Submitted:
13 June 2023
Posted:
14 June 2023
You are already at the latest version
Abstract
Background: Pulmonary sequestration (PS), generally diagnosed using computed tomography pulmonary angiography (CTPA), is a rare congenital developmental malformation of the lung that is characterized by nonfunctional lung tissue independent of the normal lung tissue. This study summarizes the imaging features of the supplying arteries and draining vessels in patients with PS with an aim to assist with timely clinical diagnosis and operation guidance.
Materials and Methods: A total of 55 patients with PS diagnosed on CTPA from multiple clinical centers were retrospectively analyzed. Data included demographic characteristics, imaging features, disease location, isolation type, and the features of supplying and draining vessels, as shown on CTPA images.
Results: Of the 55 patients reviewed, 3 (5.45%) were children, 3 (5.45%) were adolescents, and 49 (89.09%) were adults, with a mean age of 44 years. Fifty-four (98.18%) patients had intralobar sequestration and one (1.82%) had extralobar sequestration. PS was noted 3.5 times more frequently in the left lower lobe than in the right lower lobe. For the supplying arteries, 47 (85.45%) were derived from the descending thoracic aorta, 1 (1.82%) from the abdominal aorta, 7 (12.73%) from the celiac axis, and 1 (1.82%) from the bronchial artery. The draining vessels were the pulmonary veins in 49 patients (89.09%), the umbilical vein in 1 (1.82%), the venae intercostal in 1 (1.82%), the pulmonary arteries in 11 (20.00%), and not shown on the images in 2 (3.64%).
Conclusion: Clinical presentations of PS are non-specific and can be easily missed or misdiagnosed. However, CTPA can help improve the diagnostic accuracy and identify the supplying arteries and draining vessels, which significantly contribute to surgical planning.
Keywords:
Pulmonary sequestration
; computed tomography angiography
; intralobar and extralobar sequestration
; supplying artery
; draining vessel
1. Introduction
Pulmonary sequestration (PS), also known as bronchopulmonary sequestration, is a rare congenital developmental malformation of the lung characterized by nonfunctional lung tissue, independent of the normal lung tissue [1,2]. PS bifurcates into intralobar (ILS) and extralobar (ELS) sequestration [3]. ILS is incorporated within the normal lung tissue and communicates with the outer bronchus through its own trachea, whereas ELS is separated from the normal lung tissue by its own visceral pleura and presents with a lack of connection to the normal tracheobronchial tree [4].
The blood supply of nonfunctional lung tissue mainly comes from systemic circulation, especially the aorta or its branches, and most commonly from the descending thoracic aorta. It has also been reported to originate from the intercostal, phrenic, gastric, splenorenal, celiac trunk, subclavian, and innominate arteries and, more rarely, from abnormal arteries such as the coronary and pulmonary arteries [5,6]. Similarly, venous drainage varied greatly in patients with PS. In PS, the drainage of blood vessels mostly comes from the pulmonary vein (90.02%), followed by from the azygos vein (4.2%), postcava (0.74%), and vena phrenica (0.21%) [6]. In most cases of ILS, the draining vein is the pulmonary vein, whereas in most cases of ELS, it is a systemic vein [7].
PS is mainly diagnosed using conventional radiology rather than invasive angiography. If such diseases are detected early as an indicator of timely surgery to those requiring necessary surgical intervention, the complications can be prevented in a timely manner and will minimize unnecessary procedures or examinations. To avoid the risk of occult or surgical bleeding, it is important to accurately identify the blood supply to the arteries prior to surgery and eliminate the vessels during surgery [8,9]. Despite many reports on the prevalence and clinical diagnosis of PS [10,11,12], most have focused on case reports or case series. There are several retrospective studies reporting the clinical symptoms and diagnosis of PS, either documenting PS imaging appearances in adults or pediatric patients [13,14,15,16]. Wei and Li reported the largest number of PA cases that were retrieved from the Chinese National Knowledge Infrastructure database over a period of 10 years [16]. Their analysis showed that patients with PA presented with variable clinical manifestations with preoperative diagnosis frequently incorrect. Of the cases that were analysed in their study, 27% were incorrectly diagnosed before operation. Of which 36% and 21% were misdiagnosed as pulmonary cyst and lung cancer respectively. Thus, this highlights the importance of timely and correct diagnosis of PS.
In this study, we report on the computed tomography (CT) imaging features of 55 cases of PS confirmed using surgery or digital subtraction angiography (DSA) based on a multicenter experience. Our aim was to increase the diagnostic accuracy of CT for PS and decrease the misdiagnosis rate through a comprehensive analysis of imaging characteristics.
2. Materials and Methods
2.1. Patient data collection
We retrospectively reviewed 55 patients with PS from multiple clinical centers who underwent CT pulmonary angiography (CTPA) with PS proven by pathology or DSA. Demographic characteristics, imaging features, disease location, isolation type, and features of the supplying and draining vessels were collected for analysis. Due to the retrospective nature of the study with only reviewing de-identified images, ethics approval was waived with no requirement for patient consent.
2.2. CT scanning and image interpretation
The CT scanners used were different because data were collected from multiple medical centers (64- to 256-slice scanners); however, all patients were examined using plain and contrast-enhanced CT scans following the standard CTPA protocols. All radiological images were available in the picture archiving and communication system from each center and analyzed using RadiAnt DICOM (Digital Imaging and Communications in Medicine) Viewer software (2020.1.1 64-bit). All CT images were independently reviewed by two radiologists (one with 17 years and the other with 4 years of experience in cardiothoracic CT) who reached a consensus in case of discrepancy.
The following details were analyzed in each case: clinical characteristics, including the types of PS—ILS or ELS; imaging features on CTPA, including the location of PS in terms of which lobes; and supplying arteries to the sequestration area and draining vessels.
2.3. Statistical analysis
Data were analyzed using Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA). Categorical variables were presented as percentage or frequency, while continuous variables were reported as mean and standard deviation.
3. Results
3.1. Sex distribution and age at diagnosis
A total of 55 patients with PS were included in the study; 34 (61.82%) were male and 21 (38.18%) were female, with a male-to-female ratio of 1.62:1. Of the 55 cases, children aged between 3 months and 8 years accounted for 3 cases (5.45%), adolescents aged between 14 and 20 years accounted for another 3 cases (5.45%), and adults aged between 21 and 81 years accounted for 49 cases, representing the majority of cases (89.09%), with a mean age of 44 years.
3.2. Imaging appearances of CTPA
All patients underwent chest CT examinations. Of the 55 patients, 54 (98.18%) had ILS and 1 (1.82%) had ELS (Figure 1). Pulmonary masses were found in the left lower lobe in 42 (76.36%) patients, in the right lower lobe in 12 (21.82%), and in the lower lobe of both lungs in 1 (1.82%; Figure 1). Some patients had pulmonary infection, bronchiectasis, chest pain, and lung cancer (Figure 2). In addition, some patients had other cardiovascular diseases, such as anterior descending branch-right atrial fistula and levoatriocardinal vein (LACV; Figure 3).
