
Submitted:
15 May 2023
Posted:
16 May 2023
You are already at the latest version
Abstract
Background: Demographic aging is a reality in developed countries, which poses a social challenge of great responsibility. Thus, numerous studies have been developed in an attempt to understand which factors best predict healthy aging. The aim of this study was to investigate and systematize literature on intervention programs that simultaneously include cognitive stimulation and physical activity, understand the importance of the use of new technology in these programs, and understand their impact on cognitive function in older adults, giving indications about their contribution to healthy aging. Methods: A narrative approach was used for extraction and synthesis of the data. Relevant studies were identified from electronic databases such as PubMed, Scopus, Web of Science and Academic Search Complete. Results: Thirty-two articles, involving 2815 participants, were identified. All selected studies were randomized controlled studies. The studies were published between 2011 and 2020. All studies included a combination of cognitive and physical interventions. Many of the studies used technology to administer the cognitive stimulation program. Conclusions: Most of the analyzed studies use new technologies in physical and cognitive interventions, demonstrating that this new form of intervention exerts lasting and stable benefits in cognition.
Keywords:
Cognitive stimulation
; physical activity
; combined interventions
; older adults
; new technologies
; exergaming
; e-mental health
1. Introduction
Aging is a continuous and complex process characterized by progressive physical and psychological changes [1]. In the most developed countries, the proportion of older adults has increased significantly, as a result of the decrease in birth rates and the increase in average life expectancy [2]. The increase in demographic aging implies new challenges for society, such as keeping older adults healthy, active and participative for a longer period of time, as advocated by the World Health Organization [3].
Numerous researchers have attempted to understand which factors best predict healthy aging, among which are cognitive stimulation and physical exercise. When considering a prescription for healthy and successful aging, the vital role of cognitive stimulation and physical activity is remarkable. This highlights the importance of non-pharmacological interventions, related to changes in the population's lifestyle [4]. In the last decade, issues associated with new technologies have gained prominence and they have been used in the development of non-invasive intervention techniques.
1.1. Physical Activity
Numerous benefits of physical exercise are recognized for the health and well-being of the general population. Regular physical activity promotes the improvement of physical and mental functions [5] and is associated with decreased risk of mortality, diabetes, cardiovascular problems, stroke and breast and colon cancer [6]. In addition, it promotes improvements in bone health, in reducing the risk of osteoporosis, in postural stability and in increasing flexibility, promoting a decrease in the risk of falls, one of the main causes of mortality in the aging population [7].
Physical activity is also important when it comes to mental health, allowing the prevention of dementia, maintaining independence, improving quality of life [8] and is associated with improvements in the level of depression [9] stress and anxiety [7]. Physical activity can decrease the risk of dementia by 28% [10], reverse some of the unwanted effects of a sedentary lifestyle and contribute to delay brain aging and degenerative pathologies, such as Alzheimer's disease [11], being fundamental in improving memory and learning [12]. In addition, it allows attenuation of the effects of aging at the brain level, being fundamental for good cognitive functioning [10,13,14].
High levels of physical activity are associated with increased brain activity [15], increasing the brain's ability to establish new connections. Thus, by allowing higher levels of oxygen to be pumped into the body, it has a very positive impact on brain activity. Physical activity improves neuroplasticity, changing the synaptic structure and function in various brain regions [16]. Physical activity modifies trophic signaling factors and neuronal function and structure in key areas for cognition [17].
1.2. Cognitive Stimulation
In recent decades, there has been a growing interest in cognitive changes that occur in the aging population. These cognitive changes are different in each individual, in some cases they occur suddenly and in others in a gradual way [18]. Thus, the growing study of this phenomenon promotes the improvement of diagnostic techniques, capable of distinguishing between normative and pathological processes of aging, and of preventive intervention, capable of outlining the most effective methods for active and meaningful longevity.
The aging process brings losses at the cognitive and functional level [19]. The cognitive abilities that show the greatest deficit in the context of a normative aging process are memory, visuospatial capacity, and information processing speed [20]. According to Calatayud et al. (2018), interventions aimed at exercising and stimulating cognitive abilities may contribute to the reduction of the negative effects of aging, delaying the appearance of deterioration of the various cognitive functions.
Cognitive stimulation refers to a set of methods and techniques that aim to optimize the performance of cognitive functions, through compensation strategies and cognitive reserve, in order to enhance neuroplasticity [19] and it is based on the general view that a lack of cognitive activity accelerates cognitive decline [21]. Cognitive stimulation promotes “involvement in activities aimed at the general improvement of social and cognitive functioning, in order to compensate irremediable neurocognitive deficits and maintain the daily function preserved for as long as possible” [22] (p.406).
1.3. Physical Activity and Cognitive Stimulation Combined: The Role of New Technology
Physical exercise alone may not be enough to delay cognitive decline in the aging. Research has suggested that combining physical exercise with cognitive stimulation may be a more successful strategy [17,23,24].
Adcock et al. (2020) suggest that we must think about physical and cognitive activity inseparably, since muscles and body movements are controlled by the central nervous system, while feedback from peripheral structures such as muscles and sensory organs influence brain activity. For the same authors, mild cognitive decline and dementia are associated with greater physical decline, compared to older adults with normal cognitive functioning.
New technologies can be very useful in cognitive stimulation, favoring intervention tasks [25]. According to some studies, the combination of physical activity and cognitive stimulation using new technologies seems to be an effective strategy in the long term. One of these strategies is the use of exergaming. Video game playing may have cognitive benefits and it is highly motivating and likely to promote exercise adherence [26].
Thus, this systematic literature review aims to investigate and systematize the literature on intervention programs that combined cognitive stimulation and physical activity published in the last decade, giving indications about their efficacy and, additionally, to understand the importance of new technologies in the intervention with the elderly.2. Materials and Methods
The Materials and Methods should be described with sufficient details to allow others to replicate and build on the published results. Please note that the publication of your manuscript implicates that you must make all materials, data, computer code, and protocols associated with the publication available to readers. Please disclose at the submission stage any restrictions on the availability of materials or information. New methods and protocols should be described in detail while well-established methods can be briefly described and appropriately cited.
Research manuscripts reporting large datasets that are deposited in a publicly available database should specify where the data have been deposited and provide the relevant accession numbers. If the accession numbers have not yet been obtained at the time of submission, please state that they will be provided during review. They must be provided prior to publication.
Interventionary studies involving animals or humans, and other studies that require ethical approval, must list the authority that provided approval and the corresponding ethical approval code.
2. Materials and Methods
2.1. Protocol and Registration
This work adheres to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) [27] statement guidelines and was registered on PROSPERO with the number CRD42021231687.
2.2. Literature Search Strategy and Study Selection
Articles in English published in electronic databases such as PubMed, Scopus, Web of Science and Academic Search Complete, from first records to 27 July 2022. The following keywords were used: “cognitive stimulation”, “physical activity” and “older adults”. No restrictions on language or publication type were applied. Two of the authors independently conducted an initial screening of titles and abstracts and assessed full-text versions of potentially relevant articles. Disagreements were resolved by a third author. The electronic search was complemented by hand-searching the references of included papers and previous reviews.
