
Submitted:
11 May 2023
Posted:
12 May 2023
You are already at the latest version
Abstract
Peripapillary intrachoroidal cavitation (PICC) is a yellow-orange lesion, located at the outer border of the myopic conus. First described as a localized detachment of the retinal pigment epithelium, its intrachoroidal location was later disclosed, justifying its current name. PICC is related to other myopic complications like posterior staphyloma, but its pathogenesis is not clear to date. Although it has been considered a benign condition, most eyes with PICC show visual field defects, leading to diagnostic uncertainty as these deficits resemble those observed in glaucoma. Furthermore, eyes with PICC can develop macular detachment with retinoschisis. Finally, misdiagnosis of PICC as a metastatic choroidal tumor may lead to unnecessary and anxiety-provoking investigation. Advances in optical coherence tomography (OCT) imaging have improved the visualization of ocular structures, contributing to the understanding of PICC. Recently high optic nerve sheaths traction forces during eye movements in highly myopic eyes have been suggested as promoters of PICC, renewing interest around this condition. However, a review of PICC is still lacking. Therefore, we aimed to provide a concise yet comprehensive overview of the current state of the art, focusing on OCT documentation, pathophysiology and potential future perspectives based on biomechanics of the optic nerve.
Keywords:
Myopia
; peripapillary intrachoroidal cavitation
; Peripapillary staphyloma
; gamma peripapillary atrophy
; border tissue
; optic nerve sheaths
; biomechanics
1. Introduction
The current epidemic of myopia will probably be followed by that of high myopia and its complications of which peripapillary intrachoroidal cavitation (PICC).
PICC is a well-circumscribed yellow-orange lobular lesion, located at the outer border of the myopic conus [1] (Figure 1A). Advances in optical coherence tomography (OCT) have outlined that PICC is a hyporeflective intrachoroidal thickening [2] below the preserved plane of the Bruch’s membrane [3] (Figure 1C). It appears as a neural-based triangular choroidal thickening in OCT sections crossing the optic nerve (ON) head [3,4] (Figure 1D).
A discontinuity of the choroidal border tissue is often associated with PICC [3] (Figure 1E and 1F).
Visual field defects (VF) are reported in up to 73.3% of PICCs [5]. These VF deficits are similar to those observed in glaucoma [5], constituting a cause of diagnostic uncertainty. Additionally, macular detachment with or without retinoschisis can complicate the prognosis of PICC [6,7,8,9,10,11]. Knowledge of the PICC allows to avoid misdiagnosis as a metastatic choroidal tumor which can lead to unnecessary and anxiety-provoking investigations [1].
PICC is related to other myopic complications namely posterior staphyloma and myopic tilted disc [4]. It is more common in eyes with higher maculopathy category [12].
While the pathogenesis of PICC has been hypothesized for years, recent findings in biomechanics of the ON have reopened the debate. Indeed, several methods have demonstrated high traction forces exerted by the ON sheaths on the peripapillary region of myopic eyes during eye movements [13,14,15]. These biomechanics findings renew interest in the pathogenesis of peripapillary changes in myopic eyes because these tensile forces have been suggested as promoters of PICC [16]. In this context, we performed a thorough review of PICC with an emphasis on pathophysiology with OCT documentation and potential future perspectives.
2. Epidemiology
PICC is found in 5-17% of highly myopic eyes [4,17]. Variability in study populations and study designs interferes with the prevalence range of the PICC [4,17,18].
Shimada et al. first identified the PICC in the fundus and then performed OCT imaging [17]. However, more recent studies revealed that only 46.7% to 53% of PICCs documented on OCT are detected on the fundus [4,19,20]. In addition, they looked for PICCs in the area below the disc and would have missed restricted PICCs in other peripapillary portions [17]. These two aspects may explain the low prevalence of PICC in this series [17].
Some studies set the minimum age for inclusion at 50 years [4] while others also recruited younger subjects [17,21,22]. Knowing that the prevalence of PICC takes off around the age of 30 [17,19], the inclusion of subjects aged at least 50 years [4] focuses on those most likely to have a PICC, thus explaining the higher prevalence of PICC in these cases.
In their study, Choudhury et al. the prevalence of PICC was 2.2% in the overall myopic group and 22% highly myopic eyes [18].
The average age at diagnosis of PICC is around 50 years [1,2,3,5,17,21,22,23,24], ranging between 19 and 79 years [19,25]. Shimada et al. showed that the prevalence of PICC takes off at age 30 and is maintained over 70 years [17].
There is no gender predilection [1,17,22] and PICC can be unilateral (53% subjects in one series) or bilateral [1,3,19,22,23].
PICC is more common in highly myopic eyes. The reported range for AL is 25 to 32 mm [1,20] and that for refractive error is -6 D to -23 D [1,21]. However, PICC is also found in non-highly myopic eyes and even in non-myopic eyes [19,21,22]. Patients with PICC and low myopia or non-myopia were significantly older than those with high myopia, highlighting the combined role of structural weakening and time [19].
The lesion is mainly located below the ON [1,2,3,5,12,17,19,21,22,24]. However, other peripapillary areas may also be involved [4,10,12,17,22,24], and the PICC may even surround the entire ON head [17,19]. Therefore, Shimada subdivided it into three grades based to its overall circumference around the papilla [17].
3. Clinical investigations and diagnosis of PICC
3.1. Fundoscopy and OCT
The yellow orange ophthalmoscopic appearance of PICC [1,3,4,17,19] (Figure 1A) is obvious only in 46.7% to 53% of OCT-detected PICCs [4,19,20]. Therefore, OCT is the recommended tool for the screening of PICC.
By using spectral domain OCT or swept source OCT, the diagnostic features of PICC are currently well established as mentioned above [2,3,21,22,27], thus obviating the need to use other more invasive modalities such as fluorescein or indocyanine green angiography whose characteristics are summarized below.
3.2. Fluorescein angiography
The sequence of fluorescein angiography shows early hypo-fluorescence followed by late hyper-fluorescence without dye pooling in the area of PICC [1,2,17,22,23,28,29]. This angiographic sequence may be explained by structural choroidal changes. The early phase (hypo-fluorescence) results from disorganization, thinning, and loss of normal choroidal architecture while the late phase (hyper-fluorescence) without dye pooling is related to the scleral impregnation by the dye, visible through the disorganized choroid [29].
3.3. Indocyanine green angiography
3.4. OCT-Angiography
Analysis of highly myopic eyes showed that the vessel density of the radial peripapillary capillary network [30,31] (Figure 2B) and that of the ON head layers [30] were significantly reduced in eyes with than in those without PICC. Highly myopic and low myopic eyes also showed a reduced vessel density in comparison to non-myopic eyes [30].
In a study of 47 glaucomatous eyes with PICC, Kim et al., using En-face OCT images at the choroidal layer, describe two main vascular features. First, a well demarcated homogeneous area of vessel density reduction matching the location of PICC [24] (Figure 2C). Second, in 89.4% of cases, a choroidal microvasculature dropout (i.e., a focal sector with no visible choroidal and choriocapillaris network). These similar patterns were previously reported in two case-reports of non-glaucomatous PICC [32,33]. Using B scans of the OCT-A, Kim et al. showed that in the peripapillary area, the cavity inside the PICC maintains the choriocapillary signal against the posterior surface of the Bruch’s membrane whereas it shows no signal in the intrachoroidal cavity [24] (Figure 3B2 and D2).
3.5. Other modalities
4. Association of PICC with other Myopia-related changes
Although the pathophysiologic mechanisms that underpin its OCT features remain to be understood, PICC is linked to several myopic changes. It is consistently located at the outer margin of the myopic conus [1,2,3,5,17]. It is correlated with myopic tilted disc and posterior staphyloma [4]. All cases of Freund’s series exhibited fundus complications of severe myopia [1].
4.1. Gamma peripapillary atrophy
PICC is always found at the outer margin of the conus [1,2,3,5,17,21]. Recent studies have shown that this region also called γ-peripapillary atrophy (γPPA) is acquired [37,38], and results from stresses applied locally during myopic elongation of the eye [13,15,38]. It extends from the opening of the scleral canal to the edge of Bruch’s membrane. The disappearance of Bruch’s membrane in this area is confirmed by histological studies [39] and visible on OCT [40].
4.2. Tilted disc
Dai et al., by intraindividual inter-eye comparison of patients having unilateral PICC, showed that the eye with PICC was more spindle-like because of a pronounced tilt [20].
4.3. Posterior staphyloma
Posterior staphyloma is reported in 40.2% to 100% of PICC [19,42]. This discrepancy in prevalence may result from the study design and the diagnostic tools used [21,43]. Recently, OCT has shown its sensitivity to detect inconspicuous cases while also revealing the outermost border in case of very wide types of posterior staphylomas. It is therefore recommended for diagnosing posterior staphyloma [43,44].
4.4. Others
5. Structural changes in the vicinity of the PICC
5.1. Peripapillary atrophy
As mentioned above, each individual PICC is located at the outer margin of γPPA. The area of γPPA exhibits a posterior deformation of the sclera. Recent studies have suggested that the stress exerted in the peripapillary region during adduction may promote the emergence of γPPA. This stress is more marked at the location of γPPA [45].
5.2. Choroid
Intrachoroidal hyporeflective cysts and hyporeflective hollows, disclosed by OCT, witness that in addition to choroidal thickening, PICC exhibits other structural changes inside the choroid [3,19,21,22,27]. These hyporeflective intrachoroidal cysts (Figure 4B) were found in 19% to 39% of eyes with PICC [19,22]. Wei et al. described them as choroidal splitting or schisis adjacent to pocket-like spaces [22], while Yeh et al. reported intrachoroidal schisis characterized by intracavitary cleavage bands and fluidlike images [19].
Additionnaly, areas adjacent to intrachoroidal cysts show abnormal patterns of choroidal vessel [3]. Changes in the choroidal vascular signal are discussed in the OCT-A section above.
Considering the intrachoroidal hyper-reflective line located in front of the hypo-reflective space and separating this space from what seems to be the residual initial choroid, Spaide et al. suggested that PICC is a suprachoroidal detachment [3]. This hypothesis is supported by a more recent study in which a suprachoroidal detachment was identified exclusively in cases of PICC [16].
Finally, Ehongo et al. studied the configuration of the posterior curvature of the choroid from the peripapillary polar regions to the opening of Bruch’s membrane using OCT. They highlighted a peculiar sequence of choroidal deformity associated with PICC, suggesting the role of mechanical forces in its pathogenesis. Especially, they described the presence of a posterior wedge deformity of the choroidal wall on the γPPA side implying the existence of cross-forces at the level of the polar peripapillary regions [16].
5.3. Posterior scleral curvature
The sclera is deformed backwards in the PICC [3,17,21]. Spaide et al. have suggested that the choroidal thickening presented by PICC results from a posterior excursion of the sclera while the profile of the pigment epithelium remains preserved [3].
A defect in the deep scleral layer allowing the exit of the inferior temporal vein into the extrascleral space has been reported in a case in addition to an unusual anatomy of the parapapillary region [46].
5.4. Border tissue of the choroid
The border tissue is a fibro-astrocytic differentiation separating the nerve fibers from the surrounding structures in the neural canal: the choroid and the sclera. It extends from the sclera at the level of lamina cribrosa to the Bruch’s membrane [47,48,49]. It is divided in two parts: the border tissue of choroid (Elschnig) at the level of choroid and the border tissue of sclera (Jacoby) lining the sclera [47]. As the myopic conus extends during the myopic lengthening of the eye, the border tissue of choroid stretches [39]. A discontinuity in this structure has been disclosed using OCT [1,3,17,19,21,22,23] (Figure 1E-1F).
This discontinuity was first described as a cleft in the junction between the conus and the edge of the PICC in several studies since Freund’s paper [1,3,17,19,21,22,23] (Figure 4C). Its prevalence varies from 10% to 46.2% [1,22]. Through this full thickness defect that allows communication between the PICC and vitreous cavity, nerve fibers (Figure 3B1 and Figure 4C) and retinal vessels (Figure 4E) have been shown to herniate into the PICC [1,3,17,25].
Discontinuity of the border tissue of the choroid would be caused by mechanical stresses exceeding its resistance and leading to its rupture. Several mechanisms have been mentioned; Toranzo et al. discuss stress resulting from the posterior progression of peripapillary staphyloma [2]. Spaide et al. mention the stress related to the posterior deformation of the sclera within the thinned and fragile structures of the myopic conus [3]. Dai et al. suggest mechanical forces caused by papillary tilting [20]. Ehongo et al. discuss the mechanical stress induced by the traction of the ON meninges during adduction [16].
5.5. Vessels
There is often a marked bending of the inferotemporal retinal vein (Figure 4E) into the steep excavation exhibited by the PICC at its junction with the conus [3,17,19,23]. This vessel sometimes disappears on part of its course in some PICCs with deep and steep excavations [3,17,19].
