Submitted:
29 May 2023
Posted:
30 May 2023
You are already at the latest version
Abstract
Background: Routine human papillomavirus (HPV) vaccine uptake continues to be suboptimal since its recommendation in 2006 for girls and in 2011 for boys. This paper aims to review published quality improvement (QI) methodologies on interventions to improve HPV vaccine uptake among adolescents; Methods: Science Direct and Scopus databases were searched for QI initiatives evaluating the effect of multimodal interventions to improve HPV vaccination rates (initiation and/or completion of series) among adolescents. Studies that included an outcome of interest among adolescents aged 10 to 18 years old were included. Two investigators worked independently to screen for potential articles and a designated investigator extracted data on study characteristics and evaluated the outcomes; Results: Preliminary search yielded a total of 523 articles and 13 were included in the final analysis. Common strategies were provider-specific and patient- and/or parent-specific interventions, with an emphasis on education and knowledge empowerment. System-level interventions such as policy changes and revised protocol were less commonly prescribed despite being associated with more significant weight on the overall outcome; Conclusions: Creative, sustainable, and economical multilevel interventions that focus not only on provider training and public education but also incorporate local policy and system enhancement can substantially improve HPV vaccination coverage among adolescents.
Keywords:
quality improvement
; systematic review
; papillomavirus vaccine
; vaccination coverage
; adolescent
1. Introduction
Human papillomavirus (HPV) vaccine administration is recommended for adolescents by the age of 11 or 12 years to protect them from cancer-causing infections and precancers caused by HPV infection. HPV vaccination has been shown to be an effective primary prevention method to reduce the associated healthcare costs [1] through the 2-dose 6-monthly interval vaccination series for all children aged 11 to 12 years old [2]. In addition, the 9-valent HPV vaccine is highly protective against most HPV-related cancers and genital warts that are associated with high morbidity and mortality [1,3].
In the United States (US), recent data on the coverage of at least one dose of HPV vaccine among adolescents age 13 to 17 years old had increased from 71.5% in 2019 to 75.1% in 2020 [4]. Despite this promising observation, the figure is still well below the recommendation towards Healthy People 2020 HPV vaccine goal of 80% [1,5]. The Healthy People initiative is part of the US federal government’s prevention agenda towards a healthier nation in which several key domains were led by the US Centers for Disease Control and Prevention (CDC). The CDC has been playing pivotal role in supporting efforts by various organizations and institutions that aim at improving the uptake of HPV vaccination.
Globally, multitudinal quality improvement strategies have been devised to improve HPV vaccination rates; focusing on provider education on effective communication and HPV vaccine recommendations, prioritizing HPV vaccination along with other scheduled vaccinations, establishing strong partnerships between local healthcare facilities and departments, as well as developing and disseminating HPV-related resources for the public and providers [6]. In Malaysia for example, HPV vaccination program targeting school-based 13-year-old girls was launched since August 2010 as part of the National Immunization Program. Within two years of its implementation, approximately 250,000 girls were successfully vaccinated, achieving the national target [7].
To date, the barriers to complete HPV vaccine administration among adolescents largely stem from the lack of knowledge or misinformation among the public. Such misconception contributes to parental concerns regarding vaccine safety and efficacy and subsequently hesitations to receive the vaccination [5]. The literature also recognizes the perceived lack of necessity among parents or caregivers for HPV vaccination because their child is still young and not sexually active as a barrier. HPV vaccine is commonly misconstrued as a clearance to engage in risky sexual activity, thus further impeding its acceptance among certain populations [8,9]. The evaluation of current practices is vital to formulate best approaches to overcome these barriers and misconceptions. An improved level of health literacy among the public can promote the uptake of HPV vaccination. In this study, we aim to review published quality improvement reports on the interventions to improve HPV vaccination rates among adolescents in healthcare settings.
2. Methods
2.1. Database search
This review involved a database search using pre-defined search strategy on Scopus and Science Direct databases. The keywords ‘human papillomavirus’ OR ‘HPV’ AND ‘vaccination’ AND ‘quality improvement’ were used.
