Submitted:
18 June 2026
Posted:
22 June 2026
You are already at the latest version
Abstract
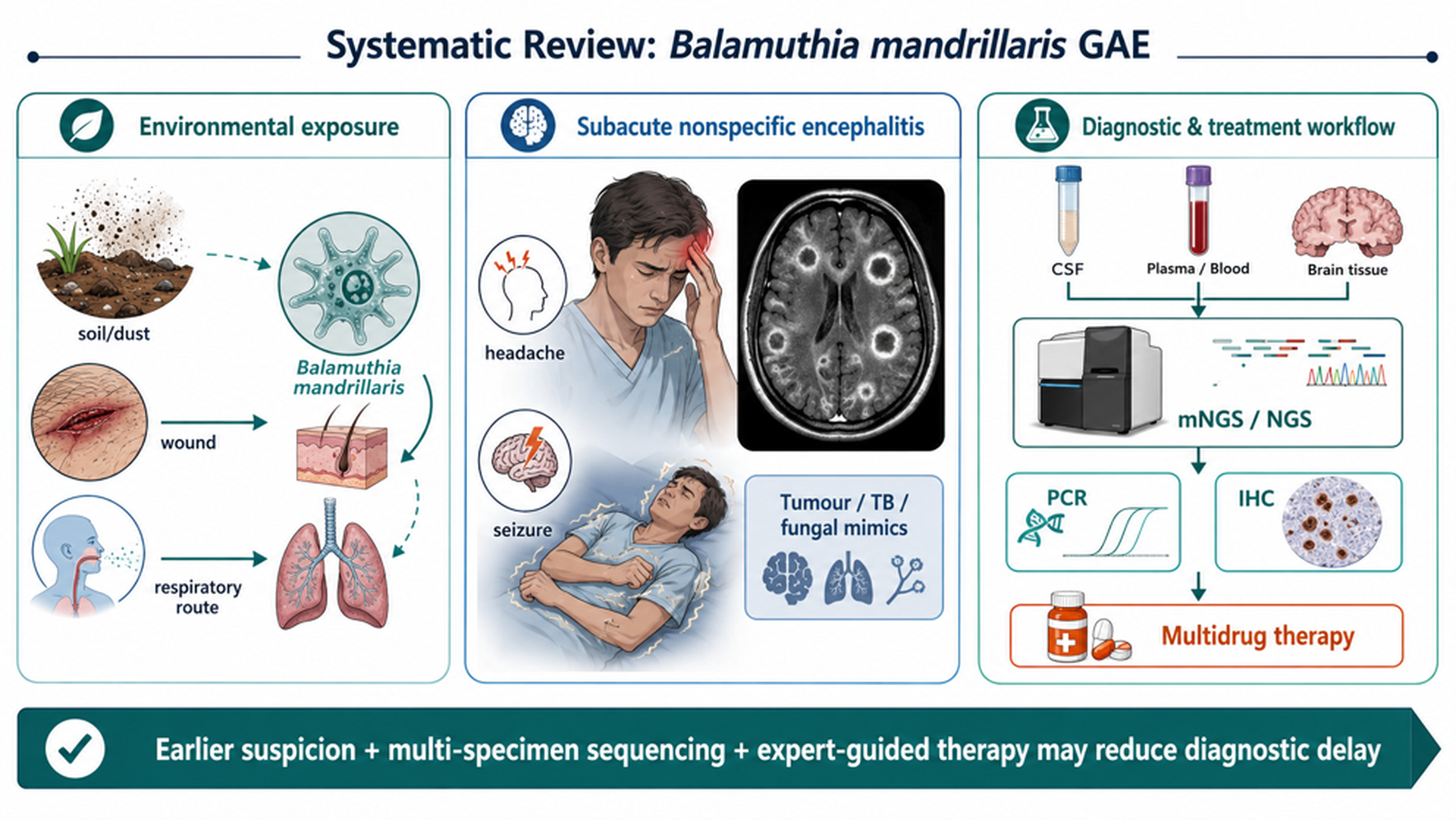
Background and Objectives: Balamuthia mandrillaris granulomatous amoebic encephalitis (GAE) is a rare, frequently fatal central nervous system infection in which delayed recognition remains a major determinant of outcome. The increasing use of metagenomic next-generation sequencing (mNGS), plasma microbial cell-free DNA sequencing and targeted sequencing has changed the diagnostic pathway for unexplained encephalitis, but the survival implications of earlier molecular diagnosis remain unclear. Materials and Methods: A systematic review of peer-reviewed reports published from January 2015 to June 2026 was designed according to PRISMA 2020. Eligible records reported human B. mandrillaris GAE, encephalitis, meningoencephalitis or encephalomyelitis with extractable patient-level diagnostic, treatment or outcome information. Data were narratively synthesised because case definitions, sample types, timing of testing and follow-up were heterogeneous. Results: The evidence base consisted mainly of case reports, small case series and retrospective clinical summaries. Across recent reports, B. mandrillaris GAE commonly mimicked malignancy, tuberculosis, fungal infection, autoimmune encephalitis or bacterial brain abscess. Diagnostic delay was driven by nonspecific symptoms, ring-enhancing lesions, negative routine cultures and limited clinician familiarity with free-living amoebae. Molecular methods, particularly mNGS/NGS applied to cerebrospinal fluid, plasma, blood, brain tissue or bronchoalveolar lavage fluid, repeatedly enabled antemortem diagnosis when routine tests were unrevealing. Survival reports shared a pattern of earlier tissue diagnosis or molecular identification, neurosurgical intervention when feasible, and prolonged multidrug therapy, sometimes including miltefosine or nitroxoline. Conclusions: B. mandrillaris GAE should be considered in subacute encephalitis with mass-like or multifocal enhancing lesions and negative conventional investigations. Early biopsy or non-invasive sequencing, followed by confirmatory testing and expert-guided combination therapy, represents the most actionable strategy to reduce diagnostic delay.
