
Submitted:
19 April 2023
Posted:
24 April 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
(1) Background: The prevalence of SARS-CoV-2 infection among healthcare workers (HCWs) in Poland is not exactly known. This study aims to present secondary epidemiological data identifying the scale of the spread of novel coronavirus infection in selected professional groups of HCWs in Poland. (2) Methods: The secondary epidemiological data included both the number of infections and the number and percentages of deaths in individual occupational groups, which occurred throughout the observation period, both in the country and in individual voivodeships. (3) Results: The prevalence of SARS-CoV-2 infections among HCWs was 16.48%. The highest percentage of infected concerned laboratory scientists (21.62%) and paramedics (18%). The highest frequency of infections among HCWs occurred in the province of Zachodnio-Pomorskie (18.9%). Due to COVID-19, 558 healthcare workers died during the analysed period, mostly nurses (n=236) and doctors (n=200). The results regarding the vaccination coverage of HCWs against COVID-19 indicate the highest percentage of vaccinated were among doctors (83.63%) and the smallest among physiotherapists (38.2%). (4) Conclusions: In general, the percentage of infections was high in Poland during the pandemic (16.48%). Significant territorial differences were observed in the frequency of infections, deaths, and percentage of vaccinated workers in individual voivodeships.
Keywords:
COVID-19
; healthcare workers
; pandemics
; SARS-CoV-2
; vaccination coverage
1. Introduction
The prevalence of SARS-CoV-2 infection among healthcare workers (HCWs) in Poland is not exactly known. So far, attempts to determine the number of infected HCWs have been limited to estimating the incidence based on cross-sectional studies, often single-centre [1,2,3]. Naturally, the infection rate was related to the period of observation in a particular phase of the epidemic. According to data from other centres, the average incidence was 8.5% in the initial phase of the pandemic in Europe (2020) [4], and in Poland, the value determined based on a multi-centre study was 25.2% in 2021 [5].
In February 2022, the Ministry of Health announced that the number of infected medics since the beginning of the pandemic was over 200,000 [6]. Despite the data provided by the Ministry on the number of infections among HCWs since September 2020 [7], a separate register enabling the analysis of the necessary epidemiological data in individual professional groups was implemented in Poland only in January 2021. Earlier information on the scale of infections among HCWs was incomplete and concerned only with selected medical professions [8,9]. Data collected from 1st January 2021, allows for more accurate tracking of both the number of infected and deceased medical workers, as well as the percentage of fully vaccinated HCWs in our country, depending on the region.
Knowing the prevalence of novel coronavirus infections among HCWs has a huge impact on maintaining the quality of healthcare during the epidemiological crisis that the COVID-19 pandemic has become. Infections of people working in the health care system directly affect, among others, absenteeism at work (nationally, an increase from 5.6% in 2019 to 9.3% in 2020) [10], which causes an increase in the workload of staff performing their professional duties, results in longer waiting times for scheduled diagnostic appointments and treatment procedures and worsens the quality of care provided to patients, also for COVID-19 [10,11,12].
This study aims to present secondary epidemiological data identifying the scale of the spread of novel coronavirus infection in selected professional groups of HCWs in Poland.
2. Materials and Methods
Secondary epidemiological data provided by the e-Health Centre, a unit subordinate to the Ministry of Health, was obtained for the study [13]. The data included both the number of SARS-CoV-2 infections registered among HCWs and the number of deaths, as well as the number of doses of COVID-19 vaccinations. The data obtained included the employee's occupational group, place of employment in the individual voivodeships, and the month in which the infection or death occurred. In addition, the number of vaccinations performed in individual occupational groups in all voivodeships was analysed. The observation period covered the time from January 2021 to July 2022. The data embraced particular categories of medical professions, including the following: doctor, nurse, paramedic, laboratory scientist, dentist, pharmacist, physiotherapist, and midwife.
After organizing the collected data, the numbers of first-time and all infections as well as deaths in individual occupational groups, which occurred throughout the observation period, both in the country and in individual voivodeships, were summed up. Then, taking into account the data identifying the number of medical employees authorized to practice [14], the percentages of first-time infected staff and all other employees of selected occupational groups (doctors, dentists, nurses, midwives, laboratory diagnosticians, and pharmacists) were calculated. Concerning the group of paramedics, the source data only present the number of people working in the State Medical Rescue System, so in the absence of more precise data, this number was adopted as the official number of paramedics employed in our country (as a denominator). Similarly, in the group of physiotherapists, we only have access to the number of physiotherapists employed in the public health care system [14]. Considering the large number of specialists in this professional category working outside public health care units, it was decided that the data of the National Chamber of Physiotherapy should be used to determine the percentage of infections in this group (as a denominator) [15].
To determine the percentage of deceased employees in particular occupational groups, the infection fatality rate (IFR) was calculated. This coefficient represents the percentage of deaths in the group of all infected people [16], the values were determined for separate professional categories.
At the same time, data were obtained on the number of vaccinations against COVID-19 in individual professional groups in all voivodeships in subsequent months, starting from December 2020 (the beginning of the vaccination campaign) until July 2022. Although these data identify the number of vaccination doses, there is no information on how many employees were vaccinated. In addition, accounting for the considerable dynamics of changes in the availability of subsequent vaccines and a different vaccination schedule, including the introduction of a single-dose vaccine in April 2021 [17] and the possibility of performing another (booster) vaccination from September 2021, the following procedure was adopted to calculate the percentage of staff vaccination status. The number of vaccination doses performed, reported from December 2020 to April 2021, was divided by two due to the availability of two doses of preparations for one employee in the period under review. It was assumed that this is the number appropriate for determining the percentage of vaccinated employees in particular occupational categories and entitled to receive vaccination by the rules in force at the time [18].
Due to the scope of available data (cumulative number of vaccinations performed, without considering the dose number or the name of the preparation), the authors refrained from attempting to interpret the vaccination status of individual professional groups in terms of booster doses.
Descriptive statistics methods were used in the data analysis. The number and percentages of staff infected with SARS-CoV-2, the IFR rate, and the percentage of those vaccinated with two doses in the individual voivodships, with the separation of the professional category, were presented. The capabilities of Microsoft Office Excel 4.0 software were used, and QGIS 3.16 was used for map construction, license: GNU GENERAL PUBLIC LICENSE, Copyright (C) 1989, 1991 Free Software Foundation, Inc.
3. Results
During the analysed period, from 1st January 2021 to 30th June 2022, a total of 114,213 SARS-CoV-2 infections were registered in Poland among HCWs, which accounted for 16.48% of all employees authorized to practice at that time. It is worth noting that the vast majority of infections were first-time infections (n=98,896; 86.59% of all notifications).
