
Submitted:
12 January 2023
Posted:
17 January 2023
You are already at the latest version
Abstract
Aim: This study aimed to evaluate the sociodemographic, behavioral, and biological profile and its relationship with the emergence of chronic non-communicable diseases in riverside populations in the Xingu region, Pará, Brazil. Methods: Characteristics related to health indicators and which risk factors are considered most important were also analyzed. This is a cross-sectional, exploratory, and descriptive study. The sample consisted of riverside people over 18 years of both sexes. The sample size (n.86) was calculated with a confidence level of 95% and a sample error of 5%. To divide the groups, the K-means clustering algorithm was adopted through an unsupervised method and the values were expressed as median. For continuous and categorical data, the Mann-Whitney and Chi-square tests were used, respectively, and the significance level was set at p<5%. To classify the degree of importance of each variable, the multi-layer perceptron algorithm was applied. Results: Based on this information, the sample was divided into two groups: the group with low or no education, with bad habits and worse health conditions, and the group with opposite characteristics. The risk factors considered for cardiovascular diseases and diabetes in the groups were low education (p < 0.001), sedentary lifestyle (p < 0.01), smoking, alcoholism, body mass index (p < 0.05) and the waist-hip ratio, with values above the expected, in both groups. Conclusions: The factors considered important to have a good health condition or not were the educational and social conditions of these communities and a part of the riverside population was considered healthier than the other.
Keywords:
education level
; eating behavior
; healthy lifestyle habits
; non-communicable chronic diseases
; machine learning
1. Introduction
Environmental determinants can be regarding to the lifestyle, the appearance of diseases and imply the health and quality of life of a certain population. In addition, populations undergo changes in their epidemiological profile due to the influence of chronic non-communicable diseases (CNCDs) that are related to multiple causes [1].
According to Global Burden of Disease Study, in Brazil, CNCDs like dyslipidemia, systemic arterial hypertension and diabetes mellitus account for about 75% of the causes of death [2], being a major problem for health services. Thus, the importance of surveillance of risk factors such as sociodemographic, behavioral, and biological profile are effective ways to establish primary prevention measures and early detection of cardiovascular diseases [3]. Therefore, it is essential to adopt these practices, as they still are challenges for managers and health professionals, especially in isolated areas where riverside populations live [4].
Riverine or, in portuguese, "Ribeirinho" is a generic name that refers to a type of peasant existence in Brazil, and in the Amazon in particular. It presents as striking sociological characteristics, the intimate relationship with nature, markedly with the river. In the Xingu region, they are specifically called "beiradeiros", who live in the Riverside [5]. The Amazon riverside populations have characteristics that make it difficult to access basic services that urban populations have with a certain ease, such as, for example, they are rural and remote locations far from urban centers, low-income, limited access to health services (e.g. access to doctors and nurses) and health precariousness [6,7,8,9]. The main subsistence activities of these populations are based on artisanal fishing, family farming and extractivism [10], however, with migratory processes, their life habits have been changing [11] due to large infrastructure projects such as the Belo Monte Hydroelectric Power Plant, installed ten years ago in the middle Xingu River region, Pará, Brazil. Projects of this magnitude cause a big impact to the point of changing the quality of life and the morbidity and mortality profile of this population [12,13].
The middle Xingu is a complex region of conflicts and territorial and political disputes, marked by the installation of large enterprises such as HPPBM and, gold mining and deforestation [5,14,15,16]. The riverside population of the middle Xingu River is distributed over several islands that are scattered along the river, making health care for this population difficult. In addition, after the installation of the Belo Monte Hydroelectric Power Plant, the riverside population of this region, especially the families living in the middle Xingu River, suffered inestimable impacts such as territorial expropriation (estimated that 56% of the population was relocated), contamination of the river (water contamination due to construction works and damming) and reduction of fishing resources, reducing the life quality and way of living of the remaining population [5,17].
Epidemiological information for the riverside populations of the middle Xingu region is incipient in Brazil, since the health services provided in these communities are sporadic and the access of riverine people to the urban area is limited due to financial conditions and difficulty in moving around [7]. In addition, factors such as low education, illiteracy, lack of basic sanitation and poverty contribute to the emergence of endemic diseases that, until then, are unknown regarding their epidemiological profile within these populations [7,10].
Despite Brazil having a single health system (Sistema Único de Saúde, SUS) where access is free for the population, it can be seen that, to a certain extent, it is excluding, since some vulnerable groups, especially the Amazon riverside populations, do not are efficiently served by such a system. This is due in part to the geographic isolation and the deficiency of public policies aimed at these populations [18,19]. In addition, the demand for education in riverside communities faces many barriers such as cultural, ideological, educational and/or institutional [20]. This socioeconomic aspect associated with the lack of care can influence the absence of healthy habits in this population [21].
Although there are specific studies on the health profile of riverside populations [22], more in-depth and integrative studies are essential to better characterize the sociodemographic, behavioral, and biological patterns that contribute to the emergence of CNCDs, especially in the riverside population of the middle Xingu River, city of Altamira, state of Pará, Brazil.
The factors that influence CNCDs are complex and multifactorial, so that the use of algorithms associated with machine learning, such as K-means, can identify non-linear patterns that allow a more accurate and possible classification associations between lifestyle habits and the presence or absence of the most varied types of diseases [23,24,25]. Thus, the use of this algorithm with the input of data (e.g. sociodemographic, behavioral, and biological) obtained from the riverside populations of interest, allows us to assess whether the behavior of these populations maintains a single general pattern or whether there are distinct patterns. In addition, it is possible to identify whether the variables that have not yet been studied in these populations are similar or not to other riverside communities based on the literature. Based on these assumptions, it is believed that the riverside population of the middle Xingu River have two riverine profiles: the first profile of people with less schooling, bad habits and worse health condition, and a second profile with people with opposite characteristics.
In this sense, this study evaluated in an exploratory way, through the machine learning technique, the sociodemographic, behavioral, and biological profile, and its relationship to the emergence of CNCDs in riverside populations in the middle Xingu region and analyzed the characteristics of these patterns regarding to health indicators and which risk factors are considered most important.
2. Materials and Methods
2.1. Participants
This is a cross-sectional, exploratory, and descriptive study carried out in a riverside community on the middle Xingu River, Altamira town, Pará State, from March to September of 2019. The study was developed in the Espelho community, consisting of ~60 families, distributed in small communities (Cajueiro, Chicote, Espelho, Jabuti, Itapuâma, Jabota, Transassurini, Espanhol and Firma) along the banks of the middle Xingu River (Figure 1). Two expeditions were carried out that took place in the Chicote Island community, considered a geographically privileged place among the other communities, so it was used as a data collection base. Regarding the profile of the interviewees, the inclusion criterion was for convenience, so the profile was traced by the presence of riverine people in each field campaign, which was widely publicized a month in advance.
The sample size resulted from the total number of riverine people present in each field survey. Thus, 40 families accepted to be part of this research, which had an average of 4.3 ± 1.59 people per family, totaling 172 individuals. Of which an average of 2.2 ± 0.79 per family were over 18 years old, totaling 86 individuals of both sexes who signed the informed CONSENT and answered the questionnaire.
People with cognitive problems and who refused to participate in the research at any time of the action even if they signed the CONSENT were excluded.
To assess the representativeness of the number of individuals who agreed to participate in the research, Slovin's Formula was used: n = N / (1 + Ne2), where: n = Number of samples, N = Total population and e = Error tolerance (level) [26,27], considering a confidence level of 90% and a margin of error of 5%. After applying the equation, it was verified that this study would need at least 84 individuals, therefore, the sample obtained is representative. Furthermore, the sampling effort of this study is like that of others that analyzed small riverside communities[28,29,30].
This study was approved by the Ethics Committee of the Tropical Medicine Center at the Federal University of Pará (Opinion No. 3,678,493), in compliance with the Resolutions 441/2011/CNS e 466/2012/MS.
2.2. Procedures
In Figure 2 it is possible to observe the chronological flow and the operational procedures developed during the research. We emphasize that the CONSENT was read and explained to all participants who could not read or write, who, after agreeing, signed with the fingerprint of their thumb. Data collection from the participants included: 1) Sociodemographic characteristics: sex, ethnicity, reading and education level; 2) Behavioral habits: smoking, classification of smokers (light or moderate to heavy categories) [31], alcohol consumption, physical exercise, healthy diet (including weekly consumption of fish, nuts, fruits, vegetables) / bad diet (fried foods, soft drinks, sausages, among others); 3) Biological predictors: age, blood pressure, body mass index (BMI), waist/hip ratio (WHR) and personal physiological history (dyslipidemia, arterial hypertension - SAH, diabetes - DM, stroke - CVA, cardiovascular disease - CVD).
2.3. Data Analysis
Assuming that the development of CNCDs is multifactorial [1], which means that it can arise through different factors (eg, level of physical exercise, eating habits, smoking), the sample was divided by clustering, using the algorithm K-means clustering method that, through an unsupervised method, this algorithm learns how all the variables of a data set are related to each other by dividing the participants into different predetermined groups, which can help to discover different hidden patterns present in the data. This grouping occurs by minimizing the sum of squares of the distances between the data, and corresponds to the geometric center of a characteristic, called centroid [34].
