
Submitted:
11 May 2023
Posted:
12 May 2023
You are already at the latest version
Abstract
A widely discussed topic in the pathophysiology of thyroid nodules is the role of obesity that leads to increased systemic inflammatory markers. Leptin plays a vital role in forming thyroid nodules and cancer through several mechanisms. Together with chronic inflammation, there is an augmentation in the secretion of tumor necrosis factor (TNF) and cytokines interleukin 6 (IL-6), contributing to cancer development, progression and metastasis. In addition, leptin exerts a modulatory action in the growth, proliferation and invasion of thyroid carcinoma cell lines via activating various signal pathways, such as Janus kinase/signal transducer and activator of transcription, mitogen-activated protein kinase (MAPK) and/or phosphoinositide 3-kinase (PI3K) /protein kinase B (Akt). Through several proposed mechanisms, aberrant endogenous estrogen levels have been suggested to play a vital role in the development of both benign and malignant nodules. Metabolic syndrome triggers the development of thyroid nodules by stimulating thyroid proliferation and angiogenesis due to hyperinsulinemia, hyperglycemia and dyslipidemia. Insulin resistance influences the distribution and structure of the thyroid blood vessels. Insulin growth factor -1 (IGF-1) and insulin affect the regulation of the expression of thyroid genes and the proliferation and differentiation of thyroid cells. TSH can promote the differentiation of pre-adipocytes to mature adipocytes, but also, in the presence of insulin, TSH possesses mitogenic properties. This review aims to summarize the underlying mechanisms explaining the role of obesity in the pathophysiology of thyroid nodules and discuss potential clinical implications.
Keywords:
thyroid nodules
; obesity
; inflammation
; leptin
; estrogen
; cytokines
; metabolic syndrome
; car-cinogenesis
1. Introduction
Thyroid nodule prevalence has been rising along with a parallel increase in obesity worldwide over the past few decades[1,2,3,4]. Together with the rising incidence of thyroid nodules, thyroid cancer detection rapidly increased [5]. The low-grade, chronic inflammation commonly observed during obesity leads to a non-specific immune response by increasing systemic inflammatory molecules, which contributes to developing thyroid nodules and cancer [6,7]. The increased release of leptin and decreased secretion of adiponectin from white adipose tissue of obese individuals, along with high oxidative stress, enhance cell proliferation and angiogenesis [8]. Aberrant endogenous estrogen levels have been suggested to play a vital role in the development of both benign and malignant nodules. Obesity leads to increased aromatase activity in the peripheral adipose tissue resulting in higher levels of circulating estrogens. Several pathways are involved in the molecular effects of estrogen in follicular cells. Estrogens have a regulatory effect on vascular endothelial growth factor (VEGF) secretion in thyroid cells that increases angiogenesis. [9] Metabolic syndrome stimulates thyroid proliferation and angiogenesis due to hyperinsulinemia, hyperglycemia, and dyslipidemia [10,11]. It triggers the secretion of IGF-1, and insulin regulates the expression of thyroid genes to control the proliferation and differentiation of thyroid cells. Furthermore, expression of TSH receptors in extrathyroidal tissues, specifically in adipose tissue, where TSH can promote the differentiation of pre-adipocytes to mature adipocytes, and in the presence of insulin, TSH exerts mitogenic properties [12]. In this review, we summarize the latest evidence regarding the molecular links between obesity and thyroid cancer development and discuss emerging diagnostic and therapeutic implications.
2. Epidemiological Evidence Linking Thyroid Nodules, Thyroid Cancer and Obesity
Thyroid nodularity is common, with an increased prevalence worldwide. Palpable thyroid nodules are present in 3-7% of the general population [13]. The prevalence of thyroid nodules by high-resolution ultrasound is 19-68% in randomly selected individuals, with annually rising trends globally [14]. As expected, the detection rates of thyroid nodules are higher with ultrasound when compared to palpation since there has been a widespread application of sensitive imaging techniques which diagnose thyroid nodules in recent years [14,15].
Several studies have shown that the prevalence of thyroid nodules depends on risk factors such as age, gender, iodine intake and history of radiation exposure [16]. In the United States, it is estimated that approximately half of the adults older than 60 years have thyroid nodules. Although there is a correlation between advanced age and a high prevalence rate of thyroid nodules, the etiology of this relationship is unclear [17]. A relatively recent multicenter-based study in Korea (N=72,319) found that the prevalence of thyroid nodules detected by ultrasound at health check-ups was 34%, rising to 55% for patients aged ≥70 years [15]. Female gender has also been proven to be a strong risk factor for thyroid nodules. The gender differences in thyroid nodules might be due to physiology, pregnancy, and female estrogen exposure [18]. It is worth noting that the development of thyroid nodules is four times more frequent in women than men, and their prevalence increases with age and body mass index [19]. Another risk factor that influences the presence of thyroid nodules is iodine intake, which has been the subject of numerous studies. Thyroid nodules were found to be more prevalent in iodine-deficient countries. It has been reported that the prevalence of thyroid nodules ranged from 2.6% in iodine-sufficient countries to 20.2% in iodine-deficient areas [20]. Furthermore, hypertension, fasting glucose and diabetes were associated with a higher risk of thyroid nodules. Contrary to the previously mentioned risk factors that negatively influence the occurrence of thyroid nodules, smoking, alcohol drinking, exercise and a Mediterranean diet might have protective effects [21].
In recent years, numerous studies have associated metabolic syndrome with the increased prevalence of thyroid nodules [21,22]. Metabolic syndrome has rising rates with an overall prevalence of approximately 25% worldwide [22,23]. The increased incidence of metabolic syndrome is attributed to economic development and change in diet and lifestyle [23,24]. Previous studies showed that diabetic patients had a higher incidence of thyroid nodules [24]. In addition, a strong association was demonstrated between thyroid nodule development and specific components of metabolic syndrome, such as waist circumference (WC), hypertension, and hyperglycemia [22]. A recent study in China reflected the relationship between waist circumference and thyroid nodule risk [25]. Males and older adults (≥60 years old) with metabolic syndrome had a higher risk of thyroid nodules than females and younger people. Patients with poorly controlled metabolic syndrome, especially those with uncontrolled, abnormal glucose metabolism, are more prone to develop thyroid nodules [26]. Despite these findings, the correlation between metabolic syndrome and the occurrence of thyroid nodules remains questionable [24].
