Submitted:
25 June 2026
Posted:
29 June 2026
You are already at the latest version
Abstract
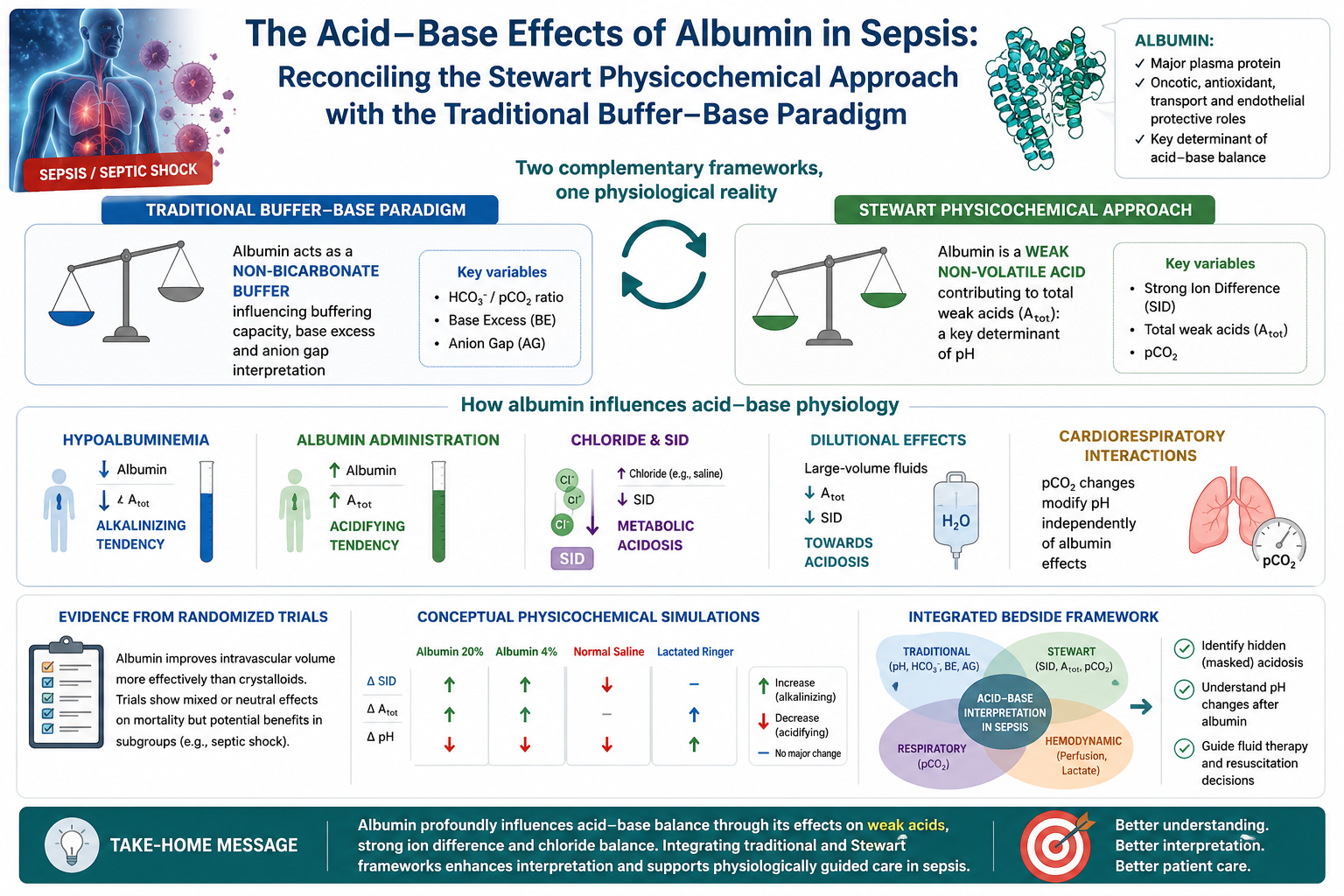
Albumin administration in sepsis and septic shock remains controversial because of uncertain clinical benefits and complex acid–base effects. Unlike crystalloids, albumin influences acid–base equilibrium through effects on chloride balance, strong ion dif-ference (SID), buffering systems, and weak acid concentration. These effects may be in-terpreted differently by the traditional bicarbonate-centered framework and Stewart’s physicochemical approach. In the traditional paradigm, albumin acts mainly as a non-bicarbonate plasma buffer influencing base excess and anion gap interpretation. In the Stewart framework, albumin is a weak non-volatile acid contributing to total weak ac-ids (Atot), thereby influencing hydrogen ion dissociation and pH regulation. This nar-rative review compares these two approaches to albumin-related acid–base physiolo-gy in sepsis, with emphasis on chloride balance, strong ion difference, hypoalbu-minemia, dilutional effects, and cardiorespiratory interactions during mechanical ven-tilation and septic shock. We also contextualize these mechanisms within major ran-domized trials of albumin and resuscitation fluids and provide conceptual simulations illustrating the directional acid–base effects of different fluid compositions. The review focuses on masked acidosis in hypoalbuminemic patients and on the interpretation of pH changes after albumin administration. Finally, we propose an integrated bedside framework combining traditional, physicochemical, respiratory, and hemodynamic variables for acid–base interpretation during fluid resuscitation.
Keywords:
albumin
; Stewart approach
; acid–base physiology
; sepsis
; strong ion difference
; critical care
; hypoalbuminemia
1. Introduction
Fluid resuscitation remains one of the cornerstones of sepsis management [1,2,3]. However, the physiological consequences of different resuscitation fluids remain incompletely understood, particularly regarding acid–base equilibrium. Although crystalloids have traditionally dominated initial resuscitation strategies, albumin continues to attract interest because of its unique physiological properties and its potential role in severe sepsis and septic shock [4,5,6].
Albumin differs fundamentally from crystalloid solutions because it simultaneously influences oncotic pressure, endothelial function, drug transport, antioxidant activity, intravascular volume, and acid–base physiology [7,8,9,10]. Unlike balanced crystalloids or saline, albumin administration modifies both strong ion balance and the circulating concentration of weak acids.
