Submitted:
10 June 2026
Posted:
11 June 2026
You are already at the latest version
Abstract
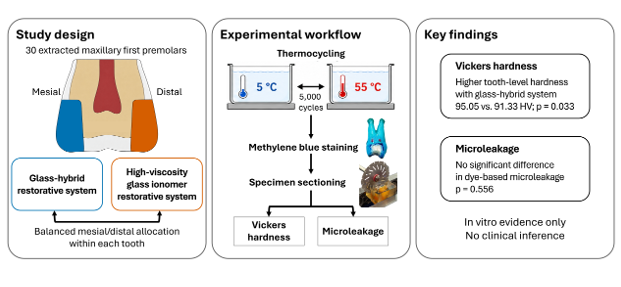
Background/Objectives: Glass-hybrid and high-viscosity glass-ionomer systems aim to improve conventional glass-ionomer performance. This in vitro study compared Vickers hardness and microleakage of a coated glass-hybrid system and a coated high-viscosity glass-ionomer system in thermocycled conservative Class II cavities in human maxillary first premolars. Methods: Thirty extracted maxillary first premolars were used in a paired within-tooth design. Two standardized conservative Class II cavities, one mesial and one distal, were prepared in each tooth, and each tooth received both systems: EQUIA Forte HT Fil with EQUIA Forte Coat and GC Gold Label IX EXTRA CAPSULE with GC G-Coat Plus. After restoration and thermocycling, Vickers hardness was measured on restoration cross-sections at occlusal and gingival locations. Microleakage was assessed on sectioned specimens using dye penetration measurements and ordinal infiltration scores. Results: EQUIA Forte HT showed a higher tooth-level mean Vickers hardness than Gold Label IX Extra after thermocycling (95.05 ± 6.58 HV vs. 91.33 ± 7.50 HV), with a mean paired difference of 3.72 HV (95% CI: 0.32 to 7.11; p = 0.033). In the location-dependent analysis, the effect of the restorative system was significant (p = 0.025), whereas testing location and the interaction were not significant. The microleakage index and the distributions of occlusal-wall and gingival-wall ordinal infiltration scores did not differ significantly between the two restorative systems. Conclusions: Under the conditions of this in vitro study, EQUIA Forte HT showed a slight tooth-level hardness advantage over Gold Label IX Extra after thermocycling. Neither system showed a statistically significant advantage in dye-based marginal sealing.
Keywords:
class II restoration
; glass-hybrid restorative system
; high-viscosity glass-ionomer cement
; Vickers hardness
; microleakage
; thermocycling
1. Introduction
Posterior Class II restorations remain difficult to manage because proximal access, cervical margins, isolation, finishing, and marginal protection all influence restoration adaptation and durability. The progressive reduction in the use of dental amalgam and the increasing demand for tooth-colored restorations have encouraged wider use of adhesive and ion-releasing restorative materials for posterior cavities [1]. The proximal box and cervical margin are particularly vulnerable because they are difficult to isolate, adapt, finish, and protect from marginal degradation.
Glass ionomer cements (GICs) are water-based acid-base cements formed by the reaction between an ion-leachable fluoroaluminosilicate glass powder and an aqueous polyalkenoic acid [2]. Their clinical value is related to chemical interaction with enamel and dentin, fluoride release and recharge, biocompatibility, favorable thermal compatibility with dental hard tissues, and relative simplicity of placement [2]. For these reasons, GICs remain useful in caries-prone patients and in clinical situations where simplified placement is desirable. However, conventional GICs have important limitations in stress-bearing posterior restorations, including brittleness, low fracture toughness, reduced wear resistance, and sensitivity to water gain or loss during the early maturation phase [2,3]. Since GICs continue to mature after the initial set, surface protection during the early post-placement period may influence subsequent mechanical behavior [3].
High-viscosity GICs and glass-hybrid restorative systems were introduced to improve the mechanical limitations of conventional formulations while preserving features such as fluoride release, chemical interaction with tooth structure, and simplified placement. High-viscosity GICs generally rely on a higher powder-to-liquid ratio and refined glass-particle distribution, which may improve material density and selected mechanical properties [4]. Glass-hybrid systems represent a further development, incorporating glass particles of different sizes, including smaller highly reactive particles with high-molecular-weight polyacrylic acid to support matrix formation and particle packing [4,5]. In coated GIC-based systems, the resin-based surface coating is intended to protect the immature cement surface by sealing surface porosities and reducing early degradation [1,4].
Whether newer glass-hybrid systems consistently offer better mechanical or marginal behavior than high-viscosity GICs remains unresolved. In vitro studies on EQUIA Forte or related glass-hybrid materials have reported a more favorable flexural strength, compressive strength, or surface hardness than conventional, resin-modified, or earlier high-viscosity GIC formulations [5,6]. Other work has shown that newer GIC materials marketed for stress-bearing areas may not provide a fracture toughness advantage over conventional GICs, although resin coating can increase surface hardness [1]. Comparative studies of high-viscosity and glass-hybrid GICs have also shown that mechanical behavior is material- and protocol-dependent rather than uniformly superior for a single material category [7]. More recent studies indicate that coating protocols and thermal aging can influence Vickers microhardness, water sorption, solubility, surface characteristics, and elemental composition of contemporary GIC-based restorative materials [4,8,9]. This makes it more appropriate to evaluate these materials as complete restorative systems, including coating and aging, rather than as uncoated base cements alone.
Clinical evidence supports the selected posterior use of glass-hybrid and high-viscosity GIC restorations, but the findings suggest that these restorations depend on material, cavity, and protocol. Long-term trials have reported acceptable performance of coated glass-hybrid or high-viscosity GIC restorations in selected Class II cavities. However, esthetic surface properties, retention, and marginal adaptation continue to be concerns [10,11,12]. A recent systematic review and meta-analysis found very low-certainty evidence suggesting that bulk-fill resin-based restorations may perform more favorably than high-viscosity glass ionomer-based restorations for retention and marginal adaptation, although coated high-viscosity glass ionomer restorations showed acceptable clinical behavior [13]. Laboratory studies cannot establish clinical superiority, but they can clarify material behavior under standardized conditions that are difficult to isolate in vivo.
