
Submitted:
12 May 2023
Posted:
12 May 2023
You are already at the latest version
Abstract
The affected upper limb in children with Unilateral Spastic Cerebral Palsy (US CP) has motor and somatosensory impairments, that contribute negatively to children’s bimanual performance and quality of life. Mirror Therapy (MT) is being studied to become an approachable intensive and home-based therapy, suitable for children with US CP. The aim of this study is to examine the feasibility of a 5-week home-based program of MT for children with US CP. Six children aged 8-12 years old performed the therapy, five days per week, 30 minutes per day. A minimum of an 80% of compliance was required. The evaluations included the feasibility of the therapy (compliance, total dosage, perceived difficulty of the exercises, and losses of follow-ups and evaluations), the bimanual performance, the somatosensory function and the quality of life at baseline, at the end of the intervention, and at 1-month follow-up. All children completed the therapy and were included in the analysis. The total accomplishment was 86.47 ± 7.67. The perceived difficulty of the exercises ranged from 2,37 to 4,51. As a conclusion, a home-based program of Mirror Therapy is suitable and feasible for children with US CP.
Keywords:
Unilateral Spastic Cerebral Palsy
; Mirror Therapy
; feasibility
; bimanual performance
; somatosensory function
; quality of life.
1. Introduction
Unilateral Spastic Cerebral Palsy (US CP) is the second most frequent type of Cerebral Palsy (CP), representing approximately a 30% of the total [1,2]. Children with US CP have functional impairments in one side of their body, affecting both the upper and the lower limb [3].
The affected upper limb (AUL) suffers from different impairments at the areas highlighted by the International Classification of Functioning, Disability, and Health: body functions and structures, activities, and participation [4].
Even though spasticity is the main characteristic, especially in flexor muscles, problems related to limitations in the range of movement and low muscle strength are also present. These structural impairments mostly affect the distal parts of the AUL [5]. The somatosensory function of the hand is also affected, but the exact extent of the problem remains unclear [5]. In some studies, the percentage of children with these impairments ranges from 50% to 86% [5,6,7,8].
Both motor and sensory impairments have demonstrated to be partly responsible of the functional limitations of the AUL. The unimanual capacity of the AUL is determined by these functional limitations. Those include poor grip strength and dexterity, and decreased velocity, among others [7,9,10]. Kinematic abnormalities are usually observed, especially at the distal parts of the AUL [6,11].
A poorer unimanual capacity of the AUL is related to poorer bimanual performance of children with US CP. This may explain the fact that children with US CP show low performance of the activities of daily living, as they mainly imply bimanual performance and coordination of both bands [12]. This finding is also correlated with the functional level in the Manual Ability Classification System (MACS) [5,11]. Usually, children with US CP are classified in the first three levels in MACS, mostly in level II [13].
Some therapies have been highly recommended to improve both unimanual capacity and bimanual performance in children with US CP, such as Constrained-Induced Movement Therapy, Hand-Arm Bimanual Intensive Training, and Goal Directed Trainings, among others [14,15,16,17,18]. Considering that intensity is an important predictor for treatment success, is it assumable that in the last two decades, literature recommending intensive approaches for improving motor activities and function in children with CP has increased [16,18]. Intensity, meaning the duration of the intervention and the distribution of the total dosage of the targeted therapy, may be a key point in all these approaches. This is especially crucial when considering the best therapy and its suitability for responding to parents’ and children’s goals [19].
Another key factor when considering the best approach is the setting of the therapy. All these therapies suitable for children with US CP have usually been provided in a natural environment, as home [14,15,16,17,18]. The home setting offers the possibility to increase the intensity and repetition, especially when compared to interventions completely set in a clinical environment [15].
In general, the family-centered care is related with improvements on the well-being of children with disabilities. It also improves the well-being of their families, as it enhances the participation of parents into the interventions and focuses on real context approaches [20]. Moreover, therapies performed at home with the supervision of parents have demonstrated to increase the enjoyment and positiveness of families about their children, as they are capable of experiencing the improvements in a real context [21].
However, families can sometimes find it difficult to fit the home-based programs into their daily routines, when the designed programs or therapies are too demanding. Some strategies may help to improve and facilitate this adaptation [21]. Among them, coaching models, where the communication between therapists and families forms the basis for the clinical approach of the interventions, are recommended [20]. In the last years, tele-rehabilitation and video-monitoring have improved the participation and the goals’ achievement of home-based therapies, and have showed to improve the implication of the families into the therapies[22].
Different home-based approaches for children with US CP have demonstrated their feasibility, in terms of acceptability and safety. When parents act as either the providers or the supervisors of the therapies, the compliance of the treatment is high [21].
Studies analyzing the effectiveness of Mirror Therapy (MT) have recently emerged. MT is a therapy consisting of placing a mirror in the sagittal plane of a patient suffering from a unilateral condition affecting upper or lower limbs, in such a manner that the view of the non-affected limb is superimposed to the image of the affected limb. This results in an illusion of the movement of the affected limb [23].
In the last decade, research of MT for children with US CP has increased. It has been included in the therapeutic approach for children with US CP alone or combined with other interventions. In some studies, it has been showed as a therapy capable of improving pinch and grasp strength [24,25], dexterity [26], upper limb function [24,27], gross motor skills [28], bimanual skills [27,29], activity performance [29], in children with US CP, but to a limited extend. Other benefits still remain unclear [25,29,30,31,32].
Some authors have studied MT or mirror conditions in a clinical environment [26,28,29,31,32]. Nevertheless, it is a suitable therapy to be performed at home [24,27,30], as it is a cost-efficient, easy and approachable therapy. Thus, more research is needed in order to recommend the implementation of MT in the therapeutic strategies for children with US CP [16,18,25,33,34,35].
The aim of this study is to analyze the feasibility of a home-based program of MT in children with US CP.
