Submitted:
12 June 2026
Posted:
15 June 2026
You are already at the latest version
Abstract
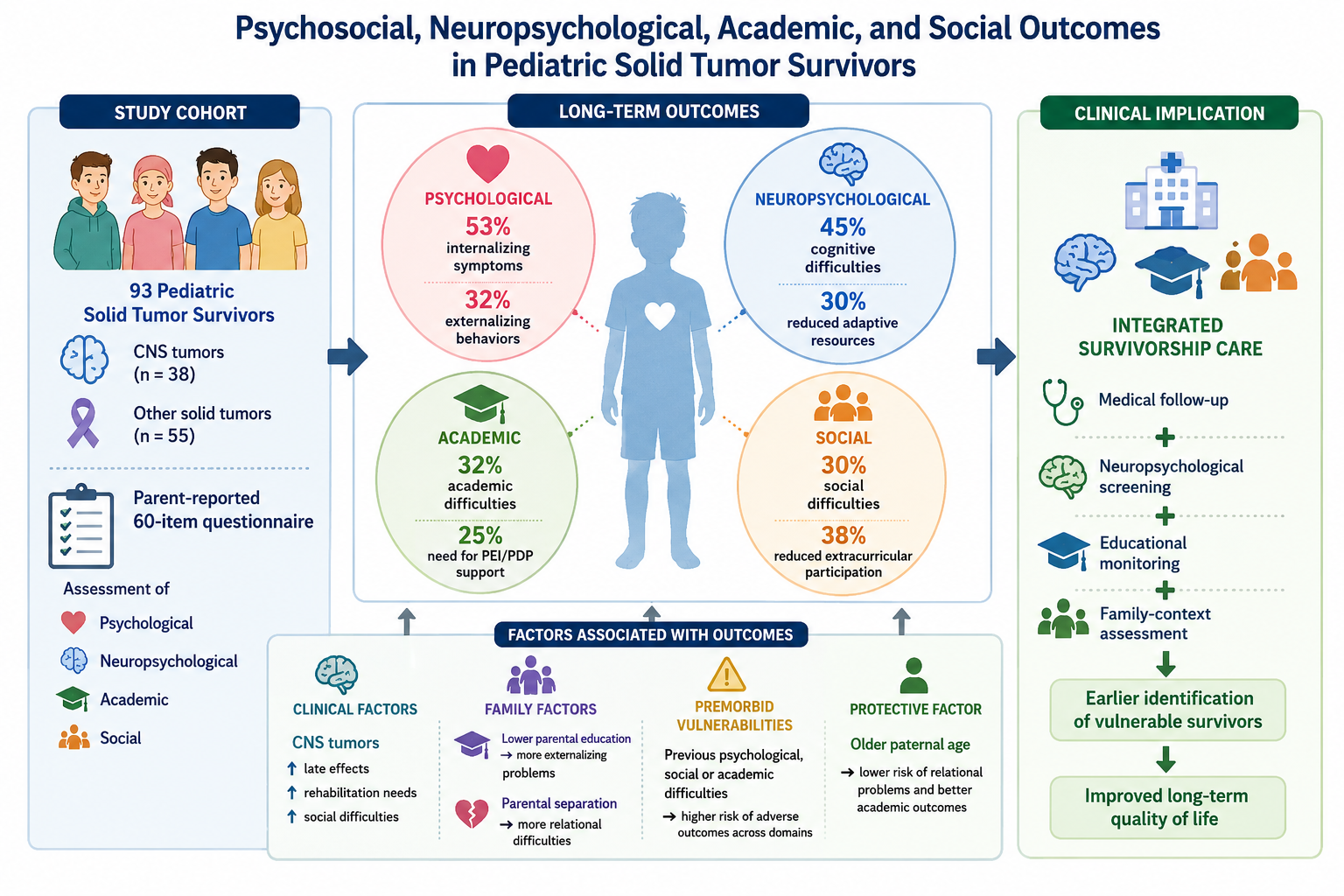
Background/Objectives: Long-term psychosocial/neurocognitive sequelae are frequently observed in survivors of pedi-atric cancer and adversely affect quality of life in adulthood. Although clinical predictors are well established, the con-tribution of familial, cultural, and socio-economic factors has received less attention. Methods: Between November 2022-January 2023, 93 survivors parents of pediatric patients with solid tumors including 38 individuals with central nervous system (CNS) tumors, completed a specifically designed 60-item questionnaire. Outcomes were evaluated across four domains—psychological, neurocognitive, academic, and social—along with a broad range of potential pre-dictors encompassing demographic, clinical, family-related, cultural, socio-economic, and premorbid characteristics. Statistical analyses included Fisher’s exact test and non-parametric methods. Results: New-onset or aggravated inter-nalizing symptoms were reported in 53% of survivors, externalizing behaviors in 32%, neurocognitive impairments in 45%. Academic difficulties were identified in 32%, with 25% requiring an Individualized-Education-Plan. Social chal-lenges affected 30% of participants and were more prevalent among CNS tumor survivors, who also demonstrated greater functional losses and rehabilitation needs. Lower parental educational attainment was associated with exter-nalizing symptoms (p = 0.039), whereas household income, parental occupation, and residential setting were not. Premorbid psychological or learning difficulties were strong predictors of adverse outcomes (all p < 0.01). Older paternal age was protective for relational and academic functioning, while having more siblings was linked to increased cogni-tive risk. Conclusions: Psychosocial and neurocognitive late effects remain common among pediatric cancer survivors. Educational background and premorbid vulnerabilities appear more influential than economic factors, supporting the need for targeted neuropsychological surveillance and family-centered screening strategies.
