rats | -D4 is considered to impair fertility in rats. | [225] | |
| Musk ambrette, musk ketone and musk xylene | Rats and mice | dose level of 0.5 mg/kg (11 μg/cm2 of skin) | - Affects liver tissues. | [249] |
| Flame retardants | ||||
| Polybrominated diphenyl ethers (PBDEs) | mice | -Rapidly bioaccumulating-doubling every two to five years. | [236] | |
| Endocrine disrupting chemicals | ||||
| Estradiol benzoate Aroclor 1221 PCBs |
Pregnant Sprague-Dawley rats | 50 μg/kg | -Irregular oestrous cycles. | [250] |
| Bisphenol A (BPA) | mice | 1μg /kg to 10 mg /kg | -Number of primordial follicles in the primordial follicle pool decreases significantly. | [251] |
| Estradiol and diethylstilbestrol | mice | 0.02, 0.2, and 2.0 ng/g of body weight | -Prostate weight first increased then decreased with dose, resulting in an inverted-U dose-response. | [252] |
| Gasoline additives | ||||
| MTBE | mice and rats | -Cause testicular, uterine, and kidney cancer, as well as harm the kidney, immune system, liver, and central nervous system. | [119] | |
| MTBE | Sprague- Dawley rats | 1000, 250, or 0 mg/kg b.w | -The contaminant caused an increase in Leydig interstitial cell tumors of the testes and a dose-related increase in lymphomas and leukemias in the female rats. | [253] |
| Per- and Polyfluoroalkyl Substances (PFAS) | ||||
| PFOA, PFOS or N-EtFOSE | rats and mice | Injection at 100 mg/kg | -Decrease cytochrome oxidase activity in liver tissue. -Hepatomegaly as indicated by the increase in liver weight. |
[254] |
| PFOA | mice | 1, 5, 10, and 20 mg/kg body weight orally | -Trigger inflammatory markers e.g, HGF, IFN-γ, IL-6, TNF-α, and hepatic enzymes ALT and AST. | [255] |
| Perfluorononanoic acid (PFNA) | Mice | 1, 3, 5 or 10 mg/kg | -Could not carry their pregnancy successfully. -The majority of the PFNA-exposed pups survived a few days longer after birth. |
[256] |
| Perfluorooctanoic acid (PFOA) | Mice | exposed orally to 0.3 mg PFOA/kg/day | -Showed increased femoral periosteal area as well as decreased mineral density of tibias. | [257] |
| Artificial food sweeteners | ||||
| Artificial sweeteners | Mice | maximum Acceptable Daily Intake (ADI) ad libitum | -Increased body weight; food intake remained unchanged. | [258] |
| Artificial sweeteners | Mice | -Development of glucose intolerance through the induction of compositional and functional modifications to intestinal microbiota. | [259] | |
| Artificial sweeteners | rat | aspartame (3 mg/kg/day) or saccharin (3 mg/kg/day) or sucralose (1.5 mg/kg/day) | -Chronic intake of sweeteners significantly impaired PAL performance, lowered neuronal count in aspartame and increase Brain lipid peroxides. | [260] |
| Food colourants or dyes | ||||
| Amaranth, Sunset Yellow, Curcumin | Rats | an oral dose of 47-157.5 mg/kg | -Significantly decreased the weight of the thymus gland, a significant decrease in neutrophils and monocytes and a compensatory increase in lymphocytes. | [261] |
| Tartrazine and carmoisine, saccharin | Rats | -Alter biochemical markers in vital organs e.g. liver and kidney not only at higher doses but also at low doses | [262] | |
| Carmoisine, | Rats | 100 -1200 mg/kg body weight | -Increased incidences of adrenal blood/fibrin cysts or internal hyperplasia/medial hypertrophy of the pancreatic blood vessels and reduced body-weight gain. |
[263] |
| Ultraviolet sunscreening agents or UV blockers/filters | ||||
| Benzophenone-3 | mice | 1μM -5μM BP-3 |
R-loops and DNA damage were also detected in mammary epithelial cells of mice. | [246] |
| Benzophenone-3 | rats | BP-3 raised oxidative stress and induced apoptosis in the brain, as well as impaired spatial memory. | [264] | |
6.1.1. Pharmaceuticals
Mixtures of pharmaceuticals such as sulfonamides at concentrations ranging from 20.06 µg/L to1281.50 μg/L are reported to have adverse effects on age groups less than 12 months old [218]. A study suggested that sulfamethoxazole, sulfapyridine, metronidazole, chloramphenicol, levofloxacin, norfloxacin, doxycycline, florfenicol, and enrofloxacin ciprofloxacin at the concentration range of 0.5 - 21.4 ng/L can potentially induce antimicrobial resistance [219]. Sulfapyridine and estrogen pose the same health risk but at lower concentrations (0.09 – 304 ng/L) [219]. Antibiotics such as macrolides, β-lactams, tetracyclines, fluoroquinolones, sulfonamides, and phenicols at a very low concentrations in the range of 6.4 ng/L - 8.9 ng/L have been detected in urine and blood samples [223]. In fact, a related study suggested that, at a concentration of 226.8-498.1 ng/L, antibiotics pose non-carcinogenic risk [224]. However, the age of the individual influences the risk in the order: adults>adolescents>children.
6.1.2. Personal Care Products
The human health risk of personal care products in drinking water has not attracted adequate research interest. The majority of literature on personal care products is restricted to the environmental occurrence, and also their general human health risks without specifically linking it to drinking water (Table 4). Personal care products such as siloxanes [265], nitro musk [249], fragrances [227,266], Glycol ether , insect repellents , and butylparaben and propylparaben have been reported to cause the following in humans: (1) cyclic siloxanes affect enzyme activities in human livers and reproduction in rats [225], (2) at a concentration of 5-10 mmol/L, nitro musk competitively binds to estrogen receptors in humans [267]. A range of personal care products cause loss of body weight, reduced fecundity, and loss of liver tissues [228,249], (3) glycol ether affects the reproduction system and infant development [229,230], and (4) insect repellents and parabens have been reported to cause health risks in gestation period [268].
6.1.3. Plasticizers
Plasticizers at a concentration of 13.42–265.48 ng/L can potentially cause cancer [198]. A human risk assessment showed that, exposure of polyethylene terephthalate at a concentration range of 0.046 - 0.71 μg/L to solar radiation carries a carcinogenic risk of 2.8 × 10−7 [233]. These data suggest that, prolonged exposure of drinking water in plastic bottles to solar radiation poses potential cancer risks. Plasticizers in drinking water have been reported to accumulate in human bodies and were detected in blood plasma and urine (Table 4).
6.1.4. Surfactants
In comparison with other EOCs in drinking water, there are limited data on the human health risks posed by surfactants (Table 4). The rare exceptions have concentrated on the health risks of surfactants in model animals. For illustration, the toxicity of linear alkylbenzene sulfonates, alcohol ethoxylates, alkyl sulfates, alcohol ethoxy sulfates, alkyl phenol ethoxylates, secondary alkane sulfonates, and alpha-olefin sulfonates was investigated [235]. According to the findings, surfactants in adult vertebrates have: (1) acute oral toxicity at doses of 650 to > 25,000 mg/kg, and (2) no evidence for carcinogenic or mutagenic effects. Therefore, more studies are required to understand the human health risk of surfactants.
6.1.5. Flame Retardants
Compared to other EOCs, the public health risks associated with flame retardants have gained considerable research attention. Humans are exposed to flame retardants in drinking water at different levels, typically up to 9.65 ng/kg body weight/day [238]. Several studies, most of which used model animals, have investigated the human health risks associated with flame retardants to generate data for inferring human health risks (Table 2). Different types of flame retardants have been reported to cause human health risks. Examples of flame retardants include organophosphate compounds [82,83,238] and polybrominated diphenyl ethers [236]. As expected, flame retardants pose different human health risks at different concentrations. For example, at a concentration of 85.1 ng/L to 325 ng/L organophosphate flame retardants had no major health risk in both adults or children [83], while organophosphate esters at a concentration of 13.42–265.48 ng/L carry a potential cancer risk (>1.00x10-6) in humans [32]. Flame retardants such as tris(1,3-dichloropropyl) phosphate and triphenyl phosphate at a concentration of 1.1 ng/mL and 1.2 ng/mL, respectively pose neurotoxic, carcinogenic, and endocrine-disrupting properties [237]. Exposure to flame retardants through drinking water can bioaccumulate in the human body [236]. For instance, a study ion the effects of triphenyl phosphate and tris(1,3-dichloropropyl) phosphate on human health reported that flame retardants were detected 100% in the urine [237].
6.1.6. Endocrine Disrupting chemicals
Endocrine-disrupting chemicals such as phenols, phthalates, and organochlorines, are widely used and pose a significant risk to public health. Irregular oestrous cycles have been observed in rats given oral daily doses of 50 μg/kg estradiol benzoate, Aroclor 1221, and PCBs [250]. In another study, the quantity of primordial follicles within the primordial follicle pool significantly decreased in mice exposed to bisphenol A [251]. Bisphenol A at concentrations of 0.4 to 25.5 μg/L were found to cause oocyte aneuploidy, reduced oestradiol production, decreased peak oestradiol levels, decreased ovarian response, decreased number of oocytes retrieved, and decreased pregnancy rates in humans in another study [239]. Additionally, it was found that 29% of the study participants exposed to concentrations of up to 65.3 g/L were infertile.
6.1.7. Gasoline Additives
The occurrence of gasoline additives in drinking water systems and its exposure to humans has been associated with various health risks (Table 4). For example, compounds such as MTBE, ETBE, and TAME were found to occur in DWS with concentrations ranging from 10 to 100 ng/L [110]. However, there are few studies reporting health risks as a result of direct human exposure. Much of the evidence is through inference to exposure to model animal and test tube experiments. For instance, several studies showed that MTBE is toxic to animals and may cause cancer, primarily in rodents [241,269]. MTBE can cause cancers (e.g., kidney, testicular, and uterine) and damage the liver, central nervous system, and immune system [119]. The same authors associated an increase in wheezing and asthma symptoms in the winters of 1993–1994 and 1994–1995 to an increase in MTBE exposure. In a related laboratory study, male Sprague-Dawley rats exposed to MTBE developed more testicular Leydig interstitial cell tumours, and female rats developed lymphomas and leukaemias at higher doses [253]. However, because MTBE is quickly excreted through urine, it is not toxic to humans [270]. Although this study corroborated previous studies that linked the EOCS to the development of tumours in rats and mice, the tumours were not qualitatively relevant to humans [271]. Another study found that insulin formed a molten globule-like structure when exposed to 8 µM of MTBE [241]. This indicates that MTBE promotes protein oxidation and the generation of reactive oxygen species, and may reflect what can occur in the human body upon exposure.