Forty-three (78.18%) patients had only one supplying artery and 12 (21.82%) had two or more supplying arteries. For the supplying arteries, 47 (85.45%) were derived from the descending thoracic aorta, 1 (1.82%) from the abdominal aorta, 7 (12.73%) from the celiac axis, and 1 (1.82%) from the bronchial artery. The supplying arteries were tortuous in 15 (27.27%) patients. The supplying arteries had dilated outside the lung, and the maximum diameter of the dilated artery was 13.0 mm. Similarly, in the lungs, the maximum diameter of the dilated artery was 13.0 mm.
The draining vessels were pulmonary veins in 49 patients (89.09%), umbilical vein in 1 (1.82%), venae intercostal in 1 (1.82%), pulmonary arteries in 11 (20.00%; Figure 4), and not shown on the plane in 2 (3.64%). One patient (1.82%) had significant dilatation of the drainage vessel, which was the pulmonary artery (Figure 5) (Table 1).
4. Discussion
This multi-centre study presented CT findings of PS in both adults and pediatric patients with majority of the PS noticed in the left lower lobe than right lower lobe. More than 80% of the supplying arteries were from descending thoracic aorta with nearly 90% of the draining vein from pulmonary vein. The study findings add valuable information to the existing literature with regard to comprehensive CT analysis of patients with PS.
PS is a rare congenital developmental anomaly of unknown etiology, accounting for 0.15–6.40% of all congenital lung malformations [10], which is often found on imaging examination after symptomatic change occurs. Patients with PS can present with conditions such as recurrent pulmonary infections, chest pain, hemoptysis, and dyspnea [11]. Symptoms recur until the cause is resolved.
ILS is the most common type of PS (75%), the most common site of which is the posterior basal segment of the left lower lobe [12]. This is also reported by other studies showing even higher prevalence of ILS, which is about 93% [13,14]. In our study, among the 55 patients, 42 had lesions located in the left lower lobe, which is in agreement with the previous literature [13,14,15,16]. ELS, which accounts for 25% of all cases of PS, is mainly located between the left lower lobe and the diaphragm adjacent to the esophagus, as well as in the pericardial region of the anterior superior mediastinum, occasionally under the diaphragm, but rarely in the middle mediastinum [13]. Previous studies have indicated that the incidence of ELS in men is approximately three- or four-fold that in women [11]. Our study included too few ELS cases to derive any comparative significance, because in our study, only one patient with ELS was female.
In symptomatic patients or when cancer cannot be excluded, surgical resection is recommended with mass excision preferred for ELS and lobectomy preferred for ILS [17]. Excessive bleeding can occur if the feeding artery is improperly ligated or destroyed during surgery; therefore, clinicians must weigh the risk of surgery and complications of PS. Consequently, it is particularly important to preoperatively identify the feeding and draining vessels. Compared with Doppler ultrasound and magnetic resonance imaging, CTPA has gradually become the primary choice for examination of PS because of the advantages of slice reconstruction, multiplanar reconstruction, 3D re-formatting, and faster scanning (reduced need for sedation and intravenous contrast media), which can also provide relevant information about the lung parenchyma, including the airway. A study by Yue et al. reported high accuracy (>95%) and sensitivity (>95%) in vessel-based evaluation of PS [18]. On our patients’ CTPA images, the feeding arteries mostly arose from the descending thoracic aorta (T9–T11), and most of the draining vessels were pulmonary veins, which is consistent with the previous literature.
CTPA imaging indicated a “dual blood supply” in 11 patients, in which both the pulmonary artery and systemic circulation vessels headed into the lesion area. However, the systemic circulation vessels provide the real blood supply. The pulmonary artery does not play a role in blood supply but only plays a role in drainage, because the aorta and pulmonary artery can be visualized simultaneously in the aortic stage, whereas pulmonary artery blood flow in the direction of the lesion is stagnant in the pulmonary artery stage. Thus, we consider the pulmonary artery of “dual blood supply” is the draining vessel but not the supplying vessel. Blood supply to the pulmonary vein will be reduced because the pulmonary artery is a draining vessel. The pulmonary artery may become chronically high and, thus, form pulmonary hypertension with fewer or no pulmonary veins. Over time, lung tissue atrophy on the affected side results in complete or partial occlusion of the pulmonary vein in the lesion area. Systemic circulation blood vessels always distorted abnormally in PS with “dual blood supply,” which may be because the pulmonary venous return is impeded, resulting in the obstruction of pulmonary circulation and congestion of systemic circulation. Under huge pressure differences, systemic circulation blood vessels will be twisted and sometimes dilated.
Patients with PS are more likely to develop other cardiovascular malformations. In one patient (Figure 3), the image showed abnormal communication between the pulmonary veins and interior vena cava (IVC), which is a type of LACV. LACV is an embryological remnant usually found on the right side, in which a malformed vessel communicates between the left atrium or pulmonary and systemic vein [19], and the pulmonary vein itself (from which the LACV arises) has normal connection with the left atrium. LACV is often associated with left-sided obstructive lesions, such as mitral atresia, aortic atresia, mitral stenosis, aortic coarctation, and hypoplastic left heart syndrome [20,21]. Under normal conditions, vascular pressure in the systemic circulation is considerably higher than that in the lungs, whereas that in the systemic vein is considerably higher than that in the pulmonary vein. However, blood flow in the LACV is directed from the pulmonary vein to the systemic venous system, which can lead to a shunt from left to right and reduce venous stasis [22]. Moreover, this abnormal connection might result in two-way flow and potential paradoxical embolism [23,24].
Malignancy in PS is exceedingly rare. Lung cancer caused by bronchopulmonary sequestration was first described by Hertzog et al. in 1963; however, the relationship between them remains unclear [25]. Malignant lesions can occur not only in the isolated lungs but also in segmental bronchi separated from the isolated lungs. In this study, in two cases of PS combined with lung cancer, malignant lesions developed in the isolated lungs. A large mass in the left lower lobe lung of patient no. 54 and in the right lower lobe lung of patient no. 55 was adjacent to the diaphragm, with an area of low density in the center. Both lesions were supplied by small branches of the descending thoracic aorta and drained by their respective pulmonary veins. If a mass is detected with an abnormal supply of blood from the systemic circulation in contrast-enhanced CT scans, it confirms the diagnosis of PS. However, surprisingly, we found cancer cells in the isolated lungs in pathology after surgery. Isolated lungs combined with malignancy usually appear as well-defined, lobulated, and nearly round-shaped masses with swelling margins. The corresponding bronchi of the lesions were narrow and occluded. Owing to the small number of cases of PS combined with malignancy, it is important to increase the sample size and assess it repeatedly in future studies. Nonetheless, the potential for the development of malignancy combined with PS must be considered. Attention should be paid not to transect the abnormal artery of ILS during the resection of such lesions as this may cause massive bleeding.
This study has some limitations. Despite multicenter data collection, the number of PS cases was relatively small. Furthermore, we did not follow-up the patients who received treatment with regard to the clinical outcomes as our focus is about detailed analysis of imaging features of patients with PS.