2. Materials and Methods
This study is a feasibility study. It includes the feasibility analysis of a group of children performing a Mirror Therapy program. This analysis is prior to a single-blinded Randomized Clinical Trial (RCT) (NCT05244083). The RCT has been approved by the Ethics Committee of FIDMAG Germanes Hospitalàries (PR-2021-18) and the Ethics Committee of the International University of Catalonia (FIS-2021-07).
The MT group analyzed in this study included six children between 8 and 12 years old, diagnosed with Unilateral Spastic Cerebral Palsy, and classified in levels I and II in the MACS. The exclusion criteria were: a) botulinum toxin injections and/or radial shock waves applied in the affected upper limb in less than 3 months prior to enrollment; b) surgeries in the affected upper limb 6 months prior to enrollment; c) being performing any intensive therapy for the affected upper limb); d) moderate and severe intellectual disabilities; e) existing comorbidities affecting attention or behavior; f) non-corrected visual impairments and; g) non-controlled epilepsies. Two more exclusion criteria were applied for the families, as at least one of the parents should be able to answer questionnaires in Spanish, and they should have a table and a chair at home to perform the therapy.
The intervention of the MT group consisted of a home-based program of Mirror Therapy, that was expected to be performed during 5 weeks, 5 days a week, 30 minutes a day. A 5-minute rest could be done in the middle of the therapy. All exercises were designed to be done by children themselves, and the families were involved in the supervision and maintenance of the concentration. The MT program included four bimanual exercises (forearm pronosupination, sponge squeezing, finger-by-finger modeling clay pressing, and clockwise and anti-clockwise wrist spins), following exercises recommended by other authors [24,26,29,30,36] (see Figure 1). When doing the therapy, children were asked to introduce the affected upper limb in a Mirror Box [37] (available from: www.noigroup.com), that was placed at their sagittal plane. All the exercises had to be done bimanually and symmetrically, moving both hands.
In order to increase motivation, children were told to do at least 2 of the 4 exercises suggested each day, letting them to choose which exercises they wanted to practice, and their order. Families were not told when they should do the therapy, to increase the adaptability to perform the intervention at home. A minimum of an 80% of compliance of the total dosage (600 out of the total 750 minutes) was required.
Regarding the follow-up of the home-based intervention, a mobile health application was used. Each family was logged in the app, where they could find a video of each of the exercises. Every day, families were told to register which exercises they performed, the minutes they were doing the exercises, and the perceived difficulty of the exercises by the child. Moreover, the principal investigator (A.O-M) set a weekly videocall with each family, to encourage and help them. When the videocall could not be set, the family was asked to send video recordings to the principal investigator doing the therapy. A training day was set before the beginning of the intervention, in which both the child and the family were instructed by the principal investigator about the procedure of the intervention and the functioning of the app. Moreover, all families were given all the materials needed for implementing the intervention (Mirror Box [37], two cubes of modelling clay, and two sponges), so as the study had no cost for them (cost lower than 70 €, even neglectable).
Regarding the registration of the compliance of the intervention, as previously said, the application had a user-friendly approach. It allowed the family and the child to use a chronometer, in order to quantify the daily total amount of time of the duration of the intervention. Therefore, the registration of the completed time was performed automatically. In addition, the application also allowed to report the exercises performed each day, as well as the perceived difficulty of each of them, through a very simple visual scale. It was rated from 0 – no perceived difficulty to 10 – extremely difficult.
Nevertheless, in order to avoid difficulties with the usage of the app, a registration form was also given to all the families, allowing them to write down the same information that was demanded in the app. A printed version of the explanation of the exercises was also given.
During the entire duration of the study, three evaluations were established: at baseline, at the end of the intervention, and at 1-month follow-up. In these, the bimanual performance, the somatosensory function of the affected upper limb and quality of life were assessed.
Firstly, bimanual performance was assessed with the Children’s Hand-use Experience Questionnaire 2.0 (CHEQ 2.0) [38,39,40]. The CHEQ 2.0 is a valid and reliable questionnaire designed to assess the quality of the bimanual performance of children with Unilateral Cerebral Palsy from 6 to 18 years old. The Spanish version was used for this study, available online (www.cheq.se). It analyses the grasp efficacy, the time taken and the bothering feeling that children and/or parents perceive when performing 27 different daily activities, rating into a four-category scales. Then, punctuation is transformed in a 0-100 scale. CHEQ 2.0 can be answered by children or by parents. Nevertheless, the recommendation for children under 12 years is to be answered by children helped by parents, or only by parents as proxy [39,40]. In this study, parents were the responders of the CHEQ 2.0.
Secondly, the somatosensory function assessment was done performing six tests described and recommended by Auld et al [41,42]. The assessment was done by a Physiotherapist. A newly calibrated 20-item Semmes Weinstein Monofilaments (SWM) was used to test tactile registration [43], as well as for the single-point localization (SPL), and the double simultaneous (DS). The two-point discrimination tests, both static (s2PD) and moving (m2PD) were performed by using a Disk-Criminator [44]. From all these tests, SWM, s2PD, m2PD and SPL are considered the most reliable in terms of detecting changes over time [41]. Finally, stereognosis was assessed with nine common objects [41,42]. The procedure of these tests can be found in the study of Auld et al [41,42].
Thirdly, quality of life was assessed with the Child and Parent Reports of the Pediatric Inventory of Quality of Life for Cerebral Palsy (PedsQL 3.0 ™), Cerebral Palsy module for children aged 8-12 [45,46]. PedsQL™ are valid and reliable questionnaires to assess the quality of life of children with Cerebral Palsy. For the range of age to which this study was addressed, the tool offers two questionnaires to be answered by the children and by the parents, respectively. Both are 5-point Likert scale questionnaires, that include 35 items, regarding the areas of daily activities, school activities, movement and balance, pain and hurt, fatigue, eating activities and speech and communication. After completing the questionnaires, the obtained punctuation is transformed in a 0-100 scale [46].
Due to the structure of the included evaluations, the evaluator could only be blinded for the somatosensory function assessment. C.V-F acted as the blinded evaluator.
Apart from these assessments, age, sex, MACS level, and impaired side were registered for all participants at the baseline evaluation.