Eligible studies were included if they met the inclusion criteria, i.e., published quality improvement (QI) reports aiming to boost HPV vaccination rate among adolescents 10 to 18 years old, with the primary outcome analyzed statistically, published between 1 January 2019 and 25 March 2023. Review articles, letters to the editor, comments, and case reports were excluded. The references of the included articles were also checked to ensure inclusivity. Only articles published in the English language were included.
2.2. Data collection
A single author [K.K.] independently collected and collated search results based on predefined search strategies. Pooled abstracts from the citations were combined using Mendeley Desktop Version 1.19.8 and independently examined by two authors for article selection [K.Y.L. & N.F.M.] for final analysis. Discrepancies were resolved by the third author [O.W.]. Final articles included for analysis were reviewed and analyzed by a single author whose primary interest lies in quality improvement methodology [K.K.].
2.3. Study registration
The study protocol was registered with the National Medical Research Register of the Ministry of Health Malaysia (NMRR ID-23-01062-XDU). The study was exempted from institutional review board based on the Malaysian National Institutes of Health Guidelines for Conducting Research in Ministry of Health (MOH) Institutions & Facilities 3rd ed. (2021).
3. Results
3.1. Search results
The article selection process followed the recommendation by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Figure 1).
Figure 1.
PRISMA flowchart for study selection.
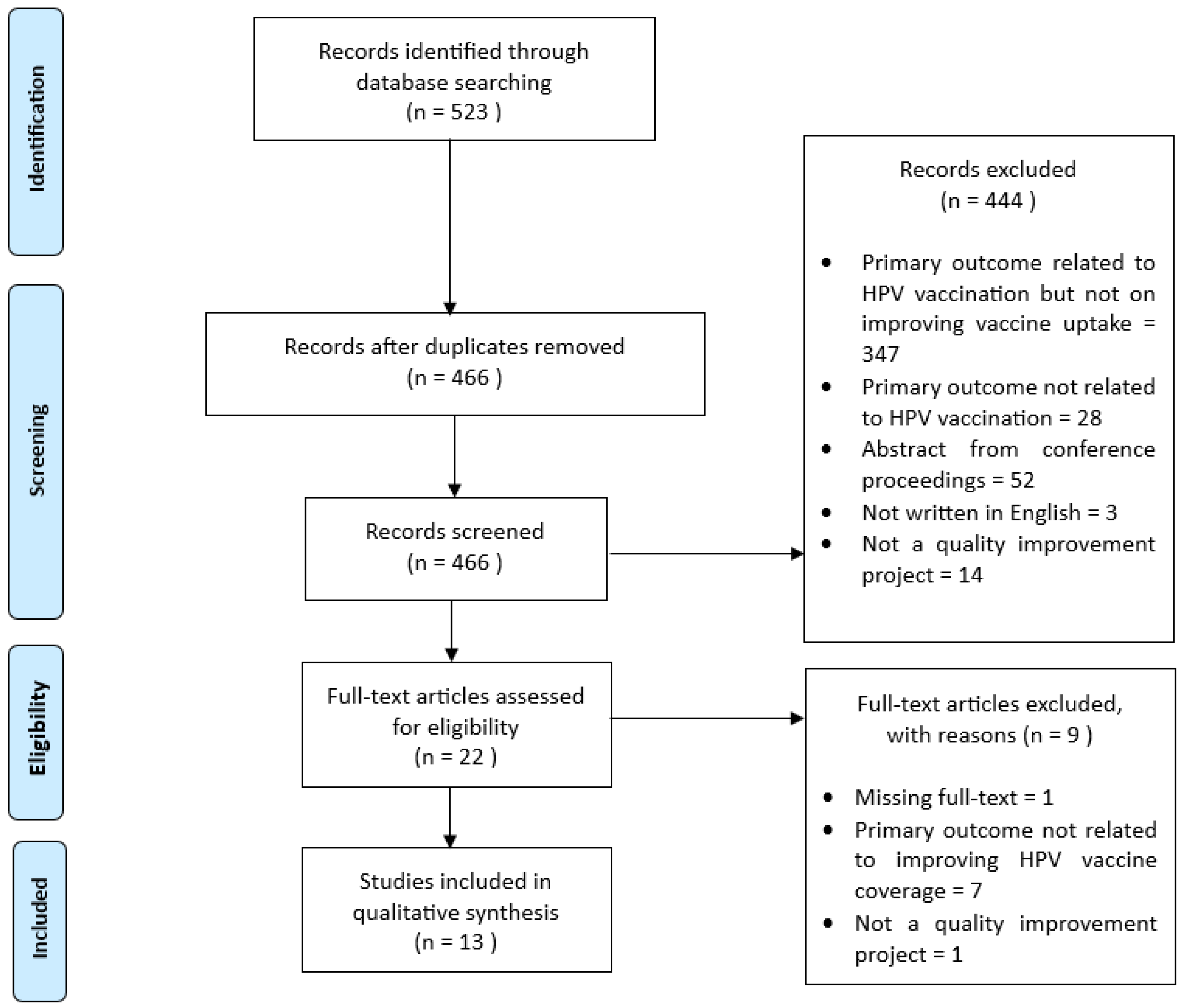
Table 1 presents the main characteristics of the 13 quality improvement reports included in the systematic review. Three key intervention targets emerged as the QI approach towards improving HPV vaccination rates among adolescents, i.e., from the perspectives of the healthcare provider, the adolescents and/or the caregivers, as well as the refinement of the local healthcare system. .

Table 1.
Summary of studies included in the final analysis.
| No. | First author, year | Intervention focus group | Mode of intervention | Primary outcome | Results |
|---|---|---|---|---|---|
| 1 | Berstein, 2022 [10] | System/policy | Inclusion of HPV vaccination with other scheduled vaccines for adolescents | HPV vaccines rates among 11-12 years-old teens | HPV vaccination rate increased from 17.8% to 63.6% |
| Patients | Parents were sent pre-visit email - contains vaccine information prior to annual healthcare visit |
||||
| HCP | Initiatives to improve provider communication skills | ||||
| 2 | Davis, 2022 [1] | HCP | Educational intervention |
HPV vaccination rates in children 11−12 years old |
|
| 3 | Gilkey, 2019 [11] | HCP | An in-clinic training session (include instruction and video on effective communication) | HPV vaccination coverage among patients aged 12 to 14 years |
HPV vaccination coverage increased in the QI arm by 8.6% |
