Submitted:
14 January 2023
Posted:
25 January 2023
You are already at the latest version
Abstract
Introduction People are presenting with chronic musculoskeletal pain at a younger age, and many fulfil criteria for fibromyalgia. We have recently shown a strong association between fibromyalgia symptoms and autistic traits in a self-selected community population, with the relationship mediated in part by the presence of hypermobility. Many respondents also described food sensitivities and intolerances. This study explores relationships between food issues and fibromyalgia symptoms in this population Methods The study used a nonexperimental, correlational design with data collected from a volunteer sample of 442 adults (aged 18-60) who completed online self-report questionnaires assessing each of fibromyalgia symptoms (ACR criteria), autistic traits (RAADS score) and hypermobility (Beighton’s test). Subjects were also asked to record any food sensitivities, allergies, or intolerances, along with their consequences. Correlation analyses and linear regressions were used to test the relationships between these features and each of fibromyalgia, autistic traits and hypermobility. Data was analysed using parametric and non-parametric techniques to assess the strength and significance of relationships, causes of variance and the potential mediating effect of food-related symptoms in the correlation between fibromyalgia features and autistic traits Results Our self-selected community population had a mean age of 24 years and was 77% female. The prevalence of fibromyalgia, autistic traits and hypermobility was 40%, 65% and 44% respectively. Half of all subjects reported food sensitivity and 31% reported food intolerance. The incidence of food-related symptoms was higher among subjects who met criteria for fibromyalgia than those who reported autistic traits or hypermobility. Food sensitivity and food intolerance were both more significantly associated with fibromyalgia (r=0.24, p>0.001 and r=0.38, p>0.001) than with autistic traits (r=0.15, p>0.01 and r=0.17, p>0.01). Discussion This is the first community study to provide evidence for a direct association between features of fibromyalgia and reported food intolerance and sensitivity. Although self-selected, the findings in our predominantly young population suggest that gluten and lactose consumption may be associated with higher levels of musculoskeletal pain. Avoidance of these foodstuffs was commonly reported to reduce symptoms. Dietary adjustment may merit further investigation as a therapeutic modality for some patients with fibromyalgia.
Keywords:
FIBROMYALGIA
; FOOD INTOLERANCE
; FOOD SENSITIVITY
; AUTISM
; HYPERMOBILITY
Introduction
People are presenting with chronic musculoskeletal pain at a younger age, and many fulfil criteria for fibromyalgia. We have recently shown a strong association between fibromyalgia symptoms and autistic traits in a self-selected community population, with the relationship mediated in part by the presence of hypermobility. Many respondents also described food sensitivities and intolerances. This study explores the relationships between food issues and fibromyalgia symptoms in this population.
Methods
The study used a nonexperimental, correlational design with data collected from a volunteer sample of 442 adults (aged 18-60) who completed online self-report questionnaires assessing each of fibromyalgia symptoms (ACR criteria), autistic traits (RAADS score) and hypermobility (Beighton’s test). Subjects were also asked to record any food sensitivities, allergies, or intolerances, along with their consequences. Correlation analyses and linear regressions were used to test the relationships between these features and each of fibromyalgia, autistic traits and hypermobility. Data was analysed using parametric and non-parametric techniques to assess the strength and significance of relationships, and the potential mediating effect of food-related symptoms in the correlation between fibromyalgia features and autistic traits.
Results
Our self-selected community population had a mean age of 24 years and was 77% female. The prevalence of fibromyalgia, autistic traits and hypermobility was 40%, 65% and 44% respectively. Half of all subjects reported food sensitivity and 31% reported food intolerance. The incidence of food-related symptoms was higher among subjects who met criteria for fibromyalgia than those who reported autistic traits or hypermobility. Food sensitivity and food intolerance were both more significantly associated with fibromyalgia (r=0.24, p>0.001 and r=0.38, p>0.001) than with autistic traits (r=0.15, p>0.01 and r=0.17, p>0.01).
Discussion
This is the first community study to provide evidence for a direct association between features of fibromyalgia and reported food intolerance and sensitivity. Although self-selected, the findings in our predominantly young population suggest that gluten and lactose consumption may be associated with higher levels of musculoskeletal pain. The study population commonly reported that avoidance of gluten and / or lactose containing foods reduced symptoms. Dietary adjustment may merit further investigation as a therapeutic modality for some patients with fibromyalgia.
INTRODUCTION
Chronic widespread musculoskeletal (MSK) pain lasting over 3 months is the hallmark of fibromyalgia [1]. The prevalence of fibromyalgia approaches 5% in the UK population [2] and is highest among young and middle-aged women [3]. Fatigue and cognitive dysfunction (brain-fog) are essential components of the symptom complex [4]. Many sufferers report a variety of psychological complaints [5], and strong associations with migraine [6] and gastrointestinal upset are well-described. Irritable bowel syndrome is co-morbid in up to 50% of fibromyalgia sufferers [7].
Speculation about a link between fibromyalgia and gluten sensitivity arose over a decade ago, and reports of remission of musculoskeletal pain with the adoption of a gluten free diet [8] led to a formal comparison of this approach with a low-calorie diet [9]. Other foods were also recorded as triggering or worsening symptoms of fibromyalgia [10], so a diet low in fermentable sugars was developed (FODMAP) with subsequent evidence that it also improved symptoms [11]. A subsequent systematic review showed that the modest benefits attained in these studies were largely confined to those with some objective evidence of gluten sensitivity in the form of lymphoid enteritis on duodenal biopsy, so recommendations for a widespread adoption of a gluten-free diet were not made [12].
The prevalence of gastrointestinal issues among young neurodivergent people is also high [13], with food sensitivity and intolerance both well described [14]. Again, gluten sensitivity has been reportedly associated with triggering of autistic symptoms, while a gluten free diet (GFD) has been described as improving these in selected cases [15]. However, there is limited evidence for the role of exclusion diets in the treatment of autism [16], and a systematic review concluded there was insufficient evidence to recommend adoption of this approach more widely [17]. Indeed, there is evidence that highly selective eating can contribute towards both physical and psychological damage [18], as the prevalence of eating disorders such as binge eating, and avoidant restrictive food intake disorders (ARFID) are both elevated in autistic females and may contribute significantly to the increased morbidity and mortality associated with these conditions [19].