Keywords:
socio-economic determinants
; pediatric cancer survivors
; solid tumors
1. Introduction
Advances in pediatric oncology have led to a substantial increase in long-term survival, shifting clinical and research attention toward the late effects of cancer and its treatment. Among these, psychosocial, neuropsychological, academic, and social difficulties are increasingly recognized as major determinants of long-term functioning and quality of life in childhood cancer survivors [1,2,3,4,5,6]. These difficulties may persist into adolescence and adulthood, influencing educational attainment, interpersonal relationships, and social participation, sometimes to a degree comparable to or exceeding that of physical sequelae [7,8,9,10,11,12]. A large body of literature has documented the role of medical factors—such as tumor location, surgical excision, treatment intensity, exposure to radiotherapy, and neurological complications—in shaping neurocognitive and psychosocial outcomes [5,11,13,14,15,16]. Survivors of central nervous system (CNS) tumors, in particular, have consistently been shown to be at increased risk for cognitive impairment, emotional difficulties, academic decline, and social maladjustment. In parallel, individual and family-level variables, including parent–child communication, attachment quality, illness awareness, and coping strategies, have been identified as important protective or risk-modifying factors [17,18,19,20,21,22,23,24,25,26,27,28]. In contrast, broader socio-cultural and socioeconomic determinants have received comparatively less attention within pediatric oncology research. In the general pediatric population and in children with acquired brain injuries, socioeconomic conditions—particularly parental education—are robustly associated with cognitive development, emotional regulation, and adaptive functioning [30,31]. However, their role in pediatric cancer survivorship remains less clearly defined, especially when family educational background, cultural context, and structural characteristics are considered alongside traditional economic indicators such as income or occupation [5,11,16,28,29,30,31,32,33,34]. Moreover, most existing evidence derives from North American or Northern European settings, limiting the generalizability of findings to other healthcare and cultural contexts.
Understanding how family, cultural, and socioeconomic variables interact with medical factors is therefore essential for the development of equitable and targeted survivorship care models. In clinical practice, these contextual determinants may influence access to cognitive stimulation, educational support, emotional scaffolding, and rehabilitation services, thereby shaping long-term adjustment trajectories beyond disease-related risk alone.
Within this framework, the present study focused on a cohort of survivors of pediatric solid tumors, including CNS tumors, followed at a specialized oncology center. The objectives were twofold: (i) to describe psychological, neuropsychological, academic, and social outcomes after completion of therapy, and (ii) to explore their associations with family, cultural, and socioeconomic characteristics, as well as premorbid vulnerabilities. We hypothesized that family educational level and pre-existing psychological or scholastic difficulties would be associated with less favorable post-treatment outcomes, whereas traditional socioeconomic indicators and demographic variables would play a more limited role.
2. Materials and Methods
In the study period (November 2022–January 2023), an anonymous, purpose-built 60-item questionnaire was administered to parents of survivors who had completed therapy and were attending routine follow-up at our pediatric outpatient clinic (Supplementary material 1). The instrument was designed by a multidisciplinary team of psychologists, oncologists, and statisticians to collect information on socio-cultural, educational, and family variables that are not adequately covered by existing validated tools. Using multiple validated Italian scales (e.g., for anxiety, depression, cognition) would have substantially increased respondent burden and jeopardized feasibility across settings, potentially introducing non-response bias and limiting inclusiveness (especially for lower-literacy participants).
Most items are single-item factual or categorical indicators, for which internal consistency metrics (e.g., Cronbach’s α) are not appropriate. The psychological/cognitive items were included as brief contextual indicators, not as diagnostic measures. Several items were conceptually adapted from established Italian instruments assessing family functioning and socio-economic background (e.g., ISTAT and Ministry of Education surveys) to ensure cultural and linguistic appropriateness. Formal psychometric validation was not performed, as the primary aim of the study was exploratory and descriptive.
