Submitted:
02 July 2026
Posted:
03 July 2026
You are already at the latest version
Abstract
The San Francisco Javier Psychogeriatric Centre in Pamplona occupies the former Manicomio Vasco Navarro, a psychiatric complex designed by Máximo Goizueta, be-gun in the late nineteenth century and brought into use in the early twentieth century. Over time, land transfers, additions, refurbishments and functional changes altered its configuration, producing technical and healthcare obsolescence. Nevertheless, the complex preserved the essential logic of a pavilion-based healthcare model: low-rise buildings, ground-floor galleries, courtyards, gardens and open spaces shaped by a hy-gienist and therapeutic understanding of architecture, in which sunlight, ventilation, domestic scale and outdoor space formed part of the care environment. This article analyses the refurbishment not as the preservation of a historic image, but as the reac-tivation of the complex’s typological logic, environmental qualities and tectonic ade-quacy. In the context of the renewal and adaptive reuse of healthcare infrastructures, the study examines functional reprogramming, contemporary extensions through new volumes, material continuity and innovative construction solutions applied to existing heritage. The refurbishment and extension of psychiatric units U1.1 and U1.2 are se-lected as a case study in the sustainable management of healthcare heritage through a strategy of prosthetic memory. The research draws on primary documentation from the architects’ archive and site supervision process.
Keywords:
healthcare heritage
; psychiatric architecture
; prosthetic memory
; tectonic continuity
; architectural concrete
; sustainable refurbishment
; material authenticity
; passive strategies
; pavilion-based architecture
; active conservation
1. Introduction
The refurbishment of historic healthcare heritage raises a specific issue within the contemporary debate on conservation, sustainability and adaptive reuse. Unlike other heritage programmes, former hospitals, sanatoria and psychiatric complexes were conceived as complex care infrastructures. In these buildings, architectural form, functional organisation, hygiene, ventilation, sunlight, circulation, control and the relationship with the exterior formed a single environmental and therapeutic system. Their heritage value does not lie solely in the preservation of façades or singular elements, but in the persistence of a spatial, technical and environmental logic capable of articulating architecture and care.
Modern conservation theory has progressively shifted the debate from stylistic restoration towards a critical understanding of the cultural, material, social and temporal values of heritage assets. Alois Riegl identified early on the tension between historical value, age value, use value and newness value [1]. Cesare Brandi later introduced a decisive reflection on the potential unity of the work, the distinction between historical and aesthetic instances, and the limits of reintegration [2]. The Venice Charter (1964) consolidated the need to preserve monuments as historical evidence, avoiding falsification and drawing on all available sciences and techniques for their study and safeguarding [3]. Subsequently, the Nara Document on Authenticity (1994) expanded the concept of authenticity beyond the visual, incorporating material, form, use, function, tradition, techniques, spirit, setting and sources of information [4].
This expanded understanding is especially relevant to healthcare architecture. In these complexes, use is not a secondary condition, but a constitutive part of heritage value. The Burra Charter (first published in 1979), as revised in 2013, defined conservation as the processes of looking after a place so as to retain its cultural significance, allowing for preservation, restoration, reconstruction, adaptation and compatible use [5]. In historic hospital buildings, this notion makes it possible to move beyond the false alternative between static conservation and functional replacement. The challenge, for both designer and client, is to identify which values must remain, which elements may be transformed and which new layers may be incorporated without destroying the cultural logic of the complex.
The notion of tectonics provides a second critical framework for the refurbishment of heritage. Since Semper, architecture can be understood as an articulation between matter, technique, form and culture [6]. Sekler distinguished between structure, construction and tectonics, reserving the latter for the meaningful expression of construction [7]. Frascari emphasised the value of the detail as the place where construction, meaning and experience converge [8]. Frampton further developed this line of thought by considering tectonics as a poetics of construction capable of resisting the reduction of architecture to image or scenography [9]. In this sense, tectonics is not limited to load-bearing structure. It also includes joints, encounters, thicknesses, traces of fabrication, ageing, texture and material expression.
Sustainability introduces a third dimension. The adaptive reuse of existing buildings has been recognised as a strategy capable of reducing waste, extending the service life of structures, preserving embodied energy and maintaining cultural and social values [10,11,12,13,14]. However, when applied to heritage, reuse should not be understood merely as the reprogramming of use. It must necessarily assess the compatibility between new programmes, cultural significance, material structure, collective memory and capacity for transformation. In this respect, healthcare heritage offers a particularly fertile field: its buildings were designed to accommodate vulnerable bodies, organise care, regulate flows, generate environments and articulate relationships between architecture, nature and health.
Pavilion-based hospital architecture historically emerged in connection with hygienic, environmental and healthcare concerns. Florence Nightingale defended the importance of ventilation, cleanliness and spatial layout in hospital design [15]. The pavilion model, consolidated in the nineteenth century, separated built volumes in order to promote lighting, ventilation, infection control and contact with open spaces [16,17,18]. In psychiatric hospitals, this logic was reinforced through the presence of gardens, routes, workshops, pavilions, boundaries and open spaces associated with rest, occupational therapy, surveillance and the relationship with the landscape [19,20,21,22].
In the contemporary context, studies on therapeutic environments have shown that architecture and landscape can influence wellbeing, stress reduction, orientation, perceived safety and patient recovery [23,24,25,26]. These studies make it possible to reinterpret former psychiatric complexes not only as built heritage, but as environmental and social systems whose logic continues to offer valid criteria for contemporary healthcare architecture.
The San Francisco Javier Psychogeriatric Centre in Pamplona provides an appropriate case through which to address these issues. The complex occupies the former Manicomio Vasco Navarro, designed by Máximo Goizueta, whose original organisation followed a nineteenth-century pavilion-based healthcare scheme: low-rise buildings, ground-floor galleries, courtyards, gardens and open spaces. The project documentation describes this system as a pavilion-based typology set within a landscaped environment, with well-proportioned courtyards and a close relationship between patient, architecture and nature [27].
Over the course of its history, however, the site underwent land transfers, additions, partial refurbishments and functional changes that unevenly altered its original configuration, leading to a progressive state of dimensional, functional and technical obsolescence. Although the essential logic of the complex remained, a number of problems could be identified: parallel circulation systems, overlapping flows, lack of ventilation and natural light on the ground floor, functional rigidity, superimposed energy networks and difficulty in absorbing new healthcare programmes [28].
The central question raised by the refurbishment project is therefore the following: how can a nineteenth-century pavilion-based psychiatric complex be updated to meet contemporary healthcare requirements without reducing its heritage value to a preserved image, and without renouncing its original tectonic, environmental and therapeutic logic?
