Submitted:
29 June 2026
Posted:
30 June 2026
You are already at the latest version
Abstract
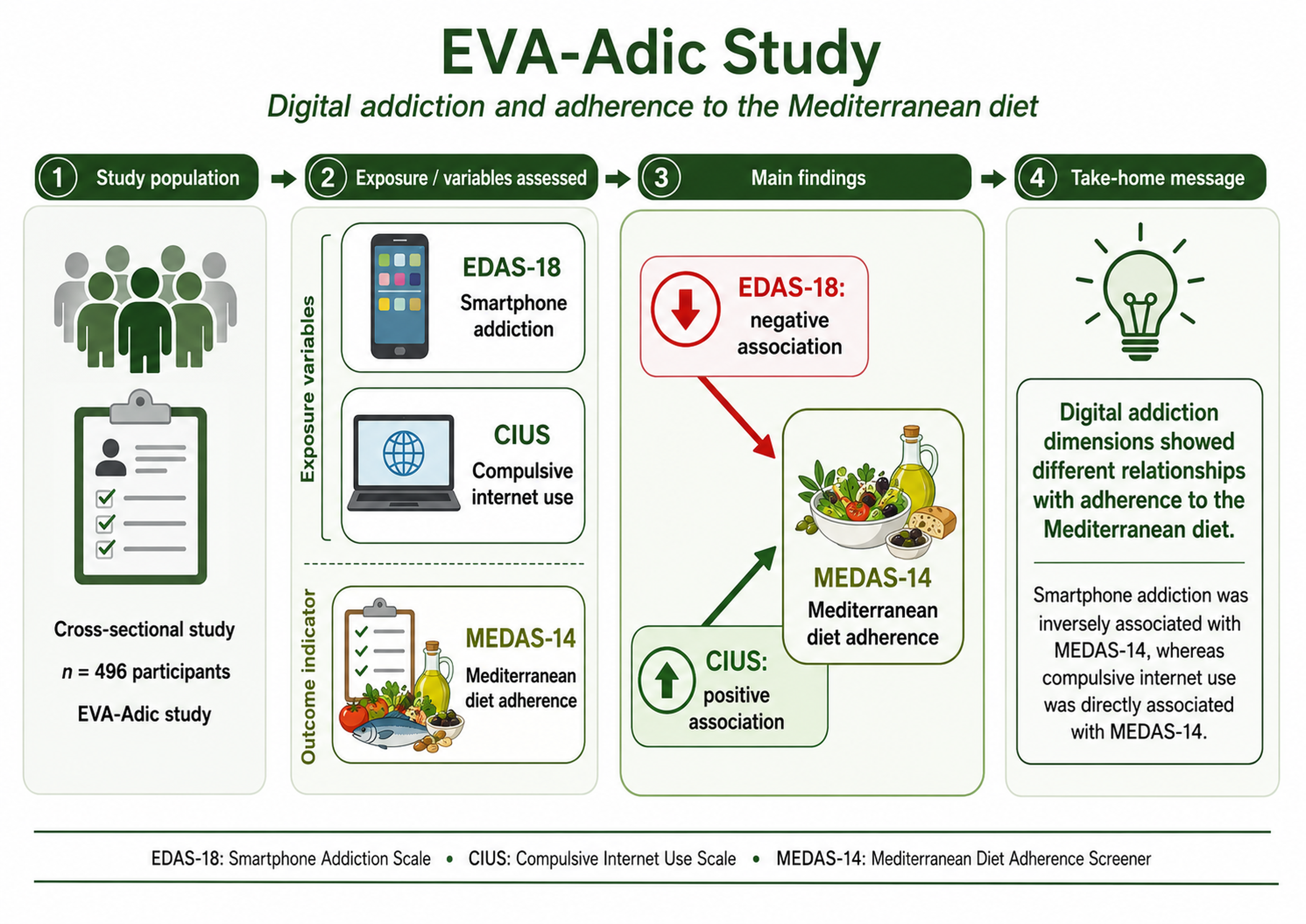
Background/Objectives: The Mediterranean diet (MedDiet) is a protective nutritional model against cardiometabolic risk, but current sociodemographic changes have favoured the abandonment of this pattern in favour of sedentary behaviours and increasing digitalisation. Screen-related behavioral addictions represent an emerging challenge for public health and nutritional psychiatry. However, scientific evidence on how different digital dependence profiles influence young adults’ diets remains scarce. The aim of this study was to evaluate the relationship between adherence to the Mediterranean diet and various dimensions of problematic screen use (smartphone dependence, compulsive internet use, and problematic experiences with video games) in a sample of young adults. Methods: Observational, descriptive and cross-sectional study conducted in 496 young adults between 18 and 34 years of age enrolled in the EVA-Adic study. Adherence to the MedDiet was assessed using the 14-item MEDAS questionnaire. Digital addictions were determined using three continuously validated psychometric instruments: the EDAS-18 scale (smartphone), the CIUS questionnaire (internet) and the CERV questionnaire (video games), also generating a Global Digital Addiction index. Hierarchical multivariate linear regression models (adjusted for sociodemographic, anthropometric and lifestyle factors) and binary logistic regression models were performed to analyze each component of the MEDAS individually. Results: The mean age of the 496 subjects analyzed was 26.60 ± 4.41 years. 339 subjects had low-moderate adherence (< 9) and 157 high adherence (≥ 9). The mean values of the psychometric scales of digital addiction were: smartphone dependence: 40.87 ± 12.24 points, for compulsive use of the internet: 13.83 ± 9.89 points, for video game dependence: 3.54 ± 5.22 points, and the global digital addiction index: 58.25 ± 21.76 points. In the multivariate linear regression analysis in the total fit model, smartphone dependence (EDAS-18) was inversely associated with the MEDAS score (β = -0.021 {95% CI} [-0.041 -0.003]). Problematic internet use (CIUS) showed a positive association with dietary adherence (β = 0.025 {95% CI} [0.002, 0.049]). Problematic experiences with video games (CERV) and the global digital addiction index did not demonstrate an association. In the logistic regression analysis of each of the components of the MEDAS: each one-point increase on the EDAS-18 scale reduced the probability of meeting the fruit consumption criterion ≥3 pieces/day (OR = 0.980); the criterion of low consumption of sugary beverages or less than one per day (OR = 0.956) and was linked to a higher probability of meeting the criterion of using olive oil as the main cooking fat (OR = 1.026). Compulsive use of the Internet (CIUS): A higher score on the CIUS scale decreased the probability of registering a low consumption of sugary drinks (OR = 0.955); positive association with compliance with olive oil consumption ≥ 4 tablespoons/day (OR = 1.035) and with the consumption of sofrito ≥ 2 times/week (OR = 1.026). Conclusions: The results of this study suggest that digital addictive behaviors are differentially associated with the quality of the Mediterranean diet. Higher smartphone addiction risk was associated with lower adherence to the Mediterranean diet, which may reflect a less healthy behavioral pattern linked to problematic mobile phone use. In contrast, problematic internet use may represent a different profile in relation to dietary habits, possibly influenced by the type of digital use, the context of exposure, or the characteristics of the participants evaluated. These findings reinforce the need to analyze different forms of digital addiction separately, rather than treating them as a homogeneous phenomenon, and suggest that interventions aimed at improving adherence to healthy dietary patterns should include the assessment of digital behavior.