Keywords:
Balamuthia mandrillaris
; granulomatous amoebic encephalitis
; metagenomic next-generation sequencing
; mNGS
; diagnostic delay
; survival
; case reports
; PRISMA
1. Introduction
Balamuthia mandrillaris is an environmentally free-living amoeba capable of causing cutaneous disease and devastating central nervous system infection. Unlike Naegleria fowleri primary amoebic meningoencephalitis, B. mandrillaris GAE usually evolves subacutely or chronically, often over weeks to months, and can affect immunocompetent as well as immunocompromised hosts [1,2]. The disease remains highly publishable and clinically important because it is rare, has a very high case-fatality rate, and continues to be recognised late in the diagnostic pathway. The proposed sequence from environmental exposure through cutaneous or respiratory entry, haematogenous dissemination, blood-brain barrier traversal and granulomatous central nervous system injury is summarised in Figure 1.
Recent epidemiological work from the United States and China has shown that Balamuthia disease is not confined to a single region or host profile, and that encephalitis accounts for the dominant life-threatening syndrome [2,3]. More recent reports from Asia, Africa, Europe and the Americas emphasise a shared clinical problem: patients are frequently investigated for tumour, tuberculosis, fungal infection, autoimmune disease, bacterial abscess or viral encephalitis before free-living amoebae are considered in the differential diagnosis [4,5,6,7,8,9,10,11]. This delay matters because the number of documented survivors remains small and survival appear linked to earlier recognition, surgical source control where possible, and sustained multidrug therapy [12,13,14,15].
The diagnostic landscape has changed since the first reports of metagenomic deep sequencing identifying B. mandrillaris in cerebrospinal fluid and tissue [16]. Subsequent reports have described next-generation sequencing of cerebrospinal fluid, plasma microbial cell-free DNA, blood, brain tissue and other specimens [4,8,17,18,19,20,21,22]. These studies suggest that unbiased or targeted sequencing may shorten the route to aetiological diagnosis, particularly when cultures are negative and histopathology is initially interpreted as nonspecific granulomatous inflammation. However, molecular testing cannot be interpreted in isolation; confirmatory polymerase chain reaction (PCR), immunohistochemistry, serology, tissue morphology, read-depth metrics and clinical plausibility remain essential to avoid over- or under-diagnosis.
The purpose of this systematic review was to synthesise the modern case-report literature from 2015 to 2026 on diagnostic delay, mNGS/NGS use and survival outcomes in B. mandrillaris GAE. The review was designed for a rare-disease evidence base in which randomised trials are absent and the most informative data comes from carefully reported individual cases, small series and national retrospective summaries.
2. Materials and Methods
This systematic review was planned and reported in accordance with PRISMA 2020. The review question was: among patients with confirmed B. mandrillaris GAE or related central nervous system infection, how are diagnostic delay, molecular diagnostic methods and survival outcomes reported in global case reports and case series published from 2015 to 2026?
Eligibility criteria followed a PECO-style framework. The population comprised human patients of any age with B. mandrillaris encephalitis, meningoencephalitis, encephalomyelitis, cerebral abscess, central nervous system vasculitis or granulomatous amoebic encephalitis. The exposure or index diagnostic feature was the method and timing of diagnosis, including histopathology, PCR, immunohistochemistry, serology, culture, mNGS, next-generation sequencing, plasma microbial cell-free DNA sequencing or targeted sequencing. Comparators were not required because the evidence base consists mainly of uncontrolled cases. Outcomes included diagnostic delay, first suspected diagnosis, specimen type, treatment regimen, neurosurgical intervention, survival, death and follow-up status.
