
Submitted:
20 May 2023
Posted:
22 May 2023
You are already at the latest version
Abstract
Several noninvasive vascular biomarkers have been suggested for improving the risk stratification for atherothrombotic events. To identify biomarkers suitable for detecting intermediate-risk individuals who might benefit from lipid-lowering treatment (L-LT) in primary prevention, the present study tested the association of plasma LDL-cholesterol with coronary artery calcification (CAC) Agatston score, high carotid and femoral intima-media thickness (IMT), low carotid distensibility and high carotid-femoral pulse-wave velocity in 260 asymptomatic individuals at intermediate cardiovascular risk and free of diabetes and L-LT. High or low vascular biomarkers were considered when their value was above the 95th or below the 5th percentile, respectively, of the distribution in the healthy or in the study population. LDL-cholesterol was independently associated with the CAC score =0 (OR 0.67; 95%CI 0.48-0.92, P=0.01), CAC score >100 (1.59; 1.08-2.39, P=0.01) and with high femoral IMT (1.89; 1.19-3.06, P<0.01), but not with other biomarkers. Our data confirm that in the presence of CAC score =0 in individuals at intermediate risk, L-LT can be avoided, while it should be used in those with CAC score >100. Femoral artery IMT could represent a useful biomarker for decision regarding L-LT, however the reference values according to sex and age should be established in a large healthy population
Keywords:
lipid-lowering treatment
; primary prevention
; coronary calcium
; intima-media thickness
; arterial stiffness
; carotid artery
; femoral artery
1. Introduction
Low-density lipoprotein cholesterol (LDL-C) is the most abundant atherogenic lipoprotein in plasma and its infiltration of the arterial wall is considered a key event in the initiation and progression of atherosclerotic process. Increased plasma LDL-C levels are causally related to atherosclerotic cardiovascular (CV) disease [1] and lowering LDL-C values by lifestyle or therapeutic interventions reduces the risk of CV events, both in primary and secondary prevention [1,2,3,4,5].
2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease [6] suggests statin treatment not only in individuals with diabetes, very high LDL-C (>190 mg/dl) or high 10-year risk of CV disease (≥20%), but even in individuals at intermediate CV risk (≥7.5-20%), in presence of risk enhancers like coronary artery calcification (CAC). In absence of CAC, statin therapy can be avoided, while with CAC score >100 statins are recommended at any age. Quantification of coronary artery calcification by means of Agatston CAC score is currently used as a sensitive predictor of CV risk [7,8], yet its value for monitoring the efficacy of statin treatment is limited, since numerous studies have shown that statins accelerate the calcification of atherosclerotic lesions [9,10]. In fact, statins have above all a plaque-stabilizing effect characterized by a reduction of lipid-rich core and inflammation and increase in calcification [11]. Therefore, repeated computed tomography scans for assessing the response to statins therapy are probably not appropriate, taking into account also the cumulative radiation dose [12].
Other noninvasive vascular biomarkers, like carotid and femoral intima-media thickness (IMT) and plaques or carotid and aortic stiffness have been proposed for risk estimation [22] and decision-making regarding statin treatment as well as for monitoring the response to therapy. Various studies have demonstrated that statins can slow the progression of carotid IMT and improve arterial stiffness [13,14,15,16]. Yet, observed favorable effects may not be necessarily related to the main action of statins, i.e., decrease in serum LDL-C levels. Statins show pleiotropic effects that include the reduction of inflammatory and proinflammatory cytokines and reactive oxygen species, inhibition of smooth muscle cell proliferation, improvement of endothelial function and lowering of blood pressure (BP) [17,18,19,20,21]. All these mechanisms could participate on reduction of arterial wall thickness and stiffness.
To identify noninvasive vascular biomarkers that could improve the selection of candidates for statin therapy in primary prevention [22], the present study evaluated the association of vascular biomarkers with plasma levels of LDL-C in an asymptomatic population at intermediate 10-year risk of CV disease, free of diabetes and lipid-lowering therapy and with LDL-C levels <190mg/dl. In such a population we identified the individuals with CAC score =0 and CAC score >100, high common carotid artery (CCA) or common femoral artery (CFA) IMT as well as those with low CCA distension and high carotid-femoral pulse wave velocity (cfPWV). High or low vascular biomarkers were considered when their value was above the 95th percentile or below the 5th percentile [23], respectively, of distribution in healthy population (if data in healthy population were available) or in the study population (if data in healthy population were not available).
2. Materials and Methods
2.1. Study population and protocol
The study population is a part of population enrolled in the prospective cohort study “MHeLP, Montignoso Heart-Lung Project” aimed to define the predictive value of CAC score for CV events in a community-based (the village of Montignoso, Tuscany, Italy) general population. Original population comprised 638 individuals. For the purpose of this study, we included only individuals with age 40-75 years, free of CV symptoms, lipid-lowering therapy and diabetes, with plasma LDL-C levels <190 mg/dl and at intermediate 10-year risk of CV disease as estimated by Framingham Risk Score. The final population consists of 260 individuals.
