Submitted:
01 July 2026
Posted:
01 July 2026
You are already at the latest version
Abstract
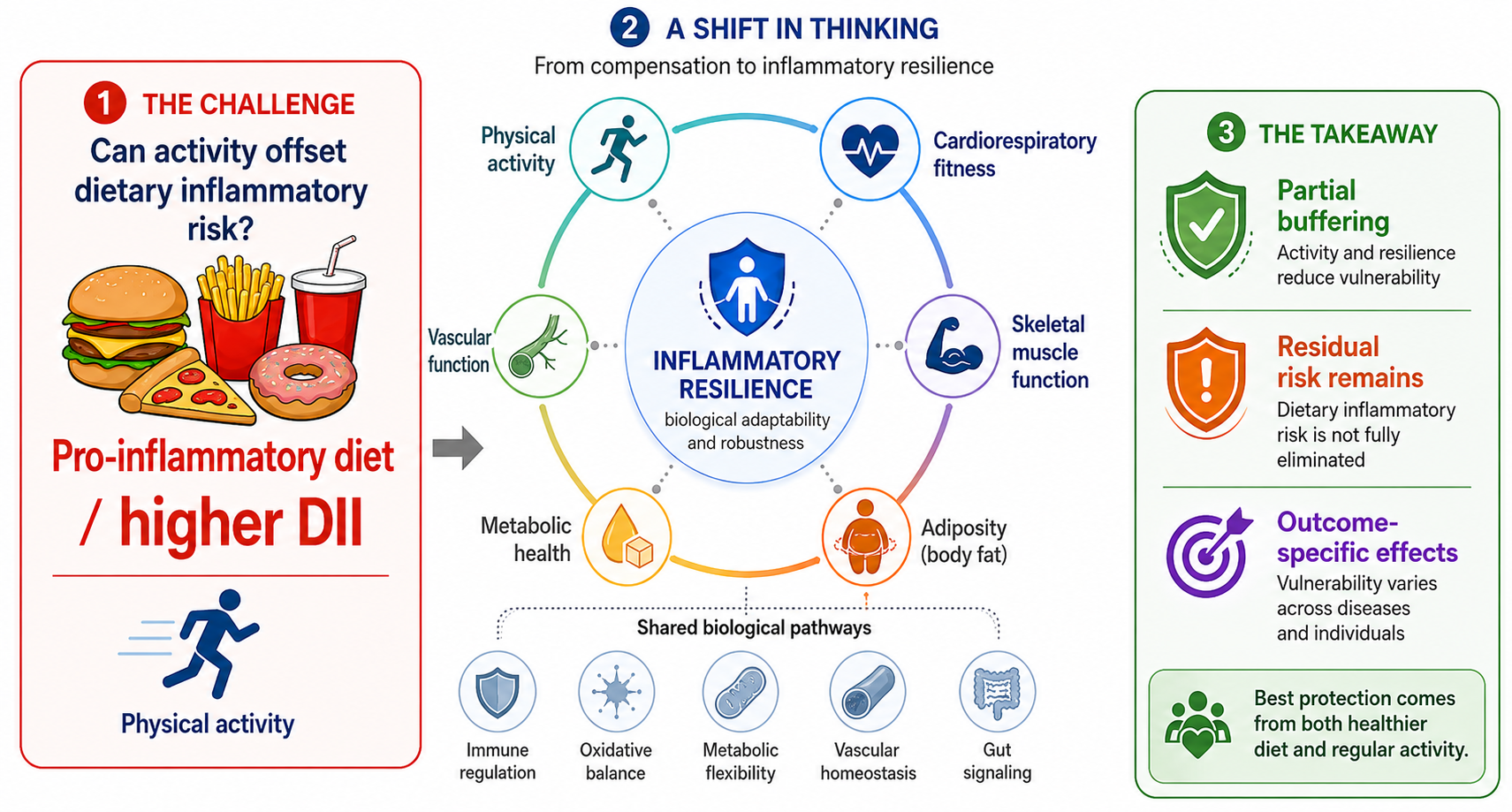
Whether physical activity can offset the health risks of a pro-inflammatory diet is a compelling question, but it becomes conceptually misleading when interpreted as simple behavioral compensation. This narrative review integrates evidence on dietary inflammatory potential, movement-related physiological capacity, and chronic disease vulnerability, with particular attention to the Dietary Inflammatory Index, biological translation pathways, and emerging joint diet–activity evidence. Pro-inflammatory dietary exposure may be translated into disease vulnerability through immune activation, oxidative stress, adipose tissue inflammation, metabolic dysfunction, endothelial impairment, and gut-related inflammatory signaling. Habitual movement and exercise training may influence many of these same pathways through skeletal muscle signaling, improved insulin sensitivity, reduced visceral adiposity, redox adaptation, vascular regulation, and higher cardiorespiratory fitness. Taken together, current human evidence is more consistent with partial buffering and joint risk stratification than with full compensation. We therefore propose an Inflammatory Resilience Framework in which physical activity, cardiorespiratory fitness, skeletal muscle function, adiposity, metabolic flexibility, vascular function, and baseline health status are positioned as modifiers of the biological translation from dietary inflammatory exposure to disease vulnerability. This framework shifts the research question from whether exercise cancels dietary risk to how movement-related physiological capacity modifies inflammatory risk expression across individuals, pathways, and outcomes.
Keywords:
dietary inflammatory index
; diet-related inflammation
; physical activity
; cardiorespiratory fitness
; metabolic flexibility
; endothelial function
1. Introduction: From Compensation to Inflammatory Resilience
Chronic low-grade systemic inflammation is increasingly understood as a cross-cutting biological process through which diet quality, adiposity, metabolic dysfunction, vascular impairment, and immune regulation may converge to shape vulnerability to non-communicable diseases. Unlike acute inflammation, which is essential for host defense and tissue repair, persistent low-grade inflammatory activation may contribute to insulin resistance, endothelial dysfunction, oxidative stress, altered immune signaling, and progressive tissue damage [1,2,3]. These processes are relevant to a wide range of health outcomes, including obesity, type 2 diabetes, cardiovascular disease, aging-related functional decline, and mortality. From a prevention perspective, inflammation is therefore better viewed as a modifiable risk context rather than a single target, because it reflects the interaction of lifestyle, metabolic, and physiological factors.
Within this context, dietary inflammatory potential offers a way to characterize diet not only by nutrient composition or food groups, but by its estimated tendency to promote or attenuate inflammatory processes. The Dietary Inflammatory Index (DII) and related energy-adjusted approaches were developed to estimate the inflammatory potential of diet based on evidence linking dietary components with inflammatory biomarkers [4,5]. In general, higher DII scores indicate a more pro-inflammatory dietary pattern, whereas lower scores reflect a more anti-inflammatory dietary profile. Evidence from review-level and outcome-specific syntheses has linked higher dietary inflammatory potential with elevated inflammatory biomarkers and greater risk of cardiometabolic, vascular, cancer-related, and mortality outcomes [6,7,8]. However, the health relevance of dietary inflammatory potential is unlikely to depend on diet alone. Its biological consequences may depend on the physiological condition of the host and the broader lifestyle context in which the diet is consumed.
Physical activity is central to this discussion because its relevance to inflammation extends beyond energy expenditure or weight control. Public health guidelines consistently identify physical activity as a core behavior for chronic disease prevention, but its biological relevance is not limited to caloric balance [9]. Regular physical activity and structured exercise may influence inflammatory risk through coordinated effects on cardiorespiratory fitness, skeletal muscle metabolism, adiposity, insulin sensitivity, endothelial function, mitochondrial adaptation, and immune–metabolic signaling [10,11,12,13]. Skeletal muscle is increasingly recognized not only as a contractile tissue, but also as an endocrine and metabolic organ capable of releasing myokines and influencing whole-body inflammatory tone [11]. These effects, however, are not uniform. They may vary according to exercise dose, intensity, modality, training status, age, sex, adiposity, baseline inflammation, and disease status. Thus, physical activity should not be viewed as a simple antidote to inflammatory risk, but as a potential modifier of how inflammatory exposures are biologically translated.
Although dietary inflammatory potential and physical activity have each been linked to inflammation-related health outcomes, they are still often examined as independent lifestyle factors rather than as interacting exposures. In many observational studies, physical activity is treated as a covariate when examining diet-related risk, while diet quality is similarly adjusted for when examining physical activity and health outcomes. This approach is useful for estimating independent associations, but it may obscure a more clinically relevant question: whether physical activity modifies the association between pro-inflammatory dietary exposure and downstream health risk. Recent cohort and population-based studies suggest that combined or joint lifestyle patterns involving diet quality, dietary inflammatory potential, and physical activity may provide a more informative risk profile than either behavior considered alone [14,15,16]. Emerging evidence has also begun to examine the joint relevance of dietary inflammatory potential and vigorous physical activity for aging-related biomarkers, although causal interpretation remains limited [17]. This perspective is important because diet and physical activity are not experienced, metabolized, or adapted to as isolated variables. A central premise of this review is that the same dietary inflammatory load may not translate into the same inflammatory or clinical consequences across different levels of physical activity, fitness, adiposity, or metabolic health.
The question “Can physical activity offset the health risks of a pro-inflammatory diet?” is therefore compelling, but the term “offset” requires careful interpretation. In public discourse, compensation often implies that one healthy behavior can cancel the harmful effects of another unhealthy exposure. Biologically, this assumption is difficult to justify as a general model. Diet and physical activity influence overlapping but non-identical pathways. Physical activity may attenuate selected downstream correlates of pro-inflammatory dietary exposure, such as excess adiposity, insulin resistance, endothelial dysfunction, or elevated inflammatory tone [10,12,14]. However, it does not remove the dietary exposure itself, nor should it be assumed to reverse all immune, oxidative, metabolic, vascular, or tissue-level effects associated with long-term pro-inflammatory dietary patterns. A compensation model is therefore insufficient, especially if it encourages the misleading interpretation that exercise provides permission for sustained dietary risk. A more precise question is not whether physical activity can erase dietary inflammatory risk, but under what conditions physical activity may buffer, reshape, or limit the biological translation of dietary inflammatory potential into disease vulnerability.
Accordingly, this narrative review moves beyond a compensation-based interpretation and proposes an inflammatory resilience framework. In this framework, physical activity does not simply counterbalance dietary risk; rather, it may modify the extent to which dietary inflammatory potential is translated into systemic inflammation, metabolic dysfunction, vascular impairment, and chronic disease vulnerability. This review does not present inflammatory resilience as a newly established biological mechanism. Rather, it adapts resilience thinking from challenge-response physiology to long-term lifestyle epidemiology by positioning physical activity, cardiorespiratory fitness, skeletal muscle function, adiposity, and metabolic flexibility as resilience-modifying factors [18]. The aims of this review are to: (1) summarize evidence linking dietary inflammatory potential to adverse health outcomes; (2) examine biological pathways through which physical activity may regulate inflammatory and metabolic risk; (3) evaluate current evidence on the joint and interactive effects of pro-inflammatory diets and physical activity; and (4) propose an inflammatory resilience framework to guide future research and integrated lifestyle recommendations. The central thesis is that physical activity should not be viewed as a license for dietary risk, but as a resilience-related factor that may partially modify the inflammatory consequences of dietary exposure.
