Submitted:
29 May 2026
Posted:
01 June 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Abstract
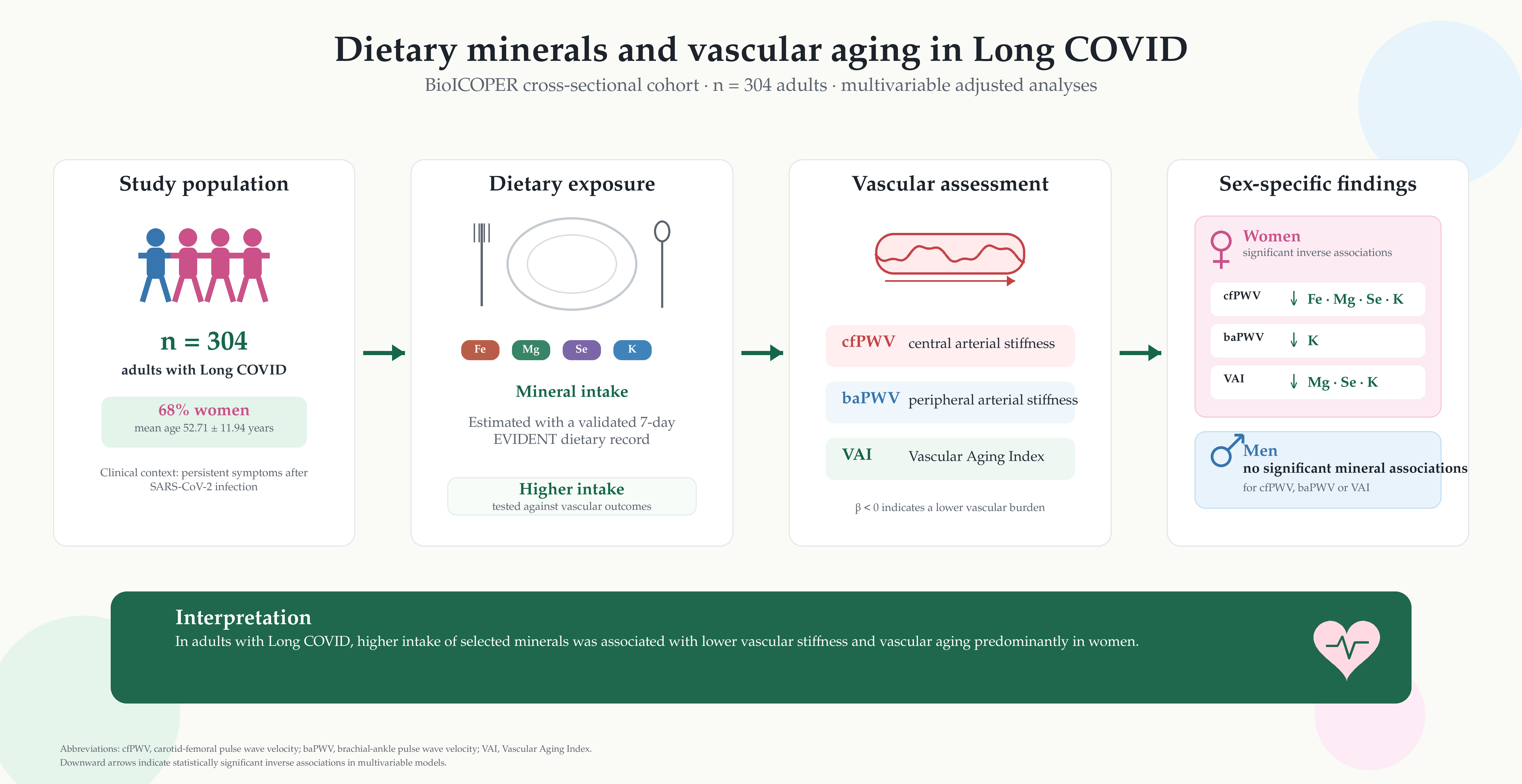
Background/Objectives: Long COVID (LC) has been associated with persistent in-flammation and impaired vascular health. Dietary minerals are involved in the regula-tion of oxidative stress, endothelial homeostasis, and arterial stiffness; however, their relationship with vascular health in LC remains poorly explored. This study aimed to examine the association between dietary mineral intake and markers of vascular stiff-ness and vascular aging in adults with LC, while exploring potential sex-specific pat-terns. Methods: A total of 304 adults with LC from the BioICOPER study were includ-ed. Dietary mineral intake was assessed using a validated 7-day dietary record from the EVIDENT tool. Vascular assessment included carotid intima–media thickness (cIMT), carotid–femoral pulse wave velocity (cfPWV), brachial–ankle pulse wave velocity (baPWV), and the vascular aging index (VAI), measured using carotid ultrasonography and validated devices, including SphygmoCor® and VaSera®. Multivariable linear re-gression models were used to evaluate the associations between dietary mineral intake and vascular outcomes, adjusting for sociodemographic, clinical, hemodynamic, an-thropometric, quality-of-life, and dietary-pattern variables. Results: Higher intakes of magnesium, selenium, potassium, and phosphorus were associated with lower cfPWV. Potassium intake was also inversely associated with baPWV, whereas selenium and phosphorus intakes were inversely associated with VAI. In sex-stratified analyses, in-verse associations were more consistent among women, particularly for cfPWV and VAI. However, formal interaction analyses did not confirm significant sex-related ef-fect modification. Conclusions: Dietary mineral intake was associated with vascular stiffness, particularly central arterial stiffness, and vascular aging in adults with LC. These findings suggest that adequate mineral intake may represent a relevant nutri-tional factor for vascular health in LC. Prospective studies and nutritional intervention trials are warranted to confirm these results and clarify their clinical relevance.
Keywords:
Long COVID
; arterial stiffness
; vascular health
; minerals intake and vascular aging
1. Introduction
Long COVID (LC) represents one of the most complex public health challenges worldwide [1,2,3]. Beyond its heterogeneous clinical manifestations, increasing evidence indicates that LC is characterized by a state of chronic low-grade inflammation and sustained endothelial dysfunction [4,5,6]. The CARTESIAN study has shown that persistent viral-related inflammation may promote accelerated vascular aging, characterized by structural elastin degradation and abnormal collagen deposition within the extracellular matrix of arterial walls [7]. Consequently, endothelial impairment may contribute to increased arterial stiffness, which can persist for months or even years after the initial infection [4,8]. In addition, the vascular consequences of LC may differ according to sex, with women with LC showing poorer arterial elasticity in some studies [7,9]. Accordingly, the assessment of arterial stiffness, an independent predictor of cardiovascular morbidity and mortality, has become a relevant clinical and research tool for monitoring subclinical cardiovascular risk in individuals with LC [10,11,12].
A comprehensive evaluation of vascular health requires tools capable of assessing different arterial segments and properties of the vascular wall. Carotid–femoral pulse wave velocity (cfPWV) remains the gold-standard measure of central arterial stiffness [13,14,15], whereas brachial–ankle pulse wave velocity (baPWV) provides information on peripheral arterial stiffness [10,16,17]. In turn, the vascular aging index (VAI) integrates carotid intima–media thickness (cIMT) and cfPWV, thereby capturing both structural and functional components of vascular aging [18]. Taken together, these vascular markers may reflect the dynamic nature of persistent endothelial injury, driven by chronic oxidative stress and impaired vascular repair capacity in patients with LC [19,20].