All individuals underwent an examination protocol that included anthropometry, brachial BP measurements, a fasting blood test, ECG, a high-resolution carotid and femoral ultrasound and computed tomography scan. In 182 individuals the measurement of carotid-femoral pulse wave-velocity was also performed. Hypertension was defined as systolic BP >140 mmHg and/or diastolic BP >90 mmHg or hypertensive treatment [24].
2.2. Body Size and BP Measurement
Body weight and height were measured and body mass index (BMI) was calculated. Waist circumference was measured as the narrowest circumference between the lower rib margin and anterior superior iliac crest. Brachial BP was measured at two different visits by a validated digital electronic tensiometer (Omron, model 705cp, Kyoto, Japan) in participants seated for at least 10 min, using regular or large adult cuffs according to the arm circumference. At both visits, two measurements were taken, separated by 2-minute intervals and the average was calculated. The average of two separate visits was used to estimate BP (mmHg). Pulse pressure was calculated as the difference between systolic and diastolic BP.
2.3. Assessment of 10-year risk of CV disease
A 10-year risk of CV disease was estimated by Framingham risk score prediction model that considers age, total cholesterol, high-density lipoprotein cholesterol (HDL-C), brachial systolic BP, ongoing treatment of hypertension, smoking and diabetes status [25]. The risk was classified as intermediate when the 10-years risk of CV disease ranged between 7.5 and 20% [6].
2.4. Coronary calcium score (CAC)
A low dose radiation scan without contrast agent was done (120 KV, 60 mA) by a 64-detector scanner (Aquilion 64; Toshiba Medical Systems, Otawara, Japan) (2-3 mSv estimated dosimetry, with 1- and 3-mm collimation and reconstruction thickness, respectively. Prospective electrocardiographic triggering in sequential slice mode was used for scanning of the heart. CAC score was calculated by the method of Agatston [26] with a dedicated program available (Vitrea 2.0; Vital Images Inc., Minnetonka, MN, USA). For the purpose of this study, we identified
2.5. Individuals with CAC score =0 and CAC score >100.
2.5.1. Vascular Examination
All vascular examinations were carried out by the same operator (G.J.) in a quiet room with a stable temperature of 22° on individuals resting comfortably for at least 15 minutes in the supine position. All individuals were asked to abstain from cigarette smoking, caffeine and alcohol consumption and vigorous physical activity for 24 hours.
Carotid ultrasound was performed on the right CCA using an ultrasound scanner equipped with a 10 MHz linear probe (MyLab 70, Esaote, Genova, Italy) and implemented with a previously validated radiofrequency-based tracking of arterial wall (QIMT®, QAS®) that allows an automatic and real-time determination of far-wall CCA IMT, CCA inter-adventitial diameter (IAD) and distension with a high spatial and temporal resolution (sampling rate of 550 Hz on 32 lines). CCA IMT, IAD and distension were measured within a rectangular ROI placed approximately 1 cm before the flow divider. IMT was defined as the distance between the lumen-intima and media-adventitia interfaces of the far (posterior) wall. Distension coefficient (DC) was calculated as previously described [27].
Femoral ultrasound was performed on the right common femoral artery (CFA) using the same ultrasound scanner with radiofrequency-based tracking of arterial wall. Far wall IMT was measured within a rectangular ROI placed approximately 1 cm before the flow divider.
To identify individuals with high CCA IMT, the sex- and age-specific normality tables deriving from IMT measurements performed by the same radiofrequency-based system in 4234 healthy men and women were used [28] and a cut-point of the 95th percentile for given sex and age was adopted [23]. To identify individuals with low CCA DC, the sex- and age-specific normality tables deriving from DC measurements performed by the same radiofrequency-based system in 3601 healthy men and women were used [27] and a cut-point of the 5th percentile for given sex and age was adopted [23]. Since no normalcy data were published for CFA IMT, a cut-point of the 95th percentile of CFA IMT distribution in our population was adopted for defining high CFA IMT.
Radiofrequency-derived measures represent an average over 6 consecutive cardiac beats. The mean of two acquisitions was used for statistical analysis. BP was measured at the left brachial artery (Omron, Kyoto, Japan) during each acquisition of the distension curves. Intra-individual variability of acquisitions was evaluated in 25 volunteers, in whom the acquisitions were performed in two different sessions separated by 30 min. Brachial pulse pressure was comparable between the different acquisitions (P=0.88). Intra-individual variability of CCA IMT, CCA distension and CFA IMT was 6.7±4.2, 8.7±6.4% and 8.1±5.4%, respectively.