Several studies have confirmed that a significant percentage of patients with fibromyalgia also have a neurodivergent condition. A South African study showed that fibromyalgia was comorbid with attention deficit hyperactivity disorder (ADHD) in almost half of cases [20] while a study from Argentina reported ADHD in 73% of patients with fibromyalgia, along with a high prevalence of narcissism [21]. Similar associations were reported in Italy [22] and Turkey [23,24], with the latter studies also suggesting that ADHD was associated with more severe symptoms of fibromyalgia. Dopamine deficiency has been suggested as a common mechanism for both conditions and a trial of dopamine agonist therapy was reported to reduce symptoms of each condition significantly [25].
Studies also confirm a higher prevalence of fibromyalgia and hypermobility among autistic females than in autistic males [26,27,28,29,30], with one estimate suggesting over three quarters of female autistic females develop MSK pain [31]. A risk ratio of 4.5 for hypermobility was reported in neurodivergent females [32], and it was proposed that hypermobility might mediate the relationship between fibromyalgia and neurodivergence [33]. In support of this, the risk ratios for ASD and ADHD are 7.4 and 6.0 respectively among hypermobile people [33]. Gastrointestinal disorders are also highly prevalent in hypermobility [34] and the combination of hypermobility with autism further increases the prevalence [35].
A recent study of the association between fibromyalgia and autistic traits in a self-selected community-based population dominated by young females suggested that the relationship was partly mediated by hypermobility [36]. Subjects in this study also reported a high prevalence of food sensitivity and intolerance to gluten and lactose. We therefore conducted an analysis of the relationship between these features and the extent of both fibromyalgia symptoms and autistic traits in the same population to explore whether food-related issues might further mediate this relationship. If this proves to be the case, it may both explain the observation and offer the prospect of more specific assessment of the therapeutic role of selective diet in fibromyalgia management.
METHODS
Participants
Participants were recruited online or through the School of Psychology’s Research Participation Scheme (RPS) at Newcastle University. Inclusion criteria were (a) being aged between 18-60 and (b) being fluent in English. Participants were excluded if they did not complete all the questionnaires. Those who did complete the study were invited to partake in a lottery draw as an incentive. Ten randomly selected participants were each awarded £10. In addition, those recruited via the RPS were granted 1 research credit upon study completion. All participants gave informed consent and were provided with a unique code and allowed to withdraw from the research at any time. Ethical approval was obtained via Newcastle University’s FMS Research Ethics Committee (15052/2021).
Procedure
Participants completed an online survey hosted by Qualtrics Survey Software. The survey was advertised to participants through online and social media platforms, including Facebook, Instagram, Twitter, Reddit, Survey Circle and LinkedIn. Researchers also displayed posters around the university campus and contacted university department facilitators across the UK to share the study nationally. For undergraduate psychology students at Newcastle University, the survey was made available via the Sona System that is part of the RPS.
Participants were directed to a welcome video explaining the purpose and procedure of the study. Participants were asked to read the digital consent form, reassured that they could withdraw at any stage and that all data would be anonymised. Participants completed a comprehensive demographic questionnaire detailing age, sex, gender, ethnicity, religion, and employment status. Then they were asked to complete self-assessment questionnaires on symptoms of fibromyalgia [37] and autistic traits [38]. In addition, all participants were asked to complete a questionnaire on food sensitivity and food intolerance, detailing any foods that they avoided and the effects that food had on them and their symptoms. Further methodological details are provided in the methods section of our previous paper describing the relationship between fibromyalgia and autistic traits [36].
Design
The study was a non-experimental, correlational design. The predictor variable was autistic traits, the outcome variable was fibromyalgia symptoms (pain/dysautonomia), and the mediator variable was food intolerance.
Materials/Measures
Fibromyalgia: The Fibromyalgia Survey Questionnaire (FSQ) adapted by the American College of Rheumatology [37] is comprised of two scales: the Widespread Pain Index (WPI) and the Symptom Severity scale (SSS). The WPI quantifies the extent of recent pain on a scale of 0-19. The SSS is composed of two parts. Part 2a assesses fatigue, waking unrefreshed and cognitive symptoms. Part 2b records severity of somatic symptoms, which may reflect autonomic dysfunction. When 2a and 2b are combined, a total score of between 0-12 is obtained.
A diagnosis of fibromyalgia must fulfil one of two conditions: WPI≥7 and SSS≥5, or WPI=3-6 and SSS ≥9. The total FSQ score (WPI+SSS) ranges between 0-31, with a score of ≥12 meeting criteria for the diagnosis of fibromyalgia. Symptoms must be present for 3 months with no other explanation. The FSQ has been widely validated with reasonable sensitivity (64-96%), specificity (60-100%) and validity (Cronbach’s α=0.60-0.87) [38].
Autistic traits: The Ritvo Autism Asperger Diagnostic Scale-Revised (RAADS-R) [39] is a modified version of the RAADS developed as a clinical adjunct diagnostic tool for autistic spectrum disorder (ASD). It is an 80-item scale which screens for the presence of autistic traits in adults based on the revised DSM-IV scale (APA, 2000). Items are comprised of four sub-scales that are lifespan focused: social relatedness, circumscribed interest, language and sensory-motor symptoms. Participants rate the degree to which they relate to each statement on a 4-point Likert scale. Cronbach alpha coefficients for the subscales in the ranged from .79 to .92, showing high internal consistency. A score of over 65 is consistent with a diagnosis of ASD but is not in itself diagnostic of this condition.
Hypermobility: The Beighton Score (BS) comprises a set of manoeuvres used as the standard measure for assessing hypermobility [40]. The items record the ability to touch the forearm with the ipsilateral thumb, hyperextension at both fifth metacarpal-phalangeal joints, hyperextension at both elbows and at both knee joints and hyperflexion at the lumbosacral spine. The maximum score is 9 and a score of at least 5 suggests hypermobility in adults aged 18-49, according to the 2017 diagnostic criteria for hypermobility [41].