Searches were designed for PubMed/MEDLINE, Scopus, Web of Science, Embase, DOAJ/Crossref and citation searching. The core search string was: (Balamuthia mandrillaris OR Balamuthia) AND (granulomatous amoebic encephalitis OR granulomatous amebic encephalitis OR encephalitis OR meningoencephalitis OR encephalomyelitis OR cerebral abscess) AND (metagenomic OR next-generation sequencing OR NGS OR mNGS OR PCR OR diagnosis OR survival OR outcome). Search was limited to January 2015 to June 2026, humans, and peer-reviewed articles with patient-level information. Non-English reports were eligible if an English abstract or full translation allowed extraction of the required variables.
Records were excluded if they involved only environmental isolation, animal infection, laboratory-only drug testing without human clinical data, cutaneous disease without central nervous system involvement, non-peer-reviewed abstracts without a citable DOI, review articles without new patient-level data, or duplicate reports of the same case. When a case report and a later cohort summary appeared to describe the same patient, the most detailed patient-level report was prioritised for extraction, and the broader cohort was used only for context.
Screening and extraction were organised using a predefined extraction framework that captured age, sex, country, immune status, suspected route of acquisition, initial symptoms, neuroimaging pattern, first working diagnosis, time from symptom onset to diagnosis, diagnostic tests, specimen type, mNGS/NGS platform where reported, confirmatory testing, treatment, neurosurgical intervention and outcome. Methodological quality was assessed using the JBI Critical Appraisal Checklist for Case Reports and the JBI tool for case series, with appraisal informing interpretation rather than automatic exclusion [23].
Generative artificial intelligence was used only to prepare initial visual drafts of the graphical abstract and conceptual schematics. No generative AI tool was used to identify, screen, extract, analyse or interpret eligible studies. All visual content was manually reviewed against the cited literature and edited by the authors.
Because case reports differ substantially in timing definitions and outcome follow-up, meta-analysis was not planned. Findings were synthesised narratively around four domains: sources of diagnostic delay; diagnostic contribution of mNGS/NGS; survival-associated clinical features; and implications for a practical diagnostic algorithm. The review framework and key eligibility decisions are summarised in Table 1.
3. Results
The PRISMA flow diagram is shown in Figure 2. The evidence base was dominated by individual case reports and small series, with a smaller number of national or regional retrospective summaries. Representative recent patient-level reports and diagnostic themes are summarised in Table 2. This distribution is expected for a rare, high-fatality infection in which prospective comparative studies are not available.
Across reports, the most consistent reason for delay was the absence of a pathognomonic early syndrome. Patients presented with headache, fever, seizures, altered mental status, cranial neuropathies, visual disturbance, gait problems or focal weakness. Cerebrospinal fluid findings were often inflammatory but nonspecific, while neuroimaging frequently showed mass-like, multifocal, ring-enhancing, necrotic or haemorrhagic lesions. These features produced repeated diagnostic confusion with glioma, metastasis, lymphoma, tuberculosis, fungal disease, pyogenic abscess, viral encephalitis, demyelinating disease and autoimmune encephalitis [5,7,9,10,11,18,21,24]. The resulting diagnostic-delay pathway is summarised in Figure 3.
Histopathology remained pivotal, particularly in reports where open biopsy or resection revealed granulomatous necrosis, trophozoites or cyst-like structures. However, pathology alone was not always sufficient at first review because organisms may be sparse and granulomatous inflammation may be attributed to tuberculosis, fungi, sarcoidosis or neoplasia. Several reports showed that retrospective re-review of earlier tissue could identify organisms after molecular confirmation, demonstrating that diagnostic delay can occur even after biopsy when the clinical suspicion is low [7,11,13].
mNGS/NGS substantially changed the diagnostic pathway in recent cases. Wilson et al. showed the feasibility of metagenomic deep sequencing for B. mandrillaris encephalitis, and later reports demonstrated detection from cerebrospinal fluid, brain tissue, plasma microbial cell-free DNA, blood and other specimens [16,17,18,19,20,21,22]. In difficult cases, sequencing provided a route to diagnosis when standard cultures, stains, bacterial and viral assays were negative. Reports also suggested that sequencing performance depends on specimen choice, pathogen burden, timing, read-depth thresholds and bioinformatic reference databases. A practical sequencing workflow for suspected rare amoebic encephalitis is presented in Figure 4.
