Submitted:
01 June 2026
Posted:
02 June 2026
You are already at the latest version
Abstract
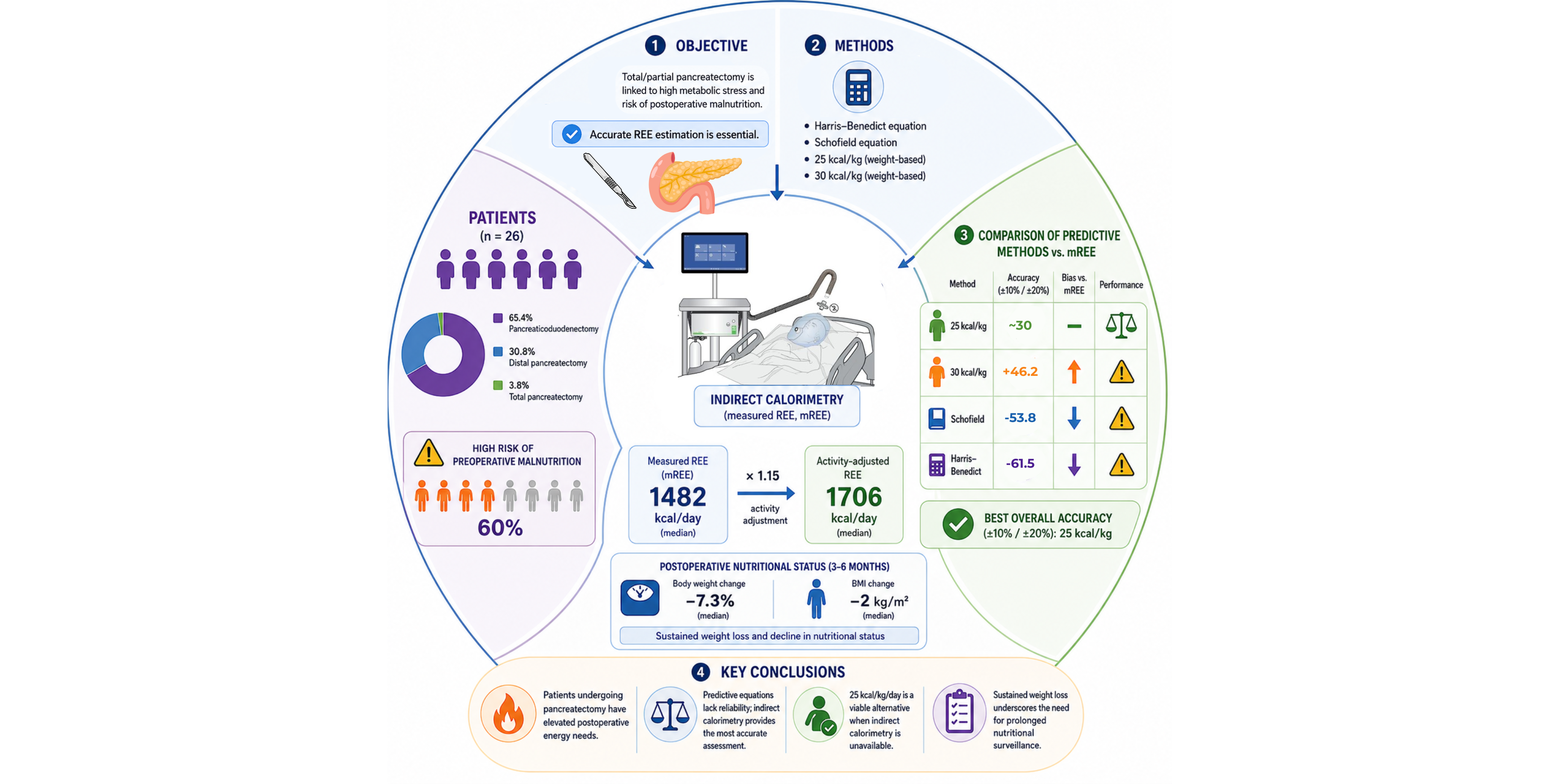
Background/Objectives: Total or partial pancreatectomy is associated with significant metabolic stress and high risk of postoperative malnutrition. Accurate estimation of resting energy expenditure (REE) is essential, as predictive equations may not reflect true energy needs. Methods: A prospective study among patients undergoing total or partial pancreatectomy for pancreatic tumors was conducted. REE was measured by indirect calorimetry (mREE) and compared with the Harris–Benedict and Schofield equations and the weight-based approaches (25 and 30 kcal/kg). Agreement was assessed using linear regression and Bland–Altman analysis, accuracy indices included ±10%, ±20%, Mean Absolute Percentage Error (MAPE) and Root Mean Square Error (RMSE). Results: In 26 patients (mean age, 66.7±8.7 years; 53.8% male) undergoing pancreatic resection (17 pancreaticoduodenectomies, 8 distal pancreatectomies, 1 total pancreatectomy), 60% were at preoperative malnutrition risk. Median measured REE was 1482 kcal/day, rising to 1706 kcal/day after activity adjustment (×1.15) within 14 postoperative days. At 3-6 months postoperatively, patients demonstrated significant declines in nutritional status with a median body weight reduction of −7.3% and a decrease in BMI of −2 kg/m2. The 30 kcal/kg method showed the lowest accuracy (MAPE 23.2%, RMSE 417 kcal/day) and overestimated energy needs. Harris–Benedict underestimated mREE in 61.5% of cases, while the 25 kcal/kg approach showed more balanced performance. Conclusions: Patients undergoing pancreatic resection exhibit elevated postoperative energy demands. Predictive equations lack reliability, favoring indirect calorimetry for precision. Sustained weight loss underscores the need for prolonged nutritional surveillance.