Traditionally, acid–base disorders have been interpreted through the Henderson–Hasselbalch equation and the bicarbonate-centered framework. Within this paradigm, albumin acts primarily as a non-bicarbonate plasma buffer affecting buffering capacity, base excess, and anion gap interpretation.
In contrast, Stewart proposed a physicochemical model in which pH is determined by three independent variables: partial pressure of carbon dioxide (pCO₂), strong ion difference (SID), and total concentration of weak acids (Atot). Within this framework, albumin is interpreted as a weak non-volatile acid directly contributing to Atot.
These two frameworks offer complementary explanations for albumin-related acid-base changes, particularly in septic patients with hypoalbuminemia, hyperchloremia, and mixed metabolic disorders.
This narrative review aims to reconcile traditional and physicochemical interpretations of albumin-related acid–base physiology in sepsis. We integrate mechanistic concepts, clinical trial context, conceptual simulations, and bedside implications to propose a practical framework for interpretation.
This article is intended as a mechanistic and clinically oriented narrative review, rather than as a systematic evidence synthesis.
2. Historical Evolution of Acid–Base Interpretation
Modern acid–base physiology emerged from more than a century of progressive conceptual refinement. Early physiological models focused primarily on the relationship between carbon dioxide and bicarbonate, whereas later approaches attempted to integrate electrolyte balance, buffering systems, and physicochemical principles into a unified interpretation of plasma acid–base equilibrium.
The Henderson equation, introduced in the early twentieth century and later reformulated by Hasselbalch into logarithmic form, established the conceptual basis of bicarbonate-centered acid–base analysis [10,11]. Within this framework, pH was interpreted as a function of bicarbonate concentration and dissolved carbon dioxide tension. This approach rapidly became clinically dominant because it was intuitive, mathematically accessible, and closely aligned with arterial blood gas measurements.
Subsequent developments by Van Slyke and Siggaard-Andersen expanded the clinical applicability of bicarbonate-centered interpretation through concepts such as buffer base and base excess [12,13,14]. These variables attempted to isolate the “metabolic” component of acid–base disorders independently of respiratory compensation. Base excess became deeply integrated into critical care and perioperative medicine because it provided a rapid bedside estimate of metabolic acid–base disturbances.
Despite its clinical usefulness, the traditional framework encountered increasing difficulties when confronted with complex ICU scenarios characterized by mixed electrolyte abnormalities, dilutional states, hypoalbuminemia, hyperchloremia, and large-volume fluid resuscitation [14,15]. In such situations, bicarbonate concentration often behaved more as a dependent variable than as a mechanistic explanation of acid–base change.
These limitations stimulated interest in alternative interpretative models. Stewart proposed a physicochemical approach in which hydrogen ion concentration was determined by three independent variables: pCO₂, strong ion difference (SID), and total concentration of weak acids (Atot) [16]. In this framework, bicarbonate was no longer considered an independent regulator of pH but rather a dependent consequence of physicochemical equilibrium.
Fencl and colleagues later translated Stewart’s mathematically complex model into a clinically accessible bedside approach by introducing simplified calculations for SID, albumin effects, and unmeasured anions [17,18,19]. This adaptation substantially increased the clinical applicability of physicochemical acid–base interpretation in critical care medicine.
The rise of Stewart physiology coincided with growing recognition of hyperchloremic metabolic acidosis during saline resuscitation and with increasing awareness that hypoalbuminemia itself exerted major acid–base effects [20,21]. Critically ill patients often exhibited apparently paradoxical combinations of normal pH, elevated lactate, low albumin, and severe electrolyte abnormalities that were incompletely explained by bicarbonate-centered interpretation alone.
Within this historical context, albumin occupies a particularly important conceptual position because it lies at the intersection of the two frameworks. In the traditional model, albumin is viewed primarily as a plasma buffer influencing base excess and anion gap interpretation. In the Stewart framework, albumin becomes one of the principal determinants of Atot and therefore a direct regulator of acid–base equilibrium.
The evolution from traditional to physicochemical interpretation should not be viewed as a replacement of one model by another. Rather, the Stewart approach expanded mechanistic understanding of acid–base physiology while traditional variables retained substantial practical and prognostic utility. Contemporary critical care practice increasingly relies on integration of both perspectives rather than exclusive adherence to either framework.
3. The Traditional Buffer–Base Interpretation
The traditional approach to acid–base physiology is centered on the Henderson–Hasselbalch equation:
Within this framework, pH is determined by the relationship between bicarbonate concentration and pCO₂ [10,11].
Albumin functions primarily as a non-bicarbonate plasma buffer because of its multiple negatively charged residues capable of binding hydrogen ions. Consequently, hypoalbuminemia reduces total plasma buffering capacity.
This phenomenon has several clinically important consequences. First, hypoalbuminemia lowers the measured anion gap despite persistent accumulation of unmeasured anions [22,23]. Correction formulas for albumin-adjusted anion gap are therefore recommended in critically ill patients. Second, severe hypoalbuminemia may itself exert an alkalinizing effect because weak acidic buffering components are reduced [24]. Conversely, albumin administration may appear acidifying because restoration of weak acid buffering may lower bicarbonate concentration and base excess despite stable or improving tissue perfusion [25,26,27].
However, the traditional framework often struggles to distinguish albumin-specific effects from concomitant changes in chloride balance, sodium concentration, dilution, renal compensation, and tissue perfusion.
4. The Stewart Physicochemical Approach
Stewart proposed that hydrogen ion concentration is determined by three independent variables:
- Partial pressure of carbon dioxide (pCO₂)
- Strong ion difference (SID)
- Total concentration of weak acids (Atot)
This framework may be summarized conceptually as:
Within plasma, albumin and phosphate constitute the principal weak acids contributing to Atot.
Strong ion difference may be simplified as:
According to Stewart physiology, increases in Atot favor hydrogen ion dissociation and therefore lower pH [16]. Conversely, reductions in Atot exert an alkalinizing tendency. Fluids with SID substantially lower than plasma SID produce metabolic acidosis, whereas fluids with higher SID are relatively alkalinizing. Importantly, albumin administration may influence acid–base equilibrium through at least two simultaneous mechanisms:
- increased Atot (weak acid effect);
- altered SID due to accompanying chloride load.
