
Submitted:
30 May 2023
Posted:
01 June 2023
You are already at the latest version
Abstract
Abstract: Presence in a recipient of antibodies directed against donor specific antigens represent a major obstacle in transplanting such patients. Removal of these antibodies represents a challenge for physicians dealing with kidney transplantation. Several strategies, techniques and old and new drugs are to date used to desensitize these patients.
Desensitization may occur before transplantation or at the time of transplantation or after transplantation according whether physicians deal with living or deceased donors. Different techniques may be used to reveal the presence of antibodies in the recipients; each technique has different sensitivity and specificity, different advantages and disadvantages.
The target of the drugs used to desensitize are B cells, Plasma cells, the antibodies themselves and finally, the complement that is the final actor causing tissue disruption.
If B cells are relatively easy to be targeted, more difficult are the plasma cell. Indeed, several new drugs are used in randomized trials also to defeat plasma cells. Antibodies may be removed rather easily, but often their removal is followed by a rebound.
Complement is not easy to be defeated and new drugs are to date used to be successful in this action. However is to date possible to desensitize many patients and to obtain successful transplantation.
Keywords:
Desensitization
; Donor specific antibodies
; HLA system
; antibodies identification
; B cells
; Plasma cells
; Complement
; New drugs
; Complemennt
Developing of sensitization
After the first alloantigen exposure, events such as pregnancies, transfusions, previous transplants or any contact with alloimmune antigens may generate a memory alloimmunity either cellular and serological [3,4].
When B cells bind to their cognate antigen, this initiates a migration toward the boundary between the B and T cell zones in lymphoid organs, where they compete for interactions with follicular helper cells. T follicular helper cells provide selection signals required for differentiation into Germinal Centers (GC) cells and antibody secreting cells. Additionally, it has been observed that after transplantation, circulating TFH expanded more significantly in patients who developed de novo anti HLA antibodies than in those who remained not sensitized [5]. An important role in generating alloimmune response is exerted by the long-lived plasma cells. After the generation of memory B cells, these transform in plasmablasts that are competent to home to survival niches. Plasmablasts migrate to bone marrow were generate long-lived plasma cells that migrate to survival niches under the effect of pathogen-associated molecular pattern (PAMP) [6,7]. Most of plasmablasts migrate to inflamed tissues, under the control of interferon gamma induced expression of CXC-chemokine receptor 3 (CXCR3) which binds CXC-chemokine ligand 9 (CXCL9), CXCL10 and CXCL11 [8,9].
Techniques to identify sensitization level and to stratify the risk
With different techniques is now possible to detect both the alloreactive serological memory and the alloreactive cellular memory in patients waiting for kidney transplantation so to stratifying the humoral and cellular risk of candidates to a solid organ transplantation [10].
The serological memory may be detected by complement dependent cytotoxicity [11], by flow cytometry [12], by solid phase assays as ELISA [13] and by bead-based assays as Luminex [14]. All these assays are shown on Table 1. Assays to evaluate alloreactive cellular memory are, among others, flow cytometry [15]. Elispot assay [16], solid phase assay [17], flow cytometry [18].
The immune-pathophysiology of DSA- mediated damages informs the prediction of antibody-mediated rejection and graft loss. The pathogenicity of DSA is routinely evaluated with their titer (MFI or dilution) or their ability to bind donor cells (by flow cytometry crossmatch). Ex vivo complement binding can be evaluated with the C1q and/or C3d assays. Analysis of complement fixing IgG subclasses or complement genetic variations, number of innate immune effectors and polymorphism of Fcγ receptors could all help to better stratify the risk of antibody-mediated rejection (AMR). Measurement of DSA affinity and glycosylation profile is not yet available. Finally, the characteristics of the target graft endothelial cell (level of expression of HLA molecules, stress-induced ligands or expression level of complement regulators or cytoprotective proteins) influence the pathogenicity of the DSA.
All the cited assays to detect the presence of HLA sensitization have different sensitivity and specificity. CDC has the lowest sensitivity that increases with the use of flow cytometry and a further increase is reached with the use of ELISA. The optimal sensitivity and sensibility is obtained with the use of single beads and with the use of complement binding. This fact allowed realizing the ENGAGE’s proposal for categorization of the humoral risk of solid organ transplant categories. The EuropeaN Guidelines for the mAnagement of Graft rEcipients (ENGAGE) [10] is an initiative from the European Society for Organ Transplantation that stratify the patient’s risk as follows:
- (a)
- If the patient has no DSA and no cellular memory, the transplant is possible with low risk for AMR;
- (b)
- If at the time of transplantation, there is absence of DSA, but there is a potential cellular memory against donor HLA, the transplant is possible with risk for AMR increased. The cellular memory is possible if there are historical DSA and/or pregnancy or previous transplant with repeat antigens. Other possibilities are transfusions with no information on blood donors.
- (c)
- If at the time of transplantation there are DSA, but with negative flow, the transplant is possible with risk for acute AMR and acceptable medium-term graft survival.
- (d)
- If at the time of transplantation there are DSA with positive flow and negative CDC, the transplant is possible, but there is a very high risk for acute AMR and accelerated chronic AMR.
- (e)
- If at the time of transplantation there are DSA with positive CDC, the transplant is not possible and there is the need of desensitization before proceeding with transplant.
Incidence of hyper immune patients and graft survival with desensitization
The number of hyper immune patients on the waiting list for kidney transplantation is increasing with the time. According Spanish data of 2020, sensitized patients with CDC-PRA >50% were from 10% to 15%, but the same patients evaluated by PRA-SAB (single antigen beads) increased to 40%- 50% [19].
