
Submitted:
21 May 2023
Posted:
29 May 2023
You are already at the latest version
Abstract
Poor medication adherence among older adults is a widespread problem worldwide. As the population ages, the design of smartphone medication management apps is critical to improving medication adherence among older adults. Taking the design of an elderly medication reminder APP as an example, this study proposes a sustainable design research method that integrates the KANO model, Analytic Hierarchy Process (AHP), Quality Function Deployment (QFD), and PUGH decision matrix. The method collects user demands through in-depth interviews, and applies the KANO model to classify these demands. The hierarchical structure of user needs is established by using AHP, and the priority is sorted according to the weight and importance determined by the judgment matrix. QFD is used to translate user needs into design requirements, and the house of quality matrix identifies key design requirements. Finally, design alternatives are evaluated using Pugh's concept selection method. The results of this study demonstrate that the integration of KANO-AHP-QFD-PUGH can be effective as a sustainable optimal design approach for the user experience of a medication reminder application for the elderly. This integrated method not only facilitates innovative optimization and sustainability of application design methods but also provides valuable theoretical and practical insights for future drug-assisted design for elderly users.
Keywords:
elderly medication reminder application
; Kano model
; AHP
; QFD
; PUGH decision matrix
1. Introduction
With the increasingly apparent trend of global population aging, the proportion of elderly people is continuously rising[1]. As elderly chronic disease patients need to take multiple medications for a long period, taking medication on time and regularly is crucial to improving their health status. However, as the elderly age, their various physical and cognitive abilities decline to varying degrees. Common problems include missing doses, taking incorrect doses, and having a biased understanding of their condition, resulting in medication cessation or reduction[2] . These problems can lead to higher readmission and mortality rates. To improve medication adherence in the elderly and help them address the challenges they may face, such as taking medication at the correct time, understanding the efficacy and side effects of medication, or organizing their medication list, digital interventions have become increasingly important. Mobile-based digital tools related to health can activate reminders for medication, maintain medication history, and furnish medication information indicating the capacity to facilitate self-care for chronic illnesses and enhance medication adherence[3] .
Currently, many scholars have developed and tested medication management applications, and research on medication reminder apps for elderly mainly focuses on two aspects. First, the development and functional research of medication reminder apps that explore the application functions, interface, and preferences of elderly users. Secondly, research on the usability of existing medication reminder apps for the elderly. Multiple test results show that although these reminder apps can significantly improve patient medication adherence, they are not user-friendly for elderly patients. Many applications have problems such as complex interface interactions and difficult operations, and the design process does not fully consider the abilities, needs, and limitations of the elderly population[3], resulting in poor usability and low satisfaction for elderly users. Although many scholars have conducted extensive research on the needs of elderly users, the usability test results of applications are not satisfactory. There is a gap between user needs and design results. Therefore, it is necessary to find a suitable design method to help designers better design the apps in the process of translating user needs into design requirements.
Therefore, this paper proposes an integrated design optimization method, combining KANO-AHP-QFD-PUGH, aiming to help reduce the gap between users and products or services from a design perspective. Taking the design of a medication reminder app for the elderly as a research case, with Chinese elderly users as the target research population, this study validates the feasibility of the proposed design method. It delves into the authentic needs of elderly users and accurately translates those needs into design requirements. By selecting the best design solution, the study aims to enhance the satisfaction and efficiency of elderly users with such applications, ultimately addressing the issue of poor medication adherence among the elderly.
The subsequent organization of this paper is as follows: Section 2 provides an overview of the theoretical framework, deficiencies in previous studies, and areas that necessitate improvement. Section 3 outlines the research methodologies and procedures employed in this study. Section 4 depicts a case study on medication management applications for elderly users. Section 5 analyzes and discusses the case study findings and offers pertinent recommendations for enhancing the user experience. Lastly, Section 6 summarizes the study's conclusions, significance, limitations, and prospective research directions.
2. Literature Review
2.1. Theoretical Background
The QFD model is a planning tool proposed by Akao in 1966. Through qualitative and quantitative analysis, user demands can be effectively transformed into functional attributes of products[4]. The fundamental principle of this approach is to employ the house of the quality matrix, which can enhance the primary design criteria of users to the maximum extent using data analysis and processing[5]. At present, as a research framework, QFD is often used in combination with other design methods to optimize design schemes, forming a complementary comprehensive theory:
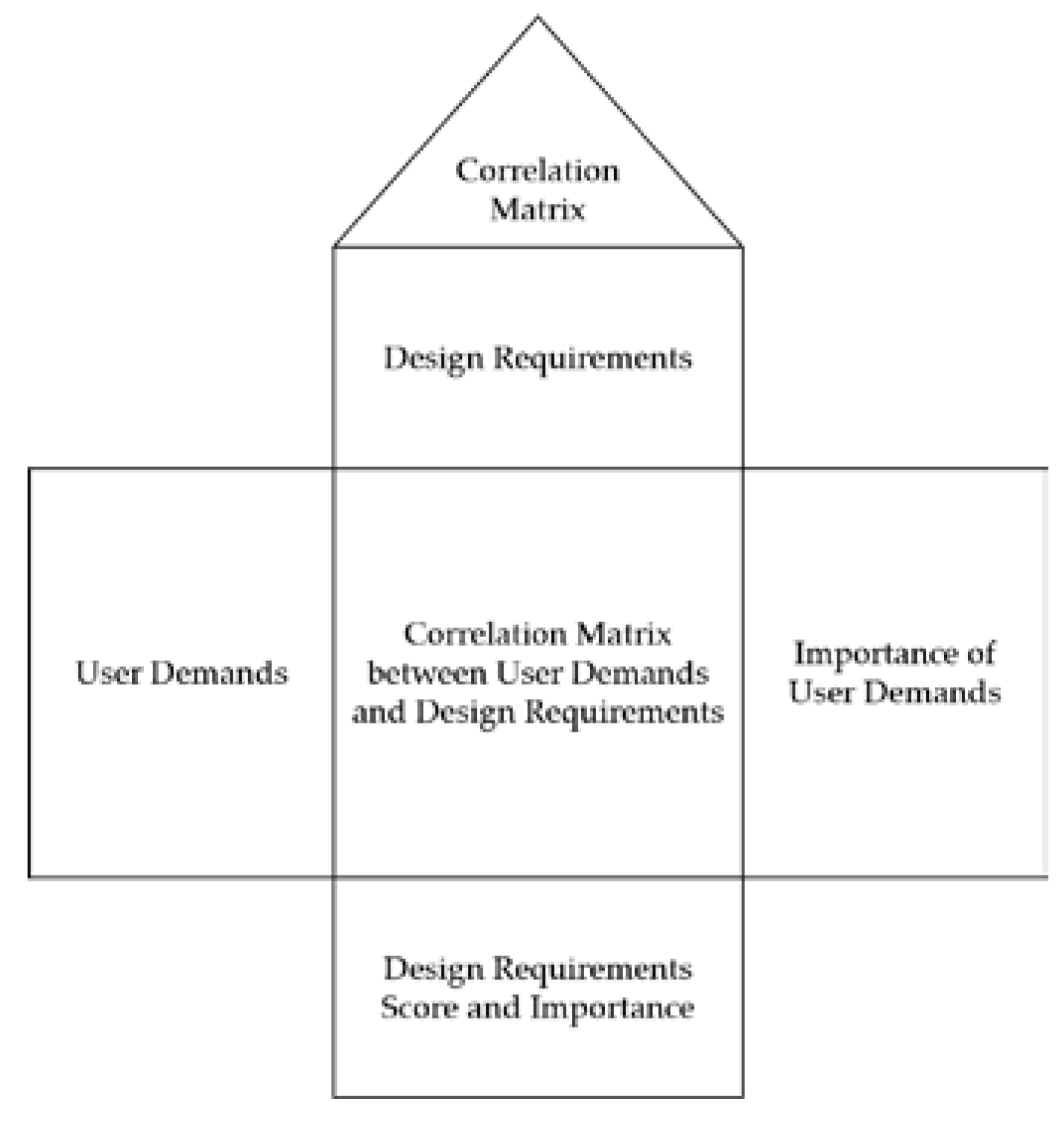
Figure 1.
House of Quality Model.
The Kano model is an effective approach for categorizing and ranking user demands, which is grounded on evaluating the influence of user needs on user contentment[6]. It highlights the non-linear correlation between product performance and user satisfaction[7]. It divides user needs into essential elements (M), expectation factor (O), attractive factor (A), indifference factor (I), and reverse factor (Q), understanding the user's demand attributes can help designers fully understand user real needs, so many scholars choose to use the Kano model[8]. The amalgamation of qualitative and quantitative research, utilizing the QFD model, has evolved into a sophisticated integrated model over time[9]. For example, Yongfeng Li and others combined QFD with the Kano model to develop a smartphone APP suitable for the elderly[9]; Kim and others used Kano-QFD to develop the shape design of medical service robots[10]; Shwetank Avikal et al. combined QFD with fuzzy kano models for the classification of SUV car appearance aesthetic attributes[5]; Xiaoli Wu et al. proposed A Kano Model, QFD and Functional Analysis SystemTechnology (FAST) Approach for Better Stroller Design[4]; Akshat Rampal et al. Importing Kano into QFD to Improve User Satisfaction with Self-Driving Electric Vehicles[12] and Jianhua Lyu et al.used this model to develop an open office wooden chair[13]. The Kano-QFD model finds applications in numerous product designs, services, satisfaction improvements, health care, and communication technology equipment improvement, etc., but when they are used alone, they cannot determine the priority of user satisfaction ranking, so they need to be combined with other Standard decision-making methods are combined to determine which design features have the greater impact on user satisfaction[14].
The Analytic Hierarchy Process (AHP) divides complex decision-making problems into several simple sub-problems at one level by using a tree-like hierarchical structure, and each sub-problem can be analyzed independently[15]. Upon constructing the hierarchy, each component's relative importance is assigned a weight value, and a pairwise comparison matrix is established to determine the eigenvector and eigenvalue. The eigenvector indicates the priority of each component at each level and can offer decision-makers adequate information for making informed decisions. Additionally, this can assist in organizing the selection criteria, analyzing the weights, and mitigating the potential risks associated with decision-making errors[16].
The application of AHP is very wide, it covers almost all areas of decision-making problems, the usability of integrating AHP with QFD, kano model, and other research methods has been confirmed in many studies, and it can solve the shortcomings of a single method, such as Rafat Mahmud Hridoy et al. used the joint method of AHP, Kano model and QFD to try to improve the design of tractor seats in Bangladesh[17]; Angie Wu et al. Integrating AHP, QFD and TRIZ Models to Innovate the Design of Scenic Mobility Vehicles[18]; Byanca Porto de Lima et al. integrate the practical application of AHP, Q,FD and PROMETHEE methods to the problem of packaging design choice in hesitant fuzzy environments[19].
