Submitted:
20 April 2023
Posted:
21 April 2023
You are already at the latest version
Abstract
Hashimoto’s thyroiditis (HT) is a gender autoimmune disease that is manifested by chronic inflammation of thyroid. Clinical trial studies (CTSs) use molecular biotechnologies (MB) to approach HT appearance.
Aims of this study was to analyze the applications of MB in CTSs carried out in HT populations (HT-CTSs). Further, to evaluate the role of MB in the context of hygiene hypothesis (HH).
From 75 HT-CTSs found at https://beta.clinicaltrials.gov/ web place, forty-five were considered for this investigation. Finally, six HT-CTSs were reported as molecular HT-CTSs (mHT-CTSs) because of these were planning to utilize MB.
Two of mHT-CTSs were settled on French population to isolate DNA viral sequences. Blood, urine, and thyroid tissues biospecimens were analyzed to pick out parvo and polyoma viruses. Two mHT-CTSs carried out in China, were aimed to identify oral and fecal microbiotas by measuring PCR sequencing of 16S rRNA gene. Two mHT-CTSs were programmed in USA and Greece, respectively, for interception of DNA polymorphisms to associate with genetic susceptibility to HT.
In conclusion, MB are mainly employed in HT-CTSs for infective pathogenesis and genetic fingerprinting of HT. Besides, MB don't prove the evidence of HH; however, they are useful for direct evidence of the presence of viruses.
Keywords:
Hashimoto’s thyroiditis
; molecular biotechnologies
; clinical trials studies
; hygiene hypothesis
; parvoviruses
1. Introduction
Hashimoto’s thyroiditis (HT) is a chronic destructive inflammatory process that develops by autoimmune mechanisms [1]. TH falls within autoimmune thyroid diseases (AIDT) precisely because of inflammatory response to immune alterations [2,3].
Basically, morphological features of HT include four signatures such as lymphoid infiltrates, fibrosis, oxyphilic changes of follicular cells and varying degree of destruction of glandular tissue [4].
Immunological hallmarks of HT enclose serum antibodies raised against various thyroid antigens encompassing from thyroid peroxidase and antithyroglobulin to thyroid-stimulating hormone receptor [5,6]. Morphological and immunological HT traits don’t emerge concurrently. In fact, there is a small proportion of patients that show cytological features of HT whereas thyroid antibodies are low detectable in their serum [7].
Reductions of serum thyroid hormones levels are noted in HT patients: this is in case no glandular cells secrete enough thyroid hormones able to meet the needs of body. However, hypothyroidism (hy-T) is diagnosed based on serum levels of several biochemical markers such as thyroid stimulating hormone (TSH) and other thyroid hormones used to confirm the diagnosis [8,9]. HT hormonal indicators report different degree of hy-T, independently by entity of morphological damages [10]. Therefore, HT may clinically present either by prominent or mild hy-T symptoms [1]. These appear related with atypic activity of muscle and nerve fibers, alteration of glucose-lipid metabolism, cognitive and psychological disorders [11,12,13].
Currently, a biochemical “grading” system is used to identify latent hy-T forms (see Table 1 in Ref. [4]) [4]. Above of all, this system is designed for HT treatment by levothyroxine (L-T4). This system is built by confrontation between serum levels of TSH and free thyroxine (T4). At the time that L-T4 replacement was indicated as the first choice for treatment of hy-T, the method of doing this hormonal comparison became essential. In fact, since 2014 the guidelines of American thyroid Association recommend L-T4 treatment strategy for hy-T forms [14,15,16]. Further, this is in according to nationwide data from the National Health Service in the United Kingdom and European thyroid association, too [17]. However, basic science and clinical evidence are inducing to development investigations on LT4/LT3 combination therapy [18,19]. New data come up about limitations of serum TSH biochemical marker because of it partially reflects total thyroid status [20,21,22]. Lastly, 10–15% of hy-T patients voice their discontent because of L-T4 treatment outcomes [23,24]. In fact, this recent evidence urges to involve in the care of hy-T above all hy-T patients themselves [25,26].
1.1. HT biomarkers and epidemiological data
At large, HT diffusion can be reported by considering two distinct types of serum biomarkers. Firstly, HT epidemiological information can be compiled based on autoimmune biomarkers of thyroid inflammation. Secondly, to archive HT epidemiological data, HT diffusion can be related to biochemical markers of hy-T and then, to onset of hy-T symptoms.
By focusing on serum immunological biomarkers, HT is considered a gender functional disorder [27]. This is because of mechanisms underlying the appearance of autoantibodies [28,29]. In fact, the disruption of immune tolerance is genetically driven [29]. Particularly, HT autoimmune anomalies are genetically based on gender and pre-existing susceptibility individual [28,30,31]. In turns, environment plays a critical role on altered genetic background by doing influence the disease development. [27,31]. Hence, HT is reported in women 10-15 times more often than men by an incidence peak around 30-50 years [32]. Conversely, in men the HT incidence increases with aging and then, incidence peak is reached 10-15 years later [32].
When HT diffusion is related to hy-T incidence, substantial differences emerge between hy-T that spreads in endemic area of iodine deficiency and what goes accompanied by HT. Zimmermann et colleague had already observed that hy-T typically emerges in HT patient independently by iodine nutrition status [33,34]. This is because of hy-T develops even in HT patients living in area with sufficient iodine intake. Instead, when population are resident in iodine-deficient localities, it is quite common to find endemic hy-T [35].
Gender differences come up even when HT is related to onset of hy-T signs and symptoms. In fact, distinctive clinical courses and different outcomes are observed in women in respect with men. Further, difference of gender is a key determinant even in therapeutic responses to L-T4 [27,36]. Usually, hy-T symptoms include fatigue, cold intolerance, and constipation. However, there is a large variation in clinical presentation of symptoms [16].
In women, hy-T develops more frequent at a later age than HT, especially, after 60 years of age [27]. In addition, hy-T symptoms have not determinant role for identification of endocrine disorder. This is because of hy-T symptoms may occur in healthy women subjects, too. Lastly, L-T4 therapy may be associate with residual symptoms despite normal thyroid tests [18,24].
In men, hy-T symptoms that accompany overt HT are more recurrent, last longer and usually less treatable. [27]. Therefore, the presence or absence of symptoms may be contributing factors to identification of hy-T. Lastly, L-T4 therapy is less frequently accompanied by other side effects in men.
1.2. Prevalence of HT diagnoses
The methods used to diagnose HT have a long history related to description of morphological alterations of thyroid gland, recognition of autoimmune pathogenesis and identification of thyroid hormones [4]. For a proper diagnosis of HT, several methods are involved, further, different biomarkers are assessed independently or in combination with each other [4]. Mainly, serum, ultrasound and pathological examinations are considered how HT diagnostic methods [4,32]. Current research has reported the global prevalence of diagnoses of HT according to different diagnostic methods [32]. Moreover, data about the prevalence of methods useful to confirm HT diagnosis have been provided [32]. Therefore, HT is prevalently diagnosed by ultrasonography (13.2%) and pathological examination (12.5%) [32]. When serum autoantibodies profile is considered, the prevalence rate of HT diagnosed stands at 7.8% (see Figure 9 in Ref. [32]) [32]. The combination of two methods, including serum antibody titres and color Doppler ultrasound, is used for HT diagnosed with a prevalence of 10.4% [32]. This prevalence is considerably lower (4.7%) if three methods such as autoantibody titres, color Doppler ultrasonography and fine needle aspiration are associated. To confirm HT diagnosis is prevalently used thyroid tissue alone (14.1%) [32].
1.3. Molecular biotechnologies (MB) and HT
MB are the pivot for new biomedical methodologies because of their capability of revealing molecular pathogenetic pathways as well as genetic susceptibility of population to develop AIDT [6]. Above all now that use of genetic analysis is turning out to be a key tool for clinical genomic investigations owing to its high accuracy, reproducibility, and reliability of results.
The effective clinical application of MB can be assessed in accordance with the advice of qualified clinical trial studies (CTSs) [37]. These investigations are the basis of genomic screenings designed to detect viral genetic material involved in pathogenesis of diseases. That too, but especially CTSs can test how well genomic screenings work to identify susceptibility to develop diseases in subgroups of populations belonging to a specific continent.
Molecular alterations occurring in the context of HT play crucial roles to promote cellular proliferation of both lymphocytes and glandular tissue. Indeed, mucosa-associated lymphoid tissue (MALT) lymphomas can originate to the site of HT [38,39]. On the other hand, it is long since HT is reported concurrent with cancerous follicular lesions such as nodular goiter, adenoma, and carcinoma [39,40,41,42]. MB are currently employed on pathotyping of MALT lymphoma [43,44]. Further, these analyses are applied in dubious diagnoses of thyroid glandular cancerous lesions [45]. Mainly, these are part of thyroid innovative medicine that point trough biomarkers to early molecular diagnose, personalized treatment, prediction of cancerous risk and prognostic information [46].
Two were the main objectives of the study: firstly, to perform a systematic analysis of CTSs conducted on HT populations living at different geophysical latitude (HT-CTSs). This was done to establish the frequency by which these CTSs were concluded in different continents and when they were planned. Secondly, to identify samples in which MB were applied.