This distinction explains why apparently similar acid–base changes may emerge through fundamentally different mechanisms.
5. Traditional Versus Stewart Interpretations
The traditional and Stewart approaches are often presented as alternative or competing models of acid–base physiology. However, in the context of albumin administration, they are better understood as complementary interpretative frameworks [28]. Both describe the same biological system, but they emphasize different explanatory levels. This conceptual contrast between the traditional buffer–base approach and the Stewart physicochemical approach is summarized in Figure 1.
The Stewart approach shifts the interpretative focus from bicarbonate to physicochemical determinants [18,19]. In this model, bicarbonate is not an independent determinant of pH but a dependent variable generated by the interaction among pCO₂, SID, and Atot. Albumin is therefore not simply a buffer but a major weak acid contributing to Atot. A fall in albumin concentration lowers Atot and tends to alkalinize plasma, whereas albumin administration increases Atot and tends to lower pH.
This difference is particularly relevant in septic shock, where hypoalbuminemia, hyperchloremia, hyperlactatemia, renal dysfunction, and large-volume fluid administration frequently coexist. In such settings, the traditional framework may correctly identify the presence of metabolic acidosis but may not fully explain why bicarbonate or base excess changes after albumin infusion. Conversely, the Stewart framework may clarify the mechanism but can be less immediately accessible at the bedside [29].
Neither interpretation necessarily implies clinical deterioration. A decrease in pH after albumin administration may occur even when hemodynamic variables improve, because the acid–base change may reflect restoration of weak acid concentration rather than worsening tissue hypoperfusion. This distinction is central to the clinical interpretation of albumin therapy in sepsis. The main conceptual differences between the two frameworks are also summarized in Table 1
6. Physicochemical Simulations of Albumin Administration
To illustrate the physiological mechanisms discussed in this review, we generated simplified conceptual simulations based on Stewart principles under fixed baseline assumptions. These simulations were not intended to provide calibrated patient-level predictions, but rather to illustrate the expected direction of acid–base changes when albumin concentration, chloride burden, SID, and lactate vary under controlled assumptions. The simulated directional effects of albumin 20%, albumin 4%, normal saline, and lactated Ringer solution are illustrated in Figure 2.
Three mechanisms were explored. First, increasing albumin concentration at stable SID and pCO₂ was used to illustrate the Atot-mediated acidifying effect of albumin. Second, saline and albumin-containing solutions were compared conceptually to distinguish SID-mediated acidosis from Atot-mediated acidification. Third, hypoalbuminemia was modeled as a condition capable of partially masking lactic or hyperchloremic acidosis, with albumin administration potentially “unmasking” the underlying metabolic disturbance.
These simulations are purely illustrative and should not be interpreted as validated quantitative physiological predictions or patient-level models. Their purpose is to clarify mechanisms, not to predict the exact pH response of individual patients.
7. Fluid Composition, Chloride Burden, and Strong Ion Difference
The relationship between chloride balance and acid–base physiology represents one of the most clinically relevant applications of Stewart’s physicochemical framework. Among critically ill patients, hyperchloremia is extremely common and frequently results from administration of chloride-rich intravenous fluids, particularly normal saline and some albumin preparations [27,29].
Within the traditional framework, saline-associated metabolic acidosis has historically been described as “dilutional” or “hyperchloremic” acidosis. However, Stewart physiology provides a mechanistic explanation by demonstrating that chloride excess reduces strong ion difference (SID), thereby favoring hydrogen ion dissociation and lowering pH [25].
Normal plasma SID is approximately 38–42 mEq/L, whereas the SID of normal saline is effectively zero because sodium and chloride concentrations are equal. Administration of large volumes of saline therefore lowers plasma SID and predictably produces metabolic acidosis. Balanced crystalloids differ substantially in this regard. Solutions such as lactated Ringer or Plasma-Lyte contain lower chloride concentrations and higher effective SID values. Consequently, they exert smaller acidifying effects compared with saline-based fluids.
This distinction has become increasingly relevant following major randomized trials comparing balanced crystalloids and saline. Trials such as SPLIT, SMART, BaSICS, and PLUS primarily evaluated clinical outcomes rather than acid–base physiology, yet they collectively reinforced the concept that fluid composition itself may influence renal function, electrolyte balance, and acid–base equilibrium [30,31,32,33,34].
Although the magnitude of clinical benefit remains debated, several mechanistic pathways have been proposed through which chloride-rich solutions may adversely affect organ function. Experimental studies suggest that hyperchloremia may induce renal vasoconstriction through tubuloglomerular feedback mechanisms, potentially reducing renal cortical perfusion and glomerular filtration [35]. Hyperchloremia may also influence inflammatory signaling, endothelial function, and microcirculatory regulation [29,35].
Albumin-containing solutions require additional interpretation because they simultaneously modify chloride balance and weak acid concentration. Albumin 4% solutions exert relatively modest Atot-related effects because of their lower weak acid concentration, whereas hyperoncotic albumin preparations may produce stronger Atot-mediated acidifying tendencies [5]. Furthermore, many commercially available albumin formulations are suspended in chloride-rich carrier solutions, thereby combining SID reduction with weak acid expansion.
From a clinical perspective, these differences are particularly relevant in septic shock, where hypoalbuminemia and cumulative chloride exposure frequently coexist. Under these conditions, isolated interpretation of bicarbonate concentration or base excess may incompletely capture the complexity of the underlying acid–base disorder. The expected directional acid–base effects of common resuscitation fluids are summarized in Table 2.
9. Masked Acidosis and Bedside Interpretation Pitfalls
Hypoalbuminemia is common in septic shock and critical illness. From a Stewart perspective, reduced albumin concentration lowers Atot and therefore exerts an alkalinizing tendency. This effect may partially offset hyperchloremia, lactic acidosis, or unmeasured anions, leading to apparently near-normal pH or base excess values despite relevant metabolic derangement [36]. This mechanism is illustrated schematically in Figure 3.
Albumin administration may reverse this masking effect. Restoration of weak acid concentration may transiently reduce pH or base excess even when hemodynamics and perfusion markers are stable or improving [25,37,38]. Therefore, isolated pH reductions after albumin infusion should be interpreted together with lactate, chloride, albumin concentration, renal function, and hemodynamic trends.
