Submitted:
05 June 2026
Posted:
09 June 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
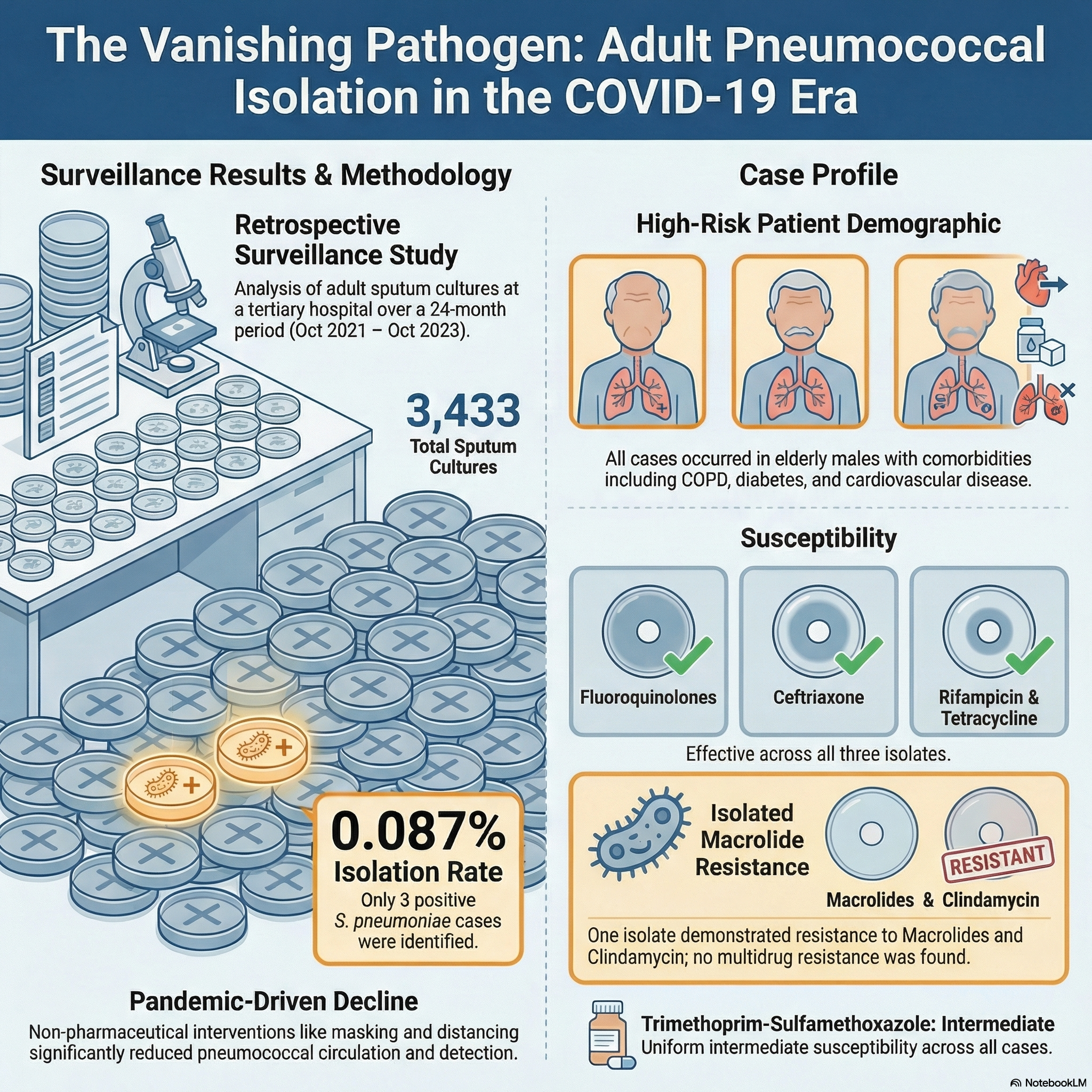
Objectives: Streptococcus pneumoniae is a major respiratory pathogen. Reports during the COVID-19 era suggest decreased pneumococcal activity. This study aimed to assess the frequency of S. pneumoniae in adult sputum cultures and its antimicrobial susceptibility in a tertiary care hospital. Materials and Methods: This retrospective laboratory-based study was conducted in a tertiary care hospital in Turkey. Sputum cultures from adult patients between October 1, 2021, and October 1, 2023, were analyzed. Demographic, clinical, and antimicrobial susceptibility data of culture-confirmed cases were obtained from medical records. Results: Among 3,433 sputum cultures, only three (0.087%; 95% CI: 0.018%–0.255%) yielded S. pneumoniae. All patients were male with comorbidities such as cardiovascular disease, COPD, or diabetes. Pneumonia developed during hospitalization for non-infectious conditions. All isolates were susceptible to fluoroquinolones, rifampicin, tetracycline, and ceftriaxone; one showed resistance to macrolides and clindamycin. No multidrug resistance was detected. Conclusion: An extremely low pneumococcal isolation rate was observed during the COVID-19 and post-pandemic period. These findings align with global reports of reduced pneumococcal activity. Continued surveillance is essential to monitor epidemiological trends and resistance patterns.
