
Submitted:
16 May 2023
Posted:
17 May 2023
You are already at the latest version
Abstract
Total bilateral Limbal Stem Cells Deficiency is a pathologic condition of the ocular surface due to the loss of corneal stem cells. Cultivated Oral Mucosa Epithelial Transplantation (COMET) is the only autologous successful treatment for this pathology in clinical application, although non-physiological peripheric corneal vascularization often occurs. Properly characterizing the regenerated ocular surface is needed for a reliable follow-up. So far, the univocal identification of transplanted oral mucosa had been challenging. Previously proposed markers were shown co-expressed by the different ocular surface epithelia in a homeostatic or perturbated environment. In this study, we compared the transcriptome profile of human oral mucosa, limbal and conjunctival cells, identifying PITX2 as a new marker that univocally distinguishes the transplanted oral tissue from the other epithelia. We validated PITX2 at RNA and protein levels to investigate 10-year follow-up cor-neal samples derived from a COMET-treated aniridic patient. Moreover, we found novel angiogenesis-related factors differentially expressed in the three epithelia and instrumental in explaining the neovascularization in COMET-treated patients. These results will support the follow-up analysis of patients transplanted with oral mucosa and provide new tools to understand the regeneration mechanism of the transplanted cornea.
Keywords:
aniridia
; biomarker
; COMET
; cornea
; LSCD
; neovascularization
; oral mucosa
; PITX2
; ocular surface
1. Introduction
Limbal stem cells (LSCs) play a major role in ocular surface homeostasis and are responsible for corneal regeneration, achieved through centripetal cell migration and differentiation from the limbus to the central cornea [1]. As a result of acquired (chemical/thermal burns) or genetic conditions, these cells can be partially or entirely lost, resulting in a pathology known as Limbal Stem Cell Deficiency (LSCD), where corneal opacity and conjunctivalization lead to visual impairment and blood vessels migration, otherwise absent over the central cornea [2,3]. With a total prevalence of 1-5:10000 individuals, LSCD received the orphan drug designation in 2008 (Orpha:171673) by the Committee for Orphan Medicinal Products [4,5,6].
Over the years, several treatments have been proposed to treat unilateral or partial bilateral LSCD, among which conjunctival limbal allograft (CLAL) [7], conjunctival limbal autograft (CLAU) [8], cultured limbal epithelial transplantation (CLET) [9] or simple limbal epithelial transplantation (SLET) [10].
The CLET treatment, consisting in the transplantation of autologous limbal cells cultured on fibrin and clinical-grade 3T3-J2 feeder cells, obtained conditional approval by the European Medicines Agency (EMA) [5,11] under the name of Holoclar® and resulted long-term effective in 85,19 % of the patients with partial LSCD [12,13]. However, none of these therapeutic options is feasible in the case of total bilateral LSCD, where the absence of LSCs available for ex vivo expansion implies the need for an alternative cell source.
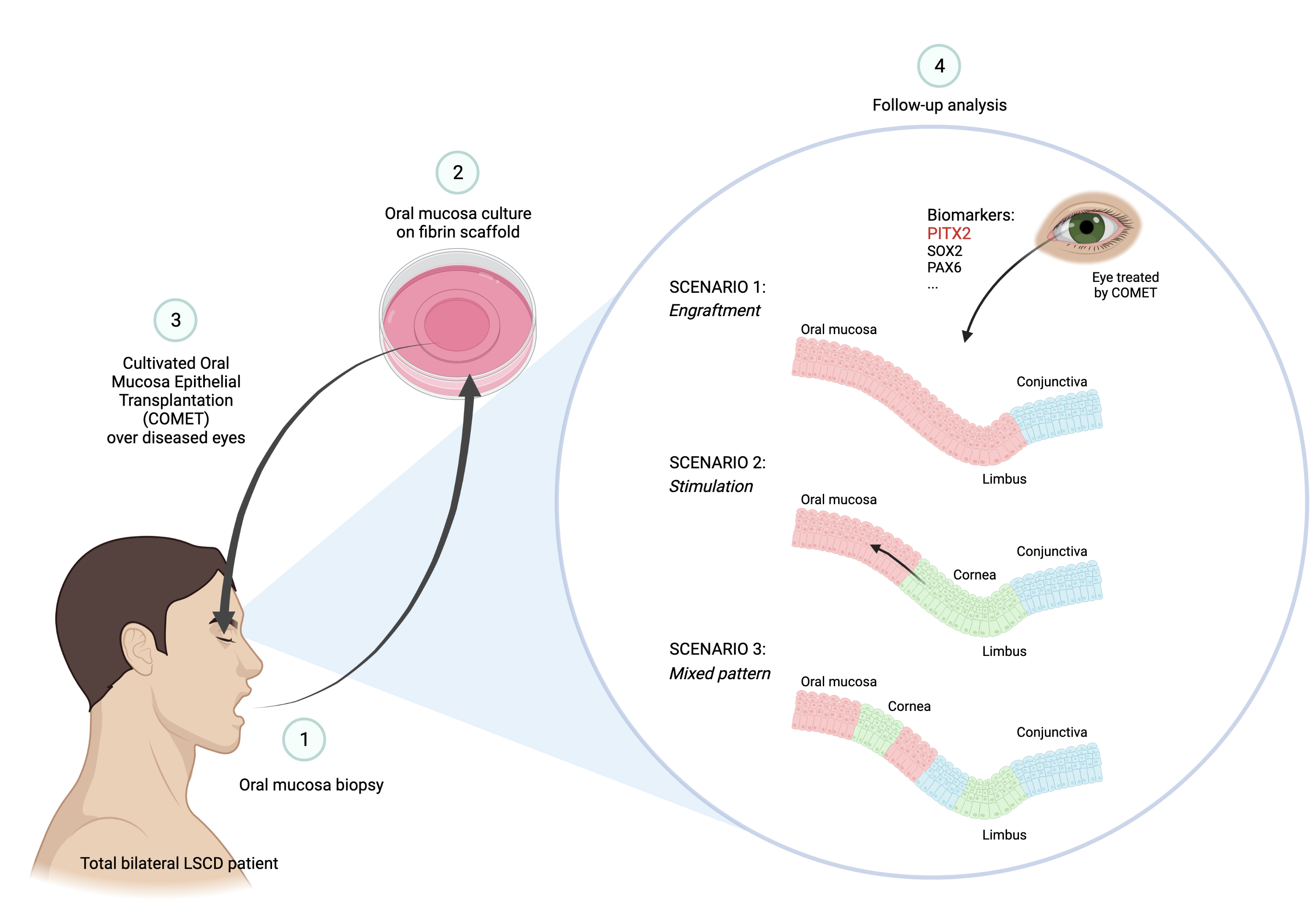
Cultivated oral mucosa epithelial transplantation (COMET) procedure proved to be well-tolerated and effective in patients affected by total bilateral LSCD [14]. However, after several years of application of this clinical procedure by different research groups, little is known about the mechanism of action that sustains corneal regeneration [15]. The two main hypotheses underlying the restoration of corneal transparency and visual acuity are the engraftment of oral mucosal transplanted cells with subsequent replacement of the epithelium ("engraftment” hypothesis), or the stimulation of few residual not detectable LSCs to proliferate and restore the ocular surface (“stimulation” hypothesis) [16].
Different studies in animal models supported both hypotheses. Transplantation of oral tissue from GFP-tagged rats onto ocular surface of nude rats LSCD models showed maintenance of oral epithelium [17], while autologous oral mucosa cells transplanted onto rabbit LSCD models revealed the stimulation of residual LSCs after repeated wounding of the ocular surface [18]. However, the various technical procedures and the different physiology of animal models limit the significance of these studies.
A targeted examination of the follow-up specimens derived from COMET patients can help to understand the biological mechanism sustaining the repair and gain new insights on oral mucosal cells’ plasticity to adapt to the corneal environment and functions and enable analysis and stratification of successes and failures. To this aim, specific markers are needed to distinguish the oral mucosa, corneal and conjunctival epithelia.
With this scope, cytokeratins have been widely employed. However, several concerns remain about their expression change in specific conditions, such as in a proliferating/wound-healing state [19,20,21]. Our previous work suggested SOX2 as a univocal marker to distinguish the oral mucosa from corneal and conjunctival cells based on an unbiased transcriptome profile analysis of single cells derived from the different districts [20].
Nevertheless, a broad panel of markers is needed to analyze the specimens derived from COMET patients, providing a more consistent picture of the clinical condition. Thus, the original analysis was integrated by additional marker investigations.
A complementary issue is peripheral corneal neoangiogenesis, especially in the limbal area after COMET treatment [14,22]. Indeed, the oral mucosa (highly vascularized in situ) leads to neo vessels formation only in the limbo-conjunctival but not in the central cornea area when transplanted over the ocular surface.
In this work, a particular focus was given to vascularization-associated factors to shed more light on this phenomenon.
In summary, this work will support the characterization of the ocular surface epithelium in patients undergoing COMET, thus understanding the biologic mechanism that drives corneal repair and peripheral neovascularization.
2. Results
2.1. Gene expression profiling of holoclones from oral mucosa, limbus and conjunctiva
The oral mucosa epithelium functional analysis for COMET patient characterization was performed by microarray analysis of stem cell-containing holoclones isolated by clonal analysis as previously described [20]. Briefly, the subcultures of 32 holoclones from oral mucosa (n=15), corneal (n=8) and conjunctival (n=9) tissues were processed for RNA extraction and microarray analysis (Figure 1).
2.2. PITX2 mRNA is overexpressed in oral mucosa compared to ocular surface tissues
To identify unique tissue markers, we focused on the most differentially expressed transcripts in the pairwise comparisons between the oral mucosa and the ocular surface epithelia (Spreadsheets S1–S3 in [20]).
Comparing the oral mucosa to the ocular surface epithelia, the most upregulated transcript was Paired Like Homeodomain 2 (PITX2, FC=65.80 and FC=77.28 in oral mucosa vs limbus and conjunctiva, respectively) (Figure 2.A).
Real-Time PCR analyses confirmed that Pitx2 was upregulated in the stem cell-containing holoclones of oral mucosa compared to holoclones from limbus and conjunctiva (Figure 2.B).
Moreover, we tested oral mucosa, limbus, and conjunctiva bulk transcriptomes by Real-Time PCR, intending to evaluate the expression of Pitx2 transcript in holoclones and primary cultures. Data confirmed the upregulation only in the oral mucosa (Figure 2.C).
The downregulation of Pitx2 was also demonstrated by comparing oral mucosa holoclones to those derived from other epithelia, such as limbus, conjunctiva, epidermis and urethra (Figure 2.D).
We further analyzed Pitx2 expression in oral mucosa meroclones, which are the progeny of the transient amplifying cells (TA-cells) and retain a lower clonogenicity if compared to holoclones [23,24]. Results showed that Pitx2 mRNA did not correlate with the clonogenicity of the clones (Figure 2.E). Moreover, we analyzed the expression of the transcript also over consecutive passages of the oral mucosa, which was cultivated until stem cells exhaustion and senescence. PITX2 was expressed in young, medium, and old passages of two different strains and showed a statistically significant upregulation in the youngest passage compared to the other passages of the lifespan (Figure 2.F). This evidence may suggest a correlation between PITX2 expression level and the high proliferative potential of the cells, which is peculiar of the youngest passages.