Keywords:
Mediterranean diet
; smartphone addiction
; compulsive internet use
; lifestyle factors
; young adults
1. Introduction
The Mediterranean diet (MedDiet) is recognized as an optimal nutritional pattern, and a comprehensive lifestyle model with metabolic and cardiovascular implications [1,2,3]. It is characterized by a high consumption of monounsaturated fats (mainly from extra virgin olive oil), fruits, vegetables, legumes, nuts and fish, along with a low intake of red meat and ultra-processed products, this dietary pattern has systemic antioxidant and anti-inflammatory effects [2,3]. A high adherence to the MedDiet, between 18 and 35 years of age, is a determining factor in mitigating premature cardiometabolic risk and consolidating healthy habits in the long term [4,5]. However, contemporary sociodemographic changes have led to a progressive move away from this traditional model, replacing it with dietary patterns of lower nutritional quality and an increase in sedentary behaviours [6,7].
At the same time, global digitalization has driven the emergence of screen-related behavioral addictions, constituting a priority challenge for public health and nutritional psychiatry [8,9]. The problematic and compulsive use of the internet, smartphones and video games has substantially reconfigured the management of free time and the behavior of the young population [10,11,12]. Biomedical studies over the past five years consistently suggest that greater exposure to screens is inversely associated with overall diet quality and, specifically, with lower adherence to the MedDiet [11,13]. However, the biological and behavioral mechanisms underlying this phenomenon are complex and multidimensional. A biological–behavioral axis has been proposed, whereby excessive technology use may alter eating patterns through the dysregulation of appetite-related hormones, such as leptin and ghrelin, thereby increasing hedonic hunger for energy-dense foods [14]. Likewise, the underlying impulsivity and deficit in inhibitory control characteristic of digital addictive behaviors undermine the ability to plan meals and make fresh food choices, inducing unstructured patterns [15].
At the epidemiological level, the evidence of this negative impact is substantial in young populations, so digital sedentary lifestyles displace the consumption of fruits and vegetables and significantly increase the intake of sweets and fast food [13,16]. In Mediterranean populations, the use of mobile devices and social networks directly during main meals has emerged as one of the distractions with the greatest predictive impact on the consumption of ultra-processed foods and the destructuring of the traditional diet [17,18]. Similarly, the specific profile of problematic use of video games (Gaming) is associated with prolonged sessions of immobility and automatic or unconscious eating (mindless eating), increasing the consumption of sugary drinks, easily accessible and simultaneous consumption with the game [19]. Despite the growing volume of publications, the translation of these findings to the population of young adults and university students has important scientific limitations. Evidence in this age group remains scattered, less homogeneous, and methodologically heterogeneous [20]. The vast majority of recent scientific studies use assessment tools such as the Mobile Phone Addiction Index, the Smartphone Addiction Scale or the Young Internet Addiction Test [8,20,21]. On the other hand, the diagnostic utility of specific instruments adapted to the Spanish-speaking population, such as the abbreviated version of the Smartphone Dependence and Addiction Scale (EDAS-18)[22] or the Questionnaire of Experiences Related to Video Games (CERV) [23], as well as using the Video Game Related Experiences Questionnaire (CIUS) [24], their direct relationship with adherence to the MedDiet quantified by the 14-item standardized MEDAS questionnaire has been little explored [25]. This knowledge gap makes it impossible to establish whether the specific digital dependence profiles of young adults act in a coordinated way in the deterioration of the protective dietary pattern par excellence [25].
To overcome this limitation, the present study aims to evaluate the relationship between adherence to the Mediterranean diet (measured through the 14-item MEDAS questionnaire) and different dimensions of problematic screen use (smartphone dependence using EDAS-18, compulsive internet use using CIUS, and problematic experiences with video games using CERV in a sample of 500 young adults between 18 and 35 years of age. It is hypothesized that subjects with higher digital behavioral addiction scores will have lower adherence to the MedDiet, characterized by a maladaptive food consumption profile driven by the disruption of everyday technological habits.
2. Materials and Methods
2.1. Study Design
The results of this work are part of the EVA-Adic study. The protocol for the EVA-Adic study has been previously published [26]. The EVA-Adic study is a cross-sectional descriptive observational study carried out at the Primary Care Research Unit of Salamanca (APISAL). It is registered in ClinicalTrials.gov with the registration number NCT05819840 (registration date: July 29, 2023).
2.2. Study Population
Using consecutive sampling, 501 people from the urban health area of Salamanca were recruited. Inclusion criteria: age between 18 and 34 years of age and sign the informed consent form to participate in the study. Exclusion criteria: being in a terminal situation and not being able to travel to the research unit to carry out the tests. This study included the 496 participants who had performed the complete analysis of the MEDAS, EDAS-18, CIUS and CERV questionnaire.
2.3. Sample Size Calculation
Sample Size Calculation. Using version 7.2 of the GRANMO software and considering the MEDAS questionnaire score as the main outcome, accepting an alpha risk of 0.05 and a statistical power greater than 0.80 in a two-sided test, with 339 subjects in Group 1 (low adherence) and 157 in Group 2 (high adherence), the study was able to detect a difference equal to or greater than 0.54 units in the Mediterranean diet score. A common standard deviation of 2.01 was assumed for the Mediterranean diet score.
In carrying out this work, they have been followed according to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) [27] guidelines (the checklist is shown in Supplementary Table S1).
2.4. Variables and Measurement Instruments
The questionnaires used were collected from each participant in a period of less than 8 days. All tests were performed by 3 previously trained researchers in a standardized way, evaluating the quality by an independent investigator. All evaluations were performed under standardized environmental conditions and measurements were performed sequentially.
2.4.1. Sociodemographic Variables and Personal History
Age and sex were recorded at the time of inclusion in the study using a structured clinical interview.
2.4.2. Lifestyle Factors
Alcohol consumption was assessed using a structured, self-administered questionnaire that recorded the amount and type of alcohol commonly consumed during a week. The amount of alcohol consumed was measured in grams/week. Smoking was recorded following the standardized four-question questionnaire of the WHO MONICA study [28]. Physical activity was estimated with the International Physical Activity Questionnaire—Short Form (IPAQ-SF) [29]. It consists of seven questions about the type of physical activity performed during the last seven days and the total time spent on these activities. The result is the metabolic equivalent of the task per minute per week (MET-min/week).
2.4.3. Mediterranean Diet
The MedDiet was assessed using the abbreviated Mediterranean Diet Adherence Screen (MEDAS) questionnaire of 14 items [25], validated and originally developed within the framework of the PREDIMED study (PREvención con DIeta MEDiterránea) by Martínez-González et al. [30], and extensively evaluated in the Spanish population [25]. This self-administered instrument is a validated nutritional screening tool that allows for a rapid and reproducible estimation of the degree of agreement of the participant’s eating habits with the traditional Mediterranean dietary pattern. The questionnaire consists of 14 closed questions that assess the frequency of consumption of essential foods and behaviors characteristic of the MedDiet pattern (Table S2 shows the 14 items evaluated). The overall score of the MEDAS is calculated by the arithmetic sum of all items, oscillating in a continuous range from 0 to 14 points, where a higher score reflects a greater qualitative and quantitative proximity to the Mediterranean standard. Following the standardized methodological criteria of the PREDIMED cohort [30,31], the participants’ adherence status was classified into two diagnostic categories: Low-to-moderate adherence: global score <9 points; high adherence: global score ≥9 points.
2.4.4. Screen Addiction and Dependence Assessment
To obtain a multidimensional assessment of the problematic use of technology and screens, three independently validated psychometric instruments were administered and then the scores were combined to generate a Global Digital Addiction index, on a continuous scale.
Smartphone Addiction: EDAS-18 Questionnaire. Mobile phone dependence was determined using the validated Smartphone Dependence and Addiction Scale in its short version (EDAS-18) [22,32]. This instrument consists of 18 self-reported items that assess the dimensions of compulsive use, abstinence, tolerance, and interference with activities of daily living. Responses are recorded using a 5-point Likert scale (from 1 = “strongly disagree” to 5 = “strongly agree”). The continuous total score (edas18_total) is calculated by adding up all items, ranging from 18 to 90 points, where higher scores reflect a higher degree of smartphone addiction.