6.1.8. Per- and Polyfluoroalkyl Substances
Numerous studies have proved that PFAS are toxic to multiple organs throughout the body, and can bioaccumulate in humans and other organisms. For example, PFOA, PFOS, and N-EtFOSE have been shown to decrease the activity of cytochrome oxidase in liver tissue, and hepatomegaly in rats and mice [254]. In some studies on mice, perfluorononanoic acid caused failure in pregnancy carriage, and the majority of the exposed pups survived a few days longer after birth [256]. Exposure of mice to perfluorooctanoic acid (0.3mg/kg daily) caused an increased femoral periosteal area as well as decreased mineral density of tibias [257]. There is a possibility that the health hazards identified in model animals can also affect humans, but more research is required.
6.1.9. Artificial Food Sweeteners
There is limited data on the human health risks posed by artificial food sweeteners in drinking water. Only a few exceptions exist [2,243]. Similar to other EOCs in water, artificial food sweeteners have different human health effects at different concentrations. For example, at maximum acceptable daily intake , artificial food sweeteners increased the body weight in mice [258]. At a concentration of 0.5-25 ng/L artificial food sweeteners did not pose health risks in humans [2]. Of note, up to 21 µg/L artificial food sweeteners were detected in human waste, showing bioaccumulation [243]. Saccharin (3 mg/kg/day), sucralose (1.5 mg/kg/day), and aspartame (3 mg/kg/day) caused impaired PAL performance, lower neuronal count in aspartame and increase brain lipid peroxides in the brain of rats [260]. Further studies directly linking the human health risks of artificial food sweeteners and drinking water are recommended especially in LICs.
6.1.10. Food Colourants or Dyes
Concerns about the harmful effects of synthetic food colourants and dyes on human health are increasing. Previous studies have investigated the toxicity of food colourants and dyes to model animals. For example, Amaranth, Sunset Yellow, and Curcumin at concentrations of 47-157.5 mg/kg administered daily to rats significantly decreased the weight of the thymus gland, as well as in neutrophils and monocytes [272]. A separate study on ratsreported that tartrazine, carmoisine, and saccharin at concentrations of 5.4 - 52.91 µg/L altered biochemical markers in vital organs such as the liver and kidney even at low doses [262]. Tartrazine has been shown to cause irritability, restlessness, and sleep disturbance in children at concentrations of 1 - 50 mg [244]. However, data on human health effects of food colourants and dyes are still limited.
6.1.11. Ultraviolet Sunscreening Agents or UV Blockers/Filters
Ultraviolet blockers/filters are frequently used in personal care products, and human exposure to these EOCs, primarily through the consumption of contaminated drinking water, may pose potential health hazards (Table 4). For instance, it has been reported that substances like 2-ethylhexyl-4-methoxycinnamate, butyl-methoxydibenzoylmethane, 4-methylbenzylidene camphor, and 2-hydroxy-4-methoxybenzophenone up-regulate the mRNA expression of cytokines [248]. The immune system may be altered as a result of this activity, which may also contribute to the emergence of asthma or allergy illnesses. In another study, the thyroid hormone thyroxine (T4) was reported to compete with several organic UV filters for the capacity to attach to transport proteins such as transthyretin (TTR). As a result, they have toxic effects that are harmful to human health [273]. Organic UV filters, 2,2′,4,4′-tetrahydroxybenzophenone, 2,4-dihydroxybenzophenone, 4,4′-dihydroxybenzophenone, and 4-hydroxybenzophenone exhibited a high affinity to TTR [273]. A related study reported that the 4-hydroxyl group of benzophenone-1 and -2 UV-filters can potently inhibit human, rat, and mouse gonadal 3β-hydroxysteroid dehydrogenases, and this would interfere with potency and progesterone secretion [274]. Octylmethoxycinnamate (OMC), a UV-B filter, altered the reactivity of the rat aorta, contributing to endothelial dysfunction [275]. Long-term human exposure to OMC may increase the risk of cardiovascular disease. Furthermore, OMC was found to reduce vasorelaxation of human umbilical arteries. This can lead to hypertensive disorders during pregnancy.
6.1.12. Musks and Fragrances
Musk fragrances are aromatic compounds used in the manufacture of personal care and household products [265,276], and in this review some musk fragrances are discussed under personal care products (Table 2). Relatively low concentrations of these compounds were detected in drinking water systems, and so human exposure is mainly via ingestion [276,277]. Although the mean concentrations of the musk fragrances recorded was relatively low, research is not conclusive on their impacts on human health risks. The detection of synthetic musk fragrances in tissues of marine organisms including crustaceans, bivalves, fish, and marine birds, as well as their ability to accumulate in tissues poses threats to animal health, including humans [276,278]. Studies have reported that musk fragrances have adverse effects on organs such as the liver. For example, musk ketone and musk xylene possess enzyme induction properties that cause changes in liver weight [249]. Musk ketone and musk xylene have been reported to have carcinogenic properties, but related studies using rats and mice showed they are nongenotoxic substances which exhibit cogenotoxicity due to their enzyme-inducing properties [169]. Nitro-musks also exhibit competitive binding capability to estrogen receptors disrupting reproductive cycles [226]. Apart from human risks, nitro musk affected the body weight and fecundity of spawning Danio rerio females and increased early life stage mortality [144,267]. More studies are required to fully understand the effects of musk fragrances on human health.
6.2. Linking EOCs in Drinking Water to Human health Risks: A Critique and Look Ahead
The human exposure and health risks of EOCs continue to attract public and research interest globally [1,210]. Despite the widespread occurrence of antibiotics in DWS, there is no conclusive evidence of human exposure risks. However, a few studies suggest that human health exposure risks of antibiotics are negligible [45]. Even then, long-term exposure may have adverse health effects. Generally, the concentrations of antibiotics in DWS is low. Therefore, focusing on concentrations in water and particular antibiotics could be misleading. Some EOCs persist within organisms and tend to bioaccumulate due to their poor biodegradability. For example, sulfadoxine and sulfamethoxazole have poor biodegradability and continue within the environment. Furthermore, drinking contaminated water can result in the bioaccumulation of pharmaceuticals in tissues [43], raising concern over cumulative effects on human health.
Although EOCs are a diverse group, a closer examination of the scientific evidence, including reviews on the human health risks revealed the following generic issues relating to all human health risks of EOCs:
- (1)
- A dire lack of quantitative evidence based on case-control epidemiological or toxicological studies establishing the link between the detection of EOCs in DWS, and even other environmental matrices to specific adverse human health outcomes.
- (2)
- Human dose-response models for EOCs that account for multiple exposure sources and routes, fate and behaviour in the human body, receptors, and toxicity mechanisms are still lacking. Moreover, the fate and behaviour of EOCs in human bodies is relatively under-studied [1].
- (3)
- Rather, human exposure and health risks are simply based on inferential evidence, where detection in drinking water or other media relevant to human exposure is interpreted to constitute a significant human health hazard.
As pointed out in our earlier reviews, this generic lack of direct evidence applies to all groups of emerging contaminants, including: (1) emerging organic contaminants as discussed here [279], (2) emerging biotoxins such as antibiotic resistance genes and antibiotic-resistant bacteria [280,281], (3) microplastics [282], and emerging inorganic contaminants such as high-technology rare earth elements [8,283].
Several reasons may account for this lack of quantitative direct evidence on human health risks, including:
- (1)
- Research on EOCs and their health risks continues to be dominated by environmental scientists, with limited expertise in conducting case-control epidemiological studies to link EOCs in environmental matrices, including drinking water, to adverse human health outcomes.
- (2)
- Medical researchers including human epidemiologists and toxicologists with expertise in conducting case-control epidemiological studies predominantly focus on human morbidity and mortality associated with pathogens, while paying limited attention to contaminants including emerging ones. In addition, medical researchers tend to focus on clinical settings, and rarely track the epidemiological origins of diseases in the environment outside clinical settings.
- (3)
- Research entailing the use of humans as experimental objects also suffers from serious ethical and safety approval issues [284]. Such stringent conditions may constrain the acquisition of direct evidence on the human health risks of EOCs.
In light of this, developed countries for instance, those in the European Union (EU) have adopted the Precautionary Principle as a basis to mitigate potential human health risks of EOCs [285]. In the EU, a maximum individual concentration of EOCs such as pharmaceuticals have been set [286]. Using Germany as an illustrative example, we briefly explore how EOCs are regulated in developed countries. In Germany, the risk assessment of parent pharmaceutical compounds and their residues in drinking water is conducted by the Federal Environmental Agency (UBA). To evaluate the public health risks of pharmaceuticals in drinking water, UBA specifies detected concentrations under three categories: (1) health orientation values, (2) guideline values, and (3) intervention values. On the one hand, in cases where the maximum guideline values and health orientation values are not exceeded, drinking water is regarded and declared safe for human consumption. On the other hand, if the values detected in drinking water reach or exceed the intervention values, the drinking water is classified as unsafe for human consumption. In such cases, the origins or sources of the pharmaceutical concern should be investigated and their concentration reduced as far as possible to concentrations below the intervention values.
For EOCs that are known to be non-genotoxic, Germany’s UBA recommends a maximum target guideline concentration of 0.1 µg/L per individual substance to minimize potential consumer health risks [286]. For concentrations below and up to this maximum concentration limit, a detailed health assessment is not necessary, because no human health risk is expected in any of the human age groups including infants, toddlers, and the elderly. In contrast, in low-income countries, it appears there have been limited efforts to date to set some guideline limits for drinking water based on the Precautionary Principle. In this regard, the European Community approach may provide a starting point for LICs. However, the guideline limits in low-income countries may need to be higher than those in developed ones due to poor technological development in the former including a lack of advanced methods for drinking water treatment to achieve very low concentrations of less than 0.1 µg/L.
Given the foregoing, establishing the link between the detection of EOCs in drinking water systems and other human-relevant environmental matrices, and adverse human health outcomes constitute the next research frontier on EOCs. Such research should entail the translation of scientific evidence into the next-generation risk assessment tools to be used as a decision-support tool to mitigate the human health risks of EOCs.
7. Future Directions and Conclusions
7.1. Future Directions and Perspectives
Compared to other aquatic environments such as wastewater systems, EOCs in drinking water systems have received relatively limited research attention. The existing literature on EOCs in drinking water systems is dominated by studies focusing on the occurrence, behaviour, and fate of EOCs. The bulk of the earlier studies on EOCs in drinking water systems is dominated by work conducted in developed countries, specifically Europe and North America. Further work is required to address five key knowledge gaps about EOCs and their human health risks.
- (1) Mass loads of EOCs from delivered into drinking water systems from various sources
Data on the sources of EOCs detected in drinking water systems remain largely qualitative. Hence, limited quantitative data exist on the influence of various sources of EOCs to drinking water sources. There is a need to quantify mass loads of EOCs contributed from various points and diffuse sources into the drinking water systems. In addition, the dominant dissemination and transfer pathways and their relative contribution of EOCs from the source to the drinking water system need to be determined.
