
Submitted:
24 January 2023
Posted:
25 January 2023
You are already at the latest version
Abstract
The rising global incidence of acute and chronic kidney diseases has increased the demand for renal replacement therapy. This issue, compounded with the limited availability of viable kidneys for transplantation, has propelled the search for alternative strategies to address the growing health and economic burdens associated with these conditions. In the search for such alternatives, significant efforts have been devised to augment the current and primarily supportive management of renal injury with novel regenerative strategies. For example, gene- and cell-based approaches that utilize recombinant peptides/proteins, gene, cell, organoid, and RNAi technologies have shown promising outcomes primarily in experimental models. Supporting research has also been conducted to improve our understanding of the critical aspects that facilitate the development of efficient gene- and cell-based techniques that the complex structure of the kidney has traditionally limited. This manuscript is intended to communicate efforts that have driven the development of such therapies by identifying the vectors and delivery routes needed to drive exogenous transgene incorporation that may support the treatment of acute and chronic kidney diseases.
Keywords:
acute kidney disease
; chronic kidney disease
; gene therapy
; cell therapy
1. Introduction
Renal dysfunction can be acute, chronic, or end-stage, manifesting in several forms. The most prevalent cases arise from congenital disorders [1,2]; nephrotoxicity [3]; ischemia-reperfusion injury [4,5]; systolic hypotension and hemorrhage [6]; hypertension [7]; trauma [8]; essential mineral deficiencies [9]; malignancies [10]; diabetes [11,12]; and viral infections, as observed with the COVID-19 pandemic [13,14]. Paradoxically, hospitalization and the complex relationship between various forms of kidney injuries are additional factors that can contribute to renal dysfunction. For decades, clinicians have been aware of the risk of patients, with and without underlying kidney injury, developing hospital-acquired kidney malfunction [15]. They have also been aware of the complex connection between acute kidney injury (AKI) and chronic kidney disease (CKD), whereby they are closely linked and likely promote one another. For instance, CKD is a reputed risk factor for developing AKI during hospitalization, while there is a growing body of evidence illustrating how AKI accelerates the progression of CKD in critically ill patients [16], particularly hospitalized COVID-19 patients [17].
From a global perspective, it is estimated that AKI affects approximately 13 million people annually, contributing to nearly 1.7 million annual deaths [18]. Traditionally, AKI is a critical stage in injury progression because of its reversibility [19]. In comparison, CKD affects over one-tenth of the general population worldwide [20], and eventually, these conditions contribute to 5-8 million patients with end-stage renal disease (ESRD) requiring renal replacement therapy [21]. AKI is a critical stage in injury progression because of its reversibility [21]. Beyond this stage, treatment options are limited to renal replacement therapy, as the dysfunction has progressed to either CKD or, unfortunately, ESRD. It was previously thought that AKI, a sudden reduction in renal function, was fully reversible in all patients [22]. Nevertheless, recent research has gone against this notion based on studies conducted on individuals with reduced filtration capacities who are more prone to ESRD progression and mortality than a reversal of the condition [23,24].
These facts highlight significant clinical problems that arise from acute and chronic disorders. Furthermore, from a financial perspective, these patients often require long-term hospitalization, which imposes substantial burdens on the healthcare systems related to the etiologies of these disorders and their complex and debilitating interconnected nature. Likewise, these conditions lead to enhanced levels of morbidity and reductions in quality of life. Overall, morbidity and mortality are expected to rise exponentially with the growing rates of diabetes and cardiovascular diseases. Given that current treatments are mainly preventive strategies and early detection and intervention can be difficult in asymptomatic patients with these conditions, there is a definite need for alternative strategies to address the growing prevalence and subtle progression of renal dysfunction and ultimately reduce the need for renal replacement therapy [5,25,26,27].
In the search for such strategies, significant efforts are being devised to augment the present-day management of kidney disease using novel regenerative strategies. For example, gene- and cell-based approaches that utilize recombinant peptides/proteins, gene, cell, organoid, and RNAi technologies have shown promising outcomes primarily in experimental models [25]. Accompanying efforts have also been devised to facilitate the development of efficient gene- and cell-based techniques. This article is intended to convey efforts that have advanced these alternative forms of therapy by highlighting vectorization and mechanisms that can elicit genetic modifications that may support the treatment of acute and chronic kidney diseases.
2. Efforts to devise effective genetic alterations in the kidney
2.1. Recombinant peptides and proteins
Various methods have been proposed to deliver exogenous genes to mammalian cells. For the kidney, attempts have been made to protect and repair renal function by targeting single genetic loci with purified protein products, plasmids, recombinant growth factors, and viruses encoding peptides and proteins. Intravenous doses of human growth factor (HGF), which has anti-fibrotic properties, have promoted kidney repair in rodents with CKD [28,29]. Injections of IL-18BP, a recombinant interleukin, improved renal function, restored tubular morphology, and decreased tubular necrosis and apoptosis in small animal models [30]. Cell-based approaches conducted with intrarenal injections of human placenta-derived stem cells have also ameliorated damage in ischemia-reperfusion settings of AKI [31].
Single intravenous doses of plasmids encoding human growth factor (HGF) have also been shown to improve tissue regeneration and protect tubular epithelial cells from injury and apoptosis during acute renal failure [32]. In such earlier studies, HGF also helped preserve renal structure in chronic injury models by activating matrix degradation and reducing fibrosis[33,34,35]. Researchers have tested growth hormone-releasing hormone (GHRH) plasmid-based therapy in feline and canine chronic injury models. GHRH-treated animals displayed better levels of erythropoiesis, urea and creatinine clearances compared to controls [36], as well as more recent findings related to its therapeutic effect in CKD patients [37].
It has been well-established that adenovirus and adeno-associated virus vectors are two of the most efficient systems for transducing non-dividing cells [38] and have been used to target a variety of genetic loci. Other experimental studies have used adeno-based vectors for gene transfer. Lately, such vectors have displayed the long noncoding RNA-H19-derived attenuation of acute ischemic kidney injury [39] and the mediation of AKI to CKD progression [40]. These vectors have also helped preserve renal microvascular morphology and suppress the progression of AKI via the upregulation of vascular endothelial growth factor (VEGF) and angiopoietin [41]. Interestingly, the inhibition of VEGF also promoted structural and functional improvements in diabetes-induced chronic kidney disease [42,43]. These findings support the long-derived notion that repairing ischemic and toxic renal injuries depended critically on regulating a redundant, interactive network of cytokines and growth factors [44]. Thus, it would be of value to devise a system that could reliably modulate gene expression levels to return kidney function to near-normal baseline levels without inducing viral-derived toxicity. However, despite its benefits regarding kidney function recovery, recombinant agents have short half-lives and require large doses [45]. Further studies are needed to demonstrate consistent safety and effectiveness levels before these experimental techniques become clinical practice [46].
3.2. Cell and organoid transplantation
Cell therapy is another option to improve tissue/organ regeneration. Research efforts initially focused on cell transfer for bone marrow and organ transplantation, blood transfusion, and in vitro fertilization [47]. Nowadays, this technique is being developed to facilitate the repair/replacement of damaged and lost compartments in solid organs. This regenerative strategy transplants cells, which deliver genes of interest, to targeted organs. To achieve this purpose, investigators use the following cells: stem or progenitor cells; mature, functional cells from humans or animals; and genetically modified and transdifferentiated cells [47,48,49,50]. More recently, organoids, transdifferentiated three-dimensional cell clusters, arose as another promising option to enhance or restore kidney function [51,52,53].
Papazova et al. published a meta-analysis of CKD and cell therapies [54]. This analysis demonstrated that more than half of all cell-based studies focused on the therapeutic effects of single intravenous doses of mesenchymal stem cells. About a third of the studies investigated the preventive benefits of such therapies, while half of the studies focused on their therapeutic benefits. For instance, in AKI animal models, mesenchymal stem cells improved renal function [55,56,57]. Even though the specific mechanisms of action are still under investigation, these cells helped reduce renal fibrosis, improve remodeling, and promote neoangiogenesis [58]. Kelly et al. also helped restore renal function using undifferentiated reprogrammed cells to generate sera amyloid A proteins in ischemia-reperfusion, plus gentamicin- and cisplatin-based nephrotoxicity acute injury rat models [59].
Additional efforts have also reported the successful differentiation of embryonic and induced pluripotent stem cells into tubular, glomerular, and whole nephron organoids [60,61,62,63,64,65,66,67]. A greater understanding of the roles of key signaling pathways has also allowed investigators to differentiate stem cell niches into various lineages. We believe that shortly, organoids derived from patients’ cells will be able to repopulate decellularized renal scaffolds and printed tissues or even be injected back into the patients to restore their native dysfunction [68,69]. Nevertheless, many technical [70,71,72,73,74,75,76] and ethical [77,78,79,80,81,82,83,84,85] issues still need to be solved in this field. It is well-established that embryonic stem cell technology offers hope for new therapies, yet societal and moral incongruences limit their use. Teratoma, a hallmark of pluripotency [86,87,88,89], is a significant concern after implantation. The ability to culture and manipulate human stem cells indefinitely while simultaneously governing their differentiation characteristics offers excellent possibilities for the future of medicine [90,91,92].
2.3. RNA interference therapy
Another option within the growing arsenal of gene and cell therapy applications is RNA interference (RNAi). The discovery of mammalian RNAi is one of the most promising therapeutic strategies because enables silencing any gene [93]. RNAi is an advantageous technique, as it is easier to silence deficient and non-functional genes than replace them [94]. Moreover, RNAi is the most practical approach thus far, as it is relatively low cost, highly specific, and can inhibit multiple genes of various pathways simultaneously [95]. This technology can help identify complex genetic loci essential to human pathology.
RNAi is an endogenous process that allows cells to regulate their genetic activity. This process remains central to gene expression and the defense against mutagenesis generated from viral genes and transposons [96]. The primary methods that induce exogenous RNAi-based gene silencing utilize micro-RNA (miRNA), small interfering RNA (siRNA), and small hairpin RNA (shRNA) systems. Since Napoli and Jorgensen first reported on this phenomenon in 1990 [97], there has been a growing interest in using RNAi technology to improve renal health [93]. This interest has directed RNAi-based research focused on improving the study and management of kidney disease by identifying miRNA targets and AKI biomarkers. It has also prompted interest in improving the delivery of exogenous silencing mediators and siRNA and shRNA targets to either reduce or protect against renal injury. Currently, lipid nanoparticles are the most frequently used formulation to mediate silencing [98], and further work has been proposed to determine in vivo silencing efficiencies and investigate other small RNAs that can affect post-transcriptional gene silencing [99,100].