Thyroid cancer represents the most common endocrine malignancy, with a rising incidence and mortality globally. Thyroid cancer is the ninth most common type in men and the fifth most common cancer among women [27]. According to data from the International Agency for Research on Cancer (IARC), the global incidence of thyroid cancer was approximately 6.7 cases per 100,000 people in 2018 [28]. Approximately 90% of all thyroid malignancies are differentiated thyroid carcinoma, comprising papillary thyroid carcinoma (PTC) and follicular thyroid carcinoma (FTC). Poorly differentiated thyroid carcinoma (PDTC) and anaplastic thyroid carcinoma (ATC) are rare tumors accounting for 5% and 1%, respectively. Medullary thyroid carcinoma (MTC) represents 5% of thyroid cancers [29]. The incidence rates of FTC, ATC and MTC thyroid carcinomas have remained relatively stable over the past 30 years [30]. Thyroid cancer is three times higher among females. The rising incidence is due to the variation of geographical regions and environmental exposures. The highest incidence is observed in higher-income countries, like the Republic of Korea, Canada, Italy, France, Israel, Croatia, Austria, and the U.S., as well as some middle- to upper-middle-income countries, such as Turkey, Brazil, Costa Rica and China. Furthermore, the incidence rates are high in some island nations and territories, including Cyprus, Cabo Verde and French Polynesia [31]. Several risk factors, such as female sex, radiation, dietary iodine content, genetic or hereditary conditions, and a history of benign thyroid disease, can increase the incidence of thyroid cancer [28].
The widespread use of imaging modalities, specifically ultrasonography, to evaluate patients has allowed a growing number of incidentally discovered thyroid nodules, which previously were undetectable [32]. A recent study found that a significant proportion of thyroid cancer (49%) was discovered incidentally in asymptomatic people through histological examination and imaging studies [33].
In recent decades, obesity has increased dramatically as it affects all ages, with a worldwide prevalence of 13%, nearly tripled between 1975 and 2016. The risk of many types of cancers is augmented in morbidly obese individuals with BMI> 40 kg/m2 or >35 kg/m2 in the presence of obesity-related comorbidities [7]. Severely obese individuals are more likely to develop thyroid nodules than non-obese individuals [11,34]. Moreover, there is some evidence that adiposity is related to more aggressive features of thyroid cancer [35,36]. Also, type 2 diabetes mellitus (T2DM), strongly associated with obesity, has been identified as a risk factor for increased TSH levels and thyroid cancer. However, T2DM may be a risk factor for thyroid cancer independent of obesity [11,35]. A 5 kg/m2 increase in BMI is correlated with a significant increase in the incidence of PTC [37]. Several studies suggested a strong association between central adiposity and thyroid cancer [37,38]. Waist circumference is an independent predictor of thyroid cancer [37]. An increase in BMI and waist-to-hip ratio also increases the risk of thyroid cancer. Nevertheless, the connection between obesity and thyroid nodules is unclear due to the different methods used to assess obesity [39]. Despite the above, some studies concluded that there was no significant association between BMI and thyroid cancer [40,41].
3. Obesity as a Chronic Inflammatory Condition
It is well established that obesity is a state of chronic low-grade inflammation. During this condition of continuing inflammation, the release of pro-inflammatory factors from tissues increases while the release of adipokines decreases, leading to a non-specific immune system activation which is believed to contribute to the development of obese-related pathologies. The resulting contraposition between adipose-resident immune cells and adipocytes further promotes the immune cell production of multiple pro-inflammatory factors with subsequent induction of insulin resistance, hyperinsulinemia, hyperglycemia, hyperlipidemia, and vascular injury; all of them are associated with oxidative stress, cancer development and progression [7].
Chronic inflammation triggers the activation and transcription of several factors such as nuclear factor-kappa-light-chain-enhancer of activated B cells (NF-κB), signal transducer and activator of transcription (STAT3), and activator protein1 (AP-1) in pre-malignant cells. Obese white tissue increases the production of leptin, which is pro-inflammatory, pro-proliferative, pro-oncogenic, and pro-angiogenic. It decreases adiponectin (APN) levels, which are anti-inflammatory, anti-angiogenic, and anti-proliferative [42]. Combined with high oxidative stress, inflammatory cytokines are upregulated, enhancing cell proliferation and angiogenesis. The activation of the obese white adipose tissue has multiple roles in cancer, including effects mediated via interleukin IL-1β (IL-1β), which promotes the proliferation and invasion of tumor cells. In addition, the increased levels of circulating free fatty acids observed in obesity may lead to steatosis of the thyroid gland [43].
In rats treated with a high-fat diet, thyroid tumor cell proliferation was found to be increased via upregulation of cyclin D1 protein levels, phosphorylation of retinoblastoma (Rb) protein, elevated leptin serum levels and increased STAT3 gene expression [7]. Studies also revealed lower APN in patients with thyroid cancer, whereas higher levels of IL-6 and leptin were associated with more advanced papillary thyroid cancer (PTC). APN is shown to be inversely associated with women's cancer risk [7].
4. Gender and Adipose Tissue
The female sex is a well-known factor associated with the development of thyroid nodules. A study by Lai et al. demonstrated that women with a high body mass index (BMI) are likelier to have thyroid nodules with a high-risk sonographic pattern. The same study revealed a significantly higher risk of thyroid nodules as weight, body fat percentage (BFP), body surface area (BSA) and body mass index (BMI) increased. In addition, statistically significant results were found between the risk of thyroid nodules with high-suspicion sonographic pattern per 10 kg increase in weight, 5% increase in BSA and 5 kg/m2 increase in the BMI [44]. The predominance of the female gender in thyroid nodules is often attributed to the different patterns of adipose tissue distribution. Song et al. showed that women tend to have larger subcutaneous fat stores than visceral fat, while men tend to have more visceral fat for any given waist circumference. Obese individuals, with a higher proportion of subcutaneous fat than visceral fat, are at a lower risk of developing metabolic syndrome [25].
Interestingly, visceral fat is a stronger predictor of insulin resistance among men and women above 50. It is supported that central abdominal obesity carries a higher risk of co-morbid disease states, while lower body adiposity is associated with a less unhealthy metabolic profile. There are two theories behind the reasoning that visceral fat is unhealthier. One hypothesis postulates that visceral fat is responsible for the secretion of several adipokines, such as IL-1, IL-6, TNF-α, and leptin. The second hypothesis suggests that the liver is directly exposed to the non-esterified fatty acid released predominately from visceral fat, making it more prone to poor glucose control [45].