2.3. Eligibility Criteria
Studies were eligible for final inclusion in the systematic review if they met cumulatively the following criteria: studies carried out with older adults and whose participants took part in physical and cognitive intervention programs simultaneously; studies with peer review; randomized controlled studies; and no restrictions on language or publication type were applied at the moment of the database search. In the present study, the following types of publication were excluded: letters to the editor; comments; editorials; systematic reviews and meta-analyses studies. Finally, studies that did not investigate the effect of the combination of physical activity and cognitive stimulation, on the cognition of the older adults were also excluded.
2.4. Data Extraction Process
At first, possible studies for inclusion in the systematic review were identified. An electronic data extraction form was used, using the Excel program. After removing the duplicates, the titles and abstracts of the studies were screened. In this way, the relevant studies were extracted, according to the pre-defined inclusion criteria. Studies that did not meet the inclusion criteria were removed. In this study, the extracted data were synthesized in a table, with the following information: authors, year, sample size, frequency of intervention, study design, existence and timing of follow-up, type of cognitive intervention, type of physical intervention, objectives, and main results.
2.5. Quality Assessment
The researchers assessed the risk of bias in individual studies using the revised Cochrane risk of bias tool for randomized trials (RBO2) [28].
Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
3. Results
3.1. Selection of Studies
As shown in Figure 1, a total of 11096 studies were identified through electronic database searching and one additional article was identified by back citation. After removing 555 duplicate records, 10542 studies were screened based upon title and abstract, but 10426 did not meet the eligibility criteria. The full text was retrieved for 116 articles of which 84 were excluded.
Thirty-two studies were identified that combined physical activity and cognitive stimulation. Of the thirty-two analyzed, eighteen studies (56,3%) presented a low risk of bias. Five (15,6%) studies had a high risk of bias. Finally, nine studies (28,1%) had some concerns (Table 1).
3.2. Type of Studies
Studies published in peer-reviewed journals were selected. Of the studies analyzed, eleven conducted a follow-up test after their interventions. Follow-up varied between 3 months [29,30,31,32], 6 months [33,34], 1 year [35] and 2 years [24]. The study developed by Van Santen et al. (2020) carried out two moments of follow-up, at 3 months and 6 months (Table 2).
3.3. Type of Participants
Most studies included people over the age of 60. Subjects with mild cognitive impairment, with dementia and cognitively healthy were included (Table 2).
Regarding the recruitment of the sample, participants were recruited from community centers [23,26,39,40], day care centers [38], residential structures for the elderly [35,41,42,43,44,45], in the community in general [16,29,34,35,36,37,46,47,48,49,50], senior organizations [16] and in hospitals and neurology clinics, normally associated with universities [24,30,32,33,51,52]. Participants in thirteen studies were diagnosed with dementia or mild cognitive impairment.
3.4. Duration of the Interventions
3.5. Intervention Groups
Several studies do not have a control group [23,36,37,40,41], and compared the effectiveness of physical activity and cognitive stimulation with each of its components administered in isolation. All other studies compared the combination of physical activity and cognitive stimulation with the isolated administration of cognitive stimulation or a control group, in the cognitive functioning of the older people.
3.6. Assessment of Participants
Regarding the neuropsychological assessment tests used, most studies used the Mini Mental State Examination (MMSE) to screen the sample, and participants should fall within a range of scores. Only six studies did not use the MMSE as a cognitive screening test [16,23,36,40,46,49]. In all studies, participants underwent an extensive battery of neuropsychological tests to assess various cognitive domains.
3.7. Type of Interventions
Studies were included if they focused on interventions combining cognitive stimulation with physical activity simultaneously, in older adults. Cognitive stimulation was focused on several domains of cognitive functioning, for example memory, attention, executive functions, spatial-temporal activities, language, and others. The intervention could include structured cognitive intervention programs [23,49]. Physical exercises included any form of structured physical activity, such as aerobic exercise, strength or functional, toning, cycling and walking.
3.8. Use of Technologies
4. Discussion
The objectives of this systematic review of the literature were to systematize all recent studies on the combined interventions of physical activity and cognitive stimulation on the cognitive functioning of older adults, to understand the impact of the use of new technology integrated in these interventions, and to obtain information about its effectiveness in contributing to healthy aging.
Many of the studies used technology to administer the cognitive stimulation program. Several studies suggest that the use of technology, namely computer programs, can be advantageous for the cognitive functioning of the older adults, namely in terms of memory [57]. Exergame training seems to be a motivating and promising option for simultaneous physical-cognitive training in older adults [22]. The use of these programs is expected to allow the prevention and treatment of cognitive decline, decreases sedentary lifestyle, a reduction in the time spent on the intervention and a decrease in the necessary resources [23]. This type of intervention seems to be more effective in treating the elderly compared to traditional interventions. They can be used in cognitive stimulation and physical activity. Most of the studies use the exergaming technique, which consists of activities that included physical activity and cognitive stimulation in an articulated way and simultaneously. One of the most well-known and publicized instruments is the Wii-Fit Pro, which has been widely used in intervention with the elderly. Exergame works as a new health strategy with the purpose of providing cognitive and functional improvement and/or maintenance in the elderly, promoting healthy aging. In fact, all analyzed studies using exergaming demonstrate significant results in improving cognitive functioning. However, the analyzed studies do not compare computerized interventions with traditional interventions, and it is not possible to deduce the difference in effectiveness between the two.
Independently of the use of technology to administer the intervention, most of the studies presented demonstrate that the combination of physical activity and cognitive stimulation is most beneficial for cognitive functioning in the aging population.
However, although this efficacy has been demonstrated, some studies reveal some differences and contradictions [36,44,48]. In two studies [36,48], no significant advantages were found in the combination of physical activity with cognitive stimulation in the aging. In one study [44] inconsistent results were found. These differences can be explained by methodological differences.
Several studies do not have a control group, namely the studies [23,36,37,40,41], although all were Randomized Control Trials. This is perhaps because these studies had the aim of identifying the additional benefit of adding a physical exercise intervention to a cognitive one. For this reason, they compared the results of combining the two interventions with a group that only received cognitive stimulation. For the authors, a control group is considered to be a group that does not benefit from any type of intervention.
Although several intervention programs used physical activity and cognitive stimulation, few investigations analyzed and compared the combination of both, with each of the components administered in isolation and with a control group [24,48,50]. The remaining studies compared the combination of physical activity and cognitive stimulation with only one of the variables in isolation. However, the results were inconclusive [24], significant differences in psychomotor speed were found in the group that received aerobic and cognitive training (exergame) when compared to the control group. However, in same studies there were no statistically significant differences, since according to the authors, combined training did not produce synergistic effects [48,50].