2. Narrative Review Approach and Literature Selection
This review was developed as a narrative review with a conceptual framework orientation, rather than as a systematic review or meta-analysis. This distinction is important because the central question of the manuscript is not whether a pooled effect can be estimated, but how several bodies of evidence can be brought together to clarify a specific lifestyle-interaction problem. Therefore, the review did not aim to exhaustively identify all available studies, calculate summary estimates, or conduct a formal risk-of-bias assessment. Instead, it synthesized evidence from related but often separately examined domains, including dietary inflammatory potential, chronic low-grade inflammation, physical activity, cardiometabolic and vascular health, joint lifestyle exposures, and resilience-related physiology. This approach was considered appropriate because the main objective was conceptual integration and framework development, not quantitative effect estimation. Consistent with recommendations for improving the quality and transparency of narrative reviews, the literature search and selection process was structured to make the scope, rationale, and evidentiary basis of the review explicit [19,20].
Relevant literature was identified through searches of PubMed, Scopus, and Web of Science, supplemented by reference-list checking, citation tracking, and targeted searches for recent studies directly examining dietary inflammatory potential in relation to physical activity. The main search period covered studies published from 2005 to 2026, although earlier foundational papers were considered when they were necessary for conceptual or methodological grounding. Searches were organized around five concept blocks that reflected the logic of the manuscript rather than a formal systematic review protocol. The first block focused on dietary inflammatory potential and included terms such as “Dietary Inflammatory Index,” “energy-adjusted Dietary Inflammatory Index,” “dietary inflammatory potential,” “pro-inflammatory diet,” and “anti-inflammatory diet” [4,5,6]. The second block addressed health outcomes associated with dietary inflammatory potential, including cardiovascular disease, metabolic syndrome, type 2 diabetes, obesity, cancer-related outcomes, mortality, and aging-related vulnerability [6,7,8]. The third block focused on physical activity and inflammatory regulation using terms such as “physical activity,” “exercise,” “inflammation,” “CRP,” “IL-6,” “TNF-alpha,” “myokines,” “cardiorespiratory fitness,” “skeletal muscle,” “insulin sensitivity,” and “endothelial function” [9,10,11,12,13]. The fourth block focused on joint and interactive lifestyle evidence, including combinations of “Dietary Inflammatory Index,” “inflammatory diet,” “diet quality,” “physical activity,” “joint association,” “combined association,” and “interaction” [14,15,16,17]. The fifth block addressed resilience-related concepts, including “inflammatory resilience,” “physiological resilience,” “metabolic resilience,” “challenge-response physiology,” and “dietary challenge” [18].
Study selection was guided by relevance to the review’s conceptual question. Priority was given to original DII development and validation papers, conceptual papers, umbrella reviews, systematic reviews and meta-analyses, large cohort or population-based studies, studies directly examining DII or inflammatory diet together with physical activity, and mechanistic reviews explaining exercise-related inflammatory regulation. Studies focused only on isolated dietary supplements, animal-only mechanisms, or athletic performance outcomes were not emphasized unless they directly informed the dietary inflammatory potential–physical activity–health framework. Exercise-only studies were also used selectively, primarily when they clarified anti-inflammatory, metabolic, vascular, skeletal muscle, or fitness-related pathways relevant to the proposed framework.
The evidence was synthesized thematically rather than quantitatively. The main themes were dietary inflammatory exposure, biological translation pathways, exercise-related inflammatory regulation, joint diet–physical activity evidence, limitations of the compensation model, and resilience-modifying factors. Because much of the directly relevant evidence is observational, cross-sectional, or derived from secondary analyses of population datasets, causal claims were avoided when the study design did not support them. Accordingly, this review emphasizes conceptual integration, mechanistic plausibility, and future research development rather than definitive clinical prescription or quantitative effect estimation [21].
3. Dietary Inflammatory Potential as a Lifestyle Exposure
Dietary inflammatory potential refers to the extent to which habitual dietary patterns are estimated to promote or attenuate inflammatory processes through their combined nutrient, food, and bioactive profiles. This concept is broader than the effect of any single nutrient, supplement, or food item, because inflammatory responses to diet are more likely to reflect the cumulative pattern of intake than an isolated dietary component. A pro-inflammatory diet is typically characterized by lower intake of fiber-rich plant foods, fruits, vegetables, and anti-inflammatory bioactive compounds, together with greater intake of refined carbohydrates, saturated fats, processed foods, and other dietary components associated with adverse metabolic profiles. Conversely, a more anti-inflammatory dietary pattern is generally characterized by higher intakes of plant-based foods, unsaturated fats, micronutrients, and polyphenol-rich foods. These distinctions should not be interpreted as rigid categories, but as pattern-level tendencies that may vary across populations and dietary assessment methods. In this review, dietary inflammatory potential is treated as a lifestyle exposure rather than a narrow nutritional variable, because its biological expression is likely to be shaped by metabolic condition, adiposity, physical activity, and the broader behavioral context in which the diet is consumed [4,5,6].
The Dietary Inflammatory Index (DII) is one of the most widely used tools for estimating the inflammatory potential of diet. It was developed as a literature-derived and population-based index based on evidence linking dietary parameters with inflammatory biomarkers [4]. Higher DII scores are generally interpreted as indicating a more pro-inflammatory dietary pattern, whereas lower scores suggest a more anti-inflammatory profile [5]. Energy-adjusted versions of the DII have also been used to account for differences in total energy intake, which is particularly important in epidemiological research where dietary inflammatory potential may otherwise partly reflect overall food consumption rather than diet composition alone [22]. Related approaches, such as the empirical dietary inflammatory index, have been developed using food groups and circulating inflammatory biomarkers [23]. These indices support the broader premise that inflammatory potential can be assessed at the dietary pattern level. However, they should be understood as exposure indicators rather than direct measures of inflammatory biology. Because this Special Issue centers on the DII and because much of the directly relevant evidence uses DII or energy-adjusted DII, these indices serve as the primary dietary exposure anchors for the present review.
The relevance of DII for inflammatory health research is supported by construct validation studies linking higher dietary inflammatory scores with inflammatory biomarkers. Early validation work in postmenopausal women showed that DII scores were associated with inflammatory markers, supporting the index as a meaningful estimate of dietary inflammatory potential [24]. Additional population-based studies have examined associations between DII or energy-adjusted DII and markers such as C-reactive protein, interleukin-6, tumor necrosis factor-related measures, and other inflammatory indicators [25,26]. Meta-analytic evidence also suggests that higher DII scores are associated with elevated serum C-reactive protein, although the strength of this association varies across study populations, dietary assessment methods, and the number of dietary components available for DII calculation [27]. These findings support the use of DII as a risk-relevant dietary exposure marker, but they do not imply that DII precisely captures individual inflammatory status. Individual inflammatory responses remain influenced by adiposity, metabolic health, physical activity, medication use, age, sex, and existing disease conditions. This limitation is important for the present review because it helps explain why similar dietary inflammatory scores may not translate into identical biological or clinical risk across individuals.
Higher dietary inflammatory potential has also been associated with multiple adverse health outcomes. Review-level syntheses have linked higher DII scores with increased risk across several non-communicable disease domains, including cardiometabolic disorders, cardiovascular disease, cancer-related outcomes, and mortality [6,28]. Disease-specific evidence further supports this pattern. Meta-analyses have reported associations between higher DII and increased risk of diabetes mellitus, metabolic syndrome, and site-specific cancers [29,30,31]. Evidence on cardiovascular morbidity and mortality also supports the relevance of DII to vascular health [7]. More broadly, umbrella-level synthesis indicates that higher dietary inflammatory potential is associated with risk across several non-communicable chronic diseases and mortality outcomes [32]. These associations are biologically plausible because chronic low-grade inflammation, oxidative stress, insulin resistance, adipose tissue dysfunction, and vascular impairment are shared pathways across many of these conditions. Nevertheless, most available evidence remains observational, and studies differ in dietary assessment tools, DII components available for scoring, energy adjustment, covariate control, population characteristics, and outcome definitions. Therefore, DII should be interpreted as a useful risk-related exposure marker rather than as a stand-alone causal explanation for chronic disease. A concise summary of major health outcome domains associated with higher dietary inflammatory potential is provided in Table 1.
This distinction is important for the present review because dietary inflammatory potential does not operate as an isolated dietary signal. Individuals with similar DII scores may differ substantially in body composition, cardiorespiratory fitness, skeletal muscle function, metabolic flexibility, sleep, smoking, alcohol intake, medication use, and baseline inflammatory status. These factors may influence whether a given dietary inflammatory exposure is amplified, buffered, or translated into measurable biological risk. For example, a person with high visceral adiposity, low physical activity, and poor metabolic health may plausibly show a different inflammatory or metabolic response to a pro-inflammatory dietary pattern than a physically active person with higher fitness and preserved skeletal muscle function. Thus, dietary inflammatory potential is best viewed as one component of a broader lifestyle and physiological system, rather than as a fixed dietary signal that produces uniform health consequences across all individuals [1,2,3,9,10,11,12,13,14,28].
Framing DII as a lifestyle exposure clarifies the central logic of this review. The key question is not simply whether pro-inflammatory diets are associated with poor health outcomes, because that association has already been examined extensively. The more integrative question is how dietary inflammatory potential is biologically translated into inflammatory and clinical vulnerability, and why this translation may differ across levels of physical activity, fitness, adiposity, metabolic health, and physiological resilience. Accordingly, DII provides the dietary exposure anchor for the manuscript, but it does not complete the explanatory model. The next step is to examine the biological pathways through which dietary inflammatory potential may contribute to disease vulnerability, including immune activation, oxidative stress, adipose tissue inflammation, metabolic dysfunction, vascular impairment, and gut-related mechanisms.
4. Biological Translation from Dietary Inflammatory Exposure to Disease Vulnerability
Dietary inflammatory potential becomes clinically meaningful when a pattern-level dietary exposure is expressed through biological pathways that influence inflammatory tone, metabolic regulation, vascular function, and tissue vulnerability. As discussed above, DII and related indices are useful exposure markers, but they should not be treated as mechanisms in themselves [4,5,6]. The relevant question is how pro-inflammatory dietary patterns interact with host physiology, including immune regulation, redox balance, adiposity, insulin sensitivity, endothelial function, and gut-related signaling. These pathways are interconnected and may help explain why higher dietary inflammatory potential has been associated with several non-communicable disease outcomes [28,32]. Importantly, many of these pathways are also modifiable, which creates the conceptual basis for considering physical activity later in this review as a resilience-related modifier rather than as a simple compensatory behavior [33].
One central pathway involves immune activation and chronic low-grade inflammation. Pro-inflammatory dietary patterns may contribute to inflammatory signaling through excess energy intake, lower dietary quality, limited intake of anti-inflammatory nutrients and bioactive compounds, and greater exposure to dietary patterns that promote metabolic and immune stress [33]. Western-style dietary patterns, in particular, have been linked with innate immune activation, altered cytokine signaling, and inflammatory reprogramming of immune cells [34]. In human studies, higher dietary inflammatory scores have been associated with inflammatory biomarkers such as C-reactive protein, interleukin-6, tumor necrosis factor-related measures, and other inflammatory indicators, although the strength of these associations varies across populations and study designs [24,25,26,27]. This pathway is important because chronic low-grade inflammation may operate as a biological bridge between dietary exposure and downstream cardiometabolic, vascular, and aging-related vulnerability [1,2,3].