A second interpretative challenge is that saline and albumin may produce similar arterial blood gas patterns through different mechanisms. Saline-associated acidosis is predominantly mediated by chloride-induced SID reduction, whereas albumin-associated acidification mainly reflects expansion of weak acid concentration. Similar pH or base excess values may therefore correspond to distinct physiological states with different implications for fluid management.
Three practical pitfalls should be avoided at the bedside. First, near-normal pH or base excess should not be considered reassuring when severe hypoalbuminemia coexists with elevated lactate, hyperchloremia, renal dysfunction, or unmeasured anions. Second, a modest fall in pH after albumin administration should not be interpreted in isolation from hemodynamic and perfusion trends [39]. Third, chloride-associated acidosis should not be considered equivalent to lactate-associated acidosis, because the former is primarily SID-mediated whereas the latter may reflect altered metabolism, impaired clearance, or tissue hypoperfusion. Representative scenarios are summarized in Table 3.
10. Integrated Bedside Interpretation
In clinical practice, conventional arterial blood gas variables should be interpreted alongside albumin concentration, chloride balance, lactate, renal function, and hemodynamic response. This integrated approach helps distinguish SID-mediated acidosis from Atot-mediated acidification, identify masked metabolic acidosis, and avoid overinterpreting isolated changes in bicarbonate or base excess [25,26,39]. A proposed bedside framework is shown in Figure 4.
Traditional variables remain essential for rapid assessment of acidemia, respiratory compensation, and the metabolic component of acid–base disturbance. Stewart-derived variables add mechanistic resolution when hypoalbuminemia, chloride exposure, renal dysfunction, or mixed metabolic disorders coexist. In this context, albumin concentration, corrected anion gap, chloride, SID, and unmeasured ions may clarify apparently paradoxical arterial blood gas findings.
Importantly, acid–base interpretation should remain linked to organ-level physiology [40,41]. Lactate kinetics, vasopressor requirements, urine output, fluid balance, renal function, respiratory status, and overall perfusion should determine whether a change in pH reflects true clinical deterioration or a predictable physicochemical shift. A suggested integrated bedside interpretation framework is summarized in Table 4.
11. Cardiorespiratory Interactions During Albumin Administration and Acid–Base Resuscitation
Acid–base physiology during sepsis cannot be fully separated from cardiopulmonary interactions. In mechanically ventilated septic patients, alveolar ventilation, dead-space fraction, pulmonary vascular tone, right ventricular loading conditions, and tissue perfusion may all influence the clinical expression of albumin-related acid–base changes.
Carbon dioxide represents the respiratory determinant of pH within both traditional and physicochemical frameworks [42]. Therefore, ventilatory settings and CO₂ clearance may interact with SID- and Atot-mediated metabolic effects, particularly in patients managed with protective ventilation or permissive hypercapnia [43,44].
Albumin may also affect respiratory physiology indirectly through changes in intravascular oncotic pressure, endothelial permeability, and pulmonary fluid distribution. Under selected conditions, restoration of oncotic pressure may favor reabsorption of extravascular lung water, although these effects are context-dependent and should not be interpreted as evidence that albumin uniformly improves oxygenation or respiratory outcomes [45,46].
Correction of effective hypovolemia may improve preload, cardiac output, microcirculatory flow, and oxygen delivery, even when arterial pH modestly decreases because of increased Atot [47,48,49]. Conversely, hyperchloremic acidosis and severe acidemia may adversely affect pulmonary vascular resistance, right ventricular afterload, myocardial contractility, and vasomotor responsiveness [35].
Positive-pressure ventilation further modifies this balance by altering venous return, pulmonary perfusion, right ventricular afterload, and CO₂ elimination [45,46]. In septic patients with ARDS, the coexistence of permissive hypercapnia, chloride-rich fluid exposure, hypoalbuminemia, and lactate accumulation may generate mixed acid–base disorders in which apparently small pH changes conceal substantial physiological heterogeneity [48,49]. These interactions are summarized schematically in Figure 5.
12. Randomized Controlled Trials: Clinical Context for Albumin and Fluid Composition
Although this review focuses on acid–base physiology, the interpretation of albumin therapy in sepsis should be anchored to the major randomized trials evaluating albumin, colloids, saline, and balanced crystalloids in critically ill patients. These trials were not designed to test Stewart physiology, Atot, SID, or chloride-mediated acid–base trajectories, but they provide the clinical background within which physiological effects must be interpreted.
The SAFE trial compared 4% albumin with normal saline in 6997 critically ill patients requiring fluid resuscitation [4]. Overall, albumin and saline produced similar 28-day outcomes. For the present review, SAFE is important because it directly compares two fluids with distinct physicochemical profiles: albumin increases weak acid concentration, whereas saline has a SID of zero and may promote hyperchloremic acidosis. However, SAFE was not designed to evaluate whether acid–base differences between albumin and saline mediated clinical outcomes.
The ALBIOS trial is the most relevant randomized trial for albumin in sepsis [5]. It randomized 1818 patients with severe sepsis to receive 20% albumin plus crystalloids or crystalloids alone, with the aim of maintaining serum albumin concentrations of at least 30 g/L. Albumin did not improve 28-day or 90-day survival in the overall population, although hemodynamic variables and fluid balance differed between groups. From an acid–base perspective, ALBIOS is particularly relevant because it involved hyperoncotic albumin and systematic albumin replacement, but it did not specifically evaluate Atot-mediated acidification, chloride balance, SID, or albumin-corrected acid–base variables.
The CRISTAL trial compared colloids with crystalloids in ICU patients with hypovolemic shock [50]. Because albumin was included among several colloid options, the trial cannot be interpreted as albumin-specific evidence. Nevertheless, it provides useful clinical context by showing that the choice between colloids and crystalloids cannot be reduced to a simple survival advantage. For this review, CRISTAL reinforces the need to separate clinical outcome questions from mechanistic physiological questions. The major randomized trials evaluating albumin or colloids in critical illness are summarized in Table 5.