In addition, short-term effects of the interventions did not reveal significant differences in most of the analyzed cognitive functions. Although the discovery that the combination of cognitive stimulation and physical activity significantly improves psychomotor speed may be clinically relevant, as psychomotor speed is an important predictor of functional decline [24], more conclusive studies are needed regarding the effect of physical activity and cognitive stimulation on different cognitive functions. Some of these cognitive functions are less sensitive to the intervention of physical activity, with no significant changes in these cases, which is why studies in this regard remain fundamental [48].
Through the results obtained, it is possible to verify that thirteen studies were carried out with a sample with mild cognitive impairment or formal diagnosis of dementia. These results suggest that there is some variety in the studies developed, not being focused only on a segment of the population. The fact that in recent years numerous studies have been carried out with cognitively healthy subjects is advantageous, since it allows the development of increasingly effective strategies to promote healthy aging.
Only eleven studies carried out follow-up after their interventions, which is consistent with what was observed by [58]. Studies with follow-up are sometimes inconclusive, not revealing any significant changes over the long term in most conditions analyzed [24].
Based on the analysis of the studies, it is possible to conclude that the factors that influence cognitive and physical dysfunction are susceptible to intervention. Thus, neuropsychological and physical interventions can be fundamental for normative aging, since they have the potential to delay the decline in cognitive and physical functions. Given the cognitive improvements, after the interventions, it is possible to infer that brain plasticity is present in the aging population and that cognitive decline can be delayed in cognitively healthy subjects and individuals with mild cognitive impairment [23].
4.1. Limitations and Future Directions
Several key limitations of this comprehensive systematic review should be acknowledged. The characteristics of the studies included in the analysis vary widely, for example, in the focus of the intervention, in the objectives, in the number and time of the sessions, in the sample size, in the cognitive functions evaluated and in the type of physical activity implemented. For this reason, meta-analysis or statistical comparisons were not possible.
Future studies should focus on the development of new technologies, applying them in their intervention programs, in an attempt to make them more effective; on the other hand, future studies should compare the effectiveness of interventions that use new technologies with traditional interventions; should use follow-up strategies to verify the effects of this type of intervention in the long term; should understand the impact of the combination of the two forms of intervention on other personal individual variables (depression, anxiety, quality of life, psychological well-being and performance, daily living activities); should compare the effects of the combination of physical activity and cognitive stimulation with each of its components administered separately; and, finally, future studies should try to distinguish the benefits of the combination of physical activity and cognitive stimulation according to the user's cognitive level (cognitively healthy, mild cognitive impairment and dementia).
5. Conclusions
As scientific research in the area of aging progresses, the results suggest that a healthy lifestyle, with regular practice of physical activity and constant investment in cognitive stimulation activity, is essential for a healthy and meaningful aging.
Despite not finding studies that compare the effectiveness of using traditional stimulation techniques with those using new technologies, the new technologies seem to have advantages compared to the rest. The use of new technology promotes, in addition to the significant improvement in cognition, the reduction of a sedentary lifestyle, the reduction of the time spent in the intervention and the reduction of the necessary resources.
Recent studies indicate that cognitive activities are complex and challenging, mobilizing more than one cognitive domain simultaneously. In the coming decades, we must join efforts to associate new technologies with cognitive stimulation activities, in order to make our interventions increasingly effective. On the other hand, future studies could be carried out to assess the needs of the elderly, with regard to technologies, specifically in terms of motivators and barriers to their use.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceptualization, RR, SMF, and IMS; Methodology, RR, SMF and IMS; Data collection, RR; Data Analysis, RR, SMF, IMS; Writing – Original Draft Preparation, RR; Writing – Review & Editing, IMS and SMF; Supervision, SMF and IMS; Funding Acquisition, SMF.
Funding
This work was funded by Portucalense Human Development Institute, Portucalense University, Porto, Portugal.
References
- Higueras-Fresnillo, S.; Cabanas-Sánchez, V.; García-Esquinas, E.; Rodríguez-Artalejo, F.; Martinez-Gomez, D. Physical activity attenuates the impact of poor physical, mental, and social health on total and cardiovascular mortality in older adults: A population-based prospective cohort study. Qual. Life Res. 2018, 27, 3293–3302. [Google Scholar] [CrossRef] [PubMed]
- Merriam, S.B.; Kee, Y. Promoting community wellbeing: The case for lifelong learning for older adults. AEQ 2014, 64, 128–144. [Google Scholar] [CrossRef]
- France, L. Preparação para a reforma: Responsabilidade individual e colectiva. Psychol. 2010, 53, 47–66. [Google Scholar]
- Ruthirakuhan, M.; Luedke, C.A.; Tam, A.; Goel, A.; Kurji, A.; Garcia, A. Use of physical and intellectual activities and socialization in the management of cognitive decline of aging and in dementia: A review. J. Aging Res. 2010, 2012, 1–14. [Google Scholar] [CrossRef]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global action plan on physical activity 2018-2030: More active people for a healthier world 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Stewart, K.J. Physical activity and aging. N. Y. Acad. Sci. 2005, 1055, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.; Norman, I.; While, A.E. Physical activity in older people: A systematic review. BMC Public Health 2013, 13, 1–17. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef]