In USA, according data from Montgomery et al. [20] more than 20.000 candidates for kidney transplant are sensitized. The authors conducted a study with desensitization on 211 sensitized patients and found that patient survival rates were 80.6% at 8 years from transplantation, as compared with 30.5% for patients that remained on waiting list. In a different multicenter study on the risk of incompatible kidney transplantation, Orandi et al. [21] compared the graft survival of patients with positive Luminex and negative flow cross match (PLNC) with positive flow and negative CDC (PFNC) and patients with positive CDC (PCC). All these patients were compared with compatible transplants. The hazard ratio (HR) for graft loss was 1.20 for PLNC, 1.65 for PFNC and 1.80 for PCC. The graft loss for the last two groups was significant (p<0.001). In a different study conducted in UK, Manook et al. [22] compared hyper immune patients desensitized before transplantation with compatible living donors (CLD) and compatible deceased donors (CDD). The 5-year graft survival rates were similar and the authors concluded that desensitization has no detrimental influence on patient survival rates, but does not offer a survival benefit.
Timing of desensitization
With respect to the day of transplantation, different timing and strategies may be applied.
In the case of living donation, an early pre-transplant desensitization is preferred until obtaining CDC or Flow X-match negative. Clearly different drugs at different dosage may be applied. In the case of deceased donors does not exist enough time and substantially two strategies may be applied. The immediate pre-transplant desensitization as used in Austria [23] or the post-transplant desensitization as used at the hospital Necker in Paris [24].
In the case of immediate pre-transplant desensitization, the Immunoadsorption (IA) is the preferred methods due to its ability to efficiently removal of IgG [25,26]. The IA treatment is immediately followed by the administration of antithymoglobulins (ATG) and/or anti-CD20 (rituximab). The graft survival rates at 3-year were similar in CDCXM positive and in CDCXM negative patients.
The protocol used at the hospital Necker in the case of deceased donors consisted in an induction therapy with ATG, which was started at the day of transplantation followed by high dose immunoglobulins (IVIg) that were repeated every 3 weeks for a total of 4 courses. At the end of plasmapheresis, 1 or 2 rituximab infusions were administered. The graft survival rates at 7-year post-transplantation were 80% even if lower to the graft survival of the control group.
Desensitization strategies and drugs
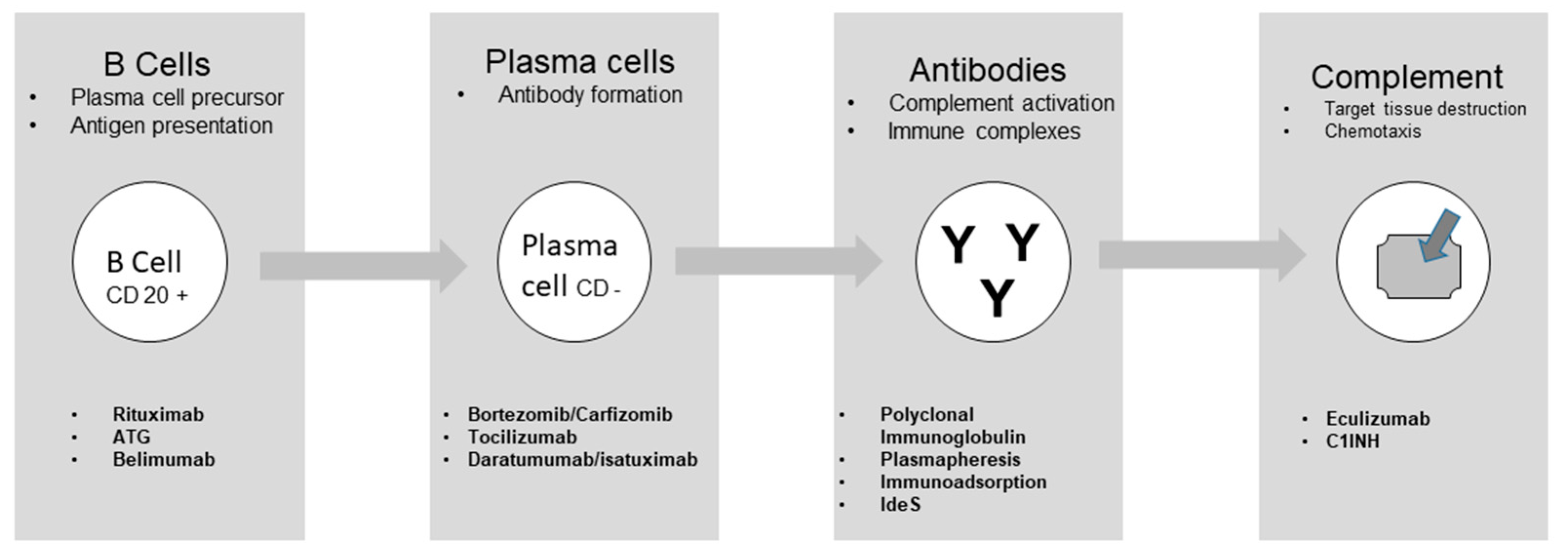
Summarizing what has been above descripted, 4 steps can be seen in the process leading to target tissue destruction. B cells are formed after antigen binding and B cells may act as antigen presentation and are precursor of Plasma cells. The second step is Plasma cells formation with consequent antibody formation. The antibodies that form immune complexes and activate the complement represent the third step. Finally, complement induces chemotaxis and lead to the target tissue destruction (Figure 1) [27].
Different drugs may act on the steps described. These drugs are well represented by the study of Jordan et al. [28] and their action is summarized in Table 2. In addition to the drugs described, there is an old, but efficient pleiotropic drug that may act at any stage. This are the IVIgs, generally given at the dose of 2g/kg for repeated times. The efficacy of IVIg, frequently associated with other drugs has been already described [24]. Vo et al. [29] conducted a study documenting the efficacy of IVIg in association with rituximab in inducing desensitization.