Plasma microbial cell-free DNA sequencing is clinically attractive because it is less invasive than brain biopsy and may detect pathogens when cerebrospinal fluid testing is negative or unavailable. Kalyatanda et al. reported rapid non-invasive diagnosis using plasma-based next-generation sequencing, and Edminster et al. later described a fatal case where plasma sequencing identified B. mandrillaris despite negative cerebrospinal fluid mNGS at the time of care, with retrospective analysis clarifying the diagnostic signal [18,22]. These cases support a multi-specimen strategy when suspicion remains high.
Survival was uncommon but repeatedly associated with a combination of factors: diagnosis before irreversible neurological decline, neurosurgical resection or decompression when feasible, early consultation with reference laboratories or public-health experts, and prolonged multidrug therapy. Surviving reports described combinations including azithromycin or clarithromycin, fluconazole, flucytosine, pentamidine, sulfadiazine or trimethoprim-sulfamethoxazole, miltefosine and, in a notable recent survivor, nitroxoline [12,13,14,15]. These observations do not establish causality, but they identify a practical window for aggressive diagnosis and treatment.
The most recent literature also expands the diagnostic horizon beyond standard shotgun mNGS. Targeted sequencing approaches such as MetaCAP have been evaluated against mNGS in a 2026 report that also described a B. mandrillaris and Epstein-Barr virus co-infective encephalitis and a retrospective landscape of 41 Chinese cases [24]. This emerging evidence suggests that broader sequencing workflows may increase diagnostic yield, although validation across independent laboratories is still limited.
4. Discussion
This systematic review highlights a central clinical message: B. mandrillaris GAE is not only rare, but diagnostically deceptive. The infection often appears in exactly the clinical spaces where clinicians must act quickly but evidence is incomplete: unexplained encephalitis, mass-like brain lesions, negative cultures, granulomatous pathology and deteriorating neurological status. In this context, the delay is not a single missed test but a cascade of low pre-test suspicion, nonspecific imaging, limited access to confirmatory assays and uncertainty about when to escalate to advanced diagnostics.
mNGS should be understood as an accelerant rather than a replacement for conventional methods. Sequencing can generate an actionable organism signal when routine assays fail, but the result needs confirmation and clinical integration. Balamuthia read counts, genome coverage, sample contamination controls, host background, specimen type and the presence of plausible pathology all influence interpretation. This is especially important for rare organisms where false reassurance from a negative cerebrospinal fluid test may be dangerous if brain tissue or plasma contains detectable pathogen nucleic acid.
The reviewed cases support a tiered diagnostic approach. First, clinicians should consider free-living amoebae when subacute encephalitis is accompanied by ring-enhancing or mass-like lesions, skin plaques, granulomatous inflammation, negative routine microbiology or apparent tumour progression despite steroids or antibacterial treatment. Second, early tissue sampling should be considered when neuroimaging suggests a focal lesion and the risk-benefit profile is acceptable. Third, mNGS/NGS should be requested from the most informative available specimen rather than restricted to cerebrospinal fluid alone. Fourth, positive sequencing should prompt confirmatory PCR, immunohistochemistry, serology or expert reference-laboratory review. This review-derived pathway is consolidated into the proposed clinical diagnostic algorithm shown in Figure 5.
The survival literature remains too sparse for definitive treatment recommendations. Nonetheless, the pattern across survivors is clinically instructive. Cases with survival commonly involve earlier diagnosis, surgical intervention, and multidrug regimens sustained for long periods. Miltefosine has become an important component in many reported regimens, although access barriers remain. Nitroxoline is particularly notable because functional drug-screening work identified activity against B. mandrillaris, and subsequent clinical use in a survivor has renewed interest in drug repurposing [14,25]. The contrast between fatal and survivor trajectories is illustrated in Figure 6. These signals justify stronger international case registries and collaborative therapeutic evaluation.
Several limitations must be acknowledged. The evidence base is vulnerable to publication bias because unusual survivors and diagnostically novel cases are more likely to be reported than rapidly fatal undiagnosed infections. Reported diagnostic delay is difficult to pool because onset, first medical contact, first imaging, first biopsy, first positive molecular test and final diagnosis are not consistently defined. Retrospective national summaries may overlap with individual case reports. In addition, sequencing methods are not standardised across laboratories, and negative results are less commonly published than positive cases.
Despite these limitations, the findings are immediately relevant to clinical practice. The threshold for including B. mandrillaris in the differential diagnosis should be lower when encephalitis is subacute, imaging is mass-like or multifocal, routine tests are negative and pathology suggests granulomatous inflammation. A practical diagnostic bundle should include early infectious diseases and neurology input, targeted history for soil/dust/wound exposure and skin lesions, broad specimen collection, mNGS/NGS when routine tests fail, and early contact with specialist reference laboratories.
