Submitted:
16 May 2023
Posted:
17 May 2023
You are already at the latest version
Abstract
Alzheimer’s disease (AD) and Parkinson’s disease (PD) are the two most common neurodegenerative diseases in elderly. The key histopathological features of these diseases are the presence of abnormal protein aggregates and the progressive and irreversible loss of neurons in specific brain regions. The exact mechanisms underlying the etiopathogenesis of AD or PD remain unknown, but there is extensive evidence indicating that excessive generation of reactive oxygen species (ROS) and reactive nitrogen species (RNS) along with a depleted antioxidant system, mitochondrial dysfunction, and intracellular Ca2+ dyshomeostasis play a vital role in the pathophysiology of these neurological disorders. Due to an improvement in life expectancy, the incidence of age-related neurodegenerative diseases has significantly increased. However, there is no effective protective treatment or therapy available but rather only very limited palliative treatment. Therefore, there is an urgent need for the development of preventive strategies and disease-modifying therapies to treat AD/PD. Because dysregulated Ca2+ metabolism drives oxidative damage and neuropathology in these diseases, the identification or development of compounds capable of restoring Ca2+ homeostasis and signaling may provide a neuroprotective avenue for the treatment of neurodegenerative diseases. In addition, a set of strategies to control mitochondrial Ca2+ homeostasis and signaling has been reported, including decreased Ca2+ uptake through voltage-operated Ca2+ channels (VOCCs). In this article, we review the modulatory effects of several heterocyclic compounds on Ca2+ homeostasis and trafficking, and their ability to regulate compromised mitochondrial function and associated free radical production during the onset and progression of AD or PD. This comprehensive review also describes the chemical synthesis of the heterocycles and summarizes the clinical trial outcomes.
Keywords:
Alzheimer’s disease
; Parkinson’s disease
; mitochondria
; oxidative stress
; calcium
; heterocyclic compounds
Introduction
The brain is particularly prone to oxidative insult due to a complex interconnected myriad of factors, such as high metabolic activity, neurotransmitter autoxidation, elevated content of redox active transition metals, modest antioxidant defense, glutamate excitotoxicity, and altered calcium (Ca2+) influx and associated signaling processes. An impaired antioxidant system or aberrant and sustained free radical formation can result in redox balance modifications and concomitant alteration in redox-sensitive signaling pathways. At physiological levels, brain reactive oxygen species (ROS) and reactive nitrogen species (RNS) are second messengers involved in intracellular signaling but increased levels of free radicals cause harmful effects to biological macromolecules that contribute to the aging process and the pathogenesis of neurodegenerative diseases. Lipid peroxidation (LPO) consists in the abstraction of allylic hydrogen atoms from side chains of polyunsaturated fatty acids (PUFAs) by ROS and RNS. A major deleterious outcome of LPO is the production of a variety of reactive aldehyde species, such as malondialdehyde (MDA) and 4-hydroxy-2-nonenal (4-HNE). The reaction between O2•− and NO• leads to the formation of peroxynitrite, which targets tyrosine residues in proteins via free radical addition to generate 3-nitrotyrosine (3-NT). Protein carbonylation is an oxidative stress-driven non-enzymatic and irreversible post-translational modification (PTM). Oxidative deamination of alkaline amino acids such as arginine, lysine, and histidine leads to protein carbonylation. Advanced glycation end products (AGEs) are generated in a non-enzymatic reaction among lipids, proteins or nucleic acids and reducing sugars. The interaction of AGEs with their receptors RAGEs causes oxidative stress. ROS/RNS may also interact with nucleobases of the DNA (e.g., guanine) to form 8-hydroxy-2-deoxyguanosine (8-OHdG) while oxidative RNA damage produces 8-hydroxyguanosine (8-OHG).
Compelling evidence has demonstrated that mitochondrial electron transport chain (ETC) is the major endogenous source of ROS/RNS generation, although the endoplasmic reticulum (ER) and peroxisomes can also be an important cause of free radical production [1]. Specifically, respiratory chain complexes I (NADH: ubiquinone oxidoreductase) and III (ubiquinol: cytochrome c oxidoreductase) generate high rates of O2•−. The ETC also comprises membrane-embedded proteins in the inner mitochondrial membrane that shuttle electrons from NADH and FADH2 to molecular oxygen. Simultaneously, protons are pumped from the mitochondrial matrix to the intermembrane space, thereby resulting in the reduction of oxygen to water. The energy released from these redox reactions is stored as a mitochondrial potential used to drive the phosphorylation of adenosine diphosphate (ADP) to form adenosine triphosphate (ATP). Moreover, PTMs involve enzyme-mediated covalent addition of specific functional groups (such as phosphorylation, ubiquitination, and nitration) to proteins after their synthesis. Redox-related PTMs can modulate the activity of proteins implicated in a variety of cellular signaling pathways, such as protein folding and degradation, transcription factor expression and activity, and energy metabolism by regulating the tricarboxylic acid cycle (TCA) and glycolytic enzymes, fatty acid metabolism, and protein cysteine thiol nitrosation, sulfenylation or glutathionylation. Mitochondria along with the ER play an important role in controlling intracellular Ca2+ homeostasis, which regulates several neuronal processes, including synaptic plasticity, metabolic regulation, proliferation, gene expression, and apoptosis.
Alzheimer's disease (AD) and Parkinson’s disease (PD) are two neurodegenerative diseases that share common pathological features, including protein misfolding and aggregation, synaptic impairment, mitochondrial deficits, axonopathy, and aberrant free radical production. Ca2+ can behave as a pathological effector in these neurological disorders. Cytosolic and organelle Ca2+ overload promotes its mitochondrial accumulation, which triggers the opening of the mitochondrial permeability transition pore (mPTP) and the disruption of the mitochondrial membrane potential (ΔΨm). Sustained mPTP opening leads to Ca2+ release, mitochondrial depolarization, OXPHOS disruption, compromised structural and functional integrity of the inner mitochondrial membrane, and release of cytochrome c (CYT C) and other apoptotic proteins from the outer mitochondrial membrane [2]. Ca2+ overload is mainly mediated by Aβ and tau in AD and α-synuclein (α-syn) and leucine-rich repeat kinase 2 (LRRK2) in PD. Modifications in neuronal Ca2+ influx via voltage-gated Ca2+ channels (VOCCs) and glutamate receptors promote excitotoxic Ca2+ accumulation and concomitant defective neurotransmission, impaired synaptic plasticity, damaged mitochondrial function, and increased ROS/RNS production. This review illustrates the potential therapeutic value of several heterocyclic compounds that modulate Ca2+ signaling and homeostasis and may be used as therapeutic agents for the treatment of neurodegenerative diseases.
Mitochondrial Deficiencies and Oxidative Stress as Close Partners in Alzheimer’s Disease
AD is the most common neurodegenerative disorder characterized by brain atrophy and impaired cognitive performance. Neuropathological studies have observed an extracellular accumulation of amyloid beta (Aβ) and an intraneuronal deposition of insoluble neurofibrillary tangles (NFTs) containing hyperphosphorylated tau protein. A large body of research has shown that impaired mitochondrial function (and related energy failure) is an early causative factor of AD. Brain metabolic variations would be primarily responsible for mitochondrial dysfunction in AD. Glucose deprivation leads to reduced activity in the default mode network, an area associated with atrophy and amyloid and tau deposition in AD. Positron emission tomography (PET) with [18F]-fluro-2-deoxyglucose demonstrated a progressive decline in cerebral glucose metabolism in AD patients [3]. There is a direct relationship between reduced brain regional glucose metabolism and downregulated thiamine-dependent enzyme activities, such as α-ketoglutarate dehydrogenase complex (α-KGDH) and the pyruvate dehydrogenase complex (PDHC). However, the most common feature observed in AD is a deficiency in mitochondrial complex IV (CYT C oxidase, COX), which has been reported in the cortical and hippocampal brain regions and platelets of patients [4,5]. Another specific event linked to mitochondrial failure in AD is the development of phenotypic changes in these organelles. Mitochondrial morphometric abnormalities and reduced numbers of intact mitochondria were found in AD brain specimens [6]. Mitochondrial dynamics serve as a quality control mechanism and are tightly regulated by the fusion-fission machinery, which promotes the generation or degradation of a mitochondrial syncytium. Axonal transport is a cellular mechanism that controls the active trafficking of proteins, lipids, organelles, and neurotransmitters. Mitochondrial axonal transport is tightly interconnected with mitochondrial dynamics. mRNA and protein levels of Opa1, Mfn1 and Mf2 were reduced while Drp1 and Fis1 were upregulated in postmortem brain samples from individuals with AD [7]. Excessive mitochondrial fragmentation was described in neurons from AβPP mice [8]. Mitochondrial axonal trafficking deficits and abnormal mitochondrial distribution were detected in transgenic (Tg) amyloid precursor protein (APP) mice [9].
Aβ aggregation may also determine mitochondrial function. Enhanced Aβ burden has been observed in mitochondria from autopsy specimens of late onset AD [10]. Aβ1-40 and Aβ1-42 mitochondrial internalization is mediated by the receptor components of the translocase of the outer membrane (TOM), which is independent of the ΔΨm [11]. Several familial and Aβ-based animal models of AD display systemic mitochondrial dysfunction, including decreased COX activity, impaired mitochondrial respiration, augmented glycolysis, and marked oxidative insult. Exposure to Aβ or overexpression of APP resulted in excessive mitochondrial fragmentation and abnormal mitochondrial distribution [12]. Partial reduction of Drp1 protected against Aβ/APP-induced mitochondrial and synaptic impairment. In addition, Aβ can induce S-nitrosylation of Drp1, which increases its translocation into mitochondria [13]. Ca2+ signaling and oxidative stress are important contributors to Aβ-induced mitochondrial fragmentation. Aβ promotes mitochondrial Ca2+ influx and Drp1-dependent mitochondrial fission via sustained Akt activation [14]. Misfolded tau can disrupt mitochondrial function. Accumulation of tau decreased complex I activity and ATP synthesis and altered mitochondrial dynamics [15]. Complex I immunoreactivity, α-KGDHC and transketolase enzyme activity, and mtDNA copy number were reduced in P301S tau mice [16]. AGEs were attenuated in those mice, which showed an important oxidative and nitrosative damage. Tau can also interact with Aβ to induce a synergistic detrimental effect on mitochondria by exacerbating respiratory capacity abnormalities, downregulating complex I and IV activities, and disturbing energy metabolism. Pathological p-tau exhibits lower affinity for the microtubule network, resulting in increased fission events. Either Tg P301L or P301S tau mice display a perturbed mitochondrial fusion-fission cycle. Tau ablation blocked Aβ-mediated activation of glycogen synthase kinase 3β (GSK3β) resulting in an improvement of the anterograde axonal transport of mitochondria [17].
Sustained mitochondrial dysfunction is a primary cause of an excessive generation of free radicals in AD brains and may lead to Aβ and tau pathology. Aggregation of Aβ or tau within mitochondria not only compromises the function of vital mitochondrial proteins but also increases oxidative damage. The interaction between Aβ1-40 and Aβ1-42 and mitochondrion interferes with its function and leads to mitochondrial oxidative damage, reduced COX activity, and increased content of H2O2 prior Aβ plaque formation. Aβ attenuates mitochondrial respiration and ∆Ψ generation induced by different substrates of complexes I and IV. The Aβ1–42 peptide enhances the levels of ROS by inhibiting complex I activity and membrane LPO associated with complex IV deficiencies. Furthermore, a significant increase in the GSSG/GSH ratio was observed in postmortem AD specimens, indicating a defective antioxidant defense system [18]. Free radical-mediated oxidative degradation of PUFAs is a key feature of AD. The LPO product malondialdehyde (MDA) is significantly increased in the cerebral cortex and hippocampus of AD patients [19]. Elevated levels of 4-HNE have been reported in different AD brain regions compared with age-matched controls [20]. Increased 4-HNE immunoreactivity and reduced levels of antioxidant proteins and enzymes were found in the superior temporal gyrus from APOE ε4 cases [21]. Moreover, high levels of 4-HNE and isoprostanes were reported in cerebral spinal fluid (CSF) samples of AD patients [22]. Redox proteomic analyses revealed a significant lipoxidation and nitration of several key mitochondrial enzymes, including the ATP synthase, in the hippocampus of AD subjects [23,24]. ROS-induced functional variations in the F1Fo-ATP synthase may represent a potential mechanism of OXPHOS deficiency in AD. Protein nitration is also a feature of AD. The number of 3-NT-positive neurons was robustly increased in postmortem brain samples from AD cases [25]. Protein carbonyls are increased in subjects with AD though the expression pattern varies between different brain regions. Carbonylation of proteins and AGEs plasma levels were specifically elevated in male AD patients [26]. The content of DNA strand breaks was higher in AD brains compared to controls. HPLC analysis showed a significant increase in 8-OHdG levels in DNA isolated from the brain of idiopathic AD cases while elevated 8-OHG immunoreactivity was found in the cerebral cortex of preclinical early-onset patients with AD [27].
Ca2+ Dysregulation and Downstream Effects in Alzheimer’s Disease
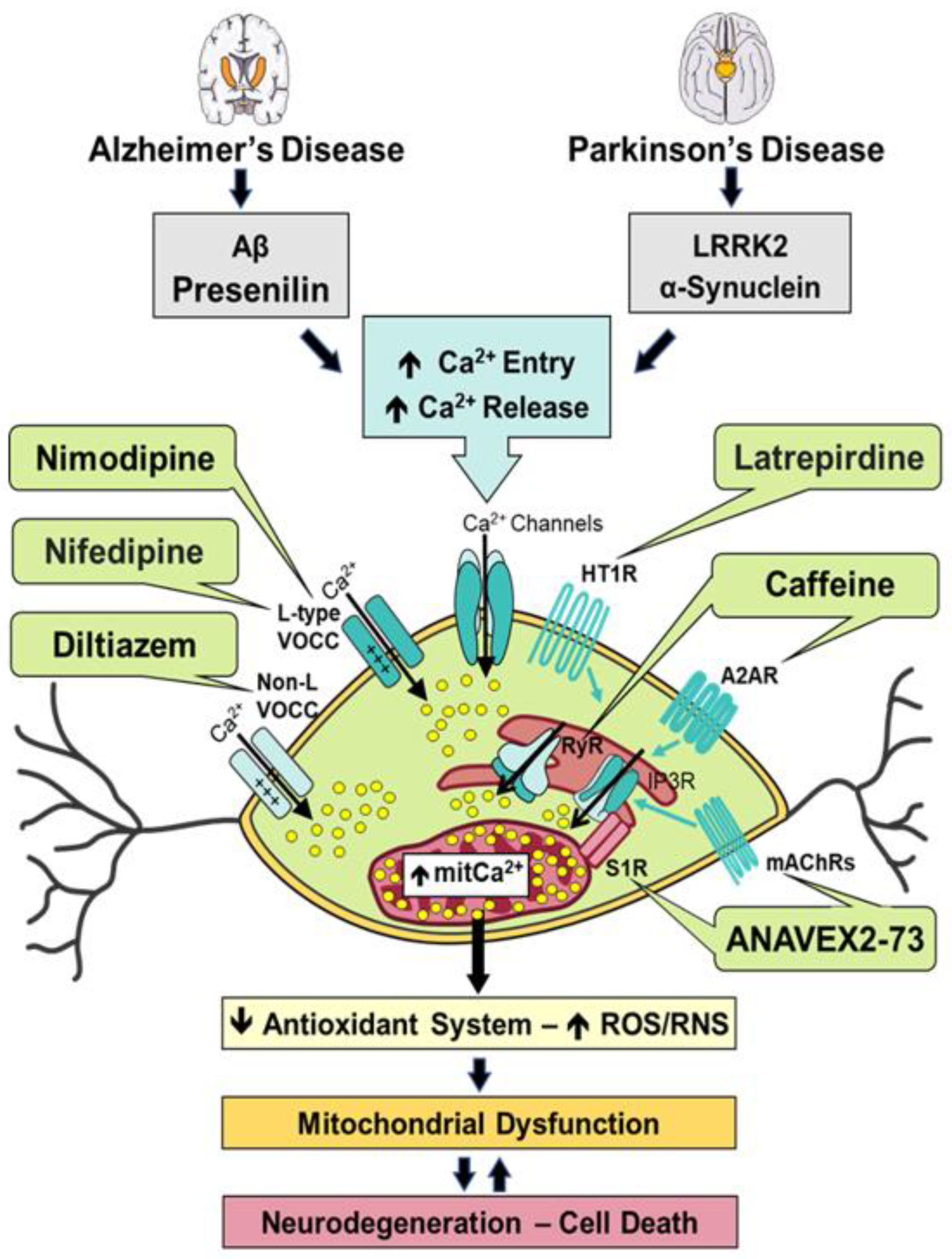
Neuronal Ca2+ signaling is mediated by activation of plasma membrane channels, including voltage-gated Ca2+ channels (VOCCs), receptor-operated Ca2+ channels (ROCCs) and Ca2+-permeable channels, such as transient receptor channels (TRP) or store-operated channels (SOCs). The opening of these channels induces Ca2+ influx with the electrochemical gradient, which is also significantly influenced by a large array of voltage-gated K+ channels that normally set the mitochondrial potential in resting conditions (Figure 1). Ca2+ signaling is also linked to the activation of Ca2+ release channels in the ER, including IP3 receptors. Release of Ca2+ from IP3-sensitive stores occurs upon the activation of G protein-coupled receptors (either glutamate metabotropic or acetylcholine muscarinic receptors) that activate phospholipase C. Moreover, activation of ryanodine receptor channels (RyRs) stimulates Ca2+ release. These channels can be activated by several messengers (including Ca2+ itself) to amplify their signaling through a Ca2+-induced Ca2+ release (CICR) mechanism. CICR mechanisms increase cytosolic free intracellular Ca2+ concentration ([Ca2+]cyt). This process is limited by endogenous Ca2+ buffers, particularly Ca2+ binding proteins (e.g., calbindin) and Ca2+ extrusion systems, such as plasma membrane Ca2+ ATPases (PMCAs), sarcoplasmic and ER Ca2+ ATPases (SERCAs), and plasma membrane and Na+/Ca2+ exchangers (NCXs) that remove Ca2+ from cytosol to the extracellular space or intracellular organelles (mainly ER). Mitochondria also influence Ca2+ levels and signaling. Cytosolic Ca2+ enters the mitochondrial matrix through the mitochondrial Ca2+ uniporter (MCU) complex, a process driven by the ΔΨm. Importantly, subtle modifications in the ΔΨm may considerably modify mitochondrial Ca2+ uptake ability [28]. Ca2+ uptake by mitochondria activates the Krebs cycle and energy production. However, mitochondrial Ca2+ overload causes oxidative stress, mPTP opening, and apoptosis. In contrast to other organelles, mitochondria cannot store Ca2+ for prolonged period, releasing it back to the cytosol in a slow fashion through the Na+-Ca2+ exchanger (NCLX).
Ca2+ hotspots or microdomains are small clusters of high concentration of Ca2+ located in so called mitochondria-associated membranes that efficiently activate the low affinity Ca2+ channel MCU. Only mitochondria in close proximity to Ca2+ channels, such as IP3 receptor channels at the ER and other Ca2+ channels at the plasma, can efficiently import Ca2+. We used mitochondria-targeted aequorin, which limits mitochondrial Ca2+ overload involved in mPTP, to monitor the coupling of Ca2+ release and mitochondrial Ca2+ uptake in the soma and neurites of neurons [29,30]. However, Ca2+ overload may occur following alterations in Ca2+ influx, release, buffers or extrusion systems, leading to neuronal death. Changes in intracellular Ca2+ homeostasis, including variations in resting levels of intracellular Ca2+ and storage, have been reported in AD. Mutations in the gene encoding presenilins (PS) 1 and 2, which process APP either directly or indirectly via Aβ production, can alter Ca2+ store content and release. The mechanism by which Aβ species induce neuronal damage is not totally understood. It has been proposed that Aβ proteins can be integrated in lipid bilayers to form Ca2+-permeable pores termed amyloid channels. We showed that Aβ1-42 oligomers increase Ca2+ influx in hippocampal neurons, followed by mitochondrial Ca2+ overload as monitored by bioluminescence imaging in individual neurons expressing mitochondria-targeted aequorin [31]. Mitochondrial Ca2+ overload induced by Aβ1-42 oligomers promote mPTP opening and subsequent CYT C release and apoptosis. A neuroprotective effect was observed after blocking mitochondrial Ca2+ uptake without affecting the increase in cytosolic Ca2+ levels. In contrast, small mitochondrial depolarization dissipated the driving force for mitochondrial Ca2+ uptake, resulting in diminished mitochondrial Ca2+ overload, release of CYT C, and apoptosis [31].