2.3. Analysis of Pitx2 isoforms
Since PITX2 transcriptional factor has three major different isoforms (PITX2A, PITX2B, PITX2C) [25], we evaluated which isoforms were expressed in the oral mucosa. Specific primers were designed, and an oral mucosa holoclone was analyzed by Real-Time PCR. The results highlighted high levels of Pitx2C isoform and low levels of Pitx2A and Pitx2B (Figure 2.G).
The same analysis was also conducted on early passages of primary oral mucosa, limbus and conjunctiva. While the Pitx2C upregulation was confirmed, we observed a high expression of Pitx2B isoform (Figure 2.H). Instead, Pitx2A was expressed at low levels. According to precedent findings, all Pitx2 isoforms were strongly downregulated in limbus and conjunctiva compared to the oral mucosa (Figure 2.H).
2.4. Validation of the results by in situ hybridization (ISH)
In order to validate the microarray results in in vivo samples, oral mucosa and corneal donor specimens were tested through ISH assay using a pan-Pitx2 probe, corresponding to a common target sequence for all isoforms. In oral mucosa epithelium, Pitx2 transcript was specifically detected in basal and suprabasal keratinocytes up to the granular layer, resulting in the absence of central cornea, limbus, and conjunctiva (Figure 3.A). Coherently with literature, corneal endothelium was Pitx2 positive [26,27].
2.5. Validation of the results at protein level
To evaluate PITX2 as a putative tissue marker at a protein level, we performed indirect immunofluorescence staining on OCT frozen samples of in vivo limbo-cornea and oral mucosa samples. PITX2 protein showed a nuclear expression in basal and suprabasal tiers of oral mucosa epithelium up to the granular layer. In contrast, we could not detect any expression in the central cornea, limbus, and conjunctiva (Figure 3.B). The same results were obtained through immunohistochemical analysis on FFPE sections (Figure 3.C).
2.6. Phenotypic characterization of the patient after COMET
Once validated PITX2 as a marker for oral mucosa epithelium, we phenotypically characterized three corneal buttons obtained from an aniridic patient who underwent consecutive interventions of penetrating keratoplasty (PK) after a COMET procedure. At admission, the patient’s left eye was covered by a conjunctival pannus, and blood vessels migrated to the central cornea. During the COMET procedure, the fibrovascular tissue was removed, and oral mucosal cells cultured over a fibrin scaffold were applied to the ocular surface. After the treatment, the epithelium was intact, and the blood vessels partially regressed, although the stroma remained opaque. PKs were performed at 1, 3 and 10 years after the COMET to restore corneal transparency. The three corneal buttons, previously analyzed for different markers [20], revealed nuclear staining in the regenerated epithelium by IHC analysis for PITX2. The marker was more expressed in the 3-yy specimen, being the most stratified (Figure 4.A.c and d). However, in this sample there were other areas resulting negative (Figure 4.A.e and f).
In the samples obtained after 1 and 10 years from the COMET, the epithelium was thinner, and PITX2 resulted positive only in a few areas (Figure 4.A.a and g) and absent in the rest (Figure 4.A.b and h). Detecting goblet cells in the 3-yy specimen confirmed the coexistence with conjunctival tissue (Figure 4.A.f) [20].
Overall, these findings revealed the presence of oral mucosa tissue up to 10 years after the surgery and several PKs, highlighting the long-term maintenance of the transplanted cells, even though the highest abundance of PITX2 marker was detected in the stratified epithelium of the 3-yy follow-up specimen (Figure 4.B).
2.7. Angiogenic and antiangiogenic comparison between oral mucosa, limbus and conjunctiva
One of the significant postoperative problems in COMET patients is the invasion of blood vessels over the graft, which causes pain and visual acuity reduction, leading to total or partial failure of the procedure [14,22]. There is no evidence of why only some patients develop such a phenomenon to date.
To unravel this issue, starting from microarray data predicting an inhibition of angiogenesis in oral mucosa versus conjunctiva (Figure 5.A), we focused on the genes differentially expressed in oral mucosa in comparison with limbus and conjunctiva and coding for factors involved in angiogenesis. We found nine transcripts codifying for proangiogenic (Agr2, Cryab, Ereg, S100A4, and Jam-3) or antiangiogenic (Col4a1, Col4a2, Il1rn, and Timp2) proteins (Figure 5.B).
2.7.1. Proangiogenic factors
Agr2 and Cryab transcripts were upregulated in the conjunctiva and in the limbus compared to the oral mucosa and have been related to neoangiogenesis. The extracellular AGR2 binds VEGF and FGF-2, increasing their proangiogenic activity [28,29], while CRYAB increases choroidal neoangiogenesis through the VEGF signaling pathway, acting as a chaperone for VEGF-A [30,31].
In comparing conjunctiva and oral mucosa, we found two more transcripts encoding for proangiogenic factors: Ereg and S100A4. The transcript Ereg is translated to epiregulin (EPR), a member of the EGF family, that is secreted via exosomes and has a key role in promoting angiogenesis through the upregulation of VEGF-A and FGF-2 [32]. At the same time, the metastasis-associated protein S100A4 induces angiogenesis by binding Annexin II and accelerates plasmin formation [33,34].
Moreover, the Jam-3 transcript, encoding the JAM-C proangiogenic peptide (often targeted in antitumoral therapies) was upregulated in oral mucosa vs limbus [35]. Although more studies are needed to explore this hypothesis, the JAM-C expression could suggest a role in the corneal peripheral vascularization post-COMET.
2.7.2. Antiangiogenic factors
Conversely, the antiangiogenic transcripts Col4a1, Col4a2, and Il1rn were upregulated in oral mucosa vs conjunctiva. The alpha chains 1 and 2 of collagen IV (COL4A1, COL4A2) produce C-terminal-derived peptides (called arresten and canstatin, respectively) endowed with antiangiogenic properties [36,37]. In addition, IL1RN (or IL1RA) decreases the inflammatory environment by downregulating IL-1β, IL-6 and vascular adhesion molecule VCAM-1, and suppresses the corneal neovascularization [38]. The ability of these factors to limit conjunctival blood vessels ingrowth could explain the avascularity of oral mucosa in the central ocular surface after COMET.
Surprisingly, the antiangiogenic metalloproteinase Timp2 was downregulated in oral mucosa vs conjunctiva. TIMP2 was shown to be released by the amniotic membrane in culture, significantly suppressing the cornea neovascularization induced by FGF-2 [39].
A deep analysis of the interplay of these factors would explain the blood vessels outgrowth over the periphery of the transplanted oral mucosa or their absence in the central part.
3. Discussion
The oral mucosa epithelium proved to be an optimal alternative to treat total bilateral LSCD patients since 2004, with a procedure named COMET [14,22]. Using an autologous source of epithelial stem cells overcomes the problems related to autologous stem cells shortage and allogenic transplantation, rejection and lifelong immunosuppression.
One of the distinctive features of the stem cells presence in the limbus is corneal avascularity. The central corneal lacks capillaries, and many factors are involved in the so-called “angiogenic privilege”. However, many alterations can affect this homeostasis, promoting corneal neovascularization [40]. Pathological conditions such as viral infections, primary or secondary inflammations, degeneration of the limbus due to congenital pathologies (e.g., congenital aniridia), traumas, hypoxia, and neoplasia can trigger corneal neoangiogenesis. Most of these conditions can also be listed among the causes of LSCD, and neovascularization is one of the consequences that exacerbates its symptoms. The presence of the conjunctival pannus also highlights the LSCD, which is associated with the invasion of blood vessels, thus participating in a positive feedback loop. In this context, the lack of the antiangiogenic factor thrombospondin-1 (TSP-1), normally expressed by corneal cells, is likely to play a major role [41]. A bilateral LSCD patient undergoing COMET treatment is characterized by this condition (pre-operation neovascularization).
Neovascularization can also arise in the transplanted corneas after the COMET procedure (post-operation neovascularization). This phenomenon is facilitated by post-operative inflammation and occurs mainly in the peripheric corneal region [14,22]. In normal conditions, the production of TSP-1 by keratocytes may limit vascularization to this area [22,41] while, after a corneal wound, a high presence of ANG2, especially released by keratocytes, helps neovessels formation [42]. Finally, the presence of oral mucosa could also trigger angiogenesis because, in vivo, this tissue requires blood supply for its maintenance.
When the balance between pro and antiangiogenic factors is altered due to physiological or pathological conditions, it results in a decrease or formation of new blood vessels. This equilibrium has been widely studied on the ocular surface, although elucidating all the mechanisms and molecules involved is still far to be described [40]. In this process, the tear film unwinds a key role, containing several proangiogenic substances, such as IL-6, IL-8 and VEGF [43].
Altogether, the absence of sFlt-1, TIMP-3 and TSP-1 has been described in COMET specimens compared to normal corneas, suggesting their involvement in the “angiogenic privilege” and therefore in the peripheric neovascularization observed in COMET patients [44]. Moreover, the FGF2 factor was also reported to participate in this process [45].
We identified nine factors related to angiogenetic processes in the presented unbiased comparison between oral mucosa and ocular surface progenitor cells. Five were associated with proangiogenic capacities (AGR2, CRYAB, EPR, S100A4, JAM-C), while four were reported to have an antiangiogenic role (COL4A1, COL4A2, IL1RN, TIMP2).
Worth of note, the upregulation of the proangiogenic JAM-C in the oral mucosa (compared to the limbus) could be an exciting clue to be investigated in the post-COMET peripheral neoangiogenesis. This factor should be studied by loss or gain-of-function experiments to correlate its expression to the prognosis.
Moreover, the transcripts of the antiangiogenic peptides COL4A1, COL4A2 and IL1RN were found upregulated in oral mucosa compared to the conjunctiva, highlighting the capacity of the former tissue to stop the progression of conjunctival blood vessels towards the central ocular surface in COMET patients. Further studies could confirm this role.
The effective mechanism of ocular surface regeneration after oral mucosa transplantation is still unclear. The literature confirms that the engraftment of the oral mucosa tissue plays an essential role in the short term after the transplantation, however, follow-up data reveal its presence up to 10 years later [20]. Together with these insights supporting the engraftment of oral mucosal cells, their possible role in stimulating some residual limbal stem cells should also be considered, as well as a mixed pattern of the two regeneration mechanisms (Figure 6). Indeed, corneal tissue was detected on COMET transplanted eyes, although presumed completely depleted in patients suffering from total bilateral LSCD [15,46,47]. Moreover, donor corneal cells were also revealed in total bilateral LSCD patients treated with limbal allografts [48,49]. Such host limbal stem cells may be too few to duplicate in a pathologic contest, and they could regenerate the corneal tissue when triggered by exogenous stimuli [16].
The ways by means the oral tissue could regenerate the ocular surface are different: paracrine signaling, cytokine stimulation, exosomes delivery, growth factors release, direct contact communications, and others. In recent investigations, exosomes and extracellular vesicles (EVs) released from oral mucosa showed a great regenerative potential [50,51]. In addition, the EPR proangiogenic factor was found in oral mucosa exosomes [32]. Considering these findings, oral mucosa EVs should be studied in the post-COMET environment, also in relation to the peripheral neovascularization. Besides, depicting the factors released by the oral mucosa could result in a pharmacological therapeutic option for LSCD patients.
Several studies assume that the presence of corneal cells observed in patients after COMET is due to a change of oral cells phenotype into corneal one, a phenomenon called transdifferentiation [22,52]. However, it has been reported that epithelial cells transplanted in ectopic districts maintain their original phenotype, making the transdifferentiation hypothesis unlikely [53,54,55].