From a diagnostic standpoint, several studies have provided fundamental insight into renal injury biomarkers. Valadi et al. showed that miRNAs recovered from urinary exosomes provide information about the kidney in standard and injury settings [101]. Zhou et al. showed that miR-27b and miR-192 in these urinary vesicles could differentiate between glomerular and tubular damage [102]. Also, from a therapeutic standpoint, exosomes containing miRNAs can enter recipient cells by membrane surface proteins. This phenomenon offers a new mechanism for cell-cell communication and gene delivery [103,104,105,106,107,108,109]. In a study by Cantaluppi, microvesicles enriched with pro-angiogenic miR-126 and miR-296 were injected into the vein, enhanced tubular cell proliferation, and reduced apoptosis and leukocyte infiltration [110]. In AKI settings, such silencing has demonstrated that the caspase-3 siRNA improved ischemic reperfusion (IR) injury with reduced caspase-3 expression and apoptosis, better renal oxygenation and acid-base homeostasis, and the silencing IKKβ using siRNA diminished inflammation and protected the kidneys against IR injury [111]. Whereas, in a glomerulonephritic chronic injury model, MAPK1 suppression remarkably improved kidney function, reduced proteinuria, and ameliorated glomerular sclerosis [111].
RNAi therapy could be a valuable surrogate for treating patients with AKI by reducing the uptake of nephrotoxins, ameliorating immunologic response mechanisms, and downregulating harmful disease mediators [112,113,114]. Such characteristics have prompted interest in the knockdown of dynamin-2 (Dyn2) and low-density lipoprotein-related protein 2 (LRP2). Dyn2 is a critical component of the endocytic pathway [115,116,117], and its knockdown blocks clathrin-coat-dependent endocytosis and coat-independent fluid phase probe uptake in several epithelial cell lines [118]. In animal models, silencing LRP2 reduced gentamicin toxicity in proximal tubule epithelial cells [119,120,121]. In a rat model of kidney transplantation, caudal vein administration of siRNAs, which targeted connective tissue growth factor (CTGF), decreased renal fibrosis [122]. CTGF is an essential pro-fibrotic cofactor that is downstream from TGF-β. Electroporation also enhanced the delivery of siRNA targeted to TGF-β1, significantly reducing glomerular matrix deposition and proteinuria four and six weeks after anti-Thy-1 administration [122,123].
In other studies, which have investigated the renotherapeutic potential of siRNA technology [124], siRNA sequences were systemically delivered to inhibit the expression of p53. This strategy significantly reduced ischemia-induced p53 upregulation and helped attenuate ischemic and cisplatin-induced AKI [125,126]. The oligonucleotides used to facilitate RNAi contained stabilizing modifications with a relatively low affinity for albumin and other plasma proteins. Such modifications diminished their hepatic distribution and degradation in serum and facilitated their renal clearance and endocytic tubular uptake [126]. This fact limits the class of therapeutic siRNAs for such procedures because of the natural tendency of systemically delivered materials to accumulate within the liver.
In comparison, the expression of transgenic shRNA targeting the proapoptotic BIM gene prevented the development of polycystic kidney disease in BCl-2 deficient mice [127]. However, the mortality rate in this study was high. Additional research is required to identify whether the high mortality rate was due to the sequence of the shRNA.
3. Mechanisms for exogenous transgene expression in mammalian cells
One major challenge to developing gene- and cell-based strategies is our need to understand their mechanisms of action. Regardless of the performance of recombinant peptides, DNA vectors, stem cells, and RNAi agents, mechanisms related to each approach still need to be discovered [46,68,128,129,130,131,132,133]. This gap in knowledge makes it difficult to optimize these techniques. Nevertheless, the basic principles for successful transgene expression have been documented [128,129,130,131,132,134,135,136,137,138,139,140]. All such therapies rely on efficiently delivering exogenous genes to widespread cellular targets. The techniques discussed earlier have achieved this by directly using DNA/RNA strands or inserting these molecules into gene transport vehicles. Once the genetic materials enter the nuclei, they either aid or inhibit the expression of the gene product(s) of interest in transformed cells and their progeny.
Likewise, the overall efficacy of RNAi in inducing gene silencing in any cell depends on the ability of the dsRNA reagent to access the subcellular compartment containing the RNA-induced silencing complex (RISC) and other components of the RNAi machinery [141,142]. This subcellular compartment is in the perinuclear region of the cytoplasm. However, if cell transplantation mediates transgene expression, the gene delivery process will rely on integrating the delivered cells, native cellular division, and intercellular communication. Furthermore, the goal is to facilitate gene expression/inhibition once exogenous cells are integrated into tissues and organs [143,144].
For instance, previous work suggests that the effectiveness of gene therapies using adenoviral [145] and siRN [146] vectors depends on the dose and timing of transgene administration. Such dependence drives variations in drug concentrations at the respective sites of the gene expression and silencing machinery.
It is, therefore, essential to understanding how effective concentrations within the cytoplasm affect therapeutic potency based on dosing and timing of transgene administrations. This factor is a topic of practical importance, as the mechanism(s) will determine the intracellular fate of exogenous transgenes from non-viral, viral, and cellular sources and aid the development of effectual medical strategies that can control the duration and extent of induced genetic traits. Alternatively, for approaches that focus on whole organ engineering and re-engineering, additional insights are needed into the mechanisms behind the successful repopulation of tissue and organ templates [64]. Researchers must also determine the characteristics required to facilitate exogenous genetic and cellular harmony for viable transplantable kidneys before these findings can translate into clinical practice.
4. Key aspects to facilitate advancements in renal genetic medicine
4.1. The development of efficient delivery techniques
Over the past 30 years, many methods have been proposed to deliver exogenous genes and cells to target organs [31,38,45,95,98,100,128,140,147,148,149,150,151,152,153,154,155]. From a fundamental viewpoint, these techniques seek to provide inexpensive and rapid alternatives to pronuclear microinjection-derived transgenic models and platforms for translational studies [119]. However, a limiting step in this process is the need for more reliable delivery systems. Several reports have indicated inconsistent outcomes regarding the effectiveness of existing gene and cell transfer techniques. Studies in the kidney have illustrated this variability [153,154,156,157,158,159,160,161,162]. In general, an in vivo gene and cell transfer system's success relies on various factors. The factors include:
- the ability to deliver vectors to the target cells/organ;
- the time the target cell/organs take to express the exogenous materials; and
- the number of cells/organs that express the required phenotype.
Other essential factors are the resulting expression levels, cellular turnover rates, the reproducibility of the process, and the severity of the injury that may result from it [93,128]. Thus, most existing strategies remain experimental [163,164,165,166].
Researchers must consider organ morphology and function variations as crucial elements to improve the overall efficacy of delivery strategies [167,168]. Thus, efficient gene and cellular therapies for treating kidney diseases remain challenging [46,169,170,171,172,173]. The structure of the renal vasculature and its unique characteristics are prominent limiting factors. Systems focusing on proximal tubular epithelial cellular uptake could be helpful [173,174,175]. However, a potential drawback to this technique is the variations in the glomerular permeability of different molecules [176,177,178,179,180,181]. Likewise, the unknown degree to which these cells are accessible for gene delivery at the basolateral surface via the peritubular capillaries provides another level of complication. Studies using adenovirus vectors have demonstrated the need to improve our understanding of renal physiology and our ability to manipulate it.
Intra-arterial kidney injections, pre-chilled for extended periods, facilitated transgene expression within the cortical vasculature [182]. Combining the pre-chilling treatment with vasodilators provided gene transfer in the outer medulla's inner and outer strips [182]. Other studies have successfully presented adenoviral vector delivery to rat glomerular and tubular compartments by infusions into the right renal artery [183,184]. This technique provided high levels of transgene expression for 2-4 weeks without causing significant damage [185,186]. Analogous concentrations of the same adenovirus vector were suspended in different volumes and delivered to the kidney via arterial injections and pelvic catheter infusions. This approach facilitated transgene expression in distinct kidney regions [186,187]. After injecting vectors into the aorta at a location proximal to the left renal artery, the investigators observed transgene expression only in proximal tubular cells.
Tail vein and retrograde ureteral adenovirus infusions that target aquaporin water channels also reported different expression levels, which depended on the transgene infusion site [128,154]. Aquaporin 1 transgenes were expressed in apical and basolateral membranes of proximal tubule epithelial cells in the renal cortex but not in the glomerulus, loop of Henle, or collecting duct. Conversely, ureteral and renal papilla transgene expression was reported through ureteral infusions. The researchers also reported less intense and patchy expression in cortical collecting ducts. Ashworth et al. [188] and Tanner et al. [159] explored the direct transfer of adenovirus vectors that carried transgenes into individual nephron segments using micropuncture techniques. They observed site-specific transgene expression within the injected tubules or vascular welling points. These results also demonstrated the utility of intravital fluorescent multiphoton microscopy to monitor protein expression in live animals directly. However, one limitation of the approach was that the injection sites were the only places where the investigators found transgene expression.
These studies further highlight the challenge of introducing genes into multiple renal cell types due to the intricate anatomy of the kidney, even when using the same type of vector. Results depend on the transgene infusion site, volume, and rate, as well as the organ temperature and the use of vasodilators. Hydroporation may address these challenges by increasing vascular permeability and thus efficiently delivering exogenous substances throughout the kidney. Hydrodynamic fluid delivery impacts fluid pressures within thin, stretchable capillaries [189,190]. The enhanced fluid flow generated from pressurized injections produces rapid and high fluctuations in blood circulation. Theoretically, it increases the permeability of the capillary endothelium and epithelial junctions by generating transient pores in plasma membranes that facilitate the cellular internalization of macromolecules of interest [46,189,191]. The unique anatomy of the kidney provides various innate delivery pathways (artery, vein, and ureter) that may be ideal for hydrodynamic gene delivery. In our recent reports, this delivery method provided efficient and lengthy plasmid and viral expression in live rat kidneys [128,140,192] and facilitated protection against moderate forms of ischemia-reperfusion injury [152,193,194]. A summary of delivery methods and associated vectors is presented in Table 1.