5. Conclusions
The clinical presentations of PS are non-specific and can be easily missed or misdiagnosed. However, CTPA can provide important clues to the diagnosis of PS. Furthermore, the identification of the feeding arteries and draining vessels has the potential to contribute significantly to guiding surgery.
Author Contributions
Conceptualization, Y.L.; methodology, T.Y and Z.W.; formal analysis, J.Q and Q.M.; investigation, T.Y and Z.W.; resources, T.Y., Z.W, J.Q., Q.M, and S.K.; data curation, Y.L. writing—original draft preparation, T.Y and Z.W.; writing—review and editing, Z.S; visualization, J.Q and Q.M.; supervision, Y.L.; project administration, Y.L.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable as this is a retrospective study.
Informed Consent Statement
Patient consent was waived due to retrospective nature of the study.
Data Availability Statement
Data are not available.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gabelloni, M.; Faggioni, L.; Accogli, S.; Aringheri, G.; Neri, E. Pulmonary sequestration: what the radiologist should know. Clin. Imaging. 2021, 73, 61–72. [Google Scholar] [CrossRef]
- Tsolakis, C.C.; Kollias, V.D.; Panayotopoulos, P.P. Pulmonary sequestration. Experience with eight consecutive cases. Scand. Cardiovasc. J. 1997, 31, 229–232. [Google Scholar] [CrossRef]
- Yangui, F.; Charfi, M.; Abouda, M.; Charfi, M.R. Pulmonary sequestration in a healthy teenage girl. Tunis. Med. 2019, 97, 604–605. [Google Scholar]
- Berna, P.; Lebied, E.I.D.; Assouad, J.; Foucault, C.; Danel, C.; Riquet, M. Pulmonary sequestration and aspergillosis. Eur. J. Cardiothroac. Surg. 2005, 27, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Salvati, F. Cardiovascular, broncho-parenchima and neoplastic anomalies related to pulmonary sequestration: a critical review. Recenti. Prog. Med. 2018, 109, 388–392. [Google Scholar] [PubMed]
- Franko, J.; Bell, K.; Pezzi, C.M. Intraabdominal pulmonary sequestration. Curr. Surg. 2006, 63, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Ulys, A.; Samalavicius, N.; Cicenas, S.; Petraitis, T.; Trakymas, M.; Sheinin, D.; Gatijatullin, L. Extralobar pulmonary sequestration. Int. Med. Case. Rep. J. 2011, 4, 21–23. [Google Scholar] [PubMed]
- Hirai, S.; Hamanaka, Y.; Mitsui, N.; Uegami, S.; Matsuura, Y. Surgical treatment of infected intralobar pulmonary sequestration: a collective review of patients older than 50 years reported in the literature. Ann. Thorac. Cardiovasc. Surg. 2007, 13, 331–334. [Google Scholar] [PubMed]
- Adzic-Vukicevic, T.N.; Radovanovic, D.V.; Acimovic, B.D.; Popovic, M.P. Pulmonary sequestration mimicring lung cancer: A case report. Vojnosanit. Pregl. 2016, 73, 1060–1063. [Google Scholar] [CrossRef] [PubMed]
- Tashtoush, B.; Memarpour, R.; Gonzalez, J.; Gleason, J.B.; Hadeh, A. Pulmonary sequestration: A 29 patient case series and review. J. Clin. Diagn. Res. 2015, 9, AC05-8. [Google Scholar] [CrossRef] [PubMed]
- Cong, C.V.; Ly, T.T.; Minh, N.M. Intralobar pulmonary sequestration supplied by vessel from the inferior vena cava: literature overview and case report. Radiol. Case. Rep. 2022, 17, 1345–1353. [Google Scholar] [CrossRef]
- Shafig, M.; Ali, A.; Dawar, U.; Setty, N. Rare cause of haemoptysis: bronchopulmonary sequestration. BMJ. Case. Rep. 2021, 14, e239140. [Google Scholar] [CrossRef]
- Sun, X.; Xiao, Y. Pulmonary sequestration in adult patients: a retrospective study. Eur. J. Cardiothorac. Surg. 2015, 48, 279–282. [Google Scholar] [CrossRef]
- Long, Q.; Zha, Y.; Yang, Z. Evaluation of pulmonary sequestration with multidetector computed tomography angiography in a select cohort of patients: A retrospective study. Clinics. 2016, 71, 392–398. [Google Scholar] [CrossRef]
- Zhang, N.; Chen, Q.; Yu, J.; Zhang, X. Distribution, diagnosis, and treatment of pulmonary sequestration: Report of 208 cases. J. Pediatr. Surg. 2019, 54, 1286–1292. [Google Scholar] [CrossRef]
- Wei, Y.; Li, F. Pulmonary sequestration: a retrospective analysis of 2625 cases in China. Eur. J. Cardiothorac. Surg. 2011, 40, 439-e42. [Google Scholar] [CrossRef]
- Fukui, T.; Hakiri, S.; Yokoi, K. Extralobar pulmonary sequestration in the middle mediastinum. Gen. Thorac. Cardiovasc. Surg. 2017, 65, 481–483. [Google Scholar] [CrossRef]
- Yue, S.W.; Guo, H.; Zhang, Y.G.; Gao, J.B.; Ma, X.X.; Ding, P.X. The clinical value of computer tomographic angiography for the diagnosis and therapeutic planning of patients with pulmonary sequestration. Eur. J. Cardiothorac. Surg. 2013, 43, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Amoretti, F.; Cerillo, A.G.; Chiappino, D. The levoatriocardinal vein. Pediatr. Cardiol. 2005, 26, 494–495. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, P.P.; Mahani, M.G.; Lu, J.C.; Dorfman, A.L. Levoatriocardinal vein and mimics: spectrum of imaging findings. AJR. Am. J. Roentgenol. 2015, 205, W162-71. [Google Scholar] [CrossRef] [PubMed]
- Saremi, F.; Ho, S.Y. Extracardiac pulmonary-systematic connection via persistent levoatriocardinal vein in adults. Ann. Vasc. Surg. 2016, 34, e1–7. [Google Scholar] [CrossRef]
- Shet, N.; Maldjian, P. Levoatriocardinal vein: an unusual cause of right-left shunting. J. Clin. Imaging. Sci. 2014, 4, 68. [Google Scholar]
- Canan, A.; Aziz, M.U.; Abbara, S. A rate pulmonary-systemic connection: levoatriocardinal vein. Radiol. Cardiothorac. Imaging. 2020, 2, e190228. [Google Scholar] [CrossRef] [PubMed]
- Karangelis, D.; Avramidis, D.; Mousiama, T.; Karamitsos, T.D.; Mitropoulos, F.; Tzifa, A. Levoatriocardinal vein: a rarely recognized cause of recurrent cardiac and cerebral thromboembolic events. Can. J. Cardiol. 2020, 36, 589.e9–589.e11. [Google Scholar] [CrossRef] [PubMed]
- Hertzog, P.; Roujeau, J.; Marcou, J. Epidermoid cancer developed on a sequestration. J. Fr. Med. Chir. Thorac. 1963, 17, 33–38. [Google Scholar] [PubMed]
Figure 1.
