
Submitted:
15 May 2023
Posted:
17 May 2023
You are already at the latest version
Abstract
Sudden unexpected death (SUD) is a fatal event that occurs in an apparently healthy subject so that such an abrupt outcome could have not been predicted. SUD - including sudden intrauterine unexplained death (SIUD), sudden neonatal unexpected death (SNUD), sudden infant death syndrome (SIDS), sudden unexpected death of the young (SUDY), sudden unexpected death in the adult (SUDA) - occurs as the first manifestation of an unknown underlying disease or within a few hours of presentation of a disease. SUD is a major unsolved, shocking form of death that occurs frequently and can happen at any time without warning. For each case of SUD, a review of clinical history data and performance of a complete autopsy, particularly focused on the study of the cardiac conduction system were carried out according to the necropsy protocol devised by the Lino Rossi Research Center, Università degli Studi di Milano, Italy. Research cases are represented by 75 SUD victims, subdivided into 15 SIUD, 15 SNUD, 15 SUDY, and 15 SUDA victims, collected and selected for this study. After the routine autopsy and clinical history analysis, the death remained unexplained and hence a diagnosis of SUD was assigned to the 75. subjects, which included45 females (60%) and 30 (40%) males, ranging in age from 27 gestational weeks to 76 years. Serial sections of the cardiac conduction system disclosed frequent congenital alterations, of the cardiac conduction system in fetuses and infants. An age-related significant difference in distribution among the 5 age-related groups was detected for the following anomalies of the conduction system: central fibrous body (CFB) islands of conduction tissue, fetal dispersion, resorptive degeneration, Mahaim fiber, CFB cartilaginous meta-hyperplasia, His bundle septation, sino-atrial node (SAN) artery fibromuscular thickening, atrio-ventricular junction hypoplasia, intramural right bundle branch, and SAN hypoplasia. The results data are useful to understand the cause of death for all SUD cases that were unexpected and would have otherwise remained unexplained, so to motivate medical examiners and pathologists to perform more in-depth studies.
Keywords:
autopsy
; post-mortem investigation
; sudden unexpected death
; sudden infant death syndrome
; sudden intrauterine unexpected death
; cardiac conduction system.
“Pallida mors pulsat aequo pede alterno pauperum tabernas regumque turres” (Pale death knocks with impartial footstep at the cottages of the poor and the palaces of kings) [Horatius QF. Carminum Libri 13 BC; IV: 13–4]
1. Introduction
Sudden unexpected death (SUD), by definition, is sudden, occurs as the first manifestation of an unknown underlying disease, or within few hours, and is unexpected by history. SUD is a common form of death, especially in the young, that represents a major public health problem with devastating impact on the involved families and communities. The dynamic of this event poses little, if any, hope for survival. The emotional consequences among families of victims are devastating, with high social costs for the loss of many potentially productive individuals [1] and for the psychological support programs for family members [2].
SUD can hit human individuals of any age, gender, ethnicity, and nationality. SUD includes sudden unexpected death of the young (SUDY), sudden infant death syndrome (SIDS), and sudden intrauterine unexpected death (SIUD), sudden neonatal unexpected death (SNUD), sudden infant death syndrome (SIDS), sudden unexpected death of the young (SUDY), sudden unexpected death in the adult (SUDA). The broad spectrum of SUD may have common risk factors affecting individuals of all ages, such as all chemicals that interfere with the way the body’s hormones work, or obstructive sleep apnea syndrome (OSAS) [3].
SIDS, or crib death, is the sudden unexpected death of an infant less than one year of age, with onset of the fatal episode apparently occurring during sleep, that remains unexplained after a thorough investigation, including performance of a complete autopsy and review of the circumstances of death and the clinical history [4]. SIDS is the most frequent death-causing syndrome in the first year of life, at a birth prevalence of 3.5‰ [5]. Since its definition introduced by the National Institute of Child Health and Human Development (NICHD) panel in 1991 [6], three decades of SIDS research have revealed only parts of its anatomo-pathological underlying features that interplay in determining SIDS.
Sudden intrauterine unexplained/unexpected death (SIUD), or unexpected stillbirth, is the late fetal death before the complete expulsion or removal of the fetus from the mother ≥25 weeks of gestation which is unexpected by history and is unexplained after review of the maternal clinical history and the performance of a general autopsy of the fetus, including examination of the placental disk, umbilical cord and membranes [7].
The causes of SUD are largely unknown due to lack of specialized post-mortem and clinical studies. The risk factors for SUD are largely unknown as the body of clinico-pathological and epidemiological research to explain SUD is scarce and fragmentary. We hypothesize that there are common risk factors for SUD affecting individuals of all ages, starting from a victim’s intrauterine existence. Except for our few previous reports [8,9,10,11], there are no studies on the cardiac conduction system in all age groups of subjects dying suddenly and unexpectedly.
This study aims to evaluate, in a more complete way as possible, series of cases of SUD of natural causes, according to the necropsy protocol devised by the Lino Rossi Research Center, Università degli Studi di Milano [12,13], in order to determine the presence and significance of the post-mortem findings in the cardiac conduction system, distributed by age groups.
2. Materials and Methods
2.1. Selection and classification of cases
The Lino Rossi Research Center of the Università degli Studi di Milano, Milan, Italy, is a specialist referral center for cases of suspected sudden unexpected death (SUD) across Italy, with a database of over 1,000 cases. Close relatives or parents of deceased subjects provided written informed consent to the autopsy examination, according to protocols approved by the institutional review board (IRB) of the Lino Rossi Research Center, with the Department of Biomedical, Surgical and Dental Sciences, Università degli Studi di Milano, Milan, Italy providing funding support PSR 2020, linea 2 on 20 November, 2020.
All cases of unexpected infant and perinatal death referred to the Lino Rossi Center underwent anatomo-clinical investigations, according to the Italian law no 31 of 2/02/06 “Regulations for diagnostic post-mortem investigation in victims of sudden infant death syndrome (SIDS) and of unexpected fetal death” [14]. Confidentiality and privacy in personal data collection and processing were ensured following the European and U.S. legislation on these matters.
In the referred cases, natural death presumably due to subtle cardiovascular or brainstem lesions was suspected because no lesions found at general autopsy could explain death, after the exclusion of non-natural cause of death and after the toxicological examinations were negative for drug or alcohol abuse. For the purposes of this work, the study population consists of 75 consecutive autopsy cases of SUD submitted to the Lino Rossi Research Center of the Università degli Studi di Milano, after the performance of a general autopsy was not able to establish the cause of death, seeking for more in-depth anatomo-pathological investigations.
Based on the age at death, the SUD cases were sub-classified post-mortem in five categories, as follows:
- 1)
- Sudden Intrauterine Unexpected Death (SIUD) when a fetus, from the 25th gestational week to term, died suddenly and unexpectedly, before complete expulsion or extraction of the fetus from the mother, resulting in a stillbirth for which there was no explanation after review of the maternal clinical history and the performance of a general autopsy of the fetus, including examination of the fetal adnexa, i.e., placental disk, umbilical cord and membranes [7,10,12].
- 2)
- Sudden Neonatal Unexpected Death (SNUD) when a newborn, aged from birth to one month, died suddenly, unexpectedly by history and unexplainably after a thorough case investigation, including performance of a general autopsy, examination of the death scene, and review of the clinical history [7,12,15].
- 3)
- 4)
- Sudden Unexpected Death in the Young (SUDY), when the death occurred in an individual aged 1-35 years, suddenly and unexpectedly in an apparently healthy subject so that such an abrupt outcome could have not been predicted, unexplained after the review of the scene of death and the clinical history, and the performance of a general autopsy.
- 5)
- Sudden Unexpected Death in the Adult (SUDA), when the death occurred in an individual older than 35 years, suddenly and unexpectedly in an apparently healthy subject so that such an abrupt outcome could have not been predicted, unexplained after the review of the scene of death and the clinical history, and the performance of a general autopsy.
A case was classified as Sudden Unexpected Death (SUD) - including SIUD, SNUD, SIDS, SUDY SUDA - when the death occurred suddenly since the beginning of symptoms and unexpectedly by history.
A SIUD or SIDS case was classified as gray zone or borderline when it was unexpected by history and unexplained after review of the clinical history and performance of a general autopsy which disclosed another event, acting as a triggering phenomenon itself not enough to cause death, in vulnerable individual [16,17].
A total of 75 consecutive autopsy cases referred to the Lino Rossi Center were retrospectively enrolled into the study, if they met the pathological criteria to be divided in the two following groups, for comparison: 1) SIUD group: 15 cases; 2) SNUD group: 15 cases; 3) SIDS group; 4) SUDY group: 15 cases; 5) SUDA group: 15 cases.
2.2. Necropsy investigational protocol
For each study case, a full review of clinical history data and performance of a complete autopsy study were carried out according to the necropsy protocols devised by the Lino Rossi Research Center, Anatomic Pathology, Università degli Studi di Milano, Milan, Italy [12,13,16]. In particular, in all cases an in-depth histopathological examination of the cardiac conduction system and of the brainstem on serial sections was performed, with the principal aim of detecting even fine alterations in structures controlling the vital functions.
The clinical information of the SUD victims was provided by the referring pathologists or coroners.
The complete autopsy examination was carried out, including a systemic gross and microscopic evaluation of the body. In fetuses, the placental disk, the umbilical cord, and the membranes were examined. All organs were fixed in 10% phosphate-buffered formalin, processed and paraffin-embedded. The cardiac conduction system was the particular focus of this study.