Dietary composition plays a key role in arterial stiffness and vascular health [21,22]. In the context of the vascular vulnerability observed in individuals with LC, nutritional status, and particularly dietary mineral intake, may emerge as a potentially relevant modifiable factor [23]. Several minerals are involved in endothelial protection, oxidative balance, inflammatory regulation, vascular tone, and arterial wall remodeling. Magnesium (Mg), for instance, acts as a natural calcium antagonist and as a cofactor in nitric oxide synthesis, thereby helping to prevent vascular calcification and maintain arterial distensibility [24]. Magnesium deficiency, whether due to low intake or metabolic depletion, may promote oxidative stress, endothelial dysfunction, and inflammation [25,26], and this cardiovascular risk may be amplified when accompanied by high copper levels or low zinc availability [27]. In the context of COVID-19, infection-related alterations in magnesium homeostasis may contribute to vascular hypertonia, elastic fiber degradation, and fibrosis. Although short-term supplementation with magnesium citrate has not been shown to reverse arterial stiffness [28], lower dietary magnesium intake has been associated with greater clinical severity and neuropsychiatric sequelae [29,30]. Moreover, low serum magnesium levels at the onset of infection have been associated with a higher risk of developing persistent post-COVID symptoms [31]. Selenium (Se) is involved in antioxidant defense, inflammatory regulation, and immune response. Selenium deficiency may promote oxidative stress, endothelial dysfunction, low-grade inflammation, and reduced nitric oxide bioavailability, all of which are closely linked to arterial stiffness [32]. In both high-cardiovascular-risk populations and the general population, inadequate selenium intake or altered selenium status has been associated with vascular stiffness, suggesting that both deficiency and excess may be unfavorable for vascular health [32,33]. In COVID-19, low selenium concentrations have been associated with worse clinical outcomes and higher mortality, while systematic reviews indicate that patients with COVID-19 commonly show lower selenium levels than healthy controls, with deficiency being related to greater disease severity [34,35,36,37]. Iodine (I) is essential for thyroid hormone synthesis and therefore contributes indirectly to vascular homeostasis, nitric oxide production, lipid metabolism, and arterial elasticity. Iodine deficiency has been associated with increased cholesterol levels, greater arterial stiffness, and higher all-cause mortality [38,39]. Furthermore, COVID-19 may induce thyroid dysfunction during the acute phase and in individuals with LC, including thyroiditis and alterations in thyroid hormone levels [40]. Calcium (Ca) and phosphorus (P) are also essential for bone, energy, and vascular homeostasis; however, disturbances in calcium–phosphorus balance may promote endothelial dysfunction, vascular calcification, and increased cardiovascular risk, particularly in the presence of hyperphosphatemia or persistent metabolic alterations [41,42]. Recent reviews suggest that phosphate may contribute to cardiovascular disease through vascular calcification pathways, although contemporary epidemiological data do not support a direct association between higher dietary calcium or phosphorus intake per se and greater vascular or valvular calcification in the general population [43]. In COVID-19, disturbances in calcium, phosphorus, and magnesium metabolism during and after infection have been associated with poorer clinical outcomes [44]. Sodium (Na) and potassium (K) intake are central to extracellular volume regulation, blood pressure control, endothelial function, and vascular tone. High sodium intake and low potassium intake have been associated with higher blood pressure and poorer vascular function. In addition, evidence on arterial stiffness suggests that excess sodium intake, particularly when accompanied by low potassium intake, may contribute to increased pulse wave velocity, whereas sodium restriction can reduce arterial stiffness independently of blood pressure lowering [45]. Conversely, greater potassium availability or supplementation has been associated with improved endothelial function, which may help modulate the vascular impact of a sodium-rich diet [46]. In COVID-19, electrolyte disturbances, including abnormalities in sodium and potassium, have been associated with worse clinical evolution [47]. Zinc (Zn) is an essential trace element with antioxidant, anti-inflammatory, and immunomodulatory properties, and is involved in endothelial homeostasis and protection against oxidative stress. Insufficient zinc intake has been related to cardiovascular risk in a non-linear manner, suggesting that intake should be adequate but not excessive [48]. In patients with high vascular risk, zinc deficiency has also been independently associated with greater arterial stiffness [49]. In the context of COVID-19, zinc deficiency has been associated with poorer clinical outcomes and with a higher risk of hospitalization and mortality during the post-acute phase [50]. Finally, iron (Fe) is essential for oxygen transport and mitochondrial function, but its homeostasis requires tight regulation, as both deficiency and functional iron excess may contribute to inflammation, oxidative stress, and vascular damage. Regarding arterial stiffness, higher ferritin levels have been associated with greater pulse wave velocity in patients with hypertension and with higher baPWV in healthy adults [51]. Moreover, evidence supports a causal relationship between higher iron status, including serum iron, ferritin, and transferrin saturation, and increased arterial stiffness [52]. In COVID-19, dysregulation of iron metabolism and anemia are frequent during follow-up and have been related to persistent symptoms and poorer functional recovery [53].
Overall, previous evidence supports the relevance of minerals in vascular health, while also highlighting the lack of specific data in individuals diagnosed with LC. Therefore, it is necessary to examine the association between dietary mineral intake and vascular health in this population using validated dietary assessment instruments, such as those developed within the EVIDENT study [54], together with a comprehensive evaluation of the arterial tree.
Based on the hypothesis that an adequate dietary intake of essential minerals may exert an independent protective role against functional and structural vascular deterioration in individuals with LC, this study was designed with two main objectives. First, we aimed to evaluate the association between quantitative dietary intake of essential minerals and target indices of arterial stiffness and vascular aging, including cfPWV, baPWV, and VAI, in adults diagnosed with LC from the BioICOPER project. Second, we sought to explore whether these nutritional–vascular relationships differed according to biological sex, thereby providing novel evidence to support the potential development of personalized nutritional strategies aimed at mitigating cardiovascular risk in the clinical management of LC.
2. Materials and Methods
2.1. Study Design and Participants
This was a cross-sectional study including a cohort of 304 adults diagnosed with long COVID (LC). The study was conducted at the Primary Care Research Unit of Salamanca (APISAL). The present analysis forms part of the BioICOPER project, registered in April 2023 at ClinicalTrials.gov (Identifier: NCT05819840). The study protocol has been previously published [55].
Participants were recruited by consecutive sampling. The inclusion criteria were as follows: diagnosis of LC according to the World Health Organization (WHO) definition [56], namely a history of probable or confirmed SARS-CoV-2 infection and the presence of symptoms lasting for at least 2 months that could not be explained by an alternative diagnosis; and provision of written informed consent. The exclusion criteria were terminal illness, inability to attend the primary care center for assessment, a history of cardiovascular disease, including ischemic heart disease or cerebrovascular disease, or an estimated glomerular filtration rate below 30 mL/min/1.73 m². The participant flow chart is shown in Figure 1.
Sample Size Calculation
Sample size and detectable effect size were estimated using the GRANMO software (https://www.datarus.eu/ca/aplications/granmo/). For the multiple linear regression analyses, considering a total sample size of 304 participants, an alpha risk of 0.05, a beta risk below 0.20, the number of predictors included in the fully adjusted model, and, conservatively, the lowest adjusted coefficient of determination observed in the final models —cfPWV: adjusted R² = 0.347—, the available sample size was considered sufficient to assess the association between dietary magnesium intake and the main vascular parameters analyzed. In addition, assuming a standard deviation of 82 mg/day for magnesium intake, the sample of 304 participants allowed the mean dietary magnesium intake to be estimated with an approximate precision of ± 9.2 mg/day for a 95% confidence interval.
The present study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [57]. The completed STROBE checklist is provided in Supplementary Table S1.
2.2. Variables and Measurement Instruments
To reduce information bias, all analyzed variables and complementary assessments were collected by four healthcare professionals who had been trained before the start of the study and followed a standardized protocol. Data were recorded using Research Electronic Data Capture (REDCap), hosted by the Biomedical Research Institute of Salamanca (IBSAL), for data collection and management. Quality control was performed by an independent researcher [55].
2.3. Dietary Intake Assessment
Dietary mineral intake was assessed using a food record collected through the EVIDENT mobile application [54]. This application was developed and validated by the Primary Care Research Group of Castilla y León, affiliated with REDIAPP, and is registered under intellectual property number 00/2014/2207. This dietary assessment tool was designed to record food and beverage consumption. Participants recorded all foods and beverages consumed over seven consecutive days, including portion sizes. Foods were classified into predefined groups within the EVIDENT tool. Daily mineral intake was estimated using Spanish food composition tables and included iron (Fe), magnesium (Mg), selenium (Se), iodine (I), calcium (Ca), phosphorus (P), sodium (Na), potassium (K), and zinc (Zn) [54]. Dietary supplement use was not captured by the dietary assessment tool and was therefore not included in the estimation of total mineral intake.
To define groups with adequate and inadequate mineral intake, minimum requirements and reference intake values were used as cut-off points, following the combined criteria of the European Food Safety Authority (EFSA) and the Spanish Society of Community Nutrition (SENC) [58,59]. The cut-off points used for each mineral are shown in Supplementary Table S2.
2.4. Assessment of Vascular Structure, Function, and Aging
All vascular measurements were performed after 10 min of rest in the supine position, in a temperature-controlled room.
2.4.1. Carotid Intima–Media Thickness Measurement
Carotid intima–media thickness (cIMT) was measured by two investigators with demonstrated reliability. Interobserver and intraobserver intraclass correlation coefficients (ICCs), calculated in 20 participants before the start of the study, were 0.974 and 0.897, respectively. Measurements were performed using a Sonosite Micromax® ultrasound system (Sonosite Inc., Bothell, WA, USA), equipped with a high-resolution 5–10 MHz multifrequency linear transducer and Sonocal software (Washington, DC, USA), which enables automated cIMT measurement. cIMT assessments were performed according to the protocol previously published by our research group [60].
2.4.2. Arterial Stiffness Measurements
Arterial stiffness was assessed by measuring carotid–femoral pulse wave velocity (cfPWV) and brachial–ankle pulse wave velocity (baPWV).
