
Submitted:
11 April 2023
Posted:
12 April 2023
You are already at the latest version
Abstract
Pakistan is one of the few countries where poliovirus transmission still persists, despite intensive efforts to eradicate the disease. Adequate vaccination coverage is essential to achieve polio eradication, but misconceptions about polio vaccines have hindered vaccination efforts. To address this issue, we conducted a mixed-methods study to explore knowledge and perceptions regarding polio disease and immunization in high-risk areas of Pakistan. We collected quantitative data from 3780, 1258, and 2100 households in Karachi, Bajaur, and Pishin, respectively, and supplemented this with qualitative data from focus group discussions and in-depth interviews. Our findings reveal a high level of awareness about polio and its immunization; however, misperceptions about the polio vaccine persist, leading to vaccine refusal for both polio and routine immunization. Our study provides up-to-date data on knowledge and perceptions of polio and its immunization and identifies critical gaps. These findings can inform the development of future strategies and innovative approaches to improve the success of the polio program in Pakistan.
Keywords:
Polio
; polio immunization
; knowledge and perceptions
; Pakistan
Introduction
The global polio eradication initiative (GPEI) launched in 1988 has successfully eradicated and contained all wild, vaccine-related, and Sabin polioviruses globally except Pakistan and Afghanistan [1]. The GPEI was established in 1994 in Pakistan and has substantially reduced the country's polio burden [2]. However, despite concerted national efforts, the transmission of wild poliovirus is still continuing, and Pakistan continues to be affected by wild poliovirus type 1 WPV1 and circulating vaccine-derived poliovirus type 2 (cVDPV2) [3]. The lowest number of 8 cases were reported in 2017, but then again, a rise in polio cases was observed in the following years, with 12 cases in 2018, 147 cases in 2019, and 84 cases in 2020. In 2020 the polio surveillance system in Pakistan identified the poliovirus circulation in 38 districts of Pakistan, including high-risk areas of Karachi, Northern Sindh, Southern Punjab, Peshawar, and Quetta block. In 2022, the virus circulation is still ongoing, and to date, Pakistan has 20 positive cases all confined to the hard-to-reach Waziristan area [2].
The GPEI in Pakistan has implemented numerous vaccination campaigns annually to contain polio transmission. About 250,000 frontline health workers go door-to-door to ensure every child under five is vaccinated against Polio and receives the oral polio vaccine (OPV) [4]. In addition to the OPV given during the campaigns four doses of OPV are also offered at birth and the age of four, ten, and fourteen weeks as a part of routine immunization in the national Expanded Program of Immunization (EPI) [5]. In 2015, the Government of Pakistan also included one dose of Injectable Polio Vaccine (IPV) to be given at fourteen weeks in the national EPI to further boost immunity among children [6]. To eradicate Polio from Pakistan all children must receive a sufficient number of polio doses in the campaign and routine immunization mode [7]. Failure to do so will result in continued poliovirus circulation in Pakistan [8].
Despite numerous awareness campaigns and initiatives through local and international stakeholders and partners, fears and misperceptions about polio vaccinations persist among high-risk communities [9,10]. Available literature also suggests that misperceptions based on cultural and religious beliefs and customs are the critical barrier to polio vaccination [10,11,12]. For example, misperceptions about the oral polio vaccine represented by religious leaders and extremist groups and organizations in Pakistan have suggested major inhibiting factors for polio vaccine uptake [12, 13, and 14]. In addition, rumors such as OPV being anti-Islamic, having haram impermissible ingredients, being a cause of infertility and the GPEI program being a foreign agenda are prevailing in the high-risk groups [11,12,13,14].
Robust communication strategies are required to counter these misconceptions and to enhance the knowledge of the parents and caregivers about Polio and its vaccines. However, current data on the inside and perceptions about Polio and its immunization in the high-risk population are lacking [11]. Therefore, we conducted a mixed-method study in high-risk polio areas of Pakistan to identify the current knowledge and perceptions about Polio and its vaccination. In addition, to estimates the coverage of routine immunization and oral polio vaccine and compares the existing knowledge, perception and vaccine coverage with previous findings [11].
Methodology
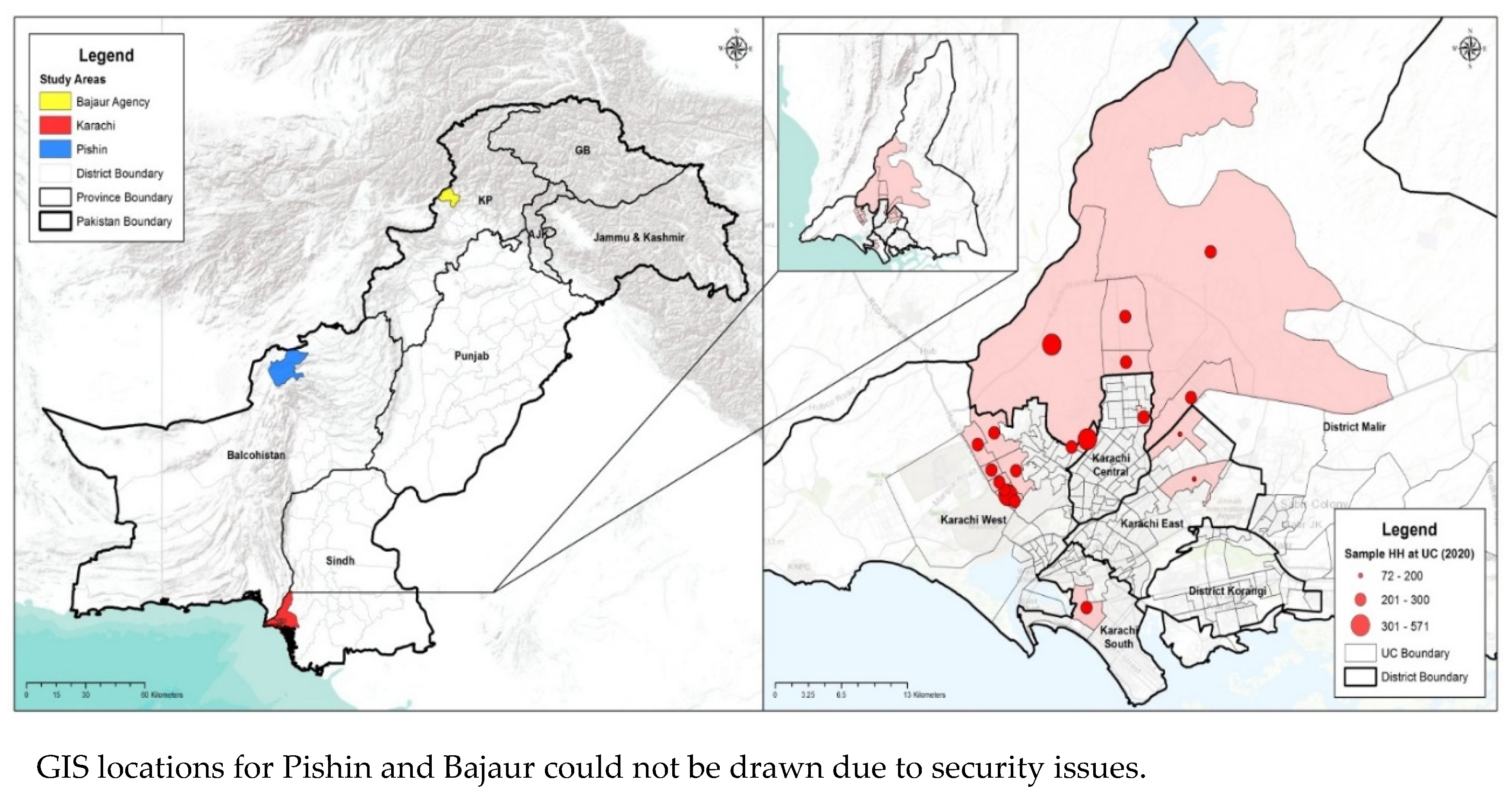