Vickers hardness was selected because it measures resistance to indentation and may indirectly reflect surface maturation or susceptibility to mechanical degradation [5,8]. In Class II cavities restored with GIC-based materials, hardness values measured at different locations may also help determine whether the material develops relatively uniform mechanical properties within the restoration. This aspect is relevant because occlusal and proximal/cervical regions differ in cavity geometry, finishing access, and exposure to moisture and thermal stress.
Marginal sealing is another key concern in Class II restorations, particularly near proximal and cervical margins [14]. Microleakage testing, commonly performed by dye penetration after sectioning, is used as a laboratory indicator of marginal sealing at the tooth–restoration interface [15]. Although dye penetration does not directly indicate clinical failure, it is still useful for comparing restorative materials and protocols under controlled conditions. Thermocycling is commonly used as an artificial aging procedure to expose restorations to repeated temperature changes, although protocols vary widely and only partly reproduce the complexity of the oral environment [15,16].
Few paired within-tooth studies have compared coated glass-hybrid and high-viscosity GIC systems in conservative Class II cavities while assessing both hardness distribution and microleakage after the same aging protocol. Therefore, this in vitro study aimed to compare the Vickers hardness and microleakage of a coated glass-hybrid restorative system and a coated high-viscosity glass-ionomer restorative system in standardized conservative Class II cavities prepared in extracted human maxillary first premolars after thermocycling. The null hypotheses were that there would be no difference between the two restorative systems in tooth-level mean Vickers hardness, location-dependent hardness, microleakage index, or ordinal dye-penetration scores.
2. Materials and Methods
2.1. Study Design
This in vitro study compared two coated glass ionomer-based restorative systems in standardized conservative Class II cavities prepared in extracted human maxillary first premolars. Each tooth received two cavities, one mesial-occlusal and one disto-occlusal, allowing both restorative systems to be tested within the same tooth in a paired design. The glass-hybrid restorative system consisted of EQUIA Forte HT Fil used with EQUIA Forte Coat, whereas the high-viscosity glass ionomer restorative system consisted of GC Gold Label IX EXTRA CAPSULE used with GC G-Coat Plus.
The primary outcome was tooth-level mean Vickers hardness after thermocycling. Secondary outcomes were location-dependent hardness, exploratory occlusal–gingival hardness difference, and microleakage at the tooth–restoration interface. The workflow included tooth selection, cavity preparation, paired restorative allocation, restoration and coating, 24 h storage in distilled water, thermocycling, dye penetration, sectioning, Vickers hardness testing, and microleakage assessment.
2.2. Ethical Considerations and Tooth Collection
The study protocol was approved by the Biomedical Research Ethics Committee of the University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam (approval No. 1129/HĐĐĐ-ĐHYD on 13 November 2023). Extracted human maxillary first premolars were obtained after extraction for orthodontic reasons at the Faculty of Dentistry, University of Medicine and Pharmacy at Ho Chi Minh City. Only one tooth was obtained from each donor. The teeth were anonymized before laboratory use. The ethics committee waived the requirement for written informed consent because the study used anonymized discarded biological tissue and involved no patient interventions.
2.3. Tooth Selection, Cleaning, and Storage
Thirty extracted human maxillary first premolars from donors aged 18–25 years were included. Teeth were eligible if the crown was intact and free of caries, previous restorations, and other visible loss of tooth structure. Teeth were excluded if they showed wear, previous endodontic treatment, cracks or fractures, fluorosis, enamel hypoplasia, dentin hypoplasia, or other conditions that could affect enamel or dentin mineralization.
After extraction, the teeth were cleaned using hand scalers (Hu-Friedy, USA), followed by polishing with fluoride-free pumice. The teeth were immersed in 5.25% sodium hypochlorite for 5 min and then stored individually in sealed containers containing 0.9% saline at 4 °C until use. The storage solution was replaced every 3 days, and the teeth were kept fully immersed throughout storage. The interval between extraction and cavity preparation did not exceed 1 month.
2.4. Sample Size
The sample size was calculated a priori using G*Power 3.1.9.7. The calculation was based on the primary outcome, defined as the paired difference in mean Vickers hardness between the two restorative systems within the same tooth. A previous in vitro study reporting higher hardness for an EQUIA Forte material compared with Fuji IX GP was used to support the expectation of a material-related hardness difference [5]. Because the reference study used independent material specimens rather than paired Class II restorations in the same tooth, and because no directly comparable paired Class II hardness data were available, a medium paired effect size was selected for the present design. With a two-tailed paired t-test, standardized paired effect size dz = 0.53, α = 0.05, and 80% power, the minimum required sample size was 30 paired observations. Therefore, 30 teeth were included, providing 60 restorations in standardized conservative Class II cavities and 30 paired within-tooth comparisons.
2.5. Restorative Materials
All restorative, coating, and conditioning materials used in this study were manufactured by GC Corporation (Tokyo, Japan) and were used according to the manufacturer’s instructions. Details of the materials are presented in Table 1.
2.6. Sample Allocation
Each tooth received two standardized conservative Class II cavities, one mesial-occlusal and one disto-occlusal. Allocation was performed using permuted block randomization with two possible configurations: In configuration A, the mesial cavity was assigned to the GC Gold Label IX EXTRA system (including GC Gold Label IX EXTRA CAPSULE used with GC G-Coat Plus) and the distal cavity to the EQUIA Forte HT system (including EQUIA Forte HT Fil used with EQUIA Forte Coat). In configuration B, the assignment was reversed. Blocks of size two were used, with one configuration A and one configuration B in each block. The order within each block was randomized in Microsoft Excel, and 15 blocks were generated to produce a balanced distribution of each material between mesial and distal cavities.
