Submitted:
26 May 2026
Posted:
27 May 2026
You are already at the latest version
Abstract
Liver regeneration is a tightly orchestrated compensatory response in which the remaining liver regains mass and function after liver injury, or surgical resection. However, it does not fully restore its original anatomy. This process involves sequential priming, proliferative, and termination phases that are controlled by inflammatory cytokines, growth factor signaling, metabolic regulation, and extracellular matrix remodeling. Clinically, regenerative capacity plays a crucial role in situations such as partial hepatectomy, acute liver failure, and chronic liver disease. Unfortunately, it can be compromised by conditions like cirrhosis, steatosis, diabetes, and other systemic or local issues. Current strategies to improve regeneration, such as portal vein modulation, cell-based therapies, organoid technology, and bioartificial liver support, show promise. However, they are limited by challenges like impaired engraftment, functional immaturity, technical complexity, and scalability restrictions. This review explores the pathophysiological basis of liver regeneration and evaluates the clinical evidence on nutritional and pharmacological interventions aimed at enhancing the natural liver repair mechanisms of the body.
Keywords:
clinical trials
; liver regeneration
; molecular physiology
; pharmacology
1. Introduction
Liver regeneration is a highly coordinated physiological process in which the residual hepatocyte population proliferates and undergoes structural remodeling aimed at restoring hepatic mass and functional capacity after liver injury [1]. Liver regeneration is more accurately described as compensatory hyperplasia that, in contrast to true anatomical regeneration - does not restore the liver to its original gross anatomical configuration [2]. The liver’s extraordinary regenerative capacity had already been captured in antiquity through Greek mythology describing the myths of Tityus and Prometheus whose livers grew back every night [3].
In clinics, liver regeneration occurs following insults owing to a variety of noxious stimuli in those situations requiring the replacement of lost or damaged hepatic tissue. These include partial hepatectomy (due to malignant disease or during living-donor liver transplantation), acute liver failure, drug-induced liver failure, or chronic liver disease and cirrhosis [4,5]. In turn, dysregulated liver regeneration is a cause of severe chronic liver disease.
Liver regeneration is a temporally phased process that is profoundly modulated by lipid metabolic circuitry. Its fundamental pathobiology comprises three interrelated stages: (i) an early priming phase, rapidly initiated by pro-inflammatory cytokines such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), which activate nuclear factor-κB (NF-κB) and signal transducer and activator of transcription 3 (STAT3); (ii) a proliferative phase orchestrated by mitogenic pathways, including hepatocyte growth factor (HGF)/c-Met and epidermal growth factor (EGF)/epidermal growth factor receptor (EGFR), in concert with Wingless (Wnt)/β-catenin and Hippo/Yes-associated protein (YAP) signaling; and (iii) a termination phase governed by transforming growth factor-β (TGF-β), metabolic checkpoints, and extracellular matrix remodeling, which collectively restrain excessive proliferation and re-establish hepatic homeostasis [3].
Current strategies for promoting liver regeneration are limited by significant biological and practical constraints. While the liver can efficiently recovery after acute injury, chronic conditions like cirrhosis create a hostile microenvironment that hinders hepatocyte engraftment, proliferation, and restoration of metabolic function.
Non-autologous cell-based therapies face challenges such as substantial cell loss during cryopreservation, low engraftment efficiency, and the requirement for long-term immunosuppression [6]. Additionally, interventional radiologic and surgical approaches like portal vein embolization (PVE) and associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) aim to stimulate liver regeneration by promoting hypertrophy of the future liver remnant through redirecting portal blood flow [7]. However, these procedures may be less effective in patients with pre-existing systemic or local conditions like diabetes, severe steatosis, or cirrhosis, which reduce regenerative capacity [8,9]. The rapid hypertrophy induced by these techniques may also lead to the development of functionally immature hepatocytes, delaying the recovery of essential synthetic and detoxification functions [10].
To address the limitations of single-cell transplantation, current research is focusing on three-dimensional liver organoids and bioartificial liver devices. However, these technologies face challenges in replicating the complex vascular and metabolic architecture of the adult human liver, as well as in large-scale manufacturing and standardization, which are significant barriers to clinical translation [11].
Within this complex landscape, this review aims to specifically explore the pathophysiology of liver regeneration, with a particular focus on clinical studies examining nutrient supplementation and pharmacological interventions aimed at enhancing the effectiveness of spontaneous hepatic regenerative responses. Given that cell-based therapies were addressed in a recent review [12], their consideration is beyond the scope of the current manuscript.
2. Methods of Bibliographic Research
The identification of relevant literature for this review was conducted through a structured bibliographic search primarily using the PubMed/MEDLINE database. The search strategy was designed to capture clinical studies evaluating mechanisms, determinants, and therapeutic modulation of liver regeneration. The principal search term used was “liver regeneration,” applied to the title field to maximize specificity for studies directly addressing the regenerative process. To focus on clinically relevant evidence, filters restricting results to clinical trials were applied when appropriate. In addition, a broader search using the query “liver regeneration” in the title or abstract fields was performed to identify complementary studies that might not have been indexed strictly as clinical trials but nonetheless provided clinically informative data. For this second search, a temporal filter restricting results to the last ten years was applied in order to capture the most recent developments in regenerative medicine, hepatobiliary surgery, and translational hepatology. Titles and abstracts retrieved through these searches were screened for relevance. Studies were considered eligible if they investigated factors influencing liver regeneration in humans, including surgical strategies, pharmacologic or nutritional interventions, metabolic optimization, regenerative medicine approaches, or biomarkers associated with regenerative performance. Particular attention was given to randomized controlled trials, prospective clinical studies, and translational investigations that included a clinical component. After the initial screening, full texts of potentially relevant articles were evaluated to determine their suitability for inclusion. Additional publications were identified through manual cross-referencing of bibliographies in key articles and review papers. This snowball approach allowed the identification of earlier landmark studies and important clinical observations that might not have been captured by the primary search filters.
Studies focusing exclusively on experimental animal models without translational relevance, purely mechanistic in vitro investigations, or reports lacking sufficient methodological detail were generally excluded from the clinical evidence synthesis, although selected experimental studies were occasionally cited to provide mechanistic context where appropriate. The final body of literature included in this review therefore reflects a combination of systematically retrieved clinical studies and additional relevant publications identified through reference tracking and expert evaluation of the field. This approach was intended to provide a balanced overview of both established and emerging clinical evidence regarding physiology, pharmacology, and therapeutic modulation of liver regeneration.
3. Liver Regeneration Pathways
Liver regeneration is a highly coordinated biological response that enables the restoration of hepatic mass and function following tissue loss or injury [13]. Instead of representing true anatomical regeneration, this process is best described as compensatory hyperplasia in which the residual hepatocyte population proliferates and reorganizes to re-establish functional capacity without fully recreating the original hepatic architecture. Clinically, the efficiency of this regenerative response is a critical determinant of outcome after major hepatectomy, living donor liver procurement, and acute or chronic liver injury [13]. A wide spectrum of molecular pathways, cellular interactions, and systemic factors contribute to the regulation of this complex process.
At the molecular level, liver regeneration proceeds through temporally overlapping phases involving priming, proliferation, and termination. The priming phase is characterized by the activation of quiescent hepatocytes through inflammatory signaling pathways. Cytokines such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) activate transcriptional programs mediated by nuclear factor-κB (NF-κB) and signal transducer and activator of transcription-3 (STAT3), thereby enabling hepatocytes to reenter the cell cycle [14,15]. This priming stage is followed by the proliferative phase, in which hepatocyte replication is driven by mitogenic signals including hepatocyte growth factor (HGF)/c-Met and epidermal growth factor (EGF)/epidermal growth factor receptor (EGFR) pathways, as well as the Wingless (Wnt)/β-catenin and Hippo/Yes-associated protein (YAP) signaling cascades [16,17]. Finally, regeneration is halted by inhibitory mechanisms, including transforming growth factor-β (TGF-β) signaling and extracellular matrix remodeling, which collectively restore hepatic homeostasis and prevent uncontrolled proliferation (Figure 1) [18].
