Submitted:
12 June 2026
Posted:
15 June 2026
You are already at the latest version
Abstract
Background: Type 2 diabetes mellitus is a progressive cardiometabolic disease in which many patients require treatment intensification despite lifestyle intervention and evidence-based pharmacotherapy. Oleanolic acid, a pentacyclic triterpenoid found in olives and other plants, has shown insulin-sensitizing, antioxidant, anti-inflammatory, and hepatometabolic effects in experimental models.Aim: This review evaluates oleanolic acid as a potential adjunctive intervention in type 2 diabetes, emphasizing translational evidence, formulation-dependent bioavailability, clinical endpoints, and patient relevance.Methods: We performed a narrative translational review of mechanistic, preclinical, pharmacokinetic, clinical, and trial-registry evidence on oleanolic acid, insulin resistance, prediabetes, and type 2 diabetes.Results: Preclinical studies support multiple mechanisms by which oleanolic acid may influence glucose homeostasis, including modulation of insulin signaling, hepatic glucose production, oxidative stress, inflammatory pathways, lipid metabolism, and beta-cell vulnerability. Human evidence remains limited but clinically relevant. PREDIABOLE reported reduced progression from prediabetes to type 2 diabetes after long-term intake of oleanolic acid-enriched olive oil. BIO-OLTRAD demonstrated measurable systemic exposure after a 30 mg dose delivered in functional olive oil, with transport through albumin and triglyceride-rich lipoproteins. OLTRAD is testing whether this formulation improves glycemic control as an adjunct to metformin-based therapy.Conclusion: Oleanolic acid is a plausible investigational adjunct for type 2 diabetes. Its clinical value depends on formulation-specific exposure, reproducible effects on glycemic and cardiometabolic endpoints, and long-term safety.Relevance for patients: Oleanolic acid-enriched functional foods may eventually complement, but should not replace, evidence-based diabetes treatment.
Keywords:
oleanolic acid
; type 2 diabetes
; metformin
; insulin resistance
; functional olive oil
; bioavailability
; translational research
; patient-centered outcomes
1. Introduction
Type 2 diabetes mellitus (T2DM) is one of the most prevalent chronic cardiometabolic diseases worldwide and remains a major driver of morbidity, mortality, health-care expenditure, and loss of quality-adjusted life years. Recent global estimates indicate that more than half a billion adults are living with diabetes, with a continued increase projected by 2050; more than 90% of cases are T2DM [1]. Despite major therapeutic progress, durable glycemic control remains difficult for many patients, particularly when insulin resistance, beta-cell dysfunction, obesity, cardiovascular disease, chronic kidney disease, treatment burden, and adherence interact over time.
Current standards of care emphasize individualized, person-centered therapy. Drug selection is guided not only by glycemic targets, but also by cardiovascular and kidney comorbidity, weight-management goals, hypoglycemia risk, cost, access, and patient preferences. Metformin remains widely used, while sodium-glucose cotransporter 2 inhibitors, glucagon-like peptide-1 receptor agonists, dual incretin agonists, insulin, and other agents are increasingly selected according to risk profile [2,3]. This expanding therapeutic landscape leaves room for adjunctive strategies only if they are safe, acceptable, affordable, compatible with standard care, and supported by reproducible metabolic benefit.
Oleanolic acid (OA) is a naturally occurring pentacyclic triterpenoid found in several edible and medicinal plants, including olives and olive-derived products [4,5]. It has attracted interest in metabolic disease because its biological effects intersect with mechanisms relevant to T2DM, including insulin resistance, hepatic glucose production, oxidative stress, low-grade inflammation, lipid metabolism, and pancreatic beta-cell vulnerability [4,5,6]. Experimental studies also suggest that OA may complement metformin in diabetic models, supporting the rationale for adjunctive rather than replacement therapy [7].
Clinical translation of OA is strongly constrained by formulation and bioavailability. OA is hydrophobic and poorly water-soluble, so systemic exposure depends on the delivery matrix, dose, intestinal absorption, and postprandial lipid transport. Early analytical work established methods for measuring OA in human serum [8], and BIO-OLTRAD later showed that OA administered as functional olive oil produced measurable postprandial serum concentrations and transport through serum albumin and triglyceride-rich lipoproteins [9]. These findings shift the question from whether OA is active in experimental systems to whether a clinically acceptable formulation can deliver sufficient and reproducible exposure in humans.
Human clinical evidence remains limited but relevant. PREDIABOLE reported that OA-enriched olive oil reduced progression from prediabetes to T2DM during long-term follow-up [10]. However, prevention in prediabetes is not equivalent to adjunctive treatment in established T2DM. Patients with diagnosed T2DM have different metabolic trajectories, background medications, comorbidity burdens, and endpoint expectations. The OLTRAD study therefore represents an important next step because it evaluates OA-enriched functional olive oil as an adjuvant to metformin-based treatment in adults with T2DM [11].
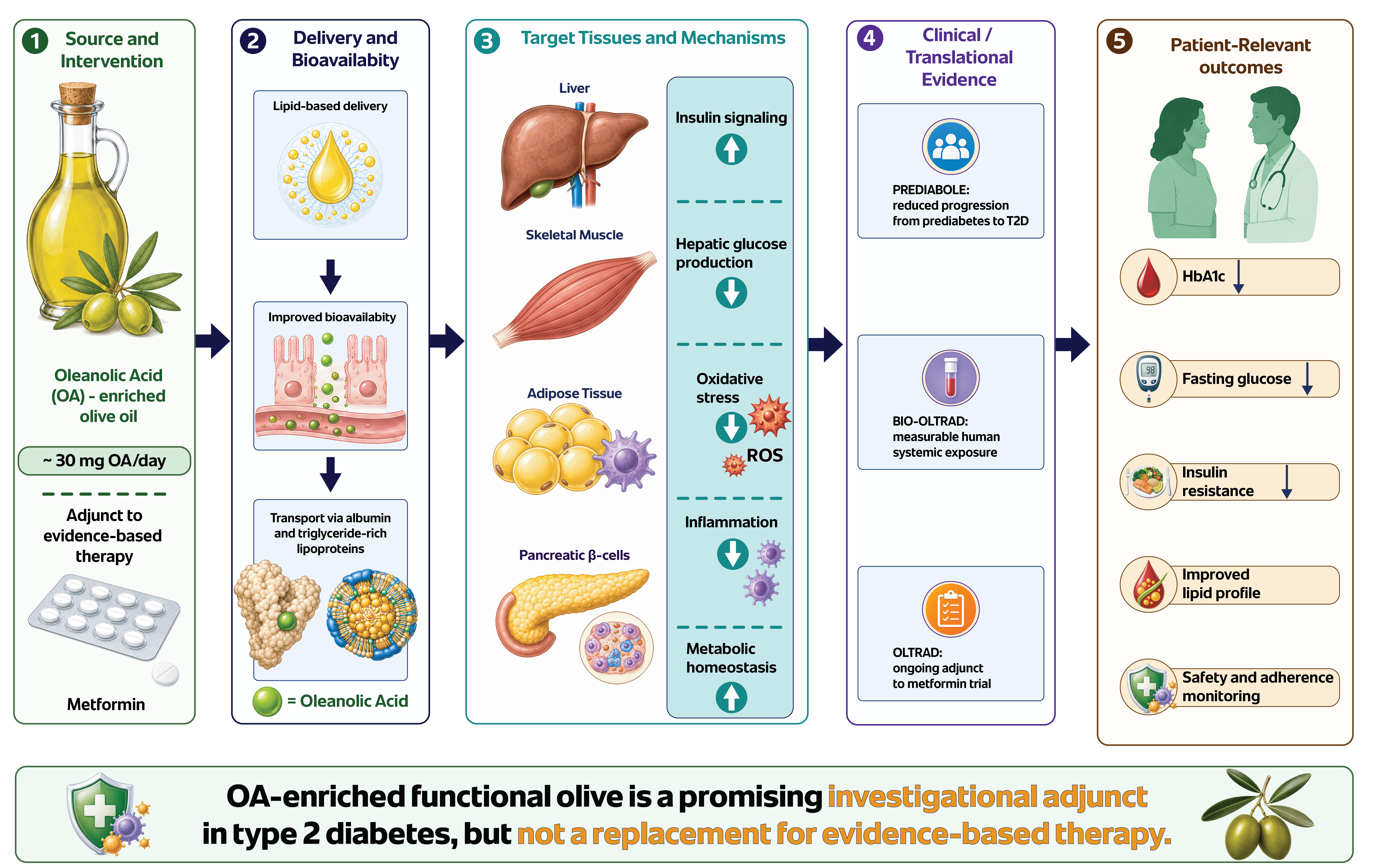
This review examines whether OA can be reasonably developed as an adjunctive strategy for T2DM. It integrates mechanistic and preclinical evidence with human bioavailability data, prevention-oriented clinical findings, ongoing adjunctive trial design, safety considerations, and outcomes relevant to clinical practice. The aim is to distinguish evidence-supported conclusions from still-hypothetical claims and to define the research needed before OA-enriched formulations can be considered for diabetes care. The proposed translational pathway from OA-enriched functional olive oil to systemic exposure, tissue-level mechanisms, and patient-relevant endpoints is summarized in Figure 1.
Oleanolic acid (OA)-enriched functional olive oil provides a lipid-based delivery matrix intended to support gastrointestinal solubilization, postprandial absorption, and systemic transport through serum albumin and triglyceride-rich lipoproteins. After systemic exposure, OA may distribute to metabolically relevant tissues, including the liver, skeletal muscle, adipose tissue, and pancreatic β-cells. The proposed pathway links formulation-dependent delivery with mechanisms relevant to type 2 diabetes, including insulin signaling, hepatic glucose production, oxidative stress, inflammation, lipid metabolism, β-cell stress, and metabolic homeostasis. These biological effects should be evaluated against clinically relevant and patient-centered endpoints, including glycated hemoglobin, fasting plasma glucose, postprandial glucose, insulin resistance indices, lipid profile, inflammatory biomarkers, hepatic and renal safety markers, adherence, and quality of life. The figure summarizes a translational hypothesis and does not imply that clinical efficacy has already been established.
Abbreviations: AMPK, adenosine monophosphate-activated protein kinase; G6Pase, glucose-6-phosphatase; HbA1c, glycated hemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance; IRS, insulin receptor substrate; NF-κB, nuclear factor kappa B; Nrf2, nuclear factor erythroid 2-related factor 2; OA, oleanolic acid; PEPCK, phosphoenolpyruvate carboxykinase; PI3K/Akt/FoxO1, phosphatidylinositol 3-kinase/protein kinase B/forkhead box O1; T2DM, type 2 diabetes mellitus.
