Submitted:
25 June 2026
Posted:
26 June 2026
You are already at the latest version
Abstract
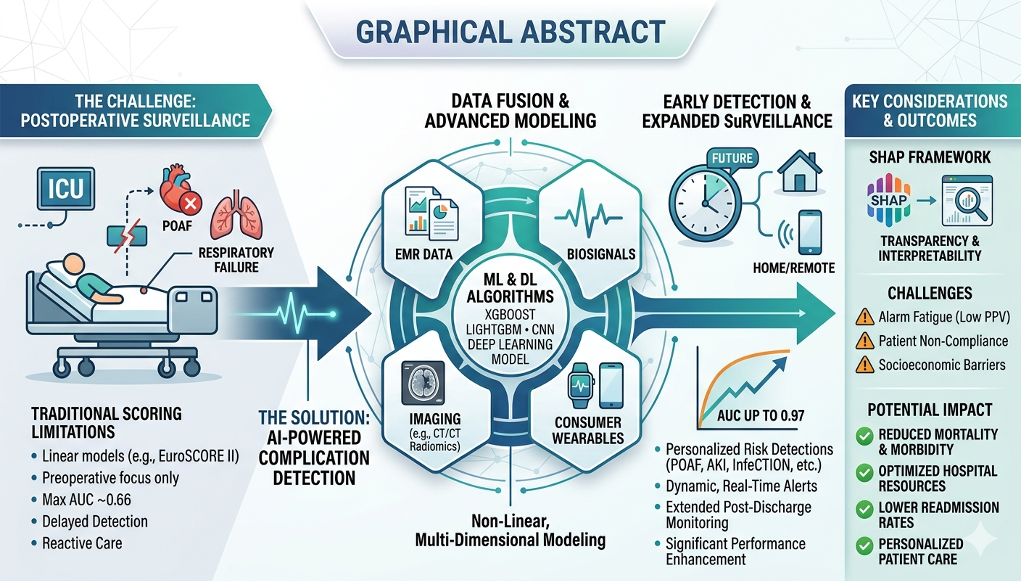
Artificial intelligence (AI) and machine learning (ML) are increasingly being evaluated as decision-support tools for forecasting postoperative complications after cardiothoracic surgery. This narrative review synthesises peer-reviewed clinical, biomedical informatics, and digital-health literature across acute kidney injury (AKI), postoperative atrial fibrillation (POAF), pulmonary complications, neurological outcomes, mortality, wound monitoring, wearable surveillance, and post-discharge monitoring. Rather than treating reported AUC values as interchangeable evidence of algorithmic superiority, this review emphasises that model performance depends on at least three interacting factors: algorithmic architecture, data richness, and validation strategy. Conventional tools such as EuroSCORE II and Society of Thoracic Surgeons (STS) models remain clinically useful because they are familiar, transparent, and externally established; however, many rely on static perioperative snapshots and are less suited to continuously updated intraoperative and postoperative data streams. Contemporary ML models, including gradient-boosting approaches, support-vector methods, convolutional neural networks, and wearable-based algorithms, may improve discrimination in selected settings, particularly when dynamic laboratory trajectories, physiological time-series, imaging data, or remote-monitoring signals are available. However, current evidence remains limited by single-centre development, heterogeneous endpoints, inconsistent calibration reporting, limited decision-curve analysis, low positive predictive values in surveillance applications, and sparse prospective implementation. Future work should prioritise multicentre external validation, calibration, clinical utility analysis, standards-based electronic medical record interoperability, and implementation pathways that preserve clinician oversight.
Keywords:
artificial intelligence
; machine learning
; deep learning
; cardiothoracic surgery
; postoperative complications
; early detection
; predictive modelling
; digital health
; medical ethics
1. Introduction
1.1. Clinical Machine Learning in Postoperative Complication Prediction
In clinical medicine, machine learning refers to computational methods that learn statistical patterns from data and generate patient-level predictions without relying solely on manually specified rules [1]. In cardiothoracic surgery, its clinical relevance is not based on the assumption that complex algorithms are intrinsically superior to conventional statistics, but on their potential to integrate heterogeneous perioperative information, including preoperative comorbidities, intraoperative haemodynamic signals, cardiopulmonary bypass variables, laboratory trajectories, imaging, operative notes, and post-discharge wearable data. This distinction is important because many postoperative complications evolve dynamically rather than being fully determined at the time of preoperative assessment.
The clinical problem is therefore twofold. First, postoperative complications such as AKI, pulmonary failure, delirium, stroke, surgical-site infection, low cardiac output syndrome, mortality, readmission, and impaired recovery impose major morbidity, mortality, cost, and resource burdens. Second, the relevant predictors often change during the operation and early recovery period. A useful AI framework must therefore be judged not only by the algorithm used, but also by whether it receives temporally appropriate data, is externally validated, is calibrated for the target population, improves clinical utility at relevant thresholds, and can be integrated into real clinical workflow.
1.2. Traditional Risk Scores
Risk-stratification models were initially developed to estimate mortality risk in cardiac surgical patients. Over time, however, the demand for predicting morbidity has increased because postoperative complications—including acute kidney injury (AKI), stroke, respiratory failure, heart failure, bleeding, and infection—significantly influence outcomes, cost, and recovery [2].
Prins et al. identified approximately 19 risk-prediction models used for open-heart surgery [2]. Widely used instruments include EuroSCORE II, Society of Thoracic Surgeons (STS) risk models, the Parsonnet score, and procedure-specific thoracic surgery models such as EuroLung. These tools remain valuable because they are familiar, transparent, externally known, and based on clinically interpretable variables. Their limitations should not be overstated as a failure of regression itself. Rather, many traditional tools are constrained by static preoperative or perioperative predictor windows, periodic recalibration requirements, procedure-specific assumptions, and historical emphasis on mortality rather than granular postoperative morbidity.
EuroSCORE II and STS models therefore provide an important clinical baseline, but they cannot fully represent continuously changing intraoperative physiology, evolving laboratory trajectories, monitor-derived time-series, wound images, or post-discharge wearable streams. This distinction is central to interpreting AI studies. Apparent gains over traditional scores may result from richer dynamic data, endpoint-specific feature engineering, or more informative monitoring windows rather than from the mathematical architecture alone. Consequently, comparisons between conventional scores and ML models should be made only within comparable endpoints, populations, predictor windows, and validation settings.
1.3. AI Applications in Cardiothoracic Surgery vs. Traditional Risk Scores
AI applications in cardiothoracic surgery should be interpreted according to the clinical data pipeline they process rather than as isolated algorithmic labels. Structured registry or electronic medical record data are usually handled by tabular ML methods such as gradient boosting, support-vector machines, random forests, or penalised regression. Imaging and wound-photograph analysis require computer-vision approaches such as convolutional neural networks. Continuous physiological monitoring and wearable-device studies rely on longitudinal time-series. The clinically relevant signal may lie in deviation from an individual patient’s baseline rather than in a single preoperative measurement. Natural language processing may be useful when operative reports, discharge summaries, or unstructured clinical notes contain information not captured in coded fields. This pipeline-based interpretation is more clinically meaningful than listing AI domains in isolation.
2. Literature Search and Synthesis Approach
This narrative review synthesised peer-reviewed literature examining AI, ML, deep learning (DL), computer vision, natural language processing, and wearable device-based monitoring for the early detection or prediction of postoperative complications after cardiothoracic surgery. The aim was not to pool effect sizes or present a systematic meta-analysis, but to map how different model architectures align with specific clinical data pipelines and to identify where current evidence remains limited by endpoint heterogeneity, data structure, validation strategy, calibration, clinical utility, and implementation feasibility.
A structured literature search was conducted using PubMed, Scopus, Web of Science, and Google Scholar for studies published between 1 January 2010 and 31 January 2026. Earlier landmark publications were also considered when they provided relevant historical or methodological context. Search terms included combinations of “artificial intelligence”, “machine learning”, “deep learning”, “cardiac surgery”, “thoracic surgery”, “cardiothoracic surgery”, “postoperative complications”, “early detection”, “risk prediction”, “wearable monitoring”, “acute kidney injury”, “postoperative atrial fibrillation”, “pulmonary complications”, “delirium”, and “surgical site infection”.
