Submitted:
22 June 2026
Posted:
24 June 2026
You are already at the latest version
Abstract
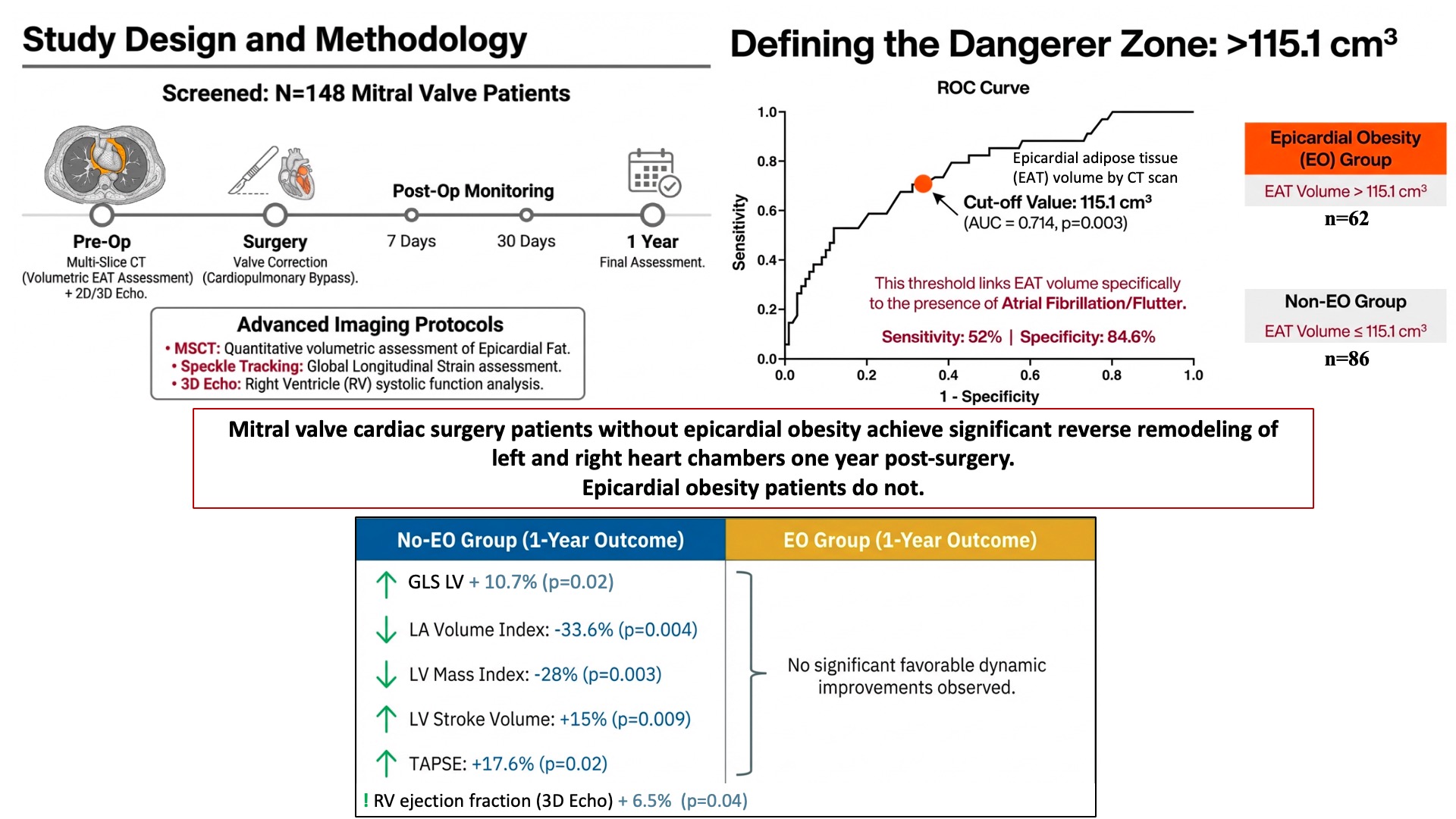
Objective To assess the relationship between epicardial obesity (EO) and the patterns of perioperative myocardial remodeling in patients undergoing surgical correction of mitral valve (MV) disease. Methods: Total of 148 patients with acquired non-infectious MV disease scheduled for surgical correction under cardiopulmonary bypass were screened in the prospective observational non-randomized study. Preoperative computed tomography (CT) of the heart was performed to assess epicardial adipose tissue (EAT) volume. Transthoracic echocardiography (Echo), including evaluation of left ventricular (LV) global longitudinal strain, right ventricular (RV) free wall longitudinal strain, and RV systolic function (3D Echo), was conducted preoperatively, as well as on postoperative during one year after surgery. Analysis of myocardial remodeling, postoperative complications, and clinical endpoints (death, reoperation) within one year was performed. Patients were divided into two groups before surgical correction of MV based on the presence of EO (EAT volume >115.1 cm³ by CT): EO group (n=62) and no-EO group (n=86). Results: Prior to MV correction, Echo showed that patients with EO exhibited larger left and right atrial (LA/RA) volumes and more pronounced RV systolic dysfunction. An EAT volume >115.1 cm³ was associated with a 4.6-fold increase in the odds of detecting a preoperative TAPSE value < 1.7 cm (OR 4.6 [95% CI 1.2543; 16.7481], p=0.02). In the early postoperative period, patients with EO exhibited larger right atrial dimensions and higher RV end-systolic volumes, as well as impaired RV-pulmonary artery coupling. At the one-year follow-up, EO patients exhibited larger indexed atrial volumes and basal RV dimensions. By the one-year follow-up, the no-EO group was characterized by dynamic improvements, including a 10.7% increase in LV global longitudinal strain (p=0.02), a 33.6% reduction in indexed LA volume (p=0.004), a 28% reduction in LV mass index (p=0.003), and a 10.3% reduction in LV end-diastolic dimension (p=0.01). Furthermore, this group exhibited a 15% increase in LV stroke volume (p=0.009), a 17.6% increase in TAPSE (p=0.02), and a 6.5% increase in RV ejection fraction (p=0.04) (3D Echo), none of which were observed in the EO group. Conclusion The presence of epicardial obesity (verified by cardiac CT) in cardiac surgery patients with acquired MV disease is associated with less favorable preoperative remodeling of both the left and right cardiac chambers and impaired reverse myocardial remodeling within one year post-surgery.
Keywords:
valvular heart disease
; mitral valve
; epicardial obesity
; surgical correction
; perioperative myocardial remodeling
1. Introduction
The process of myocardial remodeling is dynamic and occurs at various levels—ranging from the cellular (cardiomyocytes) to the organ level (alterations in cardiac geometry)—involving changes in the size as well as the structural and functional characteristics of the heart chambers [1,2]. Myocardial remodeling processes in patients with acquired valvular heart disease (VHD) clearly depend on the type and etiology of the defect, the severity of intracardiac and pulmonary circulation hemodynamics, as well as the nature and clinical significance of comorbid conditions [2]. Obesity is currently one of the most prevalent comorbid conditions among individuals with cardiovascular diseases. According to WHO data, the prevalence of obesity has doubled over the past twenty years, and as of 2022, the number of obese individuals worldwide was approaching one billion [3].
A number of studies have demonstrated the contribution of obesity to the process of myocardial remodeling in individuals with cardiovascular diseases [4,5]. However, there is an 'obesity paradox', demonstrating a lower risk of mortality following cardiac surgery in obese individuals compared to those without obesity [6]; this implies the constrained clinical and diagnostic use of body mass index (BMI) as a measure of obesity.
It is important to note that it is the visceral adipose tissue (VAT) that serves as a specific predictor of pathological myocardial remodeling, whereas there is no established correlation between BMI values and the pattern of remodeling [7,8,9].
Researchers are currently showing particular interest in epicardial adipose tissue (EAT) as a component of visceral obesity, due to its immediate proximity to the myocardium and their shared blood supply network.
