Submitted:
06 May 2023
Posted:
08 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Coronavirus 19 disease (COVID-19) may be complicated by thrombotic events, particularly venous thromboembolism (VTE), which have been reported both in critically ill hospitalized patients and in individuals with mild symptoms. It is known that the chronic use of oral contraceptive pills (OCPs) is associated with higher risk of VTE. To date, there are only few reports concerning the association of OCPs and VTE/pulmonary embolism (PE) in COVID-19 patients. Given that during the convalescent phase of disease, a state of endothelial dysfunction, hypercoagulability and a low-grade inflammation may be persistent, the occurrence of thromboembolic events following acute COVID-19 infection may be not surprising. Herein, we report a case of high-risk PE detected in a post-COVID-19 young woman under hormonal contraception, which required thrombolytic treatment. A number of prothrombotic phenomena, such as overweight, hormonal contraceptive therapy, recent COVID-19 infection and prolonged immobilization, might have synergically contributed to the development of a sublethal thromboembolic event.
Keywords:
COVID-19 Coagulopathy
; hormonal contraception
; COVID-19
; venous thromboembolism
; pulmonary embolism
; thrombolysis
1. Introduction
During the current Coronavirus 19 disease (COVID-19) pandemic, it has been documented that hospitalized patients, especially those under critical care, have an increased risk for thrombotic events, particularly venous thromboembolism (VTE) [1]. The occurrence of VTE in critically ill COVID-19 patients is associated with a significantly increased mortality rate, due to the rapid progression to pulmonary embolism (PE) [2-6]. The association between VTE/PE and COVID-19 infection has been also reported in patients with mild symptoms of COVID-19 disease [7-10], and in post-COVID patients, especially during the first three months following the infection [11,12]. The most common risk factors for VTE are overweight/obesity, previous thrombotic event, history of malignancy, smoking, uncontrolled diabetes, older age or frailty, prolonged immobilization, and chronic diseases [11]. Another risk factor for VTE is the chronic use of oral contraceptive pills (OCPs) [12]. During the last few years, OCPs have become increasingly prescribed [13]. The use of OCPs is associated with a general two- to three-fold increase in the risk of deep vein thrombosis and PE, especially for estrogenic-containing therapies, such as ethinylestradiol [14]. Currently, there are only few reports describing the association of oral hormonal contraceptives and VTE/PE in acute COVID-19 patients [15,16]. As far as we know, significant thromboembolic complications, such as saddle PE, have never been described in post-acute COVID women who did a chronic use of OCPs. Herein, we present a case of extensive PE, which occurred four weeks after mild COVID-19 disease, in a young woman under hormonal contraception. In the present case, several prothrombotic phenomena, such as overweight, chronic OCP assumption, recent COVID-19 infection and prolonged immobilization, might have synergically contributed to a sublethal thromboembolic event.
2. Results
Case Presentation
A 29-year-old, nulliparous, non-smoker, overweight (body surface area 1.97 m2; body mass index 29.4 Kg/m2) female, who had received 3 doses of mRNA COVID-19 vaccine, presented to the emergency room of our hospital for ongoing dyspnea, tachycardia and general malaise. She had recent COVID-19 infection, presenting with mild symptoms (pharyngodynia only), which occurred four weeks before and lasted one week. During the post-acute phase of disease, the patient was immobile at bedside for three weeks, due to muscle weakness. Moreover, she had a history of chronic OCP (levonorgestrel 0.10 mg and ethinylestradiol 0.02 mg daily) use for 6 years. At hospital admission, blood pressure was 90/60 mmHg, heart rate was 132 bpm, arterial oxygen saturation was 88% and body temperature was 36.5°C. The electrocardiogram revealed sinus rhythm with S1Q3T3 pattern (Figure 1).
Laboratory test results showed leukocytosis [white blood count (WBC) 12.3 x 109/L], hemoglobin 13.5 g/dl, hematocrit 42% and elevation of neutrophil-to-lymphocyte ratio (NLR) 7.8 (normal range between 1 and 3), serum levels of D-dimer (9546 ng/ml; normal range 0.0-682 ng/ml), troponin I (0.07 ng/ml; normal range 0-0.04 ng/ml) and C-reactive protein (CRP) (2.3 mg/dl; normal range 0-0.5 mg/dl); in addition, brain natriuretic peptide (BNP) and coagulation profile, assessed by prothrombin time (PT), activated partial thromboplastin time (aPTT) and international normalized ratio (INR), were normal (Table 1).
Arterial blood gases analysis showed hypocapnia (pCO2 of 27.6 mmHg) and hypoxemia (pO2 of 66 mmHg) with mild respiratory alkalosis (pH of 7.48). An urgent computed tomography (CT) pulmonary angiography revealed extensive saddle pulmonary embolism (Figure 2). CT venography documented concurrent thrombosis of the left saphenofemoral junction and great saphenous vein (Figure 3). Transthoracic echocardiography (TTE) confirmed the saddle pulmonary embolism (Figure 4, Movie) and showed a moderate right ventricular (RV) dilatation (RV to left ventricular basal diameter ratio = 1.2) and dysfunction (tricuspid annular plane systolic excursion = 15 mm) (McConnell's sign positive) with severe pulmonary hypertension (tricuspid regurgitation velocity >3.4 m/sec).