- Hamer, M.; Chida, Y. Physical activity and risk of neurodegenerative disease: A systematic review of prospective evidence. Psychol. Med. 2009, 39, 3–11. [Google Scholar] [CrossRef]
- Di Liegro, C.M.; Schiera, G.; Proia, P.; Di Liegro, I. Physical activity and brain health. Genes 2019, 10, 1–86. [Google Scholar] [CrossRef]
- Lin, T.; W; Tsai, S. F.; Kuo, Y.M. Physical exercise enhances neuroplasticity and delays Alzheimer disease. Brain Plast. 2018, 1, 95–110. [Google Scholar] [CrossRef]
- Sofi, F.; Valecchi, D.; Bacci, D.; Abbate, R.; Gensini, G.F.; Casini, A.; et al. Physical activity and risk of cognitive decline: A meta-analysis of prospective studies. J. Intern. Med. 2011, 269, 107–117. [Google Scholar] [CrossRef]
- Vance, D.E.; Marson, D.C.; Triebel, K.L.; Ball, K.; Wadley, V.G.; Humphrey, S.C. Physical activity and cognitive function in older adults: The mediating effect of depressive symptoms. J. Neurosci. Nurs. 2016, 48, 2–12. [Google Scholar] [CrossRef]
- Frutos- Lucas, J.; et al. Physical activity effects on the individual alpha peak frequency of older adults with and without genetic risk factors for Alzheimer’s disease: A MEG study. Clin. Neurophysiol. 2018, 129, 1981–1989. [Google Scholar] [CrossRef] [PubMed]
- Adcock, M.; Fankhauser, M.; Post, J.; Lutz, K.; Zizlsperger, L.; Luft, A.R.; Guimarães, V.; Shattin, A.; Bruin, E.D. Effects of an in-home multicomponent exergame training on physical functions, cognition, and brain volume of older adults: A randomized controlled trial. Front. Med. 2020, 6, 1–18. [Google Scholar] [CrossRef]
- Phillips, C.; Baktir, M.A.; Srivatsan, M.; Salehi, A. Neuroprospective effects of physical activity on the brain: A closer look at trophic factors signaling. Front. Cell. Neurosci. 2014, 8, 170. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S. Mental stimulation and brain health: Complex, challenging activities can support cognitive health in older adults. ASA 2011, 32, 58–62. [Google Scholar]
- Calatayud, E.; Plo, F.; Muro, C. Análisis del efecto de un programa de estimulación cognitiva en personas con envejecimiento normal en atención primaria: Ensayo clínico aleatorizado. Atención Primaria 2018, 52, 38–46. [Google Scholar] [CrossRef]
- Borrás, B.C.; Vina, R.J. Neurofisiología y enveje-cimiento. Concepto y bases fisiopatológicas del deteriorocognitivo. Rev. Esp. Geriatr. Gerontol. 2016, 51, 3–6. [Google Scholar] [CrossRef]
- Park, J.; Kim, M.; Shim, H. Effects of a multicomponent cognitive stimulation program on cognitive function improvement among elderly women. Asian Nurs. Res. 2019, 13, 306–312. [Google Scholar] [CrossRef]
- Silva, A. Reabilitação neuropsicológica. In Saúde mental das pessoas mais velhas; Firmino, H., Simões, M.R., Cerejeira, J., Eds.; Lidel: Lisboa, Portugal, 2016; pp. 405–421. [Google Scholar]
- González-Palau, F.; Franco, M.; Bamidis, P.; Losada, R.; Parra, E.; Papageorgiou, S.G.; Vivas, A.B. The effects of a computer-based cognitive and physical training program in a healthy and mildly cognitive impaired aging sample. Aging Ment Health 2014, 18, 838–846. [Google Scholar] [CrossRef] [PubMed]
- Karssemeijer, E.G.A.; et al. The quest for synergy between physical exercise and cognitive stimulation via exergaming in people with dementia: A randomized controlled trial. Alzheimer’s Res. Ther. 2019, 11, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Gonzáles-Moreno, J.; Satorres, E.; Soria-Urios, G.; Meléndez, J.C. Cognitive stimulation program presented through new technologies in a group of people with moderate cognitive impairment. J. Alzheimer's Dis. 2022, 88, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Maillot, P.; Perrot, A.; Hatley, A. Effects of interactive physical-activity video-game training on physical and cognitive function in older adults. Psychol. Aging 2012, 27, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elberns, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, I4898. [Google Scholar] [CrossRef]
- Linde, K.; Alfermann, D. Single versus combined cognitive and physical activity effects on fluid cognitive abilities of healthy older adults: A 4-month randomized controlled trial with follow-up. JAPA 2014, 22, 302–313. [Google Scholar] [CrossRef]
- Barban, F.; Annicchiarico, R.; Melideo, M.; Federici, A.; Lombardi, M.G.; Giuli, S.; Ricci, C.; Adriano, F.; Griffini, I.; Silvestri, M.; et al. Reducing fall risk with combined motor and cognitive training in elderly fallers. Brain Sci. 2017, 7, 19. [Google Scholar] [CrossRef]
- Norouzi, E.; Vaezmosavi, M.; Gerber, M.; Puhse, U.; Brand, S. Dual-task training on cognition and resistance training improved both balance and working memory in older people. Phys. Sportsmed. 2019, 47, 471–478. [Google Scholar] [CrossRef]
- Park, H.; Park, J.H.; Na, H.R.; Hiroyuki, S.; Kim, G.M.; Jung, M.K.; Kim, W.K.; Park, K.W. Combined intervention of physical activity, aerobic exercise, and cognitive exercise intervention to prevent cognitive decline for patients with mild cognitive impairment: A randomized controlled clinical study. J. Clin. Med. 2019, 8, 940–952. [Google Scholar] [CrossRef]
- Donnezan, L.C.; Perrot, A.; Belleville, S.; Bloch, F.; Kemoun, G. Effects of simultaneous aerobic and cognitive training on executive functions, cardiovascular fitness and functional abilities in older adults with mild cognitive impairment. Ment. Health Phys. Act. 2018, 15, 78–87. [Google Scholar] [CrossRef]
- Laatar, R.; Kachouri, H.; Boji, R.; Rebai, H.; Sahli, S. Combined physical-cognitive training enhances postural performances during daily life tasks in older adults. Exp. Gerontol. 2018, 107, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Eggenberger, P.; Schumacher, V.; Angst, M.; Theill, N.; Bruin, E.D. Does multicomponent physical exercise with simultaneous cognitive training boost cognitive performance in older adults? A 6-month randomized controlled trial with a 1-year follow-up. Clin. Interv. Aging 2015, 10, 1335–1349. [Google Scholar] [PubMed]
- Rahe, J.; Becker, J.; Fink, G.R.; Kessler, J.; Kukolja, J.; Rahn, A.; Rosen, J.B.; Szabados, F.; Wirth, B.; Kalbe, E. Cognitive training with and without additional physical activity in healthy older adults: Cognitive effects, neurobiological mechanisms, and prediction of training success. Front. Aging Neurosci. 2015, 7, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Maffei, L.; Picano, E.; Andreassi, M.; Angelucci, A.; Baldacci, F.; Baroncelli, L.; Begenisic, T.; Bellinvia, P.; Berardi, N.; Biagi, L. Randomized trial on the effects of a combined physical/cognitive training in aged MCI subjects: The train the brain study. Sci. Rep. 2017, 7, 39471. [Google Scholar]