Trials comparing balanced crystalloids with saline provide complementary evidence relevant to SID and chloride physiology. SPLIT compared Plasma-Lyte 148 with saline in ICU patients and did not show a significant reduction in acute kidney injury [30]. SMART, a larger pragmatic ICU trial, found a lower rate of major adverse kidney events with balanced crystalloids compared with saline [31]. By contrast, BaSICS and PLUS did not demonstrate clear overall survival or kidney-outcome superiority of balanced solutions over saline in broad ICU populations [33,34]. These apparently heterogeneous results do not invalidate chloride/SID physiology; rather, they suggest that measurable physicochemical effects may not consistently translate into large outcome differences across unselected trial populations.
More recently, ARISS evaluated albumin replacement in septic shock [6]. The trial reported that albumin administration appeared safe but did not improve 90-day survival; premature termination limits the certainty of conclusions. ARISS is clinically important because it directly addressed albumin replacement in septic shock, but, like previous trials, it was not designed primarily around acid–base endpoints. The major randomized trials comparing balanced crystalloids and saline are summarized in Table 6.
Overall, these trials show that predictable physiological effects do not necessarily translate into consistent mortality benefit. Albumin may modify Atot, pH, bicarbonate, base excess, and anion-gap interpretation while remaining clinically neutral at the trial level. Similarly, balanced crystalloids may reduce chloride exposure and preserve SID without producing uniform outcome benefits.
13. Future Directions
Future research should move beyond simplistic classifications of fluids as “acidifying” or “alkalinizing.” The physiological effects of albumin likely depend on dynamic interactions among Atot, SID, chloride balance, dilution, renal compensation, and tissue perfusion.
Prospective physiological studies comparing albumin 4%, albumin 20%, balanced crystalloids, and saline-based strategies using both traditional and Stewart metrics may clarify these interactions.
Integration of physicochemical analyses into future sepsis trials may also improve interpretation of arterial blood gas trajectories during resuscitation.
14. Limitations
This review has some limitations. First, many physicochemical interpretations discussed herein derive from conceptual and mechanistic models rather than from randomized physiological trials specifically designed around Stewart variables. Second, the conceptual simulations presented are illustrative and are not intended as calibrated patient-level predictions. Third, acid–base responses during sepsis are highly dynamic and influenced by renal compensation, respiratory status, vasopressor exposure, and fluid balance, factors that cannot be fully captured by simplified frameworks alone. Finally, because this is a narrative review, no systematic literature search, formal study selection process, or risk-of-bias assessment was performed; therefore, the evidence discussed should be interpreted as mechanistic and contextual rather than as a comprehensive systematic synthesis.
15. Conclusions
Albumin affects acid-base equilibrium through weak acid expansion, chloride balance, dilution, and strong ion physiology. In septic patients, particularly those with hypoalbuminemia or chloride exposure, traditional and Stewart approaches should be integrated rather than opposed. This combined interpretation may help clinicians distinguish true metabolic deterioration from predictable physicochemical changes after albumin administration.
Author Contributions
RS conceived the review. DO conceived the review, drafted the manuscript, and prepared the figures. GDR critically revised and supervised the manuscript. All authors read and approved the final manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AG | Anion gap |
| AKI | Acute kidney injury |
| Atot | Total concentration of weak acids |
| BE | Base excess |
| ICU | Intensive care unit |
| SID | Strong ion difference |
| SIG | Strong ion gap |
References
- Prescott, H.C.; Antonelli, M.; Alhazzani, W.; Møller, M.H.; Alshamsi, F.; Azevedo, L.C.P.; Belley-Cote, E.; De Waele, J.; Derde, L.; Dionne, J.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2026. Crit. Care Med. 2026, 54(4), 725–812. [Google Scholar] [CrossRef] [PubMed]
- Meyhoff, T.S.; Hjortrup, P.B.; Wetterslev, J.; Sivapalan, P.; Laake, J.H.; Cronhjort, M.; Jakob, S.M.; Cecconi, M.; Nalos, M.; Ostermann, M.; et al. Restriction of Intravenous Fluid in ICU Patients with Septic Shock. N Engl. J. Med. 2022, 386(26), 2459–2470. [Google Scholar] [CrossRef] [PubMed]
- National Heart; Lung; and Blood Institute Prevention and Early Treatment of Acute Lung Injury Clinical Trials Network; Shapiro, N.I.; Douglas, I.S.; Brower, R.G.; Brown, S.M.; Exline, M.C.; Ginde, A.A.; Gong, M.N.; Grissom, C.K.; Hayden, D.; et al. Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension. N Engl. J. Med. 2023, 388(6), 499–510. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Finfer, S.; Bellomo, R.; Boyce, N.; French, J.; Myburgh, J.; Norton, R. SAFE Study Investigators. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl. J. Med. 2004, 350(22), 2247–56. [Google Scholar] [CrossRef] [PubMed]