We used a mixed-methods approach to achieve the objectives of the study. Quantitative data were collected using a cross-sectional survey at the household level. In contrast, the qualitative data were collected using the focus group discussion (FGDs) and in-depth interviews (IDIs) with the targetted groups. The study was conducted from January 2020 to March 2020, in the Polio high-risk areas of Pakistan. We collected data from high-risk areas of Karachi in Sindh province, district Pishin in Balochistan province, and district Bajaur in Khyber Pakhtunkhwa (KP) province of Pakistan (Figure 1&2).
We employed a multi-stage sampling technique to draw a random sample from each area (i-e Karachi, Pishin, and Bajaur) and considered the union council (UC) as our cluster. A UC is the smallest administrative unit in Pakistan which usually has a population of 20000 to 30000. In the first stage, we selected 18 UCs from Karachi, 10 from district Pishin, and six from district Bajaur (Web Table 1). After choosing the UCs, we utilized the WHO 30X7 technique [15] to achieve the sample size within each union council for the quantitative part. This approach provided us with a sample size of 210 in each union council which is a suitable sample to assess the coverage of vaccines and knowledge of parents and care providers [16]. The overall sample sizes for Karachi, Pishin, and Bajaur were 3780, 2100, and 1260 respectively. For the selection of the 30 areas and seven households, we used the micro plans of the polio programs, a micro plan is a plan for each union council that the polio program uses and has the listing of vaccination areas household having an under-five child. Of the available list, we randomly selected 30 areas and from every 30 areas, seven households having an under-five child were selected for the interview.
For data collection, we developed a structured questionnaire for the household survey. The survey instrument was translated into the national language, Urdu and back-translated into English. The survey instrument was pre-tested in areas not part of the survey sample and updated as per the findings during the pre-test. We hired local teams of female data collectors who were accustomed to the local culture and language and had prior data collection experience. We conducted a four-day centralized training for the data collectors on survey methodology, sampling technique, and survey instrument followed by two days of mock field interviews. After the training, the survey teams collected data at the household level. Written consent was taken from the respondents (mother, father, or the caregiver) before all interviews.
For the qualitative component, we conducted FGDs and IDIs in Karachi, Pishin, and Bajaur. Respondents for the qualitative component included; decision-makers at the household level (including fathers, mothers, and mothers in law), Influencers at the community level prominent members of the community and health care providers, including the community health workers and vaccinators (Web Table 2). We used the purposive convenience sampling technique for selecting participants for in-depth interviews (IDIs) and focus group discussions (FGDs). Similar to the quantitative component we developed and pre-tested data collection tools (the FGD and IDI guidelines) by conducting FGDs and IDIs with various target groups to assess the clarity and relevance of the content. The qualitative data was collected by an expert team comprised of a female moderator and note-taker supported by the local facilitators.
Data analysis
Data were analyzed using STATA version 16. Descriptive analysis was carried out to assess knowledge, attitudes, and practices regarding polio vaccine, reasons for refusal, and current immunization status. Due to the categorical nature of observed variables, the data were summarized as frequency and percentages. In addition, a comparative analysis was done separately for the three districts to assess the change in key indicators over the two survey rounds, i.e. 2012 and 2020. Comparison between KAP data obtained from subjects was performed using the Chi-square test. P<0.05 was considered significant.
For qualitative data, we used topical and content analysis to convert responses into emerging and meaningful categories for each target group using a deductive approach. All transcriptions were comprehensively reviewed and coded. The qualitative data was anlyzed using the NVIVO software. We used these qualitative data to complement the quantitative part and to strengthen the overall findings of this study
Results
Quantitaive Component
In the quantitative component of the survey, data was collected from 1258, 2100, and 3780 households from Bajaur, Pishin, and Karachi, respectively. A total of 8025 households were surveyed in the Polio high-risk areas. Table 1 summarizes the demographic information from the target areas. The average household size was 9.1 for Bajaur, 12.5 for Pishin, and 7.8 for Karachi. The highest proportion of illiterate people was found in Pishin (84.2%) and the lowest in Karachi 44.1% .