To date, accumulated data regarding the influence of VAT on the structural and functional characteristics of the heart chambers have been obtained primarily from patients with coronary pathology and heart failure [10]. The influence of visceral obesity components on the cardiac valvular apparatus has been evaluated primarily in experimental studies [11,12]. This determines the relevance of further clinical studies aimed at investigating various components of obesity and their influence on the pattern of myocardial remodeling in patients with acquired VHD [13,14].
Objective of the study: To evaluate the association between epicardial obesity and the pattern of perioperative myocardial remodeling in patients undergoing surgical correction of mitral valve disease.
2. Materials and Methods
A total of 148 patients undergoing surgical correction of non-infectious mitral valve (MV) disease under cardiopulmonary bypass (CPB) were screened for a prospective, observational, non-randomized, single-center study conducted between 2024 and 2025.
All patients provided informed consent to participate in the study. The study was conducted in accordance with the Good Clinical Practice standards and the principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of the Research Institute for Complex Issues of Cardiovascular Diseases (Minutes No. 7, dated September 16, 2024);
Inclusion criteria: age between 35 and 75 years; presence of acquired mitral valve disease caused by rheumatic heart disease, connective tissue dysplasia syndrome, or degenerative lesions; planned surgical correction of the mitral valve, either isolated or in combination with aortic or tricuspid valve repair, under CPB; signed informed consent to participate in the study.
Exclusion criteria: mitral valve disease etiology associated with infectious endocarditis; hemodynamically significant stenosis of coronary or peripheral arteries requiring revascularization; body weight exceeding 120 kg; tachyform of atrial fibrillation (AF) or atrial flutter (AFL) at the time of examination, preventing multispiral computed tomography (CT) imaging; presence of an implanted pacemaker; absolute contraindications for CT; severe respiratory failure (Grade II–III); pregnancy or lactation; severe liver dysfunction (>9 points on the Child-Pugh scale, Class C); requirement for hemodialysis. history of myocardial infarction, acute cerebrovascular accident, or pulmonary embolism within six months prior to hospitalization for surgical correction; severe neurological deficit; psychiatric disorders.
Baseline characteristics of the patients prior to MV correction are presented in Table 1.
Two-dimensional and three-dimensional transthoracic echocardiography (Echo) was performed prior to the surgery, on days 7 and 30, and one year after MV correction. In addition to the standard echocardiographic protocol, myocardial strain and right ventricular (RV) systolic function were assessed using an expert-class system (Vivid E9, GE Healthcare, USA).
To identify epicardial obesity and quantify EAT volume, patients underwent cardiac CT prior to surgical MV correction. Imaging was performed on a 64-slice scanner (Siemens Somatom, Germany) with with synchronization of ECG recording (Figure 1).
Note: Epicardial adipose tissue is highlighted in yellow
Currently, there is no universally recognized criterion for epicardial obesity (EO). Therefore, ROC analysis was required to identify the threshold for epicardial fat volume that determines the presence or absence of EO. The presence of AF/AFL in patients with mitral valve disease was selected as the factor for determining the EAT threshold via ROC analysis. The choice of AF/AFL as the rhythm disorder was based on the previously confirmed association between epicardial fat and the presence of AF/AFL in patients with cardiovascular diseases [15,16].
In our study, an EAT volume exceeding 115.1 cm³ (by the MSCT data) was associated with the presence of AF/AFL (AUC = 0.714, 95% CI 0.57–0.83, p = 0.003), according to the ROC analysis, with a sensitivity of 52% and a specificity of 84.6%.
Among the included patients (n = 148), there was an equal distribution of females (47,3%) and males (52,7 %) (median age 65.0 [53.0; 67.8] years).
Based on the obtained EAT threshold, patients were divided into two groups: 62 patients with EO (EAT volume > 115.1 cm³) and 86 patients without EO (EAT volume ≤ 115.1 cm³) according to cardiac CT data.
The study design is presented in Figure 2.
Statistical data analysis was performed using standard non-parametric methods with MedCalc software. Quantitative variables are presented as median and interquartile range (Me [LQ; UQ]); qualitative variables are expressed as percentages. The Mann–Whitney U test was used to compare quantitative parameters between groups. Differences in qualitative variables were assessed using Pearson’s chi-squared test. Intragroup changes over time were evaluated using the Wilcoxon signed-rank test. Results of logistic regression analysis are presented as odds ratios (OR) and the level of statistical significance (p-values). Linear regression analysis results are reported as B-coefficients and p-values. Receiver Operating Characteristic (ROC) −curves were used to calculate threshold values (p<0.05, Area Under the Curve (AUC)>0.6). The critical level of statistical significance was set at p<0.05.
3. Results
There were no significant differences between patients with and without epicardial obesity regarding sex (31 females (50.0%] in the EO group vs. 39 (45.3%) in the non-EO group, p=0.35). The groups were also comparable in age (65.0 [61.75; 69.0] years for the EO group vs. 58.5 [51.0; 67.0] years for the non-EO group, (p=0.11)).
CT data indicates that rheumatic etiology of MV disease was more common in patients with EAT volume >115.1 cm³ (62.9% vs. 34.9%, p=0.04). Connective tissue dysplasia predominated in the non-EO group (51.16% vs. 19.35%, p=0.03).
Patients with EO were twofold less likely to present with MV regurgitation (33.87% vs. 69.8%, p=0.017), while combined MV disease was observed twice as frequently as in patients without EO (41.9% vs. 16.1%, p=0.005). Patients in the EO group had a more severe functional status; notably, while no patients in the non-EO group had NYHA Class IV chronic heart failure (CHF), it was observed in 9.7% of those with EO (p=0.037).
Patients with EO had a higher prevalence of AF/AFL compared to the non-EO group (71.9% vs. 38.4%), p=0.006), and a higher incidence of high-grade ventricular extrasystole (Lown grades IVa–V): 27.4% vs 9.3%, p=0.04. Body mass index was higher in the EO group (32.4 [28.0; 37.1] vs. 23.8 [21.98; 26.6] kg/m², p<0.001). No other differences in comorbidities were identified.
Preoperatively, patients received standard therapy according to guidelines for chronic heart failure [17]. Significant differences regarding EO were found in the use of beta-blockers and anticoagulants, which were taken by significantly more patients with EAT volume >115.1 cm³. This finding is likely attributed to the higher prevalence of high-grade ventricular extrasystole and AF/AFL in this group.
The next stage involved assessing the association between EAT volume and the pattern of left and right heart chamber remodeling prior to MV correction. According to Echo results, patients with EO were characterized by larger atrial volumes and a more pronounced decrease in RV systolic function (reduced tricuspid annular plane systolic excursion - TAPSE) (Figure 3).
According to the results of univariate logistic regression analysis, an EAT volume exceeding 115.1 cm³ is associated with an increased risk of reduced RV systolic function (TAPSE < 1.7 cm) prior to MV correction (OR 4.6 [95% CI 1.2543–16.7481], p=0.021).
In the multivariate analysis conducted to assess the direct contribution of EAT to impaired RV function (TAPSE), the significance of an EAT volume >115.1 cm3 as a predictor of RV dysfunction remained robust (Table 2), even after adjusting for other factors potentially affecting RV systolic function.
However, when AF was included in the analysis, the significance of EAT volume was eliminated, the statistical significance of EAT volume was attenuated. The presence of preoperative AF/AFL in patients with MV disease is associated with a reduction in TAPSE, with a B-coefficient of -0.396 (p < 0.001).
According to the logistic regression analysis, an EAT volume exceeding 93.9 cm³ (representing the median value for the entire patient cohort) was associated with an increased likelihood of impaired LV GLS (OR 3.75; 95% CI 1.076–13.073, p = 0.038).
When patients were devided into groups by preoperative EAT volume measured by cardiac MSCT, less favorable reverse remodeling was observed during the postoperative follow-up in the group with an EAT volume > 115.1 cm³ compared to the non-EO group (Table 3). One year after surgery, patients with EO had significantly larger left atrial (LA) diameter, indexed LA volume, and LA area compared to those without EO. During the postoperative period, left ventricular (LV) volumes and LV mass were also significantly higher in patients with EO. In the early postoperative period, patients with EO were characterized by more severely impaired LV global longitudinal strain (GLS) (Table 3).