Therefore, wide-ranging search was conducted on CTSs provided at https://beta.clinicaltrials.gov/ web site through the files covered by “autoimmune thyroiditis Hashimoto” keywords [47]. To follow, some of these findings were selected as they were referring to HT-CTSs that planned to apply molecular technologies (mHT-CTSs).
In the context of hygiene hypothesis (HH), divergences among geographic diffusion of HT and molecular fingerprint of HT patients were also considered.
Current applications of MB for pathological practices were discussed separately. Mainly, these concerned molecular aspects for diagnosis of malignant thyroid lesions associated with HT.
2. Material and Methods
2.1. Data Sources
A systematic review of CTSs for HT was performed by surveying all results of search for terms “autoimmune thyroiditis Hashimoto” at place namely, “Condition or disease” of https://beta.clinicaltrials.gov/ web site [47].
2.2. Study Selection
A number of 75 CTSs was found for these keywords that included also three synonyms of conditions or disease such as “autoimmune thyroiditis”; “thyroiditis Hashimoto” and “Hashimoto” [47]. Mainly, 29 related terms were found of which ten pertained to “autoimmune thyroiditis” synonym (Hashimoto; thyroiditis autoimmune; Hashimoto Disease; HASHIMOTO THYROIDITIS; Hashimoto's thyroiditis; Hashimoto's Disease; chronic thyroiditis; Hashimotos Disease; Chronic lymphocytic thyroiditis; Lymphocytic thyroiditis); ten to “thyroiditis Hashimoto” (Hashimoto; Hashimoto Disease; Autoimmune Thyroiditis; HASHIMOTO THYROIDITIS; Hashimoto's thyroiditis; Hashimoto's Disease; Chronic lymphocytic thyroiditis; chronic thyroiditis; Lymphocytic thyroiditis; Hashimotos Disease) and nine to “Hashimoto” (Hashimoto Disease; Autoimmune Thyroiditis; HASHIMOTO THYROIDITIS; Hashimoto's thyroiditis; Hashimoto's Disease; Chronic lymphocytic thyroiditis; chronic thyroiditis; Lymphocytic thyroiditis; Hashimotos Disease) [47].
2.3. Inclusion criteria
Two were the inclusion criteria adopted for this investigation. The enrollment of HT patients was designed as the first criteria to select CTSs, whereas the molecular analyses were used as the second.
In the first instance, the above CTSs were scrutinized to enucleate the full set of trials carried on HT population. Secondly, to assess the effective application of MB, “Study Plan” section was analyzed for all CTSs [47]. Here, there were details on how a single CTS was planned and what the study was measuring. Specially, “Outcome Measure” sub-section provided insight into the use of molecular analysis to realize the aim of CTS.
2.4. Exclusion criteria
By reviewing and studying the 75 CTSs, 30 of them were considered irrelevant. Mainly, five CTSs were eliminated from this study because of they did not recruit participants with HT: i.e., HT was an “Medical Subject Headings” term or a collateral effect to a therapy (NCT05077865, NCT04239521, NCT04349761, NCT05680376, NCT03957616).
Twenty-four CTSs remained outside because of these concerned other autoimmune, inflammatory, or lymphocytic diseases (NCT03872284, NCT04823728, NCT05225883, NCT03993262, NCT05177939, NCT04339205, NCT04175522, NCT03530462, NCT03835728, NCT03542279, NCT03004209, NCT05198661, NCT04106596, NCT04708626, NCT01456416, NCT04875975, NCT05280600, NCT05682482, NCT05605223, NCT05503264, NCT03941184, NCT05422664, NCT05711563, NCT05772611).
One’ of CTS was omitted because of “Hashimoto” keyword indicated the location of study (NCT04339127).
2.5. Data Extraction
According to the first inclusion criteria, data extraction was performed. Basically, 45 CTSs were extracted for evaluation and included in this study because of they had effectively investigated on HT populations (Table 1). These HT-CTSs were entered into systematic analysis by evaluating seven variables such as continental and geo-location, start date, primary completion date, completion date, last verified and conclusion of study (Table 1).
2.6. Data Synthesis
According to both inclusion criteria, data were synthetized. Finally, 6 mHT-CTSs were recorded because of they had scheduled to use MB to realize their aims (Table 2). To evaluate each mHT-CTSs, six additional variables were added to previous seven. These were corresponding to: target sequences, analysis, and methods, biospecimen genetic retention and description, type and model of study, time perspective, and enrollment of subjects, respectively. Responsible party and results overview were shown, too (Table 2).
3. Results
3.1. CTSs conducted on HT population.
Forty-five CTSs enrolled HT patients. Thirty-seven of them provided information about geolocations by specifying where studies have been conducted (Table 1). In fact, there were not items in 17.7% of HT-CTSs (Table 1).
HT-CTSs were geographically assigned to four continents with different distribution. Then, 0.04% of HT-CTSs were conducted in Africa, 15.5% in America, 13.3% in Asia and 48.8% in Europe (Table 1).
In Africa, HT-CTSs were planned between 2011-2018. In America, HT populations were listened in CTSs since 2006, whereas, in Asia from 2011 onwards. In Europe, the first CTS on HT population was arranged in 2004 (Table 1).
Both HT-CTSs planned in Africa were completed (Table 1). Out of a total of 7 HT-CTSs mapped in American continent, around 85.7 per cent were completed. Conclusions were found only in one of 6 Asian HT-CTSs (16.6%) and in fourteen of 22 European HT-CTSs (63.6%) (Table 1).
These data indicate HT-CTSs specially provide large amount of information about populations living at European latitude. This is due to the hugest number of planned and concluded HT-CTSs in Europe in respect with other continents.
3.2. Clinical application of MB in HT-CTSs
In the list of mHT-CTSs, six trials were included. Two of them (33.3%) were finalized to display viral sequences. For the four remaining HT-CTSs, two were designed to identify bacteria and two to set genetic polymorphisms to associate with susceptibility for HT (Table 2).
Two DNA viruses were investigated from mHT-CTSs in the French population: these corresponded to parvo and polyoma viruses (Table 2). Both viruses were identified by polymerase chain reaction (PCR) method. Specially, genetic strands of polyomavirus were detected in different biospecimen such as blood, urine, and thyroid tissues. Based on study model, the spread of parvovirus was screened through an observational study (NCT03114267). Conversely, polyoma virus was approached by an interventional CTS (NCT03103776). A cohort model with retrospective analysis was followed for the observational study. Contrariwise, a model of parallel assignment was assigned to interventional HT-CTSs (Table 2). Consequently, both mHT-CTSs were planned to have knowledge about viral pathogenesis of HT by PCR analysis. However, NCT03114267 CTS investigated viral cause and effects by longitudinal analysis that evaluated retrospectively the outcome in HT population. Differently, NCT03103776 CTS investigated viral cause and effects on several populations affected of autoimmune diseases among which also an HT population.
The mHT-CTSs investigating bacteria aimed to identify microbiotas. Oral and fecal microbiota were examined in the Chinese population by measuring PCR sequencing of 16S rRNA gene (Table 1 and Table 2). Human feces were used to pick up microbiota genetic materials for the investigation namely NCT03390582 (Table 2). Both mHT-CTSs were observational studies; however, oral microbiota was evaluated by a case-control study whereas, fecal microbiota through a cohort study (Table 2).
Among mHT-CTSs programmed for interception of HT susceptibility, NCT00958113 investigation was performed in Colorado (USA); whereas NCT02491567 CTS was set for the Greek population (Table 1 and Table 2). DNA was examined on biospecimens such as saliva and blood leucocytes. Both mHT-CTSs pertained to observational, case-control studies with cross-sectional examination.
4. Discussion
HT may appear through different clinical and histological aspects and thus, morphological and serum diagnosis of HT are not interchangeable [4]. In addition, HT may be associated to benign and malignant follicular lesions as well as lymphomatous proliferations [39,42,43]. MB are promising surveying methods to apply on HT population.
Totally, 75 CTSs were examined in this study to assess the effective clinical use of MB for planning of trials. By examination of mHT-CTSs is emerged that MB have been employed for two unique scopes. Firstly, to reveal infective etiopathogenesis of HT; and secondly, to determine molecular fingerprinting of HT in populations. Mostly, in this investigation were isolated four trials in which clinical applications of MB served to display viral or bacterial genomes. This is demonstrating how these methos are functioned properly for exploring the complexity of infective HT pathogenesis.
Viral and bacterial infections are currently involved in HT pathogenesis, by multiple and often intertwined pathways.
Based on the old Th1/Th2 paradigm, the so-called hygiene hypothesis (HH) has been adapted to infective etiology of AIDT at the end of the last century [48,49,50,51]. Briefly, this hypothesis postulates that early infections in childhood protects against establishment of autoimmunity. [48,51,52,53,54]. Further, a reduced exposures to microbial environment in childhood is considered as element conducive to increase of autoimmune diseases in adults [55]. This is because of immune system educated by pathogens exposition may better suppress autoimmunity. However, the extension of HH to support of HT pathogenesis has not reported complete agreement [51].