2. Methods of Literature Synthesis
This article was designed as a narrative translational review rather than a systematic review or meta-analysis. The aim was to integrate evidence across the translational continuum, including molecular and cellular mechanisms, animal models, human pharmacokinetics, clinical prevention data, safety considerations, and ongoing adjunctive-therapy trials. The review structure used a predefined narrative framework with explicit search procedures, balanced evidence presentation, and transparent discussion of limitations, consistent with quality principles proposed for narrative reviews [12]. Because quantitative pooling was not planned, the review was not registered in PROSPERO and was not conducted as a formal PRISMA systematic review; however, PRISMA 2020 principles were used to support transparent reporting of sources and selection procedures [13]
2.1. Search Strategy and Information Sources
A structured literature search was performed in PubMed/MEDLINE, Scopus, Web of Science, and Google Scholar from database inception to May 21, 2026. Clinical trial registries, including ClinicalTrials.gov, were searched to identify ongoing or completed human studies involving OA-enriched formulations in diabetes or prediabetes [11]. Reference lists of key reviews and primary studies were screened manually.
Search terms combined the compound, disease context, formulation, and therapeutic strategy. Core terms included “oleanolic acid,” “oleanolic acid-enriched olive oil,” “functional olive oil,” “pentacyclic triterpenes,” “type 2 diabetes,” “T2DM,” “prediabetes,” “insulin resistance,” “metformin,” “glucose metabolism,” “bioavailability,” “pharmacokinetics,” “Nrf2,” “oxidative stress,” “inflammation,” “hepatic gluconeogenesis,” “beta-cell,” “clinical trial,” “PREDIABOLE,” “BIO-OLTRAD,” and “OLTRAD.” Boolean combinations were adapted to each database.
2.2. Eligibility and Prioritization
Eligible sources included original mechanistic studies, in vitro experiments relevant to insulin signaling or glucose metabolism, animal studies of diabetes or insulin resistance, pharmacokinetic studies, human intervention studies, clinical trial protocols or registry records, systematic reviews, and high-quality narrative reviews. Evidence was prioritized when it addressed one or more translational questions: whether OA modulates T2DM-relevant mechanisms; whether OA improves glucose homeostasis in vivo; whether OA can be delivered with measurable human systemic exposure; whether OA-enriched food matrices affect diabetes prevention or glycemic control; and whether OA can plausibly complement metformin-based therapy.
Publications were excluded from detailed discussion if they focused on unrelated disease areas without a plausible metabolic link, lacked sufficient methodological detail, examined complex botanical mixtures without an identifiable OA contribution, or reported only chemical isolation without biological or translational relevance. Conference abstracts were used only to identify ongoing work and were not treated as definitive evidence.
2.3. Data Extraction and Synthesis
For each relevant source, information was extracted on study type, model or population, OA formulation, dose, route of administration, duration, comparator, co-intervention, metabolic endpoints, mechanistic endpoints, safety findings, and main limitations. Human studies and trial records were additionally reviewed for sample size, eligibility criteria, intervention matrix, background therapy, primary and secondary endpoints, and patient relevance.
Findings were synthesized narratively according to a translational framework. Mechanistic studies were used to define biological plausibility, animal studies to evaluate in vivo metabolic effects and dose-translation issues, human pharmacokinetic studies to assess systemic exposure, and clinical studies to evaluate prevention or adjunctive-treatment potential. Evidence was not pooled statistically because study designs, populations, formulations, doses, endpoints, and exposure durations were heterogeneous.
The central interpretive question was whether OA should be considered a plausible adjunctive intervention in T2DM, particularly in patients treated with metformin-based therapy. Evidence was therefore assessed in relation to glycemic endpoints, insulin resistance, lipid profile, inflammatory and oxidative stress biomarkers, hepatic and renal safety markers, adverse events, adherence, dietary acceptability, and the distinction between adjunctive benefit and unsupported replacement of evidence-based treatment.
3. Biological Rationale for Oleanolic Acid in Type 2 Diabetes
The rationale for studying OA in T2DM is based on several intersecting mechanisms rather than on a single dominant target. T2DM develops through the combined effects of insulin resistance, beta-cell dysfunction, excess hepatic glucose production, adipose tissue inflammation, ectopic lipid accumulation, oxidative stress, and vascular-metabolic injury [2,3]. In this context, OA is better viewed as a pleiotropic metabolic modulator than as a selective glucose-lowering compound [14,15,16]. This profile is attractive for adjunctive therapy, but clinical relevance depends on whether pathway-level effects are reproducible, formulation-dependent, and large enough to influence patient-relevant endpoints [17].
3.1. Insulin Signaling and Glucose Handling
Insulin resistance is central to T2DM and involves impaired insulin action in skeletal muscle, liver, adipose tissue, and other insulin-responsive organs, with downstream effects on glucose uptake, glycogen synthesis, lipid metabolism, and hepatic glucose production [17,18]. Experimental evidence suggests that OA may interact with this pathway. A systematic review of insulin-resistant cell and animal models reported improved insulin sensitivity, increased glucose uptake, and reduced hepatic glucose production, probably through modulation of insulin receptor substrate/phosphatidylinositol 3-kinase/protein kinase B/forkhead box O1 signaling and related oxidative stress signaling [6].
OA may also influence glucose and lipid handling through nuclear receptor and transporter-related mechanisms. In vitro and preclinical evidence indicates effects on peroxisome proliferator-activated receptor alpha/gamma signaling, metabolic nuclear receptor pathways, and glucose transporter 4 translocation [19,20]. This supports the idea that OA may act at the interface of dysglycemia and dyslipidemia. However, whether these molecular effects occur at achievable human tissue concentrations remains uncertain and should be tested in formulation-specific pharmacodynamic studies.
3.2. Hepatic Glucose Production and Lipid Metabolism
The liver is a key target because fasting hyperglycemia in T2DM is strongly influenced by dysregulated hepatic glucose production. In diabetic and insulin-resistant models, OA has been reported to reduce fasting glucose, improve glucose and insulin tolerance, enhance hepatic insulin signaling, suppress gluconeogenesis, reduce hepatic lipid accumulation, and attenuate inflammatory mediators [21,22,23]. These findings suggest that hepatic effects of OA may involve both glucose and lipid pathways. This is relevant to adjunctive therapy because metformin also acts partly by suppressing hepatic glucose production. In db/db mice, combined OA and metformin treatment produced greater improvements in blood glucose, insulin levels, liver pathology, insulin sensitivity, hepatic insulin signaling, and hepatic glucose production than either monotherapy alone [7]. This provides a mechanistic bridge to the adjunctive-treatment hypothesis, but animal synergy should not be assumed to translate directly to humans because dose, formulation, route, and exposure differ substantially from OA-enriched olive oil in clinical studies.
3.3. Oxidative Stress, Nrf2 Signaling, and Mitochondrial Function
Oxidative stress is closely linked to insulin resistance, beta-cell dysfunction, endothelial injury, and diabetic complications [24,25]. Chronic hyperglycemia, lipotoxicity, nutrient excess, and mitochondrial dysfunction increase reactive oxygen species production, which can impair insulin signaling and amplify inflammation. OA has repeatedly been studied as an antioxidant or redox-modulating compound, and recent reviews have summarized its natural sources, antioxidant mechanisms, therapeutic potential, and strategies for enhancing bioactivity [26]. In hepatic insulin resistance models, OA improved mitochondrial parameters and reduced oxidative injury, with evidence implicating nuclear factor erythroid 2-related factor 2 and glutathione-related antioxidant defenses [21].
The Nrf2 pathway is relevant because it regulates cytoprotective genes involved in antioxidant defense, detoxification, mitochondrial homeostasis, and cellular stress adaptation. Experimental reports suggest that OA may activate or stabilize Nrf2-related responses [4,21]. However, Nrf2 activation should be treated as context-dependent rather than uniformly beneficial. Recent work also supports viewing OA as a modulator of an integrated organelle-stress network involving mitochondria, endoplasmic reticulum stress, autophagy, mitophagy, and apoptosis [27]. Human studies should therefore pair redox and organelle-stress biomarkers with clinical endpoints and safety monitoring, because stress-response modulation may vary by dose, tissue, disease stage, and duration of exposure.
3.4. Inflammation, Adipose Tissue Dysfunction, and Immunometabolism
Low-grade chronic inflammation contributes to insulin resistance and cardiometabolic complications [28,29]. Adipose tissue expansion promotes macrophage infiltration, pro-inflammatory polarization, cytokine production, inflammasome activation, and release of mediators that interfere with insulin action. In high-fat diet-induced obese mice, OA improved insulin resistance, reduced adipocyte hypertrophy, decreased adipose tissue macrophage infiltration, and lowered the M1/M2 macrophage ratio. These effects were linked to reduced mitochondrial reactive oxygen species, mitogen-activated protein kinase signaling, and NLRP3 inflammasome activation [30].
Prediabetes models also support an immunometabolic role. In diet-induced prediabetic rats, OA improved lipid parameters and reduced platelet and immune-cell indices, pro-inflammatory cytokines, C-reactive protein, fibrinogen, and cluster of differentiation 40 ligand [31]. These findings are relevant because early dysglycemia is accompanied by inflammatory and prothrombotic changes. Still, these data remain preclinical, and it is not yet known whether OA-enriched formulations produce comparable immunometabolic effects in humans.
3.5. Beta-Cell Vulnerability and Disease Progression
Progression from insulin resistance to overt T2DM partly reflects failure of pancreatic beta cells to compensate for chronic metabolic stress. Hyperglycemia, lipotoxicity, oxidative injury, endoplasmic reticulum stress, and inflammation can impair insulin secretion and accelerate beta-cell dysfunction. OA has been reported to influence beta-cell-relevant pathways indirectly through oxidative stress reduction, inflammatory modulation, and improvement of systemic metabolic stress [4,5,14,32]. The strongest human signal compatible with disease-modifying potential comes from PREDIABOLE, in which OA-enriched olive oil reduced progression from prediabetes to T2DM [10]. This does not prove beta-cell protection, but it suggests that OA-enriched functional foods may influence upstream metabolic processes. In established T2DM, the key question is different: whether OA can improve metabolic control or slow deterioration when beta-cell dysfunction is already present and pharmacologic therapy is in use.