Reverse Transcription-Polymerase Chain Reaction (RT-PCR) test for SARS-CoV-2 was negative and the patient was transferred to the respiratory intensive care unit. Given the arterial hypotension secondary to extensive PE, the patient underwent systemic thrombolysis with recombinant tissue plasminogen activator (rtPA) 100 mg infusion over 2 h. After treatment, she showed a rapid improvement in her hemodynamic and ventilatory patterns, the ECG quickly normalized and saddle pulmonary embolism disappeared on TTE (Figure 5). During hospitalization the patient underwent a thrombophilia screening, who did negative results. Notably, protein C activity (86%; normal range 70-130%), protein S activity (88%; normal range 65-145%), antithrombin III activity (96%; normal range 80-120%) and serum homocysteine (11 micromol/L; normal values <15 micromol/L) were within normal ranges. Factor V Leiden gene mutation (G1691A), prothrombin gene mutation (G20210A) and MTHFR mutation were negative. Finally, antibodies anticardiolipin and lupus anticoagulant were not detected; accordingly, antiphospholipid syndrome was excluded. On repeated blood tests, normalization of serum inflammatory biomarkers (WBC, NLR, CRP) and troponin I was observed, whereas serum D-dimer levels were significantly decreased (Table 1).
The further use of OCP was contraindicated and the patient was discharged from our institution with the indication to a 6-months of anticoagulant therapy with a factor-XA inhibitor (apixaban 5 mg twice a day).
3. Discussion
Venous thromboembolism is a leading cause of mortality in the world [17]. Risk factors for VTE can be permanent (such as thrombophilia) or temporary (such as infections or prolonged immobilization). Accordingly, hospitalized patients with acute infectious diseases have a significantly increased risk of developing VTE [3,5,17]. An increased prevalence of VTE has been documented in COVID-19 patients, both in those with severe disease, and even among those who are not critically ill [18-20]. The main factors responsible for hypercoagulability and thrombogenesis associated with COVID-19 infection are the following: endothelial cell activation and injury, activation of the renin-angiotensin-aldosterone system and hyperimmune response [21-24]. The endothelial dysfunction resulting from the binding of angiotensin-converting enzyme 2 receptors to the virus [25,26] may induce the activation of the coagulation cascade and increase the risk of thrombotic manifestations such as VTE, mediated by the endothelial release of procoagulant plasminogen activator inhibitor (PAI-1) and inflammatory cytokines, such interleukin (IL)-6, IL-2, IL-7, interferon-gamma, and TNF-alfa [21-23].
Another risk factor for VTE is the chronic assumption of hormonal contraceptives. The OCPs-related pro-thrombotic affects are more frequently observed in women older than 35 years, smokers, women with diabetes, women with body mass index >25 Kg/m2, women with polycystic ovary syndrome or women with history of thrombophilia, particularly during the first year of treatment [27].
The literature data concerning the association between hormonal contraception and VTE/PE in COVID-19 patients are scanty. To date, only two authors have described the association between chronic OCP use and VTE/PE in the acute phase of disease [15,16]. Differently from the above-mentioned case reports, we described a case of extensive saddle PE detected during the post-acute phase of COVID-19 disease, in a young woman who did a chronic use of OCP. In our case, the patient was younger than 35 years, had never smoked, was not diabetic, did not have thrombophilia and used OCP for more than one year. The main mechanisms which could explain the development of VTE in the present case are the persistent inflammation caused by SARS-CoV-2 infection and a possible pro-thrombotic association between the virus and OCPs use [15,28]. In addition, a state of prolonged immobilization during the post-acute phase of COVID-19 disease may have exacerbated the potential risk for developing VTE/PE [29].
We reported a case of proximal PE; this finding was in contrast with the majority of reports which described segmental or subsegmental cases of PE in COVID-19 patients [5,30].
Current reasons for COVID-19-associated hypercoagulability include hypoxia and systemic inflammation secondary to COVID-19 infection, leading to high levels of inflammatory cytokines and activation of the coagulation pathway. Following mechanisms have been proposed to explain the occurrence of thromboembolic events in COVID-19 patients: 1) endothelial inflammation with very high levels of von Willebrand factor antigen and factor VIII; 2) hypoxemia-induced vasoconstriction promoting vaso-occlusion; 3) activation of hypoxia-inducible factors (HIFs) resulting in the induction or inhibition of tissue factor (TF) and plasminogen activator inhibitor 1 (PAI-1); 4) elevated levels of lupus anticoagulant; 5) direct activation coagulation cascades; and finally 6) endothelial injury by the virus [31].
Considering that the virus' spike protein binds to the Angiotensin-Converting Enzyme 2 (ACE2) receptor to enter the cell and infect the body [32] and that recent studies have demonstrated that estrogens stimulate ACE2 activity in the atrial tissue of the human heart [33], it is likely that hormonal steroid contraceptives may increase the risk of becoming infected with SARS-CoV-2 [34]. Moreover, the estrogenic component of hormonal contraception may increase the risk of venous thrombosis due to its ability to activate the coagulation system [35].
Given that during the convalescent phase of COVID-19 disease, a state of endothelial dysfunction, hypercoagulability and a low-grade inflammation may be persistent [36,37], it is likely that OCP may have exerted an additive prothrombotic effect on a substrate of chronic immuno-thrombogenicity related to COVID-19 infection. Indeed, the patient was diagnosed with increased serum levels of serum inflammatory biomakers, such as WBC, NLR and CRP, thus confirming a state of persistent inflammation during the post-acute phase of COVID-19 disease.
In the present case, serum D-dimer levels were strongly correlated with the extent of PE on CT pulmonary angiography, as observed by previous Authors [38]. According to literature data [39], the increase in serum D-dimer levels may be persistent in approximately 25% of convalescent COVID-19 patients up to 4 months following the resolution of the acute infection; these increased D-dimer levels have been observed in both hospitalized and nonhospitalized COVID-19 patients [40]. Moreover, sustained prothrombotic changes related to elevated thrombin-generating capacity have also been reported [41]. The persistent procoagulant effects following acute COVID-19 infection are likely modulated by persistent endotheliopathy and coagulation activation, independently of the acute phase response [42].