Based on the hypothesis of the existence of an association between social factors, health and habits that have an impact on health, we suggest that there could be two profiles of people: the profile of low education or no studies, with bad health habits and worse health conditions; and the profile with opposite characteristics. Therefore, the K-means clustering algorithm was used to cluster the sample into two main groups [35].
For the construction of the model, 28 variables were used (2 sociodemographic variables, 17 biological variables and 9 behavioral variables). Orange Data Mining 2.27 software was used to determine the groups (Supplementary File).
We highlight that only two sociodemographic variables were inserted because there are biological variables (sex, age, and ethnicity) already evidenced in the literature as factors associated with sociodemographic level, so they were considered in the biological variables and not in the sociodemographic variable [4,36,37,38]. The variable “fish consumption” was emphasized since this food is rich in omega-3 fatty acids, which is a nutrient known to be associated with the prevention and protection of cardiovascular diseases [39]. On the other hand, the consumption of fish by the population studied may be a risk factor for mercury contamination, since it has been reported that many species of fish in the Xingu River have levels of methylmercury concentration (the organic form of the metal heavy mercury) far above what is tolerable by the human body and which has a high power of bioaccumulation along the food chain [40,41,42,43].
2.4. Statistical Analysis
Group characteristics were expressed as median and interquartile range, mean, standard deviation and proportions. For comparisons between groups, the Mann-Whitney and Chi-square tests were used, with Fisher and Yates corrections, and p-value<0.05 was adopted as significant. Residual adjustment >2 was adopted for significant categorical analyses.
Effect size was considered to support the importance of differences between groups. For continuous data, the interpretations followed the Cohen table (2013). For categorical data, effect sizes were observed through φ in 2x2 tables, assuming: “Null effect” for φ < 0.10, “Small effect” for φ < 0.30, “Moderate effect” for φ < 0.50 and “Large effect” for higher values. In tables > 2x2 the sizes were observed by Cramer's V whose interpretations of null, small, moderate and large effects were performed respecting the variations according to the increase in degrees of freedom [44,45].
The algorithm multilayer perceptron [46] was used to assess and classify the degree of importance of each variable in determining the groups. It is a supervised machine learning algorithm that, through artificial neural networks, can find non-linear patterns among different variables in a dataset and in response provides a prediction of some predetermined variable.
Only significant variables (p<0.05) were inserted in the input layer for the prediction of groups by K-means, of which four were biological, four behavioral and one sociodemographic. Numerical variables were rescaled at intervals between 0 and 1. The sample was randomly divided into two data sets, with 70.2% of the sample (n=60 individuals) used to train the algorithm and 29.8% used for the test (n=26 individuals). The architecture of the algorithm was automatically determined by the software, and the most adequate pattern to structure the neural network was the use of a neuron and a hidden layer. The activation function used in the hidden layer and output layer was Tangent Hyperbolic and Softmax, respectively. To minimize a possible effect of overfitting (a false response in the network), the algorithm was applied three times and the application chosen was the one with the lowest cross-entropy error, 0.026 (training sample) and 0.013 (test sample).
To calculate the importance of each variable in dividing the groups, a sensitivity analysis was performed based on the combined training and test samples, creating a table that displays the importance rating for each variable.
SPSS v.23 software was used for the evaluation procedures of the division of the groups.
3. Results
After dividing the sample composed of 86, the K-means algorithm defined two groups, group 1 composed of 47 individuals with major socio demographic vulnerability, with poor health habits and with worse health conditions, and group 2 composed of 39 individuals with profile of opposite characteristics.
Regarding the sociodemographic descriptors (Table 1), when the participants were asked about knowing how to read or not, 100% of the individuals in group 1 said they did not know how to read, while group 2 was the opposite, revealing approximately half of this population. As for education, 59% of individuals who reported not having studied belonged to group 1, in addition, 16 people reported having attended elementary school, however, they could not read. Among the individuals declared to be literate and who had attended elementary school (46.8%) or high school (10.6%), they were in group 2. Only one individual declared having graduated, however, this did not influence the groups among the riverside people. The effect size was highly significant (p<0.001) for reading and schooling, evidencing a low education profile or without studies. The other social criteria were not relevant between the groups (p>0.05).
Regarding the behavioral descriptors, it was observed that in group 1, people smoked for a longer period (0-15 years; Table 2). Characteristics such as the number of cigarettes smoked per day (Table 2) and the rate of smokers and former smokers (Table 3) did not influence the comparison between the groups. It is important to note that riverside dwellers who reported being smokers (7% of the population) were included in the "light" (≤10 cigarettes/day) or "moderate to heavy" (>10 cigarettes/day) categories.
As for the frequency of alcohol consumption (Table 2), people in group 2 consume alcohol more frequently on a weekly basis when compared to group 1 (p<0.05). However, of the individuals who consume alcoholic beverages, 42.6% are in group 2, representing double those belonging to group 1 (Table 3).
A percentage of 39.5% of the riverine people declared to practice physical exercises. The weekly frequency of physical exercise was lower in group 1 (0.0 times) than in group 2 (1.5 times) (p<0.01; Table 2).
Regarding the consumption of fish per week (Table 2), it was observed that they consume fish three to four times a week and that this frequency did not differ between the groups (p>0.05). There was no difference between the groups as to whether or not they had a healthy diet (Table 3). However, most riverside dwellers stated that they preferred a healthy diet, with 61.5% in group 1 and 70.2% in group 2 (Table 3).
Considering the lipid profile, even if the values are within the acceptable limit [47], the riverside people in group 2 tends a had lower values of total cholesterol and LDL when compared to group 1 (p<0.05; Table 2). The other biochemical tests, blood pressure measurement, WHR and physiological background (SAH, CVA, CVD) showed no differences between the groups (p>0.05). In addition, SAH was within the normal range, however, it was observed that the systolic blood pressure (SBP) was at the limit (SBP=130 mmHg) recommended by the Brazilian Society of Cardiology [47].
Although the WHR did not differ between the two groups, both presented values above the desired level (Table 2). Men had WHR≥0.90 cm and women ≥0.85 cm. The BMI of this population differed between the groups, where group 1 had higher values when compared to group 2 (p<0.05; Table 2), however, both groups were considered pre-obese according to the WHO [48]. Although SAH and DM did not differ between the groups, these variables had an average frequency of the population, in general 21.3% who reported SAH and 4.7% reported having DM and SAH.
The biological descriptors observed in the group 1, showed people of more advanced ages when compared to group 2, with a mean age of 55 years (49-62 years) (p<0.001; Table 2). Although age was significant, the effect size was small.
Thus, it was evidenced by the Multilayer Perceptron that of the most important variables, social factors such as reading (100%) and level of education (11.8%) were the factors that most influenced this study; then, behavioral descriptors such as smoking time (2.7%), total cholesterol (2.6%), alcohol frequency (2.3%) and others. Although age had an influence, the effect size was small, it has a lower importance (0.9%) in relation to the other variables, as shown in Figure 3.
4. Discussion
This study evaluated the relationship of sociodemographic, behavioral, and biological patterns in Amazonian riverine population of the middle Xingu River, in order to identify the factors that most influence your health' profile. We assume that this population has two riverine profiles, and our analyzes show that in fact there are two distinct groups: a group with low education and poor health, and another group with opposite characteristics. In addition, we found that the educational and social conditions together were the most relevant aspect for having a good health condition in this population.
We observed that all individuals in group 1 are illiterate, regardless of having attended elementary school or not, showing that the lack of reading may lead people to be unable to read or interpret, for example, a medication leaflet, tables of nutritional information present in processed and industrialized foods, and documents that may provide information on health education. The population's level of schooling was low, evidenced mainly in group 1 with 59.9% of the riverside people without education, and despite the other group having higher education, most have only elementary education. These data are particularly important since they are in agreement with other studies carried out in the Amazon in other regions of the world, where the low level of schooling is a risk factor that can influence the development of CNCDs and others diseases [28,49,50,51,52].
In this scenario, we believe that low schooling can make it difficult or impossible for the population studied to understand the importance of healthy lifestyles, such as, for example, a good diet (rich in fiber and nutrients), physical activity and reduced consumption of industrialized products, which are rich in salt, fats and high glycemic indexes. In fact, recently [53] found that the level of education can influence the dietary profile of the population of London, United Kingdom, in three ways: i) low education is linked to diets rich in carbohydrates and low in fiber ; ii) low education is also associated with higher consumption of sweets and red meat, and the high education is associated with higher consumption of fruits, vegetables and fish; and, iii) areas of high educational level have greater nutritional diversity, together with lower caloric intake. In Latin America, it was observed that the main factors that hinder the state of health literacy in this population are: socioeconomic inequality (e.g., low education), social/geographical isolation and cultural barriers, linguistic and political, which mainly affect indigenous and others living in areas rural populations [54]. Considering Brazilian Amazon populations, studies in riverside populations of the Pará (Tapajós River and Tucuruí Lake) and Amazonas (Negro River and Solimões River) states, demonstrate that the profile or status educational and bad habits (food and health) of riverine people, are risk factors for the development of metabolic syndrome and cardiometabolic diseases [22,28,49,55,56].