The PUGH concept selection method is a qualitative decision analysis tool proposed by Stuart Pugh in 1980[20]. According to the principle of product concept selection, it is converted into a matrix method for evaluating concept screening, especially in the concept design stage, which can scientifically analyze the data and reduce the personal influence of subjective judgments on the results, using a standard score to help the designer determine the most preferred of the potential solutions[21]. In 1992, American scholars introduced the PUGH research method into QFD, which triggered more in-depth follow-up research[22]. Yangjing (2016) proposed an integrated AHP-PUGH evaluation model and built a comprehensive product evaluation system for conceptual design[23]. Pandit (2020) et al. combined PUGH concept selection with QFD to select the most suitable trolley design[24]; Tianlu Zhu (2022) et al. conducted research on the design of surgical aids based on AHP, QFD, and PUGH decision matrices[22]; Yongchuan Li et al. took the design of smart refrigerators for the elderly as an example, and integrated the KANO-QFD-PUGH model to optimize the sustainable user experience design of smart home products for the elderly[5]. According to the above review, the four methods of Kano, AHP, QFD, and PUGH have been combined and used in various fields, but a perfect and unified research paradigm has not yet been formed, and there is still a certain research space, and value.
2.1. Current Status of Research on the Application of Medication Reminder in the elderly
In the past few years, improving the medication compliance of the elderly has become an important topic in the world. Judging from the current research status of medication reminder applications, relevant discussions mainly focus on two aspects: one is the application of medication reminder APPs. Development and functional research; the second is to conduct usability testing and evaluation of the existing medication reminder APP.
Flávio Ferreira et al. and Anto´nio Teixeira et al. both used a short-term iterative method to develop the "Medication Assistant" application centered on the elderly and interaction design, which includes scenarios and Target definition, requirements engineering, design, prototyping and evaluation of target users, by continuously allowing users to test the prototype, discovering advantages and disadvantages and suggestions for improvement, to provide a reliable basis for further improvement and development[25].
Due to the continuous acceleration of global aging, the elderly population, as a special group, has greater challenges in medicine use[26]. Therefore, many scholars have begun to use the elderly as target users to research the functions, interfaces, and preferences of applications. S. Lakey et al. assessed the current use, knowledge, and preferences of medication management tools and supports among 152 older adults[27]; Leah M Haverhals et al. (2011) learned about Regarding Personal Health Apps (PHAs) addressing medication self-administration issues faced by older adults and caregivers, the results were shown to provide links to authoritative and reliable information on side effects, drug interactions, and other medication-related issues in a clear, concise manner, and Ease of navigation[28]; ANDREA M. RUSSELL et al. (2018) conducted an experimental discussion on the functional preferences of mobile applications for medicine self-management in the elderly, and the results showed that drug lists, mutual warnings between drugs, medication reminders, and records were considered the most needed functions[29].
This paper studies the usability testing of medication reminder applications mainly focusing on the elderly user group. Several studies have shown that current medication management applications are difficult for elderly users to use[2]. Kelly Anne Grindrod et al. The usability evaluation of mobile drug management applications shows that the two applications with simple interfaces are more popular among the elderly[30]; Rachel E. Stuck et al. A comprehensive evaluation of Medisafe showed that its design did not consider the needs, abilities, and limitations of the elderly. The results revealed three main problems: navigation difficulties, poor visibility, and lack of transparency[2]; Jaqueline Donin Noleto et al. compared the three models of Medication reminder apps (Medisafe, My Therapy, and Cuco Health) conducted a senior usability test of the interface to assess the friendliness of the application for the elderly, and the results showed that these applications lacked design for the elderly, and the general interface issues need to be improved[31]; Yongjing Ping et al. conducted a study on the prevalence and correlation of the usage intention of the elderly medication reminder application and found that the main reason for the low usage intention of the elderly is that the interface of the application is complex, user-unfriendly and dense with instructions. This may make it difficult for older adults with less education to register and navigate the app[3]. An assessment of applications showcasing drug listings revealed that certain apps exhibited subpar interfaces and lacked sufficient instructions on recording medication history and setting medication reminders[32]. Users also expressed concerns regarding the security of their personal information.
3. Materials and Methods
Our research methods consisted of 5 steps, as shown in Figure 3.
3.1. STEP1: Kano Model Collect
The method for solving the non-linear relationship between meeting customer needs (Figure 2) and overall customer satisfaction using Kano consists of the following three steps: Kano questionnaire, Kano evaluation table, and Kano category results[33].
After identifying user demands, develop structured questionnaires. According to the analysis of user demands, the Kano questionnaire is made, and both positive and negative questions are raised for a single functional demand (provide this function/not provide this function)[34], as shown in Table 2:
The demands are categorized into five items: "like", "should be", "neutral", "tolerable", and "dislike" (as shown in the Table 1). The research results are classified and counted according to the Kano evaluation table (as shown in the Table 3) to obtain the demand attributes[34]. The demand categories are determined and filtered into must-have, expected, and attractive user demands based on the maximum frequency of their corresponding categories A, O, M, I, and R while removing indifferent and reverse attributes[35].

Table 1.
Kano questionnaire
| Function | Like | Deserved | Neutral | Endurable | Dislike |
|---|---|---|---|---|---|
| Provide | √ | ||||
| Don’t provide | √ |
Table 2.
Questionnaire score table
| Function | Like | Deserved | Neutral | Endurable | Dislike |
|---|---|---|---|---|---|
| Provide | 5 | 4 | 3 | 2 | 1 |
| Don’t provide | 1 | 2 | 3 | 4 | 5 |
Table 3.
Kano evaluation list
| User Demands | Negative Questions | |||||
|---|---|---|---|---|---|---|
| Like | Deserved | Neutral | Endurable | Dislike | ||
| PositiveQuestions | Like | Q | A | A | A | O |
| Deserved | R | I | I | I | M | |
| Neutral | R | I | I | I | M | |
| Endurable | R | I | I | I | M | |
| Dislike | R | R | R | R | Q | |
3.2. STEP2: Analytic Hierarchy Process (AHP)
The Analytic Hierarchy Process (AHP) is a multi-criteria decision-making method that transforms complex decision problems into ordered hierarchical structures[15]. It involves comprehensive analysis and quantification of qualitative problems, gradually optimizing the coupling relationship between various indicator attributes[36].
AHP is characterized by strong adaptability and high flexibility, and it has been widely used in Multiple-Criteria Decision-Making (MCDM) problems[37]. The steps of the AHP method are as follows:
- Hierarchical Analysis Structure Construction
Analyze the relationships between user demands, establish a systematic hierarchical structure, and create a hierarchy chart. Design a questionnaire based on a judgment scale of 1 to 9, where 1 indicates equal importance, and 9 indicates extremely important (as shown in the Table 4). Based on this judgment scale, pairwise comparisons of first and second-level user demands are conducted to obtain weight values and to process the numerical values[38].
- 2.
- Construction of judgment matrix A
Construct the judgment matrix A. In the process of determining the importance of evaluation indicators, it is often difficult to determine the importance of one indicator compared to another. Therefore, the relationship matrix elements, ai, aj(i,j=1,2,...,n) represent the elements, and aij represents the importance of i compared to j. If the comparison is the opposite, the reciprocal 1/aij is taken[22]. Based on this, the judgment matrix A can be constructed:
- 3.
- Weight Calculations
Using the judgment matrix, calculate the geometric mean to obtain the average value Vi. Normalize the results to obtain the average value wi of each weight and the weight vector W[39]. The calculation formula is as follows:
- 4.
- Consistency test of judgment matrix
To evaluate the rationality of the above weight allocation and avoid errors caused by subjective judgments of decision-makers, it is necessary to conduct a consistency test on the judgment matrix. λmax is the maximum eigenvalue, CI is the consistency index of the judgment matrix, RI is the average random consistency index of the judgment matrix, and CR is the random consistency ratio of the judgment matrix. If the CR of the judgment matrix A is less than 0.1 or λmax=n and CI=0, it is considered to have passed the consistency test[18]. Otherwise, the matrix needs to be modified until its consistency meets the requirements. The calculation method is as follows:
(1) Calculate the consistency index CI, where n is the number of indicators, using the formula[39]:
CI=λmax-n/n-1
(2) Look up the corresponding RI.
Table 5.
Average random consistency
| n | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RI | 0.52 | 0.89 | 1.12 | 1.26 | 1.36 | 1.41 | 1.46 | 1.49 | 1.52 | 1.54 | 1.56 | 1.58 | 1.59 |
(3) Calculate the CR. CR is the random consistency ratio of the judgment matrix[40], and is calculated using the formula:
CR=CI/RI
- 5.
- Determine the weight order.
Finally, by calculating the elements at each level, the weight values for each requirement are obtained, and the importance ranking of design factors is determined, thus clarifying the key user demands.
3.3. STEP3: Quality Function Development (QFD)
- Define design requirements and objectives
By analyzing user demands using the Kano model and AHP, user demands attributes and their importance were identified. The next step is to map the various levels of requirements elements to design requirements, further quantifying the degree of correlation between user requirements and design requirements. This mapping relationship not only ensures the rationality of requirement transformation but also maximizes the implementation of functionality. In the Quality House matrix table, different symbols are used to represent the strength of the correlation, where "●" represents a strong correlation with a value of 5, "○" represents a moderate correlation with a value of 3, "△" represents a weak correlation with a value of 1, and blank spaces represent no correlation[41].
- 2.
- Build the house of quality and calculate the importance of design requirements
The establishment of the matrix relationship in the House of Quality is the core part, which calculates the weight values of various design elements. Assuming that there are n design requirements, with Wi representing the importance value of the i-th requirement for the elderly. The degree of association between the i-th elderly requirement and the j-th design requirement is denoted as Rij [42]. Consequently, the importance of the j-th design requirement can be computed using the following formula:
Sort the importance values Hj of design requirements in descending order, determine the critical design requirements, and plan the design scheme to maximize user satisfaction.
3.4. STEP4: PUGH Decision Matrix
Through PUGH decision matrix, the design proposals are evaluated[5], analyzed in detail, and screened based on the final scores to obtain the optimal proposal, thereby providing users with a satisfying user experience.