The design hypothesis developed and implemented by the architectural team is that the refurbishment and extension of units U1.1 and U1.2 of the San Francisco Javier Psychogeriatric Centre had to operate through a strategy of prosthetic memory. This strategy neither imitates nor replaces the historic masonry, but extends its functional, environmental and technical capacities through contemporary additions, selective demolition, typological continuity, the reactivation of courtyards and galleries, and an envelope of pigmented architectural concrete capable of incorporating geometric traces, chromatic continuity and material ageing.
The aim of this research is twofold. First, it analyses the intervention, both architecturally and through documentary sources, in order to identify its mechanisms of active conservation, functional reprogramming and tectonic continuity. Second, it assesses prosthetic memory as a methodological framework that may be extrapolated to the sustainable refurbishment of historic healthcare heritage, especially in complexes where authenticity is not limited to preserved material fabric, but depends on the reactivation of an environmental, constructive and social logic.
2. Materials and Methods
2.1. Case Study
The case study comprises the master plan, the overall project for the psychiatric area, and the refurbishment and extension of psychiatric units U1.1 and U1.2 of the San Francisco Javier Psychogeriatric Centre in Pamplona, Navarre. The project was developed by Vaillo+Irigaray Architects for the Servicio Navarro de Salud-Osasunbidea. As attested by the general project documentation, the master plan was awarded through a public tender in 2009 and developed in 2010. Its overall scope covered 291,455 m² and envisaged a total built area of 51,966 m². Phases I and II, corresponding to units U1.1 and U1.2, were the subject of a second competition in 2010, were designed in 2012 and were completed in 2017, with a total built area of 9,820 m² and a cost of EUR 11,635,772 [27].
The intervention forms part of a broader planning process. The construction project for U1.1 and U1.2 expressly states its continuity with the master plan for the San Francisco Javier Psychogeriatric Centre and with the Special Interior Reform Plan. The document is presented as the first formal and built implementation of the centre’s modernisation, updating and revitalisation [28]. This documentary continuity allows the case to be studied as a sequence comprising diagnosis, regulation, design, selective demolition, construction and final verification.
2.2. Documentary Sources
The research is based on the analysis of primary and original sources produced during the transformation process of the complex and preserved in the archive of Vaillo+Irigaray Architects. The documentary corpus analysed includes the Master Plan, the Special Interior Reform Plan, the Functional Plan, the preliminary design, the demolition projects for U1.1 and U1.2, the construction projects for U1.1 and U1.2, structural reports, annexes on architectural concrete, masonry drawings, elevations, sections, urbanisation drawings, furniture documentation, the final works report, photographic records and conceptual project documentation [27,28,29,30,31,32,33,34,35,36].

Table 1.
Documentary sources and analytical role.
| Document | Date | Function in the research | Analytical dimension |
|---|---|---|---|
| Plan Director Master Plan |
2010 | Defines the overall transformation strategy |
Typology, phases, circulation systems, installations |
| PERI Special Interior Reform Plan |
2010 | Establishes the urban-planning and heritage framework | Conservation, transformation, urban relationship |
| Plan Funcional Functional Plan |
2010–2011 | Determines healthcare requirements | Programme, flows, units, outpatient care |
| Anteproyecto Preliminary Design |
2011 | Translates the strategy into architectural order | Site layout, phases, functionality |
| Proyecto de Derribo U1.1 Demolition Project U1.1 |
2012 | Defines partial demolitions and elements to be retained | Selective conservation |
| Proyecto de Derribo U1.2 Demolition Project U1.2 |
2012 | Defines partial demolitions and ele-ments to be retained | Selective conservation |
| Proyecto de Ejecución U1.1 Construction Project U1.1 |
2012 | Specifies the first built phase | Programme, structure, construction |
| Proyecto de Ejecución U1.2 Construction Project U1.2 |
2012 | Specifies the first built phase | Programme, structure, construction |
| Anexos de estructura Structural Annexes |
2012 | Justify the load-bearing system | Slabs, walls, steel, micropiles |
| Anexos de hormigón Concrete Annexes |
2012 | Define the contemporary materiality | Pigments, aggregates, formwork, joints, patina |
| Final de obra Final Works Report |
2018 | Documents the built result and modifications | Verification and adjustments |
2.3. Methodological Approach
The article develops a qualitative methodology typical of architectural case-study research, constructed through three recent and complementary approaches: case-study methodology applied to architectural research (Kalua, 2024) [37], analytical models for the adaptive reuse process of built heritage (Arfa, Lubelli, Quist and Zijlstra, 2024) [38], and typological-constructive studies aimed at the integrated refurbishment of existing buildings (Rosado and Reimão, 2024) [39]. On this basis, the research combines documentary analysis, typological reading, constructive analysis and diachronic comparison between the original state, the pre-intervention state and the executed proposal.
The application of this methodology to the case study is structured through a series of analytical instruments designed to organise the available information and to relate diagnosis, design and execution. These matrices do not operate as independent categories, but as cross-reading fields that make it possible to verify how the intervention articulates heritage values, functional requirements, typological continuities, material decisions and inherited environmental principles. The method is therefore organised into four analytical matrices:
The first is a heritage-functional matrix, aimed at identifying functional pathologies, technical obsolescence, circulation conflicts, dimensional limitations and contemporary programmatic requirements.
The second is a typological matrix, which compares the original scheme, the pre-intervention state and the executed proposal. This matrix addresses pavilions, galleries, courtyards, voids, low density and growth by addition.
The third is a tectonic-material matrix, which analyses the relationship between the historic masonry, stone, brick, arches, roofs, structure, architectural concrete, pigmentation, formwork, reliefs, joints and patina.
The fourth is an environmental-passive matrix, focused on the continuity of principles related to sunlight, ventilation, courtyards, gardens, intermediate spaces, orientation, the interior–exterior relationship and the therapeutic landscape.
The analysis does not seek to measure the building’s energy performance quantitatively. Its aim is to identify, through documentary evidence, how the intervention recovers, transforms or extends environmental and constructive principles inherent to the historic system. This methodological delimitation establishes the degree to which the conclusions may be extrapolated. The results are primarily transferable to pavilion-based heritage complexes, whether healthcare or institutional, in which sustainability depends not only on material reuse, but also on the reactivation of an inherited spatial and environmental structure.
2.4. Prosthetic Memory as an Analytical Method
In this article, the term prosthetic memory is not used as an authorial metaphor, but as an analytical framework for examining the capacity of a contemporary intervention to reactivate a historic system without resorting to literal imitation or total replacement. The framework is based on the analogy of the prosthesis understood as an added device that restores lost capacities to an existing body. Applied to architectural heritage, the concept refers to interventions that preserve the structural, spatial, material and environmental logic of a historic system while incorporating the elements required for contemporary reprogramming.