In literature, different markers were adopted to identify the three possible epithelia on the ocular surface after COMET, namely the oral mucosa, the cornea or the conjunctiva [46,47,56,57,58]. Cytokeratins have been widely used to characterize these tissues; for example, K3 and K12 identify the cornea, K13 and K19 mainly the conjunctiva. However, oral mucosa shares the expression of some of these markers (K3 and K13) with the ocular tissues [59]. Worth of note, cytokeratins expression differs considering the condition of the tissue. Indeed, these markers can be activated as a result of wound healing or inflammation [19,20,21], and their expression can change considerably due to pathologic processes, included genetic conditions such as aniridia [60,61].
Recently, our group has proposed the SOX2 transcription factor as a marker that univocally distinguishes the presence of oral mucosa tissue on the ocular surface of patients who underwent COMET and does not change its expression during wound healing [20].
This study found a new marker to distinguish the oral tissue from the ocular surface. In the unbiased comparison among progenitor cells derived from the cornea, conjunctiva and oral mucosa, we found that PITX2 was the most differentially expressed gene. This finding was validated on mRNA and protein levels, both in vitro and in vivo.
Paired-like homeodomain transcription factor 2 (PITX2) is related to the development of specific tissues and organs, including the cornea [62]. It has a pivotal role in the determination of left-right asymmetry in vertebrates [63,64] and in the morphogenesis of pituitary gland [65], teeth [66], skeletal muscle [67], heart [68], brain [69], etc. Recently, PITX2-SOX2 interaction was described in the progenitor oral/dental epithelial cell signaling center specification during odontogenesis [63]. PITX2 was also associated with corneal development and was reported as necessary to establish the corneal angiogenic privilege by upregulating AP-2β and other genes [62,70]. However, in the adult cornea, PITX2 expression is confined only to endothelial cells [26,27]. Moreover, mutations in PITX2 were found in patients with defects in the eye anterior chamber, such as Rieger syndrome [71]. Finally, the overexpression of this peptide was adopted as a tumorigenic hallmark in different districts, such as esophageal squamous cell carcinoma (ESCC) [72], prostate [25], colorectal [73], ovarian [74] and thyroid cancers [75].
PITX2 can be found in at least three isoforms (namely PITX2-A, PITX2-B, and PITX2-C), that correlate to diverse roles depending on their expression [76,77].
This paper explored the different isoforms expressed by cultured oral mucosa, revealing that PITX2-B and PITX2-C were the most represented.
In vivo, we observed that PITX2 mRNA, detected by ISH assay, was mainly expressed from the basal up to granular layer. This finding was confirmed also at a protein level by IF and IHC assay. Indeed, in culture, we did not appreciate a strong correlation between oral mucosa stem cells (holoclones) and more differentiated cells (meroclones). Nevertheless, when we investigated its expression within serial passages of cultured oral mucosa, we detected a significative higher expression in the youngest passage, suggesting a possible involvement in the proliferative potential.
Finally, we used the PITX2 marker to analyze three corneal buttons obtained from the same aniridic patient who underwent repeated penetrating keratoplasties 1-, 3- and 10-years after COMET procedure. The same samples were previously analyzed for their expression of canonical markers (i.e. K3, K12, K13, Alcian Blue/PAS, PAX6) showing the presence of goblet cells, thus conjunctiva [20]. Moreover, the expression of the SOX2 marker, highlighted the presence of oral mucosa throughout different time points, especially after 3 years, when the epithelium was more stratified and morphologically closer to the in vivo oral mucosa. Herein, these observations were implemented with the analysis of PITX2, whose nuclear positivity in all three corneal button specimens confirmed the persistence of oral mucosa up to 10 years. Consistently with previous observations, the 3-year corneal button showed the highest positivity, probably due to the high epithelial stratification of the ocular surface at that time point.
The identification of markers such as SOX2 and PITX2 that unequivocally identify the oral mucosa in the follow-up samples of COMET patients will be instrumental in extending this analysis to a larger cohort of COMET patients (comprising different LSCD etiologies, oral mucosa culture methods and neovascularization stages) shedding light on the possible regenerative mechanism of this treatment.
4. Conclusions
In conclusion, microarray analysis of holoclones derived from the cornea, conjunctiva and oral mucosa tissue, highlighted the pro and antiangiogenic factors differentially expressed in these tissues, gaining insights into the mechanisms involved in ocular surface neovascularization. Moreover, we identified and validated PITX2 as a new marker that univocally identifies oral mucosa epithelium on the ocular surface regenerated through the COMET procedure. This novel marker was employed to analyze the corneal buttons of a LSCD patient followed over 10 years after COMET treatment, demonstrating the long-term stability and regeneration of oral mucosa tissue. These insights will be helpful in future investigations decrypting the biological mechanisms underpinning ocular surface regeneration through oral mucosa transplantation.
5. Materials and Methods
1. Patients and Specimens
Specimens were obtained in accordance with the tenets of the Declaration of Helsinki; donors provided informed consent for biopsies. Permission was also obtained for samples taken from organ donors. Corneal and conjunctival specimens were obtained from the ocular surface of donors or cadavers, while small oral mucosal biopsies were collected from the inner cheek or inferior labial of patients undergoing oral mucosa transplantation for urethral stricture treatment [78,79].
2. COMET Transplantation
Eleven years before the COMET procedure, a 41-year-old woman suffering from total bilateral LSCD and glaucoma due to congenital aniridia underwent an anterior lamellar keratoplasty in her left eye, which failed due to superficial neovascularization caused by limbal deficiency. Under para/retrobulbar anesthesia, the conjunctiva was released a few millimeters outside the limbus exposing the sclera and the fibrovascular corneal pannus was removed. After this step, the oral mucosa cultured on a fibrin sheet was transferred to the corneal area; the excess of the fibrin was trimmed and the edges were covered with the conjunctiva applying 2 or 3 stitches of vicryl or silk 8/0.
3. Cell Cultures
Oral mucosal, conjunctival and limbal keratinocytes were obtained from biopsies and treated with trypsin (0.05 trypsin and 0.01% EDTA) at 37°C for about 120 min. Cells were collected every 30 min and seeded at a cell density 3-4.5x104 /cm2 on feeder layer (FL) of lethally irradiated 3T3-J2 cells (a gift from Prof. Howard Green) plated at the same cell density, then cultured in incubator with 5% CO2. The culture medium was composed of DMEM and Ham’s F12 media (2:1 mixture) containing FBS (10%) and penicillin/streptomycin, insulin (5 μg/mL), adenine (0.18 mM), hydrocortisone (0.4 µg/mL), cholera toxin (0.1 nM), triiodothyronine (2 nM), glutamine (4 mM). Epidermal growth factor was added at 10 ng/mL beginning at the first feeding, 3 days after plating. Subconfluent primary cultures were then passaged at a density of 6-8.3x103 cells/cm2. In serial propagation assays, cells were passaged before confluence until replicative senescence.
4. Clonal Analysis and Colony Forming Efficiency assay
Sub-confluent epithelial cultures were trypsinized, serially diluted and plated in 96-well plates (0.5 cell per well dilution) on a lethally irradiated FL of 3T3-J2 cells. After 7 days of cultivation, colonies derived from single keratinocytes were identified using an inverted microscope and trypsinized. One quarter of the colony was used for Colony Forming Efficiency (CFE) assay. In this assay, a small aliquot of cells was cultured for 12 days onto a 100-mm dish, then fixed and stained with rhodamine B for the classification of clonal type. This was determined by the percentage of aborted colonies formed by the progeny of the founding cell [23,24]. When 0–5% of colonies were abortive, the clone was scored as holoclone (stem cell). When more than 95% of the grown colonies were abortive (or when there were no colonies formed), the clone was classified as paraclone (terminally differentiated transient amplifying (TA) cell). Finally, when the percentage of abortive colonies was between 5% and 95%, the clone was classified as a meroclone (TA cell). The remaining three quarters of the colony were used for subculture for RNA and protein analysis.
5. Microarray Analyses
Subcultures of 32 holoclones (Table 1) from oral mucosa, limbus and conjunctival epithelia were performed.
Analysis of holoclones transcriptome was carried on by Affymetrix HG-U133 Plus 2.0 array [20]. Keratinocytes subcultured from each holoclone were feeder-depleted using immunomagnetic beads (Miltenyi Biotec, Bergisch Gladbach, Germany). According to the manufacturer’s protocol, total RNA was isolated with the Invitrogen™ PureLink™ RNA Micro Scale Kit (Thermo Fisher Scientific, Waltham, MA, USA). Differentially expressed genes (DEGs) were identified on a robust multiarray average (RMA)-normalized data through the ANOVA module supplied by the Partek GS. 6.6 Software Package. The probesets displaying a fold change contrast ≥ 2 and a false discovery rate (FDR) < 0.05 were selected as DEGs among oral mucosa, limbal and conjunctival holoclones. Integral gene expression data were submitted to the Gene Expression Omnibus repository (http://www.ncbi.nlm.nih.gov/geo; series GSE198408). The network of angiogenesis related transcripts was generated using QIAGEN IPA (QIAGEN Inc., https://digitalinsights.qiagen.com/IPA) [80].
6. Real-Time PCR
Total RNA was isolated with the Invitrogen™ PureLink™ RNA Micro Scale Kit (Thermo Fisher), according to the manufacturer's protocol. RNA samples were treated with RNase-free ezDNase enzyme to digest the gDNA, and SuperScript IV VILO Master Mix (Thermo Fisher) was used to synthesize the cDNA. Real Time quantitative RT-PCR was performed by using TaqMan Gene Expression Assays probes (Thermo Fisher) PITX2 (Hs04234069_mH), complementary to all its isoforms, GAPDH (Hs99999905_m1) and TaqMan Fast Advanced Master Mix (Thermo Fisher). For isoforms analysis, RT-PCR with PowerUp SYBR Green Master Mix (Applied Biosystems, Thermo Fisher) were performed using specific primers according to literature or modified (Table 2; [25]. Reactions were ran in a QuantStudio12K Flex Real Time System or in a 7900HT Fast Real-Time PCR System (Applied Biosystems, Thermo Fisher) with specific cycling programs for each master mix, as requested by manufacturer’s instructions. The expression of target genes was normalized to the level of GAPDH in the same cDNA by using the 2−ΔΔCT quantification. For statistical analysis Mann-Whitney test or one-way ANOVA test were applied using PRISM 8 software (version 8.4.0, GraphPad Software, San Diego, CA, USA).
7. In situ Hybridization (ISH)
Human tissues from biopsies were formalin-fixed, paraffin-embedded (FFPE) and sectioned at 3-4 µm. PITX2 RNA probes were hybridized to sections using the BaseScope RED Assay kit (Advanced Cell Diagnostic, Inc.). Target retrieval was performed for 15 min with target retrieval reagent (Advanced Cell Diagnostic, Inc.) at 95°C and for 15 min with protease III (Advanced Cell Diagnostic, Inc.) at 40°C. The analyzed biopsies were samples of oral mucosa and ocular surface (N=3). Probes for peptidyl-prolyl-cis-trans isomerase B and Bacillus subtilis DapB genes were used as positive and negative controls, respectively (Advanced Cell Diagnostic, Inc.).