Each heart was regularly examined for pathological changes in the atria, septa, ventricles, pericardium, endocardium, and coronary arteries. The origin of the coronary arteries was carefully inspected. Multiple samples of the major coronary arteries (left main, left anterior descending, left circumflex, right main, right posterior descending, right marginal) were collected and examined. Samples of the myocardium and coronary arteries were stained with Hematoxylin–Eosin (HE) and Trichromic Heidenhain (Azan).
For the morphological study of the conduction system, two specimens of the heart were obtained for paraffin embedding. The first specimen contained the sino-atrial node (SAN), its atrial approaches, the crista terminalis and the SAN gangliar plexus. The main visual reference for the removal was centered upon the sulcus-crista terminalis. Two longitudinal cuts were driven, parallel to the sulcus-crista line, through the atrial wall with a medial prolongation on the right side to encompass the anterior aspect of the inlet of the superior vena cava. On the left side, the cava-cava bridge was sectioned medially, prolonging the cut on the superior vena cava wall. The second specimen contained the atrio-ventricular (AV) junction with its atrial approaches: the pinpoints of the excision were, on the right side, the outlet of the coronary sinus and the pars membranacea septi. The following cuts were driven: an inferior, longitudinal incision through the posterior part of the septum, across the AV annulus fibrous and up to the superior margin of the coronary sinus ostium; an anterior longitudinal incision parallel to the former, through the superior part of the septum, extending to the aortic valvular ring; and two cuts perpendicular to the previous two cuts. Both samples were routinely fixed in 10% buffered formalin and paraffin-embedded. The sections were cut at intervals of 20-40 μm (levels). For each level, five 8-μm sections were retained, mounted, and alternately stained with HE and Azan. All intervening sections were kept and stained as deemed necessary [10,16].
For the morphological study of the brainstem, three specimens of the brainstem were obtained for paraffin embedding. The first specimen, ponto-mesencephalic, included the upper third of the pons and the adjacent portion of caudal mesencephalon. The second specimen, ponto-medullary, extended from the caudal portion of the pons to the upper portion of the medulla oblongata. The third specimen, medullary, took as reference point the obex and extended 2–3 mm above it and below it. Transverse serial sections throughout the three samples, from the midbrain, pons and medulla oblongata, were carried out at intervals of 60-μm. For each level, six 4-μm sections were obtained, three of which were routinely stained with HE and Klüver–Barrera. The remaining sections were saved for further investigations and stained as deemed necessary [2,18].
2.3. Statistical analysis
Quantitative data were expressed as means ± SD. The significance of differences between group parameters was evaluated by Student's t-test, Chi-square test, or Fisher's test. In case of skewed distribution, a nonparametric Whitney rank sum test was used. One-way ANOVA test for continuous variables was used for quantifying and partitioning variance between groups. When the results suggested differences, pairwise differences were assessed by Bonferroni's post hoc test. The relationship between variables was analyzed by Pearson correlation test. Statistics were compiled using SigmaStat® (version 4, Systat Software Inc, Chicago, IL) and plotted using SigmaPlot ® (version 14, Systat Software Inc, Chicago, IL) statistical softwares. The selected level of significance was P < 0.05, two-tailed.
3. Results
In accordance with the aim of this study, an in-depth necropsy examination of victims of sudden unexpected death (SUD) of natural causes was carried out grouping the victims according to the age at death.
3.1. Demographic and Clinical Data
Of a series of over 1,000 cases submitted to the Lino Rossi Research Center of the Università degli Studi di Milano, Milan, Italy, for specialized anatomo-pathological post-mortem analyses, collected from January 1987 to date, 75 consecutive victims of sudden unexpected death (SUD) divided by age were selected for this study. The demographic and clinical data are shown on Table 1.
The 75 SUD victims enrolled into this study, referred to the Lino Rossi Center, Università degli Studi di Milano for more in-depth investigations, were subdivided into the following five age-related groups:
- 1)
- 15 victims of sudden intrauterine unexpected death (SIUD) aged 25th gestational week (gw) to birth,
- 2)
- 15 victims of sudden neonatal unexpected death (SNUD) aged from birth to one postnatal month,
- 3)
- 15 victims of sudden infant death syndrome (SIDS) aged from one postnatal month to one postnatal year,
- 4)
- 15 victims of sudden unexpected death in the young (SUDY) aged 1-35 years (yrs),
- 5)
- 15 victims of sudden unexpected death in the adult (SUDA) older than 35 years, as shown in Table 1.
Accordingly, in this study, in the SUD cases analyzed, a diagnosis of SIUD was established in 15 fetuses, 9 (60%) males and 6 (40%) females; age range: 27-41 gws (mean age ± SD, 37.39 + 3.69 gws). The 15 SNUD newborns were 10 (66.67%) males and 5 (33.33%) females; age range: 1 hour-28 days after birth (mean age ± SD, 7.08 + 9.92 days). The 15 SIDS infants were 7 (46.67%) males and 8 (53.33%) females; age range: 31-225 postnatal days (mean age ± SD, 105.67 + 59.84 days). The 15 SUDY young subjects were 10 (66.67%) males and 5 (33.33%) females; age range: 15 months-33 yrs (mean age ± SD, 22.92 + 10.33 yrs). The 15 SUDA adults were 9 (60%) males and 6 (40%) females; age range: 36-76 yrs (mean age ± SD, 49.69 + 11.72 yrs) (Table 1).
Among the 75 SUD cases, ranging in age from 27 gws-76 yrs, the males, 45 (60%) were statistically more frequent than the 30 (40%) females (Figure 1).
Two cases of SIUD were classified as SIUD gray zone, due respectively to a concomitant amniotic fluid aspiration and chorioamnionitis. One case of SIDS was classified as SIDS gray zone due to a concomitant diagnosis of malaria. Three cases were classified as SNUD gray zone due to coexistent multiple cerebral ventricular and periventricular hemorrhages in one case, and pneumonia in two cases.
The investigation of the SUDY cases, disclosed the anatomopathological diagnosis of dilated cardiomyopathy (DCMP) in one case (6.67%), of hepatic insufficiency in two cases (13.33%), of myocarditis in three cases (20%), coronary anomalous origin in one case (6.67%), myocardial infarction in two cases, and of arrhythmogenic right ventricular cardiomyopathy (ARVC) in five cases (33.33%). The clinico-pathological findings of the SUDA cases, disclosed DCMP in one case (6.67%), myocarditis in two cases (13.33%), lymphoma metastases in two cases (13.33%), myocardial infarction in two cases (13.33%), and ARVC in five cases (33.33%). The findings of the conducting tissue of ARVC cases, as hypoplasia of the conduction system due to fibro-fatty tissue infiltration, now belonging to the groups of SUDY and SUDA, were previously reported [11].
3.2. Cardiac Conduction System Findings
The 75 SUD cases, in which the CCS has been fully analyzed, consisted of 15 cases of SIUD, 15 cases of SNUD, 15 cases of SIDS, 15 cases of SUDY, and 15 cases of SUDA.
In the 75 SUD cases, the following anomalies of the CCS, have been detected in the following percentages of cases: Islands of conduction tissue in the central fibrous body (CFB) 54.67%; Fetal dispersion 46.67%; Resorptive degeneration in 45.33%; Mahaim fiber in in 45.33%; CFB cartilaginous meta-hyperplasia in 30.67%; Septated bifurcation in 24%; Septated His bundle (HB) in 24%; Fibromuscular thickening of the sino-atrial node (SAN) artery in 14.67%; Fibromuscular thickening of the atrio-ventricular node (AVN) artery in 13.33%; AVN duplicity in 10.67%; Intramural bifurcation in 10.67%; Hemorrhage and infarct-like lesions in the atrio-ventricular junction (AVJ) in 10.67%; AVJ hypoplasia in 9.33%; Intramural right bundle branch (RBB) in 9.33%; CBF hypoplasia in 6,67%; SAN hypoplasia in 5.33%; Septated AVN in 4%; AVN tongue in 2.67%; Intramural left bundle branch (LBB) in 2.67%; Intramural His bundle (HB) in 2.67%; HB duplicity in 2.67%; SAN hemorrhage and infarct-like lesions in 1.3% (Table 1).
An age-related statistically significant difference in distribution among the 5 age-related groups was detected for the following anomalies of the conduction system: CFB islands of conduction tissue, fetal dispersion, resorptive degeneration, Mahaim fiber, CFB cartilaginous meta-hyperplasia, HB septation, SAN artery fibromuscular thickening, AVJ hypoplasia, intramural RBB, and SAN hypoplasia (Table 1).
Although some lesions were detected only in some groups, such as the AVJ hypoplasia was detected only in SUDY and SUDA, and the AVN tongue was detected only in the SUDY group, the difference among groups was not statistically significant, not age-related (Table 1).

Table 1.
Demographic data and histopathological findings of the 75 analyzed cases, divided by sudden intrauterine unexpected death (SIUD), sudden neonatal unexpected death (SNUD), sudden infant death syndrome (SIDS), sudden unexpected death in the young (SUDY), and sudden unexpected death in the adult (SUDA) groups.
Table 1.