Keywords:
COVID
; epidemiology
; Pneumococcus
; sputum cultures
; Streptococcus pneumoniae
; surveillance
1. Introduction
Streptococcus pneumoniae has long been recognized as a leading cause of respiratory tract infections and invasive diseases, including pneumonia, bacteremia, and meningitis. Globally, the pathogen imposes a considerable burden, particularly among elderly individuals and patients with underlying comorbidities such as chronic pulmonary, cardiovascular, or renal diseases.[1] Prior to the COVID-19 pandemic, pneumococcal disease represented a significant public health concern; however, the epidemiological landscape was substantially influenced by the introduction of widespread non-pharmaceutical interventions such as social distancing, mask mandates, and lockdowns.[2,3]
International surveillance data reported a marked reduction in invasive pneumococcal disease during the early phase of the COVID-19 pandemic.[4,5] This phenomenon has been associated with decreased circulation of respiratory viruses, which are known to facilitate pneumococcal colonization and secondary bacterial infection. More recent reports suggest that pneumococcal activity may be gradually re-emerging following the relaxation of public health measures in certain regions.[6,7] These dynamic trends have generated renewed interest in the contemporary epidemiology of S. pneumoniae, particularly among adult populations with complex comorbidity profiles. However, whether this decline persists or is followed by a rebound in pneumococcal activity remains uncertain across different regions.
In Turkey, pneumococcal surveillance has primarily focused on pediatric populations and vaccine coverage studies.[8,9] Data describing pneumococcal isolation rates and antimicrobial susceptibility patterns in adult patients, especially within tertiary hospital settings, remain limited. Furthermore, the microbiological characteristics of pneumococcal isolates detected during the COVID-19 and post-pandemic period in Turkish adults have not been comprehensively described.
To address this gap, we conducted a retrospective laboratory-based surveillance study reviewing all adult sputum cultures processed at a tertiary training and research hospital between 1 October 2021 and 1 October 2023. The primary objective was to determine the frequency of S. pneumoniae isolation and to describe the clinical and antimicrobial susceptibility characteristics of detected isolates during the COVID-19 and post-pandemic period.
2. Materials and Methods
2.1. Ethical Approval and Informed Consent
The study protocol was reviewed and approved by the local Ethics Committee (Approval Number: 2023/65; Approval Date: October 12, 2023), in accordance with the Declaration of Helsinki and relevant national regulations. As this was a retrospective study using de-identified data, the requirement for informed consent was waived by the ethics committee.
2.2. Study Design and Setting
This retrospective, laboratory-based surveillance study was conducted at a tertiary care training and research hospital in Istanbul, Turkey. The study period extended from October 1, 2021, to October 1, 2023. All consecutive sputum cultures obtained from adult patients (≥18 years) as part of routine clinical care during this period were identified and systematically reviewed through the hospital’s microbiology database. No additional sampling or selective inclusion was performed. Relevant clinical data, including demographic characteristics, comorbidities, and admission details, were extracted from the hospital’s electronic medical records system.
2.3. Case Definition and Eligibility
Cases were defined as adult patients (≥18 years) with at least one sputum culture positive for S. pneumoniae during the study period. For the calculation of the pneumococcal isolation rate, all consecutive sputum cultures obtained from adult patients within the same period were included as the denominator. Repeated positive cultures from the same patient, if present, were considered a single case for descriptive analysis.
2.4. Data Collection
Data were extracted from the hospital’s electronic laboratory information system and electronic medical records. For all adult sputum cultures processed during the study period, the total number of samples was recorded to calculate the pneumococcal isolation rate. For patients with culture-confirmed S. pneumoniae, the following variables were collected: age, sex, smoking status (when available), major comorbidities (including diabetes mellitus, hypertension, cardiovascular or cerebrovascular disease, and chronic pulmonary conditions), indication for hospital admission, intensive care unit requirement, in-hospital outcome, specimen collection date, and antimicrobial susceptibility results, including minimum inhibitory concentrations (when available). These variables were selected to characterize the clinical context and microbiological features of confirmed cases.