Allocation concealment was implemented using sequentially numbered, opaque, sealed envelopes prepared by an independent researcher who was not involved in cavity preparation, restoration, or outcome assessment. The allocation envelope was opened only after both mesial and distal cavities had been prepared. Outcome assessors for Vickers hardness and microleakage were blinded to material allocation. Material-identifying marks placed on the teeth were concealed before outcome assessment. Blinding of the restorative operator was not feasible because the two restorative systems differed in handling and coating procedures. The order of restoration placement within each tooth was also prespecified in the allocation form and balanced between mesial and distal cavities to minimize cavity-order and handling-sequence effects.
2.7. Cavity Preparation
Each tooth was mounted in a gypsum block, with the cemento-enamel junction positioned at least 4 mm above the gypsum base. Standardized conservative Class II cavities were prepared on the mesial and distal surfaces of each tooth using a high-speed handpiece with water cooling and a TF-21 tapered flat-end diamond bur (Mani, Tochigi, Japan). The bur had a maximum diameter of 1.6 mm and a tip diameter of 0.8 mm. A new bur was used after every three cavity preparations. Each preparation included an occlusal access portion and a proximal component. The cavity dimensions were standardized to 4.0 mm occlusogingivally, 4.0 mm buccopalatally, and 1.5 mm mesiodistally. The gingival wall was located at least 1.0 mm coronal to the cemento-enamel junction. Dimensions were verified during preparation using a periodontal probe and digital caliper, with a tolerance of ±0.2 mm. All cavities were prepared by one operator. Before the main experiment, the operator prepared pilot cavities in 10 teeth not included in the study. These pilot preparations were independently checked by a supervising examiner to verify dimensional consistency and operator calibration.
2.8. Restorative Procedures
A Tofflemire matrix retainer (YDM, Tokyo, Japan) with a 0.035 mm stainless-steel matrix band (TOR VM, Moscow, Russia) was used during restoration placement to restore the proximal contour of each Class II cavity. Both cavities in each tooth were conditioned using GC Dentin Conditioner for 20 s, rinsed with water, and gently air-dried without desiccating the cavity surface. The restorative capsules were activated and mixed for 10 s at approximately 4000 rpm using a Capsule Mixer CM-II (GC Corporation, Tokyo, Japan). The mixed material was inserted using a GC Capsule Applier (GC Corporation, Tokyo, Japan). Before insertion, the capsule was primed by pressing the applicator twice.
The restorative material was injected into the cavity within 10 s. The working time from the start of mixing was 1 min 15 s for GC Gold Label IX EXTRA CAPSULE and 1 min 30 s for EQUIA Forte HT Fil at room temperature (approximately 25 °C). The restoration was shaped with a hand instrument. At 2 min 30 s after the start of mixing, the matrix was removed, and excess material was adjusted using a fine diamond finishing bur under water cooling.
Surface coating was then applied according to group allocation. GC G-Coat Plus was applied to GC Gold Label IX EXTRA CAPSULE restorations, and EQUIA Forte Coat was applied to EQUIA Forte HT Fil restorations. The coating was applied to the exposed restoration surface and restoration margins according to the manufacturer’s instructions. Each coating was applied with a microbrush and light-cured for 20 s using an LED light-curing unit (Led B, Woodpecker, Guilin, China; wavelength range, 420–480 nm). The irradiance was maintained at 850–1000 mW/cm² and verified before each curing session using a Light Meter LM-1 radiometer (Woodpecker, Guilin, China). The distance from the light tip to the coated surface was maintained at approximately 1 mm during curing.
After restoration and coating, all specimens were stored in distilled water at room temperature for 24 h before thermocycling.
2.9. Thermocycling
Thermocycling was performed using a custom-built thermocycling apparatus designed to automatically transfer a specimen basket between two water baths using a mechanical arm and timed relay system. All specimens were fully immersed in distilled water during thermocycling. The protocol consisted of 5,000 cycles between 5 ± 1 °C and 55 ± 1 °C, with a dwell time of 25 s in each bath and a transfer time of 5 s. The hot bath was maintained at 55 °C using a thermostatically controlled water bath. The cold bath was maintained at 5 °C by adding ice as needed. Both bath temperatures were monitored using a digital thermocouple calibrated before each experimental session and placed directly in each bath during monitoring. Temperature fluctuations were kept within ±1 °C. Thermocycling was used as a controlled laboratory thermal challenge and was not intended to reproduce the full complexity of the oral environment [15,16]. The cycle count, dwell time, and transfer time were checked against the relay timer settings before each run. Specimens were positioned in the basket to ensure complete immersion during each dwell period and to prevent direct contact between restorations.
2.10. Dye Penetration and Specimen Sectioning
After thermocycling, the root apices were sealed with Peri Compound (GC Corporation, Tokyo, Japan). Two layers of nail varnish (Felina Deluxe, Vietnam) were applied to the entire tooth surface except for the restorations and a 1 mm zone of tooth structure around the restoration margins. The specimens were immersed in 2% methylene blue solution for 24 h. After dye immersion, excess dye was removed by rinsing under running water and gentle brushing for 10 min. The teeth were then air-dried.
The roots were sectioned 2 mm apical to the cemento-enamel junction, and the crowns were embedded in transparent self-curing epoxy resin prepared using EpoFix Resin and EpoFix Hardener (Struers, Ballerup, Denmark). Each crown was sectioned longitudinally in the mesiodistal direction through the center of both restorations using a slow-speed diamond saw (Struers, Ballerup, Denmark) under water cooling. The cutting disc was replaced after every two teeth. Sectioning produced one buccal and one palatal half, and each half contained cross-sections of both restorations. For each tooth, one half was randomly assigned to microleakage assessment and the other half to Vickers hardness testing. The cut surfaces were manually polished using 1000-grit abrasive papers (Kovax, Japan). All sectioned halves were coded by an independent dentist before assessment.
2.11. Vickers Hardness Testing
Vickers hardness was measured on polished cross-sectional surfaces using a Future-Tech FV-300e hardness tester (Future-Tech Corp., Kawasaki, Japan) under a load of 0.5 kgf and a dwell time of 20 s (HV0.5/20). For each restoration, measurements were performed at two locations within the restored Class II cavity, one toward the occlusal aspect and one toward the gingival wall. The locations were positioned along the central occlusogingival axis and separated by approximately 2 mm.