Internet addiction: CIUS questionnaire. Problematic Internet use in general was assessed through the Compulsive Internet Use Scale (CIUS) validated in European and Spanish settings [24]. The scale includes 14 items that examine loss of control, mental worry, the use of the internet as an emotional escape/regulation mechanism, and the resulting social or academic conflict. Each item is scored on a 5-point Likert scale (0 = “never” to 4 = “very often”). The continuous global score (cius_total) is obtained by adding the items, with a possible range from 0 to 56 points, denoting a greater severity of compulsive use the higher the score.
Video Game Addiction: CERV Questionnaire. The pattern of problem gambling and video game dependence was measured using the Video Game Related Experiences Questionnaire (CERV) [23]. This self-administered questionnaire consists of 17 items and assesses interpersonal conflicts, intrapsychological problems and excessive use associated with game screens. Items are answered on a 4-point Likert scale (1 = “never or almost never” to 4 = “almost always”). The continuous total score (cerv_total) is calculated with the sum of the scores of each item, with a range of 17 to 68 points, where a higher score indicates a greater severity in the gambling behavior.
Calculation of the Global Digital Addiction Index. To generate the Global Digital Addiction continuous variable, the total scores of each questionnaire were mathematically standardized and transformed into scores (with mean = 0 and standard deviation = 1) based on the distribution of the sample itself. Subsequently, the arithmetic mean of the three scores was calculated for each participant. This continuous index preserves the total variability and statistical power of the data, allowing its direct use in Pearson’s correlation coefficients and multivariate linear regression models (Models 1 and 2).
2.5. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics software for Windows, version 30.0 (IBM Corp., Armonk, NY, USA). The threshold of statistical significance was set at p < 0.05 for all bilateral tests. Quantitative variables were expressed as means and standard deviations (SD), while categorical and nominal variables were summarized using absolute frequencies (n) and percentages (%). To explore possible variations in baseline sample characteristics, comparative analyses were carried out by stratified participants according to their adherence to the MedDiet (Adherents vs. Non-adherent) and according to sex. Differences between groups for categorical variables were assessed using the Chi-square test. For continuous variables, Student’s t-tests were applied for independent samples. The dependent variable (global MedDiet adherence score, MEDAS) and all digital addiction metrics (EDAS-18, CIUS, CERV, and the global digital addiction index) were treated as continuous variables to preserve the total statistical power and inherent variability of the psychometric and nutritional scales, thus avoiding the arbitrary loss of information associated with categorization. Initially, bivariate associations between the global score of the Mediterranean diet and the four digital addiction scales were assessed using Pearson’s correlation coefficient (r). Subsequently, multivariate linear regression models were constructed to explore the independent predictive value of digital addictions on adherence to the Mediterranean diet. To assess potential confounding effects, a hierarchical regression approach was employed through two sequential adjustment levels: Model 1 was adjusted for major sociodemographic factors (age and sex); Model 2 was additionally adjusted for anthropometric and lifestyle covariates, including alcohol consumption (grams/week), physical activity levels assessed by the International Physical Activity Questionnaire (IPAQ), smoking status, and Body Mass Index (BMI). To ensure the absence of multicollinearity between predictors and covariates within the fully adjusted equations, the Variance Inflation Factor (VIF) was explicitly calculated, considering a VIF value < 2.0 as the threshold for accepting a correspondingly low collinearity. To assess whether gender acted as a moderating variable in the relationship between measures of digital addiction and adherence to the Mediterranean Diet, multiplicative interaction terms (Sex Addiction Score) were explicitly calculated for each ×of the multivariable linear models analyzed. These terms were introduced into a final hierarchical block in multiple regressions. In case of detecting a statistically significant interaction (p < 0.05), we planned to perform independently sex-stratified analyses to decipher specific patterns. Otherwise, the global joint models duly adjusted for this covariate were reported. Finally, to unravel the specific dietary behaviors driving the observed global associations, independent multivariate binary logistic regression analyses were performed for each of the 14 individual dietary components that make up the MEDAS questionnaire (treated as dichotomous outcome variables: 0 = non-compliance; 1 = compliance with the healthy criterion). These item-by-item regressions assessed the specific impact of each digital addiction metric using the covariate fit structure detailed in Model 2. The results of these logistic equations were expressed as Odds Ratios (ORs) together with their corresponding 95% Confidence Intervals (95% CI).
2.6. Ethical Considerations
The Ethics Committee in Drug Research of the Salamanca Health Area approved this project on July 10, 2021 (CEIm Reference Code Ref. PI 2021 088671048) and on July 24, 2023 (CEIm Reference Code Ref. PI 2023 071332). Throughout the study, the standards of good practice in observational studies established by the Declaration of Helsinki and by the WHO were carried out [33]. The confidentiality of the participants was always guaranteed in accordance with Organic Law 3/2018, European Regulation 2016/679 and Council Directive 27/04/2016 on Data Protection. All the subjects analyzed signed an informed consent before being included in the study and after receiving detailed information about the procedures that would be performed.
2.7. Use of Artificial Intelligence Tools
During the preparation of the manuscript, ChatGPT (OpenAI, version 5.5) was used to help with the English edition and with the formatting and assembly of the handwritten figures based on the results generated by the author. Generative AI was not used to create scientific images, generate data, perform analysis, or alter study results. All results and statistical analyses were performed by the authors. The authors reviewed and approved all AI-assisted edits and assume full responsibility for the final manuscript.
3. Results
Table 1 shows the sociodemographic, anthropometric and behavioural characteristics of the sample according to the level of adherence to the Mediterranean Diet. Of the 496 participants included, 339 had low adherence to the Mediterranean pattern and 157 had high adherence. Participants with high adherence were older and had a higher proportion of women, a lower prevalence of smoking and a lower BMI compared to the low-adherence group. No differences were observed between the groups in alcohol consumption or physical activity levels. Regarding the digital addiction scales, the EDAS-18, CIUS, CERV scores and the global digital addiction score were similar between both groups.
Table 2 presents the characteristics of the participants according to sex. Men were older and showed higher values of body mass index, alcohol consumption and physical activity. No differences were observed in smoking. Regarding the variables related to the problematic use of technologies, no differences were detected by sex in EDAS-18, CIUS or in the global problematic use of screens. However, men had higher scores in CERV, indicating a greater problematic use of video games.
Figure 1 shows the differences in the Mediterranean Diet adherence score according to the presence or absence of problematic screen use. No differences in MEDAS score were observed between participants with and without problematic use of smartphones, the internet, video games or global digital addiction.
Figure 2 shows the correlation between adherence to the Mediterranean diet, assessed using the MEDAS-14 questionnaire, and digital addiction scores. A weak inverse correlation was observed between the MEDAS-14 score and smartphone addiction measured by EDAS-18 (r = −0.126), video game addiction assessed by CERV (r = −0.127) and the global digital addiction score showed a weak negative correlation with adherence to the Mediterranean diet (r = −0.112). In contrast, Internet addiction assessed by CIUS showed a positive correlation with MEDAS-14 (r = 0.012). All correlations were weak and non-significant (p > 0.05)
As shown in Figure 3, smartphone addiction was inversely associated with the MEDAS questionnaire score in both the age- and sex-adjusted model and the fully-adjusted model. Specifically, higher scores in EDAS-18 were related to lower scores on the MEDAS questionnaire. In contrast, internet addiction showed a positive association after full adjustment. Video game addiction and global digital addiction score were not associated with adherence to the Mediterranean diet in either model.