Administration of compounds targeting MCU or ΔΨm may confer protection against Aβ oligomer-induced pathology. Therefore, mitochondrial Ca2+ has become an attractive target for the development of novel AD agents. Aging plays an important role in Ca2+ homeostasis and signaling. We have developed a model of neuronal aging based on long-term culture of hippocampal neurons that, under specific conditions, acquire an aging phenotype. We showed that VOCCs-mediated Ca2+ responses following plasma membrane depolarization or toxin exposure, including the glutamate receptor agonist NMDA and Aβ oligomeric forms, were significantly elevated in aged neurons compared to young neurons [32,33]. These functional changes were related to modifications in the expression of NMDA receptor (NMDAR) subunits. Our results suggest a critical role of mitochondrial Ca2+ in neuronal death. Furthermore, our findings demonstrated that aged neurons undergo significant changes in the expression and/or activity of specific molecular players involved in Ca2+ transport, which renders them more vulnerable to damage. Long-term culture of hippocampal neurons underwent Ca2+ remodeling [34]. Aged neurons displayed a high resting [Ca2+]cyt, and Ca2+ store and release from the ER, simultaneously with an increased Ca2+ trafficking from the ER into mitochondria. Aged neurons exhibited a significant decrease in the store-operated Ca2+ entry (SOCE), a pathway related to dendritic spine stability and memory storage. Ca2+ homeostasis disruptions found in aging neurons may promote energy production but with the potential risk of increased susceptibility to mitochondrial Ca2+ overload, reduced spine stability, and neuronal loss. There is a correlation between these functional changes and altered expression of the IP3, NMDA and TLR4 receptors, the mitochondrial MCU, and the plasma membrane molecular players involved in SOCE [35]. Treatment of aged neurons with Aβ oligomers exacerbated many changes involved in Ca2+ remodeling.
The mechanism by which Aβ peptide species, particularly oligomers, cause neuronal damage remains unknown. It has been suggested that Aβ species form Ca2+ permeable pores or channels responsible for Ca2+ entry. However, a more widely accepted hypothesis proposes that Aβ oligomers bind to plasma membrane Ca2+ channels, particularly NMDAR channels. We have shown that Aβ oligomer-mediated Ca2+ responses were highly dependent on synaptic networking [36]. Generation of neural spontaneous, synchronous [Ca2+]cyt oscillations were abolished by different antagonists of synaptic transmission (NMDAR) and antagonists of action potential propagation (tetrodotoxin). Our results suggest the involvement of both NMDAR and amyloid channels in the primary response to Aβ oligomers, further enhanced by networking activity. In support of this notion, we also demonstrated that non-neuronal cells expressing NMDAR exhibit Ca2+ responses to Aβ oligomers, in contrast to cells lacking NMDA. Expression of NMDAR subunits NR1/NR2A and NR1/NR2B in these cells restored Ca2+ responses to NMDA but not to Aβ oligomers, indicating that Aβ oligomers may promote Ca2+ entry via amyloid channels and NMDAR. Aβ oligomers may also activate distant neurons intertwisted by synaptic connections, spreading excitation by recruiting additional NMDAR and specific VOCCs and leading to excessive Ca2+ entry, excitotoxicity, and neuron degeneration in AD [36]. Since dysregulated intracellular Ca2+ homeostasis plays a pivotal role in the susceptibility to neuron damage during aging, Aβ burden, PS mutations and excitotoxicity, we are currently working on the development of novel drugs targeting these pathways, specifically in the synthesis of marine heterocyclic compounds [37].
Impaired Mitochondrial Function and Associated Oxidative Damage in Parkinson’s Disease
PD is a chronic neurodegenerative disease characterized by the loss of DA neurons in the substantia nigra (SN) and their axonal projections to the striatum. A histopathological hallmark of the disease is the presence of neuronal cytoplasmic inclusions termed Lewy bodies (LB), which are predominantly composed of α-syn and, to a lesser extent, ubiquitin. SNCA and LRRK2 gene point mutations or multiplications cause familial dominant PD. It has been suggested that perturbed glucose metabolism is an early event in idiopathic PD. Using [18F]-fluro-2-deoxyglucose PET imaging, glucose hypometabolism was detected in the cerebral cortex of individuals with early-stage PD and the hippocampus and in the temporo-parietal and occipital regions of PD dementia (PDD) patients [38]. Mitochondrial defects in PD also involve morphologically abnormal mitochondria. In SN DA neurons of patients with PD, ~80% of total mitochondria exhibited an irregular shape and swollen morphology with deranged cristae patterns. Using electron microscopy, subsets of mitochondria appeared swollen and rounded or enlarged in cybrid cells prepared from platelet-derived mtDNA of sporadic PD cases [39]. In contrast to AD, the levels of thiamine remain unchanged in the plasma of PD cases. Nevertheless, free thiamine content was significantly reduced in CSF specimens of PD subjects [40]. α-KGDH enzymatic activity was declined by 50% in PD patients [41]. However, increased α-KGDH immunoreactivity was detected in the SN of patients with idiopathic PD [42]. Downregulated activity of α-KGDH, PDHC, and succinate dehydrogenase (SDH) parallel to mitigated respiratory function were observed in PC12 cells overexpressing monoamine oxidase B (MAO B) [43].
Systemic deficiencies in complex I assembly and decreased activity might result in impaired oxidative capacity, ensuing ROS/RNS overproduction, and progressive mitochondrial deficiencies, a major culprit in the degenerative process of DA neurons. Reduced complex I activity was reported in SN tissue of postmortem human samples [44,45]. Impaired catalytic activity of complex I has been found in the frontal cortex and in peripheral tissues such as, skeletal muscle, platelets and lymphocytes of late-onset PD subjects. Mounting evidence supports the notion that defects in mitochondrial dynamics are likely a common mechanism leading to mitochondrial dysfunction and neurodegenerative process in PD. OPA1 immunoreactivity was significantly attenuated in the SN tissue from patients with sporadic PD [46]. OPA1 is further linked to non-syndromic, idiopathic PD associated with aberrant changes in cristae structure and disrupted mitochondrial networks [47]. Altered trafficking along axons may represent a slow but steady feature disrupting mitochondrial homeostasis in PD, since mitochondria undergo bidirectional transport along microtubule and actin filaments. SN DA neurons displayed low levels of kinesin heavy chain (KHC) and kinase light chain (KLC1) in subjects with early-onset PD while DYNLT3 was decreased in patients with late-onset PD [48]. Parkinsonized rats exhibited decreased content in mitochondrial fusion proteins, increased levels of DRP1, and attenuated anterograde and retrograde axonal transport [49,50]. α-Syn not only localizes in the cytosol but also at or in mitochondria of DA neurons in different systems, including patients with PD. Mitochondria-targeted α-syn may cause structural damage to the organelle. Expression of α-syn compromised mitochondrial structural integrity, including massive swelling, abnormal morphology, and distorted cristae. Accumulation of α-syn led to 3-fold decrease in complex I activity in the SN of postmortem PD brains [51]. Selective reduction in complex I immunoreactivity was observed in midbrain homogenates of AAV-A53T α-syn-transduced rats [50]. Inhibition of complex I activity and altered levels of complex I-related proteins were observed following α-syn mitochondrial import, which can further increase endogenous content of α-syn, thereby initiating a feed-forward cycle.
α-Syn plays an important role in controlling mitochondrial integrity by regulating dynamics, transport, and clearance. A53T and A30P mutations in α-syn elicited mitochondrial fragmentation via a DRP1-independent pathway and increased OPA1 cleavage [52]. In a different study, α-syn-induced mitochondrial fragmentation occurred in either a Drp1-independent or -dependent mechanism [53]. The authors also showed that overexpression of MFN1 or MFN2 did not prevent fragmentation, supporting the idea that α-syn plays a selective role in fission events. α-Syn-induced mitochondrial fragmentation precedes OXPHOS disturbances, including mitochondrial respiration and ΔΨm [53]. Preformed α-syn fibrils promoted mitochondrial fission in DA neurons [54]. A53T mutant α-syn increased the amount of short round-shaped (fragmented) mitochondria, supporting a role for α-syn in regulating mitochondrial morphology probably linked to an association between the N-terminal region and the mitochondrial membrane [55]. Synthetic α-syn fibrils can cause axonal transport deficiencies, with variations in kinesin and dynein markers [54]. Overexpression of α-syn (especially A53T mutation) led to alterations in mitochondrial flux, suggesting an imbalance in mitochondrial distribution along axons. α-Syn can gradually spread to more rostral brain regions and accumulate in dystrophic axons, where is distributed and propagated in both ipsilateral and contralateral sides via axonal transport [56]. In addition, ΔΨm is required for α-syn transport and is dependent on the ATP pool. α-Syn can also promote Ca2+ trafficking from the ER to the mitochondria via mitochondria-associated ER membranes. α-Syn increases OH• concentration and protein thiol oxidation in DA neurons [51,57]. Moreover, knockdown of endogenous α-syn expression resulted in a robust reduction of protein thiol oxidation in SN DA neurons. Fibrillated α-syn augmented ROS/RNS production by increasing the MitoSox (O2•–) signal and the levels of 3-NT in DA neurons [54]. AAV-driven overexpression of human mutated A53T α-syn into the rat SN elicited systemic oxidative insult, including LPO and protein nitration in the ipsilateral hemisphere [50].
Altered Ca2+ Homeostasis and Concomitant Neurotoxicity in Parkinson’s Disease
SN DA neurons are under extreme bioenergetic demand because of three particular features: (i) the maintenance of a massive axonal tree that requires anterograde/retrograde transport of cytosolic metabolites and organelles, (ii) the maintenance and propagation of action potentials (APs) and the restoring of ionic gradients, and (iii) the large number of synaptic vesicles cycling. DA neurons display large [Ca2+]cyt oscillations that can promote mitochondrial OXPHOS activity, which may render them vulnerable to stressor-mediated damage, including genetic mutations, mitochondrial toxins, and defective aging (Figure 1). Surmeier et al. proposed that DA neurons exhibit Cav1.3 L-type Ca2+channel-dependent pacemaking activity. Reliance of pacemaking activity on these VOCCs increased in an age-dependent manner, suggesting that mature SN DA neurons might use alternative mechanisms for pacemaking activity common to other neuron types unaffected in PD [58]. A plausible mechanism involves that juvenile mechanisms remain latent in aged neurons, thereby protecting DA neurons from degeneration. Treatment with isradipine, a Cav1.3-selective L-type Ca2+ channel antagonist, can reverse the pacemaking phenotype and protect DA neurons against toxin-induced parkinsonism.
Spike-activated Ca2+ influx mediated by Cav1.3 channels may trigger Ca2+ release from the ER, which is imported into mitochondria to stimulate OXPHOS activity through two Ca2+-dependent mechanisms: (i) a MCU-dependent Ca2+ uptake mechanism that contributes to boost the Krebs cycle and mitochondrial respiration; (ii) a mechanism dependent on the malate-aspartate shuttle system that translocate electrons generated during the glycolysis across the semipermeable mitochondrial inner membrane. However, if these mechanisms are disrupted, the ability of DA neurons to sustain a spike activity is impaired. This feedforward mechanism sustains the bioenergetic demands of DA neurons, which is associated to oxidative stress and concomitant degenerative process. Epidemiological studies provided evidence of a significant correlation between low PD risk and the use of Cav1 channel inhibitors such as dihydropyridines. A Phase III clinical trial showed that chronic administration of isradipine did not slow clinical progression of early-onset PD [59]. A potential explanation for isradipine failure in clinical trials may include the extensive DA neuron degeneration in patients at the time of diagnosis or recruitment. Another reason arises from the low isradipine concentration achieved in the central nervous system (CNS) due to large drug clearance. Despite this failure, there is still a substantial interest in developing novel drugs selectively targeting Ca2+ signaling in DA neurons.
Modulation of Calcium Signaling and Homeostasis by Heterocyclic Compounds in Alzheimer’s Disease and Parkinson’s Disease
Extensive evidence has demonstrated that dysregulation of Ca2+ homeostasis and signaling are mechanisms that play an essential role in the etiopathogenesis of AD and PD. Aβ peptides are involved in the excessive accumulation of intracellular Ca2+ through the formation of Ca2+-permeable pores in the plasma membrane or by increasing Ca2+ influx via activation of L-type VOCCs and NMDA or AMPA receptors. Genetic mutations in PS or activation of inositol 1,4,5-trisphosphate (IP3) and RyRs promote Ca2+ leak in the ER, enhancing the concentration of both cytosolic and mitochondrial Ca2+. Knockdown or inhibition of IP3 kinase B led to α-syn aggregation and phosphorylation in cortical neurons treated with α-syn fibrils, which increases: (i) Ca2+ release from the ER, (ii) mitochondrial Ca2+ content, and (iii) mitochondrial respiration [60]. Moreover, mutations in the gene encoding for LRRK2 elicited transcriptional upregulation of the MCU and the mitochondrial Ca2+ uptake 1 protein (MICU1) in postmortem human PD brains, fibroblasts, and mice [61]. These findings implicate mitochondrial Ca2+ dyshomeostasis in the pathogenesis of AD and PD. Herein, we review some heterocyclic compounds with the capability of modulating Ca2+ signaling that can be considered as promising pharmacological agents for the treatment of neurodegenerative diseases (Figure 1).
Figure 1.
Heterocycles target Ca2+ dyshomeostasis leading to mitochondrial Ca2+ overlad, oxidative damage and neuronal degeneration in AD and PD.
Figure 1.
Heterocycles target Ca2+ dyshomeostasis leading to mitochondrial Ca2+ overlad, oxidative damage and neuronal degeneration in AD and PD.
1. ANAVEX2-73
ANAVEX2-73 (Blarcamesine) is a non-selective muscarinic acetylcholine receptor (mAChR) and sigma-1 receptor (S1R) ligand that exhibits an important affinity for its pharmacological targets at micromolar concentration. σ1 receptors are ubiquitously expressed in the CNS and are located at mitochondria-associated ER membranes, where they interact with IP3 receptors to regulate Ca2+ exchange between the ER and mitochondria, thereby resulting in reduced mitochondrial stress, regulation of ion channels, activation of the nuclear erythroid 2-related factor 2 (NRF2) / antioxidant response element (ARE) pathway, and limited apoptosis. IP3 receptor mediated Ca2+ release correlates with variations in the availability of mitochondrial Ca2+ and ATP synthesis. A formal concept analysis (FCA) combined with the Knowledge Extraction and Management (KEM) environment was able to identify ANAVEX2-73 as a potential genomic biomarker of disease and therapeutic response in a Phase IIa clinical trial [62]. In a double-blind, placebo-controlled Phase IIb/3 clinical study, ANAVEX2-73 improved cognition (ADAS-Cog) and function (ADCS-ADL) in patients with early AD (ANAVEX2-73-AD-004). Intraperitoneal injection of ANAVEX2-73 reversed scopolamine- and dizocilpine-induced learning impairments after intracerebroventricular injection of the neurotoxic Aβ25-35 peptide in mice [63]. Treatment with ANAVEX2-73 inhibited the phosphatidyl-inositol 3-kinase (PI3K)/Akt pathway, thereby resulting in the activation of GSK-3β, improved behavioral deficits, and reduced Aβ seeding and tau-induced pathology in Aβ25-35 injected mice [64].
ANAVEX2-73 also preserved mitochondrial integrity and function by increasing the activity of complex IV and oxygen consumption at all states [65]. Exposure to ANAVEX2-73 also mitigated the peroxidation of lipids, Bax/Bcl-2 ratio and CYT C release. Administration of ANAVEX2-73 restored mitochondrial respiration and preserved complex IV activity levels from Aβ toxicity in a Ca2+-dependent fashion [66]. ANAVEX2-73 displayed a synergic effect with donepezil (but not with memantine) and restored spontaneous alternation and passive avoidance response in a non-Tg mouse model of AD [67]. Administration of ANAVEX2-73 to Aβ42-expressing C. elegans upregulated proteostasis capacity, resulting in a dissociation and clearance of Aβ42 aggregates [68]. Also in nematodes, ANAVEX2-73 stimulated autophagic activity. In summary, ANAVEX2-73 interacts with IP3 receptors to modulate Ca2+ release and to prevent mitochondrial failure in multiple ways, including through the activation of the NRF2/ARE pathway that directly controls the expression of several antioxidant and anti-inflammatory genes. In addition, ANAVEX2-73 promotes autophagosome biogenesis and autophagic flux to degrade aggregated proteins and damaged organelles. Clinical benefits (MDS-UPDRS and CGI-I) have been reported in a 48-week Phase II extension study in patients with PDD (NCT04575259). An ongoing randomized, double-blind Phase III trial of this compound is evaluating its bioavailability and the safety, tolerability, and effectiveness of the treatment in patients with AD (NCT03790709), PD with dementia (NCT03774459) and Rett syndrome (NCT03758924).
ANAVEX2-73 (1-(2,2-diphenyltetrahydro-3-furanyl)-N,N-dimethylmethanamine hydrochloride) 1 unique synthesis was reported by Foscolos et al [69]. The key step during the production of ANAVEX2-73 is the reduction-opening of lactone 7 to provide 1,4-diol 8, which was subsequently converted by acid-catalyzed cyclodehydration to ANAVEX2-73 1 (Scheme 1).
2. Caffeine
Caffeine (Mateine), a purine alkaloid present in several plants, is the most consumed psychoactive substance in the world. Coffee is a rich source of bioactive components that contribute to its biological activity, including potassium (K+), magnesium (Mg2+), niacin and potent antioxidants. Caffeine alters Ca2+ signaling and promotes its release in a process independent of extrusion mechanisms or variations in the steady-state concentration of specific Ca2+-binding proteins. This effect was attributed to the activation of RyRs. Chronic caffeine intake promoted CSF production combined with an elevated cerebral blood flow velocity and Na+/K+-ATPase levels (which play an important role in memory and learning) [70]. Administration of caffeine upregulated protein kinase A (PKA) activity, induced cyclic adenosine monophosphate (cAMP)-response element binding protein (CREB) phosphorylation, and reduced the levels of phosphorylated c-Jun N-terminal kinase (JNK) and extracellular signal-regulated kinase (ERK), suggesting that caffeine pro-apoptotic signaling [71]. Caffeine intake resulted in memory capacity improvement and increased brain neurotrophic derived factor (BDNF) and tyrosine receptor kinase B (TrkB) levels [72]. Research studies have established a strong relationship between frequent caffeine consumption and reduced risk of developing AD and PD, with no detectable adverse effects in the CNS. A mendelian randomization study found that genetically predicted higher caffeine plasma content correlates with diminished risk of AD [73]. Following confounding adjustment, long-term coffee consumption (≥ 2 cups/day) was associated with a significant improvement in cognitive decline [74]. The CAIDE longitudinal epidemiological study established an association between mid-life moderate coffee (but no tea) consumption and late-life reduced risk of dementia and AD [75]. Long-term treatment with caffeine improved behavioral outcome and decreased the levels of Aβ, PS1 and β-secretase (BACE) in Tg APPsw mice [76]. Pathological PS induce Ca2+ accumulation and release, in part via its biochemical interaction with the IP3 receptor, thereby resulting in an anomalous regulation of Ca2+ signaling pathways and the stimulation of APP processing and Aβ synthesis, even prior the formation of plaques and NFTs [77]. Brain and plasma Aβ burden and enhanced memory performance were observed in APPsw and APP/PS1 mice following either acute or chronic caffeine administration [78]. Oral supplementation with caffeine restored motor performance, attenuated anxiety and memory deficits, prevented neuronal death in the CA1 pyramidal layer of the hippocampus, and promoted neurogenesis in both 5xFAD and Tg4-42 mouse models of AD [79]. Caffeine attenuated spatial memory abnormalities, tau phosphorylation, oxidative stress, and inflammation in THY-Tau22 mice [80].