A 41-year-old female with extralobar pulmonary sequestration. (A) Computed tomography (CT) angiography demonstrating a sharply circumscribed ang cystic solid mass in the posterior mediastinum (arrow). (B) CT coronal images in the pulmonary window demonstrating atelectatic sequestrated lung and pleural line totally separating the normal lung parenchyma from the underlying sequestrated lung (arrow). (C) Contrast-enhanced CT demonstrating solid enhancement in the periphery of the posterior mediastinal mass and patchy low-density foci without enhancement in the center (arrow). (D) Thorax CT scan coronal image (oblique maximum intensity projection image) demonstrating blood supply to the sequestrated lung from two branches of the thoracic aorta (arrow), which are small and extended directly into the sequestrated lung.
Figure 1.
A 41-year-old female with extralobar pulmonary sequestration. (A) Computed tomography (CT) angiography demonstrating a sharply circumscribed ang cystic solid mass in the posterior mediastinum (arrow). (B) CT coronal images in the pulmonary window demonstrating atelectatic sequestrated lung and pleural line totally separating the normal lung parenchyma from the underlying sequestrated lung (arrow). (C) Contrast-enhanced CT demonstrating solid enhancement in the periphery of the posterior mediastinal mass and patchy low-density foci without enhancement in the center (arrow). (D) Thorax CT scan coronal image (oblique maximum intensity projection image) demonstrating blood supply to the sequestrated lung from two branches of the thoracic aorta (arrow), which are small and extended directly into the sequestrated lung.
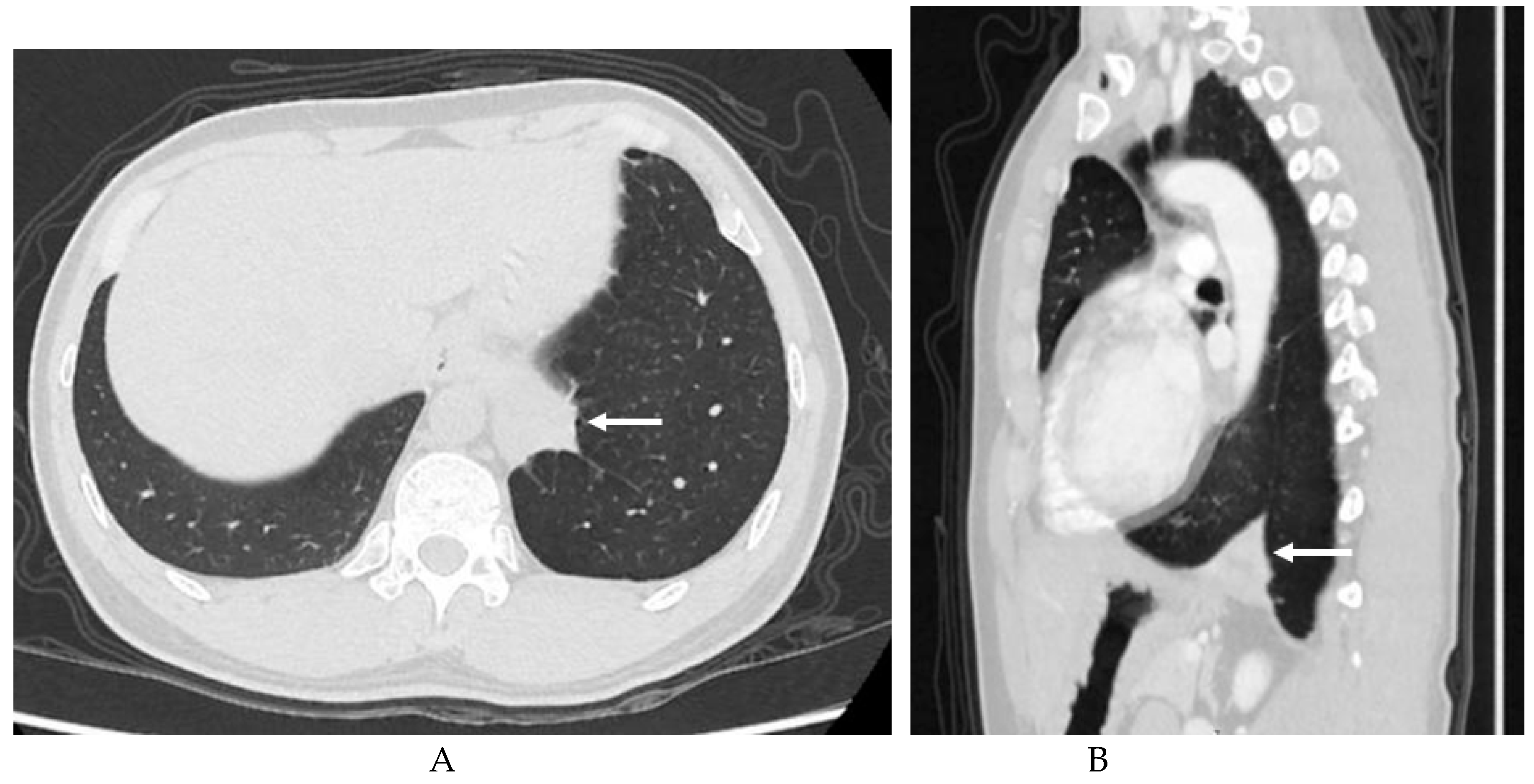
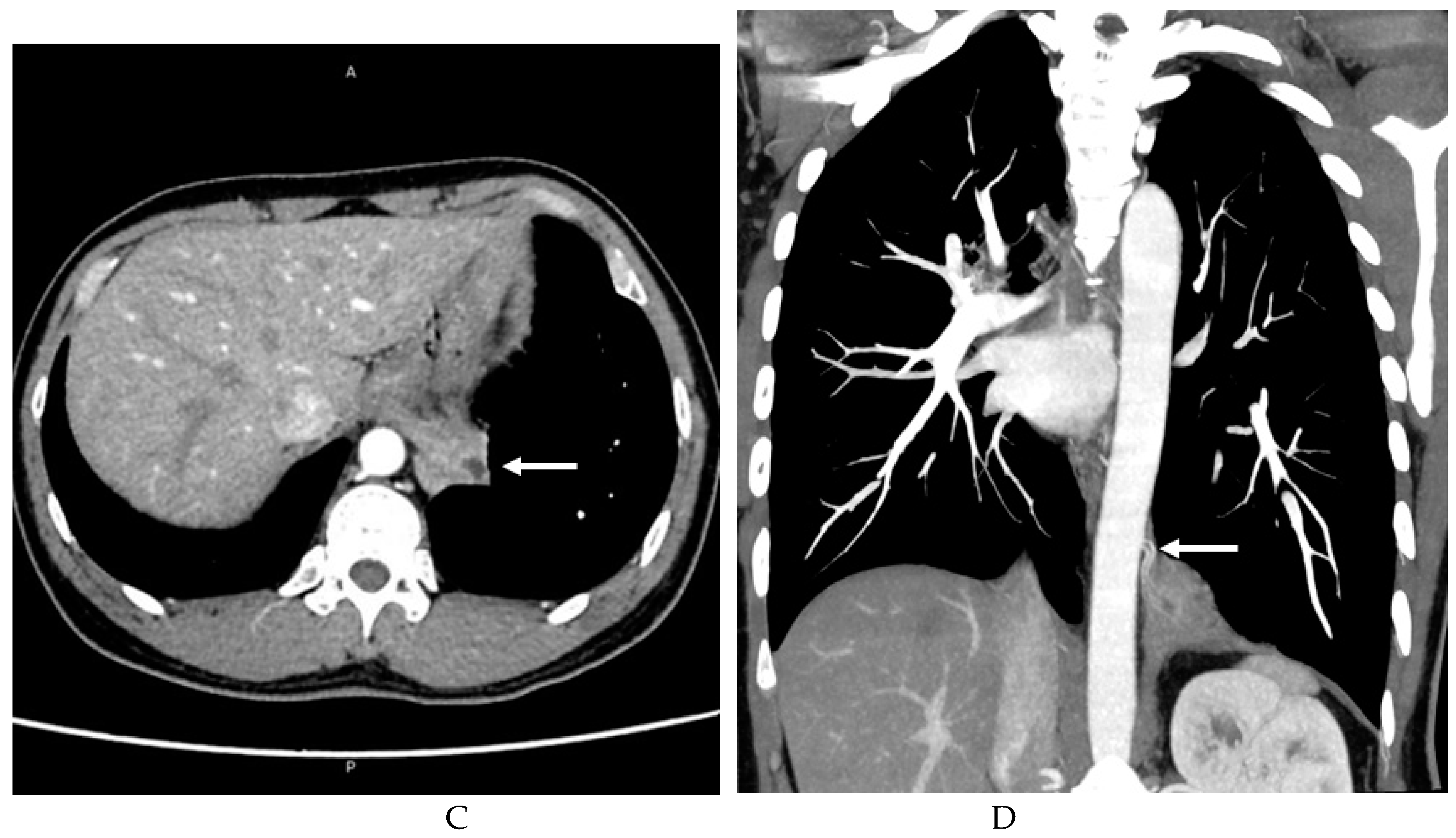
Figure 2.