OCT-A features of PICC have been discussed above (section clinical investigation): a reduced vessel density in En-face OCT-A at the choroidal level [24,32,33]. A reduction in the density of vessel of radial peripapillary capillary plexus is also present [30] as well as that of the ON head layer [30]. Finally, the intrachoroidal cavity shows no vessel signal in the B scans of OCT-A [24] (Figure 3).
An increase in visibility of peripapillary intrascleral vessels probably related to their dilation and scleral thinning has recently been disclosed in the vicinity of PICC [48]. Further studies are warranted to clarify this finding.
6. Clinical relevance of the PICC
Although the PICC has been considered a benign entity, it nevertheless deserves special attention. A recent series showed it to be more common in the eyes of higher categories of myopic maculopathy [12]. Additionally, visual field defects [5,23] and macular lesions (retinoschisis, macular detachment) can complicate the presence of a PICC [6,7,8,9,10,11].
6.1. Visual field defects and PICC
The main clinical significance of PICC is visual field defects which are reported [5,17,19,21,22,23,36,51] with a prevalence ranging from 37.5% to 73.3 % [5,22]. They mimic glaucomatous visual field defects, hence the concern about them [5,17].
A correlation has been found between the distribution of visual field defects and the location of the PICC in some cases [5,23,36]. It has thus been suggested that full-thickness defects, thinning, or disruption of nerve fibers at the PICC-conus junction may account for some of these visual field defects [23].
Recently, Okuma et al. showed a correlation between the location of PICC and that of the reduced thickness of macular ganglion cell complex in 66.7% of cases, using OCT [5]. They also showed a correlation between the distribution of visual field defects and PICC locations in 53.3% of cases, concluding that visual field defects in PICC are similar to those in early glaucoma [5].
As a correlation between the location of the PICC and the distribution of visual field defects is not found in all cases, this suggests that some of the visual field defects found in eyes with PICC could result from myopic distortions. Supporting this hypothesis, Shimada et al. found visual field defects in 23% of myopic eyes without PICC in their series [17].
6.2. Macular abnormalities and PICC
From the first descriptions of PICC, a direct communication between the PICC and vitreous cavity at the junction between the conus and PICC has been reported [1,3,17] (Figure 6). Then it was revealed that macular retinoschisis and macular detachment can complicate the presence of a PICC [6,7,8,9,10,11,12,53].
The pathophysiological mechanisms underlying macular detachment complicating a PICC involve two communications with the PICC cavity [6,7,8,10]. First a connection to the vitreous through the full-thickness defect at the junction between the PICC and the conus, allowing vitreous fluid to access to the PICC cavity. Then a second connection between the subretinal or intraretinal space and the PICC cavity (Figure 6). A narrow path connecting the PICC to the schisis has been documented in some cases [6,7,8]. It is suggested that this channel results from a rupture in the atrophic and dysplastic herniated retinal tissue, allowing vitreous fluid to track subretinally [6,7]. Vitreous traction [11] or peripapillary epiretinal membrane [8] have been implicated in some cases.
7. Differential diagnosis – Natural history of uncomplicated cases of PICC
Nowadays, the diagnosis of PICC using the new versions of OCT (spectral domain-OCT and swept source-OCT) is well defined [3], thus allowing to avoid unnecessary and more invasive and anxiety-provoking investigations.
Additionally, for physicians unaware of the condition, the sequence of fluorescein angiography helps differentiate PICC from other potentially confounding entities namely pigment epithelial detachment, peripapillary choroidal neovascularization, metastatic lesion or central serous chorioretinopathy [2,17].
Uncomplicated cases of PICC are asymptomatic [1,17] and have a good prognostic. However, other vision-threatening myopic complications may accompany PICC as mentioned above [1,22].
The aforementioned visual field defects which are correlated with PICC [17] are clinically challenging because they are of the glaucomatous type.
In general, the PICC is stable. However, Freund et al. showed in their series a case of involution of the PICC in both eyes of the same patient over a follow-up of 15 years [1]. In these eyes, the PICC became smaller as γPPA widened towards it.
A case reported by Toranzo et al. showed enlargement over 10 years [2]. Forte et al., using En-face OCT, observed PICC enlargement in one of six eyes in their series over an 18-month period [23].
Lee et al. reported an enlargement of the PICC over one year, followed by its shrinkage over another one-year period [52].
Formally, the condition being acquired and related to myopic complications, it is not surprising that it shows changes, albeit slow, over time, as the myopia progresses.
8. Pathogenetic hypotheses of PICC
So far, the pathogenesis of PICC is not established. Congenital, fluidic and mechanical hypotheses have been proposed. Similarities between PICC and the morphologic features at the border of the optic disc coloboma have been discussed [54]. All these pathogenetic hypotheses have weaknesses or shortcomings and are summarized below.
8.1. Congenital hypothesis
Some authors have suggested that PICC could be an incomplete form of choroidal coloboma because it is mainly located in the inferior peripapillary region [1].
However, PICCs can extend widely around the papilla and some PICCs are restricted to the upper part of the disc which does not support this hypothesis [17]. Moreover, PICC is noticed around the age of 30 [17], suggesting that it is an acquired condition. Finally, its correlation with myopic tilted disc, γPPA and posterior staphyloma [4] suggests that it is another myopia-related condition.
8.2. Fluidic considerations
Since the lesion is more frequent below the ON, Freund et al. hypothesized that there may be gravitational displacement of subretinal fluid from the area of the ON [1]. This fluid would come either from the vitreous or from the optic canal [1].
Yeh et al. finding that subjects with non-myopic eyes and PICC are significantly older than those with myopic eyes and PICC, suggested that with aging, the transitional weakened tissue of the conus presents impaired resorption of fluids from the subretinal space, subarachnoid space, optic canal or vitreous cavity. The progressive and asymptomatic gravitation of these fluids promotes the formation of fluid pockets at the lower edge of the conus, hence the appearance of PICC [19].
However, this gravitational hypothesis does not explain why some PICCs are confined to the upper peripapillary part [4,17,22].
Many authors have suggested that the vitreous fluid enters the PICC through the retinal defect located at the PICC-conus transition zone [17,22,23]. Supporting this hypothesis, Spaide et al. observed that PICCs with the opening against the vitreous showed more prominent posterior bowing [3], while those without this opening showed a triangular thickening of the choroid with a neural.
8.3. Mechanical considerations
Wei et al. suggested that a complex of forces combining “posterior expansion force, vitreous tractional force and vitreous fluid dynamics determine the size and shape of the PICC” [22]. However, vitreous traction has never been demonstrated in any uncomplicated case of PICC [3].
Lee et al. reported a case of PICC in a non-glaucomatous myopic eye accompanied by a large adjacent disc haemorrhage. A schisis in the prelaminar ON tissue was also noticed. At the one-year follow-up visit, the schisis and PICC had widened while the disc haemorrhage was still observed. The disc haemorrhage disappeared at 2-year follow-up, the PICC showed shrinkage while the intraneural cyst was reduced. These changes suggest the presence of peripapillary mechanical forces [52].
Dai et al. showed by intraindividual inter-eye comparison that the eye with PICC was more tilted and more rotated, also suggesting the role of mechanical factors [20].
8.3.1. PICC as a complication of peripapillary staphyloma
Toranzo et al. suggested that the increased gap between Bruch’s membrane and the scleral planes resulting from thickening of the choroid as the posterior staphyloma progresses, stretches the border tissue which eventually ruptures. Secondarily, the choroid retracts from the ON margins, leading to a PICC [2].
Wei et al. added that adhesion of the retina and retinal pigment epithelium to the margin of the conus prevents the rupture from opening into the subretinal space [22].
8.3.2. PICC as a complication of myopic tilted disc and myopic conus
As already mentioned, in the presence of γPPA (myopic conus), the sclera may be bowed posteriorly, giving rise to many suggestions.
Many authors have assumed that the posterior scleral bulge of the conus was favored by its weakening due to the absence of overlying structures [3,21]. From there, the force acting to deform the sclera depends on the author.
Shimada et al. hypothesized that during the process of γPPA extension the conus and the surrounding peripapillary area bow posteriorly. Mechanically, this induces a stretching of the tissues which then causes splitting of the neighboring intrachoroidal structures, with appearance of cysts inside the choroid. Then, the intrachoroidal cysts enlarge, coalesce, and end up in a large hyporeflective intrachoroidal space [21]. But the flaw with this hypothesis is that the phenomenon of coalescence is not instantaneous. Therefore, hyporeflective intrachoroidal cysts, as precursors of PICC should also be found in the eyes of non-PICCs, which is not described in the literature. Further studies of longitudinal design should thus focus on these intrachoroidal cysts to clarify their impact on the pathophysiology of PICC.
Spaide et al. suggested that the driving force which is intraocular pressure against the wall of the eye induces the bulging of the weakened conus [3]. These authors explain that the stress/strain relationship ends with a more scleral deformation of the conus due to the absence or thinning of the tissues covering the sclera in this area. Subsequently, the posterior bowing of the sclera would itself favor the thickening of the neighboring choroid mainly in the inferior border of the ON. Finally, the widening of the choroid at the junction of the ON ends up breaking the border tissue, the latter promoting itself and secondarily the thickening of the choroid by allowing the entry of the vitreous fluid into the PICC [3].
Since the sclera of the conus deforms backwards, Forte et al. [23] hypothesized that the overlying structures are submitted to the same trend. Unable to follow the strong posterior excursion of the sclera, they detach from choroid, thus creating the zone of cavitation inside the choroid and choroidal thickening.
8.3.3. PICC as a complication of the optic nerve sheaths traction
Toranzo et al. hypothesized that in posterior staphyloma, the choroidal border tissue ruptures when stretched by the increasing gab between the plane of the sclera and that of Bruch’s membrane [2]. The driving force that increases the gap between the sclera and the Bruch’s membrane was unknown.
Beside their main hypothesis (intraocular pressure effect), Spaide et al. also opened the door to the possibility that in the tilted disc, unknown forces may be at play to bow the sclera backwards [3].
The question that remained open for years was: why in PICC does the sclera deform posteriorly while the overlying anterior structures remain undeformed?
Recent studies on the biomechanics of the peripapillary region have shown by several methods that the ON sheaths exert strong tensile forces on the ON head and the peripapillary region [13,14,15] during eye movements. From the similarities between the tilted disc and intermittent distortions of the ON and peripapillary structures related to eye movements, some authors have suggested that tilted disc results from remodeling and permanent fixation of these repetitive deformations [15,45,55,56]. Interestingly, a case of a preoperative round disc becoming oval after trabeculectomy has been reported [57]. The eye was highly myopic and had very high preoperative intraocular pressure. It seems that this elevated pressure counteracted the ovality of the disc. Therefore, the surgical reduction of ocular pressure had promoted the return to the oval shape of the disc by altering the balance of forces acting on the ON head, suggesting that the phenomenon of tilted disc can be reversed to some extent. This constitutes an avenue to explore, because PICC and tilted disc are related.
In this regard, very recently, Ehongo et al. confirmed that PICC is a suprachoroidal detachment (Figure 7A). They suggested that it is caused by the traction exerted by the ON sheaths on their scleral insertions [16]. They observed using serial OCT sections that the beginning of the thickening of the choroid and the posterior bowing of the sclera, coincided with the detection of the scleral insertion of the dura mater (Figure 7A-F). The slope of the posterior bowing of the sclera steepened in front of the subarachnoid space, with the choroidal thickening ending in a supra-choroidal detachment (Figure 7A). They thus suggested that the posterior excursion of the sclera results from the direct posterior traction exerted by the ON sheaths on the thinned and weakened myopic sclera (Figure 8). Due to this traction, the scleral flange (the part of the sclera between the margin of the ON and the dura mater) recedes while Bruch’s membrane, due to its structural rigidity maintains its plane. This results in thickening of the choroid [16]. Further studies are warranted to confirm this hypothesis.
Again, relying on serial OCT sections, they observed that the convexity of the posterior choroidal wall is followed at its edge by an anterior elevation suggesting that ON sheaths traction force has two components [16]. The first that acts directly by protruding the sclera backwards. The second tangential component which squeezes the choroid at the edge of the scleral convexity. This choroidal sequence characterizes a peripapillary staphyloma (Figure 8). They therefore suggest that peripapillary staphyloma and γPPA, result from repetitive traction of the ON sheaths on the peripapillary sclera during eye movements [16].
9. Conclusion and perspectives
The current epidemic of myopia is paving the way to that of high myopia and its complications, in particular posterior staphyloma, the presence of which classifies an eye in the group of pathological myopia.
Peripapillary staphyloma and tilted disc are related to PICC. They have all been suggested to be promoted by the traction of the dura on its scleral attachment during eye movement. The link between these three complications of high myopia must be investigated. Biomechanical and longitudinal studies are thus warranted to clarify mechanisms leading to them.
Tractions of the ON sheath on the peripapillary region are exerted on all the eyes. On elongated myopic eyes, for obvious geometric reasons, these traction forces are more marked, promoting the occurrence of peripapillary myopic complications. However, these complications also occur, although less frequently in non-highly myopic eyes. Unknowns therefore remain as to whether the eyes undergoing these changes are more sensitive to ON sheaths traction force or whether this traction force is stronger in the eyes presenting these entities.