Regression analysis revealed that 1 cm³ increase in EAT volume was associated with an increase in right atrial (RA) volume, with a B-coefficient of 0.2759 (p=0.005) at one week and a B-coefficient of 0.2251 (p=0.0303) at one month postoperatively. Furthermore, EAT volume was associated with increased RV end-systolic and end-diastolic volumes as measured by 3D Echo, with B-coefficients of 0.1635 (p=0.016) and 0.2332 (p=0.016), respectively, at one week after the surgery.
Furthermore, each 1 cm³ increase in EAT volume was associated with an increase in RA area, with a B-coefficient of 0.04221 (p=0.0308), and an increase in RV basal diameter, with a B-coefficient of 0.00321 (p=0.039), at the one-year follow-up after mitral valve correction. One year postoperatively, the proportion of patients with Grade III tricuspid regurgitation was significantly higher in the EO group (p=0.0424) (Table 3).
Postoperative cardiac remodeling dynamics were evaluated in patients following mitral valve correction, stratified by the presence of epicardial obesity (EO).
It was found that, compared to preoperative values, more pronounced reverse remodeling of the left heart chambers was observed in the non-EO group one year postoperatively:
— left ventricular mass index (LVMI) significantly decreased by 28% (p=0.003);
— left ventricular end-diastolic diameter (LVEDD) decreased by 10.3% (p=0.01);
— LA diameter decreased by 9.4% (p=0.002) and left atrial volume index (LAVI) decreased by 33.6% (p=0.004).
In contrast, these parameters showed no significant changes in patients with EO.
Patients without excess epicardial fat demonstrated an improvement in LV GLS of 12.2% (p=0.004) between the one-month and one-year follow-up, while no significant dynamics were observed in the EO group.
The non-EO group was characterized by a 14% decrease in LV end-systolic volume (p=0.04) one month after valve correction, whereas this parameter increased in the EO group (p=0.009). A 15% increase in LV stroke volume (p=0.009) was noted in the non-EO group from the one-month to one-year follow-up.
When evaluating postoperative remodeling dynamics of the right heart chambers, the group with an EAT volume less than 115.1 cm³ showed an increase in RV stroke volume by 76% (p=0.003), RV ejection fraction by 6.5% (p=0.04), and RV fractional area change by 12.2% (p=0.005) from one month to one year, while no significant dynamics were observed in the EO group. In the non-EO group, TAPSE increased from 1.4 [1.2; 1.72] cm to 1.7 [1.5; 1.9] cm (p=0.002) between the 1-month and 1-year postoperative periods, whereas no significant increase was observed in the EO group, which had lower baseline TAPSE values.
When analyzing the incidence of early postoperative complications, a higher frequency of stroke/ transient ischemic attack was observed in the EO group (n=6; 9.7%) during the early postoperative period (p=0.047). This finding may be associated with the significantly higher prevalence of AF/AFL in this group (p=0.014).
One patient developed ventricular fibrillation, which was fatal (6 months after MV surgery). This patient had evidence of EO before MV correction. The death of the second patient was not related to cardiovascular causes.
The incidence of readmissions for HF decompensation and cardiac arrhythmias was significantly higher in the EO group, which may be attributed to a higher prevalence of pre-existing AF in this patient cohort (Table 4).
One year after MV correction, the incidence of arrhythmias (AF/AFL) was significantly higher in the group with EAT volume >115.1 cm³ compared to the group with lower EAT volume: 29 (48.33%) vs 8 (9.3%) patients, respectively (p=0.003). Among patients discharged from the hospital with AF/AFL (n=54), sinus rhythm restoration during the one-year follow-up period occurred in 12 (22.2%) patients in the EAT group and 19 (22.1%) patients in the non-EAT group (p=0.1625). No significant differences were observed in NYHA functional class between the EAT and non-EAT groups one year after surgery (Table 4).
4. Discussion
Obesity is a well-established driver of myocardial remodeling in patients with cardiovascular diseases, as evidenced by extensive fundamental and applied studies [4,8]. Pathological expansion of VAT and EAT leads to adipocyte hypertrophy and hyperplasia. This triggers an adipokine imbalance and a shift toward a pro-inflammatory profile, resulting in tissue damage, myocardial hypertrophy, and fibrosis [18]. Recent studies indicate that excessive visceral adipose tissue serves as a key predictor of pathological left ventricular remodeling, whereas BMI often shows no correlation with remodeling patterns [7,8,9].
Our study focused specifically on EAT due to its anatomical proximity to the myocardium and its potential impact on adverse cardiac chamber remodeling. Adipokines and other bioactive substances secreted by EAT maintain energy homeostasis and provide mechanical protection for the myocardium. However, its pathological expansion is associated with adipokine dysregulation and the active production of pro-inflammatory interleukins, which may affect cardiomyocytes [4,19]. Research indicates that increased EAT volume is associated with unfavorable outcomes in patients with heart failure with preserved LV ejection fraction [20,21]. Currently, most publications studying structural and functional cardiac impairments in individuals with visceral obesity focus primarily on patients with coronary pathology and chronic heart failure [10,22].
In our study, myocardial remodeling was assessed using both standard transthoracic echocardiography (cardiac chamber dimensions and volumes) and an expanded protocol. The latter included speckle-tracking echocardiography to evaluate ventricular myocardial strain, as well as RV systolic function analysis based on 2D and 3D echocardiographic data. Schulz et al. [21] in their study demonstrated that increased EAT volume was associated with impaired GLS of the left ventricle and left atrium in patients with heart failure and diastolic dysfunction (HFpEF).
Several other studies have also demonstrated a link between EAT and impaired LV systolic and diastolic function, LV enlargement, LA fibrosis, and electrophysiological remodeling, the onset and severity of AF and arterial stiffness parameters in patients with heart failure and ischemic heart disease [23,24,25,26,27]. For the cohort of patients with acquired VHD, available data are limited to associations between EAT thickness and the presence or severity of left-sided heart valve calcification [4], as well as the association between EAT thickness, measured by Echo, and the degree of LV remodeling in moderate _ to _ severe aortic stenosis [14,28]. Furthermore, in age-associated valvular diseases, EAT thickness is directly correlated with the severity of comorbid conditions, such as diabetes mellitus and obesity, as well as advanced patient age.
There is also evidence, suggesting a correlation between EAT volume (measured by 3D echocardiography) and adverse cardiovascular and neurological events one year after transcatheter aortic valve replacement [29]. Another study demonstrated that patients undergoing transcatheter aortic valve intervention with low EAT volume (<49 cm³ on CT) and high EAT attenuation (≥ -86 HU) had higher all-cause mortality (log-rank p=0.02 and p=0.01, respectively). This association remained significant even after adjusting for age, sex, and clinical characteristics (HR 1.71, p=0.02 and HR 1.73, p=0.03, respectively) [30].
To date, no studies have investigated the relationship between epicardial adipose tissue thickness or volume and the patterns of myocardial remodeling in cardiac surgery patients with MV disease of various etiologies across a wide age range.
The conducted study is the first to demonstrate a significant association between EAT and structural-functional changes in both the left and right cardiac chambers in the cohort of surgical patients with MV disease. This relationship was observed both preoperatively and during the one-year follow-up period following surgical correction.
An EAT volume exceeding 93.9 cm³, as measured by CT, is associated with a more pronounced impairment of LV global longitudinal strain. Meanwhile, a higher EAT volume (exceeding 115.1 cm³) is associated with increased atrial volumes and deterioration of the RV systolic function. Notably, the contribution of epicardial obesity to the development of RV dysfunction remains significant even after adjusting for factors such as age, sex, type of valvular heart disease, comorbid profile, and a high probability of pulmonary hypertension based on Echo data.