Adipose tissue serves as an important endocrine organ, and leptin concentration is more reflective of subcutaneous fat, while insulin is more indicative of visceral fat. Another important difference is that leptin correlates better with total adipose tissue in women than in men. On the other hand, insulin levels are better correlated with adipose tissue in men. Even though women have more fat than men, insulin sensitivity seems less affected by increased body fat than in men. Fat distribution differences among men and women have endocrine, metabolic, and health consequences [25,45].
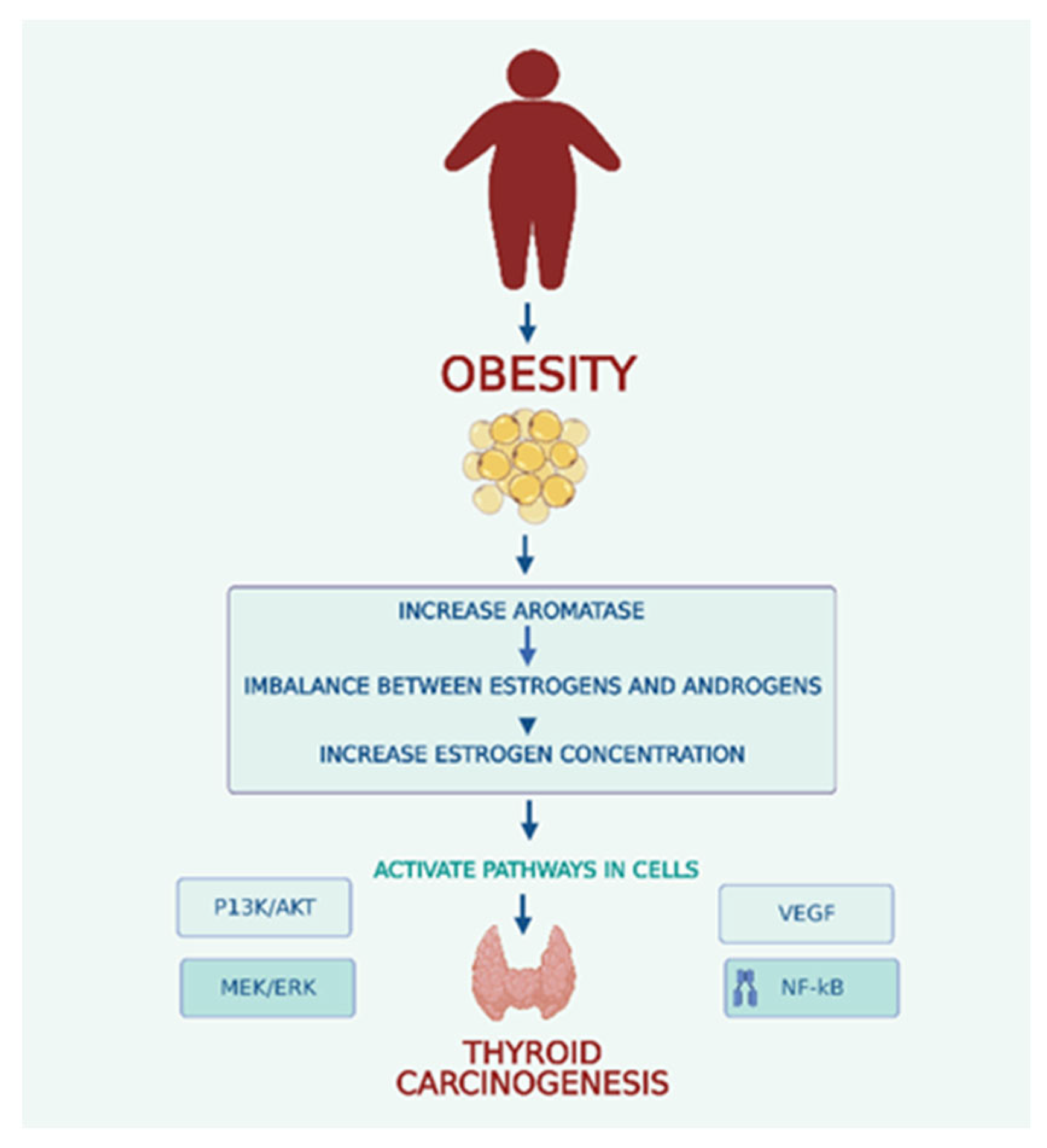
Endogenous differences in estrogen levels are considered the major factor for both benign and malignant thyroid nodules (Figure 1). Obesity causes increased aromatase activity in the peripheral adipose leading to higher levels of circulating estrogens. Hyperactivation of aromatase leads to an imbalance between estrogens and androgens that contributes to carcinogenesis in obese. Two estrogen receptors, ER-α and ER-β, mediate estrogens. ER-α is overexpressed in thyroid cells, while ER-β exhibits reduced or absent expression. Several pathways, including PI3K/AKT, MEK/ERK, VEGF and NF-k B, are involved in the molecular effects of estrogen in follicular cells [39]. The primary estrogen, 17-Beta estradiol (E2), increases cyclin D1 expression by binding to ER-α and reduces the expression of p27 and beta-catenin. E2 can lead to an increased ability for cell proliferation and survival by activation of the Bcl-2 gene [46]. E2 also stimulates reactive oxygen species (ROS) production and promotes the hyperexpression of hypoxia-inducible factor-1α (HIF1-α) [46]. In addition, estrogens can control thyroid tumor development and cancer cell invasiveness through genetic and epigenetic changes and activation of the PI3K/AKT and MAPK pathways. Estrogens can also increase angiogenesis by regulating VEGF secretion in thyroid cells. GPR30 receptor was found in thyroid carcinoma cells and represents another way estrogen stimulates cell growth that lacks expression of ERs [46].
In obese postmenopausal women, there is an increase in the conversion of endogenous sex steroids. The postmenopausal state is also responsible for a significant imbalance between levels of androgens and estrogens. Postmenopausal women with PTC exhibit an increase in ER-α expression, and these findings suggest a role in promoting cancer aggressiveness. The same increased ER-α expression levels were observed in obese women despite menopause [47].
5. Leptin and the Hypothalamic—Pituitary—Thyroid (HPT) Axis
The stimulation of the HPT axis observed in obesity is mainly due to the centrally-acting leptin, which regulates the activity of neurons in the hypothalamus and has both direct and indirect effects on thyrotropin-releasing hormone–stimulating thyroid hormone (TRH-TSH) secretion. Overnutrition caused by hyperleptinemia activates the secretion of TRH and, in turn, promotes the synthesis of TSH and thyroid hormone. Leptin can act directly on the TRH-ergic neurons within the paraventricular nucleus through the leptin receptor. Indirectly, leptin regulates the mechanism of the hypothalamic neuronal network [48].