2.5. Microbiological Procedures
Sputum samples were processed as part of routine clinical microbiology practice during the study period. Specimens were evaluated for quality using standard laboratory criteria prior to culture processing. Samples deemed acceptable were inoculated onto appropriate culture media, including sheep blood agar, and incubated under conventional conditions. Bacterial identification was performed using the automated identification system routinely employed in the laboratory at the time of analysis. When required, confirmatory phenotypic methods such as assessment of alpha-hemolysis and optochin susceptibility testing were applied in accordance with standard laboratory procedures.
2.6. Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was performed as part of routine laboratory practice using the automated system employed during the study period. Results were interpreted according to the breakpoint criteria defined by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines applicable at the time of testing. Susceptibility categories were reported as susceptible (including susceptible, increased exposure) or resistant. Minimum inhibitory concentrations (MICs) were recorded when available in the laboratory information system.
2.7. Outcomes
The primary outcome was the pneumococcal isolation rate, defined as the proportion of S. pneumoniae-positive sputum cultures among all adult sputum samples processed during the study period. In addition, the antimicrobial susceptibility profiles of confirmed isolates were evaluated. Secondary outcomes included the clinical characteristics of patients with culture-confirmed S. pneumoniae, including comorbidity burden, intensive care unit requirement, in-hospital outcome, and the temporal distribution of detected isolates across the study period.
2.8. Statistical Analysis
The pneumococcal isolation rate was calculated as the proportion of S. pneumoniae-positive cultures among all adult sputum samples processed during the study period. Exact binomial 95% confidence intervals (CIs) were calculated for the isolation rate. Given the limited number of positive isolates, all other analyses were descriptive. No formal comparative statistical analyses were performed.
3. Results
During the study period (October 1, 2021–October 1, 2023), a total of 3,433 adult sputum cultures were processed at the tertiary care center. S. pneumoniae was isolated in three cases, corresponding to a pneumococcal isolation rate of 0.087% (95% CI: 0.018%–0.255%). No additional pneumococcal isolates were identified from other respiratory or sterile site cultures during the same period.
All positive cases occurred in male patients aged 45 to 81 years (median: 57 years). Two patients were ex-smokers with significant smoking histories (30 and 50 pack-years, respectively), while one had never smoked. Each patient had at least one underlying comorbidity, including cardiovascular disease, chronic obstructive pulmonary disease (COPD), diabetes mellitus, or hyperthyroidism. In all three cases, pneumonia developed during hospitalization for non-infectious primary conditions (vascular access revision, cerebrovascular event, and orthopedic trauma), which prompted microbiological investigation. The demographic and clinical characteristics of patients with culture-confirmed S. pneumoniae are summarized in Table 1.
Antimicrobial susceptibility testing results are summarized in Table 2.
All isolates were susceptible to fluoroquinolones (levofloxacin and moxifloxacin), rifampicin, tetracycline, chloramphenicol, and ceftriaxone. One isolate (Patient 1) demonstrated resistance to erythromycin (MIC ≥8 µg/mL) and clindamycin (MIC ≥1 µg/mL). Trimethoprim/sulfamethoxazole showed intermediate susceptibility across all three isolates. None of the isolates met criteria for multidrug resistance.
The detected cases were distributed sporadically over the study period without evidence of temporal clustering. All patients responded clinically to targeted antimicrobial therapy, and no in-hospital mortality was observed.
4. Conclusions
This retrospective laboratory-based surveillance study demonstrates an extremely low pneumococcal isolation rate from adult sputum cultures in a tertiary care center over a two-year period encompassing the COVID-19 and post-pandemic era. Among 3,433 sputum cultures processed, only three yielded pneumococcal growth, corresponding to an isolation rate of 0.087% (95% CI: 0.018%–0.255%). Although sputum cultures were frequently processed during the study period, culture-confirmed detection of S. pneumoniae was rare. All identified cases occurred in male patients with underlying comorbidities, and pneumonia developed during hospitalization for non-infectious primary conditions. Given the limited number of isolates, these observations should be interpreted cautiously.