Carotid-femoral pulse wave velocity (cfPWV) was measured in 182 participants according to current guidelines [29] using the Complior device (Alam Medical, Vincennes, France). To identify individuals with high cfPWV, the sex-, age- and mean BP-specific normality tables deriving from cfPWV measurements performed in 2158 healthy men and women were used [30] and a cut-point of the 95th percentile for given sex, age and mean BP was adopted [23]. Intra-individual variability of carotid-femoral PWV measurement was 4.3±2.8%.
2.5.2. Statistical Analysis
Data are expressed as mean±SD, categorical data as percentages. Variables with skewed distribution were summarized as median [interquartile range], and were logarithmically transformed for parametric statistical analysis. Multivariate logistic regression was performed to identify risk factors associated with CAC score =0, CCA score >100, high CCA IMT, high CFA IMT, low CCA DC and high cfPWV. Results are given as odds ratio (OR) and 95% confidence interval (CI). OR were calculated for 1SD of the continuous variable. Statistical tests were two-sided, and significance was set at a value of P<0.05.
3. Results
Characteristics of study population are reported in Table 1. Table 2 reports data on CAC score, CCA IMT and distensibility, CFA IMT and cfPWV. One hundred and seventy-four individuals had CAC score =0, 36 had CAC score >100, 45 had high CCA IMT, 15 had low CCA DC, 25 had high CFA IMT, and 27 had high cfPWV.
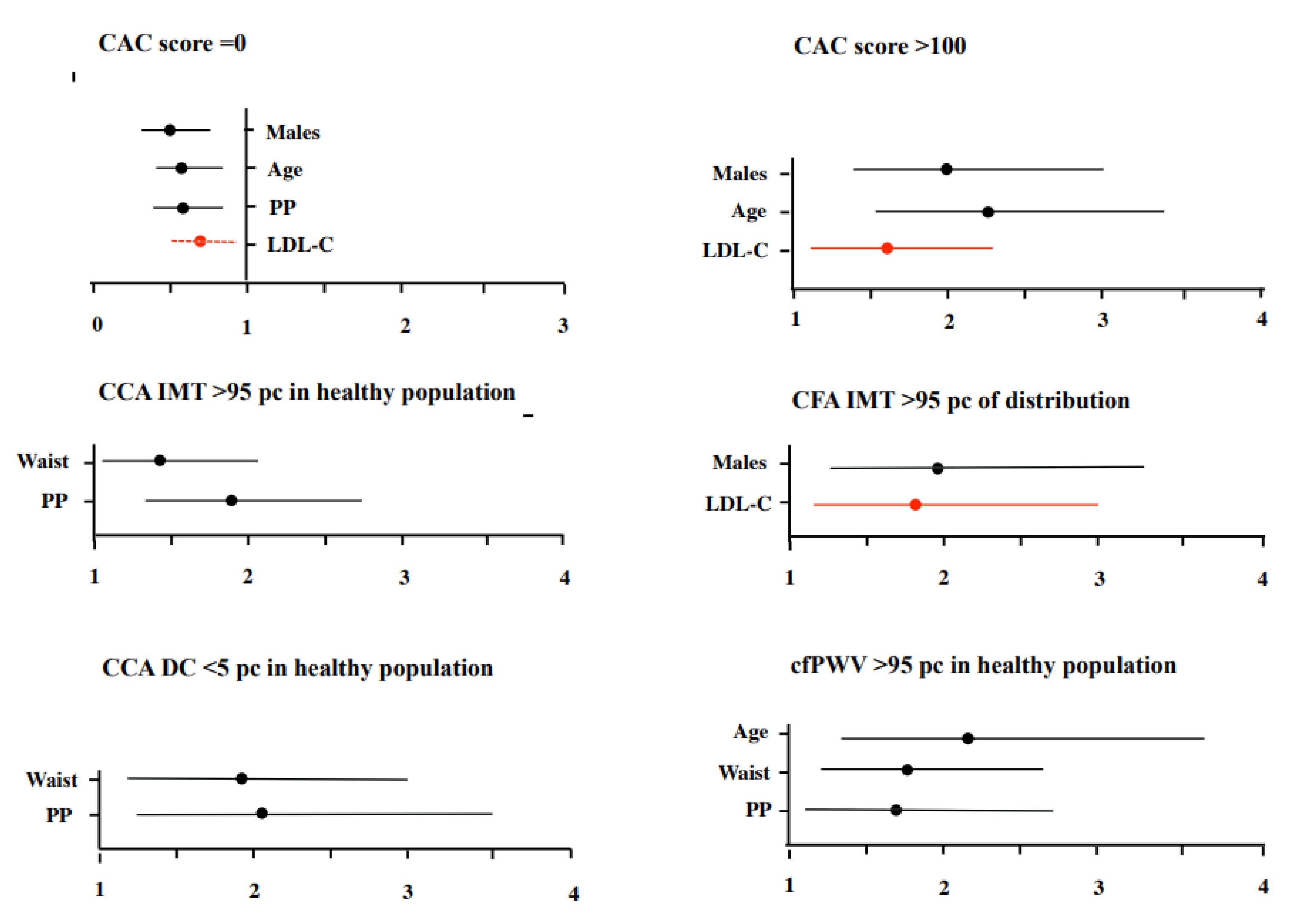
Figure 1.