Demographic data and histopathological findings of the 75 analyzed cases, divided by sudden intrauterine unexpected death (SIUD), sudden neonatal unexpected death (SNUD), sudden infant death syndrome (SIDS), sudden unexpected death in the young (SUDY), and sudden unexpected death in the adult (SUDA) groups.
| SIUD (N=15) | SNUD (N=15) | SIDS (N=15) | SUDY (N=15) | SUDA (N=15) | Total (N=75) | |
|---|---|---|---|---|---|---|
| N° of cases | 15 | 15 | 15 | 15 | 15 | 75 |
| Gender (M/F) | 9/6 | 10/5 | 7/8 | 10/5 | 9/6 | 45/30 |
| Age range; mean ± SD |
27-41 gw; 37.39 ± 3.69 gw |
1 hr-28 dy; 7.08 ± 9.92 dy |
31-225 dy; 105.67 ± 59.84 dy |
14 ms – 33 yr; 22.92 ± 10.33 yr |
36-76 yr; 49.69 ± 11.72 yr |
27 gw-76 yr |
| CFB: Islands of conduction tissue | 10 (66.67%) | 13 (86.67%) | 8 (53.33%) | 6 (40%) | 4 (26.67%) | 41 (54.67%)* |
| Fetal dispersion | 12 (80%) | 12 (80%) | 9 (60%) | 4 (26.67%) | 3 (20%) | 35 (46.67%)* |
| Resorptive degeneration | 10 (66.67%) | 14 (93.33%) | 7 (46.67%) | 2 (13.33%) | 2 (13.33%) | 34 (45.33%)* |
| Mahaim fiber | 5 (33.33%) | 10 (66.67%) | 13 (86.67%) | 3 (20%) | 3 (20%) | 34 (45.33%)* |
| CFB cartilaginous meta-hyperplasia | 5 (33.33%) | 4 (26.67%) | 12 (80%) | 2 (13.33%) | — | 23 (30.67%)* |
| BIF: Septated | 5 (33.33%) | 6 (40%) | 1 (6.67%) | 2 (13.33%) | 4 (26.67%) | 18 (24%) |
| HB Septated | 1 (6.67%) | 2 (13.33%) | 7 (46.67%) | 1 (6.67%) | 1 (6.67%) | 12 (16%)* |
| Fibromuscular thickening SAN artery | — | — | 3 (20%) | 3 (20%) | 5 (33%) | 11 (14.67%)* |
| Fibromuscular thickening AVN artery | — | 1 (6.67%) | 4 (26.67%) | 1 (6.67%) | 4 (26.67%) | 10 (13.33%) |
| AVN duplicity | 1 (6.67%) | 4 (26.67%) | 2 (13.33%) | 1 (6.67%) | — | 8 (10.67%) |
| BIF Intramural | 2 (13.33%) | 3 (20%) | 1 (6.67%) | 1 (6.67%) | 1 (6.67%) | 8 (10.67%) |
| AVJ: Hemorrhage and infarct-like lesions | — | 3 (20%) | 1 (6.67%) | 3 (20%) | 2 (13.33%) | 8 (10.67%) |
| AVJ hypoplasia | — | — | — | 1 (6.67%) | 6 (40%) | 7 (9.33%)* |
| RBB: Intramural | 4 (26.67%) | 1 (6.67%) | — | — | 1 (6.67%) | 6 (8%)* |
| CFB hypoplasia | 2 (13.33%) | — | — | 2 (13.33%) | 1 (6.67%) | 5 (6.67%) |
| SAN hypoplasia | — | — | — | 4 (26.67%) | 2 (13.33%) | 4 (5.33%)* |
| AVN Septated | — | 1 (6.67%) | 1 (6.67%) | 1 (6.67%) | — | 3 (4%) |
| AVN tongue | — | — | — | 2 (13.33%) | — | 2 (2.67%) |
| LBB: Intramural | 1 (6.67%) | — | 1 (6.67%) | — | — | 2 (2.67%) |
| HB: Intramural | 1 (6.67%) | — | — | 1 (6.67%) | — | 2 (2.67%) |
| HB duplicity | — | — | 1 (6.67%) | 1 (6.67%) | — | 2 (2.67%) |
| SAN: Hemorrhage and infarct-like lesions | — | — | — | — | 1 (6.67%) | 1 (1.3%) |
Age groups: SIUD: before birth; SNUD: 0-30 days; SIDS: 1-12 months; SUDY: 1-35 years; SUDA: > 35 years. Abbreviations: M = male; F = female; gw = gestational weeks; N = Number of cases; hr = hour; dy = days; ms, months; yr, years; SAN = sino-atrial node; HB = His bundle; AVN = atrio-ventricular node; AVJ = atrio-ventricular junction; BIF = bifurcation (of HB bundle); CFB = central fibrous body; LBB = left bundle branch; RBB = right bundle branch; — = absent. *Statistically significant: Chi-square test; P < 0.05.
We observed islands of conduction in CFB system more frequently in SNUD (86.67%) and less frequently in SUDA (26.67%) (Table 1). In such cases, we observed islands of AVJ inside the CFB (Figure 2) as a form persistent fetal dispersion, in part undergoing the process of resorptive degeneration (Figure 2B), which is the process of molding and reabsorption of the AVJ from the embryonic toward the adult shape [8,9,10,11].
We observed areas of fetal dispersions, in the forms of AVJ undergoing the process of resorptive degeneration (Figure 3), in the vast majority (80%) of both SIUD and SNUD cases. Separated areas of resorptive degeneration were mostly seen in SIDS (93.33%) cases. Mahaim fibers, as accessory pathways connecting the AVJ directly with the myocardium of the interventricular septum (Figure 3), were mostly detected in SIDS (86.67%) cases. An AVN tongue was detected in 2.67% of SUD cases (Table 1).
We observed cartilaginous meta-hyperplasia of the CFB, potentially compressing the AVJ (Figure 4), in 36.67% of SUD cases, absent in the SUDA group, with an age-related distribution (Table 1).
HB septation, characterized by fibrous tissue infiltration from the CFB into the HB (Figure 5A), was mostly present in the SIDS group (46.67%) with an age-related distribution. Septation of the bifurcation (BF), or anomalous bifurcation (Figure 5B), was present in all age groups without significant age-related differences. Septated AVN was detected in only 4% of SUD cases (Table 1).
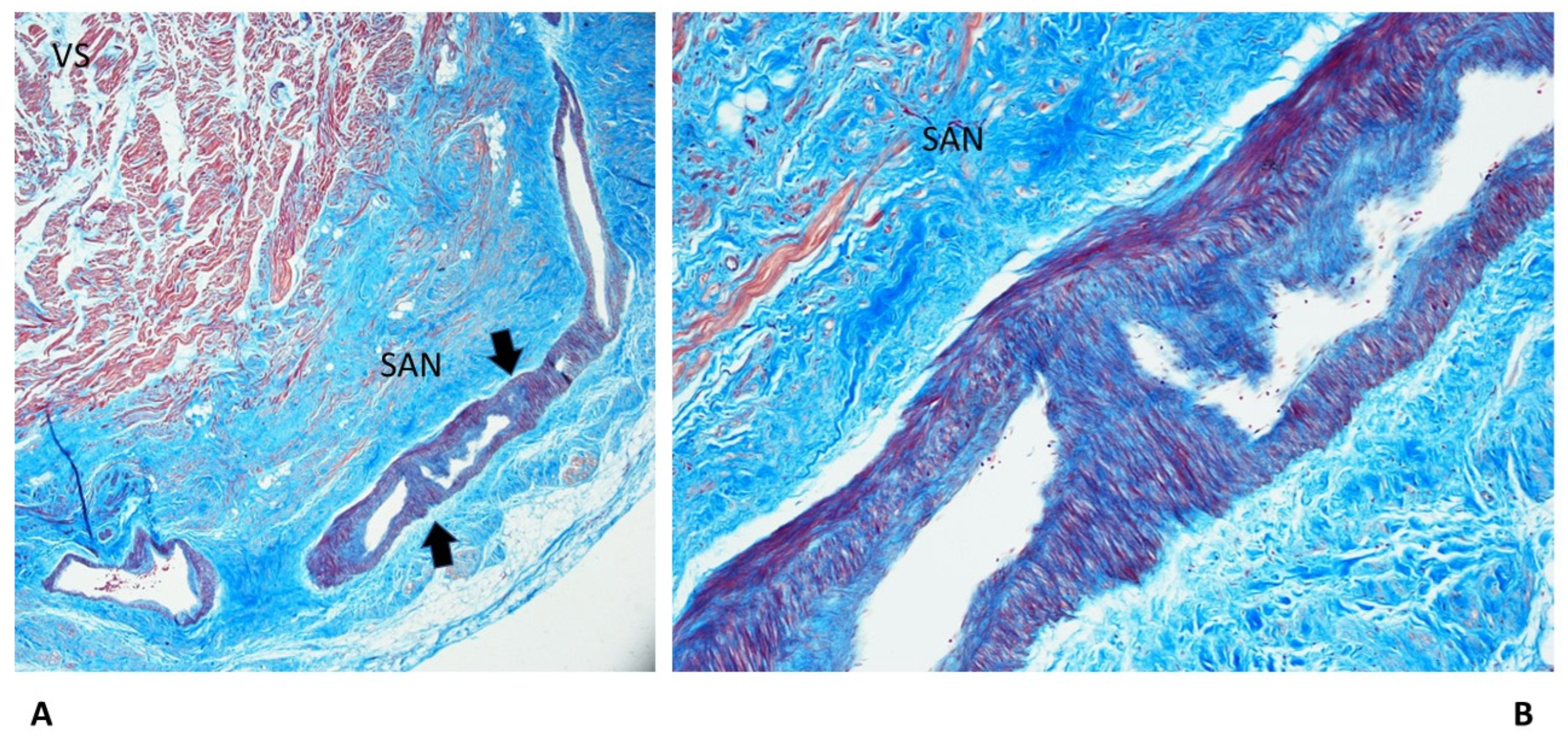
Fibromuscular thickening of the sino-atrial node (SAN) artery, as fibromuscular dysplasia (Figure 6), has been detected in 14.67% SUD cases correlated with age-increase, more frequently in the SUDA group (33%) (Table 1).