Three indentations were placed at each location and averaged to obtain one location-specific hardness value. Indentations were separated by at least 2.5 times the indentation diagonal length and placed away from visible cracks, voids, restoration margins, and dye-stained defects. The three indentations were treated as technical replicates rather than independent observations. The procedure followed the general principles of ASTM E384-22, with adaptation for sectioned dental restorative specimens.
Because all specimens underwent methylene blue immersion before sectioning, hardness testing was performed on dye-exposed restorations after polishing. Both restorative systems followed the same sequence of thermocycling, dye immersion, sectioning, polishing, and hardness testing. The examiner was blinded to the allocation.
2.12. Microleakage Assessment
Microleakage was assessed on the sectioned half, which contained cross-sections of both restorations. The specimens were examined using a stereomicroscope (Olympus SZX10, Olympus, Tokyo, Japan) at ×16 magnification. Images were captured using a Lumenera Infinite 1-3C digital camera (Lumenera, Ottawa, Canada) and Infinite Capture software (Lumenera, Ottawa, Canada). Linear measurements were performed in ImageJ 1.38e (National Institutes of Health, Bethesda, MD, USA) after calibration with a 1 mm scale under the same imaging conditions.
Dye penetration was quantified along the tooth–restoration interface on the selected section. For this study, occlusal-wall penetration was defined as dye progression from the occlusal cavosurface margin along the occlusal-wall tooth–restoration interface toward the pulpal wall. Gingival-wall penetration was defined as dye progression from the gingival cavosurface margin along the gingival-wall tooth–restoration interface toward the axial wall. The stained lengths along these two predefined interface segments were traced separately. For each measurement round, the microleakage index was calculated as the sum of the occlusal-wall and gingival-wall stained lengths divided by the total evaluated tooth–restoration interface length on the same section. The index was stored and analyzed as a dimensionless ratio ranging from 0 to 1, where 0 indicated no dye penetration and 1 indicated dye penetration along the entire evaluated interface.
Ordinal infiltration scores were recorded separately for occlusal-wall and gingival-wall penetration, using predefined dye-penetration criteria informed by ISO/TS 11405:2015 and adapted for the present conservative Class II cavity model (Table 2) [17]. Representative annotated stereomicroscopic images illustrating the measurement scheme and ordinal dye-penetration scoring criteria are provided in Supplementary Figure S1.
Microleakage measurements and scoring were performed by an examiner blinded to material allocation. Continuous measurements were repeated after a three-week interval, and the examiner had no access to the first measurement set during the second round. For each round, the microleakage index was calculated independently. The mean of the two measurement rounds was used as the microleakage index for each restoration. Intra-rater reliability between the two rounds was assessed using intraclass correlation coefficients for continuous measurements.
Ordinal scores were also assigned twice with a three-week interval. Intra-rater reliability for ordinal scoring was assessed using quadratic-weighted kappa statistics. When the two scores differed, the original image was re-evaluated under blinded conditions, and a resolved final score was assigned before statistical analysis.
2.13. Statistical Analysis
Data management was performed using Microsoft Excel 365 (Microsoft Corp., Redmond, WA, USA), and statistical analyses were conducted in R version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria). The tooth was considered the experimental unit for paired comparisons. All tests were two-sided, with α = 0.05.
Tooth-level mean Vickers hardness was compared between restorative systems using a paired t-test after assessing normality of paired differences with the Shapiro–Wilk test and Q–Q plots. Results were reported as mean ± standard deviation, mean paired difference, 95% confidence interval, and p value. Location-dependent hardness was analyzed with a linear mixed-effects model including restorative system, testing location, and their interaction as fixed effects, and random intercepts for tooth and for restoration nested within tooth. Estimated marginal means with 95% confidence intervals were calculated for visualization of location-dependent hardness. The absolute occlusal–gingival hardness difference was analyzed as an exploratory measure of hardness uniformity using a paired t-test.
The microleakage index was summarized using medians, interquartile ranges, ranges, and mean ± standard deviation, and compared between restorative systems using the Wilcoxon signed-rank test. The Hodges–Lehmann paired estimate was reported with a bootstrap 95% confidence interval obtained by paired resampling at the tooth level using 10,000 bootstrap replications. Final ordinal infiltration scores were summarized as frequencies and percentages and compared using Wilcoxon signed-rank tests. Ordinal scores were not averaged.
Intra-rater reliability was assessed using single-measure two-way mixed-effects ICCs for absolute agreement for continuous microleakage measurements and quadratic-weighted kappa statistics for ordinal infiltration scores.
3. Results
All 60 restorations from 30 teeth were included in the analysis. Each tooth received both restorative systems, with balanced mesial/distal allocation. No missing values were detected, and all microleakage indices and ordinal infiltration scores were within the predefined valid ranges.
3.1. Vickers Hardness After Thermocycling
The mean Vickers hardness was 95.05 ± 6.58 HV for the EQUIA Forte HT system and 91.33 ± 7.50 HV for the Gold Label IX Extra system. The mean paired difference in Vickers hardness was 3.72 HV (95% CI, 0.32 to 7.11; p = 0.033), with higher values observed for EQUIA Forte HT than for Gold Label IX Extra (Table 3; Figure 1a).
In the location-dependent hardness analysis, the effect of the restorative system was statistically significant (p = 0.025), whereas the effect of testing location (p = 0.299) and the restorative system × testing location interaction (p = 0.934) were not significant (Figure 1b). Location-specific descriptive hardness values are shown in Table 3.
The absolute occlusal–gingival hardness difference was 7.23 ± 4.44 HV for the EQUIA Forte HT system and 5.80 ± 4.03 HV for the Gold Label IX Extra system. The mean paired difference was 1.43 HV (95% CI, −0.66 to 3.53; p = 0.173) (Table 3).
3.2. Microleakage and Infiltration After Thermocycling
Descriptive statistics for the microleakage index are shown in Table 4A and Figure 2. The median microleakage index was 0.425 (IQR, 0.309–0.574) for the EQUIA Forte HT system and 0.391 (IQR, 0.287–0.667) for the Gold Label IX Extra system. The paired estimate was 0.012 (bootstrap 95% CI, −0.024 to 0.060; p = 0.556). Zero microleakage was observed in one restoration in the EQUIA Forte HT system and in none of the Gold Label IX Extra restorations.