The Honolulu Heart Program provided the first evidence showing a potential beneficial effect of caffeine intake in PD patients. Coffee drinkers (≥ 28 oz/day) had 5-fold lower incidence of developing PD following an adjustment for both age and pack-years of cigarette smoking [81]. This study was further supported by Ascherio et al. that carried out a prospective study of caffeine consumption and risk of PD was performed in men and women[82] Based on an open-label, dose-escalation study, caffeine had potential motor and non-motor benefits in subjects with PD, with the maximum tolerated dose of 100-200 mg/day bis in die (BID) without affecting sleep quality [83]. In a randomized controlled trial, administration of 200 mg caffeine BID for six weeks did not improve daytime somnolence but had the potential to reverse motor symptoms in PD patients [84]. Caffeine consumption mitigated the risk of PD, but its neuroprotective properties may vary depending on its interaction with other factors, such as obesity and low serum cholesterol levels [85]. A meta-analysis involving a large number of participants found a non-linear relationship between coffee consumption and the incidence of PD that achieved the maximum protective effect at 3 cups per day [86]. However, there was a linear dose relationship of reduced risk of PD with both tea and caffeine consumption, especially in men compared to women and in European and Asian population relative to USA residents. There was a negative correlation between caffeine intake and risk of developing PD in men but a U-shaped relationship among women. Interestingly, caffeine diminished the risk of PD in menopausal women that did not take hormone replacement, but there was a higher risk (4-fold) among hormone users with high caffeine [87]. The risk of PD was even lower when coffee intake was combined with cigarette smoking and non-steroidal anti-inflammatory drug use, resulting in a cumulative effect [88].
Administration of caffeine provided a dose-dependent therapeutic effect against rotenone-mediated neurotoxicity. Injection of caffeine through a peritoneal route improved the behavioral phenotype, normalized brain enzymatic activities of both acetylcholinesterase (AChE) and Na+/K+-ATPase, and mitigated oxidative damage and neuroinflammation in rotenone-treated rats [89]. Caffeine modulated the levels of CYT P450, glutathione-S-transferases, and vesicular monoamine transporter 2 (VMAT-2) in mice receiving 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) [90]. Pretreatment with caffeine increased neuronal glutamatergic and GABAergic metabolic activity and neurotransmission in MPTP-injected mice [91]. Exposure to caffeine also improved motor dysfunction and increased catecholamine levels in a 6-hydroxydopamine (6-OHDA) rat model of PD [92]. Striatal injection of 6-OHDA elicited apomorphine-induced rotation and impaired locomotor activity in parallel with a loss of DA immunoreactivity and an inflammatory response in rats, but administration of caffeine ameliorated the behavioral and pathological PD-like phenotype. Moreover, caffeine attenuated autophagy in mice injected with α-syn fibrils [93]. Regarding its potential mechanism of action, caffeine is an antagonist of the adenosine-2A receptor (A2AR), predominantly located in the GABAergic striatopallidal neurons projecting from the caudate nucleus and the putamen to the external segment of the globus pallidus. A2ARs colocalize with DA2 receptors to form heteromeric complexes that mediate the allosteric antagonism between adenosinergic and DAergic transmission. In summary, while it has complex biological and pharmacological profiles, evidence indicates that caffeine readily crosses the blood-brain barrier, exerts its action by antagonizing A2ARs and confers neuroprotection by stimulating mitochondrial function and by attenuating excitatory neurotransmitter release, oxidative insult, and neuroinflammation. In addition, caffeine has a well-established long-term safety profile. Together with its low cost and high availability, caffeine is a promising therapeutic agent for the treatment of neurodegenerative diseases.
The most recent synthesis of caffeine (1,3,7-trimethyl-3,7-dihydro-1H-purine-2,6-dione) 2 was reported by Narayan et al. and required seven reaction steps [94]. N-Methylation of uracil 9 in the presence of a strong base such as sodium hydride in dimethylsulfoxide (DMSO) produced 1,3-dimethyluracil 10, which was nitrated and subsequently reduced to 5-amino-1,3-dimethyluracil 12, using iron and hydrochloric acid. Nitro derivative 13 was obtained following two conventional steps and led to theophylline 14 formation after a catalytic reduction step and an intramolecular heterocyclization reaction with iron and acetic acid. The final methylation at position 7 led to the generation of caffeine 2. The overall reaction yield (amount of product generated by a chemical reaction) was 10% (Scheme 2).
New and improved methodologies for the N-methylation of theophylline 14 have been reported. A novel technique used the Q-tube system in which reactions were carried out under high pressure, overcoming the solvent boiling point. Consequently, there was a significant increase in the pressure and temperature, leading to a decreased reaction time [95]. Water was used as a green solvent and the target compounds were achieved generally in good yields. In a different study, Schnürch’s group optimized the quaternary ammonium salts as the methylating agents. Specifically, the authors developed a new protocol for monoselective methylation and ethylation of amides, indoles and related structures [96]. (Scheme 3).
3. Diltiazem
Diltiazem (Cardizem) is a non-dihydropyridine Ca2+ channel blocker with antihypertensive, antiarrhythmic and vasodilation properties. The drug selectively targets VOCCs, which are the primary mediators of Ca2+ influx into neurons in response to membrane depolarization. P/Q- and N-type VOCCs regulate neurotransmitter release upon arrival of the action potential to the axon terminal in the presynaptic neuron. Glutamate release promotes postsynaptic Ca2+ trafficking by activation of NMDAR or through an indirect pathway involving L-type VOCCs. Reduced Ca2+ transient at presynaptic or postsynaptic sites can mitigate glutamate-induced excitotoxicity. Therefore, administration of Ca2+ channel blockers has become an interesting approach for the treatment of neurodegenerative diseases. To the best of our knowledge, no clinical trials have been conducted studying the effects of diltiazem on patients with AD. Experimental evidence showed that exposure to diltiazem blocked Aβ25-35-induced AChE activity through modulation of the L-type VOCCs [97]. Diltiazem protected neurons from Aβ-mediated influx of Ca2+ ions and downstream toxicity, and facilitated Aβ clearance rate [98]. Treatment with diltiazem improved survival rate and decreased intracellular Ca2+ concentration by blocking L-type Ca2+ channels in vitro. Augmented APP secretion with no variations in the amount of cell-associated APP occurred in response to diltiazem [99]. Administration of diltiazem improved cell viability and proliferation following exogenous Aβ accumulation, which showed an early Ca2+-independent and a late Ca2+-dependent phase [60]. Chronic exposure to aluminum or any other of its forms in the drinking water has been associated with higher risk of developing AD. Aluminum accumulation has been detected in the brain of AD cases, where causes neurofibrillary degeneration in neurons. Increased content of aluminum within NFTs was observed in both the inferior temporal cortex and hippocampus of individuals with AD [100]. Aluminum chloride has been reported to cause dementia but administration of diltiazem reversed learning and memory deficits, AChE upregulation, and oxidative damage in mice [101].
The results of a single clinical trial found no association between diltiazem and the risk of developing PD (< 7% of cases) [102]. Cav1.2 and Cav1.3 are L-type VOCCs that regulate DAergic neuron spontaneous firing activity in the SN region of the brain [58]. DA neurons fire either in a low frequency single-spike pattern or transiently, in a high-frequency so-called burst mode. Cav1.2 and Cav1.3 L-type VOCCs are susceptible of degeneration during the progression of PD [103]. The extended opening of L-type VOCCs throughout autonomous pacemaking induces prolonged cytoplasmic Ca2+ trafficking and its overload in SN DA neurons, leading to mitochondrial oxidative stress [103]. L-type VOCCs-mediated alteration of the steady-state of DA levels was responsible for causing downstream oxidative stress and α-syn-induced toxicity [104]. Despite there is a lack of research investigating the potential antioxidant effect of diltiazem in AD or PD, it has been found that its intraperitoneal injection decreased the levels of nitrite and MDA and upregulated the activity of several antioxidant enzymes [105]. Another study confirmed a significant reduction in MDA content following diltiazem treatment [106]. Oral supplementation with diltiazem reduced the levels of thiobarbituric acid-reactive species (TBARS) and nitrite together with an upregulation of superoxide dismutase (SOD) and reduced glutathione enzymatic activities in an aluminum chloride mouse model of AD [101]. In summary, the L-type VOCC diltiazem is a Ca2+ antagonist that can be used to treat dementia and dementia-related diseases due to its capability of improving cognitive deficits, such as learning and memory capacity. In addition, epidemiological data obtained from individuals with PD indicate that long-term treatment with Ca2+ channel blockers targeting Ca2+ channels of DA neurons may represent a potential therapeutic strategy.
The first racemic production of diltiazem (2-(2-dimethylaminoethyl)-5-(4-methoxyphenyl)-3-oxo-6-thia-2-azabicyclo [5.4.0]undeca-7,9,11-trien-4-yl]ethanoate) 3 was described in 1990 [107]. The first asymmetric synthesis of diltiazem was reported by Naito et al. using a diastereoface differentiating nucleophilic addition as the key step to create the two contiguous stereogenic centers. Schwartz used the separation of diastereomeric glycidic esters (15 and 16) by direct crystallization, based on their marked difference in solubility [108]. Enantiomerically pure glycidic ester 15, the required isomer for the synthesis of diltiazem 3, was the major product obtained (54% yield). (Scheme 4)
In 1994, Jacobsen et al. used a manganese-catalyzed asymmetric epoxidation of cinnamate esters for the preparation of an enantiomerically pure key intermediate 18 in the synthesis of 3 [109] (Scheme 5).
Additional synthetic routes to generate diltiazem 3 from a chiral epoxide intermediate have been reported. The enantiomerically pure epoxide can be obtained through the introduction of a chiral auxiliary in the reaction, addition of metal complexes or by direct acquisition. A useful methodology employed to induce chirality in the product is the utilization of lipase or Baker’s yeast catalyzed reactions. The most recent approach used for the production of diltiazem 3 was reported by Chen et al [110]. Racemic keto ester 19 was converted into enantiomerically pure hydroxy ester 20 by ketoreductase-catalyzed dynamic reductive kinetic resolution. Two conventional steps (ring closure and ring opening) were further taken to generate an intermediate 21, which was readily subjected to intramolecular acid-catalyzed amidation. Two additional steps from intermediate benzothiazepinone 22 were required to obtain diltiazem 3. This chemoenzymatic synthesis involves eight steps to obtain diltiazem 3, with an ~45% overall reaction yield (Scheme 6).
4. Latrepirdine
Latrepirdine (Dimebon) is a carboline that blocks H1 histamine receptor (H1R) activity. A broad spectrum of effects on neurologically relevant targets was proposed. The compound is a potent reversible and competitive inhibitor of both AChE and butyrylcholinesterase, which leads to elevated acetylcholine content and concomitant boosting of cognitive performance. Besides its anti-histaminic properties, latrepirdine can modulate a wide range of other neurotransmitter receptors, such as DA, serotonin, glutamate, and NMDA. Latrepirdine can also block the activity of L-type VOCCs. Up to date, 21 clinical trials investigating the neuroprotective efficacy of latrepirdine in AD patients have been reported. A pilot clinical trial carried out in patients with mild-to-moderate AD given latrepirdine for 8 weeks showed an important reduction of neuropsychiatric symptoms and a significant cognitive function enhancement together with a lack of hematological and biochemical disturbances [111]. Data from a Phase II randomized, double-blind, placebo-controlled clinical study showed a significant improvement in cognition, function, and behavioral outcome following 60 mg/day latrepirdine for 26 and 52 weeks in individuals with mild-to-moderate AD with no adverse effects recorded [112]. A meta-analysis study revealed that latrepirdine did not ameliorate overall cognition, but the compound enhanced the neuropsychiatric inventory scale, used to assess psychopathology in dementia patients [113]. CONNECTION and CONTACT Phase III trials (NCT00838110) failed to show significant improvement in any primary or secondary outcome measures of cognition in patients treated with latrepirdine.
Exposure to latrepirdine preserved neurons against Aβ-mediated toxicity through inhibition of the L-type VOCCs current. Intraperitoneal administration of latrepirdine reversed learning and memory loss following chronic partial deprivation of cerebral cholinergic functions, which causes dementia [114]. Treatment with latrepirdine ameliorated scopolamine-induced memory impairment in young adult and aged Rhesus macaques [115]. Latrepirdine improved cognitive ability in 5xFAD mice, though it was unable to mitigate Aβ-associated pathology [116]. P301S tau mice consistently performed better on both the inverted grid and accelerating rotarod tests after latrepirdine treatment [117]. Administration of latrepirdine improved cognitive function although did not modify neither Aβ40 or Aβ42 content, suggesting APP processing as a direct target of the drug [118]. FDG-PET studies revealed an increased cerebral glucose utilization in aged mice in response to latrepirdine exposure [119]. SDH activity, ΔΨm, and ATP synthesis were normalized following latrepirdine administration with no differences in the mtDNA copy number, showing a restorative effect on mitochondrial function [120]. Latrepirdine prevented Aβ-mediated abnormalities in mitochondrial shape, mass, and respiratory chain complex activities. The compound can also preserve mitochondrial function by targeting the mPTP opening [121]. Either Ca2+ or the Aβ25-35 toxic fragment increased mitochondrial LPO but exposure to latrepirdine reduced oxidative damage to lipids [121,122]. Latrepirdine diminished the content of hyperphosphorylated tau-positive dystrophic neurons although no changes in the levels of inflammatory markers were found. Latrepirdine has a pro-autophagic activity. Indeed, treatment with latrepirdine promoted MTOR- and ATG5-dependent autophagy, which results in decreased levels of intracellular APP metabolites, including Aβ [123]. Though several clinical trials have been conducted in individuals with Huntington’s disease, there is a lack of clinical research investigating the symptomatic and functional outcome following latrepirdine monotherapy in PD. Nevertheless, evidence showed that latrepirdine elicits beneficial effects in experimental PD. Administration of latrepirdine attenuated methamphetamine-induced toxicity [60]. Increased lifespan and motor performance parallel to reduced γ-syn aggregation and inflammatory response were observed in Tg mice overexpressing γ-syn treated with latrepirdine [117]. In summary, psychiatric symptoms (such as depression) and learning and cognitive measures were restored in AD patients undergoing latrepirdine treatment, in part due to its ability to increase acetylcholine concentration by inhibition of either AChE or histamine receptors. Latrepirdine may elicit neuroprotective activity by promoting mitochondrial function and clearance of a range of intracellular inclusions through the stimulation of autophagy. The molecule may also regulate several targets involved in neurodegenerative diseases, such as neurotransmitter receptor activity, stabilization of Ca2+ signaling, and oxidative stress. Toxicological studies have shown that latrepirdine is safe and a well-tolerated drug. A dosage exceeding the therapeutic range by 100 times for 2 months did not cause any physiological changes or pathology [111].
Latrepirdine (2,3,4,5-tetrahydro-2,8-dimethyl-5-[2-(6-methyl-3-pyridinyl)ethyl]-1H-pyrido [4,3-b] indole) 4 was originally synthesized using the Fischer-indole reaction. Nevertheless, a more recent synthesis reported by Zheng et al. used p-toluidine 23 and 2-methyl-5-vinylpyridine 24 as commercial starting materials and achieved the desired product 4 in four reaction steps, with an ~16% overall reaction yield [124]. Cyclization of 2-methyl-5-(2-(1-(p-tolyl)hydrazinyl)ethyl)pyridine 26 and 1-methylpiperidin-4-one 27 was performed at reflux temperature with 80% HAc. (Scheme 7)
5. Nifedipine
Nifedipine (Procardia) is a first-generation dihydropyridine Ca2+ channel blocker used to treat hypertension and to control angina pectoris. Nifedipine is a selective antagonist of the L-type VOCCs that plays an essential role in neuronal processes triggered by membrane depolarization, thereby contributing to Ca2+-mediated events activated by signaling pathways and diverse stimuli, including neurotransmitter release, rhythmic firing, and gene expression. There is growing evidence that nifedipine may be an effective therapeutic agent for the treatment of neurodegenerative diseases, including AD and PD. Nifedipine counteracts APOE ε4-induced increase of intracellular Ca2+ levels and transcriptional activity of CREB, suggesting that L-type VOCCs are involved in neuron responses to APOE ε4 Exposure to nifedipine prevented Aβ-mediated increase of cytosolic Ca2+ concentration and synaptic pathology, indicating that Ca2+ influx via L-type VOCCs is involved in Aβ toxicity [126]. Up to date, nifedipine has not yet been tested in patients with AD. Administration of nifedipine significantly diminished the content of secreted Aβ1-42 and key components of the gamma secretase complex (e.g., PS1) [127]. Treatment with nifedipine promoted the survival rate of CNS neurons cultured from PS1-deficient mice (which showed higher susceptibility to oxidative stress) [128]. Treatment with nifedipine restored post-hypoxic related damage, leading to an improvement of neuron functional deficiencies such as population spike amplitude and depolarized resting ΔΨm in mice lacking APP [129]. Nifedipine blocked the increase in resting [Ca2+]cyt concentration in cortical neurons of 3xTg-AD or APPsw mice [130]. An age-dependent increase of L-type VOCC amplitude was described specifically in CA1 pyramidal neurons, consistent with the notion that CA1 neurons are prone to p-tau/NFT pathology due to an excessive Ca2+ trafficking. Nevertheless, Ca2+ current was limited by nifedipine [131]. The stromal interaction molecule 1 (STIM1), a type I transmembrane protein that plays a crucial role in Ca2+ influx, negatively modulates L-type VOCCs. STIM1-KO cells displayed an elevated Ca2+ entry in response to membrane depolarization, which was nifedipine-sensitive. Hippocampal neurons from 5xFAD mice exposed to nifedipine inhibit abnormal VOCC and store operated Ca2+ (SOC) entry, a process regulated by STIM1. Nifedipine inhibited mutant tau-induced intracellular Ca2+ responses to membrane depolarization [132]. Furthermore, administration of nifedipine limited tau-mediated Ca2+ influx, generation of ROS, and overall toxicity.
Data derived from a single available clinical study found no evidence of correlation between nifedipine and PD prevalence [133]. However, the results may be undermined by low statistical power (small sample size). The subthalamic nucleus (STN) has been proposed to play a central role in the disrupted function of the basal ganglia circuitry associated with PD. Distinct activity patterns, such as increased burst firings, have been observed in STN neurons. Treatment with nifedipine caused an irreversible reduction in burst frequency and abolished burst firing [134]. Based on nifedipine effects on the frequency and current curve, it was established that both short- and long-duration rebound bursting neurons contain nifedipine-sensitive Cav1.2-1.3 channels, which only contribute to rebound activity in STN neurons with long-lasting rebounds. Oscillations produced by high-frequency stimulation in the STN resulted from Ca2+ entry through the high-threshold potential nifedipine-sensitive L-type VOCCs [135]. Although nifedipine did not improve DA neuron survival, the drug had a positive impact on neurite length. Stimulation of D1 receptors or the cAMP pathway led to cytosolic accumulation of Ca2+ that interacts with nifedipine, resulting in Ca2+-mediated CREB phosphorylation and c-fos gene expression [136]. Subcutaneous injection of nifedipine attenuated apomorphine-induced rotation and partially restored striatal DA concentration in 6-OHDA-lesioned rats [137]. Nifedipine prevented nobiletin-induced DA release in MPTP-injected mice [138]. The high-threshold Ca2+ spike (HTS) and the slow oscillatory potential (SOP) are diverse Ca2+ conductances that play an important role in the generation of action potentials in SN DA neurons. While nifedipine showed a slight inhibitory effect on HTS, the molecule was able to block SOP. Moreover, nifedipine steadily abolished the spontaneous firing pattern [139]. Nifedipine increased cell survival, synaptic vesicle exocytosis, and neurite outgrowth as well as mitigated DA release and generation of ROS following rotenone exposure [140]. In summary, nifedipine is an antagonist of L-type VOCCs antagonist involved in Aβ and tau pathology, DA neurodegeneration, Ca2+ homeostasis and signaling, synaptic function, oxidative insult, and apoptotic cell death. Oral administration of nifedipine has a safety profile at doses of up to 50 mg/kg in rats over a period of thirteen weeks. In dogs, no damage was detected up to 100 mg/kg dosage for a period of four weeks. Rats tolerated daily intravenous administration of 2.5 mg/kg nifedipine over a period of three weeks while dogs tolerated up to 0.1 mg/kg nifedipine for six days. An overdose of nifedipine can induce severe hypotension, systemic vasodilation, and reflex tachycardia.