8. Immunofluorescence and Immunohistochemistry
For in vivo immunofluorescence (IF) studies, human tissues were embedded in an optimal cutting temperature compound (OCT) (Killik; Bio-Optica, Milan, Italy), frozen and cut into 5-7 µm sections on a cryostat (Leica 1850 UV). Subsequently, sections were fixed for 10 min with 3% PFA at room temperature (RT). Then, samples were permeabilized with 0.2% Triton X-100 in PBS (20 min, RT), treated in the dark with 3% H2O2 (5 min, RT), and blocked with 2% BSA- 5% FBS- 0.1% Triton X-100 (30 min, 37°C). After the samples’ incubation for 1 hour at 37°C with the primary polyclonal antibody anti-PITX2 (Abcam, ab98297, 1:1.000) and thereafter with the secondary antibody anti-rabbit Alexa Fluor 488 (A-21206, Thermo Fisher) (30 min, 37°C, 1:200), the nuclei were labeled with DAPI (3 min, RT), and slides were mounted with Fluorescent Mounting Medium (Dako, Agilent Technologies, Santa Clara, CA, USA). Washes after primary and secondary antibodies were performed with 0.2% BSA, the others with 1X PBS.
For immunohistochemical (IHC) analysis, human biopsy tissues were formalin-fixed, paraffin-embedded (FFPE) and sectioned at 3-4 µm, and the immunostaining was performed on the automated system Ventana BenchMark XT (Roche, Basel, Switzerland) with the primary monoclonal antibody anti-PITX2 (Abcam, ab55599, 1:100, 60 min) using diaminobenzidine as chromogen by the Ventana Ultraview Universal DAB Detection kit (Roche, Basel, Switzerland). Antigen retrieval was obtained through the Ventana Cell Conditioning 1 antigen retrieval buffer (extended, 90 min) (Roche, Basel, Switzerland). Then, slides were counterstained with Ventana Haematoxylin II (Roche, Basel, Switzerland). Immunohistochemical sections were acquired using Imager.M2 microscope (Zeiss, Oberkochen, Germany) and AxioVision SE64 software (Zeiss, Oberkochen, Germany). Measure of positive epithelium’s length for each marker was performed using MosaiX and Length software tools. Average and standard deviation (N = 3) of each marker at each follow-up timepoint was calculated. For statistical analysis, two-way ANOVA test was performed using PRISM 8 software (version 8.4.0, GraphPad Software, San Diego, CA, USA).
Author Contributions
Conceptualization, E.A., G.G. and G.P.; methodology, E.A., G.G., E.B. and G.P.; formal analysis, E.A., G.G., A.T., S.B. and E.B.; investigation, E.A., G.G., A.T., E.B., S.B. , L.L., A.L. and P.R.; data curation, E.B.; writing—original draft preparation, E.A. and G.G.; writing—review and editing, E.A., G.G., A.T., E.B., S.B., L.L, R.M., A.L., P.R. and G.P.; funding acquisition, G.P. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Awards “Lombardia è Ricerca 2018” and “Louis Jeantet Award 2020” and by Holostem Terapie Avanzate s.r.l. and by Regione Emilia-Romagna (area 1b, medicina rigenerativa) and POR-FESR 2007-13-Tecnopolo.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee “Area Vasta Emilia Nord” (protocol code 178/2009/SPER/AOUMO, date of approval 28/01/2020), by the Ethics Committee “IRCCS San Raffaele Scientific Institute” (compassionate ethical opinion n. 64, date of approval 14/10/2020) and by the Regional Ethical Committee for Clinical Trials of Toscana Region “Area Vasta Sud-Est” (protocol code 18541, date of approval 16/11/2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Integral gene expression data were submitted to the Gene Expression Omnibus repository (http://www.ncbi.nlm.nih.gov/geo; series GSE198408).
Acknowledgments
We acknowledge Luca Fabbiani for technical assistance in immunohistochemical analysis; Francesca Sanvito, Luca Giannetti, Ugo Consolo, and Guido Barbagli for biopsy and samples collection; Roza Ezteki, Valentina Masciale, Athanasios Panaras, and Anna Ribbene for microarray analysis samples preparation. We acknowledge the contribution of IRCCS San Raffaele Scientific Institute, where Dr. Paolo Rama obtained patient’s samples. Graphical abstract has been created with Biorender.com
Conflicts of Interest
E.A., G.G., E.B., S.B., L.L., R.M., A.L. and P.R. declare no conflict of interest. A.T is currently an employee and G.P. is a member of the Board of Directors and R&D Director of Holostem Terapie Avanzate s.r.l.
References
- Chiavelli C, Attico E, Sceberras V, Fantacci M, Melonari M, Pellegrini G. Stem cells and ocular regeneration. Encyclopedia of Tissue Engineering and Regenerative Medicine. 2019, 1–3, 169–179. [Google Scholar]
- Sejpal K, Bakhtiari P, Deng SX. Presentation, Diagnosis and Management of Limbal Stem Cell Deficiency. Middle East Afr J Ophthalmol. 2013, 20, 5. [Google Scholar] [CrossRef] [PubMed]
- Deng SX, Borderie V, Chan CC, Dana R, Figueiredo FC, Gomes JAP, et al. Global Consensus on Definition, Classification, Diagnosis, and Staging of Limbal Stem Cell Deficiency. Cornea. 2019, 38, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Adamo D, Attico E, Pellegrini G. Education for the translation of Advanced Therapy Medicinal Products. Front Med (Lausanne). 2023, 10, 658. [Google Scholar]
- Pellegrini G, Ardigò D, Milazzo G, Iotti G, Guatelli P, Pelosi D, et al. Navigating Market Authorization: The Path Holoclar Took to Become the First Stem Cell Product Approved in the European Union. Stem Cells Transl Med. 2018, 7, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Attico E, Sceberras V, Pellegrini G. Approaches for Effective Clinical Application of Stem Cell Transplantation. Curr Transplant Rep. 2018, 5, 244–250. [Google Scholar] [CrossRef]
- Daya, SM. Conjunctival-limbal autograft. Curr Opin Ophthalmol. 2017, 28, 370–376. [Google Scholar] [CrossRef]
- Kenyon KR, Tseng SCG. Limbal Autograft Transplantation for Ocular Surface Disorders. Ophthalmology. 1989, 96, 709–723. [Google Scholar] [CrossRef]
- 9. Pellegrini G, Traverso CE, Franzi AT, Ingirian MZ, Cancedda R, de Luca M. Long-term restoration of damaged corneal surfaces with autologous cultivated corneal epithelium. 1997.
- Sangwan VS, Basu S, MacNeil S, Balasubramanian D. Simple limbal epithelial transplantation (SLET): a novel surgical technique for the treatment of unilateral limbal stem cell deficiency. British Journal of Ophthalmology. 2012, 96, 931–934. [Google Scholar] [CrossRef]
- Maurizi E, Adamo D, Magrelli FM, Galaverni G, Attico E, Merra A, et al. Regenerative Medicine of Epithelia: Lessons From the Past and Future Goals. Front Bioeng Biotechnol. 2021, 9, 193. [Google Scholar]
- Rama P, Matuska S, Paganoni G, Spinelli A, de Luca M, Pellegrini G. Limbal Stem-Cell Therapy and Long-Term Corneal Regeneration. New England Journal of Medicine. 2010, 363, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini G, Rama P, Matuska S, Lambiase A, Bonini S, Pocobelli A, et al. Biological parameters determining the clinical outcome of autologous cultures of limbal stem cells. Regenerative Med. 2013, 8, 553–567. [Google Scholar] [CrossRef] [PubMed]
- Nakamura T, Inatomi T, Sotozono C, Amemiya T, Kanamura N, Kinoshita S. Transplantation of cultivated autologous oral mucosal epithelial cells in patients with severe ocular surface disorders. Br J Ophthalmol. 2004, 88, 1280. [Google Scholar] [CrossRef] [PubMed]
- Attico E, Galaverni G, Pellegrini G. Clinical Studies of COMET for Total LSCD: a Review of the Methods and Molecular Markers for Follow-Up Characterizations. Current Ophthalmology Reports 2021 9:1. 2021, 9, 25–37. [Google Scholar]
- Pellegrini, G. Changing the Cell Source in Cell Therapy. 2004.
- Soma T, Hayashi R, Sugiyama H, Tsujikawa M, Kanayama S, Oie Y, et al. Maintenance and Distribution of Epithelial Stem/Progenitor Cells after Corneal Reconstruction Using Oral Mucosal Epithelial Cell Sheets. PLoS One. 2014, 9, e110987. [Google Scholar]
- Sugiyama H, Yamato M, Nishida K, Okano T. Evidence of the survival of ectopically transplanted oral mucosal epithelial stem cells after repeated wounding of cornea. Mol Ther. 2014, 22, 1544–1555. [Google Scholar] [CrossRef] [PubMed]
- Zhang X, Yin M, Zhang LJ. Keratin 6, 16 and 17-Critical Barrier Alarmin Molecules in Skin Wounds and Psoriasis. Cells. 2019, 8. [Google Scholar]
- Attico E, Galaverni G, Bianchi E, Losi L, Manfredini R, Lambiase A, et al. SOX2 Is a Univocal Marker for Human Oral Mucosa Epithelium Useful in Post-COMET Patient Characterization. Int J Mol Sci. 2022, 23. [Google Scholar]
- Kalabusheva EP, Shtompel AS, Rippa AL, Ulianov S V. , Razin S V., Vorotelyak EA. A Kaleidoscope of Keratin Gene Expression and the Mosaic of Its Regulatory Mechanisms. International Journal of Molecular Sciences 2023, Vol 24, Page 5603. 2023, 24, 5603. [Google Scholar]
- Nishida K, Yamato M, Hayashida Y, Watanabe K, Yamamoto K, Adachi E, et al. Corneal reconstruction with tissue-engineered cell sheets composed of autologous oral mucosal epithelium. New England Journal of Medicine. 2004, 351, 1187–1196. [Google Scholar] [CrossRef]
- Barrandon Y, Green H. Three clonal types of keratinocyte with different capacities for multiplication. Proc Natl Acad Sci U S A. 1987, 84, 2302–2306. [Google Scholar] [CrossRef] [PubMed]
- Enzo E, Cattaneo C, Consiglio F, Polito MP, Bondanza S, De Luca M. Clonal analysis of human clonogenic keratinocytes. Methods Cell Biol. 2022, 170, 101–116. [Google Scholar]
- Vela I, Morrissey • C, Zhang • X, Chen • S, Corey • E, Strutton • G M, et al. PITX2 and non-canonical Wnt pathway interaction in metastatic prostate cancer. 2013. [CrossRef]
- Lovatt M, Yam GHF, Peh GS, Colman A, Dunn NR, Mehta JS. Directed differentiation of periocular mesenchyme from human embryonic stem cells. Differentiation. 2018, 99, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Hin-Fai Yam G, Seah X, Zahirah Binte Yusoff NM, Setiawan M, Wahlig S, Myint Htoon H, et al. Characterization of Human Transition Zone Reveals a Putative Progenitor-Enriched Niche of Corneal Endothelium. 2019. [CrossRef]
- Guo H, Zhu Q, Yu X, Merugu SB, Mangukiya HB, Smith N, et al. Tumor-secreted anterior gradient-2 binds to VEGF and FGF2 and enhances their activities by promoting their homodimerization. Oncogene. 2017, 36, 5098–5109. [Google Scholar] [CrossRef] [PubMed]
- Zhu Q, Mangukiya HB, Mashausi DS, Guo H, Negi H, Merugu SB, et al. Anterior gradient 2 is induced in cutaneous wound and promotes wound healing through its adhesion domain. FEBS Journal. 2017, 284, 2856–2869. [Google Scholar] [CrossRef] [PubMed]
- Kase S, He S, Sonoda S, Kitamura M, Spee C, Wawrousek E, et al. αB-crystallin regulation of angiogenesis by modulation of VEGF. Blood. 2010, 115, 3398–3406. [Google Scholar] [CrossRef]
- Liu L, Qi X, Chen Z, Shaw L, Cai J, Smith LH, et al. Targeting the IRE1α/XBP1 and ATF6 arms of the unfolded protein response enhances VEGF blockade to prevent retinal and choroidal neovascularization. American Journal of Pathology. 2013, 182, 1412–1424. [Google Scholar] [CrossRef]
- Yang WW, Yang LQ, Zhao F, Chen CW, Xu LH, Fu J, et al. Epiregulin promotes lung metastasis of salivary adenoid cystic carcinoma. Theranostics. 2017, 7. [Google Scholar]
- Semov A, Moreno MJ, Onichtchenko A, Abulrob A, Ball M, Ekiel I, et al. Metastasis-associated protein S100A4 induces angiogenesis through interaction with annexin II and accelerated plasmin formation. Journal of Biological Chemistry. 2005, 280, 20833–20841. [Google Scholar] [CrossRef]
- Ambartsumian N, Rg Klingelhoè Fer J, Grigorian M, Christensen C, Kriajevska M, Tulchinsky E, et al. The metastasis-associated Mts1(S100A4) protein could act as an angiogenic factor. 2001.