In the early postoperative period, patients with EO exhibited larger RA dimensions and RVESV, as well as impaired RV-pulmonary artery (RV-PA) coupling. At the one-year follow-up, patients with EO were characterized by larger dimensions of the right-sided cardiac chambers.
Perioperative reverse myocardial remodeling serves as a reflection of the functional status, quality of life, and prognosis of surgical patients with acquired VHD [20]. Our study highlights that, throughout the one-year postoperative period, EAT volume, in particular, exerts a more pronounced contribution to the adverse dynamics of myocardial remodeling. Intragroup dynamics analysis revealed that patients without EO exhibited significant reverse myocardial remodeling across several parameters by the one-year follow-up, along with improvement in RV systolic function. In contrast, these favorable changes were not observed in the group with EO.
5. Conclusions
The presence of epicardial obesity (verified by cardiac CT) in cardiac surgical patients with acquired MV disease is associated with less favorable remodeling patterns of both the left and right cardiac chambers preoperatively, as well as impaired reverse myocardial remodeling throughout the one-year follow-up period. It was demonstrated that the absence of epicardial obesity on cardiac CT in patients undergoing surgical correction is associated with significantly more favorable postoperative reverse LV myocardial remodeling and an improvement in RV systolic function. A timely and comprehensive approach to identifying various manifestations of obesity, combined with a detailed assessment of the remodeling dynamics in both the left and right cardiac chambers, would allow for the modification of factors adversely affecting the disease course in cardiac surgery patients with MV disease at the preoperative stage. The adoption of these advanced preoperative screening algorithms for patients with valvular heart disease could, in turn, enhance treatment efficacy and improve clinical outcomes.
Author Contributions
Conceptualization, Olga Barbarash and Irina Lyapina; methodology, Olga Barbarash and Irina Lyapina; investigation, Irina Lyapina, Elena Dren, Anastasia Kareeva, Aleksander Stasev, Eugenia Gorbatovskaya, Julia Yur’eva, Maria Khutornaya, Irina Mamchur; visualization – Anastasia Kareeva and Irina Mamchur; formal analysis, Elena Dren; writing—original draft, Irina Lyapina, Elena Dren; writing—review and editing, Olga Barbarash and Irina Lyapina; project administration, Irina Lyapina and Olga Barbarash.
Funding
This work was supported by the Russian Science Foundation (grant number: 24-75-10031) "Epicardial and visceral obesity as a factor influencing the remodeling of the myocardium and pulmonary vessels after surgical correction of acquired valvular heart diseases.
Institutional Review Board Statement
The study was conducted in accordance with the standards of good clinical practice and the principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of the Research Institute for Complex Issues of Cardiovascular Diseases (Minutes No. 7, dated September 16, 2024); (meeting of the local ethics committee No. 7 dated September 16, 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| AF | Atrial fibrillation |
| AFL | Atrial flutter |
| CHF | Chronic heart failure |
| CPB | Сardiopulmonary bypass |
| GLS | Global longitudinal strain |
| EAT | Epicardial adipose tissue |
| EO | Epicardial obesity |
| LA | Left atrium |
| LV | Left ventricle |
| MV | Mitral valve |
| RA | Right atrium |
| RV | Right ventricle |
| VAT | Visceral adipose tissue |
| VHD | Valvular heart disease |
References
- Mihl, C.; Dassen, W.R.; Kuipers, H. Cardiac remodelling: concentric versus eccentric hypertrophy in strength and endurance athletes. Neth. Heart J. 2008, 16(4), 129–33. [Google Scholar] [CrossRef] [PubMed]
- D'Elia, N.; D'hooge, J.; Marwick, T.H. Association Between Myocardial Mechanics and Ischemic LV Remodeling. JACC Cardiovasc Imaging 2015, 8(12), 1430–43. [Google Scholar] [CrossRef] [PubMed]
- Ostrominski, J.W.; Powell-Wiley, T.M. Risk Stratification and Treatment of Obesity for Primary and Secondary Prevention of Cardiovascular Disease. Curr. Atheroscler. Rep. 2024, 26, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Gritsenko, O.V.; Chumakova, G.A.; Elchaninova, S.A.; Veselovskaya, N.G.; Shevlyakov, I.V.; Kalugina, O.A. Lipotoxicity damage of myocardium in obesity. Cardiosomatics 2017, 8(4), 36–40. [Google Scholar] [CrossRef]
- Dronkers, J.; van Veldhuisen, D.J.; van der Meer, P.; Meems, L.M.G. Heart Failure and Obesity: Unraveling Molecular Mechanisms of Excess Adipose Tissue. J. Am. Coll. Cardiol. 2024, 84(17), 1666–1677. [Google Scholar] [CrossRef] [PubMed]
- Mariscalco, G.; Wozniak, M.J.; Dawson, A.G.; Serraino, G.F.; Porter, R.; Nath, M.; Klersy, C.; Kumar, T.; Murphy, G.J. Body mass index and mortality among adults undergoing cardiac surgery: a nationwide study with a systematic review and meta-analysis Circulation. 2017, 135(9), 850–863. [Google Scholar] [CrossRef] [PubMed]
- Dren', E.V.; Lyapina, I.N.; Golubovskaya, D.P.; Pecherina, T.B.; Barbarash, O.L. Relationship between body composition components in patients with comorbidities and the severity of acquired valvular heart disease. Sib. Med. Rev. 2025, (1), 91–97. [Google Scholar] [CrossRef]
- Nazare, J.A.; Smith, J.; Borel, A.L.; Aschner, P.; Barter, P.; Van Gaal, L.; Tan, C.E.; Wittchen, H.U.; Matsuzawa, Y.; Kadowaki, T.; Ross, R.; Brulle-Wohlhueter, C.; Alméras, N.; Haffner, S.M.; Balkau, B.; Després, J.P. INSPIRE ME IAA Investigators. Usefulness of measuring both body mass index and waist circumference for the estimation of visceral adiposity and related cardiometabolic risk profile (from the INSPIRE ME IAA study). Am. J. СArdiol. 2015, 115(3), 307–315. [Google Scholar] [CrossRef] [PubMed]
- Fuster, J.J.; Ouchi, N.; Gokce, N.; Walsh, K. Obesity–induced changes in adipose tissue microenvironment and their impact on cardiovascular disease. Circ. Res. 2016, 118(11), 1786–1807. [Google Scholar] [CrossRef] [PubMed]
- Brel, N.K.; Gruzdeva, O.V.; Kokov, A.N.; Masenko, V.L.; Belik, E.V.; Dyleva, YuA; Tarasov, R.S.; Kuzmina, A.A.; Kashtalap, V.V.; Barbarash, O.L. Relationship of coronary calcinosis and local fat deposts in patients with coronary artery disease. Complex Issues Cardiovasc. Dis. 2022, 11(3), 51–63. [Google Scholar] [CrossRef]
- Chumakova, G.A.; Veselovskaya, N.G. Methods of visceral obesity assessment in clinical practice. Russ. J. Cardiol. 2016, (4), 89–96. [Google Scholar] [CrossRef]