Keywords:
pancreatectomy
; pancreaticoduodenectomy
; Whipple procedure
; indirect calorimetry
; resting energy expenditure
1. Introduction
Pancreatectomy is divided into two major types: partial and total pancreatectomy. Total pancreatectomy leads to complete loss of the endocrine and exocrine function of the pancreas, with significant difficulties in maintaining blood glucose control [1]. Contrarily, partial pancreatectomy preserves the endocrine and exocrine functions of the pancreas and allows better control of glucose levels compared to total pancreatectomy. Therefore, partial pancreatectomy is generally the preferred surgical option, excluding cases of advanced cancer, pancreatic metastases or chronic pancreatitis [2,3].
Partial pancreatectomy is classified into two major subtypes, pancreatoduodenectomy (Whipple procedure) and distal pancreatectomy. The Whipple procedure is the standard surgery for tumors in the head of the pancreas [4]. This procedure has been shown to be effective in treating malignant and some benign conditions, but it causes major changes in the digestive system. Therefore, postoperative nutritional support is essential for patients’ recovery and overall health [4].
Most of the patients will develop malnutrition due to pancreatic insufficiency, impaired digestion and malabsorption after pancreaticoduodenectomy or total pancreatectomy and they will have higher risk of postoperative complications [5,6]. Although there are no specific guidelines for the nutritional management of these patients, the general European Society for Clinical Nutrition and Metabolism (ESPEN) recommendations for cancer patients suggest an energy intake of 25–30 kcal/kg BW/day and a protein intake of 1.0–1.5 g/kg BW/day.
Surgical stress and the postoperative inflammatory response increase measured energy expenditure (mREE), which requires nutritional support for adequate healing and functional recovery, especially when the patient is malnourished and the inflammatory response is prolonged [7]. Although most studies demonstrate that surgical patients enter a hypermetabolic state [8], data on energy metabolism following pancreatectomy remain limited. A previous study examined the association between the Whipple procedure and mREE; however, the small sample size (12 patients) did not draw clear conclusions, highlighting the need for further research in larger populations [8].
Nutritional support following pancreatectomy is a cornerstone of postoperative care, as patients are at high risk of malnutrition due to reduced oral intake, exocrine and endocrine pancreatic insufficiency, metabolic disturbances and increased energy requirements [9,10]. The primary aims of nutritional intervention are to meet energy and protein needs adequately, prevent or mitigate weight and skeletal muscle loss, promote recovery, reduce postoperative complications and improve overall quality of life.
However, the postoperative nutritional management of patients undergoing pancreatectomy varies considerably worldwide, despite its importance. Evidence suggests that less than two thirds of clinical units follow local feeding protocols [9], leading to inconsistencies in care, suboptimal nutritional interventions, delayed recovery and increased risk of complications. Thus, a comprehensive nutritional assessment and energy needs evaluation with systematic and ongoing monitoring is essential to optimize patient outcomes. Standardized evidence-based protocols for nutritional support, when developed and implemented, may standardize clinical practice, improve prognosis, reduce postoperative morbidity and provide the best possible quality of life for patients after total or partial pancreatectomy.
This study aimed to determine the mREE of patients undergoing total or partial pancreatectomy using indirect calorimetry and to conduct a comparative evaluation of mREE using commonly used estimation equations or simplified approaches for calculating energy requirements.
2. Materials and Methods
2.1. Ethical Approval
Data were collected from subjects enrolled between May 2025 and February 2026 at the Surgery Unit of Evangelismos General Hospital of Athens. It was approved by the Institutional Review Board of Evangelismos Hospital of Athens (Approval No. 484, 2025) and the Ethics Committee of the Aristotle University of Thessaloniki (Protocol No. 126/2025) and was conducted in accordance with the ethical principles of the Declaration of Helsinki. The patients were informed about the purpose of the study and consent forms were signed.
2.2. Study Population
Inclusion criteria included patients over the age of 18 undergoing total or partial pancreatectomy for pancreatic tumors. Exclusion criteria included age <18 years, pregnancy and inability to breathe into the indirect calorimetry mask for the duration required for the measurement.
2.3. Study Design
This was a prospective observational study. mREE was determined by a clinical dietitian using the Cosmed Q-NRG+ portable indirect calorimetry system. The measurement was performed using a canopy; in cases where this is not feasible, a face mask is used to enable the recording of VO₂ and VCO₂ [11]. Measurements are conducted up to 14 days postoperatively, in the morning at rest, following an 8–10-hour fast; they last approximately 10 minutes and are performed at a controlled room temperature, in accordance with the ESPEN guidelines for measuring REE.
Anthropometric measurements included body weight, which were recorded using a calibrated electronic scale, Tanita RD-953, to the nearest 0.1 kg, in accordance with standardized procedures. Body weight was measured at 3 time points: during preoperative evaluation, at discharge and 3–6 months after discharge. BMI at all 3 time points was calculated as the quotient of body weight in kilograms divided by the square of height in meters (kg/m²) [12]. For height measurement, patients removed any hats and footwear and had their hair unstyled. Patients were asked to stand upright with relaxed hands, pressing their whole foot against the base and resting their heels against the back. Attention was paid to the alignment of the patient’s head using the Frankfort method so that their eyes were level with their upper earlobes without leaning back. The height was measured by lowering the sliding plate to reach the top of the patient’s head. Additionally, the percentage of body weight loss over the last 3 and 6 months was recorded. Five patients could not be detected 3–6 months after discharge.
Biochemical parameters were determined using blood samples collected by the hospital laboratory before and after the mREE measurement and include the measurement of C-reactive protein (CRP) and serum proteins (albumin). The analyses were performed in accordance with the hospital’s established standard procedures.