Drugs acting on B cells
Three main drugs act on B cell leading to their reduction and reducing their activity. Rituximab (RTX), ATG and Belimumab. In a study of Ramos et al. [30] conducted on 25 recipients of living donors needing desensitization, was evaluated the effectiveness of RTX, IVIg and ATG in reducing the number of splenic B cells and Plasma cells. The effect of multiple plasmapheresis plus low dose IVIg resulted enable in reducing naïve B cells, plasma cells and memory B cells. Adding RTX to the treatment was effective in reducing naïve B cells, without effect on memory B cells and plasma cells. Finally, adding ATG to the treatment led to reduction of memory B cells (CD27+), but again without any effect on plasma cells.
Belimumab inhibits growth and differentiation of B cells by blocking B lymphocyte stimulator (BAFF or BlyS). Indeed in normal conditions BAFF binds to the receptors, BAFF-R, B cell maturation antigen (BCMA) and transmembrane activator and CAML interactor (TACI) leading to immature B cell survival and maturation, plasma cell survival and B cell survival and proliferation [31,32,33]. Belimumab is a complete human IgG1λ recombinant monoclonal antibody directed against BAFF and initially used for the treatment of systemic lupus erythematosus (SLE) [34].
Belimumab monotherapy was studied as a desensitization agent in kidney transplantation. Nevertheless, the study was terminated early for reported lack of efficacy (NCT01025193) [35].
Another phase 2 double-blinded randomized placebo-controlled trial of Belimumab plus standard of care is being examined for prevention of allograft rejection in renal transplant recipients (NCT01536379) [36]. Finally, the study of Banham et al. [37] in an experimental medicine, randomized, placebo controlled trial documented the Belimumab efficacy. The concentration of activated memory B cells decreased from week 21 to 28 of the treatment and the addition of Belimumab to standard of care immunosuppression significantly reduced de novo IgG antibody.
Drugs acting on Plasma cells
The second step is represented by plasma cells both short and long living that are the principal responsible of antibody production. FcγRIIb that is an inhibitory receptor for the Fc portion of IgG controls the persistence and apoptosis of bone marrow plasma cells. It is expressed on B cells [38]. The crosslinking of FcγIIb on naïve B cells May induce apoptosis of B cells [39,40]. Another study documented that FcγIIb controls bone marrow plasma cells and if crosslinked induces plasma cells apoptosis [41].
A drug efficient in acting against Plasma cells is proteasome inhibitor. It is well documented that after proteasome inhibitor administration as Bortezomib there is a reduction in number of antigen-specific plasma cells in candidates to living donor kidney transplantation [42]. Bortezomib was able to reduce serum levels of DSA in patients, which were not affected by IVIg or RTX. In addition, Bortezomib reduced the number of antigen-specific plasma cells, without decreasing the total number of plasma cells. In a different study [43], proteasome inhibition caused apoptosis of normal human plasma cells preventing alloantibody production. Treatment with Bortezomib resulted in a significant increase in the percentage of apoptotic cells, while RTX, ATG and IVIg had no effect.
However, in different well-conducted studies, Bortezomib did not confirm its efficacy with respect to other treatments in reducing DSA after transplantation in sensitized patients. In particular, Ejaz et al. [44] divided their patients in four groups. One group received ATG alone, a second group received ATG + RTX, a third group received ATG + Bortezomib, a fourth group received ATG + RTX + Bortezomib. The results in their capacity to reduce DSA post-transplant was similar for all groups as shown in Table 3. Similarly, Eskandary et al. [45] conducted the study BORTEJECT. The study was a randomized, placebo-controlled trial to investigate the effect of Bortezomib on the course of late ABMR. Bortezomib given as single agent did not obtained improvement of the course of late rejection. These studies called for new agents acting on plasma cells. Carfilzomib is a second-generation irreversible proteasome inhibitor. It is an expoxyketone nonboronated molecule that proven to be effective and with reduced toxicity in the treatment of patients with multiple myeloma [46]. In a randomized clinical trial (NCT02442648) [47] the B-Cell Targeted Desensitization with Carfilzomib for Preformed Anti-HLA Antibodies in Patients Awaiting Kidney Transplantation has been evaluated. A study from Tremblay et al. evaluated the prospective [48], iterative, adaptive trial of carfilzomib-based desensitization. The study documented that HLA antibodies were substantially reduced in the group treated with carfilzomib alone.
A different strategy to an effective desensitization is by the use of the Interleukin-6 receptor specific humanized monoclonal antibody, better known as Tocilizumab. Indeed IL-6 promotes B cells differentiation to plasma cells and induces Th17 cells. Vo et al. [49] used Tocilizumab in addition to IVIg in patients difficult to be desensitized. Tocilizumab reduced DSA strength and numbers at transplant and 12 months after transplantation. Protocol biopsies showed no evidence of antibody-mediated rejection or transplant glomerulopathy. In the study, after effective desensitization and transplantation, patients subsequently received IVIg once and Tocilizumab monthly for 6 months. The number of patients is low and the authors themselves highlight that larger controlled studies are needed. Later on, Doberer et al. [50] verified the efficacy of a different anti-IL-6 antibody, Clazakizumab, on late ABMR. Clazakizumab is a humanized monoclonal IgG1 antibody. With respect to Tocilizumab has a higher affinity for IL-6 and a longer half-life, as documented by studies on psoriatic arthritis [51].
The receptor specific for plasma cells is CD38. Daratumumab is a human immunoglobulin IgGk1 monoclonal antibody that target the CD38 surface antigen on plasma cells. Daratumumab has been used successfully in treating multiple myeloma and AL amyloidosis. Moreover, unlike Bortezomib, Daratumumab targets nonmalignant plasma cells. Hence its efficacy in desensitization and in treatment of ABMR [52,53].