A second pathway involves oxidative stress and redox imbalance. Oxidative stress refers to a disturbance in redox signaling and control, particularly when oxidant production exceeds the capacity of antioxidant and repair systems to maintain physiological balance [35]. Diets characterized by low antioxidant density, high energy load, poor nutrient quality, and greater exposure to refined or processed foods may contribute to oxidative and inflammatory stress, especially in the presence of obesity, insulin resistance, or physical inactivity. Inflammation and oxidative stress can also reinforce one another: inflammatory cells can generate reactive species, while oxidative stress can activate redox-sensitive inflammatory pathways [36]. This reciprocal relationship is relevant to endothelial dysfunction, mitochondrial stress, tissue injury, and chronic disease vulnerability. However, the implication is not that antioxidant supplementation is the central solution. Rather, redox balance should be interpreted as one component of the broader biological translation from dietary inflammatory exposure to health risk.
Adipose tissue inflammation and metabolic dysfunction represent another key translation pathway. Visceral adipose tissue is not merely an energy-storage depot; it is an endocrine and immune-active tissue capable of releasing adipokines, cytokines, and inflammatory mediators. In obesity and metabolic dysfunction, adipose tissue expansion may be accompanied by immune-cell infiltration, altered adipokine balance, and chronic low-grade inflammation, which can contribute to insulin resistance and type 2 diabetes risk [37]. Fat distribution is also important because visceral and ectopic fat are more closely related to inflammatory and cardiometabolic consequences than body mass alone [38]. Pro-inflammatory dietary patterns may contribute to this pathway by supporting excess energy intake, poor metabolic flexibility, glycemic stress, or adiposity-related inflammation. This mechanism is especially relevant to the present framework because physical activity can influence several of these same processes, including visceral adiposity, insulin sensitivity, glucose handling, and skeletal muscle metabolic function.
Dietary inflammatory exposure may also contribute to vascular vulnerability through endothelial dysfunction and vascular inflammation. The endothelium regulates vascular tone, nitric oxide bioavailability, leukocyte adhesion, thrombosis, and vascular homeostasis. Under chronic inflammatory and oxidative stress, endothelial cells may shift toward a dysfunctional phenotype that supports atherosclerosis, impaired vasodilation, arterial stiffness, and cardiovascular risk [39]. Vascular inflammation and oxidative stress are closely linked, and their interaction can promote atherogenic processes and cardiovascular disease progression [40]. This pathway is consistent with evidence linking higher dietary inflammatory potential with cardiovascular risk and mortality [7]. It is also important for the logic of this review because physical activity may later be understood as a vascular resilience factor through improved endothelial function, shear stress-mediated adaptation, and broader cardiometabolic regulation.
Gut-related mechanisms provide an additional but supporting pathway. Diet can influence gut microbiota composition, microbial metabolites, intestinal barrier integrity, and host–microbe immune communication. Western-style dietary patterns have been associated with gut dysbiosis and systemic inflammation, although specific microbiome signatures vary across populations, dietary contexts, and measurement approaches [41]. Increased intestinal permeability and translocation of microbial products, including lipopolysaccharide, may contribute to metabolic endotoxemia and systemic inflammatory activation [42]. This pathway may connect dietary quality, adiposity, insulin resistance, and inflammatory tone. Nevertheless, in the present review, gut-related mechanisms should be interpreted as one part of a broader diet–inflammation system rather than as the dominant explanatory model. The central focus remains the interaction between dietary inflammatory potential and physical activity.
Taken together, these pathways suggest that dietary inflammatory potential is biologically translated through a network of immune, oxidative, adipose, metabolic, vascular, and gut-related mechanisms. These mechanisms do not act in isolation. Adipose tissue inflammation can worsen insulin resistance; oxidative stress can amplify endothelial dysfunction; gut-derived inflammatory signals can interact with metabolic inflammation; and chronic immune activation can reinforce vascular and tissue-level vulnerability. This interconnectedness helps explain why dietary inflammatory potential may be associated with diverse chronic disease outcomes, but it also highlights why risk translation may differ across individuals. Because many of these pathways are modifiable, they provide the mechanistic basis for examining physical activity not as a strategy that cancels dietary risk, but as a resilience-related factor that may influence how dietary inflammatory exposure is biologically expressed [10,11,12,13,33,37,39,41].
5. Physical Activity as an Anti-Inflammatory and Metabolic Resilience Factor
Physical activity is relevant to dietary inflammatory risk because it can influence several of the biological pathways through which pro-inflammatory dietary exposure may be translated into disease vulnerability. As outlined in the previous section, dietary inflammatory potential may affect health through interconnected immune, oxidative, metabolic, adipose, vascular, and gut-related mechanisms [33,37,39,41]. Physical activity should therefore not be interpreted only as energy expenditure or as a behavioral counterweight to excess caloric intake. Rather, it represents a repeated physiological stimulus that may shape inflammatory tone, metabolic flexibility, vascular function, skeletal muscle regulation, and broader physiological reserve [9,10,11,12,13]. This does not mean that physical activity cancels the effects of a pro-inflammatory diet. Instead, it provides a biological basis for asking whether physically active or fitter individuals may differ in how strongly dietary inflammatory exposure is expressed as downstream biological or clinical risk.
The inflammatory effects of exercise are context-dependent. Acute exercise, particularly when prolonged or very intense, may transiently increase stress-related and inflammatory signals as part of tissue remodeling, immune surveillance, and adaptation. In contrast, regular physical activity and repeated exercise training may support more favorable immune regulation over time, depending on training dose, recovery, nutritional status, adiposity, age, and baseline health condition [43]. Meta-analytic evidence from randomized trials also suggests that long-term exercise training can influence inflammatory biomarkers, including C-reactive protein, interleukin-6, and tumor necrosis factor-α, although responses vary by population and intervention characteristics [44]. This distinction is important for the present review because physical activity should not be framed as uniformly anti-inflammatory under all circumstances. Its relevance lies in repeated adaptation and improved regulatory capacity, not in the complete suppression of inflammatory signaling.
Skeletal muscle provides a central biological link between physical activity and inflammatory resilience. Contracting muscle is not merely a mechanical tissue; it functions as an endocrine and metabolic organ capable of communicating with adipose tissue, liver, vasculature, immune cells, and other organs through myokines and related signaling molecules [11,45]. These signals may influence substrate metabolism, insulin sensitivity, lipid handling, immune regulation, and systemic inflammatory tone. Exercise also induces skeletal muscle plasticity, including changes in mitochondrial function, substrate utilization, vascularization, and metabolic regulation [46]. From the perspective of dietary inflammatory risk, skeletal muscle is important because it represents a major site of glucose disposal and metabolic buffering. Individuals with better skeletal muscle function may therefore have greater capacity to handle dietary metabolic stress than those with low muscle function, insulin resistance, or impaired metabolic flexibility.
Physical activity may also influence dietary inflammatory risk through adiposity, insulin sensitivity, and metabolic flexibility. Visceral adipose tissue is a major amplifier of inflammatory and cardiometabolic risk, and exercise interventions can reduce visceral adipose tissue, although the magnitude of change depends on intervention dose, intensity, duration, and baseline adiposity [47]. Exercise training can also improve insulin sensitivity and glucose regulation through effects on skeletal muscle glucose uptake, insulin signaling, vascular delivery of substrates, and mitochondrial function [48]. More broadly, metabolic flexibility—the ability to adapt substrate oxidation and energy metabolism to changing physiological demands—is relevant to both dietary exposure and physical activity adaptation [49]. These pathways are directly connected to the inflammatory resilience framework because pro-inflammatory dietary patterns may be more harmful when accompanied by visceral adiposity, insulin resistance, and low metabolic flexibility, whereas physical activity may partially improve these host-level conditions.
Redox adaptation provides another mechanism through which physical activity may modify inflammatory vulnerability. Exercise can acutely increase reactive oxygen and nitrogen species, but these signals are not inherently harmful. When appropriately dosed and followed by adequate recovery, exercise-induced redox signaling contributes to adaptive responses involving antioxidant enzymes, mitochondrial remodeling, repair systems, and cellular stress resistance [50]. This is consistent with the concept of exercise hormesis, in which repeated exposure to manageable physiological stress promotes improved adaptive capacity [51]. This point is particularly important in the context of pro-inflammatory diets. The goal is not to eliminate all oxidative signaling, but to improve redox regulation so that oxidative stress and inflammatory activation do not become chronically maladaptive. Physical activity may therefore reshape redox responses rather than simply suppress oxidative processes.
Physical activity also acts on vascular pathways that overlap with diet-related inflammatory risk. Endothelial dysfunction is a key mechanism linking inflammation, oxidative stress, and cardiovascular vulnerability [39,40]. Aerobic exercise can improve endothelial function, in part through repeated increases in vascular shear stress, enhanced nitric oxide bioavailability, improved vascular reactivity, and reduced inflammatory–oxidative burden [52]. Higher-level synthesis also supports beneficial effects of exercise training interventions on flow-mediated dilation across different adult populations, although responses vary by baseline vascular health and training characteristics [53]. This vascular pathway is relevant because pro-inflammatory dietary exposure may contribute to endothelial impairment, whereas physical activity may strengthen vascular adaptability and reduce susceptibility to inflammatory and oxidative stressors.
Finally, cardiorespiratory fitness provides an important bridge between physical activity behavior and physiological reserve. Physical activity is a behavior, whereas cardiorespiratory fitness reflects accumulated adaptation across cardiovascular, respiratory, metabolic, and muscular systems. Large-scale evidence indicates that cardiorespiratory fitness is a strong predictor of all-cause and cardiovascular mortality, whether measured objectively or estimated [54]. Fitness has also been examined in relation to C-reactive protein and mortality, supporting its relevance to inflammatory and long-term health risk profiles [55]. For the present review, this distinction is important because self-reported physical activity may not fully capture resilience capacity. Two individuals may report similar activity levels but differ substantially in fitness, skeletal muscle function, adiposity, and inflammatory status. Cardiorespiratory fitness may therefore serve as a more integrated indicator of physiological resilience than physical activity behavior alone.
Together, these pathways suggest that physical activity may influence several biological systems through which dietary inflammatory potential is expressed. Immune regulation, skeletal muscle signaling, adiposity, insulin sensitivity, metabolic flexibility, redox adaptation, vascular function, and cardiorespiratory fitness should not be viewed as separate mechanisms; they form an interconnected regulatory network. This network provides mechanistic plausibility for the hypothesis that physical activity may partially buffer selected consequences of a pro-inflammatory diet. However, mechanistic plausibility should not be interpreted as evidence of full compensation. The major physical activity-related pathways that may contribute to inflammatory resilience are summarized in Table 2. The next section, therefore, moves from biological plausibility to the more direct question of whether available population and cohort evidence supports joint or interactive effects between dietary inflammatory potential and physical activity.
6. Joint and Interactive Evidence: Pro-Inflammatory Diets, Physical Activity, and Health Outcomes
Mechanistic plausibility alone cannot determine whether physical activity offsets the health risks of a pro-inflammatory diet. Section 4 and Section 5 outlined that dietary inflammatory potential and physical activity may converge on several overlapping biological systems, including inflammation, adiposity, insulin sensitivity, redox regulation, endothelial function, and physiological reserve. However, the central question of this review requires evidence from studies that examine diet and physical activity together rather than as separate covariates. In this context, it is important to distinguish independent associations, joint associations, statistical interaction, and true compensation. A lower risk among physically active individuals does not automatically mean that physical activity cancels dietary inflammatory risk. It may instead indicate partial buffering, joint risk stratification, or residual benefit from one favorable behavior despite another unfavorable exposure.
