Submitted:
03 June 2026
Posted:
04 June 2026
You are already at the latest version
Abstract
Background/Objectives: Despite Hematoxylin and eosin (H&E) staining remains the cornerstone of histopathological diagnosis, substantial intra- and inter-laboratory variability persists. This issue is increasingly relevant in Digital Pathology, where staining inconsistency may affect whole-slide image interpretation and the performance of image analysis algorithms. In the present work, we evaluated the diagnostic adequacy and non-inferiority of a novel tabs-based H&E staining method compared with conventional liquid reagents. Methods: Fifty formalin-fixed paraffin-embedded tissue samples from routine practice were sectioned in duplicate and stained either conventionally or using H&E Stain Tabs. After slide review, 14 representative tissue samples were selected, scanned at 40x magnification, and used to generate 24 matched image pairs at different magnifications. A blind online survey was completed by 13 expert pathologists using high-quality monitors. Participants assessed overall staining preference and rated stromal, epithelial, cytoplasmic, and nuclear staining quality. Non-inferiority was tested using a predefined margin of −0.10, and paired rating differences were analyzed using the Wilcoxon signed-rank test. Results: Across 312 paired evaluations, the tabs-based method was preferred in 120 cases (38.5%), conventional staining in 118 cases (37.8%), and no preference was expressed in 74 cases (23.7%). The tabs-based method met the criterion for non-inferiority compared with standard staining (z = 2.7). Rating-scale analysis showed significantly better stromal evaluation with the tablet-based method (z = 2.638; p = 0.008), whereas no significant differences were observed for epithelial, cytoplasmic, or nuclear staining. All evaluated images were considered diagnostically adequate. Conclusions: The tabs-based H&E stain was non-inferior to the conventional method and showed particularly favorable performance in the assessment of stromal components. These findings support its potential role in improving staining reproducibility and standardization, particularly in Digital Pathology workflows where pre-analytical and analytical consistency is critical.
Keywords:
digital pathology
; pathology
; histology
; tissue stain
; H&E
; hematoxylin
; eosin
; pre-analytics
1. Introduction
Hematoxylin and eosin (H&E) staining has been the cornerstone of Anatomic Pathology for more than a century and remains the most adopted tissue-staining method worldwide [1]. Adequate staining highlights cellular and stromal components, thereby supporting histological examination, improving diagnostic confidence and reproducibility, and reducing the need for additional sectioning or immunohistochemistry in case of morphological uncertainty [2].
Nevertheless, a certain intra- and inter-laboratory variability in H&E staining is frequently observed and may be attributable to several causes. First, both hematoxylin and eosin are commonly supplied as prediluted solutions, which may be subject to degradation and influenced by external factors such as temperature and storage time. These issues are also associated with increased shipping and storage costs, as well as a potentially relevant environmental impact. In addition, tissue-section thickness can affect staining quality. Finally, staining variability may also reflect individual pathologists’ preferences regarding the balance between hematoxylin and eosin [3,4].
Despite valuable efforts by organizations such as the College of American Pathologists (CAP) and the United Kingdom National External Quality Assessment Service (UK NEQAS) to improve staining quality, universally accepted objective standards for assessing H&E staining adequacy are still lacking [2,4,5,6]. In routine practice, pathologists therefore assess H&E-stained sections largely based on experience and subjective preference. This issue has become increasingly relevant with the adoption of whole-slide imaging (WSI), as staining variability may affect both digital slide interpretation and the performance of artificial intelligence algorithms. Several studies have investigated digital normalization or virtual H&E staining of WSIs [7,8,9,10,11,12,13,14]. However, to the best of our knowledge, no studies have specifically addressed standardization at the staining-procedure level.
In this study, we evaluated a novel tabs-based H&E staining method designed to improve staining reproducibility. The evaluation was performed virtually by a selected group of expert pathologists using a Digital Pathology-based survey.
