Submitted:
03 June 2026
Posted:
04 June 2026
You are already at the latest version
Abstract
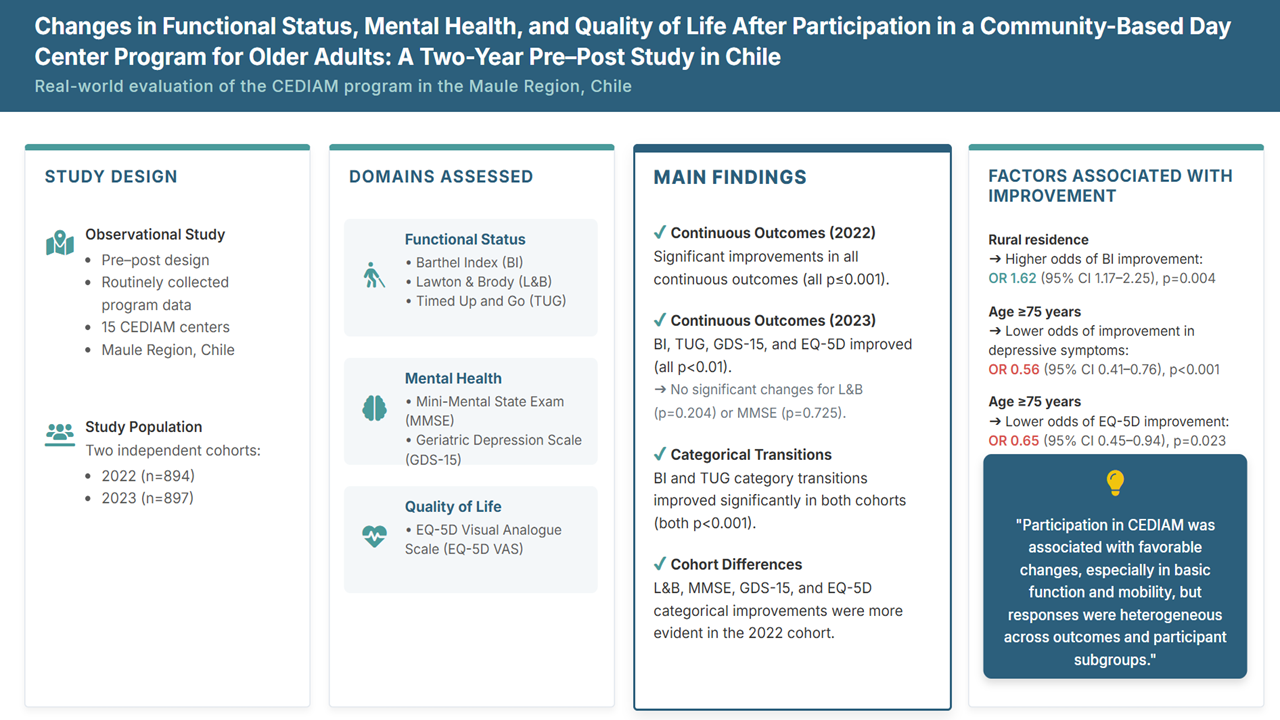
Objective: To examine changes in functional status, mental health, and quality of life among older adults participating in the CEDIAM program in the Maule Region of Chile in 2022 and 2023. Methods: Pre-post observational study using routinely collected data from 15 CEDIAM centers. The 2022 and 2023 datasets were analyzed as independent cohorts. Functional status was assessed with the Barthel Index (BI), Lawton and Brody scale (L&B), and Timed Up and Go test (TUG); mental health with the Mini-Mental State Examination (MMSE) and Geriatric Depression Scale-15 (GDS-15); and quality of life with the EuroQol-5D visual analogue scale (EQ-5D). Paired comparisons, category-transition analyses, and multivariable logistic regression models of improvement were performed. Results: Baseline samples included 894 participants in 2022 and 897 in 2023. In 2022, all continuous outcomes improved significantly (all p≤0.001). In 2023, BI, TUG, GDS-15, and EQ-5D improved (all p<0.01), whereas L&B (p=0.204) and MMSE (p=0.725) did not. Category-transition analyses showed significant improvements in BI and TUG in both cohorts (both p<0.001), while significant categorical changes in L&B, MMSE, GDS-15, and EQ-5D were observed only in 2022 (all p≤0.01). Rural residence was associated with higher odds of BI improvement (OR 1.62, 95% CI 1.17-2.25; p=0.004), whereas age ≥75 years was associated with lower odds of improvement in GDS-15 (OR 0.56, 95% CI 0.41-0.76; p<0.001) and EQ-5D (OR 0.65, 95% CI 0.45-0.94; p=0.023). Conclusion: Participation in CEDIAM was associated with favorable changes, particularly in basic functional status and mobility, although responses varied across outcomes and participant subgroups.