3.6. Translational Interpretation
Overall, the mechanistic case for OA is coherent but still largely preclinical. The most consistent themes are improved insulin signaling, reduced hepatic glucose output, modulation of oxidative and inflammatory stress pathways, and possible support of beta-cell resilience. These pathways align with major components of T2DM pathophysiology and justify clinical testing, but they do not establish efficacy.
For these mechanisms to become clinically relevant, OA must achieve reproducible systemic exposure, show pharmacodynamic activity at achievable concentrations, remain compatible with standard drugs such as metformin, and demonstrate effects on clinically useful endpoints with appropriate safety monitoring. Figure 2 summarizes the proposed network linking OA to insulin signaling, hepatic glucose production, oxidative stress, inflammation, and beta-cell vulnerability.
Oleanolic acid may influence multiple interconnected pathways involved in type 2 diabetes pathophysiology, including insulin receptor substrate/phosphatidylinositol 3-kinase/protein kinase B/forkhead box O1 signaling, adenosine monophosphate-activated protein kinase signaling, nuclear factor erythroid 2-related factor 2-mediated antioxidant responses, nuclear factor kappa B and mitogen-activated protein kinase signaling, mitochondrial reactive oxygen species, NLRP3 inflammasome activation, macrophage polarization, adipose tissue inflammation, endothelial function, and beta-cell vulnerability. These pathway-level effects may converge on improved insulin sensitivity, reduced hepatic glucose production, lower oxidative and inflammatory stress, and improved cardiometabolic risk, but their clinical relevance remains dependent on formulation-specific exposure and validation in human trials.
Abbreviations: ACC, acetyl-CoA carboxylase; AMPK, adenosine monophosphate-activated protein kinase; ARE, antioxidant response element; FoxO1, forkhead box O1; GLUT4, glucose transporter 4; GPx, glutathione peroxidase; HO-1, heme oxygenase-1; IRS, insulin receptor substrate; MAPK, mitogen-activated protein kinase; NF-κB, nuclear factor kappa B; NLRP3, NOD-like receptor family pyrin domain-containing 3; NQO1, NAD(P)H quinone dehydrogenase 1; Nrf2, nuclear factor erythroid 2-related factor 2; OA, oleanolic acid; PI3K/Akt, phosphatidylinositol 3-kinase/protein kinase B; ROS, reactive oxygen species; SOD, superoxide dismutase; T2DM, type 2 diabetes mellitus.
4. Preclinical Evidence for Adjunctive Use with Metformin
The adjunctive-treatment hypothesis for OA is clinically relevant because most patients with established T2DM are treated within a pharmacologic framework rather than with isolated experimental compounds. Metformin remains an important comparator and partner because of its long-standing use, low cost, broad accessibility, low intrinsic risk of hypoglycemia, and central role in early pharmacologic management [2,3]. An OA-metformin combination is therefore plausible if OA complements metformin’s effects on hepatic glucose production, insulin sensitivity, lipid metabolism, oxidative stress, or inflammation without adding unacceptable safety or adherence burdens.
4.1. Mechanistic Rationale for Combining Oleanolic Acid with Metformin
Metformin primarily improves hyperglycemia by reducing hepatic glucose production and improving insulin sensitivity through mechanisms involving mitochondrial function, cellular energy state, adenosine monophosphate-activated protein kinase signaling, gut-mediated pathways, and hepatic substrate handling [2,3,33]. OA has been proposed to influence overlapping but not identical processes, including hepatic insulin signaling, glycogen metabolism, oxidative stress, inflammatory activation, and lipid accumulation [6,21]. The rationale for combination therapy is therefore not duplication of effect, but convergence on hepatic and systemic metabolic dysfunction through partially distinct mechanisms.
This distinction matters clinically. OA would have limited value if it merely reproduced metformin’s action at lower potency. Its potential lies in complementary effects on oxidative-inflammatory stress, hepatic lipid handling, or insulin signaling, but this remains a hypothesis until supported by human pharmacodynamic and clinical endpoint data.
4.2. Evidence from db/db Mouse Models
The most direct preclinical evidence comes from a db/db diabetic mouse study comparing OA, metformin, combined OA plus metformin, and untreated diabetic controls. Mice received OA at 250 mg/kg, metformin at 100 mg/kg, or both for four weeks. Combination therapy produced greater improvement than monotherapy in blood glucose, insulin levels, liver pathology, oral glucose tolerance, insulin sensitivity, hepatic insulin signaling, and hepatic glucose production [7].
At the molecular level, the combined intervention increased markers of glycogen synthesis and decreased pathways linked to hepatic glucose output, including glycogen phosphorylase, peroxisome proliferator-activated receptor gamma coactivator 1 alpha, phosphoenolpyruvate carboxykinase, and glucose-6-phosphatase [7]. These findings support the adjunctive hypothesis, but they do not prove clinical synergy. Strict pharmacologic synergy would require formal interaction testing across dose combinations; therefore, the evidence is best described as additive or potentially synergistic.
4.3. Dose Translation and Model Limitations
The db/db model is useful but limited. It represents severe genetic obesity and leptin receptor deficiency, not the full heterogeneity of human T2DM. The four-week treatment period does not address durability, long-term safety, adherence, or interaction with contemporary therapies. The OA dose was also pharmacologic rather than dietary and differs substantially from the 30 mg OA dose used in human functional-oil studies [9,11].
This dose mismatch should be explicit in interpretation. A positive animal study supports biological plausibility, but it cannot be used to infer that 30 mg/day OA-enriched olive oil will produce the same effect in patients with T2DM [7,9]. Conversely, a lipid matrix may improve absorption despite a lower nominal dose. Pharmacokinetic and pharmacodynamic studies are therefore needed to connect dose, formulation, exposure, and effect.
4.4. Quality and Reproducibility Considerations
The translational value of preclinical findings depends on design quality and reporting transparency. Animal studies intended to inform clinical translation should report randomization, blinding of outcome assessment, sample-size justification, sex, strain, diet composition, route of administration, formulation, batch characterization, prespecified endpoints, and adverse events. ARRIVE 2.0 provides a useful framework for improving animal-study reporting [34].
For OA-metformin translation, future preclinical work should incorporate dose-response designs, pharmacokinetic sampling, tissue exposure data, and formal interaction modeling. Diet-induced obesity models may complement genetic models by better reflecting lifestyle-associated insulin resistance. Endpoints should include not only glucose lowering but also hepatic safety markers, renal markers, lipid profile, inflammatory biomarkers, and histology where appropriate.
4.5. Implications for OLTRAD and Future Trials
Preclinical evidence supports the plausibility of OA as an adjunct to metformin, but it does not establish clinical efficacy. The strongest animal evidence suggests that combined OA and metformin can improve glucose homeostasis, hepatic insulin signaling, and hepatic glucose production more than either treatment alone in db/db mice [7]. Additional studies support effects on oxidative stress, inflammation, lipid metabolism, hepatic dysfunction, glucose homeostasis, renal-risk markers, and prediabetes-related immune activation [6,21,22,23,30,31,32,35,36].
OLTRAD is the appropriate next step because it evaluates OA-enriched functional olive oil in patients with established T2DM receiving metformin-based therapy [11]. Its relevance will depend on whether the intervention improves HbA1c or other clinically useful endpoints beyond standard care, whether the effect size is meaningful, and whether the intervention is safe, acceptable, and sustainable. The next step is therefore to determine in human trials whether measured exposure translates into outcomes that matter clinically.
5. Human Bioavailability and Formulation-Dependent Translation
Bioavailability is central to the interpretation of OA studies. Mechanistic and animal data are difficult to translate if oral administration does not produce reproducible systemic exposure at concentrations capable of influencing relevant tissues. This issue is especially important because OA is highly lipophilic, poorly water-soluble, and strongly dependent on formulation, postprandial lipid handling, and delivery-system design [9,37,38,39,40]. Thus, the clinical question is not only whether OA has antidiabetic biology, but whether a feasible formulation can deliver OA safely and consistently during long-term diabetes care.
5.1. Poor Solubility and Formulation Dependence
OA is widely distributed in plants and olive-derived products, but its hydrophobicity limits straightforward oral translation. Like many poorly water-soluble lipophilic compounds, its exposure depends on dissolution, intestinal solubilization, permeability, food effects, and first-pass handling [37,38]. Therefore, the same nominal OA dose may produce different systemic exposure when administered as a solid preparation, extract, suspension, lipid matrix, or nanoformulation.
Early analytical studies established that OA can be quantified in human serum or plasma, supporting the feasibility of human pharmacokinetic research [8,41]. These studies also highlight a practical problem: OA products cannot be assumed to be bioequivalent. Capsules, plant extracts, purified compounds, and OA-enriched olive oil may differ in dissolution, intestinal uptake, albumin binding, lipoprotein association, tissue distribution, and adherence [40,42,43,44]. Future trials should therefore define the formulation precisely and avoid extrapolating efficacy or safety across chemically similar but pharmacokinetically distinct products.
5.2. Lipid Matrices and Functional Olive Oil
Lipid-based delivery is a rational strategy for OA because lipid vehicles can enhance solubilization, stimulate bile and pancreatic secretions, promote mixed micelle formation, influence enterocyte uptake, and potentially recruit intestinal lymphatic transport [37,38]. These mechanisms support the use of an olive oil matrix rather than an isolated poorly soluble powder.
OA-enriched functional olive oil has additional translational advantages. Olive oil is familiar in Mediterranean dietary patterns, may be acceptable for long-term intake, and can serve as a food-based delivery matrix [45]. Enrichment allows the OA dose to be standardized while preserving the lipid vehicle. This is clinically attractive, but it also complicates interpretation because olive oil itself may influence cardiometabolic outcomes [46]. Matrix-matched control oils are therefore essential when the goal is to isolate the effect of OA enrichment.
5.3. BIO-OLTRAD and Human Systemic Exposure
BIO-OLTRAD provides the most directly relevant human pharmacokinetic evidence for OA-enriched functional olive oil. In this double-blind, randomized controlled study, participants received a single 30 mg OA dose in functional olive oil. OA reached measurable postprandial serum concentrations, with reported maximum concentrations of approximately 500–600 ng/mL and an AUC0–∞ of 2862.50 ± 174.50 ng·h/mL [9]. These data show that a modest OA dose can achieve systemic exposure when delivered in a lipid matrix.
The study also reported physiological association of OA with serum albumin and triglyceride-rich lipoproteins, with lipoprotein-associated OA peaking after two to four hours. This is relevant because lipoprotein-mediated transport may influence tissue distribution, exposure duration, and access to metabolically active tissues. BIO-OLTRAD should not be interpreted as evidence of antidiabetic efficacy, but it provides the pharmacokinetic bridge needed to justify longer clinical trials such as OLTRAD [9,11].