Resolved final ordinal scores were used for the analysis of occlusal-wall and gingival-wall dye penetration. The distributions of final scores are shown in Table 4B. The between-system comparisons were not statistically significant for occlusal-wall penetration (p = 0.843) or gingival-wall penetration (p = 0.782).
Reliability estimates for repeated microleakage measurements and ordinal infiltration scores are provided in Supplementary Table S1; ICC(A,1) values ranged from 0.868 to 0.997, and quadratic-weighted kappa values ranged from 0.814 to 0.829.
4. Discussion
The main finding was that EQUIA Forte HT showed a small but statistically significant hardness advantage over Gold Label IX Extra, whereas hardness distribution and dye-based marginal leakage did not differ between systems. Therefore, the null hypotheses were partly rejected. The EQUIA Forte HT system showed a significantly higher mean Vickers hardness at the tooth level than the Gold Label IX Extra system. However, testing location and the restorative system × testing location interaction were not significant, and the exploratory occlusal–gingival hardness difference did not differ between systems. For marginal sealing, neither the microleakage index nor the ordinal dye-penetration scores differed significantly between the two systems.
The higher Vickers hardness observed for EQUIA Forte HT represents a laboratory difference in indentation resistance. The mean paired difference was 3.72 HV, with a 95% confidence interval from 0.32 to 7.11 HV, indicating a statistically significant but limited effect. Previous studies have reported favorable hardness or mechanical properties for glass-hybrid or reinforced glass ionomer materials compared with conventional, resin-modified, or earlier high-viscosity glass ionomer formulations, but the magnitude and direction of these differences vary with specimen design, storage medium, coating protocol, aging procedure, and test conditions [4,5,6,7,8,9]. Fuhrmann et al. also showed that resin coating may increase surface hardness, whereas fracture toughness was not improved compared with conventional glass ionomer materials [1]. A higher hardness value should therefore not be taken as evidence of broader mechanical or clinical superiority, because fracture resistance, wear, marginal stability, retention, and restoration survival depend on additional factors [1,10,11,12,13].
The observed hardness difference may be related to the formulation and coating of the complete restorative systems tested. Glass ionomer cements set through an acid–base reaction between ion-leachable glass and polyalkenoic acid, followed by maturation processes that involve changes in strength, water binding, and interfacial bonding [2,3]. Glass-hybrid systems incorporate modifications such as smaller, highly reactive glass particles and high-molecular-weight polyacrylic acid, which may support matrix formation and particle packing [4,5,8]. Resin-based coatings may further protect the immature cement surface by reducing early water gain or water loss and sealing surface porosities [1,4]. The combination of a modified glass-hybrid formulation and its dedicated coating may have contributed to the higher hardness observed for EQUIA Forte HT. Still, because complete coated systems were compared, the separate contributions of the restorative material, coating, dentin conditioner, and their interactions cannot be isolated.
No significant location-dependent hardness effect was detected. The absence of a significant system × location interaction suggests that the occlusal and gingival testing regions followed a similar hardness pattern in both systems after thermocycling. The occlusal and gingival regions of these conservative Class II restorations differed in cavity geometry, finishing access, and potential moisture exposure. However, the present data do not support the claim that one system achieved greater hardness uniformity. The absolute occlusal–gingival hardness difference was not significantly different between systems. This interpretation is limited to the two predefined locations along the central occlusogingival axis. Vickers hardness is also sensitive to surface preparation, load, dwell time, storage, maturation time, and the tested plane [18]. Therefore, the findings indicate no clear location-dependent hardness effect under the present conditions, but they do not demonstrate complete three-dimensional hardness uniformity within the restorations.
The microleakage results did not show superior marginal sealing for either restorative system. The median microleakage index was similar between systems, and the paired estimate was close to zero with a confidence interval crossing zero. The occlusal-wall and gingival-wall ordinal scores also showed no significant between-system differences. Thus, the higher hardness of EQUIA Forte HT did not translate into a measurable advantage in dye-based marginal sealing. This is not unexpected because hardness and microleakage measure different aspects of restorative behavior. Hardness is a property of the restorative material at the tested site, whereas dye penetration is influenced by the tooth–restoration interface, cavity configuration, marginal adaptation, coating continuity, and aging-related interfacial changes [17,19].
Both systems showed measurable dye penetration, and this should be interpreted cautiously. Dye penetration is a common laboratory method for assessing marginal leakage, but it is an indirect surrogate outcome and does not directly predict postoperative sensitivity, secondary caries, restoration retention, or clinical failure [15,17,19]. Small dye molecules may penetrate interfacial defects differently from bacteria or oral fluids, and sectioning provides only a two-dimensional view of a three-dimensional interface. The occurrence of moderate-to-severe dye-penetration scores in both systems suggests that the Class II tooth–restoration interface remained susceptible to dye penetration after thermocycling, while the paired protocol supports the validity of the between-system comparison.
Marginal behavior in Class II restorations depends strongly on both material and protocol. Sahli et al. evaluated Class II restorations using marginal and internal adaptation outcomes after fatigue testing and reported material-dependent adaptation patterns [14]. Their outcomes were based on interfacial adaptation rather than dye penetration, so direct comparison with the present microleakage index is not appropriate. Wuersching et al. used a bacterial penetration model in Class II cavities and also found material-dependent bacterial microleakage patterns [20]. This model approximates bacterial challenge more closely than dye penetration, but it measures a different phenomenon. These methods should be viewed as complementary because dye leakage, bacterial penetration, marginal continuity, and internal adaptation each assess different aspects of interfacial behavior.