Regarding the smoking habit, the variable “Time of smoking” was the most influenced the study, especially in group 1, which was also considered to have poor health conditions. In riverside communities in the Amazon, smoking was associated with weight gain, development of DM2, onset of systemic arterial hypertension, metabolic syndrome and chronic kidney disease [57,58]. Although the harmful effects of smoking on the body and on the emergence of diseases are already widely known [59,60], the data reported here are particularly important, since it involves traditional populations that are historically neglected or excluded. of public health policies in Brazil.
Considering alcohol consumption, the results showed that the consumption of alcoholic beverages and educational qualifications (literate) belonged to group 2, corroborating previous studies that associate the existence of a higher consumption of alcohol among individuals with higher education [61,62,63,64]. In relation to the consumption of alcohol in riverside communities, it was reported that in riverside communities of Amazonas and Paraíba states it reaches 34.8% and 30.4%, respectively [57,65]. These studies corroborate our data, which pointed out that about 30% of riverside people are considered consumers. The level of education shapes social position and opportunities in life, promoting circumstances that favor alcohol consumption [66].
Contrary to previous studies on dyslipidemia in riverine and quilombola populations in the region [4,67], this study showed that the values for cholesterol and LDL were considered desirable for both groups of this population, however, group 2 presented relatively lower values, suggesting that a part of the population has healthier lifestyle habits than the other. Perhaps the limitations on access to processed foods, due to poverty and scarcity of financial resources, are an influencing factor [68,69,70].
Age, despite being significant, the effect size was small in relation to other sociodemographic and biological variables such as education and lipid profile, respectively, thus not influencing the health of riverine [71] . On the other hand, the level of knowledge and age may have a possible association, since the riverside people who had no education were in the same group as those who were older (group 1), as also demonstrated by Peres [72]. This may be mainly associated with the absence of educational programs in the past decades as well as financial difficulties, difficult access, and transportation [20].
The population studied presented a typical food profile of riverside populations in the Amazon region, in which riverine people reported having a good diet (natural food) based on vegetables, Brazil nuts, fruits and mainly fish, the latter item being consumed three to four times per week [56,73]. We highlight the “fish consumption” factor for two interesting aspects: i) an positive aspect, since there is a high concentration of unsaturated fats and omega-3 fatty acids in this food, which can substantially contribute to the prevention of cardiovascular diseases in this population, since this nutrient has been proven to prevent this disease [39,74]; and, ii) an negative aspect, since there is a strong possibility that this food is contaminated by methylmercury, which in turn can bioaccumulate in riverine people who consume them [40,41,42,43]. The contamination of the river waters and, consequently, the contamination of fish by this metal, may be because of the irregular dumping of mercury used in illegal gold mining that takes place along the river [40,75,76]. Indeed, Souza-Araujo and collaborators (2022) [43] identified fish contamination and mercury biomagnication in food webs in the Belo Monte Hydroelectric Power Plant rebaratnaoegion, in the middle Xingu River, Pará state. Recent studies have reported mercury contamination of traditional (e.g., riverine and indigenous) and urban communities in the lower Tapajós basin and in the Tucurí Lake influence area, Pará state [41,42,77]. Therefore, it is possible that the population studied may be at risk of methylmercury contamination, since they may be consuming contaminated fish.
We observed that a large part of the population studied had blood pressure within the limits of what is recommended by the Brazilian Cardiology Medical Society [47]. This condition may be associated with possible mercury exposition, since concentrations of this metal in the bloodstream are positively associated with blood pressure, hypertension and other cardiovascular diseases. In addition, the exposure dose is an important factor in determining the effects on hypertension [78,79,80].
Despite these results, the riverside population of the current survey reported having some of the NCDs, such as SAH and DM. Even not influencing the study, these variables presented a average frequency of the general population of 21.3% reported to have SAH and 4.7% declared to have DM and SAH. Studies carried out in riverside communities in the interior of Amazonas show a higher prevalence of SAH (30.7%) and DM (8.9%), whereas in the interior of Pará, 20.47% reported being hypertensive and 4.13% reported having diabetes, such prevalence corroborate with our studies [57,81].
Regarding the frequency of physical exercises per week, a low frequency of exercise was evidenced in both groups and less than half of the population is practitioner. Such results confront the idea that populations residing in rural areas have higher levels of physical activity, which is most often represented by walking [82,83,84]. Although it is not possible to say, it is possible that the National Policy for the Comprehensive Health of Rural and Forest Populations [18] can be an inducer for greater attention to these populations with the objective of encouraging physical activities and thus reducing the prevalence of CNCDs [85,86].
Anthropometric indicators showed that BMI and WHR presented values above the expected in both groups evaluated, as well as in both sexes, considered pre-obese for BMI and high risk for metabolic complications for WHR, suggesting an excess of intra-abdominal adipose tissue, as also evidenced by other studies [48,87,88]. According to Pereira et al. [89], the WHR has a greater predictive capacity of hypertension, allowing greater discrimination of individuals at risk of chronic diseases. However, BMI and WHR were not determining predictors among the risk factors for classifying the importance of quantitative variables in the present study, thus not indicating a possible association with CNCDs.
In this sense, public policies should be worked on with these riverside populations, which lack medical care. As the study carried out by Machado et al. [21], with riverside populations of the lower Madeira in Rondônia, using telemedicine as a technological resource for health promotion and prevention and developing the population's responsibility for a better quality of life in the region.
The Brazilian educational system does not have public policies of national scope aimed specifically for the traditional populations (e.g., indigenous, riverine, quilombolas, etc.), so the only program that exists does not meet the breadth of distribution of these populations in the national territory. For example, the government of the state of Pará launched the program “Modular Education Organization”, which is regulated by law no. 7,806 of April 29, 2014, and that aims to bring education and literacy to traditional populations and the interior of the state. However, although this program has significantly contributed to the schooling of approximately 36,000 students from 465 locations in the interior of the state [90], it is still limited and cannot serve more distant and isolated communities such as the population of the region around the middle Xingu River, from so that this population remains unassisted by public education policies. Therefore, given the importance of education for the critical understanding of individuals regarding their social context, robust public policies for schooling and health education (in cooperation with states, municipalities and the federal government), are essential to mitigate the impact of this factor on the quality of life and health of traditional populations.
In general, this study was able to confirm the hypotheses based on the literature that an individual without study and with a lower level of education, probably will not have knowledge and information about how harmful certain behaviors are and therefore will not change them and as a result will have worse health indicators. Only alcohol intake showed a different pattern from the other factors, since its influence could be observed within the best level of education, probably because education provides better social conditions and opportunities, favoring this consumption. Finally, healthy eating, mainly due to the high consumption of fish, was considered a positive criterion for the health of riverside dwellers.
The riverside population studied has an important peculiarity, which is its relative geographic isolation, since this population is surrounded by numerous waterfalls in the middle Xingu River, which makes navigation in this region difficult. In addition, with the installation of the Belo Monte Hydroelectric Power Plant, many families who lived in influence of the dam (e. g., “Volta Grande” of the Xingu River region) lost their land and were “relocated” to another region, so that the local riverine population was reduced. This region is also an area of intense conflict with political disputes, illegal gold mining and deforestation [5,17,75]. Therefore, the difficult access to the collection site, high financial cost for the study and the population size profile of the studied community (considered small and dispersed along of the middle Xingu River, may have hindered the adherence and participation of a greater number of riverine people in the survey. However, we believe that the sampling effort did not affect our results, which are in agreement with other studies that analyzed small or large Amazonian riverside communities.
Finally, although this study brings relevant results, especially regarding to the degree of importance of health indicators, the research had some limitations, such as the experimental design, which has a transversal characteristic. Studies more longitudinal are needed to better understand how the population would behave if there was an intervention and monitoring by health professionals in relation to the most important variable: education. Could it be that by encouraging and intervening in education, in a positive way, the other indicators would also improve? Another limitation was that the procedure was not laboratory, the process was not systematized and controlled, despite this, the study valued a view of the subject in a real environment.
5. Conclusions
It can be concluded that there are two patterns in the riverside community, being a pattern of people with low education, with longer exposure to cigarettes and low frequency of physical exercise, factors that can be considered as risk factors for cardiovascular diseases and diabetes in this population and consequently, can affect your health. And the other pattern has opposite characteristics, being considered healthier. On the other hand, food, mainly due to the high consumption of fish, was considered a positive criterion for the health of riverside dwellers in both groups.
This is the first study in this population, which has important peculiarities that distinguish it from other Amazonian riverine populations. Finally, the most important variables for determining these groups were sociodemographic (education), behavioral (smoking and weekly alcohol consumption) and health (cholesterol).
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
conception, planning, analysis, interpretation, and writing: D. L. J.; R. S.; F. N. V. Interpretation, writing and critical review of the manuscript: A. L. P.; O. S. S.; Y. M. I. Writing, final revision, formatting, and translation: M. C. F. P. All authors have read and agreed to the published version of the manuscript.