Eligible source types included peer-reviewed original model-development or validation studies, retrospective and prospective cohort studies, clinical implementation or feasibility studies, systematic reviews, meta-analyses, and established biomedical informatics or digital-health implementation papers. During screening, abstract-only records, case reports, small uncontrolled case series without model-performance data, editorials without original or methodological contribution, non-clinical engineering studies without cardiothoracic relevance, and preprint-only publications were not used as primary evidence for clinical implementation, comparative performance claims, or clinical benchmarking. Preprint-only sources were retained only when they addressed an emerging topic for which no directly equivalent peer-reviewed source was available, and they were explicitly treated as contextual evidence rather than as definitive clinical evidence.
Featured studies were selected using explicit narrative evaluation filters: (1) relevance to cardiothoracic, cardiac, thoracic, or postoperative complication prediction; (2) clear definition of the target endpoint; (3) description of model inputs, architecture, or clinical data pipeline; (4) reporting of discrimination, calibration, sensitivity, specificity, predictive values, decision-curve analysis, or another clinically interpretable performance measure; (5) internal, temporal, external, or multicentre validation strategy; and (6) relevance to implementation, workflow integration, remote monitoring, or clinical decision support. Findings were then synthesised by clinical domain, including conventional risk scoring, AKI, POAF, pulmonary complications, wound monitoring, postoperative delirium, mortality, global recovery outcomes, wearable surveillance, and post-discharge monitoring. Because this article was designed as a narrative synthesis rather than a systematic or scoping review, formal PRISMA screening, individual risk-of-bias scoring, and quantitative meta-analysis were not undertaken.
3. Principles of AI for the Clinician
AI encompasses computational techniques that enable machines to perform tasks requiring human-like cognition, including pattern recognition, learning, and decision-making. In clinical medicine, AI is predominantly applied through ML, which allows algorithms to learn from structured datasets and generate predictive models without explicit programming [5,6]. A more advanced subset, deep learning (DL), uses multilayered artificial neural networks (ANNs) capable of capturing complex, non-linear relationships within high-dimensional data such as imaging and physiological signals [6,7]. ANNs consist of interconnected processing units that adaptively learn from data inputs, improving performance with increased exposure to training datasets [6,7]. Additionally, NLP enables the extraction of clinically relevant information from unstructured data sources, including electronic health records and operative reports [7].
For clinicians, key principles include understanding model training and validation, overfitting, generalizability, and the importance of high-quality data inputs. Unlike traditional statistical approaches, AI models can incorporate large numbers of variables and continuously evolve with new data. However, they often lack transparency, necessitating careful interpretation and clinical oversight [5].
The reviewed evidence was organised according to the intended clinical use of each AI application rather than by chronology. This approach was selected because the included studies varied substantially in patient population, target complication, data source, model architecture, validation strategy, calibration reporting, and intended decision point. Accordingly, model performance estimates should be interpreted within their clinical context rather than as directly interchangeable measures of superiority. Particular caution was applied when models used dynamic postoperative data that are unavailable to conventional preoperative scores, because such comparisons reflect both data superiority and algorithmic modelling. Similarly, a model with high discrimination but poor calibration, low positive predictive value, or no demonstrated clinical utility may not be suitable for deployment.
4. AI vs Traditional Risk Scores
Traditional risk scores in cardiothoracic surgery, such as EuroSCORE II and STS models, are based on selected clinical variables and have been widely validated for perioperative risk estimation [6,7]. They remain useful at the bedside because they are transparent, familiar, externally benchmarked, and easy to communicate. Their main mathematical and practical constraints are their reliance on pre-specified variables, additive or near-linear assumptions, fixed assessment windows, periodic recalibration, and limited ability to update risk as intraoperative and postoperative physiology evolves.
AI-based models may address some of these constraints when they incorporate richer data streams or detect non-linear interactions among variables [8]. However, improved discrimination should not automatically be attributed to the algorithm alone. In several reviewed studies, performance was probably influenced by superior data acquisition, dynamic laboratory or physiological trajectories, endpoint-specific feature engineering, and validation design. AI should therefore be viewed as a complementary decision-support approach rather than a direct replacement for established risk stratification.
Pandey et al. performed a review and meta-analysis of 43 studies involving 63,847 patients to evaluate the predictive accuracy of conventional risk scores for POAF after cardiac surgery [7]. The aggregated findings indicated that traditional clinical scores provide only modest discrimination. The reported AUC values and their associated 95% CIs were as follows:
- EuroSCORE II: 0.59 (95% CI: 0.54–0.65)
- STS Score: 0.60 (95% CI: 0.56–0.63)
- Logistic EuroSCORE: 0.63 (95% CI: 0.58–0.68)
- CHADS2: 0.66 (95% CI: 0.57–0.75)
- POAF Score: 0.66 (95% CI: 0.63–0.68)
The meta-analysis demonstrated considerable diversity in diagnostic performance at specific clinical cut-offs. Sensitivity varied from 46% to 87%, while specificity ranged from 31% to 70%, reflecting low-to-moderate discrimination for POAF in the settings studied [7]. These values should not be interpreted as a universal ceiling for all conventional models or all postoperative complications, because the meta-analysis addressed a specific arrhythmic endpoint rather than AKI, pulmonary complications, mortality, delirium, recovery quality, or post-discharge events.
These findings support the rationale for exploring ML approaches, particularly models capable of incorporating non-linear relationships and dynamic perioperative variables. However, they also illustrate the danger of overgeneralisation: a POAF risk-score meta-analysis cannot be used as a direct comparator for AI models trained on different endpoints, different predictor windows, richer postoperative data, or different validation structures. Conventional regression-based models remain valuable, especially when they are well calibrated, externally validated, and applied to structured datasets with clinically selected predictors.
4.1. AI vs. Risk Scores for Specific Morbidities
Acute Kidney Injury (AKI)
Acute kidney injury is a common complication following cardiothoracic surgery and is closely linked to renal hypoperfusion, venous congestion, haemodilution, transfusion burden, nephrotoxic exposure, haemolysis, inflammatory injury, and cardiopulmonary bypass-related physiology. Traditional AKI risk models generally rely on preoperative or intraoperative summaries, whereas AI-based AKI models often gain information from postoperative creatinine, haemoglobin, urine-output, haemodynamic, and infection trajectories. Any apparent performance advantage must therefore be interpreted as a combined effect of algorithmic modelling and access to more clinically proximate dynamic data [8,9,10,14].
Kalisnik et al. evaluated Detect-A(K)I, an AI-based system designed to identify cardiac surgery-associated AKI within 12 hours after surgery [14]. The study is important less because of the headline AUC alone and more because of its vertical data architecture: baseline renal risk, operative characteristics, haemodynamic data, infection status, urine output, and early laboratory trends were combined into a time-sensitive detection pipeline.
The external cohort details reported below are taken from the original Detect-A(K)I publication and are not primary data generated by this review. They are retained only to clarify the source population and event burden. The model was developed from consecutive patients at Klinikum Nürnberg, Germany, including 7,507 patients, of whom 1,699 (22.6%) developed CSA-AKI [14]. This single-health-system setting supports technical feasibility but also underlines the need for external validation and transportability testing in centres with different bypass protocols, creatinine measurement schedules, renal-protection pathways, coding practices, and EMR structures.
The source-study cohort is summarised in Table 1.
Detect-A(K)I incorporated preoperative factors, intraoperative variables, postoperative clinical observations, and dynamic laboratory trends, especially serum creatinine and haemoglobin. This design is clinically plausible because CSA-AKI after cardiopulmonary bypass is not a single baseline-risk event; it emerges through renal hypoperfusion, haemolysis, inflammatory activation, venous congestion, and evolving postoperative haemodynamics.
The reported AUC of 0.88, sensitivity of 78.0%, specificity of 78.9%, and test accuracy of 82.1% should therefore be interpreted as performance within a dynamic early-warning pipeline rather than as proof that an algorithm alone outperforms static clinical scores [14]. For clinical deployment, such discrimination would also need to be accompanied by calibration assessment, threshold-specific utility, workflow integration, and external validation.
The model’s multidimensional input structure is shown in Figure 1.
Beyond the Detect-A(K)I model, related AI applications have also been reported across postoperative complication domains, including AKI risk prediction and dynamic early-warning models [15,16], AI-assisted wound and surgical-site monitoring [17,18,19], broader AKI prediction reviews and hybrid models [20,21], and paediatric cardiac surgery survival or low-cardiac-output risk prediction [22,23].