In particular, the influence of time and age justifies additional investigations since subjects with PICC and non-high myopia were found to be older than those with PICC and high myopia.
Visual field defects in PICC pose diagnostic difficulties with glaucoma (the prevalence of which is also increasing). Understanding the pathogenesis underpinning the occurrence of PICC and other peripapillary myopic complications will allow the development of strategies to slow or reverse their onset and associated visual field defects.
A synopsis of publications on PICC is presented in the Appendix A.
Author Contributions
Conceptualization, AE; Methodology AE and NB; analysis, AE. writing—original draft preparation, AE and NB. writing—review and editing, AE and NB; Visualization, AE, Supervision, AE. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
A synopsis of publications on PICC.
|
Year Author [Ref] |
Objective- Material-Methods | Relevant results for PICC | Pathogenetic clues | Strength |
| 2003 Freund [1] |
Objective: To describe a newly recognized fundus lesion in HM Design: retrospective study, Case-series (20 eyes of 15 patients included) Examinations: fundus pictures and OCT (and FA) |
Location: the inferior border of the myopic conus Associations: TD (75%), Myopic conus (100%), PS (90%), Fundus myopic changes (100%) Connection with vitreous at PICC-conus junction in 10% of PICC Stable in the follow-up period (1-15 years) except for one patient with bilateral reduction of PICC. |
Distinct complication of high myopia. Located at the inferior border of the myopic conus. Hypothesis: incomplete form of coloboma or gravitational accumulation of subretinal fluid coming from the optic disc/vitreous. |
First description of PICC and recognition as a distinct fundus anomaly in highly myopic eye Description of a PICC-Vitreous communication in 10% cases. |
| 2005 Toranzo [2] |
Objective: To refine the PICC features Design: Observational case report Examinations: OCT- FA - ICG |
The intrachoroidal location of PICC is revealed (with a preserved RPE plane and no detachment of the RPE) The size of PICC increased during the 10 years follow-up. |
Mechanical hypothesis: progression of posterior staphyloma would stretch and break the BT, resulting in an intrachoroidal cavitation. | Intrachoroidal site of PICC revealed by OCT. Proposition of the current name (PICC) The RPE/BM plane and anterior structures is preserved |
| 2006 Shimada [17] |
Objective: To study the prevalence and clinical characteristics of PICC Analysis of VF in cases of PICC Design: Prospective design (632 eyes with HM included) Comparison between PICC and a control group of HM. Examinations: OCT, FA, ICG and VF |
Prevalence:4.9% of PICC in HM (on fundus examination) Location: inferior part in all cases Full thickness defect at the conus-PICC junction in 10% of PICC Marked posterior bowing of the sclera where PICC lies in 83.9% of cases. Association: TD: 93.5%. Myopic conus: 100%. PS: 64.3%. VFD: 71% FA sequence: early hypofluorescence and late hyperfluorescence without dye pooling |
The hypothesis of an incomplete form of coloboma unlikely: Lesion not confined to the inferior sector but can extent around the entire ON. No PICC in young patients: lesion probably acquired. Hypothesis: VFD could be caused by tissular distortion (TD and excavation of the myopic conus) and not by the PICC itself (could explain why the main location of PICC and VF defects don’t always match). |
VFD in 71% of PICC, no consistent correlation with PICC location VFD significantly more frequent in PICC group than in control group. Communication with vitreous cavity in 10%. Marked bending of the infero-temporal vein in 83.9% of PICC. No PICC in subjects under 30 years old. Large series (632 eyes). |
| 2007 Shimada [21] |
Objective: To study peripapillary changes in eyes with HM using OCT. Design: Observational case-series (127 eyes with HM included) Control group with low myopic and emmetropic eyes Examinations: Fundus images, VF, OCT |
Prevalence of PICC in HM on fundus examination: 9.4%. None in controls (emmetropic or low myopia) Prevalence of PICC in HM using OCT: 11%. PICC features on OCT: intrachoroidal hypo-reflective space showing multiple cystic spaces. Retinal full thickness defects: in 7% of PICC. VFD in 64.3% of PICC and in 19.5% of HM without PICC. |
Posterior excavation of conus related to PICC location. Hypothesis: Mechanical stress at peripapillary tissues associated with posterior excavation of the myopic conus could split the intrachoroidal structures and produce cystoid spaces leading to the PICC by coalescence. Description of retinal full thickness defects leading to PICC-vitreous communication |
Glaucoma-like VFD in cases of PICC, and significantly more frequent than in the control group. OCT recommended for PICC diagnosis. |
| 2008 Forte [23] |
Objective: Evaluation of the thickness and lateral extent of PICC using En-face OCT. Design: prospective case-series: 6 eyes/3 patients. Examinations: En-face OCT, FA, ICG, VF |
Retinal full thickness defect in 2/6 eyes, allowing a PICC-vitreous communication. VFD in 4/4 eyes with anormal central fixation. VFD matching the PICC location in 3 of the 4 cases. |
Hypothesis: steep excavation of the myopic conus stretches the retina/RPE complex, causing a splitting of the choroid and a hypo-reflective intrachoroidal space Gravitational accumulation of fluid from the vitreous cavity through a cleft at the border of the PICC could be an additional factor |
VFD in 4/4 eyes (Humphrey) The VFD matched the PICC location in 3 of the 4 cases. |
| 2009 Wei [22] |
Objective: Evaluation of OCT features and clinical aspects of PICC Design: Observational case series (16 PICC diagnosed on fundus) Examinations: OCT, fundus, FA |
Associations: Myopic conus: 100% Vitreous connection at the PICC-conus junction: 46.2% Intrachoroidal cystic spaces: 19% of PICC (intrachoroidal splitting/schisis without optical empty cavity) Inferior location in 94% of cases HM in all cases of PICC except one (moderate myopia) |
Hypothesis: Vitreous fluid would gain access to the suprachoroidal space through the path caused by the breaking of the BT Fluid accumulation induces a choroidal schisis and splitting of the choroidal structures. BT discontinuity is caused by the PS progression |
PICC and choroidal schisis would be different stages of the same pathologic spectrum. PICC are also in other locations than the inferior border of the optic nerve. History of glaucoma in 37.5% of cases |
| 2009 Shimada [6] |
Objective: To report a case of a macular retinal detachment related to a PICC. Design: case report Examinations: OCT, fundus, FA |
Retinal detachment in a highly myopic eye with PICC. No dye leakage on FA. A PICC-vitreous connection at the PICC-vitreous junction and a PICC- retinal detachment connection through subretinal space at the conus area |
Hypothesis: A retinal detachment can complicate a PICC through a subretinal connection with the full retinal thickness defect located at the PICC-conus margin. | PICC can be complicated by retinal detachment. |
| 2011 Freund [27] |
Objective: To study the PICC characteristics using OCT-EDI. Design: Case series Examinations: fundus, OCT-EDI. |
On OCT-EDI, PICC is characterized by thickening of the choroid with or without hypo-reflective “cavitation”. | PICC shows a choroidal thickening with variable hypo-reflectivity. | PICC has several facets of presentation |
| 2012 Spaide [3] |
Objective: To provide a pathogenic hypothesis based on anatomical characteristics of PICC Design: Case-series, 16 PICC included Examinations: fundus images, FA, ICG, SS-OCT and OCT-EDI. |
Associations: TD: 100%, myopic conus: 100%. Vitreous communication: 25% of cases (associated with more prominent cavitation). Posterior scleral bowing with normal retina-RPE plane in all PICCs. dipping of infero-temporal vein into PICC at the conus edge |
Hypothesis: the posterior displacement of the sclera would be the primary cause of PICC. Rupture of BT by excessive stretching might lead to more prominent PICC. |
PICC would start at suprachoroidal space. The radial section of PICC is triangular in the absence of a full thickness defect and shows a more pronounced and rounded protrusion in its presence. |
| 2012 Akimoto [53] |
Objective: To report of a self-limited recurrent macular detachment associated with PICC Design: case report |
Description of a PICC in a low myopic eye (-1D) associated with a retinoschisis and a macular detachment. | A connection between PICC and retinoschisis may promote retinal detachment | Macular detachment in PICC may occur in non-highly myopic eyes. |
| 2013 Yeh [19] |
Objective: Evaluation of the clinical features of peripapillary area associated with PICC Design: Retrospective observational case-series (inclusion of 122 PICC diagnosed on OCT, no control group) Examinations: OCT, VF, Fundus pictures |
Only 46.7% of PICC diagnosed on OCT are detected on fundus examination. Associations: PS: 40.2%, PPA: 98.4%, TD: 69.7%, VFD: 37.7% Maculopathy :14% Non-highly myopic patients with PICC are older (p<0.05) Only 3 PICC in patients younger than 30 Fragmented aspect of the choroidal cavitation seen in 39% Connection with vitreous cavity detected in 16% of PICC (26.4% in case of marked excavation of the myopic conus) Inferotemporal vein bent at the PICC border in 43.4% |
Hypothesis: possible impact of age in the pathogenesis of PICC (due to age-related reduced resorption of fluids). By gravitational effect, fluids would accumulate and form fluid pocket at the inferior border of the myopic conus This could lead to the onset of PICC | Less than 50% of PICC diagnosed on OCT are detected on the fundus examination. The presence of marked excavation of the myopic conus increases the incidence of PICC communication with the vitreous cavity. Implication of age in the pathogenesis of PICC. |
| 2013 You [4] |
Objective: Determine the prevalence, size, location of PICC and their associations Design: Population-based study, (3468 patients included) Examinations: OCT-EDI, fundus pictures |
PICC prevalence: 16.9% in HM (No PICC found in non-highly myopic eyes). Only 53% of PICC diagnosed on OCT were seen on fundus. Associations with TD and PS Location predominantly the inferior area No association with other ocular or systemic parameters |
Hypothesis: Distortions of the posterior fundus associated with PS and TD could be the primary cause of PICC in highly myopic eyes HM is not the primary cause of PICC (no association between PICC and AL on multivariate analysis) |
Only 50% of PICCs are detected on fundus examination. Only TD and PS were associated with PICC. No association with other ocular or systemic parameters. |
| 2013 Ohno [42] |
Objective: Evaluation of ICC located temporal to the optic disc in highly myopic eyes Design: retrospective design, 125 highly myopic eyes included Examinations: SS-OCT, FA |
Prevalence of temporal ICC in highly myopic eyes: 12.8% Temporal ICC are larger than inferior ones Associations: myopic conus (100%), PS (100%) FA and OCT results are similar than those of PICC. Defects of the border tissue detected in some temporal ICC |
ICC can develop in temporal area only, without involving the inferior peripapillary area. Hypothesis: The separation of the temporal ICC develops at the suprachoroidal level (the entire thickness of the choroid remains attached to the RPE) |
Consistent association between temporal ICC and both PS and myopic conus Temporal ICC is a suprachoroidal lesion |
| 2014 Holak [54] |
Comments on the Yeh et al (2013) article | Similarities exist between morphologic features at the border of optic disc coloboma and PICC | They suggest exploring genetic, environmental, congenital impacts on the pathogenesis of PICC. Hypothesis: cystoid spaces found in coloboma or PICC could be different stages of the same spectrum disease |
Mutations in cell adhesion molecules like cadherin could promote coloboma and PICC formation? |
| 2014 Yoshizawa [8] |
Objective: To report a case of retinoschisis with macular detachment in a PICC treated by vitrectomy and outcome Design: case report Examinations: OCT Intervention: Vitrectomy |
Retinoschisis with macular detachment. A connection between PICC and the schisis cavity was disclosed. Epiretinal membrane was adjacent to the PICC-conus connection. Complete regression of retinoschisis and closure of the PICC-retinoschisis channel |
The connection PICC-retinoschisis was suggested to be promoted by the traction on the PICC | Good outcome of macular detachment associated by PICC when treated by vitrectomy. |
| 2014 Rajagopal [7] |
Objective: To report a case of macular detachment in a PICC Design: retrospective, case report Examinations: OCT, FA |
