Submitted:
28 May 2026
Posted:
29 May 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
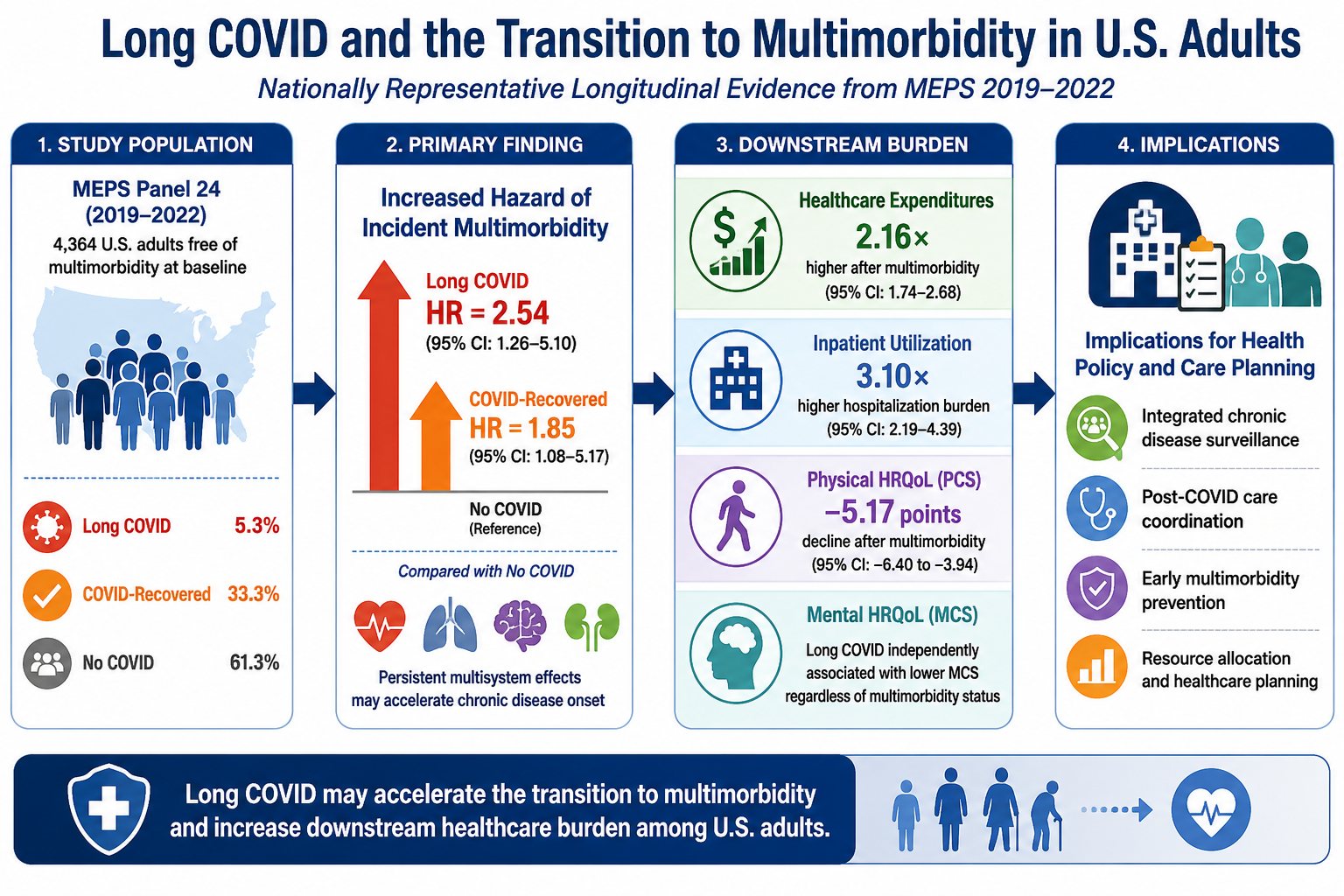
Long COVID has been associated with elevated risks of individual chronic conditions, but its role in the transition to multimorbidity remains unclear. We analyzed MEPS Panel 24 (2019-2022) data from 4,364 adults free of multimorbidity at baseline. COVID-19 exposure was classified as Long COVID, COVID-recovered, or no COVID. Discrete-time survival models estimated incident multimorbidity risk, and generalized estimating equations assessed healthcare expenditures, health-related quality of life, and inpatient utilization. Long COVID was associated with a 2.54-fold higher hazard of incident multimorbidity compared with no COVID (HR = 2.54; 95% CI: 1.26-5.10), while COVID-recovered participants also had elevated hazard (HR = 1.85; 95% CI: 1.08-3.17). Incident multimorbidity onset was associated with lower physical HRQoL, increased inpatient utilization, and higher healthcare expenditures. Long COVID was independently associated with lower mental HRQoL, while evidence for Long COVID-specific expenditure growth was model-dependent. These findings suggest that Long COVID and resolved COVID-19 infection may increase the risk of transitioning into multimorbidity, supporting integrated chronic disease surveillance, mental health assessment, and coordinated post-COVID care.
