
Submitted:
09 April 2023
Posted:
10 April 2023
You are already at the latest version
Abstract
The standard treatment for early-stage lung cancer is complete tumor excision by limited resection of the lung. Pre-operative localization is used before video-assisted thoracoscopic surgery (VATS) to improve the accuracy of pulmonary nodule excision. However, lung atelectasis and hypoxia resulting from controlling apnea during the localization procedure may affect the localization accuracy. Pre-procedural pulmonary recruitment may improve respiratory mechanics and oxygenation during localization. In this study, we investigated the potential benefits of pre-localization pulmonary recruitment prior to pulmonary ground-glass nodule localization in a hybrid operating room. We hypothesized that pre-localization pulmonary recruitment would increase localization accuracy, improve oxygenation, and prevent the need for re-inflation during the localization procedure. We retrospectively enrolled patients with multiple pulmonary nodule localizations before surgical intervention in our hybrid operating room. We compared localization accuracies between patients who had undergone pre-procedure pulmonary recruitment and patients who had not. Saturation, re-inflation rate, apnea time, procedure-related pneumothorax, and procedure time were also recorded as secondary outcomes. Patients who had undergone pre-procedure recruitment had better saturation, shorter procedure time, and higher localization accuracy. The pre-procedure pulmonary recruitment maneuver was effective in increasing regional lung ventilation, leading to improved oxygenation and localization accuracy.
Keywords:
Hybrid computer tomography
; pulmonary ground glass nodule localization
; video-assisted thoracic surgery
; pulmonary recruitment
1. Introduction
Lung cancer was the leading cause of cancer-related deaths worldwide in 1990 Bray, et al. [1]. The Taiwan Lung Cancer Screening in Never Smoker Trial (TALENT) revealed an approximately 2.6% lung cancer detection rate in Taiwan. In all, 96.5% of lung cancer cases were detected at stage 0–1. VATS has improved the long-term survival rate of lung cancer and provides a minimally invasive approach for the removal of pulmonary nodules [2]. However, early lung adenocarcinomas are difficult to palpate during VATS and unfeasible to pathologically evaluate from fine needle aspiration or biopsy [3]. Therefore, preoperative and intraoperative localization, using materials such as microcoils, hookwires, contrast media, dyes, and fluorescence tracers, is important for thoracic surgeons [4]. Several techniques have recently been proposed for preoperative or intraoperative pulmonary nodule localization, including “two-stage” localization using conventional computer tomography and “one-stage” localization in a hybrid operating room. Computer tomography-guided localization in a hybrid operating room followed by immediate resection has been shown to be a safe and efficient localization technique, reducing the “risky period” [5,6,7]. However, pulmonary localization in a hybrid operating room requires general anesthesia with endotracheal intubation and localization in the same end-inspiratory phase. During general anesthesia, lung atelectasis develops in 90% of patients because of muscle paralysis, intravenous or inhalational anesthetics, and surgical position [8,9]. This lung atelectasis may progress rapidly during apnea in the end-inspiratory phase, resulting in a hypoxia event and interfering with the final localization accuracy. In a single pulmonary ground glass nodule localization, the total apnea time is around 1-2 minutes, whereas in the localization of multiple pulmonary ground glass nodules, the full localization procedure typically takes 3–5 minutes and may take longer depending on the location or number of lesions. Appropriate ventilator settings and experienced localization teamwork are important issues for the procedure.
Prompt pulmonary recruitment in the perioperative phase has been proven to improve respiratory mechanics, chest wall compliance, and oxygenation in patients undergoing abdominal and cardiothoracic surgery [8,9,10]. In this clinical study, we sought to identify the benefits of pre-procedure pulmonary recruitment prior to pulmonary ground glass nodule localization in a hybrid operating room. We hypothesized that pulmonary recruitment would improve oxygenation, prevent the need for re-inflation during the multiple pulmonary ground glass nodules localization procedure, and further increase the localization accuracy.
2. Materials and Methods
We retrospectively reviewed all patients who underwent hybrid operating room multiple pulmonary nodule localization before surgical intervention at Chung Shan Medical University Hospital (CSMUH) between January 1, 2022 and December 31, 2022. The inclusion criteria were: (1) age greater than 18 years, (2) lung function examination classification as low risk on the American College of Chest Physicians (ACCP) perioperative surgical risk evaluation (both forced expiratory volume and diffusion capacity of carbon monoxide ≧ 80 percent predicted), and (3) multiple pulmonary ground glass nodules for localization. In all, 23 patients underwent pre-procedure pulmonary recruitment, and 69 patients did not undergo recruitment. The decision to perform pre-procedure pulmonary recruitment was based on the surgeon’s and anesthesiologist’s preference and recorded in the anesthesia record. Details of the inclusion, exclusion, and classification of patients in the study are shown in Figure 1. Perioperative parameters, including pulse oximetry, apnea time, re-inflation rate, pneumothorax, and total procedure time were analyzed. This study was approved by the CSMUH Ethics Committee (Approval No. CS1-23036).
All patients underwent chest computed tomography with contrast and had a multidisciplinary team review their case prior to their operation. The size of patients’ lesions was between 4 and 15 mm as shown on the CT prior to their operation. The solid portion of the pulmonary lesions in our study were less than 10 mm and all the lesions are eligible for wedge resection as both diagnostic and therapeutic surgery based on the Japan Clinical Oncology Group (JCOG) 0804 trial [11].