Keywords:
1. Introduction
2. METHODOLOGY
2.1. Study design and data source
2.2. Participants
2.3. Geriatric assessment and study outcomes
2.4. Functional status
2.5. Mental health
2.6. Quality of life
2.7. Definition of improvement
2.8. Covariates
2.9. Statistical analysis
2.10. Data authorization and ethical considerations
3. RESULTS
3.1. Baseline characteristics of the 2022 and 2023 cohorts
3.2. Changes in continuous scores between entry and exit
3.3. Category transitions between entry and exit



3.4. Factors associated with improvement across outcomes
4. DISCUSSION
5. CONCLUSION
Supplementary Materials
Competing interest statement
Funding statement
References
- Albala, C. EL ENVEJECIMIENTO DE LA POBLACIÓN CHILENA Y LOS DESAFÍOS PARA LA SALUD Y EL BIENESTAR DE LAS PERSONAS MAYORES. Rev. Médica Clínica Las Condes 2020, 31(1), 7–12. [Google Scholar] [CrossRef]
- Lunenfeld, B. An Aging World--demographics and challenges. Gynecol. Endocrinol. 2008, 24(1), 1–3. [Google Scholar] [CrossRef] [PubMed]
- Thumala, D.; Kennedy, B.K.; Calvo, E.; Gonzalez-Billault, C.; Zitko, P.; Lillo, P.; et al. Aging and Health Policies in Chile: New Agendas for Research. Health Syst. Reform. 2017, 3(4), 253–60. [Google Scholar] [CrossRef] [PubMed]
- Quevedo, I.; Ormeño, J.C.; Weissglas, B.; Opazo, C. Epidemiology and Direct Medical Cost of Osteoporotic Hip Fracture in Chile. J. Osteoporos. 2020, 2020, 5360467. [Google Scholar] [CrossRef] [PubMed]
- Saldivia, S.; Aslan, J.; Cova, F.; Bustos, C.; Inostroza, C.; Castillo-Carreño, A. Life satisfaction, positive affect, depression and anxiety symptoms, and their relationship with sociodemographic, psychosocial, and clinical variables in a general elderly population sample from Chile. Front Psychiatry 2023, 14, 1203590. [Google Scholar] [CrossRef] [PubMed]
- Villalobos Dintrans, P. [Aging and long-term care in Chile: challenges in the OECD context]. Rev. Panam. Salud Publica 2017, 41, e86. [Google Scholar] [PubMed]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; et al. The World report on ageing and health: a policy framework for healthy ageing. Lancet 2016, 387(10033), 2145–54. [Google Scholar] [CrossRef] [PubMed]
- Kuzuya, M.; Masuda, Y.; Hirakawa, Y.; Iwata, M.; Enoki, H.; Hasegawa, J.; et al. Day care service use is associated with lower mortality in community-dwelling frail older people. J. Am. Geriatr. Soc. 2006, 54(9), 1364–71. [Google Scholar] [CrossRef] [PubMed]
- Lunt, C.; Dowrick, C.; Lloyd-Williams, M. What is the impact of day care on older people with long-term conditions: A systematic review. Health Soc. Care Community 2021, 29(5), 1201–21. [Google Scholar] [PubMed]
- Orellana, K.; Manthorpe, J.; Tinker, A. Day centres for older people: a systematically conducted scoping review of literature about their benefits, purposes and how they are perceived. Ageing Soc. 2020, 40(1), 73–104. [Google Scholar] [PubMed]
- Jönsson, M.; Pettersson, C.; Lindvall, M.A. Rehabilitation interventions at senior day centres for older adults: a scoping review. Front Public Health 2025, 13, 1659493. [Google Scholar] [CrossRef] [PubMed]
- Tuohy, D.; Kingston, L.; Carey, E.; Graham, M.; Dore, L.; Doody, O. A scoping review on the psychosocial interventions used in day care service for people living with dementia. PLoS ONE 2023, 18(12), e0295507. [Google Scholar] [CrossRef] [PubMed]
- SENAMA. Guía de Operaciones para Centros Diurnos Comunitarios. 2025.