4.2. Postoperative Atrial Fibrillation (POAF)
POAF remains one of the most frequent complications after cardiac surgery. Conventional risk models provide modest discrimination in POAF-specific studies, but their limitations partly reflect static predictor windows and the complex interaction among atrial substrate, inflammation, autonomic tone, electrolyte shifts, cancer status, and operative stress [7,13,38]. ML approaches may improve risk stratification when they incorporate ECG-derived features, perioperative trajectories, or endpoint-specific variables, but comparisons must remain endpoint matched.
Accurate prediction of POAF is clinically important because targeted prophylaxis and monitoring may reduce downstream morbidity. However, the reviewed POAF evidence should not be used as a direct comparator for AI models addressing AKI, pulmonary complications, mortality, delirium, recovery quality, or post-discharge events. The key interpretive issue is whether the model uses clinically relevant predictors available before the decision point at which the prediction is intended to influence management.
Similar approaches have been applied to respiratory outcomes, but those models address different endpoints and therefore require separate interpretation.
4.3. Postoperative Pulmonary Complications (PPCs)
The ensemble ML framework developed by Chen et al. for the early detection of PPCs after lung cancer surgery achieved an internal validation AUC of 0.860 (95% CI: 0.809-0.911) [8]. This result supports the feasibility of explainable ML for pulmonary-risk prediction, but it should not be read as a direct 20-25% improvement over POAF-oriented conventional scores, because the endpoint, population, event prevalence, predictor set, and validation design differ.
The main contribution of Chen et al. is the combination of endpoint-specific perioperative features with SHAP-based explanation [8]. SHAP can identify which variables contribute most to an individual prediction, making the model more clinically interpretable than a black-box risk label. Its limitation is that internal validation does not guarantee performance across hospitals with different lung-resection pathways, anaesthetic protocols, coding practices, postoperative pulmonary-care bundles, and calibration requirements.
An endpoint-specific two-panel presentation is shown in Figure 2.
4.4. Paediatric Congenital Heart Surgery (CHS)
Beyond adult cardiothoracic surgery, ML approaches have also been explored in paediatric congenital heart surgery, where risk prediction is complicated by anatomical, physiological, and procedural heterogeneity.
Tong et al. evaluated ML models for major adverse outcomes after paediatric congenital heart surgery in a large retrospective cohort [9]. The study illustrates the potential of LightGBM-style modelling in a setting where anatomical complexity, age, procedure type, bypass exposure, and postoperative physiology interact non-linearly. However, the reported AUC values across LCOS, pneumonia, renal failure, and DVT should be read as endpoint-specific results within one paediatric data environment, not as a single global benchmark for cardiothoracic AI. These endpoints differ in baseline prevalence, timing, phenotype definition, and clinical consequences.
Figure 3.
Endpoint-specific AUC values reported by Tong et al. for selected paediatric postoperative complications after congenital heart surgery. The values are presented by clinical endpoint and should not be interpreted as interchangeable or directly ranked because LCOS, pneumonia, renal failure, and DVT differ in event prevalence, phenotype definition, predictor structure, and validation context [9].
Figure 3.
Endpoint-specific AUC values reported by Tong et al. for selected paediatric postoperative complications after congenital heart surgery. The values are presented by clinical endpoint and should not be interpreted as interchangeable or directly ranked because LCOS, pneumonia, renal failure, and DVT differ in event prevalence, phenotype definition, predictor structure, and validation context [9].

4.5. Delirium/Recovery/Mortality
AI models have also been evaluated for broader postoperative outcomes, including delirium, recovery quality, readmission, and mortality. These endpoints are clinically important, but direct comparison with complication-specific models is limited by differences in outcome definition, predictor timing, event prevalence, validation design, and calibration reporting. Broader peer-reviewed postoperative models have been developed to support post-discharge complication prediction, hospital readmission prediction, and mortality-risk estimation after cardiothoracic or cardiac surgery [24,26,27]. One additional preprint-only study has reported machine-learning models for adverse events after cardiac surgery, but this is treated here only as emerging contextual evidence and is not used for clinical benchmarking [25].
Guo et al. performed a systematic review and meta-analysis of 28 studies involving 80,143 patients undergoing heart surgery to assess the prediction efficacy of ML for neurological problems [28]. The investigation evaluated methods intended to identify patients at risk for postoperative delirium (POD). The meta-analysis of the validation datasets indicated that ML models attained a pooled c-index (AUC) of 0.805 (95% CI: 0.759–0.852). The aggregated data produced a sensitivity of 0.72 (95% CI: 0.65–0.79) and a specificity of 0.78 (95% CI: 0.71–0.83). Logistic regression served as the predominant baseline modelling technique, achieving a pooled c-index of 0.773; nevertheless, advanced ML algorithms exhibited significant overall discriminatory capability for the early identification of cognitive decline. Additional recent studies have extended machine-learning approaches to early delirium prediction after cardiac surgery, intraoperative biosignal-based delirium prediction, interpretable delirium prediction after lung cancer surgery, and postoperative complication prediction after pneumonectomy [29,30,31,32].
Interpretable ML has also been explored for global postoperative recovery quality. Such models are attractive because they can link patient-centred outcomes to modifiable perioperative factors such as frailty, operative duration, lactate, and ASA classification. However, recovery-quality models should be interpreted cautiously unless they have undergone peer-reviewed publication, multicentre validation, calibration assessment, and clinical utility testing in the intended pathway.
In this review, recovery-quality evidence is therefore used primarily to illustrate the type of pathophysiological feature mapping that ML can perform, rather than to establish a definitive benchmark. Elevated lactate may reflect tissue hypoperfusion, impaired oxygen delivery, or bypass-related stress; prolonged operative duration may proxy cumulative inflammatory exposure and technical complexity; and frailty may reduce physiological reserve after CPB and major thoracic trauma.
Predictive Accuracy: Where recovery models report very high AUCs, these estimates should be treated as hypothesis-generating until externally reproduced. Very high discrimination in a small or highly curated dataset may reflect local practice patterns, narrow endpoint definitions, temporal leakage, selection effects, or unrecognised calibration problems rather than generalisable clinical performance.
Principal Predictors: SHAP-style interpretation is valuable when it links model outputs to plausible biological mechanisms. In recovery modelling, predictors such as prolonged surgical duration, elevated lactate, high ASA grade, and frailty are clinically credible because they correspond to operative stress, hypoperfusion, systemic inflammation, and reduced resilience.
The SHAP feature-importance profile is shown in Figure 4.
Other interpretable or biosignal-based models have also been applied to postoperative recovery and pain prediction in surgical patients [34,35]. Sinha et al. used a UK national adult cardiac surgery database comprising 224,318 patients to develop a feature-selected XGBoost model for in-hospital and 30-day mortality [36]. Its key strength was the use of a large-scale registry and decision-curve analysis; its key limitation, shared by most registry models, is that structured variables may already represent extensive human feature selection. In such settings, ML may offer useful recalibration or interaction modelling, but the incremental gain over well-specified conventional models may be modest. In addition to raw measurements, decision curve analysis revealed that the AI demonstrated a greater net benefit up to a threshold probability of 60%, principally influenced by operation type, patient age, renal function (creatinine clearance), and procedural urgency.
Key features and performance metrics are summarised in Table 2.
Similar machine-learning approaches have also been evaluated for short-term mortality prediction after coronary artery bypass grafting [37]. In relation to POAF, cancer has also been reported as an important determinant after cardiac surgery, supporting the need for more refined postoperative risk modelling [38].
4.6. AI for Visual, Wearable, and Post-Discharge Monitoring
In addition to structured clinical and laboratory data, AI has increasingly been applied to visual and continuous physiological data streams. These approaches are particularly relevant after discharge, when direct clinical observation is limited and complications may evolve outside the hospital environment.
To identify early surgical site infections in patients recovering from cardiothoracic surgery, Pereira et al. created and assessed an artificial intelligence-based image analysis system [17]. In addition to detecting and localising wound sites, the system uses a deep learning segmentation model (MobileNet-UNet) to categorise wound types into chest, drain, and leg categories. The presence of wound modifications for each type of wound was then predicted using ML methods, such as random forest, support vector machine, and k-nearest neighbours. Using wound-specific models instead of a single generalised classifier improved classification performance much more.
The wound-analysis workflow and classifier performance are shown in Figure 5.
The MobileNet-UNet model achieved a Mean Intersection over Union (mIoU) of 0.887 in the first segmentation phase of the image analysis system, showing promising segmentation performance for surgical wound localisation across different anatomical sites. The researchers discovered that wound-specific models performed noticeably better than a single global classifier in the following categorization of wound modifications, especially for complex drain and leg wounds. With an accuracy of 91.1% for chest wounds and 89.5% for leg wounds, the Random Forest (RF) classifier proved to be the most reliable of the ML architectures examined.