Central arterial stiffness was assessed using cfPWV, measured with the SphygmoCor system (AtCor Medical Pty Ltd., West Ryde, Australia). Pulse waves were recorded at the carotid and femoral arteries. Transit time was estimated in relation to the R wave of the electrocardiogram. Distances were measured with a measuring tape from the suprasternal notch to the carotid and femoral recording sites. cfPWV was calculated according to established measurement guidelines [13,14,15].
baPWV was measured using the VaSera VS-2000 device (Fukuda Denshi Co., Ltd., Tokyo, Japan). Electrodes were placed on both arms and ankles, and measurements were obtained with the participant in the supine position, remaining silent and still. Measurements were considered valid after at least three consecutive stable cardiac cycles. According to the manufacturer’s instructions, baPWV was calculated using the following equation:
2.4.3. Vascular Aging Index Measurement
The vascular aging index (VAI) was calculated as previously described by Wadström et al. [18]. The index was derived by standardizing cIMT and cfPWV into z-scores and summing both components, according to the following formula:
2.5. Sociodemographic Variables, Lifestyle Factors, and Laboratory Analyses
Sociodemographic and lifestyle variables were collected using standardized questionnaires. Age and sex were recorded, together with lifestyle factors such as tobacco and alcohol consumption, which were assessed using questionnaires adapted from the WHO MONICA study [61]. Adherence to the Mediterranean diet was evaluated using the 14-item Mediterranean Diet Adherence Screener (MEDAS) [62]. Physical activity was assessed using the short version of the International Physical Activity Questionnaire (IPAQ-SF) [63], with results expressed as metabolic equivalent task minutes per week (MET-min/week). Health-related quality of life was evaluated using the 36-item Short Form Health Survey (SF-36) [64].
Fasting blood samples were obtained to determine lipid profile and plasma glucose levels. Blood pressure and heart rate were measured using a validated automated sphygmomanometer (OMRON M10-IT; Omron Healthcare Co., Ltd., Kyoto, Japan), following the recommendations of the European Society of Hypertension [14].
2.6. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 30.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p < 0.05. For descriptive analyses, quantitative variables were expressed as mean ± standard deviation (SD), and comparisons between men and women were performed using Student’s t-test for independent samples. Qualitative variables were expressed as frequencies and percentages, and comparisons between sexes were performed using the chi-square test. Analysis of covariance (ANCOVA) was used to compare age- and sex-adjusted means of vascular function and vascular aging parameters between participants with adequate and inadequate mineral intake. Results were expressed as estimated marginal means. Multiple linear regression models were used to evaluate the independent association between vascular function and vascular aging parameters and dietary mineral intake. cfPWV, baPWV, and VAI were included as dependent variables. Dietary intakes of iron (Fe), magnesium (Mg), selenium (Se), iodine (I), calcium (Ca), phosphorus (P), sodium (Na), potassium (K), and zinc (Zn) were entered individually as independent variables. Age in years, sex (0 = women; 1 = men), alcohol consumption in grams, Mediterranean diet score, physical activity expressed as MET-min/week, presence of hypertension, type 2 diabetes mellitus, dyslipidemia, abdominal obesity, and smoking status (0 = absence; 1 = presence of the risk factor), as well as SF-36 score, were included as covariates. Before performing the analyses, the assumptions of the linear regression models were checked. Multicollinearity was assessed using the variance inflation factor (VIF), with all values being <2.0. Results were expressed as unstandardized regression coefficients (β) with their corresponding 95% confidence intervals (95% CIs). Finally, to evaluate potential sex-related effect modification, interactions between sex and the intake of minerals that showed significant associations were examined in Model 2 by introducing a multiplicative interaction term, sex × each mineral, into the fully adjusted multiple linear regression model. It was established a priori that, if the interaction term was statistically significant (p < 0.05), analyses would be repeated after stratification by sex.
2.7. Ethical Considerations
This study was approved on 27 June 2022 by the Drug Research Ethics Committee of the Salamanca Health Area, Spain (CEIm: Ref. PI 2022 06 1048). Throughout the study, the standards of good practice for observational studies established by the Declaration of Helsinki and the World Health Organization were followed [65]. Participant confidentiality was guaranteed in accordance with Spanish Organic Law 3/2018, European Regulation 2016/679, and Council Directive 27/04/2016 on data protection. All participants provided written informed consent before inclusion in the study, after receiving detailed information about the procedures to be performed.
2.8. Use of Artificial Intelligence Tools
During manuscript preparation, ChatGPT (OpenAI, GPT-5.5 Thinking) was used to assist with English-language editing and with the formatting and assembly of manuscript figures based on results generated by the authors. Generative artificial intelligence was not used to create scientific images, generate data, perform statistical analyses, or alter the study results. All figures were compared against the original data and statistical outputs by the authors. The authors reviewed and approved all AI-assisted edits and take full responsibility for the final manuscript.
3. Results
3.1. Study Participants
The characteristics of the study population, both overall and according to sex, are presented in Table 1. Women accounted for 68% of the sample. Men were older than women and had higher alcohol consumption, systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting plasma glucose (FPG), triglyceride levels, and body mass index (BMI). Conversely, high-density lipoprotein cholesterol (HDL-C) levels were higher in women. Regarding vascular assessment, men exhibited higher values for the analyzed vascular structure and function parameters. The mean interval between the diagnosis of acute SARS-CoV-2 infection and inclusion in the study was 38.7 ± 9.6 months.
3.2. Dietary Mineral Intake Assessed Using the EVIDENT Tool
Dietary mineral intake estimated from the 7-day dietary record using the EVIDENT tool is presented in Table 2, both for the overall sample and stratified by sex. No statistically significant differences were found between men and women in the intake of the minerals analyzed.
Figure 2 illustrates the proportion of participants meeting adequate mineral intake recommendations in the overall sample and stratified by sex. The proportion of participants achieving adequate intake differed markedly across minerals, being highest for selenium, zinc, and iron, and lowest for iodine, sodium, calcium, and phosphorus. Adequate iron intake was significantly more prevalent among men, whereas women showed significantly higher adherence to magnesium and zinc recommendations. No significant differences between men and women were observed for the other minerals analyzed.
3.3. Estimated Marginal Means of Function, and Aging Parameters According to Minerals Intake Adherence
Table 3 shows the age- and sex-adjusted estimated marginal means of vascular stiffness parameters according to mineral intake adequacy. Participants with adequate iron intake had lower baPWV values than those with insufficient or at-risk intake (p = 0.049), while adequate magnesium intake was associated with lower cfPWV values (p = 0.037). No statistically significant differences were found for the other minerals analyzed. Overall, although several vascular stiffness parameters tended to be numerically lower among participants meeting mineral intake recommendations, most comparisons did not reach statistical significance.Los análisis estratificados por sexo se presentan en las Tablas Suplementarias S3 y S4. En los hombres, no se observaron diferencias. Sin embargo, en las mujeres, una ingesta adecuada de Fe, Mg y Zn se asoció con valores más bajos de cfPWV y VAI.
3.4. Multiple Linear Regression Analysis of Function, and Aging Parameters in Relation to Minerals Intake Assessed by the EVIDENT Tool
As shown in Figure 3, higher dietary intakes of magnesium, selenium, potassium, and phosphorus were significantly associated with lower cfPWV values (all p < 0.05).
As shown in Figure 4, potassium intake was inversely associated with baPWV, indicating that higher dietary potassium intake was related to lower peripheral arterial stiffness.
As shown in Figure 5, dietary selenium and phosphorus intakes were inversely associated with VAI, indicating that higher intakes of these minerals were related to lower vascular aging index values.
Figure 6 illustrates the association between dietary mineral intake and cfPWV stratified by sex. In men, no significant associations were observed between mineral intake and cfPWV. In women, however, higher intakes of iron, magnesium, selenium, and potassium were inversely associated with cfPWV.
Figure 7 shows the sex-stratified association between dietary mineral intake and baPWV. No significant associations were observed in either men or women.
Figure 8 shows the sex-stratified association between dietary mineral intake and VAI. No significant associations were observed in men. In contrast, among women, higher intakes of magnesium, selenium, and potassium were inversely associated with VAI.
Finally, potential effect modification by sex was assessed by including sex × mineral intake interaction terms in the regression models. No significant interactions were observed for the associations between dietary mineral intake and cfPWV, baPWV, or VAI (p > 0.05 in all cases), indicating that the observed associations did not differ significantly by sex.
4. Discussion
In this cross-sectional study of 304 adults with long COVID (LC), dietary mineral intake was associated with markers of arterial stiffness and vascular aging. In adjusted models, higher intakes of magnesium (Mg), selenium (Se), potassium (K), and phosphorus (P) were independently associated with lower central arterial stiffness, assessed by cfPWV. In addition, K intake was inversely associated with baPWV, whereas Se and P intakes were associated with lower VAI values. In contrast, no consistent independent associations were observed for iodine (I), sodium (Na), calcium (Ca), zinc (Zn), or iron (Fe) in the overall fully adjusted regression models. Taken together, these findings suggest that specific minerals involved in endothelial function, oxidative stress, inflammation, electrolyte balance, and mineral metabolism may be related to the vascular profile of individuals with LC.
The results also showed heterogeneous adherence to adequate mineral intake recommendations, with higher adequacy for Se, Zn, and Fe, and lower adherence for Ca, Mg, K, Na, P, and iodine. This pattern is consistent with previous studies conducted in Spanish and Mediterranean populations, such as the ANIBES and MEAL studies [66,67], which reported insufficient intakes particularly for Ca, Mg, Na, and K. Moreover, recent global estimates have identified Ca, I, and Fe among the micronutrients with the highest prevalence of inadequate intake, with sex-related differences [68]. Therefore, these findings suggest the presence of potential dietary gaps among patients with LC, although they should not be interpreted as biochemical deficiencies in the absence of analytical confirmation.