Risk factors associated with CACs score =0, CAC score >100, high CCA IMT, high CFA IMT, low CCA DC and high cfPWV. Odds ratios are calculated for 1SD of the continuous variable. Figure 1 reports risk factors associated with CAC score =0, CAC score >100, high CCA IMT or CFA IMT, low CCA DC and high cfPWV. LDL-C was independently associated with CAC score =0, CAC score >100 and high CFA IMT, but not with high CCA IMT, low CCA DC or high cfPWV. Neither HDL-C or triglycerides were related to any vascular biomarker.
Figure 1.
Risk factors associated with CACs score =0, CAC score >100, high CCA IMT, high CFA IMT, low CCA DC and high cfPWV. Odds ratios are calculated for 1SD of the continuous variable. Figure 1 reports risk factors associated with CAC score =0, CAC score >100, high CCA IMT or CFA IMT, low CCA DC and high cfPWV. LDL-C was independently associated with CAC score =0, CAC score >100 and high CFA IMT, but not with high CCA IMT, low CCA DC or high cfPWV. Neither HDL-C or triglycerides were related to any vascular biomarker.
4. Discussion
In our asymptomatic population at intermediate CV risk, LDL-C was associated with coronary calcification and with CFA IMT in the highest 5 percent of distribution. Neither high CCA IMT, low carotid distensibility or high aortic stiffness were associated with plasma lipids.
These results confirm the association between LDL-C levels and coronary calcification in asymptomatic patients at intermediate CV risk. Indeed, the 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease [6] does not suggest statin therapy in intermediate-risk individuals with CAC score =0 and recommends to initiate statin therapy at any age in intermediate-risk individuals with CAC score >100. The relationship between LDL-C exposure and vascular calcification has been demonstrated both in clinical and experimental studies and reflects the fact that in the arterial wall are present cells capable of osteoblastic differentiation and mineralization and that oxidized lipids accumulated in the subendothelial space induce differentiation of these cells and promote the calcification [31,32]. However, calcification in atherosclerotic lesions is associated with both progression of disease (microcalcification) and healing of inflammation (macrocalcification), and statins have been shown to reduce arterial wall inflammation [33]. In the Heinz Nixdorf Recall Study, statin intake enhanced CAC progression, mostly in the less advanced stage of atherosclerosis, but this progression did not increase the risk for coronary events [10]. A meta-analysis of 7 studies suggested that in asymptomatic populations at high risk of CV diseases, statins do not reduce or enhance CAC as measured by Agatston score, but slightly slow down CAC progression, above all in individuals with CAC score >400 [34]. Coronary calcification may therefore help to identify candidates for statin therapy, but its value for monitoring the effectiveness of treatment is less clear.
Within other vascular biomarkers tested in our study, neither high CCA IMT, low CCA distensibility or high aortic stiffness were related to plasma LDL-C. On the other hand, all these biomarkers were independently associated with pulse pressure and waist circumference. BP is an established determinant of carotid and aortic stiffness [35] and different studies have suggested that increase in carotid IMT reflects, rather than atherosclerosis, a physiologic remodeling aimed at maintaining stable circumferential wall stress as BP increases [36,37]. Since one of the pleiotropic effects of statins is BP reduction [19], above all in individuals with higher BP and in users of anti-hypertensive medication [38,39], deceleration of carotid IMT progression and improvement in arterial stiffness with statins therapy, as reported in various studies [13,14,15,16], could be partially explained by a decrease in BP. Furthermore, central obesity is related to low-grade systemic inflammation [40,41] and in our study all three vascular biomarkers were independently associated with waist circumference. Therefore, anti-hypertensive and anti-inflammatory action of statins might explain the positive effect of stain therapy on elastic arteries structure and function, independent of LDL-C levels.
In contrast to CCA IMT, high CFA IMT was independently associated with plasma LDL-C. Previous studies comparing the relationships between risk factors and IMT in carotid and femoral arteries did not observe significant differences. In the AXA study [42] both carotid and femoral IMT were associated with age, BMI, BP, total cholesterol, triglycerides, glucose and smoking, though the association with BP was stronger for elastic than for muscular artery. In a study including normocholesterolemic and hypercholesterolemic subjects, carotid and femoral IMTs increased with total cholesterol (r= 0.35, P<0.001 for both arteries) and LDL-C (r= 0.33, P< 0.001 and r = 0.34, P< 0.001, respectively) in a similar way [43]. Yet, in the study evaluating the impact of 2-year simvastatin treatment on carotid and femoral IMT in patients with familial hypercholesterolemia, a more important IMT regression was observed in femoral as compared to carotid artery (-0.283 vs. -0.053 mm), and hypercholesterolemic patients with history of CV diseases had significantly higher CFA IMT at baseline as compared to patients without CV disease (P<0.001), while the differences in CCA IMT were less significant (P=0.01) [44]. Based on these results authors suggested that femoral artery could be more sensitive to reduction of LDL-C levels and that a larger regression of femoral IMT could be clinically relevant, since the association between IMT and CV disease was more significant in the femoral than in the carotid artery.