Each patient underwent double-lumen endotracheal tube intubation in the supine position after induction. After positioning the patient into decubitus or 30^ lateral tilt position, the anesthesiologist confirmed the double-lumen endotracheal tube position by bronchoscopy, ensuring pulmonary recruitment and ventilation safety. The pre-procedural recruitment maneuver was performed with sustained inspiration pressure at 30 cmH2O for 30 seconds by the anesthesia workstation (Aisys CS2™ anesthesia workstations, General Electric Healthcare, Chicago, IL). After recruitment, the radiologist and the thoracic surgeon perform the pre-procedural scan for localization planning. The localization hookwires placement or dye injection are dependent on the lesion to pleura distance; the lesions with dye injection did not exceed 20 mm to the pleura. After localization, the patient immediately underwent the VATS operation in the hybrid operation room. When the resected nodule was diagnosed as adenocarcinoma in situ (AIS) or adenocarcinoma in situ at least (AIS at least) based on the frozen section, we closed the incision without additional lung resection. If invasive adenocarcinoma or another histological tumor was confirmed, we then checked the lesions size and considered performing lobectomy or segmentectomy as extensive resection. The entire algorithm of multiple pulmonary ground glass nodule localization procedure and surgery is shown in Figure 2.
The hybrid localization system was implemented using C-arm CBCT (ARTIS Pheno ®; Siemens Healthcare GmbH, Erlangen, Germany) and localization data (such as distance between the chest wall to the nodule and characteristics of the nodule) were obtained from the hybrid room software. Saturation was recorded using pulse oximetry via a sensor from the contralateral fingernail bed, displayed in the anesthesia workstations and the localization monitor. These parameters were based on previous literature and our anesthesiologist’s preference [12,13]. Ventilation during localization was performed in pressure control and volume guarantee mode (PCV-VG) or volume control mode (VCV). The tidal volume was set at 8-10 mL/kg predicted body weight and fraction of inspired oxygen (FiO2) was set at 50%. Re-inflation was performed if pulse oximetry was < 90% (SpO2 < 90). Apnea time was recorded by the anesthesiologist, starting with localization and ending with completion of the procedure successfully without SpO2 < 90. The localization accuracy was determined using the hybrid computed tomography film with the distance between the localization needles and the lesion not exceeding 5 mm in a three-dimensional view. The film was reviewed immediately after the procedure by two radiologists. The secondary outcomes were apnea time, saturation, re-inflation rate, procedure time, and pneumothorax rate.
The significance of differences between the two groups was evaluated using the χ2-test, Fisher's exact test, and Mann-Whitney U test. The localization accuracy and rate of re-inflation were calculated using multivariate analysis with logistic regression and odds ratios. Statistical significance was defined as p< 0.05. All statistical analyses were performed using Statistical Package for Social Sciences (IBM SPSS Statistics, version 25) and Excel software (Microsoft Corporation, Seattle, WA, USA).
3. Results
Ninety-two patients had multiple pulmonary ground glass nodule localizations in the CSMUH hybrid operating room between January 1, 2022 and December 31, 2022 (Figure 1). Table 1 shows the characteristics of the patients included in the study. Most of our patients had two pulmonary lesions (N = 63, 68.5%), 18 patients had three pulmonary lesions (N = 18, 19.6%), and 11 patients (N = 11, 12.0%) had four pulmonary lesions. All pulmonary localization procedures were completed using a tidal volume of at least 8–10 mL/kg, based on our anesthesiologist’s previous experience. Twenty-one patients underwent contralateral wedge resection before multiple pulmonary nodule localizations (N = 21, 22.8%). Most pulmonary nodule localization procedures were completed in the pressure control and volume guarantee mode (N = 83, 77.2%), and few localization procedures were completed in volume control mode (N = 9, 22.8%). There were no significant differences in age, sex, height, weight, body mass index, preoperative pulmonary function, functional vital capacity (FVC), forced expiratory volume in 1s (FEV1), diffusing lung capacity for carbon monoxide (DLCO), lesion numbers, and other localization characteristics between the groups.
Most of the patients had wedge resection of the lung when frozen section confirmed only AIS or adenocarcinoma of the lung with only a small proportion of solid part, whereas five patients (7.2%) in the non-recruitment group and two patients (8.7%) in the recruitment group underwent segmentectomy and lobectomy, respectively, after pathologic diagnosis of lung adenocarcinoma or to achieve an adequate resection margin. There was no hookwires dislodgment induced by lobectomy in our study. There was no significant difference in surgery type between the groups.
The final pathology reports showed primary pulmonary malignancy in 177 nodules, including invasive adenocarcinoma, AIS, and minimally invasive adenocarcinoma (MIA). There were only five secondary pulmonary malignancies, comprising metastasis from clear-cell renal cell carcinoma, nasopharyngeal carcinoma, and hepatocellular carcinoma (five nodules in three patients); all were treated with wedge resection. There were also 42 nodules composed of fibrosis or chronic inflammation. There was no significant difference in the pathology report between the groups.
Twenty-three patients underwent pulmonary recruitment prior to their localization (25.0%), and 69 patients did not (75.0%). The average total procedure time across both groups was 20.0 min (Table 2). However, the recruitment group had significantly shorter procedure times (median 17 vs. 19 min, p = 0.043). Twenty-nine patients developed pneumothorax after the localization (N = 29, 31.5%), none of which required immediately thoracentesis due to iatrogenic pneumothorax for procedure completion. There was no significant difference in apnea time (median 5.60 vs 5.90 minutes, p = 0.658) or in the incidence of post-procedural pneumothorax (median 66.7% vs 73.9, p = 0.610) between the two groups. However, the recruitment group had better saturation (92% vs. 88%, p = 0.016) and higher localization accuracy (82.6% vs. 55.1%, p = 0.025) at the end of the procedure.
A univariate logistic regression revealed that pre-procedure recruitment, history of lung operation, and BMI were all factors associated with localization accuracy (odds ratio, 0.23, 0.25, and 0.76, respectively). Pre-procedure recruitment, history of lung operation, and higher BMI were also significant predictors in the multivariate logistic analysis of localization accuracy (Wald’s test p = 0.024, 0.033, and 0.002, respectively, Table 3).
A univariate logistic regression revealed that pre-procedure recruitment and higher lesion number were both factors associated with the need for re-inflation during localization (odds ratio, 3.09 and 1.87, respectively). However, pre-procedure recruitment was the only significant factor in the multivariate logistic analysis for the need for re-inflation during localization (Wald’s test p = 0.043, Table 4).