The instrument was purpose-built to (i) characterize four outcome domains (psychological, neuropsychological, social and academic, Supplementary Table 1) and (ii) record potential determinants drawn from six conceptual areas (demographic, clinical, family, cultural, socio-economic and premorbid characteristics, Supplementary Table 2). The questionnaire was divided into six thematic sections addressing: (i) patient demographics and clinical history, (ii) family composition and parental characteristics, (iii) socio-economic background, (iv) perinatal and developmental history, (v) schooling and extra-curricular activities, and (vi) psychological and behavioral functioning. Items were mainly dichotomous (yes/no) or categorical, allowing respondents to indicate the presence or absence of specific conditions both before and after cancer diagnosis. This design enabled the identification of cross-sectional associations as well as qualitative trajectories of change (e.g., emergence, persistence, or resolution of a given problem). Operational definitions and coding rules for all questionnaire items including are provided in the Supplementary material 2.
The sections addressing psychological, academic, and social outcomes were completed by parents based on their direct observation of the child’s behavior and functioning in everyday contexts.
We summarized continuous variables by medians and inter-quartile ranges and categorical variables by counts and percentages. Associations between candidate determinants and each outcome, and between treatment/disease consequences/outcomes and tumor type (brain vs. other) were examined with Pearson’s chi-squared or Fisher’s exact test for categorical data and with the Wilcoxon–Mann–Whitney or Kruskal–Wallis test for ordinal or continuous data, selecting the statistic that matched the number of comparison groups and the data distribution. Given the sample size (n = 93) and the large number of potential determinants, we limited inference to bivariate associations to avoid overfitting and low events-per-variable in multivariable models. Due to the exploratory purpose of the work, we retained a two-sided significance level of 0.05 without correcting for multiple comparisons and results should be interpreted as descriptive and hypothesis-generating. All analyses were performed in R (version 4.1.2).
3. Results
The distribution of variables potentially associated with psychological, neurocognitive, social, and academic difficulties is presented in Supplementary Tables 3–5, while the results of association analyses are shown in Table 1.
A total of 93 survivors were enrolled, with questionnaires completed by their parents. The patient cohort comprised 49 males (53%) and 44 females (47%). At the time of assessment, the median age was 16.2 years (IQR 10.9–20.5). The median time elapsed since diagnosis was 52.5 months (IQR 27.9–76.8), and the median age at diagnosis was 11.8 years (IQR 6.0–15.5). Most participants were students (78, 84%), while 9 (10%) were employed and 5 (5%) were unemployed. Thirty-eight survivors (41%) had been treated for central nervous system (CNS) tumors and 55 (59%) for non-CNS solid tumors. Treatment had consisted of combined surgery, chemotherapy, and radiotherapy in 29 cases (31%), surgery plus chemotherapy in 19 (20%), surgery alone in 24 (26%), and alternative treatments or follow-up only in 20 (23%). Fourteen patients (15%) had not been informed of their cancer diagnosis, whereas 71 (76%) received information during the acute phase and 8 (9%) after treatment completion. Subsequently, 76 survivors (83%) requested additional information about their illness, and 71 (77%) sought clarification regarding diagnostic or follow-up procedures. No functional sequelae were reported in 43 participants (47%); impairments involving one domain were noted in 41 (45%), and two domains in 8 (9%). Academic difficulties ranged from none (53/93, 58%) to four domains affected (1/93, 1%). Physical rehabilitation had been prescribed to 33 survivors (36%), and neuropsychological rehabilitation to 20 (22%).
According to parental reports, comparing post-treatment status with pre-diagnosis functioning, new or aggravated difficulties emerged across multiple areas. Relationship problems were described in 14 of 90 survivors (16%), social participation issues in 27 of 90 (30%), and discontinuation of at least one extracurricular activity in 33 of 87 (38%) (Figure 1).
These observations were based on parental qualitative comparisons rather than prospective longitudinal assessments.
Exploratory analyses indicated links between family or socio-demographic characteristics and reported outcomes. Among the 29 survivors exhibiting externalizing behaviors, 21 (71%) belonged to families with low-to-medium parental educational levels, compared with 8 (29%) from highly educated households (p = 0.039; Figure 1). No other socio-economic indicators—including household income, parental occupation, municipality size, or geographic region—showed significant associations, despite similar descriptive patterns (all p > 0.10).
Median paternal and maternal ages were 51.0 years (IQR 46.0–56.8) and 49.5 years (IQR 44.0–55.0), respectively. Higher paternal age was associated with fewer relational difficulties (p = 0.013) and showed a borderline association with academic stability (p = 0.048).