Statistical analysis was performed using descriptive statistics to show general characteristics. Kolmogorov-Smirnov test was used to test normality. Mann-Whitney U test was used to analyze intra-group effect differences. The significance level was set at α = 0.05. All analyses were performed by using the v.29 SPSS software package.
3. Results
3.1. Participants
Six participants were included in this feasibility study. The mean age was 10.37 ± 2.05. Table 1 shows the main characteristics of the whole group.
3.2. Compliance and Total Dosage
All the participants acquired the minimum compliance required (80% of the total therapy), ranging from 80.0% to 96.0%. The mean percentage of compliance was 86.47 ± 7.67. When considering the total minutes of therapy performed, the mean was 648.55 ± 57.55. Table 2 shows the total minutes of MT performed by each child, and Figure 1 shows the individual compliance.
3.3. Perceived Difficulty of the Exercises
The data extraction of the perceived difficulty of the exercises was performed considering n = 5, as one child did not complete the registration. From the four included exercises in the MT program (forearm pronosupination, sponge squeezing, finger-by-finger modeling clay pressing, and clockwise and anti-clockwise wrist spins), all children rated them below 8, when scoring their perceived difficulty. The forearm pronosupination and the sponge squeezing exercises were considered the easiest, with a weekly individual mean ranging from 2.37 to 3.17, and from 2.56 to 3.19, respectively.
No differences were shown at the perceived difficulty regarding age, sex or MACS level of the participants (p > 0.05).
Table 3 shows the weekly mean perceived difficulty of all exercises. No statistical differences were shown when comparing the evolution of the perceived difficulty of any exercise.
3.4. Losses of Follow-Ups and Evaluations
There were no losses of follow-ups in this group. All six children completed the entire therapy. Only one participant needed the paper form registration, as the family had difficulties with the app functioning. Although one child did not use the app, all six children registered the daily therapy. The six families were available weekly to either do a videocall with A.O-M or to send videos performing the therapy.
Regarding the evaluations, all were completed at baseline and at the end of the intervention. Only one family missed to complete entirely the PedsQL™ at the one-month follow-up evaluation. Thus, this last questionnaire was excluded from the register. Table 4 shows the completed evaluations from the whole group.
4. Discussion
This study aimed to analyze the feasibility of a home-based program of Mirror Therapy, designed for improving motor and somatosensory impairments, as well as the quality of life, of children with Unilateral Spastic Cerebral Palsy. Concretely, this study analyzes the compliance, the total dosage, the children’s perceived difficulty of the included exercises, as well as the existence of losses of follow-ups and evaluations.
Other authors had previously studied MT in the same population. Bruchez et al. [30], designed a home-based protocol that included seven exercises, comprising symmetrical movements of both distal and proximal parts of the upper limbs (finger-by-finger modelling clay pressing, thumb-index pinch-extension, palmar squeezing, wrist rotations, pronation and supination of the forearms, shoulder antepulsion and retropulsion, and shoulder abduction and adduction). Narimani et al. [26], designed a 6-week clinical-based program of MT, that included flexion and extension of the fingers and wrists, supination and pronation, and functional movements. The pilot study of Gygax et al. [24], described a MT intervention of 3 weeks, that included three bilateral exercises (two regarding thumb-finger pinch, and one of forearm pronosupination). Kara et al. [29], proposed a combination of MT and upper limb strength and power exercises. The MT was performed by doing four exercises (two of thumb-finger pinch, one of grasping a ball, and one of forearm pronosupination), during 30 minutes, 3 days a week, for 12 weeks. Auld et al. [31], designed a MT intervention that combined motor and tactile exercises, during 1,5 hours in two sessions. Farzamfar et al. [28], included several exercises that involved the whole upper limb. Palomo-Carrión et al. [27], designed a 4-week intervention with MT combined with Action-Observation Therapy. In this study, MT was performed during 15 minutes per day, and included six exercises.
In our study, the intervention was designed to comprise 750 minutes of MT, distributed in 5 weeks, 30 minutes daily. This goes in line with other studies implementing MT, where the designed total dosage ranged between 94 to 1080 minutes [24,26,27,28,29,30,31]. The distribution of the therapy is not consistent. While other studies distributed the therapy between 2 days and 12 weeks, our study designed a 5-week therapy. Moreover, the duration of the sessions varied between 15 minutes and 90 minutes [24,26,27,28,29,30,31]. Nevertheless, a duration of 30 minutes of each session, as our study proposed, is the most designed intervention [26,28,29]. A systematic review showed that different home-based programs for children with US CP had a duration between 2 weeks and 6 months, with an intensity between 70 minutes to 56 hours a week [21]. In these terms, our study was designed likewise these recommendations, regarding the total dosage and the distribution of the therapy. A 5-week duration was the minimum duration of an intensive program for Myrhaug et al. [15]. This study also accomplished that specification, as all children completed the 5-week program. For Beckers et al. [47], a duration of 12 weeks was experienced as too hard for families and children.
A compliance of more than 85% was shown in this study. This result agrees with other studies analyzing the feasibility of different home-based programs, where a compliance from 56% to 99% was shown [21,27,48,49]. The compliance in a MT intervention was only reported by Palomo-Carrión et al. [27], where 96% of the total dosage of the intervention was completed by all participants. This high compliance achieved could be explained by many factors. First of all, the fact that parents act as providers of the therapy could engage families to participate and continue until the end of the intervention. It has been stated that home-based therapies provided by parents are the most used home-based approaches, as it increases confidence and satisfaction of families with the therapies, without giving a therapist role to parents [20,21,47,50]. The family-provider approach has been studied and recommended as a key aspect of treating children with CP. Nevertheless, there is a lack of consensus in some terms regarding the relationship between the therapist and the family [20]. Although coaching parents who act as providers of the therapy seems to be an important factor that may influence participation and compliance, most of the studies do not provide or report it specifically. From different studies that showed results of a home-based MT intervention, only the ones by Bruchez et al. [30] and Palomo-Carrión et al. [27], were provided by parents and coached by the therapist. Bruchez et al. [30], gave a DVD with instructions and the training regimen to the families, as well as the contact of the coordinator. In the same way, the families of the study by Palomo et al. [27], received a weekly online follow-up. Gygax et al. [24], also proposed a home-based intervention, but no coaching was described. Finally, the study from Auld et al. [31], varied among others, as the home-based intervention was provided by the therapist. None of these studies reported the compliance, even we could expect a high compliance in the study of Auld et al. [31], as it was therapist-delivered. Other studies with different home-based interventions used other ways to coach families. Some of them used a webcam-monitoring during the performance of the intervention [17], while others maintain weekly phone calls and home visits [51,52].