The first synthesis of nifedipine 5 (3,5-dimethyl 2,6-dimethyl-4-(2-nitrophenyl)-1,4-dihydropyridine-3,5-dicarboxylate) was reported by Singh et al., using an acid-catalyzed reaction of an enamine with two perhydro-heterocycles. Other synthetic procedures (solid phase or one-pot solvent-free synthesis) were developed. The most common synthetic procedure to obtain pyridines is using the Hantzsch reaction. The preparation of 1,4-dihydropyridines requires two equivalents of β-keto ester, an aldehyde and a nitrogen donor. Sudalai and co-workers utilized dimethylmalonate 35 as the β-keto ester, 2-nitro-benzaldehyde 36 for the aldehyde and ammonium acetate as the nitrogen donor [141]. (Scheme 9)
More recently, nifedipine 5 was synthesised through a photoinduced iron-catalysed ipso-nitration via single-electron transfer [142]. Aryl iodine 37 changed the iodine to nitro substituent to obtain 5 with good yield induced by photocatalysis (Scheme 10).
The first flow multicomponent production of nifedipine 5 was reported elsewhere [143]. Methanol solutions of compounds 36, 38 and 39 were loaded to a heated 10 mL stainless steel coil reactor (150 °C) at 0.167 mL min−1 to obtain nifedipine 5 in 71% yield. (Scheme 11)
A green methodology for nifedipine 5 production was reported [144]. A metal-free multicomponent cycloaddition of ketones with an ammonium cation under a CO2 atmosphere was used to obtain dihydropyridine derivatives. Nifedipine 5 was obtained in 32% yield by using methyl acetoacetate 38 and o-nitrobenzaldehyde 36 in the presence of ammonium chloride (NH4Cl) and CO2 in aqueous solution (Scheme 12).
6. Nimodipine
Nimodipine (Nimotop) is a Ca2+ channel blocker utilized to prevent brain damage as a consequence of reduced blood flow. The molecule antagonizes the Cav1.2-1.3 L-type VOCCs, showing a greater affinity for the Cav1.2 channel. As a highly lipophilic compound, nimodipine can easily cross the BBB and reach elevated concentrations in the CSF. The drug has specific binding affinity for dihydropyridine receptors, in contrast to nifedipine that shows predominantly peripheral effects. Nimodipine has been proposed to be of potential therapeutic utility in clinical trials of subjects with AD or PD. The beneficial effects attributable to nimodipine are related to clinical symptoms, cognitive function, and overall physical activity. A multicenter, double-blind, placebo controlled, randomized clinical trial of nimodipine demonstrated its efficacy to prevent behavioral, cognitive, and affective impairments in patients with primary degenerative dementia of the Alzheimer's type [145]. A systematic review comprising 14 randomized clinical trials found that treatment with nimodipine improved the Sandoz Clinical Assessment-Geriatric (SCAG) scale and cognitive function on AD-related dementia, mixed AD and cerebrovascular disease [146]. Long-term administration of nimodipine prevented aged-related imparired learning and memory through modulation of synaptosome Ca2+-binding proteins [147]. Nimodipine improved reversal spatial learning impairment and synaptic current deficits associated with Aβ pathology [148]. Age-related increase of the L-type Ca2+ channel protein α1D in the CA1 region of the hippocampus correlated with higher working memory defect, but nimodipine-treated rats for several months exhibited lower α1D immunoreactivity and improved spatial working memory [149]. Nimodipine ameliorated scopolamine-induced cognitive decline via its regulatory effect on BDNF and acetylcholine [150]. Nimodipine also ameliorated memory failure in aged rhesus monkeys [151]. Exposure to nimodipine reduced Ca2+ influx and associated Aβ1-42 accumulation [152]. In addition, nimodipine inhibited Aβ25-35-mediated toxic effects, including Ca2+ uptake and apoptosis. These results suggest that Aβ significantly enhances Ca2+ trafficking via nimodipine-sensitive L-type VSCCs, which leads to free radical-induced neuronal loss. Okadaic acid promoted phosphorylation of tau by increasing Ca2+ influx through L-type VOCCs, since nimodipine attenuates phospho-tau levels [153]. Tau overexpression increased sensitivity of Ca2+ transients to nimodipine [154]. Furthermore, nimodipine limited Aβ aggregation through upregulation of the glutathione S-transferase activity, which results in reduced oxidative damage.
To date, there have been no clinical trials with nimodipine in individuals with PD. Elevated Ca2+ content worsened Aβ-mediated behavioral impairment and defective chemotaxis, but exposure to nimodipine extended lifespan and rescued motor lesions, synaptic deficiencies, and DAergic degeneration [155]. Subcutaneous delivery of nimodipine reversed behavioral abnormalities and preserved the number of DAergic neurons in the locus coeruleus [156]. Exposure to nimodipine blocked DA neuron pacemaker activity, which can be restored by virtual Cav1.3 channels [157]. Moreover, nimodipine abolishes autonomous pacemaking in DA neurons and the underlying ΔΨm oscillations [58]. Nimodipine limited MPP+-induced increase in cytosolic Ca2+ content, mitochondrial depolarization and fragmentation, and neuronal death [158]. In addition, nimodipine also ameliorated MPTP-induced behavioral phenotype and limited striatal DA depletion, SN neuronal loss, and oxidative insult without regulating MAO-B activity. In MPTP-treated mice, treatment with nimodipine protected DA neurons in the SN but no changes were found in the striatum [159]. Nimodipine had no effect on behavioral impairment and striatal DA depletion but preserved DA neurons from death in marmosets injected with MPTP [160]. Nimodipine simultaneously upregulated DA release whilst suppress AChE release. Nimodipine prevented dendritic spine loss and behavioral abnormalities but not associated rotational asymmetry in DA-grafted rats [161]. Exposure to nimodipine did not impact DA graft survival but promoted graft reinnervation of striatum. Continuous-release pellets of nimodipine prevented locomotor disturbances, in unilateral 6-OHDA mesencephalic lesions [162]. Nimodipine significantly decreased the amount of NO• and LPS-activated microglia [163]. Nimodipine also downregulated DA uptake in neuron-glia cultures from mice lacking functional NADPH oxidase (involved in the production of O2•−). In summary, the L-type Ca2+ channel blocker antagonist nimodipine shows beneficial effects on AD and PD. The molecule ameliorates behavioral outcome, increases synaptic transmission and neuron survival, improves mitochondrial function, and attenuates oxidative stress and inflammation. Nimodipine is, in general, well-tolerated although sensations of warmth and skin reddening can occur. High concentrations of the nimodipine can result in reduced blood pressure, headache, nausea, muscle weakness, and gastrointestinal issues [145]. Isolated CNS symptoms, such as insomnia, tachycardia, and increased motor activity have also been reported.
A solid-phase synthesis was reported by Gordeev et al. for the preparation of nimodipine (3-(2-Methoxyethyl) 5-propan-2-yl 2,6-dimethyl-4-(3-nitrophenyl)-1,4-dihydropyridine-3,5-dicarboxylate) 6 and other bioactive dihydropyridines [164]. Condensation of the immobilized N-tethered enamino component 42 with the corresponding 2-benzylidene α-keto ester 43 provided the conjugated enamine 44. This intermediate was treated with trifluoroacetic acid to obtain the free enamino ester, which spontaneously cyclizes in solution to obtain the desired product 6. (Scheme 13)
More recently, due to a considerable demand of nimodipine in the Russian market, Pharm. Sintez Co. developed a new methodology to produce the drug in pilot batches [165]. The approach includes the production of 1-methylethyl-3-amino-crotonate 48 and 2-methoxyethyl-2-(3-nitrobenzyl-idene)acetoacetate 49. Cyclocondensation of both compounds employing iPrOH as the solvent and in the presence of hydrochloric acid, afforded the final product 6 in high yield and purity. (Scheme 14)
Conclusions and Future Directions
Multiple candidate drugs for treating AD or PD have failed over the last years. Further research is still needed to determine the therapeutic time window and the stage of the disease that should be used in clinical trials. Neuropathological and biochemical assessments support the notion that mitochondrial dysfunction causes an increase of free radicals and Ca2+-induced toxicity, which are important factors in the neurodegenerative process described in AD and PD. Based on the combination of preclinical and clinical data, there is a general consensus that development of therapeutic interventions targeting mitochondrial Ca2+ signaling may slow or stop the progression of neurodegenerative diseases, including AD and PD. A set of strategies to normalize mitochondrial Ca2+ homeostasis and signaling has been described. One potential approach involves Ca2+ uptake blockade through the L-type VOCCs, which inhibits Ca2+ transient at either presynaptic or postsynaptic sites and attenuates glutamate-mediated excitotoxicity. Selective antagonists of Cav1.2-1.3 L-type VOCCs also exhibit beneficial properties since prolonged opening of L-type channels results in augmented Ca2+ release and influx and its accumulation in DA neurons. The capability of heterocyclic agents of modulating mitochondrial Ca2+ content and signaling and the ability to preserve mitochondrial biogenesis and function provide a plausible biological basis for their neuroprotective effect (Table 1).
Author Contributions
VT: LN, and CV participated in the conceptualization of the article, wrote the initial manuscript, prepared the figures and tables, and contributed to revisions. AB, PGA, and LFP discussed the chemical synthesis, prepared the chemical equations and structural formulas, and revised the manuscript. All authors read and approved the final version of the manuscript.
Funding
This work was supported by the Excellence Program #CCVC8485 from Junta de Castilla y León, Spain, and by grant #RTI2018-099298-B-100 from Ministry of Science and Innovation, Spain, to CV and LN, and grant #VA294P18 from Junta de Castilla y León, Spain, to LN. VT is supported by the Maria Zambrano’s Excellence Program (#CL-EI-2021 IBGM) from the Ministry of Science and Innovation and the University of Valladolid, Spain, as well as by the Internationalization program of Junta de Castilla y León, Spain.
Abbreviations
Ac: acetate; DBU: 1,8-diazabicyclo [5.4.0]undec-7-ene; DMAP: 4-dimethylaminopyridine; DMF: dimethylformamide; DMSO = dimethyl sulfoxide; Dppf = 1,1'-bis(diphenylphosphino)ferrocene; GDH: glutamate dehydrogenase; NADP+: nicotinamide-adenine dinucleotide phosphate; Tf: trifluoromethanesulfonate; TFA: trifluoroacetic acid; THF: tetrahydrofuran; Tos = Ts: toluenesulfonyl.
References
- Yoboue, E.D.; Sitia, R.; Simmen, T. Redox crosstalk at endoplasmic reticulum (ER) membrane contact sites (MCS) uses toxic waste to deliver messages. Cell Death Dis 2018, 9, 331. [CrossRef]
- Rao, V.K.; Carlson, E.A.; Yan, S.S. Mitochondrial permeability transition pore is a potential drug target for neurodegeneration. Biochim Biophys Acta 2014, 1842, 1267-1272. [CrossRef]
- Kim, E.J.; Cho, S.S.; Jeong, Y.; Park, K.C.; Kang, S.J.; Kang, E.; Kim, S.E.; Lee, K.H.; Na, D.L. Glucose metabolism in early onset versus late onset Alzheimer's disease: an SPM analysis of 120 patients. Brain 2005, 128, 1790-1801. [CrossRef]
- Bosetti, F.; Brizzi, F.; Barogi, S.; Mancuso, M.; Siciliano, G.; Tendi, E.A.; Murri, L.; Rapoport, S.I.; Solaini, G. Cytochrome c oxidase and mitochondrial F1F0-ATPase (ATP synthase) activities in platelets and brain from patients with Alzheimer's disease. Neurobiol Aging 2002, 23, 371-376. [CrossRef]
- Parker, W.D., Jr.; Filley, C.M.; Parks, J.K. Cytochrome oxidase deficiency in Alzheimer's disease. Neurology 1990, 40, 1302-1303. [CrossRef]
- Hirai, K.; Aliev, G.; Nunomura, A.; Fujioka, H.; Russell, R.L.; Atwood, C.S.; Johnson, A.B.; Kress, Y.; Vinters, H.V.; Tabaton, M.; et al. Mitochondrial abnormalities in Alzheimer's disease. J Neurosci 2001, 21, 3017-3023. [CrossRef]
- Manczak, M.; Calkins, M.J.; Reddy, P.H. Impaired mitochondrial dynamics and abnormal interaction of amyloid beta with mitochondrial protein Drp1 in neurons from patients with Alzheimer's disease: implications for neuronal damage. Hum Mol Genet 2011, 20, 2495-2509. [CrossRef]
- Calkins, M.J.; Manczak, M.; Mao, P.; Shirendeb, U.; Reddy, P.H. Impaired mitochondrial biogenesis, defective axonal transport of mitochondria, abnormal mitochondrial dynamics and synaptic degeneration in a mouse model of Alzheimer's disease. Hum Mol Genet 2011, 20, 4515-4529. [CrossRef]
- Du, H.; Guo, L.; Yan, S.; Sosunov, A.A.; McKhann, G.M.; Yan, S.S. Early deficits in synaptic mitochondria in an Alzheimer's disease mouse model. Proc Natl Acad Sci U S A 2010, 107, 18670-18675. [CrossRef]
- Devi, L.; Prabhu, B.M.; Galati, D.F.; Avadhani, N.G.; Anandatheerthavarada, H.K. Accumulation of amyloid precursor protein in the mitochondrial import channels of human Alzheimer's disease brain is associated with mitochondrial dysfunction. J Neurosci 2006, 26, 9057-9068. [CrossRef]
- Hansson Petersen, C.A.; Alikhani, N.; Behbahani, H.; Wiehager, B.; Pavlov, P.F.; Alafuzoff, I.; Leinonen, V.; Ito, A.; Winblad, B.; Glaser, E.; et al. The amyloid beta-peptide is imported into mitochondria via the TOM import machinery and localized to mitochondrial cristae. Proc Natl Acad Sci U S A 2008, 105, 13145-13150. [CrossRef]
- Wang, X.; Su, B.; Siedlak, S.L.; Moreira, P.I.; Fujioka, H.; Wang, Y.; Casadesus, G.; Zhu, X. Amyloid-beta overproduction causes abnormal mitochondrial dynamics via differential modulation of mitochondrial fission/fusion proteins. Proc Natl Acad Sci U S A 2008, 105, 19318-19323. [CrossRef]
- Cho, D.H.; Nakamura, T.; Fang, J.; Cieplak, P.; Godzik, A.; Gu, Z.; Lipton, S.A. S-nitrosylation of Drp1 mediates beta-amyloid-related mitochondrial fission and neuronal injury. Science 2009, 324, 102-105. [CrossRef]
- Kim, D.I.; Lee, K.H.; Gabr, A.A.; Choi, G.E.; Kim, J.S.; Ko, S.H.; Han, H.J. Abeta-Induced Drp1 phosphorylation through Akt activation promotes excessive mitochondrial fission leading to neuronal apoptosis. Biochim Biophys Acta 2016, 1863, 2820-2834. [CrossRef]
- Li, X.C.; Hu, Y.; Wang, Z.H.; Luo, Y.; Zhang, Y.; Liu, X.P.; Feng, Q.; Wang, Q.; Ye, K.; Liu, G.P.; et al. Human wild-type full-length tau accumulation disrupts mitochondrial dynamics and the functions via increasing mitofusins. Sci Rep 2016, 6, 24756. [CrossRef]
- Tapias, V.; Jainuddin, S.; Ahuja, M.; Stack, C.; Elipenahli, C.; Vignisse, J.; Gerges, M.; Starkova, N.; Xu, H.; Starkov, A.A.; et al. Benfotiamine treatment activates the Nrf2/ARE pathway and is neuroprotective in a transgenic mouse model of tauopathy. Hum Mol Genet 2018, 27, 2874-2892. [CrossRef]
- Vossel, K.A.; Xu, J.C.; Fomenko, V.; Miyamoto, T.; Suberbielle, E.; Knox, J.A.; Ho, K.; Kim, D.H.; Yu, G.Q.; Mucke, L. Tau reduction prevents Abeta-induced axonal transport deficits by blocking activation of GSK3beta. J Cell Biol 2015, 209, 419-433. [CrossRef]
- Bobba, A.; Amadoro, G.; Valenti, D.; Corsetti, V.; Lassandro, R.; Atlante, A. Mitochondrial respiratory chain Complexes I and IV are impaired by beta-amyloid via direct interaction and through Complex I-dependent ROS production, respectively. Mitochondrion 2013, 13, 298-311. [CrossRef]
- Lovell, M.A.; Ehmann, W.D.; Butler, S.M.; Markesbery, W.R. Elevated thiobarbituric acid-reactive substances and antioxidant enzyme activity in the brain in Alzheimer's disease. Neurology 1995, 45, 1594-1601. [CrossRef]
- Markesbery, W.R.; Lovell, M.A. Four-hydroxynonenal, a product of lipid peroxidation, is increased in the brain in Alzheimer's disease. Neurobiol Aging 1998, 19, 33-36. [CrossRef]
- Youssef, P.; Chami, B.; Lim, J.; Middleton, T.; Sutherland, G.T.; Witting, P.K. Evidence supporting oxidative stress in a moderately affected area of the brain in Alzheimer's disease. Sci Rep 2018, 8, 11553. [CrossRef]
- Quinn, J.F.; Montine, K.S.; Moore, M.; Morrow, J.D.; Kaye, J.A.; Montine, T.J. Suppression of longitudinal increase in CSF F2-isoprostanes in Alzheimer's disease. J Alzheimers Dis 2004, 6, 93-97. [CrossRef]
- Sultana, R.; Poon, H.F.; Cai, J.; Pierce, W.M.; Merchant, M.; Klein, J.B.; Markesbery, W.R.; Butterfield, D.A. Identification of nitrated proteins in Alzheimer's disease brain using a redox proteomics approach. Neurobiol Dis 2006, 22, 76-87. [CrossRef]
- Reed, T.; Perluigi, M.; Sultana, R.; Pierce, W.M.; Klein, J.B.; Turner, D.M.; Coccia, R.; Markesbery, W.R.; Butterfield, D.A. Redox proteomic identification of 4-hydroxy-2-nonenal-modified brain proteins in amnestic mild cognitive impairment: insight into the role of lipid peroxidation in the progression and pathogenesis of Alzheimer's disease. Neurobiol Dis 2008, 30, 107-120. [CrossRef]
- Castegna, A.; Thongboonkerd, V.; Klein, J.B.; Lynn, B.; Markesbery, W.R.; Butterfield, D.A. Proteomic identification of nitrated proteins in Alzheimer's disease brain. J Neurochem 2003, 85, 1394-1401. [CrossRef]
- Sharma, A.; Weber, D.; Raupbach, J.; Dakal, T.C.; Fliessbach, K.; Ramirez, A.; Grune, T.; Wullner, U. Advanced glycation end products and protein carbonyl levels in plasma reveal sex-specific differences in Parkinson's and Alzheimer's disease. Redox Biol 2020, 34, 101546. [CrossRef]
- Mecocci, P.; MacGarvey, U.; Beal, M.F. Oxidative damage to mitochondrial DNA is increased in Alzheimer's disease. Ann Neurol 1994, 36, 747-751. [CrossRef]
- Valero, R.A.; Senovilla, L.; Nunez, L.; Villalobos, C. The role of mitochondrial potential in control of calcium signals involved in cell proliferation. Cell Calcium 2008, 44, 259-269. [CrossRef]
- Nunez, L.; Senovilla, L.; Sanz-Blasco, S.; Chamero, P.; Alonso, M.T.; Villalobos, C.; Garcia-Sancho, J. Bioluminescence imaging of mitochondrial Ca2+ dynamics in soma and neurites of individual adult mouse sympathetic neurons. J Physiol 2007, 580, 385-395. [CrossRef]
- Núñez, L.; Villalobos, C.; García-Sancho, J. Coupling or not coupling of mitochondria to Ca2+ sources in neurones. Soma and neurites differ. Physiol News. 2008, 70, 23-24.