The survey reflected (Table 2) that most of the respondents were knowledgeable about Polio in all three site areas. 99% in Karachi, 98% in Bajaur, and 97% in Pishin have heard about Polio. Information sources about Polio were reported to be television with 47% in Karachi, and Pishin 39%. Along with it, Radio in Bajaur, and LHWs in Pishin 39% were reported as the primary sources of knowledge about Polio. It is a health problem between 60% to 93% of the respondents. However, half of the respondents in all areas linked immunization as a preventive method.
This survey also tried to explore the knowledge about different causes of polio disease, findings indicated that over a third of all people, 36% in Bajaur and 40% in Pishin referred to it as Allah's will. Interestingly, many residential respondents of Karachi believed that the evil eye could cause polio disease. Moreover, the transmission of polio disease was linked by respondents to drinking dirty water 33% and contaminated air 41% – 47 % in Bajaur and Pishin. Surprisingly, despite being relatively knowledgeable about Polio, respondents from Karachi were unaware of polio transmission. Data showed that the Expanded Program on Routine Immunization (EPI) was perceived as the most comprehensive preventive measure for Polio 53 % in Karachi, 72% in Bajaur, and 65% in Pishin.
Table 3 shows that the knowledge about Oral Polio Vaccine (OPV) was reportedly high from 97% to 99% in all three study areas. Its effectiveness for polio prevention when assessed, 69% of respondents from Pishin, 89% from Karachi, and 94% from Bajaur perceived it as a necessary preventive measure against Polio. A substantial proportion of people reported Polio due to not receiving OPV. There are still concerns regarding OPV, which was perceived as utterly safe in Karachi 77%, and Bajaur 63%, but only by 42% of the people in Pishin.
Reported vaccine refusal issues were also assessed. These were highest in Bajaur (42%), followed by Karachi 23% and Pishin with 20%. The most cited OPV refusal reasons indicated by the survey were concerns about induction of sterility by the vaccine, 19% in Karachi and 68% in Pishin; this sterility misconception was compounded by other misconceptions that the vaccine was not Halal or impermissible under Islamic laws. This was found to be highest in Pishin 45%. The vaccine is unsafe, and children received Polio drops too many times. However, the proportion of refusals influenced by local/community leader was highest in Bajaur 21% with respondents reporting that these local or community leaders had prohibited them.
When specifically asked to cite reasons for not giving polio drops on National Immunization Days (NID) or campaigns , local respondents reported that the children didn't receive OPV due to the absence of the polio team or visits by LHWs (Table 4).
Polio immunization coverage reflected at different time points, findings showed the highest immunization at birth in Bajaur 94% followed by Karachi 89%, and Pishin 85%. Survey findings on immunization card availability showed that retention of immunization cards was relatively low in Pishin 45% and Karachi 48%. However, in Bajaur, the majority of them had immunization cards.
Comparison with previous similar survey conducted in 2012:
We also compared the data of key indicators (Table 5) of our survey with a comparable survey conducted in 2012 [11]. The data on knowledge and perception about Polio and OPV, the refusal for OPV and availability of vaccination cards, and routine immunization status were compared. The data showed that the knowledge about Polio among the respondents remains high and a significant increase in the level of knowledge was observed in Karachi, similarly, a high proportion of respondents considers Polio as a health problem in both surveys in Karachi and Bajaur however a significant decline in Pishin was observed. Moreover, the respondent's knowledge about OPV was also found to be high in both surveys. We did not find any significant change in the perception about the safety of OPV in Karachi and Bajaur, however, we found a significant reduction to 41.9% from 49.7% among the respondents who think OPV is completely safe. Data on the refusal of OPV showed that there was a significant change in Karachi and Pishin where the refusal rate increased from 5% to 23.1% and 17.4% to 25.0% respectively.
We found a significant positive change in the availability of vaccination cards in all three sites where the availability of vaccination cards increased from 26.4% to 47.7%, 12.9% to 78.1%, and 6.9% to 44.5% in Karachi, Bajaur, and Pishin respectively. We also observed a significant increment in fully immunized children in all three areas alongwith a substantial reduction in proportion of unimmunized (zero dose) children.
Qualitative Component:
Qualitative component findings were derived from the focus group discussions and in-depth interviews, adding to the study's finding. Sources of information shared by respondents are the doctors, grandmothers, polio health workers, mosque announcements, TV, radio, IEC material, banners, and posters.
"Grandmothers guide our daughters-in-laws' about child-rearing and caring, counsel what to feed if the child has fever or pain, what type is food is good in hot and cold weather to keep the child healthy."
"Polio workers give knowledge and guide us about health and vaccine, we are thankful to them that they visit repeatedly to our doorstep for the sake of community health."
Half of the respondents perceived the children's health is good.
"The health of my grandchild is good because his height and weight are perfect."
Others verbalized that the health of the under 5 children is not good because of compromised environmental conditions, socioeconomic status, and negligence of mothers towards themselves and their children.
"Mostly children are weak because they live and play in a dirty environment, and where there are open sewerage lines."
"Health of our children is not good, as most children don't get the vaccination, they don't get proper nutrition and live in unhygienic conditions. Nowadays diet of mothers is also not good that's why children are weak."
"Community people don't care about their children's health. I think to feed balanced diet to my child, but I can't buy fruit and chicken for them"
When specifically talked about routine immunization, received responses were of mix nature. Most parents were aware of the importance of polio vaccine and its vaccination among children. Whereas, some were against vaccination due to the side effects, misconceptions, and rumors that give rise to vaccine hesitancy.
"People believe that these vaccines are for family planning, cause infertility to decrease their generation."
"People think that because of vaccines child get a reaction and if one child dies so they do protest and refuse to give the vaccination."
Polio is perceived as a severe disease. Therefore, depiction of respondents' perception about polio disease is prominently reflected during these discussions.
"Only legs are not affected by polio disease it may cause many other problems like weakness, low immunity, heart problem, indigestion, weakens of an arm or leg and it can also lead to death."
"Polio disease spreads through our breath, sewerage, and air."
Findings revealed that most respondents were knowledgeable about polio disease, but some wrongly perceived polio-related signs and symptoms. For example, it was shared that if a child suffers from polio disease, they become physically weak, their hands and feet get twisted, and children got paralyzed.