A 68-year-old male with intralobar pulmonary sequestration. (A) Computed tomography angiography maximum-intensity projection recombination coronary image demonstrating that the feeding artery (arrow) originates from the branch of the descending thoracic aorta, and the draining vessel is the pulmonary vein. (B) CT imaging (pulmonary window) demonstrating a round mass in the left lower lobe with distended margins and obstruction of the corresponding bronchus. Axial plain (C) and sagittal contrast-enhanced (D) CT image demonstrating an uneven density mass with heterogeneous moderate enhancement of peripheral solid components (arrows) and without any enhancement of central liquefaction necrosis. (E) At low magnification, the tumor cells show a papillary growth pattern, and the fibrovascular axis can be seen in the stroma. Higher magnification showing cells displaying evident atypia with a high nucleoplasm ratio and a large nucleus.
Figure 2.
A 68-year-old male with intralobar pulmonary sequestration. (A) Computed tomography angiography maximum-intensity projection recombination coronary image demonstrating that the feeding artery (arrow) originates from the branch of the descending thoracic aorta, and the draining vessel is the pulmonary vein. (B) CT imaging (pulmonary window) demonstrating a round mass in the left lower lobe with distended margins and obstruction of the corresponding bronchus. Axial plain (C) and sagittal contrast-enhanced (D) CT image demonstrating an uneven density mass with heterogeneous moderate enhancement of peripheral solid components (arrows) and without any enhancement of central liquefaction necrosis. (E) At low magnification, the tumor cells show a papillary growth pattern, and the fibrovascular axis can be seen in the stroma. Higher magnification showing cells displaying evident atypia with a high nucleoplasm ratio and a large nucleus.
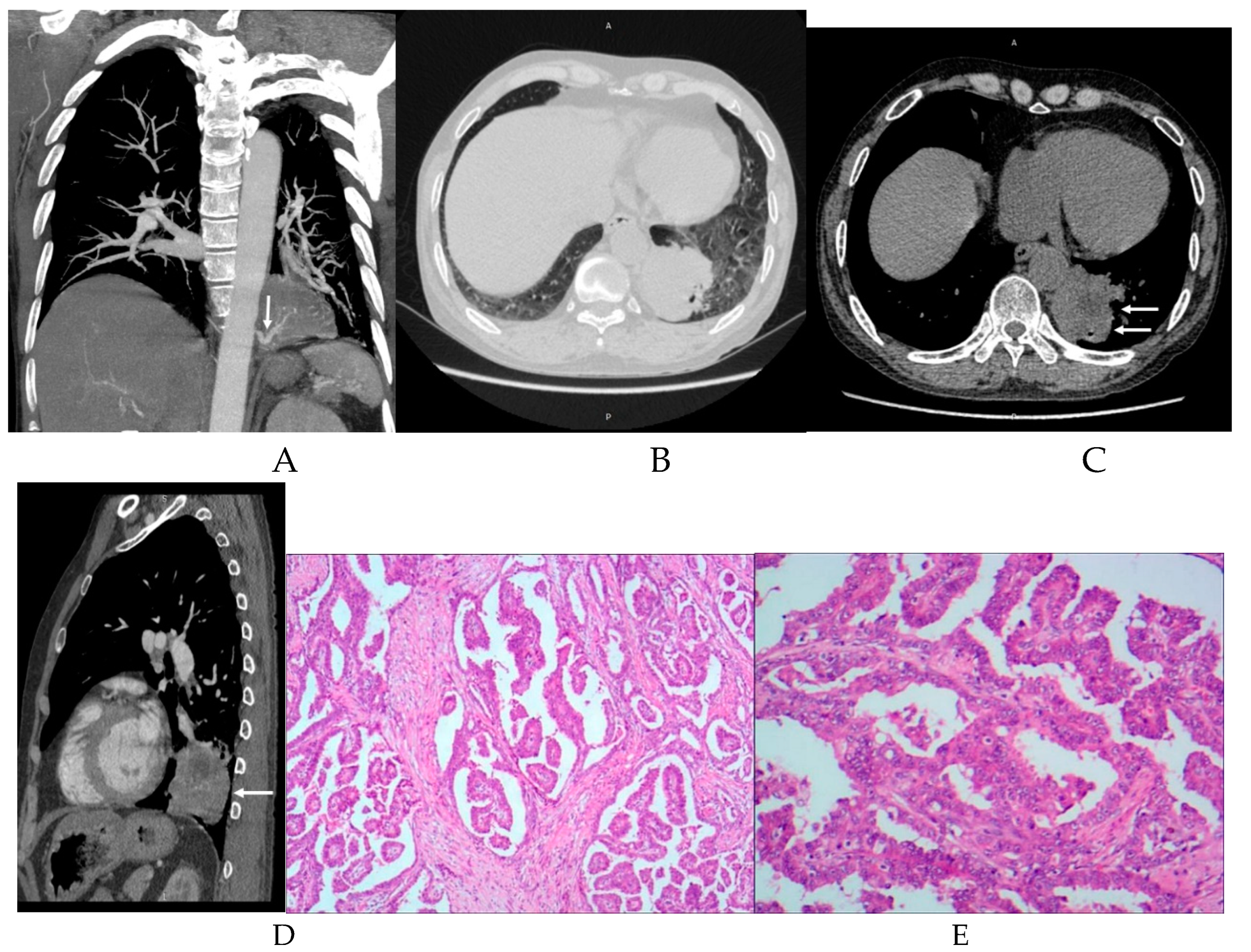
Figure 3.