Similarly, to the general population, the occurrence of an increased number of infections among HCWs was influenced by the period of increased virus infectivity. In each phase of the epidemic, we were dealing with a slightly different predominance of mutations responsible for most infections with subsequent variants of the SARS-CoV-2: by June 2021 - alpha variant, by January 2022 - delta variant, by the end of February 2022 omicron BA.1 and by the end of June 2022 - Omicron BA.4 [19]. Representatives of medical professional groups were infected most frequently in January and February 2022. More than 25,000 HCWs became infected in these two months (Figure 1).
The percentage of infected HCWs in particular professional categories varied, with the highest among laboratory scientists (21.62%), paramedics (18.34%), and nurses (18.07%). The smallest percentage of infected with coronavirus was registered at dentists (8.62%). The full list of values describing the percentage of infected HCW in the individual professional categories by voivodeships is presented in Table 1.
Figure 2 shows a sample map identifying regional differences in the percentage of infected physicians. The highest values were recorded in the voivodeships: Zachodniopomorskie (18.9%), Warmińsko-Mazurskie (18.2%), and Kujawsko-Pomorskie (18.5%). The smallest percentage of infected doctors was observed in the voivodeships of Podkarpackie (12.2%), Dolnośląskie (12.92%), Małopolskie (12.96%), and Śląskie (13.0%). The highest number of recurrent SARS-CoV-2 infections concerned HCWs from the Kujawsko-Pomorskie Voivodeship, while the lowest percentage of recurrent infections was recorded in Małopolska.
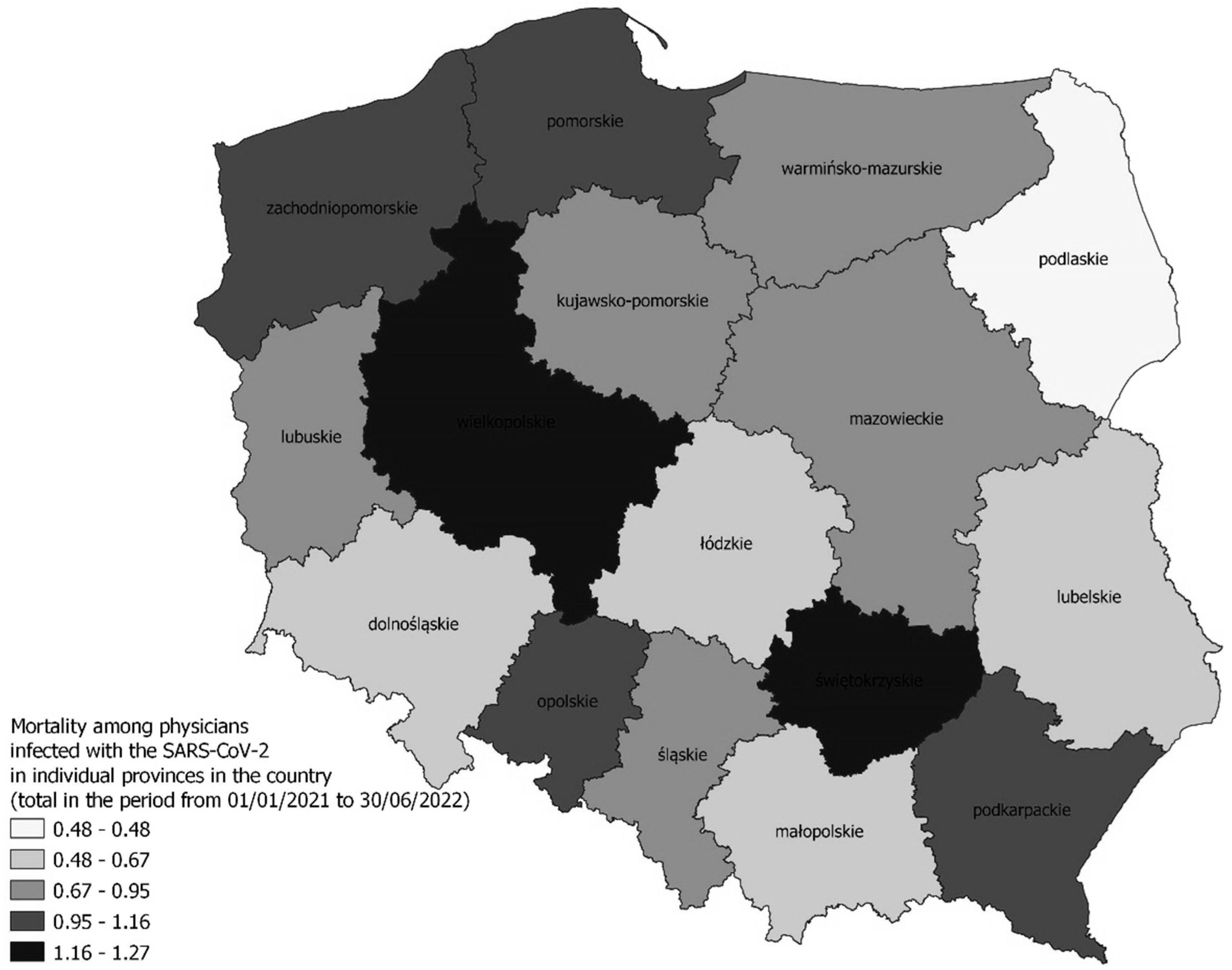
Due to COVID-19, 558 HCWs died during the analysed period, of which the largest group were nurses (n=236) and doctors (n=200). However, the highest infection mortality rate (IFR) concerned a group of dentists (1.45%). The lowest IFR rate concerned physiotherapists (0.06%). Detailed data on the differences in the IFR rate depending on the professional group and voivodship are presented in Table 2. Figure 2, in turn, presents a map of the percentage of registered deaths among infected physicians.
Figure 3.
Mortality among physicians infected with the SARS-CoV-2 in individual provinces in the country (total in the period from 01/01/2021 to 30/06/2022).
Figure 3.
Mortality among physicians infected with the SARS-CoV-2 in individual provinces in the country (total in the period from 01/01/2021 to 30/06/2022).
The results regarding the vaccination status of HCWs against COVID-19 indicate that during the period from December 2020 to March 2021, medical doctors were the group with the highest percentage of vaccination (83.63%) and the smallest were physiotherapists (38.2%). Detailed data in this regard, including voivodeships, is presented in Table 3. In turn, Figure 4 presents regional differences in the percentage of vaccinated doctors.