| 4 | Mackey, 2019 [12] | HCP | Reminder system for both physicians and patients | HPV vaccination coverage among patients aged 11 to 12 | The immunization rate (for the first injection) was significantly greater than baseline |
| Patients | Reminder mails to caregivers of patients aged 11-12 years | ||||
| 5 | Mathur, 2019 [13] | HCP | Four 1-hour webinars highlighting on effective communication with parents regarding the HPV vaccine. |
HPV vaccination coverage (dose 1) for all 11- and 12-year-old | Initiation of HPV vaccination increased in all participating practices (from 56.4% to 71.2%) |
| 6 | McGaffey, 2019 [14] | HCP | Periodic training on presumptive approach in HPV vaccine recommendation | HPV vaccination rate among 9-26 years-old patients (both male and female) |
|
| Patients |
|
||||
| System/policy |
|
||||
| 7 | Nissen, 2019 [15] | Patients | Implement reminder and recall system for eligible patients who were unvaccinated or with incomplete vaccination | The rate of HPV vaccine administration |
|
| HCP |
|
||||
| 8 | Oliver, 2020 [16] | HCP |
|
Impact on HPV immunization rates (HPV initiation, series completion, and missed opportunities) |
|
| 9 | Perkins, 2021 [17] | HCP |
|
Adolescent vaccination rates among adolescents who turned 13 years |
|
| 10 | Singh, 2022 [18] | Patients |
|
HPV vaccination rates among young adults |
The vaccination rate among patients who were seen in person at the clinic improved from 2.5% (1 of 40) to 46.6% (21 of 45). |
| HCP |
|
||||
| 11 | Smajlovic, 2023 [19] | Patients |
|
HPV-vaccination series completion rate to 70% among the 13-year-old patient population | The overall HPV vaccination series completion rates in increased from 27% to 65% |
| HCP | QI team provided feedback via email to providers on a 6-monthly basis to a year on the monitored HPV vaccine completion rates among 13-year-old adolescents | ||||
| System | A licensed professional-initiated protocol (LPIP) dedicated for nursing staff is triggered when an eligible patient is scheduled for a visit | ||||
| 12 | Wallace-Brodeur, 2020 [20] | HCP | Training sessions on effective recommendation for HPV vaccine, strategies to reduce MOs, and techniques on motivational interviewing |
Reduction in MOs (defined as any visit that a patient did not receive the vaccination dose despite being eligible) | LHDs reduced MOs for HPV vaccination by 25.3% |
| 13 | Zorn, 2023 [21] | HCP | Provider and staff training, with peer-to-peer coaching by QI champion | HPV initiation at age 9 and series completion rates |
|
| Setting/system | Electronic medical records support | ||||
| Patients |
|
Abbreviations: ACS=American Cancer Society; HCP=Healthcare professional; HPV=Human papillomavirus; LHDs=Local health departments; MO=Missed opportunities; PP=Percentage points; QI=Quality improvement.
3.2. Healthcare provider-targeted empowerment approach