The method evaluates the intervention through five verifiable indicators (Table 2):
- Typological continuity: the extent to which the intervention preserves or reactivates the original spatial structure, including pavilion layout, galleries, courtyards, gardens, voids, circulation axes and low-density occupation.
- Environmental continuity: the extent to which the intervention maintains or reactivates passive principles such as natural light, ventilation, orientation, open spaces, intermediate spaces and the relationship between architecture and landscaped areas.
- Tectonic continuity: the extent to which the new work engages with structural systems, constructive logic, thicknesses, joints, openings, roofs, surfaces, traces of previous elements and construction processes.
- Material compatibility: the extent to which the new materials avoid false historical imitation while establishing physical, chromatic, mineral, constructive or ageing compatibility with the existing fabric.
- Temporal continuity: the extent to which the intervention accepts ageing, weathering, patina and future transformation as part of the conservation strategy.
These indicators are applied to the documentary corpus through a comparative reading of three states: the original pavilion-based complex, the pre-intervention state and the refurbishment completed in 2018. This approach makes it possible to assess whether the new construction operates as a functional and tectonic extension of the existing system, rather than as an autonomous and independent addition.
3. Results
3.1. Evidence 1: The Historic Complex Operated as a Pavilion-Based Environmental System
The documentary analysis shows that the heritage value of the complex cannot be reduced to a set of isolated buildings. The original organisation of the former Manicomio Vasco Navarro responded to a pavilion-based healthcare system composed of low-rise volumes connected by galleries and articulated through courtyards, gardens and open spaces. The project documentation describes the proposal as an operation that preserves and enhances the original values of the complex: a nineteenth-century pavilion-based typology, a human scale, a landscaped setting, well-proportioned courtyards and a close relationship between patient, environment and nature [27].
This structure can be observed through the comparison between the historic plan of the asylum, the pre-intervention state in 2010 (Figure 2) and the master plan proposal. The evolutionary master plan diagram (Figure 3) shows how the original scheme was organised around a large U-shaped structure, with lateral pavilions, longitudinal galleries, inner courtyards and partial symmetries. The pre-intervention state appears more fragmented, with additions and occupations that had altered the clarity of the initial layout. The proposal restores a logic of growth by addition, maintains the main axes and reorganises the new volumes in continuity with the pavilion-based matrix [29].
The main result of this first reading is that the existing architecture operated as an environmental infrastructure. The pavilions were not autonomous elements. Their separated arrangement generated courtyards, distances, open spaces, routes and conditions of ventilation. Consequently, the conservation of the complex could not be limited to its façades. It had to address the relationship between built volumes and voids.
Result: the heritage value of the complex depended on a spatial and environmental system composed of pavilions, galleries, courtyards, gardens, voids and circulation structures.
3.2. Evidence 2: The Pre-Existing Condition Presented Functional, Dimensional and Technical Obsolescence
The project documents identify a series of problems that prevented the direct adaptation of the complex to contemporary healthcare requirements. The Construction Project for U1.1 identifies the double circulation scheme as the main problem: an inner circulation system through the courtyards and an outer perimeter circulation system that enclosed the ground-floor rooms. This arrangement prevented adequate ventilation and natural lighting in these spaces, restricting or rendering many of their uses unviable [28].
Figure 1.
Territorial position of the complex in Pamplona in relation to the topography, the river, the urban fabric and the other pavilion-based hospital complex in Pamplona. Source: Vaillo+Irigaray Architects archive, 2010–2012.
Figure 1.
Territorial position of the complex in Pamplona in relation to the topography, the river, the urban fabric and the other pavilion-based hospital complex in Pamplona. Source: Vaillo+Irigaray Architects archive, 2010–2012.

Figure 2.
Historical photographs and plan of the former Manicomio Vasco Navarro. Pre-intervention state. Source: Vaillo+Irigaray Architects archive, 2010–2012.
Figure 2.
Historical photographs and plan of the former Manicomio Vasco Navarro. Pre-intervention state. Source: Vaillo+Irigaray Architects archive, 2010–2012.

Figure 3.
Master plan evolution. Comparison between the original 1906 master plan, the pre-intervention state in 2010 and the new planning proposal. Source: Vaillo+Irigaray Architects archive, 2015.
Figure 3.
Master plan evolution. Comparison between the original 1906 master plan, the pre-intervention state in 2010 and the new planning proposal. Source: Vaillo+Irigaray Architects archive, 2015.

The same document identifies the overlapping of flows as another relevant limitation. The existing circulation systems encouraged intersections between inpatients, outpatients, healthcare staff, catering supply routes, energy distribution and logistical routes. The absence of circulation hierarchies made it impossible to differentiate between patients, staff, central services and general services [28].
In addition, the complex suffered from what the documentation defines as “dimensional stenosis”: narrow structural bays, pavilions of insufficient length and difficulty in accommodating efficient healthcare units of 28–30 rooms per nursing unit. The documentation also identifies the obsolescence of the building services, the dispersion of heat-generation plants, outdated transformers and distribution networks superimposed onto the architecture, resulting in energy losses, maintenance difficulties and an inability to supply new uses [28].
This diagnosis (Table 3) demonstrates that the obsolescence of the complex was not merely material. It was also circulatory, dimensional, energy-related and healthcare-related. For this reason, an intervention based solely on restoring the appearance of the pavilions would have been insufficient. The updating of the complex required action on the functional logic of the system.
Result: the intervention was necessary because the existing system could no longer support contemporary psychiatric care without structural, functional and technical transformation.
3.3. Evidence 3: Selective Dismantling Functioned as an Active Conservation Tool
The demolition projects for U1.1 and U1.2 show that the intervention was not conceived as indiscriminate demolition, but as an operation of selective conservation. Both documents state that the project formed part of a Special Interior Reform Plan, required because the building was a listed asset of significant relevance, and that the aim of this instrument was not the strict protection of the built complex, but the definition of a strategy for the functional recovery of the original building [30,31,35].
The demolition documentation justifies the need to partially remove certain buildings because of their condition, their incompatibility with the morphological characteristics of the preliminary design and the need to develop the construction project. However, the process also had to ensure the permanence of the constructive elements that were to be retained, linking the demolition project and the construction project in parallel [30,31].
In U1.1, the documentation records partial interior demolitions and the complete removal of the north-west gallery within a building constructed with stone load-bearing walls, ceramic brick arcades, a ventilated ground floor, a metal structure with ceramic hollow-block floor slabs and timber trusses with a tiled roof [30]. In U1.2, the north-east façade was retained, having previously been stabilised by means of a metal structure and bracing in successive phases, while work was carried out on a construction comprising stone walls, internal pillars, brick arcades, ceramic floor slabs and timber trusses [31].