Clinical data were collected from patients’ medical records and include postoperative complications, length of hospital stay and any readmissions. Prior to surgery, all patients underwent a nutritional risk assessment using the Perioperative Nutrition Screen (PONS) [13], a weighted tool based on four main areas: recent weight loss, reduced food intake or the presence of anorexia, low BMI and the presence of an underlying disease with high metabolic risk.
2.4. Primary and Secondary Outcomes
The main outcomes of the study included mREE, as determined by indirect calorimetry, as well as the percentage of patients’ energy needs met in relation to both the measured mREE and current guidelines.
mREE was calculated from the VO₂ and VCO₂ values using the Weir equation [14]: mREE = (3.94 × VO₂ + 1.11 × VCO₂) × 1.44. The respiratory quotient (RQ) was calculated as the ratio of VCO₂ to VO₂. Subsequently, mREE was compared with estimated predicted resting energy expenditure (pREE) values, which were calculated using the Harris–Benedict [15] and Schofield [16] equations.
The Harris-Benedict equation was applied as follows: for men, pREE = 66.47 + 13.75 × weight (kg) + 5.0 × height (cm) - 6.75 × age (years) and for women pREE = 665.09 + 9.56 × weight (kg) + 1.84 × height (cm) - 4.67 × age (years). The Schofield equation was calculated based on gender and age group: for men aged 30–59, pREE = 11.472 × weight (kg) + 873.1 and for those aged 60 and older, pREE = 11.711 × weight (kg) + 587.7, while for women aged 30–59, pREE = 8.126 × weight (kg) + 845.6 and for those aged 60 and older, pREE = 9.082 × weight (kg) + 658.5. For the calculation, ideal weight was used for overweight patients and corrected weight [Corrected Weight = Ideal Body Weight + 0.25 x (Actual Weight - Ideal Body Weight)] for obese patients. In addition, a comparison was made of total energy requirements, as estimated by mREE adjusted with an activity/stress factor of 1.15 (mREE x 1.15), with the body weight-based equations proposed by the ESPEN guidelines. Ideal body weight was used for the calculation, adjusted based on BMI, using a BMI value of 22 kg/m² for overweight patients and 24.9 kg/m² for obese patients. Comparisons were made between mREE x 1.15 and 25 kcal/kg of ideal body weight, as well as between mREE x 1.15 and 30 kcal/kg of ideal body weight.
Secondary outcomes included length of hospital stay and the incidence of postoperative complications. In addition, the association between mREE and selected biochemical markers of nutritional status and inflammation was evaluated. The relationship between PONS score, mREE and clinical outcomes was also analyzed.
2.5. Statistical Analysis
Statistical analysis was conducted using Jamovi version 2.7.15. All (two-tailed) statistical analyses were conducted with a significance level of α = 0.05, and the null hypothesis rejected.
Continuous variables with normal distribution are presented as mean (± standard deviation) and continuous variables with non-normal distribution as median (interquartile range). Qualitative variables are expressed as n and relative frequency [n (%)]. The distribution normality of all variables was assessed using the Shapiro-Wilk test. For quantitative variables in three groups, Repeated Measures ANOVA was used for variables with normal distribution and Friedman’s test was used for variables without normal distribution.
To further explore the relationship between body weight of patients and mREE, adjusting for other confounding factors, multiple linear regression models were developed. Bland-Altman analysis was performed to evaluate the agreement between the two measurement methods to provide information on the systematic bias and limits of agreement.
Finally, an additional accuracy analysis was conducted by calculating the percentage error for each equation using the formula: % Error = (pREE - mREE)/mREE × 100. The estimates were classified as underestimation (<10%), accuracy (±10), or overestimation (>10%). The percentage of patients in each category was calculated, along with overall error metrics such as Root Mean Square Error (RMSE) and Mean Absolute Percentage Error (MAPE). These metrics give a quantitative measure of the clinical accuracy of the equations, and enable a more direct comparison of their performance.
3. Results
The total study sample consisted of 26 patients, 46.2% of whom were women, with a mean age of 66.7 ± 8.78 years. The most common site of pancreatic cancer was the head of the pancreas (50.0%), followed by the body of the pancreas (15.4%), unspecified pancreatic tumor location (15.4%), the ampulla of Vater (7.7%), Intraductal Papillary Mucinous Neoplasm (IPMN) (7.7%) and the tail of the pancreas (3.8%). The majority of patients underwent a Whipple procedure (65.4%), while a partial pancreatectomy was performed in 30.8% and a total pancreatectomy in 3.8%. The following tables present the patients’ anthropometric and clinical characteristics.

Table 1.
Descriptive characteristics of patients after total or partial pancreatectomy1.
| Variable | n=26 |
| Gender (women, n, %) | 12 (46.2%) |
| Age (years) | 66.7 (±8.78) |
| Pancreatic cancer site (n, %) | |
| Ampulla of Vater | 2 (7.7%) |
| Body | 4 (15.4%) |
| Head | 13 (50.0%) |
| Tail | 1 (3.8%) |
| IPMN | 2 (7.7%) |
| Unspecified | 4 (15.4%) |
| Type of surgical procedure (n, %) | |
| Whipple procedure | 17 (65.4%) |
| Distal pancreatectomy | 8 (30.8%) |
| Total pancreatectomy | 1 (3.8%) |
| Comorbidities (n, %) | 23 (88.5%) |
| Preoperative diabetes mellitus (n, %) | 11 (42.3%) |
| Positive PONS (n, %) | 16 (61.5%) |
| Length of hospital stay (days) | 22 (17.8) |
| Incidence of complications (n, %) | 4 (15.3%) |
| 3-month mortality (n, %) | 1 (3.8%) |
1The values correspond to the mean (± standard deviation) or median (interquartile range) for continuous variables with normal and non-normal distributions, respectively. The values correspond to absolute numbers (%) for categorical variables. Abbreviations: IPMN = Intraductal Papillary Mucinous Neoplasm, PONS = Perioperative Nutrition Screen.