- Van Santen, J.; Dröes, R.M.; Twisk, J.W.R.; Henkemans, O.A.B.; Straten, A.; Meiland, F.J.M. Effects of exergaming on cognitive and social functioning of people with dementia: A randomized controlled trial. JAMDA 2020, 21, 1958–1967. [Google Scholar] [CrossRef]
- McDaniel, M.A.; Binder, E.F.; Bugg, J.M.; Waldum, E.R.; Dufault, C.; Meyer, A.; Johanning, J.; Zheng, J.; Schechtman, K.B.; Kudelka, C. Effects of Cognitive Training with and without Aerobic Exercise on Cognitively-Demanding Everyday Activities. Psychol. Aging 2014, 29, 717–730. [Google Scholar] [CrossRef]
- Rahe, J.; Petrelli, A.; Kaesberg, S.; Fink, G.R.; Kessler, J.; Kalbe, E. Effects of cognitive training with additional physical activity compared to pure cognitive training in healthy older adults. Clin. Interv. Aging 2015, 10, 297–310. [Google Scholar] [CrossRef]
- Yoon, J.; Lee, S.; Lim, H.; Kim, T.; Jeon, J.; Mun, M. The effects of cognitive activity combined with active extremity exercise on balance, walking activity, memory level and quality of life of an older adult sample with dementia. JPTS 2013, 25, 1601–1604. [Google Scholar] [CrossRef]
- Htut, T.Z.C.; Hiengkaew, V.; Jalayondeja, C.; Vongsirinavarat, M. Effects of physical, virtual reality-based, and brain exercise on physical, cognition, and preference in older persons: A randomized controlled trial. EUROPA 2018, 15, 10. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Yamada, M.; Tanigawa, T.; Sekiyama, K.; Kawagoe, T.; Suzuki, M.; Yoshikawa, S.; Abe, N.; Otsuka, Y.; Nakai, R.; et al. A 12-week physical and cognitive exercise program can improve cognitive function and neural efficiency in community-dwelling older adults: A randomized controlled trial. JAGS 2015, 63, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Rezola- Pardo, C.; Arrieta, H.; Gil, S.M.; Zarrazquin, I.; Yanguas, J.J.; López, M.A.; Irazusta, J.; Rodriguez-Larrad, A. Comparison between multicomponent and simultaneous dual-task exercise interventions in long-term nursing home residents: The Ageing-on dual-task randomized controlled study. Age Ageing 2019, 48, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Van het Reve, E.; de Bruin, E. Strength-balance supplemented with computerized cognitive training to improve dual task gait and divided attention in older adults: A multicenter randomized-controlled trial. BMC Geriatr. 2014, 14, 134. [Google Scholar] [CrossRef] [PubMed]
- Barnes, D.E.; Santos-Modesitt, W.; Poelke, G.; Kramer, A.F.; Castro, C.; Middleton, L.E.; Yaffe, K. The mental activity and eXercise (MAX) trial: A randomized, controlled trial to enhance cognitive function in older adults. JAMA Intern. Med. 2013, 173, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Boa Sorte Silva, N.C.; Gill, D.P.; Owen, A.M.; Liu-Ambrose, T.; Hachinski, V.; Shigematsu, R.; Petrella, R.J. Cognitive changes following multiple-modality exercise and mind-motor training in older adults with subjective cognitive complaints: The M4 study. PLoS ONE 2018, 13, e0196356. [Google Scholar] [CrossRef]
- Desjardins-Crépeau, L.; Berryman, N.; Fraser, S.A.; Vu, T.T.M.; Kergoat, M.J.; Li, K.; Bosquet, L.; Bherer, L. Effects of combined physical and cognitive training on fitness and neuropsychological outcomes in healthy older adults. Clin. Interv. Aging 2016, 11, 1287–1299. [Google Scholar] [CrossRef]
- Legault, C.; Jennings, J.M.; Katula, J.A.; Dagenbach, D.; Gaussoin, S.A.; Sink, K.M.; Rapp, S.R.; Rejeski, W.J.; Shumaker, S.A.; Espeland, M.A. Designing clinical trials for assessing the effects of cognitive training and physical activity interventions on cognitive outcomes: The seniors health and activity research program pilot (SHARP-P) study, a randomized controlled trial. BMC Geriatr. 2011, 11, 27. [Google Scholar] [CrossRef]
- Shatil, E. Does combined cognitive training and physical activity training enhance cognitive abilities more than either alone? A four-condition randomized controlled trial among healthy older adults. Front. Aging Neurosci. 2013, 5, 1–12. [Google Scholar] [CrossRef]
- Anderson-Hanley, C.; Barcelos, N.M.; Zimmrman, E.A.; Gillen, R.W.; Dunnam, M.; Cohen, B.D.; Yerokhin, V.; Miller, K.E.; Hayes, D.J.; Arciero, P.J.; et al. The aerobic and cognitive exercise study (ACES) for community-dwelling older adults with or at-risk for mild cognitive impairment (MCI): Neuropsychological, neurobiological and neuroimaging outcomes of a randomized clinical trial. Aging Neurosci. 2018, 10, 76. [Google Scholar] [CrossRef]
- Maci, T.; Le Pira, F.; Quattrocchi, G.; Di Nuovo, S.; Perciavalle, V.; Zappia, M. Physical and cognitive stimulation in alzheimer disease. AJADD 2012, 27, 107–113. [Google Scholar]
- Bacha, J.M.R.; Gomes G, C.V.; de Freitas, T.B.; Viveiro, L.A.P.; da Silva, K.G.; Bueno, G.M.; Pompeu, J.E. Effects of Kinect adventures games versus conventional physical therapy on postural control in elderly people: A randomized controlled trial. Games Health J. 2018, 7, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Schimada, H.; Makizako, H.; Doi, T.; Park, H.; Tsutumimoto, K.; Verghese, J.; Suzuki, T. Effects of combined physical and cognitive exercises on cognition and mobility in patients with mild cognitive impairment: A randomized clinical trial. JAMDA 2018, 19, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Barcelos, N.; Shan, N.; Cohen, K.; Hogan, M.J.; Mulkerrin, E.; Arciero, P.J.; Cohen, B.D.; Kramer, A.F.; Anderson-Hanley, C. Aerobic and cognitive exercise (ACE) pilot study for older adults: Executive function improves with cognitive challenge while exergaming. J. Int. Neuropsychol. Soc. 2015, 21, 768–779. [Google Scholar] [CrossRef] [PubMed]
- Eggenberger, P.; Wolf, M.; Schumann, M.; de Bruin, E.D. Exergame and balance training modulate prefrontal brain activity during walking and enhance executive function in older adults. Front. Aging Neurosci. 2016, 8, 66. [Google Scholar] [CrossRef]
- Flak, M.M.; Hernes, S.S.; Skranes, J.; Lohaugen, G.C.C. The memory aid study: Protocol for a randomized controlled clinical trial evaluating the effect of computer-based working memory training in elderly patients with mild cognitive impairment (MCI). Trials 2014, 17, 1–7. [Google Scholar] [CrossRef]
- Joubert, C.; Chainay, H. Aging brain: The effect of combined training on cognition as compared to cognitive and physical training alone- a systematic review. Clin. Interv. Aging 2018, 13, 1267–1301. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the selection process of studies for inclusion in the systematic review.