Drugs acting on antibodies
Plasma cells produce antibodies that are dangerous because may form immune complexes and may activate the complement cascade.
Removal of DSA antibodies is mandatory in the different methods of desensitization or of treating ABMR.
The use of IVIg has been already treated and represents an important strategy for desensitization as used at the Hospital Necker [24].
A pioneer study suggested that polyclonal Ig could be efficient at decreasing anti-HLA antibodies [59]. Later on, a randomized trial (NIH IG02) compared pre-transplant administration of polyclonal Ig with placebo in highly sensitized patients [60]. Unfortunately, the NIH IG02 documented that, even if the transplantation rate was higher in the IVIg group, there was only a mild and transient effect on PRA. This fact led to a higher incidence of ABMR in the IVIg treatment group.
IVIg seems to be more efficient when associated with mechanical antibody removal as obtained with plasmapheresis. Montgomery et al. [61] conducted a study in sensitized living-donor kidney transplant recipients. Desensitization was conducted with a combination of plasmapheresis (PE) and subministration of IVIg. Post-transplant ABMR occurred as effect of antibody rebound after contact with allogenic antigens. The ABMR was easier controlled with new cycle of PE and low dose IVIg. As recommended by the already mentioned desensitization protocol [24], it is essential that the administration of IVIg always follow the PE to avoid the removal of Ig with the PE treatment.
According the European Guideline for the management of kidney transplant patients with HLA antibodies both PE and Immunoadsorption are effective [62]. Their efficacy is higher when associated with IVIg and RTX. IA is more selective and is the preferred method by some authors, in particular in the preparation of AB0 incompatible kidney transplantation [63,64,65].
A different method to neutralize antibodies is the use of the IgG-degrading enzyme derived from Streptococcus pyogenes (IdeS) that cleaves intact IgG. Intact human IgG is cleaved by IdeS in two steps. The first step results in a single cleavage of the IgG molecule in which one heavy chain remains intact. The second step generates a fully cleaved molecule that cannot mediate complement-dependent cytotoxicity (CDC) or antibody-dependent cytotoxicity (ADCC) by means of Fcγ receptors [66,67]. A study from Jordan et al. [68] represents the first pilot study that combines 2 phase 1-2 trials undertaken independently. Overall, 25 highly immunized recipients were treated: 14 in the USA, 11 in Sweden. 1 shot of IdeS 4 to 6 hours before transplantation. IdeS is extremely potent at cleaving circulating IgG, but the effect may be transient. The extent and frequency of DSA rebound after transplantation highly varied between the Swedish and the American arms of the study. Indeed, in the Swedish group DSA remained undetectable up to 14 days from transplantation, with a subsequent rebound. In the USA patients, the rebound was very low. This possibly is the effect of the use of IVIg plus RTX before and after transplantation [69,70]
Drugs acting on complement
The fourth and final step to be targeted is the complement that favors chemotaxis and lead to tissue destruction. It has been documented that terminal complement inhibition decreases ABMR rates in sensitized renal transplant recipients [71]. In this study, complement inhibition and desensitization was made with the use of the anti C5 eculizimab. Eculizumab was given at the dose of 1200 mg immediately prior to transplantation, 600 mg on postoperative day 1 and 600 mg weekly for 4 weeks. Eculizumab was than discontinued if DSA had significantly decreased or continued until B flow crossmatch channel shift was < 200. Graft survival and ABMR rates were significantly lower in the eculizumab group with respect to control group. However, looking at the outcomes beyond 1 year, the incidence of transplant glomerulopathy did not differ in the two groups [72]. In a more recent study, Marks et al. [73] conducted a randomized trial on the safety and efficacy of eculizumab in the prevention of antibody-mediated rejection in living-donor kidney transplant recipients requiring desensitization. There was a lower rate of ABMR in the eculizumab arm compared to the arm with standard of care. However, at 3 years there was a similar graft survival.
A different and new way of targeting complement is to target the enzymes of the initiating complement cascade [74]. This can be obtained by the use of the serine protease inhibitor (C1INH) [75]. There are two forms of C1INH: the ultra-pure derived C1INH and the full-length recombinant C1INH. This drug has its advantage and its drawback. Advantage is its knowledge for the fact of being the standard of care for hereditary angioedema [76,77]. Additionally, plasma derived molecules are not immunogenic and it has a broad effect on classical and lectin pathways. Main drawback is the lack of specificity. Indeed, C1INH also controls Mannose-binding lectin-associated serine protease (MASP) and protease in the coagulation and kinin systems. Though being new and promising, to date C1INH is only used in preliminary results of ABMR treatment, but it is not yet used as prophylaxis.
Author Contributions
M.S. designed the study, performed the last revision. Collected data from literature and wrote the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The Author does not have any conflict of interest in relation to the manuscript.
References
- Salvadori M. Strategies for access to kidney transplantation for highly sensitized and incompatible patients Transplantology 2023; 4:85-89.
- Luque S, Lúcia M, Bestard O. Refinement of humoral immune monitoring in kidney transplantation: the role of “hidden” alloreactive memory B cells. Transpl Int. 2017 ; 30 : 955-968. [CrossRef]
- orija A, Favà A, Meneghini M, Crespo E, Bestard O. Novel insights into the pathobiology of humoral alloimmune memory in kidney transplantation. Curr Opin Organ Transplant. 2020; 25 :15-21. [CrossRef]
- Chong AS. New insights into the development of B cell responses: Implications for solid organ transplantation. Hum Immunol. 2019; 80 :378-384. /: :378-384 ttps.