2. Materials and Methods
2.1. Sample Cohort
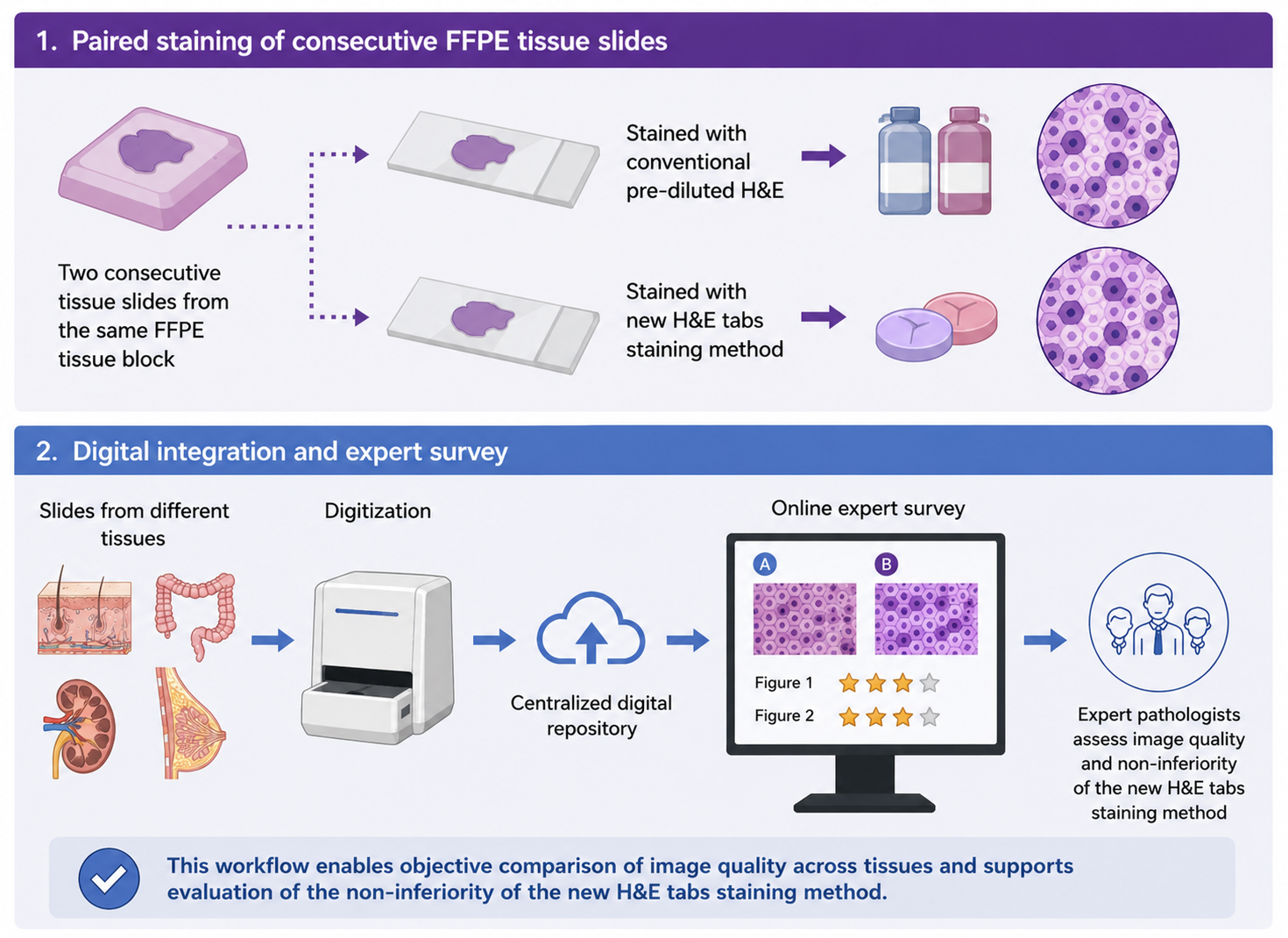
A total of 50 consecutive formalin-fixed and paraffin-embedded (FFPE) tissue samples from routine clinical practice were sectioned in duplicate at 5 µm thickness. For each sample, one section was stained conventionally, whereas the paired section was stained using Stain Tabs (Diapath®) for a total of 100 slides. After a careful review of tissue slides by three pathologists (L.N., E.I., and E.M.), 14 samples were selected based on histological and tissue variability, and 28 slides were digitized at 40x magnification by NanoZoomer 360SD (Hamamatsu®). A total of 48 images at different magnification levels (5x, 10x, 20x and 40x) were obtained focusing on both normal and pathological tissue features. Figure 1 represents the tissue-sample workflow.
All tissue samples enrolled, and magnification levels are reported in Table 1.