In order to determine whether the impact of problematic use of technology on dietary patterns differed between men and women, the effects of interaction with sex were evaluated for each psychometric scale individually and for the global construct. In no case did the terms of interaction reach statistical significance (Model 1 [Smartphone]: p= 0.668; Model 2 [Internet]: p = 0.361; Model 3 [Video games]: p = 0.790; Model 4 [Global]: p = 0.578). These findings robustly confirm that the strength and direction of the observed associations between digital addictions and MEDAS-14 score remain constant and homogeneous in both the male and female subsamples, fully justifying the use of unified joint multivariate models.
Figure 4 shows the adjusted association between EDAS-18 and CIUS scores and compliance with each of the 14 criteria of the MEDAS questionnaire using the total fit model. A higher score on EDAS-18 was associated with a higher probability of meeting the criterion for olive oil consumption ≥4 tablespoons/day (OR=1.026). Conversely, higher EDAS-18 scores were associated with a lower probability of meeting the fruit consumption criterion ≥3 pieces/day (OR=0.980) and the criterion of low consumption of sugary drinks (<1/day) (OR=0.956). No significant associations were observed with the rest of the MEDAS criteria. Similarly, a higher CIUS score was associated with a higher probability of meeting the criterion for olive oil consumption ≥4 tablespoons/day (OR=1.035) and sofrito consumption ≥2 times/week (OR=1.026). However, an inverse association was also observed with the criterion of low consumption of sugar-sweetened beverages (<1/day) (OR=0.955). The criterion related to wine consumption had unstable confidence intervals and should therefore be interpreted with caution and was not considered conclusive.
Figure 5 shows the adjusted association between CERV and global digital addiction scores with compliance with each of the 14 criteria of the MEDAS questionnaire using the total fit model. A higher score on CERV was associated with a higher probability of meeting the criterion of low consumption of butter, margarine or cream (<1 serving/day) (OR=1.641). No significant associations were observed between CERV and the rest of the MEDAS criteria. The criterion for wine consumption had unstable confidence intervals and should therefore be interpreted with caution. In relation to global digital addiction, higher scores were significantly associated with a higher probability of meeting the criterion for olive oil consumption ≥4 tablespoons/day (OR=1.016). Conversely, a higher global digital addiction score was associated with a lower probability of meeting the fruit consumption criterion ≥3 pieces/day (OR=0.990) and the criterion of low consumption of sugary drinks (<1/day) (OR=0.975). No associations were observed with the other components of MEDAS.
4. Discussion
The main findings of the EVA-Adic study, conducted in a sample of 496 subjects, suggest that smartphone dependence (assessed by EDAS-18) is independently associated with lower overall adherence to the MedDiet. At the level of specific components, this deterioration is mainly driven by a significant reduction in the likelihood of meeting daily fruit consumption recommendations and an increase in the intake of sugary drinks. In contrast, compulsive internet use in general (CIUS) showed a slightly positive association with the global adherence score after multivariate adjustment. Finally, problematic experiences with video games (CERV) and the global digital addiction construct did not show deleterious effects on the total diet quality score in the adjusted models. Nor was a moderating effect detected by the sex of the participants. From a conceptual perspective, the results suggest that the component of immediacy, portability, use during meals, attentional interruption and continuous exposure of the smartphone could have a more direct relationship with less favorable dietary patterns than the use of the internet understood globally. The positive association observed with CIUS should be interpreted with caution: it does not necessarily imply a healthy effect of problematic internet use, but may reflect differences in the type of online activity, in the profile of the participants, in access to nutritional information or in residual factors not fully captured by the models. Overall, EVA-Adic provides a relevant message for behavioral nutrition research: it is not enough to measure “screen time” or “digital addiction” as unique constructs; It is necessary to differentiate between the device, content, purpose of use, time of day and food context.
The inverse association between EDAS-18 and adherence to the MetDiet is consistent with recent literature that relates greater exposure to screens with poorer diet quality. In the Spanish population, the PASOS study showed that more screen time was associated with poorer adherence to the MetDiet, including lower consumption of foods characteristic of the Mediterranean pattern such as fruits, vegetables, fish, legumes and nuts [34]. Along the same lines, a study published in Italy found that certain digital activities, especially digital games and time spent on television or streaming platforms, were associated with lower adherence to the Mediterranean diet [16]. In addition, several publications indicate that the problematic use of mobile devices alters eating routines and is inversely associated with diet quality [8,11]. The specific association found in this study between EDAS-18 scores, reduced fruit consumption, and increased sugar-sweetened beverages supports the biological-behavioral axis theory proposed by Helvacı and Tayhan (2025)[13]. According to this model, the constant distraction of screens and the use of mobile devices directly during main meals encourage unstructured and unconscious eating (mindless eating), displacing fresh foods that require preparation for ultra-processed options that are easy to consume simultaneously [17,18]. On the other hand, although EVA-Adic focuses on addictive behavior scales and not only on exposure time, these results support a common interpretation: the digitalization of daily habits can displace protective eating routines and favor less structured eating behaviors. There are also prospective data that reinforce this hypothesis. In a large cohort of U.S. adolescents, different screen time modalities, including television, video games, videos, messages, and social media, were associated cross-sectionally and prospectively with lower overall diet quality as measured by a MIND index, which shares elements with the Mediterranean pattern and with the DASH dietary approaches to stop hypertension (DASH) diet [35]. Likewise, in Turkish adolescents it has been described that levels of digital addiction tend to decrease as adherence to the Mediterranean diet and physical activity increase, suggesting that digital addiction is usually integrated into a cluster of lower behavioral health: more sedentary lifestyle, greater probability of eating during the use of social networks, more nighttime intake and less adherence to healthy dietary patterns [13]. These findings are consistent with the negative direction observed between EDAS-18 and MEDAS-14 in EVA-Adic. The literature on smartphones and eating behavior offers plausible mechanisms to explain this association. A recent systematic review found that problematic smartphone use and longer daily use time are associated with more symptoms of eating disorders, body dissatisfaction, emotional eating, loss of control, and food addiction, although the overall certainty of the evidence is limited by the predominance of cross-sectional designs [36]. Observational studies in university students have also described relationships between smartphone addiction, risk of eating disorders, poorer sleep quality, evening chronotype and lifestyle changes [21,37]. In this context, the smartphone can act as a marker of impulsivity, emotional dysregulation, insufficient sleep, exposure to food marketing, social comparison and distracted eating, all factors capable of deteriorating adherence to a structured dietary pattern.
The main discrepancy of EVA-Adic with respect to part of the literature is the positive association between CIUS and MEDAS-14. In adolescents, a study of mediation and network analysis observed that problematic use of the internet was associated with lower adherence to the MetDiet and that diet quality partially mediated the relationship between problematic use of the internet and risk of altered eating behavior [38]. Similarly, Helvacı and Tayhan’s work found an inverse relationship between digital addiction and adherence to the MetDiet [13]. At first glance, these data contrast with the positive result observed for CIUS in VAS-Adic. However, there are several reasons that may explain this apparent discrepancy. First, CIUS measures compulsive use of the internet in a broad sense, but does not distinguish whether the use is oriented towards social networks, search for information, work, study, social interaction, shopping, passive leisure or health content. It is possible that, in certain profiles, greater use of the internet coexists with greater exposure to information on nutrition, healthy recipes, physical activity or Mediterranean eating patterns. Second, the scales used in other studies are not necessarily equivalent to CIUS, and much research has been carried out in adolescents or university students, so extrapolation to the EVA-Adic sample should be prudent. Third, some recent studies have not found a direct relationship between Mediterranean adherence and internet addiction. For example, a pilot study published in Nutrients in Greek adolescents and university students observed that Mediterranean adherence was not significantly associated with internet addiction or altered eating behavior; On the other hand, female sex and moderate internet addiction were associated with an increased risk of disordered eating [11]. This result supports the idea that the relationship between the internet, the Mediterranean diet and eating behavior is complex and may depend on the digital phenotype evaluated.