A 58-year-old male with intralobar pulmonary sequestration. (A) Intralobar pulmonary sequestion lesion in the computed tomography angiography axial image presenting as a mass (arrow) in the lower lobe of the right lung with thickening of the pulmonary vessels around. (B) Oblique coronal CTPA (maximum-intensity projection [MIP]) reformatted image demonstrating that the feeding arteries arose from a branch of the abdominal aorta with a slender lumen (arrows). (C) Oblique sagittal CTPA (MIP) reformatted image showing the levoatriocardinal vein (LACV) with anomalous connection between the right inferior pulmonary vein and the interior vena cava (IVC) (arrows). The normal communication between the left superior pulmonary vein (LSPV) and left atrium is not disrupted. CTPA-computed tomography pulmonary angiography.
Figure 3.
A 58-year-old male with intralobar pulmonary sequestration. (A) Intralobar pulmonary sequestion lesion in the computed tomography angiography axial image presenting as a mass (arrow) in the lower lobe of the right lung with thickening of the pulmonary vessels around. (B) Oblique coronal CTPA (maximum-intensity projection [MIP]) reformatted image demonstrating that the feeding arteries arose from a branch of the abdominal aorta with a slender lumen (arrows). (C) Oblique sagittal CTPA (MIP) reformatted image showing the levoatriocardinal vein (LACV) with anomalous connection between the right inferior pulmonary vein and the interior vena cava (IVC) (arrows). The normal communication between the left superior pulmonary vein (LSPV) and left atrium is not disrupted. CTPA-computed tomography pulmonary angiography.
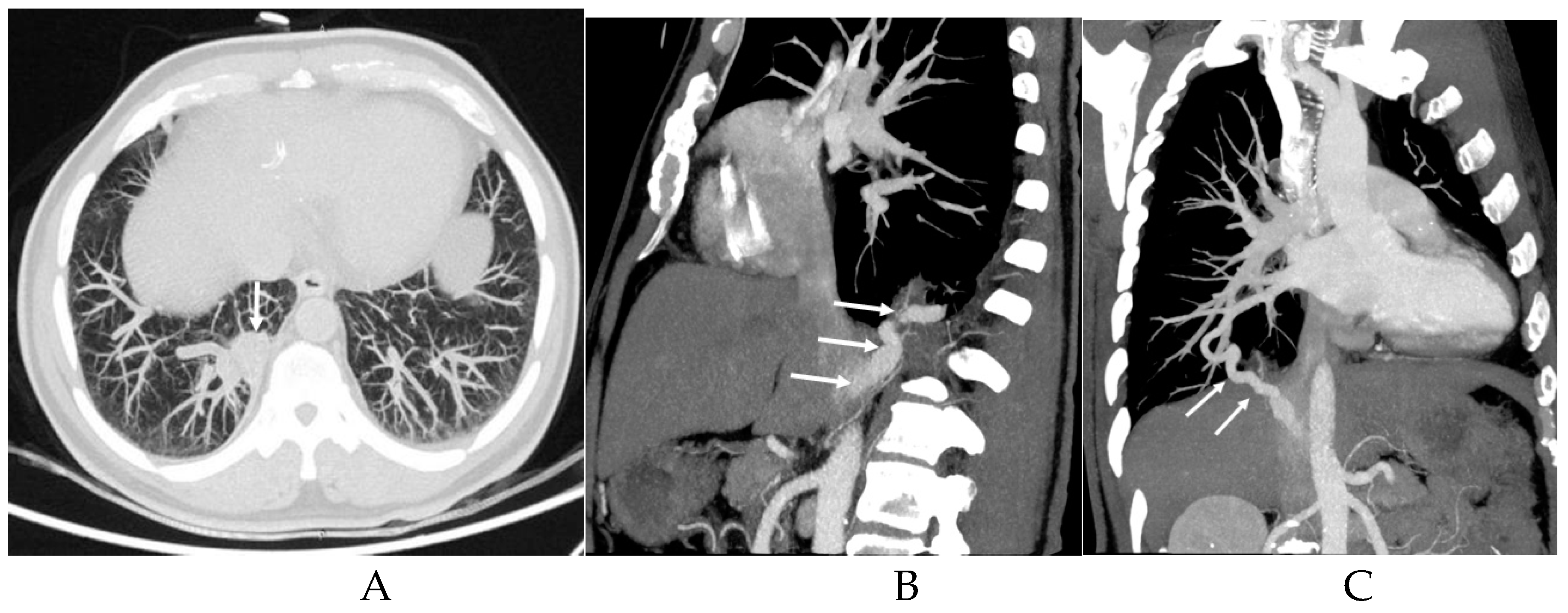
Figure 4.
A 71-year-old male with intralobar pulmonary sequestration. Axial (A) and sagittal (B) computed tomography angiography demonstrating an intralobar polycystic sequestration in the lower lobe of the left lung that is cystic and heterogeneous. CTPA MIP (C) and volume rendering (D) reconstruction images of the same abnormal arterial lumen showing that both the pulmonary artery and thoracic aortic branches run to the sequestrated lung. The supplying artery-the branch of the thoracic aorta is abnormally tortuous and has localized cystic dilation at the origin of the supplying artery. The pulmonary artery extends straight into the sequestrated lung. Arrows refer to the supplying arteries to the pulmonary sequestion, CTPA-computed tomography pulmonary angiography, MIP- maximum-intensity projection.
Figure 4.
A 71-year-old male with intralobar pulmonary sequestration. Axial (A) and sagittal (B) computed tomography angiography demonstrating an intralobar polycystic sequestration in the lower lobe of the left lung that is cystic and heterogeneous. CTPA MIP (C) and volume rendering (D) reconstruction images of the same abnormal arterial lumen showing that both the pulmonary artery and thoracic aortic branches run to the sequestrated lung. The supplying artery-the branch of the thoracic aorta is abnormally tortuous and has localized cystic dilation at the origin of the supplying artery. The pulmonary artery extends straight into the sequestrated lung. Arrows refer to the supplying arteries to the pulmonary sequestion, CTPA-computed tomography pulmonary angiography, MIP- maximum-intensity projection.