- Sanz-Blasco, S.; Valero, R.A.; Rodriguez-Crespo, I.; Villalobos, C.; Nunez, L. Mitochondrial Ca2+ overload underlies Abeta oligomers neurotoxicity providing an unexpected mechanism of neuroprotection by NSAIDs. PLoS One 2008, 3, e2718. [CrossRef]
- Calvo, M.; Sanz-Blasco, S.; Caballero, E.; Villalobos, C.; Nunez, L. Susceptibility to excitotoxicity in aged hippocampal cultures and neuroprotection by non-steroidal anti-inflammatory drugs: role of mitochondrial calcium. J Neurochem 2015, 132, 403-417. [CrossRef]
- Calvo-Rodriguez, M.; Garcia-Durillo, M.; Villalobos, C.; Nunez, L. Aging Enables Ca2+ Overload and Apoptosis Induced by Amyloid-beta Oligomers in Rat Hippocampal Neurons: Neuroprotection by Non-Steroidal Anti-Inflammatory Drugs and R-Flurbiprofen in Aging Neurons. J Alzheimers Dis 2016, 54, 207-221. [CrossRef]
- Calvo-Rodriguez, M.; Garcia-Durillo, M.; Villalobos, C.; Nunez, L. In vitro aging promotes endoplasmic reticulum (ER)-mitochondria Ca(2+) cross talk and loss of store-operated Ca(2+) entry (SOCE) in rat hippocampal neurons. Biochim Biophys Acta 2016, 1863, 2637-2649. [CrossRef]
- Calvo-Rodriguez, M.; Hernando-Perez, E.; Nunez, L.; Villalobos, C. Amyloid beta Oligomers Increase ER-Mitochondria Ca(2+) Cross Talk in Young Hippocampal Neurons and Exacerbate Aging-Induced Intracellular Ca(2+) Remodeling. Front Cell Neurosci 2019, 13, 22. [CrossRef]
- Caballero, E.; Hernando-Perez, E.; Tapias, V.; Calvo-Rodriguez, M.; Villalobos, C.; Nunez, L. Amyloid Beta Oligomers-Induced Ca(2+) Entry Pathways: Role of Neuronal Networks, NMDA Receptors and Amyloid Channel Formation. Biomedicines 2022, 10. [CrossRef]
- Gonzalez-Andres, P.; Fernandez-Pena, L.; Diez-Poza, C.; Villalobos, C.; Nunez, L.; Barbero, A. Marine Heterocyclic Compounds That Modulate Intracellular Calcium Signals: Chemistry and Synthesis Approaches. Mar Drugs 2021, 19. [CrossRef]
- Edison, P.; Ahmed, I.; Fan, Z.; Hinz, R.; Gelosa, G.; Ray Chaudhuri, K.; Walker, Z.; Turkheimer, F.E.; Brooks, D.J. Microglia, amyloid, and glucose metabolism in Parkinson's disease with and without dementia. Neuropsychopharmacology 2013, 38, 938-949. [CrossRef]
- Trimmer, P.A.; Swerdlow, R.H.; Parks, J.K.; Keeney, P.; Bennett, J.P., Jr.; Miller, S.W.; Davis, R.E.; Parker, W.D., Jr. Abnormal mitochondrial morphology in sporadic Parkinson's and Alzheimer's disease cybrid cell lines. Exp Neurol 2000, 162, 37-50. [CrossRef]
- Jimenez-Jimenez, F.J.; Molina, J.A.; Hernanz, A.; Fernandez-Vivancos, E.; de Bustos, F.; Barcenilla, B.; Gomez-Escalonilla, C.; Zurdo, M.; Berbel, A.; Villanueva, C. Cerebrospinal fluid levels of thiamine in patients with Parkinson's disease. Neurosci Lett 1999, 271, 33-36. [CrossRef]
- Gibson, G.E.; Kingsbury, A.E.; Xu, H.; Lindsay, J.G.; Daniel, S.; Foster, O.J.; Lees, A.J.; Blass, J.P. Deficits in a tricarboxylic acid cycle enzyme in brains from patients with Parkinson's disease. Neurochem Int 2003, 43, 129-135. [CrossRef]
- Mizuno, Y.; Matuda, S.; Yoshino, H.; Mori, H.; Hattori, N.; Ikebe, S. An immunohistochemical study on alpha-ketoglutarate dehydrogenase complex in Parkinson's disease. Ann Neurol 1994, 35, 204-210. [CrossRef]
- Mallajosyula, J.K.; Chinta, S.J.; Rajagopalan, S.; Nicholls, D.G.; Andersen, J.K. Metabolic control analysis in a cellular model of elevated MAO-B: relevance to Parkinson's disease. Neurotox Res 2009, 16, 186-193. [CrossRef]
- Schapira, A.H.; Cooper, J.M.; Dexter, D.; Clark, J.B.; Jenner, P.; Marsden, C.D. Mitochondrial complex I deficiency in Parkinson's disease. J Neurochem 1990, 54, 823-827. [CrossRef]
- Mann, V.M.; Cooper, J.M.; Daniel, S.E.; Srai, K.; Jenner, P.; Marsden, C.D.; Schapira, A.H. Complex I, iron, and ferritin in Parkinson's disease substantia nigra. Ann Neurol 1994, 36, 876-881. [CrossRef]
- Zilocchi, M.; Finzi, G.; Lualdi, M.; Sessa, F.; Fasano, M.; Alberio, T. Mitochondrial alterations in Parkinson's disease human samples and cellular models. Neurochem Int 2018, 118, 61-72. [CrossRef]
- Lynch, D.S.; Loh, S.H.Y.; Harley, J.; Noyce, A.J.; Martins, L.M.; Wood, N.W.; Houlden, H.; Plun-Favreau, H. Nonsyndromic Parkinson disease in a family with autosomal dominant optic atrophy due to OPA1 mutations. Neurol Genet 2017, 3, e188. [CrossRef]
- Chu, Y.; Morfini, G.A.; Langhamer, L.B.; He, Y.; Brady, S.T.; Kordower, J.H. Alterations in axonal transport motor proteins in sporadic and experimental Parkinson's disease. Brain 2012, 135, 2058-2073. [CrossRef]
- Tapias, V.; McCoy, J.L.; Greenamyre, J.T. Phenothiazine normalizes the NADH/NAD(+) ratio, maintains mitochondrial integrity and protects the nigrostriatal dopamine system in a chronic rotenone model of Parkinson's disease. Redox Biol 2019, 24, 101164. [CrossRef]
- Beal, M.F.; Chiluwal, J.; Calingasan, N.Y.; Milne, G.L.; Shchepinov, M.S.; Tapias, V. Isotope-reinforced polyunsaturated fatty acids improve Parkinson's disease-like phenotype in rats overexpressing alpha-synuclein. Acta Neuropathol Commun 2020, 8, 220. [CrossRef]
- Devi, L.; Raghavendran, V.; Prabhu, B.M.; Avadhani, N.G.; Anandatheerthavarada, H.K. Mitochondrial import and accumulation of alpha-synuclein impair complex I in human dopaminergic neuronal cultures and Parkinson disease brain. J Biol Chem 2008, 283, 9089-9100. [CrossRef]
- Guardia-Laguarta, C.; Area-Gomez, E.; Rub, C.; Liu, Y.; Magrane, J.; Becker, D.; Voos, W.; Schon, E.A.; Przedborski, S. alpha-Synuclein is localized to mitochondria-associated ER membranes. J Neurosci 2014, 34, 249-259. [CrossRef]
- Nakamura, K.; Nemani, V.M.; Azarbal, F.; Skibinski, G.; Levy, J.M.; Egami, K.; Munishkina, L.; Zhang, J.; Gardner, B.; Wakabayashi, J.; et al. Direct membrane association drives mitochondrial fission by the Parkinson disease-associated protein alpha-synuclein. J Biol Chem 2011, 286, 20710-20726. [CrossRef]
- Tapias, V.; Hu, X.; Luk, K.C.; Sanders, L.H.; Lee, V.M.; Greenamyre, J.T. Synthetic alpha-synuclein fibrils cause mitochondrial impairment and selective dopamine neurodegeneration in part via iNOS-mediated nitric oxide production. Cell Mol Life Sci 2017, 74, 2851-2874. [CrossRef]
- Pozo Devoto, V.M.; Dimopoulos, N.; Alloatti, M.; Pardi, M.B.; Saez, T.M.; Otero, M.G.; Cromberg, L.E.; Marin-Burgin, A.; Scassa, M.E.; Stokin, G.B.; et al. alphaSynuclein control of mitochondrial homeostasis in human-derived neurons is disrupted by mutations associated with Parkinson's disease. Sci Rep 2017, 7, 5042. [CrossRef]
- Ulusoy, A.; Rusconi, R.; Perez-Revuelta, B.I.; Musgrove, R.E.; Helwig, M.; Winzen-Reichert, B.; Di Monte, D.A. Caudo-rostral brain spreading of alpha-synuclein through vagal connections. EMBO Mol Med 2013, 5, 1119-1127. [CrossRef]
- Di Maio, R.; Barrett, P.J.; Hoffman, E.K.; Barrett, C.W.; Zharikov, A.; Borah, A.; Hu, X.; McCoy, J.; Chu, C.T.; Burton, E.A.; et al. alpha-Synuclein binds to TOM20 and inhibits mitochondrial protein import in Parkinson's disease. Sci Transl Med 2016, 8, 342ra378. [CrossRef]
- Chan, C.S.; Guzman, J.N.; Ilijic, E.; Mercer, J.N.; Rick, C.; Tkatch, T.; Meredith, G.E.; Surmeier, D.J. 'Rejuvenation' protects neurons in mouse models of Parkinson's disease. Nature 2007, 447, 1081-1086. [CrossRef]
- Parkinson Study Group, S.-P.D.I.I.I.I. Isradipine Versus Placebo in Early Parkinson Disease: A Randomized Trial. Ann Intern Med 2020, 172, 591-598. [CrossRef]
- Abe, K.; Kimura, H. Amyloid beta toxicity consists of a Ca(2+)-independent early phase and a Ca(2+)-dependent late phase. J Neurochem 1996, 67, 2074-2078.
- Verma, M.; Callio, J.; Otero, P.A.; Sekler, I.; Wills, Z.P.; Chu, C.T. Mitochondrial Calcium Dysregulation Contributes to Dendrite Degeneration Mediated by PD/LBD-Associated LRRK2 Mutants. J Neurosci 2017, 37, 11151-11165. [CrossRef]
- Hampel, H.; Williams, C.; Etcheto, A.; Goodsaid, F.; Parmentier, F.; Sallantin, J.; Kaufmann, W.E.; Missling, C.U.; Afshar, M. A precision medicine framework using artificial intelligence for the identification and confirmation of genomic biomarkers of response to an Alzheimer's disease therapy: Analysis of the blarcamesine (ANAVEX2-73) Phase 2a clinical study. Alzheimers Dement (N Y) 2020, 6, e12013. [CrossRef]
- Villard, V.; Espallergues, J.; Keller, E.; Vamvakides, A.; Maurice, T. Anti-amnesic and neuroprotective potentials of the mixed muscarinic receptor/sigma 1 (sigma1) ligand ANAVEX2-73, a novel aminotetrahydrofuran derivative. J Psychopharmacol 2011, 25, 1101-1117. [CrossRef]
- Lahmy, V.; Meunier, J.; Malmstrom, S.; Naert, G.; Givalois, L.; Kim, S.H.; Villard, V.; Vamvakides, A.; Maurice, T. Blockade of Tau hyperphosphorylation and Abeta(1)(-)(4)(2) generation by the aminotetrahydrofuran derivative ANAVEX2-73, a mixed muscarinic and sigma(1) receptor agonist, in a nontransgenic mouse model of Alzheimer's disease. Neuropsychopharmacology 2013, 38, 1706-1723. [CrossRef]
- Lahmy, V.; Long, R.; Morin, D.; Villard, V.; Maurice, T. Mitochondrial protection by the mixed muscarinic/sigma1 ligand ANAVEX2-73, a tetrahydrofuran derivative, in Abeta25-35 peptide-injected mice, a nontransgenic Alzheimer's disease model. Front Cell Neurosci 2015, 8, 463. [CrossRef]
- Goguadze, N.; Zhuravliova, E.; Morin, D.; Mikeladze, D.; Maurice, T. Sigma-1 Receptor Agonists Induce Oxidative Stress in Mitochondria and Enhance Complex I Activity in Physiological Condition but Protect Against Pathological Oxidative Stress. Neurotox Res 2019, 35, 1-18. [CrossRef]
- Maurice, T. Protection by sigma-1 receptor agonists is synergic with donepezil, but not with memantine, in a mouse model of amyloid-induced memory impairments. Behav Brain Res 2016, 296, 270-278. [CrossRef]
- Christ, M.G.; Huesmann, H.; Nagel, H.; Kern, A.; Behl, C. Sigma-1 Receptor Activation Induces Autophagy and Increases Proteostasis Capacity In Vitro and In Vivo. Cells 2019, 8. [CrossRef]
- Foscolos, G.B.; Kolocouris, N.; Fytas, G.; Marakos, P.; Pouli, N.; Vamvakides, A. Synthesis and pharmacological study of some new beta-(dialkylaminomethyl)- gamma-butyrolactones and their tetrahydrofuran analogues. Farmaco 1996, 51, 19-26. [CrossRef]
- Han, M.E.; Kim, H.J.; Lee, Y.S.; Kim, D.H.; Choi, J.T.; Pan, C.S.; Yoon, S.; Baek, S.Y.; Kim, B.S.; Kim, J.B.; et al. Regulation of cerebrospinal fluid production by caffeine consumption. BMC Neurosci 2009, 10, 110. [CrossRef]
- Zeitlin, R.; Patel, S.; Burgess, S.; Arendash, G.W.; Echeverria, V. Caffeine induces beneficial changes in PKA signaling and JNK and ERK activities in the striatum and cortex of Alzheimer's transgenic mice. Brain Res 2011, 1417, 127-136. [CrossRef]
- Han, K.; Jia, N.; Li, J.; Yang, L.; Min, L.Q. Chronic caffeine treatment reverses memory impairment and the expression of brain BNDF and TrkB in the PS1/APP double transgenic mouse model of Alzheimer's disease. Mol Med Rep 2013, 8, 737-740. [CrossRef]
- Larsson, S.C.; Woolf, B.; Gill, D. Plasma Caffeine Levels and Risk of Alzheimer's Disease and Parkinson's Disease: Mendelian Randomization Study. Nutrients 2022, 14. [CrossRef]
- Kim, J.W.; Byun, M.S.; Yi, D.; Lee, J.H.; Jeon, S.Y.; Jung, G.; Lee, H.N.; Sohn, B.K.; Lee, J.Y.; Kim, Y.K.; et al. Coffee intake and decreased amyloid pathology in human brain. Transl Psychiatry 2019, 9, 270. [CrossRef]
- Eskelinen, M.H.; Kivipelto, M. Caffeine as a protective factor in dementia and Alzheimer's disease. J Alzheimers Dis 2010, 20 Suppl 1, S167-174. [CrossRef]
- Arendash, G.W.; Schleif, W.; Rezai-Zadeh, K.; Jackson, E.K.; Zacharia, L.C.; Cracchiolo, J.R.; Shippy, D.; Tan, J. Caffeine protects Alzheimer's mice against cognitive impairment and reduces brain beta-amyloid production. Neuroscience 2006, 142, 941-952. [CrossRef]
- Cheung, K.H.; Shineman, D.; Muller, M.; Cardenas, C.; Mei, L.; Yang, J.; Tomita, T.; Iwatsubo, T.; Lee, V.M.; Foskett, J.K. Mechanism of Ca2+ disruption in Alzheimer's disease by presenilin regulation of InsP3 receptor channel gating. Neuron 2008, 58, 871-883. [CrossRef]
- Cao, C.; Cirrito, J.R.; Lin, X.; Wang, L.; Verges, D.K.; Dickson, A.; Mamcarz, M.; Zhang, C.; Mori, T.; Arendash, G.W.; et al. Caffeine suppresses amyloid-beta levels in plasma and brain of Alzheimer's disease transgenic mice. J Alzheimers Dis 2009, 17, 681-697. [CrossRef]
- Stazi, M.; Lehmann, S.; Sakib, M.S.; Pena-Centeno, T.; Buschgens, L.; Fischer, A.; Weggen, S.; Wirths, O. Long-term caffeine treatment of Alzheimer mouse models ameliorates behavioural deficits and neuron loss and promotes cellular and molecular markers of neurogenesis. Cell Mol Life Sci 2021, 79, 55. [CrossRef]
- Laurent, C.; Eddarkaoui, S.; Derisbourg, M.; Leboucher, A.; Demeyer, D.; Carrier, S.; Schneider, M.; Hamdane, M.; Muller, C.E.; Buee, L.; et al. Beneficial effects of caffeine in a transgenic model of Alzheimer's disease-like tau pathology. Neurobiol Aging 2014, 35, 2079-2090. [CrossRef]
- Ross, G.W.; Abbott, R.D.; Petrovitch, H.; Morens, D.M.; Grandinetti, A.; Tung, K.H.; Tanner, C.M.; Masaki, K.H.; Blanchette, P.L.; Curb, J.D.; et al. Association of coffee and caffeine intake with the risk of Parkinson disease. JAMA 2000, 283, 2674-2679. [CrossRef]
- Ascherio, A.; Zhang, S.M.; Hernan, M.A.; Kawachi, I.; Colditz, G.A.; Speizer, F.E.; Willett, W.C. Prospective study of caffeine consumption and risk of Parkinson's disease in men and women. Ann Neurol 2001, 50, 56-63. [CrossRef]
- Altman, R.D.; Lang, A.E.; Postuma, R.B. Caffeine in Parkinson's disease: a pilot open-label, dose-escalation study. Mov Disord 2011, 26, 2427-2431. [CrossRef]
- Postuma, R.B.; Lang, A.E.; Munhoz, R.P.; Charland, K.; Pelletier, A.; Moscovich, M.; Filla, L.; Zanatta, D.; Rios Romenets, S.; Altman, R.; et al. Caffeine for treatment of Parkinson disease: a randomized controlled trial. Neurology 2012, 79, 651-658. [CrossRef]
- Saaksjarvi, K.; Knekt, P.; Rissanen, H.; Laaksonen, M.A.; Reunanen, A.; Mannisto, S. Prospective study of coffee consumption and risk of Parkinson's disease. Eur J Clin Nutr 2008, 62, 908-915. [CrossRef]
- Qi, H.; Li, S. Dose-response meta-analysis on coffee, tea and caffeine consumption with risk of Parkinson's disease. Geriatr Gerontol Int 2014, 14, 430-439. [CrossRef]
- Ascherio, A.; Chen, H.; Schwarzschild, M.A.; Zhang, S.M.; Colditz, G.A.; Speizer, F.E. Caffeine, postmenopausal estrogen, and risk of Parkinson's disease. Neurology 2003, 60, 790-795. [CrossRef]
- Powers, K.M.; Kay, D.M.; Factor, S.A.; Zabetian, C.P.; Higgins, D.S.; Samii, A.; Nutt, J.G.; Griffith, A.; Leis, B.; Roberts, J.W.; et al. Combined effects of smoking, coffee, and NSAIDs on Parkinson's disease risk. Mov Disord 2008, 23, 88-95. [CrossRef]
- Khadrawy, Y.A.; Salem, A.M.; El-Shamy, K.A.; Ahmed, E.K.; Fadl, N.N.; Hosny, E.N. Neuroprotective and Therapeutic Effect of Caffeine on the Rat Model of Parkinson's Disease Induced by Rotenone. J Diet Suppl 2017, 14, 553-572. [CrossRef]
- Singh, S.; Singh, K.; Patel, S.; Patel, D.K.; Singh, C.; Nath, C.; Singh, M.P. Nicotine and caffeine-mediated modulation in the expression of toxicant responsive genes and vesicular monoamine transporter-2 in 1-methyl 4-phenyl-1,2,3,6-tetrahydropyridine-induced Parkinson's disease phenotype in mouse. Brain Res 2008, 1207, 193-206. [CrossRef]
- Bagga, P.; Chugani, A.N.; Patel, A.B. Neuroprotective effects of caffeine in MPTP model of Parkinson's disease: A (13)C NMR study. Neurochem Int 2016, 92, 25-34. [CrossRef]
- Aguiar, L.M.; Nobre, H.V., Jr.; Macedo, D.S.; Oliveira, A.A.; Freitas, R.M.; Vasconcelos, S.M.; Cunha, G.M.; Sousa, F.C.; Viana, G.S. Neuroprotective effects of caffeine in the model of 6-hydroxydopamine lesion in rats. Pharmacol Biochem Behav 2006, 84, 415-419. [CrossRef]
- Luan, Y.; Ren, X.; Zheng, W.; Zeng, Z.; Guo, Y.; Hou, Z.; Guo, W.; Chen, X.; Li, F.; Chen, J.F. Chronic Caffeine Treatment Protects Against alpha-Synucleinopathy by Reestablishing Autophagy Activity in the Mouse Striatum. Front Neurosci 2018, 12, 301. [CrossRef]
- Zajac, M.A.; Zakrzewski, A.G.; Kowal, M.G.; Narayan, S. A Novel Method of Caffeine Synthesis from Uracil. Synth. Commun. 2003, 33, 3291-3297. [CrossRef]
- Scimmi, C.; Cardinali, M.; Abenante, L.; Amatista, M.; Nacca, F.G.; Lenardao, E.J.; Sancineto, L.; Santi, C. Q-Tube®-Assisted Alkylation and Arylation of Xanthines and Other N-H-Containing Heterocycles in Water. Chemistry 2021, 3, 1126-1137. [CrossRef]
- Templ, J.; Gjata, E.; Getzner, F.; Schnürch, M. Monoselective N-Methylation of Amides, Indoles, and Related Structures Using Quaternary Ammonium Salts as Solid Methylating Agents. Org. Lett. 2022, 24, 7315-7319. [CrossRef]
- Sberna, G.; Saez-Valero, J.; Beyreuther, K.; Masters, C.L.; Small, D.H. The amyloid beta-protein of Alzheimer's disease increases acetylcholinesterase expression by increasing intracellular calcium in embryonal carcinoma P19 cells. J Neurochem 1997, 69, 1177-1184. [CrossRef]
- Paris, D.; Bachmeier, C.; Patel, N.; Quadros, A.; Volmar, C.H.; Laporte, V.; Ganey, J.; Beaulieu-Abdelahad, D.; Ait-Ghezala, G.; Crawford, F.; et al. Selective antihypertensive dihydropyridines lower Abeta accumulation by targeting both the production and the clearance of Abeta across the blood-brain barrier. Mol Med 2011, 17, 149-162. [CrossRef]
- Mok, S.S.; Clippingdale, A.B.; Beyreuther, K.; Masters, C.L.; Barrow, C.J.; Small, D.H. A beta peptides and calcium influence secretion of the amyloid protein precursor from chick sympathetic neurons in culture. J Neurosci Res 2000, 61, 449-457. [CrossRef]
- Bouras, C.; Giannakopoulos, P.; Good, P.F.; Hsu, A.; Hof, P.R.; Perl, D.P. A laser microprobe mass analysis of brain aluminum and iron in dementia pugilistica: comparison with Alzheimer's disease. Eur Neurol 1997, 38, 53-58. [CrossRef]
- Rani, A.; Neha; Sodhi, R.K.; Kaur, A. Protective effect of a calcium channel blocker "diltiazem" on aluminum chloride-induced dementia in mice. Naunyn Schmiedebergs Arch Pharmacol 2015, 388, 1151-1161. [CrossRef]
- Ritz, B.; Rhodes, S.L.; Qian, L.; Schernhammer, E.; Olsen, J.H.; Friis, S. L-type calcium channel blockers and Parkinson disease in Denmark. Ann Neurol 2010, 67, 600-606. [CrossRef]
- Guzman, J.N.; Sanchez-Padilla, J.; Chan, C.S.; Surmeier, D.J. Robust pacemaking in substantia nigra dopaminergic neurons. J Neurosci 2009, 29, 11011-11019. [CrossRef]
- Mosharov, E.V.; Larsen, K.E.; Kanter, E.; Phillips, K.A.; Wilson, K.; Schmitz, Y.; Krantz, D.E.; Kobayashi, K.; Edwards, R.H.; Sulzer, D. Interplay between cytosolic dopamine, calcium, and alpha-synuclein causes selective death of substantia nigra neurons. Neuron 2009, 62, 218-229. [CrossRef]
- Anjaneyulu, M.; Chopra, K. Diltiazem attenuates oxidative stress in diabetic rats. Ren Fail 2005, 27, 335-344.