The inverse association between Mg intake and cfPWV is biologically plausible and consistent with the role of Mg in vascular homeostasis. Mg acts as a natural Ca antagonist, participates in nitric oxide synthesis, modulates vascular smooth muscle tone, and may limit oxidative stress, inflammation, endothelial dysfunction, and vascular calcification [24,25,26,27]. These mechanisms are particularly relevant in LC, a condition characterized by persistent inflammation, thromboinflammatory activation, oxidative stress, and vascular aging [4,5,20]. Although Mg supplementation trials have not consistently demonstrated short-term reductions in arterial stiffness [30], observational and mechanistic evidence supports the hypothesis that insufficient Mg status may contribute to vascular dysfunction. Furthermore, in the context of COVID-19, low Mg levels have been associated with worse clinical outcomes and a higher likelihood of developing symptoms compatible with LC [29,31]. Therefore, the observed association between higher Mg intake and lower cfPWV may reflect a potentially protective nutritional pattern against increased central arterial stiffness in a population with persistent vascular vulnerability.
Se intake was also inversely associated with cfPWV and VAI, supporting its potential role in vascular protection. Se is incorporated into selenoproteins involved in antioxidant defense, redox regulation, immune response, and inflammatory control [34]. Previous studies have linked Se deficiency to poorer arterial function in patients at high cardiovascular risk, while recent population-based data suggest an association between circulating Se levels and arterial stiffness [32]. In COVID-19, low Se and selenoprotein P concentrations have been associated with greater disease severity and mortality, and systematic reviews indicate that Se deficiency is common among patients with COVID-19 and may contribute to inflammatory and immune dysregulation [34,35,36,37]. The association observed in our study with both cfPWV and VAI suggests that Se intake may be related not only to functional arterial stiffness but also to a broader vascular aging phenotype.
The findings for K are also consistent with its physiological role in blood pressure regulation, endothelial function, vascular smooth muscle relaxation, and counter-regulation of the effects of Na. Available evidence indicates that greater K availability may improve endothelial function, whereas a dietary pattern characterized by high Na intake and low K intake has been associated with poorer vascular function and greater arterial stiffness [45,46]. In the present study, K intake was inversely associated with both cfPWV and baPWV, suggesting that it may influence both central and peripheral arterial stiffness. This finding is clinically relevant because baPWV reflects a broad arterial pathway that includes both elastic and muscular arteries and has also been associated with cardiovascular risk [10]. The absence of a significant association for Na may be explained by limitations in dietary Na estimation, adjustment for blood pressure, or the possibility that the Na/K balance is more informative than isolated Na intake.
The inverse association between P intake and both cfPWV and VAI should be interpreted with caution. From a mechanistic perspective, excess phosphate has been linked to endothelial dysfunction, osteogenic transition of vascular smooth muscle cells, vascular calcification, and cardiovascular disease, particularly in the context of chronic kidney disease or altered mineral metabolism [42,43]. However, dietary P intake does not necessarily translate into increased serum phosphate burden, and recent epidemiological studies do not support a simple positive association between higher dietary Ca or P intake and vascular or valvular calcification in the general population [41]. In the present study, the inverse association between P intake and vascular parameters may instead reflect better overall nutritional status, higher intake of protein-rich foods, or greater dietary adequacy, rather than a direct protective effect of P. Given that COVID-19 has been associated with disturbances in Ca, P, and Mg metabolism [44], future studies should distinguish between dietary intake, circulating levels, and renal regulation of P.
Regarding minerals that did not show significant associations in the fully adjusted models, the absence of association does not necessarily exclude their biological relevance. Ca is closely linked to mineral metabolism and vascular calcification, although recent evidence does not support a simple detrimental effect of higher dietary Ca intake on vascular calcification [41]. Zn and Fe also have biological plausibility because of their roles in immune response, oxidative stress, endothelial homeostasis, and inflammation. Zn deficiency has been associated with greater arterial stiffness in high-risk populations and with poorer outcomes during the post-acute phase of COVID-19 [48,49,50], whereas dysregulation of Fe metabolism and inflammatory erythropoiesis have been related to long-term recovery after COVID-19 [51,52,53]. However, these minerals may show non-linear associations, threshold effects, or closer relationships with circulating biomarkers than with estimated dietary intake. In the case of iodine, its vascular effects are probably indirect and mainly mediated by thyroid function, which could explain the absence of direct associations in this analysis [41,42,43].
Sex-stratified analyses suggested a more consistent pattern of association among women. In women, higher intakes of Fe, Mg, Se, and K were inversely associated with cfPWV, and higher intakes of Mg, Se, and K were associated with lower VAI values. In contrast, no significant associations were observed among men. These findings are consistent with recent studies suggesting sex-related differences in vascular consequences after COVID-19, with a possible greater impairment of arterial elasticity and vascular aging among women [7,9]. Potential explanations include differences in immune activation, endothelial repair, hormonal status, body composition, dietary patterns, and mineral metabolism. However, these findings should be interpreted as exploratory, particularly because formal sex interaction terms did not reach statistical significance. In addition, the smaller number of men may have reduced statistical power to detect subgroup-specific associations.
From a clinical perspective, these findings support the relevance of incorporating nutritional assessment into the follow-up of patients with LC. Arterial stiffness is a recognized marker of subclinical vascular damage and cardiovascular risk [10,11,12], and LC has increasingly been associated with endothelial dysfunction, persistent inflammation, and accelerated vascular aging [4,8]. In this context, dietary mineral intake may represent a modifiable factor related to vascular health. However, the present results do not imply that isolated supplementation should be recommended, nor do they allow causal inference. Rather, they suggest that ensuring adequate dietary intake of key minerals, particularly Mg, Se, and K, within a balanced dietary pattern may be a reasonable strategy to explore in longitudinal studies and nutritional interventions aimed at improving vascular outcomes in patients with LC.
4.1. Limitations and Strengths
This study has several limitations. First, its observational and cross-sectional design precludes the establishment of causal relationships, and reverse causality cannot be ruled out. Second, mineral intake was assessed using a validated 7-day dietary record; although this method provides detailed information, it remains subject to self-reporting bias and may not fully reflect long-term habitual intake. Third, some covariates included in the adjusted models, such as hypertension, may lie on the causal pathway between mineral intake and vascular damage, and adjustment for these variables may therefore have underestimated some associations. Fourth, residual confounding cannot be excluded, particularly due to unrecorded supplementation, renal function, circulating mineral levels, inflammatory biomarkers, hormonal status, or socioeconomic determinants of diet. Another limitation is that mineral intake from dietary supplements was not assessed. Therefore, total mineral exposure may have been underestimated, particularly for minerals commonly consumed as supplements, such as Mg, Ca, Zn, Se, or iodine. Finally, although the sample size was adequate to detect moderate associations, it may have been insufficient to identify small effects, especially in sex-stratified analyses.
Conversely, the strengths of this study include the use of a well-characterized cohort of individuals with LC, the application of a validated dietary assessment tool, the evaluation of multiple complementary markers of vascular stiffness and vascular aging, and the use of fully adjusted multivariable models. Together, these aspects strengthen the relevance of the findings and support the need for future prospective studies and nutritional interventions in this population.
5. Conclusions
Dietary mineral intake was associated with vascular stiffness and vascular aging in adults with LC. Higher intakes of Mg, Se, K, and P were associated with lower cfPWV, K intake was associated with lower baPWV, and Se and P intakes were inversely associated with VAI. Although sex-stratified analyses suggested a more consistent pattern among women, no significant sex interactions were observed. These findings support the hypothesis that adequate mineral intake may represent a potentially relevant nutritional factor for vascular health in LC. However, prospective and interventional studies are required to confirm these results and clarify their clinical relevance.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/doi/s1, Table S1: STROBE checklist. Table S2. The cut-off points used for each mineral. Table 3S. Estimated marginal means of vascular stiffness parameters according to adequate mineral intake in men. Table 4S. Estimated marginal means of vascular stiffness parameters according to adequate mineral intake in women.
Author Contributions
Conceptualization, A.N.-C., E.N.-M., L.G.-S. and M.G.-S.; methodology, M.A.G.-M., S.G.-S. and L.G.-S.; software, M.A.G.-M.; formal analysis, M.A.G.-M. and investigation, A.N-C., S.A-R., N.S-M., and A.D.-M; writing—original draft preparation, A.N.-C., E.N.-M., L.G.-S. and M.G.-S.; All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Spanish Ministry of Science and Innovation, Instituto de Salud Carlos III (ISCIII), through RD21/0016/0018 (Network for Research on Chronicity, Primary Care, and Health Promotion [RICAPPS]), funded by the European Union–Next Generation EU, Recovery and Resilience Facility, and PI25/00071, funded by Instituto de Salud Carlos III (ISCIII) and cofunded by the European Union. Additional funding was provided by the Government of Castilla y León through research projects GRS 2976/C/2024, GRS 3007/C/2024, GRS 2714/C/2023, and GRS 2501/B/22, and by the Institute of Biomedical Research of Salamanca (IBSAL) through project IBYAP23_00001. The CIBER CB22/06/00035 from the area of Respiratory Diseases. The funders had no role in the study design, data analysis, interpretation of the results, manuscript preparation, or the decision to submit the manuscript for publication.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Drug Research Ethics Committee of the Salamanca Health Area (CEIm: Ref. PI 2022 06 1048; dates of approval: 27 June 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting the findings of this study are available on ZENODO at: https://doi.org/10.5281/zenodo.14282873.