Sibling structure also appeared relevant. Newly identified cognitive-adaptive impairments were observed in 28% of only children, 50% of those with one sibling, and 65% of those with two siblings (p = 0.005), whereas academic decline did not differ significantly according to sibling number (p = 0.087). Relational difficulties were more frequent among children of separated or divorced parents compared with those from intact families (73% vs. 10%; p = 0.030). Pre-existing psychological symptoms or lower baseline academic performance were strong predictors of post-treatment difficulties (all p < 0.01).
Multimodal treatment was more common in CNS tumors (42% vs. 24%; p = 0.001). Severe functional sequelae were reported more frequently among CNS survivors (18% vs. 2%; p = 0.022), as were overall rehabilitation needs (47% vs. 27%; p = 0.031). Overall, neuropsychological impairments were reported in 45% of participants, with reduced adaptive resources in 30%. Only 10% underwent formal neuropsychological evaluation after treatment. Academic decline affected 32% of survivors, and 25% required an Individualized Education Plan or Personalized Didactic Plan. Social integration difficulties were significantly more common in CNS survivors (47% vs. 16%; p = 0.004), as was loss of adaptive resources (43% vs. 21%; p = 0.007). Structured neuropsychological assessment was prescribed and completed more frequently in the CNS group (18% vs. 4%; p = 0.047). Internalizing symptoms—such as anxiety, depression, withdrawal, or somatization—were newly reported or worsened in 48 survivors (52%), including 22 CNS patients (58%) and 26 non-CNS patients (50%) (p = 0.650). Externalizing behaviors—such as irritability, oppositionality, hyperactivity, or conduct problems—were observed in 29 participants (31%), 15 with CNS tumors (40%) and 14 with non-CNS tumors (27%) (p = 0.441). Scholastic decline showed no significant difference between groups (CNS 47% vs. non-CNS 28%; p = 0.179).
In summary, CNS survivors experienced a greater overall burden of late effects, influencing which risk factors reached statistical significance. Associations between internalizing symptoms and sex, age, and paternal age observed in the full cohort were no longer present after exclusion of CNS cases. A similar attenuation was observed for behavioral outcomes, where correlations evident in the total sample disappeared in analyses restricted to non-CNS survivors.
Conversely, two relationships became evident when CNS cases were excluded. Among the 55 non-CNS survivors, a longer treatment course was a significantly associated to reduced adaptive resources (p = 0.005), and older age at questionnaire completion inversely associated with new relational problems (p = 0.044).
Taken together, these findings outline a complex pattern of associations between medical, socio-demographic, and family variables and psychosocial outcomes after pediatric cancer. CNS tumor survivors exhibited the highest burden of late effects across domains, consistent with the greater treatment intensity and neurotoxicity typically associated with these conditions. However, socio-cultural and family-related factors—particularly parental education and family structure—also appeared to influence adjustment trajectories, suggesting that psychosocial vulnerability is not solely determined by clinical severity.
The observed variability across domains and subgroups underscores the multidimensional nature of survivorship in pediatric oncology. These exploratory data therefore highlight the need for integrated follow-up models that combine medical, neuropsychological, and socio-cultural perspectives. The implications of these findings will be further discussed in the next section.
4. Discussion
The present study explored psychosocial, neuropsychological, and academic outcomes in a cohort of pediatric cancer survivors, focusing on the role of family and socio-cultural factors. As expected, survivors of brain tumors reported the highest burden of late effects across domains, consistent with previous literature emphasizing the neurocognitive and psychosocial vulnerability of this group [5,11,15,16]. However, our findings also suggest that post-treatment adjustment is not solely determined by medical factors, but is meaningfully shaped by family-related and educational resources.
One of the most relevant findings was the association between lower parental educational level and increased externalizing behavioral problems. Unlike income, occupation, or residential area, parental education emerged as the only socioeconomic indicator significantly associated with outcome. This observation aligns with evidence from developmental and neuropsychological research highlighting parental education as a proxy for cognitive stimulation, health literacy, and capacity to navigate complex care and educational systems [28,29,35,36,37,38]. Importantly, this association was observed within a publicly funded healthcare system, suggesting that equal access to medical care does not fully mitigate the influence of educational disparities on psychosocial adjustment [9,18,19].