Closely related to HH there are socio-demographic profiles of HT population, data come from migration survey and biographic info of HT patients.
By different concentrations, HT subjects are geographically distributed on the continental territories. A geographical map created on the bases of demographic observations reveal higher concentrations of HT subjects in Africa and Oceania (Figure 1) [32]. On the bases of socio-demographic observations, two divergent findings have been recorded. In low- and middle-income countries, the highest prevalence of HT patients is found among low-middle-income subjects (11.4%) (see Figure 8 in Ref. [32]) [32]. However, HT patients are prevalently concentrated in high-income countries. [32]. Therefore, the HH pathogenetic concepts can be applied to the last phenomena, whereas the first evidence seems limited only to infectious etiology of HT.
For over fifty years, surveys on transmigration of populations are persistently reporting that subjects migrating from a country with low incidence of autoimmune disorders develop immune-related diseases by the same frequency of the original inhabitants of the host country [52,56,57,58,59,60,61]. These data suggest an environmental effect at beginning of autoimmune diseases.
By reporting biographic info of HT patients, several investigations have focused a surprising association occurring between birth month of individuals and HT. Mostly, HT patients were born in winter and autumn [62]. This data suggests that cold weather protect against TPO-Ab development [63]. Nevertheless, this evidence is consistent with infective etiology of HT due to the abundant spread of infectious agents in winter. Further, these findings support HH because of children born in winter have early exposure to infectious agents facilitating the development of autoimmune disease. However, moving from these premises, it is possible even to affirm that incidence of HT for the individual subject may be predicted based on birthday information. Summing up these phenomena, HH seems jarring with genetic features observed in autoimmune disorders, especially in HT.
Molecular analyses have mapped on the short arm of chromosome 6 (6p) a super-region of 7.6 Mb including the extended major histocompatibility complex (eMHC) [64,65]. This region lengthens telomerically from RPL12P1 to HIST1H2AA and it is composed by six clusters and six super-clusters [65]. At 6p21.3 of eMHC are localized human leukocyte antigen (HLA) genes that are highly polymorphic. HLA expressions are strongly related to infection, immunity, and inflammation [66].
In HT, genetic polymorphisms of HLA changes depending on ethnicity [67]. This is because of different expressions of haplotypes in Caucasians (DR3, DR5, DQ7, DQB1*03, DQw7 or DRB1*04-DQB1*0301) in respect with Japanese (DRB4*0101, HLA-A2, DRw53) and Chinese (DRw9) HT patients [67]. Together, these data suggest that non-genetic factors trigger on onset of autoimmune disorders through an unidentified genetic background that is common to entire HT population. Therefore, among phases composing HT pathogenesis, genetic individual susceptibility enters at a later stage in respect with environment factors.
Genetic disparities of HLA profiles are established through use of molecular techniques. These methods have the advantage of arranging systematically HLA haplotypes by symbols. The complexity of nomenclature of HLA haplotypes has been organized by multiple molecular techniques [68]. The first molecular approach to display HLA alleles concerned application of Sanger sequencing-based typing (PCR-SBT) methods [68]. High-throughput sequencing (HTS) methods, including next-generation "short-read" (NGS) and third-generation "long-read" sequencing methods, are the natural evolution of PCR-SBT. Lastly, Oxford Nanopore Technology MinION is progressively reorganizing the number of HLA alleles [69]. Genotyping investigations on Graves’s disease (GD) have identified novel HLA alleles through high-resolution NGS [70,71]. Further, the use of methods based on machine learning are useful to predict HLA subtypes in GD [72]. These investigations suggest of matching different medical biotechnologies to better explain pathogenetic stages involving HLA haplotypes for development of autoimmune disorders.
By focusing on available molecular sources for CTSs appears that parvo and polyoma viruses were investigated from mCTSs.
The role of viruses in inducing HT has been explored but it is still not completely determined [51,73,74]. New data are coming up about roles of DNA and RNA viruses to trigger HT [75,76,77]. DNA viruses namely, parvovirus 19 (B19V), human hepatitis C virus and human herpes virus-6 have been associated to viral pathogenesis of HT [75,76,77,78,79,80]. Among RNA viruses, human immunodeficiency virus (HIV) has been related with HT as it is able to activate the immune inflammatory response through IL-6 [81,82]. Specially, in HIV patients this cytokine plays an important role by orchestrating the inflammatory cascade associated with HT [82]. The importance of IL-6 has been recognized even in animal model of DNA virus infection. In fact, IL-6 amounts are incremented in lung tissues of naïve Balb/c mice that received parvoviruses [83].
Parvoviruses are widespread in different countries of American, Europe, and Asian continent. [77]. Among DNA viruses, parvoviruses display highest levels of replication and recombination [84]. These viruses can replicate autonomously or conversely, they recombine with a helper-virus to be perpetuated [84]. The International Committee on Taxonomy of Viruses (ICTV) has reported members of Parvovirinae family as small (~20 nm in diameter), icosahedral, non-enveloped viruses that have a small single-stranded DNA of 4–6 kb [85]. In 2020, the Executive Committee of the ICTV has approved a revision for taxonomic of the family Parvoviridae [86]. Although the definition to describe these viruses remained, genetic criteria used to demark members composing this family have been updated. The proposal criteria proceed from discoveries of new members of the family Parvoviridae through application of HTS methods. Basically, the classification based on the association with host has been abandoned because of these viruses infect phylogenetically disparate hosts (see Table 1 in Ref. [86]) [86]. In this family have been incorporated infectious agents for animals showing a host range large. In fact, this is enough vast to include many phyla ranging from primates, mammals, avian species to invertebrates [86]. Beyond this, the family Parvoviridae embraces pathogens for arthropods clades, namely arachnids of Chelicerata, that molecular clock estimates go back to marine fossils of the late Cambrian period [87,88,89]. In 1975, Cossart and colleagues detected for the first-time B19V in serum sample of subject screened for hepatitis B virus [90]. Thirty years later, Allander and colleagues discovered bocavirus 1 (HBoV1) in human sample of nasopharyngeal aspirates belonging to children with respiratory tract infection [91]. B19V1 may cause a widespread and self-limiting infections in children and adults, known as erythema infectiosum or fifth disease [92]. Both, B19V and HBoV1 are pathogens for humans and have been detected in cancerous thyroid cells and HT lesions [75,76,93,94].
B19V and HBoV1 exhibit a particular tropism for nuclear compartment. The host machinery for nuclear import of viral capsid is a critical step in the early phase of infection [95,96,97]. The capsid binding protein namely, cleavage and polyadenylation specificity factor 6 plays a dominant role in directing integration to euchromatin of HBoV1 and lentivirus HIV-1, too [95,96,97]. At later stages of infection, the replication of B19V leads to morphological changes of nucleus. These are due to spatial reorganization of chromatin that appears marginalized to the nuclear periphery by super-resolution microscopic examination [98].
In this investigation, MB have proved their worth for composing the future genetic makeup of individuals suffered from HT. This is because these methodologies were employed to disclose genetic susceptibility for HT in two molecular CTSs. Currently, several microsatellites have been proposed as significant elements to build up the molecular HT phenotypes. Specially, heterozygous genotype Arg/Pro of rs 1042522 located on TP 53 gene, polymorphism of IL-23R gene rs17375018, polymorphisms of IL-6 gene promoter (-572) C/G and IL-6 rs1800795 have been associated with HT susceptibility [99,100,101,102].
With the introduction of precision medicine in 2015, MB are considered instrumental to management of cancerous lesions [103]. Molecular medicine has a key role for diagnosis and treatment of thyroid cancers associated to HT by isolating molecular alterations in histological and cytological samples. On histological fragments, the application of MB concerns the diagnosis of MALT lymphoma that develops around the primary HT alterations (see Table 1 in Ref. [104]) [104]. Genomic dissections of lymphomatous cells are employed to reveal molecular phenotypes of MALT lymphoma.
5. Conclusion
Decades of biomedical research on polymorphisms of HLA have revealed many genetic regions associated with HT. However, epidemiological evidence related to HT diffusion cannot be fully explained by HLA genetic differences. This study sheds a light on the require of new linkage between MB and production of data on demographic events such as births and migrations. This is because HH has not yet been proven, this has been widely criticized but not clearly disproved.
Besides, in HT tissues are detected DNA viruses that cause mild manifestation of inflammatory disease but produce nuclear DNA damages. Therefore, DNA viruses have relevance on HT pathogenesis and would offer important opportunities to develop antiviral strategies able also to treat HT. Mostly, viral infections should be considered in future for the development and refinement of HT therapies to use as an alternative or in conjunction with hormone replacement.
Lastly, MB have enormous potential to promote precision medicine by development of robust biomarkers to use for diagnosis and personalized therapies.