The method showed promising performance in detecting early indicators of inflammation and dehiscence, which are essential precursors to deep surgical site infections (SSIs). The method employed specialised models for distinct wound types, reducing the ‘noise’ linked to diverse healing patterns and delivering a more tailored diagnostic output for postoperative monitoring.
Beqari et al. evaluated, using a Fitbit watch, whether a machine-learning algorithm, NightSignal, could detect postoperative complications after cardiothoracic surgery [10]. In this pilot study a total of 56 patients were included in the cohort, 24 patients underwent thoracic surgery (42.9%) and 32 patients (57.1%) underwent cardiac surgery. The most common thoracic surgery was a lobectomy n=13 (54.2%), and valve replacement was the most common cardiac surgery procedure, n=14 (43.8%).
The study participants wore the Fitbit watch continuously for at least 1 week preoperatively and up to 90 days postoperatively. Of the total 56 patient cohort, 20 patients (37.5%) experienced postoperative complications, during the 90-day postoperative period.
The NightSignal algorithm detected 17 out of 21 (81%) postoperative complications. Of these 17 postoperative detections, 15 (88.2%) were detected early before the postoperative complication date, and 2 events were detected after the postoperative complication date. This was due to these 2 patients intermittently wearing their Fitbit device during the postoperative event. The NightSignal algorithm had 81% sensitivity and 75% specificity, with a negative predictive value of 97% and a positive predictive value of 28%.
Post-discharge prediction is a harder deployment problem than ICU-based early warning. Santos et al. assessed a clinical decision-support system for serious events within 90 days after discharge from a cardiothoracic surgery department [24]. In a dataset of 5,045 patients, the model achieved an AUC of 0.695 on randomised testing and 0.653 on temporal testing. The drop under temporal validation is clinically important: it shows that performance may degrade when tested in a later time period and therefore provides a more realistic estimate of deployment robustness than random splitting alone. This type of temporal validation is especially relevant for implementation because clinical practice, coding behaviour, discharge thresholds, and follow-up pathways change over time.
The post-discharge decision-support workflow is shown in Figure 8.
4.7. Overall Evidence Summary
Table 3 and Figure 9 summarise the main studies discussed in this review using a critical comparative framework. Because the studies differed in clinical setting, endpoint, event prevalence, sample size, input data, validation strategy, calibration reporting, and intended decision point, performance metrics should not be interpreted as a direct ranking of model quality. The most clinically relevant comparison is not simply AUC versus AUC, but whether each model used an appropriate data pipeline for its target complication, whether it was validated beyond the development setting, whether its predicted risks were calibrated, and whether it can be integrated into real clinical workflow.
5. Clinical Implications and Implementation Challenges
The integration of AI into cardiothoracic surgery has important clinical implications. Improved risk stratification can support personalized patient counseling, optimize surgical planning, and enhance perioperative management. AI-driven models may assist clinicians in identifying high-risk patients, enabling proactive interventions and more efficient resource allocation [14]. However, successful implementation requires robust validation, integration into clinical workflows, and careful consideration of ethical issues such as data privacy, bias, and accountability. Importantly, AI should function as a decision-support tool, with clinicians maintaining ultimate responsibility for patient care.
5.1. Mathematical and Pathophysiological Limitations of Conventional Scoring Systems
The principal problem in postoperative cardiothoracic care has historically been the restricted ability of static, point-based clinical scores to update risk as physiology changes. Pandey et al. showed modest discrimination of traditional instruments for POAF, but this should be interpreted as a POAF-specific finding rather than a universal performance ceiling for all conventional modelling [7]. Sinha et al. further illustrated that conventional EuroSCORE measurements may over-calibrate or exaggerate mortality risk in contemporary adult cardiac surgery populations [36].
The biological reason complex models may help is that cardiothoracic complications often arise from non-linear interactions. During cardiopulmonary bypass, ischemia-reperfusion injury, haemodilution, non-pulsatile flow, oxidative stress, complement activation, cytokine release, endothelial dysfunction, venous congestion, transfusion exposure, and haemodynamic instability can converge into systemic inflammatory response syndrome (SIRS) and organ injury. A modestly prolonged bypass duration may be tolerated by one patient but become clinically decisive in another patient with baseline renal dysfunction, low cardiac reserve, frailty, anaemia, elevated lactate, or limited physiological reserve. These interactions are not well represented when risk factors are treated as independent additive components.
The ML architectures examined in this review may capture these interactions when they are supplied with appropriate inputs. Decision-tree ensembles such as XGBoost and LightGBM can model threshold effects and variable interactions in structured EMR data; CNNs can extract spatial features from wound images; and time-series or wearable algorithms can learn deviations from each patient’s baseline physiology. This is not evidence that complex ML is always superior. It means that the architecture should match the data pipeline, pathophysiology, timing, and intended clinical action for the target complication.
5.2. Structured Versus High-Dimensional Data
A central unresolved question is whether ML adds substantial value when applied to structured registry datasets composed of already selected clinical variables. In such datasets, much of the feature-selection process has already been performed by clinicians, registry designers, and coding systems. Consequently, ML may provide only incremental gains over well-specified and recalibrated regression models. The potential advantage of AI is likely greater when applied to genuinely high-dimensional or minimally processed data, including medical imaging, wound photographs, continuous physiological time-series, wearable-device streams, natural language extracted from clinical notes, and omics or multi-omics datasets. This distinction helps explain why some tabular ML models show modest improvements, whereas computer-vision and longitudinal monitoring pipelines may open genuinely new surveillance opportunities.
5.3. Transitioning from the ICU to the Home: Redefining the Spatiotemporal Boundaries of Surveillance
A significant similarity across the analysed research is the proliferation of AI surveillance throughout time and place, extending well beyond the closely controlled ICU environment. Historically, the danger of overlooking dynamic physiological changes post-surgery significantly escalated once patients exited active care or were discharged home. The incorporation of continuous data streams is actively transforming this proactive care timeline: [10,11,12,13,17,24]
Real-Time Acute Inpatient Monitoring: During the immediate postoperative phase, modest physiological changes frequently occur before evident clinical failure. Kalisnik et al. demonstrate that ML can analyse real-time hospital data streams to provide earlier alerts for AKI in the evaluated setting [14]. Through the analysis of continuous inputs instead of relying on daily morning laboratory draws; AI can detect little decreases in urine output or minor increases in serum creatinine several hours prior to a human clinician’s normal observation of changes on a chart.
Continuous Outpatient Remote Monitoring: Beqari et al. evaluated whether a Fitbit-based machine-learning algorithm, NightSignal, could detect postoperative complications after cardiothoracic surgery [10]. The study demonstrates that continuous biometric loops can establish an outpatient safety net by successfully identifying 81% of events, with 88.2% of these detections occurring prior to clinical diagnosis. This addresses the critical interval between hospital release and the customary two-week follow-up appointment.
Algorithmic Resource Optimization: This remote continuous technique is in complete alignment with the clinical decision support system suggested by Santos et al. [24]. Acknowledging the insufficient staff in hospitals to closely follow each discharged patient, their gradient boosting model focused on high-risk individuals for remote oversight. This enabled doctors to prioritise remote care according to real-time assessed risk instead of arbitrary scheduling, so optimizing hospital resources while supporting patient safety.
Additionally, image analysis applications, exemplified by the Convolutional Neural Network (CNN) developed by Pereira et al., demonstrate that AI can be trained to detect early wound changes and surgical site infections by analysing photographs of surgical incisions captured by patients at home using smartphones [17]. Collectively, these studies illustrate a comprehensive, hybrid AI care model that encompasses the patient from the moment they leave the operating room to many months post-discharge.
5.4. Addressing the “Black Box” Conundrum Through Explainable AI
The clinical application of advanced AI in medicine has been hindered by the opaque nature of deep learning and complex ensemble models. In high-stakes cardiothoracic surgery, clinicians are unlikely to act on an alert unless the prediction can be reconciled with physiological reasoning, the patient’s clinical trajectory, and the proposed intervention. Interpretability is therefore not a cosmetic addition; it is central to safe implementation, clinical accountability, regulatory acceptance, and trust.