On the other hand, the lack of significant association of video game score (CERV) with global diet differs from that reported by Ribeiro et al. [19], who associate the gamer’s profile with a high consumption of energy drinks and fast foods. In our sample, although men scored significantly higher on the CERV, problematic video game use was only associated in isolation with low consumption of butters or cream, suggesting that in a general college population (not exclusively esports) the pattern of problematic gaming might be more segregated from the household’s core shopping and eating habits. These opposing associations underscore that not all digital users share the same nutritional risk. Therefore, the results of EVA-Adic invite us to abandon a simplistic approach based exclusively on “more digital use = worse diet” and to move towards more precise digital phenotypes: compulsive smartphone, academic/work internet, social networks, streaming, gaming, night use, use during meals and exposure to food content.
Clinical and public health implications. From a clinical point of view, the results suggest that “screen time” or “digital addiction” should not be evaluated as a homogeneous block, since each device and technological behavior modulates health habits in different ways. Nutritional interventions aimed at students and young adults aged 18-34 cannot be limited to traditional dietary advice or the promotion of physical activity. EVA-Adic suggests that the nutritional assessment should incorporate brief questions on digital behavior, especially on smartphone use during meals, intake while checking the mobile phone, nighttime use, sleep, social networks, gaming and perceived loss of control. The negative association between EDAS-18 and MEDAS-14 indicates that the smartphone could act as a warning sign of lower adherence to healthy eating habits. In consultation, this can be translated into simple and applicable recommendations: telephone-free meals, structured digital schedules, reduction of nighttime use, conscious eating strategies, planning of Mediterranean menus and replacing ultra-processed snacks with options in line with the Mediterranean pattern [14,15]. However, the positive association with CIUS makes it necessary to avoid excessively reductionist clinical messages. The Internet can also be a tool for health promotion if it is channeled into nutritional education, goal tracking, healthy recipes, support communities, telemonitoring or brief digital interventions. Recent studies have indicated that smartphone addiction can be inversely related to health-promoting behaviors and worse intuitive eating [39], But this does not invalidate the potential of the digital environment as a vehicle for intervention when used in a structured way. Consequently, the clinical message should not only be to “reduce screens”, but to “order digital use”, separating disruptive, impulsive and nocturnal use from informative, planned and self-care oriented use. From a public health perspective, these findings suggest that the promotion of the Mediterranean diet may benefit from interventions that integrate digital literacy, food literacy, and online food marketing education. Mediterranean pattern is associated with better quality of life in adults in recent reviews published in Nutrients [40], and a healthy diet is associated with better sleep quality, while processed foods rich in free sugars are associated with worse sleep characteristics [41]. Since sleep, physical activity, digital use and diet form an interdependent behavioral system, the most promising interventions are likely to be multicomponent: limiting smartphone use at critical moments, improving sleep hygiene, increasing physical activity and reinforcing Mediterranean habits.
Limitations of the study. Despite the methodological robustness of the EVA-Adic study, which has a large sample and the inclusion of key covariates such as BMI, smoking, alcohol and physical activity measured by the IPAQ-SF. This study has several limitations that must be recognized. First, the cross-sectional design prevents causality or directionality from being established. It is not possible to determine whether problematic smartphone use leads to less Mediterranean adherence, whether poorer organization of habits favors greater digital vulnerability, or whether both phenomena share common determinants such as stress, anxiety, insufficient sleep, sedentary lifestyle, or emotional dysregulation. Second, the primary variables are based on self-reported questionnaires, which can introduce recall bias, social desirability, and misclassification. Although MEDAS-14 is a useful and brief tool, it does not replace more detailed dietary methods or allow you to fully capture total energy, portion sizes, ultra-processed foods, hourly eating patterns or episodes of distracted eating. Third, digital addiction scales assess related but not identical dimensions. EDAS-18, CIUS and scales linked to video games or gaming are not interchangeable, so the associations should be interpreted as specific to each construct. Fourth, objective measures of screen time, mobile unlocks, night-time use, specific applications, exposure to food content or use during meals are not necessarily available. This absence limits the identification of mechanisms. Fifth, although adjusted models reduce confusion, residual confusion by socioeconomic level, weight status, mental health, physical activity, sleep, shifts, coexistence, educational level or motivation towards health cannot be ruled out. Finally, the sample size of 496 subjects is adequate for detecting global associations, but certain stratified analyses or interactions may require larger samples to avoid unstable estimates.
In summary, the results of EVA-Adic provide novel evidence by showing that digital addictive behaviors are differentially related to adherence to the Mediterranean diet. The inverse association between EDAS-18 and MEDAS-14 is consistent with recent studies linking intensive or problematic screen use to poorer diet quality. On the other hand, the positive association between CIUS and MEDAS-14 introduces a relevant nuance: problematic use of the internet should not automatically be assumed as equivalent to problematic use of smartphones. These findings support the need to analyse the different digital phenotypes separately and to incorporate digital behaviour into the promotion strategies of the Mediterranean diet. Future longitudinal studies, with objective measures of digital use and more detailed dietary assessment, will clarify the causal direction and design personalized interventions that integrate digital health and preventive nutrition.
5. Conclusions
In conclusion, the results of the EVA-Adic study reveal that the relationship between problematic screen use and adherence to the Mediterranean diet in young adults is complex and depends on the specific type of digital behavior. Fully adjusted multivariate models show that greater dependence on smartphones (EDAS-18) is independently associated with lower compliance with the Mediterranean dietary pattern, specifically negatively impacting the reduction of daily fruit consumption and an increase in the consumption of sugary drinks. In contrast, compulsive internet use in general (CIUS) showed an unexpected positive association with the global MEDAS score, suggesting that global digital connectivity may harbor heterogeneous patterns of behavior. Finally, problematic video game use and the global digital addiction index showed no significant associations with total diet quality in the adjusted models. These findings underscore the importance of not assessing “screen time” or “digital addiction” as a single or homogeneous construct when analyzing its nutritional impacts. From a public health and nutritional psychiatry perspective, interventions aimed at preserving traditional and protective dietary patterns in the young population should not only promote physical activity or the control of anthropometric variables, but also incorporate digital literacy strategies and management of smartphone use, mitigating impulsivity and technological distractions associated with maladaptive eating habits. Future longitudinal and experimental studies are needed to elucidate the biological and inhibitory mechanisms underlying these specific associations.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) and Table S2: Criteria for Efficiency and Scoring of the 14-item Mediterranean Diet Adherence Screen (MEDAS).
Author Contributions
Writing—Review & Editing, A.V.-P., C.L.-S., S.V.-G., C.S.-R., S.C.-M., L.G.-S. and M.A.G.-M.; Supervision, C.L.-S.; L.G.-S., M.G.-S. and M.A.G.-M. Writing—Original A.V.-P. L.G.-S. and M.G.-S. Draft Preparation, A.V.-P. and C.L.-S.; Investigation, A.V.-P., C.L.-S., S.V.-G., C.S.-R., S.G.-S., S.C.-M. and EVA-Adic Investigators. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Spanish Ministry of Science and Innovation, Institute of Health Carlos III (ISCIII), RD21/0016/0010 (Network for Research on Chronicity, Primary Care, and Health Promotion [RICAPPS]), funded by the Institute of Health Carlos III (ISCIII) and co-funded by the European Union—NextGenerationEU, Recovery and Resilience Facility. The Institute of Biomedical Research of Salamanca (IBSAL) also contributed funding (IBYE22/00003; IBYAP23_0002). The Government of Castile and León collaboratively funded this study through the GRS research projects (GRS2714/C/2023; GRS 2500/B/22). Additional funding was provided by the Spanish Society of Family and Community Medicine (semFYC) through the ʺIsabel Fernández 2023ʺ doctoral thesis grant.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the “Medicine Research Ethics Committee of the Salamanca Health Area” (CEIm reference code: Ref. PI 2021 088671048 on 10 July 2021 and CEIm reference code: Ref. PI 2023 071332 on 24 July 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting the findings of this study are available on ZENODO under the DOI. 10.5281/zenodo.14282873. htps://Zenodo.org/Ibsal. 14282873.