- Caironi, P.; Tognoni, G.; Masson, S.; Fumagalli, R.; Pesenti, A.; Romero, M.; Fanizza, C.; Caspani, L.; Faenza, S.; Grasselli, G.; et al. Albumin replacement in patients with severe sepsis or septic shock. N Engl. J. Med. 2014, 370(15), 1412–21. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Nierhaus, A.; Schumacher, U.; Utzolino, S.; Jaschinski, U.; Petros, S.; Fichtner, F.; Eimer, C.; Putensen, C.; Tanev, I.; et al. Albumin Replacement Therapy in Septic Shock: A Randomized Clinical Trial. JAMA Netw. Open 2026, 9(2), e2559297. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vincent, J.L.; De Backer, D.; Wiedermann, C.J. Fluid management in sepsis: The potential beneficial effects of albumin. J. Crit. Care 2016, 35, 161–7. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, G.J.; Martin, G.S.; Evans, T.W. Albumin: biochemical properties and therapeutic potential. Hepatology 2005, 41(6), 1211–9. [Google Scholar] [CrossRef] [PubMed]
- Caironi, P.; Gattinoni, L. The clinical use of albumin: the point of view of a specialist in intensive care. Blood Transfus. 2009, 7(4), 259–67. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Henderson, L.J. The theory of neutrality regulation in the animal organism. Am. J. Physiol.-Leg. Content 1908, 21:4, 427–448. [Google Scholar] [CrossRef]
- Hasselbalch, K.A. Die Berechnung der Wasserstoffzahl des Blutes aus der freien und gebundenen Kohlensäure desselben, und die Sauerstoffbindung des Blutes als Funktion der Wasserstoffzahl. In Julius Springer; 1916. [Google Scholar]
- Van Slyke, D.D. Acidosis and Alkalosis. Bull. N Y Acad. Med. 1934, 10(3), 103–37. [Google Scholar] [PubMed] [PubMed Central]
- Siggaard-Andersen, O. The Acid-base Status of the Blood. In Scandinavian journal of clinical and laboratory investigation: Supplementum, Suppl; Williams & Wilkins Company, 1964; Vol 70, ISSN 0085-591X. [Google Scholar]
- Astrup, P.; Jorgensen, K.; Andersen, O.S.; Engel, K. The acid-base metabolism. A new approach. Lancet 1960, 1(7133), 1035–9. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, W.B.; Cohen, J.J. The nature of the renal response to chronic disorders of acid-base equilibrium. Am. J. Med. 1978, 64(3), 417–28. [Google Scholar] [CrossRef] [PubMed]
- Stewart, P.A. Modern Quantitative Acid-Base Chemistry. Can. J. Physiol. Pharmacol. 1983, 61, 1444–1461. [Google Scholar] [CrossRef] [PubMed]
- Fencl, V.; Jabor, A.; Kazda, A.; Figge, J. Diagnosis of metabolic acid-base disturbances in critically ill patients. Am. J. Respir. Crit. Care Med. 2000, 162(6), 2246–51. [Google Scholar] [CrossRef] [PubMed]
- Figge, J.; Rossing, T. H.; Fencl, V. The Role of Serum Proteins in Acid-Based Equilibria. J. Lab. Clin. Med. 1991, 117(6), 453–467. [Google Scholar] [PubMed]
- Figge, J.; Jabor, A.; Kazda, A.; Fencl, V. Anion gap and hypoalbuminemia. Crit. Care Med. 1998, 26(11), 1807–10. [Google Scholar] [CrossRef] [PubMed]
- Handy, J.M.; Soni, N. Physiological effects of hyperchloraemia and acidosis. Br. J. Anaesth. 2008, 101(2), 141–50. [Google Scholar] [CrossRef] [PubMed]
- Kraut, J.A.; Madias, N.E. Serum anion gap: its uses and limitations in clinical medicine. Clin. J. Am. Soc. Nephrol. 2007, 2(1), 162–74. [Google Scholar] [CrossRef] [PubMed]
- Feldman, M.; Soni, N.; Dickson, B. Influence of hypoalbuminemia or hyperalbuminemia on the serum anion gap. J. Lab Clin. Med. 2005, 146(6), 317–20. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A. Closing the gap on unmeasured anions. Crit. Care 2003, 7(3), 219–20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ystgaard, O.A. Hypoalbuminemi som årsak til metabolsk alkalose [Hypoalbuminemia as a cause of metabolic alkalosis]; Tidsskr Nor Laegeforen: Norwegian, 20 Aug 1982; Volume 102, 23, pp. 1151–2. [Google Scholar] [PubMed]
- Kellum, J.A. Clinical review: reunification of acid-base physiology. Crit. Care 2005, 9(5), 500–7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Morgan, H.G. Acid-base balance in blood. Br. J. Anaesth. 1969, 41(3), 196–212. [Google Scholar] [CrossRef] [PubMed]
- Gilfix, B.M.; Bique, M.; Magder, S. A physical chemical approach to the analysis of acid-base balance in the clinical setting. J. Crit. Care 1993, 8(4), 187–97. [Google Scholar] [CrossRef] [PubMed]
- Corey, H.E. Bench-to-bedside review: Fundamental principles of acid-base physiology. Crit. Care 2005, 9(2), 184–92. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yunos, N.M.; Bellomo, R.; Hegarty, C.; Story, D.; Ho, L.; Bailey, M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney injury in critically ill adults. JAMA 2012, 308(15), 1566–72. [Google Scholar] [CrossRef] [PubMed]
- Young, P.; Bailey, M.; Beasley, R.; Henderson, S.; Mackle, D.; McArthur, C.; McGuinness, S.; Mehrtens, J.; Myburgh, J.; Psirides, A.; Reddy, S.; Bellomo, R.; SPLIT Investigators; ANZICS, C.T.G. Effect of a Buffered Crystalloid Solution vs Saline on Acute Kidney Injury Among Patients in the Intensive Care Unit: The SPLIT Randomized Clinical Trial. JAMA Erratum in: JAMA. 2015 Dec 15;314(23):2570. doi: 10.1001/jama.2015.15495. PMID: 26444692. 2015, 314(16), 1701–10. [Google Scholar] [CrossRef] [PubMed]
- Semler, M.W.; Self, W.H.; Wanderer, J.P.; Ehrenfeld, J.M.; Wang, L.; Byrne, D.W.; Stollings, J.L.; Kumar, A.B.; Hughes, C.G.; Hernandez, A.; Guillamondegui, O.D.; May, A.K.; Weavind, L.; Casey, J.D.; Siew, E.D.; Shaw, A.D.; Bernard, G.R.; Rice, T.W. SMART Investigators and the Pragmatic Critical Care Research Group. Balanced Crystalloids versus Saline in Critically Ill Adults. N Engl. J. Med. 2018, 378(9), 829–839. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Self, W.H.; Semler, M.W.; Wanderer, J.P.; Wang, L.; Byrne, D.W.; Collins, S.P.; Slovis, C.M.; Lindsell, C.J.; Ehrenfeld, J.M.; Siew, E.D.; Shaw, A.D.; Bernard, G.R.; Rice, T.W.; SALT-ED Investigators. Balanced Crystalloids versus Saline in Noncritically Ill Adults. N Engl. J. Med. 2018, 378(9), 819–828. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zampieri, F.G.; Machado, F.R.; Biondi, R.S.; Freitas, F.G.R.; Veiga, V.C.; Figueiredo, R.C.; Lovato, W.J.; Amêndola, C.P.; Serpa-Neto, A.; Paranhos, J.L.R.; Guedes, M.A.V.; Lúcio, E.A.; Oliveira-Júnior, L.C.; Lisboa, T.C.; Lacerda, F.H.; Maia, I.S.; Grion, C.M.C.; Assunção, M.S.C.; Manoel, A.L.O.; Silva-Junior, J.M.; Duarte, P.; Soares, R.M.; Miranda, T.A.; de Lima, L.M.; Gurgel, R.M.; Paisani, D.M.; Corrêa, T.D.; Azevedo, L.C.P.; Kellum, J.A.; Damiani, L.P.; Brandão da Silva, N.; Cavalcanti, A.B. BaSICS investigators and the BRICNet members. Effect of Intravenous Fluid Treatment With a Balanced Solution vs 0.9% Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial. JAMA Epub ahead of print. 