From the review, improving the knowledge and communication skills of healthcare providers (HCP) through education sessions was the most common QI initiative undertaken to empower the HCPs and subsequently, boost the HPV vaccination rate in healthcare settings [1,10,11,12,13,14,15,16,17,18,19,20,21]. The topics covered during these sessions encompass global and national burden of HPV-related diseases, updated HPV vaccination schedule, and ways to successfully communicate with parents and adolescents about HPV vaccine.
In addition, for the QI activities to be successful, HCPs should have access to reliable resources on ways to improve HPV vaccination among adolescents in the primary care settings. More importantly, these resources should be developed based on the recommendations of key stakeholders such as the CDC, American Academy of Pediatrics (AAP), Henry F. Kaiser Family Foundation, and etc. [22]. Furthermore, all materials should be easily accessible through websites and prepared in interactive formats such as videos and articles. User-friendliness of these materials can enhance the providers’ knowledge on HPV vaccination, aid the discussion with parents and/or adolescents, as well as provide strategies to deal with difficult parents and/or adolescents [22].
As for the QI coaches, besides playing an important role in educating the participants, they should also be actively involved in the project to continually motivate and provide feedback on site performance to the team members. A dynamic team is vital to sustain the momentum and continuum of the QI project to achieve the desired objectives [22]. For example, a QI project involving 34 pediatricians designed an ‘ECHO’ program whereby HCPs convened in a monthly one-hour video conferencing with the QI project leaders for a total of nine months. The session started with a 15-20 minutes educational lesson covering topics related to HPV vaccination for the HCPs. The QI project leaders then reinforce the implementation of the evidence-based interventions. This was followed by interactive sessions involving simulation of patient encounters as well as sharing of experiences and ideas to boost HPV vaccination among the providers [16].
3.3. Reshaping adolescents, parents, and/or caregivers’ perception on HPV vaccination
It is well-established that risk communication and community engagement are fundamental to achieve high public acceptance and uptake of vaccination. This can be achieved by empowering public with adequate knowledge, awareness, and confidence through effective communication and strategic social media approach.
In this review, one of the QI strategies employed to prime the parents and/or caregivers in preparation for their child’s vaccination was to send a pre-visit email with information about HPV vaccine prior to their child’s scheduled visit [12,23]. Some QI initiatives even took a step further by discussing about HPV vaccination earlier on (by the age of 9) [19] and created a client reminder system through phone calls or text messages [24,25]. Another QI project established a recall system to trace patients who did not turn up at the vaccination appointment [26].