5. Conclusions
Balamuthia mandrillaris GAE remains a rare but highly fatal infection in which diagnostic delay is the key modifiable problem. Modern molecular diagnostics, especially mNGS/NGS of cerebrospinal fluid, plasma, blood or tissue, can shorten the time to aetiological diagnosis, but only if clinicians suspect the disease early enough to request testing and interpret results in the context of pathology and imaging. Reports of survival indicate that early diagnosis, neurosurgical intervention when feasible and prolonged expert-guided multidrug therapy may improve outcomes. Future work should prioritise a global registry, harmonised reporting of diagnostic timelines, standardised sequencing interpretation and collaborative evaluation of candidate therapies such as miltefosine-containing regimens and nitroxoline.
Author Contributions
Conceptualisation, A.I., B.F., H.K. and H.M.; methodology, A.I., B.F., H.K. and H.M.; screening and data extraction, A.I., B.F., H.K. and H.M.; formal analysis, A.I., B.F., H.K. and H.M.; visualisation, A.I., B.F., H.K. and H.M.; writing—original draft preparation, A.I., B.F., H.K. and H.M.; writing—review and editing, A.I., B.F., H.K. and H.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable because this systematic review used previously published data only.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data analysed in this systematic review were extracted from previously published studies cited in the reference list. The search strategy, eligibility framework and study-selection process are reported within the manuscript and PRISMA flow diagram.
Acknowledgments
The authors acknowledge the contribution of clinicians, microbiologists and reference laboratories whose case reports have improved recognition of this rare infection. During preparation of this manuscript, the authors used OpenAI's ChatGPT image-generation tool to create initial drafts of the graphical abstract and conceptual figures. The authors reviewed and edited the outputs and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Schafer, K.R.; Shah, N.; Almira-Suarez, M.I.; Reese, J.M.; Hoke, G.M.; Mandell, J.W.; Roy, S.L.; Visvesvara, G. Disseminated Balamuthia mandrillaris Infection. J. Clin. Microbiol. 2015, 53, 3072–3076. [Google Scholar] [CrossRef] [PubMed]
- Cope, J.R.; Landa, J.; Nethercut, H.; Collier, S.A.; Glaser, C.; Moser, M.; Puttagunta, R.; Yoder, J.S.; Ali, I.K.M.; Roy, S.L. The Epidemiology and Clinical Features of Balamuthia mandrillaris Disease in the United States, 1974-2016. Clin. Infect. Dis. 2019, 68, 1815–1822. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, B.; Zhao, T.; Wang, L.; Jian, Z.; Cheng, W.; Chen, J.; Li, C.; Wang, G.; Gao, T. Balamuthia mandrillaris infection in China. Emerg. Microbes Infect. 2020, 9, 2348–2357. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Li, G.; et al. Diagnosing Balamuthia mandrillaris encephalitis via next-generation sequencing. Emerg. Microbes Infect. 2020, 9, 1379–1387. [Google Scholar] [CrossRef] [PubMed]
- Kum, S.J.; Lee, H.W.; Jung, H.R.; Choe, M.; Kim, S.P. Amoebic Encephalitis Caused by Balamuthia mandrillaris. J. Pathol. Transl. Med. 2019, 53, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Piper, K.J.; Foster, H.; Susanto, D.; Maree, C.L.; Thornton, S.D.; Cobbs, C.S. Fatal Balamuthia mandrillaris brain infection associated with improper nasal lavage. Int. J. Infect. Dis. 2018, 77, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Yohannan, B.; Feldman, M. Fatal Balamuthia mandrillaris Encephalitis. Case Rep. Infect. Dis. 2019, 2019, 9315756. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, W.; Li, Y.; Ma, F.; Li, G. A case report of Balamuthia mandrillaris encephalitis. Heliyon 2024, 10, e26905. [Google Scholar] [CrossRef] [PubMed]
- Javed, Z.; Hussain, M.M.; Ghanchi, N.; Gilani, A.; Enam, S.A. Non-granulomatous meningoencephalitis with Balamuthia mandrillaris mimicking a tumor: First confirmed case from Pakistan. Surg. Neurol. Int. 2024, 15, 238. [Google Scholar] [CrossRef] [PubMed]
- Safavi, M.; Mehrtash, V.; Habibi, Z.; Mohammadpour, M.; Haghi Ashtiani, M.T.; Sotoudeh Anvari, M.; Zaresharifi, N.; Shafizadeh, M.; Jafarzadeh, B. Case Report: Encephalitis Caused by Balamuthia mandrillaris in a 3-Year-Old Iranian Girl. Am. J. Trop. Med. Hyg. 2021, 104, 1836–1840. [Google Scholar] [CrossRef] [PubMed]