This review emphasises a necessary transition toward explainable AI (XAI). Chen et al. and recovery-quality modelling studies used SHAP-style explanations to decompose predictions into feature-level contributions [8,33]. SHAP is useful only when interpreted clinically: variables such as bypass duration, operative time, lactate, creatinine clearance, frailty, and oxygenation are not abstract mathematical inputs; they are proxies for inflammatory burden, hypoperfusion, renal reserve, respiratory vulnerability, and physiological resilience. XAI therefore bridges model output and bedside reasoning, but it does not replace external validation, calibration, decision-curve analysis, or clinician accountability.
5.5. Assessing Algorithmic Diversity: XGBoost, LightGBM, and Convolutional Neural Networks
A key insight from synthesising these studies is that there is no universal AI strategy for cardiothoracic complications; the model architecture should be selected according to the data stream, clinical endpoint, validation environment, and deployment setting.
Gradient Boosting (XGBoost and LightGBM): These models are best suited to structured tabular EMR or registry data, including demographics, comorbidities, procedure type, bypass duration, laboratory values, haemodynamics, and medication exposure [8,9,36]. Their advantage is not algorithmic superiority by default, but their ability to model interactions and thresholds in data that are already clinically structured. Their weakness is that, when the input data are heavily preselected registry variables, their incremental gain over well-calibrated logistic regression may be modest.
Support Vector Machines (SVMs) and Ensemble Models: These approaches may perform well in smaller or moderately dimensional datasets where the aim is to separate complex clinical phenotypes, such as delirium-risk groups [28]. Their clinical value depends on careful validation and transparent reporting, because high discrimination in a small curated dataset can reflect overfitting, endpoint definition, or local practice patterns.
Convolutional Neural Networks (CNNs), Time-Series Models, and Wearable Algorithms: CNNs are appropriate when the input is visual, such as surgical wound photographs, because they learn spatial features including erythema, drainage, dehiscence, and wound-edge change [17]. Wearable algorithms and time-series models are more suitable for longitudinal physiological streams, where deviations from a patient’s baseline heart rate, sleep, activity, oxygenation, and recovery trajectory may precede clinical deterioration [10,11,24]. The central principle is pipeline matching: images require computer vision, continuous signals require temporal modelling, unstructured text requires natural language processing, and structured registries require calibrated tabular models.
5.6. Addressing Vulnerabilities and Implementation Obstacles
Notwithstanding the achievements outlined in these studies, transitioning AI from retrospective research cohorts to active clinical workflows requires resolution of several persistent challenges [11,13,24].
The False Positive Dilemma and Alarm Fatigue: In the wearable study conducted by Beqari et al., the algorithm had a high NPV of 97%, making it potentially useful for ruling out complications, but its PPV was only 28% [10]. This means that most positive alerts would not correspond to confirmed complications. If deployed at scale without careful triage logic, escalation thresholds, calibration monitoring, and clinical governance, such systems could increase alarm fatigue and reduce clinician trust.
Patient Adherence and Socioeconomic Obstacles: The effectiveness of remote monitoring systems is contingent upon human behaviour and equitable access. In the NightSignal study, two postoperative events were detected late in association with intermittent Fitbit wear [10]. Dependence on smartphones, wearable devices, home internet access, and digital literacy may therefore widen rather than reduce disparities unless implementation strategies include device provision, patient education, technical support, and non-digital fallback pathways.
EMR Interoperability Blocks: Real-time deployment requires much more than a validated model file. A bedside early-warning system must extract structured variables from the EMR, map local laboratory and medication codes to standard terminologies, ingest monitor and wearable data, run inference with low latency, return explanations inside the clinician’s workflow, and log actions for audit. Hospitals differ in vendor systems, HL7/FHIR readiness, data dictionaries, alert-routing rules, cybersecurity constraints, procurement processes, and governance approvals. Without standards-based interfaces such as SMART on FHIR, prospective monitoring, and local recalibration, a model that performs well offline may fail at the point of care because the required variables are unavailable, delayed, inconsistently coded, or not displayed in an actionable format [11,43].
Calibration and Clinical Utility: AUC is useful for discrimination, but it does not indicate whether predicted risks are numerically reliable, whether treatment thresholds are clinically sensible, or whether the model improves outcomes. A poorly calibrated model may overestimate risk in one hospital and underestimate it in another, leading to unnecessary interventions in some patients and missed deterioration in others. Future AI studies should therefore report calibration plots, calibration-in-the-large, decision-curve analysis, threshold-specific predictive values, and workflow consequences in addition to AUC. Clinical usefulness depends on whether the model changes decisions safely, not simply whether it separates patients with and without events in a retrospective dataset.
Data Heterogeneity, Generalizability, and Publication Bias: Meta-analyses and implementation studies highlight that AI models developed in one hospital may perform poorly in another hospital with different patients, coding practices, laboratory schedules, bypass protocols, perioperative pathways, and EMR configurations [7,28]. In addition, reported performance may be inflated by positive publication bias: failed institutional models, poorly calibrated tools, negative studies, and clinically unusable pilots are much less likely to appear in the literature than successful high-AUC studies. This means that published AUCs probably overestimate real-world deployment performance unless negative results, calibration failures, implementation failures, and external validations are reported with equal transparency.
5.7. Future Directions
Future research must prioritise prospective, multicentre validation and pragmatic implementation studies over retrospective database analysis alone. Standardised data inputs across hospital EMR systems are essential to support interoperability for these algorithms. The implementation of continuous wearable algorithms and structured EMR prediction models may reduce readmission rates and improve resource allocation only if they are calibrated, clinically useful at relevant thresholds, integrated into workflow without increasing avoidable staff burden, and evaluated against meaningful patient-centred outcomes [11,13,24,43].
5.8. Ethical, Legal, and Socioeconomic Considerations
As predictive AI and remote wearable monitoring transition from research cohorts to active cardiothoracic workflows, they present a complex array of ethical and regulatory problems that remain unstandardized in medicine. The primary concern relates to clinical accountability and the medicolegal framework of algorithmic decision-making. When an algorithm fails to detect a significant problem, or when a surgeon ignores a precise AI alarm leading to patient suffering, the parameters of medical negligence become unclear. Current legal frameworks are based on human-to-human medical decisions, leading to ambiguity concerning accountability among the operating surgeon, the healthcare facility, or the data scientists who created the algorithm [39]. Conventional negligence standards are also challenged by AI systems that lack sentience and autonomous culpability, as highlighted in recent clinical liability discussions [40].
The integration of these tools may further intensify socioeconomic disparities in healthcare. Many continuous outpatient monitoring systems rely heavily on patients having modern telephones, wearable devices, stable internet connection, and sufficient digital literacy. The shift to AI-assisted discharge presents a substantial barrier to fair care for vulnerable, low-income, or elderly groups. For these tools to improve cardiothoracic care equitably, healthcare systems must ensure that algorithmic safety nets are accessible to all patients, regardless of socioeconomic status or digital literacy, a substantial real-world translational challenge highlighted in recent thoracic surgery AI literature [41].
Thoracic surgery risk-prediction tools such as Predicthor further illustrate the growing movement toward AI-powered 30-day mortality and complication prediction, reinforcing the need for external validation and careful clinical governance before routine deployment [42].
6. Conclusions
AI represents an important but still immature advance in postoperative risk prediction within cardiothoracic surgery. Its greatest promise lies not in replacing conventional scores, but in extending them with dynamic perioperative data, imaging, physiological time-series, and post-discharge monitoring. The evidence reviewed here suggests that ML may improve discrimination in selected settings, especially for AKI, PPCs, wound monitoring, and remote surveillance, but reported gains must be interpreted through the lens of data richness, endpoint definition, calibration, validation, clinical utility, and implementation feasibility. Future work should focus on peer-reviewed prospective validation, transparent reporting of failed as well as successful models, interoperable EMR deployment, and hybrid systems that preserve clinician oversight while using AI to highlight evolving risk earlier than static tools can.
Author Contributions
Conceptualization, G.P.G.; methodology, A.F. and G.P.G.; validation, G.P.G.; formal analysis, G.P.G. and F.T.; investigation, G.P.G., P.G., A.F., F.T., A.G. and K.L. and N.I.; resources, A.F. and G.P.G.; data curation, A.F., A.K., and S.K.; writing—original draft preparation, A.F.; writing—review and editing, G.P.G., S.K., A.K., F.T., A.G., P.G. and K.L and N.I.; visualization, A.F.; supervision, F.T. and G.P.G.; G.P.G. and A.F. contributed equally to this paper and share joint first authorship. All authors have read and agreed to the published version of the manuscript and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analysed in this study. Data sharing is not applicable to this article. All information discussed in this review is available from the cited published literature.