- Design solutions generation
Based on the Quality House model, the importance of design requirements is determined, with higher scores indicating greater importance in improving the satisfaction of elderly users with medication reminder applications, and vice versa. The obtained design requirements serve as a reference factor for the evaluation of design proposals. Medication reminder applications usually consist of a visual interface, interaction mode, and usage functionality. The gathered user demands encompass the style and features commonly found in most applications. Among these requirements, the top four design requirements are deemed as primary elements due to their significance, while the remaining features serve as auxiliary elements[22].
- 2.
- Program evaluation
Construct a PUGH decision matrix by placing design evaluation criteria on the left and comprehensive weights of design solutions and evaluation criteria at the top. Take one design solution as a reference and use a 1-5 point rating system (1 point worse than the reference by a lot, 2 points worse than the reference, 3 points equal to the reference, 4 points better than the reference, 5 points-much better than the reference) to evaluate[22]. The formula for calculating the final evaluation score incorporates both the significance of design requirements and the magnitude of the rating score, as illustrated below:
The formula calculates the final evaluation score of a design concept by using the PUGH decision matrix. Let Vi denote the comprehensive evaluation score of concept i, Vij represents the score of concept j on the i-th evaluation criterion, Hi represents the overall weight of the i-th evaluation criterion, and n denotes the total number of evaluation criteria[22]. The design concepts are ranked based on their overall evaluation scores to determine the final design concept.
4. Results
4.1. Kano Model
1. Collected elderly user demands
Interviews are a widely employed user research method that offers distinct advantages in capturing unique information and perspectives regarding the research environment[43]. Therefore, this study employs the qualitative research method of in-depth user interviews to gather original descriptions of target user needs. To ensure the accuracy of the information and the representativeness of the sample, we conducted research on 38 elderly users who met the following criteria: (1) aged between 60-75 years old, taking two or more medications daily; (2) need of long-term or lifelong medication; (3) living independently and possessing self-care capabilities; (4) having experience in using or requiring medication reminder products and services. The sample consists of 17 males and 21 females (user information is provided in Table 6). The interviews were conducted in a one-on-one format. Prior to the interviews, three interface designers, two PhDs in interaction design, and a professor discussed the structure and content of the interviews (outlined in Table 7). Each session lasted approximately 35 minutes. The entire interview process was recorded using a tape recorder, and detailed notes were taken to capture the interviewer's perspectives. These annotations are utilized to explain and annotate the language used by the respondents, ensuring comprehensive and understandable data.
After obtaining the above information, organize the research results. The results show that the surveyed users have many similar needs with only a few differences. Therefore, all user requirements are sorted out, useless items are removed, and identical items are merged. In the end, 20 original user requirements were obtained.
Table 8.
Collection of original demands of elderly users
| Serial Number | Original Demands | Serial Number | Original Demands |
|---|---|---|---|
| U1 | Text display larger | U11 | Easy login, not too many steps |
| U2 | Patterns are easy to understand | U12 | Medication time-reminder and sound reminder |
| U3 | Do not too many colors | U13 | Dosage reminder and sound reminder |
| U4 | The interface looks more concise | U14 | Medication precautions reminder and sound reminder |
| U5 | Do not have too many pages | U15 | Family remote help reminder |
| U6 | I can go back after I made a mistake | U16 | Record previous medications |
| U7 | Feedback and tips after clicking | U17 | Add medication instructions, doctor's orders, etc. |
| U8 | Language understandable | U18 | Drug balance check reminder |
| U9 | Capable of voice prompts | U19 | Chat with doctors online |
| U10 | Operation teaching helps learn to use | U20 | Personal privacy issues |
2. Classification of elderly user demands
The 20 original user demands were renamed and defined, and Kano questionnaires were designed based on these demands. Positive and negative questions were set for each requirement item (provide this function/do not provide this function). Paper and electronic questionnaires were used in combination to survey elderly target users aged 60-75 years old, with a focus on elderly communities with dense populations. A total of 105 questionnaires were distributed, and the respondents spent a minimum of 200 seconds responding to the questions. A total of 105 questionnaires were distributed, and the respondents spent a minimum of 200 seconds responding to the questions. Out of these, 98 questionnaires were considered valid, resulting in a recovery rate of 93.3%.
According to the Kano evaluation table, the results of the requirement survey were statistically analyzed, and the elderly people's requirement attribute categories were obtained, as shown in Table 6. The necessary attributes (M) were U1, U4, U5, U10, U11, and U12. The attractive attributes (A) were U3, U6, U8, U9, U16, U17, U19, U20. The expected attributes (O) were U2, U7, U13, U14, U15. The indifferent attributes (I) were U18.
The classification results show that most of the elements of necessary attributes (M) have many similarities with other commonly used applications in the daily lives of the elderly, which is related to the elderly people's experience of use, such as large fonts, simple interfaces, and one-click log in. Therefore, when designing, it is necessary to fully consider the elderly people's operating habits and cognitive levels. Compared with necessary attributes, attractive attributes, and expected attributes have more functions and usage demands, such as operation feedback, hierarchical conversion, and voice reminders. These requirements are core needs of medication reminder applications and are crucial for improving elderly people's satisfaction with such applications. Indifferent attributes (I) do not affect user satisfaction, but there is a possibility of being converted into attractive attributes in the future. Therefore, it is also considered within the scope of this study without affecting the overall structure of the application.
Table 9.
Kano classification of elderly medication reminder mobile application
| Serial Number | User Demand Elements | Quality Dimension | Total | Quality Type | ||||
|---|---|---|---|---|---|---|---|---|
| M | O | A | I | Q | ||||
| U1 | Large font display | 42 | 8 | 5 | 0 | 0 | 55 | M |
| U2 | Easy-to-understand icons | 18 | 5 | 32 | 0 | 0 | 55 | O |
| U3 | Color unity | 8 | 29 | 18 | 0 | 0 | 55 | A |
| U4 | Simple interface | 30 | 3 | 22 | 0 | 0 | 55 | M |
| U5 | Fewer levels, less memory burden | 35 | 7 | 13 | 0 | 0 | 55 | M |
| U6 | Strong fault tolerance | 19 | 27 | 9 | 0 | 0 | 55 | A |
| U7 | Good operational feedback | 20 | 3 | 32 | 0 | 0 | 55 | O |
| U8 | The language is easy to understand | 17 | 16 | 22 | 0 | 0 | 55 | A |
| U9 | Voice broadcast | 8 | 40 | 7 | 0 | 0 | 55 | A |
| U10 | Operation guide | 32 | 4 | 2 | 0 | 17 | 55 | M |
| U11 | Login shortcut (one-click login) | 36 | 9 | 10 | 0 | 0 | 55 | M |
| U12 | Medication time reminders and voice broadcast | 41 | 11 | 3 | 0 | 0 | 55 | M |
| U13 | Dosage reminder and voice broadcast | 13 | 15 | 27 | 0 | 0 | 55 | O |
| U14 | Reminders and voice broadcasts of medication precautions | 7 | 12 | 36 | 0 | 0 | 55 | O |
| U15 | Relatives and friends can be reminded remotely and voice broadcast | 9 | 3 | 43 | 0 | 0 | 55 | O |
| U16 | Medication record management | 10 | 26 | 19 | 0 | 0 | 55 | A |
| U17 | Take pictures to add drug descriptions, doctor's orders, etc. | 8 | 35 | 9 | 0 | 3 | 55 | A |
| U18 | Medicine Inventory Check Tips | 3 | 19 | 11 | 0 | 22 | 55 | I |
| U19 | Pharmacist online communication | 6 | 25 | 24 | 0 | 0 | 55 | A |
| U20 | Personal information security | 10 | 35 | 7 | 0 | 3 | 55 | A |
4.2. Demand Hierarchy Analysis of Mobile Application of Medication Reminder for the Elderly
1. Hierarchical construction of elderly users demands
According to the Kano model, the attributes of the elderly people's needs were classified, and an Analytic Hierarchy Process (AHP) model was established. The goal level is the design of a mobile application for medication reminders for the elderly, the criterion level is the first-level demand elements, which are visual demand (U1), usage demand (U2), and functional demand (U3). The indicator level consists of the 20 second-level user needs belonging to the U1, U2, and U3 sub-levels.
Table 10.
Construction and classification of demand hierarchy
| Target Layer | First-level demands | Second-level demands | Quality Type |
|---|---|---|---|
| U: Elderly Medication Reminder Mobile Application Project |
U1: Visual demands |
U11 Large font display | M |
| U12 Easy-to-understand icons | O | ||
| U13 Color unity | A | ||
| U14 Simple interface | M | ||
| U2: Usage demands | U21 Fewer levels, less memory burden | M | |
| U22 Strong fault tolerance | A | ||
| U23 Good operational feedback | O | ||
| U24 The language is easy to understand | A | ||
| U25 Voice broadcast | A | ||
| U3: Function demands | U31 Operation guide | M | |
| U32 Login shortcut (one-click login) | M | ||
| U33 Medication time-reminder and voice broadcast | M | ||
| U34 Dosage reminder and voice broadcast | O | ||
| U35 Reminders and voice broadcasts of medication precautions | O | ||
| U36 Relatives and friends can be reminded remotely and voice broadcast | O | ||
| U37 Medication record management | A | ||
| U38 Take pictures to add drug descriptions, doctor's orders, etc. | A | ||
| U39 Medicine Inventory Check Tips | I | ||
| U310 Pharmacist online communication | A | ||
| U311 Personal information security | A |
- 3.
- Construct elderly users demands judgment matrix
To ensure the accuracy and diversity of the answers, a total of 25 relevant personnel involved in the design and research of medication reminder apps for the elderly were tested. A combination of questionnaires and open-ended interviews were used to survey the participants, including 6 app developers from internet companies, 8 UI designers, 6 professors researching the direction of aging-oriented transformation in the field of interaction design, and 5 Ph. Students. The criteria layer judgment matrix U was constructed, and the indicator layer matrices U1, U2, and U3 were constructed in the same way. Professional personnel was invited to compare each pair of hierarchical requirements based on their relative importance and score them according to the scale.
Firstly, construct the judgment matrix of the target level U of the medication reminder application, and the score calculation results are as follows:
Then, construct the judgment matrix of U1 Visual demands, and the score calculation results are as follows:
Construct the judgment matrix of U2 Usage demands, and the score calculation results are as follows:
Finally, the judgment matrix of U3 Function demands is constructed, and the score calculation results are as follows:
3. Consistency test and importance ranking
Consistency testing was used to determine if there were any logical errors in the constructed judgment matrices. If CR<0.1, it was considered that the matrix passed the consistency test, otherwise the matrix should be revised. Based on the CR values in the table, all consistency indicators of the constructed matrix were greater than 0.1 and therefore passed the consistency test. In terms of importance ranking, the weights of each primary indicator were calculated first. Then, the within-group weights and total weights of each required element in the secondary indicators were calculated separately. Finally, the total weight score was used to obtain the overall ranking, determining the importance level of each requirement. According to the table, U12 (0.0473) and U25 (0.0470) and U14 (0.1501), and U24 (0.01504) have the same values shown in the table, so select the values of the four digits after the decimal point for comparison to determine the final weight value.