Food related symptoms: The food preference questionnaire was a self-reported 16-item designed by the research team to assess individuals’ food preferences, eating patterns, intolerances, and allergies (see Appendix). It consisted of both open and closed questions, which were measured on a 2-point or 3-point Likert scale (1=No, 2=Yes; 1=No, 2=Maybe, 3=Yes). The specificity of the questions meant that not all questions could be applied to all participants so skip logic was utilised for user ease. The questions used were as follows: Are there any foods you avoid? (sensitivity); are there any foods which cause you severe symptoms that can require medical intervention? (allergy); are there any foods that cause unpleasantness that doesn’t usually require medical attention? (intolerance).
Data Analysis
To prepare the data for hypothesis testing, preliminary analyses were conducted on the raw data prior to the main analysis using the software package SPSS v27. Data from 326 participants were removed due to incomplete responses. In the remaining 442 participants with full data sets, the WPI items were scored as dichotomous (yes/no) variables, omitting analysis of internal consistency. To visually assess normality, scatterplots, histograms, outliers, skewness, and kurtosis were examined for each scale using unstandardised residuals. The SSS and RAADS met the normality assumptions, but data for the WPI and FSQ appeared skewed. Thus, a log transformation and square root transformation were applied to the skewed scales to assess the best normality fit. A log-natural transformation was confirmed for the WPI, and a square root transformation was confirmed for the FSQ. Therefore, the transformed data for the WPI and FSQ and the raw data for the SSS and RAADS was used for the main analysis.
The percentage of participants who fulfilled criteria for the diagnosis of each of food intolerance, food sensitivity, fibromyalgia and ASD was calculated for the overall group. Directional Pearson correlations were conducted to assess the strength of the relationships between both scales and food sensitivity, allergy and intolerance [42]. Data from 3 items of the food intolerance questionnaire (Q103, Q108 and Q109) were analysed. These were also found to be abnormally distributed (informed by skewness and kurtosis values). Therefore, non-parametric tests were used as follows: Spearman’s correlation, Mann-Whitney U and Kruskal-Wallis. All data analyses were performed using IBM SPSS (Version 27).
RESULTS
Demographics
There were 442 participants who provided a complete dataset suitable for analysis and inclusion within the study. Their median age was 24 (range 18-60) years. Of these, 338 identified their gender as female (76.5%), 70 as male (15.8%), 22 as non-binary (5.0%), 6 as trans-male (1.4%), 2 as trans-female (0.5%) and 4 as ‘prefer not to say’ (0.8%). These data are shown in more detail in our previous paper [36].
Thresholds and mean scores
Among the 442 participants, 180 (40.7%) fulfilled criteria for the diagnosis of fibromyalgia and 290 (65.6%) exhibited sufficient autistic traits to meet the RAADS-R threshold for suspected ASD. A further 194 (44.9%) subjects met the Beighton criteria for hypermobility. The mean (SD) scores achieved by the participants on each of the major rating scales were fibromyalgia 11.53 (6.81), RAADS-R 83.81 (34.31) and Beighton’s test 3.87 (2.77).
Correlation between fibromyalgia score and autistic traits
For the 182 participants who scored 12 or above on the combined fibromyalgia scales, the Pearson correlation coefficient between the fibromyalgia score and RAADS-R score was significant at 0.237 (P=0.01). The correlation between RAADS-R and the SSS was 0.421 (p=0.001), while the correlation between RAADS-R and the WPI was not significant at 0.006. Hence, features related to dysautonomia accounted for the observed correlation between those who met criteria for fibromyalgia and the presence of autistic traits.
Correlations between food symptoms and other variables
There were significant differences in food sensitivities between those who met criteria for fibromyalgia and those who did not (U = 17643.00, z = -5.04, r = .24 p <.001). There were also significant differences in food allergy between the two groups (U = 10286.00, z = -3.83, r = .18, p<.001) and in food intolerance between those with and without fibromyalgia (U = 15526.00, z = -6.80, r = .38, p<.001). Data presented in Table 1 indicates that correlations between all three categories of food-related symptoms were stronger for subjects meeting criteria for fibromyalgia than with those with either enhanced autistic traits or hypermobility.
There was evidence of an increase in food sensitivities in those who scored over 65 on the RAADS-R scale when compared to those who did not (U = 21157.00, z = -2.90, r = .14, p = .004). Likewise, there were associations between both food allergy (U = 20540.50, z = -2.44, r = .12, p = .015), and food intolerance (U = 19655.50, z = -2.58, r = .12, p = .010) with increased autistic traits. By contrast, there was no significant difference in food sensitivities between those who had a positive Beighton test (U = 23263.00, z = -.854, r = -.04, p = .39). However, there were associations between both food allergy (U = 11306.50, z = -2.84, r = .14, p = .004) and food intolerance (U =20323.00, z = -3.08, r = .15 p = .002,) with hypermobility.
Regressions and variance
RAADS-R scores explained 20.4% of the variance in SSS (R2 = .204, F(114.421) = 447), but RAADS-R scores accounted for just 5.9% of the variance in WPI scores (B = 1.435, t = 5.279). This again emphasises that symptoms suggesting dysautonomia account for most of the correlation with autistic traits. A significant partial mediation between fibromyalgia and autistic traits was also found through hypermobility (t = 3.606, p = 0.0001). Figure 1 shows the proposed model for role of food sensitivities in mediating the relationship between fibromyalgia, autistic traits and hypermobility.
DISCUSSION
This study demonstrated that within our self-selected sample, mainly comprising young females, those who reported features of fibromyalgia were also more likely to describe food sensitivity and / or intolerance. This manifested as gastrointestinal symptoms more often than as musculoskeletal or psychiatric features and was most often associated with either gluten or lactose consumption. Those with significant autistic traits and / or hypermobility were also statistically more likely to report food-related symptoms. Food sensitivities, along with hypermobility, may partially mediate the relationship between fibromyalgia and autistic traits. This association is much stronger for the autonomic component of fibromyalgia (SSS) than for the extent of pain and tenderness (WPI).
Women have significantly more tender musculoskeletal points than men [43,44], and Wolfe reported a much higher prevalence of fibromyalgia in women (3.4%) compared to men (0.5%) [37]. There are also important differences in perceived pain between the sexes [1,45], and this equates to multisensory hypersensitivity in females with fibromyalgia [46]. This in turn impacts on psychosocial function [47] and may offer new therapeutic avenues [48,49,50]. In particular, the link with gastrointestinal features suggests that dietary modification may have a part to play in the treatment of fibromyalgia, especially in females [51]. For example, musculoskeletal, neurological and psychiatric symptoms have all been associated with gluten consumption among people with no evidence of coeliac disease [52], and these features closely mimic those of fibromyalgia.