- Cano-Romero FL, Laguna Goya R, Utrero-Rico A, Gómez-Massa E, Arroyo-Sánchez D, Suárez-Fernández P, Lora D, Andrés A, Castro-Panete MJ, Paz-Artal E. Longitudinal profile of circulating T follicular helper lymphocytes parallels anti-HLA sensitization in renal transplant recipients. Am J Transplant. 2019; 19 :89-97. [CrossRef]
- Radbruch A, Muehlinghaus G, Luger EO, Inamine A, Smith KG, Dörner T, Hiepe F. Competence and competition: the challenge of becoming a long-lived plasma cell. Nat Rev Immunol. 2006; 6 :741-750.
- Manz RA, Thiel A, Radbruch A. Lifetime of plasma cells in the bone marrow. Nature. 1997; 388 :133-134.
- Muehlinghaus G, Cigliano L, Huehn S, Peddinghaus A, Leyendeckers H, Hauser AE, Hiepe F, Radbruch A, Arce S, Manz RA. Regulation of CXCR3 and CXCR4 expression during terminal differentiation of memory B cells into plasma cells. Blood. 2005;105 :3965-3971. [CrossRef]
- Baggiolini M. Chemokines and leukocyte traffic. Nature. 1998; 392 : 565-568. [CrossRef]
- Bestard O, Couzi L, Crespo M, Kessaris N, Thaunat O. Stratifying the humoral risk of candidates to a solid organ transplantation: a proposal of the ENGAGE working group. Transpl Int. 2021; 34 :1005-1018. [CrossRef]
- Patel R, Terasaki PI. Significance of the positive crossmatch test in kidney transplantation. N Engl J Med. 1969 ; 280 :735-739. [CrossRef]
- Bray RA, Tarsitani C, Gebel HM, Lee JH. Clinical cytometry and progress in HLA antibody detection. Methods Cell Biol. 2011; 103: 285-310. [CrossRef]
- Schlaf G, Pollok-Kopp B, Manzke T, Schurat O, Altermann W. Novel solid phase-based ELISA assays contribute to an improved detection of anti-HLA antibodies and to an increased reliability of pre- and post-transplant crossmatching. NDT Plus. 2010; 3 :527-538.
- Tait BD. Detection of HLA Antibodies in Organ Transplant Recipients - Triumphs and Challenges of the Solid Phase Bead Assay. Front Immunol. 2016; 7:570. [CrossRef]
- Zachary AA, Kopchaliiska D, Montgomery RA, Leffell MS. HLA-specific B cells: I. A method for their detection, quantification, and isolation using HLA tetramers. Transplantation. 2007; 83 :982-988. [CrossRef]
- Lúcia M, Luque S, Crespo E, Melilli E, Cruzado JM, Martorell J, Jarque M, Gil-Vernet S, Manonelles A, Grinyó JM, Bestard O. Preformed circulating HLA-specific memory B cells predict high risk of humoral rejection in kidney transplantation. Kidney Int. 2015; 88 :874-887.
- Karahan GE, Krop J, Wehmeier C, de Vaal YJH, Langerak-Langerak J, Roelen DL, Lardy NM, Bemelman FJ, Ten Berge IJM, Reinders MEJ, van Kooten C, Claas FHJ, Heidt S. An Easy and Sensitive Method to Profile the Antibody Specificities of HLA-specific Memory B Cells. Transplantation. 2019; 103 : 716-723. [CrossRef]
- Dahdal S, Saison C, Valette M, Bachy E, Pallet N, Lina B, Koenig A, Monneret G, Defrance T, Morelon E, Thaunat O. Residual Activatability of Circulating Tfh17 Predicts Humoral Response to Thymodependent Antigens in Patients on Therapeutic Immunosuppression. Front Immunol. 2019; 9 :3178. [CrossRef]
- Gobierno de España, Ministerio de Sanidad Organizatión National de Transplantes Informe 2020. [CrossRef]
- Montgomery RA, Lonze BE, King KE, Kraus ES, Kucirka LM, Locke JE, Warren DS, Simpkins CE, Dagher NN, Singer AL, Zachary AA, Segev DL. Desensitization in HLA-incompatible kidney recipients and survival. N Engl J Med. 2011; 365 :318-326.
- Orandi BJ, Garonzik-Wang JM, Massie AB, Zachary AA, Montgomery JR, Van Arendonk KJ, Stegall MD, Jordan SC, Oberholzer J, Dunn TB, Ratner LE, Kapur S, Pelletier RP, Roberts JP, Melcher ML, Singh P, Sudan DL, Posner MP, El-Amm JM, Shapiro R, Cooper M, Lipkowitz GS, Rees MA, Marsh CL, Sankari BR, Gerber DA, Nelson PW, Wellen J, Bozorgzadeh A, Gaber AO, Montgomery RA, Segev DL. Quantifying the risk of incompatible kidney transplantation: a multicenter study. Am J Transplant. 2014; 14 :1573-1580. [CrossRef]
- Manook M, Koeser L, Ahmed Z, Robb M, Johnson R, Shaw O, Kessaris N, Dorling A, Mamode N. Post-listing survival for highly sensitised patients on the UK kidney transplant waiting list: a matched cohort analysis. Lancet. 2017 ; 389 :727-734.
- Schwaiger E, Eskandary F, Kozakowski N, Bond G, Kikić Ž, Yoo D, Rasoul-Rockenschaub S, Oberbauer R, Böhmig GA. Deceased donor kidney transplantation across donor-specific antibody barriers: predictors of antibody-mediated rejection. Nephrol Dial Transplant. 2016; 31 :1342-1351. [CrossRef]
- Amrouche L, Aubert O, Suberbielle C, Rabant M, Van Huyen JD, Martinez F, Sberro-Soussan R, Scemla A, Tinel C, Snanoudj R, Zuber J, Cavalcanti R, Timsit MO, Lamhaut L, Anglicheau D, Loupy A, Legendre C. Long-term Outcomes of Kidney Transplantation in Patients With High Levels of Preformed DSA: The Necker High-Risk Transplant Program. Transplantation. 2017; 101: 2440-2448. 2448. [CrossRef]
- Lorenz M, Regele H, Schillinger M, Kletzmayr J, Haidbauer B, Derfler K, Druml W, Böhmig GA. Peritransplant immunoadsorption: a strategy enabling transplantation in highly sensitized crossmatch-positive cadaveric kidney allograft recipients. Transplantation. 2005; 79 :696-701.
