Submitted:
12 July 2026
Posted:
14 July 2026
You are already at the latest version
Abstract
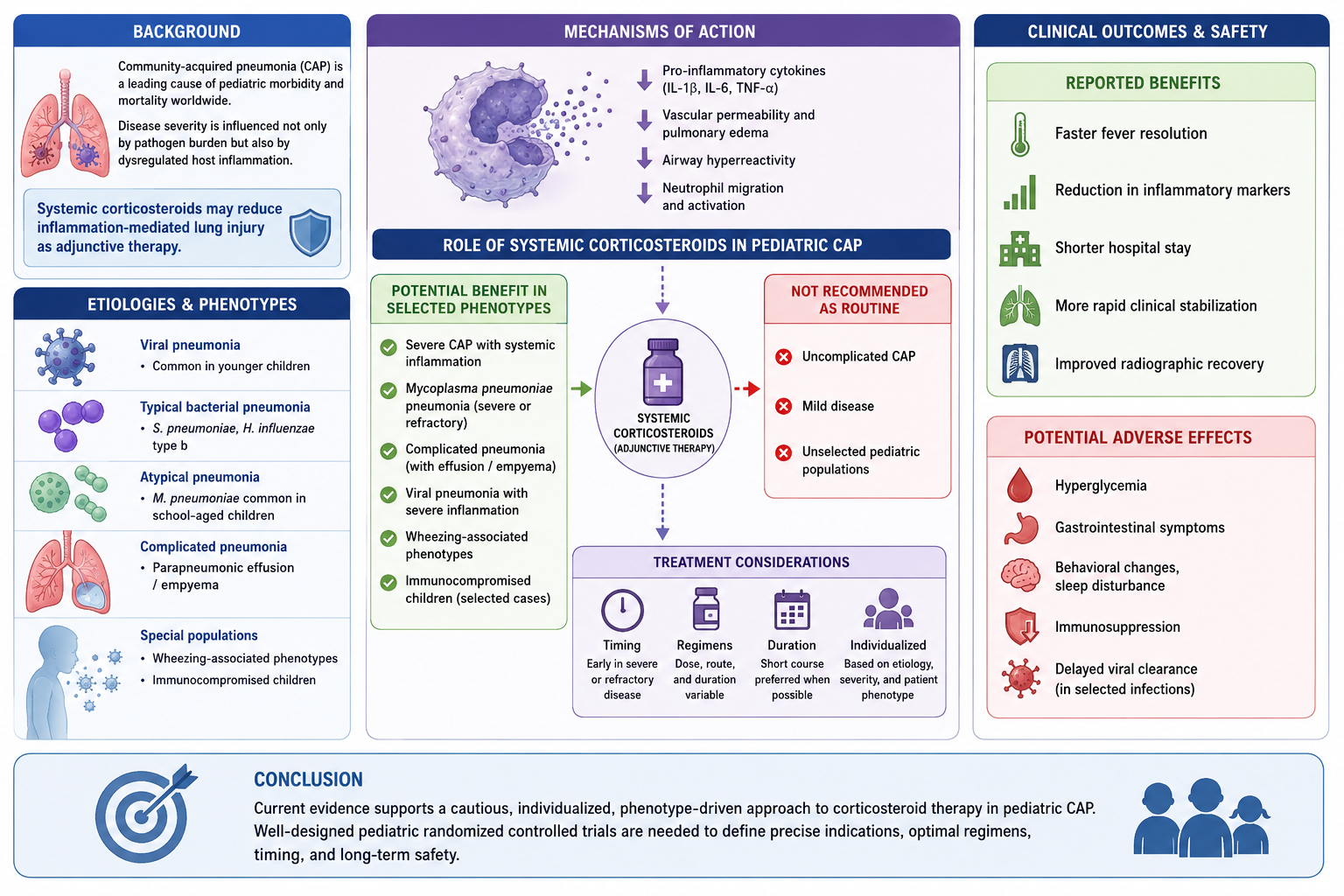
Background: Community-acquired pneumonia (CAP) remains a leading cause of pediatric morbid-ity and mortality worldwide, particularly in low-resource settings. Although antimicrobial therapy is the cornerstone of treatment, disease severity is often influenced not only by pathogen burden but also by dysregulated host inflammation. Systemic corticosteroids have therefore been investigated as adjunctive agents to reduce inflammation-mediated lung injury, but their role in children remains controversial. Methods: This narrative review summarizes current evidence on systemic cortico-steroid use in pediatric pneumonia. The review focuses on biological mechanisms, clinical indica-tions, patient selection, therapeutic regimens, timing and duration of therapy, clinical outcomes, and safety. Particular attention is given to severe CAP, Mycoplasma pneumoniae pneumonia, complicated pneumonia with parapneumonic effusion or empyema, viral pneumonia, wheezing-associated phenotypes, and immunocompromised children. Results: Available evidence suggests that cortico-steroids may provide benefit in selected pediatric phenotypes characterized by severe inflammation, respiratory compromise, refractory disease, or airway hyperreactivity. Reported benefits include faster fever resolution, reduction in inflammatory markers, shorter hospital stay, more rapid clinical stabilization, and improved radiographic recovery, particularly in severe or refractory Mycoplasma pneumoniae pneumonia and selected complicated cases. However, findings are inconsistent, and treatment effects appear strongly dependent on etiology, disease severity, timing of administration, corticosteroid regimen, and patient phenotype. Routine use in uncomplicated CAP or unselected pediatric populations is not supported. Potential adverse effects include hyperglycemia, gastroin-testinal symptoms, behavioral changes, sleep disturbance, immunosuppression, and delayed viral clearance in selected viral infections. Conclusion: Current evidence supports a cautious, individu-alized, phenotype-driven approach to corticosteroid therapy in pediatric CAP. Well-designed pe-diatric randomized controlled trials are needed to define precise indications, optimal regimens, timing, and long-term safety.
Keywords:
pediatric pneumonia
; community-acquired pneumonia
; corticosteroids
; mycoplasma pneumoniae
; adjunctive therapy
; severe pneumonia
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



