Submitted:
15 April 2020
Posted:
16 April 2020
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
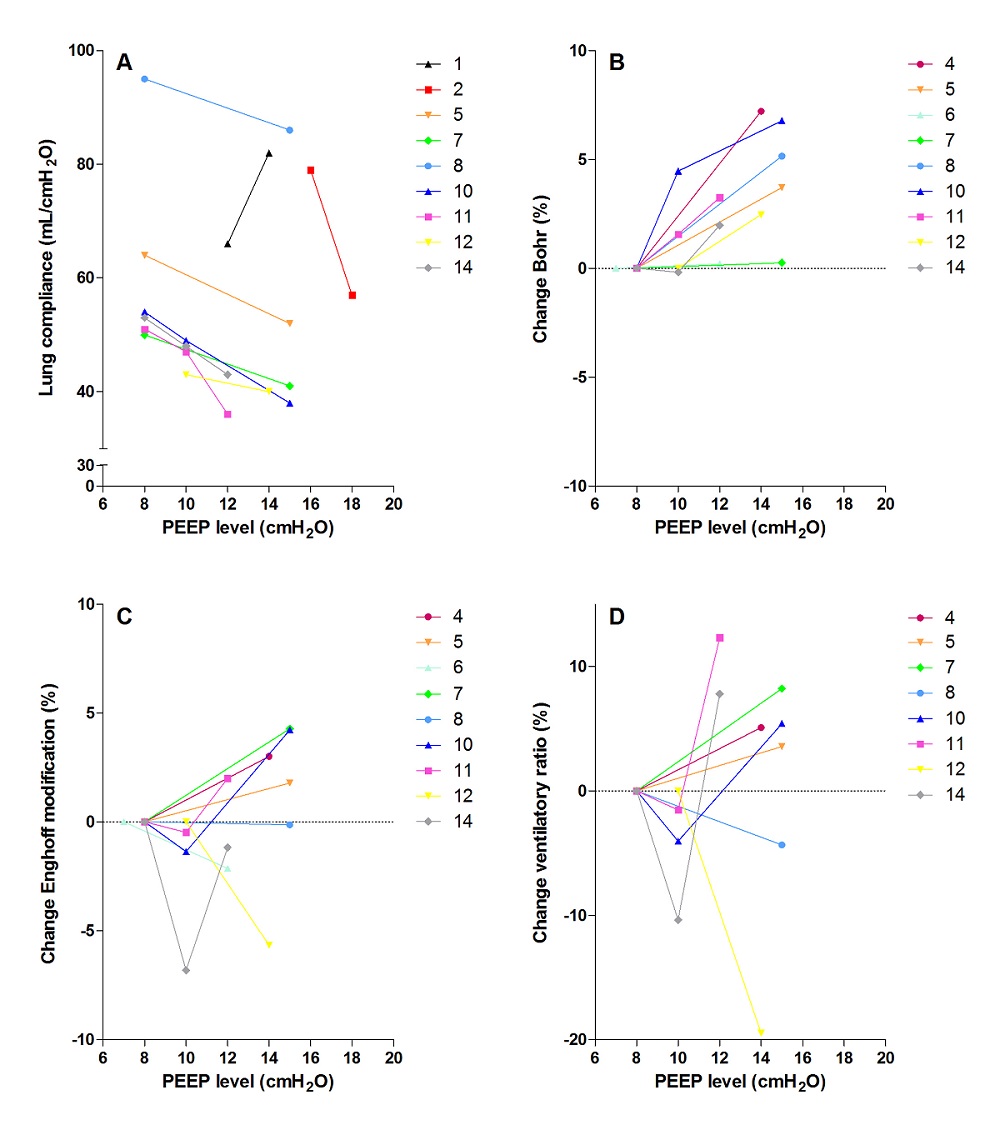
With the emergence of COVID-19 we are confronted with a new clinical picture of acute respiratory distress syndrome in the intensive care unit. In the majority of patients, the respiratory mechanics are very different from the “normal” ARDS patient. We measured transpulmonary pressure and dead space ventilation to assess the effects of high and low PEEP levels on lung compliance and ventilation-perfusion mismatching. Advanced respiratory mechanics were assessed in 14 patients. Compared to ARDS patients, lung compliance was relatively high (61 ± 5 mL/cmH2O). COVID-19 patients had high dead space ventilation and gas exchange impairment (Bohr 52 ± 3%; Enghoff modification 67 ± 2%; ventilatory ratio 2.24 ± 0.23). we show that higher PEEP levels decrease lung compliance and in most cases increase dead space ventilation, indicating that high PEEP levels probably cause hyperinflation in patients with COVID-19. We suggest using prone position for an extended period of time, and apply lower PEEP levels as much as possible.
Keywords:
COVID-19
; ARDS
; PEEP
; mechanical ventilation
; transpulmonary pressure
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