4. Discussion
In September 2021, the World Health Organization estimated that, by May 2021, between 80,000 and 180,000 HCWs died of COVID-19 [20]. At the same time, it was possible to determine, based on data from 119 countries, that by September 2021, about 40% of HCWs had been vaccinated against the disease [20]. However, due to the lack of accurate reports and the reluctance of some countries to publish accurate summaries [4], it is difficult to verify the above estimates. A local, multi-centre study conducted in Poland indicated that the percentage of infections in the group of HCWs was 25.2% [5]. At the same time, a seroepidemiological study conducted in the Upper Silesian agglomeration in the first phase of the epidemic (until the end of 2021) indicated that the probable infection rate of HCWs was in the range of 16.1% - 22.5% [3]. The results collected from the officially functioning register and presented in this paper show significant differences concerning the data from other research centres. In general, it can be seen that the percentage of infected HCWs in other countries did not significantly exceed 10% [21]. However, the cited data are most often derived from cross-sectional studies, and the percentages of infections given in them are the result of estimations. The approximate similar percentage of SARS-CoV-2 infections among HCWs to that calculated by us in the presented work was revealed in a study from Malaysia in 2021. The percentage of infected HCWs was 17.4% in their research which was similar to our study, at the same time paramedics were most often infected as well (68.4%) [22].
The risk of SARS-CoV-2 infection in HCWs is higher than the risk observed in the general population, but it is worth noting that it varies within medical and healthcare professions and the exact workplace, including the nature of the ward [23,24]. An analysis of data on medical personnel in Canada indicates that people employed in healthcare facilities accounted for 7% of all infected. At the same time, women and younger people employed in healthcare were more likely to suffer from COVID-19 than in the general population, and the risk of hospitalization and death was lower in this group than in the general population [25].
The results of another international study confirmed that declarations of HCWs regarding sufficient preparation for work in a pandemic more often concerned nurses than physicians, and at the same time more often men than women [26]. Despite the satisfactory results of this self-assessment, nurses in Poland were infected more often than medical doctors, which was reflected in the data presented in our study. Probably, the different nature of work with patients, as well as the frequency and length of contact with patients, are important factors for the observed variation in the percentage of coronavirus infections among HCWs [21,24]. The longer procedures and the nature of the care specific for paramedics or nurses mean that the percentage of infected in these groups observed in the registers was higher than, for example, recorded in medical doctors. It is worth emphasizing here that the high frequency of SARS-CoV-2 infections in the groups of paramedics and nurses does not correspond to the highest percentage of deaths in the infected, respectively IFR = 0.11% for paramedics and IFR = 0.42% in the group of nurses. The highest percentage of deaths among infected employees concerned dentists (IFR=1.45%) and doctors (IFR=0.85%). This is a hard-to-explain observation based on secondary epidemiological data and a descriptive type of study. One of the possible hypotheses could be justified based on the relatively high percentage of older age (over 65) current physicians in Poland. Similar conclusions were drawn during the analysis of international data from the beginning of the COVID-19 pandemic, where more frequent deaths were recorded among male doctors and other HCWs, indicating their advanced age [24]. It is obvious that the risk of chronic diseases increases with age [27] and comorbidity is very common [28]. As demonstrated in previous publications, the risk of death in patients with COVID-19 increases with comorbidity [29,30]. In our study, the average IFR value for all analysed professional groups was 0.48%, which is important, the average mortality rate reported in HCWs from 37 countries was at a similar level, i.e., 0.05 per 100,000 [31]. Unfortunately, the lack of relevant data in the register identifying the age of individual HCWs or their current health status (information on diagnosed diseases) makes it impossible to unequivocally assess the issue raised.
The level of vaccination against COVID-19 in the group of HCWs in Poland in the initial period of vaccination availability was not too high and amounted to 61.48% (detailed data are presented in Table 3). Such a low level of vaccination was not due to the lack of availability of the vaccine but was rather the result of employees' limited trust in the preparations used for vaccination against COVID-19 [32]. The greatest objections were declared by nurses, in the Linder-Pawłowicz study, 64.7% of surveyed physicians and 63.7% of medical students, and only 34.5% of nurses indicated trust in vaccination, while 46.6% of nurses and 40% of pharmacists did not have trust [33]. In our study, the lowest vaccination status against COVID-19 in the initial phase of vaccination availability was observed in the group of physiotherapists (38.2%). This is an important observation, especially since the results of a seroepidemiological study in Great Britain confirmed that the greatest risk of SARS-CoV-2 infection concerned physiotherapists (OR 2.78; 95% CI: 1.21 - 6.36) [34]. Their professional contact most often involves the care of elderly patients, often with multiple comorbidities, so it is worth including these issues in the training programs of future specialists. The low percentage of vaccinated employees in our study also concerned nurses (54.5%) and midwives (54.4%). The highest percentage of vaccinated HCWs was recorded in the group of medical doctors (83.63%), although some territorial variability of the indicator in individual voivodeships can be noticed. The worst situation in this respect was in the Podlaskie voivodeship (79.47%). It is worth adding here that also in other countries worldwide, physicians are the group of HCWs that most favours the obligation to vaccinate against COVID-19 [23,34,35].
In conclusion, it should be noted that in comparison to data from other research centres in various countries, the prevalence of SARS-CoV-2 infection in Poland was quite high. As for the COVID-19 vaccination prophylaxis, it was confirmed that the percentage of vaccinated HCWs differs in individual occupations, with doctors among the most frequently vaccinated.
A certain limitation of the study is the secondary nature of the analysed data and their scope. The data relate to the period of 18 months of the pandemic, and their arbitrary, rather simplified nature does not allow for conclusions about infection risk factors apart from variables related to the profession and place of work (voivodeship). Moreover, it is difficult to indicate the exact percentage of infected individuals in selected professional groups because there is no precise register of the number of persons authorized and performing particular medical professions in our country, hence the calculated values may slightly differ from the actual percentage of infected persons. However, it was recognized that the presented results may be a form of supplement to the gap resulting from the lack of more reliable data in Poland.
5. Conclusions
The percentage of SARS-CoV-2 virus infections among HCWs in general during the pandemic in Poland was high and amounted to 16.48%. Laboratory scientists, paramedics, and nurses were most often infected medical staff. The highest percentage of deaths was recorded in the professional group of dentists. Physicians accounted for the largest percentage of medical workers vaccinated against COVID-19. Significant territorial differences were observed in the frequency of infections, the percentage of deaths, and the percentage of vaccinated HCWs in individual voivodeships.