Fibromuscular thickening of the AVN artery, as fibromuscular dysplasia, has been detected in 13.33% of SUD cases. Although it was absent in the SIUD group and was more frequent in the SUDA group, the age distribution was not statistically significant (Table 1). AVJ duplicity, as AVN and HB duplicity, as split AVJ, was observed in 10.67% and 2.67% of SUD cases, respectively, without significant age differences (Table 1). Intramural AVJ, as intramural BIF, right bundle branch (RBB), left bundle branch (LBB), was observed in the decrescent prevalence of 10.67%, 8%, and 2.67% of SUD cases, respectively; also, the intramural HB was observed in 2.67% of cases, without age-related differences (Table 1). The AVJ and the SAN hemorrhage and infarct-like lesions, due to cardiac massage, were detected in 10.67% and 1.3% of SUD cases; they were absent in SIUD group, but differences were not significant (Table 1). We observed hypoplasia of the AVJ, of CFB and of SAN (Figure 6) in 9.33%, 6.67% and 5.33% of SUD cases, respectively, with age-related differences expect for the CFB hypoplasia (Table 1).
4. Discussion
Sudden unexpected death (SUD) is a fatal event that occurs in an apparently healthy subject so that such an abrupt outcome could have not been predicted. The emotional consequences among families are devastating with high social cost, considering also the post-traumatic stress disorders of family members [1,19].
Once unnatural cause of death is ruled out by the medical examiner, little attention, if any, is given to identify the pathogenesis and risk factors of SUD. There is a broad spectrum of SUD with possible common risk factors affecting individuals of all ages, starting from the intrauterine life. The anatomo-clinical substrates of SUD are largely unknown [20]. The incidence of SUD peaks in infancy and, in adults, it increases exponentially with age, surpassing the risk for infants by 35–39 years of age [21]. OSAS is the most common form of sleep-disordered breathing that affects approximately 10% of the adults and 5% of children [21]. Anastasakis et al [22] reported that sudden unexpected death of the young (SUDY) is of cardiovascular origin in 65% of cases, while remains unexplained in 18% of cases after autopsy investigations.
Unexpected stillbirth, or SIUD, has a 6-8 fold greater incidence than SIDS that has not significantly declined in the last three decades, despite modern advances in maternal-infant care [23].
Despite the valuable anatomo-pathological research over the last 30 years to explain SIDS and SIUD [8,9,24,25,26], overall, the body of literature on the findings in the heart is still scarce and fragmentary.
Among the congenital anomalies detected in SIDS and SIUD, the present abnormalities of the cardiac conduction system, including the resorptive degeneration, Mahaim fibers, and cartilaginous meta-hyperplasia (Figure 2, Figure 3 and Figure 4), have been reported along with several neuropathology anomalies of the autonomic nervous system structures, mainly the hypoplasia of the arcuate nucleus, the hypoplasia of the respiratory reticular formation and of the parabrachial/Kölliker-Fuse complex, significantly related to maternal cigarette smoking, in over 50% of cases [27,28,29,30,31,32].
Current guidelines for SIDS and other sudden arrhythmic death syndromes state the potential usefulness of molecular autopsy as cardiac channelopathies are regarded as a major genetic contributor to these sudden and otherwise unexplained deaths [20]. Massively parallel DNA-sequencing systems provide sequence of great numbers of different DNA strands at once. These technologies are revolutionizing our understanding of medical genetics, accelerating health-improvement projects, and laying the groundwork to fully understood personalized medicine in the near future. Whole-exome sequencing (WES) is the application of the next-generation technology to determine the variations of all coding regions, or exons, of known genes. Sequencing of the complete coding regions (exome) has the potential to uncover the causes of SIDS-SIUDS. There is very little knowledge about the WES application in early diagnosis of the potential SIDS-SIUD victims and healthy carriers, and in their utility in clinical screening.
Post-mortem examination is of great importance in every case of SUD sine materia, with examination of the cardiac conduction system and brainstem on serial sections, when general autopsy fails to find the cause of death, after exclusion of violent causes of death and the absence of any explained cause of death at a general autopsy.
4.1. Subjects’ Characteristics
In this study, among the 75 SUD subjects grouped by age from consecutive autopsy cases referred to the Lino Rossi Center, Università degli Studi di Milano, for more in-depth investigations, 15 were victims of Sudden Intrauterine Unexpected Death (SIUD) aged 25th gw to birth, 15 were victims of Sudden Neonatal Unexpected Death (SNUD) aged from birth to one postnatal month, 15 were victims of Sudden Infant Death Syndrome (SIDS) aged from one postnatal month to one postnatal year, 15 were victims of Sudden Unexpected Death in the Young (SUDY) aged 1-35 years, Sudden Unexpected Death in the Adult (SUDA) older than 35 years. (Table 1).
SUD of all ages were more frequent in males (60%) than in females (40%) (Figure 1).
Regarding SIUD, in the present study, we are reporting an higher incidence of males (60%) than females (40%) (Figure 1, Table 1). In a previous report of Ottaviani et al [10], another sample of 15 SIUD cases from our series presented an higher incidence in females (60%).
In the SNUD group, we found 66.67% males versus 33.33% females (Figure 1, Table 1). More epidemiological studies in larger series are needed to define the gender predominance in the sudden death occurring in the perinatal age, including both SIUD and SNUD.
Regarding SIDS, in present study, the percentage of females (53.33%) have been surprisingly higher than the percentage of males (46.67%) (Figure 1, Table 1). In a previous work Matturri et al [33], reported from our series of 102 cases, the males were 62.74% versus 37.26% females. Male sex has been considered to be a risk factor for SIDS, along with prone position, death during sleep, co-sleeping, preterm birth, among others [34,35].
In this study, the findings of SIUD, SNUD and SIDS gray zone is consistent with the proposed definition of Ottaviani [7,17] of gray zone or borderline cases. We suggest that the concept of SIDS-Gray zone, already described in the SIDS-SIUD complex [7], be applied to SUD cases of all ages, whenever an in-depth serial sections study of the conducting tissue would discover anomalies able to complete the puzzle of death cause in subjects with other pathological findings, such as ARVC in adults.
SUDY disclosed one case of DCMP (6.67%) and five cases of ARVC (33.33%). The percentages slightly differ from the reported prevalence of cardiomyopathy types in other series [36] as depended on the need for a diagnosis and the complimentary experience the referring pathologists were seeking in our institution. Thiene et al [37] reported 20% of sudden death in young athletes as “sine-materia”. Such cases could be explained as due to anomalies of the cardiac conduction system as we are now reporting them for this age group.
In the literature, there is not a clear consensus definition of SUD. In our study, SUD encompass all types of sudden unexpected death of natural causes of all ages, from pre-natal life to old age, including SIUD, SNUD, SIDS, SUDY, and SUDA. The SIUD, SNUD and SIDS have been grouped in the so-called SIDS-SIUD complex [7]. We suggest that they could all be part of Sudden arrhythmic death syndrome (SADS), as dysfunctions of the cardiac conduction and autonomic nervous systems are known to contribute to the pathogenesis of SADS [20].
4.2. Anatomo-pathological Findings in the Cardiac Conduction System
Research cases are represented by 75 SUD victims, subdivided into 15 SIUD, 15 SNUD, 15 SUDY, and 15 SUDA victims, collected and selected for this study, at the Lino Rossi research at the Università degli Studi di Milano, Italy. After the routine autopsy and clinical history analysis, the death remained unexplained and hence a diagnosis of “SUD” was made for the 75. subjects, 45 females (60%) and 30 (40%) males, ranging in age from 27 gws to 76 yrs. Serial sections of the cardiac conduction system were carried out to provide data on both topography and pathology of the specialized AV pathways.
As shown in Table 1, an age-related significant difference in distribution among the 5 age-related groups was detected for several anomalies of the conduction system, including CFB Islands of conduction tissue (Figure 2), fetal dispersion, resorptive degeneration, Mahaim fiber (Figure 3), CFB cartilaginous meta-hyperplasia (Figure 4), HB septation (Figure 5), SAN artery fibromuscular thickening and SAN hypoplasia (Figure 6) (Table 1). The fact that the same anomalies are found in all groups suggest their congenital nature.
The anomalies found in the conducting system could be the morphological bases for the development of cardiac arrhythmias. Islands of conduction system in the CFB could act as potential arrhythmogenic ectopic foci in all age groups. In 1968, James [38] suggested the idea that the resorptive degeneration of the AVJ was the process by which that conducting system of infants go through partial reabsorption toward its adult’s shape. According to Matturri et al [39], apoptosis takes part on this reabsorption process and leaves accessory pathways or ectopic foci of conduction system if it is defective. On the other hand, according to James [40], an exaggerated resorptive degeneration can cause hypoplasia of the AVJ. In this study, the resorptive degeneration has been detected in all age groups, demonstrating its role in the sudden unexpected death of all ages.
In this study, some anomalies CCS lesions detected mostly in fetuses and infants rather than in adults, such as cartilaginous meta-hyperplasia of the CFB (Table 1) (Figure 4) and AVN duplicity. Some anomalies were not detected in the SIUD, SNUD and SIDS groups, such as the AVJ and SAN hypoplasia (Table 1) (Figure 6), which has been reported to be related to metastatic infiltration or ARVC involvement in the adult groups [11,41,42]. AVN tongue was not detected in fetuses and infants (Table 1), but it was reported to be present in 13% of the SIUD cases in a previous study [10]. More research is needed as there is lack of studies on the cardiac conduction system in all age groups of subjects dying suddenly and unexpectedly.
Islands of AVJ inside the CFB (Figure 2), are also known as a form persistent fetal dispersion [8,10], but they differ from fetal dispersion (Figure 3) which is itself a normal pattern of the AVJ distribution in fetuses.
Intramural HB, bifurcation, LBB or RBB (Table 1) can be grouped into intramural AVJ and are morphological bases for cardiac arrhythmias [16] based on the different location of the itself normal conductive pathways.