Broader evidence from diet quality and physical activity research supports the need to consider these behaviors jointly. In a large UK Biobank analysis, higher physical activity and better diet quality were jointly associated with lower all-cause, cardiovascular, and cancer mortality, suggesting that the lowest-risk profile is generally observed when both lifestyle behaviors are favorable [14]. More recent prospective evidence using device-measured physical activity has strengthened this joint-lifestyle perspective by reducing reliance on self-reported activity and examining diet and movement behavior together in relation to mortality, cardiovascular disease, and cancer outcomes [56]. Similarly, findings from the EPIC-Norfolk study indicate that physical activity, diet quality, and changes in these behaviors over time are jointly relevant to mortality risk [57]. These studies do not directly measure dietary inflammatory potential, but they provide an important epidemiological foundation: diet and physical activity are not interchangeable exposures, and their combined pattern may characterize long-term health risk more informatively than either behavior considered alone.
More directly relevant evidence has begun to examine the inflammatory diet or DII together with physical activity. In U.S. adults, joint analysis of anti-inflammatory diet and vigorous leisure-time physical activity showed that the most favorable mortality profile was observed among individuals who combined an anti-inflammatory diet with sufficient vigorous activity [58]. This type of finding supports a combined-lifestyle interpretation rather than a simple compensation model. If vigorous activity is associated with lower risk but does not clearly eliminate the disadvantage associated with a pro-inflammatory diet, the evidence is more consistent with partial buffering than with full compensation. Other NHANES-based evidence has linked physical activity and DII with overweight or obesity, suggesting that high dietary inflammatory potential remains relevant to adiposity-related risk even when physical activity is considered [59]. Additional work has examined whether interaction and joint effects between physical activity and DII are associated with stroke risk, directly addressing whether physical activity modifies diet-related inflammatory vulnerability [60]. Evidence has also extended into clinical or disease-specific contexts, including diabetic kidney disease and post-myocardial infarction systemic inflammation, where DII and physical activity adherence appear to have combined or potentially synergistic relevance to inflammatory or disease-related outcomes [61,62]. Together with earlier studies on inflammatory diet, physical activity domains, abdominal adipose tissue, and phenotypic age acceleration [15,16,17], these findings suggest that the evidence base is gradually moving from isolated lifestyle-factor models toward interaction-informed approaches.
The interpretation of this literature requires methodological caution. An independent association means that dietary inflammatory potential and physical activity are each associated with an outcome after mutual adjustment. A joint association compares combined exposure categories, such as high DII with low activity or low DII with high activity, in relation to risk. Statistical interaction asks whether the association between dietary inflammatory potential and an outcome differs across levels of physical activity, either on additive or multiplicative scales. Compensation is a stronger claim because it implies that sufficient physical activity neutralizes the excess risk associated with a pro-inflammatory dietary pattern. These concepts are related but not equivalent. Recommendations for reporting interaction analyses emphasize the need to present effect modification and joint effects clearly, because statistical interaction, biological interaction, and public health interpretation may not align perfectly [63]. Therefore, even when a study reports a significant interaction or a lower-risk active subgroup, it should not be interpreted automatically as evidence that exercise cancels dietary inflammatory exposure.
The outcomes most plausibly influenced by partial buffering are those closely connected to the pathways reviewed in Section 4 and Section 5. Physical activity may be especially relevant to adiposity-related and metabolic outcomes because it can influence visceral adipose tissue, insulin sensitivity, skeletal muscle glucose disposal, and metabolic flexibility [37,38,47,48,49]. It may also be relevant to vascular and inflammatory outcomes through effects on endothelial function, vascular adaptation, redox regulation, and cardiorespiratory fitness [39,40,50,51,52,53,54,55]. This mechanistic overlap helps explain why DII–physical activity studies often focus on outcomes such as obesity, abdominal adiposity, type 2 diabetes, stroke, diabetic kidney disease, systemic inflammation, and cardiovascular mortality [15,16,17,58,59,60,61,62]. However, the plausibility of partial buffering should not be confused with uniform protection across all outcomes. Some pathways may be more responsive to physical activity than others. For example, physical activity may improve insulin sensitivity or endothelial function, but it does not remove the dietary pattern that contributes to inflammatory exposure. Similarly, higher fitness may indicate greater physiological reserve, but it does not necessarily erase long-term dietary inflammatory load, especially when exposure is persistent or accompanied by adiposity, sleep disruption, smoking, medication use, or existing disease.
Taken together, current evidence supports a cautious interpretation. Diet quality and physical activity should be considered jointly, and emerging DII-focused studies suggest that physical activity may modify or attenuate selected risks associated with pro-inflammatory dietary exposure. Nevertheless, the broader lifestyle literature does not support the conclusion that physical activity replaces diet quality. Rather, favorable diet and sufficient physical activity together are generally associated with the lowest risk [14,56,57]. Direct inflammatory diet and DII studies also suggest that physical activity may reduce vulnerability in some contexts, but they do not provide a sufficient basis for claiming full compensation [15,16,17,58,59,60,61,62]. This distinction is important for public health messaging. Interpreting physical activity as a license for dietary risk may undermine the value of improving diet quality, whereas interpreting diet and physical activity as interacting lifestyle factors allows for a more balanced and biologically plausible model.
Several limitations of the current evidence further restrict strong compensation claims. Many studies rely on self-reported physical activity, which may misclassify activity volume, intensity, domain, and sedentary behavior. DII calculation also varies according to dietary assessment method, available dietary components, energy adjustment, and population characteristics. Moreover, many directly relevant studies are cross-sectional or observational, limiting causal inference. Few studies simultaneously include dietary inflammatory potential, objectively measured physical activity, cardiorespiratory fitness, skeletal muscle function, adiposity, inflammatory biomarkers, and formal interaction testing. This is a major limitation because physical activity behavior alone may not capture the physiological resilience capacity most relevant to inflammatory risk translation. These limitations suggest that the compensation question should be reframed. The key issue is not whether physical activity cancels dietary inflammatory risk, but how physical activity, fitness, skeletal muscle, adiposity, and metabolic health modify the biological and clinical expression of that risk.
7. Why Compensation Is an Incomplete Model
The compensation question is compelling because it reflects a common public health intuition: whether one favorable behavior can counterbalance an unfavorable one. In the present context, this question is often expressed as whether physical activity can offset the health risks of a pro-inflammatory diet. This framing is understandable because diet and physical activity are commonly discussed together in clinical, athletic, and public health settings. Evidence reviewed above indicates that favorable diet quality and sufficient physical activity are jointly associated with lower risk, while emerging studies using inflammatory diet or DII-based exposures suggest that physical activity may modify selected outcomes [14,56,57,58,59,60,61,62]. However, joint relevance should not be interpreted as full cancellation. The available evidence supports a more cautious interpretation: physical activity may partially buffer or reshape some consequences of dietary inflammatory exposure, but it should not be understood as erasing that exposure.
Diet and physical activity are related but not interchangeable exposures. Diet provides energy, macronutrients, micronutrients, bioactive compounds, food matrices, and inflammatory or anti-inflammatory dietary signals [4,5,6,7,8]. Physical activity, in contrast, provides mechanical loading, muscle contraction, metabolic demand, vascular shear stress, endocrine signaling, immune regulation, and training adaptation [43,45,47,52,54]. These two lifestyle domains overlap biologically, particularly in relation to adiposity, insulin sensitivity, oxidative stress, endothelial function, and inflammatory tone [33,37,39,41]. Yet their upstream inputs and downstream consequences are not identical. A physically active individual may have better metabolic flexibility or vascular function, but this does not remove the dietary pattern that contributes to inflammatory exposure. Likewise, an anti-inflammatory dietary pattern may reduce inflammatory load, but it does not reproduce the muscle, vascular, and cardiorespiratory adaptations induced by repeated physical activity.
For this reason, buffering is a more appropriate concept than compensation. Buffering implies that one factor may reduce, delay, or reshape the biological expression of another exposure. Compensation implies a stronger form of neutralization. In aging and health research, physical resilience has been conceptualized as the capacity to resist or recover from functional decline after exposure to a health stressor [64]. This idea is useful here because a pro-inflammatory diet can be understood as a chronic lifestyle exposure that may increase inflammatory and metabolic stress over time. Physical activity may improve the host’s capacity to respond to that exposure, but this does not mean that the exposure disappears. Current joint evidence is therefore more consistent with partial buffering, residual risk, and risk modification than with a simple “exercise cancels diet” interpretation [14,58,59,60,61,62].
The limitations of compensation are also outcome-specific. Physical activity is most likely to buffer outcomes that are closely tied to adiposity, insulin sensitivity, glucose regulation, endothelial function, inflammatory tone, and cardiorespiratory fitness. This is consistent with evidence linking DII and inflammatory diet exposures with obesity, abdominal adiposity, type 2 diabetes-related outcomes, stroke risk, diabetic kidney disease, systemic inflammation, and mortality [15,16,17,58,59,60,61,62]. These outcomes overlap with pathways that are responsive to physical activity, including visceral adiposity, skeletal muscle glucose uptake, redox adaptation, endothelial function, and fitness-related physiological reserve [47,48,49,50,51,52,53,54,55]. However, the plausibility of buffering should not be generalized to all health outcomes. Long-latency diseases, cancer-related pathways, cumulative dietary exposure, medication use, aging, sleep disruption, smoking, and existing disease status may all influence whether physical activity meaningfully attenuates risk.
The compensation model also underestimates population and phenotype specificity. Physical activity behavior alone may not capture the physiological capacity most relevant to inflammatory risk translation. Two individuals may report similar activity levels but differ substantially in cardiorespiratory fitness, skeletal muscle mass and function, visceral adiposity, metabolic flexibility, vascular health, medication use, disease burden, and inflammatory status [54,55,63]. These differences may determine whether the same dietary inflammatory exposure produces minimal disturbance, moderate vulnerability, or substantial disease risk. A resilience-based framework is better suited to this heterogeneity because it can accommodate biological processes across levels and time scales rather than reducing risk interpretation to a single behavior or biomarker [65]. This is particularly important for dietary inflammatory potential, which is expressed gradually through interacting immune, metabolic, vascular, and tissue-level pathways.
This conceptual shift from compensation to inflammatory resilience is illustrated in Figure 1. The compensation model assumes a relatively simple trade-off: a pro-inflammatory diet increases risk, while physical activity counterbalances or cancels that risk. The inflammatory resilience model offers a more cautious and mechanism-informed interpretation. It views dietary inflammatory potential as an exposure whose translation into disease vulnerability may be modified by physical activity, fitness, skeletal muscle function, adiposity, metabolic health, vascular regulation, and baseline disease status. In this model, physical activity is not a license for dietary risk. It is a resilience-related modifier that may reduce vulnerability in some contexts, while residual dietary risk may remain.
For these reasons, the question should move from whether physical activity offsets a pro-inflammatory diet to how physical activity modifies the biological translation of dietary inflammatory exposure into disease vulnerability. This reframing better accommodates partial effects, pathway specificity, population heterogeneity, and the distinction between behavioral exposure and physiological capacity. The next section, therefore, formalizes this logic as an inflammatory resilience framework.