- Lamagna C, Hodivala-Dilke KM, Imhof BA, Aurrand-Lions M. Antibody against Junctional Adhesion Molecule-C Inhibits Angiogenesis and Tumor Growth. Cancer Res. 2005, 65, 5703–5710. [Google Scholar] [CrossRef]
- Wang Y, Yin H, Chen P, Xie L, Wang Y. Inhibitory Effect of Canstatin in Alkali Burn-Induced Corneal Neovascularization. Ophthalmic Res. 2011, 46, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Okada M, Yamawaki H. A current perspective of canstatin, a fragment of type IV collagen alpha 2 chain. J Pharmacol Sci. 2019, 139, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Moore JE, Mcmullen TCB, Campbell IL, Rohan R, Kaji Y, Afshari NA, et al. The Inflammatory Milieu Associated with Conjunctivalized Cornea and Its Alteration with IL-1 RA Gene Therapy. 2002.
- Ma X, Li J. Corneal neovascularization suppressed by TIMP2 released from human amniotic membranes. Yan ke xue bao = Eye science / “Yan ke xue bao” bian ji bu. 2005, 21, 56–61. [Google Scholar]
- Nicholas MP, Mysore N. Corneal neovascularization. Exp Eye Res. 2021, 202, 108363. [Google Scholar] [CrossRef] [PubMed]
- Sekiyama E, Nakamura T, Cooper LJ, Kawasaki S, Hamuro J, Fullwood NJ, et al. Unique distribution of thrombospondin-1 in human ocular surface epithelium. Invest Ophthalmol Vis Sci. 2006, 47, 1352–1358. [Google Scholar] [CrossRef] [PubMed]
- Ferrari G, Giacomini C, Bignami F, Moi D, Ranghetti A, Doglioni C, et al. Angiopoietin 2 expression in the cornea and its control of corneal neovascularisation. British Journal of Ophthalmology. 2016, 100, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Zakaria N, van Grasdorff S, Wouters K, Rozema J, Koppen C. Human Tears Reveal Insights into Corneal Neovascularization. PLoS One. 2012, 7, 36451. [Google Scholar]
- Chen HCJ, Yeh LK, Tsai YJ, Lai CH, Chen CC, Lai JY, et al. Expression of angiogenesis-related factors in human corneas after cultivated oral mucosal epithelial transplantation. Invest Ophthalmol Vis Sci. 2012, 53, 5615–5623. [Google Scholar] [CrossRef]
- Kanayama S, Nishida K, Yamato M, Hayashi R, Sugiyama H, Soma T, et al. Analysis of angiogenesis induced by cultured corneal and oral mucosal epithelial cell sheets in vitro. Exp Eye Res. 2007, 85, 772–781. [Google Scholar] [CrossRef]
- Gaddipati S, Muralidhar R, Sangwan VS, Mariappan I, Vemuganti GK, Balasubramanian D. Oral epithelial cells transplanted on to corneal surface tend to adapt to the ocular phenotype. Indian J Ophthalmol. 2014, 62, 644–648. [Google Scholar] [CrossRef]
- Kim YJ, Lee HJ, Ryu JS, Kim YH, Jeon S, Oh JY, et al. Prospective Clinical Trial of Corneal Reconstruction With Biomaterial-Free Cultured Oral Mucosal Epithelial Cell Sheets. Cornea. 2018, 37, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Henderson TRM, Coster DJ, Williams KA. The long term outcome of limbal allografts: the search for surviving cells. 2001. [CrossRef]
- Williams KA, Brereton HM, Aggarwal R, Sykes PJ, Turner DR, Russ GR, et al. Use of DNA polymorphisms and the polymerase chain reaction to examine the survival of a human limbal stem cell allograft. Am J Ophthalmol. 1995, 120, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Sjoqvist S, Kasai Y, Shimura D, Ishikawa T, Ali N, Iwata T, et al. Oral keratinocyte-derived exosomes regulate proliferation of fibroblasts and epithelial cells. Biochem Biophys Res Commun. 2019, 514, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Sjöqvist S, Ishikawa T, Shimura D, Kasai Y, Imafuku A, Bou-Ghannam S, et al. Exosomes derived from clinical-grade oral mucosal epithelial cell sheets promote wound healing. J Extracell Vesicles. 2019, 8. [Google Scholar]
- Xiao YT, Xie HT, Liu X, Duan CY, Qu JY, Zhang MC, et al. Subconjunctival Injection of Transdifferentiated Oral Mucosal Epithelial Cells for Limbal Stem Cell Deficiency in Rats. J Histochem Cytochem. 2021, 69, 177–190. [Google Scholar] [CrossRef]
- De Rosa L, Carulli S, Cocchiarella F, Quaglino D, Enzo E, Franchini E, et al. Long-term stability and safety of transgenic cultured epidermal stem cells in gene therapy of junctional epidermolysis bullosa. Stem Cell Reports. 2014, 2, 1–8. [Google Scholar] [CrossRef]
- Bianco P, Cao X, Frenette PS, Mao JJ, Robey PG, Simmons PJ, et al. The meaning, the sense and the significance: translating the science of mesenchymal stem cells into medicine. Nature Medicine 2013 19:1. 2013, 19, 35–42. [Google Scholar]
- De Luca M, Albanese E, Megna M, Cancedda R, Mangiante PE, Cadoni A, et al. Evidence that human oral epithelium reconstituted in vitro and transplanted onto patients with defects in the oral mucosa retains properties of the original donor site. Transplantation. 1990, 50, 454–459. [Google Scholar] [CrossRef]
- Inatomi T, Nakamura T, Kojyo M, Koizumi N, Sotozono C, Kinoshita S. Ocular Surface Reconstruction With Combination of Cultivated Autologous Oral Mucosal Epithelial Transplantation and Penetrating Keratoplasty. Am J Ophthalmol. 2006, 142. [Google Scholar]
- Nakamura T, Inatomi T, Cooper LJ, Rigby H, Fullwood NJ, Kinoshita S. Phenotypic Investigation of Human Eyes with Transplanted Autologous Cultivated Oral Mucosal Epithelial Sheets for Severe Ocular Surface Diseases. Ophthalmology. 2007, 114, 1080–1088. [Google Scholar] [CrossRef]
- Chen HCJ, Chen HL, Lai JY, Chen CC, Tsai YJ, Kuo MT, et al. Persistence of transplanted oral mucosal epithelial cells in human cornea. Invest Ophthalmol Vis Sci. 2009, 50, 4660–4668. [Google Scholar] [CrossRef] [PubMed]
- Moll R, Divo M, Langbein L. The human keratins: Biology and pathology. Histochemistry and Cell Biology. 2008, 129, 705–733. [Google Scholar] [CrossRef] [PubMed]
- Lagali N, Wowra B, Fries FN, Latta L, Moslemani K, Utheim TP, et al. Early phenotypic features of aniridia-associated keratopathy and association with PAX6 coding mutations. Ocular Surface. 2020, 18, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Latta L, Figueiredo FC, Ashery-Padan R, Collinson JM, Daniels J, Ferrari S, et al. Pathophysiology of aniridia-associated keratopathy: Developmental aspects and unanswered questions. Ocular Surface. 2021, 22, 245–266. [Google Scholar] [CrossRef] [PubMed]
- Gage PJ, Kuang C, Zacharias AL. The homeodomain transcription factor PITX2 is required for specifying correct cell fates and establishing angiogenic privilege in the developing cornea. Developmental Dynamics. 2014, 243, 1391–1400. [Google Scholar] [CrossRef] [PubMed]
- Yu W, Sun Z, Sweat Y, Sweat M, Venugopalan SR, Eliason S, et al. Pitx2-Sox2-Lef1 interactions specify progenitor oral/dental epithelial cell signaling centers. Development (Cambridge). 2020, 147. [Google Scholar]
- Essner JJ, Branford WW, Zhang J, Yost HJ. Mesendoderm and left-right brain, heart and gut development are differentially regulated by pitx2 isoforms. Development. 2000, 127, 1081–1093. [Google Scholar] [CrossRef]
- Suh H, Gage PJ, Drouin J, Camper SA. Pitx2 is required at multiple stages of pituitary organogenesis: pituitary primordium formation and cell specification. Development. 2002, 129, 329–337. [Google Scholar] [CrossRef]
- Liu W, Selever J, Lu MF, Martin JF. Genetic dissection of Pitx2 in craniofacial development uncovers new functions in branchial arch morphogenesis, late aspects of tooth morphogenesis and cell migration. Development. 2003, 130, 6375–6385. [Google Scholar] [CrossRef]
- Sofyanti E, Pratamawati T. Prediction of Regulatory Networks of PITX2 Gene Expression in Mandibular Asymmetry Related to Oral Muscle Function. 2018.
- Franco, D. , Campione M. The role of Pitx2 during Cardiac Development. TCM. 2003, 13, No 4, 2003. [Google Scholar]
- Martin DM, Skidmore JM, Philips ST, Vieira C, Gage PJ, Condie BG, et al. PITX2 is required for normal development of neurons in the mouse subthalamic nucleus and midbrain. Dev Biol. 2004, 267, 93–108. [Google Scholar] [CrossRef] [PubMed]
- Chen L, Martino V, Dombkowski A, Williams T, West-Mays J, Gage PJ. Ap-2β is a downstream effector of PITX2 required to specify endothelium and establish angiogenic privilege during corneal development. Invest Ophthalmol Vis Sci. 2016, 57, 1072–1081. [Google Scholar] [CrossRef] [PubMed]
- Perveen R, Lloyd IC, Clayton-Smith J, Churchill A, Van Heyningen V, Hanson I, et al. Phenotypic Variability and Asymmetry of Rieger Syndrome Associated with PITX2 Mutations. 2000.