Hemorrhage and infarct-like lesions of the AVJ or SAN (Table 1) have been considered to be a consequence of cardiac massage [43,44]. In this study, they were not detected in the SIUD group, given that usually a cardiac massage is not performed in fetuses, unless the death occurs during birth.
Fibromuscular thickening of the SAN or AVN artery (Figure 6), as fibromuscular dysplasia, is itself not of clear atherosclerotic nature [25], has been detected in 14.67% SUD cases correlated with age-increase, more frequently in the SUDA group (33%) (Table 1). In a previous study of Matturri et al [25], the fibromuscular thickening has been detected in infants and suggested to be an early stage of atherosclerotic lesions, correlated with parents’ smoking.
Our cases of SUD of all ages were unexpected by history and a cause of death was not identified after a routine general autopsy, but they were explained through a detailed post-mortem investigation of the cardiac conduction system.
The study’s methods of the investigation of the conduction system through serial sections will have a potential application for any form of sudden death occurring at any age. Potential mechanisms underlying these frequent, but yet overlooked and not always considered to be correlated forms of death. However, the applied method of cardiac sampling to analyze the cardiac conduction system on serial section is expensive, time-consuming and requires trained personnel, both cardiovascular pathologists and laboratory histotechnicians.
The results data are useful to understand the cause of death for those unexpected cases that would have otherwise remained unexplained, so to motivate medical examiners and pathologists to perform more in-depth studies.
More research is needed to explore congenital alterations involved in the SUD pathogenesis and progression, such as hypodevelopment of cardiac conduction system and brainstem nuclei; To explore the risk factors of any clinical conditions, such as obstructive sleep apnea syndrome (OSAS), and to explore the relationship between them and SUD; To increase the knowledge on SUD in order to ultimately prevent this thorny problem and mitigate social concern over the issue.
5. Conclusions
SUD - including sudden intrauterine unexplained death (SIUD), sudden neonatal unexpected death (SNUD), sudden infant death syndrome (SIDS), sudden unexpected death of the young (SUDY), sudden unexpected death in the adult (SUDA) - occurs as the first manifestation of an unknown underlying disease or within a few hours of presentation of a disease. SUD is a major unsolved, shocking form of death that occurs frequently and can happen at any time without warning.
This study analyzed the pathological findings of SUD of all ages, discussing the potential mechanisms underlying these frequent, but yet overlooked and not always considered to be correlated forms of death. Post-mortem examination is of great importance in every case of SCD sine materia, with examination of the cardiac conduction system on serial sections, when general au-topsy fails to find the cause of death.
More research is needed as there is lack of studies on the cardiac conduction system in all age groups of subjects dying suddenly and unexpectedly.
Author Contributions
Conceptualization, G.O. and S.G.R.; methodology, G.O.; software, G.O.; validation, G.O. and S.G.R.; formal analysis, G.O.; investigation, G.O.; resources, G.O.; data curation, G.O.; writing—original draft preparation, G.O.; writing—review and editing, S.G.R.; visualization, S.G.R.; supervision, S.G.R., G.O.; project administration, G.O.; funding acquisition, G.O.
Funding
This study was supported, in part, by the Italian Health’s Ministry in accordance with the Law 31/2006 “Regulations for Diagnostic Post Mortem Investigation in Victims of Sudden Infant Death Syndrome (SIDS) and Unexpected Fetal Death”.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of the Università degli Studi di Milano reviewed and approved this re-search project on November 20, 2020, providing funding support.
Informed Consent Statement
Close relatives of all the study subjects who underwent autopsy and were enrolled in this study have provided written informed consent to the autopsy and genetic investigations, in accordance with Italian and international laws
Acknowledgments
The authors express their gratitude to Dr. Graziella Alfonsi and Dr. Patrizia Leonardi for skillful technical corporation, and to Dr. Stephan G. Zajac for English language assistance.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mirzaei, M.; Joodi, G.; Bogle, B.; Chen, S.; Simpson, R.J. Years of Life and Productivity Loss Because of Adult Sudden Unexpected Death in the United States. Med. Care 2019, 57, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Ottaviani, G.; Buja, L.M. Anatomopathological Changes of the Cardiac Conduction System in Sudden Cardiac Death, Particularly in Infants: Advances over the Last 25 Years. Cardiovasc. Pathol. 2016, 25, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Ottaviani, G.; Buja, L.M. Pathology of Unexpected Sudden Cardiac Death: Obstructive Sleep Apnea Is Part of the Challenge. Cardiovasc. Pathol. 2020, 47, 107221. [Google Scholar] [CrossRef] [PubMed]
- Krous, H.F.; Beckwith, J.B.; Byard, R.W.; Rognum, T.O.; Bajanowski, T.; Corey, T.; Cutz, E.; Hanzlick, R.; Keens, T.G.; Mitchell, E. a Sudden Infant Death Syndrome and Unclassified Sudden Infant Deaths: A Definitional and Diagnostic Approach. Pediatrics 2004, 114, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Linked Birth/Infant Death Records, 2018 Results.
- Willinger, M.; James, L.S.; Catz, C. Defining the Sudden Infant Death Syndrome (SIDS): Deliberations of an Expert Panel Convened by the National Institute of Child Health and Human Development. Pediatr. Pathol. 1991, 11, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Ottaviani, G. Defining Sudden Infant Death and Sudden Intrauterine Unexpected Death Syndromes with Regard to Anatomo-Pathological Examination. Front. Pediatr. 2016, 4, 103. [Google Scholar] [CrossRef] [PubMed]
- Matturri, L.; Ottaviani, G.; Ramos, S.G.; Rossi, L. Sudden Infant Death Syndrome (SIDS): A Study of Cardiac Conduction System. Cardiovasc. Pathol. 2000, 9, 137–145. [Google Scholar] [CrossRef]
- Ottaviani, G.; Matturri, L.; Rossi, L.; James, T.N. Crib Death: Further Support for the Concept of Fatal Cardiac Electrical Instability as the Final Common Pathway. Int. J. Cardiol. 2003, 92, 17–26. [Google Scholar] [CrossRef]
- Ottaviani, G.; Matturri, L. Histopathology of the Cardiac Conduction System in Sudden Intrauterine Unexplained Death. Cardiovasc. Pathol. 2008, 17, 146–155. [Google Scholar] [CrossRef]
- Ottaviani, G.; Alfonsi, G.; Ramos, S.G.; Buja, L.M. Sudden Unexpected Death Associated with Arrhythmogenic Cardiomyopathy: Study of the Cardiac Conduction System. Diagnostics (Basel, Switzerland) 2021, 11. [Google Scholar] [CrossRef]
- Matturri, L.; Ottaviani, G.; Lavezzi, A.M. Techniques and Criteria in Pathologic and Forensic-Medical Diagnostics in Sudden Unexpected Infant and Perinatal Death. Am. J. Clin. Pathol. 2005, 124, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Matturri, L.; Ottaviani, G.; Lavezzi, A.M. Guidelines for Neuropathologic Diagnostics of Perinatal Unexpected Loss and Sudden Infant Death Syndrome (SIDS): A Technical Protocol. Virchows Arch. 2008, 452, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Constitution of the Italian Republic Italian Law N° 31. Regulations for Diagnostic Post-Mortem Investigation in Victims of Sudden Infant Death Syndrome (SIDS) and Unexpected Fetal Death. Off. Gaz. Ital. Republic, Gen. Ser. 2006, 34:4.