4.1. Study limitations
We cannot evaluate the association between plasma lipid levels and carotid or femoral plaques since the prevalence of plaques in our asymptomatic participants at intermediate CV risk was very low. C-reactive protein or other markers of systemic inflammation were not assessed.
4.2. Conclusions
Within vascular biomarkers that can be used in primary prevention for decision regarding statin therapy in asymptomatic individuals at intermediate 10-year risk of CV disease, only coronary calcification and CFA IMT in the highest 5 percent of distribution were independently related to plasma LDL-C levels. For clinical use, the reference values of CFA IMT according to sex and age should be established in a large healthy population, as already done for CCA IMT. High CCA IMT, low CCA distention and high aortic stiffness were not associated with blood lipids, but with pulse pressure and waist circumference. The latter observation suggests that positive effect of statins on elastic artery wall thickness and stiffness, which has been described by others, could be independent on LDL-C and mediated by their anti-hypertensive and anti-inflammatory actions. Taken together, our data indicate that different vascular biomarkers might reflect the impact of different risk factors on CV systems and that assessment of more than one biomarker could provide a more accurate estimate of CV risk.
Author Contributions
MK: CP, DC contributed to the study design. DC, CM, GJ, SC, DDL contributed to the acquisition and analysis of data. MK and CP contributed to the interpretation of data. All authors critically revised the paper and gave their final approval.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, and was approved by the by Tuscany Region North West Area Ethical Committee.
Informed Consent Statement
All individuals gave their informed consent to participate.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical and privacy reasons.
Conflicts of Interest
MK is responsible of clinical studies in Esaote SpA. DDL is currently affiliated with Terarecon Inc., Durham, NC 27703
References
- von Birgelen, C.; Hartmann, M.; Mintz, G.S.; Baumgart, D.; Schmermund, A.; Erbel, R. Relation between progression and regression of atherosclerotic left main coronary artery disease and serum cholesterol levels as assessed with serial long-term (> or =12 months) follow-up intravascular ultrasound. Circulation 2003, 108, 2757–2762. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Nicholls, S.J.; Sipahi, I.; Libby, P.; Raichlen, J.S.; Ballantyne, C.M.; Davignon, J.; Erbel, R.; Fruchart, J.C.; Tardif, J.C.; Schoenhagen, P.; Crowe; Cain, V.; Wolski, K.; Goormastic, M.; Tuzcu, E.M.; ASTEROID Investigators. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. JAMA 2006, 295, 1556–1565. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Tuzcu, E.M.; Sipahi, I.; Grasso, A.W.; Schoenhagen, P.; Hu, T.; Wolski, K.; Crowe, T.; Desai, M.Y.; Hazen, S.L.; Kapadia, S.R.; Nissen, S.E. Statins, high-density lipoprotein cholesterol, and regression of coronary atherosclerosis. JAMA 2007, 297, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; Graham, I.M.; Halliday, A.; Landmesser, U.; Mihaylova, B.; Pedersen, T.R; Riccardi, G.; Richter, D.J.; Sabatine, M.S.; Taskinen, M.R.; Tokgozoglu, L.; Wiklund, O.; ESC Scientific Document Group. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.M.; Choi, S.; Kim, K.; Kim, S.M.; Lee, G.; Park, S.Y.; Kim, Y.Y.; Son, J.S.; Yun, J.M.; Park, S.M. Effect of change in total cholesterol levels on cardiovascular disease among young adults. J Am Heart Assoc 2018, 7, e008819. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; Michos, E.D.; Miedema, M.D.; Muñoz, D.; Smith, S.C. Jr.; Virani, S.S.; Williams, K.A. Sr.; Yeboah, J.; Ziaeian, B. 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Sarwar, A.; Shaw, L.J.; Shapiro, M.D.; Blankstein, R.; Hoffmann, U.; Cury, R.C.; Abbara, S.M; Brady, T.J.; Budoff, M.J.; Blumenthal, R.S.; Nasir, K. Diagnostic and prognostic value of absence of coronary artery calcification. JACC Cardiovasc Imaging 2009, 2, 675–688. [Google Scholar] [CrossRef]