Author Contributions
Conceptualization, M.W. and M.K.; methodology, M.K.; software, E.N.; formal analysis, M.W. and E.N.; investigation, M.W.; resources, M.W. and M.K.; writing—original draft preparation, M.W.; writing—review and editing, M.K.; visualization, E.N.; supervision, E.N.; project administration, M.W.; funding acquisition, M.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The APC was funded by Medical University of Silesia (No. PCN-1-212/N/2/I; to MK).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data available on request. The data presented in this study are available on request from the corresponding author. The data are not publicly available due to its receiving from the “e-Health Centre” database in response to personal request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sierpiński R, Pinkas J, Jankowski M, Juszczyk G, Topór-Mądry R, Szumowski Ł. Occupational risks for SARS-CoV-2 infection: The Polish experience. Int J Occup Med Environ Health. 2020;33(6):781-789. [CrossRef]
- Wojczyk M, Kowalska M. Prevalence of SARS-CoV-2 infection and risk factors in health care workers. Przegl Epidemiol. 2020;74(4):606-619. [CrossRef]
- Wojczyk M, Kowalska M. [The frequency of positive results of serological tests against SARS-CoV-2 in healthcare workers in Upper Silesia Metropolitan Area, Poland]. Med Pr. 2022;73(2):125-133. [CrossRef]
- Galanis P, Vraka I, Fragkou D, Bilali A, Kaitelidou D. Seroprevalence of SARS-CoV-2 antibodies and associated factors in healthcare workers: A systematic review and meta-analysis. J Hosp Infect. 2021;108:120-134. [CrossRef]
- Rosińska M, Stępień M, Kitowska W, Milczarek M, Juszczyk G, Nowacka Z et al. Healthcare workers highly affected during the COVID-19 epidemic wave in Poland prior to vaccination availability: Seroprevalence study. Medycyna Pracy. 2022;73(2):109-123. [CrossRef]
- Puls Medycyny [Internet]. Warsaw: The Media; 2022 [cited 2022 Dec 21]. [Deaths of medics suffering from COVID-19 in Poland: 304 doctors and 257 nurses died]. Available from: https://pulsmedycyny.pl/zgony-medykow-chorych-na-covid-19-w-polsce-zmarlo-304-lekarzy-i-257-pielegniarek-1142088. Polish.
- Medonet [Internet]. Warsaw: The Media; 2020 [cited 2022 Dec 21]. [How many Polish doctors died of COVID-19? The Ministry of Health has provided the latest data]. Available from: https://www.medonet.pl/koronawirus/koronawirus-w-polsce,koronawirus-w-polsce--zakazenia-wsrod-personelu-medycznego,artykul,20972022.html#:~:text=Poprzednie%20dane%20dotycz%C4%85ce%20zaka%C5%BCe%C5%84%20koronawirusem%20SARS-CoV-2%20u%20personelu,lekarzy%2C%2018%20495%20piel%C4%99gniarek%20oraz%201%20644%20po%C5%82o%C5%BCne. Polish.
- [Response of the Ministry of Health to parliamentary question No. 4302 of July 20, 2020]. Available from: https://orka2.sejm.gov.pl/INT9.nsf/klucz/ATTBRXDEH/%24FILE/i04302-o1.pdf. Polish.
- Puls Medycyny [Internet]. Warsaw: The Media; 2022 [cited 2022 Dec 21]. [Ministry of Health: 43 doctors and 32 nurses - so many doctors died due to SARS-CoV-2 infection]. Available from: https://pulsmedycyny.pl/ministerstwo-zdrowia-43-lekarzy-i-32-pielegniarek-tylu-medykow-zmarlo-z-podowu-zakazenia-sars-cov-2-1102302. Polish.
- [Information on the results of the audit of the Supreme Audit Office: Functioning of hospitals in the conditions of the Covid-19 pandemic; KZD.430.006.2021; Reg No. 154/2021/P/21/055/KZD]. Available from: https://www.nik.gov.pl/plik/id,26701,v,artykul_25465.pdf. Polish.
- Labrague LJ, de Los Santos JAA. Resilience as a mediator between compassion fatigue, nurses' work outcomes, and quality of care during the COVID-19 pandemic. Appl Nurs Res. 2021;61:151476. [CrossRef]
- von Vogelsang AC, Göransson KE, Falk AC, Nymark C. Missed nursing care during the COVID-19 pandemic: A comparative observational study. J Nurs Manag. 2021;29(8):2343-2352. [CrossRef]
- Polityka Zdrowotna.com [Internet]. Warsaw: The Media; 2020 [cited 2022 Dec 19]. [How does the Ministry of Health collect data on the epidemic?]. Available from: https://politykazdrowotna.com/artykul/jak-mz-zbiera-dane-dotyczace-epidemii/828545. Polish.
- Ministry of Health [Internet]. Warsaw: The organization; 2022 [cited 30 Dec 2022]. [Statistical Bulletin of the Minister of Health 2022]. Available from: https://ezdrowie.gov.pl/portal/home/badania-i-dane/biuletyn-statystyczny. Polish.
- National Chamber of Physiotherapists [Internet]. Warsaw: The Organization; 2022 [cited 30 Dec 2022]. [Number of physiotherapists in regions]. Available from: https://kif.info.pl/regiony/. Polish.
- Zejda JE, Kowalska M, Brożek GM, Barański K, Kaleta-Pilarska A. [Infection fatality rate (IFR) during the course of COVID-19 pandemic in Upper Silesia Metropolitan Area (Poland) in 2020]. Med Pr. 2021;72(6):671-676. [CrossRef]
- Medonet [Internet]. Warsaw: The Media; 2021 [cited 2022 Dec 30]. [COVID-19 vaccine Johnson&Johnson. The most important information]. Available from: https://www.medonet.pl/porozmawiajmyoszczepionce/szczepionka-na-covid-19,szczepionka-na-covid-19-johnson-johnson--najwazniejsze-informacje,artykul,27115900.html. Polish.
- [Announcement No. 12 of the Minister of Health on vaccination against COVID-19 with a booster dose and an additional dose supplementing the basic scheme of September 28, 2021]. Available from: https://www.gov.pl/web/zdrowie/komunikat-nr-12-ministra-zdrowia-w-sprawie-szczepien-przeciw-covid-19-dawka-przypominajaca-oraz-dawka-dodatkowa-uzupelniajaca-schemat-podstawowy. Polish.
- Our World in Data [Internet]. Oxford: The Organization; 2022 [cited 8 Jan 2022]. COVID-19 Data Explorer. Available from: https://ourworldindata.org/explorers/coronavirus-data-explorer.
- World Health Organization [Internet]. Geneva: The Organization; 2021[cited 2022 Dec 30]. Health and Care Worker Deaths during COVID-19. Available from: https://www.who.int/news/item/20-10-2021-health-and-care-worker-deaths-during-covid-19.