- Lavezzi, A.M.; Ottaviani, G.; Mauri, M.; Matturri, L. Alterations of Biological Features of the Cerebellum in Sudden Perinatal and Infant Death. Curr Mol Med 2006, 6, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Ottaviani, G. Crib Death - Sudden Infant Death Syndrome (SIDS). Sudden Infant and Perinatal Unexplained Death: The Pathologist’s Viewpoint; 2nd Ed.; Springer International Publishing: Heidelberg, Germany, 2014; ISBN 978-3-319-08346-9. [Google Scholar]
- Ottaviani, G.; Matturri, L.; Bruni, B.; Lavezzi, A.M. Sudden Infant Death Syndrome “Gray Zone” Disclosed Only by a Study of the Brain Stem on Serial Sections. J. Perinat. Med. 2005, 33, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Lavezzi, A.M.; Ottaviani, G.; Matturri, L. Developmental Alterations of the Auditory Brainstem Centers--Pathogenetic Implications in Sudden Infant Death Syndrome. J. Neurol. Sci. 2015, 357, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, P.; Weisæth, L.; Heir, T. Bereavement and Mental Health after Sudden and Violent Losses: A Review. Psychiatry 2012, 75, 76–97. [Google Scholar] [CrossRef] [PubMed]
- Buja, L.M.; Ottaviani, G.; Mitchell, R.N. Pathobiology of Cardiovascular Diseases: An Update. Cardiovasc. Pathol. 2019, 42, 44–53. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–596. [Google Scholar] [CrossRef]
- Anastasakis, A.; Papatheodorou, E.; Ritsatos, K.; Protonotarios, N.; Rentoumi, V.; Gatzoulis, K.; Antoniades, L.; Agapitos, E.; Koutsaftis, P.; Spiliopoulou, C.; et al. Sudden Unexplained Death in the Young: Epidemiology, Aetiology and Value of the Clinically Guided Genetic Screening. Europace 2018, 20, 472–480. [Google Scholar] [CrossRef]
- Flenady, V.; Koopmans, L.; Middleton, P.; Frøen, J.F.; Smith, G.C.; Gibbons, K.; Coory, M.; Gordon, A.; Ellwood, D.; McIntyre, H.D.; et al. Major Risk Factors for Stillbirth in High-Income Countries: A Systematic Review and Meta-Analysis. Lancet (London, England) 2011, 377, 1331–1340. [Google Scholar] [CrossRef]
- Matturri, L.; Lavezzi, A.M.; Minoli, I.; Ottaviani, G.; Rubino, B.; Cappellini, A.; Rossi, L. Association between Pulmonary Hypoplasia and Hypoplasia of Arcuate Nucleus in Stillbirth. J. Perinatol. 2003, 23, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Matturri, L.; Ottaviani, G.; Lavezzi, A.M.; Rossi, L. Early Atherosclerotic Lesions of the Cardiac Conduction System Arteries in Infants. Cardiovasc. Pathol. 2004, 13, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Matturri, L.; Ottaviani, G.; Alfonsi, G.; Crippa, M.; Rossi, L.; Lavezzi, A.M. Study of the Brainstem, Particularly the Arcuate Nucleus, in Sudden Infant Death Syndrome (SIDS) and Sudden Intrauterine Unexplained Death (SIUD). Am. J. Forensic Med. Pathol. 2004, 25, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Lavezzi, A.M.; Ottaviani, G.; Ballabio, G.; Rossi, L.; Matturri, L. Preliminary Study on the Cytoarchitecture of the Human Parabrachial/Kölliker-Fuse Complex, with Reference to Sudden Infant Death Syndrome and Sudden Intrauterine Unexplained Death. Pediatr. Dev. Pathol. 2004, 7, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Lavezzi, A.M.; Ottaviani, G.; Rossi, L.; Matturri, L. Hypoplasia of the Parabrachial/Kölliker-Fuse Complex in Perinatal Death. Biol. Neonate 2004, 86, 92–97. [Google Scholar] [CrossRef]
- Lavezzi, A.M.; Ottaviani, G.; Rossi, L.; Matturri, L. Cytoarchitectural Organization of the Parabrachial/Kölliker-Fuse Complex in Man. Brain Dev. 2004, 26, 316–320. [Google Scholar] [CrossRef]
- Morpurgo, C. V; Lavezzi, A.M.; Ottaviani, G.; Rossi, L. Bulbo-Spinal Pathology and Sudden Respiratory Infant Death Syndrome. Eur. J. Anaesthesiol. 2004, 21, 589–593. [Google Scholar] [CrossRef]
- Lavezzi, A.M.; Ottaviani, G.; Mingrone, R.; Matturri, L. Analysis of the Human Locus Coeruleus in Perinatal and Infant Sudden Unexplained Deaths. Possible Role of the Cigarette Smoking in the Development of This Nucleus. Brain Res. Dev. Brain Res. 2005, 154, 71–80. [Google Scholar] [CrossRef]
- Lavezzi, A.M.; Ottaviani, G.; Matturri, L. Adverse Effects of Prenatal Tobacco Smoke Exposure on Biological Parameters of the Developing Brainstem. Neurobiol. Dis. 2005, 20, 601–607. [Google Scholar] [CrossRef]
- Matturri, L.; Ottaviani, G.; Lavezzi, A.M. Maternal Smoking and Sudden Infant Death Syndrome: Epidemiological Study Related to Pathology. Virchows Arch. 2006, 449, 697–706. [Google Scholar] [CrossRef]
- Hamayasu, H.; Miyao, M.; Kawai, C.; Osamura, T.; Yamamoto, A.; Minami, H.; Abiru, H.; Tamaki, K.; Kotani, H. A Proof-of-Concept Study to Construct Bayesian Network Decision Models for Supporting the Categorization of Sudden Unexpected Infant Death. Sci. Rep. 2022, 12, 9773. [Google Scholar] [CrossRef] [PubMed]
- Polavarapu, M.; Klonoff-Cohen, H.; Joshi, D.; Kumar, P.; An, R.; Rosenblatt, K. Development of a Risk Score to Predict Sudden Infant Death Syndrome. Int. J. Environ. Res. Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Corrado, D.; Basso, C.; Schiavon, M.; Thiene, G. Screening for Hypertrophic Cardiomyopathy in Young Athletes. N. Engl. J. Med. 1998, 339, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Thiene, G.; Carturan, E.; Corrado, D.; Basso, C. Prevention of Sudden Cardiac Death in the Young and in Athletes: Dream or Reality? Cardiovasc. Pathol. 2010, 19, 207–217. [Google Scholar] [CrossRef] [PubMed]
- James, T.N. Sudden Death in Babies: New Observations in the Heart. Am. J. Cardiol. 1968, 22, 479–506. [Google Scholar] [CrossRef] [PubMed]
- Matturri, L.; Ottaviani, G.; Lavezzi, A.M.; Turconi, P.; Cazzullo, A.; Rossi, L. Expression of Apoptosis and Proliferating Cell Nuclear Antigen (PCNA) in the Cardiac Conduction System of Crib Death (SIDS). Adv. Clin. Path. 2001, 5, 79–86. [Google Scholar] [PubMed]
- James, T.N. Normal and Abnormal Consequences of Apoptosis in the Human Heart. Annu. Rev. Physiol. 1998, 60, 309–325. [Google Scholar] [CrossRef]
- Ottaviani, G.; Matturri, L.; Rossi, L.; Jones, D. Sudden Death Due to Lymphomatous Infiltration of the Cardiac Conduction System. Cardiovasc. Pathol. 2003, 12, 77–81. [Google Scholar] [CrossRef]
- Ottaviani, G.; Rossi, L.; Matturri, L. Histopathology of the Cardiac Conduction System in a Case of Metastatic Pancreatic Ductal Adenocarcinoma. Anticancer Res. 2002, 22, 3029–3032. [Google Scholar]
- Matturri, L.; Ottaviani, G.; Rossi, L. Cardiac Massage in Infants. Intensive Care Med. 2003, 29, 1199–1200. [Google Scholar] [CrossRef]
- Rossi, L.; Matturri, L. His Bundle Haemorrhage and External Cardiac Massage: Histopathological Findings. Br. Heart J. 1988, 59, 586–587. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
This graph shows the gender and the frequency distribution of the 75 cases of sudden unexpected death (SUD) based on age-related five forms of death. SUD was significantly more frequent in males (M) (45/75) than in females (F) (30/75), being the gender distribution among the five diagnostic subgroups between males (60%) and females (40%) was statistically significant (p < 0.05). SIUD = sudden intrauterine unexpected death; SNUD = sudden neonatal unexpected death; SIDS = sudden infant death syndrome; SUDY = sudden unexpected death in the young; SUDA =unexpected death in the adult.
Figure 1.
This graph shows the gender and the frequency distribution of the 75 cases of sudden unexpected death (SUD) based on age-related five forms of death. SUD was significantly more frequent in males (M) (45/75) than in females (F) (30/75), being the gender distribution among the five diagnostic subgroups between males (60%) and females (40%) was statistically significant (p < 0.05). SIUD = sudden intrauterine unexpected death; SNUD = sudden neonatal unexpected death; SIDS = sudden infant death syndrome; SUDY = sudden unexpected death in the young; SUDA =unexpected death in the adult.
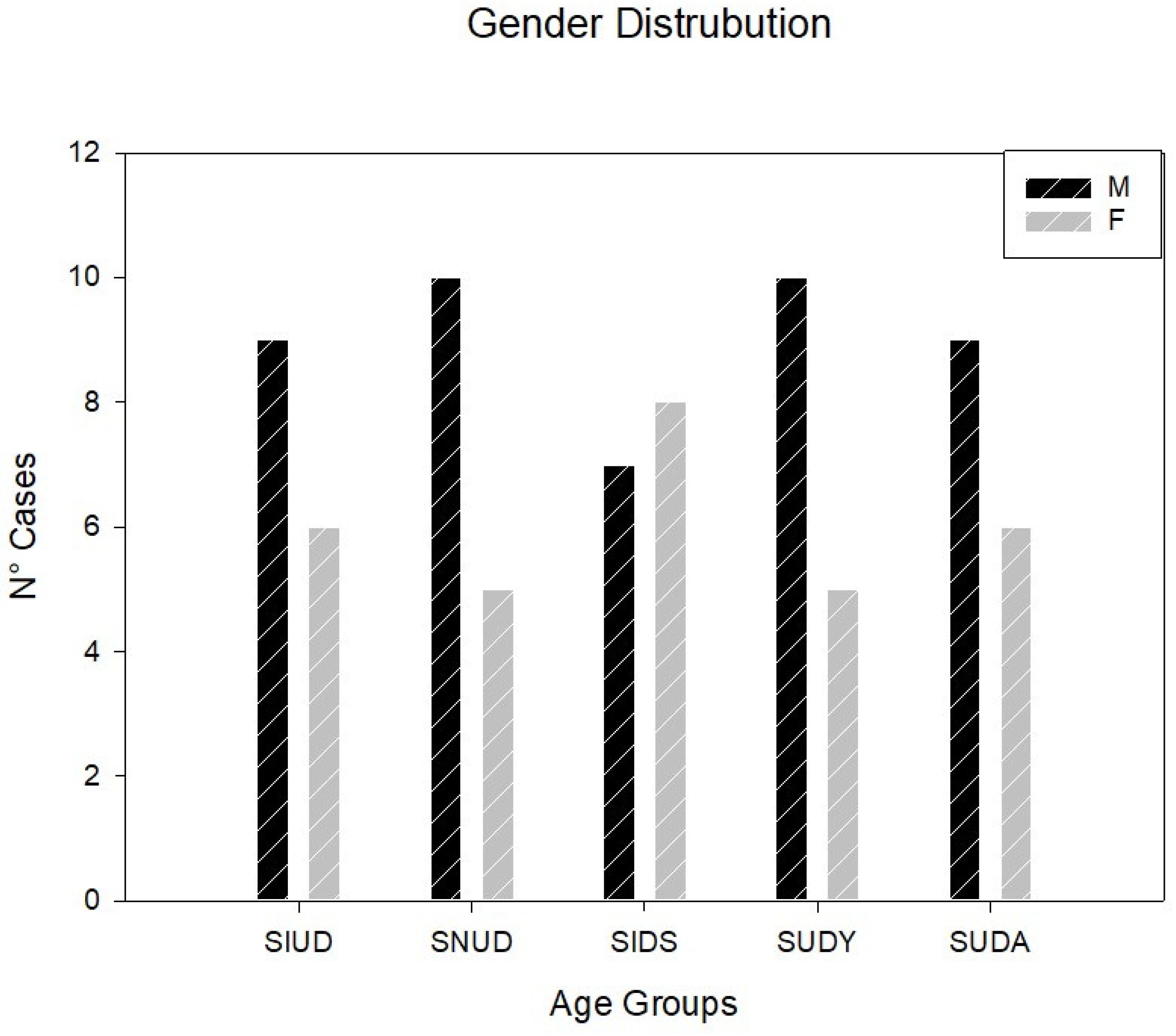
Figure 2.