Furthermore, social events to improve awareness and health literacy among the public were also organized, for example, the HPV vaccination poster contest and ‘HPV T-shirt Fridays’ [24]. By providing the right information to the public via reliable and easily accessible resources, the public can be assured of the safety and efficacy of the vaccine. This include placing HPV vaccination-related posters in high traffic clinic areas as well as distributing HPV educational brochures to eligible patients during clinic visits [27].
3.4. Redesigning healthcare system and policy changes
Last but not least, effective healthcare policy changes may also bolster public health initiatives in improving HPV vaccination uptake. For example, a QI project conducted in a private pediatric practice in suburban New England found that the inclusion of HPV vaccination along with other vaccines contributed to an increase in HPV vaccination rates among adolescents from 17.8% to 63.6% in three months [23]. Several other strategies included activating a licensed professional initiated protocol (LPIP) (led by nursing staff) when an eligible patient for vaccination is scheduled for a visit [19], daily review of patients with incomplete vaccinations for them to be individually traced [24], and an electronic medical record to support the tracking of patients eligible for vaccination [27].
4. Discussion
This review summarizes various QI methodologies used as evidence-based strategies in enhancing the uptake of HPV vaccination among adolescents. While most of the QI projects have shown a certain level of success, the implementation of these strategies in the real-world practice required careful planning and execution to ensure the feasibility and impact of the strategies.
Based on this review, most of the implemented interventions to improve HPV vaccination uptake and completion focused on advancing HCPs’ knowledge so that they can educate the patients and parents/ caregivers. Additionally, the important role of HCPs in providing effective communication is further highlighted in a study in which as high as 80% of parents agreed that the provider’s recommendation during the clinic session was the main reason for them to approve their children’s vaccination uptake [23]. Providers practicing a presumptive style over a conversational style were found to be associated with a higher rate of vaccine acceptance [1,14]. Hence, a standardized communication intervention offered as in-person sessions with free and readily available resources will enable the HCPs to successfully deliver consistent and reliable messages to patients. Improvement in vaccine uptake will only be evident once HCPs are able to communicate with their patients with confidence.
Despite HCPs being the most frequently targeted intervention group, a study conducted at three family practice clinics in Florida, US to evaluate the use of a provider-based intervention (email, resource packets, education) showed only a slight improvement of HPV vaccination rates [5]. Therefore, besides HCPs at the clinic level, change agents at multiple points in the wider healthcare systems also need to be involved for favorable decision-making and outcome of vaccination uptake.
Knowledge empowers adolescents (and their caregivers) to make proactive and appropriate decisions regarding the HPV vaccination. Hence, transparency in providing information regarding vaccine safety will alleviate fears and misperceptions and guide their decision to vaccinate [11,28]. Patient empowerment can also be achieved by partnering with neighborhood community centers or regional foundation to organize health literacy program [14].
In comparison, some of the less commonly implemented interventions often require systematic changes, such as the establishment of an integrated patient tracing system and scheduled follow-ups after missed appointments, facilitated through electronic health records. These multi-mode reminders via regular mails, telephone calls, e-mail, and text messages can be used to reach the young adult population [26]. The same paper found that staff calls made to younger patients aged 11 to 17 years yielded up to 45% attendance for vaccination as compared to just 6% among those 18–26-year-old. Similarly, the distribution of educational brochures via mail followed by a telephone discussion was also less successful at increasing HPV vaccination rates among individuals 18 to 26 years old with incomplete vaccination [18]. Therefore, while more emphasis are given to infrastructures that can improve patient recall and tracking, they should be targeted at the right age group to optimize the outcomes [29,30].
Additionally, a study found that including HPV vaccination together with other vaccinations during adolescence (Meningococcal and Tdap) also improved the overall vaccination rate [17]. Likewise, Singh (2022) reported that most of the HPV vaccination was performed during acute appointments rather than scheduled ones [18]. Hence, a system alert to trigger the arrival of any eligible patients for any type of consultations in the clinic will be beneficial to avoid missed opportunities.