2.2. Staining Methods
FFPE tissue samples were sectioned at 3–5 μm thickness, mounted on glass slides, and dried prior to staining. H&E staining was performed using an automated staining system (Giotto, Diapath), following two protocols for standard and Stain Tabs-based tissue stain, respectively. All slides were first deparaffinized in three consecutive xylene baths (10 min each) and rehydrated through graded ethanol solutions (99% for 1 min, followed by two steps in 95% ethanol for 1 min each), then rinsed in distilled water for 2 min. In the standard protocol, hematoxylin (CP813, GILLII, Diapath) staining was carried out for 3 min, followed by washing in running tap water for 5 min, in ammonia water for 40 s, in running tap water for 2 min and in 95% ethanol for 1 min. Eosin (CO355, Eosin G OR Y alcoholic 0.5%, Diapath) counterstaining was carried out for 3 min. In case of Stain Tabs, hematoxylin and eosin solutions were obtained by overnight dilution of 1 hematoxylin and 1 eosin stain-tab in 800 ml of distilled water (400 ml each for hematoxylin and eosin) and added to the Giotto stainer after proper filtration. Slides were left in hematoxylin for 5 min, followed by washing in running tap water for 5 min. Slides were then treated with ammonia water for 1 min for bluing, rinsed again in running tap water for 2 min, and in distilled water for 1 min. Then, eosin counterstaining was carried out for 3 min. In both protocols, slides were subsequently dehydrated through graded alcohols and cleared in xylene and coverslipped using a permanent mounting medium.
2.3. Tissue Stain Evaluation
The new staining method was compared to the standard staining technique by a non-inferiority approach. We identified new simple parameters inspired by the CAP H&E Troubleshooting Guide and UK NEQAS staining evaluation criteria. Therefore, an online survey was developed using the JotForm® platform to allow the tissue stain evaluation. The survey was nominal and all participants were asked to provide their surname, given name, email address, and the monitor used for the evaluation. Participants had to express preference for pairs of images stained conventionally and by tabs, even specifying if they had no preferences; that in order to collect data on the overall stain preference (in this evaluation the overall intensity, specificity, uniformity of H&E were evaluated, along with the background, presence of particles, and contrast). Moreover, readers were asked to give a rating scale (from 1 to 3) for the epithelial/inflammatory and stromal components to evaluate the interactions of hematoxylin and eosin in these compartments. Similarly, a rating scale (from 1 to 3) was adopted for the nuclear and cytoplasmic staining in each image, representing an indirect parameter of adequacy for hematoxylin and eosin, respectively. Therefore, the survey comprised a total of 216 questions. A pilot test of the survey was first conducted during the 37th European Congress of Pathology (ECP) by eight volunteer pathologists under suboptimal environmental conditions to verify its usability and technical performance.
The survey was conducted by 13 expert pathologists from different centers (C. B., G. C., B. C., A. E., G.N. F., A. G., G. I., S. M., F. M., P. P., L. R., S. U., M. V.) adopting high quality monitors (screen size ranging from 27 to 75 inches with a minimum resolution of 3840 x 2160 – 8MP). Adopted screens are summarized in Table 2. The survey is available at https://form.jotform.com/251474857931366.
2.4. Statistical Analysis
A non-inferiority test was performed to compare the proportion of subjects selecting the new option versus the standard option. Responses were categorized as New, Standard, or None, with all categories included in the denominator for the calculation of proportions. The proportions of New (pN) and Standard (pS) choices were computed over the total number of observations, and the difference in proportions (d = pN − pS) was estimated. The variance and standard error of the difference were calculated assuming a binomial distribution. Non-inferiority was assessed using a one-sided z-test with a predefined non-inferiority margin of −0.10. The null hypothesis of inferiority was rejected when the z-statistic exceeded the critical value of 1.645, corresponding to a one-sided significance level of 0.05. Descriptive statistics were used to summarize response frequencies. Wilcoxon signed-rank test was adopted to assess differences between the two groups in terms of stroma, epithelium, cytoplasm and nuclear rating scale; number of positive and negative differences were compared in case of significance to assess which method performs better. Statistical difference was defined as p < 0.05 and analyses were performed using IBM SPSS Statistics (IBM Corp., Armonk, NY, USA).
3. Results
In the preference analysis, the expert cohort of 13 pathologists evaluated 24 pairs of images, yielding a total of 312 paired assessments. No missing answers were recorded, and all evaluations were performed using high-quality monitors. Overall, the tablet-based staining method was preferred in 120/312 evaluations (38.5%), conventional staining in 118/312 evaluations (37.8%), and no preference was expressed in 74/312 evaluations (23.7%). Statistical analysis demonstrated the non-inferiority of the tablet-based method (z = 2.7). Preference results are summarized in Figure 2. By contrast, preliminary data from the eight volunteer pathologists who completed the pilot test under suboptimal environmental conditions did not demonstrate non-inferiority (standard preference: 83/192, 43%; tabs preference: 54/192, 28.1%; no preference: 27/192, 14.1%; missing data: 28/192, 14.6%; z = 1.43).