Acknowledgments
We would like to thank all members of the BioICOPER.We would also like to thank the patient advisers who collaborated with the study investigators.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| LC | long COVID; WHO, World Health Organization; cfPWV, carotid–femoral pulse wave velocity; baPWV, brachial–ankle pulse wave velocity; VAI, vascular aging index; APISAL, Salamanca Primary Care Research Unit; IBSAL, Biomedical Research Institute of Salamanca; REDCap, Research Electronic Data Capture; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; cIMT, common carotid intima–media thickness; PWV, pulse wave velocity; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; MEDAS, Mediterranean Diet Adherence Screener; SF-36, 36-item Short Form Health Survey; Ca, calcium; P, phosphorus; Mg, magnesium; Fe, iron; Zn, zinc; Na, sodium; K, potassium; I, iodine; Se, selenium; CI, confidence interval; VIF, variance inflation factor. |
References
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Topol, E. Solving the puzzle of Long Covid. Science 2024, 383, 830–832. [Google Scholar] [CrossRef]
- Gelhorn, H.L.; Ghafoori, P.; Cutts, K.; Birch, H.; Savva, Y.; Satram, S.; Lloyd, E.; Chen, W.H. Characterizing health-related quality of life and identifying disease predictors among patients suspected of having long COVID: an analysis of COMET-ICE clinical trial data. Front Public Health 2024, 12, 1278106. [Google Scholar] [CrossRef]
- Stojanovic, M.; Djuric, M.; Nenadic, I.; Bojic, S.; Andrijevic, A.; Popovic, A.; Pesic, S. Vascular Complications of Long COVID-From Endothelial Dysfunction to Systemic Thrombosis: A Systematic Review. Int. J. Mol. Sci. 2025, 27. [Google Scholar] [CrossRef]
- Cervia-Hasler, C.; Brüningk, S.C.; Hoch, T.; Fan, B.; Muzio, G.; Thompson, R.C.; Ceglarek, L.; Meledin, R.; Westermann, P.; Emmenegger, M.; et al. Persistent complement dysregulation with signs of thromboinflammation in active Long Covid. Science 2024, 383, eadg7942. [Google Scholar] [CrossRef]
- Arroyo-Romero, S.; Gomez-Sanchez, L.; Suarez-Moreno, N.; Navarro-Caceres, A.; Dominguez-Martin, A.; Lugones-Sanchez, C.; Gonzalez-Sanchez, S.; Gomez-Sanchez, M.; Rodriguez-Sanchez, E.; Garcia-Ortiz, L.; et al. Clinical Manifestations of Subjects with Long COVID and Their Associations with Drug Use: The BioICOPER Study. Biomedicines 2026, 14. [Google Scholar] [CrossRef] [PubMed]
- Bruno, R.M.; Badhwar, S.; Abid, L.; Agharazii, M.; Anastasio, F.; Bellien, J.; Burghuber, O.; Faconti, L.; Filipovsky, J.; Ghiadoni, L.; et al. Accelerated vascular ageing after COVID-19 infection: the CARTESIAN study. Eur. Heart J. 2025, 46, 3905–3918. [Google Scholar] [CrossRef]
- Theresa, C.; Katebe, B.; Shibao, C.A.; Kirabo, A. Arterial stiffness in adults with Long COVID in sub-Saharan Africa. Physiol. Rep. 2024, 12, e70029. [Google Scholar] [CrossRef]
- Durieux, J.C.; Zisis, S.N.; Mouchati, C.; Labbato, D.; Abboud, M.; McComsey, G.A. Sex Modifies the Effect of COVID-19 on Arterial Elasticity. Viruses 2024, 16. [Google Scholar] [CrossRef]
- Ohkuma, T.; Ninomiya, T.; Tomiyama, H.; Kario, K.; Hoshide, S.; Kita, Y.; Inoguchi, T.; Maeda, Y.; Kohara, K.; Tabara, Y.; et al. Brachial-Ankle Pulse Wave Velocity and the Risk Prediction of Cardiovascular Disease: An Individual Participant Data Meta-Analysis. Hypertension 2017, 69, 1045–1052. [Google Scholar] [CrossRef]
- Li, J.; Gao, F.; Cao, F.; Lv, S.; Hou, Y.; Guo, W.; Zhang, C.; Liu, A. Association of estimated pulse wave velocity with cardiovascular disease outcomes and all-cause death-a systematic review and meta-analysis. Front Cardiovasc Med. 2025, 12, 1641697. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.; Protogerou, A.D.; et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 Practice Guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 2018, 36, 2284–2309. [Google Scholar] [CrossRef]
- Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: 'establishing normal and reference values'. Eur. Heart J. 2010, 31, 2338–2350. [CrossRef] [PubMed]
- Yamashina, A.; Tomiyama, H.; Takeda, K.; Tsuda, H.; Arai, T.; Hirose, K.; Koji, Y.; Hori, S.; Yamamoto, Y. Validity, reproducibility, and clinical significance of noninvasive brachial-ankle pulse wave velocity measurement. Hypertens. Res. 2002, 25, 359–364. [Google Scholar] [CrossRef]
- Takahashi, K.; Yamamoto, T.; Tsuda, S.; Maruyama, M.; Shirai, K. The Background of Calculating CAVI: Lesson from the Discrepancy Between CAVI and CAVI(0). Vasc. Health Risk Manag 2020, 16, 193–201. [Google Scholar] [CrossRef]
- Nilsson Wadström, B.; Fatehali, A.H.; Engström, G.; Nilsson, P.M. A Vascular Aging Index as Independent Predictor of Cardiovascular Events and Total Mortality in an Elderly Urban Population. Angiology 2019, 70, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Shibata, T.; Mok, Y.; Ballew, S.H.; Tanaka, H.; Matsushita, K. Peripheral vs. Central Arterial Stiffness and Cardiovascular Events in Older Adults: The Atherosclerosis Risk in Communities (ARIC) study. Eur. J. Prev. Cardiol. 2025. [Google Scholar] [CrossRef]
- Pavlova, E.; Atanasov, P.; Ivanov, I.; Dyankov, G. Biomarkers of Oxidative Stress in COVID-19 Patients. Int. J. Mol. Sci. 2025, 26. [Google Scholar] [CrossRef]
- Stanek, A.; Grygiel-Górniak, B.; Brożyna-Tkaczyk, K.; Myśliński, W.; Cholewka, A.; Zolghadri, S. The Influence of Dietary Interventions on Arterial Stiffness in Overweight and Obese Subjects. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Campbell, M.S.; Fleenor, B.S. Whole grain consumption is negatively correlated with obesity-associated aortic stiffness: A hypothesis. Nutrition 2018, 45, 32–36. [Google Scholar] [CrossRef]
- Galmés, S.; Serra, F.; Palou, A. Current State of Evidence: Influence of Nutritional and Nutrigenetic Factors on Immunity in the COVID-19 Pandemic Framework. Nutrients 2020, 12. [Google Scholar] [CrossRef]
- Marques, B.; Klein, M.; da Cunha, M.R.; de Souza Mattos, S.; de Paula Nogueira, L.; de Paula, T.; Corrêa, F.M.; Oigman, W.; Neves, M.F. Effects of Oral Magnesium Supplementation on Vascular Function: A Systematic Review and Meta-analysis of Randomized Controlled Trials. High Blood Press Cardiovasc Prev. 2020, 27, 19–28. [Google Scholar] [CrossRef]
- Matek Sarić, M.; Sorić, T.; Juko Kasap, Ž.; Lisica Šikić, N.; Mavar, M.; Andruškienė, J.; Sarić, A. Magnesium: Health Effects, Deficiency Burden, and Future Public Health Directions. Nutrients 2025, 17. [Google Scholar] [CrossRef]
- Nielsen, F.H. The Role of Dietary Magnesium in Cardiovascular Disease. Nutrients 2024, 16. [Google Scholar] [CrossRef]
- Lin, B.; Alexander, R.; Fritzen, R.; Mills, S.; Stewart, A.J.; McCowan, C. Abnormal Plasma/Serum Magnesium, Copper, and Zinc Concentrations Associate with the Future Development of Cardiovascular Diseases. Nutrients 2025, 17. [Google Scholar] [CrossRef]
- Mazza, E.; Maurotti, S.; Ferro, Y.; Castagna, A.; Pujia, C.; Sciacqua, A.; Pujia, A.; Montalcini, T. Magnesium: Exploring Gender Differences in Its Health Impact and Dietary Intake. Nutrients 2025, 17. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Micke, O.; Simental-Mendía, L.E.; Rodríguez-Morán, M.; Vormann, J.; Iotti, S.; Banjanin, N.; Rosanoff, A.; Baniasadi, S.; Pourdowlat, G.; et al. Importance of Magnesium Status in COVID-19. Biology 2023, 12. [Google Scholar] [CrossRef]