Funding
We are grateful to PROPESP/UFPA (PAPQ) for funding the article publication fee.
Institutional Review Board Statement
“The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Tropical Medicine Center at the Federal University of Pará (Assent No. 3,678,493), in compliance with the Resolutions 441/2011/CNS e 466/2012/MS.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We thank the Study and Research Groups on Health and Education in the Amazon – GEPSEA and on Planetary Health in the Amazon - GESPA.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Brasil, M.S. Guidelines for the care of people with chronic diseases in health care networks and in priority lines of care. Health Care Department. Department of Primary Care. Brasilia: Ministry of Health Brasilia; 2013. Available in: https://bvsms.saude.gov.br/bvs/publicacoes/diretrizes%20_cuidado_pessoas%20_doencas_cronicas.pdf (accessed Jan 15, 2021).
- GBD. Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016, 388(10053), 1659-724.
- Singhal, A. The global epidemic of noncommunicable disease: the role of early-life factors. J International nutrition: achieving millennium goals beyond, 2014; 78, 123–132. [Google Scholar] [CrossRef]
- Oliveira B.F.A., Mourão D.S., Gomes N., Costa J.M.C., Souza A.V., Bastos W.R., Fonseca M.F., Mariani C.F., Abbad G., Hacon S.S. Prevalence of arterial hypertension in riverside communities on the Madeira River, Western Brazilian Amazon. J Cadernos de Saude Publica. 2013, 29(8), 1617-30. [CrossRef]
- Magalhães S.B., Cunha M.C. Study on the compulsory displacement of riverside dwellers in Belo Monte: SBPC report: São Paulo: SBPC, 2017; 448 p. Available in: http://portal.sbpcnet.org.br/publicacoes/a-expulsao-de-ribeirinhos-em-belo-monte-relatorio-da-sbpc/ (accessed nov 01, 2022).
- Arrifano G.P.F., Martin-Doimeadios R.D.C.R., Jiménez-Moreno M., Augusto-Oliveira M., Souza-Monteiro J.R., Paraense R., Machado C.R., Farina M., Macchi B., Do Nascimento J.L.M. Assessing mercury intoxication in isolated/remote populations: Increased S100B mRNA in blood in exposed riverine inhabitants of the Amazon. J Neurotoxicology. 2018, 68, 151-8. [CrossRef]
- Santos Sousa, I. , Sousa F.C., Sousa R.M.S. Living condition and water and sanitary situation in communities in the sphere of incluence of the gas pipeline Coari-Manaus in Macacapuru, state of Amazon, Brazil. J Hygeia-Revista Brasileira de Geografia Médica e da Saúde. 2009, 5(9), 88-98.
- Franco, E.C. , Santo C.E., Arakawa A.M., Xavier A., França M.d.L., De Oliveira A.N., Machado M.A.M.P., Bastos R.S., Bastos J.R.M., Caldana M.L. Health promotion on amazonic riverside population: experience report. J Revista CEFAC 2015, 17, 1521–1530. [Google Scholar] [CrossRef]
- Gama A.S.M., Fernandes T.G., Parente R.C.P., Secoli S.R. Health survey in riverside communities in Amazonas, Brazil. J Cadernos de Saúde Pública. 2018, 34(2), e00002817. [CrossRef]
- Hacon, S.S. , Dórea J.G., Fonseca M.F., Oliveira B.A., Mourão D.S., Ruiz C., Gonçalves R.A., Mariani C.F., Bastos W.R. The influence of changes in lifestyle and mercury exposure in riverine populations of the Madeira River (Amazon Basin) near a hydroelectric project. J International journal of environmental research public health. 2014, 11(3), 2437-55. [CrossRef]
- Katsuragawa, T.H. , Gil L.H.S., Tada M.S., Silva L.H.P. Endemic and epidemic diseases in Amazonia: Malaria and other emerging diseases in riverine areas of the Madeira River. A school case. J Estudos Avançados. 2008, 22(64), 111-41. Available in: https://www.scielo.br/j/ea/a/zcDwWg3XwwQWhCVR8vCLH3s/?lang=en&format=pdf.
- De Francesco, A. , Carneirom C. Atlas of the impacts of HPP Belo Monte on fisheries. São Paulo: Socio-environmental Institute; 2015. Available in: https://ox.socioambiental.org/sites/default/files/ficha-tecnica/node/202/edit/2018-06/atlas-pesca-bm.pdf (accessed Jun 21, 2021).
- Silveira, M. The implementation of hydroelectric plants in the Brazilian Amazon, socio-environmental and health impacts with the transformations in the territory: the case of the Belo Monte HPP [PhD in Geography]. University of Brasilia, Brasilia, 2016. Available in: https://repositorio.unb.br/handle/10482/20534 (accessed Jun 05, 2021).
- Gonçalves, A.C.O. , Cornetta A., Alves F., Barbosa L.J.G. Belém and Abaetetuba. In: The socio-environmental function of the Union's heritage in the Amazon, Alves F, editor, Brasília: Instituto de Pesquisa Econômica Aplicada (Ipea): 2016; p. 359. Available in: http://repositorio.ipea.gov.br/handle/11058/6619.
- Lucas, E.W.M. , De Sousa F.A.S., Dos Santos F.D.S., Rocha-Júnior R.L., Pinto D.D.C., Da Silva V.P.R. Trends in climate extreme indices assessed in the Xingu river basin-Brazilian Amazon. J Weather Climate Extremes. 2021, 31, 100306. [CrossRef]
- Siqueira, J.M. , Dal’Asta A.P., Amaral S., Escada M.I.S., Monteiro A.M.V. The Middle and Lower Xingu: the response to the crystallization of different temporalities in the production of regional space. J Revista Brasileira de Estudos Urbanos e Regionais. 2017, 19(1), 148-63. [CrossRef]
- Weißermel, S. Towards a conceptual understanding of dispossession–Belo Monte and the precarization of the riverine people. J Novos Cadernos NAEA. 2020, 23, 11–34. [Google Scholar] [CrossRef]
- Brasil, M.S. The National Policy for the Comprehensive Health of rural, forest and water populations and the environment. Support for Participatory Management (DAGEP) Brasília: Ministry of Health; 2015. Available in: https://www.arca.fiocruz.br/bitstream/icict/42147/2/Cap_A%20Pol%C3%ADtica%20Nacional%20de%20Sa%C3%BAde%20Integral%20das%20Popula%C3%A7%C3%B5es%20do.pdf (accessed 14 jan 2022).
- Pontes, F.A.R. , Silva S.S.d.C., Bucher-Maluschke J.S., Reis D.C.d., Silva S.D.B.d. The ecological engagement in the context of an Amazon river Village. J Interamerican Journal of Psychology. 2008, 42(1), 1-10.
- De Rodrigues, L.R. Accessibility in the modular teaching organization system in elementary schools in riverside communities in the municipality of Abaetetuba. J Brazilian Journal of Development. 2020, 6(3), 13147-61. [CrossRef]
- Machado, F.S.N. , de Carvalho M.A.P., Mataresi A., Mendonça E.T., Cardoso L.M., Yogi M.S., Rigato H.M., Salazar M. Use of telemedicine technology as a strategy to promote health care of riverside communities in the Amazon: experience with interdisciplinary work, integrating NHS guidelines. J Ciencia saude coletiva. 2010, 15(1), 247-54. [CrossRef]
- Arrifano, G.P. , Alvarez-Leite J.I., Macchi B.M., Campos N.F., Augusto-Oliveira M., Santos-Sacramento L., Lopes-Araújo A., Souza-Monteiro J.R., Alburquerque-Santos R., Do Nascimento J.L.M. Living in the southern hemisphere: metabolic syndrome and its components in Amazonian riverine populations. J Journal of clinical medicine. 2021, 10(16), 3630. [CrossRef]
- Anjana, R.M. , Baskar V., Nair A.T.N., Jebarani S., Siddiqui M.K., Pradeepa R., Unnikrishnan R., Palmer C., Pearson E., Mohan V., et al. Novel subgroups of type 2 diabetes and their association with microvascular outcomes in an Asian Indian population: a data-driven cluster analysis: the INSPIRED study. J BMJ Open Diabetes Research. 2020, 8(1), e001506. [CrossRef]
- Hillesheim, E. , Ryan M.F., Gibney E., Roche H.M., Brennan L., metabolism. Optimisation of a metabotype approach to deliver targeted dietary advice. J Nutrition. 2020, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tallman, D.A. , Latifi E., Kaur D., Sulaheen A., Ikizler T.A., Chinna K., Mat Daud Z.A., Karupaiah T., Khosla P. Dietary patterns and health outcomes among African American maintenance hemodialysis patients. J Nutrients. 2020, 12, 797. [Google Scholar] [CrossRef] [PubMed]
- Ryan, T.P. Sample size determination and power: John Wiley & Sons, 2013; 1118439228. 400 p.