References
- Yoo, W.S.; Chung, H.K. Recent Advances in Autoimmune Thyroid Diseases. Endocrinol Metab 2016, 31, 379. [Google Scholar] [CrossRef] [PubMed]
- Bliddal, S.; Nielsen, C.H.; Feldt-Rasmussen, U. Recent Advances in Understanding Autoimmune Thyroid Disease: The Tallest Tree in the Forest of Polyautoimmunity. F1000Res 2017, 6, 1776. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Ferrari, S.M.; Corrado, A.; Di Domenicantonio, A.; Fallahi, P. Autoimmune Thyroid Disorders. Autoimmunity Reviews 2015, 14, 174–180. [Google Scholar] [CrossRef]
- Trovato, M. A Historical Excursus of Diagnostic Methods for Hashimoto Thyroiditis and Graves’ Disease. Gazz Med Ital - Arch Sci Med 2020, 179. [Google Scholar] [CrossRef]
- Fröhlich, E.; Wahl, R. Thyroid Autoimmunity: Role of Anti-Thyroid Antibodies in Thyroid and Extra-Thyroidal Diseases. Front. Immunol. 2017, 8, 521. [Google Scholar] [CrossRef]
- Bogusławska, J.; Godlewska, M.; Gajda, E.; Piekiełko-Witkowska, A. Cellular and Molecular Basis of Thyroid Autoimmunity. European Thyroid Journal 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Thomas, T.; Sreedharan, S.; Khadilkar, U.N.; Deviprasad, D.; Kamath, M.P.; Bhojwani, K.M.; Alva, A. Clinical, Biochemical & Cytomorphologic Study on Hashimoto’s Thyroiditis. Indian J Med Res 2014, 140, 729–735. [Google Scholar]
- Kahaly, G.J.; Gottwald-Hostalek, U. Use of Levothyroxine in the Management of Hypothyroidism: A Historical Perspective. Front. Endocrinol. 2022, 13, 1054983. [Google Scholar] [CrossRef]
- Okosieme, O.; Gilbert, J.; Abraham, P.; Boelaert, K.; Dayan, C.; Gurnell, M.; Leese, G.; McCabe, C.; Perros, P.; Smith, V.; et al. Management of Primary Hypothyroidism: Statement by the British Thyroid Association Executive Committee. Clinical Endocrinology 2016, 84, 799–808. [Google Scholar] [CrossRef]
- Jordan, B.; Uer, O.; Buchholz, T.; Spens, A.; Zierz, S. Physical Fatigability and Muscle Pain in Patients with Hashimoto Thyroiditis. J Neurol 2021, 268, 2441–2449. [Google Scholar] [CrossRef]
- Lei, Y.; Yang, J.; Li, H.; Zhong, H.; Wan, Q. Changes in Glucose-lipid Metabolism, Insulin Resistance, and Inflammatory Factors in Patients with Autoimmune Thyroid Disease. J Clin Lab Anal 2019, 33. [Google Scholar] [CrossRef] [PubMed]
- Waliszewska-Prosół, M.; Bladowska, J.; Budrewicz, S.; Sąsiadek, M.; Dziadkowiak, E.; Ejma, M. The Evaluation of Hashimoto’s Thyroiditis with Event-Related Potentials and Magnetic Resonance Spectroscopy and Its Relation to Cognitive Function. Sci Rep 2021, 11, 2480. [Google Scholar] [CrossRef] [PubMed]
- Jonklaas, J.; Bianco, A.C.; Bauer, A.J.; Burman, K.D.; Cappola, A.R.; Celi, F.S.; Cooper, D.S.; Kim, B.W.; Peeters, R.P.; Rosenthal, M.S.; et al. Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement. Thyroid 2014, 24, 1670–1751. [Google Scholar] [CrossRef] [PubMed]
- Chaker, L.; Bianco, A.C.; Jonklaas, J.; Peeters, R.P. Hypothyroidism. The Lancet 2017, 390, 1550–1562. [Google Scholar] [CrossRef] [PubMed]
- Chaker, L.; Razvi, S.; Bensenor, I.M.; Azizi, F.; Pearce, E.N.; Peeters, R.P. Hypothyroidism. Nat Rev Dis Primers 2022, 8, 30. [Google Scholar] [CrossRef] [PubMed]
- Razvi, S.; Korevaar, T.I.M.; Taylor, P. Trends, Determinants, and Associations of Treated Hypothyroidism in the United Kingdom, 2005–2014. Thyroid 2019, 29, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.M.; Duntas, L.; Fadeyev, V.; Nygaard, B.; Vanderpump, M.P.J. 2012 ETA Guidelines: The Use of L-T4 + L-T3 in the Treatment of Hypothyroidism. Eur Thyroid J 2012, 1, 55–71. [Google Scholar] [CrossRef]
- Jonklaas, J.; Bianco, A.C.; Cappola, A.R.; Celi, F.S.; Fliers, E.; Heuer, H.; McAninch, E.A.; Moeller, L.C.; Nygaard, B.; Sawka, A.M.; et al. Evidence-Based Use of Levothyroxine/Liothyronine Combinations in Treating Hypothyroidism: A Consensus Document. Thyroid 2021, 31, 156–182. [Google Scholar] [CrossRef]
- Lillevang-Johansen, M.; Abrahamsen, B.; Jørgensen, H.L.; Brix, T.H.; Hegedüs, L. Over- and Under-Treatment of Hypothyroidism Is Associated with Excess Mortality: A Register-Based Cohort Study. Thyroid 2018, 28, 566–574. [Google Scholar] [CrossRef]
- Thayakaran, R.; Adderley, N.J.; Sainsbury, C.; Torlinska, B.; Boelaert, K.; Šumilo, D.; Price, M.; Thomas, G.N.; Toulis, K.A.; Nirantharakumar, K. Thyroid Replacement Therapy, Thyroid Stimulating Hormone Concentrations, and Long Term Health Outcomes in Patients with Hypothyroidism: Longitudinal Study. BMJ 2019, l4892. [Google Scholar] [CrossRef]
- Davies, T.F.; Morshed, S.A.; Mezei, M.; Latif, R. Brief Report - Monoclonal Antibodies Illustrate the Difficulties in Measuring Blocking TSH Receptor Antibodies. Front. Endocrinol. 2022, 13, 943459. [Google Scholar] [CrossRef]
- Peterson, S.J.; Cappola, A.R.; Castro, M.R.; Dayan, C.M.; Farwell, A.P.; Hennessey, J.V.; Kopp, P.A.; Ross, D.S.; Samuels, M.H.; Sawka, A.M.; et al. An Online Survey of Hypothyroid Patients Demonstrates Prominent Dissatisfaction. Thyroid 2018, 28, 707–721. [Google Scholar] [CrossRef] [PubMed]
- Bjerkreim, B.A.; Hammerstad, S.S.; Gulseth, H.L.; Berg, T.J.; Omdal, L.J.; Lee-Ødegård, S.; Eriksen, E.F. Effect of Liothyronine Treatment on Quality of Life in Female Hypothyroid Patients With Residual Symptoms on Levothyroxine Therapy: A Randomized Crossover Study. Front. Endocrinol. 2022, 13, 816566. [Google Scholar] [CrossRef] [PubMed]
- Perros, P.; Nirantharakumar, K.; Hegedüs, L. Recent Evidence Sets Therapeutic Targets for Levothyroxine-Treated Patients with Primary Hypothyroidism Based on Risk of Death. European Journal of Endocrinology 2021, 184, C1–C3. [Google Scholar] [CrossRef] [PubMed]
- Perros, P.; Hegedüs, L.; Nagy, E.V.; Papini, E.; Hay, H.A.; Abad-Madroñero, J.; Tallett, A.J.; Bilas, M.; Lakwijk, P.; Poots, A.J. The Impact of Hypothyroidism on Satisfaction with Care and Treatment and Everyday Living: Results from E-Mode Patient Self-Assessment of Thyroid Therapy, a Cross-Sectional, International Online Patient Survey. Thyroid 2022, thy.2022.0324. [Google Scholar] [CrossRef]