In obesity, high leptin levels fail to reduce appetite and increase energy expenditure. Studies in adults showed that leptin-controlled arcuate neurons were unresponsive to signals from adipose tissue and insulin, disrupting energy homeostasis and food intake regulation [48]. Furthermore, leptin is reported to have a significant role in carcinogenesis by stimulating tumor cell growth and invasion by increasing cellular hypertrophy of thyroid cells and enhancing the expression of thyroglobulin [18]. In vitro studies showed that the stimulating effects of leptin were augmented by the co-administration of TSH [48].
Evidence showed that long-term exposure of the thyroid gland to high levels of TSH due to hyperleptinemia could cause significant thyroid gland hyperplasia and thyroid nodule formation. Furthermore, studies showed that BMI levels, weight circumference (WC), TSH and fasting plasma glucose (FPG) were significantly higher in the thyroid nodule group than in the non-thyroid nodule group. In addition, single-factor logistic regression analysis revealed that thyroid nodules occurrence was positively associated with metabolic syndrome [24]. Leptin receptors in the thyroid gland could induce PTC cell proliferation and inhibit cancer cell apoptosis [7]. The mean TSH levels in obese individuals appeared to be 0.8-2 mU/L higher than in non-obese individuals as a result of the leptin effect on the Type II deiodinase on the paraventricular nucleus, which could cause a rise in the incidence of goiter, nodular goiter, and papillary thyroid carcinoma development over time [15,42].
6. Metabolic Syndrome, Hyperinsulinemia, and Insulin-like Growth Factor-1
Several studies found an association between metabolic syndrome (MS) components and thyroid nodules [44]. In a quantitative review of thirteen independent observational studies, Zhang et al. reported that metabolic syndrome was related to a higher risk of thyroid nodules [26]. Xu et al., in a large-scale study, found a statistically significant association between thyroid nodules and metabolic disorders. Overweight, central obesity, high blood glucose, hypercholesterolemia and fatty liver disease were all significantly associated with the prevalence of multiple thyroid nodules [18]. A positive relationship was found between all components of metabolic syndrome and nodular goiter, but the most significant association was reported between insulin resistance, thyroid nodules and PTC [42]. In the study of Moon et al., the prevalence of metabolic syndrome was higher in the patient group with nodules; both higher BMI and waist circumference were independently associated with thyroid nodules [15]. IGF-1 promotes the progression and mitosis of many types of cells together with the signal transduction through the Insulin-like growth factor 1 receptor (IGF1-R), leading to abnormal hyperplasia, differentiation, and apoptosis of thyrocytes. This pathway could be a TSH-independent mechanism explaining the association between thyroid nodule formation and metabolic syndrome [49].
According to Chen et al., insulin resistance caused by obesity could result in steatosis and infiltration of the thyroid gland, subsequently leading to changes in the gland's morphology and function [43]. Insulin induces tissue hyperplasia by stimulating cell division and prolongs cell survival by exerting anti-apoptotic effects. In addition, thyroid cancer tissues had higher insulin receptor levels [42].
Insulin receptor (IR) and IGF-R are structurally homologous. When insulin binds to its receptor, the PI3K pathway is activated, leading to glucose uptake, while the MAPK pathway is responsible for cell and tissue proliferation and gene expression. The MAPK pathway has a major role in insulin resistance and chronic hyperinsulinemia. The activation of insulin growth factor receptors is believed to play an important role in various types of cancer with an increased incidence of metabolic syndrome. In a state of insulin resistance, the amount of IGF-binding protein is reduced, resulting in high levels of circulating IGF [42].
IGF-R is present in higher density on the membrane of cold nodules than hyperactive and normoactive ones. Also, higher levels of insulin receptors were detected in differentiated and undifferentiated thyroid cancer tissues. Interestingly, the addition of metformin, an insulin sensitizer, inhibits tumor cell proliferation, which is associated with the activation of the adenosine monophosphate kinase in cell pathways and the subsequent inhibition of the mammalian target rapamycin (mTOR) pathway. Metformin is thought to be protective against thyroid cancer development [39,42]. Liu et al. reported that insulin resistance was closely related to the distribution, density, and structure of the thyroid blood vessels, which might promote the development of thyroid nodules [24].
Shin et al. showed that the tumorigenic effect of metabolic syndrome appears to be mediated through changes in cytokine levels due to low expression of tumor suppressor genes and an increase in the levels of oncogene expression due to inflammation and ROS production. A higher prevalence of large nodules in individuals with metabolic syndrome and hyperglycemia indicated by glycated hemoglobin (HbA1C) levels demonstrates a significant relationship with thyroid nodules in women [49].
7. Adipose Tissue and TSH Levels
Several epidemiological studies noted a positive correlation between elevated TSH levels and BMI. In patients with metabolic syndrome and subclinical hypothyroidism, serum TSH levels were correlated with the severity of obesity. TSH can promote the differentiation of pre-adipocytes to mature adipocytes. TSH was found to increase the accumulation of triglycerides by thyroid-stimulating hormone receptors (TSHR) via activation of the AMPK/PPARγ pathway. Thyrotropin and TSHR were thought to be limited only to thyrocytes. Still, the expression of TSHR in extrathyroidal tissues, including liver and adipose tissue, was also demonstrated [50].
Patients with MS have a higher prevalence of nodular thyroid disease, probably due to inflammatory levels and elevated TSH [51]. Glucose tolerance was demonstrated to have the most significant contribution to the development of nodules. Activation of the TSH receptor and the production of intracellular cyclic AMP (cAMP) leads to the activation of protein kinase A (PKA) that phosphorylates nuclear factor cAMP response element binding protein (CREB) that activates the targeted genes leading to thyroid cell proliferation. Elevated TSH can increase thyroid cell proliferation through p70S6K – mediated effects on the localization of p27 [52]. Insulin activates (IGF)-1 receptors that can increase the sensitivity of TSH, promoting thyroid cell proliferation. TSH possesses well-known mitogenic properties in the presence of insulin in cell cultures [51].
8. Oxidative Stress and Diet
Low-grade chronic inflammation associated with obesity is responsible for many pathological conditions, including hyperglycemia, hyperlipidemia, hyperinsulinemia, insulin resistance and vascular damage and are all related to oxidative stress, which leads to carcinogenesis. Excess harmful free radicals and reactive molecules characterize oxidative stress. The exact function of oxidative stress in thyroid cancer remains uncertain; nonetheless, there are indications that a plausible link exists between decreased antioxidant activity and augmented generation of Reactive Oxygen Species (ROS), which may contribute to the development of thyroid tumors. ROS's activation of MAPK and PI3K/AKT signaling pathways could lead to tumorigenesis [39].