- Yamane, T. Statistics, An Introductory Analysis, 1967: J New York Harper Row CO. USA, 1967; 919 p.
- Cabral, M.M. , Venticinque E.M., Rosas F.C.W. Perception of riverine people in relation to the performance and management of two distinct categories of protected areas in the Brazilian Amazon. J Biodiversidade Brasileira-BioBrasil. 2014, 1, 199-210.
- Feio, C.M.A. , Fonseca F.A., Rego S.S., Feio M.N., Elias M.C., Costa E.A., Izar M.C., Paola Â.A., Carvalho A.C. Lipid profile and cardiovascular risk in Amazonians. Arq Bras Cardiol. 2003, 81(6), 592-5. Available in: https://www.scielo.br/j/abc/a/kcz8gg3kBQQWJyLFbrWKFKw/?format=pdf&lang=pt.
- Murrieta, R.S.S. Dialectic of flavor: food, ecology and daily life in riverside communities on the island of Ituqui, Baixo Amazonas, Pará. J Revista Antropologia. 2001, 44, 39–88. [Google Scholar] [CrossRef]
- Pulvers, K. , Scheuermann T.S., Romero D.R., Basora B., Luo X., Ahluwalia J.S. Classifying a smoker scale in adult daily and nondaily smokers. J nicotine tobacco research. 2014, 16(5), 591-9. [CrossRef]
- SBAC. Brazilian Consensus for the Standardization of Laboratory Determination of Lipid Profile. Brazilian Society of Clinical Analysis; 2016. Available in: https://www.sbac.org.br/blog/2016/12/10/consenso-brasileiro-para-a-normatizacao-da-determinacao-laboratorial-do-per%EF%AC%81l-lipidico/ (accessed abr 27, 2021).
- SBD. Guidelines of the Brazilian Society of Diabetes 2017-2018. Brazilian Society of Diabetes: Publisher Clannad, São Paulo; 2017. Available in: https://edisciplinas.usp.br/pluginfile.php/4925460/mod_resource/content/1/diretrizes-sbd-2017-2018.pdf (accessed abr 20, 2021).
- Teknomo, K. K-means clustering tutorials 2007. Available from: http://sigitwidiyanto.staff.gunadarma.ac.id/Downloads/files/38034/M8-NotekMeans (acessed mai 05, 2021).
- Mahmoud, P. K-Means Clustering - Data Algorithms: O´Reilly Media, Inc., 1005 Gravenstein Highway North, Sebastopol, CA 95472, 2015; 725 p.
- Chatterji, P. , Joo H., Lahiri K. Racial/ethnic-and education-related disparities in the control of risk factors for cardiovascular disease among individuals with diabetes. J Diabetes Care. 2012, 35(2), 305-12. [CrossRef] [PubMed]
- Machado, P.A.N. , Sichieri R. Waist-hip ratio and dietary factors in adults. J Revista Saúde Pública. 2002, 36, 198-204. [CrossRef]
- Merz, C.N.B. , Ramineni T., Leong D. Sex-specific risk factors for cardiovascular disease in women-making cardiovascular disease real. J Current opinion in cardiology. 2018, 33, 500–5. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.U. , Lone A.N., Khan M.S., Virani S.S., Blumenthal R.S., Nasir K., Miller M., Michos E.D., Ballantyne C.M., Boden W.E. Effect of omega-3 fatty acids on cardiovascular outcomes: A systematic review and meta-analysis. J EClinicalMedicine 2021, 38, 100997. [Google Scholar]
- Santos-Sacramento, L. , Arrifano G.P., Lopes-Araújo A., Augusto-Oliveira M., Albuquerque-Santos R., Takeda P.Y., Souza-Monteiro J.R., Macchi B.M., do Nascimento J.L.M., Lima R.R. Human neurotoxicity of mercury in the Amazon: A scoping review with insights and critical considerations. J Ecotoxicology environmental safety 2021, 208, 111686. [Google Scholar] [CrossRef] [PubMed]
- Basta, P.C. , Viana P.V.d.S., Vasconcellos A.C.S.d., Périssé A.R.S., Hofer C.B., Paiva N.S., Kempton J.W., Ciampi de Andrade D., Oliveira R.A.A.d., Achatz R.W. Mercury exposure in Munduruku indigenous communities from Brazilian Amazon: Methodological background and an overview of the principal results. J International Journal of Environmental Research Public Health 2021, 18, 9222. [Google Scholar] [CrossRef] [PubMed]
- Meneses, H.N.M. , Oliveira-da-Costa M., Basta P.C., Morais C.G., Pereira R.J.B., De Souza S.M.S., Hacon S.S. Mercury contamination: a growing threat to riverine and urban communities in the Brazilian Amazon. J International Journal of Environmental Research Public Health 2022, 19, 2816. [Google Scholar] [CrossRef] [PubMed]
- Souza-Araujo, J. , Andrades R., Hauser-Davis R., Lima M., Giarrizzo T. Before the Dam: A Fish-Mercury Contamination Baseline Survey at the Xingu River, Amazon Basin Before the Belo Monte Dam. J Bulletin of Environmental Contamination Toxicology 2022, 108, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical power analysis for the behavioral sciences. 2 rd ed: Academic press, 2013; 1483276481. 579 p.
- Fritz, C.O. , Morris P.E., Richler J.J. Effect size estimates: current use, calculations, and interpretation. J Journal of experimental psychology: General. 2012, 141(1), 2-18. [CrossRef]
- Russell S., Norvig P. Artificial intelligence: a modern approach. 3rd ed: Upper Saddle River (NJ): Prentice Hall Press, 2010; 9780132071482. 1132 p.
- SBC. Brazilian Society of Cardiology - 7th Brazilian Guideline on Arterial Hypertension. Arquivos Brasileiros Cardiologia. 2016, 107(3), 1-103. Available in: http://publicacoes.cardiol.br/2014/diretrizes/2016/05_HIPERTENSAO_ARTERIAL.pdf.
- WHO. Waist circumference and waist–hip ratio: report of a WHO expert consultation. World Health Organization - Geneva; 2008. Available in: https://apps.who.int/iris/bitstream/handle/10665/44583/9789241501491_eng.pdf;jsessionid=2BE502B0C60142042631C73640261857?sequence=1 (accessed jan 15, 2022).
- Mariosa, D.F. , Ferraz R.R.N., Santos-Silva E.N. Influence of socio-environmental conditions on the prevalence of systemic arterial hypertension in two riverside communities in the Amazon, Brazil. J Ciência Saúde Coletiva 2018, 23, 1425–1436. [Google Scholar] [CrossRef] [PubMed]
- Ohlsson, A. , Eckerdal N., Lindahl B., Hanning M., Westerling R. Non-employment and low educational level as risk factors for inequitable treatment and mortality in heart failure: a population-based cohort study of register data. J BMC public health. 2021, 21(1), 1-12. [CrossRef]
- Rarau, P. , Pulford J., Gouda H., Phuanukoonon S., Bullen C., Scragg R., Pham B.N., McPake B., Oldenburg B. Socio-economic status and behavioural and cardiovascular risk factors in Papua New Guinea: A cross-sectional survey. J PloS one. 2019, 14(1), e0211068. [CrossRef]
- Rosengren, A. , Smyth A., Rangarajan S., Ramasundarahettige C., Bangdiwala S.I., AlHabib K.F., Avezum A., Boström K.B., Chifamba J., Gulec S. Socioeconomic status and risk of cardiovascular disease in 20 low-income, middle-income, and high-income countries: the Prospective Urban Rural Epidemiologic (PURE) study. J The Lancet Global Health. 2019, 7(6), e748-e60. [CrossRef]
- Fard, N.A. , Morales G.F., Mejova Y., Schifanella R. On the interplay between educational attainment and nutrition: a spatially-aware perspective. J EPJ Data Science. 2021, 10(1), 18. [CrossRef]
- Arrighi, E. , Ruiz de Castilla E., Peres F., Mejía R., Sørensen K., Gunther C., Lopez R., Myers L., Quijada J., Vichnin M. Scoping health literacy in Latin America. J Global Health Promotion. 2022, 29(2), 78-87. [CrossRef]
- De Azevedo, P.L. , Freitas S.R.S. Prevalence of major cardiometabolic diseases in the riverine populations from the interior of the State of Amazonas, Brazil. J Acta Scientiarum Health Sciences. 2018, 40. [CrossRef]
- Machado, C.L.R. , Crespo-Lopez M.E., Augusto-Oliveira M., Arrifano G.P., Macchi B.M., Lopes-Araújo A., Santos-Sacramento L., Souza-Monteiro J.R., Alvarez-Leite J.I., De Souza C.B.A. Eating in the Amazon: nutritional status of the riverine populations and possible nudge interventions. J Foods. 2021, 10(5), 1015. [CrossRef]
- Azevedo, P.L. Prevalence of the main chronic non-communicable diseases in riverside populations in the interior of Amazonas [Course Conclusion Paper]. State University of Amazonas, Manaus, 2017. Available in: http://repositorioinstitucional.uea.edu.br/handle/riuea/523 (accessed jan 15, 2022).