- Roberto Castello; Marco Caputo Thyroid Diseases and Gender. Italian Journal of Gender-Specific Medicine 2019. [CrossRef]
- Matana, A.; Popović, M.; Boutin, T.; Torlak, V.; Brdar, D.; Gunjača, I.; Kolčić, I.; Boraska Perica, V.; Punda, A.; Polašek, O.; et al. Genome-Wide Meta-Analysis Identifies Novel Gender Specific Loci Associated with Thyroid Antibodies Level in Croatians. Genomics 2019, 111, 737–743. [Google Scholar] [CrossRef]
- Ragusa, F.; Fallahi, P.; Elia, G.; Gonnella, D.; Paparo, S.R.; Giusti, C.; Churilov, L.P.; Ferrari, S.M.; Antonelli, A. Hashimotos’ Thyroiditis: Epidemiology, Pathogenesis, Clinic and Therapy. Best Practice & Research Clinical Endocrinology & Metabolism 2019, 33, 101367. [Google Scholar] [CrossRef]
- Pyzik, A.; Grywalska, E.; Matyjaszek-Matuszek, B.; Roliński, J. Immune Disorders in Hashimoto’s Thyroiditis: What Do We Know So Far? Journal of Immunology Research 2015, 2015, 1–8. [Google Scholar] [CrossRef]
- Vargas-Uricoechea, H. Molecular Mechanisms in Autoimmune Thyroid Disease. Cells 2023, 12, 918. [Google Scholar] [CrossRef]
- Hu, X.; Chen, Y.; Shen, Y.; Tian, R.; Sheng, Y.; Que, H. Global Prevalence and Epidemiological Trends of Hashimoto’s Thyroiditis in Adults: A Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 1020709. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Jooste, P.L.; Pandav, C.S. Iodine-Deficiency Disorders. The Lancet 2008, 372, 1251–1262. [Google Scholar] [CrossRef]
- Andersson, M.; Karumbunathan, V.; Zimmermann, M.B. Global Iodine Status in 2011 and Trends over the Past Decade. The Journal of Nutrition 2012, 142, 744–750. [Google Scholar] [CrossRef]
- Zimmermann, M.B. Iodine Deficiency. Endocrine Reviews 2009, 30, 376–408. [Google Scholar] [CrossRef] [PubMed]
- Devdhar, M.; Drooger, R.; Pehlivanova, M.; Singh, G.; Jonklaas, J. Levothyroxine Replacement Doses Are Affected by Gender and Weight, But Not Age. Thyroid 2011, 21, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Poste, G.; Carbone, D.P.; Parkinson, D.R.; Verweij, J.; Hewitt, S.M.; Jessup, J.M. Leveling the Playing Field: Bringing Development of Biomarkers and Molecular Diagnostics up to the Standards for Drug Development. Clinical Cancer Research 2012, 18, 1515–1523. [Google Scholar] [CrossRef] [PubMed]
- Troch, M.; Woehrer, S.; Streubel, B.; Weissel, M.; Hoffmann, M.; Müllauer, L.; Chott, A.; Raderer, M. Chronic Autoimmune Thyroiditis (Hashimoto’s Thyroiditis) in Patients with MALT Lymphoma. Annals of Oncology 2008, 19, 1336–1339. [Google Scholar] [CrossRef]
- Trovato, M.; Giuffrida, G.; Seminara, A.; Fogliani, S.; Cavallari, V.; Ruggeri, R.M.; Campennì, A. Coexistence of Diffuse Large B-Cell Lymphoma and Papillary Thyroid Carcinoma in a Patient Affected by Hashimoto’s Thyroiditis. Arch. Endocrinol. Metab. 2017, 61, 643–646. [Google Scholar] [CrossRef]
- Anil, C.; Goksel, S.; Gursoy, A. Hashimoto’s Thyroiditis Is Not Associated with Increased Risk of Thyroid Cancer in Patients with Thyroid Nodules: A Single-Center Prospective Study. Thyroid 2010, 20, 601–606. [Google Scholar] [CrossRef]
- Chen, Y.-K.; Lin, C.-L.; Cheng, F.T.-F.; Sung, F.-C.; Kao, C.-H. Cancer Risk in Patients with Hashimoto’s Thyroiditis: A Nationwide Cohort Study. Br J Cancer 2013, 109, 2496–2501. [Google Scholar] [CrossRef]
- Resende De Paiva, C.; Grønhøj, C.; Feldt-Rasmussen, U.; Von Buchwald, C. Association between Hashimoto’s Thyroiditis and Thyroid Cancer in 64,628 Patients. Front. Oncol. 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, E.T.; Pavlidis, T.E. A Review of Primary Thyroid Lymphoma: Molecular Factors, Diagnosis and Management. Journal of Investigative Surgery 2019, 32, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Sevilla, J.J.; Salar, A. Recent Advances in the Genetic of MALT Lymphomas. Cancers 2021, 14, 176. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.D.; Vielh, P. Thyroid and Molecular Testing. Advances in Thyroid Molecular Cytopathology. JMP 2021, 2, 77–92. [Google Scholar] [CrossRef]
- Trovato, M. Update on International Medical Taxonomies of Biomarkers and Their Applications in Management of Thyroid Cancers. Diagnostics 2022, 12, 662. [Google Scholar] [CrossRef]
- ClinicalTrials.Gov. Available online: https://beta.clinicaltrials.gov/ (accessed on 16 April 2023).
- Strachan, D.P. Hay Fever, Hygiene, and Household Size. BMJ 1989, 299, 1259–1260. [Google Scholar] [CrossRef]
- Tomer, Y.; Davies, T.F. Infection, Thyroid Disease, and Autoimmunity*. Endocrine Reviews 1993, 14, 107–120. [Google Scholar] [CrossRef]
- Desailloud, R.; Hober, D. Viruses and Thyroiditis: An Update. Virol J 2009, 6, 5. [Google Scholar] [CrossRef]
- Morohoshi, K.; Takahashi, Y.; Mori, K. Viral Infection and Innate Pattern Recognition Receptors in Induction of Hashimoto’s Thyroiditis. Discov Med 2011, 12, 505–511. [Google Scholar]
- Okada, H.; Kuhn, C.; Feillet, H.; Bach, J.-F. The ‘Hygiene Hypothesis’ for Autoimmune and Allergic Diseases: An Update. Clinical and Experimental Immunology 2010, 160, 1–9. [Google Scholar] [CrossRef]
- Versini, M.; Jeandel, P.-Y.; Bashi, T.; Bizzaro, G.; Blank, M.; Shoenfeld, Y. Unraveling the Hygiene Hypothesis of Helminthes and Autoimmunity: Origins, Pathophysiology, and Clinical Applications. BMC Med 2015, 13, 81. [Google Scholar] [CrossRef] [PubMed]
- Garn, H.; Potaczek, D.P.; Pfefferle, P.I. The Hygiene Hypothesis and New Perspectives—Current Challenges Meeting an Old Postulate. Front. Immunol. 2021, 12, 637087. [Google Scholar] [CrossRef] [PubMed]
- Kondrashova, A.; Seiskari, T.; Ilonen, J.; Knip, M.; Hyöty, H. The ‘Hygiene Hypothesis’ and the Sharp Gradient in the Incidence of Autoimmune and Allergic Diseases between Russian Karelia and Finland. APMIS 2013, 121, 478–493. [Google Scholar] [CrossRef] [PubMed]