- Lo-Kioeng-Shioe, M.S.; Rijlaarsdam-Hermsen, D.; van Domburg, R.T.; Hadamitzky, M.; Lima, J.A.C.; Hoeks, S.E.; Deckers, J.W. Prognostic value of coronary artery calcium score in symptomatic individuals: A meta-analysis of 34,000 subjects. Int J Cardiol 2020, 299, 56–62. [Google Scholar] [CrossRef]
- Henein, M.; Granåsen, G.; Wiklund, U.; Schmermund, A.; Guerci, A.; Erbel, R.; Raggi, P. High dose and long-term statin therapy accelerate coronary artery calcification. Int J Cardiol 2015, 184, 581–586. [Google Scholar] [CrossRef]
- Dykun, I.; Lehmann, N.; Kälsch, H.; Möhlenkamp, S.; Moebus, S.; Budde, T.; Seibel, R.; Grönemeyer, D.; Jöckel, K.H.; Erbel, R.; Mahabadi, A.A. Statin medication enhances progression of coronary artery calcification: The Heinz Nixdorf Recall Study. J Am Coll Cardiol 2016, 68, 2123–2125. [Google Scholar] [CrossRef]
- Di Giovanni, G.; Nicholls, S.J. Intensive lipid lowering agents and coronary atherosclerosis: Insights from intravascular imaging. Am J Prev Cardiol 2022, 11, 100366. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.P.; Einstein, A.J.; Berrington de González, A. Coronary artery calcification screening: estimated radiation dose and cancer risk. Arch Intern Med 2009, 169, 1188–1194. [Google Scholar] [CrossRef]
- Crouse, J.R., 3rd; Raichlen, J.S.; Riley, W.A.; Evans, G.W.; Palmer, M.K.; O'Leary, D.H.; Grobbee, D.E.; Bots, M.L.; METEOR Study Group. Effect of rosuvastatin on progression of carotid intima-media thickness in low-risk individuals with subclinical atherosclerosis: the METEOR Trial. JAMA 2007, 297, 1344–1353. [Google Scholar] [PubMed]
- Daida, H.; Nohara, R.; Hata, M.; Kaku, K.; Kawamori, R.; Kishimoto, J.; Kurabayashi, M.; Masuda, I.; Sakuma, I.; Yamazaki, T.; Yokoi, H.; Yoshida, M.; Justification for Atherosclerosis Regression Treatment (JART) Investigators. Can intensive lipid-lowering therapy improve the carotid intima-media thickness in Japanese subjects under primary prevention for cardiovascular disease?: The JART and JART extension subanalysis. J Atheroscler Thromb 2014, 21, 739–754. [Google Scholar] [CrossRef] [PubMed]
- Smilde, T.J.; van den Berkmortel, F.W.; Wollersheim, H.; van Langen, H. Kastelein, J.J.; Stalenhoef, A.F. The effect of cholesterol lowering on carotid and femoral artery wall stiffness and thickness in patients with familial hypercholesterolaemia. Eur J Clin Invest 2000, 30, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Upala, S.; Wirunsawanya, K.; Jaruvongvanich, V.; Sanguankeo, A. Effects of statin therapy on arterial stiffness: A systematic review and meta-analysis of randomized controlled trial. Int J Cardiol 2017, 227, 338–341. [Google Scholar] [PubMed]
- Koushki, K.; Shahbaz, S.K.; Mashayekhi, K.; Sadeghi, M.; Zayeri, Z.D.; Taba, M.Y.; Banach, M.; Al-Rasadi, K.; Johnston, T.P.; Sahebkar, A. Anti-inflammatory action of statins in cardiovascular disease: the role of inflammasome and toll-like receptor pathways. Clin Rev Allergy Immunol 2021, 60, 175–199. [Google Scholar] [CrossRef]
- Davignon, J.; Jacob, R.F.; Mason, R.P. The antioxidant effects of statins. Coron Artery Dis 2004, 15, 251–258. [Google Scholar]
- Liao, J.K.; Laufs, U. Pleiotropic effects of statins. Annu Rev Pharmacol Toxicol 2005, 45, 89–118. [Google Scholar] [CrossRef]
- Bellosta, S.; Arnaboldi, L.; Gerosa, L.; Canavesi, M.; Parente, R.; Baetta, R.; Paoletti, R.; Corsini, A. Statins effect on smooth muscle cell proliferation. Semin Vasc Med 2004, 4, 347–356. [Google Scholar] [CrossRef]