Acknowledgments
During the preparation of this manuscript, the authors used GenAI tools (OpenAI ChatGPT) for structural organisation and figure-generation support. The authors reviewed and edited all outputs and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AI | Artificial intelligence |
| ML | Machine learning |
| DL | Deep learning |
| AUC | Area under the curve |
| AKI | Acute kidney injury |
| POAF | Postoperative atrial fibrillation |
| PPCs | Postoperative pulmonary complications |
| ICU | Intensive care unit |
| SHAP | Shapley Additive Explanations |
| XGBoost | Extreme Gradient Boosting |
References
- Rajkomar, A.; Dean, J.; Kohane, I.S. Machine Learning in Medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef] [PubMed]
- Prins, C.; de Villiers Jonker, I.; Smit, F.E.; Botes, L. Cardiac surgery risk-stratification models. Cardiovasc. J. Afr. 2012, 23, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Georghiou, G.P.; Georghiou, P.; Georgiou, A.; Triposkiadis, F. Cardiac Surgery and Postoperative Atrial Fibrillation: The Role of Cancer. Medicina 2025, 61, 1815. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Xue, B.; Kannampallil, T.; Lu, C.; Abraham, J. A Novel Generative Multi-Task Representation Learning Approach for Predicting Postoperative Complications in Cardiac Surgery Patients. J. Am. Med. Inform. Assoc. 2025, 32(3), 459–469. [Google Scholar] [PubMed]
- Zhu, S.; Che, H.; Fan, Y.; Jiang, S. Application of Algorithms to Predict New-Onset Postoperative Atrial Fibrillation and Identify Risk Factors Following Isolated Valve Surgery. Heart Surg. Forum 2023, 26(3), 255–263. [Google Scholar] [CrossRef]
- Liu, Z.; Zheng, C.; Jia, Z.; Zhao, C.; Liu, X.; Shao, W.; Guo, H. Deep Learning Radiomics Model of Epicardial Adipose Tissue for Predicting Postoperative Atrial Fibrillation after Lung Lobectomy in Lung Cancer Patients. Front. Oncol. 2025, 15, 1623248. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Okaj, I.; Ichhpuniani, S.; Tao, B.; Kaur, H.; Spence, J.D.; Young, J.; Healey, J.S.; Devereaux, P.J.; Um, K.J.; et al. Risk scores for prediction of postoperative atrial fibrillation after cardiac surgery: a systematic review and meta-analysis. Am. J. Cardiol. 2023, 209, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Deng, T.; Yang, Q.; Li, J.; Shen, J.; Luo, X.; Tang, J.; Zhang, X.; Salvador, J.T.; Ma, J. Development and validation of an explainable machine learning model for predicting postoperative pulmonary complications after lung cancer surgery: a machine learning study. eClinicalMedicine 2025, 86, 103386. [Google Scholar] [CrossRef] [PubMed]
- Tong, C.; Du, X.; Chen, Y.; Zhang, K.; Shan, M.; Shen, Z.; Zhang, H.; Zheng, J. Machine learning prediction model of major adverse outcomes after pediatric congenital heart surgery: a retrospective cohort study. Int. J. Surg. 2024, 110, 2207–2216. [Google Scholar] [CrossRef] [PubMed]
- Beqari, J.; Powell, J.R.; Hurd, J.; Potter, A.L.; McCarthy, M.L.; Srinivasan, D.; Wang, D.; Cranor, J.; Zhang, L.; Webster, K.; et al. A pilot study using machine-learning algorithms and wearable technology for the early detection of postoperative complications after cardiothoracic surgery. Ann. Surg. 2025, 281, 514–521. [Google Scholar] [PubMed]
- Smuck, M.; Odonkor, C.A.; Wilt, J.K.; Schmidt, N.; Swiernik, M.A. The emerging clinical role of wearables: factors for successful implementation in healthcare. npj Digit. Med. 2021, 4, 45. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Li, Y.; Wang, P.; Chen, L.; Liu, K. Exploring the assessment of post-cardiac valve surgery pulmonary complication risks through the integration of wearable continuous physiological and clinical data. BMC Med. Inform. Decis. Mak. 2025, 25, 12. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Graham, M.M.; Shrivastav, R.; Thompson, D.R.; Gallagher, R.; Polat, H. Use of wearable devices to monitor post-operative activity following cardiac surgery: a systematic scoping review. Eur. J. Cardiovasc. Nurs. 2024, 23, 697–705. [Google Scholar] [CrossRef]
- Kalisnik, J.M.; Bauer, A.; Vogt, F.A.; Stickl, F.J.; Zibert, J.; Fittkau, M.; Bertsch, T.; Kounev, S.; Fischlein, T. Artificial intelligence-based early detection of acute kidney injury after cardiac surgery. Eur. J. Cardiothorac. Surg. 2022, 62, Ezac289. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, J.; Branco, T.; Lopes, J.A. Artificial intelligence in acute kidney injury risk prediction. J. Clin. Med. 2020, 9, 678. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.T.; Zeng, Z.; Chatterjee, S.; Wall, M.J.; Moon, M.R.; Coselli, J.S.; Rosengart, T.K.; Li, M.; Ghanta, R.K. Machine learning for dynamic and early prediction of acute kidney injury after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2023, 165, 1083–1093. [Google Scholar]
- Pereira, C.; Guede-Fernández, F.; Vigário, R.; Coelho, P.; Fragata, J.; Londral, A. Image Analysis System for Early Detection of Cardiothoracic Surgery Wound Alterations Based on Artificial Intelligence Models. Appl. Sci. 2023, 13, 2120. [Google Scholar] [CrossRef]
- Tanner, J.; Rochon, M.; Harris, R.; Beckhelling, J.; Jurkiewicz, J.; Mason, L.; Bouttell, J.; Bolton, S.; Dummer, J.; Wilson, K.; et al. Digital wound monitoring with artificial intelligence to prioritise surgical wounds in cardiac surgery patients for priority or standard review: protocol for a randomised feasibility trial (WISDOM). BMJ Open 2024, 14, e086486. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, R.R.; Schneider, G.; Bikorimana, L.; Rukundo, G.; Niyigena, A.; Miranda, E.; Riviello, R.; Kateera, F.; Hedt-Gauthier, B. The Use of Mobile Thermal Imaging and Deep Learning for Prediction of Surgical Site Infection. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Virtual, 1–5 November 2021; pp. 5059–5062. [Google Scholar]
- Aftab, R. A.; Butt, Z. A.; Ibrahim, B.; Kun, L. S. Machine Learning for the Prediction of Acute Kidney Injury Post Cardiac Surgery: A Systematic Review and Meta-Analysis. BMC Medical Informatics and Decision Making 2026. [Google Scholar]
- Petrosyan, Y.; Mesana, T. G.; Sun, L. Y. Prediction of Acute Kidney Injury Risk after Cardiac Surgery: Using a Hybrid Machine Learning Algorithm. BMC Med. Inform. Decis. Mak. 2022, 22(1), 137. [Google Scholar] [CrossRef] [PubMed]
- Zürn, C.; Hübner, D.; Ziesenitz, V.C.; Höhn, R.; Schuler, L.; Schlange, T.; Gorenflo, M.; Kari, F.A.; Kroll, J.; Loukanov, T.; et al. Model-Driven Survival Prediction after Congenital Heart Surgery. Interdiscip. Cardiovasc. Thorac. Surg. 2023, 37, 3. [Google Scholar] [CrossRef]
- Tong, C.; Du, X.; Zhang, K.; Shan, M.; Zhang, H.; Zheng, J. Daytime Variation of In-Hospital Mortality and Low Cardiac Output Syndrome after Pediatric Cardiac Surgery-a Retrospective Cohort Study. Ann. Med. 2024, 56(1). [Google Scholar] [CrossRef] [PubMed]
- Santos, R.; Ribeiro, B.; Sousa, I.; Santos, J.; Guede-Fernández, F.; Dias, P.; Carreiro, A.V.; Gamboa, H.; Coelho, P.; Fragata, J.; et al. Predicting Post-Discharge Complications in Cardiothoracic Surgery: A Clinical Decision Support System to Optimize Remote Patient Monitoring Resources. Int. J. Med. Inform. 2024, 182, 105307. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.; Amal, S.; Rabb, J.B.; Mazhude, F.; Shivandi, V.; Kramer, R.S.; Sawyer, D.B.; Winslow, R.L. Development and validation of machine learning models for adverse events after cardiac surgery. medRxiv [Preprint] 2025, 2025.02.24.25322811. [Google Scholar] [PubMed]
- Sherman, E.; Alejo, D.; Wood-Doughty, Z.; Sussman, M.; Schena, S.; Ong, C.S.; Etchill, E.; DiNatale, J.; Ahmidi, N.; Shpitser, I.; et al. Leveraging machine learning to predict 30-day hospital readmission after cardiac surgery. Ann. Thorac. Surg. 2022, 114, 2173–2179. [Google Scholar] [CrossRef] [PubMed]