- Paudel, A.C.; Patel, N.; Quang, J.; Casella, C.; Sigal, A.; Parajuli, P.; Oladunjoye, O.; Oke, I.O.; Khanal, S.; Bhattarai, K. Rapidly Progressive Granulomatous Amoebic Encephalitis in a Diabetic Individual. Cureus 2021, 13, e19336. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, M.E.; Glaser, C. A Balamuthia survivor. JMM Case Rep. 2016, 3, e005031. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Zhou, Q.; Wu, Y.; Cao, X.; Lv, Z.; Su, M.; Yu, Y.; Huang, W. A patient with granulomatous amoebic encephalitis caused by Balamuthia mandrillaris survived with two excisions and medication. BMC Infect. Dis. 2022, 22, 54. [Google Scholar] [CrossRef] [PubMed]
- Spottiswoode, N.; Pet, D.; Kim, A.; Gruenberg, K.; Shah, M.; Ramachandran, A.; Laurie, M.T.; Zia, M.; Fouassier, C.; Boutros, C.; Lu, R.; Zhang, Y.; Servellita, V.; Bollen, A.; Chiu, C.Y.; Wilson, M.R.; Valdivia, L.; DeRisi, J.L. Successful Treatment of Balamuthia mandrillaris Granulomatous Amebic Encephalitis with Nitroxoline. Emerg. Infect. Dis. 2023, 29, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Cuoco, J.A.; McMahon, A.; et al. Successful Treatment of a Balamuthia mandrillaris Cerebral Abscess in a 4-Year-Old Child. Pediatr. Infect. Dis. J. 2022, 41, e72–e75. [Google Scholar] [CrossRef]
- Wilson, M.R.; O'Donovan, B.D.; Gelfand, J.M.; Sample, H.A.; Chow, F.C.; Betjemann, J.P.; Shah, M.P.; Richie, M.B.; Gorman, M.P.; Hajj-Ali, R.A.; Calabrese, L.H.; DeRisi, J.L.; Greenlee, J.E. Chronic meningitis investigated via metagenomic next-generation sequencing. JAMA Neurol. 2018, 75, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Greninger, A.L.; Messacar, K.; Dunnebacke, T.; Naccache, S.N.; Federman, S.; Bouquet, J.; et al. Clinical metagenomic identification of Balamuthia mandrillaris encephalitis and assembly of the draft genome. Genome Med. 2015, 7, 113. [Google Scholar] [CrossRef] [PubMed]
- Kalyatanda, G.; Rand, K.; Lindner, M.S.; Hong, D.K.; Albayram, M.S.; Gregory, J.; Kresak, J.; Ibne, K.M.A.; Cope, J.R.; Roy, S.; et al. Rapid, Noninvasive Diagnosis of Balamuthia mandrillaris Encephalitis by a Plasma-Based Next-Generation Sequencing Test. Open Forum Infect. Dis. 2020, 7, ofaa189. [Google Scholar] [CrossRef] [PubMed]
- Hirakata, S.; Sakiyama, Y.; Yoshimura, A.; Ikeda, M.; Takahata, K.; Tashiro, Y.; Yoshimura, M.; Arata, H.; Yonezawa, H.; Kirishima, M.; et al. The application of shotgun metagenomics to the diagnosis of granulomatous amoebic encephalitis due to Balamuthia mandrillaris: a case report. BMC Neurol. 2021, 21, 392. [Google Scholar] [CrossRef] [PubMed]
- Yi, Z.; Zhong, J.; Wu, H.; Li, X.; Chen, Y.; Chen, H.; Yang, Y.; Yu, X. Balamuthia mandrillaris encephalitis in a child: case report and literature review. Diagn. Microbiol. Infect. Dis. 2021, 100, 115180. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Hu, X.; Min, L.; Dong, X.; Guan, Y. Balamuthia mandrillaris-related primary amoebic encephalitis in China diagnosed by next generation sequencing and a review of the literature. Lab. Med. 2020, 51, e20–e26. [Google Scholar] [CrossRef] [PubMed]
- Edminster, S.Y.; Rebbe, R.W.; Khatchadourian, C.; Hurth, K.M.; Mathew, A.J.; Huss-Bawab, J.; Shiroishi, M.S.; Clark, D.; Norgan, A.P.; Butler-Wu, S.M.; Hiniker, A. The role of plasma metagenomic sequencing in identification of Balamuthia mandrillaris encephalitis. Acta Neuropathol. Commun. 2025, 13, 61. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; Mu, P.F. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Zhao, Y.; He, X.; Han, Z.; Guo, F.; Xie, F.; Lin, Z.; Chen, L.; Song, X.; Luo, W.; Liu, F.; et al. Balamuthia mandrillaris-EBV co-infective encephalitis diagnosed by MetaCAP: comparative mNGS validation and epidemiological landscape from 41 Chinese cases. Int. J. Infect. Dis. 2026, 163, 108302. [Google Scholar] [CrossRef] [PubMed]