This result makes it possible to understand selective dismantling as a tool of active conservation. The intervention removes incompatible, deteriorated or functionally inefficient elements in order to recover the overall logic of the complex. Conservation is not defined by the total permanence of material fabric, but by the critical continuity of the original typological, constructive and environmental system.
Result: selective dismantling made it possible to remove incompatible or deteriorated parts while preserving the typological and material logic of the complex.
3.4. Evidence 4: The New Volumes Operated as Functional Prostheses
The intervention strategy is formulated in the project documentation through the idea of the prosthesis. The general project text states that the new prosthetic additions revitalise the intended function, reconfigure space, enable new uses, complement the structure and allow the assimilation of new healthcare technologies [27].
This functional dimension (Figure 4) is verified in the project plans. The ground floor introduces outpatient areas, consulting rooms, waiting areas, vertical cores, support areas, hierarchised circulation systems and new connections with the existing units. The first floor organises inpatient units, rooms, nursing stations, day spaces, care areas and internal routes. On both levels (Figure 5), the new pieces do not operate as formal annexes, but as infrastructures that resolve the deficiencies identified in the diagnosis [32,33].
The joint reading of both plans shows that the prosthesis operates on several levels. In plan, it extends and corrects the existing pavilion-based structure. In section, it integrates new levels, technical basements, roofs, building services and the relationship with the ground. In programme, it allows contemporary healthcare requirements to be incorporated without abandoning the scale and order of the original complex. This condition confirms that the extension was not conceived merely as a volumetric addition. Its main function was to restore operability to the system. For this reason, the term “prosthetic” is not used as a formal metaphor, but as a functional, tectonic and heritage-related category.
Result: the new volumes acted as functional prostheses because they extended the existing buildings, reorganised circulation, incorporated new healthcare programmes and preserved the pavilion-based order by reinforcing its original conception.
3.5. Evidence 5: Architectural Concrete Acted as Tectonic and Material Mediation
The most significant material result is the envelope of pigmented architectural concrete. The project documentation confirms that the entire extension is constructed in structural architectural concrete—façades and roofs—and that this concrete is mass-pigmented in the colour of the mortar binding the stones and bricks of the original buildings [27]. The geometries of the arches of the historic buildings are imprinted on the new façades as a memory of the existing masonry and as compositional continuity (Figure 6). The design decisions also anticipate that the building will progressively acquire a patina according to orientation and prevailing winds [27]. The technical annexes on architectural concrete show that this decision was not merely compositional. The document defines architectural concrete as a synergy between design, prior preparation, manufacturing, on-site execution and final protection (Firgure 7). It also states that the final result depends on the composition (Table 4) of the concrete, the texture of the formwork and the time elapsed before stripping [34].
The architectural concrete annex should not be read solely as a technical specification, but as the material basis of the integration strategy. The choice of mass-pigmented concrete, with light-coloured cement, clean aggregates, a low water/cement ratio, stable inorganic pigments and structural fibres in the façades, sought to ensure chromatic homogeneity, surface durability and shrinkage control, preventing continuity with the historic masonry from depending on an applied cladding. This constructive precision also made it possible to formalise the openings and façade recesses through specific formwork. The openings are not conceived as simple perforations, but as incisions of variable thickness that translate the memory of historic arches and rhythms into a contemporary concrete envelope (Figure 8). Thus, the new façade does not imitate the existing stone or brick, but establishes with them a mineral, tectonic and temporal continuity based on mass, relief, shadow and ageing [34].
The formwork system was equally decisive. The façade geometry was produced using moulds placed in situ on the outer formwork, with phenolic plywood boards cut by numerical control in 30 mm layers until reaching a maximum thickness of 9 cm. The window openings were executed with phenolic-board boxes 34 cm wide and sills sloping 4% towards the exterior [34].
The results show that the new envelope does not reproduce the historic masonry. Instead, it interprets it through mass, colour, relief, joint, shadow and ageing. The new façade thus operates as a contemporary tectonic surface that records the geometric memory of the complex without falsifying its original materiality (Figure 9).
Result: the new envelope did not imitate the historic masonry. It translated its tectonic memory into a contemporary mineral system based on mass, relief, colour, joint, shadow and ageing.
3.6. Synthesis of Results
The five indicators show (Table 5) that the intervention can be understood as a strategy of prosthetic memory. The project preserves the pavilion-based logic, reactivates passive environmental principles, introduces new tectonic systems, establishes material compatibility without imitation and incorporates ageing as part of the integration process.
The results also define the limits of the study. Environmental continuity is verified through spatial and documentary evidence, not through measurements of environmental performance. Temporal continuity is based on material specifications and design intentions, but would require future monitoring in order to assess the actual ageing of the concrete surfaces.
4. Discussion
4.1. From Visual Conservation to Tectonic Authenticity
The results show that the intervention shifts conservation from image to tectonic logic. This operation aligns with the Nara Document, which understands authenticity as a condition linked to diverse sources of information, including form, design, materials, techniques, use, function, tradition, location, spirit and context [4]. In the case studied, the authenticity of the complex does not reside solely in the preserved walls, but in the critical continuity of a pavilion-based, environmental and healthcare organisation. The intervention does not literally reproduce arches, masonry, roofs, galleries or other elements of the architectural language. Rather, it translates them through a new materiality. As shown in the results, this shift is decisive. The project avoids both historicist simulation and abstract rupture. It does not seek to make the new building mimic the original, but to extend the constructive memory of the complex through a contemporary technique. In this sense, the intervention may be situated within a broader line of research on the contemporary reinterpretation of inherited construction systems, in which traditional techniques are not reproduced literally but transformed through new structural, material and cultural conditions [40].
The formalisation of the façade openings is one of the operations in which tectonic continuity becomes most verifiable. The geometries of the existing arches are not reconstructed as added historical elements, but are transformed into recesses, thicknesses and variations of shadow within the concrete itself. In this way, the new envelope does not reproduce the original composition, but preserves part of its logic: rhythm, depth, modulation of openings and the relationship between mass and void. Mass pigmentation reinforces this operation, as it avoids the use of a superficial coating and brings the new material closer to the chromatic field of the existing stone, brick and mortars. Heritage integration is therefore achieved through controlled constructive and visual compatibility: the new façade declares its contemporary condition, while incorporating geometric, material and temporal rules derived from the historic complex.
4.2. Prosthetic Memory as a Conservation Strategy
The notion of prosthetic memory is confirmed as a refurbishment mechanism that allows the intervention to be interpreted as an intermediate strategy between literal conservation and functional replacement. A prosthesis neither imitates the original body nor replaces it entirely. It acts where the system has lost operational capacity. In heritage conservation, this mechanism makes it possible to describe interventions that preserve what is essential, remove what is incompatible and add what is necessary for the system to function again.