Portal hemodynamics represent a central upstream driver of regenerative signaling. Surgical techniques such as PVE take advantage of this physiologic principle by redirecting portal blood flow to the future liver remnant (FLR), thereby stimulating hypertrophy of the preserved parenchyma. PVE has become a widely adopted strategy for increasing the safety of extended hepatectomy in patients with insufficient residual liver volume [19]. However, volumetric increases do not necessarily correspond to functional improvement, highlighting the need to evaluate regeneration not only in terms of volume but also in terms of functional hepatic capacity [19].
Several clinical studies have explored approaches to enhance the regenerative response following PVE. One notable strategy involves infusing autologous bone marrow-derived CD133+ stem cells into the portal circulation after embolization [20]. In an early prospective study of patients with large hepatic malignancies and critically low future liver remnant volumes, the combination of PVE with CD133+ stem cell administration resulted in significantly greater hypertrophy of the remnant liver compared with PVE alone [20]. Specifically, the absolute increase in FLR volume rose from approximately 239 mL to 417 mL in the stem-cell group, whereas the increase was more modest in patients undergoing PVE alone [20]. Moreover, the relative gain in remnant liver volume and the daily growth rate were both significantly higher when stem-cell therapy was added, suggesting that bone marrow–derived progenitor cells may contribute to hepatocyte proliferation or enhance the regenerative microenvironment [20].
Subsequent clinical observations have supported these findings. Studies evaluating PVE combined with CD133+ bone marrow stem cells demonstrated accelerated hypertrophy of the FLR, faster daily growth, and a shorter interval between embolization and definitive resection [21]. In patients with impaired hepatic parenchyma or critically small residual liver volumes, this approach enabled safe resection within a substantially shorter time frame compared with conventional PVE alone [21]. These results support the concept that circulating progenitor cells may participate in liver regeneration either through direct differentiation into hepatocyte-like cells or by modulating regenerative signaling pathways within the hepatic microenvironment [21].
Nutritional and metabolic factors also play an important role in regulating regenerative capacity. Branched-chain amino acids (BCAAs) have been extensively studied for their potential to support hepatic function and regeneration [19]. BCAA supplementation influences cellular metabolism, protein synthesis, and mitochondrial function, and has been shown experimentally to stimulate hepatocyte growth factor production while reducing hepatocyte apoptosis [19]. In a randomized clinical trial involving patients undergoing PVE followed by major hepatectomy, oral BCAA supplementation improved functional liver regeneration compared with standard nutritional support [19]. Functional recovery was assessed using technetium-99m galactosyl human serum albumin scintigraphy, which demonstrated significantly greater increases in liver uptake values in the BCAA-treated group [19]. Notably, the enhancement of functional regeneration was more pronounced than the increase in volumetric liver growth, reinforcing the concept that metabolic interventions may preferentially improve hepatic functional recovery rather than simple tissue hypertrophy [19].
Pharmacologic modulation of inflammatory signaling pathways represents another promising avenue for enhancing regeneration. Pentoxifylline, a phosphodiesterase inhibitor with anti-inflammatory properties, has been investigated as a therapeutic agent capable of modifying cytokine signaling during liver regeneration [22]. Experimental studies have shown that pentoxifylline suppresses TNF-α signaling while enhancing IL-6–mediated regenerative pathways, thereby promoting hepatocyte proliferation and protecting against ischemia-reperfusion injury [22]. In a double-blind randomized clinical trial including more than one hundred patients undergoing major liver resection, pentoxifylline administration resulted in significantly improved volumetric regeneration in patients with small remnant livers [22] These effects were associated with enhanced IL-6 transcriptional activation and reduced postoperative transaminase levels, suggesting a protective effect against hepatocellular injury [22]. However, the clinical benefit appeared limited to patients with critically small liver remnants, and treatment was associated with a higher incidence of drug-related adverse events [22].
In addition to cytokine and metabolic pathways, platelet-derived mediators have emerged as key regulators of liver regeneration. Experimental studies have demonstrated that platelets accumulate within the regenerating liver and release growth-promoting factors that stimulate hepatocyte proliferation [23]. Among these mediators, serotonin has been identified as a critical signal in the regenerative process [23]. Clinical studies in patients undergoing hepatic resection have shown that low preoperative intraplatelet serotonin levels are associated with delayed liver regeneration and a higher risk of postoperative liver dysfunction [23]. These findings suggest that platelet serotonin may serve not only as a biomarker of regenerative capacity but also as a potential therapeutic target.
The role of endothelial and coagulation-related pathways in regeneration has also received increasing attention. von Willebrand factor (vWF), a glycoprotein released by activated endothelial cells, facilitates platelet adhesion and accumulation within the regenerating liver [24]. In experimental models, vWF has been shown to mediate platelet recruitment during the early phase of liver regeneration, a process that appears essential for adequate hepatocyte proliferation [24]. Clinical investigations have confirmed that perioperative dynamics of vWF correlate with regenerative activity in patients undergoing liver resection [24]. Specifically, a transient postoperative surge in vWF levels was observed in patients with successful liver regeneration, whereas elevated baseline vWF concentrations were associated with impaired regenerative capacity and an increased risk of postoperative dysfunction [24]. These observations highlight the interplay between endothelial activation, platelet biology, and hepatic regenerative signaling.
Recent advances in molecular pharmacology have expanded the therapeutic landscape by identifying intracellular signaling pathways that directly regulate hepatocyte proliferation. One of the most promising targets is mitogen-activated protein kinase kinase-4 (MKK4), a key component of stress-activated kinase signaling networks [25]. Experimental studies have demonstrated that inhibition of MKK4 releases a regenerative checkpoint in hepatocytes, thereby enhancing their proliferative capacity following liver injury or resection [25]. Structure-based drug discovery efforts led to the development of HRX215, a first-in-class small-molecule inhibitor of MKK4 [25].
Preclinical studies have shown that HRX215 significantly increases liver regeneration after hepatectomy in both murine and porcine models [25]. In mice, pharmacologic MKK4 inhibition significantly increased hepatocyte proliferation following partial hepatectomy without inducing uncontrolled cell growth in the intact liver [25]. In pigs, HRX215 accelerated the restoration of liver volume after major resection and, most strikingly, enabled survival after an otherwise lethal 85% hepatectomy [25]. This effect was associated with rapid expansion of functional liver mass and prevention of post-hepatectomy liver failure [25].
Importantly, the safety and pharmacokinetic profile of HRX215 has also been evaluated in humans. A first-in-human phase I clinical trial involving healthy volunteers demonstrated excellent tolerability and predictable pharmacokinetics without serious adverse effects [25]. These findings support the translational potential of MKK4 inhibition as a therapeutic strategy to prevent liver failure following major hepatectomy or small-for-size liver transplantation [25]. Beyond its pro-regenerative effects, MKK4 inhibition has also been shown to exert antisteatotic and antifibrotic effects in experimental models of chronic liver disease [25]. These additional properties may be particularly relevant in clinical contexts where hepatic steatosis or fibrosis impairs regenerative capacity, such as in patients with metabolic-associated fatty liver disease or chemotherapy-associated liver injury [25].
Taken together, current evidence indicates that liver regeneration is controlled by a complex network of hemodynamic, inflammatory, metabolic, and molecular signals. Interventions that enhance portal flow, modulate cytokine signaling, optimize metabolic conditions, or directly activate regenerative pathways can significantly impact the regenerative response. Clinical strategies, ranging from portal vein embolization and stem-cell therapy to nutritional supplementation and targeted molecular inhibitors, demonstrate the variety of approaches currently being investigated.