Keywords:
Long COVID
; post-acute sequelae of SARS-CoV-2
; multimorbidity
; incident chronic disease
; discrete-time survival analysis
; health-related quality of life
; healthcare expenditures
; MEPS
1. Introduction
The 2019 coronavirus pandemic (SARS-CoV-2) is one of the most important public health issues of the last few decades, attributable to over 770 million confirmed infections and around seven million global deaths as of 2024(World Health Organization, 2026). While much attention has been focused on understanding the nature of the disease itself, less emphasis has been placed on what happens to its survivors. Many individuals who recover from acute illness later experience lingering symptoms lasting several months or years after infection, known as Post-COVID Condition, or Long COVID (Nalbandian et al., 2021; Soriano et al., 2022). According to the World Health Organization (WHO), Long COVID is defined as the symptoms persisting three or more months after infection, lasting at least two additional months, and unexplained by an alternative diagnosis (Soriano et al., 2022). Between 10% and 30% of survivors experience persistent symptoms meeting this criterion, with variation reflecting differences in case ascertainment methods, variant exposure, and vaccination status across studies (Antonelli et al., 2022; Thaweethai et al., 2023). The economic consequences are substantial: (Cutler, 2022) estimated the present value of Long COVID-related costs in the United States at approximately $3.7 trillion, underscoring the urgency of understanding its long-term health sequelae. Long COVID's clinical phenotype is heterogeneous, including fatigue, cognitive impairment, dyspnea, cardiovascular autonomic dysfunction, and neurological, immunological, and musculoskeletal complications (Davis et al., 2023). Mechanistic investigations implicate viral persistence, immune dysregulation, reactivation of latent herpesviruses, disruption of the microbiome, vascular endothelial damage, and chronic neuroinflammation (Davis et al., 2023; Proal and VanElzakker, 2021). Critically, these pathophysiological pathways do not operate within a single organ system; they converge simultaneously on cardiovascular, respiratory, metabolic, neurological, and oncologic domains, creating biological conditions conducive to multi-system chronic disease (Proal and VanElzakker, 2021; Tran et al., 2022). Large-scale analyses using electronic health records and veterans affairs data have documented that COVID-19 survivors face significantly elevated risks of incident cardiovascular events, type 2 diabetes, chronic kidney disease, and neurological disorders, with risks appearing larger among individuals with Long COVID than among those who recovered, though residual confounding cannot be excluded in these observational studies (Al-Aly et al., 2022; Bowe et al., 2021; Xie et al., 2022).
Multimorbidity (MM), defined as the coexistence of two or more chronic conditions, represents a growing public health concern in the United States. According to recent data from the Centers for Disease Control and Prevention (CDC), almost one in every ten American adults has at least one chronic disease, and more than half of these report multiple chronic conditions, accounting for most of the national healthcare expenditures and healthcare utilization (Aborode et al., 2025; Watson et al., 2025). MM has emerged as a defining twenty-first-century healthcare challenge, affecting 25-40% of adults in high-income countries (Barnett et al., 2012). Its consequences extend well beyond additive single-condition burden: multimorbid individuals experience substantially greater healthcare utilization, higher expenditures, accelerated functional decline, and markedly reduced health-related quality of life (Barnett et al., 2012; Salisbury et al., 2011; Vogeli et al., 2007). The transition from absent or limited chronic disease to MM represents a pivotal inflection point at which complexity, costs, and trajectories of quality of life diverge sharply. Understanding what precipitates this transition is therefore of fundamental importance to chronic disease prevention and health systems planning (Wolff et al., 2002).
Primary care serves as the principal point of contact for most COVID-19 survivors seeking ongoing management in community settings. The transition from single-condition chronic disease to MM represents a clinical inflection point at which care complexity escalates with competing treatment priorities, polypharmacy risk, and the burden of coordinated referral concentrated within general practice. Despite this front-line role, much of the existing longitudinal evidence on post-COVID sequelae has been generated from specialist registers, tertiary-care electronic health record networks, or veterans affairs databases, which may not adequately represent the broader community-dwelling population whose primary contact with the healthcare system is through general practice. Nationally representative longitudinal data from community-based surveillance systems offer a complementary perspective directly relevant to how primary care teams assess post-COVID chronic disease risk, identify patients approaching the MM threshold, and design follow-up care pathways for this growing population.
Although individual post-COVID conditions have been well characterized, the literature has often examined them in isolation. Whether COVID-19 exposure and Long COVID in particular drive the simultaneous or proximal onset of multiple conditions across distinct physiological domains (incident MM) remains substantially underexamined (Davis et al., 2023; Tran et al., 2022). Prior Medical Expenditure Panel Survey (MEPS) based research established MM cluster profiles and their associations with expenditure and quality of life in participants (Alliu et al., 2025), providing a methodological reference point against which COVID-era shifts can be assessed. However, no nationally representative longitudinal study has employed a discrete-time survival framework to formally test whether COVID-19 exposure predicts the transition to MM, nor has it quantified the downstream burden consequences across expenditure, quality of life, and utilization outcomes simultaneously.
To address these gaps, we used MEPS Panel 24 (2019-2022) to examine three interrelated questions: whether Long COVID independently predicts the hazard of incident MM relative to COVID-recovered and no-COVID groups; whether the phenotype of MM at onset differs by COVID-19 exposure status; and whether post-onset trajectories of healthcare expenditures, health-related quality of life, and inpatient utilization vary across exposure groups. Together, these analyses provide a nationally representative longitudinal basis for understanding Long COVID as a potential contributor to chronic disease complexity and for informing healthcare planning and prevention policy.
2. Materials and Methods
2.1. Study Design and Data Source
This prospective longitudinal cohort study used MEPS Panel 24, which followed a nationally representative sample of U.S. non-institutionalized civilians across four annual rounds (2019–2022). MEPS employs a complex, stratified, multi-stage probability sampling design administered by the U.S. Census Bureau on behalf of AHRQ. Medical expenditures are inflation-adjusted to 2022 USD using the AHRQ Medical Price Index. Health-related quality of life was assessed via the SF-12v2 (Ware et al., 1996), yielding Physical Component Summary (PCS) and Mental Component Summary (MCS) scores standardized to a population mean of 50 (SD=10). All analyses were conducted in SAS 9.4 (SAS Institute Inc., Cary, NC). The study used publicly available de-identified data and was exempt from IRB review.
2.2. Study Population and Eligibility
Of 5,565 Panel 24 participants, 554 (9.96%) were excluded for prevalent MM at the 2019 baseline and an additional 647 for missing COVID-19 status, yielding a final analytic cohort of 4,364 individuals (weighted N≈279.2 million), as illustrated in Figure 1.
2.3. Exposure Classification
COVID-19 exposure was classified using self-reported data on diagnosis and symptom duration into three mutually exclusive groups: Long COVID (symptoms ≥3 months; n=232, 5.3%); COVID-Recovered (infection resolved within 3 months; n=1,455, 33.3%); and No COVID (no reported infection; n=2,677, 61.3%; reference). Exposure classification was established prior to the incident MM assessment window and treated as fixed across follow-up.