Gut microbiota may play an essential role in fibromyalgia [53], and a systematic review suggested that investigations into the relationship between the gut microbiota, bowel dysfunction and fibromyalgia was warranted [54]. Chronic pain patients have benefitted from the development of a diet based on carbohydrates with low glycaemic index together with fruits and vegetables, yogurt, red wine, legumes and fish with occasional meat, eggs and cheese [55], while other workers have found evidence to support the use of olive oil, ancient grains, Mediterranean diet, glutamate and aspartame-free diet and a gluten-free diet in reducing symptoms of fibromyalgia [56]. A further systematic review of antioxidants in fibromyalgia suggested that over half of the studies assessed offered good evidence for efficacy of supplementation with vitamins and coenzyme Q10, and less consistent evidence for benefit from extra virgin olive oil and turmeric [57]. Vegan and FODMAP diets have produced some benefit in fibromyalgia [58] but significant differences in opinion persist at present [11,12,59]. Another systematic review found no benefit from dietary therapy in fibromyalgia, with patients reporting greater efficacy from acupuncture and physiotherapy [60]. However, many patients themselves prefer non-pharmacological therapies, particularly dietary interventions, which were reported to be more efficacious than drugs in a recent Italian study [61].
Recent work has confirmed that patients with fibromyalgia and other forms of chronic pain are more likely to be neurodivergent [28,30] and that autistic people often develop chronic musculoskeletal pain [29,31]. This relationship also extends to close relatives [62], and hypermobility may mediate the association between fibromyalgia and autistic features [32], especially among symptomatic individuals [36,40]. Most young females with autism or ADHD who also had hypermobility reported the development of chronic pain in adulthood [39,41]. Musculoskeletal pain was described by 83% of people with hypermobility in one study, while autonomic and gastrointestinal symptoms were also reported by 70% and 71% of the same subjects [63]. A major overlap between fibromyalgia and chronic fatigue has been confirmed in people with hypermobility [64] and may also be a consequence of autonomic dysfunction. Indeed, hypersensitivity of the autonomic nervous system due to excitation of sympathetic and inhibition of parasympathetic nerves [65] can produce a range of clinical features in ASD and is also very common in fibromyalgia [66]. Gastrointestinal dysfunction has been reported by 83% of autistic women [67], mirroring the prevalence in fibromyalgia [52,53].
There is empirical evidence, along with scientific consensus, to support an association between food selectivity and ASD [68]. Studies have reported a high prevalence of non-IgE-mediated food allergies in autistic children [69], and food selectivity often continues into adulthood, primarily driven by sensitivity around textures and tastes [70]. Although gluten sensitivity itself may present with gastrointestinal or neurological symptoms, a decade ago two studies concluded that there was insufficient evidence at that time to justify recommending a GFD to autistic children [17,71]. However, the situation has evolved with increasing evidence that a GFD can produce improvement in autistic behaviours in those with allergies or intolerances to gluten [72]. There is strong anecdotal evidence of a benefit in many studies, although statistical analyses of the data are less convincing [73]. Most of the research has been conducted in autistic children and is therefore difficult to extrapolate to adults with confidence. There remains the danger of promoting ARFID in selected adults unless positive reinforcement is used appropriately [74], along with vitamin supplementation.
There is a dearth of scientific evidence on the effects of either lactose or alcohol consumption on fibromyalgia. The very limited available evidence suggests that alcohol may in fact be protective from chronic pain in moderate doses [75] but such an association cannot be assumed to relate to causation [76]. There is very limited evidence that the protein casein, found in dairy products, might exacerbate autistic features in children. A synopsis of the available data in 2014 was unable to reach a firm conclusion on the role of dairy-free diet in the management of autistic children [77].
Limitations
Self-reported surveys are always at risk of bias because of self-selection. Food related issues are subject to significant personal bias and our results were dependent on a questionnaire devised specifically for the study. No inter-observer error was calculated, and no tests of validity were made.
Despite additional effort made to avoid advertising the study onto certain platforms (eg. online autism forums) and restraining the use of hashtags that may attract specific groups, it is difficult to confirm the lack of bias without having screened for existing diagnoses. Further limitations reside in the measures used. All measures were self-reported questionnaires which decreases the internal validity as participants may exaggerate or underreport symptoms. For example, clinicians usually assess hypermobility, and the accuracy of participant’s self-diagnosis cannot be guaranteed. Alternative measures validated for use in large population studies could be used in future studies.
Future Research
Chronic pain is a frequent comorbidity for those with autistic traits and hypermobility. Food related issues, especially intolerance, are associated with heightened levels of symptomatology even within a self-selected community population, largely comprised of younger females. Intolerance to gluten, lactose and alcohol correlate most closely with symptoms of dysautonomia and further research is needed to assess whether this relationship can be demonstrated in patient populations with confirmed fibromyalgia. Exploration of the mechanisms for this association is needed, in the hope that there may be support for further formal clinical trials of exclusion of specific dietary elements in those who report adverse advents associated with their consumption.
CONCLUSIONS
In conclusion, this study demonstrated a strong relationship between food-related symptoms of intolerance or sensitivity and features of fibromyalgia in a self-selected community population comprised chiefly of young females. Food related concerns were most often provoked by gluten and lactose and were more often manifested as gastrointestinal symptoms than musculoskeletal pain. However, a significant group (1 in 6) of participants did report that certain foods were associated with worsening of symptoms of fibromyalgia. Given the highly significant association of autistic traits with fibromyalgia in this population, with indirect evidence of significant autonomic dysfunction, it is possible that certain foodstuffs trigger fibromyalgia in some individuals as a result of their antigenic effects on an immune system rendered susceptible by autonomic hypersensitivity within the gastrointestinal tract.
Funding
No funding was obtained in support of this study.
Conflicts of Interest
None of the authors have any conflicts of interest to declare.