In order to give a complete coaching, an online follow-up with an app (that contained specific videos of each of the exercises), and a weekly videocall and/or sending videos was required in this study. This coaching approach is similar that the used by Beckers et al. [47], were parents were asked to register the daily intervention and to send a video every week. Moreover, they utilized more strategies to resolve issues during the implementation of the home-based program, including home visits. Telemedicine has experimented an exponential increase since COVID-19 pandemic. It has demonstrated that it can be an opportunity for reducing travels to clinics, maintaining the continuity and the accessibility of the treatments for children with CP [53]. The systematic review from Beckers et al. [21], described these strategies and others to coach families involved in home-based programs. Finding the sufficient but not too much coaching for families involved in a home-based therapy seems to be crucial, as parents sometimes report the coaching received to be usable and valuable for them during the entire intervention, but having too much following (e.g. too much phone calls or home visits) can put extra pressure on families [47].
Other strategies for improving the preparation and confidence of the families include training sessions. In this study, a training session was set with every family, in order to explain the therapy and the functioning of the app. Other authors had also implemented this strategy [48]. Apart from the training day and the videocalls, all families could perform the entire intervention without reporting difficulties or the need for extra coaching.
Another remarkable strategy that we considered for increasing compliance and motivation of children was that we let them choose which exercises they wanted to practice every day. Other studies, like the ones by Bruchez et al. [30], Narimani et al. [26], and Kara et al. [29], described concrete protocols of intervention, where the number of repetitions and the order of the exercises were determined by the therapist or the coordinator. A different approach was utilized by Auld et al. [31], where motor and tactile exercises were included. They distributed a total amount of time of each stimulation, but did not describe a specific order of the motor exercises. Other authors did not describe the distribution of the exercises during the intervention [24,28,36]. Engaging and motivating children seems to be a key factor when considering the benefits and the achievement of outcomes in family-centered approaches, and may be increased when both children and parents are active subjects in the decision-making process of the intervention [20,47].
In this study, children were required to daily score the perceived difficulty of the exercises performed. Even though one child did not complete the difficulty assessment, we found that all the exercises were not considered as very difficult, as all children scored them below 8. Gygax et al. [24], reported that half of the children reported difficulties to maintain concentration during the entire intervention, but did not specifically found a correlation with a difficulty with the exercises. Palomo-Carrión et al. [27], reported that one family had trouble with the intervention. In our study, we decided not to change of increase the difficulty of the exercises, as MT itself can sometimes become quite difficult to perform or requires children to focus on the performing. Other authors also decided not to evolve on the difficulty nor change the exercises during the entire intervention [24,26,28,30,31,36]. Contrarily, Kara et al. [29], reported an increasing on the number of the repetitions of the exercises and the level of the putty when children were more capable of performing the exercises. Our results suggest that the difficulty of the exercises do not necessarily have to be increased, as we found no statistical differences in children’s perceived difficulty. Thus, children performing MT find the same difficulty of the exercises during the entire intervention, meaning that there is no evolution in their easiness. To our knowledge, this is the first study of MT in children with US CP that includes the assessment of the perceived difficulty of the exercises.
In means of the acceptability of the intervention, all families accomplished with these requirements and completed the registration every day. Only one family had difficulties with the usage of the app, so they were given a paper form for registration, and a paper copy of the exercises. Moreover, all families could perform the entire intervention with the initial kit of material they were given in the training day. Thus, the participation in the study had no cost for the families.
The total cost of the intervention was lower than 70 euros per child, meaning that the MT intervention was cost-efficient. A recent study in Spanish population showed that children with CP make around 22 consultations per year at the health services, with a 14,6% of those being to the rehabilitation care [54]. Moreover, it is important to consider that the individual average cost of home-based care in children with CP is considerably lower, compared to center-based care [55]. Family-centered care is still an approach that needs to be more implemented in healthcare services, and requires further investment from different institutions. The low-cost of the implementation of these therapies could be an important argument to implement them [20,56].
With regards of the adverse events, none of the families reported any adverse effects. During the videocalls, some families only reported some fatigue of children when performing the therapy. Other studies also found no adverse effects in either MT or home-based programs for children with US CP [27,29,51].
Regarding the losses of follow-ups or evaluations, all children included in this study completed the entire intervention, thus meaning we obtained no losses of follow-ups. Nevertheless, one child did not fully complete one questionnaire at the last evaluation, and therefore it was excluded. From different studies of MT, losses of follow-ups were related to failures on the execution of the intervention or evaluations [27,30], no cooperation of the children or difficulties with the transportation when the therapy was not set at home [29]. Our results go in line with other studies, that also did not report losses of follow-ups [24,26,28,31]. However, only one of the last studies was set at home, with parents delivering the intervention [24]. Comparing our results with other studies with the same population, other difficulties were described regarding personal issues of the families [47].
This study has some limitations. First of all, a limitation has been considered regarding the nature of the MT. This therapy needs children to be concentrated and focused on the mirror. Gygax et al. [24], reported this as an issue for their study. However, we planned different strategies to enhance engagement, including the mobile health application following. As the mean compliance was high and all the participants acquired the minimum required, we could assume that this issue was not as remarkable as to withdraw the study.
Given the results obtained in this study, we expect promising results in the further RCT with a larger sample size, regarding the feasibility and the effectiveness of the MT.