Long-term clinical studies have reported acceptable performance of coated glass-hybrid and high-viscosity glass ionomer restorations in selected Class II cavities, particularly when cavities are small to moderate and clinical protocols are controlled. However, retention, fracture, surface quality, anatomical form, and marginal adaptation remain relevant concerns over time [10,11,12]. A recent systematic review and meta-analysis reported very low-certainty evidence suggesting that bulk-fill resin-based restorations may perform more favorably than high-viscosity glass ionomer-based restorations for retention and marginal adaptation in permanent teeth, while coated high-viscosity glass ionomer restorations still showed acceptable clinical behavior [13]. These clinical data support a cautious interpretation of the present hardness difference, because the microleakage outcomes did not differ between systems.
Thermocycling was used as a controlled artificial aging challenge, but it only partly simulates the oral environment. The protocol exposed specimens to repeated temperature changes between 5 °C and 55 °C, which may stress the tooth–restoration interface through thermal changes and water exposure. However, thermocycling protocols vary widely, and their clinical equivalence remains uncertain [15,16]. Because other aging methods were not included, the results should be understood as the response of two coated systems to a standardized thermal and dye-penetration protocol rather than a full simulation of posterior Class II clinical treatment.
Several design features support the internal validity of this comparison. The paired within-tooth design reduced inter-tooth variability because each tooth received both restorative systems, and only one tooth was obtained from each donor. Allocation between mesial and distal cavities and the order of restoration placement were balanced and prespecified, allocation was concealed, outcome assessors were blinded, and the main laboratory procedures were standardized. Technical replicates for hardness were averaged rather than analyzed as independent observations, and ordinal infiltration scores were treated as ordinal data. These features address several reporting and bias domains recommended for preclinical dental materials research, including planning, allocation, specimen preparation, and outcome assessment [21].
Several constraints limit how far these findings can be generalized. First, the study was performed in vitro using extracted maxillary first premolars and cannot reproduce the biological and functional complexity of clinical restorations. Second, although standardized conservative Class II cavities were prepared with both occlusal and proximal components, the model did not reproduce proximal contact pressure, occlusal contact, masticatory loading, or the clinical challenges of matrix adaptation and isolation. Third, aging was limited to thermocycling. Mechanical loading, pH cycling, biofilm exposure, and dentinal fluid simulation were not included. Fourth, dye penetration is method-sensitive and provides only an indirect measure of marginal sealing [17,19]. Because the assessment was performed on a randomly selected sectioned half of each specimen, leakage outside the evaluated plane could not be captured. Fifth, Vickers hardness was measured on polished cross-sectional surfaces after thermocycling, dye immersion, sectioning, and polishing. Although this sequence was identical for both restorative systems and therefore supports the internal paired comparison, possible material-specific effects of dye exposure on the tested cross-sectional surfaces cannot be completely excluded. The absolute hardness values should therefore be considered protocol-specific and not directly compared with those from studies in which hardness was measured before dye penetration procedures.
Future studies should combine thermal aging with mechanical loading, pH cycling, simulation of dentinal fluid or pulpal pressure, and biofilm-based challenges. Multi-section or three-dimensional leakage assessments, bacterial penetration models, and interfacial microscopy could provide a more comprehensive evaluation of marginal seal degradation than a single dye-penetration section [14,20]. Longer maturation periods and repeated aging intervals may clarify whether hardness and leakage behavior change as glass ionomer-based materials continue to mature [2,3]. Clinical trials remain necessary to determine whether laboratory differences in hardness or marginal leakage translate into meaningful differences in restoration survival, marginal adaptation or secondary caries.
5. Conclusions
Within the limitations of this in vitro study using thermocycled conservative Class II premolar cavities, the EQUIA Forte HT system showed a higher tooth-level mean Vickers hardness than the Gold Label IX Extra system. However, no significant location-dependent hardness effect, restorative system × location interaction, or difference in occlusal–gingival hardness variation was detected. No statistically significant between-system difference was found in the microleakage index or ordinal dye-penetration scores.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Representative stereomicroscopic images illustrating occlusal-wall and gingival-wall microleakage measurement and ordinal dye-penetration scoring; Table S1: Intra-rater reliability of repeated microleakage measurements and ordinal infiltration scores.
Author Contributions
Conceptualization, L.T.-Q.N. and C.B.H.; methodology, L.T.-Q.N., C.B.H. and T.T.T.; software, T.T.T. and C.B.H.; validation, C.B.H. and T.T.T.; formal analysis, T.T.T.; investigation, C.B.H., L.T.-Q.N. and T.T.T.; resources, C.B.H. and L.T.-Q.N.; data curation, T.T.T.; writing—original draft preparation, C.B.H. and T.T.T.; writing—review and editing, L.T.-Q.N.; visualization, T.T.T. and C.B.H.; supervision, L.T.-Q.N.; project administration, L.T.-Q.N. and C.B.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external financial funding. GC Asia Dental Pte Ltd. provided in-kind support through the donation of restorative materials used in this study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved under expedited review by the Biomedical Research Ethics Committee of the University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam (approval No. 1129/HĐĐĐ-ĐHYD on 13 November 2023). The study used extracted and processed human teeth and did not involve any intervention or procedure performed on human participants.
Informed Consent Statement
The requirement for informed consent was waived by the Ethics Committee in Biomedical Research of the University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam, because the study used extracted and processed human teeth only, involved no intervention or procedure performed on human participants, and did not include any identifiable personal information.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The authors gratefully acknowledge GC Asia Dental Pte Ltd. for providing in-kind support through the donation of restorative materials used in this study. GC Asia Dental Pte Ltd. had no role in the study design, data collection, data analysis, data interpretation, manuscript preparation, or decision to submit the manuscript for publication.
Conflicts of Interest
The authors declare no conflicts of interest. GC Asia Dental Pte Ltd. provided in-kind support through the donation of restorative materials used in this study. GC Asia Dental Pte Ltd. had no role in the design, execution, data collection, analysis, interpretation, manuscript preparation, or decision to submit the manuscript for publication.