2.4. Outcome Definitions
2.4.1. Primary Outcome: Incident MM
Incident MM is defined as the new onset of two or more concurrent chronic conditions across distinct physiological domains (cardiovascular, respiratory, oncologic, cardiometabolic, neurological/musculoskeletal) during 2020-2022 follow-up, among participants free of MM at baseline. Each participant was classified as an incident MM case at the first follow-up round in which this criterion was met and was subsequently right-censored from the risk set. The qualifying conditions assessed were hypertension, coronary heart disease, diabetes, asthma or chronic obstructive pulmonary disease, cancer, and neurological or musculoskeletal conditions. A participant was required to have at least one qualifying condition from each of two or more distinct physiological domains to meet the incident MM criterion; conditions within the same domain did not satisfy the requirement alone.
2.4.2. Multimorbidity Cluster Taxonomy
The classification of MM cluster type at onset was based on a seven-cluster taxonomy proposed by Alliu et al. (2025) using latent class analysis applied to the full MEPS Panel 24 sample. That analysis identified seven empirically distinct MM profiles defined by naturally occurring patterns of chronic condition co-occurrence among U.S. non-institutionalized civilians, without designating any single condition as a primary anchor. The seven clusters are: Cluster 1, neurological and musculoskeletal MM; Cluster 2, cardiometabolic MM; Cluster 3, cardiorespiratory MM; Cluster 4, cancer and neurological MM; Cluster 5, cancer and cardiometabolic MM; Cluster 6, cancer and respiratory MM; and Cluster 7, complex multisystem MM involving three or more physiological domains. The taxonomy was derived prior to and independently of the incident MM analyses reported in the present study and was not modified to fit the observed incident cases. Each incident MM case was assigned to the cluster type that best matched the combination of qualifying conditions present at the first round in which the MM criterion was met. Among the 105 observed incident cases, only three cluster types were empirically represented: Clusters 3, 5, and 6, with the remaining four cluster types having no observed incident cases in this cohort. The analytical implications of this sparsity are described in the statistical analysis section.
2.4.3. Secondary Outcomes: Downstream Burden Trajectories
Five downstream burden outcomes were assessed across the three follow-up rounds: total healthcare expenditures (in thousands of 2022 U.S. dollars); out-of-pocket expenditures (OOP) (in thousands of 2022 U.S. dollars); physical health-related quality of life (HRQoL) as measured by the SF-12v2 Physical Component Summary score; mental health-related quality of life as measured by the SF-12v2 Mental Component Summary score; and count of inpatient hospital discharges (distinct admission episodes regardless of length of stay) during each follow-up round.
2.5. Statistical Analysis
Survey design variables and analytic weights were incorporated in all analyses. The longitudinal person weight (LONGWT) was applied to expenditure, utilization, and survival analyses to produce nationally representative population-level estimates. The Self-Administered Questionnaire weight (LSAQWT) was applied to health-related quality of life analyses, as PCS and MCS scores are derived from the SF-12v2 administered through the MEPS Self-Administered Questionnaire component and require this separate weight to account for the subsample that completed it.
2.5.1. Discrete-Time Hazard of Incident MM
Incident MM was analyzed using discrete-time survival methods with a complementary log-log link. The dataset was restructured into a person-period format so that each participant contributed one record for each follow-up interval until MM onset or censoring. Because no incident MM events were observed in 2022 across any exposure group, resulting in complete separation for the year indicator, the survival analysis was restricted to the 2020 and 2021 follow-up intervals. The primary model was a parsimonious survey-weighted specification including COVID-19 group, follow-up year, centered age, baseline self-rated health, and baseline chronic condition count. A more fully adjusted survey-weighted model additionally included sex, race/ethnicity, educational attainment, insurance status, and income-to-poverty category, and was treated as a sensitivity analysis because of the limited number of events relative to the number of predictors. To evaluate robustness to sparse-data bias, an unweighted Firth penalized logistic regression model was fit using the same core covariates as the primary model. Firth penalization addresses the tendency of standard maximum likelihood estimation to produce inflated coefficient estimates when event counts are small relative to the number of predictors. Since this method cannot be combined with complex survey design adjustments, the Firth model was estimated without survey weights, and its results are interpreted alongside rather than in place of the primary survey-weighted estimates. An additional sensitivity analysis restricted the sample to participants with no chronic conditions at the 2019 baseline, to examine whether the association between Long COVID and incident MM was detectable even among the most clinically unencumbered entry subgroup. This restriction yielded only seven observed events across the person-period dataset, producing quasi-complete separation and rendering the parameter estimates unstable and uninformative. Results from this analysis are therefore described qualitatively only and are not interpreted inferentially.
2.5.2. MM Cluster Type at Onset
Among participants who developed incident MM, cluster type at onset was first summarized descriptively. Because four of the seven prespecified cluster types had zero observed cases, the planned multinomial model was not estimateable. We therefore fit an exploratory binary Firth penalized logistic regression comparing cancer-involved MM onset (clusters 5 and 6) with cardiorespiratory onset (cluster 3, reference). Given the small number of cancer-involved cases, particularly among participants with Long COVID, these analyses were regarded as hypothesis generating.
2.5.3. Post-Onset Burden Trajectories
Longitudinal trajectories of downstream burden were analyzed using Generalized Estimating Equations with an autoregressive working correlation structure of order 1. Each model included COVID-19 exposure group, follow-up year as a categorical variable, the interaction between exposure group and follow-up year, an indicator for incident MM onset, years since MM onset, and the prespecified baseline covariates. Model families and link functions were selected according to outcome type: gamma with log link for total and out-of-pocket expenditures, negative binomial with log link for inpatient stays, and normal with identity link for PCS and MCS scores.
As a sensitivity analysis, we also fit hierarchical linear growth-curve models treating calendar year as a continuous linear time variable to evaluate whether conclusions regarding trajectory divergence were sensitive to modeling time categorically versus continuously. In addition, we examined interaction models for sex, age group, insurance status, and race/ethnicity.
3. Results
3.1. Study Cohort and Baseline Characteristics
Of 5,565 MEPS Panel 24 participants, 4,364 individuals free of MM at baseline met the inclusion criteria, representing an estimated 279.2 million U.S. noninstitutionalized civilians. The analytic cohort included 232 participants with Long COVID, 1,455 with COVID-recovered status, and 2,677 with no reported COVID-19 infection. During follow-up, 105 participants developed incident MM, corresponding to a weighted incidence of 1.92% (approximately 5.35 million individuals). Weighted incident MM was highest among participants with Long COVID (4.42%), followed by those with COVID-recovered status (2.54%) and those with no COVID (1.32%). Unweighted sample proportions, presented in Table 1, differ from these weighted estimates because survey weights adjust for the complex stratified sampling design to produce nationally representative population-level figures; the two sets of figures address different questions and should not be directly compared.