Despite these advances, translation of experimental insights into clinical practice remains incomplete. Many interventions that demonstrate strong regenerative effects in preclinical models still require validation in large, controlled clinical trials. Moreover, the heterogeneity of patient populations, underlying liver diseases, and surgical procedures complicates the interpretation of clinical outcomes.
Future research will likely focus on integrating volumetric, functional, and molecular biomarkers to better predict regenerative capacity and personalize perioperative management. In addition, targeted therapies such as MKK4 inhibitors represent a promising new frontier, offering the potential to pharmacologically enhance the intrinsic regenerative ability of the liver. Ultimately, a deeper understanding of the pathways governing liver regeneration may lead to novel therapeutic strategies capable of expanding the safety and applicability of modern hepatobiliary surgery.
4. Clinical Studies
Liver regeneration is a crucial factor in determining outcomes following hepatectomy, living donor liver procurement, and acute or chronic liver injury. The ability of the remaining liver tissue to regenerate and regain function directly impacts postoperative recovery and the risk of liver failure [26]. In recent years, there has been an increasing focus on strategies to enhance this regenerative response. These strategies range from technical adjustments in portal flow and perioperative care to pharmacological, nutritional, and molecular interventions. The studies summarized in Table 1 [19,20,21,22,23,24,25,27,28,29,30,31,32,33,34,35,36] demonstrate the growing interest in finding methods that not only promote rapid regrowth of liver volume but also improve functional recovery and enhance the safety of major liver resections, especially in high-risk settings. However, the existing evidence is varied, highlighting the importance of distinguishing between interventions with genuine therapeutic potential and those that primarily investigate predictive or mechanistic aspects of regeneration.
Interventions associated with enhanced liver regenerative capacity included portal vein embolization combined with autologous CD133+ bone marrow stem cells [20,21], branched-chain amino acid supplementation following PVE [19], pentoxifylline in patients with small future liver remnants [22], N-butyl cyanoacrylate (NBCA) plus iodized oil for pre-hepatectomy portal vein embolization [33], postoperative ursodeoxycholic acid administration in living liver donors [34], preoperative lifestyle optimization [35], the TTK traditional Chinese medicine regimen [30], and pharmacologic MKK4 inhibition with HRX215 [25]. Collectively, these interventions, schematically illustrated in Figure 2, were associated with greater hypertrophy of the future liver remnant, accelerated volumetric expansion, improved postoperative liver function, or biologic signatures consistent with augmented regenerative activity [19,20,21,22,25,30,33,34,35].
In parallel, observational studies have identified platelet serotonin and von Willebrand factor as potentially relevant modulators or predictors of regenerative performance. However, these findings do not constitute direct evidence of therapeutic efficacy [23,24].
Among these studies, research by Zwirner et al stands out as one of the most innovative and promising. HRX215 is a first-in-class small-molecule inhibitor of mitogen-activated protein kinase kinase 4 (MKK4), a stress-activated upstream regulator within the c-Jun N-terminal kinase signaling axis [25]. The therapeutic rationale is biologically compelling: in the injured or partially resected liver, MKK4 appears to constrain hepatocyte cell-cycle progression. Pharmacologic inhibition of MKK4 may release a regenerative checkpoint and favor proliferation of the remnant parenchyma. The study further suggests that this effect is not simply mitogenic, but context dependent, with regenerative enhancement observed principally in damaged or resected livers rather than in the intact organ [25]. This distinction is important, as it supports the concept that HRX215 may amplify endogenous repair programs rather than induce indiscriminate hepatocyte proliferation. The reported antifibrotic and antisteatotic effects are also noteworthy, as they raise the possibility that MKK4 inhibition modifies the hepatic microenvironment in ways that could secondarily facilitate regeneration. The study exhibits considerable strengths. It adopts a rigorous translational design spanning rational compound development, target engagement, mechanistic preclinical validation, efficacy testing in both murine and porcine hepatectomy models, and early human phase I evaluation. Particularly persuasive is the demonstration of survival benefit after extended hepatectomy in a large-animal model, which strengthens the biological and clinical plausibility of the approach beyond conventional rodent data alone. However, the limitations are equally substantial and should temper interpretation. Most importantly, the clinical component remains confined to phase I testing in healthy volunteers. Therefore, the study provides safety and pharmacokinetic information but no evidence of therapeutic efficacy in patients with impaired regenerative reserve. In addition, the principal efficacy signals derive from preclinical and surrogate endpoints, not from hard clinical outcomes such as post-hepatectomy liver failure, morbidity, or survival in humans. The duration of follow-up is also limited, leaving unresolved whether sustained MKK4 inhibition could have unintended consequences for inflammatory signaling, maladaptive repair, or oncologic risk. Accordingly, while HRX215 is an innovative and promising candidate, its clinical relevance remains provisional pending well-powered patient-based trials.
By contrast, other investigations have failed to demonstrate a clear pro-regenerative effect or have only yielded inconclusive evidence. In fulminant hepatic failure, insulin plus glucagon did not improve survival, hepatic synthetic function, or histologic indices of regeneration [27]. Similarly, the comparison between isoflurane and propofol in donor hepatectomy did not reveal a significant difference in regenerated liver volume [36]. Synbiotic supplementation also produced equivocal results, with a possible benefit limited to a subgroup of patients without postoperative complications and no consistent overall advantage in the pilot trial [29]. Moreover, several studies, including postoperative volumetric analyses after hepatectomy and prognostic models based on remnant liver volume or the TACIA score (a prognostic system used to gauge disease severity and estimate short-term survival among subjects with acute-on-chronic liver failure) [32], primarily characterized determinants or predictors of regeneration rather than evaluating interventions designed to actively promote it [28,31,32].
Taken together, these studies indicate that liver regeneration may be influenced by a wide spectrum of strategies, including technical interventions, perioperative optimization, pharmacologic treatments, nutritional support, and emerging molecular approaches. Nevertheless, the available evidence remains markedly heterogeneous with respect to patient populations, underlying hepatic pathology, study design, and outcome measures. Many of the studies reporting favorable effects are limited by small sample sizes, single-center enrollment, reliance on surrogate volumetric endpoints, or highly selected cohorts, all of which constrain the external validity of their findings. In addition, a substantial proportion of the literature focuses on biomarkers or prognostic correlates of regeneration rather than on interventions capable of improving clinically meaningful outcomes. Future investigations should therefore prioritize adequately powered multicenter randomized trials employing standardized definitions of regeneration, integrated volumetric and functional endpoints, and extended follow-up, in order to determine whether accelerated regenerative responses translate into reduced rates of post-hepatectomy liver failure, improved operative safety, and superior survival outcomes. Further research is also warranted to define the setting-specific efficacy of these strategies in steatotic or cirrhotic livers, living donor transplantation, and extended hepatectomy, as well as to explore biomarker-informed approaches for personalized regenerative support.
In conclusion, current literature supports the concept that liver regeneration is not simply a passive biological response to tissue loss, but a process that can be significantly influenced by specific perioperative, nutritional, technical, and molecular interventions. The most clinically relevant implication is that strategies aimed at optimizing the future liver remnant, whether through portal vein modulation, metabolic support, lifestyle optimization, or emerging targeted therapies, may increase the pool of patients eligible for major hepatectomy and reduce the risk of postoperative liver insufficiency. At the same time, the translation of these findings into routine practice requires careful patient selection and stronger evidence linking enhanced regenerative kinetics to tangible clinical benefits. The key message is therefore two-fold: regenerative support is a promising addition to modern hepatobiliary surgery, and its integration into clinical decision-making should be evidence-driven, context-specific, and guided by both volumetric and functional assessment of the remnant liver.