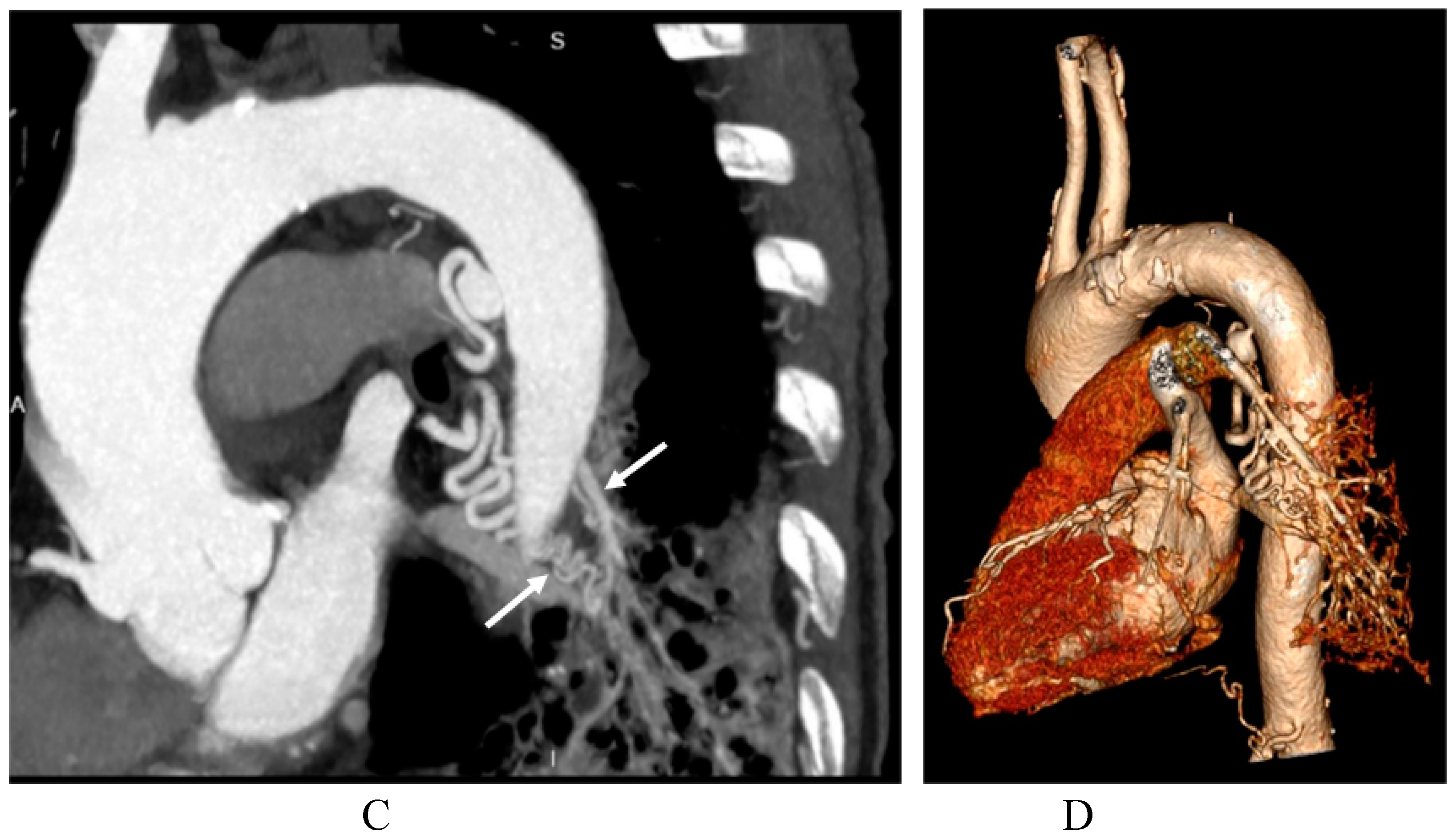
Figure 5.
An 81-year-old female with intralobar pulmonary sequestration. (A) CTPA MIP reconstruction image showing that both the pulmonary artery and thoracic aortic branches extend to the sequestrated lung. The supplying arteries-the branches of the thoracic aortic are abnormally tortuous (arrows), but the pulmonary artery is straight forward to the sequestrated lung. (B) Axial CT scan showing the main pulmonary trunk and pulmonary arteries to the right and left lungs are dilated (arrows). (C) Contrast-enhanced CT of the venous phase showing that the left inferior pulmonary vein is occluded. (D) Axial view of CT images (lung window) demonstrating a significant reduction in the volume of the left lower lung. CTPA-computed tomography pulmonary angiography.
Figure 5.
An 81-year-old female with intralobar pulmonary sequestration. (A) CTPA MIP reconstruction image showing that both the pulmonary artery and thoracic aortic branches extend to the sequestrated lung. The supplying arteries-the branches of the thoracic aortic are abnormally tortuous (arrows), but the pulmonary artery is straight forward to the sequestrated lung. (B) Axial CT scan showing the main pulmonary trunk and pulmonary arteries to the right and left lungs are dilated (arrows). (C) Contrast-enhanced CT of the venous phase showing that the left inferior pulmonary vein is occluded. (D) Axial view of CT images (lung window) demonstrating a significant reduction in the volume of the left lower lung. CTPA-computed tomography pulmonary angiography.