Abbreviations
The following abbreviations are used in this manuscript:
| CI | Confidence interval |
| GICs | Glass-ionomer cements |
| HV | Vickers hardness |
| ICC | Intraclass correlation coefficient |
| IQR | Interquartile range |
| SD | Standard deviation |
References
- Fuhrmann, D.; Murchison, D.; Whipple, S.; Vandewalle, K. Properties of New Glass-Ionomer Restorative Systems Marketed for Stress-Bearing Areas. Oper. Dent. 2020, 45, 104–110. [Google Scholar] [CrossRef]
- Sidhu, S.; Nicholson, J. A Review of Glass-Ionomer Cements for Clinical Dentistry. J. Funct. Biomater. 2016, 7, 16. [Google Scholar] [CrossRef]
- Nicholson, J.W. Maturation Processes in Glass-Ionomer Dental Cements. Acta Biomater. Odontol. Scand. 2018, 4, 63–71. [Google Scholar] [CrossRef]
- Alqasabi, S.Y.; Sulimany, A.M.; Almohareb, T.; Alayad, A.S.; Bawazir, O.A. The Effect of Different Coating Agents on the Microhardness, Water Sorption, and Solubility of EQUIA Forte® HT. Coatings 2024, 14, 751. [Google Scholar] [CrossRef]
- Moshaverinia, M.; Navas, A.; Jahedmanesh, N.; Shah, K.C.; Moshaverinia, A.; Ansari, S. Comparative Evaluation of the Physical Properties of a Reinforced Glass Ionomer Dental Restorative Material. J. Prosthet. Dent. 2019, 122, 154–159. [Google Scholar] [CrossRef]
- Poornima, P.; Koley, P.; Kenchappa, M.; Nagaveni, N.; Bharath, K.; Neena, I. Comparative Evaluation of Compressive Strength and Surface Microhardness of EQUIA Forte, Resin-Modified Glass-Ionomer Cement with Conventional Glass-Ionomer Cement. J. Indian Soc. Pedod. Prev. Dent. 2019, 37, 265–270. [Google Scholar] [CrossRef]
- Šalinović, I.; Stunja, M.; Schauperl, Z.; Verzak, Ž.; Ivanišević Malčić, A.; Brzović Rajić, V. Mechanical Properties of High Viscosity Glass Ionomer and Glass Hybrid Restorative Materials. Acta Stomatol. Croat. 2019, 53, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Franić, K.; Brundić, A.; Matijević, J.; Ivanišević, A.; Miletić, I.; Baraba, A. Influence of Human Blood Contamination on Microhardness of Glass-Ionomer Cements and Glass-Hybrid Material. Materials 2025, 18, 4075. [Google Scholar] [CrossRef] [PubMed]
- Birant, S.; Gümüştaş, B. The Effect of Thermal Aging on Microhardness and SEM/EDS for Characterisation Bioactive Filling Materials. BMC Oral Health 2024, 24, 1142. [Google Scholar] [CrossRef] [PubMed]
- Miletić, I.; Baraba, A.; Krmek, S.J.; Perić, T.; Marković, D.; Basso, M.; Ozkaya, C.A.; Kemaloglu, H.; Turkun, L.S. Clinical Performance of a Glass-Hybrid System in Comparison with a Resin Composite in Two-Surface Class II Restorations: A 5-Year Randomised Multi-Centre Study. Clin. Oral Investig. 2024, 28, 104. [Google Scholar] [CrossRef] [PubMed]
- Wafaie, R.A.; Ali, A.I.; El-Negoly, S.A.E.; Mahmoud, S.H. Five-year Randomized Clinical Trial to Evaluate the Clinical Performance of High-viscosity Glass Ionomer Restorative Systems in Small Class II Restorations. J. Esthet. Restor. Dent. 2023, 35, 538–555. [Google Scholar] [CrossRef] [PubMed]
- Heck, K.; Frasheri, I.; Diegritz, C.; Manhart, J.; Hickel, R.; Fotiadou, C. Six-Year Results of a Randomized Controlled Clinical Trial of Two Glass Ionomer Cements in Class II Cavities. J. Dent. 2020, 97, 103333. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Zhang, R.; Yu, X.; Sun, W.; Zhang, L.; Hua, F.; Chen, Z. The Clinical Performance of High-Viscosity Glass Ionomer-Based and Bulk-Fill Resin-Based Restorations in Permanent Teeth with Occlusal or Proximal Cavities: A Systematic Review and Meta-Analysis. Clin. Oral Investig. 2025, 29, 50. [Google Scholar] [CrossRef] [PubMed]
- Sahli, A.; Daeniker, L.; Rossier, I.; Caseiro, L.; Di Bella, E.; Krejci, I.; Bortolotto, T. Comparison of Class II Bulk-Fill, Self-Adhesive Composites, Alkasite, and High-Viscosity Glass Ionomer Restorations in Terms of Marginal and Internal Adaptation. Materials 2024, 17, 4373. [Google Scholar] [CrossRef] [PubMed]
- Rossomando, K.J.; Wendt, S.L. Thermocycling and Dwell Times in Microleakage Evaluation for Bonded Restorations. Dent. Mater. 1995, 11, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Gale, M.S.; Darvell, B.W. Thermal Cycling Procedures for Laboratory Testing of Dental Restorations. J. Dent. 1999, 27, 89–99. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Standardization. ISO/TS 11405:2015; Dentistry—Testing of Adhesion to Tooth Structure. ISO: Geneva, Switzerland, 2015.
- ASTM International. ASTM E384-22, Standard Test Method for Microindentation Hardness of Materials; ASTM International. West Conshohocken, PA, USA, 2022. [CrossRef]
- Heintze, S.D. Clinical Relevance of Tests on Bond Strength, Microleakage and Marginal Adaptation. Dent. Mater. 2013, 29, 59–84. [Google Scholar] [CrossRef] [PubMed]
- Wuersching, S.N.; Kohl, L.; Hickel, R.; Schwendicke, F.; Kollmuss, M. Assessing the Marginal Seal of Bioactive Restorative Materials in Class II Cavities with a Bacterial Penetration Model. Dent. Mater. 2025, 41, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Delgado, A.H.; Sauro, S.; Lima, A.F.; Loguercio, A.D.; Della Bona, A.; Mazzoni, A.; Collares, F.M.; Staxrud, F.; Ferracane, J.; Tsoi, J.; et al. RoBDEMAT: A Risk of Bias Tool and Guideline to Support Reporting of Pre-Clinical Dental Materials Research and Assessment of Systematic Reviews. J. Dent. 2022, 127, 104350. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Vickers hardness after thermocycling. (a) Paired tooth-level mean Vickers hardness of the EQUIA Forte HT system and the Gold Label IX Extra system. Each light-gray line connects paired restorations from the same tooth. Colored symbols show individual observations, and larger symbols with error bars show the group means and 95% CI. (b) Location-dependent Vickers hardness at occlusal and gingival testing locations. Points and error bars represent estimated marginal means and 95% CI from the linear mixed-effects model.