5. Conclusions: Impact in the Context of Translational Approaches and Future Studies
Liver regeneration is a remarkable example of physiological tissue repair in humans and is crucial for recovery after major hepatic injury or surgical resection. The studies discussed in this article show that hepatic regeneration is a complex, highly regulated process that can be influenced by multiple therapeutic strategies. Interventions targeting portal hemodynamics, metabolic support, inflammatory signaling, cellular therapy, and emerging molecular pathways demonstrate that regenerative capacity can be modulated in meaningful ways. One of the most clinically relevant strategies is optimizing the future liver remnant (FLR) before major resection. PVE remains the cornerstone of this approach, as it redirects portal blood flow toward the non-embolized liver segments and stimulates compensatory hypertrophy of the remnant parenchyma. However, the evidence discussed in this review indicates that technical interventions alone may not always be sufficient to ensure adequate regenerative recovery, particularly in patients with compromised liver quality due to steatosis, fibrosis, chemotherapy-associated injury, or metabolic comorbidities. Consequently, increasing attention has shifted toward combined strategies that integrate hemodynamic modulation with pharmacologic or metabolic support.
The addition of autologous CD133⁺ bone marrow–derived stem cells to PVE exemplifies a translational approach aimed at enhancing the endogenous regenerative response. Clinical studies have demonstrated that this combination can significantly increase the hypertrophy of the FLR and accelerate its growth rate compared with PVE alone, potentially allowing earlier and safer resection in patients with critically low residual liver volumes. These findings support the concept that circulating progenitor cells may participate in regeneration either through direct differentiation into hepatocyte-like cells or through paracrine mechanisms that modify the hepatic microenvironment. Although still limited by small patient cohorts and single-center experiences, this strategy highlights the broader therapeutic potential of regenerative medicine in hepatobiliary surgery.
Metabolic and nutritional interventions also represent a promising avenue for translational research. Branched-chain amino acid supplementation, for example, has been shown to improve functional regeneration and hepatic metabolic performance following PVE and major hepatectomy, suggesting that targeted nutritional support may facilitate recovery of liver function even when volumetric growth is modest. Similarly, postoperative administration of ursodeoxycholic acid has been associated with improved liver function parameters in living donors after hepatectomy, indicating that hepatoprotective agents may play a supportive role during the early regenerative phase. Lifestyle optimization before surgery has also emerged as an effective strategy, demonstrating that preoperative interventions aimed at reducing steatosis and improving metabolic fitness can enhance postoperative regeneration and graft outcomes. Beyond metabolic interventions, pharmacologic modulation of inflammatory signaling pathways has shown encouraging results. Pentoxifylline, a phosphodiesterase inhibitor with anti-inflammatory properties, has been shown to enhance regeneration in patients with small liver remnants, potentially through modulation of interleukin-6 signaling pathways. While the benefits appear most pronounced in patients with critically reduced residual liver volumes, these findings underscore the importance of cytokine-mediated signaling networks in the regulation of hepatocyte proliferation.
Recent translational advances have also identified novel molecular targets capable of directly modulating hepatocyte proliferation. Among these, inhibition of MKK4 represents one of the most innovative developments. Preclinical studies have demonstrated that pharmacologic inhibition of MKK4 with the small-molecule compound HRX215 markedly enhances hepatocyte proliferation and accelerates liver regeneration after partial hepatectomy. In large-animal models, this approach has even enabled survival following otherwise lethal extended hepatectomy, highlighting its potential to prevent post-hepatectomy liver failure. Importantly, early-phase clinical evaluation has shown favorable pharmacokinetics and safety profiles in healthy volunteers, providing the first step toward clinical translation. Nevertheless, the therapeutic efficacy of MKK4 inhibition in patients with impaired regenerative capacity remains to be established in well-designed clinical trials.
In parallel with therapeutic interventions, a growing body of research is identifying biomarkers capable of predicting regenerative performance and guiding clinical decision-making. Observational studies have shown that platelet-derived serotonin levels correlate with regenerative capacity and postoperative outcomes, suggesting that platelet signaling pathways play a significant role in hepatic repair. Similarly, perioperative dynamics of von Willebrand factor have been associated with platelet accumulation within the regenerating liver and with postoperative regenerative success, providing further evidence of the interplay between vascular biology, platelet activation, and hepatocyte proliferation. Although these markers currently serve primarily as predictors rather than therapeutic targets, their integration into perioperative risk stratification may enable more personalized approaches to liver surgery.
Despite these promising advances, several limitations must be acknowledged. The clinical studies available to date remain heterogeneous in terms of patient populations, underlying liver disease, surgical procedures, and outcome measures. Many trials rely on surrogate endpoints such as volumetric liver growth rather than clinically meaningful outcomes such as postoperative liver failure or long-term survival. Moreover, the small sample sizes and single-center designs of many studies limit the generalizability of their findings. For these reasons, translating experimental insights into routine clinical practice requires careful validation through adequately powered multicenter randomized trials.
Future research should therefore focus on integrating multiple complementary approaches to optimize hepatic regeneration. This includes combining technical strategies such as portal flow modulation with pharmacologic agents, metabolic interventions, and regenerative therapies targeting specific molecular pathways. In addition, advances in systems biology, metabolomics, and biomarker discovery may allow the development of predictive models capable of identifying patients at high risk for postoperative liver insufficiency. Such approaches would enable personalized perioperative strategies tailored to the regenerative capacity of each patient.
In conclusion, the expanding body of clinical and experimental evidence reviewed here supports the concept that liver regeneration is a dynamic and therapeutically modifiable process (Figure 3). Interventions ranging from portal vein modulation and stem cell therapy to nutritional supplementation and targeted molecular inhibitors have demonstrated the potential to enhance hepatic regenerative responses. Among these strategies, emerging targeted therapies such as MKK4 inhibition represent particularly promising candidates for future translational research. However, the integration of these approaches into clinical practice will require robust evidence demonstrating not only improved regenerative kinetics but also meaningful reductions in postoperative liver failure and improvements in patient survival. Ultimately, advances in molecular physiology and clinical pharmacology of liver regeneration may expand the boundaries of hepatobiliary surgery and improve outcomes for patients undergoing major hepatic resection or suffering from acute and chronic liver disease.
Author Contributions
Conceptualization, A.L. and R.W.; methodology, A.L. and RW.; data curation, A.L. and RW.; writing—original draft preparation, A.L. and RW.; writing—review and editing, A.L. and RW.; visualization, A.L. and RW.; supervision, A.L. and RW.; project administration, A.L. and RW. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
During the preparation of this manuscript/study, the authors used Copilot for creating original illustrations based on the text. Additionally, the same AI tool was used to edit English and to identify specific references supporting the text. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
A. L. serves on the Editorial Board of the International Journal of Molecular Sciences. However, he was involved in any stage of the editorial handling of this manuscript. R. W. has nothing to declare.