Baseline characteristics are presented in Table 1. Compared with the COVID-recovered and no-COVID groups, participants with Long COVID were older, had poorer baseline self-rated health, and had a higher baseline chronic condition count. Distributions of race/ethnicity and poverty category also differed across exposure groups, whereas sex and insurance status were broadly similar. The Long COVID group had the highest proportion of non-Hispanic White participants and the lowest proportion in the high-income category.
3.2. Incident MM Risk
Since no additional incident MM events were observed in 2022, the discrete-time survival models were restricted to the 2020 and 2021 follow-up intervals. Event rates showed a consistent gradient across both years, with the highest rates in the Long COVID group, intermediate rates in the COVID-recovered group, and the lowest rates in the non-COVID group.
In the primary survey-weighted model, adjusted for follow-up year, centered age, baseline self-rated health, and baseline chronic condition count, Long COVID was associated with a higher hazard of incident MM than no COVID (HR, 2.54; 95% CI, 1.26-5.10). COVID-recovered status was also associated with elevated hazard relative to no COVID, although the magnitude was smaller (HR, 1.85; 95% CI, 1.08-3.17). Baseline chronic condition count was the strongest independent predictor of incident MM (HR, 2.84; 95% CI, 1.93-4.17). There was no evidence that hazards differed between 2020 and 2021 or varied by age or baseline self-rated health in the reduced model. These findings indicate a graded association, with the highest risk of new-onset MM among participants with Long COVID.
Sensitivity analyses were directionally consistent. In the fully adjusted survey-weighted model, Long COVID remained associated with incident MM (HR, 2.50; 95% CI, 1.13-5.54). In the unweighted Firth penalized logistic model, the association was similar in direction and larger in magnitude (Exp(β), 3.30; 95% CI, 1.91-5.71), supporting robustness of the primary finding.
As shown in Table 2, Long COVID was associated with a higher hazard of incident MM than no COVID in the primary survey-weighted complementary log-log (cloglog) model, and this pattern remained directionally consistent in the fully adjusted and Firth-penalized sensitivity analyses.
3.3. MM Cluster Type at Onset
Among the 105 incident MM cases, only 3 of the 7 prespecified cluster types were observed. Cardiorespiratory MM was the predominant phenotype, accounting for 78 cases (74.3%), followed by cancer + cardiometabolic MM (23 cases, 21.9%) and cancer + respiratory MM (4 cases, 3.8%). Notably, cancer + respiratory phenotypes occurred only among COVID-exposed participants.
Because four cluster types had zero observed cases and several of the remaining cells were sparse, the planned multinomial model was not estimable. We therefore fit an exploratory Firth-penalized logistic regression comparing cancer-involved onset with cardiorespiratory onset. In that model, there was no clear evidence that onset phenotype differed by COVID-19 exposure group [Long COVID vs no COVID (OR 1.27, 95% CI 0.32-5.02); COVID-recovered vs no COVID: (OR 1.51, 95% CI 0.44-5.20)]. Increasing age, however, was associated with higher odds of cancer-involved onset (OR 1.09 per year, 95% CI 1.03–1.15). Given the small number of cancer-involved cases, particularly among participants with Long COVID, these estimates were imprecise and do not support definitive inference but can be viewed as exploratory.
The distribution of MM phenotypes at onset and estimates from the exploratory Firth-penalized logistic model are shown in Table 3.
3.4. Post-Onset Burden Trajectories
In the primary GEE analyses, incident MM onset was associated with greater downstream burden across several domains. Specifically, onset was associated with higher total healthcare expenditures (RR 2.16, 95% CI 1.32-3.52), higher inpatient utilization (RR 3.10, 95% CI 1.72-5.64), and lower physical HRQoL, with a 5.17-point decline in PCS score (95% CI -8.66 to -1.67). Inpatient stays also increased with each additional year after onset (RR 3.84, 95% CI 1.19-12.43). By contrast, incident MM onset was not clearly associated with out-of-pocket expenditures or mental HRQoL.
Across the primary GEE models, there was no clear evidence that Long COVID was associated with differential year-specific post-onset trajectories for total expenditures, out-of-pocket expenditures, PCS, MCS, or inpatient stays. However, Long COVID was independently associated with lower mental HRQoL (β -2.38, 95% CI -4.38 to -0.38), suggesting a persistent mental health burden irrespective of MM onset. In sensitivity analysis, the hierarchical linear growth-curve model identified a positive Year × Long COVID interaction for log-transformed total expenditures (β 0.259, 95% CI 0.057-0.461), consistent with steeper annual expenditure growth under a linear time specification. Taken together, these findings suggest that incident MM was associated with substantial downstream burden, whereas evidence for Long COVID-specific divergence in burden trajectories was limited in the primary analyses and remained model-dependent for expenditures.
There was no evidence of effect modification by sex. Although interactions by age group and insurance status reached statistical significance, those models showed quasi-complete separation and unstable coefficients, precluding reliable subgroup inference.

Table 4.
Longitudinal associations of incident multimorbidity onset and Long COVID with healthcare burden trajectories.
Table 4.
Longitudinal associations of incident multimorbidity onset and Long COVID with healthcare burden trajectories.
| Outcome | Incident MM onset estimate (95% CI) | Years since MM onset estimate (95% CI) | Long COVID main effect (95% CI) | Long COVID × follow-up year interaction |
| Total expenditures | RR 2.16 (1.32-3.52) | — | — | NS |
| Out-of-pocket expenditures | NS | — | — | NS |
| Physical HRQoL (PCS) | β = -5.17 (-8.66 to -1.67) | — | — | NS |
| Mental HRQoL (MCS) | NS | — | β = -2.38 (-4.38 to -0.38) | NS |
| Inpatient stays | RR 3.10 (1.72–5.64) | RR 3.84 (1.19-12.43) | — | NS |
Note: Expenditure and inpatient models used log links; HRQoL models used identity links. RR indicates exponentiated beta for log-link models. NS indicates no clear association in the primary GEE model. Models adjusted for COVID-19 group, follow-up year, COVID-19 group × follow-up year interaction, centered age, sex, race/ethnicity, insurance status, educational attainment, poverty category, baseline self-rated health, and baseline chronic condition count.