Although the present case was only a case report, it highlights the risk of sublethal PE following COVID-19 infection, even in patients with mild-to-moderate disease and confirms the wide interindividual variability of SARS-CoV-2 infection. The main clinical implication of our findings is that, for convalescent patients, regardless of the severity of infection, clinicians need to be vigilant for possible post-infective thrombotic sequelae as well as consider the importance of differentiating the immunologic and genetic characteristics of each patient [43]. In individuals at increased risk of thrombotic events, the thromboprophylaxis should be considered, even after resolution of mild-to-moderate forms of COVID-19 disease [31]. Moreover, frequent mobilization should be encouraged in patients with mild COVID-19 disease who can functionally perform activities of daily life. In addition, the discontinuation of prothrombotic drugs such as OCPs and selective cyclooxygenase-2 (COX-2) inhibitors [44] and weight loss in individuals with obesity [45] should be considered. Finally, it could be useful to employ individualized risk stratification for non-critical COVID-19 patients, by using scores that still need validation [46].
Author Contributions
AS, ML and GN: conceptualization. AS, GR, DM and RC: performed the clinical and instrumental evaluation of the patient. AS, ML, GR and DM: data analysis and curation. AS: writing original draft preparation. AS, ML, AA, DN, GN and SH: writing review and editing. AA and DN: funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Ministero della Salute ricerca corrente progetto RCR-2021-23671212. Studies are partially funded by the Italian Ministry of Health Ricerca Corrente-IRCCS MultiMedica.
Institutional Review Board Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements.
Informed Consent Statement
The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Guzik, T.J.; Mohiddin, S.A.; Dimarco, A.; Patel, V.; Savvatis, K.; Marelli-Berg, F.M.; Madhur, M.S.; Tomaszewski, M.; Maffia, P.; D'Acquisto, F.; et al. COVID-19 and the cardiovascular system: Implications for risk assessment, diagnosis, and treatment options. Cardiovasc Res 2020, 116, 1666–1687. [Google Scholar] [CrossRef] [PubMed]
- Fauvel, C.; Weizman, O.; Trimaille, A.; Mika, D.; Pommier, T.; Pace, N.; Douair, A.; Barbin, E.; Fraix, A.; Bouchot, O.; et al. Pulmonary embolism in COVID-19 patients: A French multicentre cohort study. Eur Heart J 2020, 41, 3058–3068. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med 2020, 46, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Kruip, M.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res 2020, 191, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Middeldorp, S.; Coppens, M.; van Haaps, T.F.; Foppen, M.; Vlaar, A.P.; Muller, M.C.A.; Bouman, C.C.S.; Beenen, L.F.M.; Kootte, R.S.; Heijmans, J.; et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J Thromb Haemost 2020, 18, 1995–2002. [Google Scholar] [CrossRef] [PubMed]
- Poissy, J.; Goutay, J.; Caplan, M.; Parmentier, E.; Duburcq, T.; Lassalle, F.; Jeanpierre, E.; Rauch, A.; Labreuche, J.; Susen, S.; et al. Pulmonary Embolism in Patients With COVID-19: Awareness of an Increased Prevalence. Circulation 2020, 142, 184–186. [Google Scholar] [CrossRef]
- Clavijo, M.M.; Vicente Reparaz, M.L.A.; Ruiz, J.I.; Acuna, M.A.; Casali, C.E.; Aizpurua, M.F.; Mahuad, C.V.; Eciolaza, S.; Ventura, A.; Garate, G.M. Mild COVID-19 Illness as a Risk Factor for Venous Thromboembolism. Cureus 2021, 13, e18236. [Google Scholar] [CrossRef] [PubMed]
- De Pace, D.; Ariotti, S.; Persampieri, S.; Patti, G.; Lupi, A. Unexpected Pulmonary Embolism Late After Recovery from Mild COVID-19? Eur J Case Rep Intern Med 2021, 8, 002854. [Google Scholar] [CrossRef]
- Joseph, J.W.; Roberts, J.C.; Weaver, C.N.; Anderson, J.S.; Wong, M.L. Patients with Mild COVID-19 Symptoms and Coincident Pulmonary Embolism: A Case Series. Clin Pract Cases Emerg Med 2020, 4, 295–298. [Google Scholar] [CrossRef]
- Suwanwongse, K.; Shabarek, N. Bilateral Popliteal Vein Thrombosis, Acute Pulmonary Embolism and Mild COVID-19. Cureus 2020, 12, e11213. [Google Scholar] [CrossRef]