4. Discussion
This study highlights the importance of pre-procedural pulmonary recruitment in the preoperative localization of partial solid ground glass nodules of the lung in hybrid operation rooms. We believe this study to be the first of its kind that examines the application of pulmonary recruitment in hybrid operation room localization. Compared to traditional two-stage localization in CT rooms, one-stage localization in hybrid operation rooms by a thoracic surgeon can avoid delayed treatment of localization-related complications. In addition, the localization performed by the thoracic surgeon can guide the resection planning based on the accuracy of the localization. This is a crucial step in the preoperative planning of lung cancer surgeries, as it allows the surgeon to accurately locate and remove the partially solid ground glass nodule of the lung while minimizing the risk of damage to healthy tissue.
The accurate localization of these partially solid nodules is essential for successful limited resection of lung. However, during the localization process, regional atelectasis can occur, which can cause uneven lung collapse and interfere with the accuracy of the procedure. Research has shown that the amount of atelectasis is affected by the patient's BMI and apnea time, and can be minimized by pulmonary recruitment [14,15]. In obese patients, an impeded diaphragm and muscle weakness limit the ability to hold their breath for an extended period, resulting in less apnea time and potentially accelerated atelectasis [16]. This physiology limitation may accelerate the atelectasis and result in difficult localization accuracy. The number of lesions is another important factor in accuracy. In our experience in single pulmonary ground glass nodule localization, the apnea time is always < 2 min and most patients will not develop atelectasis interfering the localization accuracy as evidenced by the final hybrid CT film review. However, in multiple ground glass nodules localization, the apnea time lasted approximately 5 to 6 min resulting in increased oxygen consumption during the apnea phase and increased risk of atelectasis formation. The region of collapsed lung can significantly alter the localization plan from the pre-scan planning and thereby affect the accuracy of the procedure. In patients undergoing a contralateral lung operation, the atelectasis between the bilateral lung fields is typically uneven and may interfere with the accuracy of the localization. However, we found that after patients underwent pre-procedure recruitment, the atelectasis lung alveolar re-expansion kept the entire lung field open, causing the lung to collapse much more evenly during the localization procedure. As showed in Table 3, pre-procedural pulmonary recruitment had a positive effect on elevation accuracy, and a history of contralateral wedge resection and high BMI interfered with the localization accuracy with statistical significance (p = 0.024, 0.033 and 0.002 respectively).
In the literature review, various methods of pulmonary recruitment were discussed, including stepwise incremental PEEP, stepwise increase in tidal volume to a plateau pressure of 30 cm H2O, and sustained inflations to a peak inspiratory pressure of 30-40 cm H2O [13,17,18,19]. However, there remains uncertainty about which pulmonary recruitment method is best for use in general anesthesia, one-lung ventilation, or pre-localization recruitment in clinical practice. To determine the success of pulmonary recruitment, various physiological measurements such as arterial partial oxygen pressure (PaO2) plus arterial partial pressure of carbon dioxide (PaCO2) greater than 400 mmHg, or electrical impedance tomography may be used [20,21]. However, in general anesthesia practice these measurements may not always be practical. As a result, sustained inspiration pressure at 30 cm H2O for 30 seconds by the anesthesia workstation may be chosen as a pulmonary recruitment method due to its time efficiency and effectiveness. An inappropriate position of the double-lumen endotracheal tube during pulmonary recruitment may lead to overdistension of one lobe and lung injury, which could have severe consequences for the patient. Therefore, proper positioning of the double-lumen endotracheal tube should always be ensured before the initiation of any pulmonary recruitment technique.
In this study, we defined localization accuracy as 5 mm in three-dimensional post-procedure CT, despite several studies having considerably different definitions of the accuracy of pulmonary ground glass nodule localization [22,23]. The more precise localization not only increased the lung parenchymal preservation, but also applied the safety margin much more easily. Most of the partially solid ground glass nodules of lung are around 6-10 mm in our study. The distance between the localization needles and the lesion did not exceed 5 mm, approximately equal to the half of the tumor size, making it easy to apply the surgical stapler for wedge resection of lung in our surgical experience. In our study, we choose localization hookwires and patent dye as the localization materials, although some comparative studies showed that hookwires have a lower success rate compared with Lipiodol localization and microcoils localization. Some hookwires dislodgment or migration can occur after localization and may require extensive lung parenchymal resection or lobectomy of lung for hookwires removal [4,24,25]. We choose a 20-gauge Chiba needle (Hakko Co., Naganogen, Japan) as the vector to deliver the localization hookwires. Once the hybrid room CT confirmed the Chiba needle hit the target of localization, the hookwires were delivered carefully.
Hypoxia during the apnea phase of the localization was another issue in this study. Hypoxia is the leading cause of anesthesia-related mortality, and patients with hypoxia require immediate oxygenation [26,27]. A previous observational study found that mild hypoxia (SpO2 86–90%) lasting from 2 to 30 min developed in more than half of the patients who underwent surgery [28]. Perioperative hypoxia events increase the incidence of cardiac complications and delirium [29,30]. In an in vivo rat model, local hypoxia resulting from lung atelectasis also induced an inflammatory response [31]. Perioperative hypoxia events are associated with obesity, age, chronic obstructive pulmonary disease, interstitial lung disease, and history of lung surgery, especially lobectomy [32,33]. A previous study found only a mild vital capacity change after wedge resection, which was recovered after 12 months [34]. In our study, 39 (N = 39, 42.4%) patients developed desaturation (SpO2 < 90%) during the apnea phase of the localization procedure and needed re-inflation. The pre-procedural pulmonary recruitment group had better saturation and fewer desaturation events during localization (SpO2 92% vs. 88%, re-inflation 26.1% vs. 35.9%). In multivariate logistic regression analysis, only pre-procedural recruitment was a significant predictor for the need for re-inflation (odds ratio 2.99, Wald’s test, p = 0.043). A history of contralateral wedge resection, lesion numbers, BMI, and ventilator mode were not associated with hypoxia and re-inflation rate. None of our patients had adverse effect after the hypoxia events.