A PICC-vitreous connection at the PICC-vitreous junction and a PICC- retinal detachment connection through subretinal space at the conus area | / | Confirm that a connection between PICC and subretinal space may promote a macular detachment |
| 2014 Dai [46] |
Objective: To describe the course of the inferotemporal vein into peripapillary region and to evaluate the characteristics of beta and gamma PPA Design: case report Examinations: fundus pictures and OCT |
Description of a case combining PICC, PPA and TD The infero-temporal vein disappeared in the Peripapillary area next to ON. On OCT, the detection of a scleral lamellar defect suggests an intrascleral or extra-scleral pathway of this vein |
/ | Description of the abnormal course of the infero-temporal vein in an eye with PICC and PPA and TD |
| 2015 Chen [9] |
Objective: To investigate clinical characteristics and treatment outcomes of macular detachment associated with PICC. Design: retrospective case-series Examinations: |
Depending on the case, a connection between the subretinal space and PICC or peripapillary area was found. Variable results with gas tamponade, topical carbonic inhibitors |
/ | / |
| 2015 Dai [20] |
Objective: Intra-individual comparative study of ON morphology in unilateral PICC. Design: Hospital-based observational Examinations: OCT-EDI, fundus pictures |
Intra-individual comparison: eyes with PICC have lower ovality index, are more tilted, have a shorter vertical diameter and a shorter minimal diameter of ON compared to the contralateral eye. Only 53% of PICC are detected on fundus examination. |
A shorter ovality index implies a rotation of the optic disc around the vertical or horizontal axis. Hypothesis: PICC is caused by the disruption of BT due to excessive disc tilting |
Optic disc is more tilted in eyes with PICC. 53% of PICC detected on OCT are not seen on fundus |
| 2015 Lee [52] |
Objective: Description of a disc haemorrhage associated with a PICC in the absence of a glaucomatous neuropathy Design: Case report Examinations: OCT-EDI, fundus pictures |
A disc haemorrhage associated with PICC in a non-glaucomatous eye lasted more than a year. It showed a disappearance in conjunction with the reduction in size of the PICC and papillary schisis. | Peripapillary haemorrhages may be a manifestation of peripapillary stress. Hypothesis: Mechanical modifications due to PICC may alter the vessels and cause peripapillary haemorrhages without any glaucoma. |
Impact of mechanical damage to peripapillary structures associated with PICC enlargement. |
| 2015 Azar [29] |
Objective: Multimodal imaging of PICC Design: Case report Examinations: SD-OCT, En-face OCT, ICG, FA, VF |
En-face OCT combined with FA show an early hypo fluorescence resulting from the absence of choroidal tissue and a late staining resulting from the scleral impregnation. | / | Early hypo-fluorescence due to choroidal alteration. Late hyper-fluorescence due to scleral impregnation |
| 2015 Ando [10] |
Objective: To report features of a macular detachment associated with PICC and the outcomes of vitrectomy. Design: Retrospective, case-series (3eyes). Examinations: Chart review. OCT. |
All 3 eyes were non highly myopic. No vitreous detachment observed in any case. Definite vitreous-PICC connection in 2 cases. Definite subretinal space-PICC connection in 2 cases. Vitrectomy resolved the macular detachment in all cases. |
/ | Macular detachment can complicate PICC even in non-highly myopic eyes. |
| 2016 Jonas [56] |
Objective: Comment (on Wang’s biomechanical study) | / | Suggestion that the stress exerted by the ON on its head during adduction movement could be part of the pathogenesis of the PICC | Impact of ON biomechanics in the pathogenesis of PICC |
| 2016 Okuma [5] |
Objective: Evaluation of the VF and the macular ganglion cell complex in PICC and evaluation of the similarities between these results and those typical of glaucomatous changes Design: retrospective, 16 eyes affected by PICC included Examinations: OCT, VF |
VF defects were detected in 73.3% of PICC. Good correlation between PICC location and VF defects distribution in 53.3% of cases. Thinning of ganglion cell complex was correlated with PICC location in 66.7%. |
/ | VF defects observed in 75% of PICC. PICC-VF defects correlation present in half of the with a PICC. Ganglion cell complex and VF defects found in PICC are very similar to those observed in early glaucoma. |
| 2016 Kita [25] |
Objective: Study of a PICC associated with a full thickness retinal defect in the papillo-macular bundle Design: Case report Examinations: SS-OCT, VF |
No visual field defect detected in the full-thickness defect located at the papillo-macular. Retina herniated in PICC may preserve some function despite the apparent retinal defect. |
/ | / |
| 2017 Mazzaferro [33] |
Objective: Evaluation of the characteristics of PICC on OCT-A Design: Case report Examinations: OCT-A |
Absence of choroidal and choriocapillary network in the choroidal cavitation PICC associated with a PS and a TD |
/ | Absence of any intra-choroidal vascular tissue in this case of PICC |
| 2017 Chen [30] |
Objective: To study the peripapillary, ONH vasculature by OCT-A in highly myopic eyes with PICC Design: Hospital-based cross-sectional study Examinations: OCT-A |
Highly myopic eyes show a lower peripapillary capillary vessel density than non-highly myopic eyes. The peripapillary vascular density is more reduced in PICC than non-PICC eyes (especially in temporal area) |
/ | The peripapillary vascular density is more reduced in PICC than non-PICC eyes (especially in temporal area) |
| 2018 Chen [34] |
Objective: Multimodal imaging of PICC associated with myopic sinkhole Design: Case report Examinations: fundus image, OCT-EDI US, VF |
Description of a PICC associated with an inferotemporal sinkhole in the myopic conus. Presence of a cleft between the ICC and the vitreous cavity |
Hypothesis: myopic sinkhole could favour the flow of vitreous fluid through the suprachoroidal space and facilitate the formation of a PICC | Possible role of the myopic sinkhole in the physiopathology of PICC |
| 2018 Choudhury [18] |
Objective: Estimation of the prevalence of myopic degeneration in Chinese Americans Design: Population-based cross-sectional Study |
1523 myopic Chinese included (<-0.5D) Prevalence of ICC: 2.2% overall myopic eyes and in the 22% of HM eyes. |
/ | Population-based study (Chinese Americans) |
| 2019 Venkatesh [50] |
Objective: To study the prevalence and clinical characteristics of PICC Design: Case-series. Retrospective, non-interventional, comparative study Examinations: fundus photography, OCT |
Prevalence of ICC in highly myopic eyes: 55.8% (15.8% of PICC and 84.2% of macular ICC) |
/ | There is not a clear separation between two concepts in this study: PPA and patchy chorioretinal atrophy. |
| 2019 Parlak [32] |
Objective: Description of a case of PICC Design: Case report Examinations: Fundus photography, autofluorescence, OCT, OCT-A |
Reduction of the vessel density at the level of the PICC with OCT-A | / | PICC is characterised by a hypo signal on OCT-A |
| 2020 Markan [26] |
Objective: to describe a case of an acquired PICC secondary to intercalary membrane detachment Design: Case report |
Description of an irido-fundal coloboma with intercalary membrane detachment associated with a ICC at the edge of a coloboma. | Hypothesis of a new pathogenic mechanism of ICC formation: the intercalary membrane detachment allows fluid from the sub-ICM communicating with the choroid space | ICC secondary acquired in a case of irido-fundal coloboma |
| 2020 Comune [31] |
Objective: To analyse the vessel density of radial peripapillary capillary in HM with (32eyes) and without (23 eyes) PICC Design: Prospective. Examinations: OCT-A |
Myopic eyes with PICC had a significantly lower vessel density than eyes without PICC, especially those with choroidal neovascularization. | / | Radial peripapillary capillary vessel density is significantly influenced (reduced) by the presence of PICC. |
| 2021 Kim [24] |
Objective: To study the choroidal microvasculature in glaucomatous eyes with PICC Design: Retrospective Examinations: SD-OCT, OCT-A, SS-OCT, Fundus examination, VF |
PICC showed larger hypovascular area on En-face OCT-A 89.4% of PICC had choroidal microvascular dropout (focal sectoral capillary dropout with no visible microvascular network on deep-layers En-face images) in the area proximal to the PICC. Concordance between location of PICC and area of dropout 98% of PICC had hemifield VF defects corelating PICC hemispheric location |
Hypothesis: common pathogenesis of PICC and microvascular dropout due to their close spatial proximity Distortions of peripapillary tissues (due to tensile stress) induce both PICC and damage of RNFL and micro-vessels leading to microvascular dropout |
98% VFD corresponding to the PICC hemispheric location. Probable common pathogenic mechanisms of PICC and microvascular dropout in glaucoma OCT-A characteristics of PICC |
| 2021 Liu [12] |
Objective: Characterisation of PICC in Chinese highly myopic eyes and its associated risk factors Design: Observational cross-sectional study, 890 patients with HM included Examinations: fundus photography, OCT |
Prevalence of PICC in high myopia 3.6% (diagnosis based on the presence of typical lesion on both the fundus and the OCT) Location mainly inferior (87.5%), multiple (9.4%), superior (3.1%) Association with age, axial length and myopic spherical equivalent (based on the multiple linear logistic regression model) |
Hypothesis: Impact of mechanical forces. Axial elongation during myopia progression stretches the posterior tissues leading to the appearance and progression of PICC. The lack of overlying tissues and relative thinness of the myopic conus leads to more pronounced deformation and is thus more susceptible to mechanical stress. |
Prevalence of PICC in a large highly myopic population with a wide range of age (7-70 years old) PICC more frequent in eyes with severe myopic maculopathy and eyes with PS |
| 2022 Fujimoto [36] |
Objective: To evaluate 3D parameters of PICC using SS-OCT and deep learning and to correlate with VF sensitivity Design: Retrospective Examinations: SS-OCT, deep learning |
The correlation between 3D volume of PICC and VF sensitivity | / | The 3D rendering has a potential to improve detection and pathological understanding of PICC |
| 2022 Ehongo [16] |
Objective: To compare the peripapillary polar regions in eyes with gamma PPA and PPS in the presence or absence of PICC Design: Observational cross-sectional study, Examinations: fundus pictures, serial SD-OCT |
PICC is a suprachoroidal detachment. PICC is aligned with the subarachnoid space. PICC is detected up on the visualisation of the ON sheaths. |
Hypothesis: The pulling of ON sheaths on the scleral flange during eye movements would promote PICC. | Confirmation that PICC is as suprachoroidal detachment. Suggestion that it is promoted by tractions of the ON sheaths during eye movement. |
| 2022 Aoki [11] |
Objective: To report a case of macular lamellar hole with retinoschisis in a PICC eye that underwent vitrectomy with gas tamponade Design: Case report Examinations: OCT Intervention: Vitrectomy |
Non-highly myopic eye. Anatomical recovery after vitrectomy with gas tamponade Visual acuity improvement. But a full thickness defect at the PICC-conus junction appeared after vitrectomy. |
/ | Retinoschisis with lamellar macular hole may complicate a PICC even in non-highly myopic eyes. |
| BM: Bruch membrane. BT: border tissue. ICG: indocyanine green angiography. FA: fluorescein angiography. HM: high myopia. OCT: Optical coherence tomography. SD-OCT: spectral-domain OCT. SS-OCT: swept-source OCT. OCT-A: OCT angiography. ON: optic nerve. OHN: optic nerve head. PICC: peripapillary intra-choroidal cavitation. PPA: peripapillary atrophy, PS: posterior staphyloma, RNFL: retinal nerve fibre layer. RPE: retinal pigment epithelium. TD: tilted disc. VF: visual field. VFD: visual field defects. | ||||
References
- Freund KB, Ciardella AP, Yannuzzi LA, Pece A, Goldbaum M, Kokame GT, Orlock D. Peripapillary detachment in pathologic myopia. Arch Ophthalmol. 2003 Feb;121(2):197-204. PMID: 12583785. [CrossRef]
- Toranzo J, Cohen SY, Erginay A, Gaudric A. Peripapillary intrachoroidal cavitation in myopia. Am J Ophthalmol. 2005 Oct;140(4):731-2. PMID: 16226529. [CrossRef]
- Spaide RF, Akiba M, Ohno-Matsui K. Evaluation of peripapillary intrachoroidal cavitation with swept source and enhanced depth imaging optical coherence tomography. Retina. 2012 Jun;32(6):1037-44. PMID: 22466483. [CrossRef]