4.2. Exogenous transgene vectors
The gene of interest is infused either systemically or directly into the kidney. Apart from the artery, vein, and ureter, direct infusions into the renal capsule and parenchyma using micro-needles [159,188] or blunt-tip needles [155,195] have also been proposed, along with indirect tail vein [189,194,196] and peritoneum [197,198] gene delivery schemes. As indicated before, the success of these methods varies per the anatomical location of the targeted cells and the types of vectors used to support gene expression. These vectors include PRC-amplified DNA fragments; plasmid DNA; liposomes; polycations; viral vectors; and stem cells [128]. If transformed cells act as gene vectors to promote transgene expression, they may be engineered with various anchoring or binding proteins/peptides to assist their integration into the tissue of interest [199]. This process mimics endogenous viral capsid components, which mediate receptor binding and support entry into mammalian cells. As observed in some injured kidney animal models, local healing/regeneration factors facilitate the incorporation of exogenous renal cells delivered intravenously [54]. An outline of transgene vector incorporation into the renal epithelium is presented in Figure 1.
Apart from achieving successful genetic modifications, we must also focus on exogenous transgene delivery and expression effects. Such considerations relate to the levels of cellular toxicity and injury that may occur during and after the transfer process. Endo- and exonucleases efficiently degrade DNA fragments [200,201]. However, an overload of exogenous DNA fragmentation may stimulate Ca2+ endonuclease activity, degrade endogenous DNA, and mediate cell death [202]. Similarly, plasmid DNA, prepared from bacteria, may induce unmethylated CpG motif toxicity that can trigger lower respiratory tract inflammatory responses [203]. Oligonucleotide therapies have also been shown to stimulate immune system responses and induce hepatotoxicity and nephrotoxicity [204]. Virus-induced toxic and immunogenic responses from high titers, protein overexpression, and capsid protein infections are also topics of significant concern [205]. Long-term mutagenesis may also be an issue. Reports have shown such events using recombinant adenovirus systems [206,207]. Specifically, slow-transforming insertional mutagenesis may arise from retroviruses that incorporate into an organism's genome [208], and in vivo stem cell quiescence can tamper with DNA repair mechanisms to further support mutagenesis [209].
5. Conclusions
There is a dire need to improve the clinical management of acute and chronic renal diseases. Preliminary outcomes in experimental models with kidney dysfunction managed by gene-based and cell-based approaches are promising. Recent findings echo the traditional need to address several challenges before these therapies become viable clinical options. Existing techniques provide a wide range of success rates and, in some instances, also induce harmful side effects. Thus, further research is needed to develop methods to induce transient or permanent modifications with minimal physiological interference or damage as we aim to improve the treatment of acute and chronic kidney diseases.
Author Contributions
P.R.C. conceived project, drafted, edited, and approved final version of manuscript.
Funding
This study was supported in part by the Khalifa University's College of Medicine and Health Sciences and Grant Number: FSU-2020-25 and funding from RC2-2018-022 (HEIC) awarded to Dr. Peter Corridon.
Acknowledgments
The author would like to thank Mrs. Maja Corridon for reviewing the manuscript.
Conflict of Interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Isert, S.; Müller, D.; Thumfart, J. Factors Associated With the Development of Chronic Kidney Disease in Children With Congenital Anomalies of the Kidney and Urinary Tract. Front. Pediatr. 2020, 8, 298. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, C. , et al., Polycystic kidney disease. Nature Reviews Disease Primers, 2018. 4(1): p. 50.
- Al-Kuraishy, H.M.; Al-Naimi, M.S.; Rasheed, H.; Hussien, N.R.; Al-Gareeb, A. Nephrotoxicity: Role and significance of renal biomarkers in the early detection of acute renal injury. J. Adv. Pharm. Technol. Res. 2019, 10, 95–99. [Google Scholar] [CrossRef]
- Burek, M.; Burmester, S.; Salvador, E.; Möller-Ehrlich, K.; Schneider, R.; Roewer, N.; Nagai, M.; Förster, C.Y. Kidney Ischemia/Reperfusion Injury Induces Changes in the Drug Transporter Expression at the Blood–Brain Barrier in vivo and in vitro. Front. Physiol. 2020, 11. [Google Scholar] [CrossRef]
- Pantic, I.; Cumic, J.; Dugalic, S.; Petroianu, G.A.; Corridon, P.R. Gray level co-occurrence matrix and wavelet analyses reveal discrete changes in proximal tubule cell nuclei after mild acute kidney injury. Sci. Rep. 2023, 13, 1–12. [Google Scholar] [CrossRef]
- Qureshi, A.I.; Huang, W.; Lobanova, I.; Hanley, D.F.; Hsu, C.Y.; Malhotra, K.; Steiner, T.; Suarez, J.I.; Toyoda, K.; Yamamoto, H.; et al. Systolic Blood Pressure Reduction and Acute Kidney Injury in Intracerebral Hemorrhage. Stroke 2020, 51, 3030–3038. [Google Scholar] [CrossRef] [PubMed]
- Jankowski, J. , et al., Cardiovascular Disease in Chronic Kidney Disease. Circulation, 2021. 143(11): p. 1157-1172.
- Jheong, J.-H.; Hong, S.-K.; Kim, T.-H. Acute Kidney Injury After Trauma: Risk Factors and Clinical Outcomes. J. ACUTE CARE Surg. 2020, 10, 90–95. [Google Scholar] [CrossRef]
- Lombardi, Y., C. Ridel, and M. Touzot, Anaemia and acute kidney injury: the tip of the iceberg? Clinical Kidney Journal, 2020. 14(2): p. 471-473.
- Malyszko, J.; Tesarova, P.; Capasso, G.; Capasso, A. The link between kidney disease and cancer: complications and treatment. Lancet 2020, 396, 277–287. [Google Scholar] [CrossRef]
- Forst, T.; Mathieu, C.; Giorgino, F.; Wheeler, D.C.; Papanas, N.; Schmieder, R.E.; Halabi, A.; Schnell, O.; Streckbein, M.; Tuttle, K.R. New strategies to improve clinical outcomes for diabetic kidney disease. BMC Med. 2022, 20, 1–15. [Google Scholar] [CrossRef]
- Alicic, R.; Nicholas, S.B. Diabetic Kidney Disease Back in Focus: Management Field Guide for Health Care Professionals in the 21st Century. Mayo Clin. Proc. 2022, 97, 1904–1919. [Google Scholar] [CrossRef] [PubMed]
- Adapa, S.; Chenna, A.; Balla, M.; Merugu, G.P.; Koduri, N.M.; Daggubati, S.R.; Gayam, V.; Naramala, S.; Konala, V.M. COVID-19 Pandemic Causing Acute Kidney Injury and Impact on Patients With Chronic Kidney Disease and Renal Transplantation. J. Clin. Med. Res. 2020, 12, 352–361. [Google Scholar] [CrossRef]
- Geetha, D.; Kronbichler, A.; Rutter, M.; Bajpai, D.; Menez, S.; Weissenbacher, A.; Anand, S.; Lin, E.; Carlson, N.; Sozio, S.; et al. Impact of the COVID-19 pandemic on the kidney community: lessons learned and future directions. Nat. Rev. Nephrol. 2022, 18, 724–737. [Google Scholar] [CrossRef]
- CKD increases risk of acute kidney injury during hospitalization. Nature Clinical Practice Nephrology, 2008. 4(8): p. 408-408.
- Hsu, R.K.; Hsu, C.-Y. The Role of Acute Kidney Injury in Chronic Kidney Disease. Semin. Nephrol. 2016, 36, 283–292. [Google Scholar] [CrossRef]
- Bell, J.S.; James, B.D.; Al-Chalabi, S.; Sykes, L.; A Kalra, P.; Green, D. Community- versus hospital-acquired acute kidney injury in hospitalised COVID-19 patients. BMC Nephrol. 2021, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Minja, N.W. , et al., Acute Kidney Injury and Associated Factors in Intensive Care Units at a Tertiary Hospital in Northern Tanzania. Can J Kidney Health Dis, 2021. 8: p. 20543581211027971.
- Tanemoto, F.; Mimura, I. Therapies Targeting Epigenetic Alterations in Acute Kidney Injury-to-Chronic Kidney Disease Transition. Pharmaceuticals 2022, 15, 123. [Google Scholar] [CrossRef]
- Kovesdy, C.P. Epidemiology of chronic kidney disease: an update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.C. and L.X. Zhang, Prevalence and Disease Burden of Chronic Kidney Disease. Adv Exp Med Biol, 2019. 1165: p. 3-15.
- Goyal, A. , et al., Acute Kidney Injury (Nursing), in StatPearls. 2022: Treasure Island (FL).
- Palevsky, P.M. Endpoints for Clinical Trials of Acute Kidney Injury. Nephron 2018, 140, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Muroya, Y.; He, X.; Fan, L.; Wang, S.; Xu, R.; Fan, F.; Roman, R.J. Enhanced renal ischemia-reperfusion injury in aging and diabetes. Am. J. Physiol. Physiol. 2018, 315, F1843–F1854. [Google Scholar] [CrossRef]
- Corridon, P.R.; Wang, X.; Shakeel, A.; Chan, V. Digital Technologies: Advancing Individualized Treatments through Gene and Cell Therapies, Pharmacogenetics, and Disease Detection and Diagnostics. Biomedicines 2022, 10, 2445. [Google Scholar] [CrossRef]
- Pantic, I.V.; Shakeel, A.; Petroianu, G.A.; Corridon, P.R. Analysis of Vascular Architecture and Parenchymal Damage Generated by Reduced Blood Perfusion in Decellularized Porcine Kidneys Using a Gray Level Co-occurrence Matrix. Front. Cardiovasc. Med. 2022, 9, 797283. [Google Scholar] [CrossRef]
- Pantic, I.; Paunovic, J.; Cumic, J.; Valjarevic, S.; Petroianu, G.A.; Corridon, P.R. Artificial neural networks in contemporary toxicology research. Chem. Interactions 2023, 369, 110269. [Google Scholar] [CrossRef]
- Oka, M.; Sekiya, S.; Sakiyama, R.; Shimizu, T.; Nitta, K. Hepatocyte Growth Factor–Secreting Mesothelial Cell Sheets Suppress Progressive Fibrosis in a Rat Model of CKD. J. Am. Soc. Nephrol. 2019, 30, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Flaquer, M.; Franquesa, M.; Vidal, A.; Bolaños, N.; Torras, J.; Lloberas, N.; Herrero-Fresneda, I.; Grinyó, J.M.; Cruzado, J.M. Hepatocyte growth factor gene therapy enhances infiltration of macrophages and may induce kidney repair in db/db mice as a model of diabetes. Diabetologia 2012, 55, 2059–2068. [Google Scholar] [CrossRef] [PubMed]
- Hirooka, Y.; Nozaki, Y. Interleukin-18 in Inflammatory Kidney Disease. Front. Med. 2021, 8, 639103. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H. , et al., The Delivery of the Recombinant Protein Cocktail Identified by Stem Cell-Derived Secretome Analysis Accelerates Kidney Repair After Renal Ischemia-Reperfusion Injury. Frontiers in Bioengineering and Biotechnology, 2022. 10.