One solution to apnea phase-related hypoxia is to conduct the localization procedure without any respiratory hold. However, as inspiration and expiration continue, in some electromagnetic navigation-guided localization software the target motion between inspiration and expiration will be recorded and may increase from 5 mm to 18 mm [23]. These respiratory motions maybe unremarkable in the traditional CT room but may prevent an adequate image for pulmonary nodule localization due to severe motion artifacts. This contrasts with the “two-stage” preoperative CT-guided pulmonary nodule localization. Another solution to apnea phase-related hypoxia is to provide high inspiratory fraction oxygenation 2–3 min before the procedure for reduction of the alveolar nitrogen fraction and elevation of alveolar oxygenation [35]. However, high alveolar oxygenation may lead to rapid absorption atelectasis, which may cause lung atelectasis within 2 min [36,37,38]. After the onset of apnea, alveolar oxygen is consumed at 250 mL per minute, while carbon dioxide is excreted at 20 mL per minute [39]. Therefore, we regard pre-procedure pulmonary recruitment as the best way to prevent hypoxic events during the localization procedure.
Pre-procedure pulmonary recruitment is useful in maintaining lung opening and has been used to reduce postoperative pulmonary complications and acute respiratory distress syndrome for several decades [12,40]. However, no study has discussed the relationship between pulmonary recruitment and pulmonary nodule localization. Our study is the first to observe both the technical and physiological benefits of pre-procedure pulmonary recruitment in pulmonary nodule localization in a hybrid operating room. The pre-procedure pulmonary recruitment re-expanded the collapsed alveoli and improved chest wall compliance before the hybrid computer tomography scan, which prevented hypoxic events during the procedure.
This study had several limitations. First, we included only relatively healthy patients to observe the effect of recruitment on localization accuracy, patient oxygenation, and re-inflation rate. The physiological benefits of pre-procedure pulmonary recruitment may be more beneficial in patients with cardiopulmonary disease and morbidity-related obesity. Only two patients with morbid obesity (BMI: 31 and 30, based on the World Health Organization definition) were included in our study, which may underestimate the effect of pre-procedure pulmonary recruitment in patients with morbid obesity. Future studies should focus on evaluating the effects of pulmonary recruitment in a broader range of patient populations. Second, the study was not randomized, and pre-procedure pulmonary recruitment was performed based on the preference and experience of the anesthesiologist and surgeon without exact inclusion criteria. While patient characteristics were reviewed, there may have been unmeasured confounding variables that could have affected the results. A randomized controlled trial would provide more convincing evidence of the benefits of pre-procedure pulmonary recruitment. Another comparative study has been conducted in our hospital to analyze the processing of multiple ground glass nodules in the lungs of morbidly obese patients within a hybrid operation room. The study also considered various risk factors for analysis. The decision making for whether to use pre-procedure pulmonary recruitment may be made clearer by further study. Third, the study was retrospective, and the patient population undergoing pre-procedure pulmonary recruitment was not balanced with the non-recruitment group. Allocation bias may have influenced the results, and a prospective study with a well-designed protocol would be necessary to confirm the benefits of pre-procedure pulmonary recruitment. Fourth, we did not record pulmonary recruitment hemodynamics. Some studies have reported recruitment-induced hypotension, which may cause morbidities and mortality [41]. During recruitment, bilateral hyperinflation of the lung and high transpulmonary pressure promptly restricted venous return, resulting in hypotension. In our study, none of the patients developed severe hypotension during the recruitment procedure. We also included only patients classified as low risk on the ACCP perioperative surgical risk evaluation, and no cardiovascular patients were included for the study. This study has only provided preliminary evidence of the benefits of pre-procedure pulmonary recruitment in relatively healthy patients undergoing multiple partially solid ground glass nodules of lung localization in a hybrid operation room. The limitations of the study should be taken into consideration, and future studies should evaluate the effects of pulmonary recruitment in a more diverse patient population, using a randomized controlled design and assessing the safety of the procedure in high-risk patients.
5. Conclusions
In this retrospective observational study, the pre-procedure pulmonary recruitment maneuver was effective in increasing regional lung ventilation, leading to improved localization accuracy and patient oxygenation. The patient BMI, the pre-procedure pulmonary recruitment maneuver, and any history of contralateral lung wedge resection were all significant predictors of localization accuracy. Our study demonstrates the efficacy and feasibility of the pulmonary recruitment prior to multiple pulmonary ground glass nodule localization in the hybrid operating room. Further randomized control study is needed to confirm our observations and determine the decision criteria in the future.
Author Contributions
Conceptualization, Y.H.W. and P.C.S.,; formal analysis, Y.H.W, and K.A.; Drafting of the manuscript: Y.H.W, P.C.S and F.L.; Critical revision of the manuscript for important intellectual content: All authors. review and editing, J.Y.H. and C.C.Y. and M.C.C.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethical Review Board of the Chung Shan Medical University Hospital (CS1-23036), which approved our study.
Informed Consent Statement
Patient consent was waived by both the National Health Insurance Administration and the Institutional Review Board of Chung Shan Medical University Hospital due to the database-processing nature of the current study.
Data Availability Statement
The datasets analyzed during the current study are not available publicly due to our IRB policy but are available from the corresponding author upon reasonable request.