- Schutten, J.C.; Joris, P.J.; Groendijk, I.; Eelderink, C.; Groothof, D.; van der Veen, Y.; Westerhuis, R.; Goorman, F.; Danel, R.M.; de Borst, M.H.; et al. Effects of Magnesium Citrate, Magnesium Oxide, and Magnesium Sulfate Supplementation on Arterial Stiffness: A Randomized, Double-Blind, Placebo-Controlled Intervention Trial. J. Am. Heart Assoc. 2022, 11, e021783. [Google Scholar] [CrossRef]
- La Carrubba, A.; Veronese, N.; Di Bella, G.; Cusumano, C.; Di Prazza, A.; Ciriminna, S.; Ganci, A.; Naro, L.; Dominguez, L.J.; Barbagallo, M.; et al. Prognostic Value of Magnesium in COVID-19: Findings from the COMEPA Study. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Zhao, K.; Qiao, L.; Hu, W.; Sui, W.; Li, X.; Zhang, G. Association between circulating selenium levels and arterial stiffness: a nationwide cross-sectional study. Int. J. Surg. 2026, 112, 202–212. [Google Scholar] [CrossRef]
- Hawkes, W.C.; Laslett, L.J. Selenium supplementation does not improve vascular responsiveness in healthy North American men. Am. J. Physiol. Heart Circ. Physiol. 2009, 296, H256–262. [Google Scholar] [CrossRef]
- Golin, A.; Tinkov, A.A.; Aschner, M.; Farina, M.; da Rocha, J.B.T. Relationship between selenium status, selenoproteins and COVID-19 and other inflammatory diseases: A critical review. J. Trace Elem. Med. Biol. 2023, 75, 127099. [Google Scholar] [CrossRef]
- Fakhrolmobasheri, M.; Mazaheri-Tehrani, S.; Kieliszek, M.; Zeinalian, M.; Abbasi, M.; Karimi, F.; Mozafari, A.M. COVID-19 and Selenium Deficiency: a Systematic Review. Biol. Trace Elem. Res. 2022, 200, 3945–3956. [Google Scholar] [CrossRef]
- Schomburg, L. Selenium Deficiency in COVID-19-A Possible Long-Lasting Toxic Relationship. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Moghaddam, A.; Heller, R.A.; Sun, Q.; Seelig, J.; Cherkezov, A.; Seibert, L.; Hackler, J.; Seemann, P.; Diegmann, J.; Pilz, M.; et al. Selenium Deficiency Is Associated with Mortality Risk from COVID-19. Nutrients 2020, 12. [Google Scholar] [CrossRef]
- Delitala, A.P.; Orrù, M.; Filigheddu, F.; Pilia, M.G.; Delitala, G.; Ganau, A.; Saba, P.S.; Decandia, F.; Scuteri, A.; Marongiu, M.; et al. Serum free thyroxine levels are positively associated with arterial stiffness in the SardiNIA study. Clin. Endocrinol. (Oxf) 2015, 82, 592–597. [Google Scholar] [CrossRef]
- Maldonado-Araque, C.; Valdés, S.; Badía-Guillén, R.; Lago-Sampedro, A.; Colomo, N.; Garcia-Fuentes, E.; Gutierrez-Repiso, C.; Goday, A.; Calle-Pascual, A.; Castaño, L.; et al. Iodine Deficiency and Mortality in Spanish Adults: Di@bet.es Study. Thyroid 2021, 31, 106–114. [Google Scholar] [CrossRef]
- Panesar, A.; Gharanei, P.; Khovanova, N.; Young, L.; Grammatopoulos, D. Thyroid function during COVID-19 and post-COVID complications in adults: a systematic review. Front Endocrinol. 2024, 15, 1477389. [Google Scholar] [CrossRef]
- Nohara-Shitama, Y.; Mok, Y.; Ballew, S.H.; Rebholz, C.M.; Budoff, M.J.; Anderson, C.; Ishigami, J.; Blaha, M.J.; Matsushita, K. Associations of Dietary Calcium and Phosphorus With Vascular and Valvular Calcification: The ARIC Study. JACC Adv. 2024, 3, 100993. [Google Scholar] [CrossRef]
- Villa-Bellosta, R. Vascular Calcification: Key Roles of Phosphate and Pyrophosphate. Int. J. Mol. Sci. 2021, 22. [Google Scholar] [CrossRef]
- Turner, M.E.; Beck, L.; Hill Gallant, K.M.; Chen, Y.; Moe, O.W.; Kuro, O.M.; Moe, S.M.; Aikawa, E. Phosphate in Cardiovascular Disease: From New Insights Into Molecular Mechanisms to Clinical Implications. Arterioscler. Thromb. Vasc. Biol. 2024, 44, 584–602. [Google Scholar] [CrossRef]
- Anghel, L.; Manole, C.; Nechita, A.; Tatu, A.L.; Ștefănescu, B.I.; Nechita, L.; Bușilă, C.; Zainea, P.; Baroiu, L.; Mușat, C.L. Calcium, Phosphorus and Magnesium Abnormalities Associated with COVID-19 Infection, and Beyond. Biomedicines 2023, 11. [Google Scholar] [CrossRef]
- D'Elia, L.; Galletti, F.; La Fata, E.; Sabino, P.; Strazzullo, P. Effect of dietary sodium restriction on arterial stiffness: systematic review and meta-analysis of the randomized controlled trials. J. Hypertens. 2018, 36, 734–743. [Google Scholar] [CrossRef]
- D'Elia, L.; Cappuccio, F.P.; Masulli, M.; La Fata, E.; Rendina, D.; Galletti, F. Effect of Potassium Supplementation on Endothelial Function: A Systematic Review and Meta-Analysis of Intervention Studies. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Song, H.; Chia, A.Z.Q.; Tan, B.K.J.; Teo, C.B.; Lim, V.; Chua, H.R.; Samuel, M.; Kee, A. Electrolyte imbalances as poor prognostic markers in COVID-19: a systemic review and meta-analysis. J. Endocrinol. Invest 2023, 46, 235–259. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, S.; Gu, X.; Qiu, H.; Zhang, Y. L-shaped association between dietary zinc intake and the risk of developing cardiovascular disease in Chinese adults: A cohort study. Front Nutr. 2023, 10, 1032048. [Google Scholar] [CrossRef]
- Ishioka, K.; Hidaka, S.; Fujiwara, N.; Yamano, M.; Mochida, Y.; Oka, M.; Maesato, K.; Moriya, H.; Ohtake, T.; Kobayashi, S. Association between zinc deficiency and aorta stiffness in non-diabetic hemodialysis patients. PLoS ONE 2023, 18, e0268875. [Google Scholar] [CrossRef] [PubMed]
- Hung, L.W.; Liu, M.Y.; Yu, T.; Hung, K.C.; Tsai, Y.W.; Lai, C.C.; Wu, J.Y. Zinc Deficiency and Post-acute Outcomes in Patients With COVID-19: A Six-Month Retrospective Cohort Analysis of 3,726 Patients. Cureus 2024, 16, e71609. [Google Scholar] [CrossRef] [PubMed]
- Valenti, L.; Maloberti, A.; Signorini, S.; Milano, M.; Cesana, F.; Cappellini, F.; Dongiovanni, P.; Porzio, M.; Soriano, F.; Brambilla, M.; et al. Iron Stores, Hepcidin, and Aortic Stiffness in Individuals with Hypertension. PLoS ONE 2015, 10, e0134635. [Google Scholar] [CrossRef] [PubMed]
- Qiao, W.; Liu, Q.; Ding, H.; Wang, G.; Sun, Y.; Yao, Z.; Huang, X.; Wang, X.; Fu, C.; Hou, J. The Role of Iron and Other Micronutrients in Arterial Stiffness: Univariable and Multivariable Mendelian Randomization. Rev. Cardiovasc Med. 2025, 26, 27920. [Google Scholar] [CrossRef] [PubMed]
- Hanson, A.L.; Mulè, M.P.; Ruffieux, H.; Mescia, F.; Bergamaschi, L.; Pelly, V.S.; Turner, L.; Kotagiri, P.; Göttgens, B.; Hess, C.; et al. Iron dysregulation and inflammatory stress erythropoiesis associates with long-term outcome of COVID-19. Nat. Immunol. 2024, 25, 471–482. [Google Scholar] [CrossRef]
- Recio-Rodriguez, J.I.; Rodriguez-Martin, C.; Gonzalez-Sanchez, J.; Rodriguez-Sanchez, E.; Martin-Borras, C.; Martínez-Vizcaino, V.; Arietaleanizbeaskoa, M.S.; Magdalena-Gonzalez, O.; Fernandez-Alonso, C.; Maderuelo-Fernandez, J.A.; et al. EVIDENT Smartphone App, a New Method for the Dietary Record: Comparison With a Food Frequency Questionnaire. JMIR Mhealth Uhealth 2019, 7, e11463. [Google Scholar] [CrossRef]
- Gómez-Sánchez, L.; Tamayo-Morales, O.; Suárez-Moreno, N.; Bermejo-Martín, J.F.; Domínguez-Martín, A.; Martín-Oterino, J.A.; Martín-González, J.I.; González-Calle, D.; García-García, Á.; Lugones-Sánchez, C.; et al. Relationship between the structure, function and endothelial damage, and vascular ageing and the biopsychological situation in adults diagnosed with persistent COVID (BioICOPER study). A research protocol of a cross-sectional study. Front Physiol. 2023, 14, 1236430. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, N., and Allergies (NDA) Scientific Opinion on Dietary Reference Values for carbohy-drates and dietary fibre. EFSA J. 2010a, 8((3) 8), 1462.