- Smallwood N, Harrex W, Rees M, Willis K, Bennett CM. COVID-19 infection and the broader impacts of the pandemic on healthcare workers. Respirology. 2022;27(6):411-426. [CrossRef]
- Ramli NS, Fauzi MFM, Moktar NMA, Hajib N, Nawi AM. Prevalence, characteristics, and predictors of healthcare workers with COVID-19 infection in an urban district in Malaysia. Pan Afr Med J. 2022;41:243. [CrossRef]
- Browne SK, Feemster KA, Shen AK, Green-McKenzie J, Momplaisir FM, Faig W; et al. Coronavirus disease 2019 (COVID-19) vaccine hesitancy among physicians, physician assistants, nurse practitioners, and nurses in two academic hospitals in Philadelphia. Infect Control Hosp Epidemiol. 2022;43(10):1424-1432. [CrossRef]
- Bandyopadhyay S, Baticulon RE, Kadhum M, Alser M, Ojuka DK, Badereddin Y; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob Health. 2020;5(12):e003097. [CrossRef]
- The Government of Canada [Internet]. Ottawa: The Government; 2022 [cited 30 Dec 2022]. COVID-19 infections among healthcare workers and other people working in healthcare settings. Available from: https://www.canada.ca/en/public-health/services/diseases/coronavirus-disease-covid-19/epidemiological-economic-research-data/infections-healthcare-workers-other-people-working-healthcare-settings.html.
- Huy NT, Chico RM, Huan VT, Shaikhkhalil HW, Uyen VNT, Qarawi ATA; et al. Awareness and preparedness of healthcare workers against the first wave of the COVID-19 pandemic: A cross-sectional survey across 57 countries. PLoS ONE. 2021;16(12):e0258348. [CrossRef]
- Kambhampati AK, O’Halloran AC, Whitaker M, Magill SS, Chea N, Chai SJ; et al. COVID-19–Associated Hospitalizations Among Health Care Personnel — COVID-NET, 13 States, March 1–May 31, 2020. MMWR Morb Mortal Wkly Rep 2020;69:1576–1583. [CrossRef]
- Iaccarino G, Grassi G, Borghi C, Ferri C, Salvetti M, Volpe M; SARS-RAS Investigators. Age and Multimorbidity Predict Death Among COVID-19 Patients: Results of the SARS-RAS Study of the Italian Society of Hypertension. Hypertension. 2020;76(2):366-372. [CrossRef]
- Kowalska M, Barański K, Brożek G, Kaleta-Pilarska A, Zejda Jan E. COVID-19 related risk of in-hospital death in Silesia, Poland. Pol.Arch.Med.Wewn. 2021,131(4):339-344. [CrossRef]
- Mason K.E, Maudsley G, McHale P, Pennington A, Day J, Barr B. Age-Adjusted Associations Between Comorbidity and Outcomes of COVID-19: A Review of the Evidence From the Early Stages of the Pandemic. Front Public Health. 2021, 6;9:584182. [CrossRef]
- Erdem H, Lucey DR. Healthcare worker infections and deaths due to COVID-19: A survey from 37 nations and a call for WHO to post national data on their website. Int J Infect Dis. 2021;102:239-241. [CrossRef]
- Paczkowska A, Hoffmann K, Michalak M, Hans-Wytrychowska A, Bryl W, Kopciuch D; et al. Safety Profile of COVID-19 Vaccines among Healthcare Workers in Poland. Vaccines (Basel). 2022;10(3):434. [CrossRef]
- Lindner-Pawłowicz K, Mydlikowska-Śmigórska A, Łampika K, Sobieszczańska M. COVID-19 Vaccination Acceptance among Healthcare Workers and General Population at the Very Beginning of the National Vaccination Program in Poland: A Cross-Sectional, Exploratory Study. Vaccines (Basel). 2021;10(1):66. [CrossRef]
- Cooper DJ, Lear S, Sithole N, Shaw A, Stark H, Ferris M; CITIID-NIHR BioResource COVID-19 collaboration consortium; Bradley J, Maxwell P, Goodfellow I, Weekes MP, Seaman S, Baker S. Demographic, behavioural and occupational risk factors associated with SARS-CoV-2 infection in UK healthcare workers: A retrospective observational study. BMJ Open. 2022;12(11):e063159. [CrossRef]
- Briko NI, Korshunov VA, Mindlina AY, Polibin RV, Antipov MO, Brazhnikov AI; et al. Healthcare Workers' Acceptance of COVID-19 Vaccination in Russia. Int J Environ Res Public Health. 2022;19(7):4136. [CrossRef]
Figure 1.
Dynamics of changes in the total number of infected healthcare workers in individual months of the study period (January 1, 2021 - June 30, 2022) in Poland.
Figure 1.
Dynamics of changes in the total number of infected healthcare workers in individual months of the study period (January 1, 2021 - June 30, 2022) in Poland.