Arrows point to an Island of conduction system embedded into the central fibrous body (CFB), separated from the atrio-ventricular node (AVN), in part undergoing the process of resorptive degeneration (*), in a 28-day old baby boy victim of sudden neonatal unexpected death (SNUD). VS = ventricular septum. Trichromic Heidenhain; Original magnification: A) 20 x B) 100 x.
Figure 2.
Arrows point to an Island of conduction system embedded into the central fibrous body (CFB), separated from the atrio-ventricular node (AVN), in part undergoing the process of resorptive degeneration (*), in a 28-day old baby boy victim of sudden neonatal unexpected death (SNUD). VS = ventricular septum. Trichromic Heidenhain; Original magnification: A) 20 x B) 100 x.
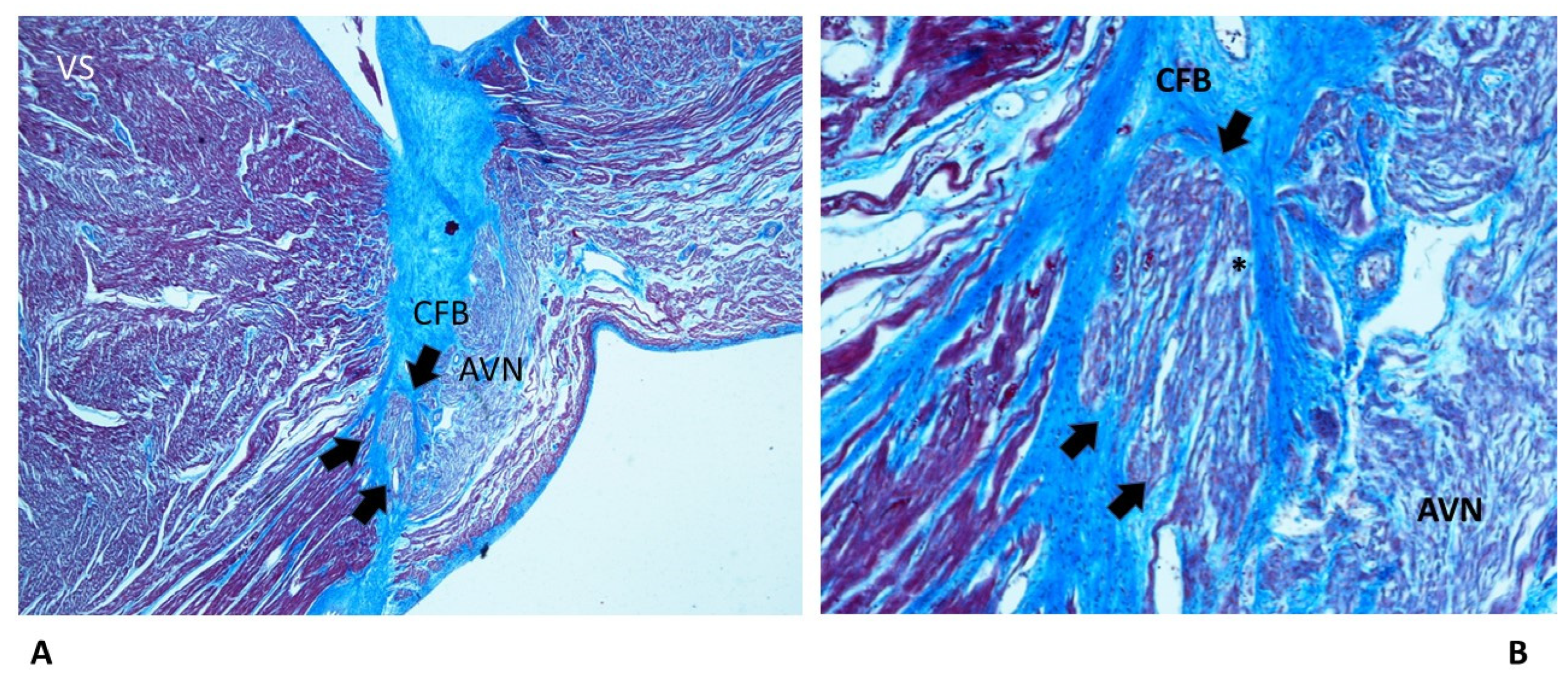
Figure 3.
Two serial sections of the atrio-ventricular junction (AVJ) showing a Mahaim fiber (arrows), in a 39+6-week-gestation female fetus, victim of sudden intrauterine unexpected death (SIUD). In the central fibrous body (CFB), the pattern of fetal dispersion, separated from the atrio-ventricular node (AVN), in part undergoing the process of resorptive degeneration (*), is shown. VS = ventricular septum. Trichromic Heidenhain; Original magnification: A) B) 20 x.
Figure 3.
Two serial sections of the atrio-ventricular junction (AVJ) showing a Mahaim fiber (arrows), in a 39+6-week-gestation female fetus, victim of sudden intrauterine unexpected death (SIUD). In the central fibrous body (CFB), the pattern of fetal dispersion, separated from the atrio-ventricular node (AVN), in part undergoing the process of resorptive degeneration (*), is shown. VS = ventricular septum. Trichromic Heidenhain; Original magnification: A) B) 20 x.
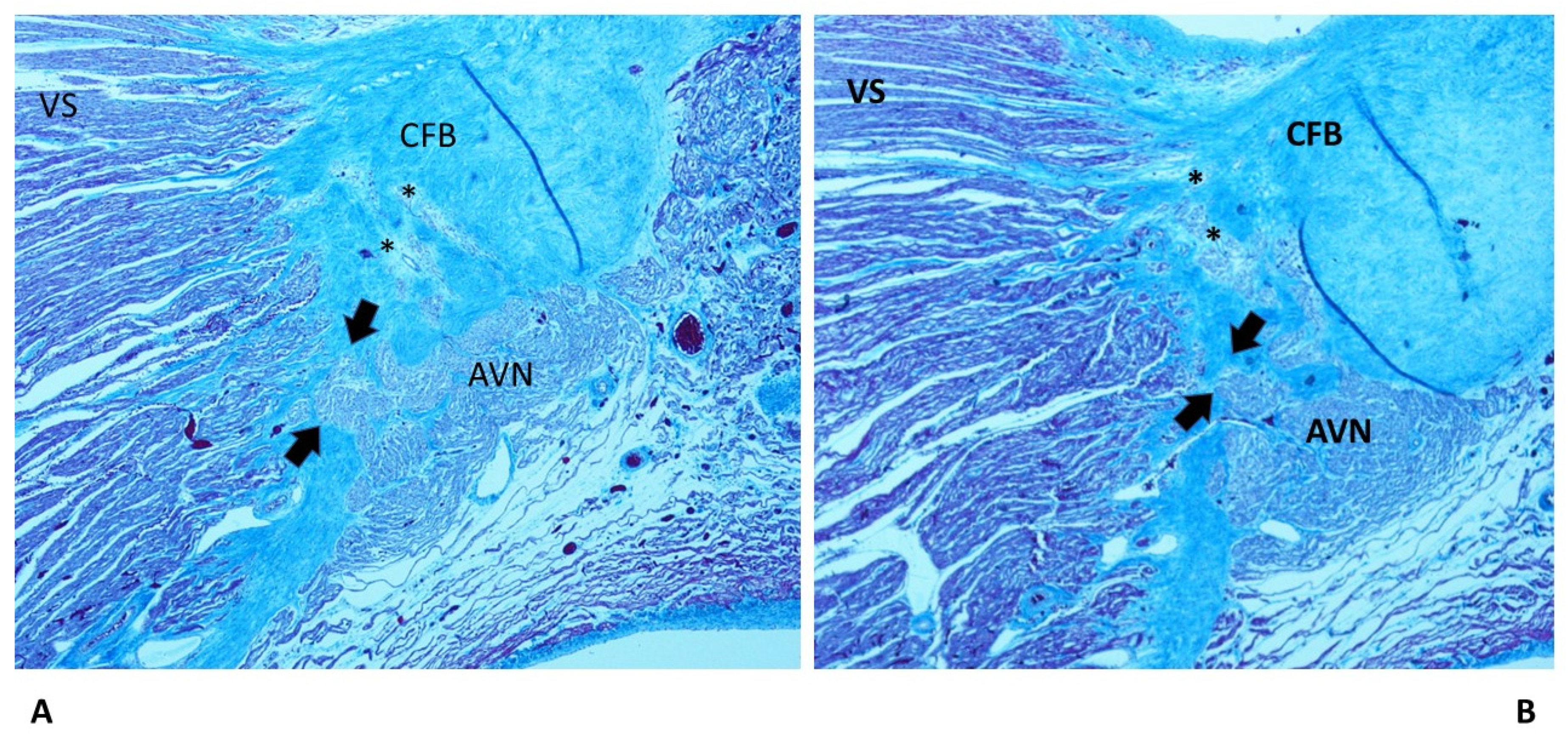
Figure 4.