Apart from these evidence-based QI approaches, potential cultural factors may also influence the decision to vaccinate. A relevant study across 12 clinics in Ohio, US found that Latino children recorded the highest HPV vaccination completion rate (80%) while White children showed the lowest rate at 64% [19]. However, any observed ethnic disparity in study outcomes should be interpreted with caution as it might be affected by the demographic distribution of the study population of interest because the income status of the neighborhood and the proportion of publicly-insured patients would affect the access to medical treatment [31,32]. Therefore, when designing and implementing any QI strategies, local cultural influence must be taken into account to ensure the highest program outreach, especially in multiethnic, multicultural, and multilingual regions.
The findings from our review highlighted that QI initiatives for the improvement of HPV vaccine uptake among adolescents require holistic efforts that incorporate improvement in any given measure to overcome conventional practices [14]. Due attention ought to be paid to capture, update the process and methods of improvements, define individual roles, and learnings points from the project. The procedures and practices developed during the QI project should also be integrated as part of the institutional practice to ensure sustainability. Lastly, future QI reports should adhere to the SQUIRE guidelines in an effort to strengthen the evidence for improvement in healthcare [33].
5. Conclusion
Multilevel interventions that focus not only on provider training, but also incorporates local policy and system refinements can substantially improve HPV vaccination uptake. Provider-based QI interventions are instrumental in improving the communication between clinicians and their patients with the aim of straightening HPV vaccine awareness and uptake. However, the implementation of these QI strategies in the real-world can be challenging due to limited resources and demanding commitment. Therefore, a consistent and continuous HPV vaccination communication, supplemented by low-cost sensory rewards, as well as dynamic engagement between clinicians, supporting clinical staff, and the community are needed to ensure a high HPV vaccination uptake and completion among adolescents and young adults.
Author Contributions
Conceptualization, K.K., K.Y.L. and O.W.; methodology, K.K. and K.Y.L.; selection of articles, K.Y.L. and N.F.M.; formal analysis, K.K.; writing—original draft preparation, K.K., K.Y.L. and N.F.M.; writing—review and editing, K.Y.L and O.W.; supervision, O.W. All authors have read and agreed to the published version of the manuscript.
Funding Information
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Acknowledgments
The authors would like to thank the Director General of Health Malaysia for his permission to publish the paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Davis, K.R.; Norman, S.L.; Olson, B.G.; Demirel, S.; Taha, A.A. A Clinical Educational Intervention to Increase HPV Vaccination Rates Among Pediatric Patients Through Enhanced Recommendations. J. Pediatr. Heal. Care 2022, 36, 589–597. [Google Scholar] [CrossRef] [PubMed]
- CDC HPV Vaccination Recommendations. Centers Dis. Control Prev. 2021, 1–2.
- Wallace-Brodeur, R.; Li, R.; Davis, W.; Humiston, S.; Albertin, C.; Szilagyi, P.G.; Rand, C.M. A Quality Improvement Collaborative to Increase Human Papillomavirus Vaccination Rates in Local Health Department Clinics. Prev. Med. (Baltim). 2020, 139, 106235. [Google Scholar] [CrossRef]
- Pingali, C.; Yankey, D.; Elam-Evans, L.D.; Markowitz, L.E.; Williams, C.L.; Fredua, B.; McNamara, L.A.; Stokley, S.; Singleton, J.A. National, Regional, State, and Selected Local Area Vaccination Coverage Among Adolescents Aged 13-17 Years — United States, 2020. MMWR Recomm. Reports 2021, 70, 1184–1190. [Google Scholar] [CrossRef] [PubMed]
- Austin, B.; Morgan, H. Improving Human Papillomavirus Vaccine Uptake in the Family Practice Setting. J. Nurse Pract. 2019, 15, e123–e125. [Google Scholar] [CrossRef]
- Mitchell, K.; Saraiya, M.; Bhatt, A. Increasing HPV Vaccination Rates Through National Provider Partnerships. J. Women’s Heal. 2019, 28, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Malaysia Action Plan - Towards the Elimination of Cervical Cancer in Malaysia 2021-2030; Abdul Samad, S., Ed.; 1st ed.; Ministry of Health, Malaysia: Putrajaya, 2021. Ministry of Health, Malaysia: Putrajaya.