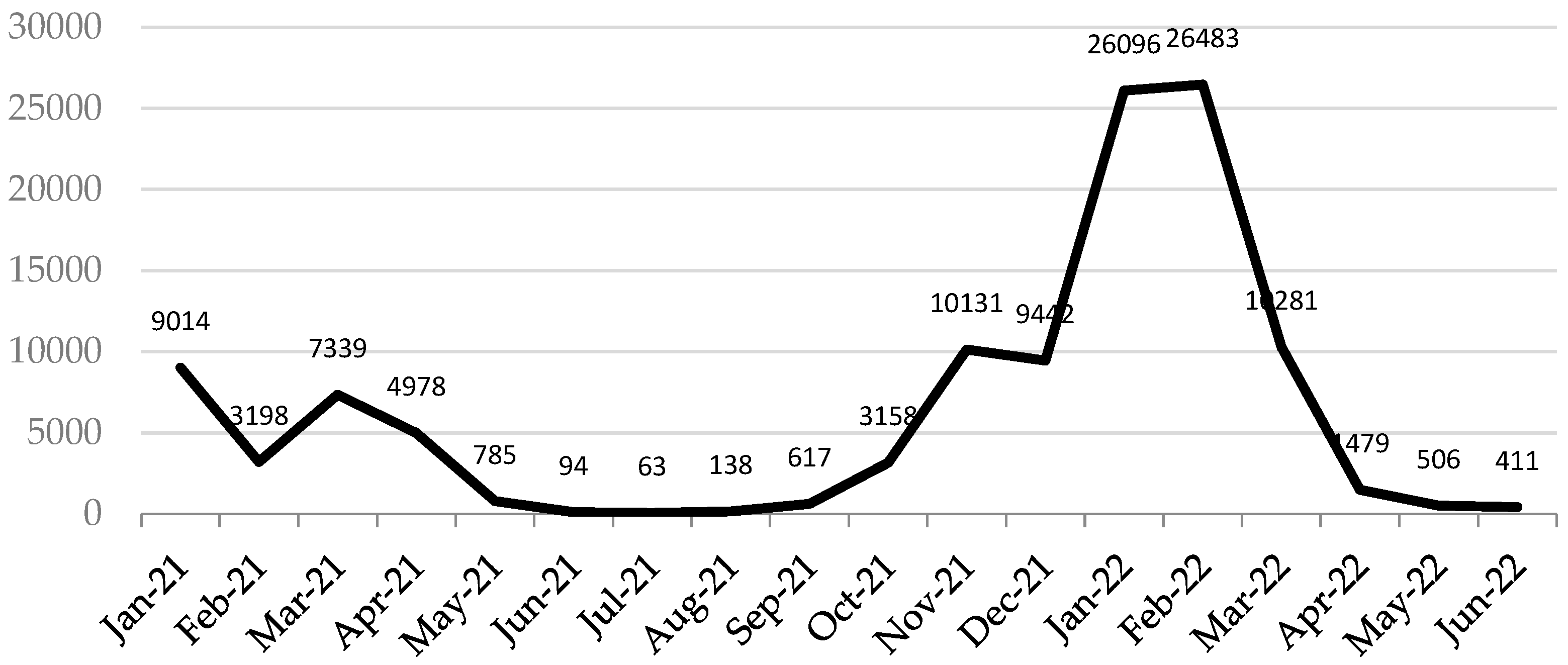
Figure 2.
Percentage of infections among physicians, registered during the period from 01/01/2021 to 30/06/2022 in individual provinces of the country.
Figure 2.
Percentage of infections among physicians, registered during the period from 01/01/2021 to 30/06/2022 in individual provinces of the country.
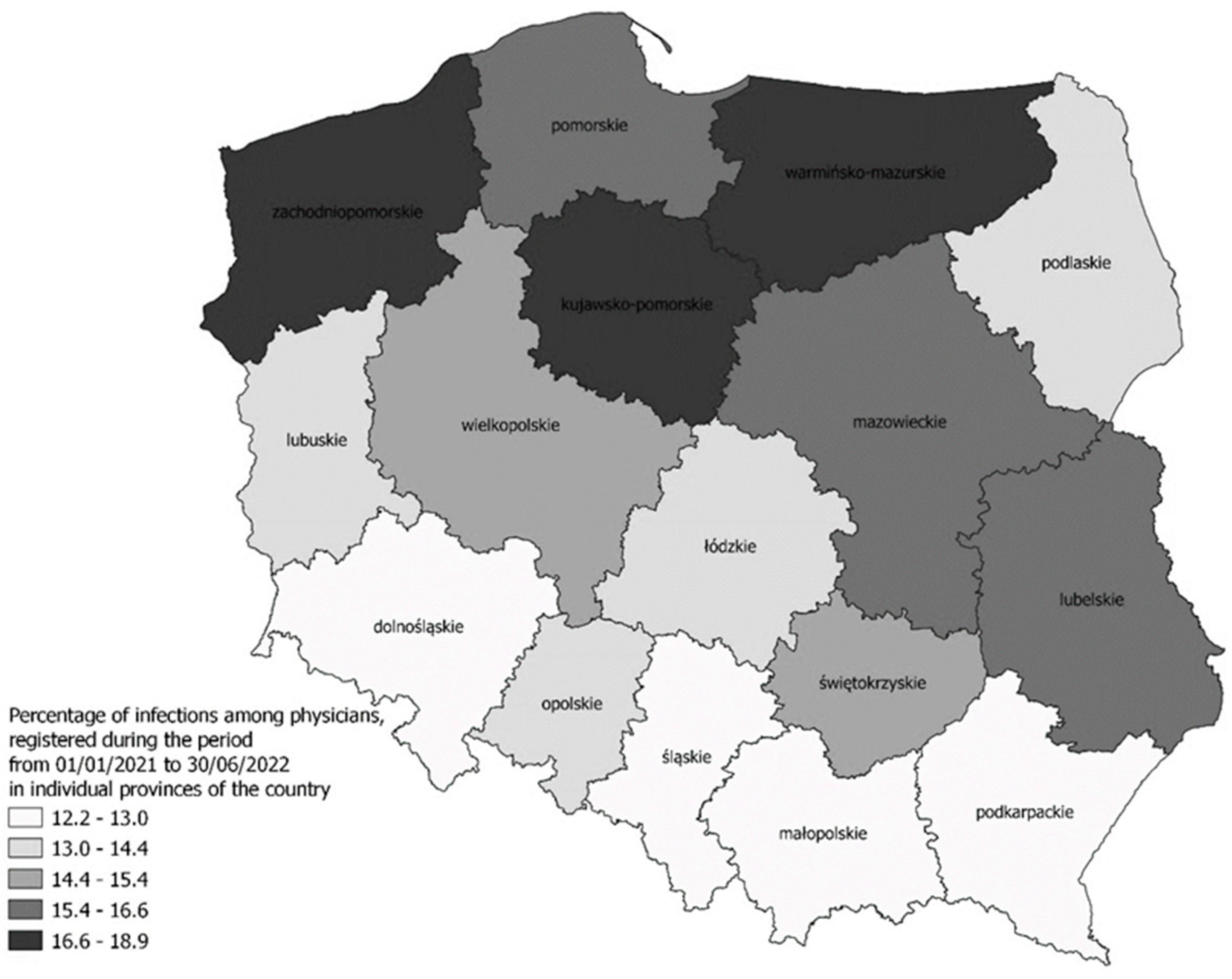
Figure 4.
Percentage of physicians vaccinated against COVID-19 depending on the provinces (status during the period from 12/2020 to 31/03/2021).
Figure 4.
Percentage of physicians vaccinated against COVID-19 depending on the provinces (status during the period from 12/2020 to 31/03/2021).