- Rubio, M.; Miranda, C. Centros diurnos para personasmayores, Servicio Nacional del AdultoMayor: realidad y desafíos a tres añosde su implementación. In Propuestas para Chile2017; Católica, P.U., Ed.;
- Glasinovic, A.; Rodríguez, C.; Martín, P.S.; González, D.; Guzmán, R.; Ureta, M.D.P.; et al. Efectividad a mediano plazo de un programa multidimensional en personas mayores en centros diurnos en Chile. Rev. Médica De Chile 2022, 150, 23–32. [Google Scholar] [CrossRef]
- Cid-Ruzafa, J.; Damián-Moreno, J. Valoración de la discapacidad física: el indice de Barthel. Rev. Española De Salud Pública 1997, 71, 127–37. [Google Scholar] [CrossRef]
- Salud Md. ESTRATEGIA DE RESIDENCIAS SANITARIAS. GUÍA DE RECOMENDACIONES PARA EL CUIDADO DE PERSONAS MAYORES EN LAS RESIDENCIAS SANITARIAS. 2020.
- Graf, C. The Lawton instrumental activities of daily living scale. Am. J. Nurs. 2008, 108(4), 52-62; quiz -3. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2019, 48(1), 16–31. [Google Scholar] [CrossRef] [PubMed]
- Quiroga, P.; Albala, C.; Klaasen, G. [Validation of a screening test for age associated cognitive impairment, in Chile]. Rev. Med. Chil. 2004, 132(4), 467–78. [Google Scholar] [PubMed]
- Yesavage, J.A.; Sheikh, J.I. 9/Geriatric Depression Scale (GDS). Clin. Gerontol. 1986, 5(1-2), 165–73. [Google Scholar] [CrossRef]
- Badia Llach, X.; Herdman, M.; Schiaffino, A. Determining correspondence between scores on the EQ-5D "thermometer" and a 5-point categorical rating scale. Med. Care 1999, 37(7), 671–7. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Badia, X.; Berra, S. [EuroQol-5D: a simple alternative for measuring health-related quality of life in primary care]. Aten. Primaria 2001, 28(6), 425–30. [Google Scholar] [PubMed]
- Kitamura, M.; Izawa, K.P.; Kurihara, K.; Yamamoto, S.; Ozawa, S.; Uchida, E.; et al. Relationship between IADL, physical function, physical activity, and fall-related efficacy among older people using daycare centers. Discov. Public Health 2025, 22(1), 478. [Google Scholar] [CrossRef]
- Jacob, M.E.; Abraham, V.J.; Abraham, S.; Jacob, K.S. The effect of community based daycare on mental health and quality of life of elderly in rural south India: a community intervention study. Int. J. Geriatr. Psychiatry 2007, 22(5), 445–7. [Google Scholar] [PubMed]
- Malone, M.; Hill, A.; Smith, G. Three-month follow up of patients discharged from a geriatric day hospital. Age Ageing 2002, 31(6), 471–5. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Seo, K.; Choi, S.; Choi, J.; Ko, H.; Lee, S.J. Seniors centre-based health intervention programmes in the United States and South Korea: A systematic review. Int. J. Nurs. Pract. 2017, 23(5). [Google Scholar] [PubMed]