Family structure also appeared to play a role. Relational difficulties were more frequently reported among survivors from separated or divorced families, supporting previous findings that family instability may exacerbate vulnerability during and after pediatric illness. Additionally, premorbid psychological and scholastic difficulties were strong predictors of post-treatment problems across domains, reinforcing the notion that cancer-related stressors often interact with pre-existing vulnerabilities rather than acting in isolation. An original and exploratory finding was the apparent protective association between older paternal age and both relational and academic stability [23,24]. While this result should be interpreted cautiously, it may reflect greater emotional maturity, stability, or caregiving resources associated with older parenthood. Similar mechanisms have been hypothesized in studies examining family adaptation to chronic pediatric conditions, but this observation warrants confirmation in larger samples. Consistent with prior literature, CNS tumor survivors showed higher rates of neuropsychological difficulties, loss of adaptive resources, and social integration problems compared with survivors of non-CNS solid tumors [5,11,13,14,15,16]. Notably, only a minority of survivors underwent formal neuropsychological assessment after treatment, despite a substantial proportion showing difficulties in everyday functioning. This gap underscores the need for systematic neuropsychological follow-up, particularly for CNS survivors, but also highlights that non-CNS survivors may experience significant difficulties that risk being overlooked. Several limitations must be acknowledged. The questionnaire used in this study was purpose-built and not formally validated, and outcomes were based on parental report rather than standardized assessments. The cross-sectional design limits causal inference and relies on retrospective comparison with pre-diagnosis functioning, which may be subject to recall bias. In addition, the sample size constrained statistical power and precluded multivariable modeling, and the exploratory nature of the analyses increases the risk of type I error. Finally, the exclusion of hematological malignancies reflects the clinical focus of the center and limits generalizability.
5. Conclusions
Despite the above described limitations, this study provides preliminary evidence that family educational background, family structure, and premorbid functioning are relevant correlates of psychosocial and neuropsychological outcomes in pediatric cancer survivorship. These findings support an integrated model of follow-up care that combines medical surveillance with systematic assessment of family and socio-cultural resources. Future research should employ validated instruments, longitudinal designs, and multicenter samples to clarify causal pathways and to determine whether the observed patterns extend across different healthcare and cultural contexts. In conclusion, survivorship care in pediatric oncology should extend beyond disease-related risk stratification to include structured evaluation of family educational and relational resources. Such an approach may facilitate earlier identification of vulnerable survivors and support the development of personalized, equitable interventions aimed at optimizing long-term quality of life [40].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization: PG, AA, MM, FB; Data curation: all authors; Formal analysis: PG, AA, FB, MM; Investigation: LC, ON, VB, ES, MT, MM; Methodology: AA, PG, FB, MM; Project administration: MM; Resources: MM; Software: FB; Writing – original draft: AA, FB; Writing – review & editing: PG, FB, MM.
Funding
This research received no external funding.
Institutional Review Board Statement
This protocol was approved by Comitato Etico Territoriale Lombardia 4 OPERATIVO in CTIS – OPERATIVO in OsSC email: comitato.etico@istitutotumori.mi.it with the code INT 0019/22 and followed the Declaration of Helsinki.
Informed Consent Statement
Informed consent forms were provided and signed by parents and/or patients.
Data Availability Statement
Data available on request from the authors.
Acknowledgments
Parents and patients who were available for the research are heartily acknowledged.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Armstrong, F. D., Horn, M. Educational issues in childhood cancer. School Psychology Quarterly, 1995; 10: 292–304. [CrossRef]
- Kahalley L.S., Wilson S.J., Tyc V.L. et al. Are the psychological needs of adolescents’ survivors of pediatric cancer adequately identified and treated? In Psychooncology 2013; 22: 447-458. [CrossRef]
- Schultz K., Ness K, Whitton J. Et al. Behavioral and social outcomes in adolescent survivors of childhood cancer: a report from the childhood Cancer Survivor Study. J Clin Oncol 2007; 3649-3656. [CrossRef]