- Relvas, A. , Camargo J., Basano S., Camargo L.M.A., Development. Prevalence of chronic noncommunicable diseases and their associated factors in adults over 39 years in riverside population in the western Brazilian amazon region. J Journal of Human Growth. 2022, 32, 55–63. [Google Scholar] [CrossRef]
- Omare, M.O. , Kibet J.K., Cherutoi J.K., Kengara F.O. A review of tobacco abuse and its epidemiological consequences. J Journal of Public Health. 2021, 1–16. [Google Scholar] [CrossRef]
- Larsson, S.C. , Burgess S. Appraising the causal role of smoking in multiple diseases: A systematic review and meta-analysis of Mendelian randomization studies. J EBioMedicine 2022, 82, 104154. [Google Scholar] [CrossRef]
- Huerta, M.C. , Borgonovi F. Education, alcohol use and abuse among young adults in Britain. J Social science & Medicine. 2010, 71(1), 143-51. [CrossRef]
- Jefferis, B. , Manor O., Power C. Cognitive development in childhood and drinking behaviour over two decades in adulthood. J Journal of Epidemiology Community Health. 2008, 62, 506–12. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.E.S. , Helman B., Luz e Silva D.C., Aquino É.C., Freitas P.C., Santos R.O., Brito V.C.A., Garcia L.P., Sardinha L.M.V. Prevalence of heavy episodic drinking in the Brazilian adult population: National Health Survey 2013 and 2019. J Epidemiologia e Serviços de Saúde. 2022, 31. [CrossRef]
- Plens, J.A. , Valente J.Y., Mari J.J., Ferrari G., Sanchez Z.M., Rezende L.F. Patterns of alcohol consumption in Brazilian adults. J Scientific reports. 2022, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, W.P. , Caetano K.A.A., Brandão G.C.G., Freire M.E.M., Reis R.K., Oliveira e Silva A.C. Harmful alcohol consumption and associated factors in riverine communities. 2022. 2022. [Google Scholar] [CrossRef]
- Macinko, J. , Mullachery P., Silver D., Jimenez G., Neto O.L.M. Patterns of alcohol consumption and related behaviors in Brazil: Evidence from the 2013 National Health Survey (PNS 2013). J PLoS one. 2015, 10(7), e0134153. [CrossRef]
- Sales, F.M.A.M. , Silva L.M.C., Oliveira A.P.P., Reis R.C., Guerreiro J.F. Risk of excess weight/body fat and dyslipidemia associated with hemoglobin A2 levels. Revista Paraense de Medicina. 2014, 28(4), 57-64.
- Adams, C. , Murrieta R., Neves W.A. Amazonian caboclo societies: modernity and invisibility: Annablume, 2006; 8574196444. 364 p. São Paulo.
- Tomita, L.Y. , Cardoso M.A. Assessment of the food list and serving size of a Food Frequency Questionnaire in an adult population. J Cadernos de Saúde Pública, 2002; 18, 1747–1756. [Google Scholar] [CrossRef]
- Silva, A.L. , Begossi A. Biodiversity, food consumption and ecological niche dimension: a study case of the riverine populations from the Rio Negro, Amazonia, Brazil. J Environment, Development Sustainability. 2009, 11(3), 489-507. [CrossRef]
- Nyberg, S.T. , Singh-Manoux A., Pentti J., Madsen I.E., Sabia S., Alfredsson L., Bjorner J.B., Borritz M., Burr H., Goldberg M. Association of healthy lifestyle with years lived without major chronic diseases. J JAMA internal medicine. 2020, 180(5), 760-8. [CrossRef]
- Peres, M.A.C. Old age and illiteracy, a paradoxical relationship: educational exclusion in rural contexts in the Northeast region. J Sociedade e estado. 2011, 26, 631–662. [Google Scholar] [CrossRef]
- Vasquez-Rojas, W.V. , Martín D., Miralles B., Recio I., Fornari T., Cano M.P. Composition of Brazil Nut (Bertholletia excels HBK), Its Beverage and By-Products: A Healthy Food and Potential Source of Ingredients. J Foods. 2021, 10(12), 3007. [CrossRef]
- Matos, Â.P. , Matos A.C., Moecke E.H.S. Polyunsaturated fatty acids and nutritional quality of five freshwater fish species cultivated in the western region of Santa Catarina, Brazil. J Brazilian Journal of Food Technology 2019, 22, e2018193. [Google Scholar] [CrossRef]
- Mataveli, G. , Chaves M., Guerrero J., Escobar-Silva E.V., Conceição K., De Oliveira G. Mining Is a Growing Threat within Indigenous Lands of the Brazilian Amazon. J Remote Sensing. 2022, 14(16), 4092. [CrossRef]
- Azevedo-Santos, V.M. , Arcifa M.S., Brito M.F., Agostinho A.A., Hughes R.M., Vitule J.R., Simberloff D., Olden J.D., Pelicice F.M. Negative impacts of mining on Neotropical freshwater fishes. J Neotropical Ichthyology. 2021, 19. [Google Scholar] [CrossRef]
- Arrifano, G.P. , Martín-Doimeadios R.C.R., Jiménez-Moreno M., Ramírez-Mateos V., da Silva N.F., Souza-Monteiro J.R., Augusto-Oliveira M., Paraense R.S., Macchi B.M., Do Nascimento J.L.M. Large-scale projects in the amazon and human exposure to mercury: The case-study of the Tucuruí Dam. J Ecotoxicology environmental safety. 2018, 147, 299-305. [CrossRef]
- Hu, X.F. , Singh K., Chan H.M. Mercury exposure, blood pressure, and hypertension: A systematic review and dose–response meta-analysis. J Environmental health perspectives. 2018, 126(07), 076002. 0760. [Google Scholar] [CrossRef]
- Yan, J. , Pan Y., Tang Z., Song Y. Mercury poisoning presenting with hypertension: report of 2 cases. J The American Journal of Medicine. 2019, 132(12), 1475-7. [CrossRef]
- Hu, X.F. , Lowe M., Chan H.M. Mercury exposure, cardiovascular disease, and mortality: A systematic review and dose-response meta-analysis. J Environmental research. 2021, 193, 110538. [CrossRef]
- Rocha, J.P.S. , Lopes I.S.S., Henriques C.E.L., Minekawa T.B., Bastos M.S.C.B.O., editors. Katuana from Baía do Guajará: diabetes and self-reported arterial hypertension in a riverside population of Combú. III Congress on Health Education in the Amazon (COESA); 2014; Federal University of Pará, Pará, Brazil.
- Rodrigues, D.N. , Mussi R.F.d.F., Almeida C.B.d., Nascimento Junior J.R.A., Moreira S.R., Carvalho F.O. Sociodemographic determinants associated with the level of physical activity of Bahian quilombolas, 2016 survey. J Epidemiologia e Serviços de Saúde 2020, 29, e2018511. [Google Scholar] [CrossRef]
- Wanzeler, F.S.d.C. Physical activity and associated factors in riverside adolescents in the Amazon [Master’s Degree]. University of Brasilia, Brasília, 2017. Available in: https://repositorio.unb.br/handle/10482/24652 ((accessed jan 15, 2021).
- Wanzeler, F.S.d.C. , Nogueira J.A.D. Physical activity in rural populations of Brazil: a review of literature. Revista Brasileira de Ciência e Movimento. 2019, 27(4), 228-40.
- Cercato, C. , Mancini M.C., Arguello A.M.C., Passos V.Q., Villares S.M.F., Halpern A. Systemic hypertension, diabetes mellitus, and dyslipidemia in relation to body mass index: evaluation of a Brazilian population. J Revista do Hospital das Clínicas. 2004, 59(3), 113-8. [CrossRef]
- Costa-Font, J. , Gil J., Biology H. Obesity and the incidence of chronic diseases in Spain: a seemingly unrelated probit approach. Economics & Human Biology. 2005, 3(2), 188-214. [CrossRef]
- Brasil, M.S. Protocols of the Food and Nutrition Surveillance System - SISVAN in health care. Primary Care, Health Care Secretariat. Brasília: Ministry of Health; 2008. Available in: http://189.28.128.100/dab/docs/portaldab/publicacoes/protocolo_sisvan.pdf (accessed fev 10, 2022).
- de Araújo, I.M. , Antunes Paes N. Quality of anthropometric data of hypertensive users seen at the family health program and its correlation with risk factors. Texto & Contexto Enfermagem. 2013, 22(4), 1030-40.
- Pereira, R.A. , Sichieri R., Marins V.M. Razão cintura/quadril como preditor de hipertensão arterial. J Cadernos de Saúde Pública. 1999, 15, 333-44. Available in: https://www.scielo.br/j/csp/a/QL4w8KBLPPh9sTds769ZS9g/?lang=pt&format=pdf.
- Rodrigues, J.M.P. , Da Silva G.P. The Modular Teaching Organization System (MTOS) from the perspective of graduates in the municipality of Breves - Pará. J Revista Brasileira de Educação do Campo. 2018, 3(1), 260-86. [CrossRef]
Figure 1.