8.8. The Inflammatory Resilience Framework
The Inflammatory Resilience Framework conceptualizes dietary inflammatory potential as a chronic lifestyle exposure whose biological translation into disease vulnerability may be modified by physical activity and related physiological traits. Rather than presenting inflammatory resilience as a newly established biological mechanism, the framework uses resilience thinking to address a lifestyle-interaction problem: why individuals with similar dietary inflammatory exposure may differ in inflammatory, metabolic, vascular, and clinical vulnerability. Within this framework, DII and related indices represent the dietary exposure layer [4,5]. Immune activation, adipose tissue inflammation, and endothelial impairment represent key biological translation pathways [33,37,39]. Physical activity, skeletal muscle function, cardiorespiratory fitness, and baseline physiological reserve are positioned as resilience modifiers rather than as compensatory substitutes for diet [43,45,54,64].
The first layer of the framework is the dietary inflammatory exposure layer. DII, E-DII, and related inflammatory diet indices are useful because they summarize the inflammatory potential of habitual dietary intake across nutrients, foods, and bioactive components [4,22]. These indices are not mechanisms by themselves; they are exposure markers that estimate whether a dietary pattern is more likely to promote or attenuate inflammatory tone. Their interpretation depends on dietary assessment quality, available dietary components, energy adjustment, population characteristics, and the broader dietary pattern in which individual nutrients are consumed [23,24]. For this reason, the framework treats DII as an entry point into biological risk translation, not as a complete causal explanation. A higher inflammatory diet score should therefore be interpreted as a risk-relevant exposure whose biological expression may vary according to host physiology and lifestyle context [28,32].
The second layer is the biological translation layer. Dietary inflammatory potential may be expressed through several interacting pathways rather than through one isolated mechanism. Pro-inflammatory dietary patterns may contribute to chronic low-grade immune activation and altered cytokine signaling [33,34]. They may also interact with oxidative stress and redox imbalance, particularly when inflammatory activation and reactive species production reinforce each other [35,36]. Adipose tissue inflammation and insulin resistance provide another translation pathway, especially when visceral adiposity amplifies metabolic and inflammatory stress [37,38]. Vascular pathways are also relevant because endothelial dysfunction links inflammation, oxidative stress, and cardiovascular vulnerability [39,40]. Gut-related mechanisms, including changes in microbiota composition, intestinal barrier function, and metabolic endotoxemia, may further contribute to systemic inflammatory tone [41,42]. These pathways should be understood as interconnected nodes within a risk-translation network, not as a single linear sequence from diet to disease.
The third layer consists of resilience modifiers. Physical activity is the primary behavioral modifier in this framework, but its biological meaning extends beyond movement volume alone. Regular physical activity and exercise training may influence immune regulation and chronic inflammatory biomarkers [43,44]. Skeletal muscle contraction and exercise-induced myokine signaling connect muscle function with adipose tissue, liver, vasculature, and immune regulation [45,46]. Exercise may also reduce visceral adiposity, improve insulin sensitivity, and enhance metabolic flexibility, thereby modifying the host conditions through which dietary inflammatory exposure may become metabolically harmful [47,48,49]. Redox and vascular adaptation are also important because exercise-induced physiological stress can promote antioxidant defense, endothelial function, and vascular responsiveness when appropriately dosed [50,52]. Cardiorespiratory fitness then represents an integrated marker of physiological reserve and long-term health risk [54,55]. Together, these modifiers help explain why the same dietary inflammatory exposure may have different biological and clinical consequences across individuals.
The fourth layer is the outcome vulnerability layer. The framework does not assume that all outcomes are equally modifiable by physical activity. Instead, it accommodates outcome-specific vulnerability. Outcomes closely related to adiposity, glucose regulation, endothelial function, systemic inflammation, and fitness may be more plausibly influenced by physical activity than outcomes driven by long-latency exposures or less modifiable biological processes. This interpretation is consistent with evidence linking dietary inflammatory potential with cardiometabolic disease, metabolic syndrome, diabetes, cancer-related outcomes, and mortality [7,32]. It is also consistent with emerging studies showing joint or interactive relevance of inflammatory diet and physical activity for mortality, overweight or obesity, stroke, diabetic kidney disease, and systemic inflammation [58,59,60,61,62]. Thus, the framework supports risk stratification and pathway-specific modification, not a universal claim that exercise protects equally against all consequences of a pro-inflammatory diet.
A central contribution of the framework is that it distinguishes several possible patterns of risk translation. The first is amplified translation, in which high dietary inflammatory potential occurs alongside low physical activity, low fitness, poor muscle function, visceral adiposity, and metabolic dysfunction. In this pattern, dietary exposure is more likely to be expressed as systemic inflammation and disease vulnerability. The second is partial buffering, in which high dietary inflammatory potential occurs in a physically active or higher-fitness individual. In this pattern, physical activity may attenuate selected downstream pathways, but residual dietary risk remains. The third is low-exposure resilience, in which lower dietary inflammatory potential and sufficient physical activity coexist, producing the most favorable lifestyle profile. The fourth is latent vulnerability, in which moderate dietary inflammatory exposure appears clinically tolerable under stable conditions but may become more harmful with aging, inactivity, weight gain, illness, poor sleep, or declining fitness. These patterns are more consistent with a resilience-based interpretation than with a binary compensation model [56,58,64,65].
The framework also has measurement implications. Future studies should not rely only on DII and self-reported physical activity. A stronger test of inflammatory resilience would combine inflammatory diet indices with objective physical activity, sedentary behavior, cardiorespiratory fitness, skeletal muscle mass or function, adiposity distribution, glycemic markers, inflammatory biomarkers, endothelial or vascular indicators, and longitudinal outcomes. Device-based physical activity measurement can strengthen exposure assessment by capturing intensity, duration, and movement patterns more precisely than self-report alone [66]. Similarly, muscle function should be considered because grip strength and related functional indicators are associated with major disease outcomes and all-cause mortality, making them relevant markers of physiological reserve [67]. These measures would allow researchers to test whether physical activity behavior, fitness, and muscle function modify the translation of dietary inflammatory exposure into biological and clinical risk, rather than merely coexist with lower-risk profiles.
Conceptually, the framework improves on compensation language in three ways. First, it preserves the importance of diet quality by treating dietary inflammatory potential as an exposure that cannot simply be erased. Second, it preserves the biological value of physical activity by recognizing its effects on immune, metabolic, vascular, muscular, and fitness-related systems. Third, it accommodates heterogeneity: individuals differ in age, sex, adiposity, fitness, disease status, medication use, sleep, smoking, and baseline inflammatory burden. These differences may determine whether the same dietary inflammatory exposure is amplified, buffered, or only weakly expressed. For clinical and public health communication, this framing avoids the misleading message that exercise cancels a poor diet while still recognizing that physical activity may reduce vulnerability under some conditions [14,57,60].
The proposed Inflammatory Resilience Framework is summarized in Figure 2. Its purpose is not to replace existing diet or physical activity guidelines, but to provide a structure for studying their interaction more precisely. The framework encourages future research to move beyond mutual adjustment models and toward interaction testing, mediation analysis, objective movement assessment, physiological reserve indicators, and longitudinal risk trajectories. The next section translates this framework into applications, research gaps, and future study designs.
9. Applications, Research Gaps, and Future Directions
The Inflammatory Resilience Framework provides a structure for moving future research beyond the question of whether physical activity compensates for a pro-inflammatory diet. The preceding sections suggest that dietary inflammatory potential should be treated as a measurable exposure, while physical activity, cardiorespiratory fitness, skeletal muscle function, adiposity, and metabolic health may shape how strongly this exposure is translated into biological and clinical vulnerability [4,5,64,65]. Emerging joint evidence also indicates that diet and physical activity are better studied together than as isolated covariates [56,58,60]. The next stage of research should therefore test not only whether physical activity is associated with lower risk, but whether it modifies the pathway from dietary inflammatory exposure to inflammatory biomarkers, metabolic dysfunction, vascular impairment, and disease outcomes.
A first priority is to improve exposure and behavior measurement. DII and E-DII depend on dietary assessment quality, available dietary components, energy adjustment, and population-specific dietary patterns [4,5,22]. This is particularly important because emerging DII–physical activity studies often rely on observational datasets with heterogeneous dietary inputs and self-reported lifestyle variables [58,60]. Studies using self-reported diet should therefore follow best practices for validation and interpretation of dietary assessment methods [68]. Physical activity measurement also requires greater precision. Device-based methods can capture intensity, duration, and movement patterns more directly than self-report, but accelerometer data collection and processing require transparent decisions [66,69]. Sedentary behavior should also be measured explicitly rather than treated as the absence of exercise, because sedentary behavior and physical inactivity are related but distinct constructs [70]. These improvements would strengthen both the dietary exposure layer and the resilience-modifier layer of the framework.
A second priority is to include physiological reserve indicators. Section 5 and Section 8 emphasized that physical activity behavior is not identical to physiological capacity. Skeletal muscle signaling, exercise-induced adaptation, and cardiorespiratory fitness provide resilience-relevant information that cannot be fully captured by asking whether a person is active [45,46,54]. Cardiorespiratory fitness should therefore be considered because it reflects integrated cardiovascular, respiratory, muscular, and metabolic function and has been proposed as a clinically meaningful vital sign [71]. Muscular fitness and function should also be included, especially in older adults or metabolically vulnerable populations. Sarcopenia-related consensus definitions emphasize muscle strength and function rather than muscle mass alone, supporting the idea that functional capacity is central to health risk assessment [72]. Within this framework, fitness and muscle function help distinguish movement behavior from biological reserve.
A third priority is to measure biological translation pathways directly. Earlier sections showed that dietary inflammatory potential may be linked with inflammatory biomarkers and may be expressed through immune, adipose, metabolic, vascular, redox, and gut-related pathways [24,27,33,37]. Future studies should therefore include biomarker panels that can capture inflammatory status, metabolic dysfunction, adipose-related signaling, vascular impairment, and redox regulation. Human nutrition studies require careful biomarker selection because no single marker can fully represent chronic inflammation [73]. Dietary biomarkers and omics-informed approaches may also help validate exposure assessment and clarify how dietary patterns are biologically expressed [74]. These methods would allow researchers to test whether physical activity modifies the biological translation from dietary inflammatory exposure to disease vulnerability, rather than merely associating with final outcomes.
A fourth priority is to strengthen analytic design. Direct DII–physical activity studies have begun to test joint effects and interactions, but many remain observational, cross-sectional, or limited by available variables [58,60,61]. Mediation analysis can help test whether inflammatory biomarkers, adiposity, insulin resistance, or endothelial function explain part of the relationship between dietary inflammatory potential and health outcomes [75]. When randomized trials are not available, observational cohorts may be strengthened through causal inference approaches, including target trial emulation [76]. Repeated-measure designs are also important because lifestyle behaviors, body composition, fitness, and inflammatory status can change over time. Evidence from physical activity trajectory research shows that changes in activity patterns can be meaningfully related to mortality risk, supporting the need to model diet, physical activity, biomarkers, and fitness longitudinally rather than relying only on baseline exposure [77].
A fifth priority is to move from observational evidence toward combined lifestyle interventions. Existing joint evidence suggests that a favorable diet and sufficient physical activity together generally define the lowest-risk profile, but this does not prove that physical activity fully buffers dietary inflammatory risk [14,56,58]. A stronger test of inflammatory resilience would come from trials that combine anti-inflammatory dietary strategies with structured physical activity or exercise training while also measuring mechanistic endpoints. The Diabetes Prevention Program remains an important precedent showing that lifestyle intervention can reduce type 2 diabetes incidence in high-risk adults [78]. However, longer-term lifestyle intervention evidence also shows that effects may vary by outcome, population, and disease context, as illustrated by Look AHEAD in adults with type 2 diabetes [79]. Future trials should therefore include both clinical endpoints and mechanistic endpoints, rather than relying only on final disease outcomes.