- Van der Heijden, C.A.J.; Verheule, S.; Olsthoorn, J.; Mihl, C.; Lexan Poulina, L.; van Kuijk, S.M.J.; Heuts, S.; Maessen, J.G.; Bidar, E.; Maesen, B. Postoperative atrial fibrillation and atrial epicardial fat: Is there a link? Int. J. Cardiol. Heart Vasc. 2022, 39, 100976. [Google Scholar] [CrossRef] [PubMed]
- Dren', E.V.; Lyapina, I.N.; Stasev, A.N.; Mamchur, I.N.; Brel, N.K.; Kareeva, A.I.; Barbarash, O.L. Relationship between epicardial/visceral obesity and features of myocardial remodeling in patients with acquired mitral valve disease. Cardiovasc. Ther. Prev. 2025, 24(2), 4301. [Google Scholar] [CrossRef]
- Coisne, A.; Ninni, S.; Ortmans, S.; Davin, L.; Kasprzak, K.; Longère, B.; Seunes, C.; Coppin, A.; Mouton, S.; Ridon, H.; Klein, C.; Noirot-Cosson, B.; Staels, B.; Lancellotti, P.; Montaigne, D.; Pontana, F. Epicardial fat amount is associated with the magnitude of left ventricular remodeling in aortic stenosis. Int. J. Cardiovasc Imaging 2019, 35(2), 267–273. [Google Scholar] [CrossRef] [PubMed]
- Golukhova, E.Z.; Bulaeva, N.I.; Alexandrova, S.A.; Saparbaev, A.A.; Abgaryan, A.A.; Berdibekov, BSh. Quantification of epicardial adipose tissue by computed tomographic scanning as a prognostic criterion of atrial fibrillation recurrence after catheter ablation. Kardiologiia 2023, 63(8), 3–10. [Google Scholar] [CrossRef] [PubMed]
- Abgaryan, A.A.; Berdibekov, BSh; Bulaeva, N.I.; Golukhova, E.Z. Epicardial elastic tissue as a substrate for atrial structural remodeling in atrial fibrillation. Kreat. Kardiol. 2025, 19(2), 122–130. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; Cleland, J.G.F.; Crespo-Leiro, M.G.; Farmakis, D.; Gilard, M.; Heymans, S.; Hoes, A.W.; Jaarsma, T.; Jankowska, E.A.; Lainscak, M.; Lam, C.S.P.; Lyon, A.R.; McMurray, J.J.V.; Mebazaa, A.; Mindham, R.; Muneretto, C.; Francesco Piepoli, M.; Price, S.; Rosano, G.M.C.; Ruschitzka, F.; Skibelund, A.K.; ESC Scientific Document Group. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. Erratum in: Eur Heart J. 2024 Jan 1;45(1):53. doi: 10.1093/eurheartj/ehad613. PMID: 37622666. 2023, 44(37), 3627–3639. [Google Scholar] [CrossRef] [PubMed]
- Chumakova, G.A.; Kuznetsova, TYu; Druzhilov, M.A.; Veselovskaya, N.G. Visceral adiposity as a global factor of cardiovascular risc. Russ. J. Cardiol. 2018, (5), 7–14. [Google Scholar] [CrossRef]
- Mustafina, I.A.; Ionin, V.A.; Dolganov, A.A.; Ishmetov, V.Sh.; Pushkareva, A.E.; Yagudin, T.A.; Danilko, K.V.; Zagidullin, N.Sh. Role of epicardial adipose tissue in the development of cardiovascular diseases. Russ. J. Cardiol. 2022, 27(1S), 4872. [Google Scholar] [CrossRef]
- Van Woerden, G.; Gorter, T.M.; Westenbrink, B.D.; Willems, T.P.; van Veldhuisen, D.J.; Rienstra, M. Epicardial fat in heart failure patients with midrange and preserved ejection fraction. Eur. J. Heart Fail. 2018, 20, 1559–1566. [Google Scholar] [CrossRef] [PubMed]
- Schulz, A.; Backhaus, S.J.; Lange, T.; Evertz, R.; Kutty, S.; Kowallick, J.T.; Hasenfu, G.; Schuster, A. Impact of epicardial adipose tissue on cardiac function and morphology in patients with diastolic dysfunction. ESC Heart Fail. 2024, 11(4), 2013–2022. [Google Scholar] [CrossRef] [PubMed]
- Zain, S.; Shamshad, T.; Kabir, A.; Khan, A.A. Epicardial Adipose Tissue and Development of Atrial Fibrillation (AFIB) and Heart Failure With Preserved Ejection Fraction (HFpEF). Cureus 2023, 15(9), 46153. [Google Scholar] [CrossRef] [PubMed]
- Song, X.T.; Zhang, P.Y.; Fan, L.; Rui, Y.F. Epicardial adipose tissue and right ventricular function in type 2 diabetes mellitus using two-dimensional speckle tracking echocardiography. Diab Vasc. Dis. Res. 2022, 19(4), 14791641221118622. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Li, J.; Li, F.; Chen, Z.; Chen, Z.; Luo, J.; Qiu, H.; Chen, W.; Hu, J.; Luo, X.; Tan, Y.; Rathinasabapathy, A.; Chen, J.; Li, J. Impact of Epicardial Adipose Tissue on Right Cardiac Function and Prognosis in Pulmonary Arterial Hypertension. Chest 2024, 165(5), 1211–23. [Google Scholar] [CrossRef] [PubMed]
- Druzhilov, M.A.; Beteleva, Y.E.; Druzhilova, O.Y.; Andreeva, E.S.; Kuznetsova, TYu. The role of epicardial obesity in the development of structural and functional remodeling of the heart. Russ. J. Cardiol. 2017, 4, 35–9. [Google Scholar] [CrossRef]
- Blinova, N.V.; Azimova, M.O.; Zhernakova, Y.V.; Zheleznova, E.A.; Yarovaya, E.B.; Orlovskiy, A.A.; Azimova, M.R.; Dobrovolskaya, S.V.; Ternovoy, S.K.; Chazova, I.E. Epicardial adipose tissue as a marker of visceral obesity and its association with metabolic parameters and remodeling of the left chambers of the heart in young people with abdominal obesity. Ther. Arch.> 2019, 91(9), 68–76. [Google Scholar] [CrossRef] [PubMed]
- Matloch, Z.; Kotulak, T.; Haluzik, M. The Role of Epicardial Adipose Tissue in Heart Disease. Physiol. Res. 2016, 65, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Ayton, S.L.; Aslam, S.; Dattani, A.; Yeo, J.L.; Gulsin, G.S.; Slomka, P.J.; Dey, D.; McCann, G.P.; Singh, A. Association of epicardial adipose tissue with markers of cardiac remodelling and clinical outcomes in asymptomatic aortic stenosis. Open Heart 2026, 13(1), e003804. [Google Scholar] [CrossRef] [PubMed]
- Özbek, K.; Dağlı, M.; Balun, A.; Yigitbasi, M.M.; Çetin, Z.G.; Demirtaş, B.; Çamur, E.; Çetin, M.; Çiçekçioğlu, H. Increased epicardial adipose tissue volume may adversely affect outcomes in patients undergoing transcatheter aortic valve implantation. Postep. Kardiol. Interwencyjnej 2024, 20(4), 420–427. [Google Scholar] [CrossRef] [PubMed]
- Piña, P.; Lorenzatti, D.; Filtz, A.; Scotti, A.; Gil, E.V.; Torres, J.D.; Perea, C.M.; Shaw, L.J.; Lavie, C.J.; Berman, D.S.; Iacobellis, G.; Slomka, P.J.; Pibarot, P.; Dweck, M.R.; Dey, D.; Garcia, M.J.; Latib, A.; Slipczuk, L. Epicardial adipose tissue, cardiac damage, and mortality in patients undergoing TAVR for aortic stenosis. Int. J. Cardiovasc Imaging 2025, 41(2), 279–290. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Assessment of epicardial adipose tissue volume using cardiac multislice computed tomography.
Figure 1.
Assessment of epicardial adipose tissue volume using cardiac multislice computed tomography.

Figure 2.
Study design.

Figure 3.
- Differences in atrial volumes and right ventricular systolic function depending on the presence of epicardial obesity in patients prior to MV correction.
Figure 3.
- Differences in atrial volumes and right ventricular systolic function depending on the presence of epicardial obesity in patients prior to MV correction.


Table 1.
Baseline clinical and medical history characteristics of patients with mitral valve disease prior to surgery.
Table 1.