The low culture yield observed in our cohort is consistent with recent epidemiological shifts reported globally in the wake of the COVID-19 pandemic. Non-pharmaceutical interventions (e.g., masking, physical distancing), reduced transmission of respiratory pathogens, and changes in healthcare-seeking behavior have collectively led to a decline in community-acquired pneumococcal disease.[10]
Furthermore, empirical use of antibiotics—especially macrolides and beta-lactams—in outpatient and inpatient settings may have reduced culture positivity, either by suppressing viable pneumococci or altering the airway microbiome.[11]
Another plausible contributor is the impact of adult pneumococcal vaccination programs. Turkey introduced pneumococcal conjugate vaccines into the national childhood immunization schedule in 2008 with PCV7, which was replaced by PCV13 in 2011 as part of the routine program.[8] Recent studies have also shown that targeted adult vaccination, particularly among the elderly and high-risk groups, can significantly reduce invasive pneumococcal disease and possibly carriage. Targeted adult immunization, particularly in high-risk groups such as the elderly and those with chronic diseases, may further reduce pneumococcal disease burden in hospitalized populations.[13]
Microbiologically, all isolates in our cohort were susceptible to ceftriaxone, moxifloxacin, levofloxacin, rifampicin, and tetracycline, agents commonly employed in empirical pneumonia treatment. These findings are in line with recent surveillance studies from Turkey and Europe, which report high susceptibility rates to beta-lactams and fluoroquinolones in respiratory S. pneumoniae isolates.[14]
However, resistance to macrolides and lincosamides was observed in one patient, with erythromycin MIC ≥8 µg/mL and clindamycin resistance. This pattern reflects trends showing rising macrolide resistance, particularly in regions with extensive outpatient macrolide use.[14,15]
The detected intermediate susceptibility to trimethoprim/sulfamethoxazole (TMP-SMX) in all isolates is also noteworthy. Previous studies have reported substantial variability in TMP-SMX resistance among Streptococcus pneumoniae isolates, with approximately one-third of isolates showing resistance in some settings, highlighting the heterogeneity in susceptibility patterns.[16] Although not a first-line agent for pneumococcal pneumonia, TMP-SMX susceptibility data may still provide supportive information for step-down or oral therapy decisions in selected cases, particularly in resource-limited settings.
Importantly, none of the isolates in our study met criteria for multidrug resistance (MDR), a reassuring finding given the recognized presence of MDR pneumococcal lineages reported in surveillance studies.[17] However, the small sample size precludes broader conclusions, and continuous surveillance is essential to monitor emerging resistance patterns.
The present findings also highlight the diagnostic limitations of sputum cultures. Pre-analytical factors such as prior antibiotic exposure, poor sputum quality, or delayed transport can reduce yield.[11] Additionally, in the elderly or debilitated population, lower respiratory tract infection may present atypically, further complicating microbiological confirmation.[18] Nonetheless, the detection of S. pneumoniae in these patients—each with documented clinical deterioration and radiographic findings—supports its role as a relevant pathogen in selected hospital-acquired or secondary pneumonia cases.
5. Limitations
This study has several important limitations. First, the retrospective design limits the ability to establish causal relationships and prevents direct comparison with the pre-pandemic period. Second, the extremely small number of pneumococcal isolates restricts generalizability and limits the scope of statistical inference beyond descriptive analysis. Third, only sputum cultures were evaluated; data from other respiratory or sterile site specimens were not systematically included, which may have led to underestimation of the true pneumococcal disease burden. In addition, information on vaccination status, prior antibiotic exposure, and radiological findings was not uniformly available and therefore could not be systematically analyzed. Finally, variability in sputum specimen quality and other pre-analytical factors may have influenced culture yield.
6. Conclusions
This retrospective laboratory-based surveillance study demonstrates an extremely low pneumococcal isolation rate from adult sputum cultures in a tertiary hospital during the COVID-19 and post-pandemic period. Although direct comparison with pre-pandemic data was not possible, the observed findings are consistent with international reports describing reduced pneumococcal detection during the pandemic era. The limited number of isolates prevents definitive conclusions regarding resistance trends; however, susceptibility to commonly used antimicrobial agents was largely preserved. Continued microbiological surveillance remains essential to monitor evolving epidemiological patterns and antimicrobial susceptibility profiles.
Ethics Approval: The study protocol was reviewed and approved by the Ethics Committee of Fatih Sultan Mehmet Training and Research Hospital (Approval Number: 2023/65; Approval Date: October 12, 2023), in accordance with the Declaration of Helsinki and relevant national regulations. As this was a retrospective study using de-identified data, the requirement for informed consent was waived by the ethics committee.