- Dai, C.; Yang, J.; Liu, Y. Single Injection of Naked Plasmid Encoding Hepatocyte Growth Factor Prevents Cell Death and Ameliorates Acute Renal Failure in Mice. J. Am. Soc. Nephrol. 2002, 13, 411–422. [Google Scholar] [CrossRef]
- Mihajlovic, M.; Wever, K.E.; van der Made, T.K.; de Vries, R.B.; Hilbrands, L.B.; Masereeuw, R. Are cell-based therapies for kidney disease safe? A systematic review of preclinical evidence. Pharmacol. Ther. 2019, 197, 191–211. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y. , et al., Endogenous hepatocyte growth factor ameliorates chronic renal injury by activating matrix degradation pathways. Kidney Int, 2000. 58(5): p. 2028-43.
- Zhou, D.; Tan, R.J.; Fu, H.; Liu, Y. Wnt/β-catenin signaling in kidney injury and repair: a double-edged sword. Mod. Pathol. 2015, 96, 156–167. [Google Scholar] [CrossRef]
- A Brown, P.; Bodles-Brakhop, A.M.; A Pope, M.; Draghia-Akli, R. Gene therapy by electroporation for the treatment of chronic renal failure in companion animals. BMC Biotechnol. 2009, 9, 4–4. [Google Scholar] [CrossRef] [PubMed]
- Rieger, A.C.; Bagno, L.L.; Salerno, A.; Florea, V.; Rodriguez, J.; Rosado, M.; Turner, D.; Dulce, R.A.; Takeuchi, L.M.; Kanashiro-Takeuchi, R.M.; et al. Growth hormone-releasing hormone agonists ameliorate chronic kidney disease-induced heart failure with preserved ejection fraction. Proc. Natl. Acad. Sci. USA 2021, 118, e2019835118. [Google Scholar] [CrossRef]
- Wang, A.Y.; Peng, P.D.; Ehrhardt, A.; Storm, T.A.; Kay, M.A. Comparison of Adenoviral and Adeno-Associated Viral Vectors for Pancreatic Gene DeliveryIn Vivo. Hum. Gene Ther. 2004, 15, 405–413. [Google Scholar] [CrossRef]
- Haddad, G.; Kölling, M.; Wegmann, U.A.; Dettling, A.; Seeger, H.; Schmitt, R.; Soerensen-Zender, I.; Haller, H.; Kistler, A.D.; Dueck, A.; et al. Renal AAV2-Mediated Overexpression of Long Non-Coding RNA H19 Attenuates Ischemic Acute Kidney Injury Through Sponging of microRNA-30a-5p. J. Am. Soc. Nephrol. 2021, 32, 323–341. [Google Scholar] [CrossRef]
- Dong, X. , et al., The Long Noncoding RNA-H19 Mediates the Progression of Fibrosis from Acute Kidney Injury to Chronic Kidney Disease by Regulating the miR-196a/Wnt/β-Catenin Signaling. Nephron, 2022. 146(2): p. 209-219.
- Qin, Z.; Li, X.; Yang, J.; Cao, P.; Qin, C.; Xue, J.; Jia, R. VEGF and Ang-1 promotes endothelial progenitor cells homing in the rat model of renal ischemia and reperfusion injury. . 2017, 10, 11896–11908. [Google Scholar] [PubMed]
- Tanabe, K.; Maeshima, Y.; Sato, Y.; Wada, J. Antiangiogenic Therapy for Diabetic Nephropathy. BioMed Res. Int. 2017, 2017, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tao, Q.-R.; Chu, Y.-M.; Wei, L.; Tu, C.; Han, Y.-Y. Antiangiogenic therapy in diabetic nephropathy: A double-edged sword (Review). Mol. Med. Rep. 2021, 23, 1–1. [Google Scholar] [CrossRef]
- Torras, J. , et al., Gene therapy for acute renal failure. Contrib Nephrol, 2008. 159: p. 96-108.
- AlQahtani, A.D.; O’connor, D.; Domling, A.; Goda, S.K. Strategies for the production of long-acting therapeutics and efficient drug delivery for cancer treatment. Biomed. Pharmacother. 2019, 113, 108750. [Google Scholar] [CrossRef] [PubMed]
- Rubin, J.D.; Barry, M.A. Improving Molecular Therapy in the Kidney. Mol. Diagn. Ther. 2020, 24, 375–396. [Google Scholar] [CrossRef] [PubMed]
- Hunt, C.J. Cryopreservation of Human Stem Cells for Clinical Application: A Review. Transfus. Med. Hemotherapy 2011, 38, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Shakeel, A. and P.R. Corridon, Mitigating challenges and expanding the future of vascular tissue engineering—are we there yet? Frontiers in Physiology, 2023. 13.
- Wang, X.; Chan, V.; Corridon, P.R. Decellularized blood vessel development: Current state-of-the-art and future directions. Front. Bioeng. Biotechnol. 2022, 10, 951644. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Chan, V.; Corridon, P.R. Acellular Tissue-Engineered Vascular Grafts from Polymers: Methods, Achievements, Characterization, and Challenges. Polymers 2022, 14, 4825. [Google Scholar] [CrossRef] [PubMed]
- Geuens, T.; van Blitterswijk, C.A.; LaPointe, V.L.S. Overcoming kidney organoid challenges for regenerative medicine. npj Regen. Med. 2020, 5, 1–6. [Google Scholar] [CrossRef]
- Khoshdel-Rad, N.; Ahmadi, A.; Moghadasali, R. Kidney organoids: current knowledge and future directions. Cell Tissue Res. 2022, 387, 207–224. [Google Scholar] [CrossRef]
- Liu, M.; Cardilla, A.; Ngeow, J.; Gong, X.; Xia, Y. Studying Kidney Diseases Using Organoid Models. Front. Cell Dev. Biol. 2022, 10, 845401. [Google Scholar] [CrossRef] [PubMed]
- Papazova, D.A.; Oosterhuis, N.R.; Gremmels, H.; van Koppen, A.; Joles, J.A.; Verhaar, M.C. Cell-based therapies for experimental chronic kidney disease: a systematic review and meta-analysis. Dis. Model. Mech. 2015, 8, dmm.017699–293. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lin, Y.; Chen, X.; Liu, Y.; Zhou, T. Mesenchymal stem cells: A new therapeutic tool for chronic kidney disease. Front. Cell Dev. Biol. 2022, 10, 910592. [Google Scholar] [CrossRef] [PubMed]
- Eirin, A. and L.O. Lerman, Mesenchymal Stem/Stromal Cell–Derived Extracellular Vesicles for Chronic Kidney Disease: Are We There Yet? Hypertension, 2021. 78(2): p. 261-269.
- Wong, C.-Y. Current advances of stem cell-based therapy for kidney diseases. World J. Stem Cells 2021, 13, 914–933. [Google Scholar] [CrossRef] [PubMed]
- Missoum, A. Recent Updates on Mesenchymal Stem Cell Based Therapy for Acute Renal Failure. Curr. Urol. 2020, 13, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Kelly, K.J.; Kluve-Beckerman, B.; Zhang, J.; Dominguez, J.H. Intravenous cell therapy for acute renal failure with serum amyloid A protein-reprogrammed cells. Am. J. Physiol. Physiol. 2010, 299, F453–F464. [Google Scholar] [CrossRef] [PubMed]
- Fatehullah, A.; Tan, S.H.; Barker, N. Organoids as an in vitro model of human development and disease. Nat. Cell Biol. 2016, 18, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Little, M. Generating kidney tissue from pluripotent stem cells. Cell Death Discov. 2016, 2, 16053. [Google Scholar] [CrossRef] [PubMed]
- Morizane, R.; Lam, A.Q.; Freedman, B.S.; Kishi, S.; Valerius, M.T.; Bonventre, J.V. Nephron organoids derived from human pluripotent stem cells model kidney development and injury. Nat. Biotechnol. 2015, 33, 1193–1200. [Google Scholar] [CrossRef]
- Garreta, E.; Nauryzgaliyeva, Z.; Montserrat, N. Human induced pluripotent stem cell-derived kidney organoids toward clinical implementations. Curr. Opin. Biomed. Eng. 2021, 20, 100346. [Google Scholar] [CrossRef]
- Corridon, P.R. Intravital microscopy datasets examining key nephron segments of transplanted decellularized kidneys. Sci. Data 2022, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Pantic, I.V.; Shakeel, A.; Petroianu, G.A.; Corridon, P.R. Analysis of Vascular Architecture and Parenchymal Damage Generated by Reduced Blood Perfusion in Decellularized Porcine Kidneys Using a Gray Level Co-occurrence Matrix. Front. Cardiovasc. Med. 2022, 9, 797283. [Google Scholar] [CrossRef] [PubMed]
- Ciampi, O.; Bonandrini, B.; Derosas, M.; Conti, S.; Rizzo, P.; Benedetti, V.; Figliuzzi, M.; Remuzzi, A.; Benigni, A.; Remuzzi, G.; et al. Engineering the vasculature of decellularized rat kidney scaffolds using human induced pluripotent stem cell-derived endothelial cells. Sci. Rep. 2019, 9, 8001. [Google Scholar] [CrossRef] [PubMed]
- de Haan, M.J.A. , et al., Have we hit a wall with whole kidney decellularization and recellularization: A review. Current Opinion in Biomedical Engineering, 2021. 20: p. 100335.