- Zhang JX, Tong ZT, Yang L, Wang F, Chai HP, Zhang F, et al. PITX2: A promising predictive biomarker of patients’ prognosis and chemoradioresistance in esophageal squamous cell carcinoma. Int J Cancer. 2013, 132, 2567–2577. [Google Scholar] [CrossRef] [PubMed]
- Semaan A, Uhl B, Branchi V, Lingohr P, Bootz F, Kristiansen G, et al. Significance of PITX2 Promoter Methylation in Colorectal Carcinoma Prognosis. Clin Colorectal Cancer. 2018, 17, e385–93. [Google Scholar] [CrossRef] [PubMed]
- Fung FKC, Chan DW, Liu VWS, Leung THY, Cheung ANY, Ngan HYS. Increased expression of PITX2 transcription factor contributes to ovarian cancer progression. PLoS One. 2012, 7. [Google Scholar]
- Huang Y, Guigon CJ, Fan J, Cheng SY, Zhu GZ. Pituitary homeobox 2 (PITX2) promotes thyroid carcinogenesis by activation of cyclin D2. Cell Cycle. 2010, 9, 1333–1341.
- Cox CJ, Espinoza HM, McWilliams B, Chappell K, Morton L, Hjalt TA, et al. Differential regulation of gene expression by PITX2 isoforms. Journal of Biological Chemistry. 2002, 277, 25001–25010. [Google Scholar] [CrossRef]
- Lamba P, Hjalt TA, Bernard DJ. Novel forms of Paired-like homeodomain transcription factor 2 (PITX2): Generation by alternative translation initiation and mRNA splicing. BMC Mol Biol. 2008, 9. [Google Scholar]
- Sceberras V, Maria Magrelli F, Adamo D, Maurizi E, Attico E, Giuseppe Genna V, et al. The cell as a tool to understand and repair urethra. Scientific Advances in Reconstructive Urology and Tissue Engineering. 2022, 1–24. [Google Scholar]
- Sceberras V, Attico E, Bianchi E, Galaverni G, Melonari M, Corradini F, et al. Preclinical study for treatment of hypospadias by advanced therapy medicinal products. World J Urol. 2020, 38, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Krämer A, Green J, Pollard J, Tugendreich S. Causal analysis approaches in ingenuity pathway analysis. Bioinformatics. 2014, 30, 523–530. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Workflow of the study. Schematic representation of the workflow related to the present study (created with Biorender.com). Abbreviations: CFE, colony forming efficiency; COMET, cultivated oral mucosa epithelial transplantation.
Figure 1.
Workflow of the study. Schematic representation of the workflow related to the present study (created with Biorender.com). Abbreviations: CFE, colony forming efficiency; COMET, cultivated oral mucosa epithelial transplantation.
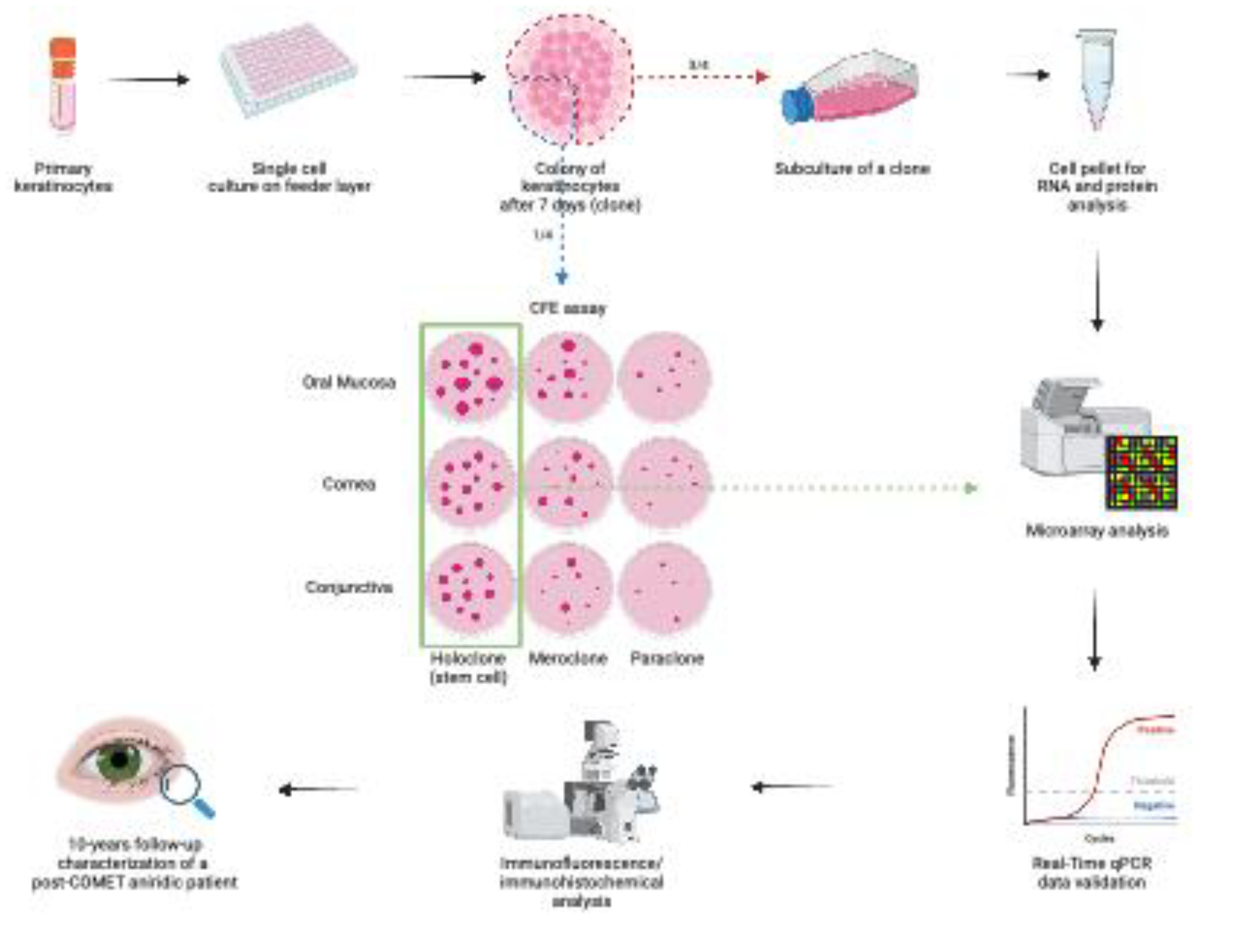
Figure 2.
Identification and validation of Pitx2 as differentially expressed transcript. (A) Boxplots showing Pitx2 signals in conjunctival, limbal and oral mucosal holoclones (results are expressed in log scale); (B) Real-time RT-PCR validation of Pitx2 transcript levels expressed as log2RQ. Mann–Whitney test performed; (C) Real-time RT-PCR of Pitx2 in primary cultures of young passages of oral mucosa, cornea and conjunctiva; (D) Real-time RT-PCR of Pitx2 expression in holoclones of oral mucosa, cornea, conjunctiva, skin and urethra; (E) Real-time RT-PCR of Pitx2 in holoclones and meroclones of a strain of oral mucosa ordered by increasing % of abortive colonies (decreasing clonogenicity); (F) Real-time RT-PCR of Pitx2 in passages of lifespans of two different donors of oral mucosa. n.s.= not significant, *** = p < 0.0004, ** = p < 0.005, * = p < 0.03 with one-way ANOVA test; (G) Real-time RT-PCR of Pitx2 isoforms in a holoclone of oral mucosa; (H) Real-time RT-PCR of Pitx2 isoforms in primary cultures of young passages of oral mucosa, cornea and conjunctiva. Abbreviations: CON, conjunctiva; LE, limbus; MO, oral mucosa; K, skin; UK, urethra; H, holoclone; M, meroclone; PITX2-tot, all PITX2 isoforms.
Figure 2.
Identification and validation of Pitx2 as differentially expressed transcript. (A) Boxplots showing Pitx2 signals in conjunctival, limbal and oral mucosal holoclones (results are expressed in log scale); (B) Real-time RT-PCR validation of Pitx2 transcript levels expressed as log2RQ. Mann–Whitney test performed; (C) Real-time RT-PCR of Pitx2 in primary cultures of young passages of oral mucosa, cornea and conjunctiva; (D) Real-time RT-PCR of Pitx2 expression in holoclones of oral mucosa, cornea, conjunctiva, skin and urethra; (E) Real-time RT-PCR of Pitx2 in holoclones and meroclones of a strain of oral mucosa ordered by increasing % of abortive colonies (decreasing clonogenicity); (F) Real-time RT-PCR of Pitx2 in passages of lifespans of two different donors of oral mucosa. n.s.= not significant, *** = p < 0.0004, ** = p < 0.005, * = p < 0.03 with one-way ANOVA test; (G) Real-time RT-PCR of Pitx2 isoforms in a holoclone of oral mucosa; (H) Real-time RT-PCR of Pitx2 isoforms in primary cultures of young passages of oral mucosa, cornea and conjunctiva. Abbreviations: CON, conjunctiva; LE, limbus; MO, oral mucosa; K, skin; UK, urethra; H, holoclone; M, meroclone; PITX2-tot, all PITX2 isoforms.
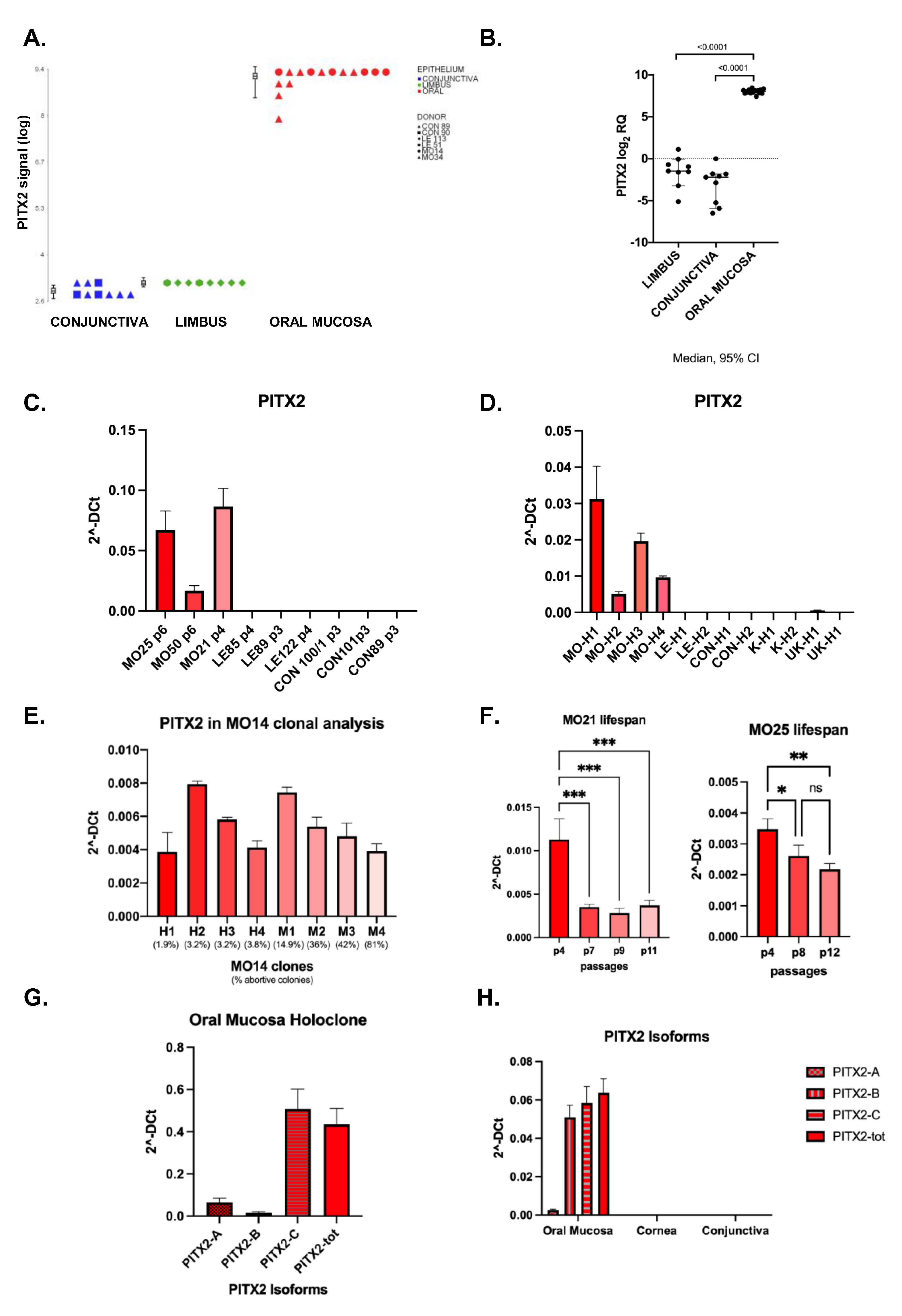
Figure 3.