Appendix. Food preference questionnaire
References
- Wolfe, F., Clauw, D. J., Fitzcharles, M. A., et al. (2010). The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis care and research, 62(5), 600-610. [CrossRef]
- Walitt, B., Nahin, R. L., Katz, R. S., Bergman, M. J., & Wolfe, F. (2015). The prevalence and characteristics of fibromyalgia in the 2012 National Health Interview Survey. PloS one, 10(9), e0138024. [CrossRef]
- Sarzi-Puttini, P., Giorgi, V., Marotto, D., & Atzeni, F. (2020). Fibromyalgia: an update on clinical characteristics, aetiopathogenesis and treatment. Nature Reviews Rheumatology, 16(11), 645-660. [CrossRef]
- Eccles, J. A., Thompson, B., Themelis, K., et al. (2021). Beyond bones: The relevance of variants of connective tissue (hypermobility) to fibromyalgia, ME/CFS and controversies surrounding diagnostic classification: an observational study. Clinical Medicine, 21(1), 53. [CrossRef]
- Bonaz B, Lane RD, Oshinsky ML, Kenny PJ, Sinha R, Mayer EA, Critchley HD. Diseases, Disorders, and Comorbidities of Interoception. Trends Neurosci. 2021 Jan;44(1):39-51. PMID: 33378656. [CrossRef]
- Whealy, M., Nanda, S., Vincent, A., Mandrekar, J., & Cutrer, F. M. (2018). Fibromyalgia in migraine: A retrospective cohort study [Abstract]. The Journal of Headache and Pain, 19(1). [CrossRef]
- Clauw DJ. Fibromyalgia and related conditions. Mayo Clin Proc. 2015 May;90(5):680-92. PMID: 25939940. [CrossRef]
- Isasi C, Colmenero I, Casco F, Tejerina E, Fernandez N, Serrano-Vela JI, W al. Fibromyalgia and non-celiac gluten sensitivity: a description with remission of fibromyalgia. Rheumatol Int. 2014 Nov;34(11):1607-12. Epub 2014 Apr 12. PMID: 24728027; PMCID: PMC4209093. [CrossRef]
- Slim, M, Calandre, E, Garcia-Leiva, J, Rico-Villademoros, F, Molina-Barea, R, Rodriguez-Lopez, C et al. The Effects of a Gluten-free Diet Versus a Hypocaloric Diet Among Patients With Fibromyalgia Experiencing Gluten Sensitivity-like Symptoms: A Pilot, Open-Label Randomized Clinical Trial. [Article] Journal of Clinical Gastroenterology. 51(6):500-507, July 2017.
- Rossi A, Di Lollo AC, Guzzo MP, Giacomelli C, Atzeni F, Bazzichi L, et al. Fibromyalgia and nutrition: what news? Clin Exp Rheumatol. 2015 Jan-Feb;33(1 Suppl 88):S117-25. Epub 2015 Mar 18. PMID: 25786053.
- Marum AP, Moreira C, Saraiva F, Tomas-Carus P, Sousa-Guerreiro C. A low fermentable oligo-di-monosaccharides and polyols (FODMAP) diet reduced pain and improved daily life in fibromyalgia patients. Scand J Pain. 2016 Oct;13:166-172. Epub 2016 Aug 22. PMID: 28850525. [CrossRef]
- Silva AR, Bernardo A, Costa J, Cardoso A, Santos P, de Mesquita MF, et al. Dietary interventions in fibromyalgia: a systematic review. Ann Med. 2019;51(sup1):2-14. PMID: 30735059; PMCID: PMC7888848. [CrossRef]
- Leader, G., Tuohy, E., Chen, J. L., Mannion, A., & Gilroy, S. P. (2020). Feeding problems, gastrointestinal symptoms, challenging behaviors and sensory issues in children and adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50(1), 1401–1410. [CrossRef]
- Cermak SA, Curtin C, Bandini LG. Food selectivity and sensory sensitivity in children with autism spectrum disorders. J Am Diet Assoc. 2010 Feb;110(2):238-46. PMID: 20102851; PMCID: PMC3601920. [CrossRef]
- Buckley, Julie A., Herbert, Martha R., (2013). Autism and dietary therapy: case report and review of the literature. Journal of Child Neurology. [CrossRef]
- Lange KW, Hauser J, Reissmann A. Gluten-free and casein-free diets in the therapy of autism. Curr Opin Clin Nutr Metab Care. 2015 Nov;18(6):572-5. PMID: 26418822. [CrossRef]
- Mulloy, A. et al., (2010), Gluten-Free and Casein free diets in the treatment of autism spectrum disorders: A systematic review. Research in Autism Spectrum Disorder, Vol 4 (3), pp.328-339.
- Hyman SL, Stewart PA, Foley J, Cain U, Peck R, Morris DD, Wang H, Smith T. The Gluten-Free/Casein-Free Diet: A Double-Blind Challenge Trial in Children with Autism. J Autism Dev Disord. 2016 Jan;46(1):205-220. PMID: 26343026. [CrossRef]
- Kelly C, Davies M. A Review of Anorexia Nervosa, Its Relationship to Autism and Borderline Personality Disorder, and Implications for Patient Related Outcomes. Journal of Psychiatry and Psychiatric Disorders 3 (2019): 207-215. Review Article Volume 3, Issue 4. [CrossRef]
- van Rensburg R, Meyer HP, Hitchcock SA, Schuler CE. Screening for Adult ADHD in Patients with Fibromyalgia Syndrome. Pain Med. 2018;19(9):1825-1831. [CrossRef]
- Moyano S, Berrios W, Gandino IJ, et al. Prevalence of Attention Deficit Hyperactivity Disorder Among Patients with Fibromyalgia [abstract]. Arthritis Rheumatol. 2018;70 (suppl 10).
- Pallanti S, Porta F, Salerno L. Adult attention deficit hyperactivity disorder in patients with fibromyalgia syndrome: Assessment and disabilities. J Psychiatr Res. 2021;136:537-542. [CrossRef]
- Karaş H, Çetingök H, İlişer R, et al. Childhood and adult attention deficit hyperactivity disorder symptoms in fibromyalgia: associations with depression, anxiety and disease impact. Int J Psychiatry Clin Pract. 2020;24(3):257-263. [CrossRef]
- Türkoğlu G. Attention-deficit hyperactivity disorder symptoms and quality of life in female patients with fibromyalgia. Turk J Med Sci. 2021;51(4):1747-1755. Published 2021 Aug 30. [CrossRef]
- Holman AJ, Neiman RA, Ettlinger RE. Preliminary efficacy of the dopamine agonist, pramipexole for fibromyalgia: the first, open label, multicenter experience. _J Musculoskeletal Pain.2004;12(1):69-74.