5.4. Dose, Timing, and Pharmacodynamic Implications
Human bioavailability data have practical implications for trial design. Dose should be interpreted in relation to formulation, not only milligrams of OA. A 30 mg dose in functional olive oil cannot be assumed equivalent to 30 mg in a capsule, extract, suspension, or nanoparticle system. Timing with meals may also matter because lipid digestion and postprandial lipoprotein formation are likely to affect systemic transport [9,37,38].
Future studies should connect OA exposure to pharmacodynamic endpoints. Short-term studies may assess postprandial glucose, insulin, triglyceride-rich lipoprotein fractions, inflammatory mediators, oxidative stress markers, and hepatic glucose-output surrogates. Longer trials should focus on HbA1c, fasting glucose, insulin resistance indices, body weight, lipid profile, liver enzymes, kidney markers, adverse events, and adherence. Without exposure-sensitive biomarkers, a negative trial could reflect inadequate delivery rather than absence of biological activity.
5.5. Alternative Delivery Systems and Clinical Interpretation
Several alternative formulation strategies have been explored to overcome OA’s solubility and absorption barriers, including liposomes, micelles, phospholipid complexes, albumin nanoparticles, solid dispersions, poly(lactic-co-glycolic acid)-based systems, cyclodextrin complexes, self-nanoemulsifying systems, and self-microemulsifying drug delivery systems [39,40,42,43,44,47,48]. These approaches may improve solubility, stability, release profile, or tissue distribution, but improved formulation performance in vitro or in animals does not automatically establish clinical readiness. Functional olive oil and nanomedicine formulations should be viewed as distinct development pathways. Functional olive oil emphasizes dietary compatibility and acceptability, whereas nanoformulations may offer more controlled exposure but face greater regulatory, manufacturing, cost, and safety challenges [47]. A positive trial using OA-enriched olive oil should not be generalized to capsules or nanoformulations unless comparable exposure is demonstrated. Conversely, a negative trial using a poorly absorbed preparation would not necessarily disprove OA biology. For OA, clinical interpretation should therefore remain tied to the formulation being tested.
6. Clinical Evidence: From Prediabetes Prevention to Adjunctive Therapy
Clinical evidence for OA in diabetes remains limited, but it follows a relatively clear translational sequence. The available human data do not yet establish OA as a treatment for established T2DM, but they do provide three clinically relevant building blocks: a prevention trial in individuals with prediabetes, a human bioavailability trial using OA-enriched functional olive oil, and an ongoing adjunctive-therapy trial in patients with T2DM receiving metformin-based treatment [9,10,11]. This sequence is important because it follows a recognizable translational pathway: first, identify a plausible biological effect; second, demonstrate systemic exposure in humans; third, test whether the intervention improves clinically meaningful endpoints in the intended patient population.

Table 1.
Translational evidence map for oleanolic acid in type 2 diabetes.
| Evidence level | Main evidence type | Key findings | Translational value | Main limitations | Key reference |
| Mechanistic plausibility | Cell and pathway-focused studies | OA may modulate insulin signaling, oxidative stress, inflammation, lipid metabolism, and glucose handling | Defines biological rationale and candidate biomarkers | Achievable human tissue concentrations remain uncertain | [4,5,6,19] |
| In vivo metabolic effects | Rodent models of diabetes, obesity, insulin resistance, and prediabetes | OA improved glucose tolerance, insulin sensitivity, hepatic metabolic markers, inflammation, and lipid parameters in selected models | Supports in vivo plausibility and endpoint selection | Species differences, high doses, short exposure, variable formulations | [7,21,30,31,49] |
| Adjunctive preclinical therapy | OA plus metformin in db/db mice | Combined treatment improved glycemic and hepatic outcomes more than monotherapy in one model | Supports adjunct-to-metformin hypothesis | Does not prove human synergy; dose and exposure differ from functional olive oil | [7] |
| Human bioavailability | BIO-OLTRAD | A 30 mg OA dose in functional olive oil produced measurable serum exposure and albumin/lipoprotein-associated transport | Demonstrates formulation-dependent human systemic exposure | Healthy volunteers; acute dosing; no efficacy endpoints | [9] |
| Prevention-oriented clinical trial | PREDIABOLE | OA-enriched olive oil reduced progression from prediabetes to T2DM compared with control olive oil | Proof of concept in a clinically relevant risk population | Prevention trial, not established T2DM treatment | [10] |
| Adjunctive clinical trial | OLTRAD trial registry | OA-enriched olive oil is being tested as an adjunct to metformin-based therapy in established T2DM | Directly tests the main clinical hypothesis | Results not yet available; formulation-specific conclusions | [11] |
| Safety and regulation | Preclinical toxicology, interaction studies, regulatory guidance | Hepatic safety, drug interactions, health claims, and formulation classification require monitoring | Defines risk-management and communication needs | Long-term human safety in complex T2DM populations remains limited | [50,51,52,53,54,55,56,57,58,59] |
6.1. PREDIABOLE and the Prevention Signal
PREDIABOLE is the most important published intervention trial of OA-enriched olive oil in glucose-metabolism disorders. In this multicenter, randomized, double-blind, controlled trial, adults with prediabetes received either 55 mL/day of OA-enriched olive oil, providing approximately 30 mg OA/day, or the same olive oil without OA enrichment [10]. The matrix-controlled design is important because olive oil itself may influence cardiometabolic outcomes [46].
The main clinical signal was reduced progression from prediabetes to T2DM. The trial reported 48 new diabetes cases: 31 in the control group and 17 in the OA-enriched group. The multivariable-adjusted hazard ratio for incident T2DM was 0.45, with a 95% confidence interval of 0.24–0.83, and intervention-related adverse effects were not reported [10]. These findings support prevention-oriented potential and long-term functional-food feasibility.
However, PREDIABOLE should not be interpreted as proof of treatment efficacy in established T2DM. Participants were not selected for inadequate glycemic control on metformin, and the endpoint was diabetes onset rather than HbA1c reduction in diagnosed T2DM. Its main value for this review is therefore proof of concept: OA-enriched olive oil can be administered long-term, compared with a matched oil control, and associated with clinically meaningful metabolic outcomes [10].
6.2. BIO-OLTRAD and OLTRAD: From Exposure to Adjunctive Testing
BIO-OLTRAD provides the pharmacokinetic bridge between prevention-oriented findings and adjunctive-treatment trials. In this double-blind, randomized, controlled human study, 22 healthy participants received a single 30 mg OA dose formulated as functional olive oil. OA reached measurable postprandial serum concentrations, with maximum concentrations around 500–600 ng/mL and an AUC0–∞ of 2862.50 ± 174.50 ng·h/mL. OA was also associated with serum albumin and triglyceride-rich lipoproteins, supporting the biological plausibility of lipid-matrix delivery [9].
These data do not establish antidiabetic efficacy, but they show that the tested formulation produces systemic exposure. This matters because a prevention or treatment signal is more credible when the intervention is known to reach circulation. BIO-OLTRAD also supports treating OA-enriched olive oil as a specific formulation rather than as generic OA [9].
OLTRAD is the key ongoing test of the adjunctive hypothesis. It is designed as a prospective, parallel-group, randomized, double-blind, controlled trial in patients with established T2DM receiving metformin therapy, either alone or with other antidiabetic drugs. Participants receive 55 mL/day of OA-enriched or control olive oil for 12 months, with HbA1c as the main glycemic variable [11]. This design directly addresses whether OA-enriched functional olive oil adds metabolic benefit beyond metformin-based standard care.
6.3. Clinical Interpretation and Evidence Gaps
The clinical interpretation of OA will depend on effect size, safety, adherence, and formulation specificity. A modest HbA1c reduction may be meaningful if the intervention is safe, inexpensive, acceptable, weight-neutral or weight-favorable, and compatible with current therapy [2,3]. Conversely, a statistically significant but very small effect would not justify adoption if adherence is poor, caloric intake increases, or adverse effects emerge.
Because the intervention is delivered as olive oil, glycemic outcomes should be interpreted together with body weight, waist circumference, lipid profile, blood pressure, liver enzymes, kidney markers, inflammatory biomarkers, adverse events, medication changes, and dietary substitution. Intake of 55 mL/day of oil contributes substantial dietary fat and energy; therefore, trials should assess whether participants replace other culinary fats or simply add the study oil to their usual diet [10,11].
Several gaps remain. No completed large trial has shown that OA lowers HbA1c in patients with established T2DM receiving standard therapy. Human evidence is concentrated on OA-enriched olive oil, which prevents direct extrapolation to capsules, extracts, or nanoformulations. Exposure-response relationships remain undefined, and long-term safety data are sparse in patients with polypharmacy, liver disease, kidney disease, or cardiovascular disease.
At present, OA-enriched functional olive oil should be viewed as an investigational adjunct. PREDIABOLE provides prevention-oriented proof of concept, BIO-OLTRAD confirms formulation-dependent systemic exposure, and OLTRAD is positioned to test adjunctive benefit in metformin-treated T2DM [9,10,11]. Together, these studies provide a coherent development pathway, but not yet enough evidence for clinical recommendation.
7. Safety, Interactions, and Regulatory Considerations
Any adjunctive intervention for T2DM would likely be used chronically and in patients with comorbidities, polypharmacy, and variable dietary adherence; safety is therefore a central issue for OA development. A food-derived compound should not be assumed to be safe once it is enriched, concentrated, reformulated, or consumed at a standardized daily dose. For OA, this issue is particularly important because experimental studies describe both hepatometabolic benefits and dose- or duration-dependent hepatic toxicity signals [51,52,58].
7.1. Exposure Scenario and Hepatic Safety
A key distinction is the difference between habitual dietary exposure and controlled exposure to OA-enriched formulations. Conventional olive products contain variable amounts of OA depending on cultivar, processing, fraction, storage, and analytical method [5]. In contrast, PREDIABOLE and OLTRAD use a standardized intervention of 55 mL/day olive oil providing approximately 30 mg/day OA [9,10,11]. This improves trial control but creates a different exposure scenario from ordinary dietary intake.
The liver is both a potential target of OA benefit and a potential organ of toxicity. OA has been reported to improve hepatic insulin resistance, lipid accumulation, oxidative stress, inflammation, and metabolic signaling in experimental diabetes models [21,49]. However, repeated oral OA administration in mice produced cholestatic liver injury at higher doses, and longer exposure to lower doses has been associated with liver injury, fibrosis, altered bile acid-metabolism genes, and transforming growth factor beta/Smad activation [51,58]. Additional work supports the view that OA may be hepatoprotective in some contexts but hepatotoxic at higher dose or prolonged exposure [52].