- Bavaro, D.F.; Diella, L.; Fabrizio, C.; Sulpasso, R.; Bottalico, I.F.; Calamo, A.; Santoro, C.R.; Brindicci, G.; Bruno, G.; Mastroianni, A.; et al. Peculiar clinical presentation of COVID-19 and predictors of mortality in the elderly: A multicentre retrospective cohort study. Int J Infect Dis 2021, 105, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Sitruk-Ware, R. Hormonal contraception and thrombosis. Fertil Steril 2016, 106, 1289–1294. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, K.; Kobayashi, T.; Ojima, T. The epidemiological characteristics of thromboembolism related to oral contraceptives in Japan: Results of a national survey. J Obstet Gynaecol Res 2021, 47, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Stegeman, B.H.; de Bastos, M.; Rosendaal, F.R.; van Hylckama Vlieg, A.; Helmerhorst, F.M.; Stijnen, T.; Dekkers, O.M. Different combined oral contraceptives and the risk of venous thrombosis: Systematic review and network meta-analysis. BMJ 2013, 347, f5298. [Google Scholar] [CrossRef] [PubMed]
- Fiorini, N.B.; Garagoli, F.; Bustamante, R.C.; Pizarro, R. Acute pulmonary embolism in a patient with mild COVID-19 symptoms: A case report. Eur Heart J Case Rep 2021, 5, ytaa563. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela-Vallejo, L.; Corredor-Orlandelli, D.; Alzate-Ricaurte, S.; Hernandez-Santamaria, V.; Aguirre-Ruiz, J.F.; Pena-Pena, A. Hormonal Contraception and Massive Pulmonary Embolism in a COVID-19 Ambulatory Patient: A Case Report. Clin Pract 2021, 11, 914–918. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jimenez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J 2020, 41, 543–603. [Google Scholar] [CrossRef]
- Ahmed, S.; Zimba, O.; Gasparyan, A.Y. Thrombosis in Coronavirus disease 2019 (COVID-19) through the prism of Virchow's triad. Clin Rheumatol 2020, 39, 2529–2543. [Google Scholar] [CrossRef]
- Gorog, D.A.; Storey, R.F.; Gurbel, P.A.; Tantry, U.S.; Berger, J.S.; Chan, M.Y.; Duerschmied, D.; Smyth, S.S.; Parker, W.A.E.; Ajjan, R.A.; et al. Current and novel biomarkers of thrombotic risk in COVID-19: A Consensus Statement from the International COVID-19 Thrombosis Biomarkers Colloquium. Nat Rev Cardiol 2022, 19, 475–495. [Google Scholar] [CrossRef]
- Martinelli, I.; Ferrazzi, E.; Ciavarella, A.; Erra, R.; Iurlaro, E.; Ossola, M.; Lombardi, A.; Blasi, F.; Mosca, F.; Peyvandi, F. Pulmonary embolism in a young pregnant woman with COVID-19. Thromb Res 2020, 191, 36–37. [Google Scholar] [CrossRef]
- Kasinathan, G.; Sathar, J. Haematological manifestations, mechanisms of thrombosis and anti-coagulation in COVID-19 disease: A review. Ann Med Surg (Lond) 2020, 56, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Manne, B.K.; Denorme, F.; Middleton, E.A.; Portier, I.; Rowley, J.W.; Stubben, C.; Petrey, A.C.; Tolley, N.D.; Guo, L.; Cody, M.; et al. Platelet gene expression and function in patients with COVID-19. Blood 2020, 136, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological findings and complications of COVID-19. Am J Hematol 2020, 95, 834–847. [Google Scholar] [CrossRef] [PubMed]
- Muresan, A.V.; Halmaciu, I.; Arbanasi, E.M.; Kaller, R.; Arbanasi, E.M.; Budisca, O.A.; Melinte, R.M.; Vunvulea, V.; Filep, R.C.; Marginean, L.; et al. Prognostic Nutritional Index, Controlling Nutritional Status (CONUT) Score, and Inflammatory Biomarkers as Predictors of Deep Vein Thrombosis, Acute Pulmonary Embolism, and Mortality in COVID-19 Patients. Diagnostics (Basel) 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Albini, A.; Di Guardo, G.; Noonan, D.M.; Lombardo, M. The SARS-CoV-2 receptor, ACE-2, is expressed on many different cell types: Implications for ACE-inhibitor- and angiotensin II receptor blocker-based cardiovascular therapies. Intern Emerg Med 2020, 15, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Albini, A.; Calabrone, L.; Carlini, V.; Benedetto, N.; Lombardo, M.; Bruno, A.; Noonan, D.M. Preliminary Evidence for IL-10-Induced ACE2 mRNA Expression in Lung-Derived and Endothelial Cells: Implications for SARS-Cov-2 ARDS Pathogenesis. Front Immunol 2021, 12, 718136. [Google Scholar] [CrossRef] [PubMed]
- Dulicek, P.; Ivanova, E.; Kostal, M.; Sadilek, P.; Beranek, M.; Zak, P.; Hirmerova, J. Analysis of Risk Factors of Stroke and Venous Thromboembolism in Females With Oral Contraceptives Use. Clin Appl Thromb Hemost 2018, 24, 797–802. [Google Scholar] [CrossRef]
- Spratt, D.I.; Buchsbaum, R.J. COVID-19 and Hypercoagulability: Potential Impact on Management with Oral Contraceptives, Estrogen Therapy and Pregnancy. Endocrinology 2020, 161. [Google Scholar] [CrossRef]
- Lacey, J.; Corbett, J.; Forni, L.; Hooper, L.; Hughes, F.; Minto, G.; Moss, C.; Price, S.; Whyte, G.; Woodcock, T.; et al. A multidisciplinary consensus on dehydration: Definitions, diagnostic methods and clinical implications. Ann Med 2019, 51, 232–251. [Google Scholar] [CrossRef]