- Critchley, H. D., & Eccles, J. A. (2020). Increased rate of joint hypermobility in autism and related neurodevelopmental conditions is linked to dysautonomia and pain. MedRxiv. [CrossRef]
- Dietz, P. M., Rose, C. E., McArthur, D., & Maenner, M. (2020). National and state estimates of adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50(12), 4258-4266. [CrossRef]
- Eccles, J. A., Iodice, V., Dowell, N. G., et al. (2014). Joint hypermobility and autonomic hyperactivity: relevance to neurodevelopmental disorders. Journal of Neurology, Neurosurgery & Psychiatry, 85(8), e3-e3. [CrossRef]
- Baeza-Velasco C, Cohen D, Hamonet C, Vlamynck E, Diaz L, Cravero C, Cappe E, Guinchat V. Autism, Joint Hypermobility-Related Disorders and Pain. Front Psychiatry. 2018 Dec 7;9:656. PMID: 30581396; PMCID: PMC6292952. [CrossRef]
- Casanova EL, Baeza-Velasco C, Buchanan CB, Casanova MF. The Relationship between Autism and Ehlers-Danlos Syndromes/Hypermobility Spectrum Disorders. J Pers Med. 2020 Dec 1;10(4):260. PMID: 33271870; PMCID: PMC7711487. [CrossRef]
- Asztély K, Kopp S, Gillberg C, Waern M, Bergman S. Chronic pain and health-related quality of life in women with autism and/or ADHD: a prospective longitudinal study. J Pain Res. (2019) 12:2925–32. [CrossRef]
- Csecs, J. L., Iodice, V., Rae, C. L., et al. (2022). Joint Hypermobility Links Neurodivergence to Dysautonomia and Pain. Frontiers in Psychiatry, 2568. [CrossRef]
- Cederlöf, M., Larsson, H., Lichtenstein, P., Almqvist, C., Serlachius, E., and Ludvigsson, J. F. (2016). Nationwide population-based cohort study of psychiatric disorders in individuals with Ehlers–Danlos syndrome or hypermobility syndrome and their siblings. BMC psychiatry, 16(1), 1-7. [CrossRef]
- Wolfe, F., Ross, K., Anderson, J., Russell, I. J., & Hebert, L. (1995). The prevalence and characteristics of fibromyalgia in the general population. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology, 38(1), 19-28. [CrossRef]
- Castori, M., Morlino, S., Pascolini, G., Blundo, C., & Grammatico, P. (2015, March). Gastrointestinal and nutritional issues in joint hypermobility syndrome/Ehlers–Danlos syndrome, hypermobility type. In American Journal of Medical Genetics Part C: Seminars in Medical Genetics (Vol. 169, No. 1, pp. 54-75). [CrossRef]
- Ryan L, Beer H, Thomson E, Philcox E and Kelly CA. Neurodivergent traits correlate with chronic musculoskeletal pain: a self-selected population-based survey. In press Neurobiology; 2022.
- Wolfe F., Clauw D.J., Fitzcharles M.A., Goldenberg D.L., Häuser W., Katz R.S., Mease P., Russell A.S., Russell I.J., Winfield J.B. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: A modification of the ACR preliminary diagnostic criteria for fibromyalgia. JRheumatol. 2011; 38:1113–1122. [CrossRef]
- Aguirre Cárdenas C, Oñederra MC, Esparza Benavente C, Durán J, González Tugas M, Gómez-Pérez L. Psychometric Properties of the Fibromyalgia Survey Questionnaire in Chilean Women With Fibromyalgia. J Clin Rheumatol. 2021 Sep 1;27(6S):S284-S293. PMID: 32897990. [CrossRef]
- Ritvo, R. A., Ritvo, E. R., Guthrie, D., et al. (2011). The Ritvo Autism Asperger Diagnostic Scale-Revised (RAADS-R): a scale to assist the diagnosis of autism spectrum disorder in adults: an international validation study. Journal of autism and developmental disorders, 41(8), 1076-1089. [CrossRef]
- Juul-Kristensen B, Schmedling K, Rombaut L, Lund H, Engelbert RH. Measurement properties of clinical assessment methods for classifying generalized joint hypermobility-A systematic review. Am J Med Genet C Semin Med Genet. 2017 Mar;175(1):116-147. PMID: 28306223. [CrossRef]
- Bockhorn, L. N., Vera, A. M., Dong, D., Delgado, D. A., Varner, K. E., & Harris, J. D. (2021). Interrater and intra-rater reliability of the Beighton score: A systematic review. Orthopaedic Journal of Sports Medicine, 9(1), 2325967120968099. [CrossRef]
- https://www.statisticshowto.com/probability-and-statistics/correlation-coefficient-formula/.
- Yunus, M. B., Inanici, F. A. T. M. A., Aldag, J. C., & Mangold, R. F. (2000). Fibromyalgia in men: comparison of clinical features with women. The Journal of rheumatology, 27(2), 485-490. https://pubmed.ncbi.nlm.nih.gov/10685818.
- Guzzo, M. P., Iannuccelli, C., Gerardi, M. C., Lucchino, B., Valesini, G., & Di Franco, M. (2017). AB0925 Gender difference in fibromyalgia: comparison between male and female patients from an italian monocentric cohort. [CrossRef]
- Stubbs D, Krebs E, Bair M, Damush T, Wu J, Sutherland J, et al. Sex Differences in Pain and Pain-Related Disability among Primary Care Patients with Chronic Musculoskeletal Pain. Pain Medicine. 2010;11(2):232–9. pmid:20002591.