Diet has a significant role in the pathophysiology of chronic inflammation; The Dietary Inflammatory Index (DII) is a measure that explores the correlation between diet and biomarkers of inflammation. Two recent studies have linked high DII scores to thyroid cancer and other inflammatory conditions [39].
Figure 2.
Mechanisms associating obesity and thyroid nodules.
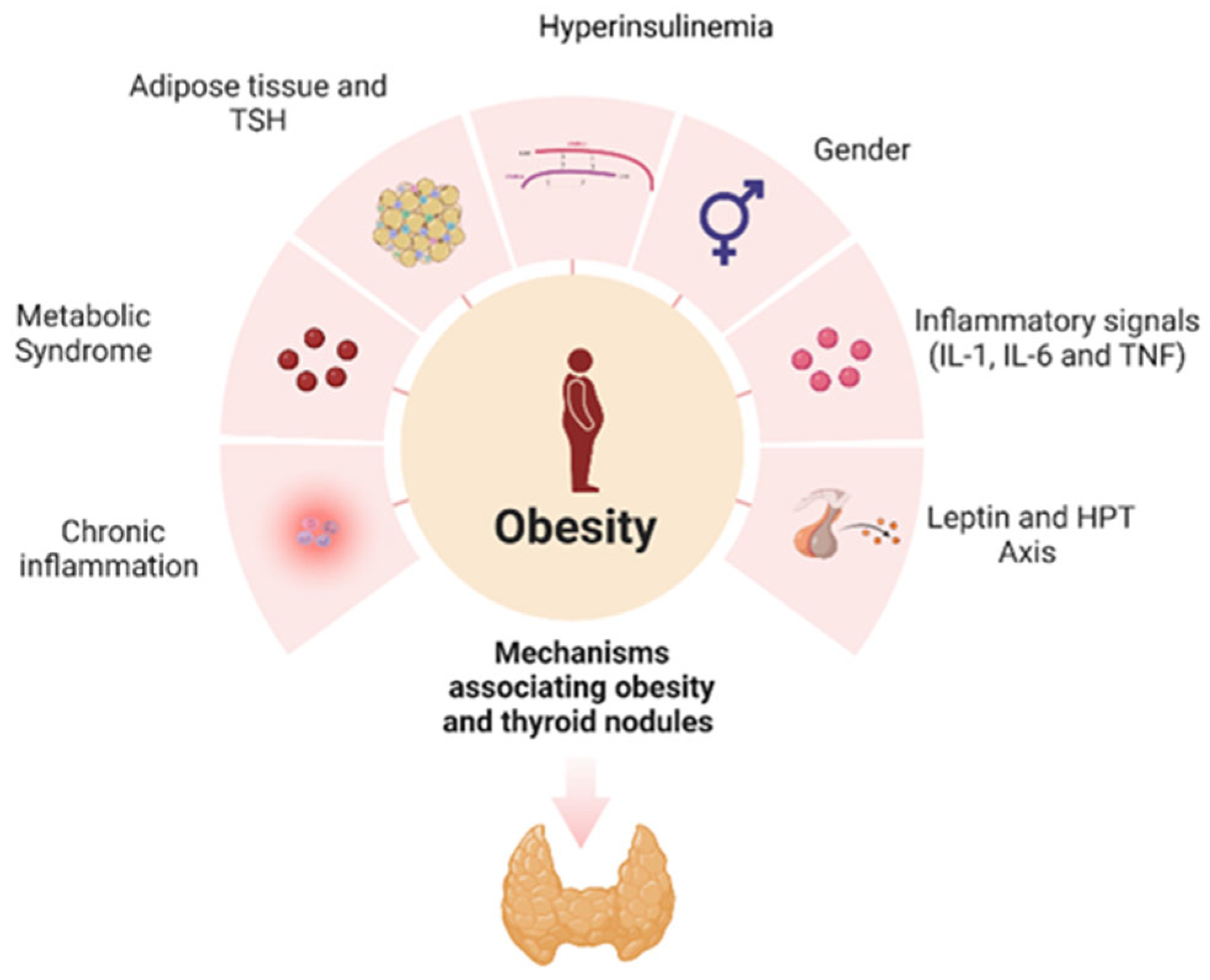
Obesity, a state of chronic, low-grade inflammation, causes an immune response that promotes carcinogenesis. Leptin plays a vital role in the development and progression of thyroid nodules, and estrogen is also involved in thyroid nodule formation. Obesity results in increased levels of circulating estrogens due to increased aromatase activity. Metabolic syndrome stimulates proliferation and angiogenesis in the thyroid gland through hyperinsulinemia, hyperglycemia and dyslipidemia. Thyroid-stimulating hormone (TSH) can turn pre-adipocytes into mature adipocytes and exerts mitogenic effects.
9. Conclusions and Future Perspectives
The pathophysiology of thyroid nodules and thyroid cancer is complex, with various parameters and biological pathways involved. The correlation between obesity and thyroid cancer is established and can be explained, at least in part, through a plethora of molecular mechanisms. The main mechanisms linking obesity with the development of thyroid nodules are shown in Figure 2. Obesity alone, as a state of chronic inflammation, is a key factor in the pathophysiology of thyroid nodules. Obesity, through increased leptin secretion, insulin resistance and activation of the HPT Axis, contributes to the genesis and development of thyroid nodules. Further investigation is needed to elucidate the mechanisms involved in the multifactorial link between thyroid nodules, thyroid cancer, obesity, and metabolic syndrome.
According to a study by Luo et al., intentional weight loss among postmenopausal women in the Women's Health Initiative (WHI) study was associated with a decreased risk of developing obesity-related cancer. The WHI study consisted of 58,667 postmenopausal women aged 50-79, whose body weight and waist circumference were measured at baseline and year 3. During the average 12-year follow-up period, 6033 cases of obesity-related cancers were reported [53]. A meta-analysis of 24 million cohorts conducted to evaluate the association between obesity and weight change and the risk of developing thyroid cancer demonstrated that obesity and weight gain are significant risk factors for thyroid cancer. Specifically, obesity increases the risk of thyroid cancer in women, and conversely, maintaining a healthy weight was associated with a reduced risk of thyroid cancer in both men and women [54].