Further studies comparing different coaching approaches for families and the suitability of this coaching into home-based therapies are needed, in order to define a balanced follow-up for them, that is not too less, but not too many.
5. Conclusions
A home-based Mirror Therapy intervention is feasible for children with Unilateral Spastic Cerebral Palsy, when the therapist acts as a coach and gives support to parents who are in charge of providing the intervention.
Author Contributions
Conceptualization, A.O-M., MC.B-C., R.P-C, and C.V-F.; methodology, A.O-M., MC.B-C., R.P-C.; software, A.O-M.; validation, A.O-M., MC.B-C., R.P-C, and C.V-F.; formal analysis, A.O-M., MC.B-C., R.P-C, and C.V-F; investigation, A.O-M and C.V-F.; resources, A.O-M., MC.B-C., R.P-C, and C.V-F.; data curation, A.O-M.; writing—original draft preparation, A.O-M.; writing—review and editing, A.O-M., MC.B-C., R.P-C, and C.V-F.; visualization, A.O-M.; supervision, MC.B-C., and R.P-C.; project administration, MC.B-C., and R.P-C.; funding acquisition, A.O-M., MC.B-C., R.P-C, and C.V-F.
Funding
This research was funded by the X award for Research of the Societat Catalano-Balear de Fisioteràpia.
Acknowledgments
We acknowledge the support of Fundació Aspace Catalunya for their administrative and technical support in this study. We also aknowledge Societat Catalano-Balear de Fisioteràpia for having awarded this project, and Universitat International de Catalunya for making available material needed to complete this study.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- National Institute For Health and Care Excellence. Cerebral palsy in under 25s: assessment and management. NICE Guidel 2017; 47.
- Wimalasundera, N.; Stevenson, V.L. Cerebral palsy. Pr. Neurol. 2016, 16, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Waikato District Health Board. Cerebral Palsy Clinical Practice Guidelines. 2014.
- World Health Organization. International Classification of Functioning, Disability, and Health: Children & Youth Version: ICF-CY. 2017; 91: 399–404.
- Klingels, K.; Demeyere, I.; Jaspers, E.; De Cock, P.; Molenaers, G.; Boyd, R.; Feys, H. Upper limb impairments and their impact on activity measures in children with unilateral cerebral palsy. Eur. J. Paediatr. Neurol. 2012, 16, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Chaleat-Valayer, E.; Bard-Pondarre, R.; Ganne, C.; Roumenoff, F.; Combey, A.; Bernard, J. Relation between unimanual capacities and bimanual performance in hemiplegic cerebral-palsied children: Impact of synkinesis. Eur. J. Paediatr. Neurol. 2015, 19, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Sakzewski, L.; Ziviani, J.; Boyd, R. The relationship between unimanual capacity and bimanual performance in children with congenital hemiplegia. Dev. Med. Child Neurol. 2010, 52, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Auld, M.L.; Boyd, R.; Moseley, G.L.; Ware, R.; Johnston, L.M. Tactile function in children with unilateral cerebral palsy compared to typically developing children. Disabil. Rehabilitation 2012, 34, 1488–1494. [Google Scholar] [CrossRef] [PubMed]
- Auld, M.L.; Boyd, R.N.; Moseley, G.L.; Ware, R.S.; Johnston, L.M. Impact of Tactile Dysfunction on Upper-Limb Motor Performance in Children With Unilateral Cerebral Palsy. Arch. Phys. Med. Rehabilitation 2012, 93, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Arnould, C.; Bleyenheuft, Y.; Thonnard, J.-L. Hand Functioning in Children with Cerebral Palsy. Front. Neurol. 2014, 5. [Google Scholar] [CrossRef]
- Gaillard, F.; Cretual, A.; Cordillet, S.; Le Cornec, C.; Gonthier, C.; Bouvier, B.; Heyman, R.; Marleix, S.; Bonan, I.; Rauscent, H. Kinematic motion abnormalities and bimanual performance in children with unilateral cerebral palsy. Dev. Med. Child Neurol. 2018, 60, 839–845. [Google Scholar] [CrossRef]
- James, S.; Ziviani, J.; Ware, R.S.; Boyd, R.N. Relationships between activities of daily living, upper limb function, and visual perception in children and adolescents with unilateral cerebral palsy. Dev. Med. Child Neurol. 2015, 57, 852–857. [Google Scholar] [CrossRef]
- Park, E.S.; Rha, D.W.; Park, J.H.; Park, D.H.; Sim, E.G. Relation among the Gross Motor Function, Manual Performance and Upper Limb Functional Measures in Children with Spastic Cerebral Palsy. Yonsei Med J. 2013, 54, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Klevberg, G.L.; Østensjø, S.; Elkjær, S.; Kjeken, I.; Jahnsen, R.B. Hand Function in Young Children with Cerebral Palsy: Current Practice and Parent-Reported Benefits. Phys. Occup. Ther. Pediatr. 2016, 37, 222–237. [Google Scholar] [CrossRef] [PubMed]
- Myrhaug, H.T.; Østensjø, S.; Larun, L.; Odgaard-Jensen, J.; Jahnsen, R. Intensive training of motor function and functional skills among young children with cerebral palsy: a systematic review and meta-analysis. BMC Pediatr. 2014, 14, 1–19. [Google Scholar] [CrossRef]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Mc Namara, M.; Paton, M.C.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef] [PubMed]