- Wilbarger, J. L., & Cook, D. B. (2011). Multisensory hypersensitivity in women with fibromyalgia: implications for well being and intervention. Archives of physical medicine and rehabilitation, 92(4), 653-656. [CrossRef]
- Bair, M. J., & Krebs, E. E. (2020). Fibromyalgia. Annals of internal medicine, 172(5), ITC33-ITC48. [CrossRef]
- Häuser, W., Ablin, J., Fitzcharles, M. A., Littlejohn, G., Luciano, J. V., Usui, C., & Walitt, B. (2015). Fibromyalgia. Nature reviews Disease primers, 1(1), 1-16. [CrossRef]
- English, B. (2014). Neural and psychosocial mechanisms of pain sensitivity in fibromyalgia. Pain Management Nursing, 15(2), 530-538. [CrossRef]
- Littlejohn G., Guymer E. Key milestones contributing to the understanding of the mechanisms underlying fibromyalgia. Biomedicines. 2020;8:223. [CrossRef]
- Slim, M., Calandre, E. P., & Rico-Villademoros, F. (2015). An insight into the gastrointestinal component of fibromyalgia: clinical manifestations and potential underlying mechanisms. Rheumatology international, 35(3), 433-444. [CrossRef]
- Losurdo G, Principi M, Iannone A, Amoruso A, Ierardi E, Di Leo A, Barone M. Extra-intestinal manifestations of non-celiac gluten sensitivity: An expanding paradigm. World J Gastroenterol. 2018 Apr 14;24(14):1521-1530. PMID: 29662290; PMCID: PMC5897856. [CrossRef]
- Minerbi A, Gonzalez E, Brereton NJB, et al. Gut microbiota may play a pivotal role in fibromyalgia. Pain. 2019 Nov;160(11):2589-2602. [CrossRef]
- Erdrich, S., Hawrelak, J.A., Myers, S.P. et al. Determining the association between fibromyalgia, the gut microbiome and its biomarkers: A systematic review. BMC Musculoskelet Disord 21, 181 (2020). [CrossRef]
- Rondanelli, M., Faliva, M., Miccono, A., Naso, M., Nichetti, M., Riva, A et al. (2018). Food pyramid for subjects with chronic pain: Foods and dietary constituents as anti-inflammatory and antioxidant agents. Nutrition Research Reviews, 31(1), 131-151. [CrossRef]
- Pagliai G, Giangrandi I, Dinu M, Sofi F, Colombini B. Nutritional Interventions in the Management of Fibromyalgia Syndrome. Nutrients. 2020 Aug 20;12(9):2525. PMID: 32825400; PMCID: PMC7551285. [CrossRef]
- Fernández-Araque A, Verde Z, Torres-Ortega C, Sainz-Gil M, Velasco-Gonzalez V, González-Bernal JJ, et al. Effects of Antioxidants on Pain Perception in Patients with Fibromyalgia-A Systematic Review. J Clin Med. 2022 Apr 27;11(9):2462. PMID: 35566585; PMCID: PMC9099826. [CrossRef]
- Lowry E, Marley J, McVeigh JG, McSorley E, Allsopp P, Kerr D. Dietary Interventions in the Management of Fibromyalgia: A Systematic Review and Best-Evidence Synthesis. Nutrients. 2020 Aug 31;12(9):2664. PMID: 32878326; PMCID: PMC7551150. [CrossRef]
- Tomaino L, Serra-Majem L, Martini S, Ingenito MR, Rossi P, La Vecchia C, et al. Fibromyalgia and Nutrition: An Updated Review. J Am Coll Nutr. 2021 Sep-Oct;40(7):665-678. Epub 2020 Sep 9. PMID: 32902371. [CrossRef]
- Almutairi NM, Hilal FM, Bashawyah A, Dammas FA, Yamak Altinpulluk E, Hou JD, et al. Efficacy of Acupuncture, Intravenous Lidocaine, and Diet in the Management of Patients with Fibromyalgia: A Systematic Review and Network Meta-Analysis. Healthcare (Basel). 2022 Jun 23;10(7):1176. PMID: 35885703; PMCID: PMC9320380. [CrossRef]
- Demori I, Molinari E, Rapallo F, Mucci V, Marinelli L, Losacco S, et al. Online Questionnaire with Fibromyalgia Patients Reveals Correlations among Type of Pain, Psychological Alterations, and Effectiveness of Non-Pharmacological Therapies. Healthcare (Basel). 2022 Oct 9;10(10):1975. PMID: 36292422; PMCID: PMC9602604. [CrossRef]
- Kelly C, Martin R and Saravanan V. The links between fibromyalgia, hypermobility and neurodivergence. TouchReviews March 15th 2022.
- Clark, C. J., Khattab, A. D., & Carr, E. C. (2014). Chronic widespread pain and neurophysiological symptoms in joint hypermobility syndrome (JHS). International Journal of Therapy and Rehabilitation, 21(2), 60-67. [CrossRef]
- Critchley, H. D., & Davies, K. A. (2021). Beyond bones: The relevance of variants of connective tissue (hypermobility) to fibromyalgia, ME/CFS and controversies surrounding diagnostic classification: an observational study. Clinical Medicine, 21(1), 53. [CrossRef]
- Song, R; Liu, J PhD; Kong, X. Autonomic Dysfunction and Autism: Subtypes and Clinical Perspectives. N A J Med Sci. 2016;9(4):172-180. DOI: 10.7156/najms.2016.0904172.
- Puri BK, Lee GS. Clinical Assessment of Autonomic Function in Fibromyalgia by the Refined and Abbreviated Composite Autonomic Symptom Score (COMPASS 31): A Case-Controlled Study. Rev Recent Clin Trials. 2022;17(1):53-57. PMID: 34126910. [CrossRef]
- Brent Goodman. Autonomic Dysfunction in Autism Spectrum Disorders (ASD) (P5.117) Neurology Apr 2016, 86 (16 Supplement) P5.117-9.