These animal toxicology findings are not directly comparable to 30 mg/day OA-enriched olive oil in humans, but they identify a plausible safety domain. Future trials should therefore monitor alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, gamma-glutamyl transferase, bilirubin, albumin, and prespecified hepatic adverse-event thresholds. This is especially relevant in T2DM because metabolic dysfunction-associated steatotic liver disease, gallbladder disease, alcohol exposure, and concomitant hepatotoxic medications may modify risk.
7.2. Renal, Cardiovascular, and Drug-Interaction Considerations
Renal safety is also important because chronic kidney disease is a common diabetes complication requiring systematic screening and longitudinal monitoring [59], and preclinical studies of OA have reported effects on diabetic nephropathy and renal inflammatory or injury markers [35,36,60]. The clinical history of bardoxolone methyl, a synthetic triterpenoid Nrf2 activator, is a useful cautionary example: despite early improvement in estimated glomerular filtration rate, the BEACON trial in patients with T2DM and advanced chronic kidney disease was terminated because of excess heart failure events [53]. Bardoxolone methyl is not OA, but this experience shows that triterpenoid-related mechanisms can produce unexpected safety signals in high-risk diabetic populations.
For OA-enriched olive oil, renal monitoring should include serum creatinine, estimated glomerular filtration rate, urinary albumin-to-creatinine ratio, and adverse events related to edema or volume status, especially if future trials include patients with chronic kidney disease or combine OA with sodium-glucose cotransporter 2 inhibitors, renin-angiotensin system blockers, diuretics, or other drugs affecting renal hemodynamics.
Potential drug interactions should be considered at pharmacokinetic and pharmacodynamic levels. In vitro data show that OA can inhibit CYP1A2- and CYP3A4-mediated reactions and can be metabolized by CYP3A4 to hydroxylated products [54,55]. The clinical relevance of these findings at concentrations achieved with OA-enriched olive oil is uncertain. Metformin is less likely to be affected by CYP-mediated interaction because it is not substantially metabolized by cytochrome P450 enzymes and relies mainly on membrane transporters for pharmacokinetics and response [50]. Nevertheless, trials should document concomitant medications, hypoglycemia events, dose changes, and adverse events, particularly in participants using insulin, sulfonylureas, glinides, anticoagulants, antiplatelet agents, statins, or antihypertensive drugs.
7.3. Dietary Safety, Adherence, and Implementation Risk
The olive oil matrix introduces safety and feasibility issues that are absent from purified-compound trials. A daily dose of 55 mL oil contributes substantial fat and energy [10,11]. If it replaces other culinary fats, it may fit a Mediterranean-style diet; if it is added without compensation, it could increase total energy intake and affect body weight, lipid profile, and glycemic control. Trials should therefore record dietary substitution, total energy intake, body weight, waist circumference, gastrointestinal symptoms, taste acceptability, and adherence.
Adherence should not be treated as a minor operational detail. For a chronic functional-food adjunct, feasibility depends on taste, cost, culinary habits, gastrointestinal tolerability, cultural dietary fit, and willingness to consume a fixed daily volume of oil. Returned oil volume, bottle weight, dietary records, structured interviews, and exposure markers such as serum or lipoprotein-associated OA should be used where possible.
7.4. Regulatory Positioning and Communication
The regulatory status of OA-enriched products depends on jurisdiction, formulation, concentration, intended use, and claims. A product positioned as a food, dietary supplement, nutraceutical, medical food, or drug-like formulation may face different evidentiary, manufacturing, labeling, and surveillance requirements. In the United States and European Union, OA-enriched products may fall under food, supplement, botanical, or drug-related frameworks depending on formulation, intended use, and claims [57,61].
Disease claims are especially sensitive in diabetes. Products claiming to cure, treat, mitigate, or prevent diabetes may be considered unapproved drugs unless evaluated and authorized for that intended use [56]. Therefore, OA should currently be described as an investigational adjunct rather than a proven antidiabetic therapy. Patient-facing communication should clearly state that OA-enriched functional foods may complement, but should not replace, evidence-based pharmacotherapy.
7.5. Translational Interpretation
The safety profile of OA is promising but not settled. Human functional olive oil studies have not reported major intervention-related adverse effects to date, and BIO-OLTRAD supports measurable systemic exposure after a 30 mg OA dose [9,10]. However, preclinical toxicology shows hepatic risk under certain dose and duration conditions [51,52,58], and in vitro data raise theoretical but unproven interaction concerns [54,55]. The appropriate development pathway is therefore controlled, formulation-specific, and safety-monitored.
Future trials should report adverse events, serious adverse events, discontinuations, hypoglycemia, gastrointestinal symptoms, hepatic and renal laboratory markers, medication changes, adherence, and dietary displacement. If OA-enriched olive oil demonstrates clinically relevant benefit without hepatic, renal, cardiovascular, or interaction-related concerns, it may justify consideration as an adjunctive option. Until then, it should remain investigational rather than being promoted as a natural antidiabetic product.
8. Patient-Centered Outcomes and Clinical Trial Endpoints
Endpoint selection in OA trials should reflect both the proposed mechanism of action and the practical realities of a food-based adjunctive intervention. Table 2 proposes a practical endpoint framework for future OA trials in T2DM.
Because OA-enriched olive oil is both a dietary intervention and a bioactive formulation, trial outcomes should not be limited to glycated hemoglobin. HbA1c remains the most appropriate primary endpoint for longer adjunctive-treatment trials because it reflects average glycemia over approximately two to three months and is embedded in diabetes guidelines and clinical decision-making [2,3,62]. However, HbA1c should be interpreted alongside fasting plasma glucose, postprandial glucose, insulin resistance indices, body weight, lipid profile, cardiometabolic markers, hepatic and renal safety markers, adherence, and patient-reported outcomes [16,63,64,65].
Continuous glucose monitoring may be particularly informative in OA trials because the intervention is consumed with meals and may influence postprandial glucose and lipid handling. A prespecified CGM substudy could assess time in range, time above range, time below range, mean glucose, glycemic variability, and postprandial excursions after meals containing the study oil. These metrics may detect changes in glycemic quality that are not captured by HbA1c alone and may also identify hypoglycemia risk in patients receiving insulin or insulin secretagogues [66].
Mechanistic endpoints should be selected to match the proposed biology of OA. Fasting insulin, C-peptide, HOMA-IR, oral glucose tolerance-derived indices, triglycerides, liver enzymes, high-sensitivity C-reactive protein, interleukin-6, oxidative stress markers, and lipoprotein-associated OA may help clarify whether any clinical effect is linked to insulin sensitivity, hepatic metabolism, inflammation, oxidative stress, or formulation-dependent exposure [6,7,9,21,30,31]. These biomarkers should remain supportive rather than substituting for clinical endpoints.
Safety endpoints are essential because OA has shown both hepatometabolic benefit and hepatic toxicity signals in experimental settings. Core monitoring should include alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, gamma-glutamyl transferase, bilirubin, albumin, serum creatinine, estimated glomerular filtration rate, urinary albumin-to-creatinine ratio, hypoglycemia events, gastrointestinal symptoms, body weight, blood pressure, edema, adverse events, serious adverse events, and medication changes [51,52,53,58,59,60]. Hepatic, renal, and cardiovascular monitoring should be proportionate to baseline risk and background therapy.
Adherence and dietary substitution should be treated as clinical outcomes, not only as trial logistics. In PREDIABOLE and OLTRAD, the assigned oil dose was 55 mL/day [10,11]. This amount may be feasible in Mediterranean-style dietary patterns, but it can increase total energy intake if it is added rather than substituted for other fats. Trials should therefore assess returned oil volume, bottle weight, dietary records, total energy intake, replacement of other culinary fats, taste acceptability, gastrointestinal tolerability, cost, and willingness to continue.
Patient-reported outcomes are also important because the real-world value of a functional-food adjunct depends on daily use. Relevant domains include treatment burden, dietary satisfaction, gastrointestinal comfort, perceived ease of use, diabetes-related distress, quality of life, and compatibility with usual meals. These outcomes should be prespecified and reported according to established guidance for patient-reported outcomes in randomized trials [67,68].
Overall, the endpoint framework for OA trials should match its hypothesized role: adjunctive metabolic support rather than replacement pharmacotherapy. A favorable study would need to show not only improved HbA1c or glycemic variability, but also acceptable safety, stable or favorable weight and lipid effects, good adherence, and patient acceptability. Conversely, biomarker improvement without patient-relevant benefit would not be enough to support clinical use.
9. Translational Gaps and Future Research Agenda
The evidence base for OA in T2DM has moved beyond isolated mechanistic observations, but it remains insufficient for clinical recommendation. Current support comes from four connected domains: preclinical studies showing biological plausibility, human pharmacokinetic data demonstrating formulation-dependent exposure, PREDIABOLE suggesting prevention-oriented benefit in prediabetes, and OLTRAD testing the adjunctive-treatment hypothesis in metformin-treated T2DM [6,9,10,11]. The next stage should clarify which patients may benefit, which formulation is clinically relevant, whether exposure predicts response, and whether long-term use is safe.
9.1. Target Population and Responder Phenotype
The first unresolved question is the intended clinical niche. OA could be evaluated in at least three different groups: individuals with prediabetes, patients with early T2DM and preserved beta-cell function, and patients with established T2DM characterized by insulin resistance, hepatic steatosis, hypertriglyceridemia, or low-grade inflammation. These populations should not be merged without stratification. Prevention trials should focus on incident diabetes and cardiometabolic-risk modification, whereas adjunctive-treatment trials should prioritize HbA1c, CGM-derived metrics, safety, adherence, and medication burden. PREDIABOLE supports the prevention hypothesis, while OLTRAD addresses the established-T2DM adjunctive hypothesis [10,11]. Future studies should therefore prespecify whether OA is being tested as a prevention strategy, a dietary adjunct, a formulation platform, or a pharmaceutical lead. Phenotype-guided designs may be particularly useful. Patients with higher insulin resistance, elevated triglycerides, metabolic dysfunction-associated steatotic liver disease, inflammatory activation, early renal-risk markers, or early disease duration may be more likely to show a measurable response, although this remains unproven [15,16,23,32,35].
9.2. Exposure-Response and Formulation Standardization
A major translational gap is the lack of exposure-response data. BIO-OLTRAD showed that 30 mg OA in functional olive oil produces measurable serum concentrations and transport through albumin and triglyceride-rich lipoproteins [9]. However, it is unknown whether higher OA exposure predicts greater glycemic improvement, stronger biomarker changes, more adverse events, or no clinically relevant difference. Future trials should include pharmacokinetic or sparse-sampling substudies to link adherence, absorption, systemic exposure, and clinical response.