Future directions for research include large-scale studies to assess the impact of weight loss on thyroid cancer in obese individuals. While epidemiological studies suggest a link between obesity and thyroid cancer, further research is needed to fully understand the mechanisms underlying this association and develop effective prevention and treatment strategies based on this knowledge. Additionally, randomized controlled trials are needed to assess the effects of targeting obesity and its potential mediators like inflammation, insulin resistance, IGF-1, and low adiponectin on thyroid cancer prevention. However, there are challenges, such as disentangling the effects of obesity from other factors, the heterogeneity of thyroid cancers, and a lack of consensus on specific mechanisms.
Ongoing research can lead to a better understanding of disease and the development of more effective prevention and treatment strategies. Nonetheless, given that obesity is a risk factor that can be modified, it is an important target for public health initiatives to reduce the incidence of thyroid cancer and the formation of thyroid nodules. Encouraging healthy weight management and weight loss through public health initiatives can help lower the risk of developing thyroid cancer.
Funding
This review received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Avgerinos, K. I.; Spyrou, N.; Mantzoros, C. S.; Dalamaga, M. Obesity and Cancer Risk: Emerging Biological Mechanisms and Perspectives. Metabolism: Clinical and Experimental. W.B. Saunders March 1, 2019, pp 121–135. [CrossRef]
- Iyengar, N. M.; Gucalp, A.; Dannenberg, A. J.; Hudis, C. A. Obesity and Cancer Mechanisms: Tumor Microenvironment and Inflammation. Journal of Clinical Oncology 2016, 34 (35), 4270–4276. [CrossRef]
- Steele, C. B.; Thomas, C. C.; Henley, S. J.; Massetti, G. M.; Galuska, D. A.; Agurs-Collins, T.; Puckett, M.; Richardson, L. C. Morbidity and Mortality Weekly Report Vital Signs: Trends in Incidence of Cancers Associated with Overweight and Obesity-United States, 2005-2014; 2017; Vol. 6.
- Schmid, D.; Ricci, C.; Behrens, G.; Leitzmann, M. F. Adiposity and Risk of Thyroid Cancer: A Systematic Review and Meta-Analysis. Obesity Reviews. December 1, 2015, pp 1042–1054. [CrossRef]
- Durante, C.; Grani, G.; Lamartina, L.; Filetti, S.; Mandel, S. J.; Cooper, D. S. The Diagnosis and Management of Thyroid Nodules a Review. JAMA - Journal of the American Medical Association. American Medical Association March 6, 2018, pp 919–924.
- Ferrari, S. M.; Fallahi, P.; Galdiero, M. R.; Ruffilli, I.; Elia, G.; Ragusa, F.; Paparo, S. R.; Patrizio, A.; Mazzi, V.; Varricchi, G.; Marone, G.; Antonelli, A. Immune and Inflammatory Cells in Thyroid Cancer Microenvironment. International Journal of Molecular Sciences. MDPI AG September 1, 2019. [CrossRef]
- Masone, S.; Velotti, N.; Savastano, S.; Filice, E.; Serao, R.; Vitiello, A.; Berardi, G.; Schiavone, V.; Musella, M. Clinical Medicine Morbid Obesity and Thyroid Cancer Rate. A Review of Literature. J. Clin. Med 2021, 10, 1894.
- Tumminia, A.; Vinciguerra, F.; Parisi, M.; Graziano, M.; Sciacca, L.; Baratta, R.; Frittitta, L. Adipose Tissue, Obesity and Adiponectin: Role in Endocrine Cancer Risk. International Journal of Molecular Sciences. MDPI AG June 2, 2019. [CrossRef]
- Derwahl, M.; Nicula, D. Estrogen and Its Role in Thyroid Cancer. Endocr Relat Cancer 2014, 21 (5), T273–T283. [CrossRef]
- Bener, A.; Özdenkaya, Y.; Barışık, C. C.; Öztürk, M. The Impact of Metabolic Syndrome on Increased Risk of Thyroid Nodules and Size. Health Serv Res Manag Epidemiol 2018, 5, 233339281877551.
- Buscemi, S.; Massenti, F. M.; Vasto, S.; Galvano, F.; Buscemi, C.; Corleo, D.; Barile, A. M.; Rosafio, G.; Rini, N.; Giordano, C. Association of Obesity and Diabetes with Thyroid Nodules. Endocrine 2018, 60 (2), 339–347. [CrossRef]
- Fernández-Trujillo, C.; Pérez-Zaballos, J.; Rodríguez-Pérez, C. A.; López-Plasencia, Y.; Marrero-Arencibia, D.; Cabrera-Galván, J. J.; Boronat, M. TSH Level and Risk of Malignancy in Patients with Bethesda Category IV Thyroid Nodules. 2020. [CrossRef]
- Jiang, H.; Tian, Y.; Yan, W.; Kong, Y.; Wang, H.; Wang, A.; Dou, J.; Liang, P.; Mu, Y. The Prevalence of Thyroid Nodules and an Analysis of Related Lifestyle Factors in Beijing Communities. Int J Environ Res Public Health 2016, 13 (4). [CrossRef]
- Yao, Y.; Chen, X.; Wu, S.; Guo, L.; Zhang, H.; Zhu, Q.; Tang, J.; Luan, F.; Zhao, Y.; Lv, F.; He, Y. Thyroid Nodules in Centenarians: Prevalence and Relationship to Lifestyle Characteristics and Dietary Habits. Clin Interv Aging 2018, 13, 515–522. [CrossRef]
- Moon, J. H.; Hyun, M. K.; Lee, J. Y.; Shim, J. I.; Kim, T. H.; Choi, H. S.; Ahn, H. Y.; Kim, K. W.; Park, D. J.; Park, Y. J.; Yi, K. H. Prevalence of Thyroid Nodules and Their Associated Clinical Parameters: A Large-Scale, Multicenter-Based Health Check-up Study. Korean Journal of Internal Medicine 2018, 33 (4), 753–762. [CrossRef]
- Kobaly, K.; Kim, C. S.; Mandel, S. J. Annual Review of Medicine Contemporary Management of Thyroid Nodules. 2021.
- Ospina, N. S.; Papaleontiou, M. Thyroid Nodule Evaluation and Management in Older Adults: A Review of Practical Considerations for Clinical Endocrinologists. Endocrine Practice. Elsevier B.V. March 1, 2021, pp 261–268. [CrossRef]
- Xu, L.; Zeng, F.; Wang, Y.; Bai, Y.; Shan, X.; Kong, L. Prevalence and Associated Metabolic Factors for Thyroid Nodules: A Cross-Sectional Study in Southwest of China with More than 120 Thousand Populations. BMC Endocr Disord 2021, 21 (1). [CrossRef]
- Kant, R.; Davis, A.; Verma, V. Thyroid Nodules Advances. Am Fam Physician 2020, 102 (5), 298–304.