Considering the rating scale, Stain Tabs outperformed the standard staining method in terms of stromal evaluation (z = 2.638; p = 0.008) while no statistically significant differences were found for epithelium (z = 0.334; p = 0.738), cytoplasm (z = 1.107; p = 0.268) and nuclei (z = 1.340; p = 0.180). In detail, 106 positive and 67 negative differences were found for stromal rating scale, 92 positive and 89 negative differences for the epithelium, 91 positive and 74 negative differences for the cytoplasm and 97 positive and 82 negative differences for the nuclei. Stromal score 1 (poor quality) was observed in 13/312 (4.2%) tabs-based–stained slides and 16/312 (5.1%) standard-stained slides. Score 2 (intermediate quality) was assigned to 89/312 (28.5%) tabs-based images and 126/312 (40.4%) standard-stained slides. Score 3 (high quality) was recorded more frequently in tabs-based slides (206/312, 66.0%) compared with standard-stained slides (170/312, 54.5%). Stromal data were missing in 4/312 images (1.3%). For the epithelial rating scale, score 1 was reported in 14/312 (4.5%) tabs-based–stained slides versus 20/312 (6.4%) standard-stained slides. Score 2 was assigned in 102/312 (32.7%) tabs-based images and 95/312 (30.5%) standard-stained slides. High-quality epithelial staining (score 3) was observed in 196/312 (62.8%) tabs-based and 197/312 (63.1%) standard-stained slides. Regarding cytoplasmic assessment, score 1 was registered in 17/312 (5.4%) tabs-based–stained slides and 22/312 (7.1%) standard-stained slides. Score 2 was observed in 103/312 (33.0%) tabs-based images and 110/312 (35.3%) standard-stained slides. Score 3 was more frequent in tabs-based slides (191/312, 61.2%) than in standard-stained slides (179/312, 57.4%). Cytoplasmic data was missing in 2/312 images (0.6%). For nuclear staining, score 1 was recorded in 22/312 (7.1%) tabs-based–stained slides compared with 33/312 (10.6%) standard-stained slides. Score 2 was assigned in 103/312 (33.0%) tabs-based images and 102/312 (32.7%) standard-stained slides. High-quality nuclear staining (score 3) was observed in 187/312 (59.9%) tabs-based slides and 176/312 (56.4%) standard-stained slides. Nuclear missing data were identified in 1/312 images (0.3%). Results are summarized in Table 3 and Figure 3.
4. Discussion
H&E staining has been used in histopathology for more than a century and remains essential for the morphological evaluation of normal and pathological tissues. However, staining quality can affect diagnosis, and it mainly relies on hematoxylin and eosin balance. In particular, hematoxylin intensity must be strong enough to highlight nuclear details already at a medium power, while contemporarily avoiding chromatin granularity loss or excessive cytoplasmic and connective tissue staining. Similarly, eosin must be selective enough to demonstrate tissue morphology and various cellular components: not too weak to affect the low power evaluation and not too strong to obscure the color and details of nuclear stain. Despite that, staining techniques suffer from high intra- and inter-laboratory variability, and standardized open-access or widely shared criteria for stain evaluation are still not available. Ultimately, these features and considerations represent critical limitations for standardization and improvement of Digital Pathology.
Nowadays, an increasing number of anatomic pathology departments are adopting Digital Pathology workflows to increase the traceability and control of laboratory phases. That implies the use of traceability systems and slide scanners to obtain WSIs, thus enabling observation by a viewer software on a computer instead of traditional optical light microscopes [15,16,17,18]. In this context, standardization of histopathological techniques (including staining) is pivotal to minimize technical variability and maximize the benefits of digital transformation. In detail, the WSIs adoption opened the door for application of deep learning and machine learning approaches aimed at extracting diagnostic and predictive information from histopathological images [19,20,21]. Interestingly, a quantitative analysis revealed that about 40% of tissue samples from 247 laboratories undertaken by UK NEQAS CPT and National Pathology Imaging Co-operative (NPIC), registered clearly perceptible staining differences; notably, this percentage could be even higher in laboratories that do not undergo voluntary H&E quality control. Considering these data and the possibility that image analysis performance may be affected by staining variability, several studies have investigated the potential for digital standardization of H&E-stained tissue slides; based on that, standardization tools are commercially available [7,8]. Similarly, other authors developed a deep-learning-based virtual staining, directly on unstained slides or fresh (not formalin-fixed) tissues. Limitations of these approaches mainly lie in the reliance on the ground truth identification and scanner adoption; in fact, most of these models are trained and tested by slides, staining reagents, and digital scanners from a limited number of centers, therefore being unable to capture the real-world variability. Thus, real-life feasibility and reproducibility of these techniques should still be demonstrated [11,12,13,22,23,24].