- van Dam, L.F.; Kroft, L.J.M.; van der Wal, L.I.; Cannegieter, S.C.; Eikenboom, J.; de Jonge, E.; Huisman, M.V.; Klok, F.A. Clinical and computed tomography characteristics of COVID-19 associated acute pulmonary embolism: A different phenotype of thrombotic disease? Thromb Res 2020, 193, 86–89. [Google Scholar] [CrossRef]
- Ali, S.; Mathew, S.; Pappachan, J.M. Acute cor pulmonale from saddle pulmonary embolism in a patient with previous COVID-19: Should we prolong prophylactic anticoagulation? Int J Infect Dis 2020, 97, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zetter, M.A.; Guerra, E.C.; Hernandez, V.S.; Mahata, S.K.; Eiden, L.E. ACE2 in the second act of COVID-19 syndrome: Peptide dysregulation and possible correction with oestrogen. J Neuroendocrinol 2021, 33, e12935. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Sun, X.; J, L.V.; Kon, N.D.; Ferrario, C.M.; Groban, L. Estrogen receptors are linked to angiotensin-converting enzyme 2 (ACE2), ADAM metallopeptidase domain 17 (ADAM-17), and transmembrane protease serine 2 (TMPRSS2) expression in the human atrium: Insights into COVID-19. Hypertens Res 2021, 44, 882–884. [Google Scholar] [CrossRef] [PubMed]
- Stelzig, K.E.; Canepa-Escaro, F.; Schiliro, M.; Berdnikovs, S.; Prakash, Y.S.; Chiarella, S.E. Estrogen regulates the expression of SARS-CoV-2 receptor ACE2 in differentiated airway epithelial cells. Am J Physiol Lung Cell Mol Physiol 2020, 318, L1280–L1281. [Google Scholar] [CrossRef] [PubMed]
- Cagnacci, A. Hormonal contraception: Venous and arterial disease. Eur J Contracept Reprod Health Care 2017, 22, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Dalan, R.; Boehm, B.O. The implications of COVID-19 infection on the endothelium: A metabolic vascular perspective. Diabetes Metab Res Rev 2021, 37, e3402. [Google Scholar] [CrossRef]
- Fan, B.E.; Umapathi, T.; Chua, K.; Chia, Y.W.; Wong, S.W.; Tan, G.W.L.; Chandrasekar, S.; Lum, Y.H.; Vasoo, S.; Dalan, R. Delayed catastrophic thrombotic events in young and asymptomatic post COVID-19 patients. J Thromb Thrombolysis 2021, 51, 971–977. [Google Scholar] [CrossRef]
- Gao, H.; Liu, H.; Li, Y. Value of D-dimer levels for the diagnosis of pulmonary embolism: An analysis of 32 cases with computed tomography pulmonary angiography. Exp Ther Med 2018, 16, 1554–1560. [Google Scholar] [CrossRef]
- Townsend, L.; Fogarty, H.; Dyer, A.; Martin-Loeches, I.; Bannan, C.; Nadarajan, P.; Bergin, C.; O'Farrelly, C.; Conlon, N.; Bourke, N.M.; et al. Prolonged elevation of D-dimer levels in convalescent COVID-19 patients is independent of the acute phase response. J Thromb Haemost 2021, 19, 1064–1070. [Google Scholar] [CrossRef]
- Alyousefi, N.A. An oral combined contraceptive user with elevated D-dimer post COVID-19: A case report. BMC Womens Health 2021, 21, 320. [Google Scholar] [CrossRef]
- von Meijenfeldt, F.A.; Havervall, S.; Adelmeijer, J.; Lundstrom, A.; Magnusson, M.; Mackman, N.; Thalin, C.; Lisman, T. Sustained prothrombotic changes in COVID-19 patients 4 months after hospital discharge. Blood Adv 2021, 5, 756–759. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, H.; Townsend, L.; Morrin, H.; Ahmad, A.; Comerford, C.; Karampini, E.; Englert, H.; Byrne, M.; Bergin, C.; O'Sullivan, J.M.; et al. Persistent endotheliopathy in the pathogenesis of long COVID syndrome. J Thromb Haemost 2021, 19, 2546–2553. [Google Scholar] [CrossRef] [PubMed]
- Di Maria, E.; Latini, A.; Borgiani, P.; Novelli, G. Genetic variants of the human host influencing the coronavirus-associated phenotypes (SARS, MERS and COVID-19): Rapid systematic review and field synopsis. Hum Genomics 2020, 14, 30. [Google Scholar] [CrossRef] [PubMed]
- Dutch, C.; Thrombosis, C.; Kaptein, F.H.J.; Stals, M.A.M.; Grootenboers, M.; Braken, S.J.E.; Burggraaf, J.L.I.; van Bussel, B.C.T.; Cannegieter, S.C.; Ten Cate, H.; et al. Incidence of thrombotic complications and overall survival in hospitalized patients with COVID-19 in the second and first wave. Thromb Res 2021, 199, 143–148. [Google Scholar] [CrossRef]
- Caci, G.; Albini, A.; Malerba, M.; Noonan, D.M.; Pochetti, P.; Polosa, R. COVID-19 and Obesity: Dangerous Liaisons. J Clin Med 2020, 9. [Google Scholar] [CrossRef]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J Am Coll Cardiol 2020, 75, 2950–2973. [Google Scholar] [CrossRef]
Figure 1.
12-lead ECG, showing mild right ventricular delay and S1Q3T3 pattern, indicative of acute pulmonary embolism.
Figure 1.
12-lead ECG, showing mild right ventricular delay and S1Q3T3 pattern, indicative of acute pulmonary embolism.