- Koller, P.T.; Bergmann, S.R. Reduction of lipid peroxidation in reperfused isolated rabbit hearts by diltiazem. Circ Res 1989, 65, 838-846. [CrossRef]
- Gizur, T.; Harsànyi, K. Some Applications of Isopropenyl Acetate To O-, N-and C-Acetylation. Synthetic Communications 1990, 20, 2365-2371. [CrossRef]
- Schwartz, A.; Madan, P.B.; Mohacsi, E.; O'Brien, J.P.; Todaro, L.J.; Coffen, D.L. Enantioselective synthesis of calcium channel blockers of the diltiazem group. The Journal of Organic Chemistry 1992, 57, 851-856. [CrossRef]
- Jacobsen, E.N.; Deng, L.; Furukawa, Y.; Martínez, L.E. Enantioselective catalytic epoxidation of cinnamate esters. Tetrahedron 1994, 50, 4323-4334. [CrossRef]
- Yue, X.; Li, Y.; Liu, M.; Sang, D.; Huang, Z.; Chen, F. Biocatalytic dynamic reductive kinetic resolution of aryl α-chloro β-keto esters: divergent, stereocontrolled synthesis of diltiazem, clentiazem, and siratiazem. Chemical Communications 2022, 58, 9010-9013. [CrossRef]
- Bachurin, S.; Bukatina, E.; Lermontova, N.; Tkachenko, S.; Afanasiev, A.; Grigoriev, V.; Grigorieva, I.; Ivanov, Y.; Sablin, S.; Zefirov, N. Antihistamine agent Dimebon as a novel neuroprotector and a cognition enhancer. Ann N Y Acad Sci 2001, 939, 425-435. [CrossRef]
- Doody, R.S.; Gavrilova, S.I.; Sano, M.; Thomas, R.G.; Aisen, P.S.; Bachurin, S.O.; Seely, L.; Hung, D.; dimebon, i. Effect of dimebon on cognition, activities of daily living, behaviour, and global function in patients with mild-to-moderate Alzheimer's disease: a randomised, double-blind, placebo-controlled study. Lancet 2008, 372, 207-215. [CrossRef]
- Cano-Cuenca, N.; Solis-Garcia del Pozo, J.E.; Jordan, J. Evidence for the efficacy of latrepirdine (Dimebon) treatment for improvement of cognitive function: a meta-analysis. J Alzheimers Dis 2014, 38, 155-164. [CrossRef]
- Lermontova, N.N.; Lukoyanov, N.V.; Serkova, T.P.; Lukoyanova, E.A.; Bachurin, S.O. Dimebon improves learning in animals with experimental Alzheimer's disease. Bull Exp Biol Med 2000, 129, 544-546. [CrossRef]
- Webster, S.J.; Wilson, C.A.; Lee, C.H.; Mohler, E.G.; Terry, A.V., Jr.; Buccafusco, J.J. The acute effects of dimebolin, a potential Alzheimer's disease treatment, on working memory in rhesus monkeys. Br J Pharmacol 2011, 164, 970-978. [CrossRef]
- Peters, O.M.; Shelkovnikova, T.; Tarasova, T.; Springe, S.; Kukharsky, M.S.; Smith, G.A.; Brooks, S.; Kozin, S.A.; Kotelevtsev, Y.; Bachurin, S.O.; et al. Chronic administration of Dimebon does not ameliorate amyloid-beta pathology in 5xFAD transgenic mice. J Alzheimers Dis 2013, 36, 589-596. [CrossRef]
- Bachurin, S.O.; Shelkovnikova, T.A.; Ustyugov, A.A.; Peters, O.; Khritankova, I.; Afanasieva, M.A.; Tarasova, T.V.; Alentov, II; Buchman, V.L.; Ninkina, N.N. Dimebon slows progression of proteinopathy in gamma-synuclein transgenic mice. Neurotox Res 2012, 22, 33-42. [CrossRef]
- Wang, J.; Ferruzzi, M.G.; Varghese, M.; Qian, X.; Cheng, A.; Xie, M.; Zhao, W.; Ho, L.; Pasinetti, G.M. Preclinical study of dimebon on beta-amyloid-mediated neuropathology in Alzheimer's disease. Mol Neurodegener 2011, 6, 7. [CrossRef]
- Day, M.; Chandran, P.; Luo, F.; Rustay, N.R.; Markosyan, S.; LeBlond, D.; Fox, G.B. Latrepirdine increases cerebral glucose utilization in aged mice as measured by [18F]-fluorodeoxyglucose positron emission tomography. Neuroscience 2011, 189, 299-304. [CrossRef]
- Zhang, S.; Hedskog, L.; Petersen, C.A.; Winblad, B.; Ankarcrona, M. Dimebon (latrepirdine) enhances mitochondrial function and protects neuronal cells from death. J Alzheimers Dis 2010, 21, 389-402. [CrossRef]
- Bachurin, S.O.; Shevtsova, E.P.; Kireeva, E.G.; Oxenkrug, G.F.; Sablin, S.O. Mitochondria as a target for neurotoxins and neuroprotective agents. Ann N Y Acad Sci 2003, 993, 334-344; discussion 345-339. [CrossRef]
- Shevtzova, E.F.; Kireeva, E.G.; Bachurin, S.O. Effect of beta-amyloid peptide fragment 25-35 on nonselective permeability of mitochondria. Bull Exp Biol Med 2001, 132, 1173-1176. [CrossRef]
- Steele, J.W.; Gandy, S. Latrepirdine (Dimebon(R)), a potential Alzheimer therapeutic, regulates autophagy and neuropathology in an Alzheimer mouse model. Autophagy 2013, 9, 617-618. [CrossRef]
- Gao, M.; Wang, M.; Hutchins, G.D.; Zheng, Q.-H. [11C]Dimebon, radiosynthesis and lipophilicity of a new potential PET agent for imaging of Alzheimer’s disease and Huntington’s disease. Bioorganic Med. Chem. Lett. 2010, 20, 2529-2532. [CrossRef]
- Dong, H.; Latka, R.T.; Driver, T.G. Ruthenium-Catalyzed γ-Carbolinium Ion Formation from Aryl Azides; Synthesis of Dimebolin. Org. Lett. 2011, 13, 2726-2729. [CrossRef]
- Liu, S.J.; Gasperini, R.; Foa, L.; Small, D.H. Amyloid-beta decreases cell-surface AMPA receptors by increasing intracellular calcium and phosphorylation of GluR2. J Alzheimers Dis 2010, 21, 655-666. [CrossRef]
- Lovell, M.A.; Abner, E.; Kryscio, R.; Xu, L.; Fister, S.X.; Lynn, B.C. Calcium Channel Blockers, Progression to Dementia, and Effects on Amyloid Beta Peptide Production. Oxid Med Cell Longev 2015, 2015, 787805. [CrossRef]
- Nakajima, M.; Miura, M.; Aosaki, T.; Shirasawa, T. Deficiency of presenilin-1 increases calcium-dependent vulnerability of neurons to oxidative stress in vitro. J Neurochem 2001, 78, 807-814. [CrossRef]
- Hefter, D.; Kaiser, M.; Weyer, S.W.; Papageorgiou, I.E.; Both, M.; Kann, O.; Muller, U.C.; Draguhn, A. Amyloid Precursor Protein Protects Neuronal Network Function after Hypoxia via Control of Voltage-Gated Calcium Channels. J Neurosci 2016, 36, 8356-8371. [CrossRef]
- Lopez, J.R.; Lyckman, A.; Oddo, S.; Laferla, F.M.; Querfurth, H.W.; Shtifman, A. Increased intraneuronal resting [Ca2+] in adult Alzheimer's disease mice. J Neurochem 2008, 105, 262-271. [CrossRef]
- Wang, Y.; Mattson, M.P. L-type Ca2+ currents at CA1 synapses, but not CA3 or dentate granule neuron synapses, are increased in 3xTgAD mice in an age-dependent manner. Neurobiol Aging 2014, 35, 88-95. [CrossRef]
- Furukawa, K.; Wang, Y.; Yao, P.J.; Fu, W.; Mattson, M.P.; Itoyama, Y.; Onodera, H.; D'Souza, I.; Poorkaj, P.H.; Bird, T.D.; et al. Alteration in calcium channel properties is responsible for the neurotoxic action of a familial frontotemporal dementia tau mutation. J Neurochem 2003, 87, 427-436. [CrossRef]
- Pasternak, B.; Svanstrom, H.; Nielsen, N.M.; Fugger, L.; Melbye, M.; Hviid, A. Use of calcium channel blockers and Parkinson's disease. Am J Epidemiol 2012, 175, 627-635. [CrossRef]
- Beurrier, C.; Congar, P.; Bioulac, B.; Hammond, C. Subthalamic nucleus neurons switch from single-spike activity to burst-firing mode. J Neurosci 1999, 19, 599-609. [CrossRef]
- Garcia, L.; Audin, J.; D'Alessandro, G.; Bioulac, B.; Hammond, C. Dual effect of high-frequency stimulation on subthalamic neuron activity. J Neurosci 2003, 23, 8743-8751. [CrossRef]
- Eaton, M.E.; Macias, W.; Youngs, R.M.; Rajadhyaksha, A.; Dudman, J.T.; Konradi, C. L-type Ca2+ channel blockers promote Ca2+ accumulation when dopamine receptors are activated in striatal neurons. Brain Res Mol Brain Res 2004, 131, 65-72. [CrossRef]
- Wang, R.; Ma, Z.; Wang, J.; Xie, J. L-type Cav1.2 calcium channel is involved in 6-hydroxydopamine-induced neurotoxicity in rats. Neurotox Res 2012, 21, 266-270. [CrossRef]
- Yabuki, Y.; Ohizumi, Y.; Yokosuka, A.; Mimaki, Y.; Fukunaga, K. Nobiletin treatment improves motor and cognitive deficits seen in MPTP-induced Parkinson model mice. Neuroscience 2014, 259, 126-141. [CrossRef]
- Nedergaard, S.; Flatman, J.A.; Engberg, I. Nifedipine- and omega-conotoxin-sensitive Ca2+ conductances in guinea-pig substantia nigra pars compacta neurones. J Physiol 1993, 466, 727-747.
- Sai, Y.; Chen, J.; Ye, F.; Zhao, Y.; Zou, Z.; Cao, J.; Dong, Z. Dopamine Release Suppression Dependent on an Increase of Intracellular Ca(2+) Contributed to Rotenone-induced Neurotoxicity in PC12 Cells. J Toxicol Pathol 2013, 26, 149-157. [CrossRef]
- Paraskar, A.; Sudalai, A. Cu(OTf)2 Catalyzed High Yield Synthesis of Hantzsch 1,4-Dihydropyridines. Cheminform 2007, 38. [CrossRef]
- Wu, C.; Bian, Q.; Ding, T.; Tang, M.; Zhang, W.; Xu, Y.; Liu, B.; Xu, H.; Li, H.-B.; Fu, H. Photoinduced Iron-Catalyzed ipso-Nitration of Aryl Halides via Single-Electron Transfer. ACS Catalysis 2021, 11, 9561-9568. [CrossRef]
- Guidi, M.; Moon, S.; Anghileri, L.; Cambié, D.; Seeberger, P.H.; Gilmore, K. Combining radial and continuous flow synthesis to optimize and scale-up the production of medicines. Reaction Chemistry & Engineering 2021, 6, 220-224. [CrossRef]
- Xiang, S.; Fan, W.; Zhang, W.; Li, Y.; Guo, S.; Huang, D. Aqueous CO2 fixation: construction of pyridine skeletons in cooperation with ammonium cations. Green Chemistry 2021, 23, 7950-7955. [CrossRef]
- Ban, T.A.; Morey, L.; Aguglia, E.; Azzarelli, O.; Balsano, F.; Marigliano, V.; Caglieris, N.; Sterlicchio, M.; Capurso, A.; Tomasi, N.A.; et al. Nimodipine in the treatment of old age dementias. Prog Neuropsychopharmacol Biol Psychiatry 1990, 14, 525-551. [CrossRef]
- Lopez-Arrieta, J.M.; Birks, J. Nimodipine for primary degenerative, mixed and vascular dementia. Cochrane Database Syst Rev 2002, CD000147. [CrossRef]
- Batuecas, A.; Pereira, R.; Centeno, C.; Pulido, J.A.; Hernandez, M.; Bollati, A.; Bogonez, E.; Satrustegui, J. Effects of chronic nimodipine on working memory of old rats in relation to defects in synaptosomal calcium homeostasis. Eur J Pharmacol 1998, 350, 141-150. [CrossRef]
- Gholami Pourbadie, H.; Naderi, N.; Janahmadi, M.; Mehranfard, N.; Motamedi, F. Calcium channel blockade attenuates abnormal synaptic transmission in the dentate gyrus elicited by entorhinal amyloidopathy. Synapse 2016, 70, 408-417. [CrossRef]
- Veng, L.M.; Mesches, M.H.; Browning, M.D. Age-related working memory impairment is correlated with increases in the L-type calcium channel protein alpha1D (Cav1.3) in area CA1 of the hippocampus and both are ameliorated by chronic nimodipine treatment. Brain Res Mol Brain Res 2003, 110, 193-202. [CrossRef]
- Topcu, A.; Saral, S.; Ozturk, A.; Saral, O.; Kaya, A.K. The effect of the calcium channel blocker nimodipine on hippocampal BDNF/Ach levels in rats with experimental cognitive impairment. Neurol Res 2023, 1-10. [CrossRef]
- Sandin, M.; Jasmin, S.; Levere, T.E. Aging and cognition: facilitation of recent memory in aged nonhuman primates by nimodipine. Neurobiol Aging 1990, 11, 573-575. [CrossRef]
- Pierrot, N.; Ghisdal, P.; Caumont, A.S.; Octave, J.N. Intraneuronal amyloid-beta1-42 production triggered by sustained increase of cytosolic calcium concentration induces neuronal death. J Neurochem 2004, 88, 1140-1150. [CrossRef]
- Ekinci, F.J.; Ortiz, D.; Shea, T.B. Okadaic acid mediates tau phosphorylation via sustained activation of the L-voltage-sensitive calcium channel. Brain Res Mol Brain Res 2003, 117, 145-151. [CrossRef]
- Higham, J.P.; Hidalgo, S.; Buhl, E.; Hodge, J.J.L. Restoration of Olfactory Memory in Drosophila Overexpressing Human Alzheimer's Disease Associated Tau by Manipulation of L-Type Ca(2+) Channels. Front Cell Neurosci 2019, 13, 409. [CrossRef]
- Zheng, Z.; Wu, K.; Ruan, Q.; Li, D.; Liu, W.; Wang, M.; Li, Y.; Xia, J.; Yang, D.; Guo, J. Suppression of Selective Voltage-Gated Calcium Channels Alleviates Neuronal Degeneration and Dysfunction through Glutathione S-Transferase-Mediated Oxidative Stress Resistance in a Caenorhabditis elegans Model of Alzheimer's Disease. Oxid Med Cell Longev 2022, 2022, 8287633. [CrossRef]
- Hopp, S.C.; Royer, S.E.; D'Angelo, H.M.; Kaercher, R.M.; Fisher, D.A.; Wenk, G.L. Differential neuroprotective and anti-inflammatory effects of L-type voltage dependent calcium channel and ryanodine receptor antagonists in the substantia nigra and locus coeruleus. J Neuroimmune Pharmacol 2015, 10, 35-44. [CrossRef]
- Putzier, I.; Kullmann, P.H.; Horn, J.P.; Levitan, E.S. Cav1.3 channel voltage dependence, not Ca2+ selectivity, drives pacemaker activity and amplifies bursts in nigral dopamine neurons. J Neurosci 2009, 29, 15414-15419. [CrossRef]
- Singh, A.; Verma, P.; Balaji, G.; Samantaray, S.; Mohanakumar, K.P. Nimodipine, an L-type calcium channel blocker attenuates mitochondrial dysfunctions to protect against 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine-induced Parkinsonism in mice. Neurochem Int 2016, 99, 221-232. [CrossRef]
- Kupsch, A.; Gerlach, M.; Pupeter, S.C.; Sautter, J.; Dirr, A.; Arnold, G.; Opitz, W.; Przuntek, H.; Riederer, P.; Oertel, W.H. Pretreatment with nimodipine prevents MPTP-induced neurotoxicity at the nigral, but not at the striatal level in mice. Neuroreport 1995, 6, 621-625. [CrossRef]
- Kupsch, A.; Sautter, J.; Schwarz, J.; Riederer, P.; Gerlach, M.; Oertel, W.H. 1-Methyl-4-phenyl-1,2,3,6-tetrahydropyridine-induced neurotoxicity in non-human primates is antagonized by pretreatment with nimodipine at the nigral, but not at the striatal level. Brain Res 1996, 741, 185-196. [CrossRef]
- Soderstrom, K.E.; O'Malley, J.A.; Levine, N.D.; Sortwell, C.E.; Collier, T.J.; Steece-Collier, K. Impact of dendritic spine preservation in medium spiny neurons on dopamine graft efficacy and the expression of dyskinesias in parkinsonian rats. Eur J Neurosci 2010, 31, 478-490. [CrossRef]
- Schuster, S.; Doudnikoff, E.; Rylander, D.; Berthet, A.; Aubert, I.; Ittrich, C.; Bloch, B.; Cenci, M.A.; Surmeier, D.J.; Hengerer, B.; et al. Antagonizing L-type Ca2+ channel reduces development of abnormal involuntary movement in the rat model of L-3,4-dihydroxyphenylalanine-induced dyskinesia. Biol Psychiatry 2009, 65, 518-526. [CrossRef]
- Li, Y.; Hu, X.; Liu, Y.; Bao, Y.; An, L. Nimodipine protects dopaminergic neurons against inflammation-mediated degeneration through inhibition of microglial activation. Neuropharmacology 2009, 56, 580-589. [CrossRef]
- Gordeev, M.F.; Patel, D.V.; Gordon, E.M. Approaches to Combinatorial Synthesis of Heterocycles: A Solid-Phase Synthesis of 1,4-Dihydropyridines. J. Org. Chem. 1996, 61, 924-928. [CrossRef]
- Balaev, A.N.; Osipov, V.N.; Fedorov, V.E. Development of nimodipine production technology. Pharm. Chem. J. 2012, 46, 285-287. [CrossRef]
Scheme 1.