- Mu, C.; Ming, X.; Tian, Y.; Liu, Y.; Yao, M.; Ni, Y.; Liu, Y.; Li, Z. Mapping Global Epidemiology of Thyroid Nodules among General Population: A Systematic Review and Meta-Analysis. Frontiers in Oncology. Frontiers Media S.A. November 10, 2022. [CrossRef]
- Dong, X.; Li, Y.; Xie, J.; Li, L.; Wan, Z.; Kang, Y.; Luo, Y.; Wang, J.; Duan, Y.; Ding, S.; Cheng, A. S. K. The Prevalence of Thyroid Nodules and Its Factors among Chinese Adult Women: A Cross-Sectional Study. Front Endocrinol (Lausanne) 2022, 13. [CrossRef]
- Zhang, Y.; Wehbe, A.; Wang, X.; Sun, R.; Zheng, Z.; Zhao, D. The Prevalence of Thyroid Nodules and Risk Factors of Thyroid Nodules with Metabolic Disorder in Beijing: A Cross-Sectional Study. Environ Dis 2022, 7 (1), 22. [CrossRef]
- Hu, L.; Li, T.; Yin, X. L.; Zou, Y. An Analysis of the Correlation between Thyroid Nodules and Metabolic Syndrome. Endocr Connect 2020, 9 (9), 933–938. [CrossRef]
- Liu, J.; Wang, C.; Tang, X.; Fu, S.; Jing, G.; Ma, L.; Sun, W.; Li, Y.; Wu, D.; Niu, Y.; Niu, Q.; Guo, H.; Song, P. Correlation Analysis of Metabolic Syndrome and Its Components with Thyroid Nodules. Diabetes, Metabolic Syndrome and Obesity 2019, 12, 1617–1623. [CrossRef]
- Song, B.; Zuo, Z.; Tan, J.; Guo, J.; Teng, W.; Lu, Y.; Liu, C. Association of Thyroid Nodules with Adiposity: A Community-Based Cross-Sectional Study in China. BMC Endocr Disord 2018, 18 (1). [CrossRef]
- Zhang, C.; Gao, X.; Han, Y.; Teng, W.; Shan, Z. Correlation Between Thyroid Nodules and Metabolic Syndrome: A Systematic Review and Meta-Analysis. Front Endocrinol (Lausanne) 2021, 12. [CrossRef]
- Parad, M. T.; Fararouei, M.; Mirahmadizadeh, A. R.; Afrashteh, S. Thyroid Cancer and Its Associated Factors: A Population-Based Case-Control Study. Int J Cancer 2021, 149 (3), 514–521. [CrossRef]
- Zhou, Y.; Yang, Y.; Zhou, T.; Li, B.; Wang, Z. Adiponectin and Thyroid Cancer: Insight into the Association between Adiponectin and Obesity. Aging and Disease. International Society on Aging and Disease April 1, 2021, pp 597–613. [CrossRef]
- Prete, A.; Borges de Souza, P.; Censi, S.; Muzza, M.; Nucci, N.; Sponziello, M. Update on Fundamental Mechanisms of Thyroid Cancer. Frontiers in Endocrinology. Frontiers Media S.A. March 13, 2020. [CrossRef]
- Filetti, S.; Durante, C.; Hartl, D.; Leboulleux, S.; Locati, L. D.; Newbold, K.; Papotti, M. G.; Berruti, A. Thyroid Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Annals of Oncology 2019, 30 (12), 1856–1883. [CrossRef]
- Kitahara, C. M.; Schneider, A. B. Epidemiology of Thyroid Cancer. Cancer Epidemiology Biomarkers and Prevention 2022, 31 (7), 1284–1297.
- Li, M.; Zheng, R.; Dal Maso, L.; Zhang, S.; Wei, W.; Vaccarella, S. Mapping Overdiagnosis of Thyroid Cancer in China. The Lancet Diabetes and Endocrinology. Lancet Publishing Group June 1, 2021, pp 330–332. [CrossRef]
- Lincango-Naranjo, E.; Solis-Pazmino, P.; El Kawkgi, O.; Salazar-Vega, J.; Garcia, C.; Ledesma, T.; Rojas, T.; Alvarado-Mafla, B.; Young, G.; Dy, B.; Ponce, O. J.; Brito, J. P. Triggers of Thyroid Cancer Diagnosis: A Systematic Review and Meta-Analysis. Endocrine. Springer June 1, 2021, pp 644–659. [CrossRef]
- de Siqueira, R. A.; Noll, M.; Rodrigues, A. P. dos S.; Silveira, E. A. Factors Associated with the Occurrence of Thyroid Nodules in Severely Obese Patients: A Case-Control Study. Asian Pacific Journal of Cancer Prevention 2019, 20 (3), 693–697. [CrossRef]
- Fussey, J. M.; Beaumont, R. N.; Wood, A. R.; Vaidya, B.; Smith, J.; Tyrrell, J. Does Obesity Cause Thyroid Cancer? A Mendelian Randomization Study. Journal of Clinical Endocrinology and Metabolism 2020, 105 (7). [CrossRef]
- Economides, A.; Giannakou, K.; Mamais, I.; Economides, P. A.; Papageorgis, P. Association Between Aggressive Clinicopathologic Features of Papillary Thyroid Carcinoma and Body Mass Index: A Systematic Review and Meta-Analysis. Frontiers in Endocrinology. Frontiers Media S.A. June 30, 2021. [CrossRef]
- Eissa, M. S.; Abdellateif, M. S.; Elesawy, Y. F.; Shaarawy, S.; Al-Jarhi, U. M. Obesity and Waist Circumference Are Possible Risk Factors for Thyroid Cancer: Correlation with Different Ultrasonography Criteria. Cancer Manag Res 2020, 12, 6077–6089. [CrossRef]
- Jang, Y.; Kim, T.; Kim, B. H. S.; Park, B. Association between Obesity Indexes and Thyroid Cancer Risk in Korean Women: Nested Case–Control Study. Cancers (Basel) 2022, 14 (19). [CrossRef]
- Franchini, F.; Palatucci, G.; Colao, A.; Ungaro, P.; Macchia, P. E.; Nettore, I. C. Obesity and Thyroid Cancer Risk: An Update. International Journal of Environmental Research and Public Health. MDPI February 1, 2022.