- Ferre, C.L.; Brandão, M.; Surana, B.; Dew, A.P.; Moreau, N.G.; Gordon, A.M. Caregiver-directed home-based intensive bimanual training in young children with unilateral spastic cerebral palsy: a randomized trial. Dev. Med. Child Neurol. 2016, 59, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Lake, A.; Haas, T.; Shierk, A. Review of Therapeutic Interventions for the Upper Limb Classified by Manual Ability in Children with Cerebral Palsy. Semin. Plast. Surg. 2016, 30, 014–023. [Google Scholar] [CrossRef]
- Klepper, S.E.; Krasinski, D.C.; Gilb, M.C.; Khalil, N. Comparing Unimanual and Bimanual Training in Upper Extremity Function in Children With Unilateral Cerebral Palsy. Pediatr. Phys. Ther. 2017, 29, 288–306. [Google Scholar] [CrossRef]
- King, G.; Chiarello, L. Family-Centered Care for Children With Cerebral Palsy. J. Child Neurol. 2014, 29, 1046–1054. [Google Scholar] [CrossRef]
- E Beckers, L.W.M.; E Geijen, M.M.; Kleijnen, J.; A A Rameckers, E.; Schnackers, M.L.A.P.; Smeets, R.J.E.M.; Janssen-Potten, Y.J.M. Feasibility and effectiveness of home-based therapy programmes for children with cerebral palsy: a systematic review. BMJ Open 2020, 10, e035454. [Google Scholar] [CrossRef]
- Agarwal, S.; Scher, M.S.; Tilton, A. Cerebral Palsy and Rehabilitative Care: The Role of Home-Based Care and Family-Centered Approach. Indian Pediatr. 2021, 58, 813–814. [Google Scholar] [CrossRef]
- Thieme, H.; Mehrholz, J.; Pohl, M.; Behrens, J.; Dohle, C. Mirror therapy for improving motor function after stroke. Cochrane Database Syst. Rev. 2012, 2012, CD008449. [Google Scholar] [CrossRef] [PubMed]
- Gygax, M.J.; Schneider, P.; Newman, C.J. Mirror therapy in children with hemiplegia: a pilot study. 2011, 53, 473–476. [CrossRef]
- Oliva-Sierra, M.; Ríos-León, M.; Abuín-Porras, V.; Martín-Casas, P. Effectiveness of mirror therapy and action observation therapy in infantile cerebral palsy: a systematic review. An. del Sist. Sanit. de Navar. 2022, 45. [Google Scholar] [CrossRef] [PubMed]
- Narimani, A.; Kalantari, M.; Dalvand, H.; Tabatabaee, S.M. Effect of Mirror Therapy on Dexterity and Hand Grasp in Children Aged 9-14 Years with Hemiplegic Cerebral Palsy. 2019, 13, 135–142.
- Carrión, R.P.; Escobar, J.C.Z.; Guerra, M.C.; Martínez, P.B.; Cepa, C.B.M. Terapia en espejo y de observación de la acción en niños con parálisis cerebral espástica unilateral: estudio de viabilidad. 2022, 75, 325–332. [CrossRef]
- Farzamfar, P.; Heirani, A.; Sedighi, M. The Effect of Motor Training in Mirror Therapy on Gross Motor Skills of the Affected Hand in Children With Hemiplegia. Iran. Rehabilitation J. 2017, 15, 243–248. [Google Scholar] [CrossRef]
- Kara, O.K.; Yardimci, B.N.; Sahin, S.; Orhan, C.; Livanelioglu, A.; Soylu, A.R. Combined Effects of Mirror Therapy and Exercises on the Upper Extremities in Children with Unilateral Cerebral Palsy: A Randomized Controlled Trial. Dev. Neurorehabilit. 2019, 23, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Bruchez, R.; Gygax, M.J.; Roches, S.; Fluss, J.; Jacquier, D.; Ballabeni, P.; Grunt, S.; Newman, C.J. Mirror therapy in children with hemiparesis: a randomized observer-blinded trial. Dev. Med. Child Neurol. 2016, 58, 970–978. [Google Scholar] [CrossRef] [PubMed]
- Auld, M.L.; Johnston, L.M.; Russo, R.N.; Moseley, G.L. A Single Session of Mirror-based Tactile and Motor Training Improves Tactile Dysfunction in Children with Unilateral Cerebral Palsy: A Replicated Randomized Controlled Case Series. Physiother. Res. Int. 2016, 22, e1674. [Google Scholar] [CrossRef] [PubMed]
- Smorenburg, A.R.; Ledebt, A.; Deconinck, F.J.; Savelsbergh, G.J. Matching accuracy in hemiparetic cerebral palsy during unimanual and bimanual movements with (mirror) visual feedback. Res. Dev. Disabil. 2012, 33, 2088–2098. [Google Scholar] [CrossRef] [PubMed]
- Auld, M.L.; Johnston, L.M. Perspectives on tactile intervention for children with cerebral palsy: a framework to guide clinical reasoning and future research. Disabil. Rehabilitation 2017, 40, 1849–1854. [Google Scholar] [CrossRef]
- Sakzewski, L.; Ziviani, J.; Boyd, R.N. Efficacy of Upper Limb Therapies for Unilateral Cerebral Palsy: A Meta-analysis. PEDIATRICS 2014, 133, e175–e204. [Google Scholar] [CrossRef]
- Auld, M.L.; Russo, R.; Moseley, G.L.; Johnston, L.M. Determination of interventions for upper extremity tactile impairment in children with cerebral palsy: a systematic review. Dev. Med. Child Neurol. 2014, 56, 815–832. [Google Scholar] [CrossRef]
- Palomo-Carrión, R.; Zuil-Escobar, J.C.; Cabrera-Guerra, M.; Barreda-Martínez, P.; Martínez-Cepa, C.B. Mirror Therapy and Action Observation Therapy to Increase the Affected Upper Limb Functionality in Children with Hemiplegia: A Randomized Controlled Trial Protocol. Int. J. Environ. Res. Public Heal. 2021, 18, 1051. [Google Scholar] [CrossRef] [PubMed]
- Neuro Orthopaedic Institute. NOI Group. 2023; Im Internet. Available online: https://www.noigroup.com/.
- Karolinska Institutet. Children’s Hand-use Experience Questionnaire 2.0. 2011; Im Internet. Available online: https://www.cheq.se/questionnaire.