Validation of Pitx2 expression in vivo. (A) In situ hybridization of Pitx2 transcript (red) on formalin-fixed paraffin-embedded (FFPE) biopsies of oral mucosa, central cornea, conjunctiva and corneal endothelium (n=3). Black arrows highlight positive signals; (B) in vivo immunofluorescence analysis of PITX2 protein (green) in samples of oral mucosa (n=7), central cornea, limbus and conjunctiva (n=3); (C) immunohistochemical analysis of PITX2 protein (brown) on formalin-fixed paraffin-embedded biopsies of oral mucosa, central cornea, limbus and conjunctiva (n=3). Scale bars = 50 μm.
Figure 3.
Validation of Pitx2 expression in vivo. (A) In situ hybridization of Pitx2 transcript (red) on formalin-fixed paraffin-embedded (FFPE) biopsies of oral mucosa, central cornea, conjunctiva and corneal endothelium (n=3). Black arrows highlight positive signals; (B) in vivo immunofluorescence analysis of PITX2 protein (green) in samples of oral mucosa (n=7), central cornea, limbus and conjunctiva (n=3); (C) immunohistochemical analysis of PITX2 protein (brown) on formalin-fixed paraffin-embedded biopsies of oral mucosa, central cornea, limbus and conjunctiva (n=3). Scale bars = 50 μm.
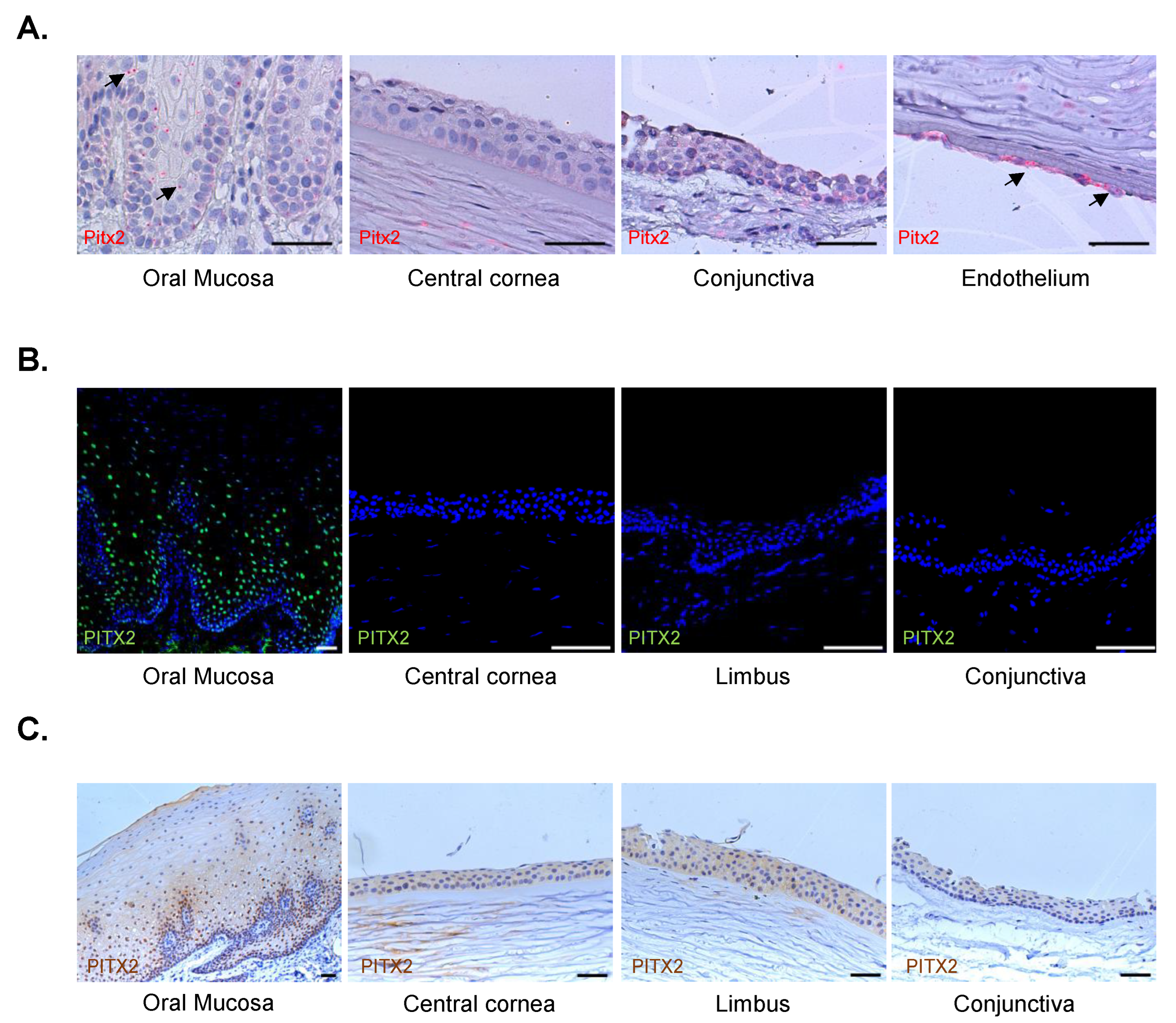
Figure 4.
Phenotypic characterization of the corneal buttons derived from the PKs of a patient treated by COMET. (A) Immunohistochemical analysis of the corneal buttons from the PKs at 1-, 3- and 10-years post-COMET. Representative images of positive (a, c, d, g) and negative (b, e, f, h) areas are shown in the panel; the images related to the 3-years corneal button highlighted a transitional zone between oral mucosa and another epithelium (d) and a zone with conjunctival epithelium with a cluster of goblet cells (f). Scale bars = 50 μm. (B) Graph showing the percentage of the positive epithelial length for PITX2 in the three PKs corneal buttons (n=3). Abbreviations: PK., penetrating keratoplasty; y./yy., year/s.
Figure 4.
Phenotypic characterization of the corneal buttons derived from the PKs of a patient treated by COMET. (A) Immunohistochemical analysis of the corneal buttons from the PKs at 1-, 3- and 10-years post-COMET. Representative images of positive (a, c, d, g) and negative (b, e, f, h) areas are shown in the panel; the images related to the 3-years corneal button highlighted a transitional zone between oral mucosa and another epithelium (d) and a zone with conjunctival epithelium with a cluster of goblet cells (f). Scale bars = 50 μm. (B) Graph showing the percentage of the positive epithelial length for PITX2 in the three PKs corneal buttons (n=3). Abbreviations: PK., penetrating keratoplasty; y./yy., year/s.
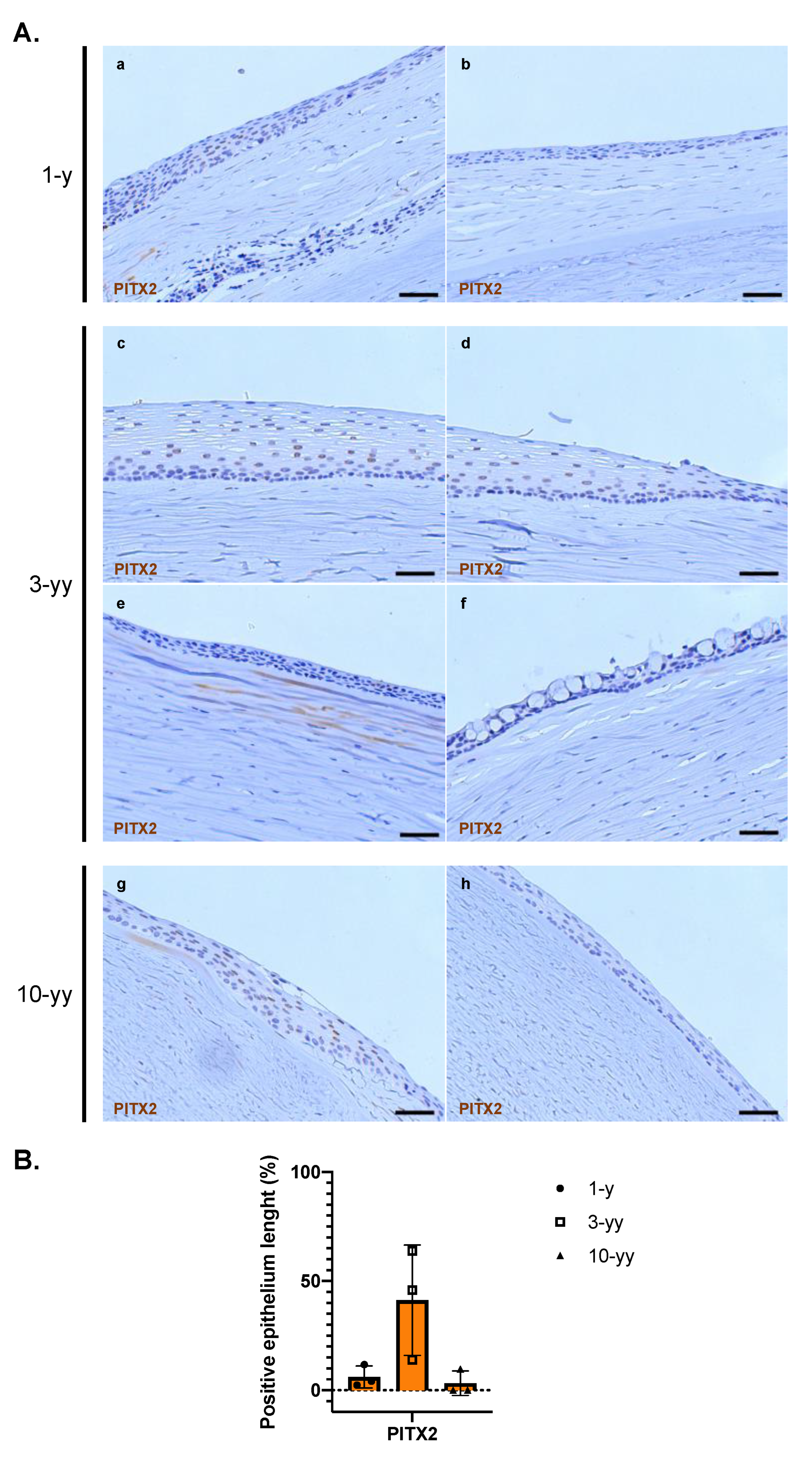
Figure 5.