A sixth priority is to examine heterogeneity and precision prevention. Not all individuals with high dietary inflammatory potential will show the same biological response, and not all physically active individuals will have the same resilience capacity. Fitness, skeletal muscle function, age, adiposity, baseline inflammation, disease status, medication use, sleep, smoking, and socioeconomic context may all modify risk translation [54,55,67]. Personalized nutrition frameworks emphasize that dietary responses vary across individuals and contexts [80]. Similarly, treatment-effect heterogeneity frameworks can help identify who benefits most from a specific intervention or combined lifestyle strategy [81]. For the present framework, future studies should not ask only whether physical activity modifies DII-related risk on average, but for whom, under what conditions, and through which biological pathways.
The main research priorities for testing and applying the Inflammatory Resilience Framework are summarized in Table 3. Together, these directions can help move the field from compensation-oriented questions toward mechanism-informed, phenotype-sensitive lifestyle research. The practical goal is not to suggest that physical activity permits a pro-inflammatory diet, but to clarify how diet quality, movement behavior, physiological reserve, and biological vulnerability interact in shaping long-term health risk.
10. Conclusions
The question of whether physical activity can offset the health risks of a pro-inflammatory diet is important, but it becomes too narrow when framed as simple behavioral compensation. The evidence reviewed in this article suggests that dietary inflammatory potential and physical activity should be understood as interacting lifestyle exposures rather than interchangeable behaviors. Pro-inflammatory dietary patterns may contribute to disease vulnerability through immune activation, oxidative stress, adipose tissue inflammation, metabolic dysfunction, endothelial impairment, and gut-related inflammatory signaling. Physical activity may influence several of these same systems through skeletal muscle signaling, improved insulin sensitivity, lower visceral adiposity, redox adaptation, vascular regulation, and higher cardiorespiratory fitness. However, overlap in biological pathways should not be interpreted as evidence that one behavior cancels the other.
The proposed Inflammatory Resilience Framework reframes the issue from whether exercise cancels dietary risk to how physical activity modifies the biological translation of dietary inflammatory exposure into disease vulnerability. This distinction is central to the manuscript. Physical activity may partially buffer selected inflammatory, metabolic, and vascular consequences of a pro-inflammatory diet, but it should not be interpreted as eliminating dietary inflammatory exposure or removing residual risk. The most defensible interpretation is that favorable diet quality and sufficient physical activity together are likely to provide the most protective lifestyle profile, whereas physical activity alone should not be presented as permission for sustained dietary risk.
Future research should test this framework using repeated dietary assessment, objective physical activity and sedentary behavior measures, cardiorespiratory and muscular fitness indicators, inflammatory and metabolic biomarkers, longitudinal designs, interaction and mediation analyses, and combined lifestyle interventions. Such studies can clarify which outcomes are most responsive, which populations benefit most, and which biological pathways explain heterogeneity in response. For clinical and public health communication, the message should remain balanced: physical activity is not a license for dietary risk, but it may be an important resilience-related modifier within a broader strategy of inflammatory risk reduction.
Author Contributions
Conceptualization, J.Y., H.Y. and C.-H.S.; methodology, J.Y., H.Y. and C.-H.S.; literature search and evidence synthesis, J.Y., J.D. and C.-C.W.; writing—original draft preparation, J.Y.; writing—review and editing, J.Y., J.D., H.Y., C.-C.W. and C.-H.S.; visualization, J.Y. and C.-H.S.; supervision, H.Y. and C.-H.S.; project administration, H.Y. and C.-H.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CRP | C-reactive protein |
| DII | Dietary Inflammatory Index |
| E-DII | Energy-adjusted Dietary Inflammatory Index |
| IL-6 | Interleukin-6 |
| METs | Metabolic equivalents |
| NHANES | National Health and Nutrition Examination Survey |
| TNF-α | Tumor necrosis factor-alpha |
| VO₂max | Maximal oxygen uptake |
| VO₂peak | Peak oxygen uptake |
References
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Fabbri, E. Inflammageing: Chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 2018, 15, 505–522. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S. Inflammation, metaflammation and immunometabolic disorders. Nature 2017, 542, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Hébert, J.R.; Shivappa, N.; Wirth, M.D.; Hussey, J.R.; Hurley, T.G. Perspective: The Dietary Inflammatory Index (DII)—Lessons learned, improvements made, and future directions. Adv. Nutr. 2019, 10, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Marx, W.; Veronese, N.; Kelly, J.T.; Smith, L.; Hockey, M.; Collins, S.; Trakman, G.L.; Hoare, E.; Teasdale, S.B.; Wade, A.; et al. The Dietary Inflammatory Index and human health: An umbrella review of meta-analyses of observational studies. Adv. Nutr. 2021, 12, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Godos, J.; Hébert, J.R.; Wirth, M.D.; Piuri, G.; Speciani, A.F.; Grosso, G. Dietary Inflammatory Index and cardiovascular risk and mortality—A meta-analysis. Nutrients 2018, 10, 200. [Google Scholar] [CrossRef]
- Yi, Q.; Li, X.; He, Y.; Xia, W.; Shao, J.; Ye, Z.; Song, P. Associations of dietary inflammatory index with metabolic syndrome and its components: A systematic review and meta-analysis. Public Health Nutr. 2021, 24, 5463–5470. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.M.W.; Pedersen, B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Khalafi, M.; Akbari, A.; Symonds, M.E.; Pourvaghar, M.J.; Rosenkranz, S.K.; Tabari, E. Influence of different modes of exercise training on inflammatory markers in older adults with and without chronic diseases: A systematic review and meta-analysis. Cytokine 2023, 169, 156303. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Van Buskirk, J.; Nguyen, B.; Stamatakis, E.; Elbarbary, M.; Veronese, N.; Clare, P.J.; Lee, I.M.; Ekelund, U.; Fontana, L. Physical activity, diet quality and all-cause cardiovascular disease and cancer mortality: A prospective study of 346,627 UK Biobank participants. Br. J. Sports Med. 2022, 56, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Yin, S.; Du, L.; Xue, X.; He, Q.; Zhao, N.; Chen, S.; Zhang, X. Independent and combined associations of physical activity in different domains and inflammatory diet with type 2 diabetes: A population-based cohort study. Nutrients 2025, 17, 47. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Fan, W.; Liu, Y.; Li, S.; Yu, W. Combined effects of dietary inflammatory index and vigorous physical activity on abdominal adipose tissue: Analysis of NHANES 2011–2018. J. Health Popul. Nutr. 2025, 44, 254. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhou, J.; Zhang, D.; Du, Q. Association of dietary inflammatory index and vigorous physical activity on phenotypic age acceleration: A cross-sectional study with machine learning. Front. Nutr. 2025, 12, 1602821. [Google Scholar] [CrossRef] [PubMed]
- Wopereis, S.; Wolvers, D.; van Erk, M.; Gribnau, M.; Kremer, B.; van Dorsten, F.A.; Boelsma, E.; Garczarek, U.; Cnubben, N.; Frenken, L.; et al. Assessment of inflammatory resilience in healthy subjects using dietary lipid and glucose challenges. BMC Med. Genom. 2013, 6, 44. [Google Scholar] [CrossRef] [PubMed]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—A scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Sukhera, J. Narrative reviews: Flexible, rigorous, and practical. J. Grad. Med. Educ. 2022, 14, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Hirt, J.; Nordhausen, T.; Appenzeller-Herzog, C.; Ewald, H. Citation tracking for systematic literature searching: A scoping review. Res. Synth. Methods 2023, 14, 563–579. [Google Scholar] [CrossRef] [PubMed]
- DiNatale, J.C.; Azarmanesh, D.; Hébert, J.R.; Wirth, M.D.; Pearlman, J.; Crowe-White, K.M. Relationship between non-energy-adjusted and energy-adjusted Dietary Inflammatory Index and the Healthy Eating Index-2015: An analysis of the National Health and Nutrition Examination Survey (NHANES) 2015–2018. Ann. Med. 2023, 55, 2236551. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Smith-Warner, S.A.; Chavarro, J.E.; Wu, K.; Fuchs, C.S.; Hu, F.B.; Chan, A.T.; Willett, W.C.; Giovannucci, E.L. Development and validation of an empirical dietary inflammatory index. J. Nutr. 2016, 146, 1560–1570. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Steck, S.E.; Zhang, J.; Ma, Y.; Liese, A.D.; Agalliu, I.; Hingle, M.; Hou, L.; Hurley, T.G.; Jiao, L.; et al. Construct validation of the Dietary Inflammatory Index among postmenopausal women. Ann. Epidemiol. 2015, 25, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Kotemori, A.; Sawada, N.; Iwasaki, M.; Yamaji, T.; Shivappa, N.; Hébert, J.R.; Ishihara, J.; Inoue, M.; Tsugane, S. Dietary Inflammatory Index is associated with inflammation in Japanese men. Front. Nutr. 2021, 8, 604296. [Google Scholar] [CrossRef] [PubMed]
- Azarmanesh, D.; Pearlman, J.; Carbone, E.T.; DiNatale, J.C.; Bertone-Johnson, E.R. Construct validation of the Dietary Inflammatory Index (DII) among young college-aged women. Nutrients 2023, 15, 4553. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, S.; Hosseinikia, M.; Ghaffarian-Bahraman, A.; Clark, C.C.T.; Davies, I.G.; Yousefi Rad, E.; Saboori, S. Dietary inflammatory index and elevated serum C-reactive protein: A systematic review and meta-analysis. Food Sci. Nutr. 2023, 11, 5786–5798. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.M.; Chen, L.-W.; Heude, B.; Bernard, J.Y.; Harvey, N.C.; Duijts, L.; Mensink-Bout, S.M.; Polanska, K.; Mancano, G.; Suderman, M.; Shivappa, N.; Hébert, J.R. Dietary Inflammatory Index and non-communicable disease risk: A narrative review. Nutrients 2019, 11, 1873. [Google Scholar] [CrossRef] [PubMed]
- Tan, Q.-Q.; Du, X.-Y.; Gao, C.-L.; Xu, Y. Higher Dietary Inflammatory Index scores increase the risk of diabetes mellitus: A meta-analysis and systematic review. Front. Endocrinol. 2021, 12, 693144. [Google Scholar] [CrossRef] [PubMed]
- Bakhshimoghaddam, F.; Chaharlang, R.; Mansoori, A.; Dehghanseresht, N. Dietary inflammatory index and its association with risk of metabolic syndrome and its components: A systematic review and meta-analysis of observational studies. J. Health Popul. Nutr. 2024, 43, 87. [Google Scholar] [CrossRef] [PubMed]
- Jayedi, A.; Emadi, A.; Shab-Bidar, S. Dietary Inflammatory Index and site-specific cancer risk: A systematic review and dose-response meta-analysis. Adv. Nutr. 2018, 9, 388–403. [Google Scholar] [CrossRef] [PubMed]
- Farazi, M.; Jayedi, A.; Shab-Bidar, S. Dietary inflammatory index and the risk of non-communicable chronic disease and mortality: An umbrella review of meta-analyses of observational studies. Crit. Rev. Food Sci. Nutr. 2023, 63, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Minihane, A.M.; Vinoy, S.; Russell, W.R.; Baka, A.; Roche, H.M.; Tuohy, K.M.; Teeling, J.L.; Blaak, E.E.; Fenech, M.; Vauzour, D.; et al. Low-grade inflammation, diet composition and health: Current research evidence and its translation. Br. J. Nutr. 2015, 114, 999–1012. [Google Scholar] [CrossRef] [PubMed]