- Dunn, J., Adams, C., Holland, J., & Watson, M. Reinforcing the role of psycho-social oncology in global cancer prevention: applying psycho-oncology research in programmes and practice. Psycho-Oncology 2015; 24: 1217-1221. [CrossRef]
- Fuemmeler, B.F., Elkin, T.D. & Mullins, L.L. Survivors of childhood brain tumors: Behavioral, emotional, and social adjustment. Clinical Psychological Review 2002; 22:547-585. [CrossRef]
- Zeltzer LK, Recklitis C, Buchbinder D, et al. Psychological status in childhood cancer survivors: A report from the Childhood Cancer Survivor Study. J Clin Oncol 2009; 27:2396-404. [CrossRef]
- Hedström, M., Haglund, K., Skolin, I., & Von Essen, L. Distressing events for children and adolescents with cancer: child, parent, and nurse perceptions. J Ped Oncol Nursing, 2003; 20: 120-132. [CrossRef]
- Hicks, J., Bartholomew, J., Ward-Smith, P., & Hutto, C. J, Quality of life among childhood leukemia patients. J of Ped Oncol Nursing 2003; 20: 192-200. [CrossRef]
- Kazak, A. E., & Noll, R. B. The integration of psychology in pediatric oncology research and practice: collaboration to improve care and outcomes for children and families. American Psychologist 2015; 70: 146. [CrossRef]
- Kinahan, K. E., Sharp, L. K., Seidel, K., et al. Scarring, disfigurement, and quality of life in long-term survivors of childhood cancer: a report from the Childhood Cancer Survivor study. J Clin Oncol, 2012; 30: 24662474. [CrossRef]
- Lannering, B., Marky, I., Lundberg, A. & Olsson, E. Long-term sequelae after pediatric brain tumors: their effect on disability and quality of life. Med Ped Oncol, 1990; 18: 304-310. [CrossRef]
- LeBaron, S., Zeltzer, P.M., Zeltzer, L.K., Scott, S. & Marlin, A.E. Assessment of quality of survival in children with medulloblastoma and cerebellar astrocytoma. Cancer 1988; 62:1215-1222. [CrossRef]
- Mulhern RK, Carpentieri S, Shema S, et al. Factors associated with social and behavioral problems among children recently diagnosed with brain tumor. J Pediatr Psychol 1993; 18:339-350. [CrossRef]
- Maurice-Stam, H., Silberbusch, L. M., Last, B. F., & Grootenhuis, M. A. (2009). Evaluation of a psycho-educational group intervention for children treated for cancer: A descriptive study. Psycho-Oncology 2009; 18:762-766. [CrossRef]
- Poggi G., Liscio M., Galbiati S., Adduci A., et al. Brain tumors in Children and Adolescents: cognitive and psychological disorders at different ages. Psychooncology 2005; 14:386-95. [CrossRef]
- Ris, M.D. & Noll, R.B.. Long-term neurobehavioral outcome in pediatric brain tumor patients: review and methodological critique. J Clin Exp Neuropsychol. 1994;, 16: 21-42. [CrossRef]
- Adduci A., Jankovic M., Strazzer S., Massimino M., Clerici CA,Poggi G. Parent-Child communication and psychological adjustment in children with a brain tumor. Ped BloodCancer 2012; 59:290-294. [CrossRef]
- Barlow JH, Ellard DR. The psychosocial well-being of children with chronic disease, their parents and siblings: an overview of the research evidence base. Child: Care, Health & Development 2005; 32: 19-31. [CrossRef]
- Barrera M, Fleming CF, Khan FS. The role of emotional social support in the psychological adjustment of siblings of children with cancer. Child: Care, Health & Development 2004;30: 103-111. [CrossRef]
- Branstetter JE, Domian EW, Williams PD, Graff JC, Piamjariyakul U. Communication themes in families of children with chronic conditions. Comprehensive Pediatric Nursing 2008; 31: 171-184. [CrossRef]
- Hildenbrand, A. K., Clawson, K. J., Alderfer, M. A., & Marsac, M. L. Coping with pediatric cancer: Strategies employed by children and their parents to manage cancer-related stressors during treatment. Journal of Pediatric Oncology Nursing, 2011; 28: 344-354. [CrossRef]
- Hilden MJ, Watterson J, Chrastek J. Tell the children. J Clin Oncol 2003; 21: 37-39. [CrossRef]
- Horwitz WA, Kazak AE. Family adaptation to childhood cancer: sibling and family system variables. J of Clin Child Psychol 1990; 19: 221-228.
- Houtzager BA, Grooetnhuis MA, Hoekstra-Weebers J, Last BF. One month after diagnosis: quality of life, coping and previous functioning in siblings of children with cancer. Child: Care, Health & Development 2005; 31: 75-87. [CrossRef]
- Zeltzer L.K., Recklitis C., Buchbinder D., et al. Psychological status in childhood cancer survivors: a report from the Childhood Cancer Survivor Study. J Clin Oncol., 2009; 27: 2396-404. [CrossRef]
- Spinetta J., Masera G., Jankovic M., Oppenheim D., Martins A., Arush M., et al.. Valid informed consent and participative decision-making in children with cancer and their parents: a report of the SIOP Working Committee on psychosocial issues in pediatric oncology. Med Pediatr Oncol2003; 40: 244-6. [CrossRef]
- Hentea C., Cheng E.R., Bauer N.S, Mueller E.L. Parent-centered communication at time of pediatric cancer diagnosis: a systematic review. In Pediatric Blood and Cancer 2019; 66: e27624.