Acknowledgments
We greatly appreciate Jiun Yi Hsia and Chen Chih-Yi for the technical support they provided.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Lin, M.-W.; Chen, J.-S. Image-guided techniques for localizing pulmonary nodules in thoracoscopic surgery. Journal of Thoracic Disease 2016, 8, S749. [Google Scholar] [CrossRef]
- Migliore, M.; Palmucci, S.; Nardini, M.; Basile, A. Imaging patterns of early stage lung cancer for the thoracic surgeon. Journal of Thoracic Disease 2020, 12, 3349. [Google Scholar] [CrossRef]
- Park, C.H.; Han, K.; Hur, J.; Lee, S.M.; Lee, J.W.; Hwang, S.H.; Seo, J.S.; Lee, K.H.; Kwon, W.; Kim, T.H. Comparative effectiveness and safety of preoperative lung localization for pulmonary nodules: a systematic review and meta-analysis. Chest 2017, 151, 316–328. [Google Scholar] [CrossRef]
- Fang, H.-Y.; Chang, K.-W.; Chao, Y.-K. Hybrid operating room for the intraoperative CT-guided localization of pulmonary nodules. Annals of Translational Medicine 2019, 7. [Google Scholar] [CrossRef]
- Chao, Y.-K.; Pan, K.-T.; Wen, C.-T.; Fang, H.-Y.; Hsieh, M.-J. A comparison of efficacy and safety of preoperative versus intraoperative computed tomography-guided thoracoscopic lung resection. The Journal of Thoracic and Cardiovascular Surgery 2018, 156, 1974–1983. [Google Scholar] [CrossRef]
- Kwok, Y.; Irani, F.; Tay, K.; Yang, C.; Padre, C.; Tan, B. Effective dose estimates for cone beam computed tomography in interventional radiology. European radiology 2013, 23, 3197–3204. [Google Scholar] [CrossRef]
- Hu, M.-C.; Yang, Y.-L.; Chen, T.-T.; Lee, C.-I.; Tam, K.-W. Recruitment maneuvers to reduce pulmonary atelectasis after cardiac surgery: A meta-analysis of randomized trials. The Journal of Thoracic and Cardiovascular Surgery 2022, 164, 171–181. [Google Scholar] [CrossRef]
- Oh, E.J.; Lee, E.J.; Heo, B.-y.; Huh, J.; Min, J.-J. Physiological benefits of lung recruitment in the semi-lateral position after laparoscopic surgery: a randomized controlled study. Scientific Reports 2022, 12, 3909. [Google Scholar] [CrossRef]
- Pei, S.; Wei, W.; Yang, K.; Yang, Y.; Pan, Y.; Wei, J.; Yao, S.; Xia, H. Recruitment Maneuver to reduce postoperative pulmonary complications after laparoscopic abdominal surgery: a systematic review and meta-analysis. Journal of Clinical Medicine 2022, 11, 5841. [Google Scholar] [CrossRef]
- Suzuki, K.; Watanabe, S.-i.; Wakabayashi, M.; Saji, H.; Aokage, K.; Moriya, Y.; Yoshino, I.; Tsuboi, M.; Nakamura, S.; Nakamura, K. A single-arm study of sublobar resection for ground-glass opacity dominant peripheral lung cancer. The Journal of thoracic and cardiovascular surgery 2022, 163, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Cao, R.; Li, G.; Gong, T.; Ou, Y.; Huang, J. The effect of lung recruitment maneuvers on post-operative pulmonary complications for patients undergoing general anesthesia: a meta-analysis. PLoS One 2019, 14, e0217405. [Google Scholar] [CrossRef] [PubMed]
- Hartland, B.L.; Newell, T.J.; Damico, N.J.R.c. Alveolar recruitment maneuvers under general anesthesia: a systematic review of the literature. 2015, 60, 609–620. [Google Scholar] [CrossRef] [PubMed]
- Reinius, H.; Jonsson, L.; Gustafsson, S.; Sundbom, M.; Duvernoy, O.; Pelosi, P.; Hedenstierna, G.; Freden, F. Prevention of atelectasis in morbidly obese patients during general anesthesia and paralysis: a computerized tomography study. The Journal of the American Society of Anesthesiologists 2009, 111, 979–987. [Google Scholar]
- Hedenstierna, G.; Tokics, L.; Reinius, H.; Rothen, H.U.; Östberg, E.; Öhrvik, J. Higher age and obesity limit atelectasis formation during anaesthesia: an analysis of computed tomography data in 243 subjects. British journal of anaesthesia 2020, 124, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Pépin, J.L.; Timsit, J.F.; Tamisier, R.; Borel, J.C.; Lévy, P.; Jaber, S. Prevention and care of respiratory failure in obese patients. The lancet Respiratory medicine 2016, 4, 407–418. [Google Scholar] [CrossRef]
- Almarakbi, W.; Fawzi, H.; Alhashemi, J. Effects of four intraoperative ventilatory strategies on respiratory compliance and gas exchange during laparoscopic gastric banding in obese patients. British journal of anaesthesia 2009, 102, 862–868. [Google Scholar] [CrossRef]
- Pang, C.; Yap, J.; Chen, P. The effect of an alveolar recruitment strategy on oxygenation during laparascopic cholecystectomy. Anaesthesia and intensive care 2003, 31, 176–180. [Google Scholar] [CrossRef]
- Severgnini, P.; Selmo, G.; Lanza, C.; Chiesa, A.; Frigerio, A.; Bacuzzi, A.; Dionigi, G.; Novario, R.; Gregoretti, C.; de Abreu, M.G. Protective mechanical ventilation during general anesthesia for open abdominal surgery improves postoperative pulmonary function. Anesthesiology 2013, 118, 1307–1321. [Google Scholar] [CrossRef]
- Borges, J.B.; Okamoto, V.N.; Matos, G.F.; Caramez, M.P.; Arantes, P.R.; Barros, F.; Souza, C.E.; Victorino, J.A.; Kacmarek, R.M.; Barbas, C.S. Reversibility of lung collapse and hypoxemia in early acute respiratory distress syndrome. American journal of respiratory and critical care medicine 2006, 174, 268–278. [Google Scholar] [CrossRef]
- Costa, E.L.; Borges, J.B.; Melo, A.; Suarez-Sipmann, F.; Toufen, C.; Bohm, S.H.; Amato, M.B. Bedside estimation of recruitable alveolar collapse and hyperdistension by electrical impedance tomography. Applied Physiology in Intensive Care Medicine 1: Physiological Notes-Technical Notes-Seminal Studies in Intensive Care 2012, 165–170.