Formulation standardization is equally important. The current human evidence mainly concerns OA-enriched olive oil, not generic OA. A 30 mg OA dose delivered in olive oil cannot be assumed to be equivalent to the same nominal dose in a capsule, extract, suspension, or nanoformulation [9,47]. Trial reports should specify OA source, purity, enrichment method, oil volume, fatty acid profile where relevant, coexisting triterpenes or phenolics, storage conditions, batch consistency, and analytical confirmation of dose. Comparator selection should also match the scientific question: testing OA enrichment requires a matrix-matched control oil, whereas capsule-based formulations require a different comparator strategy [46].
9.3. Trial Design, Biomarkers, and Reporting Quality
Future OA trials should follow standards expected for pharmacologic adjuncts, even when the intervention is positioned as a functional food or nutraceutical. Protocols should prespecify the primary endpoint, statistical analysis plan, rescue medication rules, adherence criteria, safety thresholds, missing-data handling, subgroup analyses, and exposure-response analyses. TIDieR, SPIRIT, and CONSORT provide useful frameworks for intervention description, protocol design, and trial reporting [69,70,71].
Mechanistic biomarkers should be included, but they should not replace clinical endpoints. Preclinical evidence implicates insulin signaling, hepatic glucose production, oxidative stress, Nrf2-related defenses, inflammatory signaling, macrophage activation, and lipid metabolism [6,21,30,31,49]. Human studies should therefore select biomarkers that directly map to the hypothesized mechanism, such as fasting insulin, C-peptide, HOMA-IR, triglycerides, liver enzymes, high-sensitivity C-reactive protein, interleukin-6, oxidative stress markers, and lipoprotein-associated OA. Broad exploratory biomarker panels without prespecified interpretation should be avoided.
9.4. Long-Term Safety and Implementation
Long-term safety remains a central uncertainty. Human studies of OA-enriched olive oil are reassuring but limited in size, duration, and population complexity [9,10]. Preclinical toxicology also shows that OA can produce hepatotoxic or cholestatic effects under certain dose and exposure conditions [51,52,58]. Future studies should therefore monitor hepatic, renal, cardiovascular, gastrointestinal, and hypoglycemic events, particularly in patients with metabolic dysfunction-associated steatotic liver disease, chronic kidney disease, diabetic cardiomyopathy risk, polypharmacy, gallbladder disease, insulin therapy, or sulfonylurea use [23,59,60,63,64,65].
Implementation should be studied alongside efficacy. A daily dose of 55 mL olive oil may be feasible in Mediterranean-style dietary patterns but difficult in other settings. Trials should assess dietary substitution, total energy intake, adherence, taste acceptability, gastrointestinal tolerability, cost, and willingness to continue. If OA-enriched products are expensive or marketed with exaggerated claims, they could widen disparities or divert patients from evidence-based therapy. Patient-facing communication should therefore clearly distinguish adjunctive use from medication replacement [56,61].
9.5. Proposed Research Agenda
A staged development pathway is most appropriate. First, mechanistic human studies should link OA exposure to insulin sensitivity, postprandial glucose and lipid metabolism, oxidative-inflammatory biomarkers, and hepatic safety markers. Second, randomized controlled trials in metformin-treated T2DM should test HbA1c and CGM outcomes using matrix-matched comparators and standardized dietary-substitution instructions. Third, larger multicenter studies should evaluate durability, safety, responder phenotypes, and compatibility with contemporary therapies such as sodium-glucose cotransporter 2 inhibitors and glucagon-like peptide-1 receptor agonists. Finally, pragmatic studies should assess adherence, cost, dietary fit, and generalizability across clinical settings.
The future of OA in T2DM will depend on four thresholds: reproducible systemic exposure, clinically relevant efficacy beyond standard care, acceptable long-term safety, and practical implementation. Current evidence supports continued investigation, not routine clinical use. If ongoing and future trials meet these thresholds, OA-enriched functional olive oil may become a credible adjunct for selected patients with T2DM. If they do not, OA should remain an experimental candidate with mechanistic interest but no established clinical role.
10. Conclusion
OA is a plausible adjunctive candidate for T2DM, but the evidence currently supports further clinical investigation rather than routine use. Preclinical studies link OA to insulin signaling, hepatic glucose production, oxidative stress, inflammation, lipid metabolism, and beta-cell stress. Human data add two important translational signals: PREDIABOLE suggests prevention-oriented benefit in prediabetes, and BIO-OLTRAD shows that 30 mg OA delivered in functional olive oil can achieve measurable systemic exposure [9,10]. These findings justify ongoing adjunctive testing in metformin-treated T2DM, but they do not yet establish therapeutic efficacy.
The central question is whether a standardized, bioavailable, and acceptable OA formulation can improve patient-relevant outcomes beyond standard care without unacceptable safety or adherence burdens. At present, OA should be framed as an investigational adjunct, not as an alternative to evidence-based pharmacotherapy. If ongoing and future studies demonstrate clinically meaningful glycemic benefit, acceptable hepatic and renal safety, good tolerability, and practical long-term use, OA-enriched functional olive oil may become a supportive option for selected patients with T2DM. Until then, the evidence supports cautious investigation rather than clinical adoption.
Author Contributions
Conceptualization, A.G.; methodology, A.G. writing—original draft preparation, A.G.; writing—review and editing, A.G., M.M.; visualization, A.G.; supervision, A.G and B.B.-C.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACC | acetyl-CoA carboxylase |
| AMPK | adenosine monophosphate-activated protein kinase |
| ARE | antioxidant response element |
| ARRIVE | Animal Research: Reporting of In Vivo Experiments |
| AUC0–∞ | area under the concentration–time curve from time zero to infinity |
| BEACON | bardoxolone methyl trial in type 2 diabetes and advanced chronic kidney disease |
| BIO-OLTRAD | human bioavailability study of oleanolic acid formulated as functional olive oil |
| CAT | catalase |
| CGM | continuous glucose monitoring |
| CYP1A2 | cytochrome P450 family 1 subfamily A member 2 |
| CYP3A4 | cytochrome P450 family 3 subfamily A member 4 |
| ERK | extracellular signal-regulated kinase |
| FoxO1 | forkhead box O1 |
| G6Pase | glucose-6-phosphatase |
| GLUT4 | glucose transporter 4 |
| GPx | glutathione peroxidase |
| HbA1c | glycated hemoglobin |
| HO-1 | heme oxygenase-1 |
| HOMA-B | homeostatic model assessment of beta-cell function |
| HOMA-IR | homeostatic model assessment of insulin resistance |
| IL-1β | interleukin-1 beta |
| IL-6 | interleukin-6 |
| IL-18 | interleukin-18 |
| IRS | insulin receptor substrate |
| JNK | c-Jun N-terminal kinase |
| MAPK | mitogen-activated protein kinase |
| MEDLINE | Medical Literature Analysis and Retrieval System Online |
| M1/M2 | classically activated/pro-inflammatory and alternatively activated/anti-inflammatory macrophage phenotypes |
| NF-κB | nuclear factor kappa B |
| NLRP3 | NOD-like receptor family pyrin domain-containing 3 |
| NQO1 | NAD(P)H quinone dehydrogenase 1 |
| Nrf2 | nuclear factor erythroid 2-related factor 2 |
| OA | oleanolic acid |
| OLTRAD | Oleanolic Acid as Therapeutic Adjuvant for Type 2 Diabetes Mellitus |
| p38 | p38 mitogen-activated protein kinase |
| PEPCK | phosphoenolpyruvate carboxykinase |
| PI3K/Akt | phosphatidylinositol 3-kinase/protein kinase B |
| PI3K/Akt/FoxO1 | phosphatidylinositol 3-kinase/protein kinase B/forkhead box O1 |
| PREDIABOLE | randomized controlled trial of oleanolic acid-enriched olive oil in prediabetes |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROSPERO | International Prospective Register of Systematic Reviews |
| ROS | reactive oxygen species |
| SOD | superoxide dismutase |
| SPIRIT | Standard Protocol Items: Recommendations for Interventional Trials |
| T2DM | type 2 diabetes mellitus |
| TIDieR | Template for Intervention Description and Replication |
| TNF-α | tumor necrosis factor alpha |
References
- Genitsaridi, I.; Salpea, P.; Salim, A.; Sajjadi, S.F.; Tomic, D.; James, S.; Thirunavukkarasu, S.; Issaka, A.; Chen, L.; Basit, A.; et al. 11th Edition of the IDF Diabetes Atlas: Global, Regional, and National Diabetes Prevalence Estimates for 2024 and Projections for 2050. Lancet Diabetes Endocrinol. 2026, 14, 149–156. [CrossRef]
- American Diabetes Association Professional Practice Committee for Diabetes*; Bajaj, M.; McCoy, R.G.; Balapattabi, K.; Bannuru, R.R.; Bellini, N.J.; Bennett, A.K.; Beverly, E.A.; Briggs Early, K.; ChallaSivaKanaka, S.; et al. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2026. Diabetes Care 2026, 49, S183–S215. [CrossRef]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022, 45, 2753–2786. [CrossRef]
- Castellano, J.M.; Guinda, A.; Delgado, T.; Rada, M.; Cayuela, J.A. Biochemical Basis of the Antidiabetic Activity of Oleanolic Acid and Related Pentacyclic Triterpenes. Diabetes 2013, 62, 1791–1799. [CrossRef]
- Castellano, J.M.; Ramos-Romero, S.; Perona, J.S. Oleanolic Acid: Extraction, Characterization and Biological Activity. Nutrients 2022, 14, 623. [CrossRef]
- Fernández-Aparicio, Á.; Correa-Rodríguez, M.; Castellano, J.M.; Schmidt-RioValle, J.; Perona, J.S.; González-Jiménez, E. Potential Molecular Targets of Oleanolic Acid in Insulin Resistance and Underlying Oxidative Stress: A Systematic Review. Antioxidants 2022, 11, 1517. [CrossRef]
- Wang, X.; Chen, Y.; Abdelkader, D.; Hassan, W.; Sun, H.; Liu, J. Combination Therapy with Oleanolic Acid and Metformin as a Synergistic Treatment for Diabetes. J. Diabetes Res. 2015, 2015, 1–12. [CrossRef]
- Rada, M.; Castellano, J.M.; Perona, J.S.; Guinda, Á. GC-FID Determination and Pharmacokinetic Studies of Oleanolic Acid in Human Serum. Biomed. Chromatogr. 2015, 29, 1687–1692. [CrossRef]
- García-González, A.; Espinosa-Cabello, J.M.; Cerrillo, I.; Montero-Romero, E.; Rivas-Melo, J.J.; Romero-Báez, A.; Jiménez-Andreu, M.D.; Ruíz-Trillo, C.A.; Rodríguez-Rodríguez, A.; Martínez-Ortega, A.J.; et al. Bioavailability and Systemic Transport of Oleanolic Acid in Humans, Formulated as a Functional Olive Oil. Food Funct. 2023, 14, 9681–9694. [CrossRef]
- Santos-Lozano, J.M.; Rada, M.; Lapetra, J.; Guinda, Á.; Jiménez-Rodríguez, M.C.; Cayuela, J.A.; Ángel-Lugo, A.; Vilches-Arenas, Á.; Gómez-Martín, A.M.; Ortega-Calvo, M.; et al. Prevention of Type 2 Diabetes in Prediabetic Patients by Using Functional Olive Oil Enriched in Oleanolic Acid: The PREDIABOLE Study, a Randomized Controlled Trial. Diabetes Obes. Metab. 2019, 21, 2526–2534. [CrossRef]
- Castellano, J.M. Oleanolic Acid as Therapeutic Adjuvant for Type 2 Diabetes Mellitus (OLTRAD STUDY); clinicaltrials.gov, 2025.