Unique total production of ANAVEX2-73 1.

Scheme 2.
Synthesis of caffeine 2 from uracil 9.
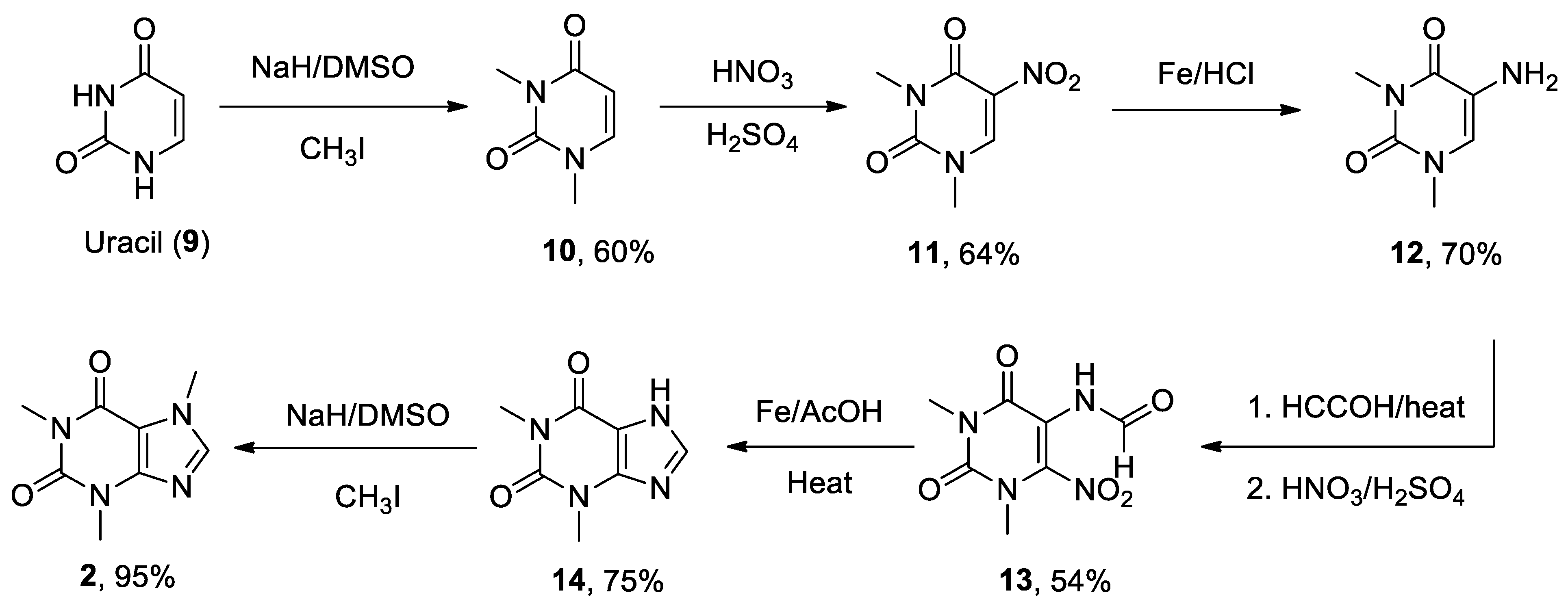
Scheme 3.
Novel approaches for the N-methylation of theophylline 14.
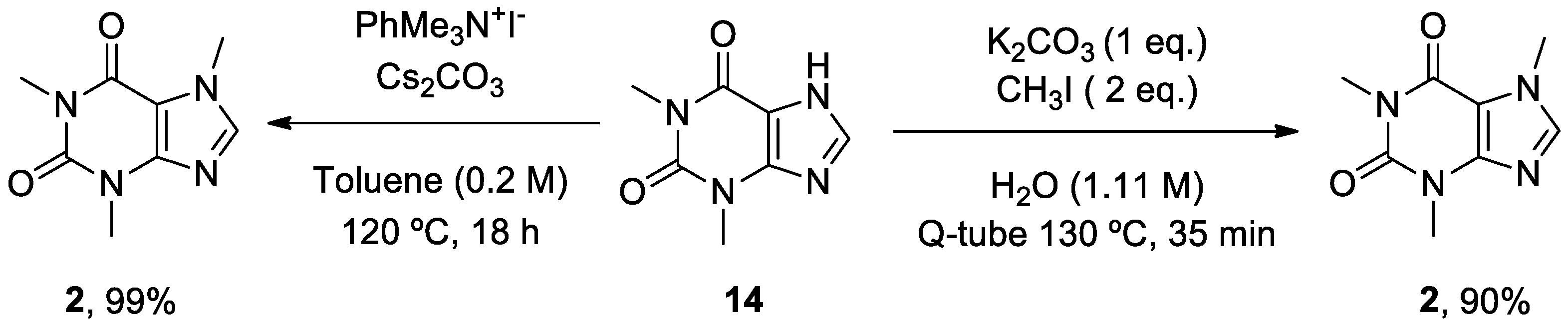
Scheme 4.
Schwartz’s strategy for the synthesis of diltiazem 3.
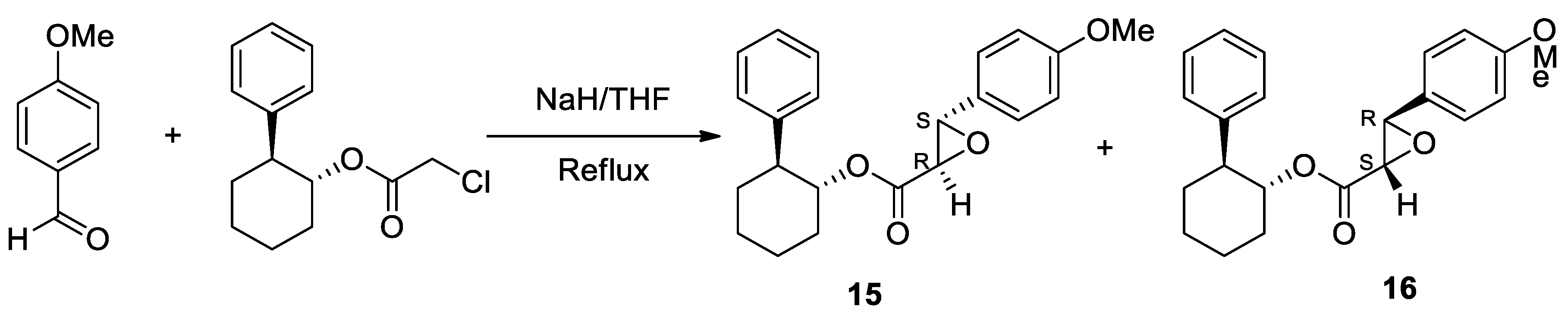
Scheme 5.
Enantiomerically pure key intermediate 18 for diltiazem 3 production.
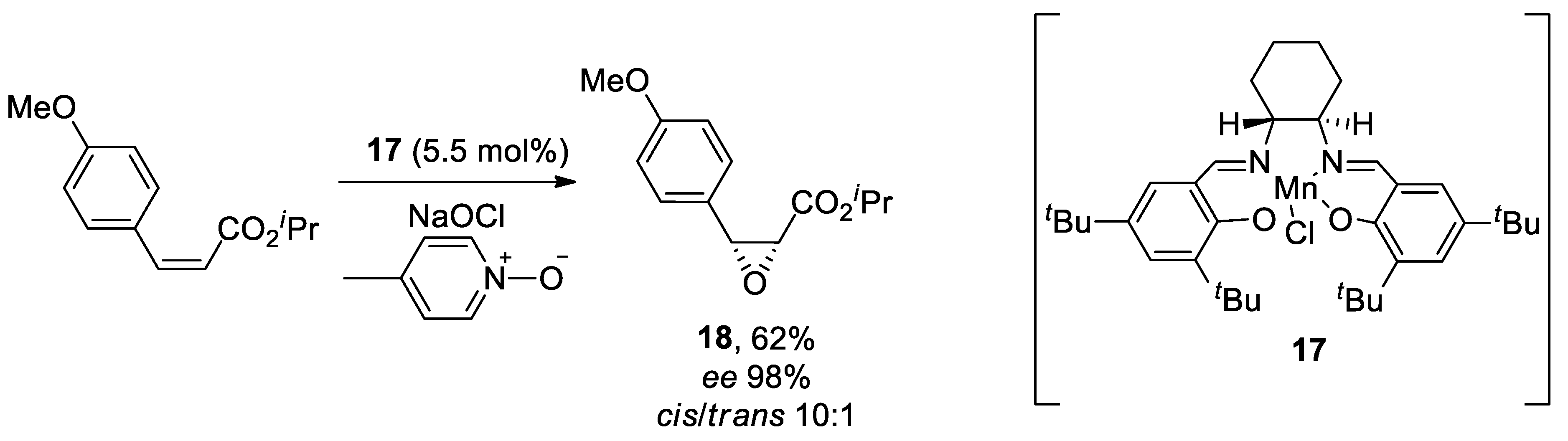
Scheme 6.
Chemoenzymatic synthesis of diltiazem 3.
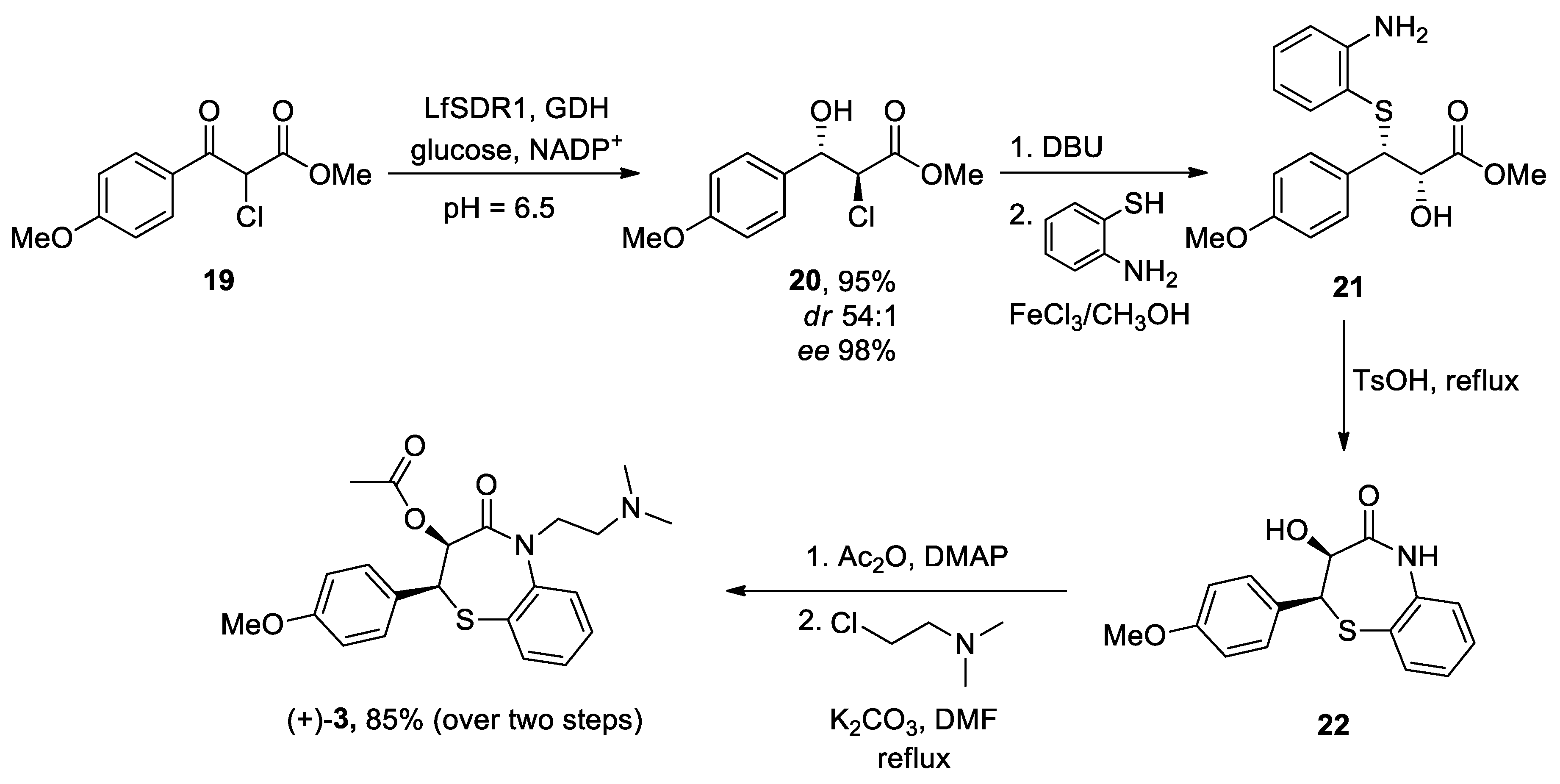
Scheme 7.
Zheng’s protocol to generate latrepirdine 4.
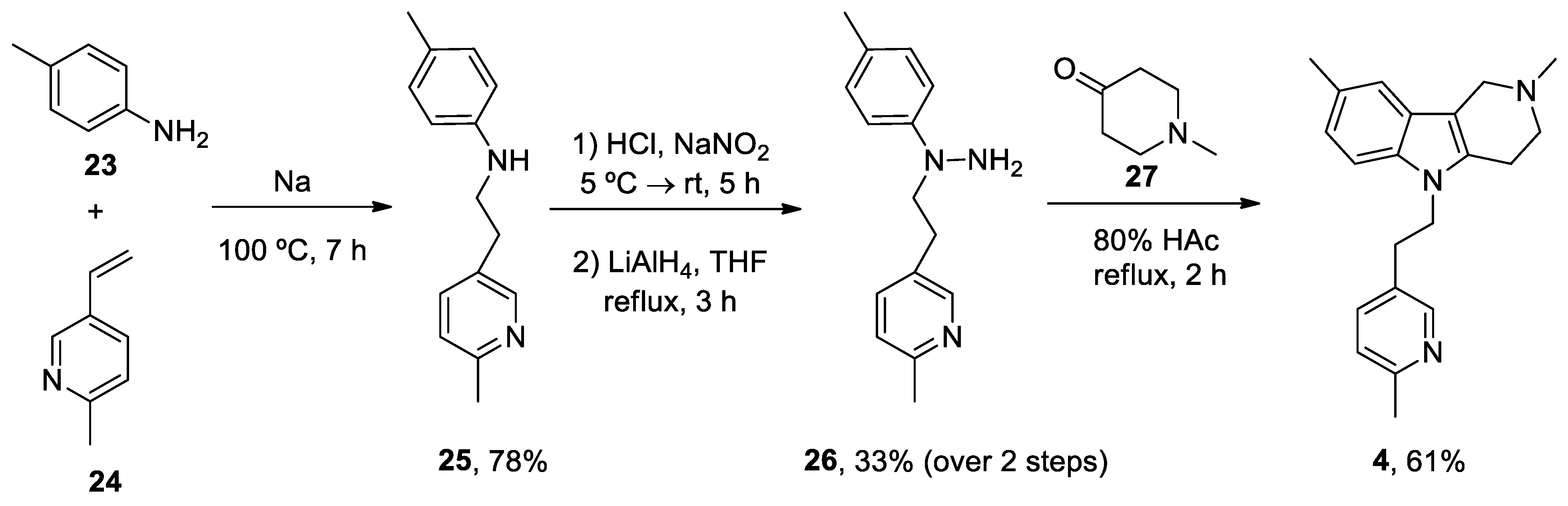
Scheme 8.
Ruthenium (III) catalysis used in the synthesis of latrepirdine 4.
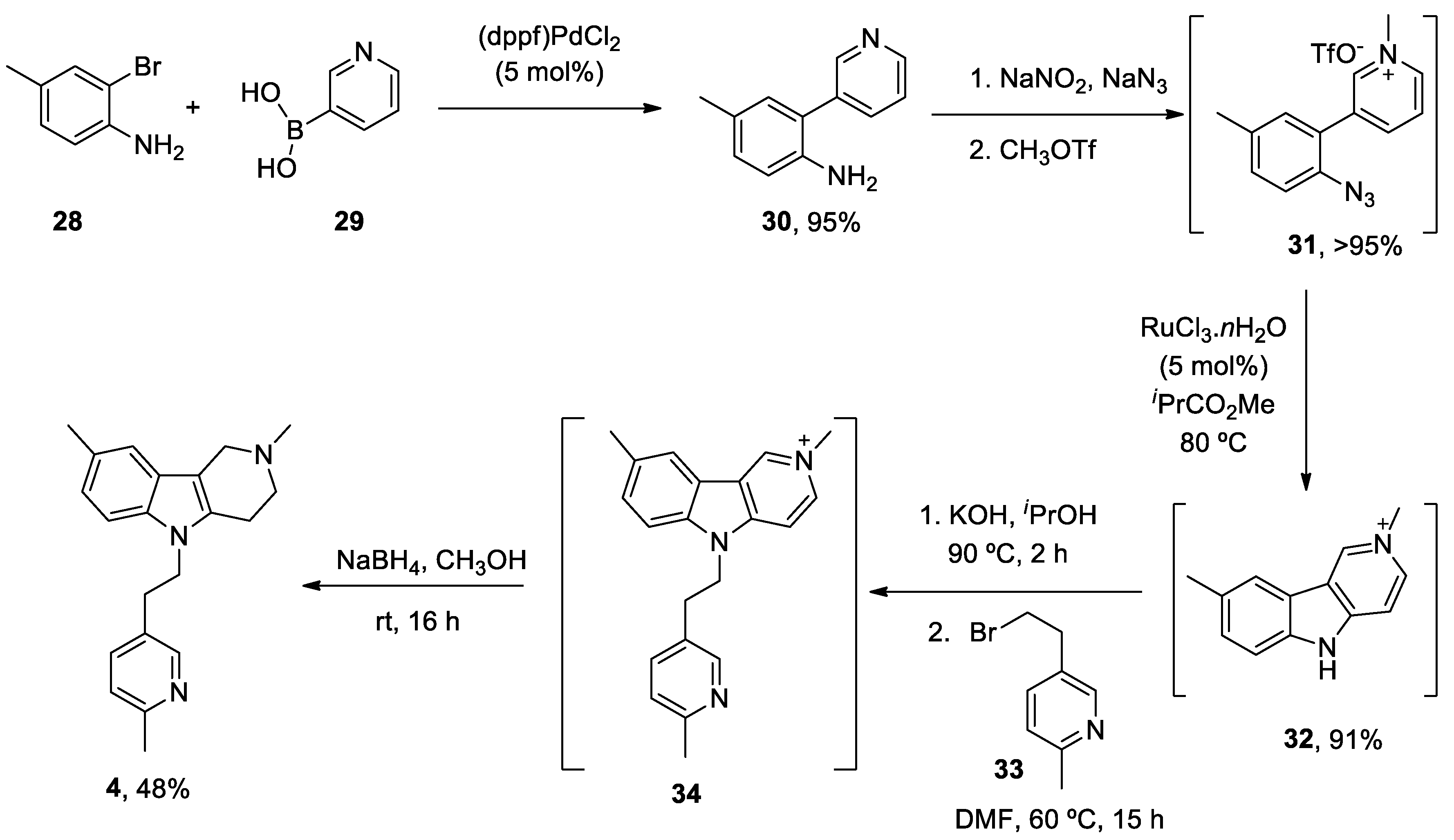
Scheme 9.