Arrows point to cartilaginous meta-hyperplasia of the central fibrous body (CFB), potentially compressing the His bundle (HB), in a 53-day old baby girl victim of sudden infant death syndrome (SIDS). VS = ventricular septum. Trichromic Heidenhain; Original magnification: A) 20 x B) 100 x.
Figure 4.
Arrows point to cartilaginous meta-hyperplasia of the central fibrous body (CFB), potentially compressing the His bundle (HB), in a 53-day old baby girl victim of sudden infant death syndrome (SIDS). VS = ventricular septum. Trichromic Heidenhain; Original magnification: A) 20 x B) 100 x.
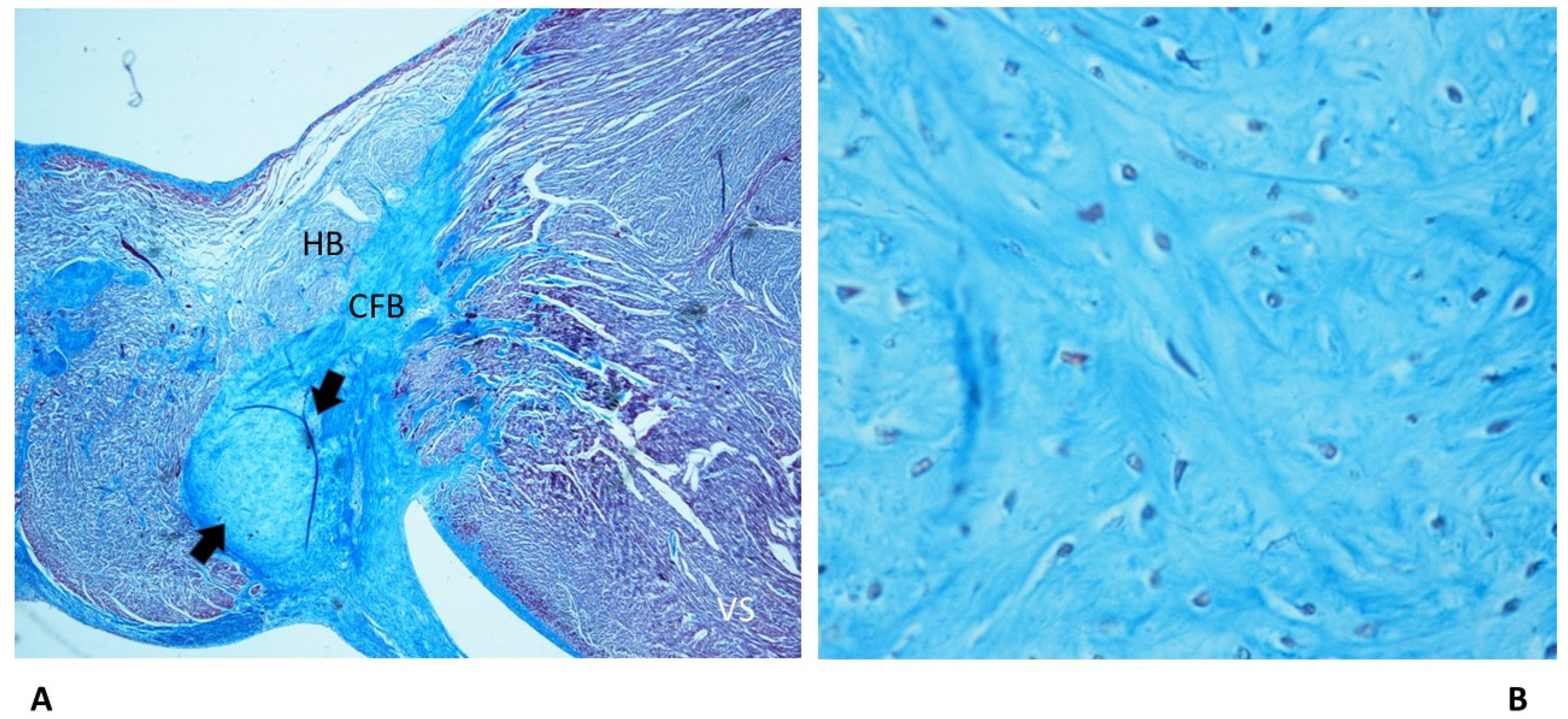
Figure 5.
Two serial sections of the atrio-ventricular junction (AVJ), in a 13-year old boy, victim of sudden unexpected death in the young sudden intrauterine unexpected death (SUDY). A) Arrows point to fibrous tissue of the central fibrous body (CFB), as the pattern of septated his bundle (HB), which is in part undergoing the process of resorptive degeneration (*). B) Arrows point to septation of the bifurcation (BIF). VS = ventricular septum. Trichromic Heidenhain; Original magnification: A) B) 20 x.
Figure 5.
Two serial sections of the atrio-ventricular junction (AVJ), in a 13-year old boy, victim of sudden unexpected death in the young sudden intrauterine unexpected death (SUDY). A) Arrows point to fibrous tissue of the central fibrous body (CFB), as the pattern of septated his bundle (HB), which is in part undergoing the process of resorptive degeneration (*). B) Arrows point to septation of the bifurcation (BIF). VS = ventricular septum. Trichromic Heidenhain; Original magnification: A) B) 20 x.
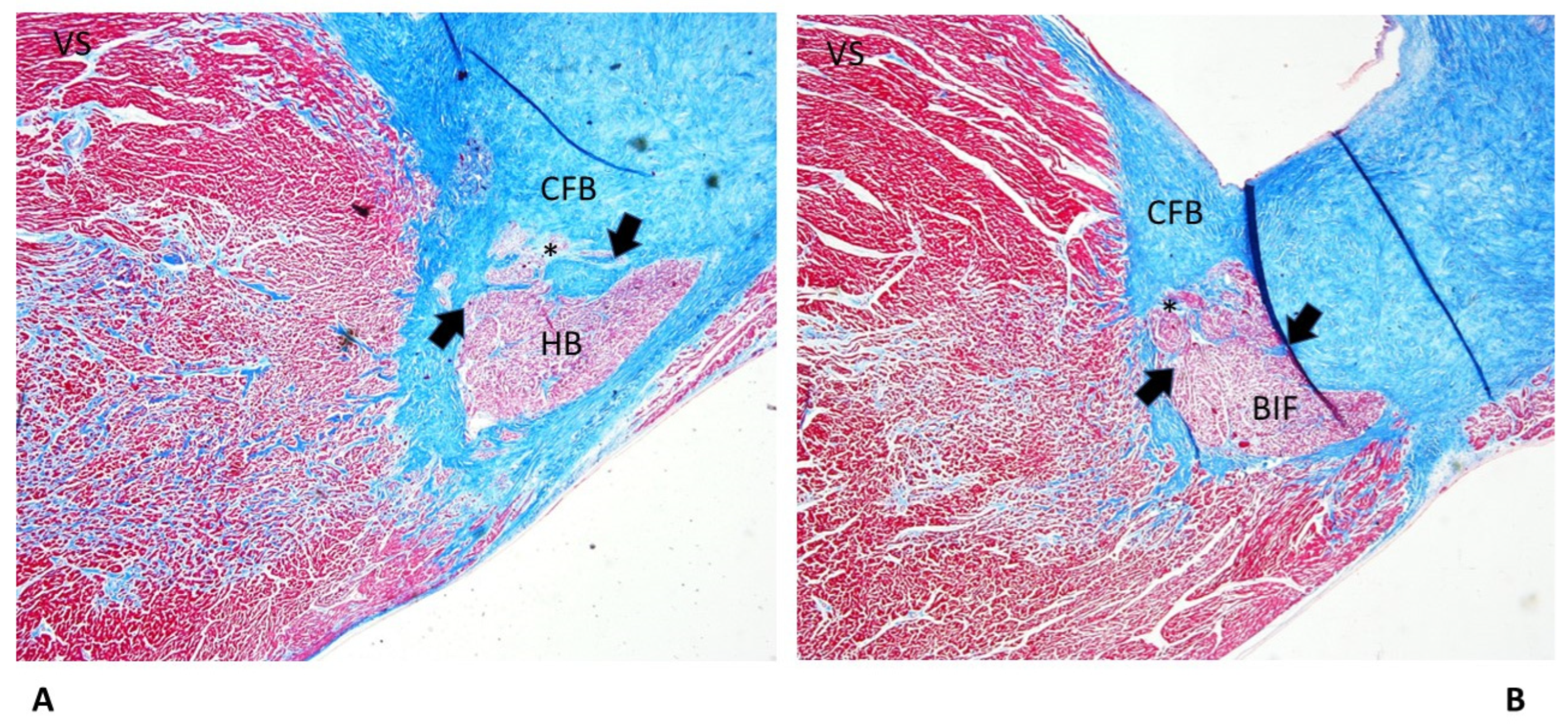
Figure 6.
Arrows point to fibromuscular thickening of the sino-atrial node (SAN) artery, as fibromuscular dysplasia, in a 50-year-old man victim of sudden unexpected death in the adult (SUDA). The SAN presents hypoplasia. Trichromic Heidenhain; Original magnification: A) 20 x B) 100 x.
Figure 6.
Arrows point to fibromuscular thickening of the sino-atrial node (SAN) artery, as fibromuscular dysplasia, in a 50-year-old man victim of sudden unexpected death in the adult (SUDA). The SAN presents hypoplasia. Trichromic Heidenhain; Original magnification: A) 20 x B) 100 x.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