- Gilkey, M.B.; Bednarczyk, R.A.; Gerend, M.A.; Kornides, M.L.; Perkins, R.B.; Saslow, D.; Sienko, J.; Zimet, G.D.; Brewer, N.T. Getting Human Papillomavirus Vaccination Back on Track: Protecting Our National Investment in Human Papillomavirus Vaccination in the COVID-19 Era. J. Adolesc. Heal. 2020, 67, 633–634. [Google Scholar] [CrossRef]
- Schneiter, M.; Rositch, A.; Levinson, K.; Stone, R.; Fader, A.; Ferriss, J.; Wethington, S.; Beavis, A. The Gynecologic Oncologist as the HPV Champion: Missed Opportunities for Cancer Prevention. Gynecol. Oncol. 2021, 162, S292–S293. [Google Scholar] [CrossRef]
- Bernstein, T.A.; Broome, M.; Millman, J.; Epstein, J.; Derouin, A. Promoting Strategies to Increase HPV Vaccination in the Pediatric Primary Care Setting. J. Pediatr. Heal. Care 2022, 36, e36–e41. [Google Scholar] [CrossRef]
- Gilkey, M.B.; Parks, M.J.; Margolis, M.A.; McRee, A.-L.; Terk, J. V Implementing Evidence-Based Strategies to Improve HPV Vaccine Delivery. Pediatrics 2019, 144. [Google Scholar] [CrossRef]
- Mackey, J.K.; Thompson, K.; Abdulwahab, A.; Huntington, M.K. A Simple Intervention to Increase Human Papillomavirus Vaccination in a Family Medicine Practice. S. D. Med. 2019, 72, 438–441. [Google Scholar] [PubMed]
- Mathur, M.; Campbell, S. Statewide Pediatric Quality Improvement Collaborative for HPV Vaccine Initiation. Wis. Med. J. 2019, 118, 42–43. [Google Scholar]
- McGaffey, A.; Lombardo, N.P.; Lamberton, N.; Klatt, P.; Siegel, J.; Middleton, D.B.; Hughes, K.; Susick, M.; Lin, C.J.; Nowalk, M.P. A “Sense”-Ational HPV Vaccination Quality Improvement Project in a Family Medicine Residency Practice. J. Natl. Med. Assoc. 2019, 111, 588–599. [Google Scholar] [CrossRef] [PubMed]
- Nissen, M.; Kerkvliet, J.L.; Polkinghorn, A.; Pugsley, L. Increasing Rates of Human Pipillomavirus Vaccination in Family Practice: A Quality Improvement Project. S. D. Med. 2019, 72, 354–360. [Google Scholar] [PubMed]
- Oliver, K.; McCorkell, C.; Pister, I.; Majid, N.; Benkel, D.H.; Zucker, J.R. Improving HPV Vaccine Delivery at School-Based Health Centers. Hum. Vaccines Immunother. 2019, 15, 1870–1877. [Google Scholar] [CrossRef]
- Perkins, R.B.; Foley, S.; Hassan, A.; Jansen, E.; Preiss, S.; Isher-Witt, J.; Fisher-Borne, M. Impact of a Multilevel Quality Improvement Intervention Using National Partnerships on Human Papillomavirus Vaccination Rates. Acad. Pediatr. 2021, 21, 1134–1141. [Google Scholar] [CrossRef]
- Singh, C. Increasing Knowledge of Human Papillomavirus Among Young Adults. J. Nurse Pract. 2022, 18, 618–621. [Google Scholar] [CrossRef]
- Smajlovic, A.; Toth, C.D. Quality Improvement Project to Increase Human Papillomavirus Two-Dose Vaccine Series Completion by 13 Years in Pediatric Primary Care Clinics. J. Adolesc. Heal. 2023. [Google Scholar] [CrossRef]
- Wallace-Brodeur, R.; Li, R.; Davis, W.; Humiston, S.; Albertin, C.; Szilagyi, P.G.; Rand, C.M. A Quality Improvement Collaborative to Increase Human Papillomavirus Vaccination Rates in Local Health Department Clinics. Prev. Med. (Baltim). 2020, 139, 106235. [Google Scholar] [CrossRef]