- EFSA Panel on Dietetic Products, N., and Allergies (NDA). Scientific Opinion on Dietary Reference Values for fats, includ-ing saturated fatty acids, polyunsaturated fatty acids, monounsaturated fatty acids, trans fatty acids, and cholesterol. EFSA J. 8(3), 1462 2010b, 8.
- Gómez-Marcos, M.A.; Recio-Rodríguez, J.I.; Patino-Alonso, M.C.; Agudo-Conde, C.; Gómez-Sanchez, L.; Gómez-Sanchez, M.; Rodríguez-Sánchez, E.; García-Ortiz, L. Protocol for measuring carotid intima-media thickness that best correlates with cardiovascular risk and target organ damage. Am. J. Hypertens. 2012, 25, 955–961. [Google Scholar] [CrossRef]
- The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): a major international collaboration. WHO MONICA Project Principal Investigators. J. Clin. Epidemiol. 1988, 41, 105–114. [CrossRef]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): a systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef]
- Alonso, J.; Prieto, L.; Antó, J.M. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): an instrument for measuring clinical results. Med. Clin. (Barc) 1995, 104, 771–776. [Google Scholar]
- World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Participants. Jama 2025, 333, 71–74. [CrossRef]
- Olza, J.; Aranceta-Bartrina, J.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, Á. Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Olza, J.; Aranceta-Bartrina, J.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, Á. Reported Dietary Intake and Food Sources of Zinc, Selenium, and Vitamins A, E and C in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Passarelli, S.; Free, C.M.; Shepon, A.; Beal, T.; Batis, C.; Golden, C.D. Global estimation of dietary micronutrient inadequacies: a modelling analysis. Lancet Glob. Health 2024, 12, e1590–e1599. [Google Scholar] [CrossRef]
Figure 1.
| Flowchart of participant selection, including inclusion and exclusion criteria, in the BioICOPER study.
Figure 1.
| Flowchart of participant selection, including inclusion and exclusion criteria, in the BioICOPER study.

Figure 2.
Percentage of participants meeting mineral intake recommendations in the overall sample and by sex. Bars represent the proportion of participants with adequate intake for each mineral. Asterisks indicate statistically significant differences between women and men according to Pearson’s chi-square test: **p<0.01; ***p<0.001 Abbreviations: Fe, iron; Mg, magnesium; Se, selenium; I, iodine; Na, sodium; K, potassium; Ca, calcium; P, phosphorus; Zn, zinc.
Figure 2.
Percentage of participants meeting mineral intake recommendations in the overall sample and by sex. Bars represent the proportion of participants with adequate intake for each mineral. Asterisks indicate statistically significant differences between women and men according to Pearson’s chi-square test: **p<0.01; ***p<0.001 Abbreviations: Fe, iron; Mg, magnesium; Se, selenium; I, iodine; Na, sodium; K, potassium; Ca, calcium; P, phosphorus; Zn, zinc.

Figure 3.
Association between dietary mineral intake and carotid–femoral pulse wave velocity (cfPWV). The plot shows unstandardized β coefficients and 95% confidence intervals derived from multivariable linear regression models assessing the association between dietary mineral intake and cfPWV. Red markers indicate significant inverse associations (p < 0.05), whereas black markers indicate non-significant associations. cfPWV: carotid–femoral pulse wave velocity; CI: confidence interval.En la figura 4 se muestra la asociación entre baPWV y los minerales. La ingesta de K mostro asociación negativa con la baPWV.
Figure 3.
Association between dietary mineral intake and carotid–femoral pulse wave velocity (cfPWV). The plot shows unstandardized β coefficients and 95% confidence intervals derived from multivariable linear regression models assessing the association between dietary mineral intake and cfPWV. Red markers indicate significant inverse associations (p < 0.05), whereas black markers indicate non-significant associations. cfPWV: carotid–femoral pulse wave velocity; CI: confidence interval.En la figura 4 se muestra la asociación entre baPWV y los minerales. La ingesta de K mostro asociación negativa con la baPWV.

Figure 4.
Association between dietary mineral intake and brachial–ankle pulse wave velocity (baPWV). The plot shows unstandardized β coefficients and 95% confidence intervals derived from multivariable linear regression models evaluating the association between dietary mineral intake and baPWV. Red markers indicate statistically significant inverse associations (p < 0.05), whereas black markers indicate non-significant associations. baPWV: brachial–ankle pulse wave velocity; CI: confidence interval.
Figure 4.
Association between dietary mineral intake and brachial–ankle pulse wave velocity (baPWV). The plot shows unstandardized β coefficients and 95% confidence intervals derived from multivariable linear regression models evaluating the association between dietary mineral intake and baPWV. Red markers indicate statistically significant inverse associations (p < 0.05), whereas black markers indicate non-significant associations. baPWV: brachial–ankle pulse wave velocity; CI: confidence interval.

Figure 5.
Association between dietary mineral intake and vascular aging index (VAI). The plot shows unstandardized β coefficients and 95% confidence intervals derived from multivariable linear regression models evaluating the association between dietary mineral intake and VAI. Red markers indicate statistically significant inverse associations (p < 0.05), whereas black markers indicate non-significant associations. VAI: vascular aging index; CI: confidence interval.
Figure 5.
Association between dietary mineral intake and vascular aging index (VAI). The plot shows unstandardized β coefficients and 95% confidence intervals derived from multivariable linear regression models evaluating the association between dietary mineral intake and VAI. Red markers indicate statistically significant inverse associations (p < 0.05), whereas black markers indicate non-significant associations. VAI: vascular aging index; CI: confidence interval.

Figure 6.
Sex-stratified associations between dietary mineral intake and carotid–femoral pulse wave velocity (cfPWV). Data are presented as unstandardized β coefficients and 95% confidence intervals. cfPWV: carotid–femoral pulse wave velocity; CI: confidence interval.
Figure 6.
Sex-stratified associations between dietary mineral intake and carotid–femoral pulse wave velocity (cfPWV). Data are presented as unstandardized β coefficients and 95% confidence intervals. cfPWV: carotid–femoral pulse wave velocity; CI: confidence interval.

Figure 7.
Sex-stratified association between dietary mineral intake and brachial–ankle pulse wave velocity (baPWV). Unstandardized β coefficients and 95% confidence intervals are shown for each mineral according to sex. baPWV: brachial–ankle pulse wave velocity; CI: confidence interval.
Figure 7.
Sex-stratified association between dietary mineral intake and brachial–ankle pulse wave velocity (baPWV). Unstandardized β coefficients and 95% confidence intervals are shown for each mineral according to sex. baPWV: brachial–ankle pulse wave velocity; CI: confidence interval.

Figure 8.
Sex-stratified association between dietary mineral intake and vascular aging index (VAI). Unstandardized β coefficients and 95% confidence intervals are shown for each mineral according to sex. Statistically significant associations were defined as p < 0.05. VAI: vascular aging index; CI: confidence interval.
Figure 8.
Sex-stratified association between dietary mineral intake and vascular aging index (VAI). Unstandardized β coefficients and 95% confidence intervals are shown for each mineral according to sex. Statistically significant associations were defined as p < 0.05. VAI: vascular aging index; CI: confidence interval.


Table 1.