- Corridon, P.R.; Ko, I.K.; Yoo, J.J.; Atala, A. Bioartificial Kidneys. Curr. Stem Cell Rep. 2017, 3, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Corridon, P.R. In vitro investigation of the impact of pulsatile blood flow on the vascular architecture of decellularized porcine kidneys. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Becerra, J.; Santos-Ruiz, L.; Andrades, J.A.; Marí-Beffa, M. The Stem Cell Niche Should be a Key Issue for Cell Therapy in Regenerative Medicine. Stem Cell Rev. Rep. 2010, 7, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Haworth, R.; Sharpe, M. The issue of immunology in stem cell therapies: a pharmaceutical perspective. Regen. Med. 2015, 10, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Jalil, R.A.; Neng, L.C.; Kofidis, T. Challenges in deriving and utilizing stem cell-derived endothelial cells for regenerative medicine: a key issue in clinical therapeutic applications. . 2011, 6, 93–9. [Google Scholar] [PubMed]
- Lepperdinger, G. , et al., Controversial issue: is it safe to employ mesenchymal stem cells in cell-based therapies? Exp Gerontol, 2008. 43(11): p. 1018-23.
- Lin, S.-Z. Era of Stem Cell Therapy for Regenerative Medicine and Cancers: An Introduction for the Special Issue of Pan Pacific Symposium on Stem Cells and Cancer Research. Cell Transplant. 2015, 24, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Sell, S. Adult Stem Cell Plasticity: Introduction to the First Issue of Stem Cell Reviews. Stem Cell Rev. Rep. 2005, 1, 001–008. [Google Scholar] [CrossRef]
- Wade, N. , An old question becomes new again: stem cell issue causes debate over the exact moment life begins. N Y Times Web, 2001: p. A20.
- Brown, M. NO ETHICAL BYPASS OF MORAL STATUS IN STEM CELL RESEARCH. Bioethics 2011, 27, 12–19. [Google Scholar] [CrossRef]
- Cohen, C.B.; Brandhorst, B.; Nagy, A.; Leader, A.; Dickens, B.; Isasi, R.M.; Evans, D.; Knoppers, B.M. The Use of Fresh Embryos in Stem Cell Research: Ethical and Policy Issues. Cell Stem Cell 2008, 2, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Cote, D.J.; Bredenoord, A.L.; Smith, T.R.; Ammirati, M.; Brennum, J.; Mendez, I.; Ammar, A.S.; Balak, N.; Bolles, G.; Esene, I.N.; et al. Ethical clinical translation of stem cell interventions for neurologic disease. Neurology 2017, 88, 322–328. [Google Scholar] [CrossRef]
- Habets, M.G.; van Delden, J.J.; Bredenoord, A.L. The inherent ethical challenge of first-in-human pluripotent stem cell trials. Regen. Med. 2014, 9, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Lo, B.; Parham, L. Ethical Issues in Stem Cell Research. Endocr. Rev. 2009, 30, 204–213. [Google Scholar] [CrossRef]
- Manzar, N.; Manzar, B.; Hussain, N.; Hussain, M.F.A.; Raza, S. The Ethical Dilemma of Embryonic Stem Cell Research. Sci. Eng. Ethic- 2011, 19, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Mauron, A.; E Jaconi, M. Stem Cell Science: Current Ethical and Policy Issues. Clin. Pharmacol. Ther. 2007, 82, 330–333. [Google Scholar] [CrossRef]
- Schuklenk, U. HOW NOT TO WIN AN ETHICAL ARGUMENT: EMBRYO STEM CELL RESEARCH REVISITED. Bioethics 2008, 22. [Google Scholar] [CrossRef]
- Suckiel, E. Human Embryonic Stem Cell Research: A Critical Survey of the Ethical Issues. Adv. Pediatr. 2008, 55, 79–96. [Google Scholar] [CrossRef]
- Cho, S.-J.; Kim, S.-Y.; Jeong, H.-C.; Cheong, H.; Kim, D.; Park, S.-J.; Choi, J.-J.; Kim, H.; Chung, H.-M.; Moon, S.-H.; et al. Repair of Ischemic Injury by Pluripotent Stem Cell Based Cell Therapy without Teratoma through Selective Photosensitivity. Stem Cell Rep. 2015, 5, 1067–1080. [Google Scholar] [CrossRef]
- Tang, C.; Weissman, I.L.; Drukker, M. The Safety of Embryonic Stem Cell Therapy Relies on Teratoma Removal. Oncotarget 2012, 3, 7–8. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W. Teratoma formation: A tool for monitoring pluripotency in stem cell research. StemBook 2014. [Google Scholar] [CrossRef]
- Angeles, A.D.L.; Ferrari, F.; Xi, R.; Fujiwara, Y.; Benvenisty, N.; Deng, H.; Hochedlinger, K.; Jaenisch, R.; Lee, S.; Leitch, H.G.; et al. Hallmarks of pluripotency. Nature 2015, 525, 469–478. [Google Scholar] [CrossRef]
- Dhawan, A.P.; D'Alessandro, B.; Fu, X. Optical Imaging Modalities for Biomedical Applications. IEEE Rev. Biomed. Eng. 2010, 3, 69–92. [Google Scholar] [CrossRef]
- Zakrzewski, W. , et al., Stem cells: past, present, and future. Stem Cell Research & Therapy, 2019. 10(1): p. 68.
- Ghasroldasht, M.M.; Seok, J.; Park, H.-S.; Ali, F.B.L.; Al-Hendy, A. Stem Cell Therapy: From Idea to Clinical Practice. Int. J. Mol. Sci. 2022, 23, 2850. [Google Scholar] [CrossRef]
- Lien, Y.-H.H.; Lai, L.-W. Renal Gene Transfer: Nonviral Approaches. Mol. Biotechnol. 2003, 24, 283–294. [Google Scholar] [CrossRef]
- Agrawal, N.; Dasaradhi, P.V.N.; Mohmmed, A.; Malhotra, P.; Bhatnagar, R.K.; Mukherjee, S.K. RNA Interference: Biology, Mechanism, and Applications. Microbiol. Mol. Biol. Rev. 2003, 67, 657–685. [Google Scholar] [CrossRef]
- Chen, X.; Mangala, L.S.; Rodriguez-Aguayo, C.; Kong, X.; Lopez-Berestein, G.; Sood, A.K. RNA interference-based therapy and its delivery systems. Cancer Metastasis Rev. 2017, 37, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Verfaillie, C.; Chmielewski, D.; Kren, S.; Eidman, K.; Connaire, J.; Heremans, Y.; Lund, T.; Blackstad, M.; Jiang, Y.; et al. Isolation and Characterization of Kidney-Derived Stem Cells. J. Am. Soc. Nephrol. 2006, 17, 3028–3040. [Google Scholar] [CrossRef]
- Sen, G.L.; Blau, H.M. A brief history of RNAi: the silence of the genes. FASEB J. 2006, 20, 1293–1299. [Google Scholar] [CrossRef]
- Bondue, T.; Heuvel, L.v.D.; Levtchenko, E.; Brock, R. The potential of RNA-based therapy for kidney diseases. Pediatr. Nephrol. 2022, 38, 327–344. [Google Scholar] [CrossRef] [PubMed]
- Kameda, S.; Maruyama, H.; Higuchi, N.; Iino, N.; Nakamura, G.; Miyazaki, J.; Gejyo, F. Kidney-targeted naked DNA transfer by retrograde injection into the renal vein in mice. Biochem. Biophys. Res. Commun. 2004, 314, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.K.W.; Chow, M.Y.T.; Zhang, Y.; Leung, S.W.S. siRNA Versus miRNA as Therapeutics for Gene Silencing. Mol. Ther. - Nucleic Acids 2015, 4, e252. [Google Scholar] [CrossRef] [PubMed]
- Thorling, C.A.; Dancik, Y.; Hupple, C.W.; Medley, G.; Liu, X.; Zvyagin, A.V.; Robertson, T.A.; Burczynski, F.J.; Roberts, M.S. Multiphoton microscopy and fluorescence lifetime imaging provide a novel method in studying drug distribution and metabolism in the rat liver in vivo. J. Biomed. Opt. 2011, 16, 086013. [Google Scholar] [CrossRef]
- Schena, F.P.; Serino, G.; Sallustio, F. MicroRNAs in kidney diseases: new promising biomarkers for diagnosis and monitoring. Nephrol. Dial. Transplant. 2013, 29, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Saal, S.; Harvey, S.J. MicroRNAs and the kidney: coming of age. Curr. Opin. Nephrol. Hypertens. 2009, 18, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Aslan, C.; Kiaie, S.H.; Zolbanin, N.M.; Lotfinejad, P.; Ramezani, R.; Kashanchi, F.; Jafari, R. Exosomes for mRNA delivery: a novel biotherapeutic strategy with hurdles and hope. BMC Biotechnol. 2021, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, Q.; Zhang, X.; Huang, H.; Tang, S.; Chai, Y.; Xu, Z.; Li, M.; Chen, X.; Liu, J.; et al. Recent advances in exosome-mediated nucleic acid delivery for cancer therapy. J. Nanobiotechnology 2022, 20, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, I.K.; Wood, M.J.A.; Fuhrmann, G. Extracellular vesicles as a next-generation drug delivery platform. Nat. Nanotechnol. 2021, 16, 748–759. [Google Scholar] [CrossRef]
- Lv, L.; Wu, W.; Feng, Y.; Li, Z.; Tang, T.; Liu, B. Therapeutic application of extracellular vesicles in kidney disease: promises and challenges. J. Cell. Mol. Med. 2017, 22, 728–737. [Google Scholar] [CrossRef]
- Xiang, H.; Zhang, C.; Xiong, J. Emerging role of extracellular vesicles in kidney diseases. Front. Pharmacol. 2022, 13, 985030. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, R.R.; Juncosa, E.M.; Masereeuw, R.; Lindoso, R.S. Extracellular Vesicles as a Therapeutic Tool for Kidney Disease: Current Advances and Perspectives. Int. J. Mol. Sci. 2021, 22, 5787. [Google Scholar] [CrossRef] [PubMed]
- Cantaluppi, V. , et al., Microvesicles derived from endothelial progenitor cells protect the kidney from ischemia-reperfusion injury by microRNA-dependent reprogramming of resident renal cells. Kidney Int, 2012. 82(4): p. 412-27.