- Laurie, M.T.; White, C.V.; Retallack, H.; Wu, W.; Moser, M.S.; Sakanari, J.A.; Ang, K.; Wilson, C.; Arkin, M.R.; DeRisi, J.L.; Bassler, B.L. Functional Assessment of 2177 U.S. and International Drugs Identifies the Quinoline Nitroxoline as a Potent Amoebicidal Agent against Balamuthia mandrillaris. mBio 2018, 9, e02051-18. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; et al. A clinical case report of Balamuthia granulomatous amoebic encephalitis in a non-immunocompromised patient and literature review. BMC Infect. Dis. 2023, 23, 283. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.M.; Chen, T.; Yang, H.; Gao, Y.; Chen, Y. Encephalomyelomeningitis Caused by Balamuthia mandrillaris: A Case Report and Literature Review. Infect. Drug Resist. 2023, 16, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Yao, S.; Chen, X.; Qian, L.; Sun, S.; Zhao, C.; Bai, Z.; Chen, Z.; Wu, Y. Diagnosing Balamuthia mandrillaris amebic meningoencephalitis in a 64-year-old woman from Southwest China. Parasites Hosts Dis. 2023, 61, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Wang, D.; Cui, K.; Wan, R.; Chi, Q.; Wu, T. 18F-FDG PET/CT findings in fatal Balamuthia mandrillaris encephalitis in brain stem: A case report. Radiol. Case Rep. 2024, 19, 1851–1854. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Chen, F.; Qin, L.; Lu, A.; Xu, H.; Zhao, M.; Zhao, Y. Application of ventriculoscopy in granulomatous amoebic encephalitis: a case report in China and literature review. Front. Med. 2024, 11, 1431225. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Liu, Y.; Chen, Z.; Sun, J.; Zhang, X.; Wang, Y. Balamuthia amoebic encephalitis directly causing intracranial infection: A case report. Radiol. Case Rep. 2025, 20, 2820–2824. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; et al. Next-Generation Sequencing for Diagnosis of Fatal Balamuthia Amoebic Encephalitis: A Case Report. Diagnostics 2025, 15, 2590. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Xu, W. A Case Report of Balamuthia mandrillaris Encephalitis: Experience from Central China. Neurosurg. Subspec. 2025, 1, 44–47. [Google Scholar] [CrossRef]
- Teng, Z.; Liu, L.; Chen, T.; Liang, J.; Yao, X.; Zhao, N.; Zhao, F.; Sun, H.; Wang, L.; Wang, Q.; Liu, G.; Qin, T. A Novel Balamuthia Lineage Causing Fatal Granulomatous Amoebic Encephalitis in an Immunocompetent Infant. Int. J. Infect. Dis. 2025, 161, 108063. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Conceptual pathogenesis of B. mandrillaris granulomatous amoebic encephalitis. Environmental exposure may be followed by entry via disrupted skin or the respiratory route, haematogenous dissemination, traversal of the blood-brain barrier, and granulomatous central nervous system injury. The schematic is a review-derived conceptual synthesis and does not establish the relative frequency of individual exposure or entry routes.
Figure 1.
Conceptual pathogenesis of B. mandrillaris granulomatous amoebic encephalitis. Environmental exposure may be followed by entry via disrupted skin or the respiratory route, haematogenous dissemination, traversal of the blood-brain barrier, and granulomatous central nervous system injury. The schematic is a review-derived conceptual synthesis and does not establish the relative frequency of individual exposure or entry routes.

Figure 2.
PRISMA 2020 flow diagram for the search and selection process. The diagram summarises database/register searches and additional-source screening, including websites, organisations and citation searching.
Figure 2.
PRISMA 2020 flow diagram for the search and selection process. The diagram summarises database/register searches and additional-source screening, including websites, organisations and citation searching.

Figure 3.
Conceptual diagnostic-delay pathway for B. mandrillaris GAE, showing how nonspecific presentation and common diagnostic traps can delay molecular confirmation and treatment.
Figure 3.
Conceptual diagnostic-delay pathway for B. mandrillaris GAE, showing how nonspecific presentation and common diagnostic traps can delay molecular confirmation and treatment.

Figure 4.
mNGS/NGS workflow for suspected rare amoebic encephalitis. Interpretation should combine sequencing evidence with neuroimaging, pathology, negative routine microbiology and expert reference-laboratory confirmation.
Figure 4.
mNGS/NGS workflow for suspected rare amoebic encephalitis. Interpretation should combine sequencing evidence with neuroimaging, pathology, negative routine microbiology and expert reference-laboratory confirmation.

Figure 5.