Baseline clinical and medical history characteristics of patients with mitral valve disease prior to surgery.
| Parameter | n=148 |
| Female, n (%) | 70 (47.3) |
| Age, years, Me [Lq; Uq] | 61.5 [51.3; 67.0] |
| Etiology of mitral valve disease, n (%) - degenerative changes - rheumatic heart disease - connective tissue dysplasia syndrome - partial chordal rupture |
16 (10.8) 69 (46.6) 56 (37.8) 7 (4.7) |
| Type of MV disease, n (%): - MV stenosis - MV regurgitation - combined MV disease |
21 (14.2) 81 (54.7) 46 (31.1) |
| Mixed valve disease, n (%): - with aortic valve stenosis/regurgitation - with secondary tricuspid regurgitation |
21 (14.8) 44 (29.7) |
| Heart rhythm characteristics, n (%): - sinus rhythm - atrial fibrillation/atrial flutter:
|
69 (46.6) 79 (53.4) 16 (10.8) 37 (25.0) 26 (17.6) 25 (16.9) |
| Obesity (BMI ≥ 30 kg/m²), n (%) | 42 (28.4) |
| Stages of chronic heart failure, n (%): - Pre-stage - Class 1 - Class 2 |
7 (4.7) 141 (95.3)0 |
| Сhronic heart failure Functional Class (NYHA) FC I FC II FC III FC IV |
5 (3.4) 77 (52.1) 60 (40.5) 6 (4.1) |
| Six-minute walk test (6MWT) distance, m, Me [LQ; UQ] | 296.3 [292.6; 387.2] |
| Diabetes mellitus / impaired glucose tolerance, n (%) | 24 (16.2) |
| Arterial hypertension, n (%) | 106 (71.6) |
Table 2.
Data from the multivariate regression analysis demonstrating the independent association between EAT volume and reduced tricuspid annular plane systolic excursion (TAPSE) prior to mitral valve correction.
Table 2.
Data from the multivariate regression analysis demonstrating the independent association between EAT volume and reduced tricuspid annular plane systolic excursion (TAPSE) prior to mitral valve correction.
| B | SE | p | |
| Intercept | 2.952 | 0.397 | <0.001* |
| Female | -0.100 | 0.129 | 0.446 |
| Age | -0.012 | 0.007 | 0.098 |
| Mitral stenosis | -0.300 | 0.308 | 0.336 |
| Chronic obstructive pulmonary disease (COPD) | 0.116 | 0.189 | 0.544 |
| Type 2 diabetes mellitus (T2DM) | -0.034 | 0.155 | 0.830 |
| Arterial hypertension (AH) | 0.107 | 0.145 | 0.485 |
| Coronary artery disease (CAD) | -0.086 | 0.147 | 0.562 |
| Preoperative ePASP ≥38 mmHg | -0.098 | 0.198 | 0.624 |
| EAT volume, cm³ | -0.003 | 0.001 | 0.044* |
Table 3.
Comparative analysis of transthoracic echocardiographic dynamics in patients with acquired mitral valve disease postoperatively, stratified by the presence of epicardial obesity as assessed by CT (EAT volume > 115.1 cm³).
Table 3.
Comparative analysis of transthoracic echocardiographic dynamics in patients with acquired mitral valve disease postoperatively, stratified by the presence of epicardial obesity as assessed by CT (EAT volume > 115.1 cm³).
| Parameter Me [Q1;Q3] |
Group | p between groups | p – dynamics in group 1 | p – dynamics in group 2 | |||||||
| EAT volume > 115.1 cm³ (n=62, 1 year follow-up in n=60) |
EAT volume ≤ 115.1 cm³ (n=86) | ||||||||||
| Preoperative | Day 7 | 24 days | 1 year | Preoperative | Day 7 | 24 days | 1 year | ||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||||
| Left heart chambers, Me [Q1;Q3] | |||||||||||
| LV mass g | 295.0 [199.75; 344.3] | - | 217.0 [177.5; 287] | 240.0 [182; 304] | 229.0 [175; 297] | - | 175.0 [138.25; 204.75] | 183.0 [153; 221] |
p 1.5=0.16 p 3.7=0.03 p 4.8=0.04 |
p 1.3=0.06 p 1.4=0.08 p 3.4=0.97 |
p 5.7=0.006 p 5.8=0.009 p 7.8=0.69 |
| LVMI, g/m²) | 140.0 [103; 166.5] | - | 109.0 [95; 144.75] | 116.0 [89.5; 145.25] | 129.0 [108; 155] | - | 92.0 [82; 123] | 101.0 [86; 111] |
p 1.5=0.84 p 3.7=0.18 p 4.8=0.13 |
p 1.3=0.12 p 1.4=0.10 p 3.4=0.78 |
p 5.7=0.003 p 5.8=0.003 p 7.8=0.48 |
| LVESD, cm | 4.0 [3.47; 4.5] |
3.5 [3.2; 3.8] |
3.7 [3.4; 4.22] |
3.9 [3.1; 4.3] |
3.8 [3.1; 4] |
3.4 [3.07; 3.92] |
3.2 [3; 3.6] |
3.3 [3.0; 3.5] |
p 1.5=0.09 p 2.6=0.52 p3.7=0.007 p 4.8=0.04 |
p 1.2=0.009 p 1.3=0.62 p 1.4=0.07 p 2.3=0.02 p 2.4=0.39 p 3.4=0.37 |
p 5.6=0.39 p 5.7=0.03 p 5.8=0.11 p 6.7=0.06 p 6.8=0.12 p 7.8=0.43 |
| LVEDD, cm | 5.9 [5.47; 6.32] |
5.2 [4.7; 5.75] |
5.2 [4.9; 5.95] |
5.6 [5; 6] |
5.8 [4.9; 6.7] |
5.0 [4.67; 5.4] |
4.9 [4.6; 5.3] |
5.2 [4.9; 5.4] |
p 1.5=0.45 p 2.6=0.68 p 3.7=0.05 p 4.8=0.08 |
p 1.2=0.0006 p 1.3=0.01 p 1.4=0.06 p 2.3=0.03 p 2.4=0.04 p 3.4=0.87 |
p 5.6=0.0004 p 5.7=0.0003 p 5.8=0.01 p 6.7=0.05 p 6.8=0.37 p 7.8=0.02 |
| LVESV, ml | 50.0 [41.75; 62.5] | 54.0 [36.25; 62.25] | 58.5 [39; 71.0] | 55.5 [35.5; 70] | 43.0 [34.5; 58] |
36.5 [27.0; 47.0] |
37.0 [32.75; 49] | 37.0 [30; 51] |
p 1.5=0.16 p 2.6=0.009 p 3.7=0.02 p 4.8=0.13 |
p 1.2=0.24 p 1.3=0.74 p 1.4=0.53 p 2.3=0.009 p 2.4=0.43 p 3.4=0.45 |
p 5.6=0.24 p 5.7=0.04 p 5.8=0.27 p 6.7=0.37 p 6.8=0.09 p 7.8=0.94 |