- Detels, R.; Brody, J.A.; Edgar, A.H. Multiple Sclerosis among American, Japanese and Chinese Migrants to California and Washington. Journal of Chronic Diseases 1972, 25, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Leibowitz, U.; Kahana, E.; Alter, M. The Changing Frequency of Multiple Sclerosis in Israel. Archives of Neurology 1973, 29, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Bodansky, H.J.; Staines, A.; Stephenson, C.; Haigh, D.; Cartwright, R. Evidence for an Environmental Effect in the Aetiology of Insulin Dependent Diabetes in a Transmigratory Population. BMJ 1992, 304, 1020–1022. [Google Scholar] [CrossRef] [PubMed]
- Staines, A.; Hanif, S.; Ahmed, S.; McKinney, P.A.; Shera, S.; Bodansky, H.J. Incidence of Insulin Dependent Diabetes Mellitus in Karachi, Pakistan. Archives of Disease in Childhood 1997, 76, 121–123. [Google Scholar] [CrossRef]
- Hammond, S.R. The Age-Range of Risk of Developing Multiple Sclerosis: Evidence from a Migrant Population in Australia. Brain 2000, 123, 968–974. [Google Scholar] [CrossRef]
- Bach, J.-F. Revisiting the Hygiene Hypothesis in the Context of Autoimmunity. Front. Immunol. 2021, 11, 615192. [Google Scholar] [CrossRef]
- Krassas, G.E.; Tziomalos, K.; Pontikides, N.; Lewy, H.; Laron, Z. Seasonality of Month of Birth of Patients with Graves’ and Hashimoto’s Diseases Differ from That in the General Population. eur j endocrinol 2007, 156, 631–636. [Google Scholar] [CrossRef]
- Attard, C.C.; Sze, W.C.C.; Vella, S. Predictors of Autoimmune Thyroid Disease. Baylor University Medical Center Proceedings 2022, 35, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Flicek, P.; Amode, M.R.; Barrell, D.; Beal, K.; Brent, S.; Chen, Y.; Clapham, P.; Coates, G.; Fairley, S.; Fitzgerald, S.; et al. Ensembl 2011. Nucleic Acids Research 2011, 39, D800–D806. [Google Scholar] [CrossRef] [PubMed]
- Borchers, C.H.; Kast, J.; Foster, L.J.; Siu, K.W.M.; Overall, C.M.; Binkowski, T.A.; Hildebrand, W.H.; Scherer, A.; Mansoor, M.; Keown, P.A. The Human Proteome Organization Chromosome 6 Consortium: Integrating Chromosome-Centric and Biology/Disease Driven Strategies. Journal of Proteomics 2014, 100, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Kulski, J.K.; Suzuki, S.; Shiina, T. Human Leukocyte Antigen Super-Locus: Nexus of Genomic Supergenes, SNPs, Indels, Transcripts, and Haplotypes. Hum Genome Var 2022, 9, 49. [Google Scholar] [CrossRef] [PubMed]
- Zaletel, K.; Gaberšček, S. Hashimoto’s Thyroiditis: From Genes to the Disease. Curr Genomics 2011, 12, 576–588. [Google Scholar] [CrossRef]
- Douillard, V.; Castelli, E.C.; Mack, S.J.; Hollenbach, J.A.; Gourraud, P.-A.; Vince, N.; Limou, S. Approaching Genetics Through the MHC Lens: Tools and Methods for HLA Research. Front. Genet. 2021, 12, 774916. [Google Scholar] [CrossRef]
- De Santis, D.; Truong, L.; Martinez, P.; D’Orsogna, L. Rapid High-resolution HLA Genotyping by MinION Oxford Nanopore Sequencing for Deceased Donor Organ Allocation. HLA 2020, 96, 141–162. [Google Scholar] [CrossRef]
- Zawadzka-Starczewska, K.; Tymoniuk, B.; Stasiak, B.; Lewiński, A.; Stasiak, M. Actual Associations between HLA Haplotype and Graves’ Disease Development. JCM 2022, 11, 2492. [Google Scholar] [CrossRef]
- Stasiak, M.; Zawadzka-Starczewska, K.; Tymoniuk, B.; Stasiak, B.; Lewiński, A. Significance of HLA in the Development of Graves’ Orbitopathy. Genes Immun 2023, 24, 32–38. [Google Scholar] [CrossRef]
- Liao, W.-L.; Liu, T.-Y.; Cheng, C.-F.; Chou, Y.-P.; Wang, T.-Y.; Chang, Y.-W.; Chen, S.-Y.; Tsai, F.-J. Analysis of HLA Variants and Graves’ Disease and Its Comorbidities Using a High Resolution Imputation System to Examine Electronic Medical Health Records. Front. Endocrinol. 2022, 13, 842673. [Google Scholar] [CrossRef]
- Mori, K.; Yoshida, K. Viral Infection in Induction of Hashimotoʼs Thyroiditis: A Key Player or Just a Bystander? : Current Opinion in Endocrinology, Diabetes and Obesity 2010, 17, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Weider, T.; Genoni, A.; Broccolo, F.; Paulsen, T.H.; Dahl-Jørgensen, K.; Toniolo, A.; Hammerstad, S.S. High Prevalence of Common Human Viruses in Thyroid Tissue. Front. Endocrinol. 2022, 13, 938633. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; Zhang, W.P.; Liu, H.X.; Wang, D.; Li, Y.F.; Wang, W.Q.; Wang, L.; He, F.R.; Wang, Z.; Yan, Q.G.; et al. Detection of Human Parvovirus B19 in Papillary Thyroid Carcinoma. Br J Cancer 2008, 98, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, W.; Liu, H.; Wang, D.; Wang, W.; Li, Y.; Wang, Z.; Wang, L.; Zhang, W.; Huang, G. Parvovirus B19 Infection Associated with Hashimoto’s Thyroiditis in Adults. Journal of Infection 2010, 60, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Heidari, Z.; Jami, M. Parvovirus B19 Infection Is Associated with Autoimmune Thyroid Disease in Adults. Int J Endocrinol Metab 2021, 19. [Google Scholar] [CrossRef] [PubMed]
- Pastore, F. Hepatitis C Virus Infection and Thyroid Autoimmune Disorders: A Model of Interactions between the Host and the Environment. WJH 2016, 8, 83. [Google Scholar] [CrossRef]
- Caselli, E.; Zatelli, M.C.; Rizzo, R.; Benedetti, S.; Martorelli, D.; Trasforini, G.; Cassai, E.; Degli Uberti, E.C.; Di Luca, D.; Dolcetti, R. Virologic and Immunologic Evidence Supporting an Association between HHV-6 and Hashimoto’s Thyroiditis. PLoS Pathog 2012, 8, e1002951. [Google Scholar] [CrossRef]
- Seyyedi, N.; Dehbidi, G.R.; Karimi, M.; Asgari, A.; Esmaeili, B.; Zare, F.; Farhadi, A.; Dabbaghmanesh, M.H.; Saki, F.; Behzad-Behbahani, A. Human Herpesvirus 6A Active Infection in Patients with Autoimmune Hashimoto’s Thyroiditis. The Brazilian Journal of Infectious Diseases 2019, 23, 435–440. [Google Scholar] [CrossRef]
- Trovato, M.; Sciacchitano, S.; Facciolà, A.; Valenti, A.; Visalli, G.; Di Pietro, A. Interleukin-6 Signalling as a Valuable Cornerstone for Molecular Medicine (Review). Int J Mol Med 2021, 47, 107. [Google Scholar] [CrossRef]