- Christ, A.; Lauterbach, M.; Latz, E. Western diet and the immune system: An inflammatory connection. Immunity 2019, 51, 794–811. [Google Scholar] [CrossRef] [PubMed]
- Sies, H.; Berndt, C.; Jones, D.P. Oxidative stress. Annu. Rev. Biochem. 2017, 86, 715–748. [Google Scholar] [CrossRef] [PubMed]
- Reuter, S.; Gupta, S.C.; Chaturvedi, M.M.; Aggarwal, B.B. Oxidative stress, inflammation, and cancer: How are they linked? Free Radic. Biol. Med. 2010, 49, 1603–1616. [Google Scholar] [CrossRef] [PubMed]
- Zatterale, F.; Longo, M.; Naderi, J.; Raciti, G.A.; Desiderio, A.; Miele, C.; Beguinot, F. Chronic adipose tissue inflammation linking obesity to insulin resistance and type 2 diabetes. Front. Physiol. 2020, 10, 1607. [Google Scholar] [CrossRef] [PubMed]
- Chait, A.; den Hartigh, L.J. Adipose tissue distribution, inflammation and its metabolic consequences, including diabetes and cardiovascular disease. Front. Cardiovasc. Med. 2020, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Gimbrone, M.A., Jr.; García-Cardeña, G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef] [PubMed]
- Steven, S.; Frenis, K.; Oelze, M.; Kalinovic, S.; Kuntic, M.; Bayo Jimenez, M.T.; Vujacic-Mirski, K.; Helmstädter, J.; Kröller-Schön, S.; Münzel, T.; et al. Vascular inflammation and oxidative stress: Major triggers for cardiovascular disease. Oxid. Med. Cell. Longev. 2019, 2019, 7092151. [Google Scholar] [CrossRef] [PubMed]
- Malesza, I.J.; Malesza, M.; Walkowiak, J.; Mussin, N.; Walkowiak, D.; Aringazina, R.; Bartkowiak-Wieczorek, J.; Mądry, E. High-fat, Western-style diet, systemic inflammation, and gut microbiota: A narrative review. Cells 2021, 10, 3164. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, S.; Thiemermann, C. Role of metabolic endotoxemia in systemic inflammation and potential interventions. Front. Immunol. 2021, 11, 594150. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C.; Wentz, L.M. The compelling link between physical activity and the body’s defense system. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-H.; Tan, J.; Zhou, H.-H.; Cao, M.; Zou, Y. Long-term exercise training and inflammatory biomarkers in healthy subjects: A meta-analysis of randomized controlled trials. Front. Psychol. 2023, 14, 1253329. [Google Scholar] [CrossRef] [PubMed]
- Severinsen, M.C.K.; Pedersen, B.K. Muscle–organ crosstalk: The emerging roles of myokines. Endocr. Rev. 2020, 41, 594–609. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.A.B.; Murach, K.A.; Dyar, K.A.; Zierath, J.R. Exercise metabolism and adaptation in skeletal muscle. Nat. Rev. Mol. Cell Biol. 2023, 24, 607–632. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-H.; Yang, H.-Y.; Shun, S.-C. Effect of exercise intervention dosage on reducing visceral adipose tissue: A systematic review and network meta-analysis of randomized controlled trials. Int. J. Obes. 2021, 45, 982–997. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino, G.; Franco, D.; Sorriento, D.; Strisciuglio, T.; Barbato, E.; Morisco, C. Modulation of insulin sensitivity by exercise training: Implications for cardiovascular prevention. J. Cardiovasc. Transl. Res. 2021, 14, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.L.; Soeters, M.R.; Wüst, R.C.I.; Houtkooper, R.H. Metabolic flexibility as an adaptation to energy resources and requirements in health and disease. Endocr. Rev. 2018, 39, 489–517. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.K.; Radak, Z.; Ji, L.L. Exercise-induced oxidative stress: Past, present and future. J. Physiol. 2016, 594, 5081–5092. [Google Scholar] [CrossRef] [PubMed]
- Radak, Z.; Chung, H.Y.; Koltai, E.; Taylor, A.W.; Goto, S. Exercise, oxidative stress and hormesis. Ageing Res. Rev. 2008, 7, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Tao, X.; Chen, Y.; Zhen, K.; Ren, S.; Lv, Y.; Yu, L. Effect of continuous aerobic exercise on endothelial function: A systematic review and meta-analysis of randomized controlled trials. Front. Physiol. 2023, 14, 1043108. [Google Scholar] [CrossRef] [PubMed]
- Shivgulam, M.E.; Liu, H.; Schwartz, B.D.; Langley, J.E.; Bray, N.W.; Kimmerly, D.S.; O’Brien, M.W. Impact of exercise training interventions on flow-mediated dilation in adults: An umbrella review. Sports Med. 2023, 53, 1161–1174. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Cadenas-Sanchez, C.; da Costa, B.G.G.; Castro-Piñero, J.; Chaput, J.-P.; Cuenca-García, M.; Maher, C.; Marín-Jiménez, N.; McGrath, R.; Molina-García, P.; et al. Comparison of objectively measured and estimated cardiorespiratory fitness to predict all-cause and cardiovascular disease mortality in adults: A systematic review and meta-analysis of 42 studies representing 35 cohorts and 3.8 million observations. J. Sport Health Sci. 2025, 14, 100986. [Google Scholar] [CrossRef] [PubMed]
- Farrell, S.W.; Leonard, D.; Barlow, C.E.; Shuval, K.; Pavlovic, A.; Cooper, K.H.; DeFina, L.F. Associations among cardiorespiratory fitness, C-reactive protein, and all-cause mortality in men and women. J. Investig. Med. 2023, 71, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Inan-Eroglu, E.; Ahmadi, M.; Biswas, R.K.; Ding, D.; Rezende, L.F.M.; Lee, I.M.; Giovannucci, E.L.; Stamatakis, E. Joint associations of diet and device-measured physical activity with mortality and incident CVD and cancer: A prospective analysis of the UK Biobank study. Cancer Epidemiol. Biomark. Prev. 2024, 33, 1028–1036. [Google Scholar] [CrossRef] [PubMed]
- Aryannezhad, S.; Mok, A.; Imamura, F.; Wareham, N.J.; Brage, S.; Forouhi, N.G. Combined associations of physical activity, diet quality and their changes over time with mortality: Findings from the EPIC-Norfolk study, United Kingdom. BMC Med. 2024, 22, 464. [Google Scholar] [CrossRef] [PubMed]
- Tu, D.; Xu, Q.; Sun, J.; Zuo, X.; Ma, C. Joint association of anti-inflammatory diet and vigorous leisure-time physical activity on all-cause and cardiovascular disease mortality in U.S. adults: Findings from NHANES, 2007–2014. Eur. J. Nutr. 2025, 64, 45. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Liang, Z.; Zhang, X.; Ren, S.; Cheng, Y.; Liu, Y.; Zhang, M. Association of physical activity and dietary inflammatory index with overweight/obesity in US adults: NHANES 2007–2018. Environ. Health Prev. Med. 2023, 28, 40. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Wang, L.; Qian, Y.; Mei, L.; Zhang, M. Do interaction and joint effects between physical activity and dietary inflammatory index modify stroke risk? Complement. Ther. Clin. Pract. 2024, 57, 101898. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zheng, M. The combined effect of dietary inflammatory index and physical activity on patients with diabetic kidney disease: A cross-sectional study based on NHANES. Nutr. Metab. (Lond.) 2026, 23, 3. [Google Scholar] [CrossRef] [PubMed]
- Bu, L.; Zhang, K.; Fan, Y.; Huang, X.; Zhang, D.; Ren, L.; Zhao, B. Dietary inflammatory potential and physical activity adherence as synergistic predictors of systemic inflammation in post-myocardial infarction patients: A retrospective cohort study. Front. Nutr. 2026, 13, 1782921. [Google Scholar] [CrossRef] [PubMed]
- Knol, M.J.; VanderWeele, T.J. Recommendations for presenting analyses of effect modification and interaction. Int. J. Epidemiol. 2012, 41, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Whitson, H.E.; Duan-Porter, W.; Schmader, K.E.; Morey, M.C.; Cohen, H.J.; Colón-Emeric, C.S. Physical resilience in older adults: Systematic review and development of an emerging construct. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Promislow, D.; Anderson, R.M.; Scheffer, M.; Crespi, B.; DeGregori, J.; Harris, K.; Horowitz, B.N.; Levine, M.E.; Riolo, M.A.; Schneider, D.S.; et al. Resilience integrates concepts in aging research. iScience 2022, 25, 104199. [Google Scholar] [CrossRef] [PubMed]
- Strain, T.; Wijndaele, K.; Dempsey, P.C.; Sharp, S.J.; Pearce, M.; Jeon, J.; Lindsay, T.; Wareham, N.; Brage, S. Wearable-device-measured physical activity and future health risk. Nat. Med. 2020, 26, 1385–1391. [Google Scholar] [CrossRef] [PubMed]
- Celis-Morales, C.A.; Welsh, P.; Lyall, D.M.; Steell, L.; Petermann, F.; Anderson, J.; Iliodromiti, S.; Sillars, A.; Graham, N.; Mackay, D.F.; et al. Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all cause mortality: Prospective cohort study of half a million UK Biobank participants. BMJ 2018, 361, k1651. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, S.I.; Baranowski, T.; Subar, A.F.; Tooze, J.A.; Frongillo, E.A. Best practices for conducting and interpreting studies to validate self-report dietary assessment methods. J. Acad. Nutr. Diet. 2019, 119, 1801–1816. [Google Scholar] [CrossRef] [PubMed]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: A systematic review and practical considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. SBRN Terminology Consensus Project Participants. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.-P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of assessing cardiorespiratory fitness in clinical practice: A case for fitness as a clinical vital sign: A scientific statement from the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Ahluwalia, N.; Albers, R.; Bosco, N.; Bourdet-Sicard, R.; Haller, D.; Holgate, S.T.; Jönsson, L.S.; Latulippe, M.E.; Marcos, A.; et al. A consideration of biomarkers to be used for evaluation of inflammation in human nutritional studies. Br. J. Nutr. 2013, 109, S1–S34. [Google Scholar] [CrossRef] [PubMed]
- Maruvada, P.; Lampe, J.W.; Wishart, D.S.; Barupal, D.; Chester, D.N.; Dodd, D.; Djoumbou-Feunang, Y.; Dorrestein, P.C.; Dragsted, L.O.; Draper, J.; et al. Perspective: Dietary biomarkers of intake and exposure—Exploration with omics approaches. Adv. Nutr. 2020, 11, 200–215. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.J. Mediation analysis: A practitioner’s guide. Annu. Rev. Public Health 2016, 37, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Hernán, M.A.; Robins, J.M. Using big data to emulate a target trial when a randomized trial is not available. Am. J. Epidemiol. 2016, 183, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Mok, A.; Khaw, K.-T.; Luben, R.; Wareham, N.; Brage, S. Physical activity trajectories and mortality: Population based cohort study. BMJ 2019, 365, l2323. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Look AHEAD Research Group. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N. Engl. J. Med. 2013, 369, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Ordovas, J.M.; Ferguson, L.R.; Tai, E.S.; Mathers, J.C. Personalised nutrition and health. BMJ 2018, 361, k2173. [Google Scholar] [CrossRef] [PubMed]
- Kent, D.M.; Paulus, J.K.; van Klaveren, D.; D’Agostino, R.; Goodman, S.; Hayward, R.; Ioannidis, J.P.A.; Patrick-Lake, B.; Morton, S.; Pencina, M.J.; et al. The Predictive Approaches to Treatment effect Heterogeneity (PATH) statement. Ann. Intern. Med. 2020, 172, 35–45. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
From compensation to inflammatory resilience. The compensation model assumes that physical activity can counterbalance or cancel the health risks associated with a pro-inflammatory diet. In contrast, the inflammatory resilience model views dietary inflammatory potential as an exposure whose biological translation may be modified by physical activity, cardiorespiratory fitness, skeletal muscle function, adiposity, metabolic health, vascular regulation, and baseline disease status. This model emphasizes partial buffering, residual risk, and pathway-specific modification rather than full cancellation.