General characteristics in subjects with LC, overall and by sex.
| Variable | Overall (n=304) | Men (n=97) | Women (n=207) | p |
| Age, years (mean ± SD) | 52.71 ± 11.94 | 55.70 ± 12.28 | 51.32 ± 11.54 | 0.001 |
| Time of evolution, months (mean ± SD) | 38.66 ± 9.58 | 38.50 ± 9.96 | 38.74 ± 9.41 | 0.990 |
| SF-36 HTS, mean ±SD | 50.34 ±25.46 | 51.84 ±25.06 | 49.63 ±25.67 | 0.486 |
| Alcohol, g/week (mean ± SD) | 29.35 ± 52.87 | 60.39 ± 76.35 | 14.88 ± 27.19 | <0.001 |
| No alcohol consumption (n, %) | 163 (53.6) | 36 (37.1) | 127 (61.4) | <0.001 |
| MD score (mean ± SD) | 7.80 ± 2.33 | 7.71 ± 2.23 | 7.84 ± 2.39 | 0.437 |
| MD adherence (n, %) | 123 (40.50) | 38 (39.2) | 85 (41.1) | 0.427 |
| MET-min/week | 1226 ± 126 | 1358 ± 196 | 1164 ± 75 | 0.377 |
| Current smoker, (n, %) | 17 (5.7) | 8 (8.4) | 9 (4.5) | 0.065 |
| SBP, mmHg (mean ± SD) | 119.95 ± 16.75 | 129.45 ± 14.37 | 115.52 ± 15.94 | <0.001 |
| DBP, mmHg (mean ± SD) | 76.85 ± 11.11 | 82.34 ± 11.04 | 74.30 ± 10.20 | <0.001 |
| Hypertension, (n, %) | 109 (35.9) | 52 (53.6) | 57 (27.5) | <0.001 |
| Total cholesterol, mg/dL (mean ± SD) | 187.45 ± 34.30 | 182.11 ± 32.94 | 189.95 ± 34.71 | 0.029 |
| LDL-c, mg/dL (mean ± SD) | 113.03 ± 31.76 | 113.59 ± 32.12 | 112.77 ± 31.67 | 0.417 |
| HDL-c, mg/dL (mean ± SD) | 56.92 ± 13.58 | 48.78 ± 10.86 | 60.73 ± 13.06 | <0.001 |
| Triglycerides, mg/dL (mean ± SD) | 102.23 ± 50.81 | 117.47 ± 54.39 | 95.09 ± 47.52 | <0.001 |
| Dyslipidemia, (n, %) | 201 (66.3) | 71 (73.2) | 130 (63.1) | 0.053 |
| FPG, mg/dL (mean ± SD) | 87.88 ± 17.67 | 94.37 ± 19.77 | 84.84 ± 15.74 | <0.001 |
| Diabetes mellitus, (n, %) | 37 (12.2) | 22 (22.7) | 15 (7.3) | <0.001 |
| Weight, kg (mean ± SD) | 75.95 ± 17.39 | 88.09 ± 14.95 | 70.29 ± 15.46 | <0.001 |
| Height, cm (mean ± SD) | 164.50 ± 8.71 | 172.51 ± 7.35 | 160.77 ± 6.52 | <0.001 |
| BMI, kg/m² (mean ± SD) | 27.97 ± 5.55 | 29.60 ± 4.64 | 27.21 ± 5.78 | <0.001 |
| Obesity, (n, %) | 99 (32.5) | 44 (45.4) | 55 (26.4) | <0.001 |
| cIMT, mm | 0.64 ± 0.09 | 0.68 ± 0.12 | 0.62 ± 0.07 | <0.001 |
| cfPWV, m/s | 7.67 ± 2.36 | 8.85 ± 2.95 | 7.12 ± 1.79 | <0.001 |
| baPWV, m/s | 12.79 ± 2.38 | 13.63 ± 2.40 | 12.40 ± 2.27 | <0.001 |
| VAI | 65.54 ± 13.75 | 72.89 ± 16.66 | 62.13 ± 10.59 | <0.001 |
Continuous variables are presented as mean ± standard deviation, between-sex comparisons were performed using Student’s t test. Categorical variables are shown as n (%) and were compared with χ² or Fisher’s exact test, as appropriate. A p-value < 0.05 was considered statistically significant. Abbreviations: SD, Standard Deviation; SF-36 HTS, Short Form-36 Health Transition Score; MD, Mediterranean Diet; MET, Metabolic Equivalent; SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure; LDL, Low–Density Lipoprotein; HDL, High–Density Lipoprotein; FPG, Fasting Plasma Glucose; BMI, Body Mass Index; cIMT: Intima–Media Thickness of Common Carotid; cfPWV, Carotid-Femoral Pulse Wave Velocity; baPWV, Brachial-Ankle Pulse Wave Velocity; VAI, Vascular Aging Index.
Table 2.
Mineral Intake, overall and by Sex.
| Variable | Overall (n=304) | Men (n=97) | Women (n=207) | P value |
| Fe, mg | 13.82 ± 4.03 | 13.90 ± 4.39 | 13.78 ± 3.86 | 0.830 |
| Mg, mg | 288.15 ± 82.32 | 287.78 ± 88.73 | 288.32 ± 79.35 | 0.960 |
| Se, µg | 99.91 ± 36.76 | 105.03 ± 39.29 | 97.50 ± 35.34 | 0.118 |
| I, µg | 98.78 ± 39.29 | 101.18 ± 41.57 | 97.65 ± 38.18 | 0.490 |
| Na, mg | 3012 ± 1148 | 3135 ± 1259 | 2954 ± 1090 | 0.235 |
| K, mg | 3149 ± 900 | 3179 ± 950 | 3135 ± 877 | 0.705 |
| Ca, mg | 767 ± 275 | 769 ± 267 | 767 ± 279 | 0.947 |
| P, mg | 429 ± 183 | 450 ± 204 | 419 ± 172 | 0.270 |
| Zn, mg | 9.62 ± 2.76 | 9.65 ± 2.96 | 9.61 ± 2.67 | 0.923 |
Continuous variables are presented as mean ± standard deviation (SD). Fe, iron; Mg, magnesium; Se, selenium; I, iodine; Na, sodium; K, potassium; Ca, calcium; P, phosphorus; Zn, zinc.
Table 3.
Estimated marginal means of vascular stiffness and vascular aging parameters according to adequate mineral intake.
Table 3.
Estimated marginal means of vascular stiffness and vascular aging parameters according to adequate mineral intake.
| Mineral | Vascular parameter | Inadequate/risk EMM (95% CI) | Adequate EMM (95% CI) | p value |
| Fe | cfPWV | 8.38 (7.96–8.81) | 7.88 (7.53–8.22) | 0.065 |
| Fe | baPWV | 13.26 (12.89–13.62) | 12.80 (12.50–13.09) | 0.049 |
| Fe | VAI | 69.65 (67.34–71.96) | 66.92 (65.05–68.78) | 0.065 |
| Mg | cfPWV | 8.24 (7.93–8.56) | 7.66 (7.19–8.13) | 0.037 |
| Mg | baPWV | 13.03 (12.76–13.30) | 12.81 (12.41–13.22) | 0.362 |
| Mg | VAI | 68.74 (67.03–70.45) | 66.00 (63.44–68.57) | 0.070 |
| Se | cfPWV | 8.43 (7.83–9.03) | 7.99 (7.70–8.29) | 0.192 |
| Se | baPWV | 13.06 (12.55–13.57) | 12.95 (12.69–13.20) | 0.694 |
| Se | VAI | 69.70 (66.43–72.97) | 67.56 (65.96–69.17) | 0.237 |
| I | cfPWV | 8.09 (7.81–8.38) | 7.88 (7.04–8.71) | 0.633 |
| I | baPWV | 12.94 (12.70–13.19) | 13.20 (12.49–13.91) | 0.499 |
| I | VAI | 68.09 (66.54–69.64) | 66.59 (62.09–71.08) | 0.531 |
| Na | cfPWV | 8.01 (7.71–8.30) | 8.44 (7.78–9.10) | 0.226 |
| Na | baPWV | 12.94 (12.69–13.19) | 13.12 (12.56–13.69) | 0.555 |
| Na | VAI | 67.61 (66.03–69.19) | 69.86 (66.26–73.46) | 0.250 |
| K | cfPWV | 8.14 (7.82–8.46) | 7.92 (7.44–8.39) | 0.436 |
| K | baPWV | 13.03 (12.76–13.31) | 12.82 (12.41–13.22) | 0.365 |
| K | VAI | 68.16 (66.42–69.90) | 67.44 (64.87–70.00) | 0.637 |
| Ca | cfPWV | 8.18 (7.88–8.48) | 7.66 (7.10–8.23) | 0.103 |
| Ca | baPWV | 13.01 (12.75–13.26) | 12.84 (12.36–13.33) | 0.543 |
| Ca | VAI | 68.47 (66.84–70.10) | 66.13 (63.07–69.19) | 0.173 |
| P | cfPWV | 8.14 (7.83–8.44) | 7.84 (7.29–8.40) | 0.351 |
| P | baPWV | 12.93 (12.67–13.18) | 13.12 (12.64–13.58) | 0.479 |
| P | VAI | 68.23 (66.57–69.88) | 66.92 (63.92–69.93) | 0.445 |
| Zn | cfPWV | 8.21 (7.82–8.61) | 7.94 (7.55–8.32) | 0.327 |
| Zn | baPWV | 12.90 (12.57–13.24) | 13.03 (12.70–13.35) | 0.608 |
| Zn | VAI | 68.76 (66.62–70.89) | 67.18 (65.12–69.24) | 0.297 |
Values are expressed as estimated marginal means and 95% confidence intervals. Models were adjusted for age and sex. p values were obtained from pairwise comparisons between participants with inadequate or risk intake and those with adequate intake. Statistically significant results are shown in bold. Abbreviations: EMM, estimated marginal mean; CI, confidence interval; Fe, iron; Mg, magnesium; Se, selenium; I, iodine; Na, sodium; K, potassium; Ca, calcium; P, phosphorus; Zn, zinc; cfPWV, carotid–femoral pulse wave velocity; baPWV, brachial–ankle pulse wave velocity; VAI, vascular aging index; Long COVID.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