| LVEDV, ml | 142.0 [97.75; 167.5] | 112.0 [84.75; 132.0] | 126.5 [87; 142.5] | 113.0 [89.5; 136] | 126.0 [93.5; 153] | 81.5 [69.0; 105.0] |
99.0 [77.25; 118] | 104.0 [89; 125] |
p 1.5=0.39 p 2.6=0.02 p 3.7=0.05 p 4.8=0.61 |
p 1.2=0.02 p 1.3=0.07 p 1.4=0.05 p 2.3=0.04 p 2.4=0.91 p 3.4=0.29 |
p 5.6=0.0003 p 5.7=0.0002 p 5.8=0.12 p6.7=0.005 p 6.8=0.0007 p 7.8=0.02 |
| LVEF, % | 61.0 [55.75; 64.5] |
53.0 [47.5; 59.5] | 54.0 [46.5; 59.5] | 59.5 [45.5; 66] | 64.0 [59.75; 66.5] | 57.0 [46.0; 64.0] |
60.0 [52; 62.5] |
63.5 [56; 68] |
p 1.5=0.10 p 2.6 =0.46 p 3.7=0.08 p 4.8=0.31 |
p 1.2=0.02 p 1.3=0.005 p 1.4=0.56 p 2.3=0.86 p 2.4=0.24 p 3.4=0.11 |
P 5.6=0.0007 P 5.7=0.04 P 5.8=0.30 P 6.7=0.007 P 6.8=0.03 P 7.8=0.05 |
| LA, cm | 5.8 [5.15; 6.65] |
5.2 [4.8; 5.72] | 5.2 [4.55; 5.65] | 5.6 [4.95; 6.1] | 5.2 [4.5; 5.6] |
4.5 [4.2; 4.7] |
4.45 [4.05; 4.7 |
4.7 [4.2; 5.0] |
p 1.5=0.01 p 2.6 <0.0001 p 3.7=0.002 p 4.8=0.0007 |
p 1.2=0.02 p 1.3=0.002 p 1.4=0.23 p 2.3=0.47 p 2.4=0.31 p 3.4=0.18 |
P 5.6=0.0002 P 5.7=0.0014 P 5.8=0.002 p 6.7=0.60 p 6.8=0.38 p 7.8=0.005 |
| LA volume, ml | 149.0 [113.25; 209.75] | 125.0 [105.5; 176.5] | 110 [94.25; 144.75] | 137.5 [97.5; 174.5] | 114.0 [97.5; 144] | 81.0 [62.0; 89.75] |
67.5 [59; 83] |
75.0 [65; 84] |
p 1.5=0.04 p 2.6 =0.0001 p 3.7=0.001 p 4.8=0.0012 |
p 1.2=0.13 p 1.3=0.0009 p 1.4=0.15 p 2.3=0.21 p 2.4=0.91 p 3.4=0.91 |
P 5.6=0.004 p 5.7=0.0001 p 5.8=0.005 p 6.7=0.001 p 6.8=0.75 p 7.8=0.28 |
| LAind, ml/m2 | 74 [55; 93.5] |
70.0 [52.5; 99.25] | 56 [46.5; 61] |
59 [45.75; 85] |
61.0 [50; 75] |
46.0 [35.0; 54.0] |
35.5 [33; 44] |
40.5 [34; 47] |
p 1.5=0.16 p 2.6 =0.004 p 3.7=0.005 p 4.8=0.01 |
p 1.2=0.82 p 1.3=0.04 p 1.4=0.15 p 2.3=0.008 p 2.4=0.008 p 3.4=1.0 |
p 5.6=0.03 p 5.7=0.0004 p 5.8=0.004 p 6.7=0.03 p 6.8=0.53 p 7.8=0.45 |
| LV GLS % | - 15.6 [- 18.9; -13.37] |
- 12.1 [-13.55; -10.15] |
- 12.35 [- 14; -9.9] |
-15.6 [-17.12; -11.37] |
- 19.0 [- 21.37; - 13.25] |
-14.3 [-16.4; -11.6] |
- 15.1 [- 16.2; - 13.4] |
-17.2 [-18.2; -14.8] |
p 1.5=0.09 p 2.6=0.04 p 3.7=0.008 p 4.8=0.10 |
p 1.2=0.20 p 1.3=0.22 p 1.4=1.0 p 2.3=0.67 p 2.4=0.14 p 3.4=0.56 |
p 5.6=0.0006 p 5.7=0.02 p 5.8=0.02 p 6.7=0.21 p 6.8=0.005 p 7.8=0.004 |
| Right heart chambers, Me [Q1;Q3] | |||||||||||
| RA volume, ml | 96.0 [75.75; 113.25] | 78.0 [68.0; 99.0] | 73.0 [60; 95] |
88.0 [62.5; 111.5] | 65.0 [50; 86] |
53.0 [42.5; 76.5] |
50.0 [40.25; 60.25] | 55.5 [50.5; 64] |
p 1.5=0.01 p 2.6=0.006 p 3.7=0.003 p 4.8=0.02 |
p 1.2=0.04 p 1.3=0.04 p 1.4=0.02 p 2.3=0.62 p 2.4=0.31 p 3.4=0.84 |
p5.6=0.20 p 5.7=0.007 p 5.8=0.08 p 6.7=0.74 p 6.8=0.92 p 7.8=0.32 |
| RA area, cm² | 27.8 [24; 30.5] |
23.7 [20.82; 32.55] | 22.5 [19.9; 29.5] | 25 [18.75; 28.85] | 23.8 [16.9; 25.75] | 19.0 [16.0; 23.1] |
18 [16.45; 19.92] |
19.35 [18; 22] |
p 1.5=0.09 p2.6=0.006 p 3.7=0.02 p 4.8=0.07 |
p 1.2=0.44 p 1.3=0.07 p 1.4= - p 2.3=0.81 p 2.4=0.63 p 3.4=0.31 |
p 5.6=0.15 p 5.7=0.16 p 5.8=0.46 p 6.7=0.87 p 6.8=0.60 p 7.8=0.68 |
| RAind, ml/m2 | 49.0 [37.25; 61.5] | 40.0 [32.0; 51.0] | 39.0 [30.5; 48] | 45.5 [32; 54.5] | 36.5 [29; 44] |
29.0 [23.0; 33.0] |
26.5 [22.5; 34.5] | 30.5 [27.5; 34.5] |
p 1.5=0.05 p 2.6=0.03 p 3.7=0.02 p 4.8=0.04 |
p 1.2=0.04 p 1.3=0.01 p 1.4=0.02 p 2.3=0.93 p 2.4=0.51 p 3.4=0.73 |
p 5.6=0.36 p 5.7=0.07 p 5.8=0.07 p 6.7=0.41 p 6.8=0.65 p 7.8=0.38 |
| Right ventricular basal diameter, cm | 3.9 [3.37; 4.27] |
4.2 [3.85; 4.35] | 4.0 [3.67; 4.32] | 4.2 [3.95; 4.4] | 3.5 [3.17; 4] |
3.9 [3.65; 4.0] |
3.6 [3.2; 3.8] |
3.8 [3.6; 4.2] |
p1.5=0.39 p 2.6=0.11 p 3.7=0.02 p 4.8=0.04 |
p 1.2=0.12 p 1.3=0.87 p 1.4=0.40 p 2.3=0.06 p 2.4=0.74 p 3.4=0.13 |
p 5.6=0.20 p 5.7=0.98 p 5.8=0.71 p 6.7=0.07 p 6.8=0.13 p 7.8=0.15 |
| RV fractional area change, % | 38.0 [30.5; 45] |
34.0 [29.5; 41.0] | 42.0 [36.75; 46.25] | 41.5 [36.0; 47.0] | 45.0 [36.8; 48.5] | 39.0 [35.25; 44.25] | 41.0 [38.5; 43.5] | 46.0 [40.5; 48.0] |
p 1.5=0.13 p2.6=0.17 p 3.7=0.96 p 4.8=0.28 |
p 1.2=0.34 p 1.3=0.38 p 1.4=0.25 p 2.3=0.31 p 2.4=0.25 p 3.4=0.21 |
p 5.6=0.007 p 5.7=0.17 p 5.8=0.23 p 6.7=0.58 p 6.8=0.08 p 7.8=0.005 |
| TAPSE, cm | 1.6 [1.5; 1.9] |
1.3 [1.1; 1.5] | 1.5 [1.1; 1.65] |
1.5 [1.2; 1.7] |
2.0 [1.7; 2.3] |
1.5 [1.3; 1.6] |
1.4 [1.2; 1.72] |
1.65 [1.5; 1.9] |
p 1.5=0.02 p 2.6=0.16 p 3.7=0.86 p 4.8=0.12 |
p 1.2=0.02 p 1.3=0.04 p 1.4=0.23 p 2.3=0.21 p 2.4=0.17 p 3.4=0.73 |
p 5.6=0.0001 p 5.7=0.0002 p 5.8=0.009 p 6.7=0.004 p 6.8=0.004 p 7.8=0.002 |
| ePASP, mmHg | 50.0 [41.0; 61.25] | 33.0 [25.75; 40.5] | 33.0 [28.75; 38.5] | 33.0 [26.5; 42.5] | 42.0 [31.0; 60.0] | 28.0 [24.0; 31.0] |
28.0 [22; 30.0] |
29.0 [24; 34.5] |