- Zorn, S.; Darville - Sanders, G.; Vu, T.; Carter, A.; Treend, K.; Raunio, C.; Vasavada, A. Multi-Level Quality Improvement Strategies to Optimize HPV Vaccination Starting at the 9-Year Well Child Visit: Success Stories from Two Private Pediatric Clinics. Hum. Vaccines Immunother. 2023, 19, 1–11. [Google Scholar] [CrossRef]
- Austin, B.; Morgan, H. Improving Human Papillomavirus Vaccine Uptake in the Family Practice Setting. J. Nurse Pract. 2019, 15, e123–e125. [Google Scholar] [CrossRef]
- Bernstein, T.A.; Broome, M.; Millman, J.; Epstein, J.; Derouin, A. Promoting Strategies to Increase HPV Vaccination in the Pediatric Primary Care Setting. J. Pediatr. Heal. Care 2022, 36, e36–e41. [Google Scholar] [CrossRef] [PubMed]
- McGaffey, A.; Lombardo, N.P.; Lamberton, N.; Klatt, P.; Siegel, J.; Middleton, D.B.; Hughes, K.; Susick, M.; Lin, C.J.; Nowalk, M.P. A “Sense”-Ational HPV Vaccination Quality Improvement Project in a Family Medicine Residency Practice. J. Natl. Med. Assoc. 2019, 111, 588–599. [Google Scholar] [CrossRef] [PubMed]
- Singh, C. Increasing Knowledge of Human Papillomavirus Among Young Adults. J. Nurse Pract. 2022, 18, 618–621. [Google Scholar] [CrossRef]
- Nissen, M.; Kerkvliet, J.L.; Polkinghorn, A.; Pugsley, L. Increasing Rates of Human Pipillomavirus Vaccination in Family Practice: A Quality Improvement Project. S. D. Med. 2019, 72, 354–360. [Google Scholar]
- Zorn, S.; Darville - Sanders, G.; Vu, T.; Carter, A.; Treend, K.; Raunio, C.; Vasavada, A. Multi-Level Quality Improvement Strategies to Optimize HPV Vaccination Starting at the 9-Year Well Child Visit: Success Stories from Two Private Pediatric Clinics. Hum. Vaccines Immunother. 2023. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.R.; Norman, S.L.; Olson, B.G.; Demirel, S.; Taha, A.A. A Clinical Educational Intervention to Increase HPV Vaccination Rates Among Pediatric Patients Through Enhanced Recommendations. J. Pediatr. Heal. Care 2022, 36, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Handayani, P.W.; Hidayanto, A.N.; Budi, I. User Acceptance Factors of Hospital Information Systems and Related Technologies: Systematic Review. Informatics Heal. Soc. Care 2018, 43, 401–426. [Google Scholar] [CrossRef]
- Askelson, N.M.; Ryan, G.; Seegmiller, L.; Pieper, F.; Kintigh, B.; Callaghan, D. Implementation Challenges and Opportunities Related to HPV Vaccination Quality Improvement in Primary Care Clinics in a Rural State. 2019, 44, 790–795. [Google Scholar] [CrossRef]
- Perkins, R.B.; Brogly, S.B.; Adams, W.G.; Freund, K.M. Correlates of Human Papillomavirus Vaccination Rates in Low-Income, Minority Adolescents: A Multicenter Study. J. Women’s Heal. 2012, 21, 813–820. [Google Scholar] [CrossRef]
- Hirth, J. Disparities in HPV Vaccination Rates and HPV Prevalence in the United States: A Review of the Literature. Hum. Vaccines Immunother. 2019, 15, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Davidoff, F.; Batalden, P.; Stevens, D.; Ogrinc, G.; Mooney, S. Publication Guidelines for Quality Improvement in Health Care: Evolution of the SQUIRE Project. In Proceedings of the Quality and Safety in Health Care; BMJ Publishing Group Ltd, October 1 2008; Vol. 17, pp. i3–i9.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