Location of the Espelho communities in middle Xingu River.
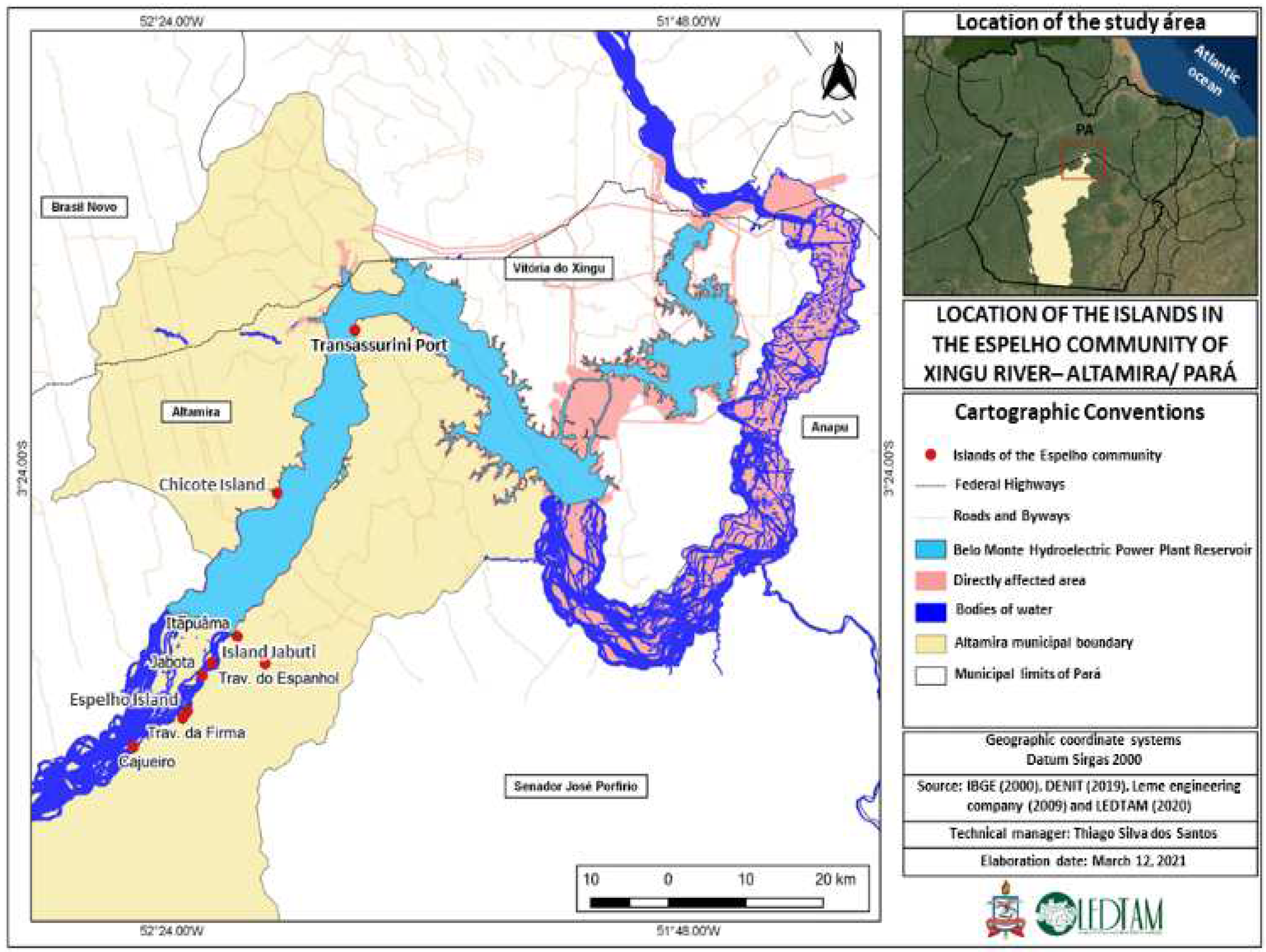
Figure 2.
Flowchart of service on the day of the action.
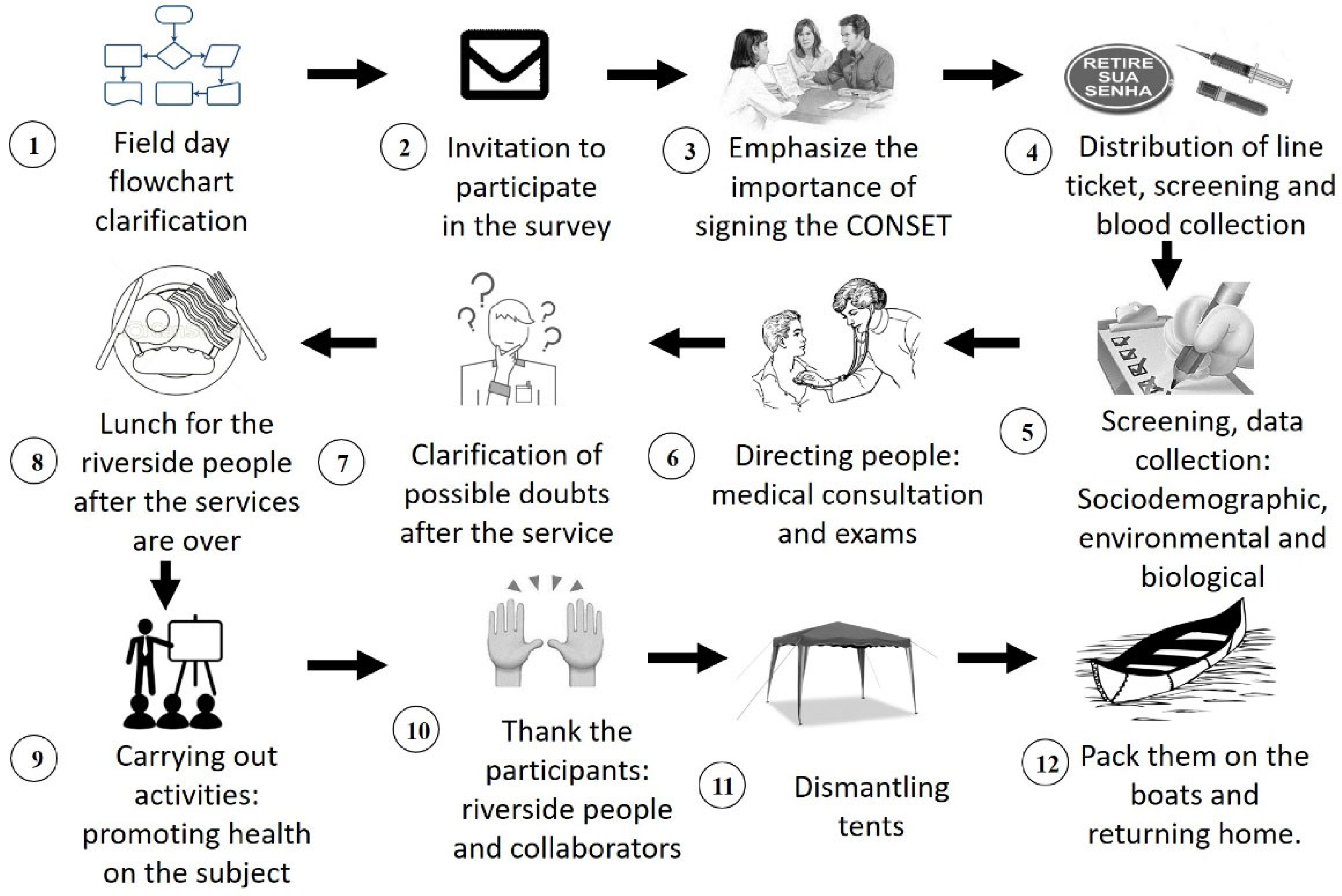
Figure 3.
Ranking of importance of quantitative variables rescaled in intervals between 0 and 1, showing the degree of importance of the variables (from highest to lowest). Personal source.
Figure 3.
Ranking of importance of quantitative variables rescaled in intervals between 0 and 1, showing the degree of importance of the variables (from highest to lowest). Personal source.