Figure 1.
Vickers hardness after thermocycling. (a) Paired tooth-level mean Vickers hardness of the EQUIA Forte HT system and the Gold Label IX Extra system. Each light-gray line connects paired restorations from the same tooth. Colored symbols show individual observations, and larger symbols with error bars show the group means and 95% CI. (b) Location-dependent Vickers hardness at occlusal and gingival testing locations. Points and error bars represent estimated marginal means and 95% CI from the linear mixed-effects model.

Figure 2.
Microleakage index after thermocycling. Each light-gray line connects paired restorations from the same tooth. Colored symbols indicate individual observations for the EQUIA Forte HT and Gold Label IX Extra systems. Large symbols with vertical bars show the median and interquartile range.
Figure 2.
Microleakage index after thermocycling. Each light-gray line connects paired restorations from the same tooth. Colored symbols indicate individual observations for the EQUIA Forte HT and Gold Label IX Extra systems. Large symbols with vertical bars show the median and interquartile range.


Table 1.
Restorative materials used in the study.
| Material | Category | Shade | Lot Number |
|---|---|---|---|
| EQUIA Forte HT Fil† | Glass-hybrid restorative | A3 | 2209221 |
| EQUIA Forte Coat† | Resin-based coating | N/A | 2304121 |
| GC Gold Label IX EXTRA CAPSULE‡ |
High-viscosity GIC restorative | A3 | 2210121 |
| GC G-Coat Plus‡ | Resin-based coating | N/A | 2305021 |
| GC Dentin Conditioner | Dentin conditioner | N/A | 2210151 |
†Components of the EQUIA Forte HT system. ‡Components of the GC Gold Label IX Extra system. N/A, not applicable.
Table 2.
Ordinal scoring criteria for dye penetration along the tooth–restoration interface.
| Assessment | Score | Criterion |
|---|---|---|
|
Occlusal-wall penetration |
0 | No dye penetration |
| 1 | Dye penetration limited to enamel | |
| 2 | Dye penetration beyond the dentino-enamel junction | |
| 3 | Dye penetration reaching the pulpal wall or extending deeper along the tooth–restoration interface | |
|
Gingival-wall penetration |
0 | No dye penetration |
| 1 | Dye penetration within one-half of the gingival wall | |
| 2 | Dye penetration beyond one-half of the gingival wall | |
| 3 | Dye penetration reaching the axial wall or extending deeper along the tooth–restoration interface |
Scores were treated as ordinal variables and were not averaged.
Table 3.
Descriptive and paired Vickers hardness outcomes after thermocycling.
| Outcome | EQUIA Forte HT |
Gold Label IX Extra |
Paired difference |
95% CI | p value |
|---|---|---|---|---|---|
| Occlusal hardness, HV | 95.53 ± 8.83 | 91.90 ± 9.01 | — | — | — |
| Gingival hardness, HV | 94.57 ± 6.70 | 90.77 ± 7.50 | — | — | — |
| Mean hardness, HV | 95.05 ± 6.58 | 91.33 ± 7.50 | 3.72 | 0.32 to 7.11 | 0.033 |
| Absolute occlusal– gingival difference, HV |
7.23 ± 4.44 | 5.80 ± 4.03 | 1.43 | −0.66 to 3.53 | 0.173 |
Values are presented as mean ± standard deviation unless otherwise stated. Paired differences were calculated as EQUIA Forte HT system − Gold Label IX Extra system. —, not applicable; HV, Vickers hardness; CI, confidence interval.
Table 4.
Microleakage index and ordinal infiltration scores after thermocycling.
| A. Microleakage index | |||||||||
| Outcome |
EQUIA Forte HT |
Gold Label IX Extra |
Paired estimate |
95% CI | p value | ||||
| Median (IQR) |
0.425 (0.309–0.574) |
0.391 (0.287–0.667) |
0.012 | −0.024 to 0.060 | 0.556 | ||||
| Range | 0.000–0.965 | 0.059–0.919 | — | — | — | ||||
| Mean ± SD | 0.457 ± 0.243 | 0.454 ± 0.240 | — | — | — | ||||
| The paired estimate represents the Hodges–Lehmann paired estimate calculated as EQUIA Forte HT system − Gold Label IX Extra system. The 95% confidence interval was obtained by paired bootstrap resampling at the tooth level. The p value was calculated using the Wilcoxon signed-rank test. | |||||||||
| B. Ordinal infiltration scores | |||||||||
| Assessment | Score |
EQUIA Forte HT, n (%) |
Gold Label IX Extra, n (%) |
p value | |||||
| Occlusal-wall penetration | 0 | 2 (6.7%) | 2 (6.7%) | 0.843 | |||||
| 1 | 11 (36.7%) | 11 (36.7%) | |||||||
| 2 | 10 (33.3%) | 11 (36.7%) | |||||||
| 3 | 7 (23.3%) | 6 (20.0%) | |||||||
|
Gingival-wall penetration |
0 | 2 (6.7%) | 1 (3.3%) | 0.782 | |||||
| 1 | 11 (36.7%) | 11 (36.7%) | |||||||
| 2 | 7 (23.3%) | 11 (36.7%) | |||||||
| 3 | 10 (33.3%) | 7 (23.3%) | |||||||
| Ordinal scores were analyzed as paired ordinal data and were not averaged. p values were calculated using Wilcoxon signed-rank tests. | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