"One of my grandchildren was healthy at the time of his birth. However, three days later he got fever, fits and his leg was affected. After consulting, the doctor diagnosed that the child has Polio."
"In our neighbors, the boy is born. After two or three days after his birth, he started trembling, got a fever, and was later affected by Polio. Same symptoms were seen in a couple of children here and nearby hospitals also confirm polio disease."
The risk of getting polio disease was indicated. Prone to which are the weak children, have poor health, don't receive polio drops, or frequently fall ill. However, polio vaccine and a clean and healthy environment were mentioned as the only preventive and safety measure.
"My niece gets affected by polio disease because her mother never gives her polio drops, when she took her to the doctor, he told them she got attacked by Polio. Now she is 18 years old but disabled. After this incident, my sister gives polio drops to every child to prevent them from Polio."
"Water testing from drainage was done to identify the poliovirus in our area and it has been proven that this is one of the main reasons for spreading this disease. Unfortunately, no vaccine and medicine can save children, until and unless the environment can be cleaned."
"After giving vaccines there is a chance that child can get polio disease, but this vaccine improves the immunity to fight against polio disease."
The majority were being aware of the OPV vaccine. The community people highly admired the rigorous efforts of polio workers as they address their queries and concerns, counsel and motivate them for vaccination against Polio. However, a misconception was found about its treatment and prevention. Few of the respondents were confused about whether Polio is treatable. Some believed of them that every treatment is possible if treated timely.
"I have seen that there was one girl who was 18 months old and she got polio attack and she became disabled. So her family took her to the Syed's and within 5 days she becomes normal. another child was in the last stage and they took the child to the Molvi and then the child becomes normal."
"Science is so advanced these days that there is the treatment of every disease, there are so many laboratories, people can be treated through medicine."
Shared refusal reasons for the Polio vaccine are that some people are still against it due to their misconceptions, doubts and fears, religious beliefs, family or cultural norms, limitations and preferences, fake news, and rumors.
"Pakhtoon community wants a large family and like to have more children. That's why they fear giving polio drops as it might stop their generations."
"This vaccine may cause infertility and can affect the lungs and kidneys of the children. So it is suspicious that why the Government is doing it free of cost."
"Mostly people refuse to give polio drops to their male child. When asked about the reason for refusal during the polio campaign, they say that we have an only male child in our home and these drops cause impotence."
Discussion
The study illustrated that while most parents had some knowledge about routine immunization and polio disease, the depth of understanding was limited. Many of the respondents did not have sufficient information regarding immunization and polio disease and lacked basic knowledge about polio-related signs and symptoms, these finding corroborates other studies conducted on the same subject [17,18]. Some of the respondents wrongly perceive Polio as treatable. The common perceptions for polio transmission were highlighted that it occurs due to living in unhygienic conditions, not vaccinating children, and by the migrants whose polio vaccine status is unknown. Quite unlike the misperceptions of the role of clergy or mosques, sources of information shared by respondents were doctors, grandmothers, Community Health Workers (CHWs)/Lady Health Workers (LHWs), Televesion, radio, Information, Education and Counselling (IEC) material, banners, and posters.
Despite some negative perceptions the overall opinion by respondents about vaccines was positive. Data evidence for routine immunization showed that most children under 5 receive timely vaccination for preventing diseases except for refusals. Despite the rigorous collective efforts of the polio health workers and other stakeholders, the views among those refusing vaccines are still very rigid. However, these were wild conspiracy ideas about a hidden agenda to destroy the nation, inducing infertility or not being Halal [19]. These perceptions by a few also influence other community-decisions and in moving forward is the most critical barrier to overcome. [20,21] The corollary to the strength of the current anti-vaccination movements worldwide couldn't be more stark.
There were difference in the way elders perceived health and immunization issues. Most of the grandmothers in the current survey considered their grandchildren as healthy compared to community elders who considered child health in their communities suboptimal. To our surprise, most participants couldn't relate childhood vaccination to optimizing a child's health. There is much need to improve community understanding of childhood immunizations' importance.
A substantial proportion of respondents display a negative attitude towards polio immunization. Community mobilization is a cornerstone of vaccine confidence and acceptance [17,22] Analysis revealed that these mobilization activities are very much helpful as initially people were rigid and didn't have any understanding of it, didn't even use to open their doors but after a rigorous and collective effort of all the stakeholders, a drastic change was being observed. The involvement of CHWs/LHWs positively impacted the vaccine coverage rate. [23] Steps of the CHWs and LHWs were being highly admired as they were prominent in terms of communication and has a good rapport with families as they have day-to-day interaction with mothers and guide them in health and vaccine-related issues by timely addressing their concerns which help them in minimizing their doubts and fears concerning vaccination. It was quoted that a figure of zero dozers has drastically declined. Studies suggested that developing a trusted relationship with parents, is the key to influence parental decision-making about Polio and routine immunization. [24]
Comparitive data of 2012 and 2020 surveys recognized key gaps in the progress of Polio program in Pakistan. Although we found significant improvement in some areas, there are areas that need urgent attention. For example, the data on the perceived safety of OPV is still concerning, as 25% in Karachi, 37% in Bajaur, and 48% in Pishin either consider OPV as unsafe or are unaware of the safety of the OPV. This lack of knowledge was consequently reflected in OPV's refusal rate and we found a significant increase in the refusals in Karachi and Bajaur. Furthermore, the comparative data also identified that a substantial proportion of children, 10% in Karachi, 5% in Bajaur and 13.4% in Pishin are unimmunized (Zero Dosers), thus reflecting the compromised quality of routine immunization in these areas.
Religious and social beliefs are the most prominent barriers that prevent the disease from tipping over into complete eradication. We believe there is an utmost need for a coalition campaign involving religious scholars, civil society stakeholders, and media that could turn the tide against the polio vaccine in Pakistan. Inadequate knowledge, false religious beliefs, and misconceptions are essential drivers of people's understanding of polio disease. These factors are more likely to be the source of potential barriers to behavior change which could help reduce the burden of Polio from high-risk polio countries. Furthermore, there is a need to evaluate the strategy effectiveness in parents' and health care providers' relationship. Supported by inline literature [17,25,26] Additionally, Polio prevalent areas should be targeted to alter the negative attitude of the refusals through identification and subsequent counseling by the community leaders/influential, CHWs/LHWs, and other civil society stakeholders. To improve the attitude of the people along with their knowledge of Polio to aid in turning the dream of a polio-free world into reality for all the children.