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—a Scale for the Quality Assessment of Narrative Review Articles. Res. Integr. Peer Rev. 2019, 4, 5. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, n71. [CrossRef]
- Sasmita, D.; Gurudutta, P.; Nityananda, S.; Biswakanth, K. The Promising Role of Oleanolic Acid in the Management of Diabetes Mellitus: A Review. J. Appl. Pharm. Sci. 2021. [CrossRef]
- Claro-Cala, C.M.; Jiménez-Altayó, F.; Zagmutt, S.; Rodriguez-Rodriguez, R. Molecular Mechanisms Underlying the Effects of Olive Oil Triterpenic Acids in Obesity and Related Diseases. Nutrients 2022, 14, 1606. [CrossRef]
- Luo, Q.; Wei, Y.; Lv, X.; Chen, W.; Yang, D.; Tuo, Q. The Effect and Mechanism of Oleanolic Acid in the Treatment of Metabolic Syndrome and Related Cardiovascular Diseases. Molecules 2024, 29, 758. [CrossRef]
- DeFronzo, R.A. From the Triumvirate to the Ominous Octet: A New Paradigm for the Treatment of Type 2 Diabetes Mellitus. Diabetes 2009, 58, 773–795. [CrossRef]
- Kahn, B.B.; Flier, J.S. Obesity and Insulin Resistance. J. Clin. Invest. 2000, 106, 473–481. [CrossRef]
- Loza-Rodríguez, H.; Estrada-Soto, S.; Alarcón-Aguilar, F.J.; Huang, F.; Aquino-Jarquín, G.; Fortis-Barrera, Á.; Giacoman-Martínez, A.; Almanza-Pérez, J.C. Oleanolic Acid Induces a Dual Agonist Action on PPARγ/α and GLUT4 Translocation: A Pentacyclic Triterpene for Dyslipidemia and Type 2 Diabetes. Eur. J. Pharmacol. 2020, 883, 173252. [CrossRef]
- Radwan, M.O.; Kadasah, S.F.; Aljubiri, S.M.; Alrefaei, A.F.; El-Maghrabey, M.H.; El Hamd, M.A.; Tateishi, H.; Otsuka, M.; Fujita, M. Harnessing Oleanolic Acid and Its Derivatives as Modulators of Metabolic Nuclear Receptors. Biomolecules 2023, 13, 1465. [CrossRef]
- Wang, X.; Liu, R.; Zhang, W.; Zhang, X.; Liao, N.; Wang, Z.; Li, W.; Qin, X.; Hai, C. Oleanolic Acid Improves Hepatic Insulin Resistance via Antioxidant, Hypolipidemic and Anti-Inflammatory Effects. Mol. Cell. Endocrinol. 2013, 376, 70–80. [CrossRef]
- Zeng, X.-Y.; Wang, Y.-P.; Cantley, J.; Iseli, T.J.; Molero, J.C.; Hegarty, B.D.; Kraegen, E.W.; Ye, Y.; Ye, J.-M. Oleanolic Acid Reduces Hyperglycemia beyond Treatment Period with Akt/FoxO1-Induced Suppression of Hepatic Gluconeogenesis in Type-2 Diabetic Mice. PLoS ONE 2012, 7, e42115. [CrossRef]
- Gamede, M.; Mabuza, L.; Ngubane, P.; Khathi, A. Plant-Derived Oleanolic Acid Ameliorates Markers Associated with Non-Alcoholic Fatty Liver Disease in a Diet-Induced Pre-Diabetes Rat Model. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, Volume 12, 1953–1962. [CrossRef]
- Brownlee, M. Biochemistry and Molecular Cell Biology of Diabetic Complications. Nature 2001, 414, 813–820. [CrossRef]
- Ceriello, A.; Motz, E. Is Oxidative Stress the Pathogenic Mechanism Underlying Insulin Resistance, Diabetes, and Cardiovascular Disease? The Common Soil Hypothesis Revisited. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 816–823. [CrossRef]
- Günther, A.; Bednarczyk-Cwynar, B. Oleanolic Acid: A Promising Antioxidant—Sources, Mechanisms of Action, Therapeutic Potential, and Enhancement of Bioactivity. Antioxidants 2025, 14, 598. [CrossRef]
- Günther, A.; Bednarczyk-Cwynar, B. Oleanolic Acid in Organelle Stress: Mitochondrial Dysfunction, Endoplasmic Reticulum Stress, Autophagy, and Apoptosis. Stresses 2026, 6, 22. [CrossRef]
- Hotamisligil, G.S. Inflammation and Metabolic Disorders. Nature 2006, 444, 860–867. [CrossRef]
- Donath, M.Y.; Shoelson, S.E. Type 2 Diabetes as an Inflammatory Disease. Nat. Rev. Immunol. 2011, 11, 98–107. [CrossRef]
- Li, W.; Zeng, H.; Xu, M.; Huang, C.; Tao, L.; Li, J.; Zhang, T.; Chen, H.; Xia, J.; Li, C.; et al. Oleanolic Acid Improves Obesity-Related Inflammation and Insulin Resistance by Regulating Macrophages Activation. Front. Pharmacol. 2021, 12, 697483. [CrossRef]
- Gamede, M.; Mabuza, L.; Ngubane, P.; Khathi, A. Plant-Derived Oleanolic Acid Ameliorates Markers of Subclinical Inflammation and Innate Immunity Activation in Diet-Induced Pre-Diabetic Rats. Ther. Adv. Endocrinol. Metab. 2020, 11, 2042018820935771. [CrossRef]
- Gamede, M.; Mabuza, L.; Ngubane, P.; Khathi, A. The Effects of Plant-Derived Oleanolic Acid on Selected Parameters of Glucose Homeostasis in a Diet-Induced Pre-Diabetic Rat Model. Molecules 2018, 23, 794. [CrossRef]
- Rena, G.; Hardie, D.G.; Pearson, E.R. The Mechanisms of Action of Metformin. Diabetologia 2017, 60, 1577–1585. [CrossRef]
- Percie Du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE Guidelines 2.0: Updated Guidelines for Reporting Animal Research. PLOS Biol. 2020, 18, e3000410. [CrossRef]
- Dubey, V.K.; Patil, C.R.; Kamble, S.M.; Tidke, P.S.; Patil, K.R.; Maniya, P.J.; Jadhav, R.B.; Patil, S.P. Oleanolic Acid Prevents Progression of Streptozotocin Induced Diabetic Nephropathy and Protects Renal Microstructures in Sprague Dawley Rats. J. Pharmacol. Pharmacother. 2013, 4, 47–52. [CrossRef]
- Iskender, H.; Dokumacıoglu, E.; Hayirli, A.; Terim Kapakin, K.A.; Bolat, I.; Manavoglu Kirman, E. Effects of Oleanolic Acid Administration on Renal NF-κB/IL-18/IL-6 and YKL-40/KIM-1 Pathways in Experimental Diabetic Rats. Iran. J. Basic Med. Sci. 2023, 26. [CrossRef]
- Porter, C.J.H.; Trevaskis, N.L.; Charman, W.N. Lipids and Lipid-Based Formulations: Optimizing the Oral Delivery of Lipophilic Drugs. Nat. Rev. Drug Discov. 2007, 6, 231–248. [CrossRef]
- Rezhdo, O.; Speciner, L.; Carrier, R. Lipid-Associated Oral Delivery: Mechanisms and Analysis of Oral Absorption Enhancement. J. Controlled Release 2016, 240, 544–560. [CrossRef]
- Wasim, M.; Bergonzi, M.C. Unlocking the Potential of Oleanolic Acid: Integrating Pharmacological Insights and Advancements in Delivery Systems. Pharmaceutics 2024, 16, 692. [CrossRef]
- Xi, J.; Chang, Q.; Chan, C.K.; Meng, Z.Y.; Wang, G.N.; Sun, J.B.; Wang, Y.T.; Tong, H.H.Y.; Zheng, Y. Formulation Development and Bioavailability Evaluation of a Self-Nanoemulsified Drug Delivery System of Oleanolic Acid. AAPS PharmSciTech 2009, 10, 172–182. [CrossRef]
- Song, M.; Hang, T.; Wang, Y.; Jiang, L.; Wu, X.; Zhang, Z.; Shen, J.; Zhang, Y. Determination of Oleanolic Acid in Human Plasma and Study of Its Pharmacokinetics in Chinese Healthy Male Volunteers by HPLC Tandem Mass Spectrometry. J. Pharm. Biomed. Anal. 2006, 40, 190–196. [CrossRef]
- De Stefani, C.; Lodovichi, J.; Albonetti, L.; Salvatici, M.C.; Quintela, J.C.; Bilia, A.R.; Bergonzi, M.C. Solubility and Permeability Enhancement of Oleanolic Acid by Solid Dispersion in Poloxamers and γ-CD. Molecules 2022, 27, 3042. [CrossRef]
- Su, L.; Yang; Huang; Dou; Zhai Self-Microemulsifying Drug Delivery System for Improved Oral Bioavailability of Oleanolic Acid: Design and Evaluation. Int. J. Nanomedicine 2013, 2917. [CrossRef]
- Stelling-Férez, J.; López-Miranda, S.; Gabaldón, J.A.; Nicolás, F.J. Oleanolic Acid Complexation with Cyclodextrins Improves Its Cell Bio-Availability and Biological Activities for Cell Migration. Int. J. Mol. Sci. 2023, 24, 14860. [CrossRef]
- Salas-Salvadó, J.; Bulló, M.; Babio, N.; Martínez-González, M.Á.; Ibarrola-Jurado, N.; Basora, J.; Estruch, R.; Covas, M.I.; Corella, D.; Arós, F.; et al. Reduction in the Incidence of Type 2 Diabetes With the Mediterranean Diet. Diabetes Care 2011, 34, 14–19. [CrossRef]
- Schwingshackl, L.; Lampousi, A.-M.; Portillo, M.P.; Romaguera, D.; Hoffmann, G.; Boeing, H. Olive Oil in the Prevention and Management of Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Cohort Studies and Intervention Trials. Nutr. Diabetes 2017, 7, e262–e262. [CrossRef]
- Das, I.; Rajagopal, N.; Reddy, Y.; Kampa Sundara, B. Oleanolic Acid in Nanomedicine: Emerging Formulation Strategies and Applications. J. Pharm. Innov. 2025, 20, 266. [CrossRef]