From the perspective of tectonic theory, this operation is not limited to volume. It affects structure, joints, thicknesses, materials, rhythms, traces and construction procedures. As outlined in the Introduction, Sekler defined tectonics as an expressive dimension of construction, distinct from structure and mere technique [7], while Frampton understood it as a constructive poetics capable of restoring cultural depth to the act of building [9]. In the San Francisco Javier Psychogeriatric Centre, this dimension appears in the way architectural concrete absorbs the geometric memory of the historic masonry without replicating it.
The prosthesis operates on four levels. First, as a typological prosthesis, because it extends the pavilion-based pattern of growth. Second, as a functional prosthesis, because it separates flows, reorganises units and enables new healthcare standards. Third, as a technical prosthesis, because it introduces structure, building services, basements and construction systems capable of updating the building. Fourth, as a temporal prosthesis, because it accepts that integration does not occur instantly, but through material ageing.
The results make it possible to specify that prosthetic memory does not operate as a formal metaphor, but as a strategy that can be verified at several scales of the intervention. At the typological level, the new volumes extend the pavilion-based logic of the complex and maintain the relationship between built elements, courtyards, galleries and voids. At the functional level, the extension corrects the obsolescences identified, separates flows, reorganises care units and incorporates programmes compatible with contemporary healthcare standards. At the technical level, the intervention introduces new structures, basements, services and construction systems capable of restoring operability to the existing building. Finally, at the temporal level, the pigmented architectural concrete shifts integration from immediate resemblance towards a process of material compatibility, patina and shared ageing with the historic masonry.
4.3. Adaptive Reuse and Sustainable Heritage Management
Adaptive reuse has been recognised as a sustainability strategy because of its capacity to extend the service life of buildings, reduce waste, preserve embodied energy and maintain cultural values [10,11,12,13,14]. However, in a historic psychiatric complex, sustainability cannot be measured solely in terms of reduced material impact. It must also address the continuity of the care-related meaning of the site, the recovery of open spaces, the preservation of scale, the relationship with the garden and the capacity of architecture to support forms of care. The intervention analysed shows that heritage sustainability operates on three simultaneous levels. At the material level, it avoids the total replacement of the complex through conservation, selective demolition and addition. At the environmental level, it reactivates courtyards, galleries, voids and relationships with the landscape. At the social level, it adapts obsolete healthcare heritage to new care models while maintaining a scale compatible with patient experience.
This reading makes it possible to broaden the meaning of sustainable heritage management. It is not only a matter of conserving physical resources, but of preserving and updating a spatial culture of care.
4.4. Passive Environmental Reactivation beyond Energy Efficiency
Sustainability in refurbishment should not be understood only through parameters of energy efficiency. The documentation reveals a broader strategy, based on the reuse of the complex, the recovery of its low density, the continuity of courtyards and gardens, the reorganisation of circulation systems and the relationship between architecture and domesticated nature. The historic complex already incorporated environmental principles characteristic of pre-industrial healthcare architecture: separation between pavilions, courtyards, ventilation, sunlight, galleries and therapeutic outdoor spaces. The intervention does not invent these principles, but reactivates them under new conditions. This reading is consistent with the hygienist tradition of hospital architecture, in which ventilation, light and separation between built volumes operated as healthcare resources [15,16,17,18].
The most relevant operation does not consist in adding isolated passive devices, but in restoring the spatial structure that made a more balanced environmental performance possible: well-proportioned courtyards, intermediate spaces, façades with differentiated orientations, continuity of outdoor routes and visual relationships with the garden. In this sense, the project updates the hygienist and therapeutic spirit of the complex.
4.5. Architectural Concrete as Tectonic and Temporal Mediation
Pigmented architectural concrete constitutes the main device of material mediation. The project’s technical documentation specifies a precise strategy: structural concrete in façades and roofs, mass pigmentation, aggregate control, water/cement dosage, use of fibres, mechanised phenolic formwork and reliefs derived from historical geometries [34].
This decision must be situated within a broader discussion on architectural concrete, self-compacting concrete and surface durability. Self-compacting concrete makes it possible to fill complex geometries and areas with high reinforcement density without vibration, although it requires rigorous control of viscosity, segregation, pressure on formwork and surface finish [41,42,43,44]. In the case analysed, this technology is placed at the service of a heritage purpose: to inscribe the abstract memory of the arches onto the new façade while avoiding literal reproduction.
Mass pigmentation prevents colour from becoming a superficial layer. Inorganic pigments, stable against weathering and UV radiation, allow colour to be understood as an internal condition of the material [45]. In this way, chromatic continuity with stone, brick and mortar does not depend on an applied coating, but on the concrete mass itself. The new façade does not represent history. It incorporates it as a construction procedure, as relief and as a potential for ageing.
4.6. Limits of Transferability
The transferability of the case has limits. Prosthetic memory is especially suitable for complexes in which heritage logic resides in an open and repetitive system: pavilions, galleries, courtyards, structural bays, rhythms and intermediate spaces. In buildings whose authenticity depends on irreplaceable singular masonry, specific artisanal decoration or monumental values concentrated in unique elements, the margin for transformation should be assessed according to other criteria.
Nevertheless, the case offers a methodological contribution to interventions on healthcare, care-related or institutional heritage. Its main contribution lies in showing that conservation, functional adaptation, environmental sustainability and tectonic continuity do not have to be addressed as separate objectives. They can be integrated (Figure 10) through a strategy of diagnosis, selection, addition and controlled ageing.
5. Conclusions
The analysis of the refurbishment and extension of units U1.1 and U1.2 of the San Francisco Javier Psychogeriatric Centre makes it possible to validate the main hypothesis of this article: the intervention does not operate as the formal conservation of a historic image, nor as the functional replacement of the existing building, but as a strategy of prosthetic memory. The project preserves essential elements of the inherited system, removes incompatible or deteriorated parts and incorporates new volumes, technical systems and material solutions that restore the healthcare, environmental and constructive operability of the complex.
The first conclusion is that historic hospital heritage, especially in pavilion-based models, must be understood as a spatial, environmental and therapeutic system. Its value does not reside solely in façades or protected elements, but in the relationship between pavilions, galleries, courtyards, gardens, low density, ventilation, sunlight and circulation routes.
The second conclusion is that its sustainable refurbishment requires a diagnosis that is simultaneously functional, technical, typological and environmental. The obsolescence identified was circulatory, dimensional, energy-related and healthcare-related; therefore, restoring the historic appearance would have been insufficient.
The third conclusion is that selective demolition acts as active conservation. By removing deteriorated or incompatible elements, the intervention recovers the pavilion-based order, clarifies circulation systems and prepares the incorporation of new uses without cancelling the logic of the complex.
The fourth conclusion is that contemporary additions can operate as architectural prostheses when they extend lost capacities of the historic building. In this case, they continue the typological logic, reorganise units and flows, introduce structure, basements and building services, and shift integration towards a process of patina and material ageing.