In our study, we developed a survey for the histopathological evaluation of an innovative tabs-based H&E staining method. The new product consists of one eosin and one hematoxylin tab which must be diluted in distilled water. In contrast with digital staining, the new method represents a chemical stain based on affinity between acids and bases, therefore not affected by ground-truth-related limitations inherent to virtual staining approaches; this staining technique was developed to limit the risk of decay that affects all pre-diluted solutions, and to increase intra and interlaboratory reproducibility. Since there are no validated and open-access criteria for the adequacy assessment of H&E tissue stains, we evaluated the non-inferiority of the new staining method via a user-friendly on-line form that has been distributed to a selected group of expert pathologists. The form was designed to capture the synthesis of several described parameters in few questions. Importantly, in all cases the staining was adequate for a histopathological diagnosis and statistical analysis demonstrated non-inferiority of the new staining technique (z = 2.7). In detail, no preference (74/312; 23.7%) and Stain Tabs preference (120/312; 38.5%) were registered in 194/312 answers (62.2%), while standard stain preference was observed in 118/312 (37.8%) cases. Moreover, the new stain method outperformed conventional staining in terms of stromal rating scale (z = 2.638; p = 0.008). This result is probably due to the paler hematoxylin stain which enhances the stromal component, while not compromising nuclear evaluation and making nucleoli and mitoses more easily visible. In fact, the tabs-based method obtained a higher number of nuclei scores 2 and 3 and a lower number of scores 1 compared with the standard method, globally ensuring excellent and good stains in most cases, in face of a low number of poor-quality stains (Figure 4).
In addition, our data highlight the potential impact of dedicated equipment (in particular, monitor quality) and environmental context on the WSIs evaluation. In fact, it was possible to demonstrate non-inferiority only by the expert cohort that completed the survey in optimal environmental setting, using high-quality monitors, in contrast to the initial pilot analysis in suboptimal conditions. These findings emphasize the importance of monitor quality as an analytical variable in Digital Pathology [25,26].
The limitations of our study lie primarily in the incomplete representation of tissues; for example, the survey did not include tissues from the lung, bladder, lymph nodes, bone, and central nervous system. Additionally, all specimens were collected and stained at a single institution, precluding assessment of interlaboratory variability. Nevertheless, these findings provide a pivotal foundation for future investigations using the same described approach, with broader inclusion of tissue types and samples from multiple centers.
Nevertheless, to the best of our knowledge, this is the first attempt to develop a Digital Pathology-based platform for H&E quality assessment. Our survey proposed a compromise between a detailed and user-friendly evaluation, avoiding a huge number of specific questions for each single image, and considering the judgment of a selected group of expert pathologists. The value of our results is reinforced by the strict selection of the users: all highly experienced and respected Italian pathologists.
5. Conclusions
Given the lack of widely accepted standards for assessing H&E staining adequacy, we developed a user-friendly digital survey to evaluate the non-inferiority of a tablet-based H&E staining method. Our results demonstrated the non-inferiority of this method compared with conventional staining and showed particularly favourable performance in the assessment of stromal components.
In view of the increasing need for standardization in anatomic pathology departments, the development and dissemination of shared criteria for evaluating H&E-stained tissue sections should be strongly encouraged. H&E staining quality, monitor characteristics, and environmental conditions should be regarded as relevant pre-analytical and analytical variables in digital pathology. Careful control of these parameters may reduce intra- and inter-laboratory variability and further improve the effectiveness of digital pathology workflows and image analysis algorithms in routine clinical practice.
Author Contributions
Conceptualization, G.P., L.N. and A.C.; methodology, G.P., L.N., M.D. and R.V.; software, L.N., E.I., E.M., V.V. A.C.; validation, C. B., B. C., G.C., V.L., A. E., G.N. F., A. G., L.M., G. I., S. M., F. M., P. P., L. R., S. U., and M. V.; formal analysis, L.N., E.I.; investigation, L.N.; resources, supervision, and project administration G.P.; data curation and writing—original draft preparation, L.N.; writing—review and editing, L.N., S.M., A.G., B.C., and A.C.; visualization, L.N. All authors have read and agreed to the published version of the manuscript.
Funding
Diapath provided the H&E Stain Tabs used in this study free of charge. The company had no role in study design, data collection, data analysis, interpretation of results, manuscript preparation, or the decision to submit the manuscript for publication.
Institutional Review Board Statement
This study used archival formalin-fixed paraffin-embedded tissue specimens obtained from routine diagnostic practice. All samples were anonymized before digitization and survey preparation, and no patient-identifying information was included in the study dataset. According to local institutional policy, studies based exclusively on fully anonymized archival diagnostic material and not affecting patient management do not require formal Ethics Committee approval. The study was conducted in accordance with applicable institutional and national regulations.