Acknowledgments
We would like to thank all members of the EVA-Adic. We would also like to thank the patient advisers who collaborated with the study investigators.
Abbreviations
| APISAL | Primary Care Research Unit of Salamanca; |
| BMI | Body Mass Index; |
| CERV | Video Game-Related Experiences Questionnaire; |
| CIUS | Compulsive Internet Use Scale; |
| EDAS-18 | Smartphone Dependency and Addiction Scale, short 18-item version; |
| IBSAL | Institute of Biomedical Research of Salamanca; |
| IPAQ-SF / IPAQ | International Physical Activity Questionnaire—Short Form; |
| MEDAS / MEDAS-14 | Mediterranean Diet Adherence Screener; |
| MedDiet | Mediterranean Diet; |
| METs / MET | Metabolic Equivalent of Task; |
| OR | Odds Ratio; |
| PREDIMED | Prevention with Mediterranean Diet; |
| RICAPPS | Network for Research on Chronicity, Primary Care, and Health Promotion; |
| SACyL | Regional Health Management of Castile and León; |
| SD | Standard Deviation; |
| SE | Standard Error; |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology; |
| VIF | Variance Inflation Factor; |
| WHO | World Health Organization. |
Appendix A
EVA-Adic Investigators Group: The members of the EVA-Adic Group are: Manuel A. Gómez Marcos, Luis García-Ortiz, Emiliano Rodríguez-Sánchez, Cristina Lugones-Sánchez, Olaya Tamayo-Morales, Susana González-Sánchez, Leticia Gómez-Sánchez, Sara M. Vicente-Gabriel, Alberto Vicente-Prieto, Sandra Conde-Martín, Marta Gómez-Sánchez, Elena Navarro Matias, Carmen Patino-Alonso, José A. Maderuelo-Fernández, Angela de Cabo-Laso, Benigna Sanchez-Salgado, and Laura Fernandez-Matas.
References
- Baydemir, C.; Ozgur, E.G.; Balci, S. Evaluation of adherence to Mediterranean diet in medical students at Kocaeli University, Turkey. J. Int. Med. Res. 2018, 46, 1585–1594. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferré, M.; Willett, W.C. The Mediterranean diet and health: a comprehensive overview. J. Intern Med. 2021, 290, 549–566. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean Diet and Cardiovascular Health. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M.; Albawardi, N.M. Obesity, Lifestyle Behaviors, and Dietary Habits of Saudi Adolescents Living in Riyadh (ATLS-2 Project): Revisited after a Ten-Year Period. Life 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Hershey, M.S.; Martínez-González, M.; Álvarez-Álvarez, I.; Martínez Hernández, J.A.; Ruiz-Canela, M. The Mediterranean diet and physical activity: better together than apart for the prevention of premature mortality. Br. J. Nutr. 2022, 128, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M.; Albawardi, N.M. Activity energy expenditure, screen time and dietary habits relative to gender among Saudi youth: interactions of gender with obesity status and selected lifestyle behaviours. Asia Pac. J. Clin. Nutr. 2019, 28, 389–400. [Google Scholar] [CrossRef] [PubMed]
- Porri, D.; La Rosa, E.; Pepe, G.; Morabito, L.A.; Arena, V.; Luppino, G.; Fazio, C.; Li Pomi, A.; Corica, D.; Alibrandi, A.; et al. Promoting Healthy Lifestyles in Early Childhood at School with the 0-6 EpPOI Project: Efficacy on Motor Skills and Mediterranean Diet Adherence. Nutrients 2025, 17. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, H.; Meriç Ç, S.; Bülbül, K.; Türkkan, T. Is problematic use of the Internet and smartphone predictor of unhealthy eating behaviors and abnormal body weight in Turkish young adults? J. Health Psychol. 2025, 30, 186–198. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.X.; Song, K.R.; Deng, H.Y.; Geng, X.M.; Zhang, J.L.; Fang, X.Y.; Potenza, M.N.; Zhang, J.T. Beyond screen time: The core influences of problematic screen use on adolescent development networks. J. Behav. Addict 2025, 14, 724–737. [Google Scholar] [CrossRef] [PubMed]
- Ayran, G.; Süleyman, Z.; Avcı, Ü.; Arık, U. The effect of Internet addiction on eating attitude and body image in university students. J. Child Adolesc. Psychiatr. Nurs. 2021, 34, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Stavraki, C.; Georgiadis, N.; Kornarou, E.; Tsitsika, A.K.; Sergentanis, T.N.; Vassilakou, T. Exploring the Association Between Internet Use and Dietary Habits of Adolescents and University Students in Greece: A Pilot Study. Nutrients 2026, 18. [Google Scholar] [CrossRef] [PubMed]
- Votsi, I.C.; Koutelidakis, A. How Screen Time Affects Greek Schoolchildren’s Eating Habits and Functional Food Consumption?-A Cross-Sectional Study. Nutrients 2025, 17. [Google Scholar] [CrossRef] [PubMed]
- Helvacı, G.; Tayhan, F. Determinants and relationships of digital addiction, diet quality, and physical activity in adolescents. Front Public Health 2025, 13, 1654322. [Google Scholar] [CrossRef] [PubMed]
- Say, Y.H.; Nordin, M.S.; Ng, A.L.O. Association of chronotype and sleep behaviors with mental well-being, eating behaviors, and adiposity traits: a cross-sectional study among a sample of urban Malaysian adults. BMC Public Health 2025, 25, 1168. [Google Scholar] [CrossRef] [PubMed]
- Mohammad Johari, M.H.; Tan, S.T. Internet addiction and its relationship with food choice motives and the risk of eating disorders among young adults in Malaysia. Sci. Rep. 2024, 14, 5643. [Google Scholar] [CrossRef] [PubMed]
- Buja, A.; Miatton, A.; Zanovello, A.; Brocadello, F.; Baldovin, T.; Muhiddin, M.N.; Spreghini, I. Media Usage and Adherence to the Mediterranean Diet in Children. Nutrients 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- López-Gil, J.F.; Quiroz-Cárdenas, F.; Montenegro-Espinosa, J.A.; Cisneros-Vásquez, E.; Miño, C.; Castillo-Miñaca, M.E.; Unda-López, R.A.; Sánchez-Charcopa, L.A.; Zalamea-Delgado, M.P.; Masache-Cruz, M.J.; et al. Eating distractions as predictors of ultra-processed food consumption and Mediterranean diet adherence in adolescents. Sci. Rep. 2025, 15, 7579. [Google Scholar] [CrossRef] [PubMed]
- Yong, J.Y.Y.; Tong, E.M.W.; Liu, J.C.J. Meal-time Smartphone Use in an Obesogenic Environment: Two Longitudinal Observational Studies. JMIR Mhealth Uhealth 2021, 9, e22929. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, F.J.; Teixeira, R.; Poínhos, R. Dietary Habits and Gaming Behaviors of Portuguese and Brazilian Esports Players. Nutrients 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Örnek, B.Y.; Gündoğmuş, İ. The Effects of Smartphone and Internet Gaming Addiction on Eating Attitudes Among University Students. Psychiatry Investig. 2022, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Hao, Q.H.; Peng, W.; Tu, Y.; Zhang, L.; Zhu, T.M. Relationship between smartphone addiction and eating disorders and lifestyle among Chinese college students. Front Public Health 2023, 11, 1111477. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Domingo, M.; Fuentes, V.; Perez-Padilla, J.; Aranda, M. EDAS-18: validation of the dependency and addiction to smartphone scale short-form. Ter. Psicológica 2020, 38, 339–361. [Google Scholar]
- Chamarro, A.; Carbonell, X.; Manresa, J.M.; Munoz-Miralles, R.; Ortega-Gonzalez, R.; Lopez-Morron, M.R.; Batalla-Martinez, C.; Toran-Monserrat, P. The Questionnaire of Experiences Associated with Video games (CERV): an instrument to detect the problematic use of video games in Spanish adolescents. Adicciones 2014, 26, 303–311. [Google Scholar] [PubMed]