4. Discussion
4.1. Principal Findings
In this nationally representative longitudinal cohort of participants free of MM at baseline, Long COVID was associated with a higher hazard of incident MM during follow-up than no COVID, while COVID-recovered status was also associated with an elevated, but smaller hazard. These findings extend prior post-COVID literature, which has largely focused on individual incident conditions in administrative or health-system cohorts, by showing that COVID-19 exposure, particularly Long COVID, may also be associated with crossing the clinically important threshold into MM (Al-Aly et al., 2021; Bowe et al., 2021; Xie et al., 2022). This threshold is consequential because MM reflects not simply the accumulation of diagnoses, but the emergence of greater treatment complexity, care fragmentation, competing clinical priorities, and increasing healthcare utilization (Barnett et al., 2012; Salisbury et al., 2011; Vogeli et al., 2007).
The graded pattern observed across the no-COVID, COVID-recovered, and Long COVID groups is notable. The association in the COVID-recovered group suggests that the long-term consequences of COVID infection may not be limited to individuals meeting formal Long COVID criteria. This finding is consistent with evidence showing that acute COVID infection can produce persistent endothelial dysfunction, immune dysregulation, and inflammatory activation after acute infection, offering plausible pathways through which post-COVID risk may extend beyond clinically recognized Long COVID (Davis et al., 2023; Proal and VanElzakker, 2021; Swank et al., 2023). From a public health perspective, these findings suggest that longitudinal chronic disease surveillance after COVID-19 may need to extend beyond patients with persistent symptoms alone.
The temporal concentration of incident MM in 2020 and 2021, with no additional events observed in 2022, may indicate that the highest-risk individuals transitioned early during follow-up. Longer-term studies will be needed to determine whether this reflects early depletion of high-risk individuals, limited follow-up time, or other features of the pandemic period.
4.2. MM Phenotype at Onset
Among incident cases, all observed MM involved combinations spanning multiple physiological domains. This multi-domain pattern is substantively important because conventional MM frameworks do not require cross-domain clustering. In this cohort, incident MM was dominated by cardiorespiratory and cancer-related combinations, suggesting that post-COVID chronic disease accumulation may be systemic rather than confined to a single organ pathway. The recognized multisystem effects of COVID infection and Long COVID provide biological plausibility for this pattern (Davis et al., 2023; Proal and VanElzakker, 2021). Because only 3 of the 7 prespecified cluster types were observed and several cells were sparse, the results do not warrant firm conclusions regarding differences in cluster type at onset by COVID-19 exposure status.
The exclusive occurrence of cancer + respiratory cluster among COVID-exposed participants was a notable distributional signal, although the number of cases was very small. Emerging literature on persistent respiratory injury and post-COVID biological disruption provides a plausible context for this pattern (Al-Aly et al., 2021). However, this study lacked enough power to make definitive inferences about rare cluster types, and replication in larger cohorts will be essential before stronger conclusions can be drawn.
4.3. Downstream Burden After MM Onset
The burden analyses suggest that incident MM was associated with substantial downstream consequences, particularly for physical functioning, healthcare expenditures, and inpatient utilization. Physical HRQoL declined by more than 5 PCS points after MM onset, a magnitude that exceeds commonly cited thresholds for clinical importance based on the minimal clinically important difference of 2-3 points established for the SF-12 PCS (Ware et al., 1996; Wyrwich et al., 1999). In contrast, Long COVID itself was associated with poorer mental HRQoL independent of MM onset. Taken together, these findings suggest partially distinct burden pathways: MM onset was more closely linked to deterioration in physical functioning, whereas Long COVID was associated with persistent mental health burden. Prior studies documenting anxiety, depression, cognitive symptoms, and other neuropsychiatric sequelae after COVID-19 provide context for this pattern (Huang et al., 2022; Taquet et al., 2022, 2021).
Inpatient utilization showed the clearest evidence of progressive worsening after incident MM onset. Hospital use increased at the point of onset and continued to rise thereafter, suggesting that COVID-era MM may have implications not only for individual health status but also for health-system demand. This finding aligns with broader MM literature showing that hospitalization risk rises nonlinearly as chronic conditions accumulate (Barnett et al., 2012; Salisbury et al., 2011). From a health-services perspective, the results highlight the importance of identifying COVID survivors who transition into MM as a potentially high-risk subgroup for avoidable inpatient use.
By contrast, out-of-pocket expenditures were not clearly associated with incident MM onset, while poverty category remained a stronger predictor of financial burden. This suggests that the financial consequences borne directly by patients may be shaped more strongly by socioeconomic position and insurance structure than by MM onset alone. That finding is consistent with prior work showing that financial toxicity in chronic disease is strongly patterned by income, coverage gaps, and cost-sharing exposure (Himmelstein et al., 2009). The pandemic period itself was associated with substantial increases in depression and anxiety globally (Santomauro et al., 2021), providing a broader context for the mental health burden observed in Long COVID survivors in the present study.
4.4. Methodological Considerations
An additional methodological finding was the difference between the GEE and hierarchical linear model results for total expenditures. The primary GEE analysis did not identify a clear Long COVID-by-year interaction, whereas the HLM sensitivity analysis suggested steeper expenditure growth over time among Long COVID participants. These models address related but not identical questions: the GEE framework emphasizes average population-level year-specific differences, while the growth-curve model evaluates differences in slope over time. Together, the two analyses suggest that any Long COVID-related expenditure divergence may be gradual rather than concentrated within a single follow-up interval. Future studies examining the economic consequences of Long COVID may benefit from presenting both population-averaged and subject-specific trajectory models.