Informed Consent Statement
Not applicable.
Data Availability Statement
The aggregated data supporting the findings of this study are available from the corresponding author upon reasonable request. Individual reader-level data are not publicly available in order to protect participant confidentiality.
Acknowledgments
Special thanks to Irene Amat, Alessandro Cioce, Adrian Dumitru, Constanze Nemes, Carolina Padrao, Ebru Sener, Eric Walk who volunteered their time and energy to conduct a mock survey during the 37th European Congress of Pathology (ECP).
Conflicts of Interest
The study evaluated a staining product. The authors declare that they have no personal financial relationships, honoraria, employment, stock ownership, patents, or other competing interests related to the product evaluated in this study.
References
- Tissue Diagnostics Market, Forecast 2022, Size, share and Trends. 6 Jan 2026. Available online: https://store.frost.com/global-tissue-diagnostics-market-forecast-to-2022.html.
- Dunn, C.; Brettle, D.; Hodgson, C.; Hughes, R.; Treanor, D. An international study of stain variability in histopathology using qualitative and quantitative analysis. J. Pathol. Inform. 2025, 17, 100423. [Google Scholar] [CrossRef] [PubMed]
- Wick, M.R. The hematoxylin and eosin stain in anatomic pathology—An often-neglected focus of quality assurance in the laboratory. Semin Diagn. Pathol. 2019, 36, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Lillie, R.D.; Fullmer, H.M. Histopathologic technic and practical histochemistry, 4th edn; McGraw Hill Book Company: New York, 1976. [Google Scholar]
- College of American Pathologists. H&E Troubleshooting Guide. In CAP H&E Troubleshooting Guide; Available online; CAP: Northfield, IL, USA, 2026; (accessed on 21 May 2026). [Google Scholar]
- Haematoxylin; Eosin. Muscle Histochemistry Staining Criteria Handbook Edition 004 Index Haematoxylin and Eosin Assessment Criteria 3 Special Stains Assessment Criteria 6 Assessment Criteria Definitions 23.
- Salvi, M.; Caputo, A.; Balmativola, D.; Scotto, M.; Pennisi, O.; Michielli, N.; et al. Impact of Stain Normalization on Pathologist Assessment of Prostate Cancer: A Comparative Study. In Cancers (Basel); 2023. [Google Scholar] [CrossRef]
- Cazzaniga, G.; Caputo, A.; L’Imperio, V.; Gibilisco, F.; Scotto, M.; Pennisi, O.M.A.; et al. Not all stains are made equal: impact of stain normalization on prostate cancer diagnosis. Pathologica 2024, 116, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Rana, A.; Lowe, A.; Lithgow, M.; Horback, K.; Janovitz, T.; Da Silva, A.; et al. Use of Deep Learning to Develop and Analyze Computational Hematoxylin and Eosin Staining of Prostate Core Biopsy Images for Tumor Diagnosis. JAMA Netw. Open 2020, 3. [Google Scholar] [CrossRef] [PubMed]
- Iwuajoku, V.; Ekici, K.; Haas, A.; Khan, M.Z.; Kazemi, A.; Kasajima, A.; et al. An equivalency and efficiency study for one year digital pathology for clinical routine diagnostics in an accredited tertiary academic center. Virchows Arch. 2025, 2025 487:1, 487: 3–12. [Google Scholar] [CrossRef] [PubMed]
- Rivenson, Y.; Wang, H.; Wei, Z.; de Haan, K.; Zhang, Y.; Wu, Y.; et al. Virtual histological staining of unlabelled tissue-autofluorescence images via deep learning. Nat. BioMed Eng. 2019, 3, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Bayramoglu, N.; Kaakinen, M.; Eklund, L.; Heikkilä, J. Towards Virtual H&E Staining of Hyperspectral Lung Histology Images Using Conditional Generative Adversarial Networks. Proceedings - 2017 IEEE International Conference on Computer Vision Workshops, ICCVW 2017, 2018;2018-January; pp. 64–71. [Google Scholar] [CrossRef]
- Lahiani, A.; Gildenblat, J.; Klaman, I.; Albarqouni, S.; Navab, N.; Klaiman, E. Virtualization of Tissue Staining in Digital Pathology Using an Unsupervised Deep Learning Approach. In Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); 2019; Volume 11435 LNCS, pp. 47–55. [Google Scholar] [CrossRef]
- Ji, X.; Salmon, R.; Mulliqi, N.; Khan, U.; Wang, Y.; Blilie, A.; et al. Physical Color Calibration of Digital Pathology Scanners for Robust Artificial Intelligence–Assisted Cancer Diagnosis. Mod. Pathol. 2025, 38, 100715. [Google Scholar] [CrossRef] [PubMed]