Table 11.
Weight arising from the AHP Analysis.
| Criteria | Consistency test | Weight | Sub-Criteria | Quality Type | Weight within group | Rank Within group | Overall weight | Overall rank | Consistency test |
|---|---|---|---|---|---|---|---|---|---|
| U1 |
max=3.009 CR=0.009 CI=0.005 |
0.297 | U11 | M | 0.321 | 2 | 0.107 | 3 |
max=4.081 CR=0.030 CI=0.027 |
| U12 | O | 0.142 | 3 | 0.047 | 8 | ||||
| U13 | A | 0.087 | 4 | 0.029 | 12 | ||||
| U14 | M | 0.450 | 1 | 0.150 | 2 | ||||
| U2 | 0.164 | U21 | M | 0.254 | 2 | 0.085 | 4 |
max=5.244 CR=0.055 CI=0.06 |
|
| U22 | A | 0.054 | 5 | 0.018 | 15 | ||||
| U23 | O | 0.100 | 4 | 0.033 | 11 | ||||
| U24 | A | 0.451 | 1 | 0.150 | 1 | ||||
| U25 | A | 0.141 | 3 | 0.047 | 9 | ||||
| U3 | 0.539 | U31 | M | 0.028 | 8 | 0.009 | 18 |
max=11.812 CR=0.053 CI=0.081 |
|
| U32 | M | 0.016 | 9 | 0.005 | 20 | ||||
| U33 | M | 0.232 | 1 | 0.077 | 5 | ||||
| U34 | O | 0.218 | 2 | 0.073 | 6 | ||||
| U35 | O | 0.115 | 4 | 0.038 | 10 | ||||
| U36 | O | 0.160 | 3 | 0.053 | 7 | ||||
| U37 | A | 0.073 | 5 | 0.024 | 13 | ||||
| U38 | A | 0.045 | 6 | 0.015 | 16 | ||||
| U39 | I | 0.031 | 7 | 0.010 | 17 | ||||
| U310 | A | 0.066 | 6 | 0.022 | 14 | ||||
| U311 | A | 0.017 | 10 | 0.006 | 19 |
4. Result analysis
According to the weight results of the indicators for the elderly medication reminder application, the indicator weight rankings of the requirement layer are as follows: functional demands (U3) > visual demands (U1) > usage demands (U2). Therefore, when designing the elderly medication reminder application, it is important to fully consider the functional needs of the elderly. Functional requirements are the most basic and core part of the entire application. According to the table, the design elements that need to be emphasized in this part include U12 Medication time reminder and voice broadcast, U13 Dosage reminder and voice broadcast, U15 Remote reminder for relatives and voice broadcast, and U14 Medication note reminder and voice broadcast. Visual demands are key elements in improving the ease of use for the elderly. Through previous research experience, it has been found that the same application lacks care for the elderly in terms of interaction interface design, such as difficulties in navigation and low identification, etc. Therefore, in the process of interface design, attention should be paid to whether the interface of the entire application is concise (U4), and whether the font size (U1) and icons (U2) are easy for the elderly to read and understand. Finally, usage requirements, combined with the elderly's operating habits, can greatly improve their efficiency and reduce the difficulty of learning to use. Therefore, in the design process, it is important to fully consider the cognitive ability of the elderly. Using easy-to-understand language descriptions (U8), fewer interface levels (U5), and voice prompts (U9) can better enhance the satisfaction of elderly users.
4.3. Quality Function Deployment
1. Define design requirements
Based on the Kano model analysis of user requirements in the previous stage and the weights of each requirement obtained through the analytic hierarchy process, the next step is to transform the user demands into design requirements through mapping relationships. 4 interface designers, 5 UI designers, and 5 doctoral students specializing in user experience were invited to participate in the process of refining user demands, and the characteristics of the medication reminder mobile app for the elderly were comprehensively summarized to finally obtain First-level design requirements and 16 second-level design requirements, as shown in the Table10.
Table 12.
Design requirements.
| First-Level Design Requirements | Second-Level Design Requirements |
|---|---|
| D1: Interface Design | D11 Interface font design (font type, font size) |
| D12 Interface icon design (graphics, size, spacing) | |
| D13 Interface color design | |
| D14 Interface layout design | |
| D2: Operation Design | D21 Information architecture design (Page hierarchy) |
| D22 Voice broadcast (Sound design) | |
| D23 Confirm & Return operation design | |
| D24 Intelligibility & Legibility design | |
| D25 Feedback design (Visual, Auditory, Haptic) | |
| D3: Function Design | D31 Easy to log in |
| D32 Reminder settings (medication time, dose of medication, Precautions, Medicine Remaining) | |
| D33 Connect with relatives and friends (Share with others) | |
| D34 Medication records | |
| D35 Medication instructions | |
| D36 Online consultation with doctors | |
| D37 Personal Information Security |
2. Matrices solution to determine the relationship between user demands and design requirements
Based on the elderly user demands (Table 8) and design requirements (Table 10), a quality house matrix model is constructed to represent the correlation between the two. The "left wall" of the quality house represents the elderly user requirements, the "ceiling" represents the design requirements, and the correlation between the two is represented by scores. A score of 5 indicates a strong correlation, 3 indicates a moderate correlation, 1 indicates a weak correlation, and a blank space indicates no correlation. The scores were given by 4 elderly target users and experts in interaction design and interface design, and the results are shown in Figure 4.
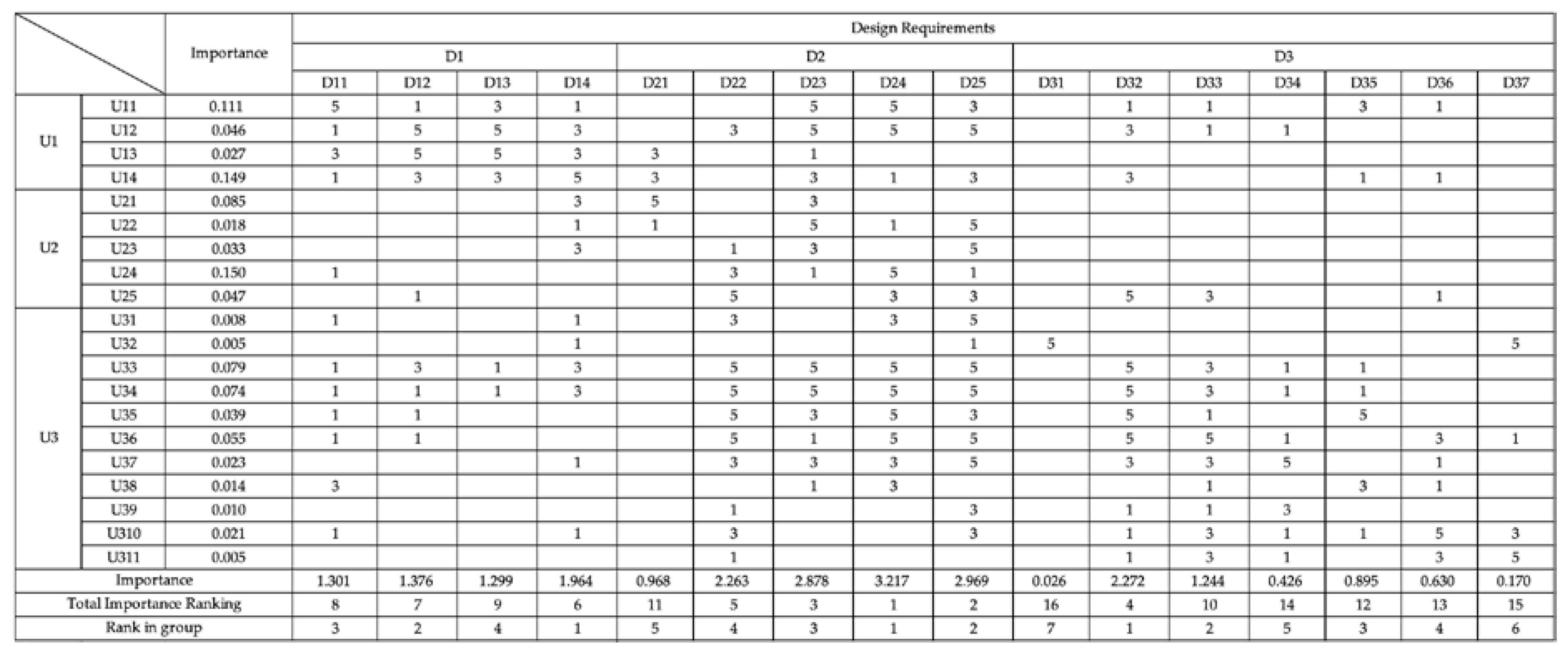
Figure 3.
User demands and design requirements house of quality.
4.4. PUGH Decision Matrix
In this project, the PUGH decision matrix technique was employed to evaluate the generated plans for the elderly medication reminder app. The scores obtained were utilized to identify the optimal plan, aiming to ensure a satisfactory user experience and enhance the efficiency of usage for the elderly.