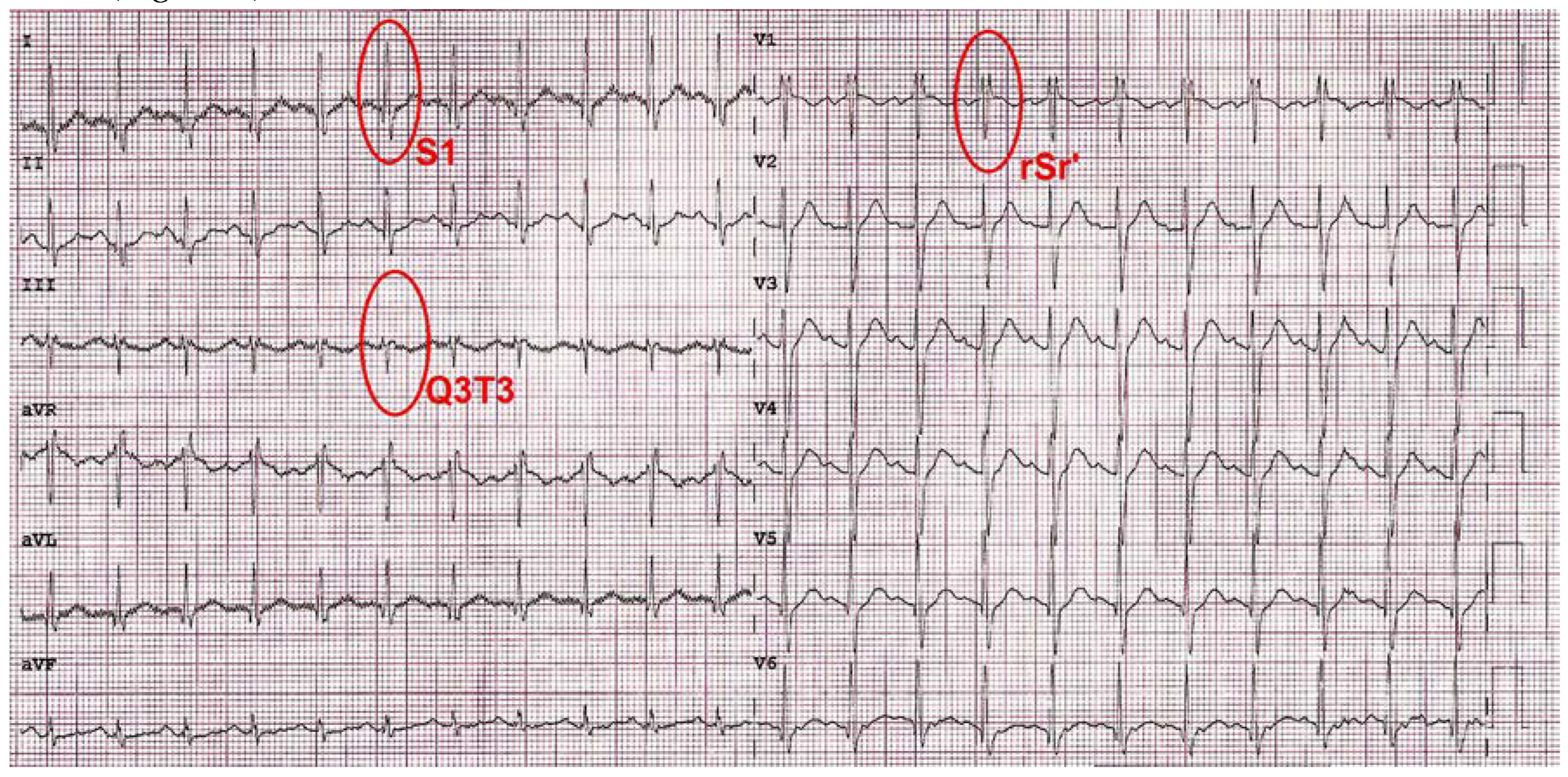
Figure 2.
Axial view of the computed tomographic pulmonary angiography, showing a saddle pulmonary embolism extending in both the right and left pulmonary arteries.
Figure 2.
Axial view of the computed tomographic pulmonary angiography, showing a saddle pulmonary embolism extending in both the right and left pulmonary arteries.
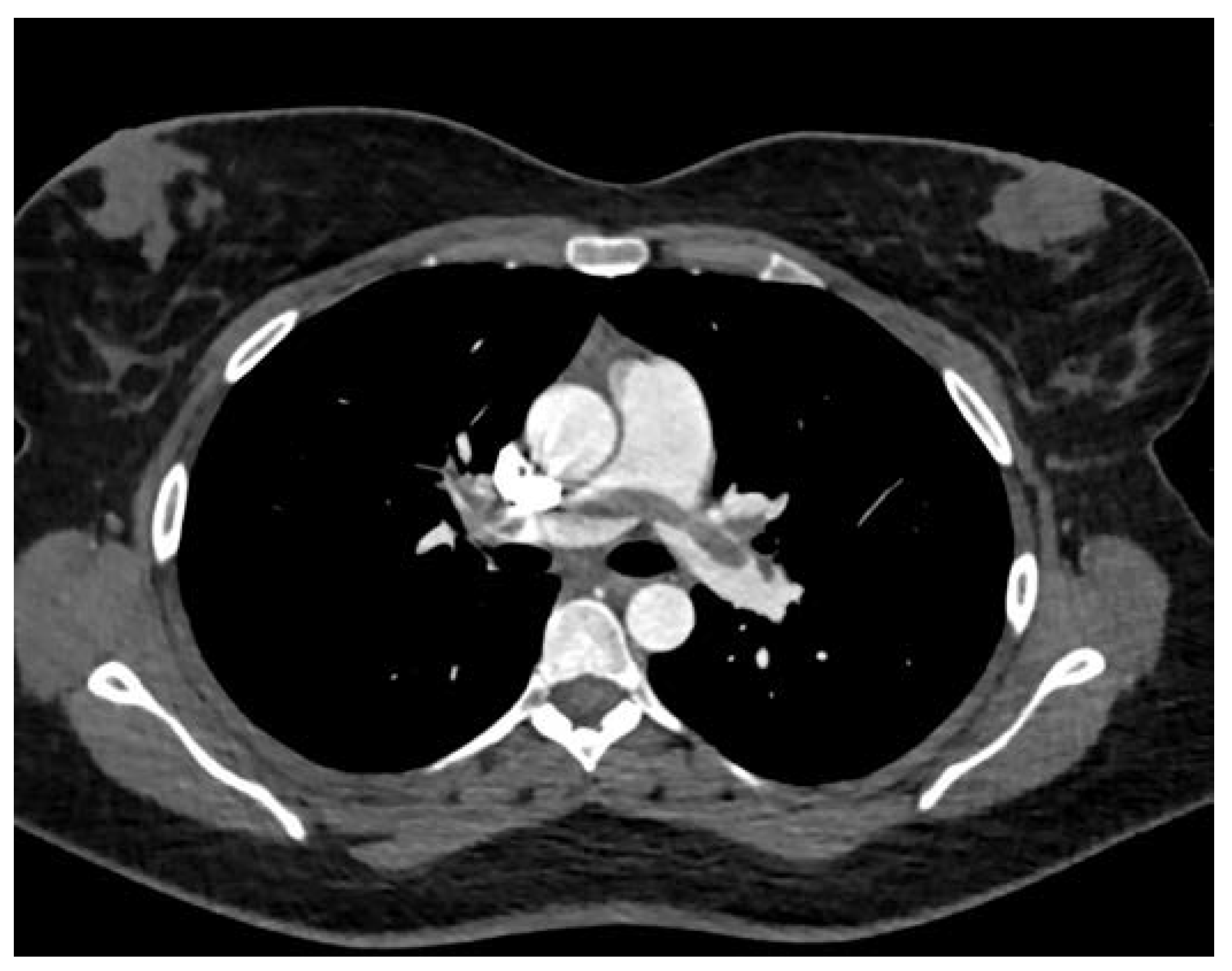
Figure 3.