- Morath C, Beimler J, Opelz G, Scherer S, Schmidt J, Macher-Goeppinger S, Klein K, Sommerer C, Schwenger V, Zeier M, Süsal C. Living donor kidney transplantation in crossmatch-positive patients enabled by peritransplant immunoadsorption and anti-CD20 therapy. Transpl Int. 2012; 25: 506-517. [CrossRef]
- Fehr T, Gaspert A. Antibody-mediated kidney allograft rejection: therapeutic options and their experimental rationale. Transpl Int. 2012; 25 :623-632. [CrossRef]
- Jordan SC, Ammerman N, Choi J, Huang E, Peng A, Sethi S, Najjar R, Toyoda M, Lim K, Louie S, Vo A. Novel Therapeutic Approaches to Allosensitization and Antibody-mediated Rejection. Transplantation. 2019; 103 :262-272.
- Vo AA, Lukovsky M, Toyoda M, Wang J, Reinsmoen NL, Lai CH, Peng A, Villicana R, Jordan SC. Rituximab and intravenous immune globulin for desensitization during renal transplantation. N Engl J Med. 2008; 359 :242-251. [CrossRef]
- Ramos EJ, Pollinger HS, Stegall MD, Gloor JM, Dogan A, Grande JP. The effect of desensitization protocols on human splenic B-cell populations in vivo. Am J Transplant. 2007; 7 :402-407. [CrossRef]
- Dhilleswara RV, Belimumab: therapeutic mechanism and current status of clinical trials Biomed Res 2018; 29: 3034-3039. 3: RV, Belimumab: therapeutic mechanism and current status of clinical trials Biomed Res 2018; 29. [CrossRef]
- Treml JF, Hao Y, Stadanlick JE, Cancro MP. The BLyS family: toward a molecular understanding of B cell homeostasis. Cell Biochem Biophys. 2009; 53 :1-16.
- Mackay F, Schneider P. Cracking the BAFF code Nat Rev Immunol. 2009 ; 9 :491-502. [CrossRef]
- Dubey AK, Handu SS, Dubey S, Sharma P, Sharma KK, Ahmed QM. Belimumab: First targeted biological treatment for systemic lupus erythematosus. J Pharmacol Pharmacother. 2011; 2 :317-319.
- NCT01025193 Clinical trial.gov Naji A University of Pennsylvania Desensitization With Belimumab in Sensitized Patients Awaiting Kidney Transplant. Accessed May 19, 2023. [CrossRef]
- NCT01536379 Clinical trial.gov GSK Investigational Site Cambridge UK A Study of Belimumab in the Prevention of Kidney Transplant Rejection. Accessed May 19, 2023.
- Banham GD, Flint SM, Torpey N, Lyons PA, Shanahan DN, Gibson A, Watson CJE, O’Sullivan AM, Chadwick JA, Foster KE, Jones RB, Devey LR, Richards A, Erwig LP, Savage CO, Smith KGC, Henderson RB, Clatworthy MR. Belimumab in kidney transplantation: an experimental medicine, randomised, placebo-controlled phase 2 trial. Lancet. 2018 Jun 30;391(10140):2619-2630.
- Ravetch jv, Bolland S IgG Fc receptors Ann Rev Immunol 2001; 19: 275-290.
- Pearse RN SHIP recruitment attenuates FcγIIB-induced apoptosis. Immunity 1999; 10: 753-760.
- Mackay M, Stanevsky A, Wang T, Aranow C, Li M, Koenig S, J Ravetch JV, Diamond B Selective dysregulation of the FcgammaIIB receptor on memory B cells in SLE J Exp Med 2006; 203 :2157-2164.
- Xiang Z, Cutler AJ, Brownlie RJ, Fairfax K, Lawlor KE, Severinson E, Walker EU, Manz RA, Tarlinton DM, Smith KG. FcgammaRIIb controls bone marrow plasma cell persistence and apoptosis. Nat Immunol. 2007; 8 : 419-429.
- Diwan TS, Raghavaiah S, Burns JM, Kremers WK, Gloor JM, Stegall MD. The impact of proteasome inhibition on alloantibody-producing plasma cells in vivo. Transplantation. 2011; 9 :536-541.
- Perry DK, Burns JM, Pollinger HS, Amiot BP, Gloor JM, Gores GJ, Stegall MD. Proteasome inhibition causes apoptosis of normal human plasma cells preventing alloantibody production. Am J Transplant. 2009; 9 : 201-209. [CrossRef]
- Ejaz NS, Shields AR, Alloway RR, Sadaka B, Girnita AL, Mogilishetty G, Cardi M, Woodle ES. Randomized controlled pilot study of B cell-targeted induction therapy in HLA sensitized kidney transplant recipients. Am J Transplant. 2013 ;13 :3142-3154. [CrossRef]
- Eskandary F, Regele H, Baumann L, Bond G, Kozakowski N, Wahrmann M, Hidalgo LG, Haslacher H, Kaltenecker CC, Aretin MB, Oberbauer R, Posch M, Staudenherz A, Handisurya A, Reeve J, Halloran PF, Böhmig GA. A Randomized Trial of Bortezomib in Late Antibody-Mediated Kidney Transplant Rejection. J Am Soc Nephrol. 2018; 29 :591-605. [CrossRef]
- Gandolfi S, Laubach JP, Hideshima T, Chauhan D, Anderson KC, Richardson PG. The proteasome and proteasome inhibitors in multiple myeloma. Cancer Metastasis Rev. 2017; 36: 561-584. [CrossRef]
- NCT 02442648 Clinical Trial.gov. Woodle ES B-Cell Targeted Desensitization With Carfilzomib for Preformed Anti-HLA Antibodies in Patients Awaiting Kidney Transplantation. Accessed May 22, 2023. 22 May. [CrossRef]
- Tremblay S, Driscoll JJ, Rike-Shields A, Hildeman DA, Alloway RR, Girnita AL, Brailey PA, Woodle ES. A prospective, iterative, adaptive trial of carfilzomib-based desensitization. Am J Transplant. 2020 ;20 :411-421.