Abbreviations
The following abbreviations are used in this manuscript:
| AFP | Alpha-fetoprotein |
| ALB | Albumin |
| ALP | Alkaline phosphatase |
| ALT | Alanine aminotransferase |
| AST | Aspartate aminotransferase |
| AUROC | Area under the receiver operating characteristic curve |
| BCAA | Branched-chain amino acids |
| CCC | Cholangiocellular carcinoma |
| CT | Computed tomography |
| CTx | Chemotherapy |
| EGF | Epidermal growth factor |
| EGFR | Epidermal growth factor receptor |
| FLR | Future liver remnant |
| FLRV | Future liver remnant volume |
| HBV | Hepatitis B virus |
| HBV-ACLF | Hepatitis B virus–associated acute-on-chronic liver failure |
| HCC | Hepatocellular carcinoma |
| HGF | Hepatocyte growth factor |
| HRX215 | Mitogen-activated protein kinase kinase-4 inhibitor (investigational compound) |
| ICG | Indocyanine green |
| IL-6 | Interleukin-6 |
| INR | International normalized ratio |
| LD | Liver dysfunction |
| LR | Liver regeneration |
| MAPK | Mitogen-activated protein kinase |
| MKK4 | Mitogen-activated protein kinase kinase-4 |
| mCRC | Metastatic colorectal cancer |
| NBCA | N-butyl cyanoacrylate |
| NF-κB | Nuclear factor-κB |
| PDR | Plasma disappearance rate |
| PH | Partial hepatectomy |
| POD | Postoperative day |
| PT | Prothrombin time |
| PVE | Portal vein embolization |
| PVA | Polyvinyl alcohol |
| RCT | Randomized controlled trial |
| RgLV | Regenerated liver volume |
| RLV | Remnant liver volume |
| STAT3 | Signal transducer and activator of transcription-3 |
| TBIL | Total bilirubin |
| TGF-β | Transforming growth factor-β |
| TNF-α | Tumor necrosis factor-α |
| TTK | Tonifying the kidney to promote liver regeneration and repair by affecting stem cells and their microenvironment |
| TQD | Tonifying qi and detoxification |
| UDCA | Ursodeoxycholic acid |
| vWF | von Willebrand factor |
| Wnt | Wingless signaling pathway |
| YAP | Yes-associated protein |
References
- Liu Q, Wang S, Fu J, Chen Y, Xu J, Wei W, Song H, Zhao X, Wang H. Liver regeneration after injury: Mechanisms, cellular interactions and therapeutic innovations. Clin Transl Med. 2024;14(8):e1812. [CrossRef]
- Mao SA, Glorioso JM, Nyberg SL. Liver regeneration. Transl Res. 2014 Apr;163(4):352-62. [CrossRef]
- Weiskirchen R, Lonardo A. Lipids at the helm: a metabolic playbook for liver regeneration. Metab Target Organ Damage. 2026;6:8. doi: 10.20517/mtod.2025.222.
- Korchilava B, Khachidze T, Megrelishvili N, Svanadze L, Kakabadze M, Tsomaia K, Jintcharadze M, Kordzaia D. Liver regeneration after partial hepatectomy: Triggers and mechanisms. World J Hepatol. 2025;17(7):107378. [CrossRef]
- Wirth KM, Kizy S, Steer CJ. Liver Regeneration in the Acute Liver Failure Patient. Clin Liver Dis. 2018;22(2):269-287. [CrossRef]
- Huppert SS, Campbell KM. Emerging advancements in liver regeneration and organogenesis as tools for liver replacement. Curr Opin Organ Transplant. 2016;21(6):581-587. [CrossRef]
- Nature Index Associating Liver Partition and Portal Vein Ligation Techniques in Hepatic Surgery. Available at: https://www.nature.com/nature-index/topics/l4/associating-liver-partition-and-portal-vein-ligation-techniques-in-hepatic-surgery (last accessed 23 May 2026).
- Hora S, Wuestefeld T. Liver Injury and Regeneration: Current Understanding, New Approaches, and Future Perspectives. Cells. 2023;12(17):2129. [CrossRef]
- Rodimova S, Mozherov A, Elagin V, Karabut M, Shchechkin I, Kozlov D, Krylov D, Gavrina A, Bobrov N, Zagainov V, Zagaynova E, Kuznetsova D. Effect of Hepatic Pathology on Liver Regeneration: The Main Metabolic Mechanisms Causing Impaired Hepatic Regeneration. Int J Mol Sci. 2023;24(11):9112. [CrossRef]
- Serenari M, Ratti F, Hilal MA, Ardito F, Berardi G, Boggi U, Cappelli A, Cescon M, Cillo U, Cucchetti A, De Carlis L, De Cobelli F, Di Benedetto F, Ercolani G, Ettorre GM, Fedi M, Ferrero A, Giuliante F, Grazi GL, Gringeri E, Gruttadauria S, Izzo F, Maestri M, Magistri P, Massani M, Mazzaferro V, Memeo R, Mocchegiani F, Mosconi C, Patrono D, Ravaioli M, Romano F, Rompianesi G, Russolillo N, Ruzzenente A, Sposito C, Troisi R, Vennarecci G, Viganò L, Vivarelli M, Zanus G, Baptista PM, Oldhafer K, Schadde E, Aldrighetti L, Jovine E. Liver hypertrophy techniques: a position paper from the Italian Group of Regenerative and Occlusive Worldwide-used techniques of hepatic Hypertrophy (I GROWtoH). Updates Surg. 2025;77(8):2155-2171. [CrossRef]
- Gong D, Mo J, Zhai M, Zhou F, Wang G, Ma S, Dai X, Deng X. Advances, challenges and future applications of liver organoids in experimental regenerative medicine. Front Med (Lausanne). 2025;11:1521851. [CrossRef]
- Choi S, Jeong J. Mesenchymal Stromal/Stem Cell-Based Therapies for Liver Regeneration: Current Status and Future Directions. Int J Mol Sci. 2026;27(2):619. [CrossRef]
- Wang N, Guo M, Zhang C, Jiang R, Bi J, Sun J, Liu B. Liver regeneration: unraveling the molecular mechanisms and clinical application. J Transl Med. 2025;23(1):1409. [CrossRef]
- Ma X, Huang T, Chen X, Li Q, Liao M, Fu L, Huang J, Yuan K, Wang Z, Zeng Y. Molecular mechanisms in liver repair and regeneration: from physiology to therapeutics. Signal Transduct Target Ther. 2025;10(1):63. [CrossRef]
- Zhang C, Sun C, Zhao Y, Ye B, Yu G. Signaling pathways of liver regeneration: Biological mechanisms and implications. iScience 2023;27(1):108683. [CrossRef]
- Zhao Y, Ye W, Wang YD, Chen WD. HGF/c-Met: A Key Promoter in Liver Regeneration. Front Pharmacol. 2022;13:808855. [CrossRef]
- Ye B, Yue M, Chen H, Sun C, Shao Y, Jin Q, Zhang C, Yu G. YAP/TAZ as master regulators in liver regeneration and disease: insights into mechanisms and therapeutic targets. Mol Biol Rep. 2024;52(1):78. [CrossRef]
- Arendt E, Ueberham U, Bittner R, Gebhardt R, Ueberham E. Enhanced matrix degradation after withdrawal of TGF-beta1 triggers hepatocytes from apoptosis to proliferation and regeneration. Cell Prolif. 2005;38(5):287-99. [CrossRef]