The case makes it possible to broaden the concept of sustainability as applied to the refurbishment of hospital heritage. Sustainability here is not limited to waste reduction, the extension of service life or the preservation of embodied energy. It also includes the recovery of a spatial culture of care: domestic scale, relationship with the garden, intermediate spaces, circulation clarity, ventilation, natural light and continuity between architecture and therapeutic landscape. In historic healthcare complexes, adaptive reuse should be assessed according to its capacity to keep these values active, in addition to its technical or constructive efficiency.
Author Contributions
Conceptualization, methodology, Y.V.U.; validation, formal analysis, investigation, resources, data curation, writing—original draft preparation, writing—review and editing, visualization, Y.V.U. and A.A.-O.; supervision, Y.V.U. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Restrictions apply to the availability of these data. Data were obtained from Vaillo+Irigaray Architects Archive and are available upon request via email: media@vailloirigaray.com.
Acknowledgments
The authors would thank Vaillo+Irigaray Architects practice for the availability of all the data acquired in the elaboration of the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Riegl, A. Der moderne Denkmalkultus: Sein Wesen und seine Entstehung; W. Braumüller: Vienna, Austria, 1903. [Google Scholar]
- Brandi, C. Teoria del restauro; Edizioni di Storia e Letteratura: Rome, Italy, 1963. [Google Scholar]
- ICOMOS. International Charter for the Conservation and Restoration of Monuments and Sites (The Venice Charter 1964). Available online: https://www.icomos.org/charters/venice_e.pdf (accessed on 12 May 2026).
- ICOMOS. The Nara Document on Authenticity. Available online: https://www.icomos.org/charters/nara-e.pdf (accessed on 10 May 2026).
- Australia ICOMOS. The Burra Charter: The Australia ICOMOS Charter for Places of Cultural Significance, 2013. Available online: https://australia.icomos.org/wp-content/uploads/The-Burra-Charter-2013-Adopted-31.10.2013.pdf (accessed on 10 May 2026).
- Semper, G. The Four Elements of Architecture and Other Writings; Mallgrave, H.F.; Herrmann, W., Translators; Cambridge University Press: Cambridge, UK, 1989. [Google Scholar]
- Sekler, E.F. Structure, construction, tectonics. In Structure in Art and in Science; Kepes, G., Ed.; George Braziller: New York, NY, USA, 1965; pp. 89–95. [Google Scholar]
- Frascari, M. The tell-the-tale detail. VIA 1984, 7, 23–37. [Google Scholar]
- Frampton, K. Studies in Tectonic Culture: The Poetics of Construction in Nineteenth and Twentieth Century Architecture; Cava, J., Ed.; MIT Press: Cambridge, MA, USA, 1995. [Google Scholar]
- Bullen, P.A. Adaptive reuse and sustainability of commercial buildings. Facilities 2007, 25, 20–31. [Google Scholar] [CrossRef]
- Langston, C.; Wong, F.K.W.; Hui, E.C.M.; Shen, L.-Y. Strategic assessment of building adaptive reuse opportunities in Hong Kong. Build. Environ. 2008, 43, 1709–1718. [Google Scholar] [CrossRef]
- Bullen, P.A.; Love, P.E.D. Adaptive reuse of heritage buildings. Struct. Surv. 2011, 29, 411–421. [Google Scholar] [CrossRef]
- Plevoets, B.; Van Cleempoel, K. Adaptive reuse as a strategy towards conservation of cultural heritage: A literature review. WIT Trans. Built Environ. 2011, 118, 155–164. [Google Scholar] [CrossRef]
- Foster, G. Circular economy strategies for adaptive reuse of cultural heritage buildings to reduce environmental impacts. Resour. Conserv. Recycl. 2020, 152, 104507. [Google Scholar] [CrossRef]
- Nightingale, F. Notes on Hospitals, 3rd ed.; Longman, Green, Longman, Roberts, and Green: London, UK, 1863. [Google Scholar]
- Taylor, J. The Architect and the Pavilion Plan: Dialogue and Design Creativity in England, 1850–1914; Leicester University Press: Leicester, UK, 1977. [Google Scholar]
- Cook, G.C. Henry Currey FRIBA (1820–1900): Leading Victorian hospital architect, and early exponent of the “pavilion principle”. Postgrad. Med. J. 2002, 78, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Verderber, S.; Fine, D.J. Healthcare Architecture in an Era of Radical Transformation; Yale University Press: New Haven, CT, USA, 2000. [Google Scholar]
- Foucault, M. Naissance de la clinique: Une archéologie du regard médical; Presses Universitaires de France: Paris, France, 1963. [Google Scholar]
- Laget, P.-L.; Laroche, C.; Duhau, I. L’Hôpital en France: Histoire et architecture; Lieux Dits: Lyon, France, 2012. [Google Scholar]
- Chrysikou, E. Architecture for Psychiatric Environments and Therapeutic Spaces; IOS Press: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Scavuzzo, G. Il parco della guarigione infinita: Un dialogo tra architettura e psichiatria; LetteraVentidue: Siracusa, Italy, 2020. [Google Scholar]
- Ulrich, R.S. View through a window may influence recovery from surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, R.S.; Zimring, C.; Zhu, X.; DuBose, J.; Seo, H.-B.; Choi, Y.-S.; Quan, X.; Joseph, A. A review of the research literature on evidence-based healthcare design. HERD 2008, 1, 61–125. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C.C.; Devlin, A.S.; Pereira, C.R.; Lima, M.L. Do the hospital rooms make a difference for patients’ stress? A multilevel analysis of the role of perceived control, positive distraction, and social support. J. Environ. Psychol. 2017, 53, 63–72. [Google Scholar] [CrossRef]