1. Creating design solutions
Based on the quality house matrix's prioritized ranking of design requirements, the highest-ranked design requirements serve as the main reference for the design of medication reminder applications for the elderly, which include "D24 Intelligibility & Legibility design," "D25 Feedback design," "D23 Confirm & Return operation design," "D32 Reminder settings," and "D22 Voice broadcast." To avoid the limitations and one-sidedness of the design, we have integrated the design standards and requirements of interface functionality layouts with high usage and recognition rates in current reminder applications, and have designed the following four schemes:
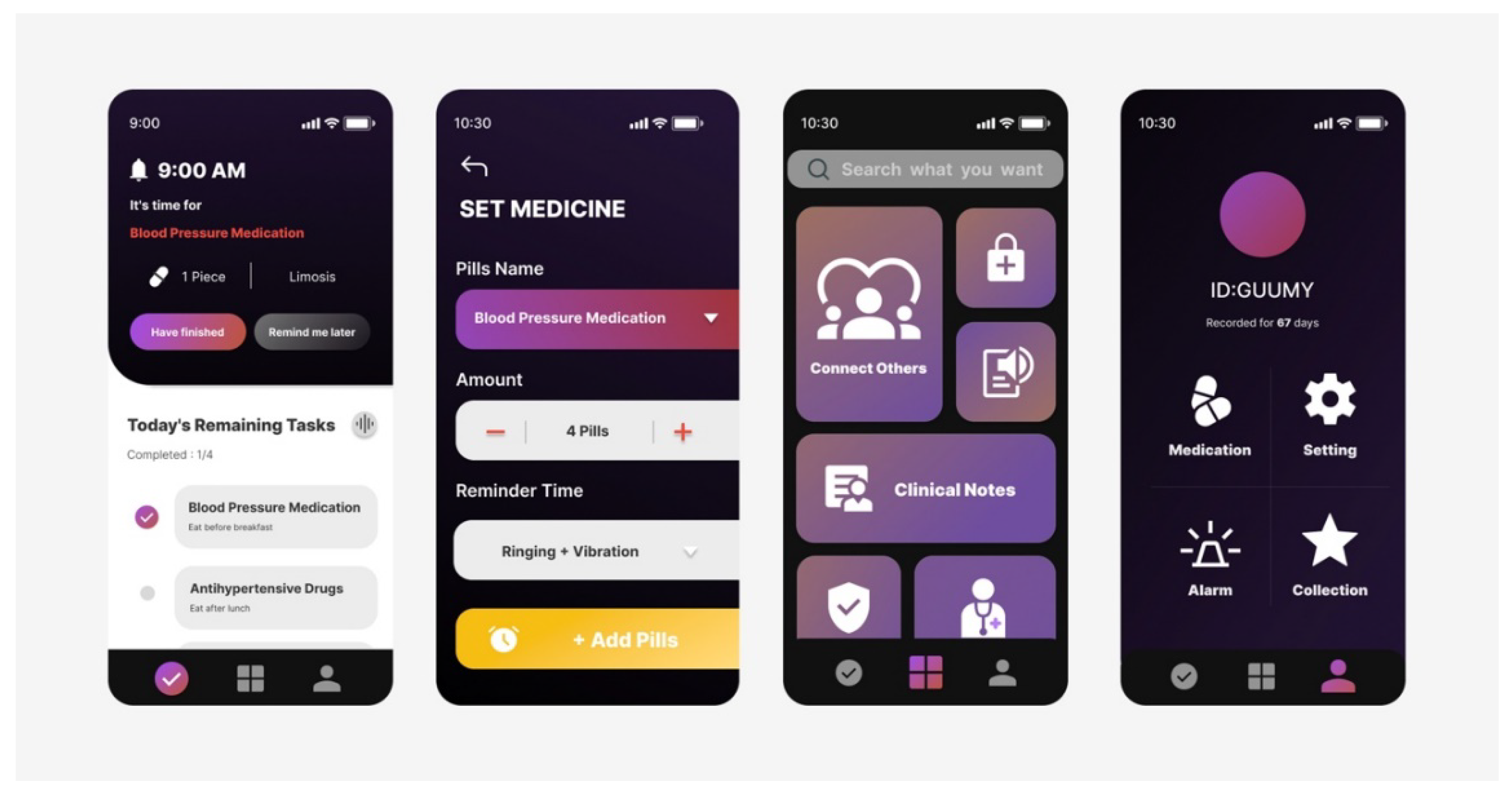
Figure 5.
Project B Interaction Interface.
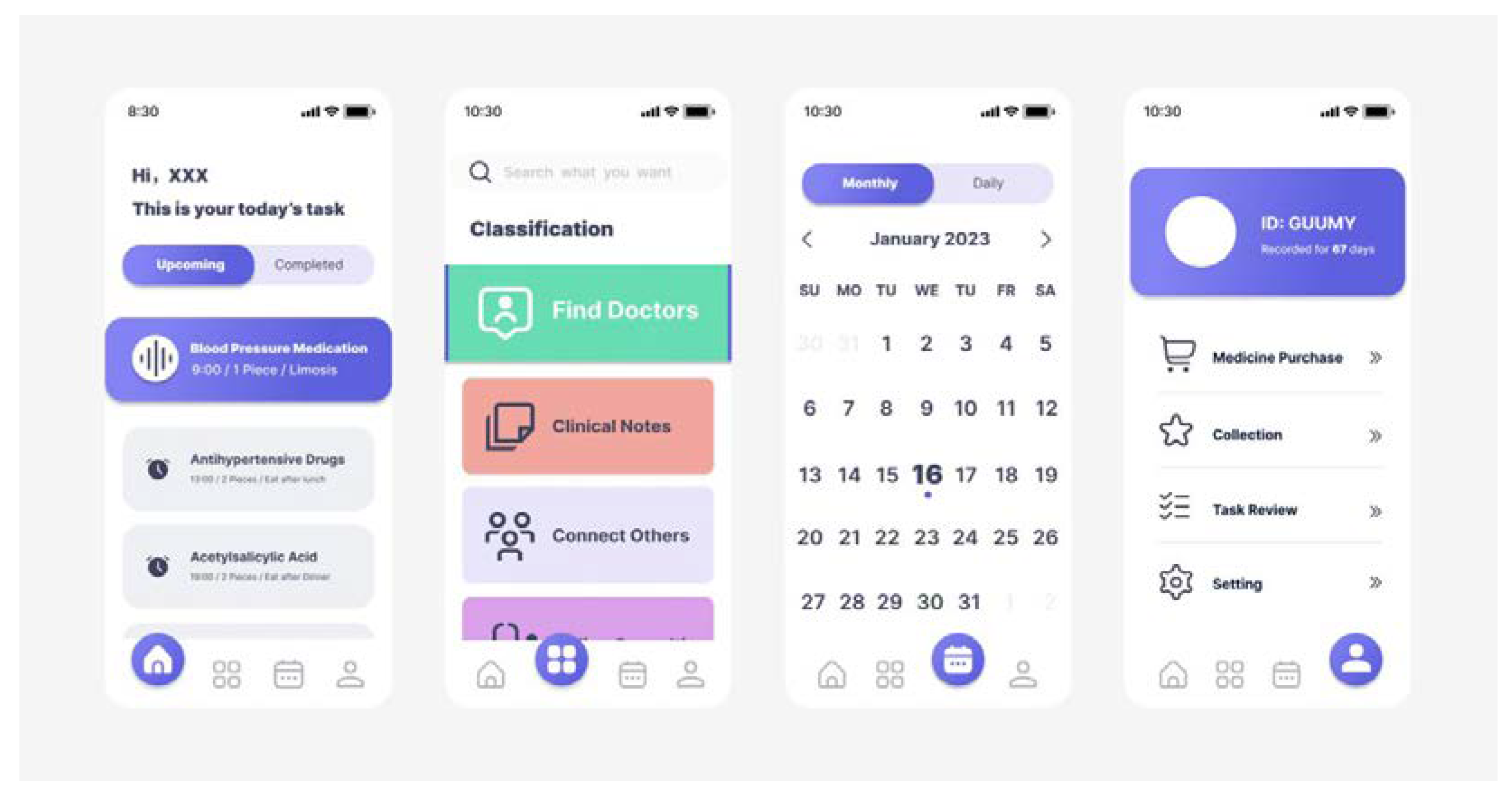
Figure 6.
Project C Interaction Interface.
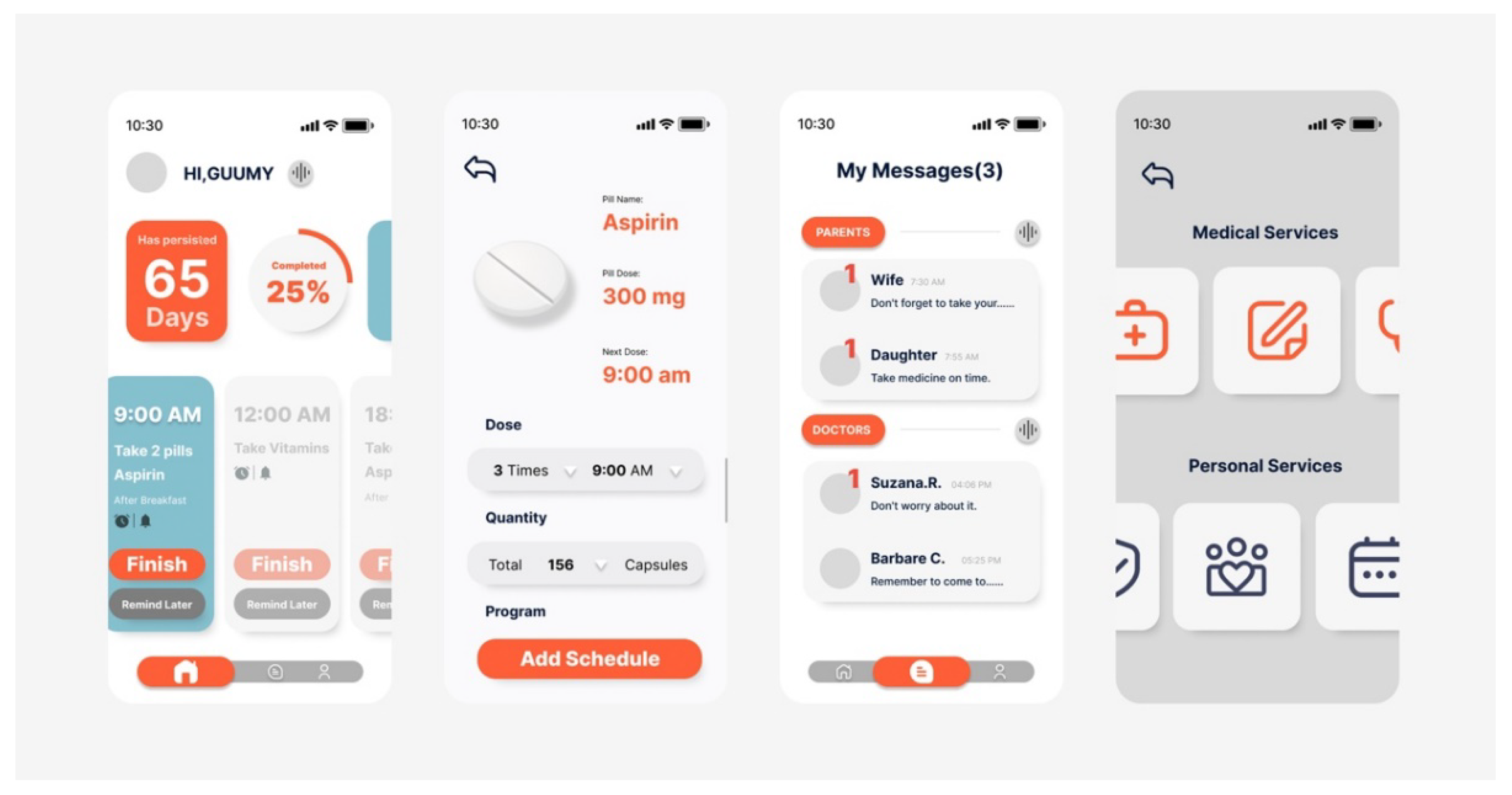
Figure 7.