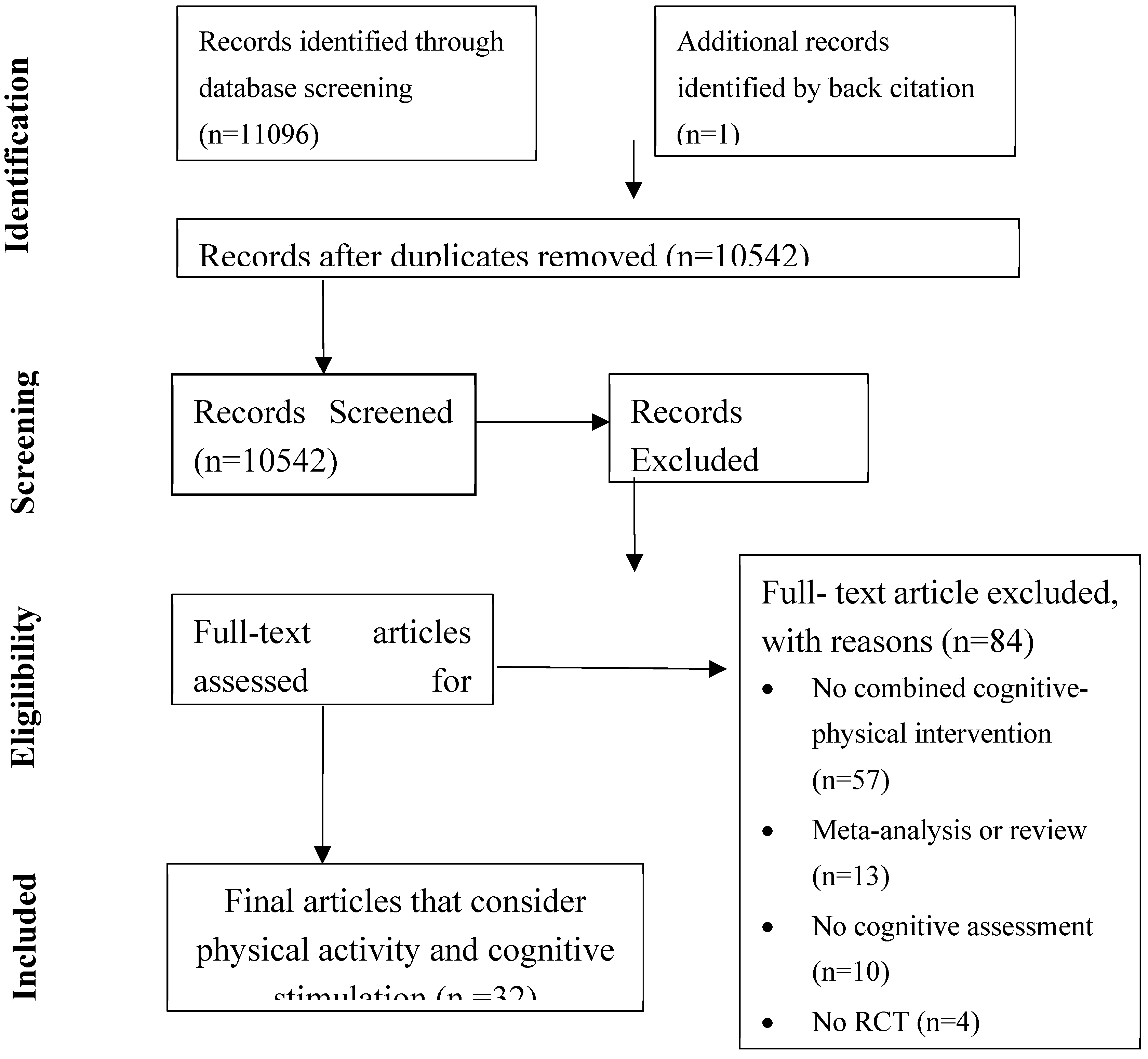

Table 1.
Critical appraisal of the studies with randomized design included in the review, based on Cochrane risk of bias tool.
Table 1.
Critical appraisal of the studies with randomized design included in the review, based on Cochrane risk of bias tool.
| Study | Random sequence generation | Allocation concealment | Blinding of patients, personnel | Incomplete outcome data | Selective outcome reporting | Overall bias |
|---|---|---|---|---|---|---|
| [16] | Low | Low | High | Some concerns | Low | Some concerns |
| [23] | Some concerns | High | High | Some concern | Some Concern | High |
| [24] | Low | Some concerns | Some concerns | Low | Low | Low |
| [26] | Some concern | Some concern | Low | Some concern | Some concern | Some concern |
| [29] | Low | Some concern | Some concern | Some concern | Some concern | Some concern |
| [30] | Low | Some concerns | Some concerns | Low | Low | Low |
| [31] | Low | Low | Low | Low | Low | Low |
| [32] | Some concerns | Some concerns | Some concerns | Low | Some concerns | Some concerns |
| [33] | Some concerns | High | High | Some concerns | Some Concerns | High |
| [34] | Low | Low | Low | Low | Low | Low |
| [35] | Some concerns | Some concerns | High | Some concerns | Some concerns | Some concerns |
| [36] | Low | Some concerns | Some concerns | Low | Low | Low |
| [37] | Low | Low | Some concerns | Low | Low | Low |
| [38] | Some concerns | Some concerns | High | Some concerns | Some concerns | Some concerns |
| [39] | Low | Some concern | Low | Low | Low | Low |
| [40] | Low | Low | High | Low | Low | Low |
| [41] | Low | Some concerns | Some concerns | High | High | High |
| [42] | Some concerns | Low | Low | Low | Low | Low |
| [43] | Low | Some concerns | Low | Low | Some concerns | Low |
| [44] | Some concern | Some concern | Some concern | Low | Low | Some concern |
| [45] | Low | Some concern | Low | Low | Low | Low |
| [46] | Low | Low | Low | Low | Low | Low |
| [47] | Low | Low | Low | Some concern | Low | Low |
| [48] | Some concerns | High | Some concerns | High | Some concerns | High |
| [49] | Some concerns | Some concerns | Some concerns | Low | Low | Some concerns |
| [50] | Some concerns | Some concerns | Some concerns | High | High | High |
| [51] | Low | Some concern | Low | Low | Low | Low |
| [52] | Low | Some concerns | Low | Low | Some concerns | Low |
| [53] | Low | Some concern | Low | Low | Low | Low |
| [54] | Low | Low | Low | Low | Low | Low |
| [55] | Low | Low | Low | Low | Low | Low |
| [56] | Low | Some concern | High | Some concern | Low | Some concern |
Table 2.