- Yang, C.; Zhang, C.; Zhao, Z.; Zhu, T.; Yang, B. Fighting against kidney diseases with small interfering RNA: opportunities and challenges. J. Transl. Med. 2015, 13, 39. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.P.; Tadagavadi, R.K.; Ramesh, G.; Reeves, W.B. Mechanisms of Cisplatin Nephrotoxicity. Toxins 2010, 2, 2490–2518. [Google Scholar] [CrossRef] [PubMed]
- Pabla, N.; Dong, Z. Cisplatin nephrotoxicity: Mechanisms and renoprotective strategies. Kidney Int. 2008, 73, 994–1007. [Google Scholar] [CrossRef] [PubMed]
- Peres, L.A.B.; Júnior, A.D.d.C. Acute nephrotoxicity of cisplatin: Molecular mechanisms. Braz. J. Nephrol. 2013, 35, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Bosch, B.; Grigorov, B.; Senserrich, J.; Clotet, B.; Darlix, J.-L.; Muriaux, D.; Este, J.A. A clathrin–dynamin-dependent endocytic pathway for the uptake of HIV-1 by direct T cell–T cell transmission. Antivir. Res. 2008, 80, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Marina-García, N.; Franchi, L.; Kim, Y.-G.; Hu, Y.; Smith, D.E.; Boons, G.-J.; Núñez, G. Clathrin- and Dynamin-Dependent Endocytic Pathway Regulates Muramyl Dipeptide Internalization and NOD2 Activation. J. Immunol. 2009, 182, 4321–4327. [Google Scholar] [CrossRef] [PubMed]
- Wiejak, J.; Surmacz, L.; Wyroba, E. Dynamin- and clathrin-dependent endocytic pathway in unicellular eukaryoteParamecium. Biochem. Cell Biol. 2004, 82, 547–558. [Google Scholar] [CrossRef]
- McFarland, M.J.; Bardell, T.K.; Yates, M.L.; Placzek, E.A.; Barker, E.L. RNA Interference-Mediated Knockdown of Dynamin 2 Reduces Endocannabinoid Uptake into Neuronal dCAD Cells. Mol. Pharmacol. 2008, 74, 101–108. [Google Scholar] [CrossRef]
- Hall, A.M.; Rhodes, G.J.; Sandoval, R.M.; Corridon, P.R.; Molitoris, B.A. In vivo multiphoton imaging of mitochondrial structure and function during acute kidney injury. Kidney Int. 2013, 83, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Mahadevappa, R.; Nielsen, R.; Christensen, E.I.; Birn, H. Megalin in acute kidney injury: foe and friend. Am. J. Physiol. Physiol. 2014, 306, F147–F154. [Google Scholar] [CrossRef] [PubMed]
- Nagai, J.; Saito, M.; Adachi, Y.; Yumoto, R.; Takano, M. Inhibition of gentamicin binding to rat renal brush-border membrane by megalin ligands and basic peptides. J. Control. Release 2006, 112, 43–50. [Google Scholar] [CrossRef]
- Stokman, G.; Qin, Y.; Rácz, Z.; Hamar, P.; Price, L.S. Application of siRNA in targeting protein expression in kidney disease. Adv. Drug Deliv. Rev. 2010, 62, 1378–1389. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Du, C.; Yan, L.; Wei, J.; Wu, H.; Shi, Y.; Duan, H. CTGF siRNA ameliorates tubular cell apoptosis and tubulointerstitial fibrosis in obstructed mouse kidneys in a Sirt1-independent manner. Drug Des. Dev. Ther. 2015, ume 9, 4155–4171. [Google Scholar] [CrossRef]
- Thompson, J.D.; Kornbrust, D.J.; Foy, J.W.-D.; Solano, E.C.; Schneider, D.J.; Feinstein, E.; Molitoris, B.A.; Erlich, S. Toxicological and Pharmacokinetic Properties of Chemically Modified siRNAs Targeting p53 RNA Following Intravenous Administration. Nucleic Acid Ther. 2012, 22, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Imamura, R.; Isaka, Y.; Sandoval, R.M.; Ori, A.; Adamsky, S.; Feinstein, E.; Molitoris, B.A.; Takahara, S. Intravital Two-Photon Microscopy Assessment of Renal Protection Efficacy of siRNA for p53 in Experimental Rat Kidney Transplantation Models. Cell Transplant. 2010, 19, 1659–1670. [Google Scholar] [CrossRef] [PubMed]
- Molitoris, B.A.; Dagher, P.C.; Sandoval, R.M.; Campos, S.B.; Ashush, H.; Fridman, E.; Brafman, A.; Faerman, A.; Atkinson, S.J.; Thompson, J.D.; et al. siRNA Targeted to p53 Attenuates Ischemic and Cisplatin-Induced Acute Kidney Injury. J. Am. Soc. Nephrol. 2009, 20, 1754–1764. [Google Scholar] [CrossRef] [PubMed]
- Bouillet, P.; Robati, M.; Bath, M.; Strasser, A. Polycystic kidney disease prevented by transgenic RNA interference. Cell Death Differ. 2005, 12, 831–833. [Google Scholar] [CrossRef]
- Corridon, P.; Rhodes, G.J.; Leonard, E.C.; Basile, D.; Ii, V.H.G.; Bacallao, R.L.; Atkinson, S.J. A method to facilitate and monitor expression of exogenous genes in the rat kidney using plasmid and viral vectors. Am. J. Physiol. Physiol. 2013, 304, F1217–F1229. [Google Scholar] [CrossRef]
- Duvshani-Eshet, M., T. Haber, and M. Machluf, Insight concerning the mechanism of therapeutic ultrasound facilitating gene delivery: increasing cell membrane permeability or interfering with intracellular pathways? Hum Gene Ther, 2014. 25(2): p. 156-64.
- Felgner, J.; Kumar, R.; Sridhar, C.; Wheeler, C.; Tsai, Y.; Border, R.; Ramsey, P.; Martin, M.; Felgner, P. Enhanced gene delivery and mechanism studies with a novel series of cationic lipid formulations. J. Biol. Chem. 1994, 269, 2550–2561. [Google Scholar] [CrossRef] [PubMed]
- Grandinetti, G., A. E. Smith, and T.M. Reineke, Membrane and Nuclear Permeabilization by Polymeric pDNA Vehicles: Efficient Method for Gene Delivery or Mechanism of Cytotoxicity? Molecular Pharmaceutics, 2012. 9(3): p. 523-538.
- Wickham, T. A Novel Approach and a Novel Mechanism for Stealthing Gene Delivery Vehicles. Mol. Ther. 2000, 2, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.; Park, F. Gene therapy research for kidney diseases. Physiol. Genom. 2019, 51, 449–461. [Google Scholar] [CrossRef] [PubMed]
- Ang, D.; Nguyen, Q.; Kayal, S.; Preiser, P.; Rawat, R.; Ramanujan, R. Insights into the mechanism of magnetic particle assisted gene delivery. Acta Biomater. 2011, 7, 1319–1326. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.S.; Kim, H.H.; Yang, J.M.; Shin, S. An insight into the gene delivery mechanism of the arginine peptide system: Role of the peptide/DNA complex size. Biochim. et Biophys. Acta (BBA) - Gen. Subj. 2006, 1760, 1604–1612. [Google Scholar] [CrossRef]
- Elnaggar, R.; Hanawa, H.; Liu, H.; Yoshida, T.; Hayashi, M.; Watanabe, R.; Abe, S.; Toba, K.; Yoshida, K.; Chang, H.; et al. The effect of hydrodynamics-based delivery of an IL-13-Ig fusion gene for experimental autoimmune myocarditis in rats and its possible mechanism. Eur. J. Immunol. 2005, 35, 1995–2005. [Google Scholar] [CrossRef] [PubMed]
- Liu, H. , et al., Effect of hydrodynamics-based gene delivery of plasmid DNA encoding interleukin-1 receptor antagonist-Ig for treatment of rat autoimmune myocarditis: possible mechanism for lymphocytes and noncardiac cells. Circulation, 2005. 111(13): p. 1593-600.
- McKay, T.; Reynolds, P.; Jezzard, S.; Curiel, D.; Coutelle, C. Secretin-Mediated Gene Delivery, a Specific Targeting Mechanism with Potential for Treatment of Biliary and Pancreatic Disease in Cystic Fibrosis. Mol. Ther. 2002, 5, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Simeoni, F. Insight into the mechanism of the peptide-based gene delivery system MPG: implications for delivery of siRNA into mammalian cells. Nucleic Acids Res. 2003, 31, 2717–2724. [Google Scholar] [CrossRef] [PubMed]
- Corridon, P.R.; Karam, S.H.; Khraibi, A.A.; Khan, A.A.; Alhashmi, M.A. Intravital imaging of real-time endogenous actin dysregulation in proximal and distal tubules at the onset of severe ischemia-reperfusion injury. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Filipowicz, W. RNAi: The Nuts and Bolts of the RISC Machine. Cell 2005, 122, 17–20. [Google Scholar] [CrossRef]
- Pratt, A.J.; MacRae, I.J. The RNA-induced Silencing Complex: A Versatile Gene-silencing Machine. J. Biol. Chem. 2009, 284, 17897–17901. [Google Scholar] [CrossRef]
- Zhang, X.; Edwards, J.P.; Mosser, D.M. The Expression of Exogenous Genes in Macrophages: Obstacles and Opportunities; Humana Press: 2009; Volume 531, pp. 123–143. [CrossRef]
- Arrighi, N. , 3 - Stem Cells at the Core of Cell Therapy, in Stem Cells, N. Arrighi, Editor. 2018, Elsevier. p. 73-100.
- Crystal, R.G. Adenovirus: The First EffectiveIn VivoGene Delivery Vector. Hum. Gene Ther. 2014, 25, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Manfredsson, F.P., A. S. Lewin, and R.J. Mandel, RNA knockdown as a potential therapeutic strategy in Parkinson's disease. Gene Therapy, 2006. 13(6): p. 517-524.