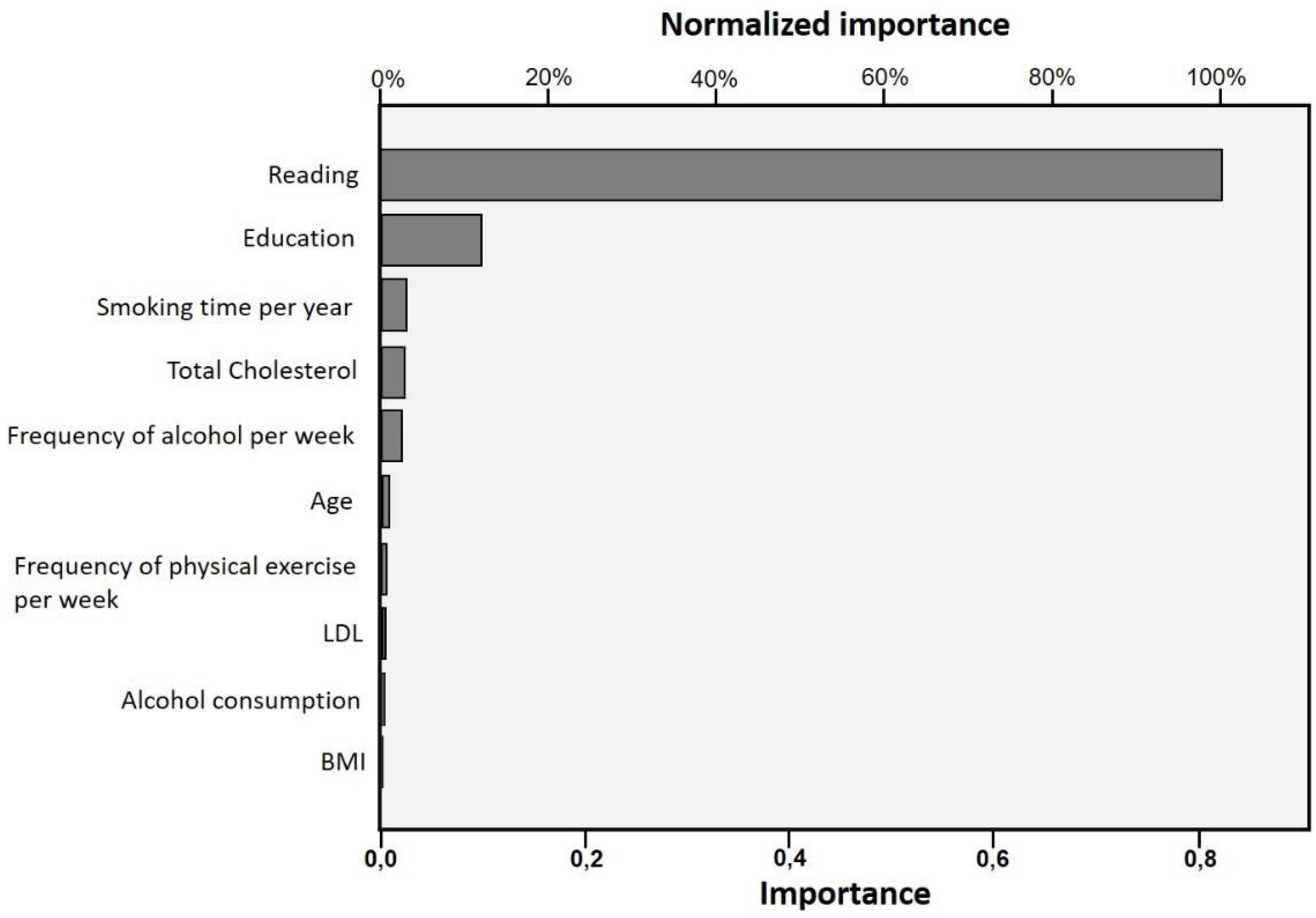

Table 1.
Categorical data on the sociodemographic profile of the riverside population of Group 1 and Group 2 in the Xingu River region.
Table 1.
Categorical data on the sociodemographic profile of the riverside population of Group 1 and Group 2 in the Xingu River region.
| Descriptors | Group 1 n=39 |
Group 2 n=47 |
Effect size |
p |
|---|---|---|---|---|
| SOCIODEMOGRAPHIC | ||||
| Sex | F = 51.3% | F = 48.9% | Φ = 0.02 | 0.83 |
| M = 48.7% | M = 51.1% | |||
| Ethnicity | ||||
| Asian | 2.6% | 4.3% | V = 0.23++ | 0.35 |
| White | 17.9% | 21.3% | ||
| Indigenous | 2.6% | 6.4% | ||
| Mixed race | 43.6% | 53.2% | ||
| Black | 33.3% | 14.9% | ||
| Education | ||||
| No education | 59.0% a | 0.0% a | V = 0.77+++ | < 0.001*** |
| Initial Elementary School | 41.0% | 40.5% | ||
| Final Elementary School | 0.0% b | 46.8% b | ||
| High School | 0.0% c | 10.6% c | ||
| University graduate | 0.0% | 2.1% | ||
| Reading | ||||
| No | 100.0% | 0.0% | Φ = 1.00+++ | < 0.001*** |
| Yes | 0.0% | 100.0% |
Letter “a” represents the highest adjusted residual value (above 2) and the subsequent letters characterize lower values respectively, representing the categories that influenced the statistical significance (p value <0.05) between the groups. *p < 0.05, **p < 0.01, ***p < 0.001. + Small effect, ++ moderate effect, +++ Large effect.
Table 2.
Continuous data on the behavioral and biological profile of the riverine population of Group 1 and Group 2 in the Xingu River region.
Table 2.
Continuous data on the behavioral and biological profile of the riverine population of Group 1 and Group 2 in the Xingu River region.
| Descriptors | Group 1 n=39 |
Group 2 n=47 |
Effect size |
p |
|---|---|---|---|---|
| BEHAVIORAL | ||||
| Smoking Time/year | 0.0 (0-15) | 0.0 (0-0) | 0.04 | < 0.05* |
| Number of cigarettes/day | 0.0 (0-0) | 0.0 (0-0) | 0.00 | 0.50 |
| Frequency Alcohol/week | 0.0 (0-0) | 0.0 (0-3) | 0.04 | < 0.05* |
| Exercise Frequency | 0.0 (0-0) | 1.5 (0-4) | 0.11+ | < 0.01** |
| Fish Consumption/week | 3.0 (2-6) | 4.0 (2-6) | 0.01 | 0.32 |
| BIOLOGICAL | ||||
| SBP | 130.0 (120-142) | 130.0 (120-140) | 0.01 | 0.30 |
| DBP | 80 (80-90) | 80 (80-92) | 0.00 | 0.80 |
| WHR | 1.0 (0.9-1.0) | 0.9 (0.9-1.0) | 0.01 | 0.27 |
| BMI kg/m2 | 29.4 (25-34) | 27 (24-30) | 0.05 | < 0.05* |
| Total Cholesterol mg/dL | 185 (165-215) | 166 (140-200) | 0.07 | < 0.05* |
| HDL mg/dL | 55 (50-68) | 54 (41-65) | 0.02 | 0.23 |
| LDL mg/dL | 103 (81-123) | 83.8 (72-104) | 0.08 | < 0.05* |
| Triglycerides mg/dL | 120 (85-159) | 115 (80-183) | 0.00 | 0.90 |
| Blood glucose mg/dL | 70 (68-85) | 72 (70-84) | 0.01 | 0.40 |
| Age | 55.0 (49-62) | 40.0 (32-48) | 0.29+ | < 0.001*** |
Continuous data that influenced the statistical significance (p value <0.05) between the groups. *p < 0.05, **p < 0.01, ***p < 0.001. + Small effect, ++ moderate effect, +++ Large effect. Abbreviations: SBP: systolic blood pressure; DBP: diastolic blood pressure; WHR: waist-hip ratio; BMI: body mass index; HDL: high density lipoprotein; LDL: low density lipoprotein.
Table 3.
Categorical data on the behavioral and biological profile of riverine populations in Group 1 and Group 2 in the Xingu River region.
Table 3.
Categorical data on the behavioral and biological profile of riverine populations in Group 1 and Group 2 in the Xingu River region.
| Descriptors | Group 1 n=39 |
Group 2 n=47 |
Effect size |
p |
|---|---|---|---|---|
| BEHAVIORAL | ||||
| Smoker | ||||
| No | 89.7% | 95.7% | Φ = 0.12+ | 0.40 |
| Yes | 10.3% | 4.3% | ||
| Ex-smoker | ||||
| No | 64.1% | 85.1% | V = 0.24++ | 0.09 |
| Yes | 25.6% | 10.6% | ||
| No reply | 10.3% | 4.3% | ||
| Alcohol consumption | ||||
| No | 79.5% | 57.4% | Φ = 0.23+ | < 0.05* |
| Yes | 20.5% | 42.6% | ||
| Healthy eating | ||||
| No | 38.5% | 29.8% | Φ = 0.09 | 0.40 |
| Yes | 61.5% | 70.2% | ||
| BIOLOGICAL | ||||
| SAH | ||||
| No | 74.4% | 83.3% | Φ = 0.10+ | 0.33 |
| Yes | 25.6% | 17.0% | ||
| Diabetes | ||||
| No | 94.9% | 95.7% | Φ = 0.02 | 1.00 |
| Yes | 5.1% | 4.3% | ||
| Stroke | ||||
| No | 100% | 97.9% | Φ = 0.10+ | 1.00 |
| Yes | 0.0% | 2.1% | ||
| CVD | ||||
| No | 84.6% | 85.1% | V = 0.10+ | 0.87 |
| Don’t know | 15.4% | 12.8% | ||
| Other | 0.0% | 2.1% |
Categories that influenced the statistical significance (p value <0.05) between the groups. *p < 0.05, **p < 0.01, ***p < 0.001. + Small effect, ++ moderate effect, +++ Large effect.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