Our data on vaccine hesitancy and refusal can be explained by the fact that families mistrust and doubt the polio program, resulting in the recent upsurge in infection [2]. The majority of these families are impoverished and underserved and lack basic needs. Additionally, in the recent years social media has also played in important role in spreading false rumors rapidly about the polio program [27]. Furthermore, the weakened essential immunization services, poor water and sanitation, and lack of maternal and child health care further compound the polio eradication challenge in Pakistan [28]. To overcome these challenges an integrated approach is required where all of these services should be given to communities holistically. A large population based trial conducted in polio high risk areas of Pakistan provided a community mobilization strategy. It targeted community-based health and immunisation camps during polio immunisation campaigns which resulted in the effective increase in vaccine coverage in campaigns and routine immunization [29]. This model can be scaled up further along with integrating services to achieve the maximum coverage for OPV in high-risk areas.
The study's strengths are that it has focused on the mix-method approach to set the ground for the areas where the availability of the literature is limited. In addition, the qualitative approach expanded the light on the respondents' desirable responses, which helped triangulate the data more proficiently. Including participants from the high-risk polio areas is another key strength of the study. Results would help the stakeholders and other health officials from the Government and civil sector to evaluate and alter the current program's effectiveness and policies concerning the polio eradication program in Pakistan. However, these stakeholders should be cautious, considering that study findings are not country-wise generalizable. Participants may not be accountable for the difference within the population as they were recruited using convenient purposive sampling. Moreover, the temporal relationship is not established as it is a cross-sectional survey study.
Author Contributions
ZAB, conceived the study and prepared the data analysis plan. MAH supervised the field operation and data collection. IH and NS were responsible for quantitative data collection. FT and TJ lead the qualitative part. FS conducted the data analysis. All authors provided substantial contributions to the study design. All authors critically revised the manuscript and approved its final version.
Funding
The study was supported by the Bill & Melinda Gates Foundation [grant number: INV OPP1211074].
Acknowledgments
We want to thank all participants who consented to participate in the study. We would also like to acknowledge Mr Muhammad Umer, Mr Khalid Feroze and Mr Imran Ahmed at Aga Khan University and Mr Rehman Tahir of Trust for Vaccines and Immunization (TVI) for their outstanding support in field operations and data management.
Conflicts of Interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in conflict with the subject matter or materials discussed in the manuscript.
References
- Initiative, G.P.E. Our Mission. [cited February 2021]; Available from: http://polioeradication.org/who-we-are/our-mission/.
- Programme, P.P.E. Polio in Pakistan. [cited December 2022]; Available from: https://www.endpolio.com.pk/polioin-pakistan.
- Organization, W.H. Pakistan: Polio Eradication Initiative. 2020 [cited Febrary 2021 January 11]; Available from http: //www.emro.who.int/pak/programmes/polio-eradication-initiative.html#:~:text=Pakistan%20is%20one%20of%20only, poliovirus%20transmission%2C%20along%20with%20Afghanistan.&text=Since%20its%20initiation%20in%201994; 20p. [Google Scholar]
- Initiative, G.P.E. Where We Work. [cited February 2021]; Available from: http://polioeradication.org/where-we-work/. 20 February.
- Khowaja AR, Zaman U, Feroze A, Rizvi A, Zaidi AK. Routine EPI coverage: subdistrict inequalities and reasons for immunization failure in a rural setting in Pakistan. Asia pacific journal of public health. 2015, 27, NP1050–9.
- Immunization, F.E.P.o. , National EPI Policy & Strategic Guidelines Pakistan 2015.
- Global Polio Eradication Program. (2016) Global emergency action plan 2012–2013,http://www.polioeradication.org/portals/0/document/resources/strategywork/eap_201205.pdf,.
- Kew, O. Reaching the last one per cent: progress and challenges in global polio eradication. Current opinion in virology. 2012, 2, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Obregón R, Chitnis K, Morry C, Feek W, Bates J, Galway M, Ogden E. Achieving polio eradication: a review of health communication evidence and lessons learned in India and Pakistan. Bulletin of the World Health Organization. 2009, 87, 624–630.
- Khan T, Qazi J. Hurdles to the global antipolio campaign in Pakistan: an outline of the current status and future prospects to achieve a Polio free world. J Epidemiol Community Health. 2013, 67, 696–702.
- Habib MA, Soofi SB, Ali N, Hussain I, Tabassum F, Suhag Z, Anwar S, Ahmed I, Bhutta ZA. Knowledge and perceptions of polio and polio immunization in Polio high-risk areas of Pakistan. Journal of public health policy. 2017, 38, 16–36.
- Shah SZ, Saad M, Khattak MH, Rizwan M, Haidari A, Idrees F. Why we could not eradicate Polio from pakistan and how can we?. Journal of Ayub Medical College Abbottabad. 2016, 28, 423–425.
- Khan TM, Chiau LM. Polio vaccination in Pakistan: by force or by volition?. The Lancet. 2015, 386, 1733.
- Khan MU, Ahmad A, Salman S, Ayub M, Aqeel T, Haq NU, Saleem F, Khan MU. Muslim scholars' knowledge, attitudes and perceived barriers towards polio immunization in Pakistan. Journal of religion and health. 2017, 56, 635–648.
- Lemeshow S, Stroh G. Sampling techniques for evaluating health parameters in developing countries. DC^ eWashington Washington: National Academy Press; 1988.
- Nath DC, Patowari B. Estimation and comparison of immunization coverage under different sampling methods for health surveys. International Journal of Population Research. 2014, 2014.