Figure 1.
From compensation to inflammatory resilience. The compensation model assumes that physical activity can counterbalance or cancel the health risks associated with a pro-inflammatory diet. In contrast, the inflammatory resilience model views dietary inflammatory potential as an exposure whose biological translation may be modified by physical activity, cardiorespiratory fitness, skeletal muscle function, adiposity, metabolic health, vascular regulation, and baseline disease status. This model emphasizes partial buffering, residual risk, and pathway-specific modification rather than full cancellation.

Figure 2.
Inflammatory Resilience Framework linking dietary inflammatory potential, physical activity, and disease vulnerability. The framework conceptualizes dietary inflammatory potential as a chronic lifestyle exposure whose biological translation into disease vulnerability occurs through immune, oxidative, adipose, metabolic, vascular, and gut-related pathways. Physical activity and related physiological traits—including cardiorespiratory fitness, skeletal muscle function, adiposity, insulin sensitivity, metabolic flexibility, redox adaptation, vascular function, and baseline health status—may modify this translation process. The framework supports partial buffering, residual risk, and outcome-specific vulnerability rather than full compensation.
Figure 2.
Inflammatory Resilience Framework linking dietary inflammatory potential, physical activity, and disease vulnerability. The framework conceptualizes dietary inflammatory potential as a chronic lifestyle exposure whose biological translation into disease vulnerability occurs through immune, oxidative, adipose, metabolic, vascular, and gut-related pathways. Physical activity and related physiological traits—including cardiorespiratory fitness, skeletal muscle function, adiposity, insulin sensitivity, metabolic flexibility, redox adaptation, vascular function, and baseline health status—may modify this translation process. The framework supports partial buffering, residual risk, and outcome-specific vulnerability rather than full compensation.


Table 1.
Dietary inflammatory potential and major health outcome domains relevant to the inflammatory resilience framework.
Table 1.
Dietary inflammatory potential and major health outcome domains relevant to the inflammatory resilience framework.
| Health 7. | Representative outcomes | Main inflammatory relevance | Evidence type emphasized in this review | Key supporting references |
| Cardiovascular and vascular outcomes | Cardiovascular disease risk, cardiovascular mortality, vascular morbidity | Chronic low-grade inflammation, oxidative stress, endothelial dysfunction, vascular impairment, and cardiometabolic risk clustering | Meta-analysis and umbrella-level evidence linking higher dietary inflammatory potential with cardiovascular risk and mortality | [7,28,32] |
| Metabolic disease and glucose regulation | Type 2 diabetes, impaired glucose regulation, insulin resistance-related risk | Diet-related inflammation may contribute to insulin resistance, metabolic dysfunction, adipose tissue inflammation, and impaired glucose handling | Systematic review and meta-analysis evidence linking higher DII scores with diabetes risk | [29,32] |
| Metabolic syndrome and cardiometabolic clustering | Metabolic syndrome and its components, including central adiposity, dyslipidemia, hypertension, and glucose abnormalities | Pro-inflammatory dietary patterns may interact with adiposity, metabolic inflammation, and vascular risk factors | Systematic review and meta-analysis of observational studies on DII and metabolic syndrome | [8,30,32] |
| Obesity and adiposity-related vulnerability | General obesity, central adiposity, visceral adipose tissue-related risk | Excess adiposity can amplify inflammatory responses through adipokine imbalance, macrophage infiltration, and low-grade systemic inflammation | Narrative and umbrella-level evidence linking DII with non-communicable disease risk and adiposity-related pathways | [6,28,32] |
| Cancer-related outcomes | Site-specific cancer risk and broader cancer-related vulnerability | Chronic inflammation, oxidative stress, immune dysregulation, and altered metabolic signaling may contribute to carcinogenic environments | Systematic review and dose-response meta-analysis of DII and site-specific cancer risk | [28,31,32] |
| Mortality and long-term non-communicable disease burden | All-cause mortality, non-communicable chronic disease risk, long-term health vulnerability | Persistent inflammatory exposure may contribute to cumulative disease burden across cardiometabolic, vascular, cancer-related, and aging-related pathways | Umbrella reviews and meta-analyses of observational evidence | [6,28,32] |
| Aging-related vulnerability | Functional decline, biological aging-related risk, multimorbidity vulnerability | Low-grade inflammation and diet-related inflammatory exposure may contribute to inflammaging, metabolic dysfunction, vascular impairment, and reduced physiological reserve | Narrative and umbrella-level synthesis; interpreted cautiously because aging-specific evidence varies by outcome and design | [1,2,6,28,32] |
Note: DII, Dietary Inflammatory Index. The table summarizes major health domains relevant to the present review. It is not intended to provide an exhaustive disease-by-disease review. Most evidence linking dietary inflammatory potential with health outcomes is observational; therefore, the associations should be interpreted as risk-related patterns rather than definitive causal effects.
Table 2.
Physical activity-related mechanisms relevant to inflammatory resilience.
| Physical activity-related factor | Anti-inflammatory or metabolic mechanism | Relevant biomarkers/pathways | Potential buffering role against pro-inflammatory diet | Key supporting references |
| Regular moderate-to-vigorous physical activity | Supports immune regulation and may reduce chronic inflammatory tone over time | CRP, IL-6, TNF-α, innate and adaptive immune regulation | May reduce baseline inflammatory tone, thereby limiting downstream expression of dietary inflammatory exposure | [43,44] |
| Exercise training adaptation | Repeated training may shift inflammatory responses from transient stress signals toward longer-term adaptation | Cytokine balance, recovery, training dose, anti-inflammatory signaling | Provides biological plausibility for partial buffering rather than full compensation | [10,12,43,44] |
| Skeletal muscle contraction and myokines | Contracting muscle releases myokines involved in interorgan communication | Myokine signaling, muscle–adipose–liver–vascular crosstalk | May influence immune–metabolic pathways affected by pro-inflammatory dietary patterns | [11,45,46] |
| Skeletal muscle metabolic plasticity | Exercise promotes metabolic adaptation and functional plasticity of skeletal muscle | Mitochondrial remodeling, substrate use, glucose disposal, metabolic flexibility | May improve host capacity to handle dietary metabolic stress | [46,49] |
| Visceral adiposity reduction | Exercise can reduce visceral adipose tissue, an important inflammatory tissue depot | Visceral adiposity, adipokines, adipose inflammation | May reduce adipose-driven amplification of dietary inflammatory exposure | [37,38,47] |
| Insulin sensitivity and glucose regulation | Exercise improves skeletal muscle glucose uptake and insulin sensitivity | Insulin signaling, glucose handling, substrate delivery | May buffer diet-related metabolic dysfunction and glycemic stress | [48,49] |
| Redox adaptation | Exercise-induced redox signals may stimulate adaptive antioxidant and repair responses | Reactive oxygen species, redox signaling, antioxidant enzymes, hormesis | May improve redox regulation rather than simply suppress oxidative stress | [35,36,50,51] |
| Endothelial function and vascular adaptation | Aerobic training can improve endothelial function and vascular reactivity | Flow-mediated dilation, nitric oxide bioavailability, vascular inflammation | May reduce vascular vulnerability related to inflammatory and oxidative dietary stress | [39,40,52,53] |
| Cardiorespiratory fitness | Represents accumulated physiological reserve from habitual activity and training | VO₂max/VO₂peak, METs, CRP, mortality risk | May indicate higher resilience capacity and lower vulnerability under inflammatory exposure | [54,55] |
| Integrated inflammatory resilience | Physical activity effects across immune, adipose, metabolic, redox, vascular, and fitness pathways are interconnected | Multi-system regulation rather than single biomarker change | Supports partial buffering of dietary inflammatory risk, not complete cancellation | [43,44,45,46,47,48,49,50,51,52,53,54,55] |
Note: CRP, C-reactive protein; IL-6, interleukin-6; METs, metabolic equivalents; TNF-α, tumor necrosis factor-α; VO₂max/VO₂peak, maximal or peak oxygen uptake. The table summarizes mechanisms relevant to the proposed inflammatory resilience framework. It does not imply that physical activity fully compensates for the health risks of a pro-inflammatory diet.
Table 3.
Research agenda for testing the Inflammatory Resilience Framework.
| Research priority | Current limitation | Recommended design or measurement | Framework component tested | Key supporting references |
| Dietary inflammatory exposure assessment | Single baseline dietary assessment and variable DII component availability | Repeated dietary assessment, E-DII, validation, and sensitivity analysis by dietary components | Exposure layer | [4,5,22,68,74] |
| Objective physical activity and sedentary behavior | Reliance on self-reported physical activity and incomplete sedentary behavior characterization | Accelerometry, device-based PA, sedentary behavior assessment, and 24-hour movement composition | Resilience modifier layer | [66,69,70] |
| Cardiorespiratory and muscular fitness | Physical activity behavior measured without physiological reserve indicators | CRF, grip strength, muscle function, gait speed, and resistance training assessment | Physiological reserve | [54,55,67,71,72] |
| Inflammatory and metabolic biomarkers | Outcomes measured without biological translation markers | CRP, IL-6, TNF-α, adipokines, glycemic markers, endothelial markers, and redox markers | Biological translation layer | [24,27,33,37,39,73] |
| Interaction and mediation modeling | Diet and PA often treated only as covariates | Additive and multiplicative interaction, mediation, moderated mediation, and causal inference | Risk translation | [60,63,75,76] |
| Longitudinal risk trajectories | Cross-sectional or single-time-point designs | Repeated measures of diet, PA, biomarkers, fitness, and outcomes | Time-dependent resilience | [56,57,77] |
| Combined lifestyle intervention trials | Observational evidence cannot prove buffering or compensation | Diet–exercise trials, factorial designs, pragmatic interventions, and mechanistic endpoints | Intervention testing | [78,79] |
| Population heterogeneity and responder profiling | Limited stratification by baseline phenotype | Stratification by age, sex, adiposity, CRF, muscle function, baseline inflammation, and disease status | Phenotype-specific resilience | [64,65,80,81] |
| Public health and clinical translation | Oversimplified “exercise offsets diet” messaging | Communication of partial buffering, residual risk, and combined lifestyle benefit | Translational application | [14,56,58,60,80] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