Analysis of angiogenesis-related factors in the microarray comparisons. (A) Ingenuity Pathway Analysis of the DEGs in oral mucosa versus conjunctiva related to angiogenesis; (B) Heatmap describing gene expression profiles of DEGs in oral mucosa in comparison with limbus and conjunctiva related to angiogenesis (created using Partek® software). Abbreviations: CON, conjunctiva; LE, limbus; MO, oral mucosa. The ANOVA-based pairwise comparison among the three epithelia highlighted the differentially expressed genes (DEGs, fold change (FC) ≥ 2 and FDR < 0.05 for upregulated; FC ≤ -2 and FDR < 0.05 for downregulated) in oral mucosa vs. cornea or vs. conjunctiva (Spreadsheets S1–S3 in [20]).
Figure 5.
Analysis of angiogenesis-related factors in the microarray comparisons. (A) Ingenuity Pathway Analysis of the DEGs in oral mucosa versus conjunctiva related to angiogenesis; (B) Heatmap describing gene expression profiles of DEGs in oral mucosa in comparison with limbus and conjunctiva related to angiogenesis (created using Partek® software). Abbreviations: CON, conjunctiva; LE, limbus; MO, oral mucosa. The ANOVA-based pairwise comparison among the three epithelia highlighted the differentially expressed genes (DEGs, fold change (FC) ≥ 2 and FDR < 0.05 for upregulated; FC ≤ -2 and FDR < 0.05 for downregulated) in oral mucosa vs. cornea or vs. conjunctiva (Spreadsheets S1–S3 in [20]).
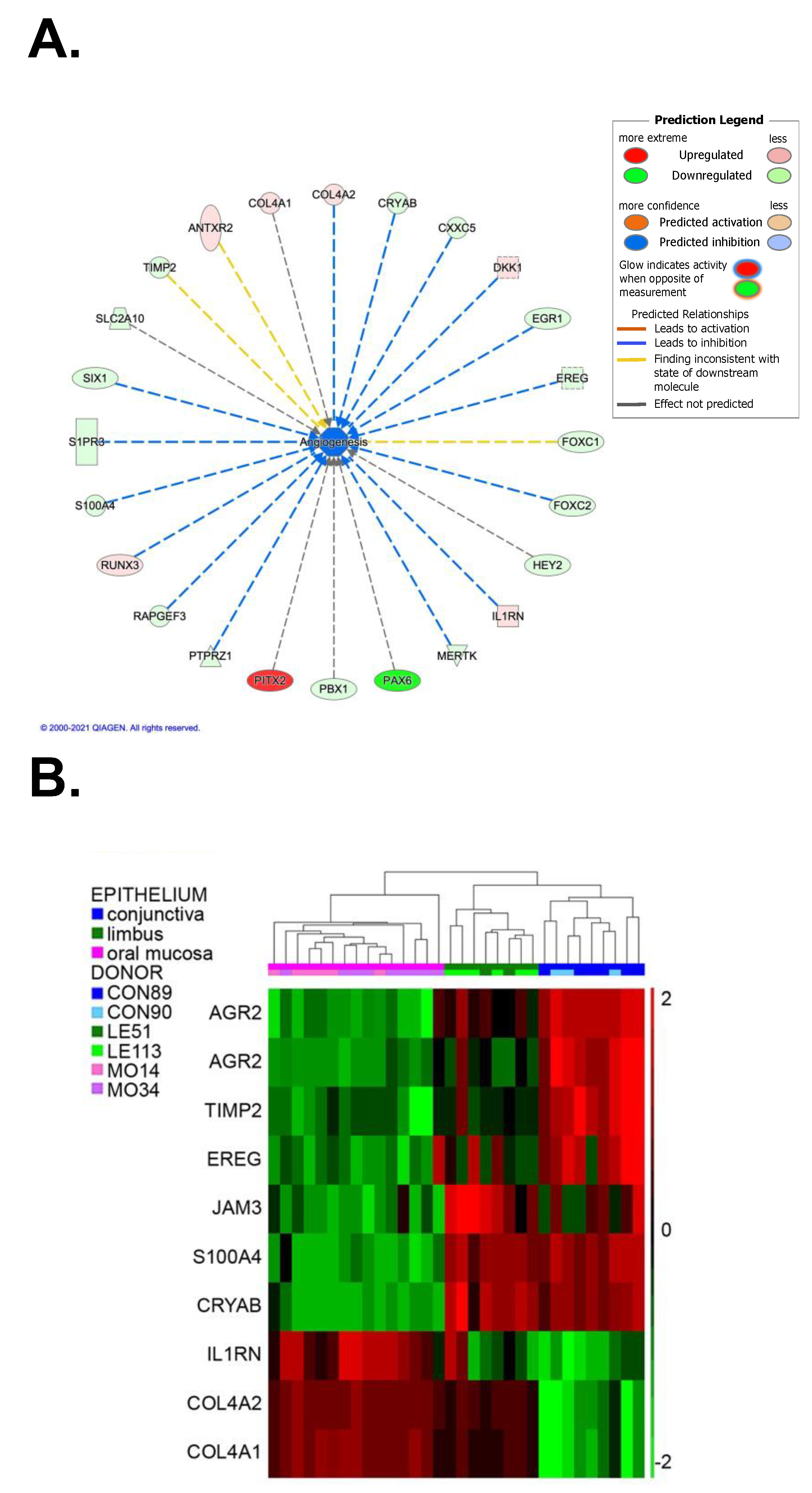
Figure 6.
Possible scenarios of the mechanisms of ocular surface regeneration after COMET procedure (created with Biorender.com).
Figure 6.
Possible scenarios of the mechanisms of ocular surface regeneration after COMET procedure (created with Biorender.com).
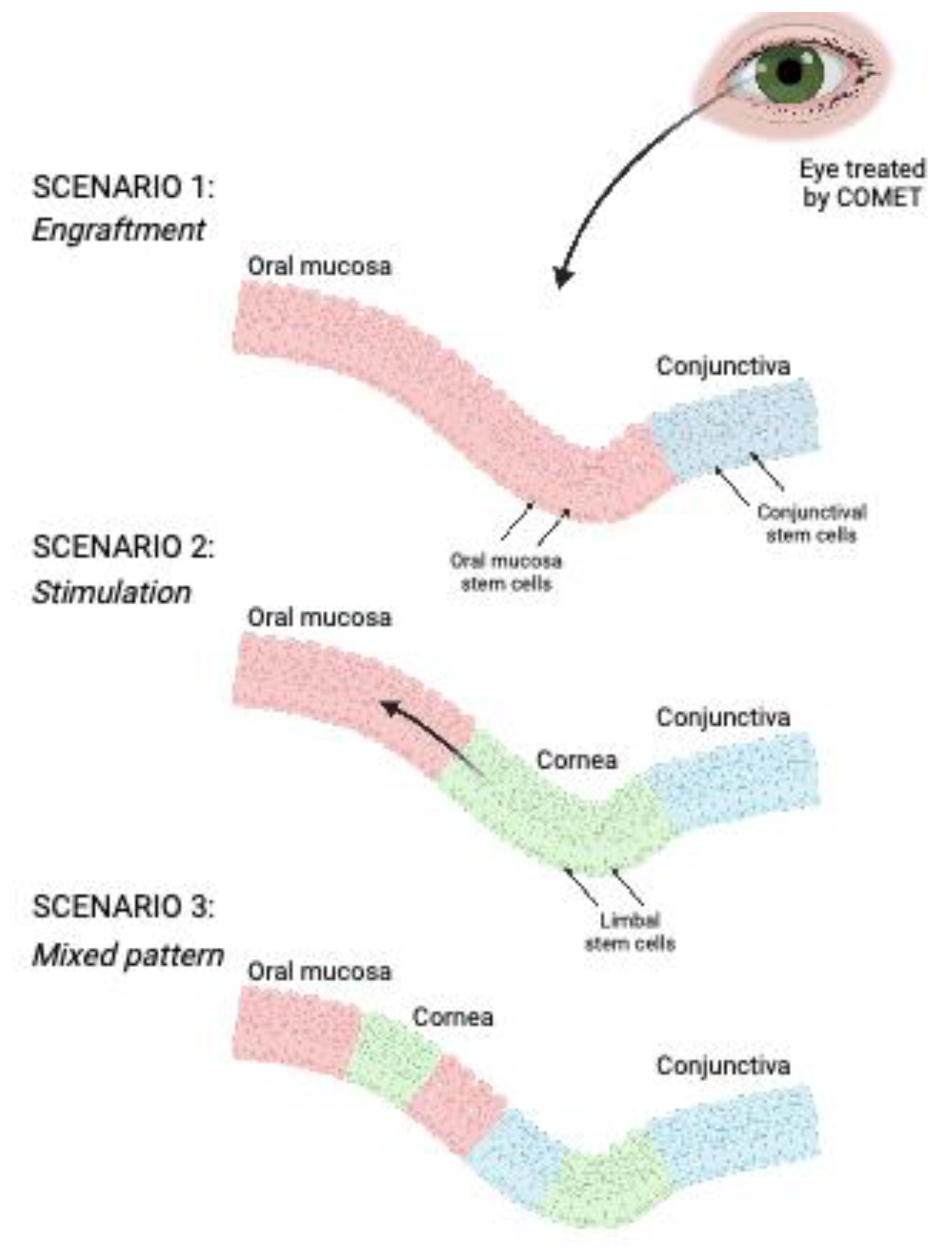

Table 1.
Strains and their holoclones analyzed. Abbrevations: CON: Conjunctiva; LE: Limbus; MO: Oral mucosa.
Table 1.
Strains and their holoclones analyzed. Abbrevations: CON: Conjunctiva; LE: Limbus; MO: Oral mucosa.
| Epithelium | Strain | N. of holoclones |
|---|---|---|
| Conjunctiva | CON-89 | 6 |
| CON-90 | 3 | |
| Limbus | LE-51 | 2 |
| LE-113 | 6 | |
| Oral Mucosa | MO-14 | 6 |
| MO-34 | 9 |
Table 2.
List of forward and reverse primers used for isoforms analysis of PITX2 [25].
Table 2.
List of forward and reverse primers used for isoforms analysis of PITX2 [25].
| Target gene | Forward Primer (5’-3’) | Reverse Primer (5’-3’) |
|---|---|---|
| PITX2 tot | CAGCCTGAGACTGAAAGCA | GCCCACGACCTTCTAGCAT |
| PITX2A | GCGTGTGTGCAATTAGAGAAAG | CCGAAGCCATTCTTGCATAG |
| PITX2B | GCCGTTGAATGTCTCTTCTC | CCTTTGCCGCTTCTTCTTAG |
| PITX2C | ACTTTCCGTCTCCGGACTTT | CGCGACGCTCTACTAGTC |
| GAPDH | GACCACAGTCCATGCCATCAC | TCCACCACCCTGTTGCTGTAG |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