- Khan MU, Ahmad A, Aqeel T, Salman S, Ibrahim Q, Idrees J, Khan MU. Knowledge, attitudes and perceptions towards polio immunization among residents of two highly affected regions of Pakistan. BMC public health. 2015, 15, 1–8.
- Ogwumike OO, Kaka B, Adeniyi AF. Children with paralytic poliomyelitis: a cross-sectional study of knowledge, attitudes and beliefs of parents in Zamfara state. Nigeria BMC public health. 2012, 12, 888.
- Knowledge, Attitudes and Practices (KAPs) Polls in Pakistan and Nigeria. 2014.
- Shawn DH, Gold R. Survey of parents' attitudes to the recommended Haemophilus influenzae type b vaccine program. CMAJ: Canadian Medical Association Journal. 1987, 136, 1038.
- Baumgaertner B, Carlisle JE, Justwan F. The influence of political ideology and trust on willingness to vaccinate. PloS one. 2018, 13.
- Bhutta, ZA. Infectious disease: Polio eradication hinges on child health in Pakistan. Nature News. 2014, 511, 285. [Google Scholar] [CrossRef] [PubMed]
- Loevinsohn B, Hong R, Gauri V. Will more inputs improve the delivery of health services?: Analysis of district vaccination coverage in Pakistan. The International journal of health planning and management. 2006, 21, 45–54.
- Edwards KM, Hackell JM, Diseases CoI, Practice Co, Medicine A. Countering vaccine hesitancy. Pediatrics. 2016, 138.
- Khowaja AR, Khan SA, Nizam N, Omer SB, Zaidi A. Parental perceptions surrounding Polio and self-reported non-participation in Polio supplementary immunization activities in Karachi, Pakistan: a mixed methods study. Bull World Health Organ. 2012, 90, 822–830.
- Nasir SG, Aliyu G, Ya’u I, Gadanya M, Mohammad M, Zubair M, et al. From intense rejection to advocacy: How Muslim clerics were engaged in a polio eradication initiative in Northern Nigeria. PLoS Med. 2014, 11, e1001687.
- Bhattacharjee S and Dotto C. Vaccine case study: Understanding the impact of polio vaccine disinformation in Pakistan. Available at https://firstdraftnews.org/long-form-article/first-draft-case-study-understanding-the-impact-of-polio-vaccine-disinformation-in-pakistan/.
- Pakistan Polio Eradication Program. National Emergency Action Plan for Polio Eradication 2020. Available at https://www.endpolio.com.pk/images/Stories/NEAP-2020.pdf.
- Habib MA, Soofi S, Cousens S, Anwar S, Haque N, Ahmed I, Ali N, Tahir R, Bhutta ZA. Community engagement and integrated health and polio immunisation campaigns in conflict-affected areas of Pakistan: a cluster randomised controlled trial. The Lancet Global Health. 2017, 5, e593–e603.
Figure 1.
Survey areas in Pakistan and GIS locations of study areas in Karachi.

Web Table 1.
Study sites and sample distribution of survey.
| Karachi (18 UCs ~ 210 HH/UC ) | Bajaur (6 UCs ~ 210 HH/UC) | Pishin (10 UCs ~ 210 HH/UC) |
|---|---|---|
| Gujro, Songal, Maymarabad, Yousaf Goth, Mangopir, Godhra, Gulshan-e-Ghazi, Itehad Town, Islam Nagar, Nai Abbadi, Saeedabad, Muslim Mujahid Colony, Muhajir Camp, Islamia Colony, Pehlwan Goth, Metrovile Colony, Hijrat Colony, Baloch Goth, | Khar, Mamund, Salarzai, Nawagai, Uttamkhel, Barang | Bazar Kona, Muchan, Bazar Pishin, Karbala, Batazai, Khanozai, Bostan, Dilsora, Malikyar, Kaza Villa, |
Web Table 2.
Distribution of Qualitative components.
| Karachi | Bajaur | Pishin | ||||
|---|---|---|---|---|---|---|
| FGDs | IDIs | FGDs | IDIs | FGDs | IDIs | |
| Mothers | 4 | - | 2 | - | 2 | - |
| Fathers | 4 | - | 2 | - | 2 | - |
| Mothers in Law | 4 | - | 2 | - | 2 | - |
| Community influencers | - | 8 | - | 4 | - | 4 |
| Health Care Providers | - | 8 | - | 4 | - | 4 |
| 12 | 16 | 6 | 8 | 6 | 8 | |
Table 1.
Basic demographic information of study sites.
| Karachi | Bajaur | Pishin | |
|---|---|---|---|
| Indicators | |||
| Union councils | 18 | 6 | 10 |
| Households surveyed | 3780 | 1258 | 2099 |
| HH density | 7.8 | 9.1 | 12.5 |
| Total population | 29381 | 11507 | 26223 |
| Male (%) | 50.8 | 51 | 49.8 |
| Total children under 5 years of age | 6181 | 2144 | 4774 |
| Male (%) | 51.73 | 53.26 | 49.79 |
| Illiteracy rate (among respondents) | 44.1 | 74.7 | 84.2 |
| Ownership of household (owned households) | 61.3 | 92.6 | 81.6 |
| Hand-washing practice (after defecation) | 99.7 | 96.5 | 92.3 |
| Water treatment practices (% treats water) | 45.3 | 31.2 | 42.3 |
Table 2.