- (2) Removal of EOCs in low-cost drinking water treatment systems
Studies investigating the removal of EOCs in aquatic systems tend to focus on advanced methods commonly used or applicable n high-income settings. In LICs, several low-cost water treatment approaches such as solar disinfection, boiling, chlorination, bio-sand filtration, and ceramic filters are widely used and promoted for water treatment. However, the behaviour and fate, including the removal of EOCs in such low-cost drinking water treatment systems are poorly understood. Therefore, it is unclear what low-cost drinking water treatment methods are most appropriate for the removal of EOCs in contaminated drinking water. This highlights the need to investigate the removal of EOCs by various low-cost drinking water treatment methods.
- (3) Human exposure and intake of EOCs via drinking water
Potable water from drinking water systems serves multiple purposes including drinking, cooking, and bathing. Each of these uses may constitute a potential human exposure pathway via ingestion, dermal intake, and inhalation. Yet evidence on the extent of human exposure to EOCs via the various possible intake routes is still lacking. In addition, quantitative data on the total daily intake of EOCs via drinking water is currently unknown. Such information is crucial for understanding human exposure and health risks. Further work is required to quantify human intake via individual and combined intake routes.
- (4) Human health risks of EOCs in drinking water systems
Current evidence on human health risks of EOCs in drinking water systems remains largely inferential – the mere occurrence of EOCs in drinking water is construed to constitute human exposure and health risks. Such inferential evidence does not seem to consider the behaviour and fate of EOCs in the human body, including possible degradation, and biotransformation. In addition, the concept of the dose-response relationship is not addressed in such evidence. Thus, systematic human health risk assessments are based on quantitative tools such as: (1) disability-adjusted life years, and (2) case-control epidemiological experiments. Such studies should also quantify the human health burden of individuals and combined EOCs with regard to morbidity and mortality.
Research on human health risks of EOCs should also harness emerging or novel tools. These emerging tools include big data analytics, genomics, spatial tools (GIS and remote sensing), in silico computational methods, network analysis, and advanced analytical tools such as hyphenated and 2-D and 3-D methods. The use of emerging or novel tools in investigating the human and health risks of EOCs has been discussed in our earlier papers [4,27], hence is beyond the scope of the present review.
Understanding the health risks and burden of EOCs requires the contribution of medical experts including toxicologists, and epidemiologists. Yet currently, research on the human health risks of EOCs is dominated by environmental scientists, with limited contribution from experts in the medical field. In addition, the ‘human factor’ comprising of knowledge, attitudes, and practices of people at risk of exposure to EOCs via drinking water requires further investigation [1]. In particular, there is a need to investigate the level of awareness about EOCs, their health risks, and mitigation among people in high-risk areas such as informal settlements in LICs.
- (5) Comparative human health risks of legacy and emerging organic contaminants
In most LICs EOCs and legacy contaminants often co-occur in drinking water systems. This is due to high levels of aquatic pollution, and overreliance on unsafe drinking water sources coupled with poor access to centralized DWS [4]. In this regard, informal settlements such as refugee camps, squatter camps, and slums could be potential hotspots for human exposure to both legacy and emerging organic contaminants. However, comparative studies on human exposure and health risks, including morbidity and mortality are still lacking. Such information is critical for prioritizing the mitigation of legacy and EOCs to safeguard human health risks.
7.2. Conclusions
The present review investigates the occurrence, behaviour, fate, and human health risks of emerging organic contaminants in drinking water systems using the source-pathway-receptor-impact-mitigation continuum concept. Analysis of the evidence revealed the following:
- (1)
- A diverse range of EOCs belonging to the following classes was detected: pharmaceuticals, personal care products, solvents, plasticizers, endocrine disrupting compounds, gasoline additives, food colourants, artificial sweeteners, and musks and fragrances have been detected in drinking water systems.
- (2)
- The anthropogenic sources of EOCs detected in DWS including wastewater systems and industrial emissions were summarized, but data on mass loading from the various sources are currently unavailable
- (3)
- The behaviour and fate of EOCs in drinking water systems including removal processes in conventional and advanced drinking water systems were discussed. Limited data exist on the capacity of low-cost point-of-use drinking water treatment systems to remove EOCs, yet such methods are commonly used in LICs where human exposure and health risks could be high.
- (4)
- Human exposure to EOCs in drinking water systems may occur predominantly via ingestion of contaminated drinking water, and possibly via cooked foods, possibly dermal contact, and inhalation (e.g, during bathing). However, limited evidence exists on the relative contribution of the various human intake routes and intake rates.
- (5)
- The high-risk environments such as informal settlements (squatter camps, refugee camps slums) in LICs, and risk factors and behaviours predisposing humans to EOC exposure are discussed.
- (6)
- Existing data on the human health risks of the various EOCs are presented and critiqued. Overall, although EOCs pose potential human health risks, the evidence base remains weak, with the bulk of it being inferential data. This requires further research to produce quantitative epidemiological evidence directly relating the occurrence of EOCs in drinking water systems to specific adverse human health outcomes is still scarce.
To address the various information gaps highlights, future research directions were discussed under five thematic topics, including the need for quantitative human health risk assessment, and the application of emerging detection tools are discussed.
Author Contributions
Conceptualization, finalization, submission, and facilitating waiver of APC, WG; methodology, software, validation, formal analysis, investigation, resources, data curation, writing—original draft preparation, writing—review and editing, visualization, TTS, ZM, TK, RA, MG, CG, NC, WG; supervision, WG, APC funding acquisition, WG. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding and The APC was funded by MDPI waiver awarded to WG.
Acknowledgments
WG thanks the Alexander von Humboldt Foundation – this work was conducted during the course of an Alexander von Humboldt Fellowship.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gwenzi, W., Emerging contaminants: A handful of conceptual and organizing frameworks, in Emerging Contaminants in the Terrestrial-Aquatic-Atmosphere Continuum:. 2022, Elsevier. p. 3-15.
- Sharma, B.M., et al., Health and ecological risk assessment of emerging contaminants (pharmaceuticals, personal care products, and artificial sweeteners) in surface and groundwater (drinking water) in the Ganges River Basin, India. 2019. 646: p. 1459-1467. [CrossRef]
- Houtman, C.J.J.J.o.I.E.S., Emerging contaminants in surface waters and their relevance for the production of drinking water in Europe. 2010. 7(4): p. 271-295.
- Gwenzi, W. and N.J.S.o.t.T.E. Chaukura, Organic contaminants in African aquatic systems: current knowledge, health risks, and future research directions. 2018. 619: p. 1493-1514.
- Ouda, M., et al., Emerging contaminants in the water bodies of the Middle East and North Africa (MENA): A critical review. 2021. 754: p. 142177. [CrossRef]
- Selwe, K.P., et al., Emerging contaminant exposure to aquatic systems in the Southern African Development Community. 2022. 41(2): p. 382-395. [CrossRef]
- Picó, Y., D.J.A. Barceló, and b. chemistry, Emerging contaminants in biota. 2012, Springer. p. 2525-2526. [CrossRef]
- Gwenzi, W., et al., Sources, behaviour, and environmental and human health risks of high-technology rare earth elements as emerging contaminants. 2018. 636: p. 299-313. [CrossRef]
- Petrovic, M., et al., Emerging contaminants in waste waters: sources and occurrence. 2008: p. 1-35.
- Tran, N.H., M. Reinhard, and K.Y.-H.J.W.r. Gin, Occurrence and fate of emerging contaminants in municipal wastewater treatment plants from different geographical regions-a review. 2018. 133: p. 182-207. [CrossRef]
- Naidu, R., et al., Emerging contaminants in the environment: Risk-based analysis for better management. 2016. 154: p. 350-357. [CrossRef]
- Stuart, M., et al., Review of risk from potential emerging contaminants in UK groundwater. 2012. 416: p. 1-21. [CrossRef]
- Jardim, W.F., et al., An integrated approach to evaluate emerging contaminants in drinking water. 2012. 84: p. 3-8. [CrossRef]
- Schriks, M., et al., Toxicological relevance of emerging contaminants for drinking water quality. 2010. 44(2): p. 461-476. [CrossRef]
- Webb, S., et al., Indirect human exposure to pharmaceuticals via drinking water. Toxicol Lett, 2003. 142(3): p. 157-67. [CrossRef]
- Varjani, S.J. and M.J.W.r. Chaithanya Sudha, Treatment technologies for emerging organic contaminants removal from wastewater. 2018: p. 91-115.
- Wee, S.Y., et al., Tap water contamination: Multiclass endocrine disrupting compounds in different housing types in an urban settlement. 2021. 264: p. 128488. [CrossRef]
- Lu, C., et al., Neonicotinoid insecticides in the drinking water system–Fate, transportation, and their contributions to the overall dietary risks. 2020. 258: p. 113722.
- Luoma, S.N.J.T.p.o.e.n.r., Silver nanotechnologies and the environment. 2008. 15: p. 12-13.
- Shi, J., et al., Groundwater antibiotics and microplastics in a drinking-water source area, northern China: Occurrence, spatial distribution, risk assessment, and correlation. 2022. 210: p. 112855. [CrossRef]
- He, P., et al., Pharmaceuticals in drinking water sources and tap water in a city in the middle reaches of the Yangtze River: occurrence, spatiotemporal distribution, and risk assessment. 2022. 29(2): p. 2365-2374. [CrossRef]
- Offiong, N.-A.O., E.J. Inam, and J.B.J.C.A. Edet, Preliminary review of sources, fate, analytical challenges and regulatory status of emerging organic contaminants in aquatic environments in selected African countries. 2019. 2: p. 573-585. [CrossRef]
- Hellar-Kihampa, H.J.A.J.o.E.S. and Technology, Another decade of water quality assessment studies in Tanzania: status, challenges and future prospects. 2017. 11(7): p. 349-360.
- Sorensen, J., et al., Emerging contaminants in urban groundwater sources in Africa. 2015. 72: p. 51-63.
- Hirsch, P., et al., National interests and transboundary water governance in the Mekong. 2006: Australian Mekong Resource Centre, in collaboration with Danish ….
- Gwenzi, W., et al., Occurrence, human health risks, and removal of pharmaceuticals in aqueous systems: Current knowledge and future perspectives. 2021: p. 63-101.
- Gwenzi, W.J.S.o.t.T.E., Leaving no stone unturned in light of the COVID-19 faecal-oral hypothesis? A water, sanitation and hygiene (WASH) perspective targeting low-income countries. 2021. 753: p. 141751.