Proposed clinical diagnostic algorithm for suspected B. mandrillaris GAE. In patients with subacute encephalitis, mass-like or ring-enhancing lesions, or unexplained granulomatous pathology, negative or non-diagnostic routine investigations should prompt multi-specimen sampling, molecular testing and specialist reference-laboratory confirmation. The algorithm is a review-derived clinical framework and has not been prospectively validated as a decision rule.
Figure 5.
Proposed clinical diagnostic algorithm for suspected B. mandrillaris GAE. In patients with subacute encephalitis, mass-like or ring-enhancing lesions, or unexplained granulomatous pathology, negative or non-diagnostic routine investigations should prompt multi-specimen sampling, molecular testing and specialist reference-laboratory confirmation. The algorithm is a review-derived clinical framework and has not been prospectively validated as a decision rule.

Figure 6.
Horizontal clinical timeline comparing fatal and survivor trajectories in B. mandrillaris GAE. The highlighted diagnostic window indicates the period between first neuroimaging and neurological decline when biopsy, mNGS/NGS, confirmatory testing, surgery when feasible and expert-guided multidrug therapy may alter outcome.
Figure 6.
Horizontal clinical timeline comparing fatal and survivor trajectories in B. mandrillaris GAE. The highlighted diagnostic window indicates the period between first neuroimaging and neurological decline when biopsy, mNGS/NGS, confirmatory testing, surgery when feasible and expert-guided multidrug therapy may alter outcome.


Table 1.
Review framework aligned with PRISMA reporting and the systematic review question.
| Domain | Specification |
|---|---|
| Population | Human patients with confirmed B. mandrillaris central nervous system infection, including GAE, encephalitis, meningoencephalitis, encephalomyelitis, cerebral abscess or CNS vasculitis. |
| Publication window | Peer-reviewed literature from January 2015 to June 2026, prioritising open-access case reports, case series and retrospective patient-level summaries. |
| Primary focus | Diagnostic delay, role of mNGS/NGS or related molecular methods, specimen type, confirmatory testing and survival outcomes. |
| Key exclusions | Environmental-only studies, animal-only studies, laboratory drug screens without clinical cases, cutaneous-only infection without CNS disease, non-peer-reviewed abstracts without DOI, and duplicate case reports. |
| Synthesis approach | Narrative synthesis; no meta-analysis because timing definitions, diagnostic platforms and follow-up periods were heterogeneous. |
Table 2.
Representative recent patient-level reports and diagnostic themes included in the narrative synthesis.
Table 2.
Representative recent patient-level reports and diagnostic themes included in the narrative synthesis.
| Study | Country/setting | Diagnostic feature | Outcome theme |
|---|---|---|---|
| Wilson et al., 2015 [16] | USA | Metagenomic deep sequencing detected B. mandrillaris in CSF and supported confirmatory testing. | Landmark proof-of-concept for sequencing in unexplained encephalitis. |
| Vollmer and Glaser, 2016 [12] | USA | Survivor report after prolonged multidrug therapy. | Demonstrated that recovery is possible despite high fatality. |
| Piper et al., 2018 [6] | USA | Brain infection linked to improper nasal lavage; diagnosis delayed by nonspecific symptoms. | Fatal outcome; reinforces exposure history and risk communication. |
| Yohannan and Feldman, 2019 [7] | USA | Fatal encephalitis with diagnostic challenge. | Emphasises low recognition and rapid deterioration. |
| Kalyatanda et al., 2020 [18] | USA | Plasma-based NGS enabled rapid non-invasive diagnosis. | Supports multi-specimen molecular strategy. |
| Hirakata et al., 2021 [19] | Japan | Shotgun metagenomics of tissue identified B. mandrillaris. | Shows value when histology is granulomatous but aetiology unclear. |
| Peng et al., 2022 [13] | China | High-throughput NGS in blood, CSF and brain tissue; two excisions and medication. | Survival reported after combined surgical-medical management. |
| Spottiswoode et al., 2023 [14] | USA | Nitroxoline added after functional drug-screening rationale. | Important survivor and drug-repurposing signal. |
| Li et al., 2024 [8] | China | mNGS diagnosed B. mandrillaris encephalitis. | Highlights role of modern diagnostics in reducing missed diagnosis. |
| Javed et al., 2024 [9] | Pakistan | Non-granulomatous meningoencephalitis mimicked tumour. | First confirmed case from Pakistan; atypical pathology can mislead. |
| Edminster et al., 2025 [22] | USA | Plasma metagenomic sequencing identified infection despite CSF limitations. | Fatal case; underscores specimen choice and retrospective signal review. |
| Zhao et al., 2026 [24] | China | MetaCAP compared with mNGS and national 41-case landscape. | Suggests targeted sequencing may improve sensitivity for rare pathogens. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