- Eloy, C.; Fraggetta, F.; van Diest, P.J.; Polónia, A.; Curado, M.; Temprana-Salvador, J.; et al. Digital transformation of pathology - the European Society of Pathology expert opinion paper. Virchows Arch. 2025, 2025 487 487, 5 971–981. [Google Scholar] [CrossRef] [PubMed]
- Fraggetta, F.; Garozzo, S.; Zannoni, G.; Pantanowitz, L.; Rossi, E. Routine Digital Pathology Workflow: The Catania Experience. J. Pathol. Inform. 2017, 8, 51. [Google Scholar] [CrossRef]
- Eccher, A.; Fabbri, V.P.; L’Imperio, V.; Die Tos, A.P.; Pagni, F.; Dominici, M. Pathology Laboratory Archive at the University and Hospital Trust of Modena/UNIMORE: “Disaster Recovery” frame by frame. Pathologica-Journal of the Italian Society of Anatomic Pathology and Diagnostic Cytopathology 2025, 117, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Eccher, A.; Marletta, S.; Sbaraglia, M.; Guerriero, A.; Rossi, M.; Gambaro, G.; et al. Digital pathology structure and deployment in Veneto: a proof-of-concept study. 2024, 485, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Nibid, L.; Greco, C.; Cordelli, E.; Sabarese, G.; Fiore, M.; Liu, C.Z.; et al. Deep pathomics: A new image-based tool for predicting response to treatment in stage III non-small cell lung cancer. PLoS ONE 2023, 18. [Google Scholar] [CrossRef] [PubMed]
- Rakaee, M.; Tafavvoghi, M.; Ricciuti, B.; Alessi, J. V.; Cortellini, A.; Citarella, F.; et al. Deep Learning Model for Predicting Immunotherapy Response in Advanced Non−Small Cell Lung Cancer. JAMA Oncol. 2025, 11, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Bülow, R.D.; Hölscher, D.L.; Costa, I.G.; Boor, P. Extending the landscape of omics technologies by pathomics. npj Syst. Biol. Appl. 2023 2023, 9, 1 38. [Google Scholar] [CrossRef] [PubMed]
- Koivukoski, S.; Khan, U.; Ruusuvuori, P.; Latonen, L. Unstained Tissue Imaging and Virtual Hematoxylin and Eosin Staining of Histologic Whole Slide Images. Lab. Investig. 2023, 103. [Google Scholar] [CrossRef] [PubMed]
- Fereidouni, F.; Todd, A.; Li, Y.; Chang, C.-W.; Luong, K.; Rosenberg, A.; et al. Dual-mode emission and transmission microscopy for virtual histochemistry using hematoxylin- and eosin-stained tissue sections. BioMed Opt. Express 2019, 10, 6516. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.J.; Azizgolshani, N.; Andersen, M.J.; Suriawinata, A.; Liu, X.; Lisovsky, M.; et al. A large-scale internal validation study of unsupervised virtual trichrome staining technologies on nonalcoholic steatohepatitis liver biopsies. Mod. Pathol. 2021, 34, 808–822. [Google Scholar] [CrossRef] [PubMed]
- Cazzaniga, G.; Mascadri, F.; Marletta, S.; Caputo, A.; Guidi, G.; Gambaro, G.; et al. Benchmarking digital displays (monitors) for histological diagnoses: the nephropathology use case. J. Clin. Pathol. 2025, 78, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Marletta, S.; Caputo, A.; Guidi, G.; Pantanowitz, L.; Pagni, F.; Bavieri, I.; et al. Digital Pathology Displays Under Pressure: Benchmarking Performance Across Market Grades. J. Imaging Inform. Med. 2025, 38, 4090–4099. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Cohort selection and tissue-sample workflow. 50 FFPE tissue slides were sectioned in duplicate, 50 stained conventionally and 50 by the stain-tabs. All 100 slides obtained were revised and, based on tissue sample variability, 14 pairs of slides were selected to obtain 24 image pairs at different magnification levels. Therefore, 48 images were adopted to conduct a blind survey.
Figure 1.
Cohort selection and tissue-sample workflow. 50 FFPE tissue slides were sectioned in duplicate, 50 stained conventionally and 50 by the stain-tabs. All 100 slides obtained were revised and, based on tissue sample variability, 14 pairs of slides were selected to obtain 24 image pairs at different magnification levels. Therefore, 48 images were adopted to conduct a blind survey.

Figure 2.
Histogram representing preferences evaluation among standard (violet), and new tabs-based tissue staining (blue). The gray column represents the number of cases in which no preference between the two methods was registered.