- Zaman, M.; Bilal, H.; Woo, C.Y.; Tang, A. In patients undergoing video-assisted thoracoscopic surgery excision, what is the best way to locate a subcentimetre solitary pulmonary nodule in order to achieve successful excision? Interactive cardiovascular and thoracic surgery 2012, 15, 266–272. [Google Scholar] [CrossRef]
- Hsu, P.-K.; Wu, Y.-C. Electromagnetic navigation-guided one-stage dual localization of small pulmonary nodules. Chest 2018, 154, 1462–1463. [Google Scholar] [CrossRef]
- Hwang, S.; Kim, T.G.; Song, Y.G. Comparison of hook wire versus coil localization for video-assisted thoracoscopic surgery. Thoracic cancer 2018, 9, 384–389. [Google Scholar] [CrossRef]
- Kleedehn, M.; Kim, D.H.; Lee, F.T.; Lubner, M.G.; Robbins, J.B.; Ziemlewicz, T.J.; Hinshaw, J.L. Preoperative pulmonary nodule localization: a comparison of methylene blue and hookwire techniques. American Journal of Roentgenology 2016, 207, 1334–1339. [Google Scholar] [CrossRef]
- Ehrenfeld, J.M.; Funk, L.M.; Van Schalkwyk, J.; Merry, A.F.; Sandberg, W.S.; Gawande, A. The incidence of hypoxemia during surgery: evidence from two institutions. Canadian journal of anaesthesia= Journal canadien d'anesthesie 2010, 57, 888. [Google Scholar] [CrossRef]
- Yuan, X.; Lee, J.W.; Bowser, J.L.; Neudecker, V.; Sridhar, S.; Eltzschig, H.K. Targeting hypoxia signaling for perioperative organ injury. Anesthesia and analgesia 2018, 126, 308. [Google Scholar] [CrossRef]
- Moller, J.; Johannessen, N.; Berg, H.; Espersen, K.; Larsen, L. Hypoxaemia during anaesthesia—an observer study. British Journal of Anaesthesia 1991, 66, 437–444. [Google Scholar] [CrossRef]
- Aakerlund, L.; Rosenberg, J. Postoperative delirium: treatment with supplementary oxygen. BJA: British Journal of Anaesthesia 1994, 72, 286–290. [Google Scholar] [CrossRef]
- Gill, N.; Wright, B.; Reilly, C. Relationship between hypoxaemic and cardiac ischaemic events in the perioperative period. British journal of anaesthesia 1992, 68, 471–473. [Google Scholar] [CrossRef]
- Duggan, M.; McNamara, P.J.; Engelberts, D.; Pace-Asciak, C.; Babyn, P.; Post, M.; Kavanagh, B.P. Oxygen attenuates atelectasis-induced injury in the in vivo rat lung. The Journal of the American Society of Anesthesiologists 2005, 103, 522–531. [Google Scholar] [CrossRef]
- Gunnarsson, L.; Tokics, L.; Gustavsson, H.; Hedenstierna, G. Influence of age on atelectasis formation and gas exchange impairment during general anaesthesia. BJA: British Journal of Anaesthesia 1991, 66, 423–432. [Google Scholar] [CrossRef]
- Ueda, K.; Kaneda, Y.; Sudou, M.; Jinbo, M.; Li, T.-S.; Suga, K.; Tanaka, N.; Hamano, K. Prediction of hypoxemia after lung resection surgery. Interactive CardioVascular and Thoracic Surgery 2005, 4, 85–89. [Google Scholar] [CrossRef]
- Mori, S.; Shibazaki, T.; Noda, Y.; Kato, D.; Nakada, T.; Asano, H.; Matsudaira, H.; Ohtsuka, T. Recovery of pulmonary function after lung wedge resection. Journal of Thoracic Disease 2019, 11, 3738. [Google Scholar] [CrossRef]
- Danish, M.A. Preoxygenation and anesthesia: A detailed review. Cureus 2021, 13. [Google Scholar]
- Joyce, C.; Williams, A. Kinetics of absorption atelectasis during anesthesia: a mathematical model. Journal of applied physiology 1999, 86, 1116–1125. [Google Scholar] [CrossRef]
- Joyce, C.; Baker, A.; Kennedy, R. Gas uptake from an unventilated area of lung: computer model of absorption atelectasis. Journal of Applied Physiology 1993, 74, 1107–1116. [Google Scholar] [CrossRef]
- Magnusson, L.; Spahn, D. New concepts of atelectasis during general anaesthesia. British journal of anaesthesia 2003, 91, 61–72. [Google Scholar] [CrossRef]
- Eger, E.; Severinghaus, J. The rate of rise of PaCO2 in the apneic anesthetized patient. In Proceedings of the The Journal of the American Society of Anesthesiologists; 1961; pp. 419–425. [Google Scholar]
- Oczenski, W.; Hörmann, C.; Keller, C.; Lorenzl, N.; Kepka, A.; Schwarz, S.; Fitzgerald, R.D. Recruitment maneuvers during prone positioning in patients with acute respiratory distress syndrome. Critical care medicine 2005, 33, 54–61. [Google Scholar] [CrossRef]
- Wesselink, E.; Kappen, T.; Torn, H.; Slooter, A.; Van Klei, W. Intraoperative hypotension and the risk of postoperative adverse outcomes: a systematic review. British journal of anaesthesia 2018, 121, 706–721. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of patient classification after initial inclusion in the study.