- Chen, M.; Zhong, Z.; Tan, W.; Wang, S.; Wang, Y. Recent Advances in Nanoparticle Formulation of Oleanolic Acid. Chin. Med. 2011, 6, 20. [CrossRef]
- Iskender, H.; Dokumacioglu, E.; Terim Kapakin, K.A.; Bolat, I.; Mokhtare, B.; Hayirli, A.; Yenice, G. Effect of Oleanolic Acid Administration on Hepatic AMPK, SIRT-1, IL-6 and NF-κB Levels in Experimental Diabetes. J. Diabetes Metab. Disord. 2023, 22, 581–590. [CrossRef]
- Liang, X.; Giacomini, K.M. Transporters Involved in Metformin Pharmacokinetics and Treatment Response. J. Pharm. Sci. 2017, 106, 2245–2250. [CrossRef]
- Xu, Y.; Yang, X.; Lu, Y.; Liu, J. Hepatotoxicity from Long-Term Administration of Hepatoprotective Low Doses of Oleanolic Acid in Mice. Toxicol. Appl. Pharmacol. 2025, 497, 117277. [CrossRef]
- Liu, J.; Lu, Y.; Wu, Q.; Xu, S.; Shi, F.; Klaassen, C.D. Oleanolic Acid Reprograms the Liver to Protect against Hepatotoxicants, but Is Hepatotoxic at High Doses. Liver Int. 2019, 39, 427–439. [CrossRef]
- De Zeeuw, D.; Akizawa, T.; Audhya, P.; Bakris, G.L.; Chin, M.; Christ-Schmidt, H.; Goldsberry, A.; Houser, M.; Krauth, M.; Lambers Heerspink, H.J.; et al. Bardoxolone Methyl in Type 2 Diabetes and Stage 4 Chronic Kidney Disease. N. Engl. J. Med. 2013, 369, 2492–2503. [CrossRef]
- Kim, K.-A.; Lee, J.-S.; Park, H.-J.; Kim, J.-W.; Kim, C.-J.; Shim, I.-S.; Kim, N.-J.; Han, S.-M.; Lim, S. Inhibition of Cytochrome P450 Activities by Oleanolic Acid and Ursolic Acid in Human Liver Microsomes. Life Sci. 2004, 74, 2769–2779. [CrossRef]
- Cao, N.T.; Nguyen, N.A.; Le, T.-K.; Cha, G.S.; Park, K.D.; Yun, C.-H. Regioselective Hydroxylation of Oleanolic Acid Catalyzed by Human CYP3A4 to Produce Hederagenenin, a Chiral Metabolite. Catalysts 2021, 11, 267. [CrossRef]
- Program, H.F. FDA and FTC Send Warning Letters to 10 Companies for Illegally Selling Dietary Supplements Claiming to Treat Diabetes. FDA 2024.
- Botanicals | EFSA Available online: https://www.efsa.europa.eu/en/topics/topic/botanicals (accessed on 21 May 2026).
- Lu, Y.-F.; Wan, X.-L.; Xu, Y.; Liu, J. Repeated Oral Administration of Oleanolic Acid Produces Cholestatic Liver Injury in Mice. Molecules 2013, 18, 3060–3071. [CrossRef]
- American Diabetes Association Professional Practice Committee for Diabetes*; Bajaj, M.; McCoy, R.G.; Balapattabi, K.; Bannuru, R.R.; Bellini, N.J.; Bennett, A.K.; Beverly, E.A.; Briggs Early, K.; ChallaSivaKanaka, S.; et al. 11. Chronic Kidney Disease and Risk Management: Standards of Care in Diabetes—2026. Diabetes Care 2026, 49, S246–S260. [CrossRef]
- Pan, D.; Qu, Y.; Shi, C.; Xu, C.; Zhang, J.; Du, H.; Chen, X. Oleanolic Acid and Its Analogues: Promising Therapeutics for Kidney Disease. Chin. Med. 2024, 19, 74. [CrossRef]
- Program, H.F. Dietary Supplements Available online: https://www.fda.gov/food/dietary-supplements (accessed on 21 May 2026).
- American Diabetes Association Professional Practice Committee for Diabetes*; Bajaj, M.; McCoy, R.G.; Balapattabi, K.; Bannuru, R.R.; Bellini, N.J.; Bennett, A.K.; Beverly, E.A.; Briggs Early, K.; ChallaSivaKanaka, S.; et al. 6. Glycemic Goals, Hypoglycemia, and Hyperglycemic Crises: Standards of Care in Diabetes—2026. Diabetes Care 2026, 49, S132–S149. [CrossRef]
- Li, W.-F.; Wang, P.; Li, H.; Li, T.-Y.; Feng, M.; Chen, S.-F. Oleanolic Acid Protects against Diabetic Cardiomyopathy via Modulation of the Nuclear Factor Erythroid 2 and Insulin Signaling Pathways. Exp. Ther. Med. 2017, 14, 848–854. [CrossRef]
- Li, C.; He, J.; Li, Y.; Zhang, C.; Wang, Z.; Wu, X.; Qi, F. Cardioprotective Role of Oleanolic Acid in Patients with Type 2 Diabetes Mellitus. Heliyon 2024, 10, e31303. [CrossRef]
- Mapanga, R.F.; Rajamani, U.; Dlamini, N.; Zungu-Edmondson, M.; Kelly-Laubscher, R.; Shafiullah, M.; Wahab, A.; Hasan, M.Y.; Fahim, M.A.; Rondeau, P.; et al. Oleanolic Acid: A Novel Cardioprotective Agent That Blunts Hyperglycemia-Induced Contractile Dysfunction. PLoS ONE 2012, 7, e47322. [CrossRef]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [CrossRef]
- Calvert, M.; Blazeby, J.; Altman, D.G.; Revicki, D.A.; Moher, D.; Brundage, M.D.; Consort Pro Group, F.T. Reporting of Patient-Reported Outcomes in Randomized Trials: The CONSORT PRO Extension. JAMA 2013, 309, 814. [CrossRef]
- Research, C. for D.E. and Patient-Focused Drug Development: Selecting, Developing, or Modifying Fit-for-Purpose Clinical Outcome Assessments Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/patient-focused-drug-development-selecting-developing-or-modifying-fit-purpose-clinical-outcome (accessed on 21 May 2026).
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) Checklist and Guide. BMJ 2014, 348, g1687–g1687. [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 Statement: Defining Standard Protocol Items for Clinical Trials. Ann. Intern. Med. 2013, 158, 200–207. [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; for the CONSORT Group CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 340, c332–c332. [CrossRef]
Figure 1.
Proposed translational pathway of oleanolic acid in type 2 diabetes.

Figure 2.
Mechanistic network linking oleanolic acid to insulin resistance and glucose metabolism.

Table 2.
Proposed clinical and patient-centered endpoints for future oleanolic acid trials in type 2 diabetes.
Table 2.
Proposed clinical and patient-centered endpoints for future oleanolic acid trials in type 2 diabetes.
| Endpoint domain | Core endpoints | Purpose | Suggested priority |
|---|---|---|---|
| Glycemic efficacy | HbA1c, fasting plasma glucose, postprandial glucose | Determine clinical metabolic benefit | Primary or key secondary |
| Glucose dynamics | Time in range, time above range, time below range, mean glucose, glycemic variability | Capture effects missed by HbA1c and identify hypoglycemia risk | CGM substudy or secondary |
| Insulin resistance and beta-cell function | Fasting insulin, C-peptide, HOMA-IR, HOMA-B, oral glucose tolerance test indices | Clarify mechanism and responder phenotype | Secondary or mechanistic |
| Cardiometabolic risk | Body weight, waist circumference, blood pressure, lipid profile, apolipoprotein B where feasible | Assess broader metabolic benefit or harm | Secondary |
| Inflammation and oxidative stress | High-sensitivity C-reactive protein, interleukin-6, tumor necrosis factor alpha, oxidative stress markers, Nrf2-related markers | Test mechanistic hypotheses | Exploratory unless powered |
| Hepatic safety | Alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, gamma-glutamyl transferase, bilirubin, albumin | Detect hepatocellular or cholestatic signals | Core safety |
| Renal safety | Estimated glomerular filtration rate, serum creatinine, urinary albumin-to-creatinine ratio | Monitor kidney safety in T2DM populations | Core safety |
| Drug interaction and medication burden | Hypoglycemia events, background medication changes, rescue therapy, concomitant drugs | Interpret adjunctive effect and safety | Core safety/clinical |
| Exposure and adherence | Serum OA, lipoprotein-associated OA, bottle counts, dietary records, returned oil volume | Link formulation exposure to response and adherence | Pharmacokinetic subset/core adherence |
| Patient-reported outcomes | Gastrointestinal tolerability, taste acceptability, treatment burden, dietary satisfaction, quality of life, willingness to continue | Evaluate feasibility and patient relevance | Secondary or implementation |
Abbreviations: AMPK, adenosine monophosphate-activated protein kinase; CGM, continuous glucose monitoring; HbA1c, glycated hemoglobin; HOMA-B, homeostatic model assessment of beta-cell function; HOMA-IR, homeostatic model assessment of insulin resistance; Nrf2, nuclear factor erythroid 2-related factor 2; OA, oleanolic acid; T2DM, type 2 diabetes mellitus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