- Rodríguez-Labajos, L.; Kinloch, J.; Grant, S.; O’Brien, G. The role of the built environment as a therapeutic intervention in mental health facilities: A systematic literature review. HERD 2024, 17, 281–308. [Google Scholar] [CrossRef] [PubMed]
- Vaillo+Irigaray Architects. Psychogeriatric Center: Project Summary and Conceptual Documentation; Unpublished project documentation, Vaillo+Irigaray Architects Archive; Vaillo+Irigaray Architects: Pamplona, Spain, 2017. [Google Scholar]
- Vaillo+Irigaray Architects. Proyecto de Ejecución: Reforma y Ampliación Unidad Psiquiátrica U1.1. Centro Psicogeriátrico San Francisco Javier; Unpublished project documentation, Vaillo+Irigaray Architects Archive; Vaillo+Irigaray Architects: Pamplona, Spain, 2012. [Google Scholar]
- Vaillo+Irigaray Architects. Plan Director del Centro Psicogeriátrico San Francisco Javier; Unpublished project documentation, Vaillo+Irigaray Architects Archive; Vaillo+Irigaray Architects: Pamplona, Spain, 2010. [Google Scholar]
- Vaillo+Irigaray Architects. Proyecto de Derribo: Reforma y Ampliación Unidad Psiquiátrica U1.1. Centro Psicogeriátrico San Francisco Javier; Unpublished project documentation, Vaillo+Irigaray Architects Archive; Vaillo+Irigaray Architects: Pamplona, Spain, 2012. [Google Scholar]
- Vaillo+Irigaray Architects. Proyecto de Derribo: Reforma y Ampliación Unidad Psiquiátrica U1.2. Centro Psicogeriátrico San Francisco Javier; Unpublished project documentation, Vaillo+Irigaray Architects Archive; Vaillo+Irigaray Architects: Pamplona, Spain, 2012. [Google Scholar]
- Vaillo+Irigaray Architects. Proyecto de Ejecución: Planos de Planta Baja, Reforma y Ampliación Unidades Psiquiátricas U1.1 y U1.2; Unpublished project documentation, Vaillo+Irigaray Architects Archive; Vaillo+Irigaray Architects: Pamplona, Spain, 2012. [Google Scholar]
- Vaillo+Irigaray Architects. Proyecto de Ejecución: Planos de Planta Primera, Reforma y Ampliación Unidades Psiquiátricas U1.1 y U1.2; Unpublished project documentation, Vaillo+Irigaray Architects Archive; Vaillo+Irigaray Architects: Pamplona, Spain, 2012. [Google Scholar]
- Vaillo+Irigaray Architects. Anexo de Hormigón Arquitectónico U1.1 y U1.2. Centro Psicogeriátrico San Francisco Javier; Unpublished project documentation, Vaillo+Irigaray Architects Archive; Vaillo+Irigaray Architects: Pamplona, Spain, 2012. [Google Scholar]
- Vaillo+Irigaray Architects. Plan Especial de Reforma Interior del Centro Psicogeriátrico San Francisco Javier; Unpublished project documentation, Vaillo+Irigaray Architects Archive; Vaillo+Irigaray Architects: Pamplona, Spain, 2010. [Google Scholar]
- Vaillo+Irigaray Architects. Memoria Final de Obra: Reforma y Ampliación de las Unidades Psiquiátricas U1.1 y U1.2. Centro Psicogeriátrico San Francisco Javier; Unpublished project documentation, Vaillo+Irigaray Architects Archive; Vaillo+Irigaray Architects: Pamplona, Spain, 2018. [Google Scholar]
- Kalua, A. The case study methodology in architectural research: Evaluation of epistemological adequacy. Open House Int. 2024, 49, 638–649. [Google Scholar] [CrossRef]
- Arfa, F.H.; Lubelli, B.; Quist, W.; Zijlstra, H. A model of the adaptive reuse process of heritage buildings: Validation on four cases in the Netherlands. Des. Stud. 2024, 91–92, 101252. [Google Scholar] [CrossRef]
- Rosado, A.C.; Reimão Costa, M. The contribution of typological studies to the integrated rehabilitation of traditional buildings: Heritage enhancement of urban centres in Inner Alentejo, Portugal. Architecture 2024, 4, 35–45. [Google Scholar] [CrossRef]
- Ugalde-Blázquez, I.; Masó-Sotomayor, T.; Morán-García, P. The Bosch Vault: Reinterpretation and Exploration of the Limits of the Traditional Thin-Tile Vault in the Post-War Context. Buildings 2026, 16, 159. [Google Scholar] [CrossRef]
- Okamura, H.; Ouchi, M. Self-compacting concrete. J. Adv. Concr. Technol. 2003, 1, 5–15. [Google Scholar] [CrossRef]
- EFNARC. The European Guidelines for Self-Compacting Concrete: Specification, Production and Use; EFNARC: Surrey, UK, 2005. [Google Scholar]
- Domone, P.L.J. Self-compacting concrete: An analysis of 11 years of case studies. Cem. Concr. Compos. 2006, 28, 197–208. [Google Scholar] [CrossRef]
- Daczko, J.A. Self-Consolidating Concrete: Applying What We Know; CRC Press: Boca Raton, FL, USA, 2012. [Google Scholar]
- EN 12878; Pigments for the Colouring of Building Materials Based on Cement and/or Lime—Specifications and Methods of Test. European Committee for Standardization: Brussels, Belgium, 2014.
Figure 4.
General plan of uses. Intervention strategy-prosthesis. Source: Vaillo+Irigaray Architects archive, 2015.
Figure 4.
General plan of uses. Intervention strategy-prosthesis. Source: Vaillo+Irigaray Architects archive, 2015.

Figure 5.
(a) Ground-floor plan. Functional reprogramming of the ground floor, incorporating the outpatient area and a new circulation structure; (b) First-floor plan. Organisation of inpatient units, nursing stations, rooms and day spaces. Source: Vaillo+Irigaray Architects archive, 2018.
Figure 5.
(a) Ground-floor plan. Functional reprogramming of the ground floor, incorporating the outpatient area and a new circulation structure; (b) First-floor plan. Organisation of inpatient units, nursing stations, rooms and day spaces. Source: Vaillo+Irigaray Architects archive, 2018.

Figure 6.
Conceptual section and final image. Relationship between the historic volume and the new prosthetic body. Source: Vaillo+Irigaray Architects archive, 2018.
Figure 6.
Conceptual section and final image. Relationship between the historic volume and the new prosthetic body. Source: Vaillo+Irigaray Architects archive, 2018.