- Amer, A.; Eliasson, A.; Peny-Dahlstrand, M.; Hermansson, L. Validity and test–retest reliability of Children’s Hand-use Experience Questionnaire in children with unilateral cerebral palsy. Dev. Med. Child Neurol. 2015, 58, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Sköld, A.; Hermansson, L.N.; Krumlinde-Sundholm, L.; Eliasson, A.-C. Development and evidence of validity for the Children’s Hand-use Experience Questionnaire (CHEQ). Dev. Med. Child Neurol. 2011, 53, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Auld, M.L.; Ware, R.S.; Boyd, R.N.; Moseley, G.L.; Johnston, L.M. Reproducibility of Tactile Assessments for Children with Unilateral Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2012, 32, 151–166. [Google Scholar] [CrossRef] [PubMed]
- Auld, M.L.; Boyd, R.N.; Moseley, G.L.; Johnston, L.M. Tactile Assessment in Children with Cerebral Palsy: A Clinimetric Review. Phys. Occup. Ther. Pediatr. 2011, 31, 413–439. [Google Scholar] [CrossRef] [PubMed]
- Bell-Krotoski, J.; Tomancik, E. The repeatability of testing with Semmes-Weinstein monofilaments. J. Hand Surg. 1987, 12, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Dellon, A.L.; Mackinnon, S.E.; Crosby, P.M. Reliability of two-point discrimination measurements. J. Hand Surg. 1987, 12, 693–696. [Google Scholar] [CrossRef] [PubMed]
- Varni JW, MAPI. PedsQL TM Módulo de Parálisis Cerebral. Versión 3.0 - Spanish (Spain).
- Varni, J.W.; Burwinkle, T.M.; Berrin, S.J.; A Sherman, S.; Artavia, K.; Malcarne, V.L.; Chambers, H.G. The PedsQL in pediatric cerebral palsy: reliability, validity, and sensitivity of the Generic Core Scales and Cerebral Palsy Module. Dev. Med. Child Neurol. 2006, 48, 442–449. [Google Scholar] [CrossRef]
- Beckers, L.; van der Burg, J.; Janssen-Potten, Y.; Rameckers, E.; Aarts, P.; Smeets, R. Process evaluation of two home-based bimanual training programs in children with unilateral cerebral palsy (the COAD-study): protocol for a mixed methods study. BMC Pediatr. 2018, 18, 1–10. [Google Scholar] [CrossRef]
- Palomo-Carrión, R.; Romay-Barrero, H.; Lirio-Romero, C.; Arroyo-Fernádez, R.; M-Guijarro-Herraiz, M.; Ferri-Morales, A. Feasibility of family-directed home-based bimanual intensive therapy combined with modified constraint induced movement therapy (h-BITmCI) in very low and low bimanual functional level: A brief report. Dev. Neurorehabilit. 2022, 26, 63–70. [Google Scholar] [CrossRef]
- Beani, E.; Menici, V.; Ferrari, A.; Cioni, G.; Sgandurra, G. Feasibility of a Home-Based Action Observation Training for Children With Unilateral Cerebral Palsy: An Explorative Study. Front. Neurol. 2020, 11, 16. [Google Scholar] [CrossRef] [PubMed]
- Almasri, N.A.; An, M.; Palisano, R.J. Parents’ Perception of Receiving Family-Centered Care for Their Children with Physical Disabilities: A Meta-Analysis. Phys. Occup. Ther. Pediatr. 2017, 38, 427–443. [Google Scholar] [CrossRef] [PubMed]
- Beckers, L.; Rameckers, E.; Aarts, P.; van der Burg, J.; Smeets, R.; Schnackers, M.; Steenbergen, B.; de Groot, I.; Geurts, A.; Janssen-Potten, Y. Effect of Home-based Bimanual Training in Children with Unilateral Cerebral Palsy (The COAD-study): A Case Series. Dev. Neurorehabilit. 2021, 24, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Schnackers, M.; Beckers, L.; Janssen-Potten, Y.; Aarts, P.; Rameckers, E.; van der Burg, J.; de Groot, I.; Smeets, R.; Geurts, S.; et al.; COAD Focus Group Home-based bimanual training based on motor learning principles in children with unilateral cerebral palsy and their parents (the COAD-study): rationale and protocols. BMC Pediatr. 2018, 18, 1–9. [Google Scholar] [CrossRef]
- Ben-Pazi, H.; Beni-Adani, L.; Lamdan, R. Accelerating Telemedicine for Cerebral Palsy During the COVID-19 Pandemic and Beyond. Front. Neurol. 2020, 11, 746. [Google Scholar] [CrossRef]
- Pérez-Ardanaz, B.; Morales-Asencio, J.M.; León-Campos, A.; Kaknani-Uttumchandani, S.; López-Leiva, I.; Garcia-Piñero, J.M.; Martí-García, C.; García-Mayor, S. Quality of Life and Health Services Utilization for Spanish Children With Cerebral Palsy. J. Pediatr. Nurs. 2020, 53, e121–e128. [Google Scholar] [CrossRef]
- Azar, E.S.; Ravanbakhsh, M.; Torabipour, A.; Amiri, E.; Haghighyzade, M. Home-based versus center-based care in children with cerebral palsy: a cost-effectiveness analysis. 2015, 8, 245–251.
- Majnemer, A.; Shikako-Thomas, K.; Lach, L.; Shevell, M.; Law, M.; Schmitz, N.; Poulin, C. ; QUALA Group Rehabilitation service utilization in children and youth with cerebral palsy. Child: Care, Heal. Dev. 2013, 40, 275–282. [Google Scholar] [CrossRef]
Figure 1.
Mirror Therapy exercises. (a) Forearm pronosupination; (b) Sponge squeezing; (c) Finger-by-finger modeling clay pressing; (d) Clockwise and anti-clockwise wrist spins.
Figure 1.
Mirror Therapy exercises. (a) Forearm pronosupination; (b) Sponge squeezing; (c) Finger-by-finger modeling clay pressing; (d) Clockwise and anti-clockwise wrist spins.