4.5. Clinical and Policy Implications
These findings carry several implications for primary care practice and policy. First, the association between Long COVID and a higher hazard of incident MM suggests that primary care practitioners may benefit from treating Long COVID not merely as a symptomatic condition requiring symptom relief, but as a potential harbinger of accelerating chronic disease complexity. Proactive monitoring of chronic condition accumulation, particularly across cardiovascular, cardiometabolic, and respiratory domains among patients with documented Long COVID, may support earlier identification of those crossing the MM threshold and allow timely enrolment in structured chronic disease management programs before complexity fully manifests (Salisbury et al., 2011; Wolff et al., 2002). If Long COVID is associated with a higher risk of incident MM, then prevention and prompt treatment of prolonged post-COVID sequelae may also function as upstream chronic disease prevention (Hung et al., 2025), a framing with direct relevance to commissioning priorities in primary care.
Second, the independent association between Long COVID and poorer mental health-related quality of life, irrespective of MM onset, provides a practical basis for integrating routine mental health screening into post-COVID follow-up protocols within general practice. Structured assessment for depression, anxiety, and cognitive symptoms using validated brief instruments appropriate to primary care workflows is warranted for Long COVID patients, even in the absence of newly established physical diagnoses (Mazza et al., 2022; Taquet et al., 2022). This recommendation is reinforced by the broader context of pandemic-associated increases in anxiety and depressive disorders globally (Santomauro et al., 2021).
Third, the marked increase in inpatient utilization observed after MM onset underscores the potential value of proactive care coordination in primary care for COVID survivors who cross the MM threshold. MM-oriented management frameworks, including structured care plans, team-based case reviews, and coordinated referral pathways, may reduce the risk of avoidable hospitalization in this population and are consistent with evidence-based frameworks for managing MM in general practice (Barnett et al., 2012; Salisbury et al., 2011).
Finally, the finding that out-of-pocket financial burden was more strongly associated with poverty category than with MM onset suggests that financial protection strategies for COVID survivors should be prioritized on the basis of socioeconomic vulnerability rather than diagnosis alone. Primary care practitioners are often well-positioned to identify patients at the intersection of clinical complexity and economic precarity and to connect them with relevant social support services. From a policy perspective, these findings support investment in integrated primary care pathways that combine chronic disease surveillance, mental health assessment, and social prescribing for Long COVID survivors, particularly those from lower-income groups.
4.6. International Relevance
Although the present study draws on a nationally representative U.S. data source, its substantive findings have implications that extend beyond the specific institutional context of the U.S. healthcare system. The association between Long COVID and incident MM reflects biological pathways post-viral immune dysregulation, endothelial dysfunction, and chronic disease accumulation that are not specific to any particular health system structure (Davis et al., 2023; Proal and VanElzakker, 2021). MM is a recognized challenge across high-income countries, with prevalence estimates of 25-40% in adult populations in settings including the United Kingdom, Canada, Australia, and continental Europe (Barnett et al., 2012). In these settings, the general practice or community health team bears primary responsibility for MM identification and ongoing management, making the present findings directly relevant to practitioners and health system planners across diverse contexts.
The implications for primary care are particularly salient in universal or near-universal coverage systems such as the National Health Service in the United Kingdom or analogous structures in Scandinavia and Australia, where Long COVID clinics have been developed as extensions of primary care infrastructure and where general practitioners serve as the initial assessment and referral point for post-COVID sequelae. In these settings, evidence supporting the association between Long COVID and incident MM strengthens the case for maintaining longitudinal chronic disease surveillance as a component of structured Long COVID follow-up pathways, even after initial symptom management has been completed.
In low- and middle-income country contexts, where primary care infrastructure may be more resource-constrained and where MM surveillance systems are less developed, the findings emphasize the importance of building longitudinal chronic disease monitoring capacity as populations of COVID-19 survivors age and accumulate comorbid conditions. Cross-national harmonization of definitions of MM, classification of Long COVID exposure, and follow-up protocols would strengthen the comparative evidence base for international primary care planning for COVID survivors.
4.7. Limitations
This study has several limitations that warrant consideration. First, the observational design does not support causal inference. Despite the temporal ordering of exposure and outcome, unmeasured confounding, including preexisting subclinical disease, inflammatory burden, and other health vulnerabilities not fully captured in MEPS, may have contributed to the observed associations. Second, Long COVID classification was based on self-reported COVID-19 history and symptom duration rather than on biomarker confirmation or validated symptom scales, potentially leading to exposure misclassification. Any such misclassification would likely be non-differential and bias associations toward the null. Third, MEPS represents the noninstitutionalized U.S. civilian population and excludes groups in whom the burden of Long COVID and MM may be especially high, including nursing home residents and incarcerated populations; therefore, the estimates may be conservative and not generalizable to institutionalized populations.
Statistical power was limited in several analyses, particularly the cluster-type analysis at onset and the subgroup and trajectory interaction models. Rare cluster types yielded imprecise estimates, and sparse data limited precision for several subgroup comparisons. The fully adjusted survey-weighted survival model was also affected by quasi-complete separation in the highest educational attainment category, reducing the stability of some covariate estimates. In addition, the 4-year observation window may not capture the full long-term consequences of chronic disease associated with Long COVID. Finally, the MM taxonomy was based on a preexisting cluster framework and may not fully capture novel co-occurrence patterns emerging in the COVID era.
5. Conclusion
In this nationally representative longitudinal study, Long COVID was associated with a higher hazard of incident MM among participants free of MM at baseline, with an intermediate elevation also observed among COVID-recovered participants. These findings suggest that the long-term health consequences of COVID infection may include not only persistent symptoms or single-organ sequelae but also transition into clinically consequential MM. Incident MM was associated with deterioration in physical HRQoL and substantial increases in inpatient utilization, while Long COVID was independently associated with poorer mental HRQoL. Together, these results support the need for post-COVID care strategies that integrate chronic disease surveillance, mental health assessment, and MM-oriented management, particularly for individuals at elevated social and clinical risk.
Author Contributions
Ibrahim Alliu: Conceptualization; Data curation; Formal analysis; Methodology; Visualization; Writing – original draft; Writing – review and editing. Subash Thapa: Conceptualization; Writing – review and editing. Emmanuel Azu: Formal analysis. Timothy Kizza: Formal analysis. Logan Cowan: Writing – review and editing.
Funding
No external funding was received for this study.