Table 2.
Nutritional assessment and laboratory parameters of patients1.
| Variable | Preoperatively | At Discharge | 3–6 months after discharge | within groups p-value |
| Body weight (kg) | 72.3 (16.5) | 68.0 (18.9) | 67 (15.0) (n=21) | <0.001* |
| BMI (kg/m2) | 25.5 (5.17) | 24.6 (5.85) | 23.5 (5.63) (n=21) | <0.001* |
| Albumin (g/dl) | 3.90 (0.75) | 3.10 (0.67) | - | <0.001* |
| C-reactive protein (mg/dL) | 7.80 (3.45) | 5.86 (4.56) | - | <0.001* |
1The values correspond to the median (interquartile range) for continuous variables with a non-normal distribution. *Indicates a statistically significant difference between the measurements using Friedman’s test. Abbreviations: BMI = Body Mass Index.
Table 3.
Measured energy consumption and estimated energy consumption of patients1.
| Variable | n=26 |
| mREE (kcal/day) | 1484 (444) |
| RQ | 0.70 (0.05) |
| Harris-Benedict (kcal/day) | 1268 (90) |
| Schofield (kcal/day) | 1268 (122) |
| mREE x 1.15 (kcal/day) | 1706 (510) |
| 25 kcal/kg x ideal body weight | 1608 (223) |
| 30kcal/kg x ideal body weight | 1929 (269) |
1The values correspond to the median (interquartile range) for continuous variables with a non-normal distribution. Abbreviations: mREE = Measured Resting Energy Expenditure, RQ = Respiratory Quotient.
The linear regression analysis showed that the mREE differed significantly from the Harris–Benedict equation (p-value = 0.03) but not from the Schofield equation (p-value = 0.60) and it also differed significantly from estimates based on 25 kcal/kg and 30 kcal/kg of ideal body weight (p-value = 0.04 for both comparisons) (Figure 1).
The Bland-Altman plots showed wide limits of agreement between mREE and all estimated methods, suggesting significant clinical inconsistency at the individual level. Specifically, for the Harris-Benedict equation, the mean difference was (MD = 175 kcal), with relatively symmetrical but wide limits of agreement (-649.7 to 565.5 kcal) and an indication of proportional bias (p-value = 0.008). Similarly, the Schofield equation showed a slightly smaller mean difference compared to the previous equation (MD = 118 kcal) and wide but also larger limits of agreement (-828.8 to 567.2 kcal), without statistically significant proportional bias (p-value = 0.10). In contrast, methods based on mREE × 1.15 combined with 25 or 30 kcal/kg of ideal body weight showed greater dispersion and clinically significant deviation, particularly the 30 kcal/kg approach, where significant proportional bias was observed (p-value = 0.009), with the deviation increasing as the mean values increase. Overall, the wide limits of agreement across all methods demonstrate limited accuracy and interchangeability with mREE (Figure 2).
The analysis presented in Table 4 compared pREE with mREE in 26 patients. Among the resting equations, the Harris-Benedict equation showed the lowest total deviation (RMSE 350 kcal) but the highest percentage of underestimations <10% of mREE (61.5%) and the Schofield equation also showed a high percentage of underestimations <10% of mREE (53.8%). When the body weight-based equations were compared to the adjusted energy requirements (mREE × 1.15), the 25 kcal/kg equation showed moderate accuracy (30.8% within ±10% and 34.6% less than or greater than 10%, RMSE 369 kcal), while the 30 kcal/kg equation showed greater deviation (MAPE 23.2%, RMSE 417 kcal) and lower clinical accuracy, suggesting a tendency to overestimate energy requirements.
Multiple linear regression showed that the model explained 65% of the variance in mREE. Among the variables included in the model (age, sex, CRP, albumin), body weight is an independent predictor of mREE in every model and for every 1 kg increase in body weight, mREE increases by 8.01 kcal (95% CI: 1.39–14.6, p-value = 0.020) (Table 5).
Figure 3 and Figure 4 illustrate the changes in patients’ body weight and BMI from the preoperative period to hospital discharge and the 3–6-month postoperative follow-up. A statistically significant reduction in both body weight and BMI was observed over time (p = 0.001). More specifically, body weight decreased significantly by the time of discharge and continued to decline further during the 3–6 months following discharge. A similar pattern was observed for BMI. Pairwise comparisons demonstrated significant differences both between the preoperative period and discharge and between the preoperative period and the 3–6-month follow-up. These findings indicate that the surgical intervention was associated with progressive postoperative weight loss during the first months after surgery.
4. Discussion
Most patients who undergo total or partial pancreatectomy become malnourished due to pancreatic insufficiency, impaired digestion and malabsorption, thereby increasing the risk of postoperative complications [5,6]. The aim of this study was to determine mREE in patients undergoing total or partial pancreatectomy, as well as to conduct a comparative assessment of their energy requirements and clinical outcomes. The results showed that mREE amounts to 1482 kcal/day, while with an activity factor of mREE × 1.15, it amounts to 1700 kcal/day up to 14 days postoperatively, with the estimation equations showing significant deviations from mREE, while significant postoperative weight loss and a reduction in BMI were also recorded during the first 3–6 months. The patients’ RQ was 0.70 ± 0.09, suggesting greater lipid utilization, mobilization of fat stores and consequent weight loss during hospitalization.
Hypermetabolism is defined as an increase in REE [17]. When evaluated in relation to cancer type, some studies have observed normal REE levels in patients with breast cancer, melanoma, gastric cancer, or rectal cancer [18], while a hypermetabolic state has been observed in patients with pancreatic cancer [8,19].