Author Contributions
Conceptualization, I.K.; methodology, I.K. and M.E.; data curation, M.E. and S.D.T.; formal analysis, I.K.; investigation, I.K., M.E., and S.D.T.; writing-original draft preparation, I.K.; writing-review and editing, I.K., M.E., and S.D.T.; supervision, I.K. All authors have read and agreed to the published version of the manuscript.
Funding
No external funding was received for the conduct of this research or the preparation of the manuscript. The study was carried out without financial support from any public, commercial, or not-for-profit sectors. The sponsors had no role in the study design, data collection, analysis, or interpretation, manuscript writing, or the decision to submit the article for publication.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to patient privacy and institutional data protection policies. However, anonymized data may be available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank the laboratory staff of Fatih Sultan Mehmet Training and Research Hospital for their support in data collection and processing.
Declaration of Artificial Intelligence (AI)–Assisted Technology: AI-assisted tools were used only for language editing and grammatical refinement. The authors reviewed and approved the final version of the manuscript and take full responsibility for its content.
Abbreviations
| CI | Confidence Interval |
| COPD | Chronic Obstructive Pulmonary Disease |
| EUCAST | European Committee on Antimicrobial Susceptibility Testing |
| MIC | Minimum Inhibitory Concentration |
| MDR | Multidrug Resistance |
| PCV7 | 7-valent Pneumococcal Conjugate Vaccine |
| PCV13 | 13-valent Pneumococcal Conjugate Vaccine |
| TMP-SMX | Trimethoprim-Sulfamethoxazole |
References
- Vaughn, V.M.; Dickson, R.P.; Horowitz, J.K.; Flanders, S.A. Community-acquired pneumonia: a review. JAMA 2024, 332, 1282–1295. [Google Scholar] [CrossRef] [PubMed]
- Amin-Chowdhury, Z.; Aiano, F.; Mensah, A.; et al. Impact of the coronavirus disease 2019 (COVID-19) pandemic on invasive pneumococcal disease and risk of pneumococcal coinfection with SARS-CoV-2: prospective national cohort study, England. Clin. Infect. Dis. 2021, 72, e65–e75. [Google Scholar] [CrossRef] [PubMed]
- Steens, A.; Knol, M.J.; Freudenburg-de Graaf, W.; de Melker, H.E.; van der Ende, A.; van Sorge, N.M. Pathogen- and type-specific changes in invasive bacterial disease epidemiology during the first year of the COVID-19 pandemic in the Netherlands. Microorganisms 2022, 10, 972. [Google Scholar] [CrossRef] [PubMed]
- Danino, D.; Ben-Shimol, S.; van der Beek, B.A.; et al. Decline in pneumococcal disease in young children during the COVID-19 pandemic in Israel associated with suppression of seasonal respiratory viruses. Clin. Infect. Dis. 2022, 75, e1154–e1164. [Google Scholar] [CrossRef] [PubMed]
- GBD 2021 Lower Respiratory Infections and Antimicrobial Resistance Collaborators. Global, regional, and national incidence and mortality burden of non-COVID-19 lower respiratory infections and aetiologies, 1990–2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Infect. Dis. 2024, 24, 974–1002. [CrossRef]
- Takeuchi, N.; Chang, B.; Ishiwada, N.; et al. Nationwide population-based surveillance of invasive pneumococcal disease in children in Japan (2014–2022): impact of 13-valent pneumococcal conjugate vaccine and COVID-19 pandemic. Vaccine 2025, 54, 127138. [Google Scholar] [CrossRef] [PubMed]
- Zintgraff, J.; Gagetti, P.; Eluchans, N.S.; et al. Invasive pneumococcal disease in Argentina: a retrospective study on serotypes, resistance, and the impact of the COVID-19 pandemic (2018–2022). Lancet Reg. Health Am. 2025, 46, 101113. [Google Scholar] [CrossRef] [PubMed]
- Soysal, A.; Karabağ-Yılmaz, E.; Kepenekli, E.; et al. Impact of a pneumococcal conjugate vaccination program on nasopharyngeal carriage and resistance of Streptococcus pneumoniae among healthy children in Turkey. Vaccine 2016, 34, 3894–3900. [Google Scholar] [CrossRef] [PubMed]