Project D Interaction Interface.
2. Program evaluation
According to the design requirements, a PUGH decision matrix was established to conceptually evaluate the interaction interface and functional usage of the four high-fidelity design schemes. Scheme C was selected as the reference scheme. The left side of the matrix is the design requirements, and the top is the comprehensive weight and design schemes for each design requirement. To ensure the rationality and objectivity of the scoring results, formula (7) was used for calculation. Finally, the best scheme was obtained through total score and importance ranking, as shown in Table 10.
Table 13.
Correlation between user needs and evaluation elements.
| Design Requirements | Importance | Ranking | Alternative | ||||
|---|---|---|---|---|---|---|---|
| Project A | Project B | Project C | Project D | ||||
| D1 | D11 | 1.301 | 8 | 2 | 3 | 3 | 2 |
| D12 | 1.376 | 7 | 1 | 5 | 2 | 3 | |
| D13 | 1.299 | 9 | 2 | 5 | 5 | 2 | |
| D14 | 1.964 | 6 | 3 | 4 | 2 | 2 | |
| D2 | D21 | 0.968 | 11 | 2 | 5 | 2 | 4 |
| D22 | 2.263 | 5 | 2 | 4 | 3 | 3 | |
| D23 | 2.878 | 3 | 2 | 3 | 5 | 4 | |
| D24 | 3.217 | 1 | 4 | 5 | 2 | 3 | |
| D25 | 2.969 | 2 | 3 | 4 | 2 | 3 | |
| D3 | D31 | 0.026 | 16 | 2 | 4 | 5 | 3 |
| D32 | 2.272 | 4 | 2 | 5 | 4 | 3 | |
| D33 | 1.244 | 10 | 3 | 4 | 2 | 4 | |
| D34 | 0.426 | 14 | 2 | 3 | 2 | 2 | |
| D35 | 0.895 | 12 | 5 | 4 | 3 | 2 | |
| D36 | 0.630 | 13 | 4 | 3 | 5 | 3 | |
| D37 | 0.170 | 15 | 2 | 5 | 2 | 3 | |
| Total Score | 62.976 | 99.659 | 71.297 | 70.898 | |||
5. Discussion
5.1. Optimization of design method by integrating the KANO-AHP-QFD-PUGH model
This paper proposes an integration of QFD theory with the Kano model, AHP, and PUGH decision matrices to enhance the objectivity and accuracy of design decisions and outcomes. The Kano model captures user demand information through surveys and qualitative feedback but lacks a quantitative measurement of the importance of different user needs. By incorporating AHP, subjective evaluations of various needs can be converted into weights using a quantitative judgment matrix and calculation process, thereby addressing the limitations of the Kano model[15]. Dionicio Neira-Rodado et al. verified the feasibility of combining kano with analytic hierarchy process research in the design of hip implants. The QFD model facilitates the transformation of user needs into specific design requirements, determining the prioritization of design demands through the construction of a house of quality. These output design requirements serve as evaluation criteria in the Pugh decision matrix, enabling a structured comparison and assessment of different designs. The combination of QFD and PUGH methods enables decision-makers to comprehensively understand the strengths and weaknesses of each design option, mitigating subjective biases and yielding more objective evaluation results[22] The research method of integrating AHP-QFD-PUGH in the study of surgical auxiliary equipment by TianLu Zhu et al. can improve the innovation and scientificity of the design results. Combining the 4 methods of Kano model, AHP, QFD and Pugh decision matrix can provide comprehensive requirements identification, prioritization, decision support, risk reduction and quality assurance, thereby helping the design team to better meet user demands and improve design quality and user satisfaction.
5.2. Implications of case study results for UX design for older adults
According to the research results of the Kano-AHP-QFD-PUGH integrated model, three primary requirements and twenty secondary requirements were identified. Through these requirements, it was discovered that elderly users prioritize interface design simplicity (D14 Interface layout design) for their visual needs. Displaying too much information creates a memory burden and distracts their attention during the trial period. Therefore, the interface layout should prioritize the primary and core functions and content, followed by font size design (D11 Interface font design). Using characters that are too large or too thick can result in too little content displayed on a single page and visually unappealing. Characters that are too small or thin may make it difficult for the elderly to read. Icon design within the application (D12 Interface icon design) is also critical for easy recognition. Abstract icons can affect the elderly's cognition, and flat design is the better choice to overcome cognitive barriers. Overall, the design should be simple, clear, and easy to identify. Additionally, they hope that the interface color will remain uniform (D13 Interface color design). Too many color combinations can confuse, affecting the visual experience during use. Although tones such as red and yellow can improve interface recognition, their strong stimulus can cause eye discomfort when viewed for a long time. Therefore, when considering recognition, one must also consider the physiological characteristics of the elderly.
Regarding usage requirements, elderly users need language descriptions that are easy to understand (D24 Intelligibility & Legibility design). They are concerned about whether they can fully understand the text and operational prompts displayed in the app. Otherwise, they will experience greater psychological anxiety. Therefore, in the design process, we should first consider the cognitive and memory levels of most elderly people regarding text understanding. During use, the elderly will continuously confirm their actions' correctness or incorrectness through the app's timely feedback, such as sound, visual, and tactile feedback (D25 Feedback design). These feedback modes will enhance the elderly users' perception of safety, allowing them to know the task or project they are undertaking. The prompt to confirm and return operations (D23 Confirm & Return operation design) is an effective error prevention measure. Due to the decline in cognitive ability and physiological function, elderly users have a higher likelihood of miss-operation than younger people. Therefore, more confirmation information is needed to prevent errors. Voice broadcasting (D22 Voice broadcast) is particularly favored by elderly users, as they believe that playing voice information can effectively reduce their visual burden. Furthermore, they can receive medication reminders at any time while doing other things. Additionally, there should be fewer page hierarchies (D21 Information architecture design), as multiple hierarchical information structures can create memory difficulties for the elderly. Basic functions and buttons are more suitable for the primary page, saving users' search time, and improving ease of use and efficiency. This research result is similar to Rahul Malhotra et al.'s findings on low usage rates and willingness to use medication reminder applications for the elderly[3]. A complex interface, dense usage instructions, and language barriers greatly affect elderly users' willingness to use.
Finally, we also found that in terms of functional requirements, older adults are more concerned about the most basic and primitive functions of this application - reminders of medication time and dosage (D32 Reminder settings). They are also very willing to share their medication information with their family members, or complete medication reminders and notifications from their family members through electronic devices (D33 Connect with relatives and friends). According to the summary of the changes in reports on medication adherence challenges by Mushfique Ahmed et al., reminders may become more feasible, especially reminders from family members[44]. The main reason for this is that many older adults feel a strong sense of loneliness, and receiving care and greetings from their family and friends will make them feel warm. Therefore, in future designs, the connection between older users and their relatives and friends should be emphasized.
In addition to the above requirements, according to the experimental discussion results of the mobile application functional preferences for medication self-management in older adults by Andrea M. Russell et al., medication records (D34 Medication records) and medication instructions (D35 Medication instructions) are considered to be one of the most important functions[29]. Due to the COVID-19 pandemic, many older users with chronic diseases often have other complications and need to take multiple medications at the same time, so it is necessary to ensure the mutual warning effects between medications, making the design of these two functions particularly important. The privacy issues (D37 Personal information security) and convenience of logging in (D31 Easy to log in) for older users also need to be considered. A previous research report in Singapore stated that privacy issues are a major barrier to the widespread adoption of technology, especially in the healthcare field[45]. Providing offline data or privacy settings is necessary, and the login method is the first step for users to start using the app[3]. Therefore, more convenient login methods can effectively save time and improve usability, such as logging in by connecting with other social accounts, otherwise, it may reduce users' willingness to continue using the app.
6. Conclusion and Limitation
Due to the impact of the COVID-19 pandemic, older adults face a heightened memory burden when it comes to medication use. In order to help improve the medication compliance of the elderly and the usability, efficiency, and satisfaction of the medication management APP for the elderly, this study attempts to improve the design problems of the medication management APP and proposes a possible integrated Kano-AHP-QFD-PUGH The continuous optimization design method not only solves the limitations of the single design method, but also makes up for the shortcomings of the medication management application in the aging transformation, and improves the user experience of the elderly.
In the case study, we demonstrate how to obtain user needs through qualitative research and classify them into Kano attributes. We then use AHP to construct a hierarchical structure of user needs and determine the weight rankings of each need. QFD method maps user needs to design requirements and uses a quality house to determine the importance of each design requirement, ultimately identifying key needs. Finally, PUGH concept selection is used to verify the feasibility of the design scheme, and the results indicate that Project B is the best design solution.
The entire design process focuses on the elderly user group and uses a combination of qualitative and quantitative methods to integrate their special needs into the app design. The results of this study have both theoretical and practical significance. It not only provides a theoretical basis for designers to develop app design methods in the future but also offers specific targeted design solutions. This study demonstrates that this research framework can effectively be applied to the age-appropriate transformation of medication reminder apps for the elderly, and is not only suitable for the elderly but also for other user groups researching sustainable user experience optimization design for apps.
Future work will need to collect more data on the needs of elderly users in different regions. While continuously improving the usability of the case study, more attention needs to be paid to the emotional needs of the elderly, to eliminate their psychological burden towards technology products and enhance their operational experience. In addition, attention should be given to the elderly users' willingness to use medication reminder apps continuously, and through continuous iteration and updates, improve their user experience and satisfaction.
There are still some limitations to this study. Although the research team collected a wide range of data, due to practical limitations, the selection of research objects was limited to elderly communities in first-tier and second-tier cities in China. There is limited research on elderly users in other countries and regions. Different regions have differences in cultural background, living environment, and economic level, and there may be corresponding differences in user needs. Therefore, in future research, more influencing factors such as education level, cultural background, and income should be incorporated into the model.