Computed tomography venography in sagittal reconstruction, showing concurrent thrombosis of the left saphenofemoral junction and great saphenous vein (red arrows).
Figure 3.
Computed tomography venography in sagittal reconstruction, showing concurrent thrombosis of the left saphenofemoral junction and great saphenous vein (red arrows).

Figure 4.
Two-dimensional transthoracic echocardiography. Basal short-axis view, demonstrating a saddle pulmonary embolism (red arrow) extending in both the right and left pulmonary arteries. PA, pulmonary artery.
Figure 4.
Two-dimensional transthoracic echocardiography. Basal short-axis view, demonstrating a saddle pulmonary embolism (red arrow) extending in both the right and left pulmonary arteries. PA, pulmonary artery.
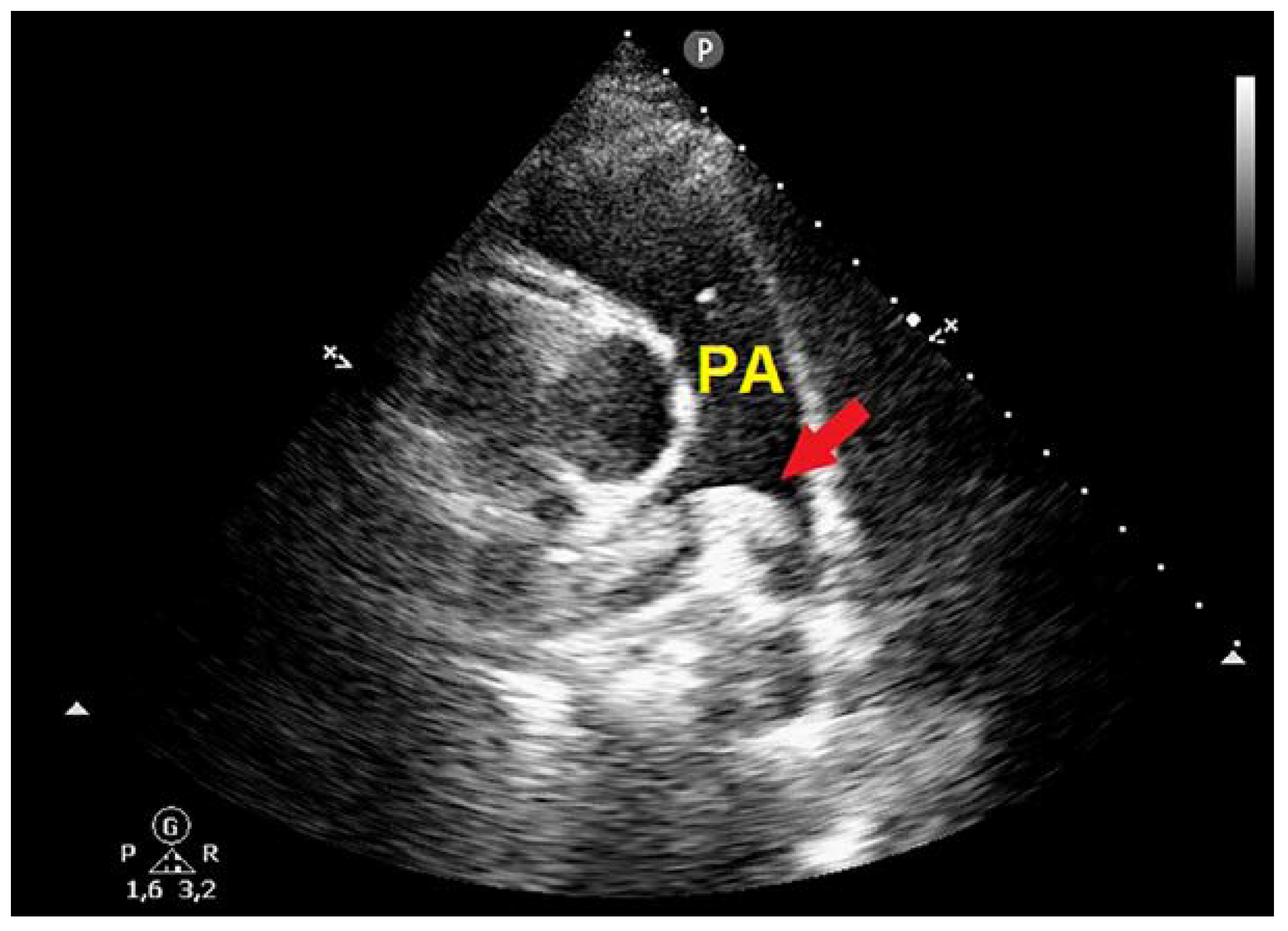
Figure 5.