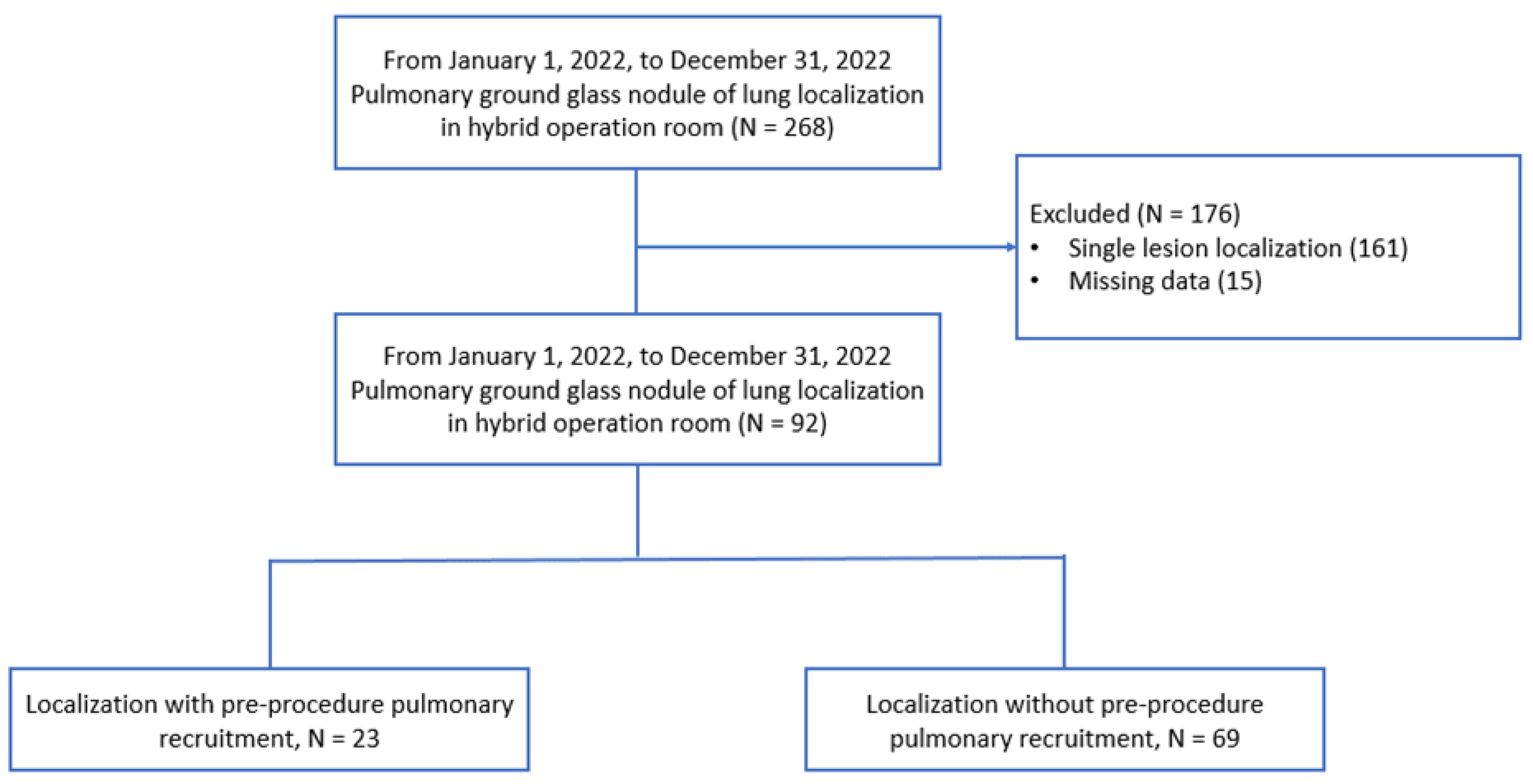
Figure 2.
Phases of multiple pulmonary ground glass nodule localization and tumor excision operation.
Figure 2.
Phases of multiple pulmonary ground glass nodule localization and tumor excision operation.
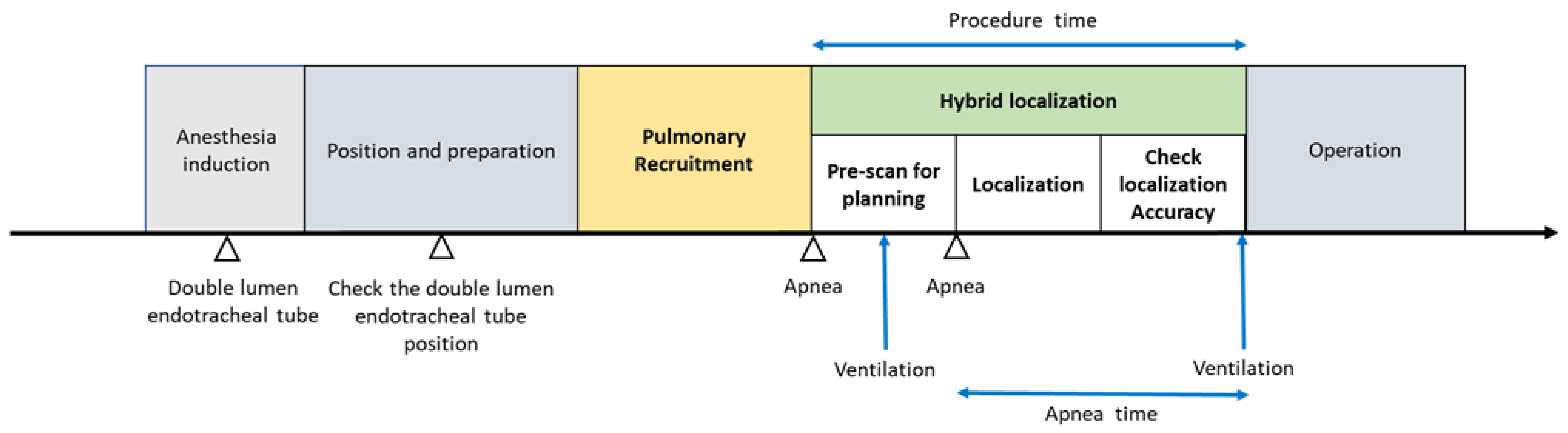

Table 1.