Summary of studies involving physical activity and cognitive stimulation.
| Authors and year | n | Interventions frequency | Follow-up | Cognitive intervention component | Physical intervention component | Participant type | Aims | Major findings |
|---|---|---|---|---|---|---|---|---|
| Adcock et al., (2020) | 37 | 30-40 minutes; 3x /week 16 weeks |
No | Step-based cognitive exercises | Tai-chi, dancing, step training (exergame) | Cognitively health | Evaluate the effect of an Exergaming workout, performed at home, on physical activity, cognitive functioning, and brain volume. | The findings indicated a positive influence of exergame training on executive functioning. No improvements in physical functions or brain volume were evident in this study. |
| Anderson-Hanley et al. (2018) | 13 | 45 minutes; 4x /week 24 week |
No | Exergame | Cycling | Mild Cognitive Impairment | The Aerobic and Cognitive Exercise Study (ACES) sought to replicate and extend prior findings of added cognitive benefit from exergaming to those with or at risk for mild cognitive impairment (MCI). | There were significant moderate improvements in executive functions and verbal memory. Effects appeared to generalize to self-reported everyday cognitive function. |
| Bacha et al. (2018) | 46 | 60 minutes; 2x/ week; 7 weeks |
No | Exergame | Exergame | Cognitively health | To compare the effectiveness of Kinect Adventures games versus conventional physiotherapy to improve postural control, gait, cardiorespiratory fitness, and cognition of the elderly. | Both interventions provided positive effects on postural control, gait, cardiorespiratory fitness, and cognition of the elderly. |
| Barban et al., (2017) | 481 | CT=30 minutes; 2x week PA= 30 minutes; 2x week 12 weeks |
Yes (3 months) | Multidomain CCT- Executive function | Motor training | Cognitively health | Study the impact of physical activity and cognitive stimulation on fear of falling | The results demonstrated significant improvements in executive functions. |
| Barcelos et al. (2015) | 17 | 20-45 minutes; 2-5x/ week 12 weeks |
Exergaming – Executive function | Cycling | Cognitively health | Investigate whether greater cognitive challenge while exergaming would yield differential outcomes in executive function and generalize to everyday functioning. | Pilot data indicated that for older adults, cognitive benefit while exergaming increased concomitantly with higher doses of interactive mental challenge. | |
| Barnes et al., (2013) | 126 | 1 hour; 3x/ week 12 weeks |
No | Multidomain | Aerobic exercise and strength exercise | Mild Cognitive Impairment | Examine the combined effects of physical plus mental activity on cognitive function. | In inactive older adults with cognitive complaints, physical and mental activity was associated with significant improvements in global cognitive function. |
| Boa Sorte Silva et al. (2018) | 127 | 60 minutes; 3x/ week 24 weeks |
No | Square-stepping exercise, memorizing complex stepping patterns | Aerobic, stepping training and resistance | Mild Cognitive Impairment | Investigated the effects of multiple-modality exercise with additional mind-motor training on cognition in community-dwelling older adults with subjective cognitive complaints. | Additional mind-motor training did not impart greater immediate benefits to cognition among the study participants. |
| Desjardins-Crépeau et al., (2016) | 76 | 12 weeks; 24 sessions of 60-minutes of physical exercise 12 sessions of 60-minutes of cognitive stimulation 3x/week (2 physical and 1 cognitive) |
No | Dual Task Exercises | Treadmill walking and resistance training |
Cognitively healthy | Examine the effects of combined physical and cognitive interventions on physical fitness and neuropsychological performance in healthy elderly people. | There were no significant improvements. |
| Donnezan et al., (2018) | 69 | 24 sessions lasting 1 hour over 12 weeks 2x /week |
Yes (six months) | Executive functions, working memory, namely, mental flexibility, inhibition, reasoning and updating. | Aerobic training on bikes, | Mild Cognitive Impairment | Compare the benefits of cognitive and physical training simultaneously, with each training administered separately in executive, cardiorespiratory and walking functions, to assess a potential additional additive effect. | It was more advantageous to administer cognitive training and physical activity simultaneously than alone. |
| Eggenberger et al., (2015) | 89 | 1 hour; 2x/ week 6 months |
Yes (1 year) | Verbal memory training | Dance, walk, strength and balance exercises | Mild Cognitive Impairment | Understand if the combination of physical activity and cognitive stimulation has greater benefits for the elderly, compared to physical activity practiced in isolation. | Executive functions benefited from simultaneous cognitive–physical training compared to exclusively physical multicomponent training. |
| Eggenberger et al. (2016) | 33 | 30 minutes; 3x/ week 8 weeks |
No | Videogame dancing | Videogame dancing, with exergaming | Cognitively healthy | This study aimed to investigate if exercise training induces functional brain plasticity during challenging treadmill walking and elicits associated changes in cognitive executive functions. | There were improvements in executive functioning. |
| González-Palau et al., (2014) | 50 | 1h of physical training 40 minutes of cognitive stimulation 3x/ week 12 weeks |
No | Attention, perception, episodic memory and working memory. | Warm-up, aerobic exercises, endurance, strength, balance, stretching and cool-down training exercises. | Cognitively healthy and Mild Cognitive Impairment | The main objective of this study was to present the preliminary results that determine the possible effectiveness of the Long Lasting Memories program in the improvement of cognitive functions and symptoms of depression in healthy elderly and subjects with mild cognitive impairment. |
Significant improvements after the implementation of the program. |
| Htut et al. (2018) | 84 | 30 minutes; 3x/ week 8 weeks |
No | X-box360 games (exergaming) | X-box 360 games (exergaming) | Cognitively healthy | Compared the effects of Physical exercise, virtual reality-based exercise, and brain exercise on balance, muscle strength, cognition, and fall concern. | Significant improvements in checking physical and cognition |
| Karssemeijer et al., (2019) | 115 | 12 weeks, 30- 50 minutes; 3x/ week. | Yes (12 and 24 months) | Executive functions, episodic memory, working memory, psychomotor speed. (exergaming) | Aerobic training, relaxation, and flexibility exercises. | Dementia | Investigate the effect of training with exergame and aerobic training on cognitive functioning in elderly people with dementia. | Significant improvements were found in the combination of physical activity and cognitive stimulation. |
| Laatar, et al. (2018) | 24 | 60 minutes; 3x/ week 24 week |
Yes (6 months) | Cognitive tasks | Balance- strength exercises | Cognitively healthy | This study examined postural, physical and cognitive performances and postural performance during daily life tasks in older adults pre- and post- 6-months physical and physical-cognitive interventions. | Only simultaneous physical-cognitive training modality enhanced performance in some tasks relative to everyday abilities. Nonetheless, these gains were lost after 3 months of detraining period suggesting a need for older people to participate regularly in such training for their daily life independence. |
| Legault et al., (2011) | 67 | CT= 10-12 minutes.; 2x/week 2 months PA= 150minutes/week 4 months |
No | Memory, executive functions | Aerobic and flexibility | Cognitively healthy | Understand the effectiveness of a physical and cognitive intervention program on the cognitive functioning of the elderly. | The interventions produced marked improvements in cognitive and physical performance measures. |
| Linde and Alfermann (2014) | 55 | 40 minutes 16 weeks |
Yes (12 weeks) | Information processing speed, short-term memory, spatial relations, concentration, reasoning, and cognitive speed |