2021, 326(9), 1–12. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Finfer, S.; Micallef, S.; Hammond, N.; Navarra, L.; Bellomo, R.; Billot, L.; Delaney, A.; Gallagher, M.; Gattas, D.; Li, Q.; Mackle, D.; Mysore, J.; Saxena, M.; Taylor, C.; Young, P.; Myburgh, J. PLUS Study Investigators and the Australian New Zealand Intensive Care Society Clinical Trials Group. Balanced Multielectrolyte Solution versus Saline in Critically Ill Adults. N Engl. J. Med. 2022, 386(9), 815–826. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, C.S. Regulation of renal blood flow by plasma chloride. J. Clin. Invest. 1983, 71(3), 726–35. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hatherill, M.; Waggie, Z.; Purves, L.; Reynolds, L.; Argent, A. Correction of the anion gap for albumin in order to detect occult tissue anions in shock. Arch. Dis. Child 2002, 87(6), 526–9. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pompili, E.; Zaccherini, G.; Baldassarre, M.; Iannone, G.; Caraceni, P. Albumin administration in internal medicine: A journey between effectiveness and futility. Eur. J. Intern Med. 2023, 117, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.M.; Greenslade, J.H.; Hills, A.Z.; Ray, M.T. Intervention With Concentrated Albumin for Undifferentiated Sepsis in the Emergency Department (ICARUS-ED): A Pilot Randomized Controlled Trial. Ann. Emerg. Med. 2025, 86(1), 59–69. [Google Scholar] [CrossRef] [PubMed]
- Magder, S.; Emami, A. Practical approach to physical-chemical acid-base management. Stewart at the bedside. Ann. Am. Thorac. Soc. 2015, 12(1), 111–7. [Google Scholar] [CrossRef] [PubMed]
- Bihari, S.; Bannard-Smith, J.; Bellomo, R. Albumin as a drug: its biological effects beyond volume expansion. Crit. Care Resusc. 2020, 22(3), 257–265. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- van de Wouw, J.; Joles, J.A. Albumin is an interface between blood plasma and cell membrane, and not just a sponge. Clin. Kidney J. 2021, 15(4), 624–634. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pippalapalli, J.; Lumb, A.B. The respiratory system and acid-base disorders. BJA Educ. 2023, 23(6), 221–228. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ijland, M.M.; Heunks, L.M.; van der Hoeven, J.G. Bench-to-bedside review: hypercapnic acidosis in lung injury--from 'permissive' to 'therapeutic'. Crit. Care 2010, 14(6), 237. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Magder, S. Bench-to-bedside review: ventilatory abnormalities in sepsis. Crit. Care 2009, 13(1), 202. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, T.H.; Kuo, G.; Chang, C.H.; Huang, Y.T.; Yen, C.L.; Lee, C.C.; Fan, P.C.; Chen, J.J. Diuretic effect of co-administration of furosemide and albumin in comparison to furosemide therapy alone: An updated systematic review and meta-analysis. PLoS ONE 2021, 16(12), e0260312. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Roch, A.; Guervilly, C.; Papazian, L. Fluid management in acute lung injury and ards. Ann. Intensive Care 2011, 1(1), 16. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Price, L.C.; Wort, S.J.; Finney, S.J.; Marino, P.S.; Brett, S.J. Pulmonary vascular and right ventricular dysfunction in adult critical care: current and emerging options for management: a systematic literature review. Crit. Care 2010, 14(5), R169. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kuper, M.; Gunning, M.P.; Halder, S.; Soni, N. The short-term effect of hyperoncotic albumin, given alone or with furosemide, on oxygenation in sepsis-induced acute respiratory distress syndrome. Anaesthesia 2007, 62(3), 259–63. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.S.; Pelosi, P.; Schultz, M.J.; Rocco, P.R.M.; Silva, P.L. Fluids in ARDS: more pros than cons. Intensive Care Med. Exp. 2020, 8 (Suppl 1), 32. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Annane, D.; Siami, S.; Jaber, S.; Martin, C.; Elatrous, S.; Declère, A.D.; Preiser, J.C.; Outin, H.; Troché, G.; Charpentier, C.; Trouillet, J.L.; Kimmoun, A.; Forceville, X.; Darmon, M.; Lesur, O.; Reignier, J.; Abroug, F.; Berger, P.; Clec'h, C.; Cousson, J.; Thibault, L.; Chevret, S.; CRISTAL Investigators. Effects of fluid resuscitation with colloids vs crystalloids on mortality in critically ill patients presenting with hypovolemic shock: the CRISTAL randomized trial. JAMA Erratum in: JAMA. 2013 Mar 12;311(10):1071. Régnier, Jean [corrected to Reignier, Jean]; Cle'h, Christophe [corrected to Clec'h, Christophe]. PMID: 24108515. 2013, 310(17), 1809–17. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Comparison between the traditional buffer–base interpretation and the Stewart physicochemical approach to albumin-related acid–base physiology.
Figure 1.
Comparison between the traditional buffer–base interpretation and the Stewart physicochemical approach to albumin-related acid–base physiology.

Figure 2.
Conceptual physicochemical simulations comparing albumin 20%, albumin 4%, normal saline, and lactated Ringer solution. Illustrative conceptual simulations based on simplified Stewart principles; values are intended to demonstrate directional trends rather than calibrated physiological predictions.
Figure 2.
Conceptual physicochemical simulations comparing albumin 20%, albumin 4%, normal saline, and lactated Ringer solution. Illustrative conceptual simulations based on simplified Stewart principles; values are intended to demonstrate directional trends rather than calibrated physiological predictions.