Characteristics of Study Patients.
| Non-recruitment group (N =69) |
Recruitment group (N =23) |
p value | |
|---|---|---|---|
| Age, median (IQR) | 53 (47 - 63) | 57 (49 - 66) | 0.281 |
| Gender | †0.778 | ||
| Female | 52 (75.4%) | 18 (78.3%) | |
| Male | 17 (25.6%) | 5 (21.7%) | |
| Height, median (IQR) | 160.0 (156.0 – 166.0) | 160.0 (155.0 – 163.0) | 0.857 |
| Weight, median (IQR) | 63.0 (55.0 – 70.0) | 57.0 (52.0 – 69.0) | 0.328 |
| BMI | 24.20 (22.20 – 26.20) | 22.80 (20.30 – 26.00) | 0.229 |
| Preoperative lung function | |||
| FVC | 102 (94 – 110) | 103 (96 – 108) | 0.921 |
| FEV1 | 97 (88 – 107) | 103 (91 – 108) | 0.195 |
| DLCO | 94 (85 – 102) | 99 (90 – 104) | 0.116 |
| History of lung contralateral wedge resection | 17 (24.6%) | 4 (17.4%) | †0.473 |
| Ventilation mode | †0.441 | ||
| VCV | 8 (11.6%) | 1 (4.3%) | |
| PCVVG | 61 (88.4%) | 22 (95.7%) | |
|
Tidal volume during procedure Median (IQR) |
550 (525 - 600) | 550 (500 - 600) | 0.281 |
| Lesions | †0.394 | ||
| 2 lesions | 47 (68.1%) | 16 (69.6%) | |
| 3 lesions | 12 (17.4%) | 6 (26.1%) | |
| 4 lesions | 10 (14.5%) | 1 (4.3%) | |
| Size (mm) | 6.90 (5.70 – 8.30) | 6.50 (5.50 – 8.20) | 0.850 |
| Dye/ hook localization | †0.146 | ||
| Dye localization | 26 (37.7%) | 13 (56.5%) | |
| Hook localization | 43 (62.3%) | 10 (43.5%) | |
| Depth, median (IQR) | 70.0 (55.0 – 80.0) | 65.0 (51.7 – 75.0) | 0.691 |
| Puncture times | †0.326 | ||
| 1 time | 64 (92.8%) | 23 (100%) | |
| > 1 time | 5 (7.2%) | 0 | |
| Extent of resection | †> 0.999 | ||
| Wedge resection | 64 (92.8%) | 21 (91.3%) | |
|
Segmentectomy + Wedge resection |
2 (2.9%) | 1 (4.3%) | |
|
Lobectomy + Wedge resection |
3 (4.3%) | 1 (4.3%) | |
| Diagnosis | †0.591 | ||
| Invasive adenocarcinoma | 6 (3.5%) | 3 (5.6%) | |
| Adenocarcinoma in situ (AIS) | 81 (47.6%) | 21 (38.9%) | |
| Minimally invasive adenocarcinoma (MIA) | 51 (30.0%) | 15 (18.5%) | |
| Secondary pulmonary malignancy | 3 (1.8%) | 2 (3.7%) | |
| Benign lesion | 29 (17.1%) | 13 (24.1%) | |
| Min, minutes; IQR, interquartile range BMI, Body mass index, FVC, forced vital capacity; FEV1, forced expiratory volume in one second; DLCO, Diffusion capacity of carbon monoxide VCV: Volume control mode PCV-VG: Pressure control and volume guarantee mode †Fisher's exact test/ Chi square test Mann-Whitney U test | |||
Table 2.
Comparisons Between the Recruitment and Non-Recruitment Groups.
| Outcome Setting | Non-recruitment Group (N =69) |
Recruitment Group (N =23) |
p value | |
|---|---|---|---|---|
|
Apnea time (Min, Median, IQR) |
5.60 (4.60 – 6.80) | 5.90 (4.80 – 6.30) | 0.658 | |
| SpO2 (%, Median, IQR) | 88.0 (84.0 – 93.0) | 94.0 (87.0 – 97.0) | 0.016 | |
| Re-inflation | †0.033 | |||
| No need for inflation | 36 (52.2%) | 17 (73.9%) | ||
| Need for inflation | 33 (35.9%) | 6 (26.1%) | ||
|
Procedure time (Min, Median, IQR) |
19.0 (15.0 – 24.0) | 17.0 (14.0 – 19.0) | 0.043 | |
| Pneumothorax | †0.610 | |||
| Pneumothorax | 46 (66.7%) | 17 (73.9%) | ||
| No pneumothorax | 23 (33.3%) | 6 (26.1%) | ||
| Accuracy (5 mm) | 38 (55.1%) | 19 (82.6%) | †0.025 | |
Min, minutes; IQR, interquartile range. †Fisher's exact test/ Chi square test. Mann-Whitney U test.
Table 3.
Predictors of Localization Accuracy.
| Accuracy | Univariant logistic regression analysis | Multivariant logistic regression analysis | ||
|---|---|---|---|---|
| Odds ratio (95% CI) |
p value | Odds ratio (95% CI) |
p value | |
| Pre-localization recruitment | 0.26 (0.08 – 0.84) |
0.024 | 0.23 (0.06 -0.82) |
0.024 |
| Lesions | 0.61 (0.33 – 1.11) |
0.106 | ||
| History of lung contralateral wedge resection | 0.29 (0.09 – 0.94) |
0.039 | 0.25 (0.07 – 0.90) |
0.033 |
| BMI | 0.76 (0.64 – 0.89) |
0.001 | 0.76 (0.64 – 0.90) |
0.002 |
| Ventilation mode | 2.43 (0.48 – 12.41) |
0.286 | ||
CI, confidence intervals. BMI, Body mass index.
Table 4.
Predictors of Re-inflation.
| Re-inflation | Univariant regression analysis | Multivariant regression analysis | ||
|---|---|---|---|---|
| Odds ratio (95% CI) |
p value | Odds ratio (95% CI) |
p value | |
| Pre-localization recruitment | 3.09 (1.08 - 8.78) |
0.034 | 2.99 (1.04 – 8.64) |
0.043 |
| Lesions | 1.87 (1.01 – 3.47) |
0.048 | 1.84 (0.97 – 3.48) |
0.084 |
| Previous lung operation | 0.43 (0.16 – 1.16) |
0.093 | ||
| BMI | 1.15 (0.99 – 1.32) |
0.055 | ||
| Ventilation mode | 0.31 (0.06 – 1.57) |
0.156 | ||
CI, confidence intervals. BMI, Body mass index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