Declarations Ethics Approval and Consent to Participate
Not required. This study used publicly available, de-identified data from the Medical Expenditure Panel Survey (MEPS), administered by the Agency for Healthcare Research and Quality (AHRQ). All procedures were performed in compliance with applicable federal regulations governing the protection of human research subjects. Because the data are de-identified and publicly available, the study is exempt from institutional review board (IRB) oversight under 45 CFR 46.104(d)(4). No personally identifiable information was accessed or analyzed.
Consent for Publication
Not applicable.
Availability of Data and Materials
MEPS Panel 24 data are publicly available at https://meps.ahrq.gov. SAS code is available from the corresponding author upon reasonable request.
Conflicts of Interest
The author declares no competing interests.
Acknowledgments
The author thanks the Agency for Healthcare Research and Quality (AHRQ) for maintaining and disseminating the MEPS data.
Abbreviations
The following abbreviations are used in this manuscript:
| AHRQ | Agency for Healthcare Research and Quality |
| AR(1) | Autoregressive Correlation Structure of Order 1 |
| CDC | Centers for Disease Control and Prevention |
| CHE | Catastrophic Healthcare Expenditure |
| CI | Confidence Interval |
| COVID-19 | Coronavirus Disease 2019 |
| GEE | Generalized Estimating Equations |
| HR | Hazard Ratio |
| HRQoL | Health-Related Quality of Life |
| IRR | Incidence Rate Ratio |
| Long COVID | Post-Acute Sequelae of SARS-CoV-2 |
| MCS | Mental Component Summary |
| MEPS | Medical Expenditure Panel Survey |
| MM | Multimorbidity |
| OOP | Out-of-Pocket |
| PCS | Physical Component Summary |
| RR | Rate Ratio |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| SAS | Statistical Analysis System |
| SD | Standard Deviation |
| SE | Standard Error |
| SF-12v2 | 12-Item Short Form Health Survey Version 2 |
| U.S. | United States |
| WHO | World Health Organization |
References
- Aborode, A.T.; Oginni, O.; Abacheng, M.; Edima, O.; Lamunu, E.; Folorunso, T.N.; Oko, C.I.; Iretiayo, A.R.; Lawal, L.; Amarachi, R.; et al. Healthcare debts in the United States: A silent fight. Annals of Medicine & Surgery 2025, 87, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat. Med. 2022, 28, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Alliu, I.; Thapa, S.; Yu, L.; Shehaj, B.; Asifat, O. Economic and Humanistic Burden of Multimorbidity in the United States: A Longitudinal Study of Expenditure and Quality of Life Trajectories, 2019–2022. Int. J. Environ. Res. Public Health 2025, 22, 1870. [Google Scholar] [CrossRef]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID Symptom Study app: A prospective, community-based, nested, case-control study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. The Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Bowe, B.; Xie, Y.; Xu, E.; Al-Aly, Z. Kidney Outcomes in Long COVID. Journal of the American Society of Nephrology 2021, 32, 2851–2862. [Google Scholar] [CrossRef]
- Cutler, D.M. The Costs of Long COVID. JAMA Health Forum 2022, 3, e221809. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Himmelstein, D.U.; Thorne, D.; Warren, E.; Woolhandler, S. Medical Bankruptcy in the United States, 2007: Results of a National Study. Am. J. Med. 2009, 122, 741–746. [Google Scholar] [CrossRef]
- Huang, L.; Li, X.; Gu, X.; Zhang, H.; Ren, L.; Guo, L.; Liu, M.; Wang, Y.; Cui, D.; Wang, Y.; et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: A longitudinal cohort study. Lancet Respir. Med. 2022, 10, 863–876. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.; Wang, L.; Lee, Y.; Suk, C.; Kok, C. Association of Nirmatrelvir/Ritonavir and the Risk of Long COVID Among US Adults: A Multicenter Retrospective Cohort Study. J. Med. Virol. 2025, 97. [Google Scholar] [CrossRef]
- Mazza, M.G.; Palladini, M.; Poletti, S.; Benedetti, F. Post-COVID-19 Depressive Symptoms: Epidemiology, Pathophysiology, and Pharmacological Treatment. CNS Drugs 2022, 36, 681–702. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Proal, A.D.; VanElzakker, M.B. Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front. Microbiol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Salisbury, C.; Johnson, L.; Purdy, S.; Valderas, J.M.; Montgomery, A.A. Epidemiology and impact of multimorbidity in primary care: A retrospective cohort study. British Journal of General Practice 2011, 61, e12–e21. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Mantilla Herrera, A.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021. [Google Scholar]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Swank, Z.; Senussi, Y.; Manickas-Hill, Z.; Yu, X.G.; Li, J.Z.; Alter, G.; Walt, D.R. Persistent Circulating Severe Acute Respiratory Syndrome Coronavirus 2 Spike Is Associated With Post-acute Coronavirus Disease 2019 Sequelae. Clinical Infectious Diseases 2023, 76, e487–e490. [Google Scholar] [CrossRef]
- Taquet, M.; Luciano, S.; Geddes, J.R.; Harrison, P.J. Bidirectional associations between COVID-19 and psychiatric disorder: Retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry 2021, 8, 130–140. [Google Scholar] [CrossRef]
- Taquet, M.; Sillett, R.; Zhu, L.; Mendel, J.; Camplisson, I.; Dercon, Q.; Harrison, P.J. Neurological and psychiatric risk trajectories after SARS-CoV-2 infection: An analysis of 2-year retrospective cohort studies including 1 284 437 patients. Lancet Psychiatry 2022, 9, 815–827. [Google Scholar] [CrossRef]
- Thaweethai, T.; Jolley, S.E.; Karlson, E.W.; Levitan, E.B.; Levy, B.; McComsey, G.A. Development of a Definition of Postacute Sequelae of SARS-CoV-2 Infection. JAMA 2023, 329, 1934. [Google Scholar] [CrossRef]
- Tran, V.-T.; Porcher, R.; Pane, I.; Ravaud, P. Course of post COVID-19 disease symptoms over time in the ComPaRe long COVID prospective e-cohort. Nat. Commun. 2022, 13, 1812. [Google Scholar] [CrossRef] [PubMed]
- Vogeli, C.; Shields, A.E.; Lee, T.A.; Gibson, T.B.; Marder, W.D.; Weiss, K.B.; Blumenthal, D. Multiple Chronic Conditions: Prevalence, Health Consequences, and Implications for Quality, Care Management, and Costs. J. Gen. Intern. Med. 2007, 22, 391–395. [Google Scholar] [CrossRef]
- Ware, J.E.; KOSINSKI, M.; KELLER, S.D. A 12-Item Short-Form Health Survey. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Watson, K.B.; Wiltz, J.L.; Nhim, K.; Kaufmann, R.B.; Thomas, C.W.; Greenlund, K.J. Trends in Multiple Chronic Conditions Among US Adults, By Life Stage, Behavioral Risk Factor Surveillance System, 2013–2023. Prev. Chronic Dis. 2025, 22. [Google Scholar] [CrossRef]
- Wolff, J.L.; Starfield, B.; Anderson, G. Prevalence, Expenditures, and Complications of Multiple Chronic Conditions in the Elderly. Arch. Intern. Med. 2002, 162, 2269. [Google Scholar] [CrossRef]
- World Health Organization. WHO COVID-19 dashboard [WWW Document]. COVID-19 Cases, World 2026. [Google Scholar]
- Wyrwich, K.W.; Tierney, W.M.; Wolinsky, F.D. Further Evidence Supporting an SEM-Based Criterion for Identifying Meaningful Intra-Individual Changes in Health-Related Quality of Life. J. Clin. Epidemiol. 1999, 52, 861–873. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Participant flow diagram. MM = multimorbidity.