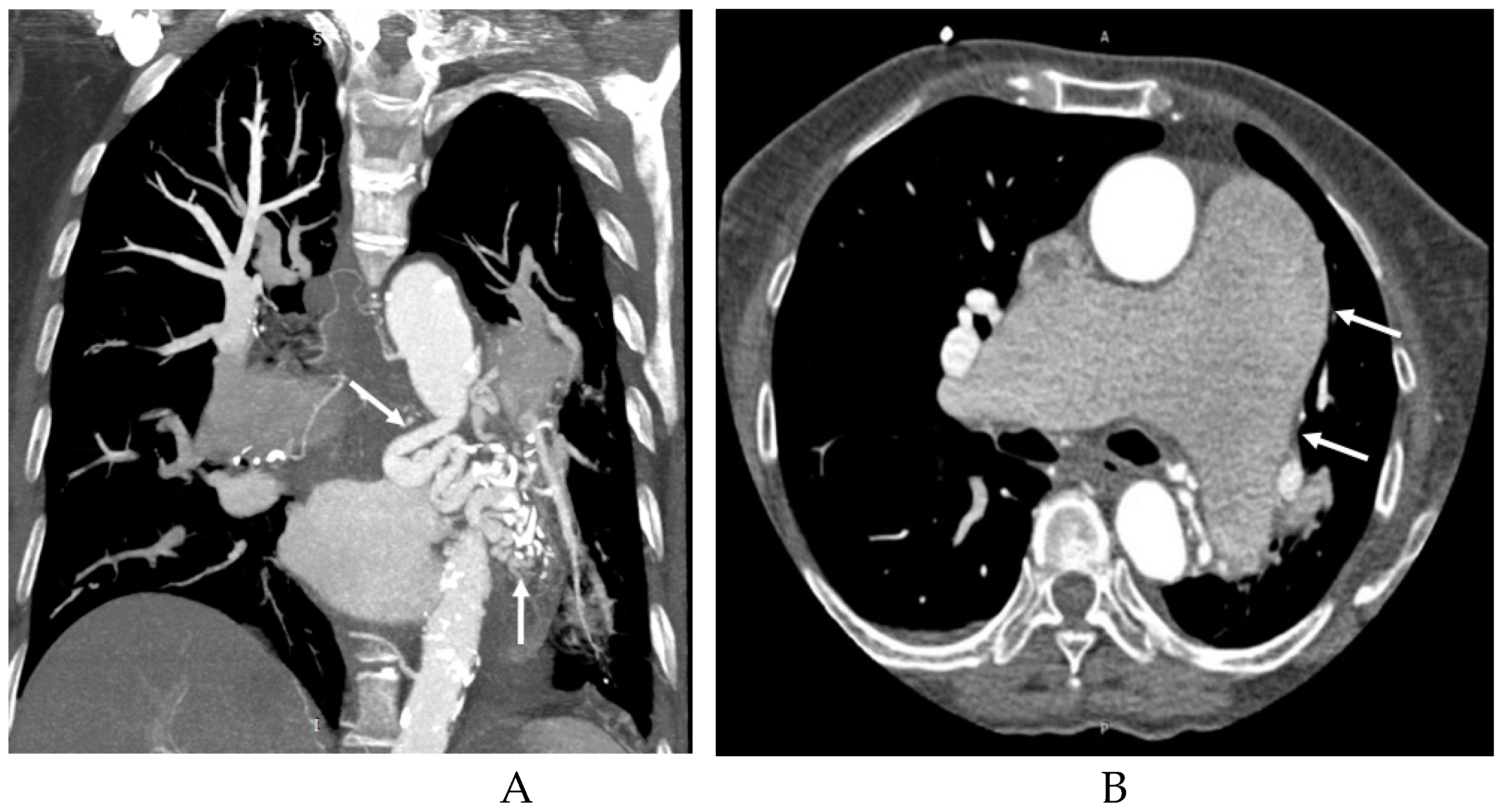
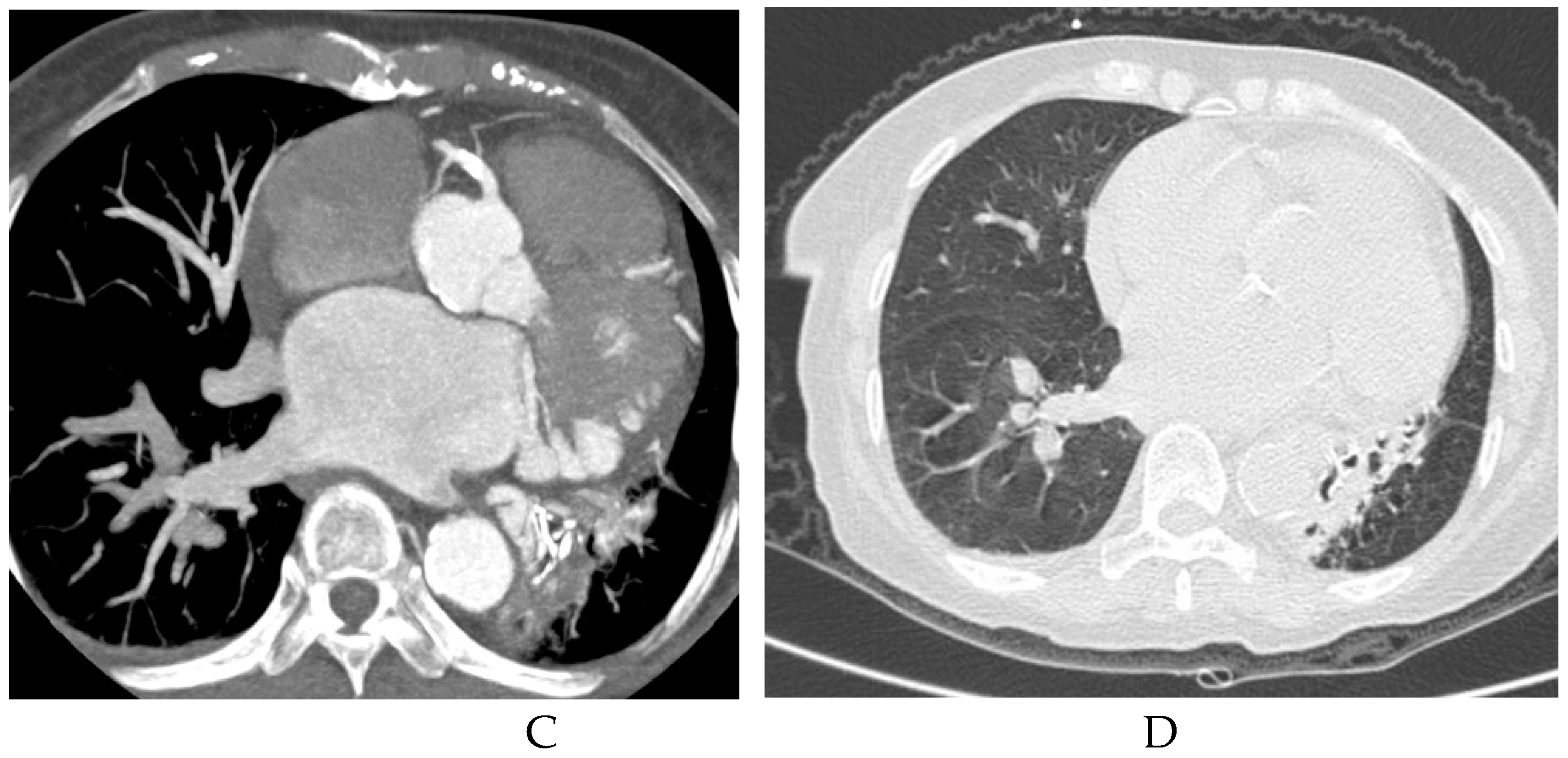

Table 1.
Imaging appearances of chest computed tomography pulmonary angiography in patients with pulmonary sequestration (n=55).
Table 1.
Imaging appearances of chest computed tomography pulmonary angiography in patients with pulmonary sequestration (n=55).
| Imaging appearances | Subtype | Number of cases |
| Subtype of disease | ILS | 54(98.18%) |
| ELS | 1(1.82%) | |
| Location of disease | LLL | 42(76.36%) |
| RLL | 12(21.82%) | |
| BLL | 1(1.82%) | |
| Supplying artery | Aorta A | 1(1.82%) |
| Aorta D | 47(85.45%) | |
| CA | 7(12.73%) | |
| BA | 1(1.82%) | |
| Draining vessels | PV | 49(89.09%) |
| UV | 1(1.82%) | |
| IV | 1(1.82%) | |
| PA | 11(20.00%) | |
| NF | 2(3.64%) |
ILS, intralobar sequestration; ELS, extralobar sequestration; RLL, right lower lobe, LLL, left lower lobe; BLL, both lower lobe; Aorta A, abdominal aorta; Aorta D, descending aorta; CA, celiac axis; BA, bronchial artery; PV, pulmonary vein; UV, Umbilical vein; IV, intercostal vein; PA, pulmonary artery; NF, not found.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