Aerobic and strength | Cognitively healthy | The objective of this study was to analyze the short- and long-term effects of physical, cognitive, and combined physical plus cognitive training regimens on age-sensitive fluid cognitive abilities. |
Physical, cognitive, and combined physical plus cognitive activity can be seen as cognition-enrichment behaviors in healthy older adults that showed different rather than equal intervention effects. |
| Maci et al., (2012) | 14 | 3 months; 1 hour of physical activity, 1 hour of cognitive stimulation and 30 minutes of group discussion; 5x/ week. |
No | Spatiotemporal orientation, memory, executive skills, and language. | Aerobic exercise of mild intensity. | Dementia | Evaluate the effect of cognitive stimulation, physical activity, and socialization in patients with AD and on the quality of life and mood of their informal caregivers. | Significant improvements were found in the combination of physical activity and cognitive stimulation. |
| Maffei et al. (2017) | 113 | CT= 60 minutes; 3x/week 7 months PA= 1hour; 3x/week 7 months |
Yes (1 year) | Multidomain | Aerobic, strength and flexibility |
Mild Cognitive Impairment | Assess the efficacy of combined physical-cognitive training on cognitive decline, Gray Matter (GM) volume loss and Cerebral Blood Flow (CBF) in hippocampus and parahippocampal areas, and on brain-blood-oxygenationlevel- dependent (BOLD) activity elicited by a cognitive task |
The results showed that a non-pharmacological, multicomponent intervention improved cognitive status and indicators of brain health in MCI subjects. |
| Maillot et al. (2012) | 32 | 60 minutes; 2x/ week 12 weeks |
No | Nintendo Wii games (exergaming) | Nintendo Wii games (exergaming) | Cognitively healthy | The purpose of this study was to assess the potential of exergame training based on physically simulated sport play as a mode of physical activity that could have cognitive. benefits for older adults. |
The trainees improved significantly in measures of game performance. They also improved significantly more than the control participants in measures of physical function and cognitive measures of executive control and processing speed functions, but not on visuospatial measures. |
| McDaniel et al. (2014) | 79 | 60 minutes; 6x/ week (CT=3; PA=3) 24 weeks (PA=24; CT=8) |
No | Attentional coordination, prospective memory, and retrospective-memory retrieval |
Aerobic Exercise | Cognitively healthy | Investigate the potential benefits of a novel cognitive training protocol and an aerobic exercise intervention, both individually and in concert, on older adults’ performances in laboratory simulations of select real-world tasks. | The findings suggested that at least for everyday oriented prospective memory tasks involving cognitive challenges, well-designed cognitive training programs may confer more robust gains in performance than a standard aerobic exercise program over a limited (6-month) period. |
| Nishiguchi et al., (2015) | 48 | 90 minutes; 1x/week 12 weeks |
No | Multidomain | Walking, strength | Cognitively healthy | Investigate whether a 12-week physical and cognitive exercise program can improve cognitive function and brain activation efficiency in community dwelling older adults. | Physical activity alone and combined cognitive and exercise training can improve cognitive function in older adults. |
| Norouzi et al. (2019) | 60 | 60-80 minutes; 3x/ week 4 weeks |
Yes (12 weeks) | Cognitive tasks | Resistance | Cognitively healthy | The aim of this study was to investigate whether and to what extent two different dual-task interventions improved both working memory and balancing. | Dual-task interventions improved both balance performance and working memory, but more so if cognitive performance was specifically trained along with resistance training |
| Park et al., (2019) | 49 | 110 minutes 24 weeks |
Yes (3months) | Word games, memory, numerical calculations | Aerobic exercise (stair stepping, walking and stair climbing) warm-up, stretching, balance exercise, | Mild Cognitive Impairment | Investigate the association between a dual-task intervention program and cognitive and physical functions. |
The 24-week combined intervention improved cognitive function and physical function in patients with MCI relative to controls. |
| Rahe et al., (2015b) | 30 | 90 minutes; 2x/week 6.5 weeks |
Yes (1 year) | Memory, attention, and cognitive functions | Strength, flexibility, and coordination/balance | Cognitively healthy | Compare the effect of the combination of cognitive stimulation and physical activity with the administration of cognitive stimulation separately, in healthy elderly people. | The results suggested that the combination of physical activity and cognitive stimulation is advantageous in terms of long-term care. |
| Rahe et al., (2015) | 68 | 90 minutes; 2x/ week 7 or 8 weeks; |
No | Multidomain and/ or counseling | Strength, flexibility, coordination, endurance, and aerobic exercise | Cognitively healthy | Understand the additional benefit of combining physical activity with cognitive stimulation in healthy aging. | Data was inconsistent concerning the question of whether cognitive-physical training yields stronger cognitive gains than cognitive training. |
| Rezola-Pardo et al. (2019) | 85 | 60 minutes; 2x/week 12 weeks; |
No | Cognitive tasks (Attention, executive function, semantic memory) |
Strength and balance | Cognitively healthy | Determine whether the addition of simultaneous cognitive training to a multicomponent exercise program offers further benefits to dual-task, physical and cognitive performance, psycho-affective status, quality of life and frailty in older adults living in long-term nursing homes. | The addition of simultaneous cognitive training did not seem to offer significantly greater benefits to the evaluated multicomponent exercise program in older adults. |
| Shatil, (2013) | 122 | CT= 40 minutes; 3x/week; 16 weeks; PA= 45 minutes; 3x/week; 16 weeks; |
No | Multidomain | Aerobic exercise, strength, flexibility, aerobic warm-up, cardiovascular workout seated and standing, aerobic cool-down | Cognitively healthy | Understand the effect of the combination of physical activity and cognitive stimulation and compare its effect with each of the interventions administered in isolation. | The results suggested that the elderly who were submitted to cognitive stimulation had more benefits in terms of cognitive functioning. |
| Shimada et al. (2018) | 308 | 90 minutes; 1x/ week 40 weeks |
No | Multidomain CT | Aerobic, strength and balance | Mild Cognitive Impairment | To compare the cognitive and mobility effects of a 40-week program of combined cognitive and physical activity with those of a health education program. | Combined physical and cognitive activity improved or maintained cognitive and physical performance in older adults with mild cognitive impairment, especially the amnestic type. |
| Van het Reve and de Bruin (2014) | 156 | CT= 10 minutes; 3x/week; PA= 40 minutes; 2x/week; 12 weeks; |
No | Single domain CCT (attention) |
Strength and balance | Cognitively healthy | To assess the effects of the combination of physical activity and cognitive stimulation on walking and cognitive functioning. | Combining strength-balance training with specific cognitive training had a positive additional effect on dual task costs of walking, gait initiation, and divided attention. |
| Van Santen et al., ( 2020) | 112 | 2x /week; 6 months; |
Yes (3 and 6 months | Multidomain (exergaming) | Cycling | Dementia | Evaluate the effects of exergaming in the cognition. |
Mixed-model analyses showed no statistically significant effects on primary outcomes |
| Yoon et al., (2013) | 30 | 30 minutes; 3x / week 12 weeks |
No | Memory | Cycling exercise | Dementia | Understand the additional benefit of combining physical activity with cognitive stimulation in healthy aging. | Significant improvements were found in the combination of physical activity and cognitive stimulation. |
Note. CCT = computerized cognitive training; CT = cognitive training; PA= physical activity; RCT= randomized control trial; AD= Alzheimer disease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