- Hascelik, G.; Soyletir, G.; Gulay, Z.; et al. Serotype distribution of Streptococcus pneumoniae and pneumococcal vaccine coverage in adults in Turkey between 2015 and 2018. Ann. Med. 2023, 55, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Brueggemann, A.B.; Jansen van Rensburg, M.J.; Shaw, D.; et al. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries. Lancet Digit Health 2021, 3, e360–e370. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Lee, N.; Cilloniz, C.; Vila, J.; Van der Eerden, M. Laboratory diagnosis of pneumonia in the molecular age. Eur. Respir. J. 2016, 48(6), 1764–1778. [Google Scholar] [CrossRef] [PubMed]
- Ceyhan, M.; Karadag-Oncel, E.; Hascelik, G.; et al. Nasopharyngeal carriage of Streptococcus pneumoniae in healthy children aged less than five years. Vaccine 2021, 39(15), 2041–2047. [Google Scholar] [CrossRef] [PubMed]
- Matanock, A.; Lee, G.; Gierke, R.; Kobayashi, M.; Leidner, A.J.; Pilishvili, T. Use of PCV13 and PPSV23 among adults aged ≥65 years: updated recommendations. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Torumkuney, D.; Aktas, Z.; Unal, S.; et al. Country data on antimicrobial resistance in Türkiye in the context of community-acquired respiratory tract infections: links between antibiotic susceptibility, prescribing guidelines, access to medicine, and clinical outcome. J. Antimicrob. Chemother. 2022, 77 (Suppl 1), i51–i60. [Google Scholar] [CrossRef] [PubMed]
- Torumkuney, D.; Keles, N.; Hasdemir, U.; et al. Results from the Survey of Antibiotic Resistance (SOAR) 2018–21 in Türkiye: data based on CLSI, EUCAST, and pharmacokinetic/pharmacodynamic breakpoints. J. Antimicrob. Chemother. 2025, 80 (Suppl 3), iii98–iii113. [Google Scholar] [CrossRef] [PubMed]
- Cherazard, R.; Epstein, M.; Doan, T.L.; Salim, T.; Bharti, S.; Smith, M.A. Antimicrobial resistant Streptococcus pneumoniae: prevalence, mechanisms, and clinical implications. Am. J. Ther. 2017, 24(3), e361–e369. [Google Scholar] [CrossRef] [PubMed]
- Metcalf, B.J.; Gertz, R.E., Jr.; Gladstone, R.A.; et al. Strain features and distributions in pneumococci from children with invasive disease before and after 13-valent conjugate vaccine implementation in the USA. Clin. Microbiol. Infect. 2016, 22(1), 60.e9–60.e29. [Google Scholar] [CrossRef] [PubMed]
- Janssens, J.P.; Krause, K.H. Pneumonia in the very old. Lancet Infect. Dis. 2004, 4, 112–124. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Demographic and Clinical Characteristics of Patients.
| Patient | Age | Sex | Smoking History | Comorbidities | Admission Reason | Diagnosis |
|---|---|---|---|---|---|---|
| 1 | 57 | Male | Ex-smoker, 30 pack-years |
Coronary artery disease, diabetes, hypertension, chronic obstructive pulmonary disease, chronic renal failure (dialysis) | Fistula revision | Pneumonia |
| 2 | 45 | Male | Nonsmoker | Hyperthyroidism | Cerebrovascular event | Pneumonia |
| 3 | 81 | Male | Ex-smoker, 50 pack-years |
Hypertension, epilepsy, cerebrovascular event, chronic obstructive pulmonary disease | Femur fracture | Pneumonia |
Table 2.
Antimicrobial Susceptibility of S. pneumoniae Isolates.
| Antibiotic | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| Erythromycin | ≥8 (R) | ≤0.12 (S) | ≤0.12 (S) |
| Clindamycin | ≥1 (R) | ≤0.25 (S) | ≤0.25 (S) |
| Levofloxacin | 0.5 (S) | 1 (S) | 0.5 (S) |
| Moxifloxacin | 0.12 (S) | 0.12 (S) | 0.12 (S) |
| Rifampicin | ≤0.06 (S) | ≤0.06 (S) | ≤0.06 (S) |
| Tetracycline | ≤0.25 (S) | ≤0.25 (S) | ≤0.25 (S) |
| Chloramphenicol | 2 (S) | 2 (S) | 2 (S) |
| Ceftriaxone | ≤0.12 (S) | ≤0.12 (S) | ≤0.12 (S) |
| Trimethoprim-sulfamethoxazole | ≤10 (I) | ≤10 (I) | ≤10 (I) |
MIC values are expressed in µg/mL. Interpretations were based on EUCAST breakpoint criteria valid during the year of testing. S: Susceptible; I: Susceptible, increased exposure; R: Resistant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