- Zwaanswijk M., Tates K, van Dulmen S., Hoogerbrugge P.M., Kamps W.A., Beishuizen A. & Bensing J.M. Communicating with child patients in pediatric oncology consultations: a vignette study on child patients’, parents’, and survivors’ communication preferences. Psycho-Oncology 2011; 20: 269-277. [CrossRef]
- Hackman DA, Farah MJ. Socioeconomic status and the developing brain. Trends Cogn Sci. 2009; 13: 65-73. [CrossRef]
- Lozoff B, Jimenez E, Smith JB. Double burden of iron deficiency in infancy and low socioeconomic status: a longitudinal analysis of cognitive test scores to age 19 years. Arch Pediatr Adolesc Med. 2006; 160: 1108-1113. [CrossRef]
- Tarazi RA, Grant ML, Ely E, Barakat LP. Neuropsychological functioning in preschool-age children with sickle cell disease: the role of illness-related and psychosocial factors. Child Neuropsychol 2007; 13 : 155-172. [CrossRef]
- Taylor HG, Swartwout M, Yeates KO, Walz NC, Stancin T, Wade SL. Traumatic brain injury in young children: post-acute effects on cognitive and school readiness skills. J Int Neuropsychol Soc. 2008; 14:734-745. [CrossRef]
- Yeates KO, Taylor HG, Walz NC, Stancin T, Wade SL. The family environment as a moderator of psychosocial outcomes following traumatic brain injury in young children. Neuropsychol 2010; 24: 345-356. [CrossRef]
- Taylor HG; Yeates KO, Wade SL, Drotar D, Stancin T, Minich N. A prospective study of short and long term outcomes after traumatic brain injury in children: Behavior and Achievement. Neuropsychol 2002; 16: 15-27. [CrossRef]
- Yeates KO, Swift E, Taylor HG, et al. Short and long-term social outcomes following pediatric traumatic brain injury. J In Neuropsychol Soc. 2004; 10: 412-426. [CrossRef]
- Patel SK, Fernandez N, Dekel N, et al. Socioeconomic status as a possible moderator or neurocognitive outcomes in children with cancer. Psycho-Oncology 2016; 25: 115-118. [CrossRef]
- Torres VA, Ashford JM, Wright E, Xu J, Zhang H, Merchant TE, Conklin HM. The impact of socioeconomic status (SES) on cognitive outcomes following radiotherapy for pediatric brain tumors: a prospective, longitudinal trial. Neuro Oncol. 2021;23:1173-1182. [CrossRef]
- Ehrhardt MJ, et al. Socioeconomic disparities and neurocognitive outcomes in childhood cancer survivors. JAMA Netw Open. 2023;6(5):e2311721.
- Bitsko MJ, Cohen D, Dillon R, Harvey J, Krull K, Klosky J. Psychosocial late effects in pediatric cancer survivors: A report from the Children’s Oncology Group. Pediatr Blood Cancer 2016;63:337-43. [CrossRef]
- Lown EA, Phillips F, Schwartz LA, Rosenberg AR, Jones B. Psychosocial follow-up in survivorship as a standard of care in pediatric oncology. Pediatr Blood Cancer 2015;62 Suppl 5:S514-29. [CrossRef]
Figure 1.
Psychological evaluation and cognitive assessment need and outcomes worsening after disease.
Figure 1.
Psychological evaluation and cognitive assessment need and outcomes worsening after disease.


Table 1.
“Heatmap” of significant relationships between considered factors and outcomes.
| OUTCOME | ||||||||
| Psychological Profile | Social profile | NPS profile | School profile | |||||
| Internalizing | Externalizing | Relational | Social | NPS | Adaptive | Need for | School | |
| problems | problems | problems | problems | problems | resources | PEI or PDP | marks | |
| Demographic and clinical factors | ||||||||
| Age at evaluation | 0.005 | |||||||
| Gender | 0.022 | |||||||
| Position/job | ||||||||
| Age at diagnosis | 0.037 | 0.002 | ||||||
| Time elapsed since diagnosis | 0.076 | 0.051 | 0.041 | |||||
| Type of tumor | 0.034 | 0.030 | ||||||
| Tumor site | 0.004 | 0.007 | ||||||
| Oncological treatment | 0.032 | |||||||
| Consequences’ severity | 0.005 | 0.001 | 0.035 | 0.039 | 0.001 | |||
| Rehabilitation needs | 0.080 | 0.025 | 0.058 | 0.040 | ||||
| Awareness about disease | ||||||||
| Communication timing about disease | 0.058 | 0.019 | ||||||
| Information requested about disease | ||||||||
| Family, cultural and economic factors | ||||||||
| Mother’s age | 0.054 | 0.079 | ||||||
| Father’s age | 0.035 | 0.013 | 0.048 | |||||
| Parents marital status | 0.030 | |||||||
| Presence of siblings | 0.019 | 0.087 | ||||||
| Number of siblings | 0.005 | |||||||
| Birth order among siblings | 0.077 | |||||||
| Family educational level | 0.039 | 0.080 | ||||||
| Populousness of residence place | ||||||||
| Geographical residence | ||||||||
| Mother’s job | ||||||||
| Father’s job | ||||||||
| Family income sources | ||||||||
| Financial benefits for child’s illness | 0.030 | |||||||
| Premorbid problems | ||||||||
| Pre-perinatal problems | ||||||||
| Previous internalizing problems | 0.009 | 0.071 | 0.030 | 0.024 | 0.045 | 0.018 | 0.006 | |
| Previous externalizing problems | 0.002 | <0.001 | 0.031 | 0.028 | ||||
| Previous relational problems | 0.002 | 0.024 | <0.001 | <0.001 | 0.034 | |||
| Previous social problems | 0.004 | <0.001 | 0.008 | 0.020 | ||||
| Previous psychological evalutaion | 0.030 | 0.079 | 0.048 | |||||
| Previous extra-curricular activities | ||||||||
| Previous NPS problems | 0.006 | |||||||
| Previous academic problems | 0.003 | |||||||
| Previous NPS evaluation | ||||||||
| Previous support scholastic path | 0.011 | |||||||
| Previous adaptive resources | 0.062 | <0.001 | 0.004 | |||||
| Previous socio-economic problems | 0.048 | |||||||
| Previous traumatic experiences | ||||||||
Abbreviations: NPS, neuro-psicological; PEI, piano educativo individualizzato (Individualized Education Plan); PDP, piano didattico personalizzato (Personalized Didactic Plan).