- You QS, Peng XY, Chen CX, Xu L, Jonas JB. Peripapillary intrachoroidal cavitations. The Beijing eye study. PLoS One. 2013 Oct 24;8(10):e78743. PMID: 24302981; PMCID: PMC3840228. [CrossRef]
- Okuma S, Mizoue S, Ohashi Y. Visual field defects and changes in macular retinal ganglion cell complex thickness in eyes with intrachoroidal cavitation are similar to those in early glaucoma. Clin Ophthalmol. 2016 Jun 29;10:1217-22. PMID: 27418805; PMCID: PMC4935007. [CrossRef]
- Shimada N, Ohno-Matsui K, Iwanaga Y, Tokoro T, Mochizuki M. Macular retinal detachment associated with peripapillary detachment in pathologic myopia. Int Ophthalmol. 2009 Apr;29(2):99-102. Epub 2007 Nov 22. PMID: 18034213. [CrossRef]
- Rajagopal J, H CK 5th, Ganesh S. Macular detachment associated with peripapillary detachment in pathologic myopia. Retin Cases Brief Rep. 2014 Spring;8(2):103-6. PMID: 25372320. [CrossRef]
- Yoshizawa C, Saito W, Noda K, Ishida S. Pars plana vitrectomy for macular schisis associated with peripapillary intrachoroidal cavitation. Ophthalmic Surg Lasers Imaging Retina. 2014 Jul-Aug;45(4):350-3. Epub 2014 Jun 30. PMID: 24972183. [CrossRef]
- Chen TC, Yang CH, Sun JP, Chen MS, Yang CM. Macular retinal detachment associated with intrachoroidal cavitation in myopic patients. Graefes Arch Clin Exp Ophthalmol. 2015 Sep;253(9):1437-46. Epub 2014 Nov 4. PMID: 25367830. [CrossRef]
- Ando Y, Inoue M, Ohno-Matsui K, Kusumi Y, Iida T, Hirakata A. Macular detachment associated with Intrachoroidal Cavitation in nonpathological myopic eyes. Retina. 2015 Oct;35(10):1943-50. PMID: 26035397. [CrossRef]
- Aoki S, Imaizumi H. Vitrectomy for macular retinoschisis associated with peripapillary intrachoroidal cavitations in a moderately myopic eye. Int J Retina Vitreous. 2022 Sep 5;8(1):62. PMID: 36064619; PMCID: PMC9446725. [CrossRef]
- Liu R, Li Z, Xiao O, Zhang J, Guo X, Loong Lee JT, Wang D, Lee P, Jong M, Sankaridurg P, He M.Characteristics of peripapillary intrachoroidal cavitation in highly myopic eyes: The Zhongshan Ophthalmic Center-Brien Holden Vision Institute High Myopia Cohort Study. Retina. 2021 May 1;41(5):1057-1062. PMID: 32833786. [CrossRef]
- Wang X, Rumpel H, Lim WE, Baskaran M, Perera SA, Nongpiur ME, Aung T, Milea D, Girard MJ. Finite Element Analysis Predicts Large Optic Nerve Head Strains During Horizontal Eye Movements. Invest Ophthalmol Vis Sci. 2016 May 1;57(6):2452-62. PMID: 27149695. [CrossRef]
- Demer JL. Optic Nerve Sheath as a Novel Mechanical Load on the Globe in Ocular Duction. Invest Ophthalmol Vis Sci. 2016 Apr;57(4):1826-38. PMID: 27082297; PMCID: PMC4849549. [CrossRef]
- Chang MY, Shin A, Park J et al. Deformation of Optic Nerve Head and Peripapillary Tissues by Horizontal Duction. Am J Ophthalmol. 2017 Feb; 174:85-94. Epub 2016 Oct 15. PMID: 27751810; PMCID: PMC5812679. [CrossRef]
- Ehongo A, Bacq N, Kisma N, Dugauquier A, Alaoui Mhammedi Y, Coppens K, Bremer F, Leroy K. Analysis of Peripapillary Intrachoroidal Cavitation and Myopic Peripapillary Distortions in Polar Regions by Optical Coherence Tomography. Clin Ophthalmol. 2022 Aug 13;16:2617-2629. PMID: 35992567; PMCID: PMC9387167. [CrossRef]
- Shimada N, Ohno-Matsui K, Yoshida T, Yasuzumi K, Kojima A, Kobayashi K, Futagami S, Tokoro T, Mochizuki M. Characteristics of peripapillary detachment in pathologic myopia. Arch Ophthalmol. 2006 Jan;124(1):46-52. PMID: 16401784. [CrossRef]
- Choudhury F, Meuer SM, Klein R, Wang D, Torres M, Jiang X, McKean-Cowdin R, Varma R; Chinese American Eye Study Group. Prevalence and Characteristics of Myopic Degeneration in an Adult Chinese American Population: The Chinese American Eye Study. Am J Ophthalmol. 2018 Mar;187:34-42. Epub 2017 Dec 27. PMID: 29288031; PMCID: PMC5837945. [CrossRef]
- Yeh SI, Chang WC, Wu CH, Lan YW, Hsieh JW, Tsai S, Chen LJ. Characteristics of peripapillary choroidal cavitation detected by optical coherence tomography. Ophthalmology. 2013 Mar;120(3):544-552. Epub 2012 Dec 1. PMID: 23207174. [CrossRef]
- Dai Y, Jonas JB, Ling Z, Wang X, Sun X. Unilateral peripapillary intrachoroidal cavitation and optic disk rotation. Retina. 2015 Apr;35(4):655-9. PMID: 25299968. [CrossRef]
- Shimada N, Ohno-Matsui K, Nishimuta A, Tokoro T, Mochizuki M. Peripapillary changes detected by optical coherence tomography in eyes with high myopia. Ophthalmology. 2007 Nov;114(11):2070-6. Epub 2007 Jun 1. PMID: 17543388. [CrossRef]
- Wei YH, Yang CM, Chen MS, Shih YF, Ho TC. Peripapillary intrachoroidal cavitation in high myopia: reappraisal. Eye (Lond). 2009 Jan;23(1):141-4. Epub 2007 Aug 24. PMID: 17721499. [CrossRef]
- Forte R, Pascotto F, Cennamo G, de Crecchio G. Evaluation of peripapillary detachment in pathologic myopia with en face optical coherence tomography. Eye (Lond). 2008 Jan;22(1):158-61. Epub 2006 Dec 15. PMID: 17173013. [CrossRef]
- Kim J, Kim J, Lee EJ, Kim TW. Parapapillary Intrachoroidal Cavitation in Glaucoma: Association with Choroidal Microvasculature Dropout. Korean J Ophthalmol. 2021 Feb;35(1):44-50. Epub 2020 Dec 11. PMID: 33307621; PMCID: PMC7904409. [CrossRef]
- Kita Y, Inoue M, Hollό G, Kita R, Sano M, Hirakata A. Preserved retinal sensitivity in spatial correspondence to an intrachoroidal cavitation area with full thickness retinal defect: a case report. BMC Ophthalmol. 2016 Oct 26;16(1):186. PMID: 27784274; PMCID: PMC5081664. [CrossRef]
- Markan A, Jain M, Singh R. Secondary intrachoroidal cavitation in a case of iridofundal coloboma. Med Hypotheses. 2020 Oct;143:110085. Epub 2020 Jul 9. PMID: 32721794. [CrossRef]
- Freund KB, Mukkamala SK, Cooney MJ. Peripapillary choroidal thickening and cavitation. Arch Ophthalmol. 2011 Aug;129(8):1096-7. PMID: 21825199. [CrossRef]
- Marticorena-Álvarez P, Clement-Fernández F, Iglesias-Ussel L. Peripapillary intrachoroidal cavitation in pathological myopia. Arch Soc Esp Oftalmol. 2014 Aug;89(8):316-9. English, Spanish. Epub 2013 Aug 3. PMID: 24269422. [CrossRef]
- Azar G, Leze R, Affortit-Demoge A, Faure C. Peripapillary Intrachoroidal Cavitation in Myopia Evaluated with Multimodal Imaging Comprising "En-Face" Technique. Case Rep Ophthalmol Med. 2015;2015:890876. Epub 2015 Oct 12. PMID: 26543655; PMCID: PMC4620261. [CrossRef]
- Chen Q, He J, Hua Y, Fan Y. Exploration of peripapillary vessel density in highly myopic eyes with peripapillary intrachoroidal cavitation and its relationship with ocular parameters using optical coherence tomography angiography. Clin Exp Ophthalmol. 2017 Dec;45(9):884-893. Epub 2017 Jun 15. PMID: 28494517. [CrossRef]
- Comune C, Montorio D, Cennamo G. Optical coherence tomography angiography in myopic peripapillary intrachoroidal cavitation complicated by choroidal neovascularization. Eur J Ophthalmol. 2021 Jul;31(4):1920-1924. Epub 2020 Jul 16. PMID: 32674595. [CrossRef]
- Parlak M, Ipek SC, Saatci AO. Peripapilläre Aufhellung bei hoher Myopie: nur ein Staphyloma posticum? [Peripapillary whitening in high myopia: only a staphyloma posticum?]. Ophthalmologe. 2020 Apr;117(4):379-383. German. PMID: 31511965. [CrossRef]
- Mazzaferro A, Carnevali A, Zucchiatti I, Querques L, Bandello F, Querques G. Optical coherence tomography angiography features of intrachoroidal peripapillary cavitation. Eur J Ophthalmol. 2017 Mar 10;27(2):e32-e34. PMID: 28233894. [CrossRef]
- Chen Y, Ma X, Hua R. Multi-modality imaging findings of huge intrachoroidal cavitation and myopic peripapillary sinkhole. BMC Ophthalmol. 2018 Feb 2;18(1):24. PMID: 29394916; PMCID: PMC5797380. [CrossRef]
- Chawla R, Kumar A, Mandal S. Three-Dimensional Reconstruction Imaging of Peripapillary Intrachoroidal Cavitation in a Myopic Patient. Ophthalmol Retina. 2019 Nov;3(11):928. PMID: 31699309. [CrossRef]
- Fujimoto S, Miki A, Maruyama K, Mei S, Mao Z, Wang Z, Chan K, Nishida K. Three-Dimensional Volume Calculation of Intrachoroidal Cavitation Using Deep-Learning-Based Noise Reduction of Optical Coherence Tomography. Transl Vis Sci Technol. 2022 Jul 8;11(7):1. PMID: 35802370; PMCID: PMC9279919. [CrossRef]
- Kim TW, Kim M, Weinreb RN, Woo SJ, Park KH, Hwang JM. Optic disc change with incipient myopia of childhood. Ophthalmology. 2012 Jan;119(1):21-6.e1-3. Epub 2011 Oct 5. PMID: 21978594. [CrossRef]
- Kim M, Choung HK, Lee KM, Oh S, Kim SH. Longitudinal Changes of Optic Nerve Head and Peripapillary Structure during Childhood Myopia Progression on OCT: Boramae Myopia Cohort Study Report 1. Ophthalmology. 2018 Aug;125(8):1215-1223. Epub 2018 Mar 14. PMID: 29550000. [CrossRef]
- Jonas JB, Jonas SB, Jonas RA, Holbach L, Dai Y, Sun X, Panda-Jonas S. Parapapillary atrophy: histological gamma zone and delta zone. PLoS One. 2012;7(10):e47237. Epub 2012 Oct 18. PMID: 23094040; PMCID: PMC3475708. [CrossRef]
- Dai Y, Jonas JB, Huang H, Wang M, Sun X. Microstructure of parapapillary atrophy: beta zone and gamma zone. Invest Ophthalmol Vis Sci. 2013 Mar 19;54(3):2013-8. PMID: 23462744. [CrossRef]
- Tay E, Seah SK, Chan SP, Lim AT, Chew SJ, Foster PJ, Aung T. Optic disk ovality as an index of tilt and its relationship to myopia and perimetry. Am J Ophthalmol. 2005 Feb;139(2):247-52. PMID: 15733984. [CrossRef]
- Ohno-Matsui K, Shimada N, Akiba M, et al. Characteristics of intrachoroidal cavitation located temporal to optic disc in highly myopic eyes. Eye (Lond) 2013; 27:630–638.
- Shinohara K, Moriyama M, Shimada N, Yoshida T, Ohno-Matsui K. Characteristics of Peripapillary Staphylomas Associated With High Myopia Determined by Swept-Source Optical Coherence Tomography. Am J Ophthalmol. 2016 Sep;169:138-144. Epub 2016 Jun 27. PMID: 27365146. [CrossRef]
- Ohno-Matsui K. Proposed classification of posterior staphylomas based on analyses of eye shape by three-dimensional magnetic resonance imaging and wide-field fundus imaging. Ophthalmology. 2014 Sep;121(9):1798-809. Epub 2014 May 9. PMID: 24813630. [CrossRef]
- Wang X, Fisher LK, Milea D, Jonas JB, Girard MJ. Predictions of Optic Nerve Traction Forces and Peripapillary Tissue Stresses Following Horizontal Eye Movements. Invest Ophthalmol Vis Sci. 2017 Apr 1;58(4):2044-2053. PMID: 28384725. [CrossRef]
- Dai Y, Jonas JB, Ling Z, Sun X. Temporal inferior vein submerging into intrachoroidal cavitation and gamma zone. Retin Cases Brief Rep. 2014 Spring;8(2):110-2. PMID: 25372322. [CrossRef]
- Anderson DR. Ultrastructure of human and monkey lamina cribrosa and optic nerve head. Arch Ophthalmol. 1969 Dec;82(6):800-14. PMID: 4982225. [CrossRef]
- Reis AS, Sharpe GP, Yang H, Nicolela MT, Burgoyne CF, Chauhan BC. Optic disc margin anatomy in patients with glaucoma and normal controls with spectral domain optical coherence tomography. Ophthalmology. 2012 Apr;119(4):738-47. Epub 2012 Jan 4. PMID: 22222150; PMCID: PMC3319857. [CrossRef]
- Sawada Y, Araie M, Shibata H, Ishikawa M, Iwata T, Yoshitomi T. Optic Disc Margin Anatomic Features in Myopic Eyes with Glaucoma with Spectral-Domain OCT. Ophthalmology. 2018 Dec;125(12):1886-1897. Epub 2018 Aug 23. PMID: 30144950. [CrossRef]
- Venkatesh R, Jain K, Aseem A, Kumar S, Yadav NK. Intrachoroidal cavitation in myopic eyes. Int Ophthalmol. 2020 Jan;40(1):31-41. Epub 2019 Jul 12. PMID: 31300972. [CrossRef]
- Belamkar AV, Dolan J, Olatunji S, Bhatti MT, Chen JJ, Mansukhani SA. The 'Fault' Lies in the Choroid: Peripapillary Intrachoroidal Cavitation Presenting with Progressive Vision Loss. Neuroophthalmology. 2022 Jan 25;46(4):254-257. PMID: 35859631; PMCID: PMC9291674. [CrossRef]
- Lee KM, Lee EJ, Lee SH, Kim TW. Disc haemorrhage associated with an enlarged peripapillary intrachoroidal cavitation in a non-glaucomatous myopic eye: a case report. BMC Ophthalmol. 2015 Oct 29;15:145. PMID: 26511202; PMCID: PMC4625871. [CrossRef]
- Akimoto M, Akagi T, Okazaki K, Chihara E. Recurrent macular detachment and retinoschisis associated with intrachoroidal cavitation in a normal eye. Case Rep Ophthalmol. 2012 May;3(2):169-74. Epub 2012 May 16. PMID: 22679435; PMCID: PMC3369248. [CrossRef]
- Holak SA, Holak N, Holak HM. Peripapillary choroidal cavitation. Ophthalmology. 2014 Jan;121(1):e6-e7. Epub 2013 Nov 16. PMID: 24252822. [CrossRef]
- Wang X, Beotra MR, Tun TA, Baskaran M, Perera S, Aung T, Strouthidis NG, Milea D, Girard MJ. In Vivo 3-Dimensional Strain Mapping Confirms Large Optic Nerve Head Deformations Following Horizontal Eye Movements. Invest Ophthalmol Vis Sci. 2016 Oct 1;57(13):5825-5833. PMID: 27802488. [CrossRef]
- Jonas JB, Dai Y, Panda-Jonas S. Peripapillary Suprachoroidal Cavitation, Parapapillary Gamma Zone and Optic Disc Rotation Due to the Biomechanics of the Optic Nerve Dura Mater. Invest Ophthalmol Vis Sci. 2016 Aug 1;57(10):4373. PMID: 27557435. [CrossRef]
- Ehongo A, Dugauquier A, Alaoui Mhammedi Y. General shape of the optic nerve head in one high myopic glaucomatous patient before and after trabeculectomy. Int J Ophthalmol. 2020 Nov 18;13(11):1836-1838. PMID: 33215019; PMCID: PMC7590865. [CrossRef]
Figure 1.