- Khan, H.K., et al., Occurrence, source apportionment and potential risks of selected PPCPs in groundwater used as a source of drinking water from key urban-rural settings of Pakistan. 2022. 807: p. 151010. [CrossRef]
- Wu, M., et al., Occurrence and fate of psychiatric pharmaceuticals in the urban water system of Shanghai, China. 2015. 138: p. 486-493. [CrossRef]
- Machado, K.C., et al., A preliminary nationwide survey of the presence of emerging contaminants in drinking and source waters in Brazil. 2016. 572: p. 138-146. [CrossRef]
- Giebułtowicz, J., G.J.E. Nałęcz-Jawecki, and E. Safety, Occurrence of antidepressant residues in the sewage-impacted Vistula and Utrata rivers and in tap water in Warsaw (Poland). 2014. 104: p. 103-109.
- Liu, J., et al., Formation of perfluorocarboxylic acids from photodegradation of tetrahydroperfluorocarboxylic acids in water. 2019. 655: p. 598-606. [CrossRef]
- Nasir, F.A.M., et al., Public awareness level and occurrence of pharmaceutical residues in drinking water with potential health risk: A study from Kajang (Malaysia). 2019. 185: p. 109681. [CrossRef]
- Wee, S.Y., et al., Occurrence of multiclass endocrine disrupting compounds in a drinking water supply system and associated risks. 2020. 10(1): p. 17755. [CrossRef]
- Kondor, A.C., et al., Occurrence and health risk assessment of pharmaceutically active compounds in riverbank filtrated drinking water. 2021. 41: p. 102039. [CrossRef]
- Santos, A.V., et al., Occurrence and risk assessment of pharmaceutically active compounds in water supply systems in Brazil. 2020. 746: p. 141011. [CrossRef]
- Kozisek, F., et al., Survey of human pharmaceuticals in drinking water in the Czech Republic. 2013. 11(1): p. 84-97. [CrossRef]
- Aristizabal-Ciro, C., et al., Monitoring pharmaceuticals and personal care products in reservoir water used for drinking water supply. 2017. 24: p. 7335-7347. [CrossRef]
- Jux, U., et al., Detection of pharmaceutical contaminations of river, pond, and tap water from Cologne (Germany) and surroundings. 2002. 205(5): p. 393-398. [CrossRef]
- Ślósarczyk, K., et al., Occurrence of pharmaceuticals and personal care products in the water environment of Poland: A review. 2021. 13(16): p. 2283.
- Oluwalana, A.E., et al., The screening of emerging micropollutants in wastewater in Sol Plaatje Municipality, Northern Cape, South Africa. 2022. 314: p. 120275. [CrossRef]
- Moodley, B., G. Birungi, and P. Ndungu, Detection and quantification of emerging organic pollutants in the Umgeni and Msunduzi Rivers. 2016.
- Tahrani, L., et al., Occurrence of antibiotics in pharmaceutical industrial wastewater, wastewater treatment plant and sea waters in Tunisia. 2016. 14(2): p. 208-213. [CrossRef]
- Chaib, O., et al., Occurrence and Seasonal Variation of Antibiotics in Fez-Morocco Surface Water. American Journal of Environmental Sciences, 2019. 15(4). [CrossRef]
- Ebele, A.J., et al., Occurrence, seasonal variation and human exposure to pharmaceuticals and personal care products in surface water, groundwater and drinking water in Lagos State, Nigeria. 2020. 6: p. 124-132. [CrossRef]
- Osunmakinde, C.S., et al., Verification and validation of analytical methods for testing the levels of PPHCPs (pharmaceutical & personal health care products) in treated drinking water and sewage: report to the Water Research Commission. 2013: Water Research Commission Pretoria.
- Mhuka, V., S. Dube, and M.M.J.E.C. Nindi, Occurrence of pharmaceutical and personal care products (PPCPs) in wastewater and receiving waters in South Africa using LC-Orbitrap™ MS. 2020. 6: p. 250-258. [CrossRef]
- Farounbi, A.I., N.P.J.E.S. Ngqwala, and P. Research, Occurrence of selected endocrine disrupting compounds in the eastern cape province of South Africa. 2020. 27(14): p. 17268-17279. [CrossRef]
- Agunbiade, F.O., B.J.E.m. Moodley, and assessment, Pharmaceuticals as emerging organic contaminants in Umgeni River water system, KwaZulu-Natal, South Africa. 2014. 186: p. 7273-7291. [CrossRef]
- Amdany, R., L. Chimuka, and E.J.W.S. Cukrowska, Determination of naproxen, ibuprofen and triclosan in wastewater using the polar organic chemical integrative sampler (POCIS): A laboratory calibration and field application. 2014. 40(3): p. 407-414. [CrossRef]
- Peng, Y., L. Gautam, and S.W.J.C. Hall, The detection of drugs of abuse and pharmaceuticals in drinking water using solid-phase extraction and liquid chromatography-mass spectrometry. 2019. 223: p. 438-447. [CrossRef]
- Wang, S., et al., Suspect screening to support source identification and risk assessment of organic micropollutants in the aquatic environment of a Sub-Saharan African urban center. 2022. 220: p. 118706. [CrossRef]
- Twinomucunguzi, F.R., et al., Emerging organic contaminants in shallow groundwater underlying two contrasting peri-urban areas in Uganda. 2021. 193: p. 1-25. [CrossRef]
- K'oreje, K., et al., Occurrence patterns of pharmaceutical residues in wastewater, surface water and groundwater of Nairobi and Kisumu city, Kenya. 2016. 149: p. 238-244. [CrossRef]
- Rutanhira, C., Occurrence of organic compounds in water and sediments in Sebakwe river. 2019.
- Caldas, S.S., et al., Occurrence of pesticides and PPCPs in surface and drinking water in southern Brazil: Data on 4-year monitoring. 2019. 30: p. 71-80. [CrossRef]
- Ramos, S., V. Homem, and L.J.J.o.C.A. Santos, Simultaneous determination of synthetic musks and UV-filters in water matrices by dispersive liquid-liquid microextraction followed by gas chromatography tandem mass-spectrometry. 2019. 1590: p. 47-57. [CrossRef]
- Wombacher, W.D. and K.C.J.J.o.E.E. Hornbuckle, Synthetic musk fragrances in a conventional drinking water treatment plant with lime softening. 2009. 135(11): p. 1192-1198.
- Relić, D., et al., Occurrence of synthetic musk compounds in surface, underground, waste and processed water samples in Belgrade, Serbia. 2017. 76: p. 1-10. [CrossRef]
- Li, C., et al., Graphene-derivatized silica composite as solid-phase extraction sorbent combined with GC–MS/MS for the determination of polycyclic musks in aqueous samples. 2018. 23(2): p. 318. [CrossRef]
- Arruda, V., M. Simões, and I.B.J.W. Gomes, Synthetic Musk Fragrances in Water Systems and Their Impact on Microbial Communities. 2022. 14(5): p. 692. [CrossRef]
- Bester, K.J.A.o.E.C. and Toxicology, Fate of triclosan and triclosan-methyl in sewage treatmentplants and surface waters. 2005. 49: p. 9-17.
- Bruchet, A., et al., Analysis of drugs and personal care products in French source and drinking waters: the analytical challenge and examples of application. 2005. 52(8): p. 53-61. [CrossRef]
- Díaz-Cruz, M.S., et al., Analysis of UV filters in tap water and other clean waters in Spain. 2012. 402: p. 2325-2333. [CrossRef]
- Jurado, A., et al., Urban groundwater contamination by residues of UV filters. J Hazard Mater, 2014. 271: p. 141-9. [CrossRef]
- Rodil, R., et al., Emerging pollutants in sewage, surface and drinking water in Galicia (NW Spain). 2012. 86(10): p. 1040-1049.
- Da Silva, C.P., et al., The occurrence of UV filters in natural and drinking water in São Paulo State (Brazil). 2015. 22: p. 19706-19715. [CrossRef]
- Rehman, H.u., et al., Heavy Metals, Pesticide, Plasticizers Contamination and Risk Analysis of Drinking Water Quality in the Newly Developed Housing Societies of Gujranwala, Pakistan. 2022. 14(22): p. 3787. [CrossRef]
- Penalver, A., et al., Determination of phthalate esters in water samples by solid-phase microextraction and gas chromatography with mass spectrometric detection. 2000. 872(1-2): p. 191-201. [CrossRef]
- Salazar-Beltrán, D., et al., Determination of phthalates in bottled water by automated on-line solid phase extraction coupled to liquid chromatography with UV detection. 2017. 168: p. 291-297.
- Zaater, M.F., Y.R. Tahboub, and A.N.J.J.o.c.s. Al Sayyed, Determination of phthalates in Jordanian bottled water using GC–MS and HPLC–UV: environmental study. 2014. 52(5): p. 447-452.
- Alshehri, M.M., et al., Determination of phthalates in bottled waters using solid-phase microextraction and gas chromatography tandem mass spectrometry. 2022. 304: p. 135214. [CrossRef]
- Annamalai, J. and N.J.A.C.A. Vasudevan, Detection of phthalate esters in PET bottled drinks and lake water using esterase/PANI/CNT/CuNP based electrochemical biosensor. 2020. 1135: p. 175-186.
- Kumar, A., et al., Bisphenol A in canned soft drinks, plastic-bottled water, and household water tank from Punjab, India. 2023. 9: p. 100205. [CrossRef]
- Struzina, L., et al., Occurrence of legacy and replacement plasticizers, bisphenols, and flame retardants in potable water in Montreal and South Africa. 2022. 840: p. 156581. [CrossRef]
- Kandie, F.J., et al., Occurrence and risk assessment of organic micropollutants in freshwater systems within the Lake Victoria South Basin, Kenya. 2020. 714: p. 136748. [CrossRef]
- Wanda, E.M., et al., Occurrence of emerging micropollutants in water systems in Gauteng, Mpumalanga, and North West Provinces, South Africa. 2017. 14(1): p. 79. [CrossRef]
- Eichhorn, P., et al., Incomplete degradation of linear alkylbenzene sulfonate surfactants in Brazilian surface waters and pursuit of their polar metabolites in drinking waters. 2002. 284(1-3): p. 123-134. [CrossRef]
- Eichhorn, P., et al., Occurrence and fate of linear and branched alkylbenzenesulfonates and their metabolites in surface waters in the Philippines. 2001. 269(1-3): p. 75-85. [CrossRef]
- Gomez, V., et al., Determination of non-ionic and anionic surfactants in environmental water matrices. 2011. 84(3): p. 859-866.