- Meerkerk, G.J.; Van Den Eijnden, R.J.; Vermulst, A.A.; Garretsen, H.F. The Compulsive Internet Use Scale (CIUS): some psychometric properties. Cyberpsychol Behav. 2009, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Gabriel, S.; Lugones-Sánchez, C.; Tamayo-Morales, O.; Vicente Prieto, A.; González-Sánchez, S.; Conde Martín, S.; Gómez-Sánchez, M.; Rodríguez-Sánchez, E.; García-Ortiz, L.; Gómez-Sánchez, L.; et al. Relationship between addictions and obesity, physical activity and vascular aging in young adults (EVA-Adic study): a research protocol of a cross-sectional study. Front Public Health 2024, 12, 1322437. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed]
- The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): a major international collaboration. WHO MONICA Project Principal Investigators. J. Clin. Epidemiol. 1988, 41, 105–114. [CrossRef] [PubMed]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): a systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: the PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- García-Domingo, M.; Fuentes, V.; Pérez-Padilla, J.; Aranda, M. EDAS-18: validación de la versión corta de la escala de dependencia y adicción al smartphone. Ter. Psicológica 2020, 38, 339–361. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Participants. Jama 2025, 333, 71–74. [CrossRef] [PubMed]
- Wärnberg, J.; Pérez-Farinós, N.; Benavente-Marín, J.C.; Gómez, S.F.; Labayen, I.; A, G.Z.; Gusi, N.; Aznar, S.; Alcaraz, P.E.; González-Valeiro, M.; et al. Screen Time and Parents’ Education Level Are Associated with Poor Adherence to the Mediterranean Diet in Spanish Children and Adolescents: The PASOS Study. J. Clin. Med. 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Nagata, J.M.; Weinstein, S.; Bashir, A.; Lee, S.; Al-Shoaibi, A.A.A.; Shao, I.Y.; Ganson, K.T.; Testa, A.; He, J.; Garber, A.K. Associations of Contemporary Screen Time Modalities With Early Adolescent Nutrition. Acad. Pediatr. 2024, 24, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Keeler, J.; Conde Ludtke, L.; Yang, Q.; Raschke Rameh, V.; Ward, R.; Treasure, J.; Carter, B. Associations of Problematic Smartphone Use and Smartphone Screen Time With Eating Disorder Psychopathology in Non-Clinical Samples: A Systematic Review. JMIR Ment. Health 2026, 13, e88572. [Google Scholar] [CrossRef] [PubMed]
- Hasan, H.; Shihab, K.A.; Mohammad, Z.; Jahan, H.; Coussa, A.; Faris, M.E. Associations of smartphone addiction, chronotype, sleep quality, and risk of eating disorders among university students: A cross-sectional study from Sharjah/United Arab Emirates. Heliyon 2023, 9, e12882. [Google Scholar] [CrossRef] [PubMed]
- Aydin Cil, M.; Carikci, S.; Foroudi Pourdeh, E.; Jahrami, H. The interaction between problematic internet use, diet quality, and disordered eating risk in adolescents: a mediation and network analysis. Eat. Weight Disord. 2025, 30, 61. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.; Pei, Q.; Fang, T.; Xiao, L.; Yin, D.; Sun, Z. Assessment of smartphone addiction and its relationship with health-promoting lifestyle profile and intuitive eating behavior: a cross-sectional study. Front Psychiatry 2025, 16, 1682921. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Guglielmetti, M.; Ferraris, C.; Frias-Toral, E.; Domínguez Azpíroz, I.; Lipari, V.; Di Mauro, A.; Furnari, F.; Castellano, S.; Galvano, F.; et al. Mediterranean Diet and Quality of Life in Adults: A Systematic Review. Nutrients 2025, 17. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Grosso, G.; Castellano, S.; Galvano, F.; Caraci, F.; Ferri, R. Association between diet and sleep quality: A systematic review. Sleep Med. Rev. 2021, 57, 101430. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Mediterranean diet adherence score according to problematic screen use. Bars represent the mean Mediterranean diet score ± standard error according to the presence or absence of problematic use of smartphone, internet, video games, and global digital addiction. Comparisons between groups were performed using Student’s t-test. MEDAS: Mediterranean Diet Adherence Screener; SE: standard error.
Figure 1.
Mediterranean diet adherence score according to problematic screen use. Bars represent the mean Mediterranean diet score ± standard error according to the presence or absence of problematic use of smartphone, internet, video games, and global digital addiction. Comparisons between groups were performed using Student’s t-test. MEDAS: Mediterranean Diet Adherence Screener; SE: standard error.

Figure 2.
Correlations between digital addiction-related scores and Mediterranean diet adherence. Scatter plots showing the association between MEDAS-14 score and: (a) smartphone addiction assessed using EDAS-18; (b) Internet addiction assessed using CIUS; (c) videogame addiction assessed using CERV; and (d) global digital addiction score. The black line represents the linear regression trend. Pearson’s correlation coefficients are shown for each panel. MEDAS-14: 14-item Mediterranean Diet Adherence Screener; EDAS-18: Smartphone Addiction Scale; CIUS: Compulsive Internet Use Scale; CERV: Questionnaire of Experiences Related to Video Games.
Figure 2.
Correlations between digital addiction-related scores and Mediterranean diet adherence. Scatter plots showing the association between MEDAS-14 score and: (a) smartphone addiction assessed using EDAS-18; (b) Internet addiction assessed using CIUS; (c) videogame addiction assessed using CERV; and (d) global digital addiction score. The black line represents the linear regression trend. Pearson’s correlation coefficients are shown for each panel. MEDAS-14: 14-item Mediterranean Diet Adherence Screener; EDAS-18: Smartphone Addiction Scale; CIUS: Compulsive Internet Use Scale; CERV: Questionnaire of Experiences Related to Video Games.

Figure 3.
Association between measures of digital addiction and adherence to the Mediterranean diet. The non-standardized β coefficients and their 95% confidence intervals are shown for each measure of digital addiction. Panel a shows the model adjusted for age and sex. Panel b shows the model with full adjustment. EDAS-18: smartphone addiction scale; CIUS: Compulsive Internet Use Scale; CERV: questionnaire of experiences related to video games; CI: confidence interval; Adjusted R²: adjusted coefficient of determination. Estimates in blue indicate statistically significant associations.
Figure 3.
Association between measures of digital addiction and adherence to the Mediterranean diet. The non-standardized β coefficients and their 95% confidence intervals are shown for each measure of digital addiction. Panel a shows the model adjusted for age and sex. Panel b shows the model with full adjustment. EDAS-18: smartphone addiction scale; CIUS: Compulsive Internet Use Scale; CERV: questionnaire of experiences related to video games; CI: confidence interval; Adjusted R²: adjusted coefficient of determination. Estimates in blue indicate statistically significant associations.

Figure 4.