Hantzsch reaction used in the preparation of nifedipine 5.
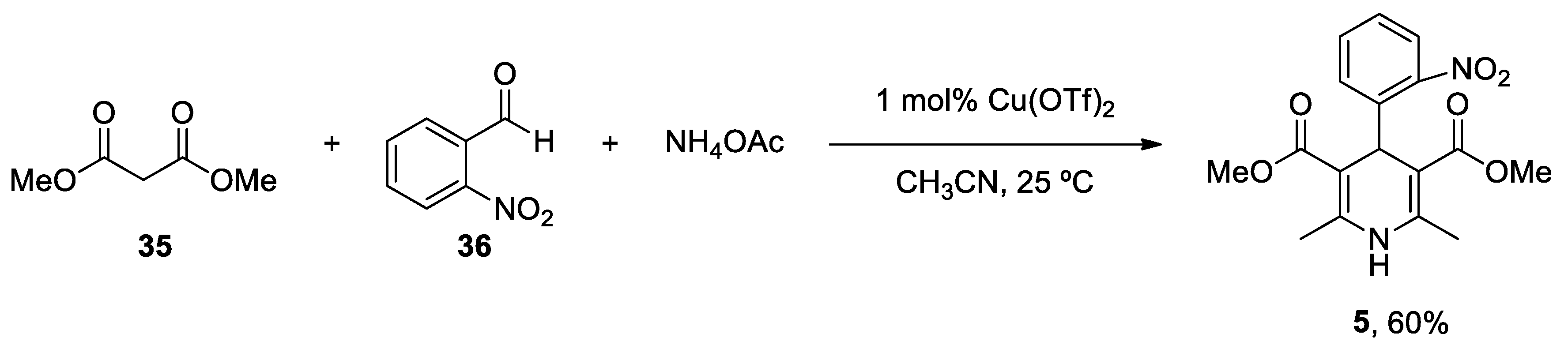
Scheme 10.
Synthesis of nifedipine 5 via photoinduced iron-catalysed ipso-nitration.
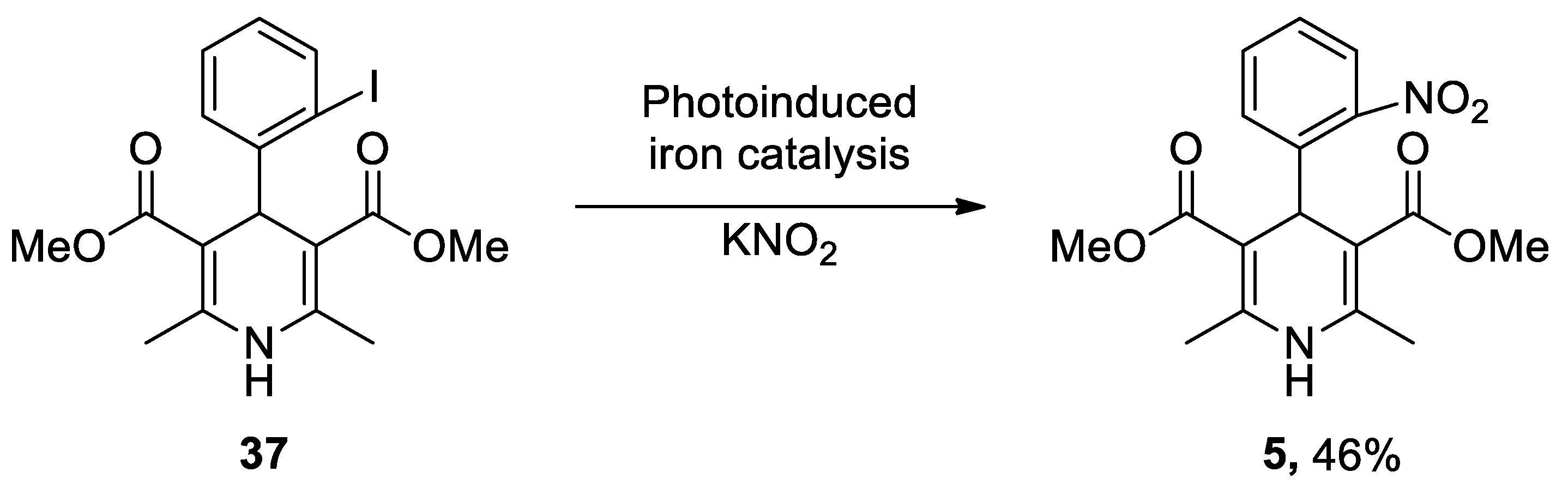
Scheme 11.
First flow multicomponent synthesis of nifedipine 5.
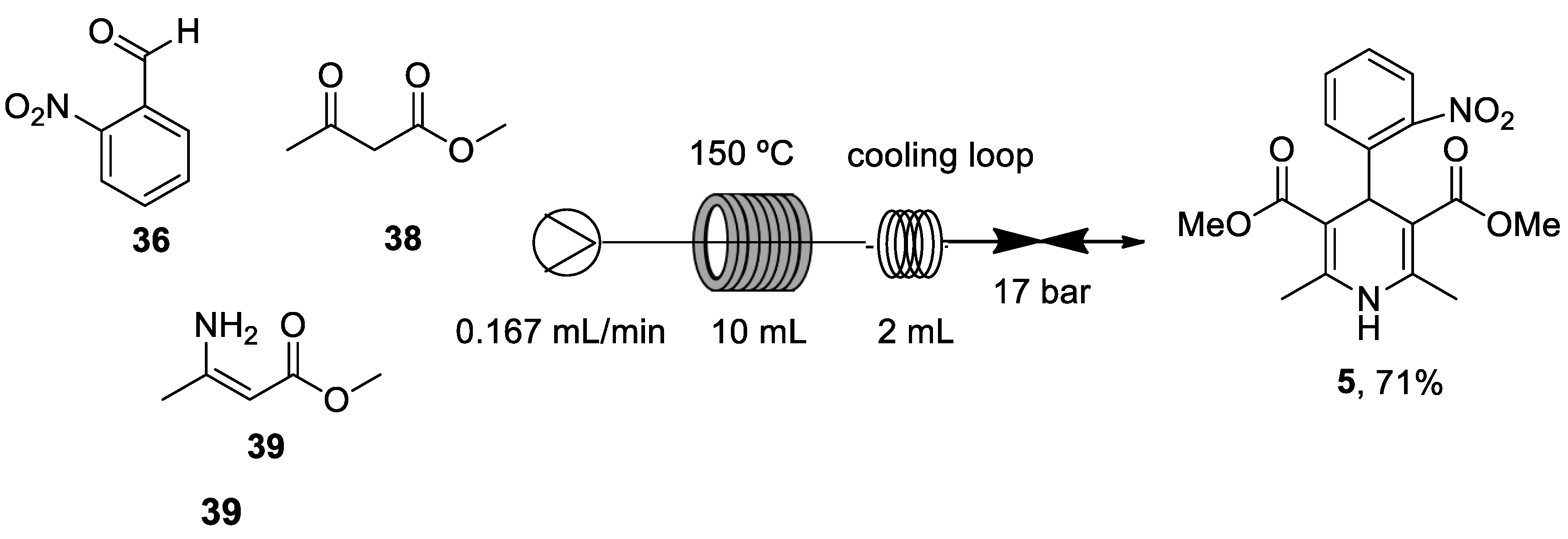
Scheme 12.
Generation of nifedipine 5 by using the green approach.
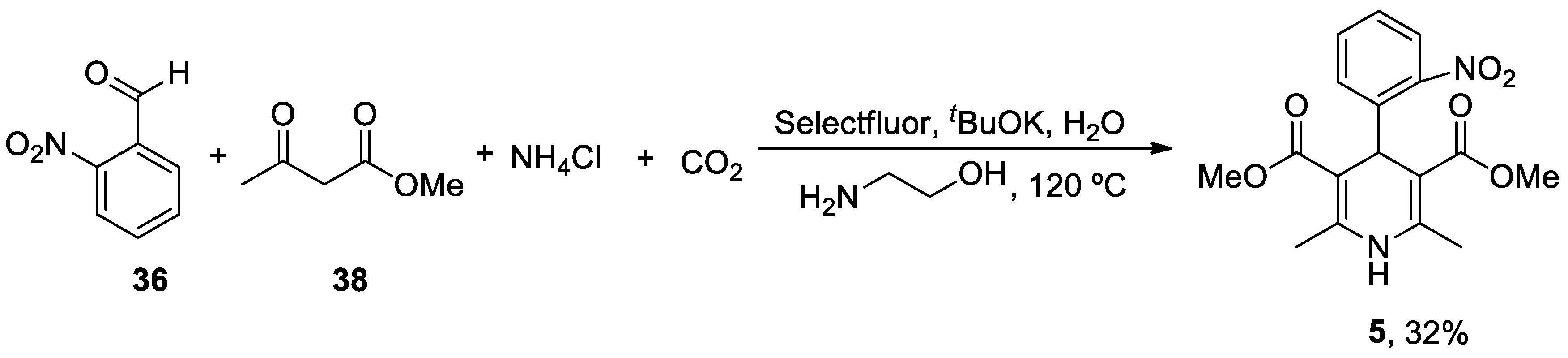
Scheme 13.
Solid-phase production of nimodipine 6.
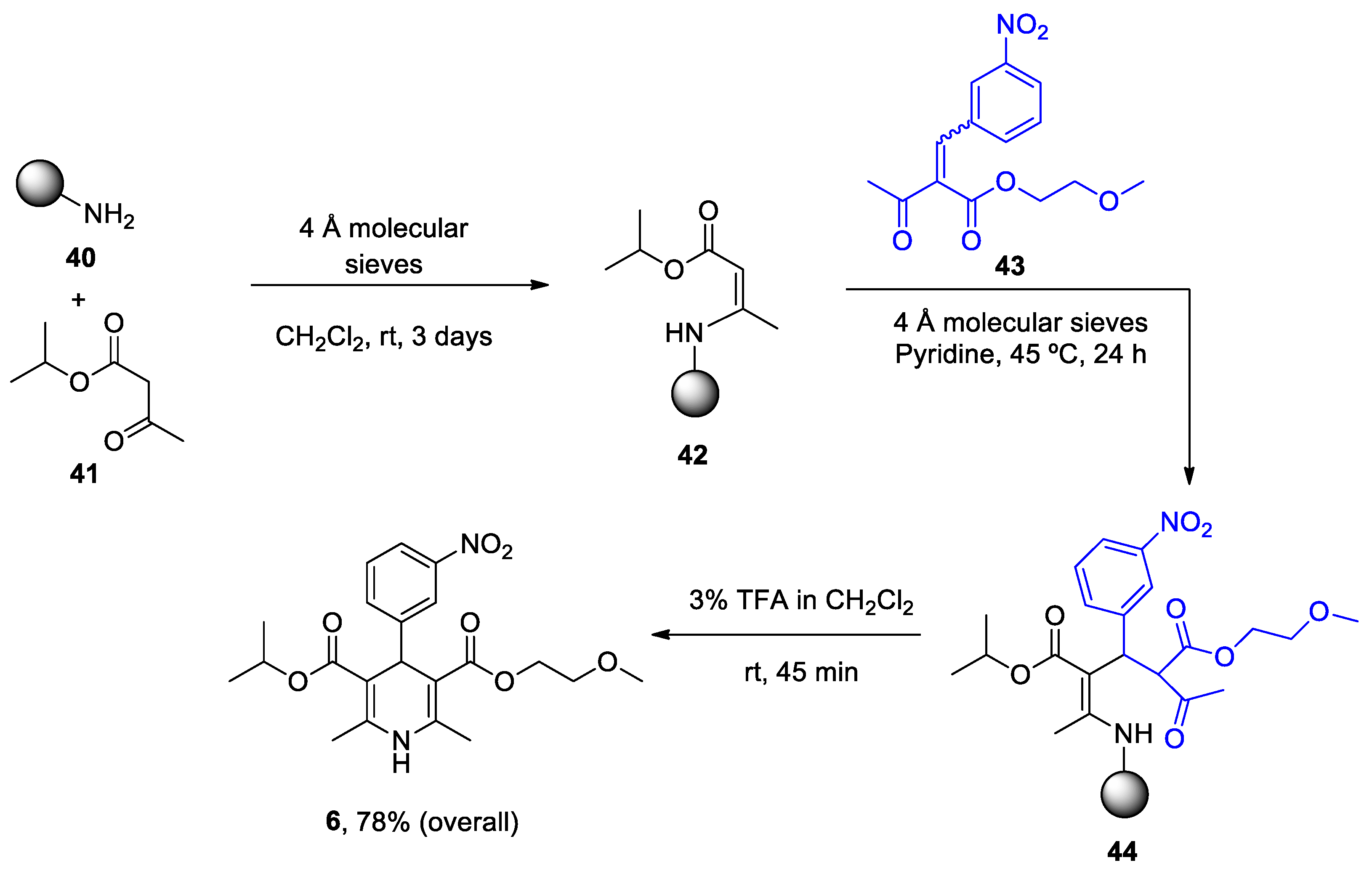
Scheme 14.
Production of nimodipine 5 in pilot batches by Pharm. Sintez. Co.
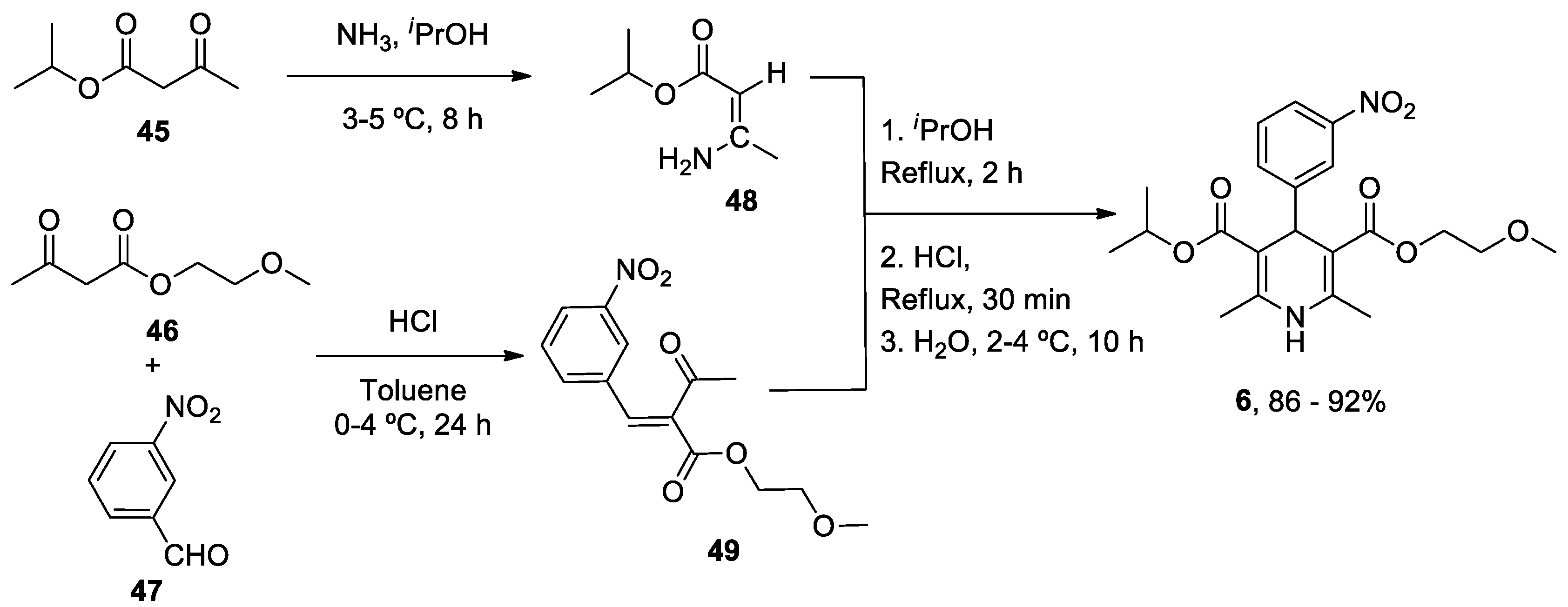

Table 1.
Summary of heterocycle compounds effects on AD and PD.
| Heterocyclic Compound | Chemical Name | Target | Proposed Mechanism | Effect on Neurodeg. Dis. Clinical Trial Status | References (Clinical Trials) |
|---|---|---|---|---|---|
| ANAVEX2-73 (Blarcamesine) | Tetrahydro-N,N-dimethyl-2,2-diphenyl-3-furanmethanamine hydrochloride |
mAChRs S1R |
↓ Ca2+ release ↓ Mitochondrial stress Activated antioxidant response pathways Limited apoptosis |
↓ Risk of developing AD and PD AD (Phase IIb/3) AD (Phase III) PDD (Phase II) PDD (Phase III) |
[62] ANAVEX2-73-AD-004 NCT03790709 NCT04575259 NCT03774459 |
|
Caffeine (Mateine) |
1,3,7-Trimethyl-3,7-dihydro-1H-purine-2,6-dione |
A2AR RyR (+) |
↓ Oxidative damage ↓ Aβ levels ↓ α-Syn aggregates Restored AChE and Na+/K+ ATPase activity |
↓ Risk of developing AD and PD Epidemiological studies: motor benefits in PD |
[73,74,75] [81,82,83,84,85,86,87,88] |
|
Diltiazen (Cardizem) |
(2S,3S)-5-(2-(Dimethylamino)ethyl)-2-(4-methoxyphenyl)-4-oxo-2,3,4,5-tetrahydrobenzo[b][1,4]thiazepin-3-yl acetate | Non-dihydro-pyridine VOCC | ↓ Ca2+ entry ↓ Oxidative damage ↓ Inflammation |
↓ Risk of developing PD Epidemiological & Randomization Studies |
[102] |
|
Latrepirdine (Dimebon) |
3,6-Dimethyl-9-(2-methyl-pyridyl-5)-ethyl-1,2,3,4-tetrahydro-γ-carboline dihydrochloride |
H1R Other Ca2+ Channels |
↓ Ca2+ release and entry ↓ Aβ levels ↓ Oxidative damage to lipids Inhibitor AChE ↓ α-Syn |
Cognitive and psychiatric benefits in AD Phase III AD: discontinued |
[111,112,113] NCT00838110 |
|
Nifedipine (Procardia) |
3,5-Dimethyl 2,6-dimethyl-4-(2-nitrophenyl)-1,4-dihydropyridine-3,5-dicarboxylate | L-Type VOCC | ↓ Ca2+ entry ↓ Aβ production ↓ Oxidative damage |
Do not ↓ risk of developing PD Epidemiological & Randomization Studies |
[133] |
|
Nimodipine (Nimotop) |
3-isopropyl 5-(2-methoxyethyl) 2,6-dimethyl-4-(3-nitrophenyl)-1,4-dihydropyridine-3,5-dicarboxylate | L-Type VOCC | ↓ Ca2+ entry Neuroprotection ↓ Aβ toxicity ↓ Oxidative damage Abolished pacemaking activity in DA neurons |
↓ Risk of developing AD Epidemiological & Randomization Studies |
[145,146] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