- Burch, S.; Longbottom, J.; McKay, M.; Borland, C.; Prevost, T. A randomized controlled trial of day hospital and day centre therapy. Clin. Rehabil. 1999, 13(2), 105–12. [Google Scholar] [CrossRef] [PubMed]
- Ho, L.; Malden, S.; McGill, K.; Shimonovich, M.; Frost, H.; Aujla, N.; et al. Complex interventions for improving independent living and quality of life amongst community-dwelling older adults: a systematic review and meta-analysis. Age Ageing 2023, 52(7), afad132. [Google Scholar] [CrossRef] [PubMed]
- Bøen, H.; Dalgard, O.S.; Johansen, R.; Nord, E. A randomized controlled trial of a senior centre group programme for increasing social support and preventing depression in elderly people living at home in Norway. BMC Geriatr. 2012, 12, 20. [Google Scholar] [CrossRef] [PubMed]
- Takemura, Y.; Inoue, K.; Sato, K.; Haseda, M.; Shiba, K.; Kondo, N. Social Participation and Depressive Symptoms Among Older Adults. JAMA Netw. Open. 2025, 8(9), e2530523–e. [Google Scholar] [CrossRef] [PubMed]
- Sadarangani, T.; Fernandez Cajavilca, M.; Qi, X.; Zagorski, W. Adult day services: a potential antidote to social isolation and loneliness in marginalized older adults. Front Public Health 2024, 12, 1427425. [Google Scholar] [CrossRef] [PubMed]

| Variables | 2022 (n=894) | 2023 (n=897) | p-value |
|---|---|---|---|
| Age (years) (median (IQR)a | 74 (68-78) | 73 (68-77.5) | 0.081 |
| Sex n (%)b | 0.830 | ||
| Women | 718 (80.3) | 724 (80.5) | |
| Men | 176 (19.7) | 173 (19.5) | |
| Residence n (%)b | <0.0001 | ||
| - Urban | 724 (81) | 647 (72.1) | |
| - Rural | 170 (19) | 250 (27.8) | |
| Multimorbidity n (%)b | <0.0001 | ||
| - < 2 diseases | 495 (55.4) | 411 (45.9) | |
| - ≥ 2 diseases | 399 (44.6) | 486 (54.1) | |
| Education level n (%)b | 0.346 | ||
| - Low education (≤ primary completed) | 542 (60.5) | 532 (59.2) | |
| - Higher education (≥ secondary uncompleted) | 327 (36.6) | 352 (39.1) | |
| - Unregistered | 25 (2.9) | 13 (1.4) | - |
| 2022 | ||||
|---|---|---|---|---|
| Functional status | ||||
| Scales | n (paired) | Entry (median [IQR]) | Exit (median [IQR]) | p-value |
| BI | 556 | 90 (85–95) | 90 (85–85) | <0.0001 |
| L&B | 437 | 7 (6–8) | 8 (7–8) | <0.0001 |
| TUG | 348 | 10 (8–13) | 9 (8–12) | <0.0001 |
| Mental health | ||||
| MMSE | 348 | 26 (20.3–29) | 27 (21.3–30) | <0.0001 |
| GDS-15 | 372 | 6 (3–10) | 5 (3–8) | <0.0001 |
| Quality of life | ||||