Author Contributions
Writing—original draft, M.F.; Software and Formal analysis—W.Y.; Visualization—H.L.; Conceptualization and Supervision—Y.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Patel, T.; Ivo, J.; Faisal, S.; McDougall, A.; Carducci, J.; Pritchard, S.; Chang, F. A Prospective Study of Usability and Workload of Electronic Medication Adherence Products by Older Adults, Caregivers, and Health Care Providers. J Med Internet Res 2020, 22, e18073. [Google Scholar] [CrossRef] [PubMed]
- Stuck, R.E.; Chong, A.W.; Tracy, L.M.; Rogers, W.A. Medication Management Apps: Usable by Older Adults? Proceedings of the Human Factors and Ergonomics Society Annual Meeting 2017, 61, 1141–1144. [Google Scholar] [CrossRef] [PubMed]
- Ping, Y.; Visaria, A.; Suppiah, S.D.; Tan, Y.W.; Malhotra, R. Prevalence and Correlates of Medication Reminder App ‘Use and Use Intention’ among Older Adults. Exploratory Research in Clinical and Social Pharmacy 2022, 6, 100150. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Hong, Z.; Li, Y.; Zhou, F.; Niu, Y.; Xue, C. A Function Combined Baby Stroller Design Method Developed by Fusing Kano, QFD, and FAST Methodologies. International Journal of Industrial Ergonomics 2020, 75, 102867. [Google Scholar] [CrossRef]
- Li, Y.; Ghazilla, R.A.R.; Abdul-Rashid, S.H. QFD-Based Research on Sustainable User Experience Optimization Design of Smart Home Products for the Elderly: A Case Study of Smart Refrigerators. IJERPH 2022, 19, 13742. [Google Scholar] [CrossRef]
- Matzler, K.; Hinterhuber, H.H. How to Make Product Development Projects More Successful by Integrating Kano’s Model of Customer Satisfaction into Quality Function Deployment. Technovation 1998, 18, 25–38. [Google Scholar] [CrossRef]
- Tontini, G.; Dagostin Picolo, J. Identifying the Impact of Incremental Innovations on Customer Satisfaction Using a Fusion Method between Importance-Performance Analysis and Kano Model. International Journal of Quality & Reliability Management 2013, 31, 32–52. [Google Scholar] [CrossRef]
- He, R. ; Research On User Experience Optimization Design Of Elderly Vehicle Information System Based On QFD. Packaging Engineering 2022, 43, 164–170. [Google Scholar] [CrossRef]
- Kang, X.; Yang, M.; Wu, Y.; Ni, B. Integrating Evaluation Grid Method and Fuzzy Quality Function Deployment to New Product Development. Mathematical Problems in Engineering 2018, 2018, 1–15. [Google Scholar] [CrossRef]
- Kim, Y.; Choi, K.; Chung, D. A Study on the Development Methodology of Intelligent Medical Devices Utilizing KANO-QFD Model. Journal of Intelligence and Information Systems 2022, 28, 217–242. [Google Scholar] [CrossRef]
- Avikal, S.; Singh, R.; Rashmi, R. QFD and Fuzzy Kano Model-Based Approach for Classification of Aesthetic Attributes of SUV Car Profile. J Intell Manuf 2020, 31, 271–284. [Google Scholar] [CrossRef]
- Rampal, A.; Mehra, A.; Singh, R.; Yadav, A.; Nath, K.; Chauhan, A.S. Kano and QFD Analyses for Autonomous Electric Car: Design for Enhancing Customer Contentment. Materials Today: Proceedings 2022, 62, 1481–1488. [Google Scholar] [CrossRef]
- Lyu, J.; Chen, R.; Yang, L.; Wang, J.; Chen, M. Applying a Hybrid Kano/Quality Function Deployment Integration Approach to Wood Desk Designs for Open-Plan Offices. Forests 2022, 13, 1825. [Google Scholar] [CrossRef]
- Tontini, G. Integrating the Kano Model and QFD for Designing New Products. Total Quality Management & Business Excellence 2007, 18, 599–612. [Google Scholar] [CrossRef]
- Neira-Rodado, D.; Ortíz-Barrios, M.; De La Hoz-Escorcia, S.; Paggetti, C.; Noffrini, L.; Fratea, N. Smart Product Design Process through the Implementation of a Fuzzy Kano-AHP-DEMATEL-QFD Approach. Applied Sciences 2020, 10, 1792. [Google Scholar] [CrossRef]
- Saaty, T.L.; Vargas, L.G. Estimating Technological Coefficients by the Analytic Hierarchy Process. Socio-Economic Planning Sciences 1979, 13, 333–336. [Google Scholar] [CrossRef]
- Hridoy, R.M.; Parvez, Md.S.; Mohsin, N. Joining Methods of Analytic Hierarchy Process (AHP), Kano Model and Quality Function Deployment (QFD) to Improve the Tractor’s Seat Design for Tractor Drivers in Bangladesh. AJIBM 2020, 10, 1073–1083. [Google Scholar] [CrossRef]
- Wu, A. ; Research on Innovative Design of Shared Scooter in Scenic Spots Based on AHP/QFD/TRIZ. Packaging Engineering 2022, 43, 151–160. [Google Scholar] [CrossRef]
- Roghanian, E.; Alipour, M. A Fuzzy Model for Achieving Lean Attributes for Competitive Advantages Development Using AHP-QFD-PROMETHEE. J Ind Eng Int 2014, 10, 68. [Google Scholar] [CrossRef]
- Renzi, C.; Leali, F.; Pellicciari, M.; Andrisano, A.O.; Berselli, G. Selecting Alternatives in the Conceptual Design Phase: An Application of Fuzzy-AHP and Pugh’s Controlled Convergence. Int J Interact Des Manuf 2015, 9, 1–17. [Google Scholar] [CrossRef]
- Schütte *, S.T.W.; Eklund, J.; Axelsson, J.R.C.; Nagamachi, M. Concepts, Methods and Tools in Kansei Engineering. Theoretical Issues in Ergonomics Science 2004, 5, 214–231. [Google Scholar] [CrossRef]
- Zhu, T.-L.; Li, Y.-J.; Wu, C.-J.; Yue, H.; Zhao, Y.-Q. Research on the Design of Surgical Auxiliary Equipment Based on AHP, QFD, and PUGH Decision Matrix. Mathematical Problems in Engineering 2022, 2022, 1–13. [Google Scholar] [CrossRef]
- Yang, J. ; Technical Research on Product Concept Selection Based on AHP PUGH. Packaging Engineering 2016, 37, 162–167. [Google Scholar] [CrossRef]
- New Hand-Cart for Old-Delhi Whole Sale Market Designed and Engineered Using Generic Product Development Process. IJPAP 2020. [CrossRef]
- Teixeira, A.; Ferreira, F.; Almeida, N.; Silva, S.; Rosa, A.F.; Pereira, J.C.; Vieira, D. Design and Development of Medication Assistant: Older Adults Centred Design to Go beyond Simple Medication Reminders. Univ Access Inf Soc 2017, 16, 545–560. [Google Scholar] [CrossRef]
- Banskota, S.; Healy, M.; Goldberg, E. 15 Smartphone Apps for Older Adults to Use While in Isolation During the COVID-19 Pandemic. WestJEM 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Lakey, S.L.; Gray, S.L.; Borson, S. Assessment of Older Adults’ Knowledge of and Preferences for Medication Management Tools and Support Systems. Ann Pharmacother 2009, 43, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Haverhals, L.M.; Lee, C.A.; Siek, K.A.; Darr, C.A.; Linnebur, S.A.; Ruscin, J.M.; Ross, S.E. Older Adults with Multi-Morbidity: Medication Management Processes and Design Implications for Personal Health Applications. J Med Internet Res 2011, 13, e44. [Google Scholar] [CrossRef]
- Russell, A.M.; Smith, S.G.; Bailey, S.C.; Belter, L.T.; Pandit, A.U.; Hedlund, L.A.; Bojarski, E.A.; Rush, S.R.; Wolf, M.S. Older Adult Preferences of Mobile Application Functionality Supporting Medication Self-Management. Journal of Health Communication 2018, 23, 1064–1071. [Google Scholar] [CrossRef]
- Grindrod, K.A.; Li, M.; Gates, A. Evaluating User Perceptions of Mobile Medication Management Applications With Older Adults: A Usability Study. JMIR Mhealth Uhealth 2014, 2, e11. [Google Scholar] [CrossRef]
- Noleto, J.D.; José Costa Rodrigues, V.; Carvalho, R.C.B.C.; Ribeiro dos Santos Júnior, F. Interfaces of Medication Reminder Applications: An Analysis Aimed at the Elder Age. In Human Aspects of IT for the Aged Population. Design for the Elderly and Technology Acceptance; Zhou, J., Salvendy, G., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, 2019; ISBN 978-3-030-22011-2. [Google Scholar]
- Zahra, F. A USABILITY MODEL FOR CHRONIC DISEASE MANAGEMENT MOBILE APPLICATIONS.
- Violante, M.G.; Vezzetti, E. Kano Qualitative vs Quantitative Approaches: An Assessment Framework for Products Attributes Analysis. Computers in Industry 2017, 86, 15–25. [Google Scholar] [CrossRef]
- Du, L.; Chen, H.; Fang, Y.; Liang, X.; Zhang, Y.; Qiao, Y.; Guo, Z. Research on the Method of Acquiring Customer Individual Demand Based on the Quantitative Kano Model. Computational Intelligence and Neuroscience 2022, 1–12. [Google Scholar] [CrossRef]
- Li, Y. ; Design of QFD-based Elderly Smart Phone APP User Interface. Packaging Engineering 2016, 37, 95–99. [Google Scholar] [CrossRef]
- Karasan, A.; Ilbahar, E.; Cebi, S.; Kahraman, C. Customer-Oriented Product Design Using an Integrated Neutrosophic AHP & DEMATEL & QFD Methodology. Applied Soft Computing 2022, 118, 108445. [Google Scholar] [CrossRef]
- Alvarez, P.A.; Ishizaka, A.; Martínez, L. Multiple-Criteria Decision-Making Sorting Methods: A Survey. Expert Systems with Applications 2021, 183, 115368. [Google Scholar] [CrossRef]
- Pakizehkar, H.; Sadrabadi, M.M.; Mehrjardi, R.Z.; Eshaghieh, A.E. The Application of Integration of Kano’s Model, AHP Technique and QFD Matrix in Prioritizing the Bank’s Substructions. Procedia - Social and Behavioral Sciences 2016, 230, 159–166. [Google Scholar] [CrossRef]
- Barzilai, J.; Golany, B. Ahp Rank Reversal, Normalization, And Aggregation Rules. INFOR: Information Systems and Operational Research 1994, 32, 57–64. [Google Scholar] [CrossRef]
- Cheng, E.W.L.; Li, H. Analytic Hierarchy Process: An Approach to Determine Measures for Business Performance. Measuring Business Excellence 2001, 5, 30–37. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, M.; Lyu, J.; Chen, S.; Chen, Y. Research on Human-Computer Interaction Design of Office Chair Based on QFD Method. IOP Conf. Ser.: Mater. Sci. Eng. 2020, 740, 012180. [Google Scholar] [CrossRef]
- Knopek, T.; Dabrowska, D. The Use of the Contamination Index and the LWPI Index to Assess the Quality of Groundwater in the Area of a Municipal Waste Landfill. Toxics 2021, 9, 66. [Google Scholar] [CrossRef]
- Hannabuss, S. Feature Article Research Interviews. New Library World 97.