- Strazzullo, P.; Kerry, S.M.; Barbato, A.; Versiero, M.; D'Elia, L.; Cappuccio, F.P. Do statins reduce blood pressure?: A meta-analysis of randomized, controlled trials. Hypertension 2007, 49, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Vlachopoulos, C.; Xaplanteris, P.; Aboyans, V.; Brodmann, M.; Cífková, R.; Cosentino, F.; De Carlo, M.; Gallino, A.; Landmesser, U.; Laurent, S.; Lekakis, J.; Mikhailidis, D.P.; Naka, K.K.; Protogerou, A.D.; Rizzoni, D.; Schmidt-Trucksäss, A.; Van Bortel, L.; Weber, T.; Yamashina, A.; Zimlichman, R.; Boutouyrie, P.; Cockcroft, J.; O'Rourke, M.; Park, J.B.; Schillaci, G.; Sillesen, H.; Townsend, R.R. The role of vascular biomarkers for primary and secondary prevention. A position paper from the European Society of Cardiology Working Group on peripheral circulation: Endorsed by the Association for Research into Arterial Structure and Physiology (ARTERY) Society. Atherosclerosis 2015, 241, 507–532. [Google Scholar] [PubMed]
- Vasan, R.S. Biomarkers of cardiovascular disease: molecular basis and practical considerations. Circulation 2006, 113, 2335–2362. [Google Scholar] [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redón, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; Galderisi, M.; Grobbee, D.E.; Jaarsma, T.; Kirchhof, P.; Kjeldsen, S.E.; Laurent, S.; Manolis, A.J.; Nilsson, P.M.; Ruilope, L.M.; Schmieder, R.E.; Sirnes, P.A.; Sleight, P.; Viigimaa, M.; Waeber, B.; Zannad, F.; Task Force Members. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2013, 31, 1281–1357. [Google Scholar] [CrossRef] [PubMed]
- D'Agostino, R.B. Sr; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Agatston, A.S.; Janowitz, W.R; Hildner, F.J.; Zusmer, N.R.; Viamonte, M. Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990, 15, 827–832. [Google Scholar] [CrossRef]
- Engelen, L.; Bossuyt, J.; Ferreira, I.; van Bortel, L.M.; Reesink, K.D.; Segers, P.; Stehouwer, C.D.; Laurent, S.; Boutouyrie, P. Reference Values for Arterial Measurements Collaboration. Reference values for local arterial stiffness. Part A: carotid artery. J Hypertens 2015, 33, 1981–1996. [Google Scholar] [CrossRef]
- Engelen, L.; Ferreira, I.; Stehouwer, C.D.; Boutouyrie, P.; Laurent, S. Reference Values for Arterial Measurements Collaboration. Reference intervals for common carotid intima-media thickness measured with echotracking: relation with risk factors. Eur Heart J 2013, 34, 2368–2380. [Google Scholar] [CrossRef]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.; Protogerou, A.D.; Schillaci, G.; Segers, P.; Vermeersch, S.; Weber, T.; Artery Society; European Society of Hypertension Working Group on Vascular Structure and Function; European Network for Noninvasive Investigation of Large Arteries. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J Hypertens 2012, 30, 445–458. [Google Scholar] [CrossRef]
- Baldo, M.P.; Cunha, R.S.; Molina, M.D.C.B.; Chór, D.; Griep, R.H.; Duncan, B.B.; Schmidt, M.I.; Ribeiro, A.L.P.; Barreto, S.M.; Lotufo, P.A.; Bensenor, I.M.; Pereira, A.C.; Mill, J.G. Carotid-femoral pulse wave velocity in a healthy adult sample: The ELSA-Brasil study. Int J Cardiol 2018, 251, 90–95. [Google Scholar] [CrossRef]
- Demer, L.L. Cholesterol in vascular and valvular calcification. Circulation 2001, 104, 1881–1883. [Google Scholar] [CrossRef]
- Parhami, F.; Morrow, A.D.; Balucan, J.; Leitinger, N.; Watson, A.D.; Tintut, Y.; Berliner, J.A; Demer, L.L. Lipid oxidation products have opposite effects on calcifying vascular cell and bone cell differentiation: a possible explanation for the paradox of arterial calcification in osteoporotic patients. Arterioscler Thromb Vasc Biol 1997, 17, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Shioi, A.; Ikari, Y. Plaque calcification during atherosclerosis progression and regression. J Atheroscler Thromb 2018, 25, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Lai, R.; Ju, J.; Lin, Q.; Xu, H. Coronary artery calcification under statin therapy and its effect on cardiovascular outcomes: A systematic review and meta-analysis. Front Cardiovasc Med 2020, 7, 600497. [Google Scholar] [CrossRef] [PubMed]
- Kozakova, M.; Morizzo, C.; Guarino, D.; Federico, G.; Miccoli, M.; Giannattasio, C.; Palombo, C. The impact of age and risk factors on carotid and carotid-femoral pulse wave velocity. J Hypertens 2015, 33, 1446–1451. [Google Scholar] [CrossRef] [PubMed]