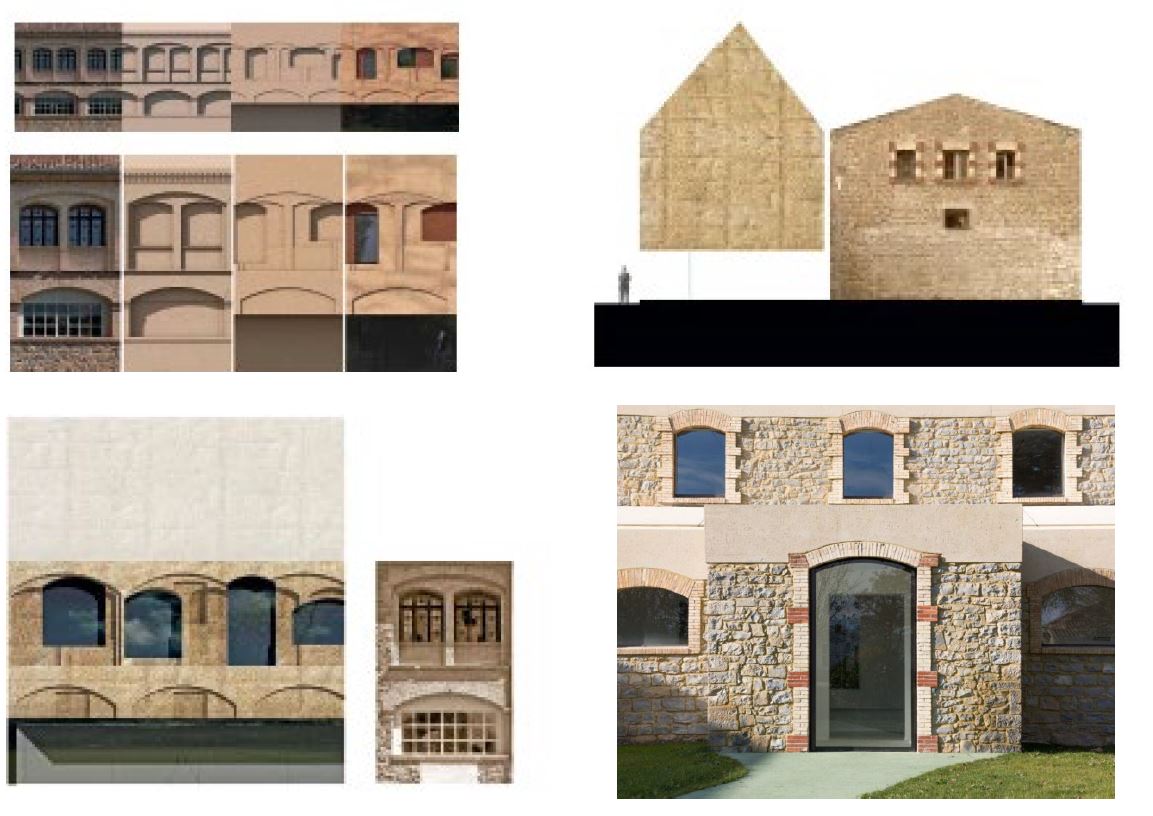
Figure 7.
South elevation development. Sequence from the existing elevation to the new volume, imprinted openings and final elevation. Source: Vaillo+Irigaray Architects archive, 2018.
Figure 7.
South elevation development. Sequence from the existing elevation to the new volume, imprinted openings and final elevation. Source: Vaillo+Irigaray Architects archive, 2018.

Figure 8.
Façade development. Translation of historic arches into reliefs in pigmented concrete. Source: Vaillo+Irigaray Architects archive, 2018.
Figure 8.
Façade development. Translation of historic arches into reliefs in pigmented concrete. Source: Vaillo+Irigaray Architects archive, 2018.

Figure 9.
Construction details. Interface between the historic masonry, the new structural system and the contemporary envelope. Source: Vaillo+Irigaray Architects archive, 2012.
Figure 9.
Construction details. Interface between the historic masonry, the new structural system and the contemporary envelope. Source: Vaillo+Irigaray Architects archive, 2012.

Figure 10.
Exterior view of the complex. Source: Vaillo+Irigaray Architects archive, 2012.

Table 2.
Analytical indicators of prosthetic memory.
| Indicator | Analytical question | Evidence used | Expected verification |
|---|---|---|---|
| Typological continuity | Does the intervention preserve or reactivate the pavilion-based logic? |
Historic plan, master plan, ground-floor plan, first-floor plan | Continuity of pavilions, courtyards, galleries, axes and voids |
| Environmental continuity | Does the intervention recover passive environmental principles? |
Sections, urbanization/landscape drawings, courtyards, circulation diagrams | Natural light, ventilation, open spaces, landscaped areas |
| Tectonic continuity |
Does the new work engage with the existing constructive logic? | Sections, elevations, details, concrete annexes |
Thicknesses, openings, joints, roofs, reliefs, structural continuity |
| Material compatibility |
Does the new material relate to the existing masonry without imitating it? | Concrete specifications, pigments, façade details, photographs | Pigmented concrete, mineral continuity, chromatic compatibility |
| Temporal continuity |
Does the intervention incorporate ageing as part of its material strategy? | Conceptual report, concrete annexes, façade studies |
Patina, weathering, durable surface, exposure according to orientation |
Table 3.
Diagnosis, evidence and intervention response.
| Diagnosed problem |
Documentary evidence | Intervention criterion | Built response |
|---|---|---|---|
| Parallel circulation systems | Inner and outer routes enclosing ground-floor rooms | Reorganisation of circulation | Hierarchised routes and clearer distribution |
| Overlapping flows | Patients, staff, supplies and technical services shared the same routes |
Functional separation | Differentiated circuits and new access points |
| Dimensional stenosis |
Narrow structural bays and insufficient pavilion length |
Selective extension | New prosthetic volumes attached to existing pavilions |
| Technical obsolescence |
Dispersed and superimposed energy networks |
Technical integration | New organisation of infrastructures and services |
| Loss of environmental performance |
Lack of natural light and ventilation in ground-floor areas |
Passive reactivation | Recovery of courtyards, openings and intermediate spaces |
| Constructive deterioration |
Poor condition of some buildings |
Selective demolition | Partial demolition and conservation of essential elements |
Table 4.
Architectural concrete as heritage mediation.
| Component | Technical specification | Constructive function | Heritage function |
|---|---|---|---|
| Cement | CEM II-AL | Reduces shrinkage and chromatic variation |
Promotes chromatic stability |
| Aggregate | Micro-concrete, maximum 12 mm |
Improves compactness and texture |
Produces mineral continuity |
| Water/cement ratio |
Maximum 0.45 | Reduces cracking | Promotes surface durability |
| Pigment | Inorganic, synthetic, 3–5% of cement weight | Colours the concrete in mass | Avoids applied imitation |
| Superplasticiser | 0.3–1% of cement weight | Ensures workability | Allows complex formwork |
| PP fibres | 3–9 kg/m³ | Controls cracking in façade reliefs |
Allows deep tectonic traces |
| Formwork | CNC-cut phenolic board | Defines the relief geometry | Translates historic arches into traces |
| Joints | Specific joint plan | Controls water and construction sequence | Makes construction legible |
Table 5.
Verification of the prosthetic memory framework.
| Indicator | Evidence found | Degree of verification |
|---|---|---|
| Typological continuity |
Master plan, pavilions, courtyards, galleries, low-rise additions |
High |
| Environmental continuity |
Courtyards, gardens, light, ventilation, intermediate spaces |
Medium–high |
| Tectonic continuity |
Sections, roofs, façade reliefs, structural concrete | High |
| Material compatibility |
Pigmented concrete, mineral continuity, non-mimetic treatment |
High |
| Temporal continuity |
Patina, weathering, ageing according to orientation and exposure |
Medium |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