Peripapillary intrachoroidal cavitation (PICC). A-F. PICC = red star. A. Fundus picture. PICC is the yellow-orange lesion at the outer border of the myopic conus (black star). B. Infrared image showing the location of sections C to F. C-F. Red arrow = Bruch’s membrane (BM). PICC is the hypo-reflective space behind the preserved plane of BM. C. Slice along the line c, below the optic nerve head (ONH). D-F. Orange arrow = border tissue of the choroid (BT). D. Section along the arrow d, through the ONH. The BT is continuous between the BM and the sclera (green arrow). E. Section through the ONH, along the arrow e. The BT is discontinuous between the red and orange arrows. F. Along the myopic conus (arrow f). The BT shows a discontinuity between the red and orange arrows.
Figure 1.
Peripapillary intrachoroidal cavitation (PICC). A-F. PICC = red star. A. Fundus picture. PICC is the yellow-orange lesion at the outer border of the myopic conus (black star). B. Infrared image showing the location of sections C to F. C-F. Red arrow = Bruch’s membrane (BM). PICC is the hypo-reflective space behind the preserved plane of BM. C. Slice along the line c, below the optic nerve head (ONH). D-F. Orange arrow = border tissue of the choroid (BT). D. Section along the arrow d, through the ONH. The BT is continuous between the BM and the sclera (green arrow). E. Section through the ONH, along the arrow e. The BT is discontinuous between the red and orange arrows. F. Along the myopic conus (arrow f). The BT shows a discontinuity between the red and orange arrows.
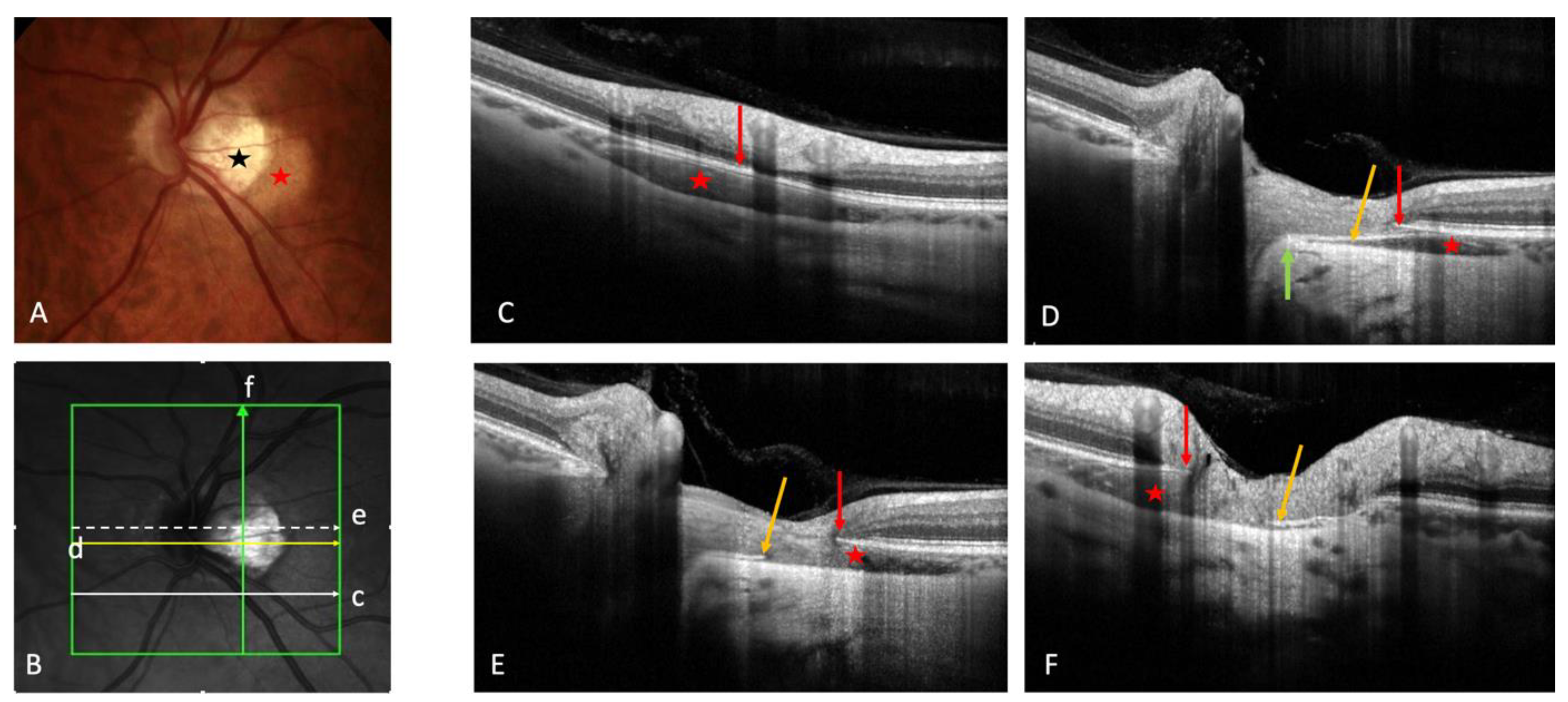
Figure 2.
OCT-angiography of a peripapillary intrachoroidal cavitation (PICC). A-C. Yellow star = PICC. A. Fundus image with a PICC. B. En-face OCT-A at the level of the superficial radial peripapillary capillary. Reduced vascular density at the area of PICC is observed. C. En-face OCT-A at the level of choroid. Reduced vascular density is also seen at the area of PICC. The device used is the PLEX Elite® 9000 SS OCTA (Carl Zeiss Meditec AG, Jena, Germany). 6x6 mm field of view centered on the papilla.
Figure 2.
OCT-angiography of a peripapillary intrachoroidal cavitation (PICC). A-C. Yellow star = PICC. A. Fundus image with a PICC. B. En-face OCT-A at the level of the superficial radial peripapillary capillary. Reduced vascular density at the area of PICC is observed. C. En-face OCT-A at the level of choroid. Reduced vascular density is also seen at the area of PICC. The device used is the PLEX Elite® 9000 SS OCTA (Carl Zeiss Meditec AG, Jena, Germany). 6x6 mm field of view centered on the papilla.
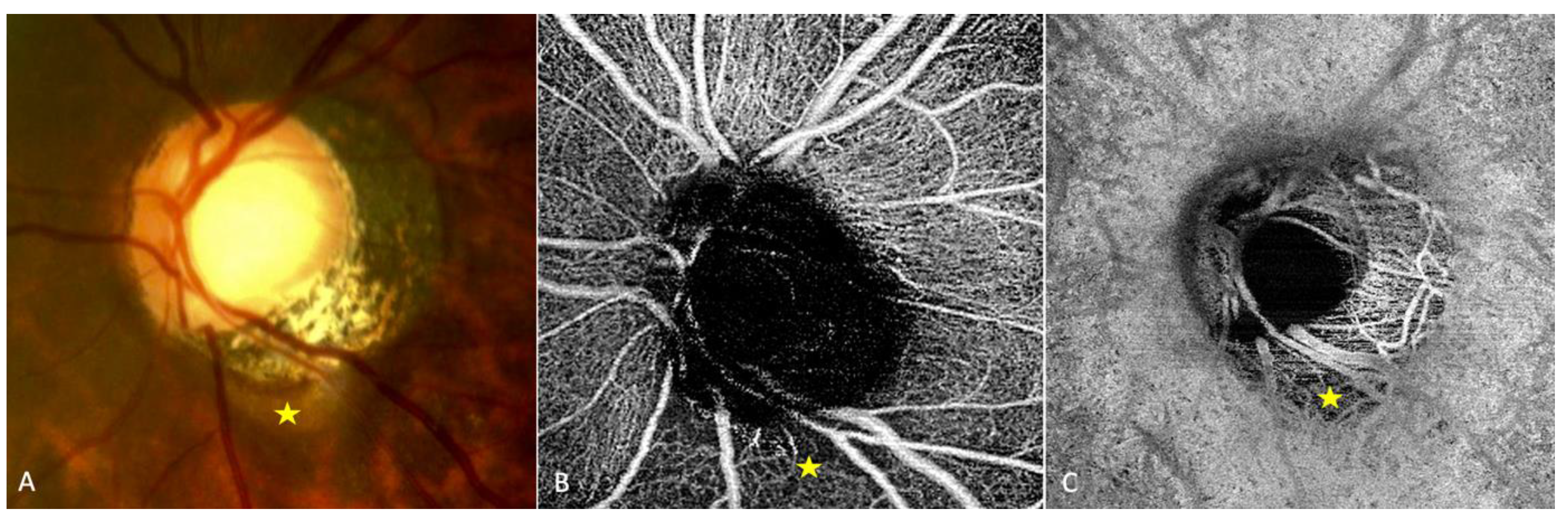
Figure 3.
Optical coherence tomography (OCT) and OCT-angiography (OCT-A) in a case of peripapillary intrachoroidal cavitation (PICC). PICC = yellow star. S = sclera. A. Fundus image with a PICC at the outer border of the conus (red arrow). B1 and B2. Sections along the green arrow in A. B1. OCT B-scan disclosing the PICC. Gamma peripapillary atrophy is between the two ends of the Bruch’s membrane (red lines). The retinal layers (dashed yellow arrow) herniate through them. B2. B-scan OCT-angiography showing the absence of signal inside the choroid. There is a signal (in pink) against Bruch’s membrane, corresponding to the choriocapillaris. Behind the intrachoroidal hyporeflective space, another signal corresponding to the sclera is perceived. The retinal vascular signal is red. C. Infra-red image with the green arrow indicating the location of sections D1 and D2. The section is below the optic disc. D2. No signal is seen in the hyporeflective choroidal space between the sclera and the choriocapillary. A signal is seen at the level of choriocapillary. The device used for OCT-angiography is the Swept source OCT Triton DRI Topcon corporation.
Figure 3.
Optical coherence tomography (OCT) and OCT-angiography (OCT-A) in a case of peripapillary intrachoroidal cavitation (PICC). PICC = yellow star. S = sclera. A. Fundus image with a PICC at the outer border of the conus (red arrow). B1 and B2. Sections along the green arrow in A. B1. OCT B-scan disclosing the PICC. Gamma peripapillary atrophy is between the two ends of the Bruch’s membrane (red lines). The retinal layers (dashed yellow arrow) herniate through them. B2. B-scan OCT-angiography showing the absence of signal inside the choroid. There is a signal (in pink) against Bruch’s membrane, corresponding to the choriocapillaris. Behind the intrachoroidal hyporeflective space, another signal corresponding to the sclera is perceived. The retinal vascular signal is red. C. Infra-red image with the green arrow indicating the location of sections D1 and D2. The section is below the optic disc. D2. No signal is seen in the hyporeflective choroidal space between the sclera and the choriocapillary. A signal is seen at the level of choriocapillary. The device used for OCT-angiography is the Swept source OCT Triton DRI Topcon corporation.