- Vo AA, Choi J, Kim I, Louie S, Cisneros K, Kahwaji J, Toyoda M, Ge S, Haas M, Puliyanda D, Reinsmoen N, Peng A, Villicana R, Jordan SC. A Phase I/II Trial of the Interleukin-6 Receptor-Specific Humanized Monoclonal (Tocilizumab) + Intravenous Immunoglobulin in Difficult to Desensitize Patients. Transplantation. 2015 ; 99 : 2356-2363. [CrossRef]
- Doberer K, Duerr M, Halloran PF, Eskandary F, Budde K, Regele H, Reeve J, Borski A, Kozakowski N, Reindl-Schwaighofer R, Waiser J, Lachmann N, Schranz S, Firbas C, Mühlbacher J, Gelbenegger G, Perkmann T, Wahrmann M, Kainz A, Ristl R, Halleck F, Bond G, Chong E, Jilma B, Böhmig GA. A Randomized Clinical Trial of Anti-IL-6 Antibody Clazakizumab in Late Antibody-Mediated Kidney Transplant Rejection. J Am Soc Nephrol. 2021; 32 : 708-722. [CrossRef]
- Mease PJ, Gottlieb AB, Berman A, Drescher E, Xing J, Wong R, Banerjee S. The Efficacy and Safety of Clazakizumab, an Anti-Interleukin-6 Monoclonal Antibody, in a Phase IIb Study of Adults With Active Psoriatic Arthritis. Arthritis Rheumatol. 2016 ; 68 : 2163-2173. [CrossRef]
- Kaufman GP, Schrier SL, Lafayette RA, Arai S, Witteles RM, Liedtke M. Daratumumab yields rapid and deep hematologic responses in patients with heavily pretreated AL amyloidosis. Blood. 2017; 130 : 900-902. [CrossRef]
- Mateos MV, Dimopoulos MA, Cavo M, Suzuki K, Jakubowiak A, Knop S, Doyen C, Lucio P, Nagy Z, Kaplan P, Pour L, Cook M, Grosicki S, Crepaldi A, Liberati AM, Campbell P, Shelekhova T, Yoon SS, Iosava G, Fujisaki T, Garg M, Chiu C, Wang J, Carson R, Crist W, Deraedt W, Nguyen H, Qi M, San-Miguel J; ALCYONE Trial Investigators. Daratumumab plus Bortezomib, Melphalan, and Prednisone for Untreated Myeloma. N Engl J Med. 2018; 378 :518-528. [CrossRef]
- Kwun J, Matignon M, Manook M, Guendouz S, Audard V, Kheav D, Poullot E, Gautreau C, Ezekian B, Bodez D, Damy T, Faivre L, Menouche D, Yoon J, Park J, Belhadj K, Chen D, Bilewski AM, Yi JS, Collins B, Stegall M, Farris AB, Knechtle S, Grimbert P Daratumumab in Sensitized Kidney Transplantation: Potentials and Limitations of Experimental and Clinical Use. J Am Soc Nephrol. 2019; 30 : 1206-1219.
- Joher N, Matignon M, Grimbert P. HLA Desensitization in Solid Organ Transplantation: Anti-CD38 to Across the Immunological Barriers. Front Immunol. 2021;12 :688301.
- Doberer K, Kläger J, Gualdoni GA, Mayer KA, Eskandary F, Farkash EA, Agis H, Reiter T, Reindl-Schwaighofer R, Wahrmann M, Cohen G, Haslacher H, Bond G, Simonitsch-Klupp I, Halloran PF, Böhmig GA. CD38 Antibody Daratumumab for the Treatment of Chronic Active Antibody-mediated Kidney Allograft Rejection. Transplantation. 2021; 105 :451-457. [CrossRef]
- Spica D, Junker T, Dickenmann M, Schaub S, Steiger J, Rüfli T, Halter J, Hopfer H, Holbro A, Hirt-Minkowski P. Daratumumab for Treatment of Antibody-Mediated Rejection after ABO-Incompatible Kidney Transplantation. Case Rep Nephrol Dial. 2019; 9 :149-157. [CrossRef]
- Aguilera Agudo C, Gómez Bueno M, Krsnik Castello I. Daratumumab for Antibody-mediated Rejection in Heart Transplant-A Novel Therapy: Successful Treatment of Antibody-mediated Rejection. Transplantation. 2021;105 : e30-e31. [CrossRef]
- Glotz D, Antoine C, Julia P, Suberbielle-Boissel C, Boudjeltia S, Fraoui R, Hacen C, Duboust A, Bariety J. Desensitization and subsequent kidney transplantation of patients using intravenous immunoglobulins (IVIg). Am J Transplant. 2002; 2 :758-760.