Basal short-axis view from transthoracic echocardiography, demonstrating total regression of mobile saddle thrombus after thrombolytic treatment. PA, pulmonary artery.
Figure 5.
Basal short-axis view from transthoracic echocardiography, demonstrating total regression of mobile saddle thrombus after thrombolytic treatment. PA, pulmonary artery.
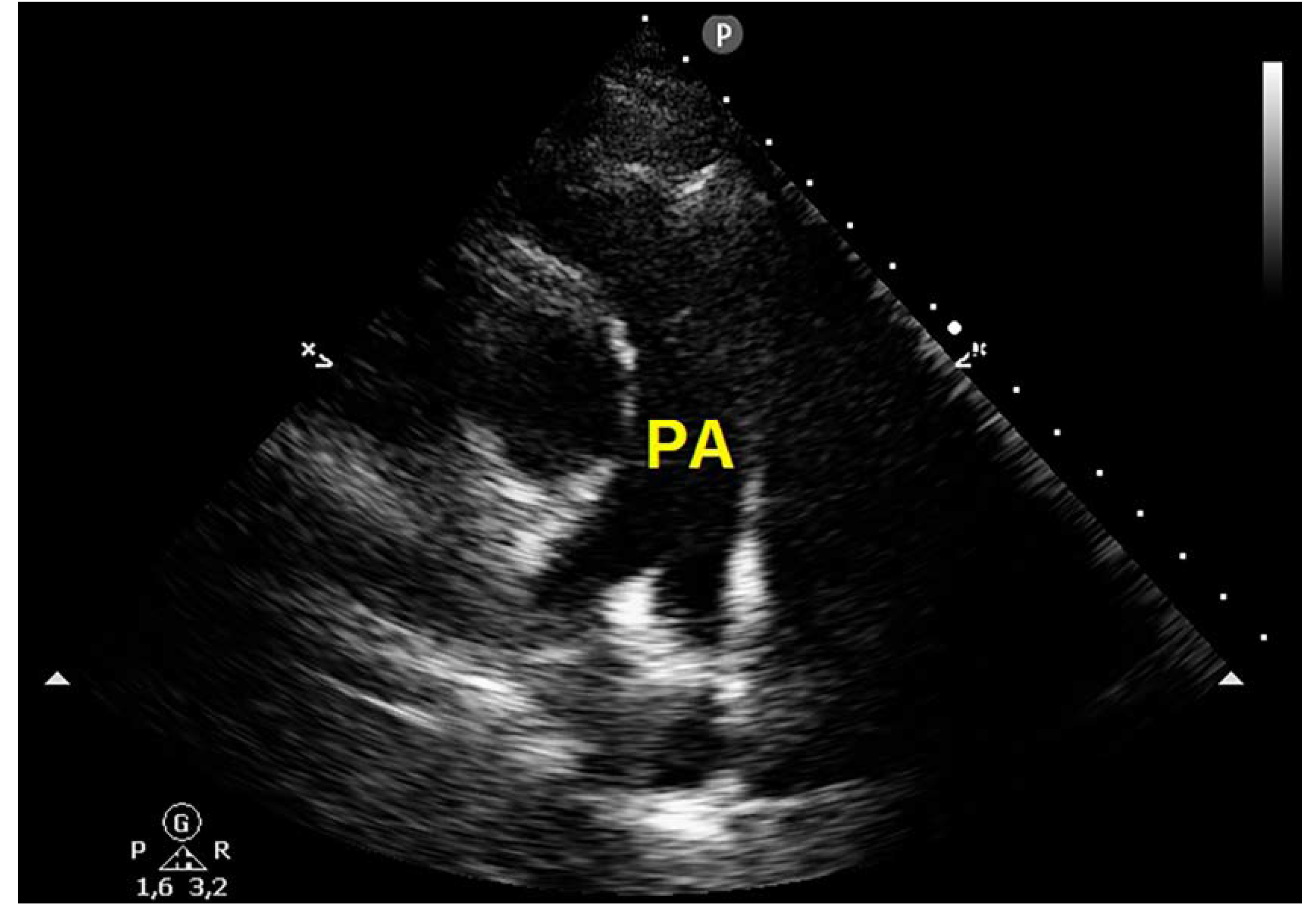

Table 1.
Biochemical parameters recorded at hospital admission and discharge. aPTT, activated partial thromboplastin time; BNP, brain natriuretic peptide; CRP, C-reactive protein; Hb, hemoglobin; HCT, hematocrit; INR, international normalized ratio; NLR, neutrophil-to-lymphocyte ratio; PLTs, platelets; PT, prothrombin time; WBC, white blood count.
Table 1.
Biochemical parameters recorded at hospital admission and discharge. aPTT, activated partial thromboplastin time; BNP, brain natriuretic peptide; CRP, C-reactive protein; Hb, hemoglobin; HCT, hematocrit; INR, international normalized ratio; NLR, neutrophil-to-lymphocyte ratio; PLTs, platelets; PT, prothrombin time; WBC, white blood count.
| Biochemical parameters | Hospital admission | Hospital discharge |
|---|---|---|
| Hb (g/dl) | 13.5 | 12.8 |
| HCT (%) | 42 | 39 |
| WBC (x 109/L) | 12.3 | 6.9 |
| NLR | 7.8 | 1.5 |
| PLTs (x 109/L) | 198 | 281 |
| Creatinine (mg/dl) | 0.8 | 0.9 |
| CRP (mg/dl) | 2.9 | 0.2 |
| D-dimer (ng/ml) | 9546 | 1763 |
| Troponin I (ng/ml) | 0.07 | 0.02 |
| BNP (pg/ml) | 19 | 6 |
| PT (sec) | 11 | 12.5 |
| aPTT (sec) | 23.4 | 19.5 |
| INR | 1.0 | 1.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