- Zhang, Q., et al., Organophosphate flame retardants in Hangzhou tap water system: Occurrence, distribution, and exposure risk assessment. 2022. 849: p. 157644. [CrossRef]
- Lee, S., et al., Occurrence and exposure assessment of organophosphate flame retardants (OPFRs) through the consumption of drinking water in Korea. 2016. 103: p. 182-188. [CrossRef]
- Li, J., et al., Occurrence of organophosphate flame retardants in drinking water from China. 2014. 54: p. 53-61. [CrossRef]
- Cristale, J., et al., Gas chromatography/mass spectrometry comprehensive analysis of organophosphorus, brominated flame retardants, by-products and formulation intermediates in water. 2012. 1241: p. 1-12. [CrossRef]
- Olukunle, O., et al., Determination of brominated flame retardants in Jukskei River catchment area in Gauteng, South Africa. 2012. 65(4): p. 743-749. [CrossRef]
- Khan, M.U., et al., First insight into the levels and distribution of flame retardants in potable water in Pakistan: an underestimated problem with an associated health risk diagnosis. 2016. 565: p. 346-359. [CrossRef]
- Onyekwere, O., et al., Occurrence and risk assessment of phenolic endocrine disrupting chemicals in shallow groundwater resource from selected Nigerian rural settlements. 2019. 30(2): p. 101-107. [CrossRef]
- Inam, E.J., et al., Ecological risks of phenolic endocrine disrupting compounds in an urban tropical river. 2019. 26: p. 21589-21597. [CrossRef]
- Chafi, S., A. Azzouz, and E.J.C. Ballesteros, Occurrence and distribution of endocrine disrupting chemicals and pharmaceuticals in the river Bouregreg (Rabat, Morocco). 2022. 287: p. 132202. [CrossRef]
- Huang, Y., A.A.J.A.S.C. Keller, and Engineering, Magnetic nanoparticle adsorbents for emerging organic contaminants. 2013. 1(7): p. 731-736. [CrossRef]
- Van Zijl, M.C., et al., Estrogenic activity, chemical levels and health risk assessment of municipal distribution point water from Pretoria and Cape Town, South Africa. 2017. 186: p. 305-313. [CrossRef]
- Aneck-Hahn, N.H., et al., Estrogenic activity, selected plasticizers and potential health risks associated with bottled water in South Africa. 2018. 16(2): p. 253-262. [CrossRef]
- Vázquez-Tapia, I., et al., Occurrence of emerging organic contaminants and endocrine disruptors in different water compartments in Mexico–A review. 2022: p. 136285. [CrossRef]
- Touraud, E., et al., Drug residues and endocrine disruptors in drinking water: risk for humans? Int J Hyg Environ Health, 2011. 214(6): p. 437-41.
- Gao, J., et al., Occurrence and distribution of organochlorine pesticides–lindane, p, p′-DDT, and heptachlor epoxide–in surface water of China. 2008. 34(8): p. 1097-1103.
- Jones, K.C. and P.J.E.p. De Voogt, Persistent organic pollutants (POPs): state of the science. 1999. 100(1-3): p. 209-221. [CrossRef]
- Rodgers-Gray, T.P., et al., Long-term temporal changes in the estrogenic composition of treated sewage effluent and its biological effects on fish. 2000. 34(8): p. 1521-1528. [CrossRef]
- Kuch, H.M., K.J.E.s. Ballschmiter, and technology, Determination of endocrine-disrupting phenolic compounds and estrogens in surface and drinking water by HRGC−(NCI)− MS in the picogram per liter range. 2001. 35(15): p. 3201-3206. [CrossRef]
- Teta, C., et al., Occurrence of oestrogenic pollutants and widespread feminisation of male tilapia in peri-urban dams in Bulawayo, Zimbabwe. 2018. 43(1): p. 17-26.
- Msigala, S.C., et al., Pollution by endocrine disrupting estrogens in aquatic ecosystems in Morogoro urban and peri-urban areas in Tanzania. 2017. 11(2): p. 122-131.
- Sörengård, M., et al., Long-distance transport of per-and polyfluoroalkyl substances (PFAS) in a Swedish drinking water aquifer. 2022. 311: p. 119981. [CrossRef]
- Skaggs, C.S. and B.A.J.J.o.C.A. Logue, Ultratrace analysis of per-and polyfluoroalkyl substances in drinking water using ice concentration linked with extractive stirrer and high performance liquid chromatography–tandem mass spectrometry. 2021. 1659: p. 462493.
- Appleman, T.D., et al., Treatment of poly-and perfluoroalkyl substances in US full-scale water treatment systems. 2014. 51: p. 246-255. [CrossRef]
- Post, G.B., et al., Occurrence of perfluorinated compounds in raw water from New Jersey public drinking water systems. 2013. 47(23): p. 13266-13275.
- Batayi, B., et al., Poly-and perfluoroalkyl substances (PFASs) in sediment samples from Roodeplaat and Hartbeespoort Dams, South Africa. 2020. 6: p. 367-375. [CrossRef]
- Dalahmeh, S., et al., Per-and polyfluoroalkyl substances (PFASs) in water, soil and plants in wetlands and agricultural areas in Kampala, Uganda. 2018. 631: p. 660-667.
- Ahrens, L., et al., Poly-and perfluoroalkylated substances (PFASs) in water, sediment and fish muscle tissue from Lake Tana, Ethiopia and implications for human exposure. 2016. 165: p. 352-357.
- Essumang, D.K., et al., Perfluoroalkyl acids (PFAAs) in the Pra and Kakum River basins and associated tap water in Ghana. 2017. 579: p. 729-735. [CrossRef]
- McCarthy, J.E. and M. Tiemann, MTBE in gasoline: clean air and drinking water issues. 2006.
- van Wezel, A., et al., Odour and flavour thresholds of gasoline additives (MTBE, ETBE and TAME) and their occurrence in Dutch drinking water collection areas. 2009. 76(5): p. 672-676.
- Mawhinney, D.B., et al., Artificial sweetener sucralose in US drinking water systems. 2011. 45(20): p. 8716-8722. [CrossRef]
- Scheurer, M., et al., Analysis and occurrence of seven artificial sweeteners in German waste water and surface water and in soil aquifer treatment (SAT). 2009. 394: p. 1585-1594. [CrossRef]
- Buerge, I.J., et al., Ubiquitous occurrence of the artificial sweetener acesulfame in the aquatic environment: an ideal chemical marker of domestic wastewater in groundwater. 2009. 43(12): p. 4381-4385.
- Scheurer, M., et al., Performance of conventional multi-barrier drinking water treatment plants for the removal of four artificial sweeteners. 2010. 44(12): p. 3573-3584. [CrossRef]
- Lange, F.T., et al., Artificial sweeteners—a recently recognized class of emerging environmental contaminants: a review. 2012. 403(9): p. 2503-2518. [CrossRef]
- Van Stempvoort, D.R., et al., Artificial sweeteners as potential tracers in groundwater in urban environments. Journal of Hydrology, 2011. 401(1): p. 126-133. [CrossRef]
- Tkaczyk-Wlizło, A., K. Mitrowska, and T. Błądek, Quantification of twenty pharmacologically active dyes in water samples using UPLC-MS/MS. Heliyon, 2022. 8(4): p. e09331. [CrossRef]
- Carneiro, P.A., et al., Assessment of water contamination caused by a mutagenic textile effluent/dyehouse effluent bearing disperse dyes. J Hazard Mater, 2010. 174(1-3): p. 694-9.
- Lei, M., et al., Overview of emerging contaminants and associated human health effects. 2015. 2015. [CrossRef]
- Naik, A.Q., et al., Environmental impact of the presence, distribution, and use of artificial sweeteners as emerging sources of pollution. 2021. 2021. [CrossRef]
- Praveena, S.M., et al., Non-nutritive artificial sweeteners as an emerging contaminant in environment: A global review and risks perspectives. 2019. 170: p. 699-707. [CrossRef]
- Tkaczyk-Wlizło, A. and K. Mitrowska, Occurrence and ecotoxicological risk assessment of pharmacologically active dyes in the environmental water of Poland. Chemosphere, 2023. 313: p. 137432. [CrossRef]
- Stackelberg, P.E., et al., Persistence of pharmaceutical compounds and other organic wastewater contaminants in a conventional drinking-water-treatment plant. 2004. 329(1-3): p. 99-113.
- Bond, T., et al., Occurrence and control of nitrogenous disinfection by-products in drinking water–a review. 2011. 45(15): p. 4341-4354. [CrossRef]
- Bond, T., M.R. Templeton, and N.J.J.o.h.m. Graham, Precursors of nitrogenous disinfection by-products in drinking water––a critical review and analysis. 2012. 235: p. 1-16. [CrossRef]
- Chaukura, N., et al., Contemporary issues on the occurrence and removal of disinfection byproducts in drinking water-a review. 2020. 8(2): p. 103659.
- Yang, X., et al., Identification of key precursors contributing to the formation of CX3R-type disinfection by-products along the typical full-scale drinking water treatment processes. 2023. 128: p. 81-92. [CrossRef]
- He, Y., et al., Prevalence, production, and ecotoxicity of chlorination-derived metformin byproducts in Chinese urban water systems. 2022. 816: p. 151665. [CrossRef]
- Trček, B., et al., The fate of benzotriazole pollutants in an urban oxic intergranular aquifer. 2018. 131: p. 264-273.
- Gowd, S.S., M.R. Reddy, and P.J.J.o.h.m. Govil, Assessment of heavy metal contamination in soils at Jajmau (Kanpur) and Unnao industrial areas of the Ganga Plain, Uttar Pradesh, India. 2010. 174(1-3): p. 113-121. [CrossRef]
- Simazaki, D., et al., Occurrence of selected pharmaceuticals at drinking water purification plants in Japan and implications for human health. 2015. 76: p. 187-200. [CrossRef]
- Sorlini, S., et al., Technologies for the control of emerging contaminants in drinking water treatment plants. 2019. 18(10).
- Valbonesi, P., et al., Contaminants of emerging concern in drinking water: Quality assessment by combining chemical and biological analysis. 2021. 758: p. 143624. [CrossRef]
- Petrović, M., S. Gonzalez, and D.J.T.T.i.A.C. Barceló, Analysis and removal of emerging contaminants in wastewater and drinking water. 2003. 22(10): p. 685-696.
- Ternes, T.A., et al., Removal of pharmaceuticals during drinking water treatment. 2002. 36(17): p. 3855-3863.
- Sillanpää, M., et al., Removal of natural organic matter in drinking water treatment by coagulation: A comprehensive review. 2018. 190: p. 54-71.
- Finkbeiner, P., et al., Understanding the potential for selective natural organic matter removal by ion exchange. 2018. 146: p. 256-263. [CrossRef]
- Jiang, J., et al., Removal of intermediate aromatic halogenated DBPs by activated carbon adsorption: a new approach to controlling halogenated DBPs in chlorinated drinking water. 2017. 51(6): p. 3435-3444. [CrossRef]
- McCleaf, P., et al., Removal efficiency of multiple poly-and perfluoroalkyl substances (PFASs) in drinking water using granular activated carbon (GAC) and anion exchange (AE) column tests. 2017. 120: p. 77-87. [CrossRef]
- Sun, M., et al., Legacy and emerging perfluoroalkyl substances are important drinking water contaminants in the Cape Fear River Watershed of North Carolina. 2016. 3(12): p. 415-419. [CrossRef]
- Khatibikamal, V., et al., Optimized poly (amidoamine) coated magnetic nanoparticles as adsorbent for the removal of nonylphenol from water. 2019. 145: p. 508-516. [CrossRef]
- Vasilachi, I.C., et al., Occurrence and fate of emerging pollutants in water environment and options for their removal. 2021. 13(2): p. 181. [CrossRef]
- Maier, R.M. and T.J. Gentry, Microorganisms and organic pollutants, in Environmental microbiology. 2015, Elsevier. p. 377-413.