In contrast, the Harris-Benedict and Schofield equations often show significant deviations from mREE, a finding that has been confirmed in multiple studies involving oncology and surgical patients. In five studies, the results showed that the predictive equations underestimated the mREE of cancer patients and in three studies, the mREE was overestimated by the predictive equations [20]. In a study with a design similar to the present study, involving 12 patients who underwent the Whipple procedure, the mREE before surgery was 1198 kcal/day and 22.4 kcal/kg/day, while the pREE estimated using the Harris–Benedict equation was 1174 kcal/day and 21.7 kcal/kg/day. Energy expenditure appeared to increase postoperatively, reaching up to 25.4 kcal/kg/day within 14 days after surgery [8]. However, this study did not compare the same predictive equations used in the present study, nor was body weight adjustment performed.
Although a correlation was observed between mREE and the Harris–Benedict equation, the Bland–Altman plots revealed wide limits of agreement, suggesting that at the individual level the equations may lead to clinically significant errors. The Harris–Benedict equation demonstrated a significant systematic underestimation of mREE, indicating that its accuracy decreases as energy requirements increase. In contrast, the Schofield equation did not demonstrate proportional bias, suggesting a more stable performance across the range of mREE values. However, the particularly wide limits of agreement indicate substantial interindividual variability. This observation is clinically important, as a discrepancy of approximately ±500 kcal/day may lead to underfeeding or overfeeding, particularly in patients experiencing high metabolic stress. The method based on 30 kcal/kg of ideal body weight showed the greatest deviation, indicating a tendency toward systematic overestimation of energy requirements, especially in patients with higher mREE values. These findings suggest that simplified body weight–based equations may not be appropriate for surgical patients.
In the accuracy analyses between pREE equations, the Harris–Benedict equation demonstrated the lowest overall error (RMSE = 350.6 kcal), but also showed the highest rate of mREE underestimation (<10% in 61.5% of cases). The Schofield equation followed with a slightly higher error (RMSE = 368.7 kcal) and greater relative error (MAPE = 21.1%), also demonstrating a significant tendency toward underestimation. In contrast, the weight-based equations compared with the adjusted value of mREE × 1.15 showed a different error distribution: the 25 kcal/kg ideal body weight equation demonstrated the lowest relative error (MAPE = 17.8%) and a more balanced distribution of under- and overestimation, whereas the 30 kcal/kg equation showed the highest overall error (RMSE = 416.8 kcal) and a strong tendency toward overestimation (>10% in 53.8% of cases). These findings further support the position that indirect calorimetry remains the reference method whenever available. Consistent with the findings of the present study, a study evaluating 61 oncology patients prior to surgery reported that the Harris–Benedict equation most frequently underestimated energy expenditure compared with indirect calorimetry, whereas the Schofield equation demonstrated the greatest accuracy among the predictive equations assessed. The reported RMSE values were 914 kcal/day and 794 kcal/day, respectively [21].
Progressive weight loss and reduction in BMI were significant from hospital admission through the first 3–6 months following surgery. A previous study in patients with pancreatic cancer reported significant weight loss and alterations in body composition up to 14 weeks after the Whipple procedure [22]. At 6 months, patients appeared to return to their body weight at admission, although with reduced body composition parameters, a finding that was not observed in the present study. In another study, patients demonstrated significant weight loss and reductions in serum albumin levels, along with a progressive decline in both lean body mass and adipose tissue up to 12 months after the Whipple procedure [23]. In a study analyzing all three major surgical procedures for pancreatic cancer resection, patients who underwent pancreatectomy had lost 8.4% of their body weight 2 months postoperatively and 9% at 4 months after surgery [24]. These findings are consistent with the results of the present study, which demonstrated a 7.8% body weight loss within 3–6 months after pancreatectomy. This degree of weight loss has been significantly associated with poorer postoperative clinical outcomes. Furthermore, an analysis of 1090 patients who underwent pancreatectomy found that the median percentage of weight loss during the first postoperative year was approximately 6.6% (−7.8% for partial pancreatectomy and −4.2% for distal pancreatectomy), with a steady decline in body weight already evident at 1 and 3 months after surgery [25]. In the present study, a statistically significant reduction in body weight was observed both when comparing preoperative values with discharge weight and when comparing preoperative values with body weight at 3–6 months following pancreatectomy. This weight loss likely reflects a combination of reduced food intake, malabsorption and metabolic stress. Moreover, the findings indicate that weight loss is not confined to the immediate postoperative period but may continue for several months after surgery. Consequently, systematic patient follow-up should extend beyond hospitalization, with particular emphasis on the first postoperative months, in order to prevent further deterioration of nutritional status.
Multiple linear regression analysis demonstrated that body weight was the only independent predictor of mREE. Specifically, for every 1 kg increase in body weight, mREE increased by approximately 8 kcal/day, while other factors, such as CRP (mg/dL) and postoperative albumin levels (g/dL), did not show an independent effect on mREE. This finding is consistent with the literature, where body weight and particularly lean lean body mass, is considered the main determinant of REE. A meta-analysis of 27 studies reported an increase in REE of 2.31 kcal/kg lean body mass/day in patients with cancer, highlighting the significant contribution of body composition to the regulation of REE [26]. However, it should be noted that certain potentially important factors, such as tumor size, were not included in the present model. It has been suggested that the additional energy expenditure associated with tumor burden may range from 100 to 1400 kcal/day. Theoretically, an additional energy requirement of approximately 400 kcal/day would correspond to nearly 25% of the REE of a patient with a daily REE of 1600 kcal, emphasizing the potentially substantial impact of tumor burden on metabolism [27].