Knowledge and Perceptions for polio and information sources.
| Karachi | Bajaur | Pishin | |
|---|---|---|---|
| Indicators | (n=3766) | (n=1258) | (n=2099) |
| Knowledge about Polio | n (%) | n (%) | n (%) |
| Yes | 3748 (99.5) | 1229 (97.7) | 2036 (97) |
| No | 18 (0.5) | 29 (2.3) | 63 (3) |
| Source of knowledge about Polio | |||
| TV | 2199 (47.1) | 199 (15.8) | 822 (39.2) |
| Radio | 23 (0.5) | 905 (71.9) | 561 (26.7) |
| Newspaper | 49 (1.1) | 31 (2.5) | 139 (6.6) |
| Posters | 388 (8.3) | 49 (3.9) | 416 (19.8) |
| Masjid Imam | 10 (0.2) | 64 (5.1) | 274 (13.1) |
| Local leaders | 24 (0.5) | 79 (6.3) | 19 (0.9) |
| Elders | 1231 (26.4) | 330 (26.2) | 526 (25.1) |
| Neighbours | 368 (7.9) | 169 (13.4) | 445 (21.2) |
| Friends | 131 (2.8) | 66 (5.3) | 264 (12.6) |
| Relatives | 682 (14.6) | 235 (18.7) | 348 (16.6) |
| Doctor | 592 (12.7) | 629 (50) | 451 (21.5) |
| Hakeem | 0 (0) | 1 (0.1) | 29 (1.4) |
| Homeopathic doctor | 0 (0) | 0 (0) | 14 (0.7) |
| Quack | 0 (0) | 0 (0) | 16 (0.8) |
| LHV | 13 (0.3) | 28 (2.2) | 26 (1.2) |
| Nurse | 0 (0) | 2 (0.2) | 27 (1.3) |
| Traditional healer | 0 (0) | 0 (0) | 8 (0.4) |
| LHWs | 58 (1.2) | 339 (27) | 822 (39.2) |
| Vaccinators | 36 (0.8) | 364 (28.9) | 83 (4) |
| Others | 37 (0.8) | 8 (0.6) | 29 (1.4) |
| Consider Polio as a health problem | |||
| Yes | 3482 (92.5) | 1088 (86.5) | 1267 (60.4) |
| No | 90 (2.4) | 69 (5.5) | 231 (11) |
| Don't know | 194 (5.2) | 101 (8) | 601 (28.6) |
| Knowledge about preventing a child from Polio | |||
| By proper disposal of waste/sewage | 487 (10.4) | 245 (19.5) | 607 (28.9) |
| By vaccinating a child/person/polio drops | 2643 (56.6) | 811 (64.5) | 1066 (50.8) |
| Avoiding contact with an infected child/ person | 86 (1.8) | 96 (7.6) | 305 (14.5) |
| Washing hands with soap and water | 204 (4.4) | 69 (5.5) | 196 (9.3) |
| Others | 997 (21.4) | 6 (0.5) | 9 (0.4) |
| Don't know | 426 (9.1) | 139 (11.1) | 438 (20.9) |
| Knowledge about how a child gets polio disease | |||
| By drinking dirty water | 602 (12.9) | 246 (19.6) | 701 (33.4) |
| By eating dirty food | 624 (13.4) | 318 (25.3) | 543 (25.9) |
| Through sewage contamination of food/water | 372 (8) | 300 (23.9) | 441 (21) |
| By air/breath | 34 (0.7) | 117 (9.3) | 452 (21.5) |
| By evil eye | 48 (1) | 212 (16.9) | 442 (21.1) |
| Don't know | 1626 (34.8) | 73 (5.8) | 367 (17.5) |
| Allah's will | 793 (17) | 452 (35.9) | 842 (40.1) |
| Others | 403 (8.6) | 4 (0.3) | 3 (0.1) |
| Knowledge about polio transmission | |||
| By air/breath | 262 (5.6) | 596 (47.4) | 855 (40.7) |
| By evil eye | 28 (0.6) | 152 (12.1) | 359 (17.1) |
| By contaminated water | 389 (8.3) | 183 (14.6) | 496 (23.6) |
| By sewage contamination | 707 (15.2) | 191 (15.2) | 697 (33.2) |
| Through polio vaccines | 43 (0.9) | 258 (20.5) | 160 (7.6) |
| Don't know | 2543 (54.5) | 334 (26.6) | 773 (36.8) |
| Others | 228 (4.9) | 0 (0) | 8 (0.4) |
| Knowledge about preventive measures for Polio | |||
| Completing routine EPI immunization | 2485 (53.3) | 900 (71.5) | 1365 (65) |
| Completing routine EPI immunization plus getting your child vaccinated in NIDs | 1327 (28.4) | 248 (19.7) | 473 (22.5) |
| Proper nutrition of child | 847 (18.2) | 116 (9.2) | 561 (26.7) |
| Proper hygiene | 1331 (28.5) | 288 (22.9) | 226 (10.8) |
| Proper care | 510 (10.9) | 138 (11) | 138 (6.6) |
| Keeping child away from the sick child | 147 (3.2) | 302 (24) | 651 (31) |
| Proper sewage disposal and sanitation | 99 (2.1) | 75 (6) | 178 (8.5) |
| Others | 429 (9.2) | 0 (0) | 7 (0.3) |
| Do not know | 282 (6) | 57 (4.5) | 247 (11.8) |
Table 3.
Knowledge & Perceptions of polio vaccines.