| EQ-5D | 324 | 60 (12–80) | 70 (14.8–80) | <0.001 |
| 2023 | ||||
|---|---|---|---|---|
| Functional status | ||||
| Scales | n (paired) | Entry (median [IQR]) | Exit (median [IQR]) | p-value |
| BI | 363 | 90 (85–95) | 95 (90–95) | <0.0001 |
| L&B | 353 | 7 (7–8) | 8 (7–8) | 0.204 |
| TUG | 276 | 9 (7–11) | 8 (7–10) | <0.0001 |
| Mental health | ||||
| MMSE | 336 | 27 (22–30) | 27 (23–30) | 0.725 |
| GDS-15 | 284 | 5 (2–9) | 4 (2–7) | <0.0001 |
| Quality of life | ||||
| EQ-5D | 223 | 60 (11–80) | 60 (11–80) | <0.01 |
| Barthel Index | Lawton & Brody | Timed Up and Go | ||||
|---|---|---|---|---|---|---|
| Covariate | OR (CI 95%) | p-value | OR (CI 95%) | p-value | OR (CI 95%) | p-value |
| Residence (rural) | 1.62 (1.17–2.25) | 0.004 | 1.38 (0.94–2.04) | 0.105 | 1.05 (0.73–1.51) | 0.788 |
| Sex (woman) | 0.86 (0.61–1.20) | 0.366 | 0.62 (0.42–0.93) | 0.019 | 1.15 (0.78–1.68) | 0.487 |
| Age ≥75 years | 0.98 (0.74–1.29) | 0.866 | 1.17 (0.83–1.66) | 0.360 | 1.02 (0.74–1.4) | 0.915 |
| Low educational level | 0.87 (0.66–1.15) | 0.326 | 1.36 (0.95–1.94) | 0.097 | 1.29 (0.93–1.78) | 0.133 |
| Multimorbidity (≥2 diseases) | 0.97 (0.70–1.35) | 0.851 | 0.55 (0.36–0.84) | 0.005 | 1.30 (0.82–2.06) | 0.259 |
| Hypertension | 0.79 (0.51–1.21) | 0.271 | 0.57 (0.34–0.98) | 0.041 | 0.89 (0.51–1.54) | 0.672 |
| Type 2 diabetes mellitus | 0.50 (0.18–1.11) | 0.083 | 0.16 (0.04–0.98) | 0.017 | 0.48 (0.17–1.34) | 0.160 |
| Mini-Mental State Examination | Geriatric Depression Scale | |||
|---|---|---|---|---|
| Covariate | OR (CI 95%) | p-value | OR (CI 95%) | p-value |
| Residence (rural) | 0.92 (0.6–1.37) | 0.677 | 1.02 (0.71–1.47) | 0.904 |
| Sex (woman) | 1.21 (0.81–1.80) | 0.347 | 1.08 (0.74–1.57) | 0.697 |
| Age ≥75 years | 0.99 (0.72–1.36) | 0.936 | 0.56 (0.41–0.76) | <0.0001 |
| Low educational level | 1.34 (0.97–1.85) | 0.080 | 0.91 (0.66–1.25) | 0.569 |
| Multimorbidity (≥2 diseases) | 1.34 (0.89–2.02) | 0.166 | 1.20 (0.79–1.81) | 0.387 |
| Hypertension | 0.52 (0.29–0.94) | 0.031 | 1.38 (0.81–2.36) | 0.234 |
| Type 2 diabetes mellitus | 1.29 (0.46–3.58) | 0.629 | 1.04 (0.35–3.07) | 0.948 |
| Covariate | OR (CI 95%) | p-value |
|---|---|---|
| Residence (rural) | 0.83 (0.55–1.24) | 0.360 |
| Sex (woman) | 1.62 (1.02–2.58) | 0.041 |
| Age ≥75 years | 0.65 (0.45–0.94) | 0.023 |
| Low educational level | 0.93 (0.63–1.37) | 0.702 |
| Multimorbidity (≥2 diseases) | 1.55 (0.93–2.60) | 0.094 |
| Hypertension | 0.57 (0.31–1.06) | 0.075 |
| Type 2 diabetes mellitus | 0.89 (0.31–2.55) | 0.826 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