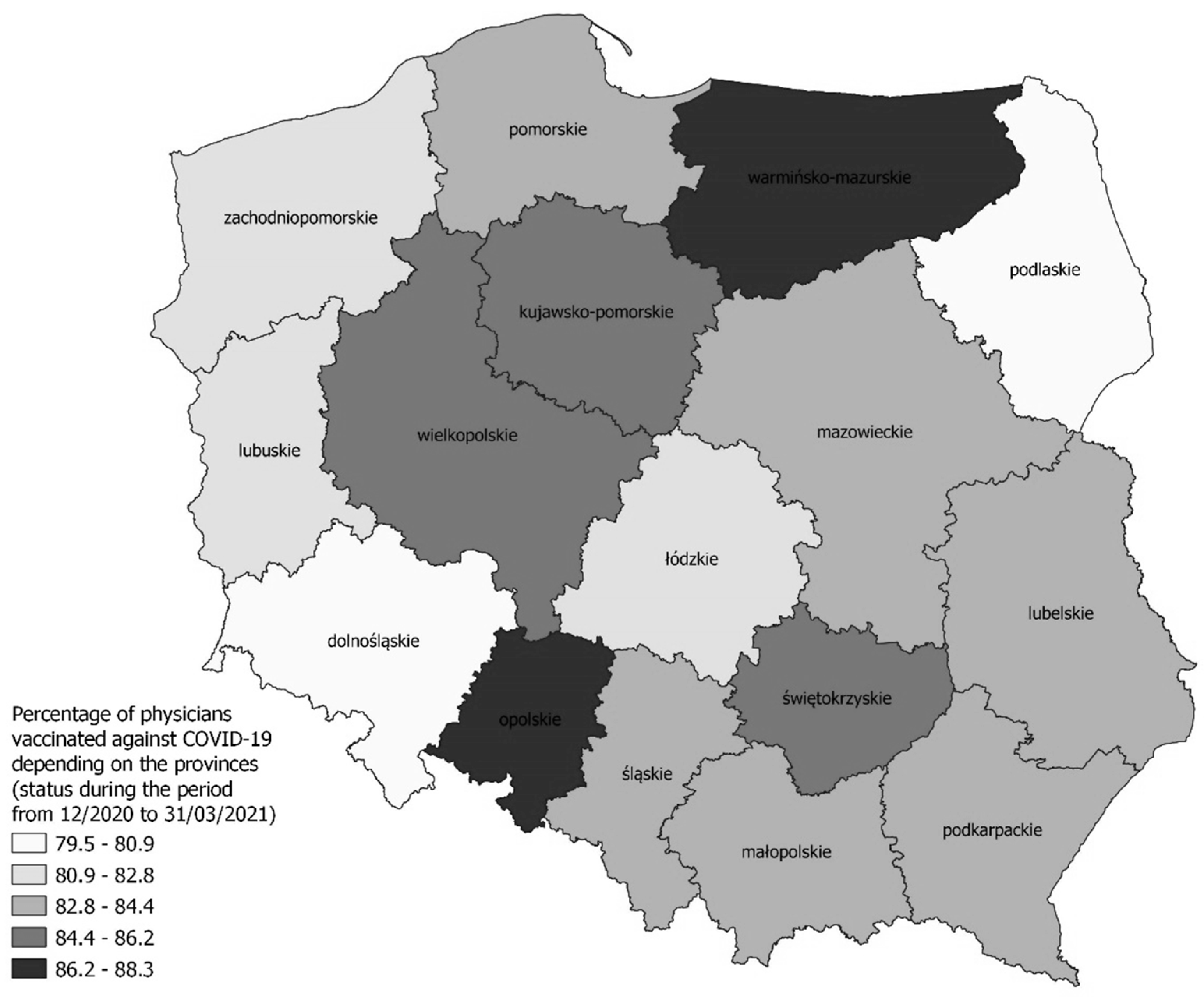

Table 1.
Percentage of SARS-CoV-2 infections among HCWs (in total and first-time) in the individual voivodship (January 1, 2021-June 30, 2022).
Table 1.
Percentage of SARS-CoV-2 infections among HCWs (in total and first-time) in the individual voivodship (January 1, 2021-June 30, 2022).
| Voivodship | Infections | %DOC | %NUR | %PM | %DEN | %LAB | %PHA | %PHY | %MID |
|---|---|---|---|---|---|---|---|---|---|
| Total in country | Generally | 14.99 | 18.07 | 18.34 | 8.62 | 21.62 | 14.44 | 16.92 | 16.84 |
| First-time | 13.12 | 15.18 | 14.91 | 8.19 | 19.40 | 13.56 | 15.11 | 15.05 | |
| Dolnośląskie | Generally | 12.92 | 17.26 | 16.20 | 6.59 | 21.27 | 13.82 | 15.98 | 16.65 |
| First-time | 11.50 | 14.79 | 12.64 | 6.13 | 19.04 | 13.10 | 14.56 | 14.97 | |
| Kujawsko-pomorskie | Generally | 18.55 | 23.25 | 16.12 | 12.47 | 26.00 | 20.41 | 19.37 | 18.74 |
| First-time | 16.19 | 18.95 | 12.00 | 12.06 | 23.07 | 18.05 | 16.70 | 15.85 | |
| Łódzkie | Generally | 13.99 | 17.14 | 24.15 | 8.90 | 19.41 | 14.14 | 15.58 | 16.42 |
| First-time | 12.05 | 14.17 | 17.53 | 8.40 | 18.07 | 13.22 | 14.10 | 14.55 | |
| Lubelskie | Generally | 16.30 | 22.13 | 19.38 | 9.78 | 23.32 | 15.53 | 16.26 | 20.49 |
| First-time | 13.58 | 18.06 | 16.83 | 9.58 | 20.85 | 14.54 | 16.26 | 17.51 | |
| Lubuskie | Generally | 14.14 | 18.55 | 20.95 | 6.65 | 18.43 | 13.98 | 22.02 | 16.93 |
| First-time | 12.69 | 15.74 | 17.06 | 6.32 | 16.08 | 13.40 | 13.68 | 15.45 | |
| Małopolskie | Generally | 12.96 | 15.51 | 13.95 | 7.88 | 17.67 | 13.85 | 14.13 | 14.16 |
| First-time | 12.04 | 13.03 | 12.50 | 7.43 | 16.34 | 13.27 | 12.81 | 13.01 | |
| Mazowieckie | Generally | 16.25 | 18.35 | 23.21 | 9.46 | 22.34 | 16.29 | 18.29 | 16.99 |
| First-time | 14.43 | 15.84 | 19.12 | 9.14 | 20.41 | 15.37 | 16.55 | 15.51 | |
| Opolskie | Generally | 13.79 | 17.96 | 16.46 | 7.76 | 22.18 | 16.72 | 14.97 | 19.22 |
| First-time | 12.23 | 15.15 | 14.71 | 7.51 | 17.41 | 14.81 | 13.35 | 16.90 | |
| Podkarpackie | Generally | 12.25 | 16.04 | 12.13 | 6.03 | 23.16 | 10.65 | 14.60 | 13.81 |
| First-time | 10.14 | 13.36 | 10.50 | 5.73 | 17.34 | 10.29 | 12.95 | 12.62 |
Legend: DEN, dentists; DOC, medical doctors; HCWs, healthcare workers; LAB, laboratory scientists; MID, midwives; NUR, nurses; PHA, pharmacists; PHY, physiotherapists; PM, paramedics.