- Caracciolo, A.B., et al., Degradation of a fluoroquinolone antibiotic in an urbanized stretch of the River Tiber. 2018. 136: p. 43-48.
- Wu, D., et al., The occurrence and risks of selected emerging pollutants in drinking water source areas in Henan, China. 2019. 16(21): p. 4109. [CrossRef]
- Schlüter-Vorberg, L., et al., Toxification by transformation in conventional and advanced wastewater treatment: the antiviral drug acyclovir. 2015. 2(12): p. 342-346.
- Wang, S. and J. Wang, Degradation of emerging contaminants by acclimated activated sludge. Environ Technol, 2018. 39(15): p. 1985-1993. [CrossRef]
- Gabarrón, S., et al., Evaluation of emerging contaminants in a drinking water treatment plant using electrodialysis reversal technology. 2016. 309: p. 192-201. [CrossRef]
- Rahman, M., et al., Endocrine disrupting compounds (EDCs) and pharmaceuticals and personal care products (PPCPs) in the aquatic environment: implications for the drinking water industry and global environmental health. 2009. 7(2): p. 224-243. [CrossRef]
- Clara, M., et al., Removal of selected pharmaceuticals, fragrances and endocrine disrupting compounds in a membrane bioreactor and conventional wastewater treatment plants. 2005. 39(19): p. 4797-4807. [CrossRef]
- Richardson, S.D., Disinfection by-products: formation and occurrence in drinking water. 2011.
- Sorlini, S., et al., CONTROL MEASURES FOR Cyanobacteria AND Cyanotoxins IN DRINKING WATER. 2018. 17(10). [CrossRef]
- Yang, Y., et al., Occurrences and removal of pharmaceuticals and personal care products (PPCPs) in drinking water and water/sewage treatment plants: A review. 2017. 596: p. 303-320. [CrossRef]
- Program, N.T., Haloacetic Acids Found as Water Disinfection Byproducts (Selected), in 15th Report on Carcinogens [Internet]. 2021, National Toxicology Program.
- Petrovic, M., et al., Occurrence and removal of estrogenic short-chain ethoxy nonylphenolic compounds and their halogenated derivatives during drinking water production. 2003. 37(19): p. 4442-4448. [CrossRef]
- Li, J., et al., Sand and sand-GAC filtration technologies in removing PPCPs: A review. 2022: p. 157680.
- Xu, L., Drinking water biofiltration: Removal of antibiotics and behaviour of antibiotic resistance genes. 2020, UCL (University College London).
- Zearley, T.L., R.S.J.E.s. Summers, and technology, Removal of trace organic micropollutants by drinking water biological filters. 2012. 46(17): p. 9412-9419. [CrossRef]
- Wee, S.Y. and A.Z.J.N.C.W. Aris, Occurrence and public-perceived risk of endocrine disrupting compounds in drinking water. 2019. 2(1): p. 4. [CrossRef]
- Bayabil, H., F. Teshome, and Y.J.E.S. Li, Emerging Contaminants in Soil and Water. Front. 2022. 10: p. 1-8.
- Schaider, L.A., et al., Pharmaceuticals, perfluorosurfactants, and other organic wastewater compounds in public drinking water wells in a shallow sand and gravel aquifer. 2014. 468: p. 384-393. [CrossRef]
- Law, I.B., et al., Validation of the Goreangab reclamation plant in Windhoek, Namibia against the 2008 Australian guidelines for water recycling. 2015. 5(1): p. 64-71. [CrossRef]
- Tortajada, C. and P.J.N. van Rensburg, Drink more recycled wastewater. 2020. 577(7788): p. 26-28.
- Muñiz-Bustamante, L., N. Caballero-Casero, and S.J.E.i. Rubio, Drugs of abuse in tap water from eight European countries: Determination by use of supramolecular solvents and tentative evaluation of risks to human health. 2022. 164: p. 107281. [CrossRef]
- Okoye, C.O., et al., Occurrence and fate of pharmaceuticals, personal care products (PPCPs) and pesticides in African water systems: A need for timely intervention. Heliyon, 2022. 8(3): p. e09143. [CrossRef]
- Duarte, D.J., et al., Human health risk assessment of pharmaceuticals in the European Vecht River. 2022. 18(6): p. 1639-1654. [CrossRef]
- Dey, S., F. Bano, and A. Malik, Pharmaceuticals and personal care product (PPCP) contamination—a global discharge inventory, in Pharmaceuticals and personal care products: waste management and treatment technology. 2019, Elsevier. p. 1-26.
- Paulsen, L., The health risks of chemicals in personal care products and their fate in the environment. 2015.
- Covaci, A., et al., Human exposure and health risks to emerging organic contaminants. 2012: p. 243-305.
- Becker, J.A. and A.I. Stefanakis, Pharmaceuticals and personal care products as emerging water contaminants, in Pharmaceutical Sciences: Breakthroughs in Research and Practice. 2017, IGI Global. p. 1457-1475.
- Mokra, K.J.I.J.o.M.S., Endocrine disruptor potential of short-and long-chain perfluoroalkyl substances (PFASs)—A synthesis of current knowledge with proposal of molecular mechanism. 2021. 22(4): p. 2148.
- Kumawat, M., et al., Occurrence and seasonal disparity of emerging endocrine disrupting chemicals in a drinking water supply system and associated health risk. 2022. 12(1): p. 9252. [CrossRef]
- Gonsioroski, A., V.E. Mourikes, and J.A.J.I.j.o.m.s. Flaws, Endocrine disruptors in water and their effects on the reproductive system. 2020. 21(6): p. 1929.
- Slama, R., S.J.E.i.o.r.h. Cordier, and fertility, Environmental contaminants and impacts on healthy and successful pregnancies. 2010.
- Fromme, H., et al., Perfluorinated compounds–exposure assessment for the general population in Western countries. 2009. 212(3): p. 239-270. [CrossRef]
- Herrick, R.L., et al., Polyfluoroalkyl substance exposure in the Mid-Ohio River Valley, 1991-2012. Environ Pollut, 2017. 228: p. 50-60. [CrossRef]
- Kibuye, F.A., et al., Influence of hydrologic and anthropogenic drivers on emerging organic contaminants in drinking water sources in the Susquehanna River Basin. 2020. 245: p. 125583. [CrossRef]
- Mukhopadhyay, A., S. Duttagupta, and A. Mukherjee, Emerging organic contaminants in global community drinking water sources and supply: A review of occurrence, processes and remediation. Journal of Environmental Chemical Engineering, 2022. 10(3): p. 107560.
- Bradley, P.M., et al., Expanded Target-Chemical Analysis Reveals Extensive Mixed-Organic-Contaminant Exposure in U.S. Streams. Environ Sci Technol, 2017. 51(9): p. 4792-4802. [CrossRef]
- Kibuye, F.A., et al., Influence of hydrologic and anthropogenic drivers on emerging organic contaminants in drinking water sources in the Susquehanna River Basin. Chemosphere, 2020. 245: p. 125583. [CrossRef]
- Bull, R.J., et al., Therapeutic dose as the point of departure in assessing potential health hazards from drugs in drinking water and recycled municipal wastewater. Regul Toxicol Pharmacol, 2011. 60(1): p. 1-19. [CrossRef]
- Kibuye, F.A., Effects of Natural and Anthropogenic Drivers on Emerging Organic Contaminants in Wastewater and Drinking Water Systems: Occurrence and Removal. 2019: The Pennsylvania State University.
- Nikolaou, A., S. Meric, and D. Fatta, Occurrence patterns of pharmaceuticals in water and wastewater environments. Anal Bioanal Chem, 2007. 387(4): p. 1225-34. [CrossRef]
- Kümmerer, K.J.J.o.e.m., The presence of pharmaceuticals in the environment due to human use–present knowledge and future challenges. 2009. 90(8): p. 2354-2366.
- Nakada, N., et al., Evaluation of pharmaceuticals and personal care products as water-soluble molecular markers of sewage. 2008. 42(17): p. 6347-6353. [CrossRef]
- Lin, A.Y.-C., T.-H. Yu, and C.-F.J.C. Lin, Pharmaceutical contamination in residential, industrial, and agricultural waste streams: risk to aqueous environments in Taiwan. 2008. 74(1): p. 131-141. [CrossRef]
- Gurr, C.J. and M. Reinhard, Harnessing natural attenuation of pharmaceuticals and hormones in rivers. 2006, ACS Publications.
- Pal, A., et al., Impacts of emerging organic contaminants on freshwater resources: review of recent occurrences, sources, fate and effects. 2010. 408(24): p. 6062-6069. [CrossRef]
- Reberski, J.L., et al., Emerging organic contaminants in karst groundwater: A global level assessment. 2022. 604: p. 127242. [CrossRef]
- Okeke, E.S., et al., Microplastic burden in Africa: A review of occurrence, impacts, and sustainability potential of bioplastics. Chemical Engineering Journal Advances, 2022. 12: p. 100402.
- Necibi, M.C., D. Dhiba, and S.J.S. El Hajjaji, Contaminants of emerging concern in African wastewater effluents: occurrence, impact and removal technologies. 2021. 13(3): p. 1125. [CrossRef]
- Olisah, C., et al., The state of persistent organic pollutants in South African estuaries: A review of environmental exposure and sources. 2021. 219: p. 112316.
- Ncube, E.J., K. Voyi, and H.J.W.S. Du Preez, Implementing a protocol for selection and prioritisation of organic contaminants in the drinking water value chain: Case study of Rand Water, South Africa. 2012. 38(4): p. 487-504. [CrossRef]
- Reaver, K.M., et al., Drinking Water Quality and Provision in Six Low-Income, Peri-Urban Communities of Lusaka, Zambia. Geohealth, 2021. 5(1): p. e2020GH000283.
- Ibor, O.R., et al., Public health implications of endocrine disrupting chemicals in drinking water and aquatic food resources in Nigeria: A state-of-the-science review. Science of The Total Environment, 2023. 858: p. 159835. [CrossRef]
- Geissen, V., et al., Emerging pollutants in the environment: A challenge for water resource management. International Soil and Water Conservation Research, 2015. 3(1): p. 57-65.