- Mari-Bauset, S., Zazpe, I., Mari-Sanchis, A., Llopis-Gonzalez, A., Morales-Suarez-Varel, M. (2014). Food selectivity in autism spectrum disorders: A systematic review. Journal of Child Neurology, 29(11), 1554–1561. [CrossRef]
- Jyonouchi H. Food allergy and autism spectrum disorders: is there a link? Curr Allergy Asthma Rep. 2009 May;9(3):194-201. PMID: 19348719.. [CrossRef]
- Kuschner, E. S., Eisenberg, I. W., Orionzi, B., Simmons, W. K., Kenworthy, L., Martin, A., et al.. (2015). A preliminary study of self-reported food selectivity in adolescents and young adults with autism spectrum disorder. Research in Autism Spectrum Disorders, 15–16, 53–59. [CrossRef]
- Buie T. The relationship of autism and gluten. Clin Ther. 2013 May;35(5):578-83. PMID: 23688532. [CrossRef]
- Sumathi T, Manivasagam T, Thenmozhi AJ. The Role of Gluten in Autism. Adv Neurobiol. 2020; 24:469-479. PMID: 32006368. [CrossRef]
- Croall ID, Hoggard N, Hadjivassiliou M. Gluten and Autism Spectrum Disorder. Nutrients. 2021 Feb 9;13(2):572. PMID: 33572226; PMCID: PMC7915454. [CrossRef]
- Pubylski-Yanofchick, W., Zaki-Scarpa, C., LaRue, R.H. et al. Treatment of Food Selectivity in an Adult With Autism Spectrum Disorder. Behav Analysis Practice 15, 796–803 (2022). [CrossRef]
- Macfarlane, G.J. and Beasley, M. (2015), Alcohol Consumption in Relation to Risk and Severity of Chronic Widespread Pain: Results From a UK Population-Based Study. Arthritis Care & Research, 67: 1297-1303. [CrossRef]
- Durán, Josefina MD, MS∗; Zitko, Pedro PhD†,‡; Barrios, Paola MD∗; Margozzini, Paula MD, MS‡. Chronic Musculoskeletal Pain and Chronic Widespread Pain in Chile: Prevalence Study Performed as Part of the National Health Survey. JCR: Journal of Clinical Rheumatology 27(6S):p S294-S300, September 2021.
- Paul Whiteley (2014) Nutritional management of (some) autism: a case for gluten and casein free diets? The Proceedings of the Nutritional Society, Vol. 74 (3), pp. 202-207 .
Figure 1.
Proposed model for role of food intolerance or sensitivity in the relationship between autism, hypermobility and fibromyalgia.
Figure 1.
Proposed model for role of food intolerance or sensitivity in the relationship between autism, hypermobility and fibromyalgia.
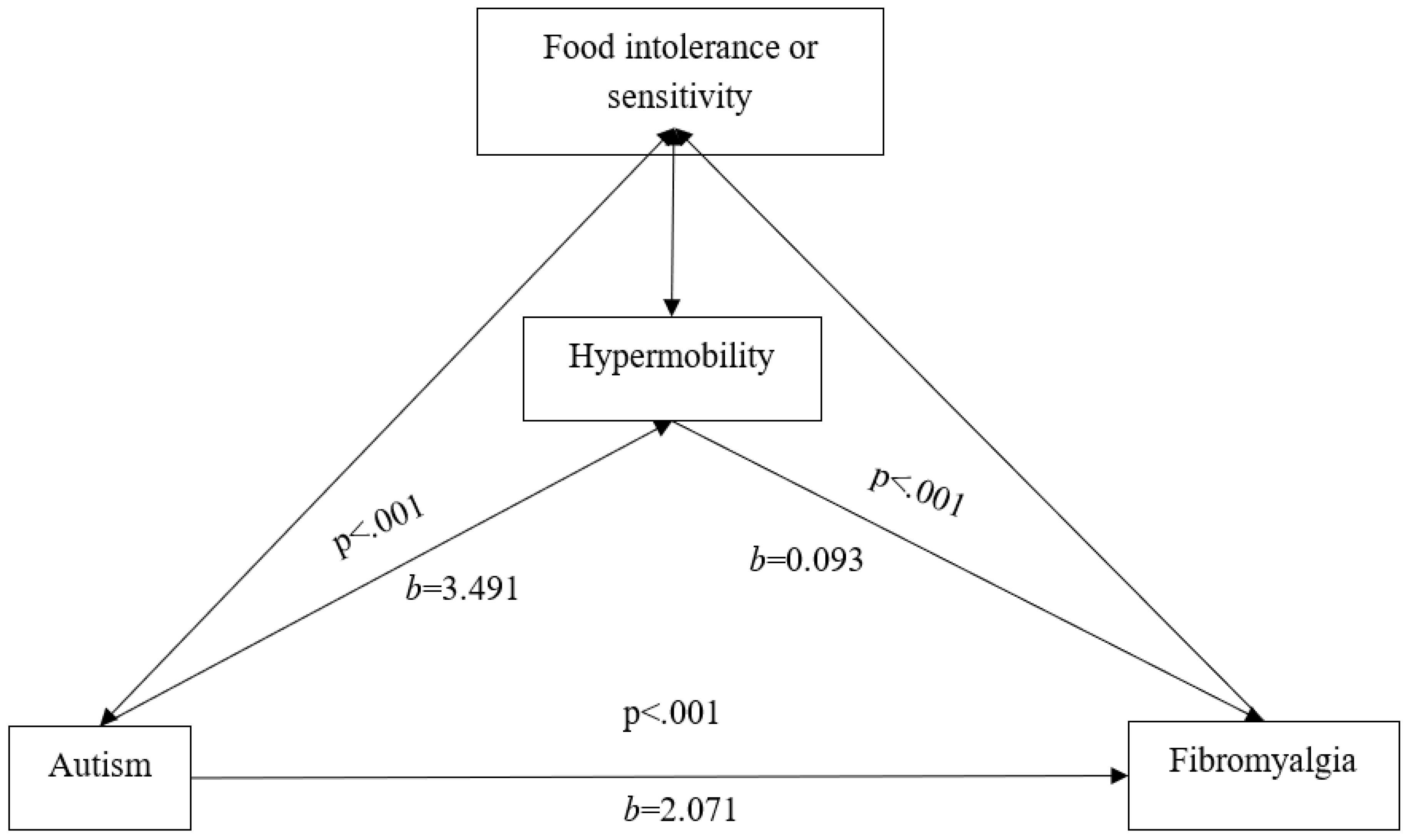

Table 1.
Spearman’s Correlation between the measures and food sensitivities, food allergies and food intolerances.
Table 1.
Spearman’s Correlation between the measures and food sensitivities, food allergies and food intolerances.
| Food sensitivity | Food allergy | Food intolerance | |
|---|---|---|---|
| Fibromyalgia RAADS-R |
.240*** .172** |
.182*** .125* |
.380*** .148** |
| Beighton | .041 | .135** | .157** |
Note: * p<.05 (2-tailed), ** p<.01 (2-tailed), ***p<.001 (2-tailed).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