- Katz, M.G.; Fargnoli, A.S.; Williams, R.D.; Bridges, C.R. Gene Therapy Delivery Systems for Enhancing Viral and Nonviral Vectors for Cardiac Diseases: Current Concepts and Future Applications. Hum. Gene Ther. 2013, 24, 914–927. [Google Scholar] [CrossRef] [PubMed]
- Nayerossadat, N.; Maedeh, T.; Ali, P. Viral and nonviral delivery systems for gene delivery. Adv. Biomed. Res. 2012, 1, 27. [Google Scholar] [CrossRef]
- Kamimura, K.; Suda, T.; Zhang, G.; Liu, D. Advances in Gene Delivery Systems. Pharm. Med. 2011, 25, 293–306. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Saini, M.; Bisht, D.; Rana, M.; Bachan, R.; Gogoi, S.M.; Buragohain, B.M.; Barman, N.N.; Gupta, P.K. Lentiviral-mediated delivery of classical swine fever virus Erns gene into porcine kidney-15 cells for production of recombinant ELISA diagnostic antigen. Mol. Biol. Rep. 2019, 46, 3865–3876. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Ren, Y.; Wang, X.; Lazar, L.; Ma, S.; Weng, G.; Zhao, J. Application of Ultrasound-Targeted Microbubble Destruction–Mediated Exogenous Gene Transfer in Treating Various Renal Diseases. Hum. Gene Ther. 2019, 30, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Kolb, A.L.; Corridon, P.R.; Zhang, S.; Xu, W.; Witzmann, F.A.; Collett, J.A.; Rhodes, G.J.; Winfree, S.; Bready, D.; Pfeffenberger, Z.J.; et al. Exogenous Gene Transmission of Isocitrate Dehydrogenase 2 Mimics Ischemic Preconditioning Protection. J. Am. Soc. Nephrol. 2018, 29, 1154–1164. [Google Scholar] [CrossRef]
- Nakamura, A. , et al., Adenoviral delivery of the beta2-adrenoceptor gene in sepsis: a subcutaneous approach in rat for kidney protection. Clin Sci (Lond), 2005. 109(6): p. 503-11.
- Verkman, A.S.; Yang, B. Aquaporin gene delivery to kidney. Kidney Int. 2002, 61, S120–S124. [Google Scholar] [CrossRef]
- Imai, E.; Isaka, Y. Strategies of gene transfer to the kidney. Kidney Int. 1998, 53, 264–272. [Google Scholar] [CrossRef]
- Boletta, A.; Benigni, A.; Lutz, J.; Remuzzi, G.; Soria, M.R.; Monaco, L. Nonviral Gene Delivery to the Rat Kidney with Polyethylenimine. Hum. Gene Ther. 1997, 8, 1243–1251. [Google Scholar] [CrossRef] [PubMed]
- Kapturczak, M.H.; Chen, S.; Agarwal, A. Adeno-associated virus vector-mediated gene delivery to the vasculature and kidney. Acta Biochim. Pol. 2005, 52, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Gordillo, D.; Trujillo-Provencio, C.; Knight, V.B.; Serrano, E.E. Optimization of gene delivery methods in Xenopus laevis kidney (A6) and Chinese hamster ovary (CHO) cell lines for heterologous expression of Xenopus inner ear genes. Vitr. Cell. Dev. Biol. - Anim. 2011, 47, 640–652. [Google Scholar] [CrossRef] [PubMed]
- Tanner, G.A.; Sandoval, R.M.; Molitoris, B.A.; Bamburg, J.R.; Ashworth, S.L. Micropuncture gene delivery and intravital two-photon visualization of protein expression in rat kidney. Am. J. Physiol. Physiol. 2005, 289, F638–F643. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cui, H.; Li, K.; Sun, C.; Du, W.; Cui, J.; Zhao, X.; Chen, W. A Magnetic Nanoparticle-Based Multiple-Gene Delivery System for Transfection of Porcine Kidney Cells. PLOS ONE 2014, 9, e102886. [Google Scholar] [CrossRef] [PubMed]
- Xing, Y.; Pua, E.C.; Lu, X.; Zhong, P. Low-amplitude ultrasound enhances hydrodynamic-based gene delivery to rat kidney. Biochem. Biophys. Res. Commun. 2009, 386, 217–222. [Google Scholar] [CrossRef]
- Zhu, G. , et al., Adenovirus-mediated beta-galactosidase gene delivery to the liver leads to protein deposition in kidney glomeruli. Kidney Int, 1997. 52(4): p. 992-9.
- Friedmann, T. A New Serious Adverse Event in a Gene Therapy Study. Mol. Ther. 2007, 15, 1899–1900. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, G.A.R. and R.M.A. Paiva, Gene therapy: advances, challenges and perspectives. Einstein (Sao Paulo), 2017. 15(3): p. 369-375.
- Tremblay, J.P.; Annoni, A.; Suzuki, M. Three Decades of Clinical Gene Therapy: From Experimental Technologies to Viable Treatments. Mol. Ther. 2021, 29, 411–412. [Google Scholar] [CrossRef] [PubMed]
- Goswami, R.; Subramanian, G.; Silayeva, L.; Newkirk, I.; Doctor, D.; Chawla, K.; Chattopadhyay, S.; Chandra, D.; Chilukuri, N.; Betapudi, V. Gene Therapy Leaves a Vicious Cycle. Front. Oncol. 2019, 9, 297. [Google Scholar] [CrossRef]
- Cai, N.; Lai, A.C.-K.; Liao, K.; Corridon, P.R.; Graves, D.J.; Chan, V. Recent Advances in Fluorescence Recovery after Photobleaching for Decoupling Transport and Kinetics of Biomacromolecules in Cellular Physiology. Polymers 2022, 14, 1913. [Google Scholar] [CrossRef]
- Shaya, J.; Corridon, P.R.; Al-Omari, B.; Aoudi, A.; Shunnar, A.; Mohideen, M.I.H.; Qurashi, A.; Michel, B.Y.; Burger, A. Design, photophysical properties, and applications of fluorene-based fluorophores in two-photon fluorescence bioimaging: A review. J. Photochem. Photobiol. C: Photochem. Rev. 2022, 52. [Google Scholar] [CrossRef]
- Hickson, L.J.; Eirin, A.; Lerman, L.O. Challenges and opportunities for stem cell therapy in patients with chronic kidney disease. Kidney Int. 2016, 89, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.A.S.; Leonard, J.P.; Flasshove, M.; Bertino, J.; Gallardo, H.; Sadelain, M. Gene therapy - the challenge for the future. Ann. Oncol. 1996, 7, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Oshimura, M.; Kazuki, Y.; Uno, N. [Challenge toward gene-therapy using iPS cells for Duchenne muscular dystrophy]. Rinsho Shinkeigaku 2012, 52, 1139–1142. [Google Scholar] [CrossRef] [PubMed]
- Sousa, F.; Passarinha, L.; Queiroz, J. Biomedical application of plasmid DNA in gene therapy: A new challenge for chromatography. Biotechnol. Genet. Eng. Rev. 2009, 26, 83–116. [Google Scholar] [CrossRef]
- Stokman, M.F.; Renkema, K.Y.; Giles, R.H.; Schaefer, F.; Knoers, N.V.; van Eerde, A.M. The expanding phenotypic spectra of kidney diseases: insights from genetic studies. Nat. Rev. Nephrol. 2016, 12, 472–483. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Chen, B.K.; Mosoian, A.; Hays, T.; Ross, M.J.; Klotman, P.E.; Klotman, M.E. Virological Synapses Allow HIV-1 Uptake and Gene Expression in Renal Tubular Epithelial Cells. J. Am. Soc. Nephrol. 2011, 22, 496–507. [Google Scholar] [CrossRef] [PubMed]
- Gusella, G.L.; Fedorova, E.; Marras, D.; Klotman, P.E.; Klotman, M.E. In vivo gene transfer to kidney by lentiviral vector. Kidney Int. 2002, 61, S32–S36. [Google Scholar] [CrossRef] [PubMed]
- Deen, W.M. , What determines glomerular capillary permeability? J Clin Invest, 2004. 114(10): p. 1412-4.
- Deen, W.M.; Lazzara, M.J.; Myers, B.D.; Navar, L.G.; Richfield, O.; Kasztan, M.; Piwkowska, A.; Kreft, E.; Rogacka, D.; Audzeyenka, I.; et al. Structural determinants of glomerular permeability. Am. J. Physiol. Physiol. 2001, 281, F579–F596. [Google Scholar] [CrossRef]
- Drumond, M.C.; Deen, W.M. Structural determinants of glomerular hydraulic permeability. Am. J. Physiol. Physiol. 1994, 266, F1–F12. [Google Scholar] [CrossRef]
- Ishida, R.; Kami, D.; Kusaba, T.; Kirita, Y.; Kishida, T.; Mazda, O.; Adachi, T.; Gojo, S. Kidney-specific Sonoporation-mediated Gene Transfer. Mol. Ther. 2016, 24, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Gao, Y.; Zhang, J.; Liu, Z.; Tan, K.; Hua, X.; Gong, J. Renal interstitial permeability changes induced by microbubble-enhanced diagnostic ultrasound. J. Drug Target. 2013, 21, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Reiser, J.; Gupta, V.; Kistler, A.D. Toward the development of podocyte-specific drugs. Kidney Int. 2010, 77, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Appledorn, D.M., S. Seregin, and A. Amalfitano, Adenovirus vectors for renal-targeted gene delivery. Contrib Nephrol, 2008. 159: p. 47-62.