Table 2.
Significant differences between brain tumor and no brain tumor patients.
| Brain tumor | No brain | P | |
| patients | tumor patients | ||
| N = 38 | N = 55 | ||
| Oncological treatment | 0.001 | ||
| Surgery + CT + RT | 16 (42.1%) | 13 (23.6%) | |
| Surgery + CT | 1 (2.6%) | 19 (34.5%) | |
| Surgery only | 10 (26.3%) | 14 (25.5%) | |
| Other/none | 11 (28.9%) | 9 (16.4%) | |
| Consequences’ severity (aesthetic problems, motor/sensorial problems, language and learning difficulties) | 0.022 | ||
| 0 | 15 (39.5%) | 28 (51.9%) | |
| 1 | 16 (42.1%) | 25 (46.3%) | |
| 2 | 7 (18.4%) | 1 (1.9%) | |
| Learn and language issues | 0.007 | ||
| 0 | 15 (39.5%) | 38 (70.4%) | |
| 1 | 13 (34.2%) | 13 (24.1%) | |
| 2 | 6 (15.8%) | 3 (5.6%) | |
| 3 | 3 (7.9%) | 0 (0.0%) | |
| 4 | 1 (2.6%) | 0 (0.0%) | |
| Rehabilitation needs | 0.031 | ||
| 0 | 20 (52.6%) | 39 (72.2%) | |
| 1 | 15 (39.5%) | 8 (14.8%) | |
| 2 | 3 (7.9%) | 7 (13.0%) | |
| Cognitive rehabilitation need (psychomotricity treatment, speech therapy, neuropsychological rehabilitation) | 0.001 | ||
| 0 | 24 (63.2%) | 48 (88.9%) | |
| 1 | 6 (15.8%) | 6 (11.1%) | |
| 2 | 5 (13.2%) | 0 (0.0%) | |
| 3 | 3 (7.9%) | 0 (0.0%) | |
| Psychological and educational intervention need | 0.033 | ||
| 0 | 23 (60.5%) | 44 (81.5%) | |
| 1 | 10 (26.3%) | 9 (16.7%) | |
| 2 | 5 (13.2%) | 1 (1.9%) | |
Abbreviations: CT, chemotherapy; RT, radiotherapy.
Table 3.
Association between tumor site and outcome.
| Brain | No Brain | p | ||
| tumor patients | tumor patients | |||
| Psychological outcome | ||||
| Onset/worsening of internalizing problems | 22 (57.9%) | 26 (50.0%) | 0.650 | |
| Onset/worsening of externalizing problems | 15 (39.5%) | 14 (26.9) | 0.441 | |
| Need for psychological assessment | 22 (57.9%) | 17 (32.1%) | 0.025 | |
| Neuro-psychological outcome | ||||
| Onset/worsening of neuropsychological disorders | 22 (57.9%) | 20 (38.5%) | 0.178 | |
| Reduction of adaptive resources | 13 (43.3%) | 9 (20.5%) | 0.007 | |
| Need for neuro-psychological assessment_ | 7 (18.4%) | 2 (3.7%) | 0.047 | |
| Social outcome | ||||
| Onset/worsening of relational problems | 7 (18.4%) | 7 (13.5%) | 0.786 | |
| Onset/worsening of social problems | 18 (47.4%) | 9 (17.3%) | 0.004 | |
| Limitation of attendance of extra-curricular activities | 13 (38.2%) | 20 (37.7%) | 0.095 | |
| Scholastic outcome | ||||
| Onset/worsening of academic performance problems _ | 16 (47.1%) | 14 (27.5%) | 0.179 | |
| Need for personalized concessions/facilitations to support scholastic path (as PEI and PDP) | 11 (31.4%) | 12 (22.2%) | 0.471 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