- Trovato, M.; Ruggeri, R.M.; Sciacchitano, S.; Vicchio, T.M.; Picerno, I.; Pellicanò, G.; Valenti, A.; Visalli, G. Serum Interleukin-6 Levels Are Increased in HIV-Infected Patients That Develop Autoimmune Disease during Long-Term Follow-Up. Immunobiology 2018, 223, 264–268. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Chung, Y.-H.; Shi, Y.-F.; Tzang, B.-S.; Hsu, T.-C. The VP1 Unique Region of Human Parvovirus B19 and Human Bocavirus Induce Lung Injury in Naïve Balb/c Mice. PLoS ONE 2018, 13, e0202667. [Google Scholar] [CrossRef] [PubMed]
- Canuti, M.; Eis-Huebinger, A.M.; Deijs, M.; De Vries, M.; Drexler, J.F.; Oppong, S.K.; Müller, M.A.; Klose, S.M.; Wellinghausen, N.; Cottontail, V.M.; et al. Two Novel Parvoviruses in Frugivorous New and Old World Bats. PLoS ONE 2011, 6, e29140. [Google Scholar] [CrossRef] [PubMed]
- Cotmore, S.F.; Agbandje-McKenna, M.; Canuti, M.; Chiorini, J.A.; Eis-Hubinger, A.-M.; Hughes, J.; Mietzsch, M.; Modha, S.; Ogliastro, M.; Pénzes, J.J.; et al. ICTV Virus Taxonomy Profile: Parvoviridae. Journal of General Virology 2019, 100, 367–368. [Google Scholar] [CrossRef] [PubMed]
- Pénzes, J.J.; Söderlund-Venermo, M.; Canuti, M.; Eis-Hübinger, A.M.; Hughes, J.; Cotmore, S.F.; Harrach, B. Reorganizing the Family Parvoviridae: A Revised Taxonomy Independent of the Canonical Approach Based on Host Association. Arch Virol 2020, 165, 2133–2146. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Fernandez, J.; Carton, R.; Tanner, A.R.; Puttick, M.N.; Blaxter, M.; Vinther, J.; Olesen, J.; Giribet, G.; Edgecombe, G.D.; Pisani, D. A Molecular Palaeobiological Exploration of Arthropod Terrestrialization. Phil. Trans. R. Soc. B 2016, 371, 20150133. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Fernandez, J.; Tanner, A.R.; Puttick, M.N.; Vinther, J.; Edgecombe, G.D.; Pisani, D. A Cambrian–Ordovician Terrestrialization of Arachnids. Front. Genet. 2020, 11, 182. [Google Scholar] [CrossRef] [PubMed]
- Pénzes, J.J.; De Souza, W.M.; Agbandje-McKenna, M.; Gifford, R.J. An Ancient Lineage of Highly Divergent Parvoviruses Infects Both Vertebrate and Invertebrate Hosts. Viruses 2019, 11, 525. [Google Scholar] [CrossRef]
- Cossart, Y.E.; Cant, B.; Field, A.M.; Widdows, D. PARVOVIRUS-LIKE PARTICLES IN HUMAN SERA. The Lancet 1975, 305, 72–73. [Google Scholar] [CrossRef]
- Allander, T.; Tammi, M.T.; Eriksson, M.; Bjerkner, A.; Tiveljung-Lindell, A.; Andersson, B. Cloning of a Human Parvovirus by Molecular Screening of Respiratory Tract Samples. Proc. Natl. Acad. Sci. U.S.A. 2005, 102, 12891–12896. [Google Scholar] [CrossRef]
- Lehmann, H.W.; Von Landenberg, P.; Modrow, S. Parvovirus B19 Infection and Autoimmune Disease. Autoimmunity Reviews 2003, 2, 218–223. [Google Scholar] [CrossRef]
- Adamson, L.A.; Fowler, L.J.; Clare-Salzler, M.J.; Hobbs, J.A. Parvovirus B19 Infection in Hashimoto’s Thyroiditis, Papillary Thyroid Carcinoma, and Anaplastic Thyroid Carcinoma. Thyroid 2011, 21, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Gravelsina, S.; Nora-Krukle, Z.; Svirskis, S.; Cunskis, E.; Murovska, M. Presence of B19V in Patients with Thyroid Gland Disorders. Medicina 2019, 55, 774. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Xu, P.; Cheng, F.; Li, Y.; Wang, Z.; Hao, S.; Wang, J.; Ning, K.; Ganaie, S.S.; Engelhardt, J.F.; et al. Cellular Cleavage and Polyadenylation Specificity Factor 6 (CPSF6) Mediates Nuclear Import of Human Bocavirus 1 NP1 Protein and Modulates Viral Capsid Protein Expression. J Virol 2020, 94, e01444–19. [Google Scholar] [CrossRef] [PubMed]
- Sowd, G.A.; Serrao, E.; Wang, H.; Wang, W.; Fadel, H.J.; Poeschla, E.M.; Engelman, A.N. A Critical Role for Alternative Polyadenylation Factor CPSF6 in Targeting HIV-1 Integration to Transcriptionally Active Chromatin. Proc. Natl. Acad. Sci. U.S.A. 2016, 113. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Schubert, H.L.; Singh, P.K.; Martins, L.J.; Engelman, A.N.; D’Orso, I.; Hill, C.P.; Planelles, V. Cleavage and Polyadenylation Specificity Factor 6 Is Required for Efficient HIV-1 Latency Reversal. mBio 2021, 12, e01098-21. [Google Scholar] [CrossRef] [PubMed]
- Mattola, S.; Hakanen, S.; Salminen, S.; Aho, V.; Mäntylä, E.; Ihalainen, T.O.; Kann, M.; Vihinen-Ranta, M. Concepts to Reveal Parvovirus–Nucleus Interactions. Viruses 2021, 13, 1306. [Google Scholar] [CrossRef] [PubMed]
- Ruggeri, R.M.; Vicchio, T.M.; Giovinazzo, S.; Certo, R.; Alibrandi, A.; Trimarchi, F.; Benvenga, S.; Trovato, M. TP53 Polymorphism May Contribute to Genetic Susceptibility to Develop Hashimoto’s Thyroiditis. J Endocrinol Invest 2015, 38, 1175–1182. [Google Scholar] [CrossRef]
- Li, Z.-H.; Han, J.; Wang, Y.-F.; Dai, J.; Zhang, H.; Li, C.-X.; Ma, Q. Association between Polymorphism of Interleukin-23 Receptor and Hashimoto’s Thyroiditis in Chinese Han Population of Shandong. Chinese Medical Journal 2015, 128, 2050–2053. [Google Scholar] [CrossRef]
- Chen, R.-H.; Chang, C.-T.; Chen, W.-C.; Tsai, C.-H.; Tsai, F.-J. Proinflammatory Cytokine Gene Polymorphisms among Hashimoto’s Thyroiditis Patients. J. Clin. Lab. Anal. 2006, 20, 260–265. [Google Scholar] [CrossRef]
- Durães, C.; Moreira, C.S.; Alvelos, I.; Mendes, A.; Santos, L.R.; Machado, J.C.; Melo, M.; Esteves, C.; Neves, C.; Sobrinho-Simões, M.; et al. Polymorphisms in the TNFA and IL6 Genes Represent Risk Factors for Autoimmune Thyroid Disease. PLoS ONE 2014, 9, e105492. [Google Scholar] [CrossRef]
- Jameson, J.L.; Longo, D.L. Precision Medicine — Personalized, Problematic, and Promising. N Engl J Med 2015, 372, 2229–2234. [Google Scholar] [CrossRef] [PubMed]
- Zucca, E.; Arcaini, L.; Buske, C.; Johnson, P.W.; Ponzoni, M.; Raderer, M.; Ricardi, U.; Salar, A.; Stamatopoulos, K.; Thieblemont, C.; et al. Marginal Zone Lymphomas: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Annals of Oncology 2020, 31, 17–29. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Global HT prevalence; data have been extracted from reference [32].
Figure 1.
Global HT prevalence; data have been extracted from reference [32].
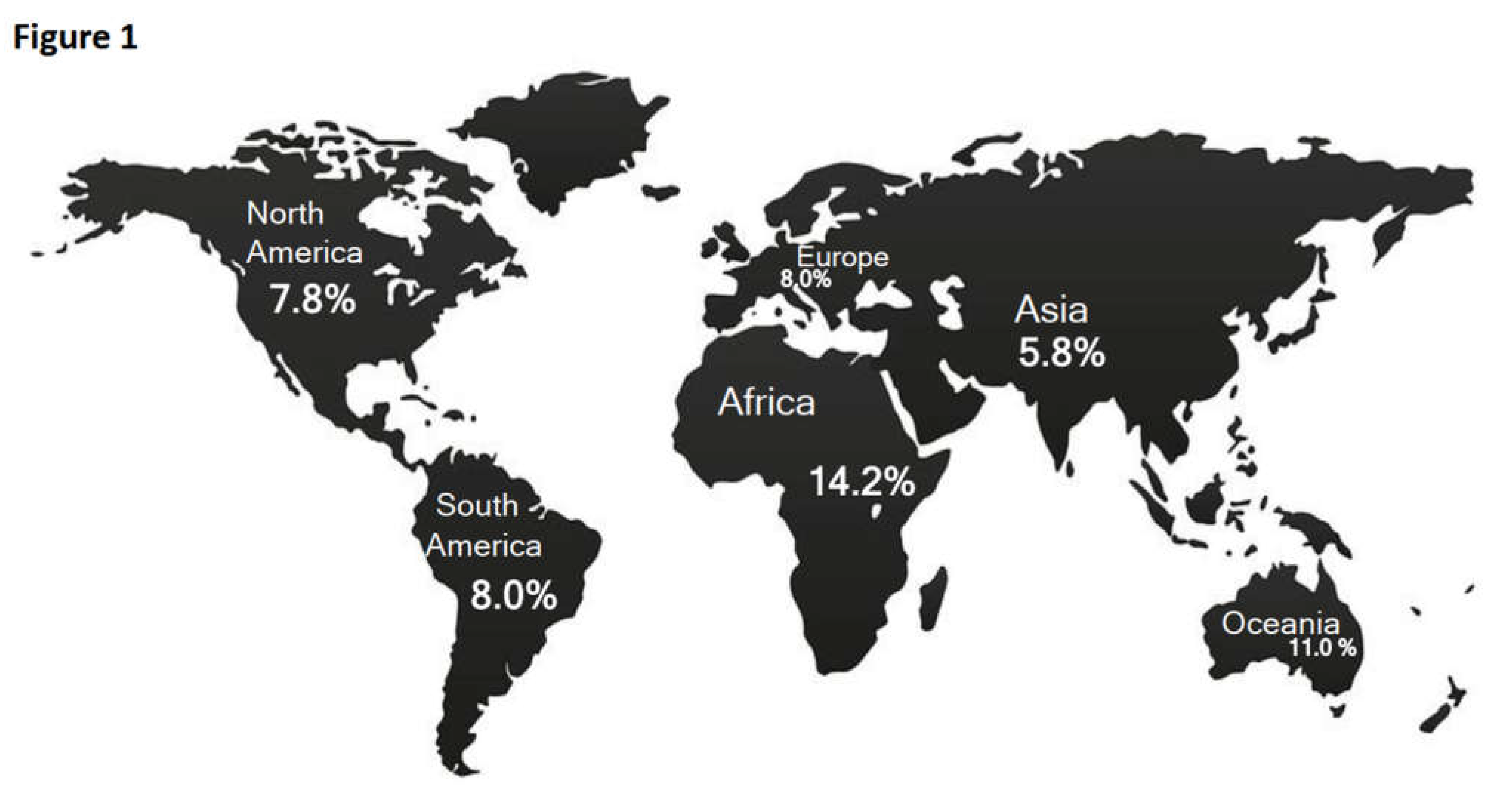

Table 1.
Clinical trials studies conducted on HT population.