- Jordan SC, Tyan D, Stablein D, McIntosh M, Rose S, Vo A, Toyoda M, Davis C, Shapiro R, Adey D, Milliner D, Graff R, Steiner R, Ciancio G, Sahney S, Light J. Evaluation of intravenous immunoglobulin as an agent to lower allosensitization and improve transplantation in highly sensitized adult patients with end-stage renal disease: report of the NIH IG02 trial. J Am Soc Nephrol. 2004; 15 :3256-3562. [CrossRef]
- Montgomery RA, Zachary AA, Racusen LC, Leffell MS, King KE, Burdick J, Maley WR, Ratner LE. Plasmapheresis and intravenous immune globulin provides effective rescue therapy for refractory humoral rejection and allows kidneys to be successfully transplanted into cross-match-positive recipients. Transplantation. 2000; 70 :887-895.
- Mamode N, Bestard O, Claas F, Furian L, Griffin S, Legendre C, Pengel L, Naesens M. European Guideline for the Management of Kidney Transplant Patients With HLA Antibodies: By the European Society for Organ Transplantation Working Group. Transpl Int. 2022 ; 35 : 10511. [CrossRef]
- Chen X, Wang Y, Dong P, Wang J, Yu X, Yu B. Efficacy of Combined Desensitization Therapy Based on Protein A Immunoadsorption on Anti-human Leukocyte Antigen Antibodies in Sensitized Kidney Transplant Recipients: A Retrospective Study. Cureus. 2022 ; 14 : e28661. [CrossRef]
- Kälble F, Süsal C, Pego da Silva L, Speer C, Benning L, Nusshag C, Pham L, Tran H, Schaier M, Sommerer C, Beimler J, Mehrabi A, Zeier M, Morath C. Living Donor Kidney Transplantation in Patients With Donor-Specific HLA Antibodies After Desensitization With Immunoadsorption. Front Med (Lausanne). 2021; 8 :781491. [CrossRef]
- Junker T, Volken T, Stehle G, Drexler B, Infanti L, Buser A, Passweg J, Schaub S, Dickenmann M, Halter J, Holbro A. Safety and Feasibility of Immunoadsorption with Heparin Anticoagulation in Preparation of ABO-Incompatible Kidney Transplantation: A Retrospective Single-Center Study. Transfus Med Hemother. 2023; 50 : 76-87.
- von Pawel-Rammingen U, Björck L. IdeS and SpeB: immunoglobulin-degrading cysteine proteinases of Streptococcus pyogenes. Curr Opin Microbiol. 2003 ; 6 :50-55. [CrossRef]
- Järnum S, Bockermann R, Runström A, Winstedt L, Kjellman C. The Bacterial Enzyme IdeS Cleaves the IgG-Type of B Cell Receptor (BCR), Abolishes BCR-Mediated Cell Signaling, and Inhibits Memory B Cell Activation. J Immunol. 2015 ; 195 : 5592-5601. [CrossRef]
- Jordan SC, Lorant T, Choi J, Kjellman C, Winstedt L, Bengtsson M, Zhang X, Eich T, Toyoda M, Eriksson BM, Ge S, Peng A, Järnum S, Wood KJ, Lundgren T, Wennberg L, Bäckman L, Larsson E, Villicana R, Kahwaji J, Louie S, Kang A, Haas M, Nast C, Vo A, Tufveson G. IgG Endopeptidase in Highly Sensitized Patients Undergoing Transplantation. N Engl J Med. 2017; 377 :442-453.
- Vo AA, Choi J, Cisneros K, Reinsmoen N, Haas M, Ge S, Toyoda M, Kahwaji J, Peng A, Villicana R, Jordan SC. Benefits of rituximab combined with intravenous immunoglobulin for desensitization in kidney transplant recipients. Transplantation. 2014; 98 :312-319. [CrossRef]
- Zachary AA, Lucas DP, Montgomery RA, Leffell MS. Rituximab prevents an anamnestic response in patients with cryptic sensitization to HLA. Transplantation. 2013; 95 : 701-704. [CrossRef]
- Stegall MD, Diwan T, Raghavaiah S, Cornell LD, Burns J, Dean PG, Cosio FG, Gandhi MJ, Kremers W, Gloor JM. Terminal complement inhibition decreases antibody-mediated rejection in sensitized renal transplant recipients. Am J Transplant. 2011;11 :2405-2413. [CrossRef]
- Cornell LD, Schinstock CA, Gandhi MJ, Kremers WK, Stegall MD. Positive crossmatch kidney transplant recipients treated with eculizumab: outcomes beyond 1 year. Am J Transplant. 2015; 15 :1293-1302. [CrossRef]
- Marks WH, Mamode N, Montgomery RA, Stegall MD, Ratner LE, Cornell LD, Rowshani AT, Colvin RB, Dain B, Boice JA, Glotz D; C10-001 Study Group. Safety and efficacy of eculizumab in the prevention of antibody-mediated rejection in living-donor kidney transplant recipients requiring desensitization therapy: A randomized trial. Am J Transplant. 2019; 19 :2876-2888. [CrossRef]
- Morgan BP, Harris CL. Complement, a target for therapy in inflammatory and degenerative diseases. Nat Rev Drug Discov. 2015; 14 :857-877. [CrossRef]
- Sharp JA, Whitley PH, Cunnion KM, Krishna NK. Peptide inhibitor of complement c1, a novel suppressor of classical pathway activation: mechanistic studies and clinical potential. Front Immunol. 2014 ; 5 : 406. [CrossRef]
- Gadek JE, Hosea SW, Gelfand JA, Santaella M, Wickerhauser M, Triantaphyllopoulos DC, Frank MM. Replacement therapy in hereditary angioedema: successful treatment of acute episodes of angioedema with partly purified C1 inhibitor. N Engl J Med. 1980; 302 : 542-546. [CrossRef]
- Zanichelli A, Mansi M, Periti G, Cicardi M. Therapeutic management of hereditary angioedema due to C1 inhibitor deficiency. Expert Rev Clin Immunol. 2013 ; 9 :477-488. [CrossRef]
Figure 1.
targeting different cells or functions.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