- Benedetto, U.; Dimagli, A.; Sinha, S.; Cocomello, L.; Gibbison, B.; Caputo, M.; Gaunt, T.; Lyon, M.; Holmes, C.; Angelini, G. D. Machine Learning Improves Mortality Risk Prediction after Cardiac Surgery: Systematic Review and Meta-Analysis. J. Thorac. Cardiovasc. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Xu, H.; Wang, A.; Zhang, M.; Zhang, S.; Xie, P. The Predictive Value of Machine Learning for Postoperative Delirium in Cardiac Surgery: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2026, 28, e72304–e72304. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Wang, Y.; Li, H.; Zang, Q.; Huang, J.; Zhang, Y.; Wu, J.; Liu, L.; Xing, Z.; Yu, Y. Early Prediction of Delirium in Postcardiac Surgery Patients: Machine Learning Model Development and External Validation. JMIR Med. Inform. 2026, 14, e73283. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Kim, H. I.; Soh, S.; Choi, J. W.; Song, J. W.; Yoon, D. Machine Learning with Clinical and Intraoperative Biosignal Data for Predicting Postoperative Delirium after Cardiac Surgery. iScience 2024, 27(6), 109932. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liang, R.; Yang, J.-J.; Zhou, C.-M. Predicting Postoperative Delirium after Lung Cancer Resection: The Utility of Synthetic Data and LIME Algorithm for Model Interpretation. Sci. Rep. 2026, 16(1). [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xie, S.; Liu, J.; Wang, H.; Yu, J.; Li, W.; Guan, A.; Xu, S.; Cui, Y.; Tan, W. Predicting Postoperative Complications after Pneumonectomy Using Machine Learning: A 10-Year Study. Ann. Med. 2025, 57(1), 2487636. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Ma, B.; Xing, Z.; Wang, Y.; Tian, S.; Zhang, Z.; Zhang, J. An interpretable machine-learning model for predicting postoperative recovery quality after cardiovascular surgery: Development, validation, and clinical applicability. medRxiv [Preprint] 2025. [Google Scholar] [CrossRef] [PubMed]
- Hua, C.; Chu, Y.; Zhou, M.; Ye, J.; Xu, X. Predictive Effect of Postoperative Recovery in General Anesthesia Patients Using Interpretable Models Based on Swarm Intelligence Machine Learning. Front. Physiol. 2025, 16, 1565548. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Lee, D.; Kang, M.; Oh, C.; Park, S.; Park, J.; Hong, B. Predictive Machine Learning for Postoperative Pain Using Biosignals: A Retrospective Observational Study. BMC Med. Inform. Decis. Mak. 2026, 26(1), 20. [Google Scholar] [PubMed]
- Sinha, S.; Dong, T.; Dimagli, A.; Judge, A.; Angelini, G. D. A Machine Learning Algorithm-Based Risk Prediction Score for In-Hospital/30-Day Mortality after Adult Cardiac Surgery. Eur. J. Cardio-Thorac. Surg. 2024, 66(4), ezae368. [Google Scholar] [CrossRef]
- Salikhanov, I.; Roth, V.; Gahl, B.; Reid, G.; Kolb, R.; Dimanski, D.; Berdajs, D. Machine Learning-Based Prediction of Short-Term Mortality after Coronary Artery Bypass Grafting: A Retrospective Cohort Study. Biomedicines 2025, 13(8), 2023. [Google Scholar] [CrossRef] [PubMed]
- Georghiou, G.P.; Xanthopoulos, A.; Kanellopoulos, G.; Georghiou, P.; Georgiou, A.; Skoularigis, J.; Giamouzis, G.; Lampropoulos, K.; Patrikios, I.; Triposkiadis, F. Cancer Is a Major Determinant of Postoperative Atrial Fibrillation After Cardiac Surgery. J. Clin. Med. 2025, 14, 2117. [Google Scholar] [CrossRef] [PubMed]
- De Micco, Francesco; Grassi, S.; Tomassini, L.; Di Palma, Gianmarco; Ricchezze, Giulia; Scendoni, R. Robotics and AI into Healthcare from the Perspective of European Regulation: Who Is Responsible for Medical Malpractice? Front. Med. 2024, 11. [Google Scholar] [CrossRef]
- Kellar, R. AI in Healthcare: Redefining Liability for Doctors and Hospitals. Br. J. Hosp. Med. 2025, 1–6. [Google Scholar] [CrossRef]
- Gritsiuta, A. I.; Su, S.; Petrov, R. V. Navigating the Challenges of Artificial Intelligence Integration in Thoracic Surgery. Curr. Chall. Thorac. Surg. 2025, 7, 31–31. [Google Scholar] [CrossRef] [PubMed]
- Durand, X.; Hédou, J.; Bellan, G.; Thomas, P. A.; Pages, P. B.; D’Journo, X. B.; Baste, J. M. Predicthor: AI-powered predictive risk model for 30-day mortality and 30-day complications in patients undergoing thoracic surgery for lung cancer. Ann. Surg. Open 2025, 6(2), e578. [Google Scholar] [CrossRef] [PubMed]
- Mandel, J.C.; Kreda, D.A.; Mandl, K.D.; Kohane, I.S.; Ramoni, R.B. SMART on FHIR: a standards-based, interoperable apps platform for electronic health records. J. Am. Med. Inform. Assoc. 2016, 23, 899–908. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Multidimensional data integration for the Detect-A(K)I model development. The schematic illustrates the distinct vertical layers of input data—preoperative factors, intraoperative variables, postoperative clinical data, and dynamic laboratory trends—and their conversion by the AI model to achieve a predictive AUC of 0.88 for CSA-AKI within 12 hours [14].
Figure 1.
Multidimensional data integration for the Detect-A(K)I model development. The schematic illustrates the distinct vertical layers of input data—preoperative factors, intraoperative variables, postoperative clinical data, and dynamic laboratory trends—and their conversion by the AI model to achieve a predictive AUC of 0.88 for CSA-AKI within 12 hours [14].

Figure 2.
Endpoint-specific presentation of reported AUC values from POAF-oriented conventional risk scores and an internally validated ML model for postoperative pulmonary complications after lung cancer surgery. The two panels are separated because the values arise from different clinical endpoints, patient populations, predictor windows, event prevalences, and validation settings. Values are shown for orientation only and should not be interpreted as a head-to-head comparison or as evidence of universal algorithmic superiority [7,8].
Figure 2.
Endpoint-specific presentation of reported AUC values from POAF-oriented conventional risk scores and an internally validated ML model for postoperative pulmonary complications after lung cancer surgery. The two panels are separated because the values arise from different clinical endpoints, patient populations, predictor windows, event prevalences, and validation settings. Values are shown for orientation only and should not be interpreted as a head-to-head comparison or as evidence of universal algorithmic superiority [7,8].

Figure 4.
Feature-importance profile illustrating how interpretable ML can map postoperative recovery risk to clinically plausible variables such as operative duration, lactate, frailty, ASA classification, and sex. The figure should be interpreted as a conceptual example of explainable modelling rather than as a definitive external benchmark unless supported by peer-reviewed validation, calibration assessment, and clinical utility testing. The source recovery-quality model is a preprint-only study and is included here solely as a conceptual example of explainable feature mapping.
Figure 4.
Feature-importance profile illustrating how interpretable ML can map postoperative recovery risk to clinically plausible variables such as operative duration, lactate, frailty, ASA classification, and sex. The figure should be interpreted as a conceptual example of explainable modelling rather than as a definitive external benchmark unless supported by peer-reviewed validation, calibration assessment, and clinical utility testing. The source recovery-quality model is a preprint-only study and is included here solely as a conceptual example of explainable feature mapping.

Figure 5.