| Continent | Geolocation | ClinicalTrials.gov Identifier |
OFFICIAL TITLE | Start Date* |
Primary Completion Date* |
Study Completion Date* |
Last Verified |
Conclusion |
|---|---|---|---|---|---|---|---|---|
| Africa (n=2) 0.04% |
Egypt | NCT03289403 | The role of immunomodulatory treatment in success of ICSI in patients with autoimmune thyroiditis |
2018 | 2019 | 2019 | 2020 | Completed |
| Israel | NCT01270425 | Sonographic and laboratory evaluation of the thyroid gland in patients with systemic sclerosis |
2011 | 2011 | 2012 (anticipated) |
2013 | Completed | |
| American (n=7) 15.5% |
Brazil | NCT01129492 | Low-level laser therapy in chronic autoimmune thyroiditis |
2006 | 2009 | 2009 | 2010 | Completed |
| Brazil | NCT02240563 | Low level laser therapy for autoimmune thyroiditis |
2014 | 2016 | 2016 | 2017 | Completed | |
| Chile | NCT04778865 | Effect of treatment for vitamin D deficiency on thyroid function and autoimmunity in Hashimoto's thyroiditis |
2020 | 2021 (estimated) |
2021 (estimated) |
2021 | Recruiting | |
| USA | NCT00958113 | Autoimmune thyroid disease genetic study |
2009 | 2013 | 2015 | 2015 | Completed | |
| USA | NCT01428167 | Hashimotos thyroiditis and thyroid cancer (thyroid cancer) |
2011 | 2012 | 2012 | 2012 | Completed | |
| USA | NCT01551498 | Evaluating the dietary supplement anatabloc in thyroid health-ASAP (antabloc supplementation autoimmune prevention) (ASAP) |
2012 | 2013 | 2013 | 2015 | Completed | |
| USA | NCT04542278 | Preoperative steroids in autoimmune thyroid disease |
2020 | 2022 | 2022 | 2022 | Completed | |
| Asian (n= 6) 13.3% |
China | NCT03447093 | The oral microbiota is associated with autoimmune thyroiditis |
2017 | 2019 (estimated) |
2021 (estimated) |
2018 | Unknown |
| China | NCT04075851 | The prevalence of serum thyroid hormone autoantibodies in autoimmune thyroid diseases |
2019 | 2022 (estimated) |
2022 (estimated) |
2021 | Recruiting | |
| China | NCT04942769 | Study on the effect of selenium supplementation on the structure and function of autoimmune thyroiditis |
2019 | 2021 (estimated) |
2021 (estimated) |
2021 | Recruiting | |
| China | NCT03390582 | Gut microbiota is associated with autoimmune thyroid disease |
2017 | 2018 (estimated) |
2021 (estimated) |
2018 | Unknown | |
| Taiwan | NCT02126683 | The effect of Plaquenil on serum inflammatory markers and goiter in euthyroid young women with Hashimoto's thyroiditis |
2014 | 2016 (estimated) |
2016 (estimated) |
2014 | Unknown | |
| Taiwan | NCT01760421 | The effect of Hydroxychloroquine treatment in Hashimoto's thyroiditis |
2011 | 2012 | 2013 | 2014 | Completed | |
| Europe (n=22) 48.8% |
Denmark | NCT02013479 | Selenium supplementation in autoimmune thyroiditis (CATALYST) |
2014 | 2022 | 2022 (estimated) |
2022 | Active, not recruiting |
| France | NCT03114267 | Involvement of viral infections in the pathogenesis of chronic lymphocytic thyroiditis (Etude thyrovir) |
2012 | 2015 | 2015 | 2017 | Completed | |
| France | NCT03103776 | Involvement of polyomaviruses in the pathogenesis of autoimmune Thyroiditis and Goitrigenesis (IPoTAIG) |
2016 | 2018 (estimated) |
2018 (estimated) |
2018 | Unknown | |
| France | NCT04789993 | Additional autoimmune diseases with type 1 diabetes in pediatrics at diabetes diagnosis and during follow-up (AADT1D) |
2021 | 2021 (estimated) |
2021 (estimated) |
2021 | Enrolling by invitation |
|
| France | NCT05544448 | In vitro effect study of Interleukin-2 muteins on regulatory T cells of patients with different autoimmune, allo-immune or inflammatory diseases (MuTreg) |
2022 | 2023 (anticipated) |
2023 (anticipated) |
2022 | Not yet recruiting |
|
| Germany | NCT00552487 | Isolated ACTH deficiency in patients with Hashimoto thyroiditis |
2005 | NA | 2006 | 2007 | Completed | |
| Greece | NCT02491567 | DNA methylation and autoimmune thyroid diseases (THYRODNA) |
2014 | 2016 | 2018 | 2019 | Completed | |
| Greece | NCT02644707 | Selenium supplementation in youths with autoimmune thyroiditis (THYROSEL) |
2014 | 2016 | 2018 | 2020 | Completed | |
| Greece | NCT04693936 | Metabolic biomarkers in hashimoto's thyroiditis and psoriasis |
2021 | 2023 (estimated) |
2024 (estimated) |
2022 | Recruiting | |
| Greece | NCT02725879 | FGF-21 levels and RMR in children and adolescents with Hashimoto's thyroiditis (THYROMETABOL) (THYROMETABOL) |
2016 | 2020 (estimated) |
2020 (estimated) |
2020 | Unknown | |
| Italy | NCT03498417 | Anti-insulin-like growth factor- 1 receptor (IGF-1R) Antibodies in Graves' Disease and Graves' orbitopathy (IGF1RAbsGO) |
2018 | 2018 | 2018 | 2018 | Completed | |
| Italy | NCT01465867 | Selenium supplementation in pregnancy (Serena) |
2012 | 2017 | 2018 | 2018 | Completed | |
| Norway | NCT02319538 | Hashimoto - a surgical disease. total thyroidectomy makes antibodies disappear and ameliorates symptoms |
2012 | 2017 | 2017 | 2018 | Completed | |
| Poland | NCT04752202 | The influence of reducing diets on changes in thyroid parameters in obese women with Hashimoto's disease |
2019 | 2019 | 2019 | 2021 | Completed | |
| Poland | NCT04682340 | Analysis of BPA concentration in serum in women of reproductive age with autoimmune thyroid disease |
2020 | 2021 | 2022 | 2022 | Completed | |
| Romania | NCT04600349 | Identity oriented psychotrauma therapy on Hashimoto in adults |
2020 | 2020 | 2021 | 2021 | Completed | |
| Romania | NCT04472988 | Eye movement desensitization and reprocessing on autoimmune thyroiditis in adults |
2020 | 2020 | 2021 | 2021 | Completed | |
| Switzerland | NCT05017142 | Swiss pediatric inflammatory brain disease registry (Swiss Ped-IBrainD) |
2020 | 2071 (estimated) |
2071 (estimated) |
2021 | Recruiting | |
| Turkey | NCT01102205 | Evaluation of oxidative stress and effect of Levothyroxine treatment on oxidative stress in Hashimoto disease |
2010 | 2010 | 2010 | 2013 | Completed | |
| Turkey | NCT04754607 | Effects of low-level laser therapy on oxidative stress levels, fatigue and quality of life in patients with Hashimoto thyroiditis |
2021 | 2022 | 2022 | 2022 | Completed | |
| Turkey | NCT00271427 | Selenium treatment in autoimmune thyroiditis (AIT) |
2004 | NA | 2005 | 2006 | Completed | |
| Turkey | NCT01644318 | CXCL9 and CXCL11 levels in patients with autoimmune thyroiditis and habitual abortions |
NA | NA | NA | 2012 | Unknown | |
| Unknown (n=8) 17.7% |
Not provided |
NCT01884649 | Fetuin A as a new marker of inflammation in Hashimoto thyroiditis |
2012 | 2012 | 2012 | 2013 | Completed |
| Not provided |
NCT02318160 | Oxidative status in children with autoimmune thyroiditis |
2014 | 2014 | 2014 | 2014 | Completed | |
| Not provided |
NCT04613323 | Management of thyroid function in Hashimoto's thyroiditis during pregnancy |
2022 (estimated) |
2022 (estimated) |
2022 (estimated) |
2021 | Not yet recruiting |
|
| Not provided |
NCT02190214 | Thyroid disorders in Malaysia: a nationwide multicentre study (MyEndo-Thyroid) |
2014 | 2016 | 2016 | 2016 | Completed | |
| Not provided |
NCT03048708 | Thyroid in bariatric surgery (ThyrBar) |
2011 | 2013 | 2016 | 2018 | Completed | |
| Not provided |
NCT02302768 | Effect of Semet (80 and 160 mcg) versus placebo in euthyroid patients with AIT |
2012 | 2014 | 2015 (estimated) |
2014 | Unknown | |
| Not provided |
NCT05435547 | Preoperative corticosteroids in autoimmune thyroid disease |
2022 | 2025 (anticipated) |
2025 (anticipated) |
2022 | Not yet recruiting |
|
| Not provided |
NCT05276063 | A Phase 2b, study of Linsitinib in subjects with active, moderate to severe thyroid eye disease (TED) (LIDS) |
2022 | 2023 (estimated) |
2025 (estimated) |
2023 | Recruiting |
* NA: not available; Data taken from reference [47].
Table 2.
Molecular clinical trials studies conducted on HT population.
| ClinicalTrials.gov identifier | Target sequences | Analysis and methods | Biospecimen genetic retention and description | Type and model of study | Time perspective** | Enrollment of subjects | Responsible Party | Results Overview |
|---|---|---|---|---|---|---|---|---|
| NCT03114267 | Parvovirus | Analysis of the viral genome by PCR*, Analysis of the presence of capsid protein |
Not provided | Observational, cohort | Retrospective | 64 | Centre Hospitalier Universitaire, Amiens | No publications available |
| NCT03103776 | Polyoma Virus | Positive PCR* Frequencies for Polyomavir us | Blood, Urine and / or Thyroid Tissue | Interventional, parallel assignment | NA | 49 | Centre Hospitalier Universitaire, Amiens | No publications available |
| NCT03447093 | Oral microbiota | Measurement of microbiota by 16S rRNA gene. | Not provided | Observational, case control | Cross-Sectional | 120 | First Affiliated Hospital of Harbin Medical University | Publications available |
| NCT03390582 | Fecal microbiota | Measureme nt of microbiota by 16S rRNA gene. | Human feces | Observational, cohort | Cross-Sectional | 200 | First Affiliated Hospital of Harbin Medical University | No publications available |
| NCT00958113 | HLA, CTLA4, thyroglobulin, THSR, CD40, PTPN2 and PTPN22 | Map and identify genes that confer susceptibility to Autoimmune Thyroid Disease | Saliva | Observational, case control | Cross-Sectional | 199 | University of Colorado, Denver, USA | No publications available |
| NCT02491567 | CD40L, FOXP3, CTLA4, PTPN22, IL2RA, FCRL3 and HLADRB1 | DNA methylatio status of CpGs within gene promoters | Blood (leukocytes) | Observational, case control | Cross-Sectional | 110 | Medical School of Aristotle University of Thessaloniki | Publications available |
* PCR: polymerase chain reaction; **NA: not available; Data taken from reference [47].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