Figure 2.
Histogram representing preferences evaluation among standard (violet), and new tabs-based tissue staining (blue). The gray column represents the number of cases in which no preference between the two methods was registered.

Figure 3.
Comparison of stroma (A), epithelium (B), cytoplasm (C) and nuclear (D) rating scale among tabs-based and standard staining method. Red columns represent negative differences while blue columns represent positive differences between tabs-based and standard stains. The Wilcoxon signed-rank test revealed a statistically significant difference between the two methods in terms of stromal (A) rating (z = 2.638; p = 0.008) highlighting a predominance of positive ranks (106) over negatives (67).
Figure 3.
Comparison of stroma (A), epithelium (B), cytoplasm (C) and nuclear (D) rating scale among tabs-based and standard staining method. Red columns represent negative differences while blue columns represent positive differences between tabs-based and standard stains. The Wilcoxon signed-rank test revealed a statistically significant difference between the two methods in terms of stromal (A) rating (z = 2.638; p = 0.008) highlighting a predominance of positive ranks (106) over negatives (67).

Figure 4.
H&E images from pleura (A, B; 40x magnification), lobular carcinoma of the breast (C, D; detail from 20x magnification) and basal cell carcinoma (E, F; 5x magnification). Slides in A, C and E were stained conventionally whereas images in B, D, and F were stained by tabs. Note the nuclei and nucleoli definition in B, D and the higher contrast between epithelium and stroma in F.
Figure 4.
H&E images from pleura (A, B; 40x magnification), lobular carcinoma of the breast (C, D; detail from 20x magnification) and basal cell carcinoma (E, F; 5x magnification). Slides in A, C and E were stained conventionally whereas images in B, D, and F were stained by tabs. Note the nuclei and nucleoli definition in B, D and the higher contrast between epithelium and stroma in F.


Table 1.
Tissues and magnification levels adopted in the survey.
| N. picture | Tissue | Pathology | Magnification |
| 1 | Skin | Actinic keratosis | 10x |
| 2 | Skin | Basal Cell Carcinoma | 5x |
| 20x | |||
| 40x | |||
| 3 | Skin | Dyskeratoma | 20x |
| 40x | |||
| 4 | Prostate | Normal and prostate cancer | 5x |
| 10x | |||
| 20x | |||
| 20x | |||
| 40x | |||
| 5 | Uterus | Leiomyoma | 10x |
| 6 | Uterus | Adenomyosis | 20x |
| 7 | Fallopian tubes | Normal | 20x |
| 8 | Breast | Lobular carcinoma | 20x |
| 9 | Breast | Apocrine metaplasia | 10x |
| 10 | Kidney | Normal and chromophobe renal cell carcinoma | 20x |
| 10x | |||
| 11 | Pleura | Pleural effusion | 20x |
| 40x | |||
| 12 | Gallbladder | Cholecystitis | 10x |
| 50x | |||
| 13 | Colon | Tubular adenoma | 40x |
| 14 | Colon | Mesenteric panniculitis | 20x |
Table 2.
High quality screens adopted by the cohort of expert Italian pathologists.
| Monitor | Inches | Resolution (Pixel) | N. users |
| LG 32HL512D | 32 | 3840 × 2160 | 7 |
| DELL U3223QE | 32 | 3840 × 2160 | 3 |
| Barco MDPC-8127 | 27 | 3840 × 2160 | 1 |
| Apple Studio Display | 27 | 5120 × 2880 | 1 |
| Samsung QLED 4K Ultra HD Q7F | 75 | 3840 × 2160 | 1 |
Table 3.
Distribution of histological quality scores by tissue compartment.
| Stroma | Epithelium | Cytoplasm | Nuclei | |||||
|
TABS n (%) |
Standard n (%) |
TABS n (%) |
Standard n (%) |
TABS n (%) |
Standard n (%) |
TABS n (%) |
Standard n (%) |
|
| 1 | 13 (4.2) | 16 (5.1) | 14 (4.5) | 20 (6.4) | 17 (5.4) | 22 (7.1) | 22 (7.1) | 33 (10.6) |
| 2 | 89 (28.5) | 126 (40.4) | 102 (32.7) | 95 (30.5) | 103 (33.0) | 110 (35.3) | 103 (33.0) | 102 (32.7) |
| 3 | 206 (66.0) | 170 (54.5) | 196 (62.8) | 197 (63.1) | 191 (61.2) | 179 (57.4) | 187 (59.9) | 176 (56.4) |
| Missing | 4 (1.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.3) | 1 (0.3) | 0 (0.0) | 1 (0.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