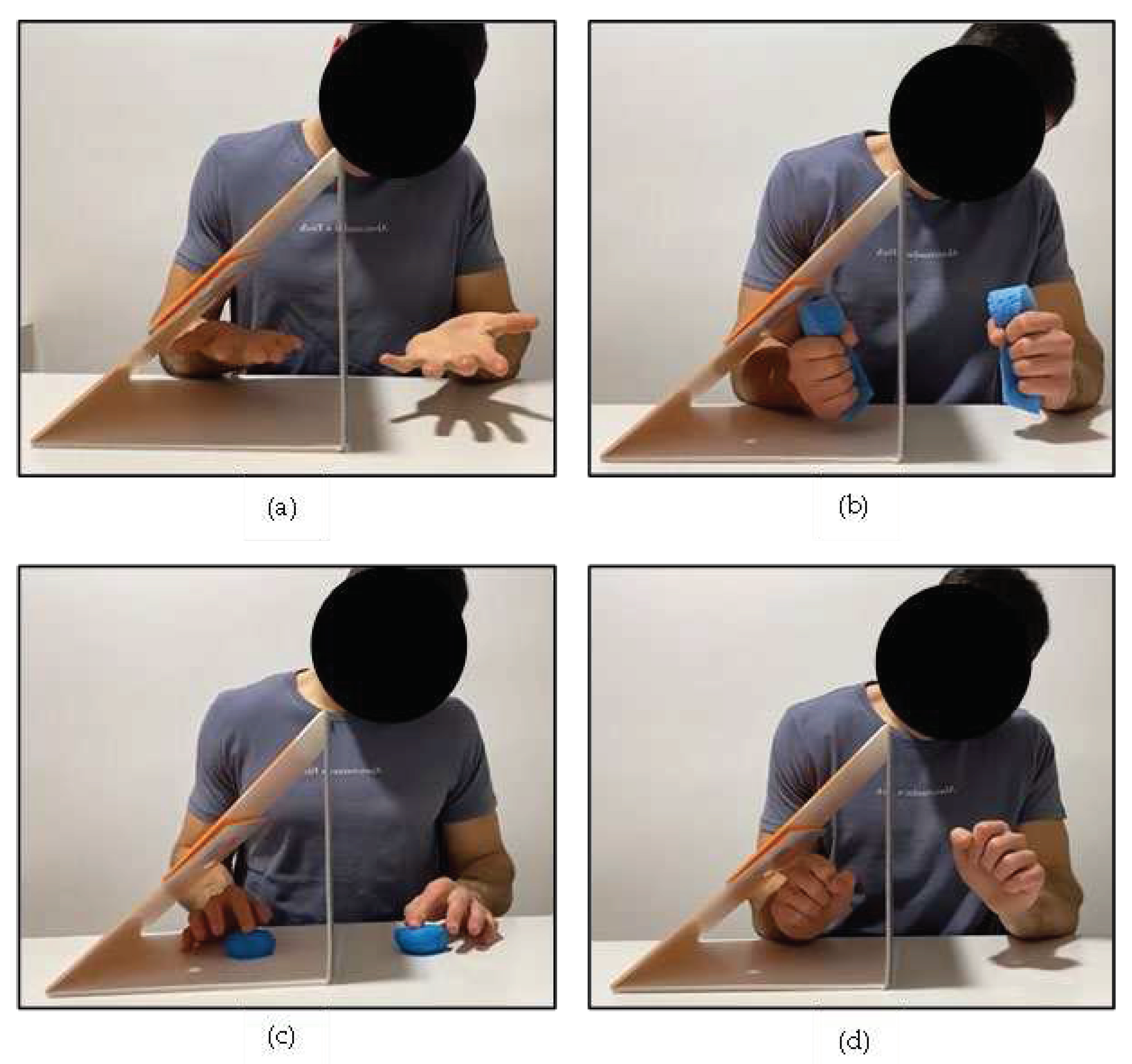

Table 1.
Characteristics of the MT group.
| Participants’ Characteristics | MT Group (n = 6) | |
|---|---|---|
| n | % | |
| Sex | ||
| Male | 2 | 33.3 |
| Female | 4 | 66.7 |
| MACS1 level | ||
| I | 3 | 50.0 |
| II | 3 | 50.0 |
| Affected side | ||
| Left | 1 | 16.7 |
| Right | 5 | 83.3 |
1 MACS: Manual Ability Classification System.
Table 2.
Compliance and total dosage of MT.
| Participant | Total minutes of MT |
|---|---|
| 1 | 600.0 |
| 2 | 651.0 |
| 3 | 717.0 |
| 4 | 720.0 |
| 5 | 603.3 |
| 6 | 600.0 |
Table 3.
Weekly perceived difficulty.
| Data (n = 5) | Forearm Pronosupination | Sponge Squeezing | Finger-by-Finger Pressing | Wrist Spins |
|---|---|---|---|---|
| Week 1 | 3.17 (2.51) | 2.91 (1.44) | 4.41 (2.49) | 4.51 (1.81) |
| Week 2 | 2.38 (2.23) | 3.19 (2.24) | 4.46 (2.57) | 4.32 (1.62) |
| Week 3 | 2.55 (2.32) | 2.56 (2.38) | 3.66 (2.59) | 3.80 (1.41) |
| Week 4 | 2.37 (2.15) | 2.82 (1.91) | 3.23 (2.04) | 4.07 (1.71) |
| Week 5 | 2.60 (2.71) | 2.68 (1.90) | 2.94 (2.04) | 3.91 (1.98) |
| Differences between week 1 and week 5 (p value) | 0.345 | 0.715 | 0.225 | 0.068 |
Table 4.
Completed evaluations.
| Evaluations | Participants | ||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | ||
| E01 | CHEQ 2.0 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| SF4 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| C-PedsQL5 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| P-PedsQL6 | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | |
| E12 | CHEQ 2.0 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| SF4 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| C-PedsQL5 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| P-PedsQL6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| E23 | CHEQ 2.0 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| SF4 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| C-PedsQL5 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| P-PedsQL6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
1 E0: Baseline evaluation; 2 E1: End of the intervention evaluation;3 E2: One-month follow-up evaluation;4 SF: Somatosensory Function; 5 C-PedsQL: Children’s Report of PedsQL; 6 P-PedsQL: Parent’s Report of PedsQL.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