- Ahmed, M.; Wheeler, C.; Franklin, B.D.; Begum, R.; Garfield, S. Resilience of Medication Adherence Practices in Response to Life Changes: Learning from Qualitative Data Obtained during the COVID-19 Pandemic. Healthcare 2021, 9, 1048. [Google Scholar] [CrossRef] [PubMed]
- Low, S.T.H.; Sakhardande, P.G.; Lai, Y.F.; Long, A.D.S.; Kaur-Gill, S. Attitudes and Perceptions Toward Healthcare Technology Adoption Among Older Adults in Singapore: A Qualitative Study. Front. Public Health 2021, 9, 588590. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
The sustainable optimization design process of the elderly medication reminder application.
Figure 2.
The sustainable optimization design process of the elderly medication reminder application.
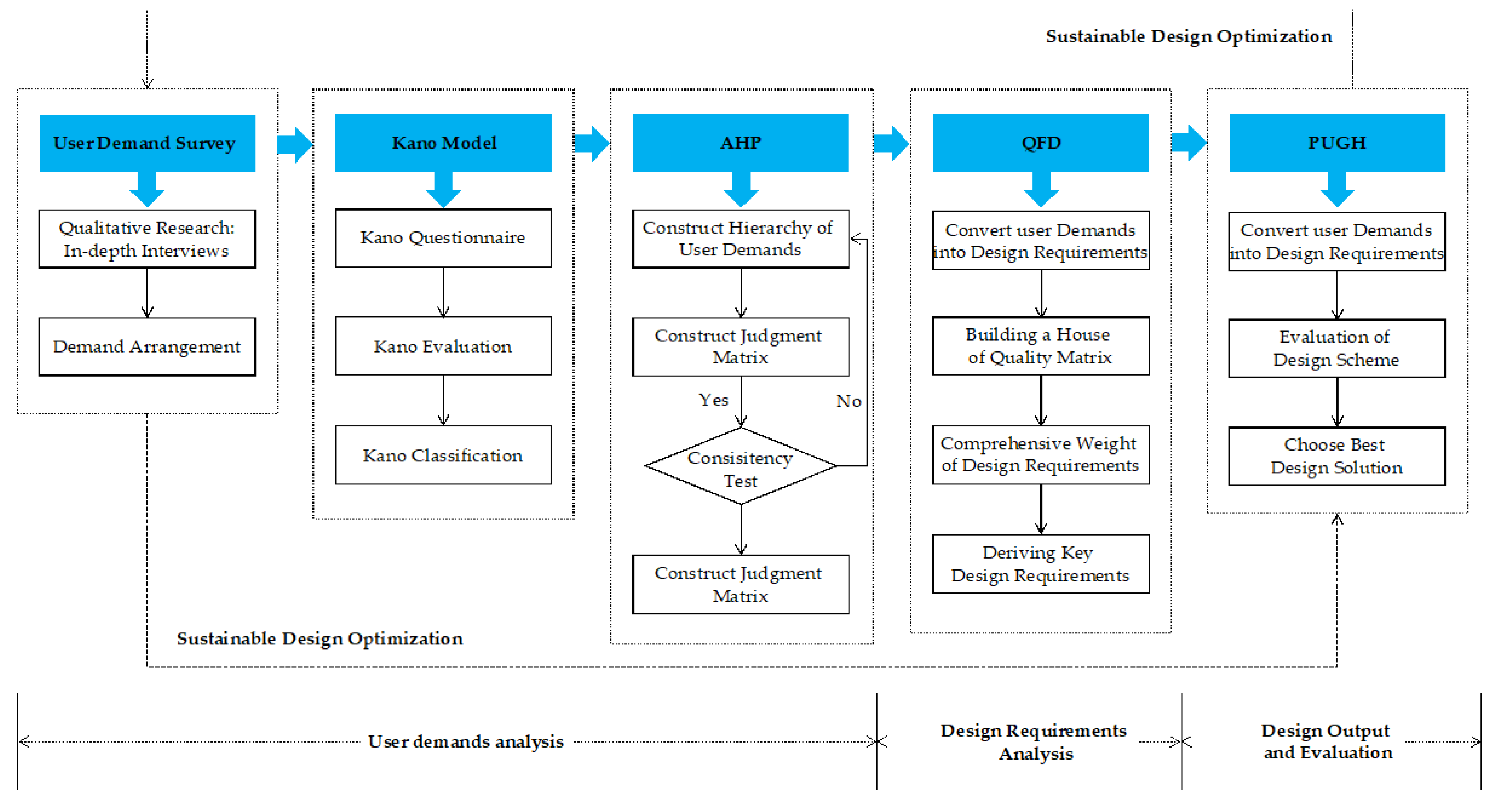
Figure 4.
Project A Interaction Interface.
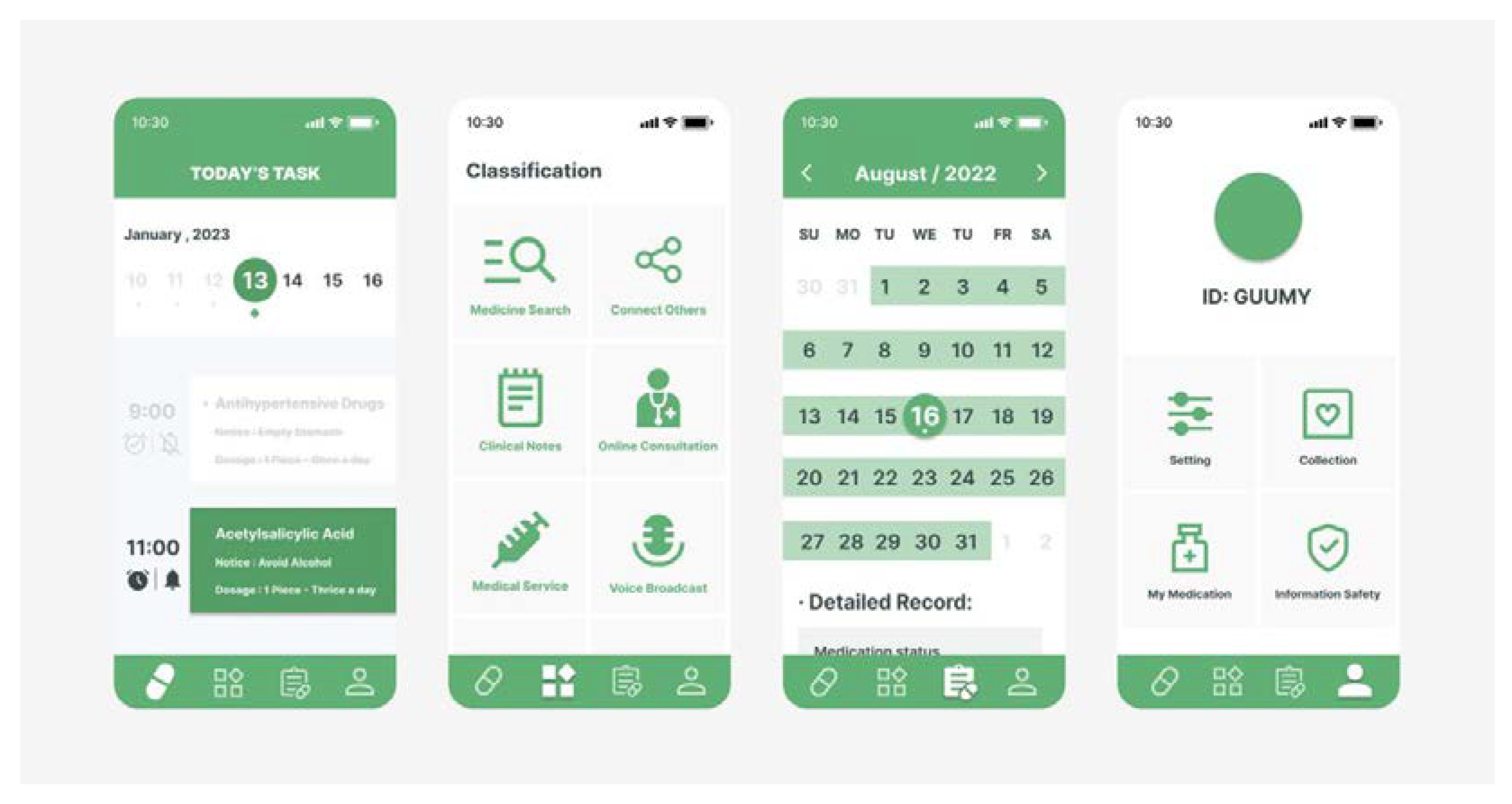
Table 4.
The 1~9 scale method
| Scale | Implication |
|---|---|
| 1 | By comparison, the two elements are equally important |
| 3 | By comparison, one element is slightly more important than the other |
| 5 | By comparison, one element is obviously more important than the other |
| 7 | By comparison, one element is strongly more important than the other |
| 9 | By comparison, one element is extremely more important than the other |
| 2,4,6,8 | The median value of the above importance |
Table 6.
User Information Form.
| Category | Item | Frequency | % |
|---|---|---|---|
| Gender | Male | 17 | 44.73 |
| Female | 21 | 55.27 | |
| Age | 60-65 | 23 | 60.53 |
| 65-70 | 11 | 28.95 | |
| 70-75 | 4 | 10.52 | |
| Types of daily medications | 2 or 3 More than 3 |
20 18 |
52.63 47.37 |
| Use Experience | Use | 15 | 39.47 |
| Have not used | 23 | 60.53 |
Table 7.
Interview outline.
| Category | Questions |
|---|---|
| Basic Information |
|
| |
| Function Requirements |
|
| |
| |
| Operating Habits |
|
| Interface Preference |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