- Gwenzi, W., T.T. Simbanegavi, and P.J.W. Rzymski, Household disposal of pharmaceuticals in low-income settings: practices, health hazards, and research needs. 2023. 15(3): p. 476. [CrossRef]
- Li, J., et al., Assessing the threats of organophosphate esters (flame retardants and plasticizers) to drinking water safety based on USEPA oral reference dose (RfD) and oral cancer slope factor (SFO). 2019. 154: p. 84-93. [CrossRef]
- Salas, L.A., et al., LINE-1 methylation in granulocyte DNA and trihalomethane exposure is associated with bladder cancer risk. Epigenetics, 2014. 9(11): p. 1532-9.
- Ye, S., et al., The comprehensive analysis based study of perfluorinated compounds-Environmental explanation of bladder cancer progression. Ecotoxicol Environ Saf, 2022. 229: p. 113059. [CrossRef]
- Elcombe, C.R., et al., Hepatocellular hypertrophy and cell proliferation in Sprague–Dawley rats from dietary exposure to potassium perfluorooctanesulfonate results from increased expression of xenosensor nuclear receptors PPARα and CAR/PXR. 2012. 293(1-3): p. 16-29.
- Cui, L., et al., Excretion of PFOA and PFOS in male rats during a subchronic exposure. Arch Environ Contam Toxicol, 2010. 58(1): p. 205-13. [CrossRef]
- Pérez, F., et al., Accumulation of perfluoroalkyl substances in human tissues. 2013. 59: p. 354-362.
- Lin, C.-Y., et al., Association among serum perfluoroalkyl chemicals, glucose homeostasis, and metabolic syndrome in adolescents and adults. 2009. 32(4): p. 702-707. [CrossRef]
- Steenland, K., et al., Association of perfluorooctanoic acid (PFOA) and perfluorooctane sulfonate (PFOS) with uric acid among adults with elevated community exposure to PFOA. 2010. 118(2): p. 229-233. [CrossRef]
- Coperchini, F., et al., Thyroid disruption by perfluorooctane sulfonate (PFOS) and perfluorooctanoate (PFOA). J Endocrinol Invest, 2017. 40(2): p. 105-121. [CrossRef]
- Joensen, U.N., et al., Do perfluoroalkyl compounds impair human semen quality? Environ Health Perspect, 2009. 117(6): p. 923-7.
- Wogan, G.N., et al., Environmental and chemical carcinogenesis. Semin Cancer Biol, 2004. 14(6): p. 473-86. [CrossRef]
- Knox, S.S., et al., Perfluorocarbon exposure, gender and thyroid function in the C8 Health Project. 2011. 36(4): p. 403-410. [CrossRef]
- Omar, T.F.T., et al., Occurrence and level of emerging organic contaminant in fish and mollusk from Klang River estuary, Malaysia and assessment on human health risk. Environ Pollut, 2019. 248: p. 763-773. [CrossRef]
- Dang, V.D., et al., Bioaccumulation of Legacy and Emerging Organochlorine Contaminants in Lumbriculus variegatus. Arch Environ Contam Toxicol, 2016. 71(1): p. 60-9. [CrossRef]
- Mimeault, C., et al., The human lipid regulator, gemfibrozil bioconcentrates and reduces testosterone in the goldfish, Carassius auratus. Aquat Toxicol, 2005. 73(1): p. 44-54. [CrossRef]
- Abdulrazaq, Y., et al., Classification, potential routes and risk of emerging pollutants/contaminant, in Emerging contaminants. 2020, IntechOpen.
- Dietrich, S., et al., Single and combined toxicity of pharmaceuticals at environmentally relevant concentrations in Daphnia magna--a multigenerational study. Chemosphere, 2010. 79(1): p. 60-6. [CrossRef]
- Shearer, J.J., et al., Serum concentrations of per-and polyfluoroalkyl substances and risk of renal cell carcinoma. 2021. 113(5): p. 580-587. [CrossRef]
- Caballero-Casero, N., et al., Identification of chemicals of emerging concern in urine of Flemish adolescents using a new suspect screening workflow for LC-QTOF-MS. Chemosphere, 2021. 280: p. 130683. [CrossRef]
- Itoh, A., et al., Interaction between Bisphosphonates and Mineral Water: Study of Oral Risedronate Absorption in Rats. Biol Pharm Bull, 2016. 39(3): p. 323-8. [CrossRef]
- Qin, L.-T., et al., Ecological and human health risk of sulfonamides in surface water and groundwater of Huixian karst wetland in Guilin, China. 2020. 708: p. 134552. [CrossRef]
- Hanna, N., et al., Presence of antibiotic residues in various environmental compartments of Shandong province in eastern China: its potential for resistance development and ecological and human risk. 2018. 114: p. 131-142. [CrossRef]
- Dai, C., et al., Human health risk assessment of selected pharmaceuticals in the five major river basins, China. 2021. 801: p. 149730. [CrossRef]
- Evans, M.R., et al., Risk factors for ciprofloxacin-resistant Campylobacter infection in Wales. 2009. 64(2): p. 424-427. [CrossRef]
- Chen, Y., et al., Occurrence of perchlorate, chlorate and bromate in drinking water in Shenzhen and related human exposure risks. 2022. 8: p. 100205. [CrossRef]
- Wang, H., et al., Antibiotics in drinking water in Shanghai and their contribution to antibiotic exposure of school children. 2016. 50(5): p. 2692-2699. [CrossRef]
- Liu, L. Occurrence and Health Risk Assessment of Antibiotics in Drinking Water of a City in Southern China. in IOP Conference Series: Earth and Environmental Science. 2021. IOP Publishing. [CrossRef]
- He, B., et al., Octamethylcyclotetrasiloxane exhibits estrogenic activity in mice via ERα. 2003. 192(3): p. 254-261. [CrossRef]
- Bitsch, N., et al., Estrogenic activity of musk fragrances detected by the E-screen assay using human mcf-7 cells. 2002. 43: p. 0257-0264. [CrossRef]
- Peng, F., et al., Patch testing in facial dermatitis using Chinese Baseline Series (60 allergens) and Cosmetic Series (58 allergens). 2018. 32(7): p. e288-e289. [CrossRef]
- Cherry, N., et al., Occupation and male infertility: glycol ethers and other exposures. 2008. 65(10): p. 708-714. [CrossRef]
- Béranger, R., et al., Prenatal exposure to glycol ethers and neurocognitive abilities in 6-year-old children: the PELAGIE cohort study. 2017. 125(4): p. 684-690.
- Charlton, N.P., et al., The toxicity of picaridin containing insect repellent reported to the National Poison Data System. 2016. 54(8): p. 655-658. [CrossRef]
- Geer, L.A., et al., Association of birth outcomes with fetal exposure to parabens, triclosan and triclocarban in an immigrant population in Brooklyn, New York. J Hazard Mater, 2017. 323(Pt A): p. 177-183.
- Aker, A.M., et al., The associations between prenatal exposure to triclocarban, phenols and parabens with gestational age and birth weight in northern Puerto Rico. 2019. 169: p. 41-51.
- Schmid, P., et al., Does the reuse of PET bottles during solar water disinfection pose a health risk due to the migration of plasticisers and other chemicals into the water? 2008. 42(20): p. 5054-5060. [CrossRef]
- Liu, Y., et al., Human Exposure to Chlorinated Organophosphate Ester Flame Retardants and Plasticizers in an Industrial Area of Shenzhen, China. 2022. 19(5): p. 3126. [CrossRef]
- Sivak, A., et al., Environmental and human health aspects of commercially important surfactants, in Solution Behavior of Surfactants: Theoretical and Applied Aspects Volume 1. 1982, Springer. p. 161-188.
- Rapidly rising PBDE levels in North America. Environmental Science & Technology, 2002. 36(3): p. 50A-52A.
- Feng, L., et al., Levels of urinary metabolites of organophosphate flame retardants, TDCIPP, and TPHP, in pregnant women in Shanghai. 2016. 2016. [CrossRef]
- Kim, U.-J., K.J.E.s. Kannan, and technology, Occurrence and distribution of organophosphate flame retardants/plasticizers in surface waters, tap water, and rainwater: implications for human exposure. 2018. 52(10): p. 5625-5633. [CrossRef]
- Scott, R.T., et al., Follicle-stimulating hormone levels on cycle day 3 are predictive of in vitro fertilization outcome. 1989. 51(4): p. 651-654. [CrossRef]
- Mok-Lin, E., et al., Urinary bisphenol A concentrations and ovarian response among women undergoing IVF. 2010. 33(2): p. 385-393. [CrossRef]
- Valipour, M., et al., Interaction of insulin with methyl tert-butyl ether promotes molten globule-like state and production of reactive oxygen species. 2015. 80: p. 610-614. [CrossRef]
- Franco, M.E., et al., Altered expression and activity of phase I and II biotransformation enzymes in human liver cells by perfluorooctanoate (PFOA) and perfluorooctane sulfonate (PFOS). 2020. 430: p. 152339.
- Spoelstra, J., S.L. Schiff, and S.J.J.P.o. Brown, Artificial sweeteners in a large Canadian river reflect human consumption in the watershed. 2013. 8(12): p. e82706. [CrossRef]
- Rowe, K.S. and K.J.J.T.j.o.p. Rowe, Synthetic food coloring and behavior: a dose response effect in a double-blind, placebo-controlled, repeated-measures study. 1994. 125(5): p. 691-698.
- Ghazipura, M., et al., Exposure to benzophenone-3 and reproductive toxicity: a systematic review of human and animal studies. 2017. 73: p. 175-183. [CrossRef]
- Majhi, P.D., et al., Effects of benzophenone-3 and propylparaben on estrogen receptor–dependent r-loops and dna damage in breast epithelial cells and mice. 2020. 128(1): p. 017002. [CrossRef]
- Lorigo, M., et al., UV-B filter octylmethoxycinnamate impaired the main vasorelaxant mechanism of human umbilical artery. 2021. 277: p. 130302.
- Ao, J., et al., Organic UV filters exposure induces the production of inflammatory cytokines in human macrophages. 2018. 635: p. 926-935. [CrossRef]
- Hawkins, D. and R.J.T.l. Ford, Dermal absorption and disposition of musk ambrette, musk ketone and musk xylene in rats. 1999. 111(1-2): p. 95-103. [CrossRef]
- Dickerson, S.M., et al., Endocrine disruption of brain sexual differentiation by developmental PCB exposure. 2011. 152(2): p. 581-594.
- Hu, Y., et al., Bisphenol A initiates excessive premature activation of primordial follicles in mouse ovaries via the PTEN signaling pathway. 2018. 25(4): p. 609-620. [CrossRef]
- Saal, F.S.v., et al., Prostate enlargement in mice due to fetal exposure to low doses of estradiol or diethylstilbestrol and opposite effects at high doses. 1997. 94(5): p. 2056-2061.