- Beppu T, Nitta H, Hayashi H, Imai K, Okabe H, Nakagawa S, Hashimoto D, Chikamoto A, Ishiko T, Yoshida M, Yamashita Y, Baba H. Effect of branched-chain amino acid supplementation on functional liver regeneration in patients undergoing portal vein embolization and sequential hepatectomy: a randomized controlled trial. J Gastroenterol. 2015;50(12):1197-205. [CrossRef]
- Fürst G, Schulte am Esch J, Poll LW, Hosch SB, Fritz LB, Klein M, Godehardt E, Krieg A, Wecker B, Stoldt V, Stockschläder M, Eisenberger CF, Mödder U, Knoefel WT. Portal vein embolization and autologous CD133+ bone marrow stem cells for liver regeneration: initial experience. Radiology 2007;243(1):171-9. [CrossRef]
- Knoefel WT, Alexander A, Tustas RY, Schmelzle M, Klein HM, Krieg A, Topp SA, Eisenberger CF, Fuerst G, Schulte am Esch J 2nd. Stammzell-induzierte Leberregeneration [Stem cell-induced liver regeneration]. Zentralbl Chir. 2013;138(2):166-72. German. [CrossRef]
- Petrowsky H, Breitenstein S, Slankamenac K, Vetter D, Lehmann K, Heinrich S, DeOliveira ML, Jochum W, Weishaupt D, Frauenfelder T, Graf R, Clavien PA. Effects of pentoxifylline on liver regeneration: a double-blinded, randomized, controlled trial in 101 patients undergoing major liver resection. Ann Surg. 2010;252(5):813-22. [CrossRef]
- Starlinger P, Assinger A, Haegele S, Wanek D, Zikeli S, Schauer D, Birner P, Fleischmann E, Gruenberger B, Brostjan C, Gruenberger T. Evidence for serotonin as a relevant inducer of liver regeneration after liver resection in humans. Hepatology 2014;60(1):257-66. [CrossRef]
- Starlinger P, Pereyra D, Haegele S, Braeuer P, Oehlberger L, Primavesi F, Kohler A, Offensperger F, Reiberger T, Ferlitsch A, Messner B, Beldi G, Staettner S, Brostjan C, Gruenberger T. Perioperative von Willebrand factor dynamics are associated with liver regeneration and predict outcome after liver resection. Hepatology 2018;67(4):1516-1530. [CrossRef]
- Zwirner S, Abu Rmilah AA, Klotz S, Pfaffenroth B, Kloevekorn P, Moschopoulou AA, Schuette S, Haag M, Selig R, Li K, Zhou W, Nelson E, Poso A, Chen H, Amiot B, Jia Y, Minshew A, Michalak G, Cui W, Rist E, Longerich T, Jung B, Felgendreff P, Trompak O, Premsrirut PK, Gries K, Muerdter TE, Heinkele G, Wuestefeld T, Shapiro D, Weissbach M, Koenigsrainer A, Sipos B, Ab E, Zacarias MO, Theisgen S, Gruenheit N, Biskup S, Schwab M, Albrecht W, Laufer S, Nyberg S, Zender L. First-in-class MKK4 inhibitors enhance liver regeneration and prevent liver failure. Cell. 2024;187(7):1666-1684.e26. [CrossRef]
- Ibis C, Asenov Y, Akin M, Azamat IF, Sivrikoz N, Gurtekin B. Factors Affecting Liver Regeneration in Living Donors After Hepatectomy. Med Sci Monit. 2017 Dec 18;23:5986-5993. [CrossRef]
- Harrison PM, Hughes RD, Forbes A, Portmann B, Alexander GJ, Williams R. Failure of insulin and glucagon infusion to stimulate liver regeneration in fulminant hepatic failure. J Hepatol. 1990;10(3):332-6. [CrossRef]
- Zappa M, Dondero F, Sibert A, Vullierme MP, Belghiti J, Vilgrain V. Liver regeneration at day 7 after right hepatectomy: global and segmental volumetric analysis by using CT. Radiology 2009;252(2):426-32. [CrossRef]
- Rayes N, Pilarski T, Stockmann M, Bengmark S, Neuhaus P, Seehofer D. Effect of pre- and probiotics on liver regeneration after resection: a randomised, double-blind pilot study. Benef Microbes. 2012;3(3):237-44. [CrossRef]
- Li HM, Ye ZH, Zhang J, Gao X, Chen YM, Yao X, Gu JX, Zhan L, Ji Y, Xu JL, Zeng YH, Yang F, Xiao L, Sheng GG, Xin W, Long Q, Zhu QJ, Shi ZH, Ruan LG, Yang JY, Li CC, Wu HB, Chen SD, Luo XL. Clinical trial with traditional Chinese medicine intervention ''tonifying the kidney to promote liver regeneration and repair by affecting stem cells and their microenvironment'' for chronic hepatitis B-associated liver failure. World J Gastroenterol. 2014;20(48):18458-65. [CrossRef]
- Gong WF, Zhong JH, Lu Z, Zhang QM, Zhang ZY, Chen CZ, Liu X, Ma L, Zhang ZM, Xiang BD, Li LQ. Evaluation of liver regeneration and post-hepatectomy liver failure after hemihepatectomy in patients with hepatocellular carcinoma. Biosci Rep. 2019;39(8):BSR20190088. [CrossRef]
- Wang X, Sun M, Yang X, Gao L, Weng M, Yang D, Li H, Zhou X, Li J, Qin S, Zhou D, Wu X, Tang S, Zeng W. Value of Liver Regeneration in Predicting Short-Term Prognosis for Patients with Hepatitis B-Related Acute-on-Chronic Liver Failure. Biomed Res Int. 2020;2020:5062873. [CrossRef]
- Luz JHM, Veloso Gomes F, Costa NV, Vasco I, Coimbra E, Luz PM, Marques HP, Coelho JS, Mega RMA, Ribeiro VNTV, da Costa Lamelas JTR, de Sampaio Nunes E Sobral MM, da Silva SRG, de Teixeira Carrelha AS, Rodrigues SCC, de Figueiredo AAFP, Santos MV, Bilhim T. BestFLR Trial: Liver Regeneration at CT before Major Hepatectomies for Liver Cancer-A Randomized Controlled Trial Comparing Portal Vein Embolization with N-Butyl-Cyanoacrylate Plus Iodized Oil versus Polyvinyl Alcohol Particles Plus Coils. Radiology 2021;299(3):715-724. [CrossRef]
- Aloun A, Akbulut S, Garzali IU, Gonultas F, Baskiran A, Hargura AS, Colak C, Yilmaz S. Effect of ursodeoxycholic acid on liver regeneration capacity after living donor hepatectomy: a prospective, randomized, double-blind clinical trial. Eur Rev Med Pharmacol Sci. 2023;27(3):999-1006. [CrossRef]
- Gupta A, Patil NS, Mohapatra N, Benjamin J, Thapar S, Kumar A, Rastogi A, Pamecha V. Lifestyle Optimization Leads to Superior Liver Regeneration in Live Liver Donors and Decreases Early Allograft Dysfunction in Recipients: A Randomized Control Trial. Ann Surg. 2023;278(3):e430-e439. [CrossRef]
- Abhinaya SV, Garg N, Sindwani G, Arora MK, Thapar S, Thomas S, Pamecha V, Sarin SK. Comparison of the effect of isoflurane and propofol on liver regeneration after donor hepatectomy - A randomized controlled trial. J Clin Anesth. 2025;104:111859. [CrossRef]
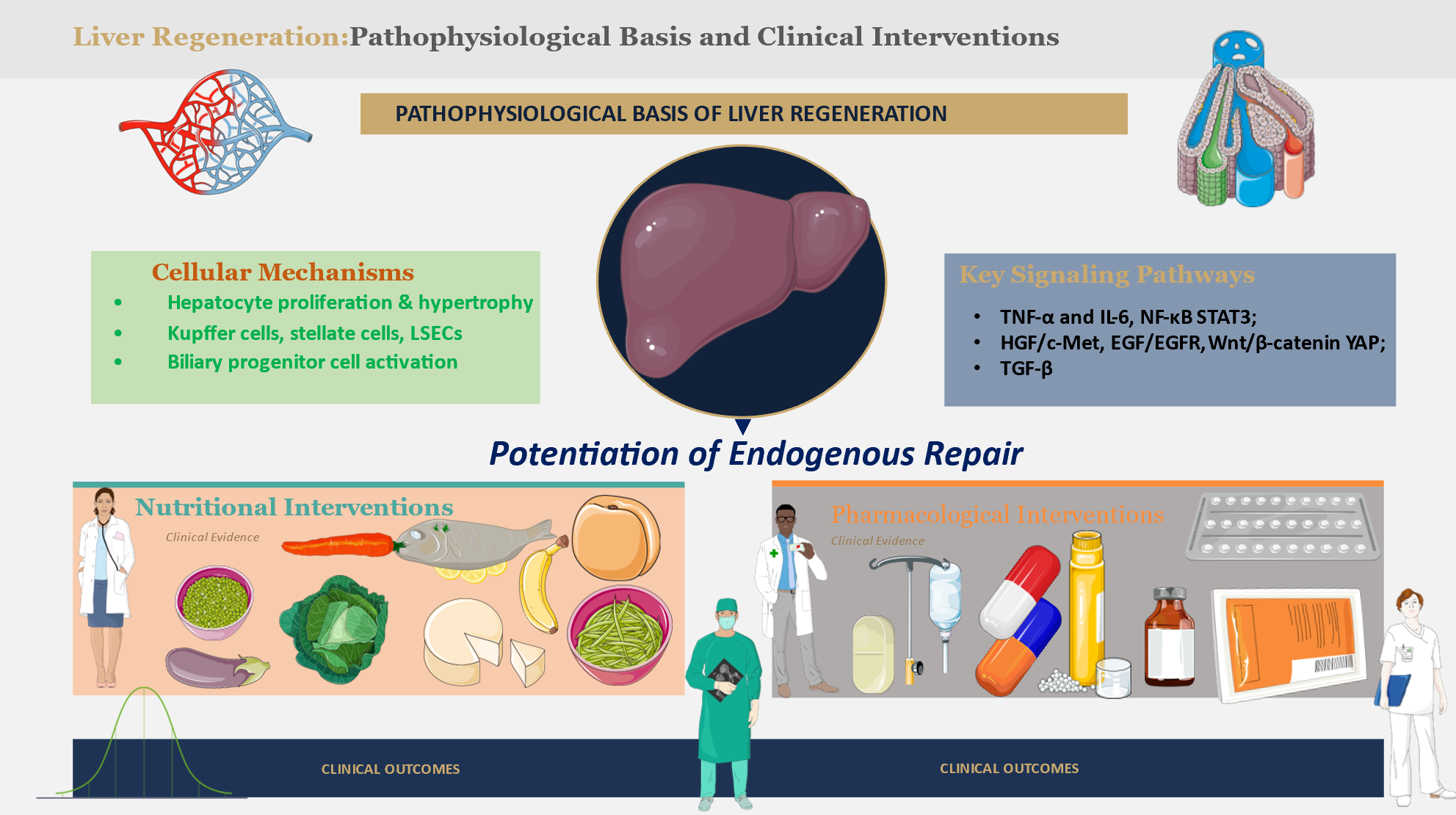
Figure 1.