Table 1.
Baseline characteristics of the analytic cohort by COVID-19 exposure status, MEPS Panel 24.
Table 1.
Baseline characteristics of the analytic cohort by COVID-19 exposure status, MEPS Panel 24.
| Characteristic |
Total (N = 4,364) |
Long COVID (n = 232) |
COVID-recovered (n = 1,455) |
No COVID (n = 2,677) |
| Age, mean (SE) | 38.69 (0.57) | 46.37 (1.37) | 41.32 (0.68) | 36.33 (0.74) |
| Sex, % | ||||
| Male | 49.66 | 41.31 | 48.86 | 50.85 |
| Female | 50.34 | 58.69 | 51.14 | 49.15 |
| Race/ethnicity, % | ||||
| Non-Hispanic White | 57.51 | 72.13 | 62.96 | 52.96 |
| Non-Hispanic Black | 12.97 | 6.72 | 11.24 | 14.55 |
| Hispanic | 19.74 | 17.21 | 16.77 | 21.77 |
| Non-Hispanic Asian | 6.25 | 2.67 | 6.00 | 6.71 |
| Non-Hispanic Other/Multiple | 3.52 | 1.28 | 3.03 | 4.01 |
| Insurance status, % | ||||
| Insured | 89.13 | 86.04 | 90.35 | 88.63 |
| Uninsured | 10.87 | 13.96 | 9.65 | 11.37 |
| Poverty category, % | ||||
| Poor/Negative/Near Poor | 16.70 | 16.12 | 11.39 | 20.13 |
| Low/Middle Income | 39.66 | 47.32 | 37.97 | 40.07 |
| High Income | 43.64 | 36.56 | 50.64 | 39.80 |
| Baseline health indicators | ||||
| Chronic count, mean | 0.34 | 0.49 | 0.34 | 0.34 |
| Self-rated health, mean | 2.07 | 2.43 | 2.07 | 2.03 |
Note: Sample sizes (n) are unweighted counts. Percentages and continuous-variable estimates are survey-weighted to represent the U.S. noninstitutionalized civilian population. Continuous variables are presented as weighted mean (SE), and categorical variables as weighted percentages. Group differences in continuous variables were evaluated using design-adjusted linear regression, while categorical variables were compared using Rao–Scott χ² tests.
Table 2.
Association between COVID-19 exposure status and incident MM among U.S. non-institutionalized civilians: Discrete-time survival model estimates, MEPS Panel 24 (2019–2021).
Table 2.
Association between COVID-19 exposure status and incident MM among U.S. non-institutionalized civilians: Discrete-time survival model estimates, MEPS Panel 24 (2019–2021).
| Model | Predictor | Estimate | 95% CI |
| Primary survey-weighted model | Long COVID vs No COVID | HR 2.54 | 1.26-5.10 |
| COVID-recovered vs No COVID | HR 1.85 | 1.08-3.17 | |
| 2021 vs 2020 | HR 1.13 | 0.67-1.92 | |
| Centered age, per year | HR 1.01 | 0.99-1.03 | |
| Baseline self-rated health, per unit | HR 1.15 | 0.92-1.44 | |
| Baseline chronic condition count, per unit | HR 2.84 | 1.93-4.17 | |
| Fully adjusted survey-weighted model | Long COVID vs No COVID | HR 2.50 | 1.13-5.54 |
| COVID-recovered vs No COVID | HR 1.60 | 0.95-2.69 | |
| Unweighted Firth penalized logistic model | Long COVID vs No COVID | Exp(β) 3.30 | 1.91-5.71 |
| COVID-recovered vs No COVID | Exp(β) 1.49 | 0.98-2.26 |
Table 3.
MM cluster type at onset and exploratory binary model.
| A. Incident MM cluster type at onset | |||||
| Cluster type |
Long COVID (n = 17) |
COVID-recovered (n = 40) |
No COVID (n = 48) |
Total (n = 105) |
|
| Cardiorespiratory (cluster 3) | 11 (62.1%) | 31 (77.5%) | 36 (74.3%) | 78 (74.3%) | |
| Cancer + cardiometabolic (cluster 5) | 4 (26.4%) | 7 (17.5%) | 12 (25.0%) | 23 (21.9%) | |
| Cancer + respiratory (cluster 6) | 2 (11.5%) | 2 (5.0%) | 0 | 4 (3.8%) | |
| Clusters 1, 2, 4, and 7 | 0 | 0 | 0 | 0 | |
| B. Exploratory Firth logistic model: cancer-involved vs cardiorespiratory onset | |||||
| Predictor | Estimate | 95% CI | |||
| Long COVID vs No COVID | OR 1.27 | 0.32-5.02 | |||
| COVID-recovered vs No COVID | OR 1.51 | 0.44-5.20 | |||
| Age, per year | OR 1.09 | 1.03-1.15 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