- Chiesa, S.T.; Charakida, M.; Georgiopoulos, G.; Dangardt, F.; Wade, K.H.; Rapala, A.; Bhowruth, D.J.; Nguyen, H.C.; Muthurangu, V.; Shroff, R.; Davey Smith, G.; Lawlor, D.A.; Sattar, N.; Timpson, N.J.; Hughes, A.D.; Deanfield, J.E. Determinants of intima-media thickness in the young: The ALSPAC Study. JACC Cardiovasc Imaging 2021, 14, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Kozakova, M.; Palombo, C.; Paterni, M.; Anderwald, C.H.; Konrad, T.; Colgan, M.P.; Flyvbjerg, A.; Dekker, J.; Relationship between Insulin Sensitivity Cardiovascular risk Investigators. Body composition and common carotid artery remodeling in a healthy population. J Clin Endocrinol Metab 2008, 93, 3325–3332. [Google Scholar] [CrossRef] [PubMed]
- Bautista, L.E. Blood pressure-lowering effects of statins: who benefits? J Hypertens 2009, 27, 1478–1484. [Google Scholar] [CrossRef]
- Briasoulis, A.; Agarwal, V.; Valachis, A.; Messerli, F.H. Antihypertensive effects of statins: a meta-analysis of prospective controlled studies. J Clin Hypertens (Greenwich) 2013, 15, 310–320. [Google Scholar] [CrossRef]
- Steene-Johannessen, J.; Kolle, E.; Reseland, J.E.; Anderssen, S.A.; Andersen, L.B. Waist circumference is related to low-grade inflammation in youth. Int J Pediatr Obes 2010, 5, 313–319. [Google Scholar] [CrossRef]
- Ackermann, D.; Jones, J.; Barona, J.; Calle, M.C.; Kim, J.E.; LaPia, B.; Volek, J.S.; McIntosh, M.; Kalynych, C.; Najm, W.; Lerman, R.H.; Fernandez, M.L. Waist circumference is positively correlated with markers of inflammation and negatively with adiponectin in women with metabolic syndrome. Nutr Res 2011, 3, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Gariepy, J.; Salomon, J.; Denarié, N.; Laskri, F.; Mégnien, J.L.; Levenson, J.; Simon, A. Sex and topographic differences in associations between large-artery wall thickness and coronary risk profile in a French working cohort: the AXA Study. Arterioscler Thromb Vasc Biol 1998, 18, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Gariepy, J.; Simon, A.; Massonneau, M.; Linhart, A.; Levenson, J. Wall thickening of carotid and femoral arteries in male subjects with isolated hypercholesterolemia. PCVMETRA Group. Prevention Cardio-Vasculaire en Medecine du Travail. Atherosclerosis 1995, 113, 141–151. [Google Scholar] [CrossRef] [PubMed]
- de Sauvage Nolting, P.R.; de Groot, E.; Zwinderman, A.H.; Buirma, R.J.; Trip, M.D.; Kastelein, J.J. Regression of carotid and femoral artery intima-media thickness in familial hypercholesterolemia: treatment with simvastatin. Arch Intern Med 2003, 163, 1837–1841. [Google Scholar] [CrossRef]

Table 1.
Characteristics of Study Population.
| Mean±SD, Median[IR], n(%) | Range | |
|---|---|---|
| Male:Female | 119(46):141(54) | |
| Age (years) | 63±6 | 50-74 |
| BMI (kg/m2) | 26.9±3.9 | 17.3-51.7 |
| Waist circumference (cm) | 95±11 | 67-147 |
| Systolic BP (mmHg) | 136±14 | 105-180 |
| Pulse pressure (mmHg) | 61±13 | 30-95 |
| Total cholesterol (mmo/L) | 5.45±0.78 | 3.28-6.88 |
| LDL-cholesterol (mmo/L) | 3.42±0.6 | 1.66-4.85 |
| HDL-cholesterol (mmo/L) | 1.58±0.37 | 0.89-2.64 |
| Triglycerides (mmo/L) | 0.89[0.75] | 0.23-3.89 |
| Fasting glucose (mmo/L) | 5.36±0.49 | 4.44-6.77 |
| Current smoking (yes) | 43(17) | |
| Hypertension (yes) | 113(43) | |
| Hypertensive treatment (yes) | 38(15) |
Table 2.
CAC Score, CCA IMT and Distensibility, CFA IMT and Aortic Stiffness.
| Mean±SD, n(%) | Range | |
|---|---|---|
| CAC score =0 | 174(67) | |
| CAC score >100 | 36(14) | |
| CCA IMT (microns) | 731±135 | 459-1202 |
| CCA IMT >95th percentile | 45(17) | |
| CCA DC (10-3kPa-1) | 14.2±4.5 | 4.31-30.2 |
| CCA DC <5th percentile | 15(6) | |
| CFA IMT (microns) | 736±202 | 340-1671 |
| CFA IMT >95th percentile | 25(10) | |
| cfPWV (m/s) (n=182) | 9.4±2.4 | 4.1-23.6 |
| cfPWV >95th percentile (n=182) | 27(15) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