Additionally, length of hospital stay is an important indicator of postoperative recovery and is directly related to nutritional support and patients’ energy requirements. A study involving a large population of patients undergoing major oncologic surgery demonstrated that hospital stay was reduced with the implementation of ERAS protocols, with an average duration of 6 days. However, length of stay was influenced by the type of surgery and postoperative complications, significantly affecting healthcare costs and resource utilization [28]. In another study including 668 patients who underwent the Whipple procedure, the mean postoperative hospital stay was 10 days and this finding was significantly associated with the severity of complications, suggesting that total hospitalization duration more comprehensively reflects the severity of the postoperative condition [29]. In the present study, the median length of hospital stay was 22 days. It also appeared that greater weight loss occurred during hospitalization compared with the post-discharge period. Prolonged hospitalization may be associated with sustained catabolism, increased energy requirements and greater body weight loss. Therefore, length of stay should not be considered solely an administrative quality indicator, but also a potential indirect marker of metabolic burden.
According to the above findings, an important strength of the present study is the use of indirect calorimetry for the measurement of REE. According to the ESPEN guidelines, indirect calorimetry is considered the preferred method for estimating energy requirements, particularly in patients with increased metabolic stress or a high risk of malnutrition. The study was not limited to a single predictive equation but compared mREE with the Harris–Benedict and Schofield equations, as well as with the simplified approaches of 25 and 30 kcal/kg. In addition, both statistical (regression models) and clinical methods of evaluation (Bland–Altman analysis, MAPE, RMSE and ±10% and ±20% accuracy) were applied, providing a comprehensive assessment of agreement rather than simple correlation alone. Multiple linear regression further strengthened the interpretation of the findings by identifying body weight as an independent predictor of mREE. Furthermore, the collection of preoperative, postoperative and 3–6-month follow-up data provided a dynamic overview of the metabolic course of patients and documented the progressive weight loss observed after pancreatectomy, a finding of particular importance for the planning of nutritional follow-up. Patients undergoing total or partial pancreatectomy for pancreatic tumors represent a unique population at high risk of malnutrition and metabolic disturbances. The present study contributes to the literature by addressing an area in which available data remain limited. Finally, to our knowledge, this is the first systematic effort in Greece to record and evaluate REE using indirect calorimetry in patients undergoing total or partial pancreatectomy. The comparative analysis with established predictive equations and simplified methods for estimating energy requirements provides primary data for the Greek population and establishes a basis for the development of individualized nutritional protocols in this particularly vulnerable group of patients.
The present study also has several limitations that should be considered when interpreting the findings. First, the relatively small sample size may limit both the statistical power and the generalizability of the results. Although the differences between mREE and the predictive equations were statistically significant, a larger sample could further confirm the consistency of the observed discrepancies. An additional limitation relates to the timing of mREE measurements, which were performed at specific predefined time points rather than continuously or repeatedly throughout hospitalization and recovery. In relation to this, preoperative body weight was used for comparison with mREE, since accurate body weight measurement during the early postoperative period is often difficult due to fluid shifts, edema and limited mobility. REE following major surgery is dynamic and likely changes substantially between the immediate postoperative phase and the recovery period. Therefore, the absence of repeated measurements at additional time points may not fully capture the metabolic trajectory of the patients. Third, body composition assessment (e.g., lean body mass) was not performed, despite being a major determinant of REE. Consequently, the observed weight loss could not be accurately differentiated into losses of fat mass or lean body mass, limiting the interpretation of metabolic adaptation. Last but not least, the attrition rate was 20% in the 3–6 month follow-up period, which may lead to follow-up bias and reduce the statistical power of the longitudinal analyses.
Despite these limitations, the study provides clinically relevant data regarding the accuracy of predictive equations in patients following total or partial pancreatectomy for pancreatic tumors and highlights the importance of individualized assessment of energy requirements. Future studies should focus on nutritional adequacy, body composition assessment and multicenter study designs.
5. Conclusions
The present study demonstrated that patients undergoing total or partial pancreatectomy for pancreatic tumors experience significant metabolic and nutritional alterations during the perioperative and early postoperative period. mREE, as determined by indirect calorimetry, differed significantly from predictive equations (Harris–Benedict and Schofield) as well as from the simplified ESPEN body weight–based approaches (25 and 30 kcal/kg), indicating that these methods are not interchangeable with direct measurement at the individual level. Specifically, the 30 kcal/kg approach demonstrated the greatest clinical error, while the Harris–Benedict equation showed the highest rate of mREE underestimation (61.5% of cases). In contrast, the 25 kcal/kg approach demonstrated a more balanced distribution of under- and overestimation but still has clinical inconsistency at the individual level.
Body weight emerged as the only independent predictor of mREE, with an increase of approximately 8 kcal/day for each additional kilogram of body weight. At the same time, a statistically significant and progressive reduction in body weight and BMI was observed from the preoperative period through discharge and up to 3–6 months postoperatively, highlighting the ongoing metabolic burden and the need for long-term nutritional follow-up. Overall, the findings support the use of individualized assessment through indirect calorimetry as the most appropriate approach for determining energy requirements in this vulnerable patient population.