- Yang, H. X.; Zhong, Y.; Lv, W. H.; Zhang, F.; Yu, H. Association of Adiposity with Thyroid Nodules: A Cross-Sectional Study of a Healthy Population in Beijing, China. BMC Endocr Disord 2019, 19 (1). [CrossRef]
- Ahmadi, S.; Pappa, T.; Kang, A. S.; Coleman, A. K.; Landa, I.; Marqusee, E.; Kim, M.; Angell, T. E.; Alexander, E. K. Point of Care Measurement of Body Mass Index and Thyroid Nodule Malignancy Risk Assessment. Front Endocrinol (Lausanne) 2022, 13. [CrossRef]
- Yildirim Simsir, I.; Cetinkalp, S.; Kabalak, T. Review of Factors Contributing to Nodular Goiter and Thyroid Carcinoma. Medical Principles and Practice. S. Karger AG January 1, 2020, pp 1–5. [CrossRef]
- Chen, X.; Wang, J. juan; Yu, L.; Wang, H. yu; Sun, H. The Association between BMI, Smoking, Drinking and Thyroid Disease: A Cross-Sectional Study in Wuhan, China. BMC Endocr Disord 2021, 21 (1). [CrossRef]
- Lai, X.; Zhang, B.; Wang, Y.; Jiang, Y.; Li, J.; Gao, L.; Wang, Y. Adiposity and the Risk of Thyroid Nodules with a High-Suspicion Sonographic Pattern: A Large Cross-Sectional Epidemiological Study. J Thorac Dis 2019, 11 (12), 5014–5022. [CrossRef]
- Power, M. L.; Schulkin, J. Sex Differences in Fat Storage, Fat Metabolism, and the Health Risks from Obesity: Possible Evolutionary Origins. British Journal of Nutrition. 2008, pp 931–940. [CrossRef]
- Chen, Y.; Zhu, C.; Chen, Y.; Wang, N.; Li, Q.; Han, B.; Zhao, L.; Chen, C.; Zhai, H.; Lu, Y. The Association of Thyroid Nodules with Metabolic Status: A Cross-Sectional SPECT-China Study. Int J Endocrinol 2018. [CrossRef]
- Pazaitou-Panayiotou, K.; Polyzos, S. A.; Mantzoros, C. S. Obesity and Thyroid Cancer: Epidemiologic Associations and Underlying Mechanisms. Obesity Reviews. December 2013, pp 1006–1022. [CrossRef]
- Walczak, K.; Sieminska, L. Obesity and Thyroid Axis. International Journal of Environmental Research and Public Health. MDPI September 1, 2021.
- Shin, J.; Kim, M. H.; Yoon, K. H.; Kang, M. Il; Cha, B. Y.; Lim, D. J. Relationship between Metabolic Syndrome and Thyroid Nodules in Healthy Koreans. Korean Journal of Internal Medicine 2016, 31 (1), 98–105. [CrossRef]
- Ma, S.; Jing, F.; Xu, C.; Zhou, L.; Song, Y.; Yu, C.; Jiang, D.; Gao, L.; Li, Y.; Guan, Q.; Zhao, J. Thyrotropin and Obesity: Increased Adipose Triglyceride Content Through Glycerol-3-Phosphate Acyltransferase 3. Sci Rep 2015, 5. [CrossRef]
- Ayturk, S.; Gursoy, A.; Kut, A.; Anil, C.; Nar, A.; Tutuncu, N. B. Metabolic Syndrome and Its Components Are Associated with Increased Thyroid Volume and Nodule Prevalence in a Mild-to-Moderate Iodine-Deficient Area. Eur J Endocrinol 2009, 161 (4), 599–605. [CrossRef]
- Li, Z.; Zhang, L.; Huang, Y.; Yang, P.; Xu, W.; Faustini-Fustini, M. A Mechanism Exploration of Metabolic Syndrome Causing Nodular Thyroid Disease; 2019. [CrossRef]
- Luo, J.; Hendryx, M.; Manson, J. A. E.; Figueiredo, J. C.; LeBlanc, E. S.; Barrington, W.; Rohan, T. E.; Howard, B. V.; Reding, K.; Ho, G. Y. F.; Garcia, D. O.; Chlebowski, R. T. Intentional Weight Loss and Obesity-Related Cancer Risk. JNCI Cancer Spectr 2019, 3 (4). [CrossRef]
- Youssef, M. R.; Reisner, A. S. C.; Attia, A. S.; Hussein, M. H.; Omar, M.; LaRussa, A.; Galvani, C. A.; Aboueisha, M.; Abdelgawad, M.; Toraih, E. A.; Randolph, G. W.; Kandil, E. Obesity and the Prevention of Thyroid Cancer: Impact of Body Mass Index and Weight Change on Developing Thyroid Cancer – Pooled Results of 24 Million Cohorts. Oral Oncol 2021, 112. [CrossRef]
Figure 1.
Obesity and Thyroid Carcinogenesis. Adipose tissue is responsible for the conversion or synthesis of endogenous sex steroids through aromatase activity. In obese individuals, the overexpression and hyperactivity of aromatase lead to an imbalance between estrogens and androgens, resulting in elevated estrogen levels that contribute to the development of thyroid cancer. Increases in estrogen concentration activate several cell pathways, including the PI3K/AKT, MEK/ERK, VEGF, and NF-kB pathways. PI3K/AKT phosphatidylinositol-3 kinase signal pathway. MEK/ERK Mitogen-activated protein kinase/extracellular signal-regulated kinase. VEGF Vascular Endothelial Growth Factor pathway. NF-Kb Nuclear Factor kappa B pathway.
Figure 1.
Obesity and Thyroid Carcinogenesis. Adipose tissue is responsible for the conversion or synthesis of endogenous sex steroids through aromatase activity. In obese individuals, the overexpression and hyperactivity of aromatase lead to an imbalance between estrogens and androgens, resulting in elevated estrogen levels that contribute to the development of thyroid cancer. Increases in estrogen concentration activate several cell pathways, including the PI3K/AKT, MEK/ERK, VEGF, and NF-kB pathways. PI3K/AKT phosphatidylinositol-3 kinase signal pathway. MEK/ERK Mitogen-activated protein kinase/extracellular signal-regulated kinase. VEGF Vascular Endothelial Growth Factor pathway. NF-Kb Nuclear Factor kappa B pathway.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