Major molecular pathways regulating liver regeneration. Liver regeneration is a coordinated process that restores hepatic mass and function after injury or surgical resection through sequential priming, proliferative, and termination phases. During the priming phase, inflammatory cytokines such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), released primarily by Kupffer cells, activate transcriptional pathways including nuclear factor-κB (NF-κB) and signal transducer and activator of transcription-3 (STAT3), enabling quiescent hepatocytes to reenter the cell cycle. The proliferative phase is driven by mitogenic signaling cascades such as hepatocyte growth factor (HGF)/c-Met and epidermal growth factor (EGF)/epidermal growth factor receptor (EGFR), together with developmental pathways including Wnt/β-catenin and Hippo/Yes-associated protein (YAP), which promote hepatocyte proliferation and expansion of liver mass. Portal hemodynamics, platelet-derived mediators such as serotonin, and endothelial factors including von Willebrand factor further modulate the regenerative response. Regeneration is ultimately restrained by termination signals, including transforming growth factor-β (TGF-β)-mediated pathways and extracellular matrix remodeling, which restore hepatic homeostasis and prevent excessive proliferation. Pharmacologic and metabolic interventions, including branched-chain amino acids, modulation of portal flow, and inhibition of mitogen-activated protein kinase kinase-4 (MKK4), may enhance regenerative signaling within this framework.
Figure 1.
Major molecular pathways regulating liver regeneration. Liver regeneration is a coordinated process that restores hepatic mass and function after injury or surgical resection through sequential priming, proliferative, and termination phases. During the priming phase, inflammatory cytokines such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), released primarily by Kupffer cells, activate transcriptional pathways including nuclear factor-κB (NF-κB) and signal transducer and activator of transcription-3 (STAT3), enabling quiescent hepatocytes to reenter the cell cycle. The proliferative phase is driven by mitogenic signaling cascades such as hepatocyte growth factor (HGF)/c-Met and epidermal growth factor (EGF)/epidermal growth factor receptor (EGFR), together with developmental pathways including Wnt/β-catenin and Hippo/Yes-associated protein (YAP), which promote hepatocyte proliferation and expansion of liver mass. Portal hemodynamics, platelet-derived mediators such as serotonin, and endothelial factors including von Willebrand factor further modulate the regenerative response. Regeneration is ultimately restrained by termination signals, including transforming growth factor-β (TGF-β)-mediated pathways and extracellular matrix remodeling, which restore hepatic homeostasis and prevent excessive proliferation. Pharmacologic and metabolic interventions, including branched-chain amino acids, modulation of portal flow, and inhibition of mitogen-activated protein kinase kinase-4 (MKK4), may enhance regenerative signaling within this framework.

Figure 2.
Schematic overview of the principal evidence-based strategies shown to enhance liver regeneration based on references listed in Table 1. These comprise quite heterogenous strategies spanning from lifestyle changes to traditional Chinese Medicine, repurposed available drugs, and new drug agents. Original illustration created using Servier Medical ART (SMART) and licensed under the Creative Commons Attribution 4.0 International License (CC BY 4.0). List of abbreviations used: BCAA, branched-chain amino acids; CD133+, cells expressing CD133 protein on their surface; MKK4, MAP kinase kinase 4; NBCA, n-butyl cyanoacrylate; PVE, portal vein embolization; TTK, tonifying the kidney to promote liver regeneration and repair by affecting stem cells and their microenvironment.
Figure 2.
Schematic overview of the principal evidence-based strategies shown to enhance liver regeneration based on references listed in Table 1. These comprise quite heterogenous strategies spanning from lifestyle changes to traditional Chinese Medicine, repurposed available drugs, and new drug agents. Original illustration created using Servier Medical ART (SMART) and licensed under the Creative Commons Attribution 4.0 International License (CC BY 4.0). List of abbreviations used: BCAA, branched-chain amino acids; CD133+, cells expressing CD133 protein on their surface; MKK4, MAP kinase kinase 4; NBCA, n-butyl cyanoacrylate; PVE, portal vein embolization; TTK, tonifying the kidney to promote liver regeneration and repair by affecting stem cells and their microenvironment.

Figure 3.
Translational framework for therapeutic enhancement of liver regeneration. Liver regeneration research increasingly follows a translational continuum that connects fundamental biological discoveries with clinical strategies aimed at improving outcomes after liver injury or resection. At the mechanistic level, regeneration is governed by complex networks involving inflammatory cytokines, growth-factor signaling, metabolic pathways, and platelet-mediated interactions that regulate hepatocyte proliferation and tissue remodeling. Insights from these pathways have enabled the identification of experimental therapeutic targets, including pharmacologic modulation of intracellular signaling pathways and regenerative cell-based approaches designed to amplify endogenous repair mechanisms. These discoveries have progressively informed clinical interventions such as portal vein embolization, stem-cell–assisted regenerative strategies, metabolic and nutritional support including branched-chain amino acid supplementation, pharmacologic modulation of inflammatory pathways, and perioperative optimization measures. Emerging molecular therapies, including inhibition of mitogen-activated protein kinase kinase-4 (MKK4), represent a new generation of targeted approaches aimed at directly stimulating hepatocyte proliferation in the context of liver injury or surgical resection. Future progress is expected to rely on the integration of molecular biomarkers, functional imaging, and individualized perioperative strategies to enable personalized regenerative support and expand the safety of major hepatobiliary surgery.