Table 2.
Percentage of deaths among HCWs infected with the SARS-CoV-2, taking into account the voivodship and professional category.
Table 2.
Percentage of deaths among HCWs infected with the SARS-CoV-2, taking into account the voivodship and professional category.
| Voivodship | % DOC | % NUR | % PM | % DEN | % LAB | % PHA | % PHY | % MID |
|---|---|---|---|---|---|---|---|---|
| Total in country | 0.85 | 0.42 | 0.11 | 1.45 | 0.13 | 0.43 | 0.06 | 0.42 |
| Dolnośląskie | 0.59 | 0.50 | 0.48 | 1.57 | 0.00 | 0.47 | 0.10 | 0.00 |
| Kujawsko-Pomorskie | 0.87 | 0.43 | 0.00 | 3.23 | 0.34 | 0.61 | 0.00 | 0.77 |
| Łódzkie | 0.64 | 0.62 | 0.00 | 0.98 | 0.00 | 0.24 | 0.00 | 0.43 |
| Lubelskie | 0.67 | 0.43 | 0.55 | 2.05 | 0.35 | 0.61 | 0.15 | 0.00 |
| Lubuskie | 0.79 | 0.55 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.67 |
| Małopolskie | 0.60 | 0.19 | 0.00 | 0.64 | 0.00 | 0.42 | 0.09 | 0.81 |
| Mazowieckie | 0.77 | 0.33 | 0.00 | 1.24 | 0.17 | 0.10 | 0.05 | 0.55 |
| Opolskie | 1.10 | 0.64 | 0.00 | 4.92 | 0.00 | 0.00 | 0.00 | 0.55 |
| Podkarpackie | 1.13 | 0.51 | 0.00 | 0.83 | 0.00 | 0.68 | 0.00 | 0.51 |
| Podlaskie | 0.48 | 0.45 | 0.00 | 0.73 | 0.00 | 0.00 | 0.00 | 1.32 |
| Pomorskie | 1.06 | 0.16 | 0.00 | 1.58 | 0.00 | 0.46 | 0.00 | 0.27 |
| Śląskie | 0.94 | 0.55 | 0.00 | 2.00 | 0.26 | 0.67 | 0.07 | 0.39 |
| Świętokrzyskie | 1.27 | 0.51 | 0.00 | 1.37 | 0.00 | 2.50 | 0.24 | 0.48 |
| Warmińsko-Mazurskie | 0.95 | 0.31 | 0.58 | 3.03 | 0.90 | 0.88 | 0.25 | 0.41 |
| Wielkopolskie | 1.19 | 0.52 | 0.00 | 1.22 | 0.00 | 0.41 | 0.00 | 0.28 |
| Zachodniopomorskie | 1.16 | 0.32 | 0.00 | 0.45 | 0.00 | 0.50 | 0.00 | 0.00 |
Legend: DEN, dentists; DOC, medical doctors; HCWs, healthcare workers; LAB, laboratory scientists; MID, midwives; NUR, nurses; PHA, pharmacists; PHY, physiotherapists; PM, paramedics.
Table 3.
Percentage of HCWs vaccinated against COVID-19 during the period from December 2020 to March 31, 2021, data by voivodship.
Table 3.
Percentage of HCWs vaccinated against COVID-19 during the period from December 2020 to March 31, 2021, data by voivodship.
| Voivodship | % DOC | % NUR | % PM | % DEN | % LAB | % PHA | % PHY | % MID |
|---|---|---|---|---|---|---|---|---|
| Total | 83.63 | 54.53 | 63.14 | 70.85 | 65.70 | 61.35 | 38.20 | 54.43 |
| Dolnośląskie | 80.92 | 54.63 | 61.28 | 69.87 | 71.07 | 60.68 | 38.97 | 55.49 |
| Kujawsko-Pomorskie | 86.16 | 62.85 | 51.55 | 76.51 | 66.59 | 74.42 | 48.78 | 61.08 |
| Łódzkie | 82.11 | 56.84 | 67.59 | 67.87 | 61.68 | 57.07 | 39.81 | 53.41 |
| Lubelskie | 83.48 | 52.98 | 60.12 | 71.53 | 59.77 | 73.20 | 32.47 | 51.70 |
| Lubuskie | 82.81 | 58.84 | 71.60 | 71.54 | 67.25 | 72.98 | 39.81 | 56.25 |
| Małopolskie | 83.65 | 53.11 | 63.72 | 71.55 | 65.08 | 57.25 | 35.18 | 51.99 |
| Mazowieckie | 83.53 | 54.74 | 83.27 | 68.23 | 68.10 | 59.15 | 42.08 | 58.43 |
| Opolskie | 87.39 | 55.46 | 60.72 | 77.16 | 62.80 | 77.61 | 36.40 | 50.00 |
| Podkarpackie | 83.49 | 43.68 | 42.26 | 68.60 | 53.09 | 66.45 | 28.63 | 46.72 |
| Podlaskie | 79.47 | 47.35 | 45.74 | 65.60 | 54.61 | 58.58 | 28.79 | 50.17 |
| Pomorskie | 83.48 | 60.38 | 51.83 | 70.31 | 72.35 | 58.51 | 47.64 | 60.78 |
| Śląskie | 84.38 | 49.52 | 62.67 | 72.41 | 65.10 | 56.81 | 36.90 | 48.81 |
| Świętokrzyskie | 85.95 | 55.29 | 71.31 | 71.37 | 59.43 | 67.79 | 35.84 | 51.40 |
| Warmińsko-Mazurskie | 88.26 | 62.78 | 72.96 | 76.89 | 72.15 | 80.13 | 41.11 | 65.19 |
| Wielkopolskie | 85.62 | 59.08 | 77.94 | 74.79 | 72.36 | 61.85 | 38.42 | 57.32 |
| Zachodniopomorskie | 82.45 | 57.95 | 68.32 | 71.14 | 70.05 | 49.54 | 38.99 | 57.84 |
Legend: DEN, dentists; DOC, medical doctors; HCWs, healthcare workers; LAB, laboratory scientists; MID, midwives; NUR, nurses; PHA, pharmacists; PHY, physiotherapists; PM, paramedics.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