A dual-phase computational paradigm for automated postoperative wound monitoring. The architecture incorporates a deep learning segmentation phase (MobileNet-UNet) for anatomical localisation alongside site-specific ML classifiers to identify early inflammatory changes in chest, drain, and leg incisions [17].
Figure 5.
A dual-phase computational paradigm for automated postoperative wound monitoring. The architecture incorporates a deep learning segmentation phase (MobileNet-UNet) for anatomical localisation alongside site-specific ML classifiers to identify early inflammatory changes in chest, drain, and leg incisions [17].

Figure 6.
Clinical cohort demographics and surgical procedure distribution in the pilot evaluation of the NightSignal ML algorithm (N = 56) [10].
Figure 6.
Clinical cohort demographics and surgical procedure distribution in the pilot evaluation of the NightSignal ML algorithm (N = 56) [10].

Figure 7.
Temporal distribution of postoperative complication detections using the NightSignal algorithm. The timeline illustrates the transition from the 1-week preoperative baseline to the 90-day postoperative monitoring period. The Critical Window (Days 0–14) accounts for the majority of “Early Detections” (n = 15), where the AI flagged complications prior to clinical diagnosis. Late detections (n = 2) were specifically correlated with periods of patient non-compliance (intermittent Fitbit wear), emphasizing the role of continuous data streams in personalized postoperative surveillance [10].
Figure 7.
Temporal distribution of postoperative complication detections using the NightSignal algorithm. The timeline illustrates the transition from the 1-week preoperative baseline to the 90-day postoperative monitoring period. The Critical Window (Days 0–14) accounts for the majority of “Early Detections” (n = 15), where the AI flagged complications prior to clinical diagnosis. Late detections (n = 2) were specifically correlated with periods of patient non-compliance (intermittent Fitbit wear), emphasizing the role of continuous data streams in personalized postoperative surveillance [10].

Figure 8.
Illustrates the clinical workflow of the ML decision support system for post-discharge cardiothoracic care. The diagram demonstrates the precise stratification of recovery risk through the integration of multi-phase patient data, which enables the targeted allocation of remote patient monitoring resources to prevent late-stage complications [24].
Figure 8.
Illustrates the clinical workflow of the ML decision support system for post-discharge cardiothoracic care. The diagram demonstrates the precise stratification of recovery risk through the integration of multi-phase patient data, which enables the targeted allocation of remote patient monitoring resources to prevent late-stage complications [24].

Figure 9.
Reported discrimination metrics grouped by clinical endpoint/domain across selected AI-based prediction models included in this review. Metrics are non-interchangeable due to heterogeneous endpoints, baseline event prevalence, input data structure, predictor timing, calibration reporting, and validation strategy. The figure is designed as an evidence map, not a league table of model quality. Studies using non-AUC-based evaluation metrics, including wound-image mIoU/accuracy and wearable PPV/NPV, are discussed separately because they are not mathematically comparable with AUC-based discrimination measures. The recovery-quality entry from Zhang et al. [33] is a preprint-only source and is included solely as contextual emerging evidence, not as a clinical benchmark [7,8,9,10,14,17,24,28,33,36].
Figure 9.
Reported discrimination metrics grouped by clinical endpoint/domain across selected AI-based prediction models included in this review. Metrics are non-interchangeable due to heterogeneous endpoints, baseline event prevalence, input data structure, predictor timing, calibration reporting, and validation strategy. The figure is designed as an evidence map, not a league table of model quality. Studies using non-AUC-based evaluation metrics, including wound-image mIoU/accuracy and wearable PPV/NPV, are discussed separately because they are not mathematically comparable with AUC-based discrimination measures. The recovery-quality entry from Zhang et al. [33] is a preprint-only source and is included solely as contextual emerging evidence, not as a clinical benchmark [7,8,9,10,14,17,24,28,33,36].


Table 1.
Source-study characteristics and incidence of cardiac surgery-associated acute kidney injury (CSA-AKI) in the Detect-A(K)I model development cohort; values are compiled from Kalisnik et al. and do not represent new primary data generated by this review (N = 7,507) [14].
Table 1.
Source-study characteristics and incidence of cardiac surgery-associated acute kidney injury (CSA-AKI) in the Detect-A(K)I model development cohort; values are compiled from Kalisnik et al. and do not represent new primary data generated by this review (N = 7,507) [14].
| Characteristic | Total Cohort (N=7,507) |
|---|---|
| Study Site | Klinikum Nürnberg, Germany |
| Model Type | Detect-A(K)I (AI-based detection) |
| Primary Outcome | Cardiac Surgery–Associated AKI (CSA-AKI) |
| Detection Window | Within 12 hours postoperatively |
| AKI Incidence, n (%) | 1,699 (22.6%) |
| Non-AKI Incidence, n (%) | 5,808 (77.4%) |
Table 2.
Overview of the XGBoost ML model for forecasting in-hospital and 30-day mortality following adult heart surgery. The system effectively reduced 61 raw clinical variables to the 23 most significant features, achieving a reported AUC of 0.846 and showing favourable decision-curve performance relative to comparator models [36].
Table 2.
Overview of the XGBoost ML model for forecasting in-hospital and 30-day mortality following adult heart surgery. The system effectively reduced 61 raw clinical variables to the 23 most significant features, achieving a reported AUC of 0.846 and showing favourable decision-curve performance relative to comparator models [36].
| Category | Study Parameter / Metric | Value / Finding |
|---|---|---|
| Study Scale | Total Patient Cohort (N) | 224,318 adults (UK National Database) |
| Baseline Mortality Rate | 2.76% (n = 6,100 deaths) | |
| Model Architecture | Algorithm Used | XGBoost (Gradient Boosting) |
| Input Variables | 23 optimized clinical features (reduced from 61) | |
| Performance Metrics | Discriminatory Power (AUC) | 0.846 |
| F1 Score | 0.277 | |
| Clinical Utility Limit | Net benefit observed up to a threshold probability of 60% | |
| Top 5 Predictors | Most Influential Features | 1. Operation Type 2. Patient Age 3. Creatinine Clearance 4. Urgency of Procedure 5. NYHA Score |
Table 3.
Critical comparative framework for selected AI-based models for postoperative complication prediction and surveillance in cardiothoracic surgery.
Table 3.
Critical comparative framework for selected AI-based models for postoperative complication prediction and surveillance in cardiothoracic surgery.
| Study | Endpoint / domain | Dominant data stream | Architecture / metric | Interpretive caution |
|---|---|---|---|---|
| Pandey et al. [7] | POAF | Static clinical risk scores | Conventional scores; highest pooled AUC ≈ 0.66 | POAF-specific evidence; not a universal benchmark |
| Kalisnik et al. [14] | CSA-AKI | Dynamic postoperative laboratory, haemodynamic, and urine-output data | Detect-A(K)I; AUC 0.88 | Reflects early dynamic data and modelling; single-system validation |
| Chen et al. [8] | Pulmonary complications | Perioperative thoracic-surgery variables | XGBoost / SHAP; AUC 0.860 | Internal validation; not directly comparable with POAF scores |
| Tong et al. [9] | Paediatric adverse outcomes | Paediatric CHS registry-style data | LightGBM; endpoint-specific AUCs | LCOS, pneumonia, renal failure, and DVT are separate endpoints |
| Guo et al. [28] | Postoperative delirium | Pooled cardiac-surgery studies | SVM / ensembles; pooled C-index 0.805 | Heterogeneity in delirium definitions, predictors, and validation |
| Zhang et al. [33] (preprint only) | Recovery quality | Perioperative structured variables | XGBoost / SHAP; high reported AUC, not benchmarked | Contextual evidence only; requires peer-reviewed validation |
| Sinha et al. [36] | 30-day mortality | Large UK adult cardiac-surgery registry | Feature-selected XGBoost; AUC 0.846 | Structured variables may limit gain over recalibrated regression |
| Pereira et al. [17] | Wound alterations | Patient wound images | CNN segmentation and wound-specific classifiers | mIoU/accuracy are not comparable with AUC metrics |
| Beqari et al. [10] | Early multi-complication detection | Fitbit-derived longitudinal signals | NightSignal; sensitivity 81%, NPV 97%, PPV 28% | Low PPV and adherence-related missingness limit deployment |
| Santos et al. [24] | Post-discharge events | Pre-, intra-, and postoperative EMR variables | Gradient boosting; temporal AUC 0.653 | Temporal performance drop highlights deployment challenge |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