Figure 3.
Translational framework for therapeutic enhancement of liver regeneration. Liver regeneration research increasingly follows a translational continuum that connects fundamental biological discoveries with clinical strategies aimed at improving outcomes after liver injury or resection. At the mechanistic level, regeneration is governed by complex networks involving inflammatory cytokines, growth-factor signaling, metabolic pathways, and platelet-mediated interactions that regulate hepatocyte proliferation and tissue remodeling. Insights from these pathways have enabled the identification of experimental therapeutic targets, including pharmacologic modulation of intracellular signaling pathways and regenerative cell-based approaches designed to amplify endogenous repair mechanisms. These discoveries have progressively informed clinical interventions such as portal vein embolization, stem-cell–assisted regenerative strategies, metabolic and nutritional support including branched-chain amino acid supplementation, pharmacologic modulation of inflammatory pathways, and perioperative optimization measures. Emerging molecular therapies, including inhibition of mitogen-activated protein kinase kinase-4 (MKK4), represent a new generation of targeted approaches aimed at directly stimulating hepatocyte proliferation in the context of liver injury or surgical resection. Future progress is expected to rely on the integration of molecular biomarkers, functional imaging, and individualized perioperative strategies to enable personalized regenerative support and expand the safety of major hepatobiliary surgery.


Table 1.
Summary of main studies on liver regeneration ordered chronologically.
| Author/Year | Method | Findings | Conclusions |
|---|---|---|---|
| Harrison et al., 1990 [27] | RCT in 18 patients with fulminant hepatic failure; insulin plus glucagon infusion versus control. | No reduction in mortality and no improvement in hepatic synthetic function or histologic regeneration. | Insulin and glucagon did not stimulate liver regeneration in this setting. |
| Fürst et al., 2007 [20] | Prospective comparative study of PVE with or without autologous CD133+ stem cells in patients with low FLRV. | Greater absolute and relative FLRV increase and faster daily liver growth in the stem-cell group. | Adding CD133+ bone marrow stem cells to PVE enhanced liver regeneration compared with PVE alone. |
| Zappa et al., 2009 [28] | Preoperative and postoperative day-7 CT volumetric analysis after right hepatectomy in 27 patients. | A 64% increase in remnant liver volume; lower segmental regeneration when the middle hepatic vein was harvested. | Early liver regeneration varies by segment and is influenced by venous outflow. |
| Petrowsky et al., 2010 [22] | Double-blind RCT in 101 patients undergoing major liver resection; pentoxifylline versus placebo. | Better volumetric regeneration in small remnant livers, lower AST levels, but more drug-related adverse events. | Pentoxifylline may enhance regeneration in small liver remnants, likely through IL-6 signaling. |
| Rayes et al., 2012 [29] | Double-blind randomized pilot study in 19 patients; synbiotics versus placebo fiber after right hepatectomy. | Overall liver function was similar between groups; a possible benefit appeared in patients without complications, but numbers were small. | Synbiotics may improve postoperative liver function, but larger studies are needed. |
| Knoefel et al., 2013 [21] | Study of PVE combined with CD133+ bone marrow stem cells versus PVE alone in patients with critically low FLRV. | Significantly greater FLRV increase, faster daily growth, and shorter time to surgery with stem-cell support. | PVE plus stem-cell therapy may make resection safer in high-risk patients. |
| Li et al., 2014 [30] | RCT in 144 patients with chronic hepatitis B-associated liver failure; traditional Chinese medicine regimens versus control. | Lower mortality and improvement in selected biochemical parameters in the treated groups, especially the TTK group. | The TTK intervention may improve survival and support liver function and regeneration. |
| Starlinger et al., 2014 [23] | Perioperative observational clinical study in 60 patients undergoing liver resection; platelet serotonin monitoring. | Low preoperative intraplatelet serotonin was associated with delayed regeneration and higher risk of liver dysfunction. | Platelet serotonin may serve as a predictive marker of liver regeneration and postoperative outcome. |
| Beppu et al., 2015 [19] | RCT in patients undergoing PVE followed by hepatectomy; BCAA supplementation versus control. | Improved functional liver regeneration and liver function in the BCAA group. | BCAAs improve functional regeneration and liver function after PVE and major hepatectomy. |
| Starlinger et al., 2018 [24] | Clinical study of perioperative von Willebrand factor dynamics in patients undergoing liver resection. | An early vWF surge was associated with adequate regeneration; high preoperative levels predicted postoperative dysfunction. | vWF is involved in liver regeneration and may be useful for preoperative risk stratification. |
| Gong et al., 2019 [31] | Clinical study in 125 patients with hepatocellular carcinoma after hemihepatectomy; serial assessment of remnant liver volume. | %FLRV below 42.7% predicted liver failure; FLRV, %FLRV, and cirrhosis influenced regeneration. | Functional remnant liver volume is a strong predictor of regeneration and post-hepatectomy liver failure. |
| Wang et al., 2020 [32] | Prognostic study in 308 patients with HBV-ACLF; development of the TACIA score using regeneration-related biomarkers. | Creatinine, age, bilirubin, AFP, and INR were independent predictors; the model showed good AUROC performance. | The TACIA score effectively predicts short-term survival in patients with HBV-ACLF. |
| Luz et al., 2021 [33] | RCT of pre-hepatectomy portal vein embolization; NBCA plus iodized oil versus PVA plus coils. | Faster and greater liver regeneration with NBCA; more patients became eligible for surgery earlier. | NBCA plus iodized oil was superior to PVA plus coils in promoting future liver remnant hypertrophy. |
| Aloun et al. 2023 [34] | Prospective double-blind RCT in 60 living liver donors; postoperative UDCA versus no UDCA. | Improved INR and several liver function test results in the UDCA group. | Postoperative UDCA improved liver tests in living donors after hepatectomy. |
| Gupta et al., 2023 [35] | RCT in living donors; preoperative lifestyle optimization versus usual routine. | Greater volumetric regeneration, less steatosis, less blood loss, and less early graft dysfunction in recipients. | Lifestyle optimization improved donor liver regeneration and recipient outcomes. |
| Zwirner et al., 2024 [25] | Preclinical and translational study of MKK4 inhibitors, including a first-in-human phase I trial. | Enhanced regeneration in murine and porcine models, survival after extended hepatectomy, and a favorable safety profile for HRX215. | MKK4 inhibitors offer a promising new strategy to prevent liver failure and promote regeneration. |
| Abhinaya et al., 2025 [36] | Randomized controlled pilot trial in 60 donor hepatectomy cases; isoflurane versus propofol. | RgLV at postoperative day 14 was comparable between groups, with no significant differences. | Propofol and isoflurane did not appear to have different effects on liver regeneration after donor hepatectomy. |
Abbreviations: AFP, alpha-fetoprotein; AST, aspartate aminotransferase; AUROC, area under the receiver operating characteristic curve; BCAA, branched-chain amino acids; CT, computed tomography; FLRV, future liver remnant volume; HBV-ACLF, hepatitis B virus-associated acute-on-chronic liver failure; HRX215, investigational compound name; IL-6, interleukin-6; INR, international normalized ratio; MKK4, mitogen-activated protein kinase kinase 4; NBCA, N-butyl cyanoacrylate; PVA, polyvinyl alcohol; PVE, portal vein embolization; RCT, randomized controlled trial; RgLV, regenerated liver volume; TTK, tonifying the kidney to promote liver regeneration and repair by affecting stem cells and their microenvironment; UDCA, ursodeoxycholic acid; vWF, von Willebrand factor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