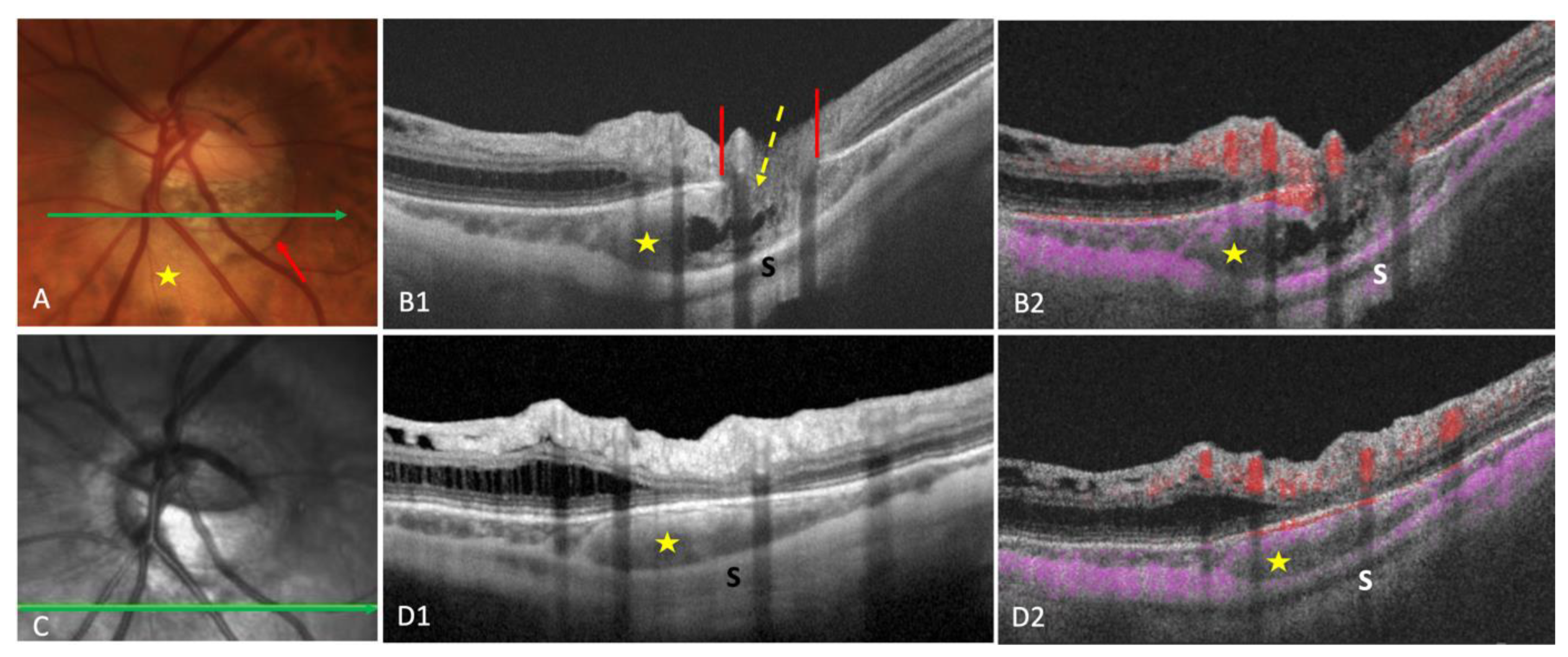
Figure 4.
Structural choroidal findings in peripapillary intrachoroidal cavitation (PICC). ON = optic nerve. Red star = PICC. A. Fundus picture showing the yellow-orange aspect of PICC at the outer border of the myopic conus (yellow star). ON = optic nerve. B. Section along the green arrow in the corresponding infra-red image. Intrachoroidal schisis (blue dots) are within the PICC cavity. C. Section along the green arrow in the corresponding infra-red image, through the full thickness defect. This defect allows communication between the PICC and vitreous cavity. Nerve fibers (yellow arrow) herniate into the PICC cavity. D. Fundus picture of the eye presented on OCT section E. The PICC is not apparent. E. Section along the green arrow in the corresponding infra-red image. The yellow arrow shows the bending of the temporal vessel in the PICC.
Figure 4.
Structural choroidal findings in peripapillary intrachoroidal cavitation (PICC). ON = optic nerve. Red star = PICC. A. Fundus picture showing the yellow-orange aspect of PICC at the outer border of the myopic conus (yellow star). ON = optic nerve. B. Section along the green arrow in the corresponding infra-red image. Intrachoroidal schisis (blue dots) are within the PICC cavity. C. Section along the green arrow in the corresponding infra-red image, through the full thickness defect. This defect allows communication between the PICC and vitreous cavity. Nerve fibers (yellow arrow) herniate into the PICC cavity. D. Fundus picture of the eye presented on OCT section E. The PICC is not apparent. E. Section along the green arrow in the corresponding infra-red image. The yellow arrow shows the bending of the temporal vessel in the PICC.
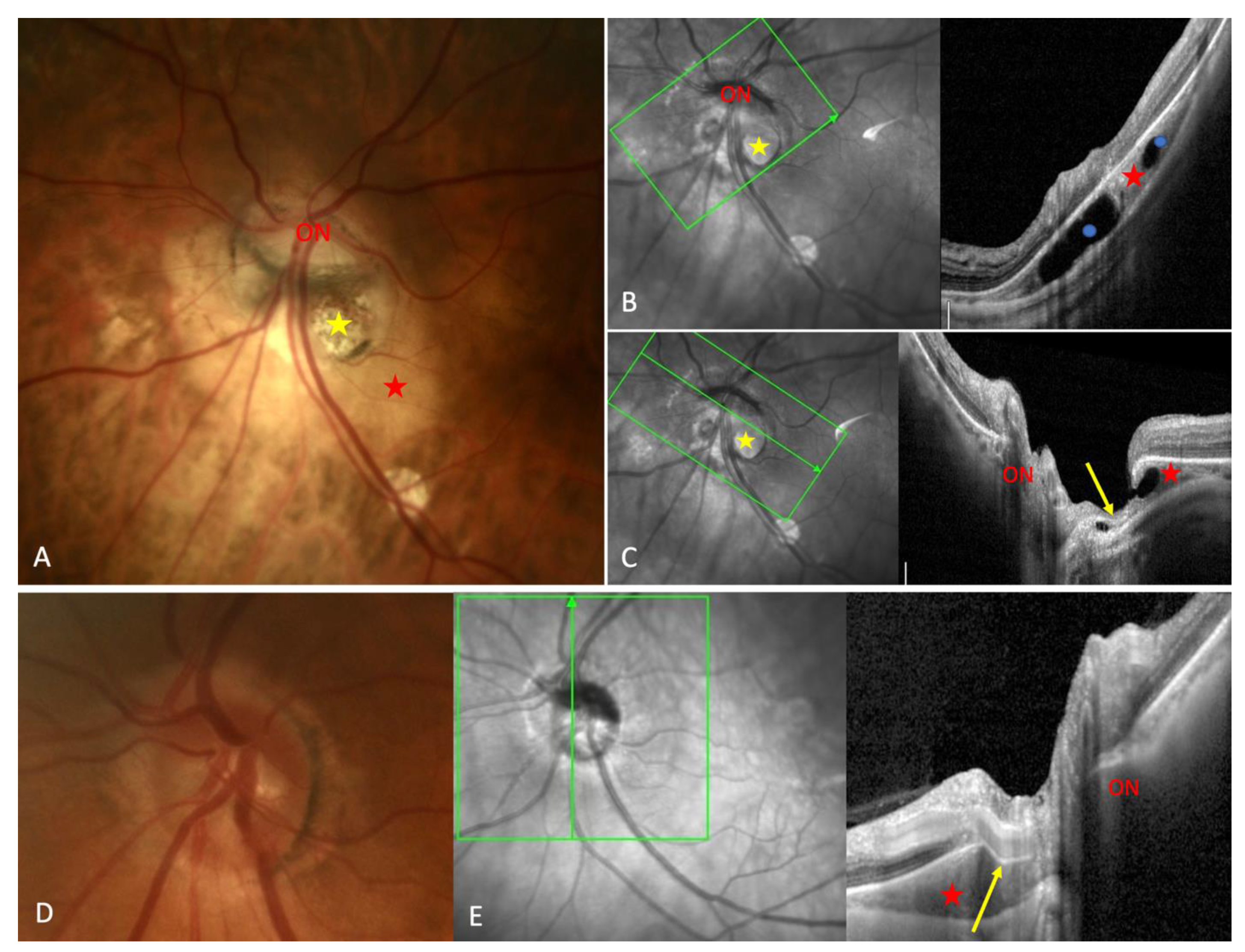
Figure 5.
Discontinuity of the border tissue of choroid in a peripapillary intrachoroidal cavitation (PICC). A-C. Red star = PICC. A. PICC presents is the hypo-reflectivity behind the preserved plane of Bruch’s membrane (red arrow). The border tissue of the choroid (yellow arrow) is the hyper-reflective line between the Bruch’s membrane (red arrow) and the border of the scleral canal (dashed blue arrow). In the opposite side, it is between the red and blue arrows. In both cases, it is intact. B and C. The border tissue of the choroid presents a discontinuity (dashed yellow arrows) on the side with gamma peripapillary atrophy.
Figure 5.
Discontinuity of the border tissue of choroid in a peripapillary intrachoroidal cavitation (PICC). A-C. Red star = PICC. A. PICC presents is the hypo-reflectivity behind the preserved plane of Bruch’s membrane (red arrow). The border tissue of the choroid (yellow arrow) is the hyper-reflective line between the Bruch’s membrane (red arrow) and the border of the scleral canal (dashed blue arrow). In the opposite side, it is between the red and blue arrows. In both cases, it is intact. B and C. The border tissue of the choroid presents a discontinuity (dashed yellow arrows) on the side with gamma peripapillary atrophy.
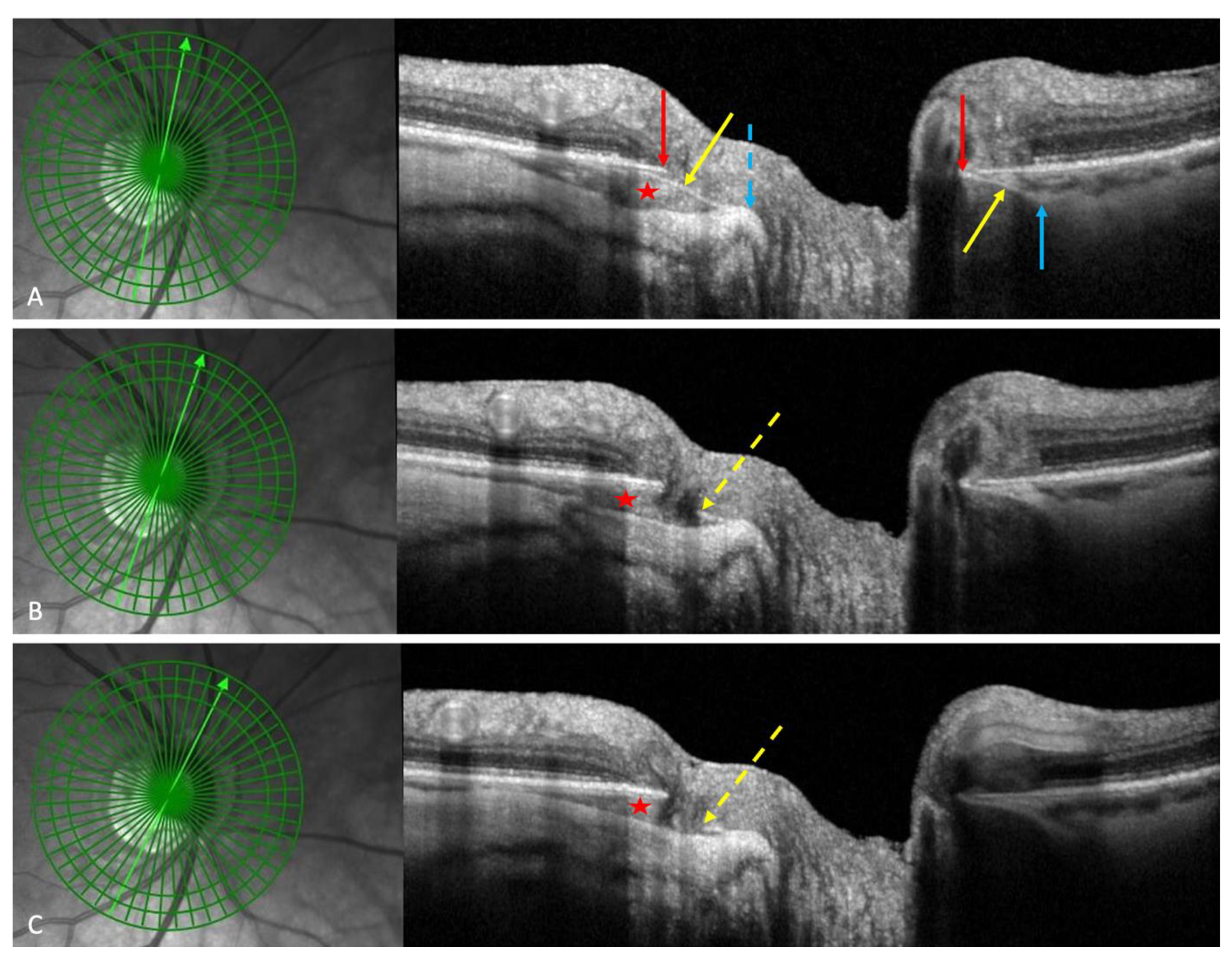
Figure 6.