Author Contributions
Conceptualization, D.K. and D.C and M.D.; methodology, D.K. and M.D.; software, P.P. and Z.B. and D.K.; investigation, P.P. and Z.B. and O.G.; resources, D.K. and D.C.; writing—original draft preparation, P.P.; writing—review and editing, P.P. and Z.B. and D.K. and O.G. and D.C. and I.G. and M.D.; supervision, M.D.; project administration, D.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Evangelismos Hospital of Athens (Approval No. 484, 2025) and the Ethics Committee of the Aristotle University of Thessaloniki (Protocol No. 126/2025).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.:
Data Availability Statement
The data presented in this study are available on request from the corresponding author (the data are not publicly available due ethical restrictions).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BMI | Body Mass Index |
| CRP | C-reactive protein |
| ESPEN | European Society for Clinical Nutrition and Metabolism |
| IPMN | Intraductal Papillary Mucinous Neoplasm |
| MAPE | Mean Absolute Percentage Error |
| mREE | Measured Resting Energy Expenditure |
| PONS | Perioperative Nutrition Screen |
| pREE | Predicted Resting Energy Expenditure |
| RMSE | Root Mean Square Error |
| RQ | Respiratory Quotient |
References
- Niwano F, Hiromine Y, Noso S, Babaya N, Ito H, Yasutake S; et al. Insulin deficiency with and without glucagon: A comparative study between total pancreatectomy and type 1 diabetes. J Diabetes Investig. 2018 Sep;9(5):1084–90. [CrossRef]
- Andrén-Sandberg Å, Ansorge C, Yadav TD. Are There Indications for Total Pancreatectomy in 2016? Dig Surg. 2016;33(4):329–34. [CrossRef]
- Furbetta N, Comandatore A, Gianardi D, Palmeri M, Di Franco G, Guadagni S; et al. Perioperative Nutritional Aspects in Total Pancreatectomy: A Comprehensive Review of the Literature. Nutrients. 2021 May 22;13(6):1765. [CrossRef]
- Robertson RH, Russell K, Jordan V, Pandanaboyana S, Wu D, Windsor J. Postoperative nutritional support after pancreaticoduodenectomy in adults. Cochrane Central Editorial Service, editor. Cochrane Database Syst Rev. 2025 Mar 14;2025(3). [CrossRef]
- Afaneh C, Gerszberg D, Slattery E, Seres DS, Chabot JA, Kluger MD. Pancreatic cancer surgery and nutrition management: A review of the current literature. Hepatobiliary Surg Nutr. 2015 Feb;4(1):59–71. [CrossRef] [PubMed] [PubMed Central]
- Schnelldorfer T, Mauldin PD, Lewin DN, Adams DB. Distal Pancreatectomy for Chronic Pancreatitis: Risk Factors for Postoperative Pancreatic Fistula. J Gastrointest Surg. 2007 Aug;11(8):991–7. [CrossRef]
- Weimann A, Braga M, Carli F, Higashiguchi T, Hübner M, Klek S; et al. ESPEN guideline: Clinical nutrition in surgery. Clin Nutr. 2017 Jun;36(3):623–50. [CrossRef]
- Sasaki M, Okamoto H, Johtatsu T, Kurihara M, Iwakawa H, Tanaka T; et al. Resting energy expenditure in patients undergoing pylorus preserving pancreatoduodenectomies for bile duct cancer or pancreatic tumors. J Clin Biochem Nutr. 2011;48(3):183–6. [CrossRef]
- Martin D, Joliat GR, Halkic N, Demartines N, Schäfer M. Perioperative nutritional management of patients undergoing pancreatoduodenectomy: An international survey among surgeons. HPB. 2020 Jan;22(1):75–82. [CrossRef]
- Russell TB, Murphy P, Tanase A, Sen G, Aroori S. Results from a UK-wide survey: The nutritional assessment and management of pancreatic resection patients is highly variable. Eur J Clin Nutr. 2022 Jul;76(7):1038–40. [CrossRef]
- Delsoglio M, Achamrah N, Berger MM, Pichard C. Indirect Calorimetry in Clinical Practice. J Clin Med. 2019 Sep 5;8(9):1387. [CrossRef]
- Nuttall FQ. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr Today. 2015 May;50(3):117–28. [CrossRef] [PubMed] [PubMed Central]
- Williams DG, Aronson S, Murray S, Fuller M, Villalta E, Haines KL; et al. Validation of the perioperative nutrition screen for prediction of postoperative outcomes. J Parenter Enter Nutr. 2022 Aug;46(6):1307–15. [CrossRef]
- Weir JB. New methods for calculating metabolic rate with special reference to protein metabolism. 1949. Nutrition. 1990;6(3):213–21. [PubMed]
- Harris JA, Benedict FG. A Biometric Study of Human Basal Metabolism. Proc Natl Acad Sci U S A. 1918 Dec;4(12):370–3. [CrossRef] [PubMed] [PubMed Central]
- Schofield WN. Predicting basal metabolic rate, new standards and review of previous work. Hum Nutr Clin Nutr. 1985;39 Suppl 1:5–41. [PubMed]
- Ishida J, Konishi M, Saito M, Springer J. Hypermetabolism: Should cancer types, pathological stages and races be considered in assessing metabolism and could elevated resting energy expenditure be the therapeutic target in patients with advanced cancer?: Correspondence. J Cachexia Sarcopenia Muscle. 2015 Dec;6(4):391–2. [CrossRef]
- Bulmuş Tüccar T, Acar Tek N. Determining the factors affecting energy metabolism and energy requirement in cancer patients. J Res Med Sci Off J Isfahan Univ Med Sci. 2021;26:124. [CrossRef] [PubMed] [PubMed Central]
- Moses AWG, Slater C, Preston T, Barber MD, Fearon KCH. Reduced total energy expenditure and physical activity in cachectic patients with pancreatic cancer can be modulated by an energy and protein dense oral supplement enriched with n-3 fatty acids. Br J Cancer. 2004 Mar 8;90(5):996–1002. [CrossRef] [PubMed] [PubMed Central]