- Belpoggi, F., et al., Methyl-tertiary-butyl ether (MTBE)—a gasoline additive—causes testicular and lympho haematopoietic cancers in rats. 1995. 11(2): p. 119-149. [CrossRef]
- Berthiaume, J. and K.B.J.T.l. Wallace, Perfluorooctanoate, perflourooctanesulfonate, and N-ethyl perfluorooctanesulfonamido ethanol; peroxisome proliferation and mitochondrial biogenesis. 2002. 129(1-2): p. 23-32.
- Soltani, M., et al., Effect of pretreatment with a synbiotic on Perfluorooctanoic acid-induced liver damage after sub-acute oral exposure in C57BL/6J mice. 2023. 459: p. 116360. [CrossRef]
- Das, K.P., et al., Developmental toxicity of perfluorononanoic acid in mice. 2015. 51: p. 133-144. [CrossRef]
- Koskela, A., et al., Effects of developmental exposure to perfluorooctanoic acid (PFOA) on long bone morphology and bone cell differentiation. 2016. 301: p. 14-21. [CrossRef]
- Polyák, É., et al., Effects of artificial sweeteners on body weight, food and drink intake. 2010. 97(4): p. 401-407.
- Suez, J., et al., Artificial sweeteners induce glucose intolerance by altering the gut microbiota. 2014. 514(7521): p. 181-186.
- Erbaş, O., et al., Evaluation of long-term effects of artificial sweeteners on rat brain: A biochemical, behavioral, and histological study. 2018. 32(6): p. e22053.
- Hashem, M.M., et al., Immunological studies on Amaranth, Sunset Yellow and Curcumin as food colouring agents in albino rats. Food Chem Toxicol, 2010. 48(6): p. 1581-6. [CrossRef]
- Amin, K., et al., Effect of food azo dyes tartrazine and carmoisine on biochemical parameters related to renal, hepatic function and oxidative stress biomarkers in young male rats. 2010. 48(10): p. 2994-2999. [CrossRef]
- Ford, G.P., B.I. Stevenson, and J.G. Evans, Long-term toxicity study of carmoisine in rats using animals exposed in utero. Food and Chemical Toxicology, 1987. 25(12): p. 919-925. [CrossRef]
- Pomierny, B., et al., Benzophenone-3 passes through the blood-brain barrier, increases the level of extracellular glutamate, and induces apoptotic processes in the hippocampus and frontal cortex of rats. 2019. 171(2): p. 485-500. [CrossRef]
- Lu, Y., et al., Concentrations and assessment of exposure to siloxanes and synthetic musks in personal care products from China. 2011. 159(12): p. 3522-3528. [CrossRef]
- Perper, M., et al., Airborne contact dermatitis caused by fragrance diffusers in U ber cars. 2017. 77(2): p. 116-117.
- Carlsson, G., et al., The impact of musk ketone on reproduction in zebrafish (Danio rerio). 2000. 50(1-5): p. 237-241.
- Prakash, S., et al., Effect of n, n-diethyl phenyl acetamide: an insect repellent on foetus and reproduction in rats. 1987. 49(6).
- Mehlman, M.A.J.A.o.t.N.Y.A.o.S., Carcinogenicity of Methyl-Tertiary Butyl Ether in Gasoline. 2002. 982(1): p. 149-159.
- McGregor, D.J.C.R.i.T., Methyl tertiary-butyl ether: studies for potential human health hazards. 2006. 36(4): p. 319-358.
- Bus, J.S., et al., Methyl-tert-butyl ether (MTBE): integration of rat and mouse carcinogenicity data with mode of action and human and rodent bioassay dosimetry and toxicokinetics indicates MTBE is not a plausible human carcinogen. 2022. 25(4): p. 135-161. [CrossRef]
- Assad, G.F. and K.J.J.P.M.S. Buraydah, Toxicological impact of amaranth, sunset yellow and curcumin as food coloring agents in albino rats. 2011. 1(2): p. 43-51.
- Cotrina, E.Y., et al., Binding of common organic UV-filters to the thyroid hormone transport protein transthyretin using in vitro and in silico studies: Potential implications in health. 2023. 217: p. 114836.
- Wang, M., et al., Benzophenone-1 and-2 UV-filters potently inhibit human, rat, and mouse gonadal 3β-hydroxysteroid dehydrogenases: Structure-activity relationship and in silico docking analysis. 2023. 230: p. 106279.
- Lorigo, M. and E.J.C. Cairrao, UV-B filter octylmethoxycinnamate-induced vascular endothelial disruption on rat aorta: In silico and in vitro approach. 2022. 307: p. 135807. [CrossRef]
- Hong, J.-H., et al., Occurrence and sources of synthetic musk fragrances in the sewage treatment plants and the Han River, Korea. 2021. 13(4): p. 392. [CrossRef]
- Vimalkumar, K., et al., Synthetic musks in surface water and fish from the rivers in India: Seasonal distribution and toxicological risk assessment. 2021. 414: p. 125558. [CrossRef]
- Schmeiser, H.H., et al., Evaluation of health risks caused by musk ketone. 2001. 203(4): p. 293-299. [CrossRef]
- Alam, M.N., et al., Linking emerging contaminants exposure to adverse health effects: Crosstalk between epigenome and environment. 2021. 41(6): p. 878-897.
- Gwenzi, W., et al., Ecological health risks of antibiotic resistance: A perspective on the evidence, challenges, and research needs, in Emerging Contaminants in the Terrestrial-Aquatic-Atmosphere Continuum:. 2022, Elsevier. p. 195-213.
- Sanganyado, E., et al., Organic pollutants in deep sea: Occurrence, fate, and ecological implications. 2021. 205: p. 117658. [CrossRef]
- Mupatsi, N.M. and W. Gwenzi, Occurrence, human exposure pathways, and health risks of (micro) plastics, in Emerging Contaminants in the Terrestrial-Aquatic-Atmosphere Continuum:. 2022, Elsevier. p. 291-306.
- Gwenzi, W., Z. Makuvara, and J. Marumure, Rare earth elements: Human exposure, risk factors, and health risks, in Emerging Contaminants in the Terrestrial-Aquatic-Atmosphere Continuum:. 2022, Elsevier. p. 273-290.
- Cordner, A. and P. Brown. Moments of uncertainty: Ethical considerations and emerging contaminants. in Sociological Forum. 2013. Wiley Online Library.
- Fuerhacker, M.J.E.S. and P. Research, EU Water Framework Directive and Stockholm Convention: can we reach the targets for priority substances and persistent organic pollutants? 2009. 16: p. 92-97.
- GmbH)., I.I.f.P., . Pharmaceutical Residues in Drinking Water. . Available at: https://www.produktqualitaet.com/en/water/pharmaceuticals.html 2022. Accessed: 23/12/2022.
Figure 1.
A depiction of the source-pathway-receptor-impact continuum of emerging organic contaminants in drinking water systems.
Figure 1.
A depiction of the source-pathway-receptor-impact continuum of emerging organic contaminants in drinking water systems.
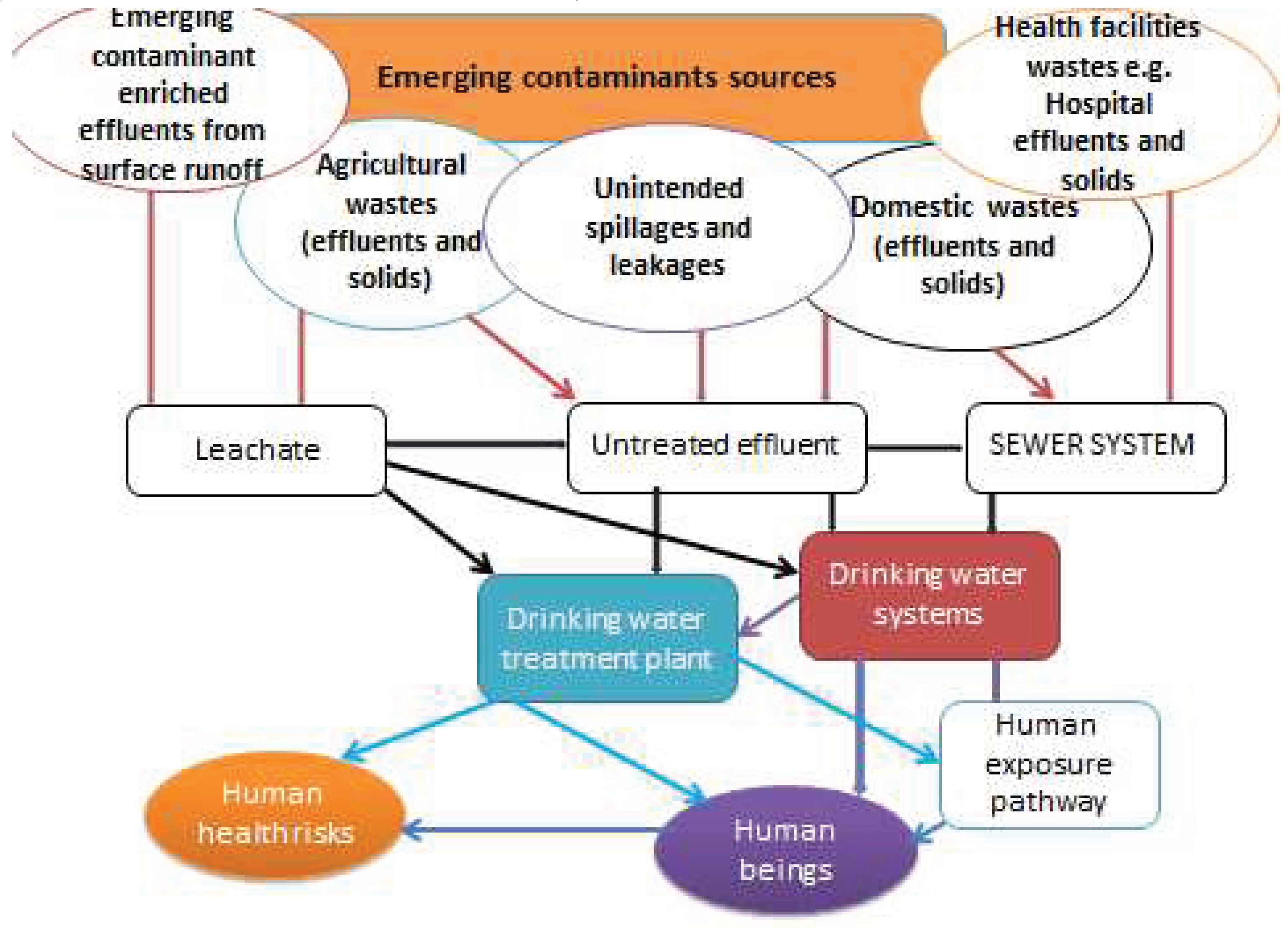
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