Illustration of a peripapillary intrachoroidal cavitations (PICC) presenting a retinoschisis. The section is along the arrow in the infra-red image. The PICC (yellow star) coexists with a huge retinoschisis (R). Nerve fiber layers herniates into the PICC cavity. The green lines indicate the ends of the Bruch’s membrane, allowing a communication between the PICC and the vitreous cavity. The appearance of a connection (double red arrow) between the PICC cavity and the retinoschisis would promote retinal detachment.
Figure 6.
Illustration of a peripapillary intrachoroidal cavitations (PICC) presenting a retinoschisis. The section is along the arrow in the infra-red image. The PICC (yellow star) coexists with a huge retinoschisis (R). Nerve fiber layers herniates into the PICC cavity. The green lines indicate the ends of the Bruch’s membrane, allowing a communication between the PICC and the vitreous cavity. The appearance of a connection (double red arrow) between the PICC cavity and the retinoschisis would promote retinal detachment.
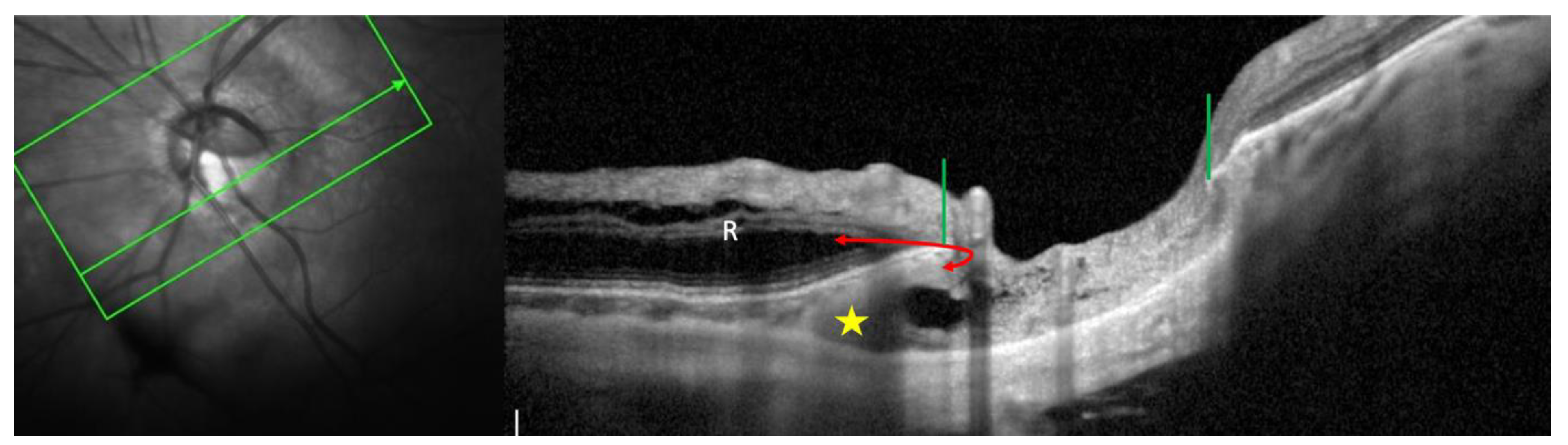
Figure 7.
Traction of the dura mater in the pathogenesis of peripapillary intrachoroidal cavitation (PICC). A-F. red star = PICC. B-F. Yellow star = subarachnoid space. d = dura mater. C-F. blue line – scleral flange. yellow dot = optic nerve. D-F. LC = lamina cribrosa. A. Fundus picture showing the yellow-orange aspect of PICC at the outer border of the myopic conus (green star). B-F. Serial OCT sections towards the optic nerve head showing changes in the posterior curvature of the choroid and landmarks of PICC. B. Wedge deformation of the posterior choroidal wall with the detachment of the supra-choroid. The dotted red and yellow lines outline the steepening of the scleral flange in front of the subarachnoid space. B-F. The scleral flange is bowed backwards due to the traction of the dura mater.
Figure 7.
Traction of the dura mater in the pathogenesis of peripapillary intrachoroidal cavitation (PICC). A-F. red star = PICC. B-F. Yellow star = subarachnoid space. d = dura mater. C-F. blue line – scleral flange. yellow dot = optic nerve. D-F. LC = lamina cribrosa. A. Fundus picture showing the yellow-orange aspect of PICC at the outer border of the myopic conus (green star). B-F. Serial OCT sections towards the optic nerve head showing changes in the posterior curvature of the choroid and landmarks of PICC. B. Wedge deformation of the posterior choroidal wall with the detachment of the supra-choroid. The dotted red and yellow lines outline the steepening of the scleral flange in front of the subarachnoid space. B-F. The scleral flange is bowed backwards due to the traction of the dura mater.
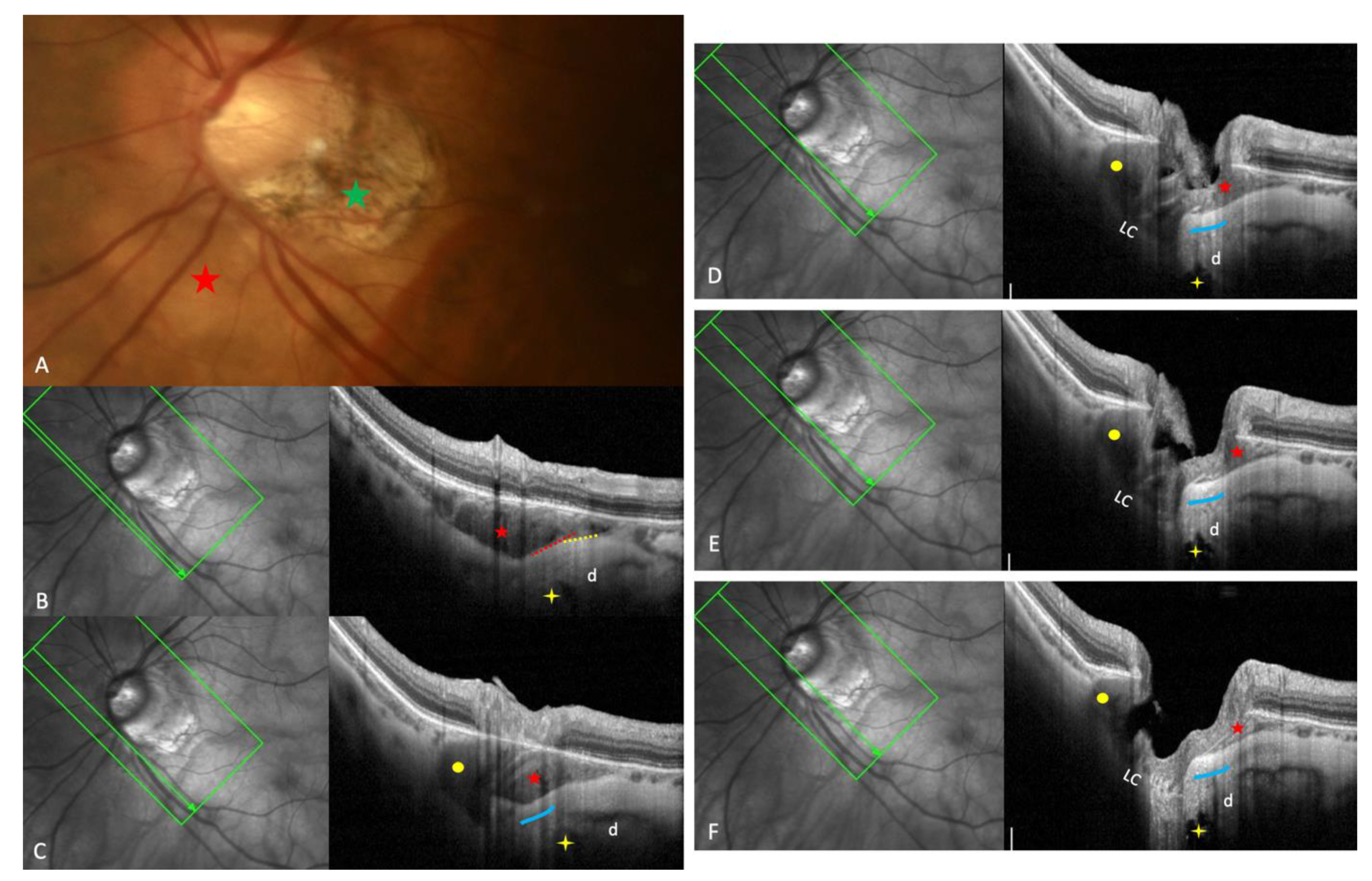
Figure 8.
Landmarks of the peripapillary intrachoroidal cavitation (PICC). LC = lamina cribrosa. SF = scleral flange, the sclera between the dura and the pia mater. D= dura mater. PICC (red star) is in front of the subarachnoid space (yellow star). It is a suprachoroidal detachment. It is suggested to be promoted by a direct traction force (blue arrow) of the dura mater during eye movements. A tangential component of this traction force squeezes the choroid at the end of the posterior outpouching (red arrowheads).
Figure 8.
Landmarks of the peripapillary intrachoroidal cavitation (PICC). LC = lamina cribrosa. SF = scleral flange, the sclera between the dura and the pia mater. D= dura mater. PICC (red star) is in front of the subarachnoid space (yellow star). It is a suprachoroidal detachment. It is suggested to be promoted by a direct traction force (blue arrow) of the dura mater during eye movements. A tangential component of this traction force squeezes the choroid at the end of the posterior outpouching (red arrowheads).
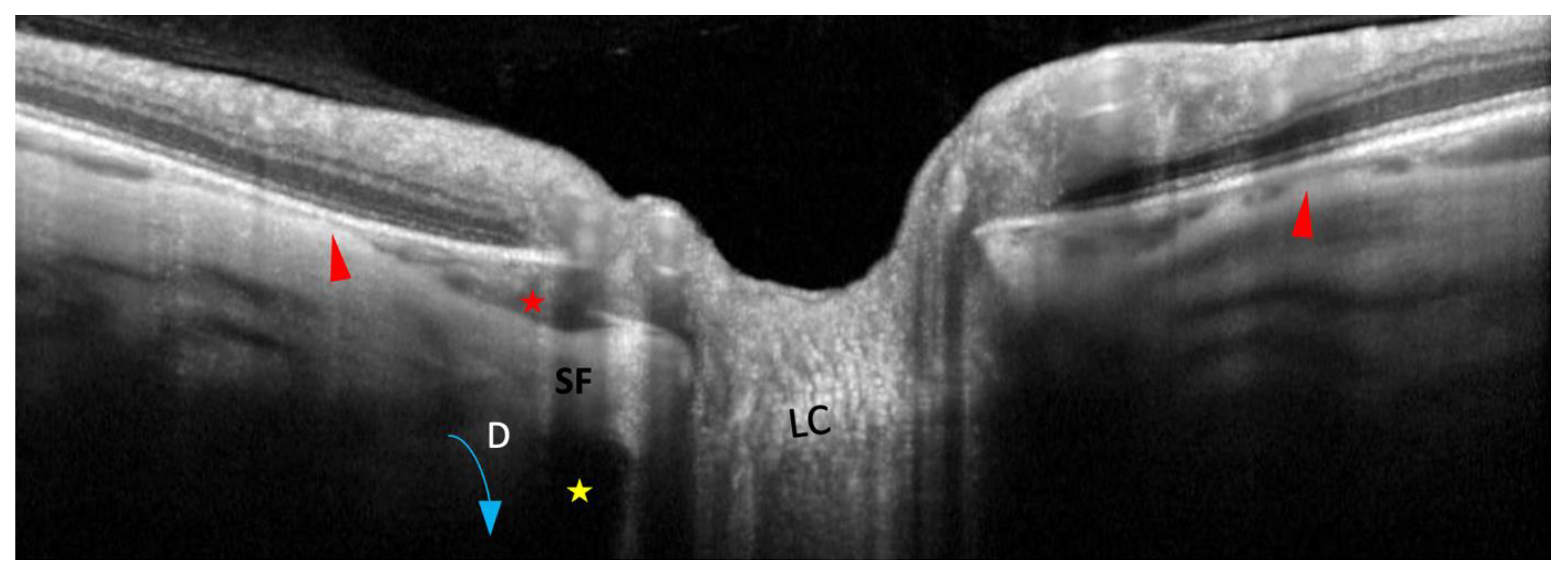
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