- Mazzo R, Ribeiro FB, Vasques ACJ. Accuracy of predictive equations versus indirect calorimetry for the evaluation of energy expenditure in cancer patients with solid tumors - An integrative systematic review study. Clin Nutr ESPEN. 2020 Feb;35:12–9. [CrossRef] [PubMed]
- Barcellos PS, Borges N, Torres DPM. Resting energy expenditure in cancer patients: Agreement between predictive equations and indirect calorimetry. Clin Nutr ESPEN. 2021 Apr;42:286–91. [CrossRef] [PubMed]
- Aslani A, Roach PJ, Smith RC. Long-term changes in body composition after pancreaticoduodenectomy. ANZ J Surg. 2012 Mar;82(3):173–8. [CrossRef] [PubMed]
- Cloyd JM, Nogueras-González GM, Prakash LR, Petzel MQB, Parker NH, Ngo-Huang AT; et al. Anthropometric Changes in Patients with Pancreatic Cancer Undergoing Preoperative Therapy and Pancreatoduodenectomy. J Gastrointest Surg. 2018 Apr;22(4):703–12. [CrossRef]
- Hashimoto D, Chikamoto A, Ohmuraya M, Abe S, Nakagawa S, Beppu T; et al. Impact of Postoperative Weight Loss on Survival After Resection for Pancreatic Cancer. J Parenter Enter Nutr. 2015 Jul;39(5):598–603. [CrossRef]
- Trudeau MT, Casciani F, Gershuni VM, Maggino L, Ecker BL, Lee MK; et al. Defining postoperative weight change after pancreatectomy: Factors associated with distinct and dynamic weight trajectories. Surgery. 2020 Dec;168(6):1041–7. [CrossRef] [PubMed]
- Nguyen TYV, Batterham MJ, Edwards C. Comparison of Resting Energy Expenditure Between Cancer Subjects and Healthy Controls: A Meta-Analysis. Nutr Cancer. 2016;68(3):374–87. [CrossRef] [PubMed]
- Purcell SA, Elliott SA, Baracos VE, Chu QSC, Prado CM. Key determinants of energy expenditure in cancer and implications for clinical practice. Eur J Clin Nutr. 2016 Nov;70(11):1230–8. [CrossRef]
- Nazzani S, Preisser F, Mazzone E, Tian Z, Mistretta FA, Shariat SF; et al. In-hospital length of stay after major surgical oncological procedures. Eur J Surg Oncol J Eur Soc Surg Oncol Br Assoc Surg Oncol. 2018 Jul;44(7):969–74. [CrossRef] [PubMed]
- Williams GA, Liu J, Chapman WC, Hawkins WG, Fields RC, Sanford DE; et al. Composite Length of Stay, An Outcome Measure of Postoperative and Readmission Length of Stays in Pancreatoduodenectomy. J Gastrointest Surg Off J Soc Surg Aliment Tract. 2020 Sep;24(9):2062–9. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Linear regression between measured resting energy expenditure and a multiplier of 1.15 using energy requirement estimation equations (analyses were performed using mREE-Harris-Benedict; mREE-Schofield; mREE x 1.15 - 25 kcal x ideal body weight; and mREE x 1.15 - 30 kcal x ideal body weight).
Figure 1.
Linear regression between measured resting energy expenditure and a multiplier of 1.15 using energy requirement estimation equations (analyses were performed using mREE-Harris-Benedict; mREE-Schofield; mREE x 1.15 - 25 kcal x ideal body weight; and mREE x 1.15 - 30 kcal x ideal body weight).

Figure 2.
Bland-Altman plots show the limits between measured resting energy expenditure predicted and values multiplied by a factor of 1.15 using the energy requirement estimation equations (the analyses were performed using the mREE-Harris-Benedict; mREE-Schofield; mREE x 1.15 - 25 kcal x ideal body weight; and mREE x 1.15 - 30 kcal x ideal body weight).
Figure 2.
Bland-Altman plots show the limits between measured resting energy expenditure predicted and values multiplied by a factor of 1.15 using the energy requirement estimation equations (the analyses were performed using the mREE-Harris-Benedict; mREE-Schofield; mREE x 1.15 - 25 kcal x ideal body weight; and mREE x 1.15 - 30 kcal x ideal body weight).

Figure 3.
Change in body weight from the preoperative period through discharge and 3–6 months after surgery.
Figure 3.
Change in body weight from the preoperative period through discharge and 3–6 months after surgery.

Figure 4.
Change in body mass index from the preoperative period through discharge and 3–6 months after surgery.
Figure 4.
Change in body mass index from the preoperative period through discharge and 3–6 months after surgery.

Table 4.
Accuracy metrics of equations estimating energy requirements and measured resting energy expenditure1.
Table 4.
Accuracy metrics of equations estimating energy requirements and measured resting energy expenditure1.
| Method | Underestimation (<10%) | Accuracy (±10%) | Overestimation (>10%) | MAPE | RMSE |
| Harris-Benedict | 61.5% | 11.5% | 26.9% | 18.9% | 350 kcal |
| Schofield | 53.8% | 15.4% | 30.8% | 21.1% | 368 kcal |
| 25 kcal/kg | 34.6% | 30.8% | 34.6% | 17.8% | 369 kcal |
| 30 kcal/kg | 19.2% | 34.6% | 46.2% | 23.2% | 416 kcal |
1Abbreviations: MAPE = Mean Absolute Percentage Error, RMSE = Root Mean Square Error.
Table 5.
Association between body weight and measured resting energy expenditure using multiple linear regression models1.
Table 5.
Association between body weight and measured resting energy expenditure using multiple linear regression models1.
| Model | β | SE | R | %95 CI | p-value |
| Model 1 | 8.98 | 3.16 | 0.50 | 2.45-15.5 | 0.009* |
| Model 2 | 8.83 | 3.06 | 0.60 | 2.48-15.2 | 0.009* |
| Model 3 | 8.01 | 3.16 | 0.65 | 1.39-14.6 | 0.020* |
1Model 1: unadjusted; Model 2: age, sex; Model 3: Model 2 plus CRP (mg/dL) and postoperative albumin (g/dL). *Indicates a statistically significant difference between groups. Abbreviations: SE = Standard Error, CI = Confidence Interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