p1.5=0.45 p 2.6=0.13 p 3.7=0.047 p 4.8=0.43 |
p 1.2=0.0005 p 1.3=0.001 p 1.4=0.008 p 2.3=0.75 p 2.4=0.96 p 3.4=0.48 |
p 5.6<0.0001 p 5.7=0.0001 p 5.8=0.0008 p 6.7=0.44 p 6.8=0.06 p 7.8=0.19 |
| RV-PA coupling, mm/mmHg | 0.32 [0.26; 0.49] | 0.37 [0.33; 0.46] | 0.37 [0.35; 0.52] | 0.39 [0.32; 0.60] | 0.42 [0.3; 0.63] |
0.5 [0.42; 0.65] |
0.52 [0.4; 0.65] |
0.55 [0.41; 0.71] |
p 1.5=0.18 p 2.6=0.02 p 3.7=0.09 p 4.8=0.24 |
p 1.2=0.02 p 1.3=0.19 p 1.4=0.02 p 2.3=0.31 p 2.4=0.63 p 3.4=0.58 |
p 5.6=1.0 p 5.7=0.67 p 5.8=0.22 p 6.7=0.47 p 6.8=0.19 p 7.8=0.26 |
| RV free wall global longitudinal strain, % | - 17.0 [- 23.3; - 13.47] |
-12.55 [- 15.4; - 10.6] | - 15.55 [- 16.8; - 13.65] | - 15.1 [-19.17; - 13.92] |
- 18.55 [- 24.3; -16] |
-16.9 [- 18.8; - 14.0] |
- 17.25 [- 19.9; - 16.5] |
17.9 [-22.22; - 15.47] |
p 1.5=0.29 p 2.6=0.15 p 3.7=0.08 p 4.8=0.09 |
p 1.2=0.80 p 1.3=0.69 p 1.4=0.33 p 2.3=0.30 p 2.4=0.43 p 3.4=0.56 |
p 5.6=0.0006 p 5.7=0.09 p 5.8=0.12 p 6.7=0.14 p 6.8=0.70 p 7.8=0.71 |
| RVEDV, ml 3D Echo |
116.0 [60.5; 121.25] | 129.0 [113.0; 138.75] | 128 [87.25; 135] | 136.0 [118.0; 167.0] | 96.5 [74; 122.5] | 96.0 [81.5; 109.75] | 86.5 [75; 117] | 129.5 [112.0; 153.0] |
p 1.5=0.87 p 2.6=0.03 p 3.7=0.04 p 4.8=0.77 |
p 1.2= - p 1.3= - p 1.4=0.31 p 2.3=0.68 p 2.4=1.0 p 3.4=0.63 |
p 5.6=0.11 p 5.7=0.28 p 5.8=0.13 p 6.7=0.10 p 6.8=0.01 p 7.8=0.01 |
| RVESV, ml 3D Echo |
59.0 [36; 67.5] | 76.0 [56.75; 83.25] | 70.0 [41.75; 83] | 73.0 [61.0; 100.0] | 52.5 [41.5; 64.5] | 53.5 [43.0; 87.0] | 47.5 [35; 69] | 67.0 [53.0; 87.0] |
p 1.5=0.85 p 2.6=0.04 p3.7=0.19 p 4.8=0.46 |
p 1.2= - p 1.3= - p 1.4= 0.44 p 2.3=0.13 p 2.4=0.38 p 3.4= - |
p 5.6=0.39 p 5.7=0.21 p 5.8=0.23 p 6.7=0.28 p 6.8=0.08 p 7.8=0.06 |
| RVSV, ml 3D Echo |
50.0 [31.75; 55] | 48.0 [42.25; 59.5] | 55.0 [44.25; 56.75] | 59.0 [51.0; 76.0] | 42.0 [37.5; 62] | 46.0 [36.25; 50.75] | 37.5 [34; 48] | 66.0 [59.25; 77.75] |
p 1.5=0.55 p 2.6=0.45 p 3.7=0.04 p 4.8=0.43 |
p 1.2= - p 1.3= - p 1.4=0.06 p 2.3=0.13 p 2.4=0.25 p 3.4=1.0 |
p 5.6=0.15 p 5.7=0.33 p 5.8=0.10 p 6.7=0.06 p 6.8=0.004 p 7.8=0.003 |
| RVEF, % 3D Echo |
46.0 [37; 47.75] | 38.0 [35.25; 40.5] | 45.0 [35.75; 45.75] | 47.0 [42; 50] | 48.5 [43; 54] | 45.0 [38.5; 48.75] | 46.0 [42; 49] | 49.0 [44; 53] |
p 1.5=0.09 p 2.6=0.12 p 3.7=0.25 p 4.8=0.27 |
p 1.2= - p 1.3= - p 1.4=0.50 p 2.3=0.81 p 2.4=0.13 p 3.4=0.12 |
p 5.6= 0.005 p 5.7=0.05 p 5.8=0.61 p 6.7=0.91 p 6.8=0.04 p 7.8=0.04 |
| Severity of tricuspid insufficiency, n (%) | |||||||||||
| Grade I | 18 (29.0) |
29 (46.8) |
21 (33.9) |
33 (55.0) |
46 (53.5) |
60 (69.76) |
58 (67.44) |
49 (57.0) |
p 1.5=0.01 p 2.6=0.16 p 3.7=0.04 p 4.8=1.0 |
- | - |
| Grade II | 25 (40.32) |
11 (17.74) |
11 (17.74) |
3 (5) |
10 (11.6) |
14 (16.3) |
5 (5.8) |
10 (11.6) |
p 1.5=0.01 p 2.6=0.75 p 3.7=0.15 p 4.8=0.13 |
- | - |
| Grade III | 7 (11.3) |
4 (6.45) |
3 (4.4) |
5 (8.33) |
16 (18.6) |
0 (0) | 0 (0) | 0 (0) |
p 1.5=0.61 p 2.6=0.15 p 4.8=0.04 |
- | - |
| Grade IV | 4 (6.45) | 0 (0) | 0 (0) | 0 (0.0) | 3 (3.5) | 0 (0) | 0 (0) | 0 (0) |
p 1.5=0.48 p 4.8=0.82 |
- | - |
Note: GLS — global longitudinal strain; PAP — pulmonary artery pressure; PA — pulmonary artery; LV — left ventricle; LA — left atrium; EDV — end-diastolic volume; ESV — end-systolic volume; EDD — end-diastolic diameter; ESD — end-systolic diameter; MV — mitral valve; RV — right ventricle; RA — right atrium; PASP — pulmonary artery systolic pressure; TV — tricuspid valve; EF — ejection fraction; and TTE/Echo — transthoracic echocardiography.
Table 4.
Causes of readmission and functional status in patients during the one-year follow-up after MV correction, stratified by the presence of preoperative epicardial obesity (EAT volume >115.1 cm3) assessed by multidetector computed tomography.
Table 4.
Causes of readmission and functional status in patients during the one-year follow-up after MV correction, stratified by the presence of preoperative epicardial obesity (EAT volume >115.1 cm3) assessed by multidetector computed tomography.
| Parameter | Patients with MV disease | p | |
| with EO (n=62) | without EO (n=86) | ||
| Hospitalizations for CHF decompensation, n (%) | 11 (17.74) | 0 (0) | 0.0152 |
| Arrhythmia-related hospitalizations, n (%) | 7 (11.3) | 0 (0) | 0.0499 |
| MV mechanical prosthesis dysfunction and re-operation, n (%) | 0 (0) | 1 (1.6) | 0.2568 |
| Death, n (%) | 2 (3.2) | 0 (0) | 0.1905 |
| CHF functional class (NYHA), n (%) I II III IV |
in 60 patients 32 (53.33) 22 (36.66) 3 (5) 3 (5) |
56 (65.1) 27 (31.4) 3 (3.5) 0 (0) |
0.39060.77610.7418 0.1901 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