Figure 3.
Schematic representation of the “masked acidosis” concept during hypoalbuminemia and after albumin administration. Illustrative conceptual simulations based on simplified Stewart principles; values are intended to demonstrate directional trends rather than calibrated physiological predictions.
Figure 3.
Schematic representation of the “masked acidosis” concept during hypoalbuminemia and after albumin administration. Illustrative conceptual simulations based on simplified Stewart principles; values are intended to demonstrate directional trends rather than calibrated physiological predictions.

Figure 4.
Integrated bedside framework combining traditional and Stewart variables for interpretation of acid–base disorders during albumin administration in sepsis.
Figure 4.
Integrated bedside framework combining traditional and Stewart variables for interpretation of acid–base disorders during albumin administration in sepsis.

Figure 5.
Cardiorespiratory interactions during albumin administration in septic shock integrating acid–base physiology, respiratory mechanics, and hemodynamic response.
Figure 5.
Cardiorespiratory interactions during albumin administration in septic shock integrating acid–base physiology, respiratory mechanics, and hemodynamic response.


Table 1.
Comparison between traditional and Stewart approaches to albumin-related acid–base physiology.
Table 1.
Comparison between traditional and Stewart approaches to albumin-related acid–base physiology.
| Feature | Traditional approach | Stewart approach |
|---|---|---|
| Main determinant of pH | HCO₃⁻ / pCO₂ ratio | SID, Atot, pCO₂ |
| Role of albumin | Non-bicarbonate buffer | Weak non-volatile acid |
| Key variables | HCO₃⁻, BE, AG | SID, Atot, SIG |
| Hypoalbuminemia | Reduced buffering; lower measured AG | ↓ Atot → alkalinizing tendency |
| Albumin administration | Restores buffer base; may reduce BE | ↑ Atot → acidifying tendency |
| Saline acidosis | Hyperchloremic/dilutional acidosis | ↓ SID acidosis |
| Clinical strength | Simplicity and bedside familiarity | Mechanistic explanation of mixed disorders |
| Main limitation | Limited mechanistic resolution in complex ICU states | Less intuitive and more calculation-dependent |
Table 2.
Conceptual acid–base effects of common resuscitation fluids.
| Fluid | Approximate SID | Chloride load | Atot effect | Expected net pH effect |
|---|---|---|---|---|
| Normal saline | 0 | High | None | Acidifying |
| Lactated Ringer | ~28 | Moderate | None | Neutral/slightly alkalinizing |
| Albumin 4% | ~0 | Moderate-high | Mild ↑ Atot | Mild acidifying |
| Albumin 20% | ~0 | High | Strong ↑ Atot | Acidifying |
Table 3.
Representative clinical scenarios interpreted through traditional and Stewart frameworks.
| Scenario | Traditional interpretation | Stewart interpretation |
|---|---|---|
| Hypoalbuminemia + high lactate | Mild metabolic acidosis | Masked acidosis |
| Albumin infusion + ↓pH | Worsening metabolic acidosis | Restoration of Atot |
| Hyperchloremia | Hyperchloremic acidosis | ↓ SID acidosis |
| Near-normal BE with low albumin | Mild derangement | Hidden metabolic abnormality |
Table 4.
Suggested integrated bedside interpretation framework.
| Variable | Physiological meaning |
|---|---|
| pH | Overall acidemia/alkalemia |
| HCO₃⁻ | Metabolic component |
| Base excess | Buffer balance |
| Lactate | Tissue hypoperfusion, impaired clearance, or altered cellular metabolism |
| Chloride | SID effect |
| Albumin | Atot |
| Corrected anion gap | Hidden anions |
| SID | Physicochemical balance |
Table 5.
Major randomized trials evaluating albumin or colloids in critical illness.
| Trial | Year | Sample size | Population | Intervention | Comparator | Main clinical finding | Relevance to this review |
|---|---|---|---|---|---|---|---|
| SAFE | 2004 | 6997 | General ICU patients requiring fluid resuscitation | 4% albumin | Normal saline | Similar 28-day outcomes in the overall population | Largest albumin–saline comparison; acid–base physiology not primary endpoint |
| ALBIOS | 2014 | 1818 | Severe sepsis/septic shock | 20% albumin plus crystalloids targeting serum albumin ≥30 g/L | Crystalloids alone | No reduction in 28-day or 90-day mortality overall | Most relevant sepsis trial; useful context for hyperoncotic albumin |
| CRISTAL | 2013 | 2857 | ICU patients with hypovolemic shock | Colloids, including albumin | Crystalloids | No significant difference in 28-day mortality | Contextual colloid evidence; not albumin-specific |
| ARISS | 2026 | 440 | Septic shock | Albumin replacement targeting serum albumin levels | Standard fluid therapy | Albumin administration appeared safe but did not improve 90-day survival | Modern septic-shock albumin trial; acid–base endpoints not primary |
Table 6.
Major randomized trials comparing balanced crystalloids and saline.
| Trial | Year | Sample size | Population | Intervention | Comparator | Main clinical finding | Relevance to acid–base physiology |
|---|---|---|---|---|---|---|---|
| SPLIT | 2015 | 2278 | ICU patients | Plasma-Lyte 148 | Normal saline | No significant difference in AKI | Demonstrated modest chloride differences in low-volume ICU resuscitation |
| SMART | 2018 | 15,802 | Critically ill adults | Balanced crystalloids | Normal saline | Lower incidence of major adverse kidney events with balanced crystalloids | Landmark trial supporting chloride/SID relevance |
| SALT-ED | 2018 | 13,347 | Non-ICU adults treated in ED | Balanced crystalloids | Normal saline | Lower major adverse kidney events with balanced crystalloids | Extended balanced fluid findings beyond ICU |
| BaSICS | 2021 | 10,520 | Critically ill adults | Plasma-Lyte 148 | Normal saline | No overall mortality difference | Suggested physiological differences may not translate into major survival effects |
| PLUS | 2022 | 5037 | ICU patients | Plasma-Lyte 148 | Normal saline | No significant difference in AKI or mortality | Large modern ICU trial contextualizing chloride-related physiology |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