Adjusted association of EDAS-18 and CIUS scores with individual 14-item MEDAS criteria. The odds ratio (OR) and their 95% confidence intervals for the fulfillment of each MEDAS criterion are shown for each one-point increase in the EDAS-18 or CIUS score. Panel a represents associations with smartphone dependence as measured by EDAS-18, and panel b represents associations with problematic internet use as measured by CIUS. Model 2 was adjusted for age, sex, body mass index, smoking, alcohol consumption, and physical activity. Blue circles and lines indicate statistically significant associations; Gray circles and lines indicate non-significant associations. The wine consumption criterion had unstable confidence intervals and is shown only as an indication. Blue color shows significant association.
Figure 4.
Adjusted association of EDAS-18 and CIUS scores with individual 14-item MEDAS criteria. The odds ratio (OR) and their 95% confidence intervals for the fulfillment of each MEDAS criterion are shown for each one-point increase in the EDAS-18 or CIUS score. Panel a represents associations with smartphone dependence as measured by EDAS-18, and panel b represents associations with problematic internet use as measured by CIUS. Model 2 was adjusted for age, sex, body mass index, smoking, alcohol consumption, and physical activity. Blue circles and lines indicate statistically significant associations; Gray circles and lines indicate non-significant associations. The wine consumption criterion had unstable confidence intervals and is shown only as an indication. Blue color shows significant association.

Figure 5.
Adjusted association of CERV and global digital addiction scores with individual MEDAS 14-item criteria. Odds ratios (ORs) and 95% confidence intervals (95% CIs) are shown for the association between digital addiction scores and each Mediterranean Diet Adherence Screener (MEDAS-14) criterion. Panel a shows the association for problematic videogame use measured by the CERV score, and panel b shows the association for the global digital addiction score. Blue estimates indicate statistically significant associations, whereas grey estimates indicate non-significant associations. For the wine criterion, the confidence interval was unstable and is therefore indicated separately. CERV: Questionnaire of Experiences Related to Videogames; MEDAS: Mediterranean Diet Adherence Screener; OR: odds ratio; CI: confidence interval. Blue color shows significant association.
Figure 5.
Adjusted association of CERV and global digital addiction scores with individual MEDAS 14-item criteria. Odds ratios (ORs) and 95% confidence intervals (95% CIs) are shown for the association between digital addiction scores and each Mediterranean Diet Adherence Screener (MEDAS-14) criterion. Panel a shows the association for problematic videogame use measured by the CERV score, and panel b shows the association for the global digital addiction score. Blue estimates indicate statistically significant associations, whereas grey estimates indicate non-significant associations. For the wine criterion, the confidence interval was unstable and is therefore indicated separately. CERV: Questionnaire of Experiences Related to Videogames; MEDAS: Mediterranean Diet Adherence Screener; OR: odds ratio; CI: confidence interval. Blue color shows significant association.


Table 1.
Sociodemographic, anthropometric, behavioral, and digital addiction characteristics of the sample according to Mediterranean diet adherence level.
Table 1.
Sociodemographic, anthropometric, behavioral, and digital addiction characteristics of the sample according to Mediterranean diet adherence level.
| Variables and instruments |
Total sample (N = 496) |
Low adherence (MEDAS < 9; n = 339) |
High adherence (MEDAS ≥ 9; n = 157) |
p-valueᵃ |
| Age (years), mean ± SD | 26.60 ± 4.41 | 26.29 ± 4.53 | 27.28 ± 4.06 | 0.015* |
| Sex, n (%) | <0.001* | |||
| Male | 220 (44.4) | 171 (50.4) | 49 (31.2) | |
| Female | 276 (55.6) | 168 (49.6) | 108 (68.8) | |
| Alcohol consumption (g/week), mean ± SD |
48.93 ± 73.90 | 52.19 ± 74.03 | 41.88 ± 73.36 | 0.149 |
| Physical activity (MET-min/week), mean ± SD |
2660.50 ± 2499.48 | 2623.46 ± 2739.65 | 2740.49 ± 1884.60 | 0.628 |
| Smoking status, n (%) | 0.002* | |||
| Non-smoker | 407 (82.1) | 266 (78.5) | 141 (89.8) | |
| Smoker | 89 (17.9) | 73 (21.5) | 16 (10.2) | |
| BMI (kg/m²), mean ± SD | 24.01 ± 3.80 | 24.30 ± 3.96 | 23.38 ± 3.35 | 0.008* |
| Digital addiction scales | ||||
| EDAS-18 (smartphone), mean ± SD |
40.87 ± 12.24 | 41.02 ± 12.63 | 40.57 ± 11.37 | 0.703 |
| CIUS (Internet), mean ± SD | 13.83 ± 9.89 | 13.57 ± 9.50 | 14.38 ± 10.70 | 0.418 |
| CERV (video games), mean ± SDᵇ | 3.54 ± 5.22 | 3.80 ± 5.29 | 2.98 ± 5.06 | 0.103 |
| Global digital addiction score, mean ± SD | 58.25 ± 21.76 | 58.39 ± 21.77 | 57.93 ± 21.80 | 0.826 |
Values are presented as mean ± standard deviation or n (%). Abbreviations: SD, standard deviation; BMI, body mass index; MEDAS, Mediterranean Diet Adherence Screener; EDAS-18, Smartphone Addiction Scale; CIUS, Compulsive Internet Use Scale; CERV, Video Game Experiences Questionnaire. ᵃ p-values were calculated using the χ² test for categorical variables and independent-samples t-tests for continuous variables, with Welch’s correction when variances were unequal. ᵇ In the supplied SPSS output, CERV scores were available for the full analytic sample (N = 496); the active-gamer subgroup size was not provided. *Statistically significant difference (p < 0.05).
Table 2.
Sociodemographic, anthropometric, behavioral, and digital addiction characteristics of the sample according to sex.
Table 2.
Sociodemographic, anthropometric, behavioral, and digital addiction characteristics of the sample according to sex.
| Variables and instruments | Men (n = 220) | Women (n = 276) | p-valueᵃ |
| Age (years), mean ± SD | 27.09 ± 4.40 | 26.22 ± 4.38 | 0.029* |
| Score mediterraneam diet, mean ± SD | 6.96 ± 2.06 | 7.81 ± 1.88 | <0.001* |
| Alcohol consumption (g/week), mean ± SD | 61.56 ± 91.54 | 38.86 ± 54.11 | 0.001* |
| Physical activity (MET-min/week), mean ± SD | 3172 ± 3140 | 2253 ± 1737 | <0.001* |
| Smoking status, n (%) | 0.413 | ||
| Non-smoker | 184 (83.6) | 223 (80.8) | |
| Smoker | 36 (16.4) | 53 (19.2) | |
| BMI (kg/m²), mean ± SD | 25.30 ± 3.67 | 22.98 ± 3.59 | <0.001* |
| Digital Addiction Scales | |||
| EDAS-18 (smartphone) | 40.37 ± 12.15 | 41.28 ± 12.31 | 0.411 |
| CIUS (internet) | 13.38 ± 9.75 | 14.18 ± 10.01 | 0.370 |
| CERV (video games) | 5.94 ± 6.18 | 1.63 ± 3.23 | <0.001* |
| Global digital addiction | 59.69 ± 22.09 | 57.09 ± 21.46 | 0.187 |
Values are presented as mean ± standard deviation or n (%). SD: standard deviation; BMI: body mass index; MET: metabolic equivalent of task; EDAS-18: Smartphone Dependency and Addiction Scale; CIUS: Compulsive Internet Use Scale; CERV: Video Game-Related Experiences Questionnaire. ᵃp-values were calculated using Student’s t-test for continuous variables, with Welch’s correction when variances were unequal, and the chi-square test for categorical variables. *p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