| Karachi | Bajaur | Pishin | |
|---|---|---|---|
| Indicators | (n=3766) | (n=1258) | (n=2099) |
| Knowledge about oral polio vaccine | n (%) | n (%) | n (%) |
| Yes | 3759 (99.8) | 1253 (99.6) | 2044 (97.4) |
| No | 7 (0.2) | 5 (0.4) | 55 (2.6) |
| Knowledge about OPV protects from Polio | |||
| Yes | 3347 (88.9) | 1186 (94.3) | 1445 (68.8) |
| No | 55 (1.5) | 21 (1.7) | 25 (1.2) |
| Don't know | 71 (1.9) | 30 (2.4) | 342 (16.3) |
| Not sure | 293 (7.8) | 21 (1.7) | 287 (13.7) |
| Knowledge about the consequences of not giving OPV | |||
| Child gets Polio | 2419 (64.2) | 669 (53.2) | 1208 (57.6) |
| The child will not get Polio | 919 (24.4) | 359 (28.5) | 492 (23.4) |
| Polio would not be eradicated from Pakistan | 172 (4.6) | 111 (8.8) | 191 (9.1) |
| Don't know | 256 (6.8) | 119 (9.5) | 208 (9.9) |
| Perceptions about the safety of OPV | |||
| Completely safe | 2891 (76.8) | 791 (62.9) | 880 (41.9) |
| Reasonably safe | 517 (13.7) | 353 (28.1) | 405 (19.3) |
| Not safe at all | 179 (4.8) | 16 (1.3) | 199 (9.5) |
| Others | 4 (0.1) | 0 (0) | 0 (0) |
| Don't Know | 175 (4.7) | 97 (7.7) | 615 (29.3) |
| Ever refused to give polio drops to your child? | |||
| Never | 2897 (76.9) | 943 (75) | 1689 (80.5) |
| Once | 294 (7.8) | 209 (16.6) | 111 (5.3) |
| More than once | 420 (11.2) | 92 (7.3) | 290 (13.8) |
| Always | 137 (3.6) | 14 (1.1) | 5 (0.2) |
| Other | 18 (0.5) | 0 (0) | 4 (0.2) |
| Are all your children immunized with OPV? | |||
| Yes | 3543 (94.1) | 1162 (92.4) | 1996 (95.1) |
| No | 95 (2.5) | 16 (1.3) | 33 (1.6) |
| Partially | 99 (2.6) | 32 (2.5) | 42 (2) |
| Not at all | 20 (0.5) | 3 (0.2) | 2 (0.1) |
| Don't know | 9 (0.2) | 45 (3.6) | 26 (1.2) |
| Did your child/children receive OPV during the recent campaign | |||
| Yes | 3526 (93.6) | 1241 (98.7) | 2067 (98.5) |
| No | 238 (6.3) | 14 (1.1) | 18 (0.9) |
| Don't know | 2 (0.1) | 3 (0.2) | 14 (0.7) |
| Decision-maker regarding the health matters of the children? | |||
| Mother-in-law | 419 (9) | 353 (28.1) | 769 (36.6) |
| Father-in-law | 136 (2.9) | 359 (28.5) | 633 (30.2) |
| Husband | 2304 (49.4) | 763 (60.7) | 1812 (86.3) |
| Mother my self | 2212 (47.4) | 259 (20.6) | 363 (17.3) |
| Other | 65 (1.4) | 0 (0) | 1 (0.1) |
| Decision-maker regarding the immunization of the children? | |||
| Mother-in-law | 336 (8.9) | 158 (12.6) | 201 (9.6) |
| Father-in-law | 92 (2.4) | 256 (20.4) | 244 (11.6) |
| Husband | 1562 (41.5) | 703 (55.9) | 1593 (75.9) |
| Mother/my self | 1717 (45.6) | 139 (11.1) | 59 (2.8) |
| Others | 59 (1.6) | 2 (0.2) | 1 (0.1) |
Table 4.
Reasons for refusals of OPV (Ever Refused).
| Karachi | Bajaur | Pishin | |
|---|---|---|---|
| Reasons | |||
| Reasons for refusing Polio drops to child? | n (%) | n (%) | n (%) |
| Vaccine is not halal | 21 (2.4) | 10 (3.2) | 187 (45.6) |
| Vaccine can cause sterility | 163 (18.8) | 62 (19.7) | 280 (68.3) |
| Vaccine is not safe | 162 (18.6) | 11 (3.5) | 161 (39.3) |
| Child has got Polio drops too many time | 31 (3.6) | 67 (21.3) | 93 (22.7) |
| Community/local leader prohibited | 0 (0) | 0 (0) | 4 (1) |
| Against my religious belief | 6 (0.7) | 0 (0) | 19 (4.6) |
| Others | 227 (26.1) | 42 (13.3) | 13 (3.2) |
| Total | 869 | 315 | 410 |
| Reasons for not giving OPV in the last polio campaign | |||
| Polio team did not visit the houses | 86 (26.5) | 90 (86.5) | 92 (83.6) |
| Did not know about OPV | 53 (16.3) | 6 (5.8) | 5 (4.6) |
| Went, but distribution point had run out of OPV | 3 (0.9) | 1 (1) | 4 (3.6) |
| Child was not at home at time of visit | 2 (0.6) | 0 (0) | 1 (0.9) |
| Child was sick | 13 (4) | 2 (1.9) | 1 (0.9) |
| Distribution site is far away | 24 (7.4) | 0 (0) | 1 (0.9) |
| Family members/elders did not allow the child to get OPV | 99 (30.5) | 5 (4.8) | 5 (4.6) |
| Others | 45 (13.9) | 0 (0) | 1 (0.9) |
| Don't Know | 86 (26.5) | 90 (86.5) | 92 (83.6) |
| Total | 223 | 96 | 103 |
Table 5.
Comparison of KAP survey 2020 and 2012.
| Karachi | Bajaur | Pishin | ||||
|---|---|---|---|---|---|---|
| Indicators | 2012 | 2020 | 2012 | 2020 | 2012 | 2020 |
| Respondent's knowledge about Polio | 94.1 | 99.5* | 97.5 | 97.7 | 98.4 | 97.0 |
| Respondent considers Polio as a health problem | 92.2 | 92.5 | 85.6 | 86.5 | 77.6 | 60.4* |
| Respondents having Knowledge about OPV | 99.3 | 99.8 | 96.8 | 99.6 | 97.8 | 97.4 |
| Perceptions about the safety of OPV completely safe | ||||||
| Completely safe | 76.5 | 76.8 | 61.6 | 62.9 | 49.7 | 41.9 |
| Reasonably safe | 11.2 | 13.7 | 11 | 28.1 | 28.9 | 19.3 |
| Not safe at all | 1.1 | 4.8 | 2.7 | 1.3 | 1.4 | 9.5 |
| Don't Know | 11.2 | 4.7 | 24.7 | 7.7 | 19.7 | 29.3 |
| Ever refused for OPV | 5.0 | 23.1* | 17.4 | 25.0* | 20.0 | 19.5 |
| Immunization card available | 26.4 | 47.7 | 12.9 | 78.1 | 6.9 | 44.5 |
| Immunization status | ||||||
| Fully immunized | 52.3 | 55.5* | 28.3 | 67.8* | 56.5 | 68.6* |
| Partially immunized | 27.9 | 35.1 | 35.4 | 27.3 | 17.2 | 18.0 |
| Un immunized | 19.8 | 9.4* | 35.1 | 5.0* | 25.6* | 13.4 |
*Represents significant difference P<0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