- Ye, X.; Jerebtsova, M.; Liu, X.-H.; Li, Z.; Ray, P.E. Adenovirus-mediated gene transfer to renal glomeruli in rodents. Kidney Int. 2002, 61, S16–S23. [Google Scholar] [CrossRef]
- Ye, X.; Liu, X.-H.; Li, Z.; Ray, P.E. Efficient Gene Transfer to Rat Renal Glomeruli with Recombinant Adenoviral Vectors. Hum. Gene Ther. 2001, 12, 141–148. [Google Scholar] [CrossRef]
- Imai, E. Gene therapy approach in renal disease in the 21st century. Nephrol. Dial. Transplant. 2001, 16, 26–34. [Google Scholar] [CrossRef]
- Moullier, P.; Friedlander, G.; Calise, D.; Ronco, P.; Perricaudet, M.; Ferry, N. Adenoviral-mediated gene transfer to renal tubular cells in vivo. Kidney Int. 1994, 45, 1220–1225. [Google Scholar] [CrossRef]
- Brunetti-Pierri, N.; E Stapleton, G.; Palmer, D.J.; Zuo, Y.; Mane, V.P.; Finegold, M.J.; Beaudet, A.L.; Leland, M.M.; E Mullins, C.; Ng, P. Pseudo-hydrodynamic Delivery of Helper-dependent Adenoviral Vectors into Non-human Primates for Liver-directed Gene Therapy. Mol. Ther. 2007, 15, 732–740. [Google Scholar] [CrossRef]
- Ashworth, S.; Sandoval, R.; Tanner, G.; Molitoris, B. Two-photon microscopy: Visualization of kidney dynamics. Kidney Int. 2007, 72, 416–421. [Google Scholar] [CrossRef]
- Suda, T.; Liu, D. Hydrodynamic Gene Delivery: Its Principles and Applications. Mol. Ther. 2007, 15, 2063–2069. [Google Scholar] [CrossRef]
- Collett, J.A.; Corridon, P.R.; Mehrotra, P.; Kolb, A.L.; Rhodes, G.J.; Miller, C.A.; Molitoris, B.A.; Pennington, J.G.; Sandoval, R.M.; Atkinson, S.J.; et al. Hydrodynamic Isotonic Fluid Delivery Ameliorates Moderate-to-Severe Ischemia-Reperfusion Injury in Rat Kidneys. J. Am. Soc. Nephrol. 2017, 28, 2081–2092. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Gao, X.; Song, Y.K.; Vollmer, R.; Stolz, D.B.; Gasiorowski, J.Z.; A Dean, D.; Liu, D. Hydroporation as the mechanism of hydrodynamic delivery. Gene Ther. 2004, 11, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Oyama, N.; Kawaguchi, M.; Itaka, K.; Kawakami, S. Efficient Messenger RNA Delivery to the Kidney Using Renal Pelvis Injection in Mice. Pharmaceutics 2021, 13, 1810. [Google Scholar] [CrossRef]
- Corridon, P.; Rhodes, G.; Zhang, S.; Bready, D.; Xu, W.; Witzmann, F.; Atkinson, S.; Basile, D.; Bacallao, R. Hydrodynamic delivery of mitochondrial genes in vivo protects against moderate ischemia-reperfusion injury in the rat kidney (690.17). FASEB J. 2014, 28, 690.17. [Google Scholar] [CrossRef]
- Woodard, L.E.; Cheng, J.; Welch, R.C.; Williams, F.M.; Luo, W.; Gewin, L.S.; Wilson, M.H. Kidney-specific transposon-mediated gene transfer in vivo. Sci. Rep. 2017, 7, srep44904. [Google Scholar] [CrossRef]
- Imai, E. Gene therapy for the treatment of renal disease: prospects for the future. Curr. Opin. Nephrol. Hypertens. 1997, 6, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Bonamassa, B.; Hai, L.; Liu, D. Hydrodynamic Gene Delivery and Its Applications in Pharmaceutical Research. Pharm. Res. 2010, 28, 694–701. [Google Scholar] [CrossRef]
- Rocca, C.J.; Ur, S.N.; Harrison, F.; Cherqui, S. rAAV9 combined with renal vein injection is optimal for kidney-targeted gene delivery: conclusion of a comparative study. Gene Ther. 2014, 21, 618–628. [Google Scholar] [CrossRef]
- Zincarelli, C.; Soltys, S.; Rengo, G.; E Rabinowitz, J. Analysis of AAV Serotypes 1–9 Mediated Gene Expression and Tropism in Mice After Systemic Injection. Mol. Ther. 2008, 16, 1073–1080. [Google Scholar] [CrossRef]
- Yao, J.; Fan, Y.; Li, Y.; Huang, L. Strategies on the nuclear-targeted delivery of genes. J. Drug Target. 2013, 21, 926–39. [Google Scholar] [CrossRef]
- Lovett, S.T. The DNA Exonucleases of Escherichia coli. EcoSal Plus 2011, 4. [Google Scholar] [CrossRef]
- Dermić, D. , Functions of multiple exonucleases are essential for cell viability, DNA repair and homologous recombination in recD mutants of Escherichia coli. Genetics, 2006. 172(4): p. 2057-69.
- Villalba, M.; Ferrari, D.; Bozza, A.; Del Senno, L.; Di Virgilio, F. Ionic regulation of endonuclease activity in PC12 cells. Biochem. J. 1995, 311, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- A Schwartz, D.; Quinn, T.J.; Thorne, P.S.; Sayeed, S.; Yi, A.K.; Krieg, A.M. CpG motifs in bacterial DNA cause inflammation in the lower respiratory tract. J. Clin. Investig. 1997, 100, 68–73. [Google Scholar] [CrossRef]
- Frazier, K.S. , Antisense oligonucleotide therapies: the promise and the challenges from a toxicologic pathologist's perspective. Toxicol Pathol, 2015. 43(1): p. 78-89.
- Tenenbaum, L.; Lehtonen, E.; Monahan, P.E. Evaluation of Risks Related to the Use of Adeno-Associated Virus-Based Vectors. Curr. Gene Ther. 2003, 3, 545–565. [Google Scholar] [CrossRef]
- Thomas, C.E.; Ehrhardt, A.; Kay, M.A. Progress and problems with the use of viral vectors for gene therapy. Nat. Rev. Genet. 2003, 4, 346–358. [Google Scholar] [CrossRef] [PubMed]
- Maggio, I.; Holkers, M.; Liu, J.; Janssen, J.M.; Chen, X.; Gonçalves, M.A.F.V. Adenoviral vector delivery of RNA-guided CRISPR/Cas9 nuclease complexes induces targeted mutagenesis in a diverse array of human cells. Sci. Rep. 2014, 4, 5105. [Google Scholar] [CrossRef]
- Uren, A.G.; Kool, J.; Berns, A.; van Lohuizen, M. Retroviral insertional mutagenesis: past, present and future. Oncogene 2005, 24, 7656–7672. [Google Scholar] [CrossRef]
- Li, T.; Zhou, Z.-W.; Ju, Z.; Wang, Z.-Q. DNA Damage Response in Hematopoietic Stem Cell Ageing. Genom. Proteom. Bioinform. 2016, 14, 147–154. [Google Scholar] [CrossRef]
Figure 1.
A schematic overview of the renal gene- and cell-based approaches highlights vectorization, delivery mode, and pathways supporting transgene incorporation and expression.
Figure 1.
A schematic overview of the renal gene- and cell-based approaches highlights vectorization, delivery mode, and pathways supporting transgene incorporation and expression.
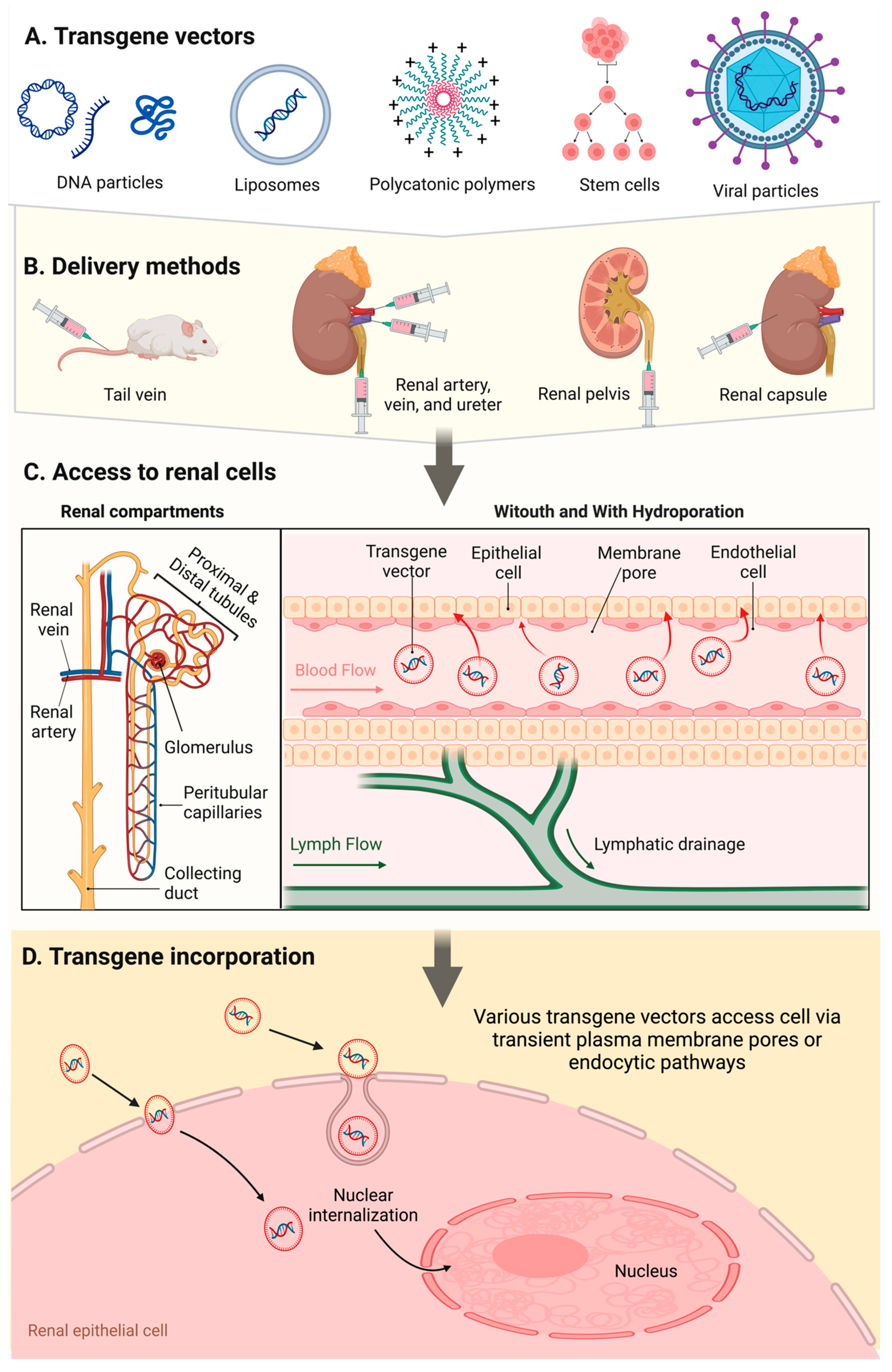

Table 1.
An overview of delivery methods and associated vectors.
| Infusion Site |
Infusion Method |
Infusion Compound |
Auxiliary Gene Enhancer |
|---|---|---|---|
| Tail vein | Systemic injection (normal volume and pressure) |
Plasmid and viral vectors, cells | None reported |
| Renal artery, renal vein, renal pelvis, ureter | Low pressure injections Hydrodynamic injections |
DNA particles, liposomes, polycations, stem cells and viral vectors |
Electroporation, microbubble cavitation, ultrasound cavitation, ultrasound and microbubble coupled cavitation |
| Renal capsule | Micropuncture and blunt needle injections | Viral vectors | None reported |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



