Submitted:
23 May 2026
Posted:
25 May 2026
You are already at the latest version
Abstract
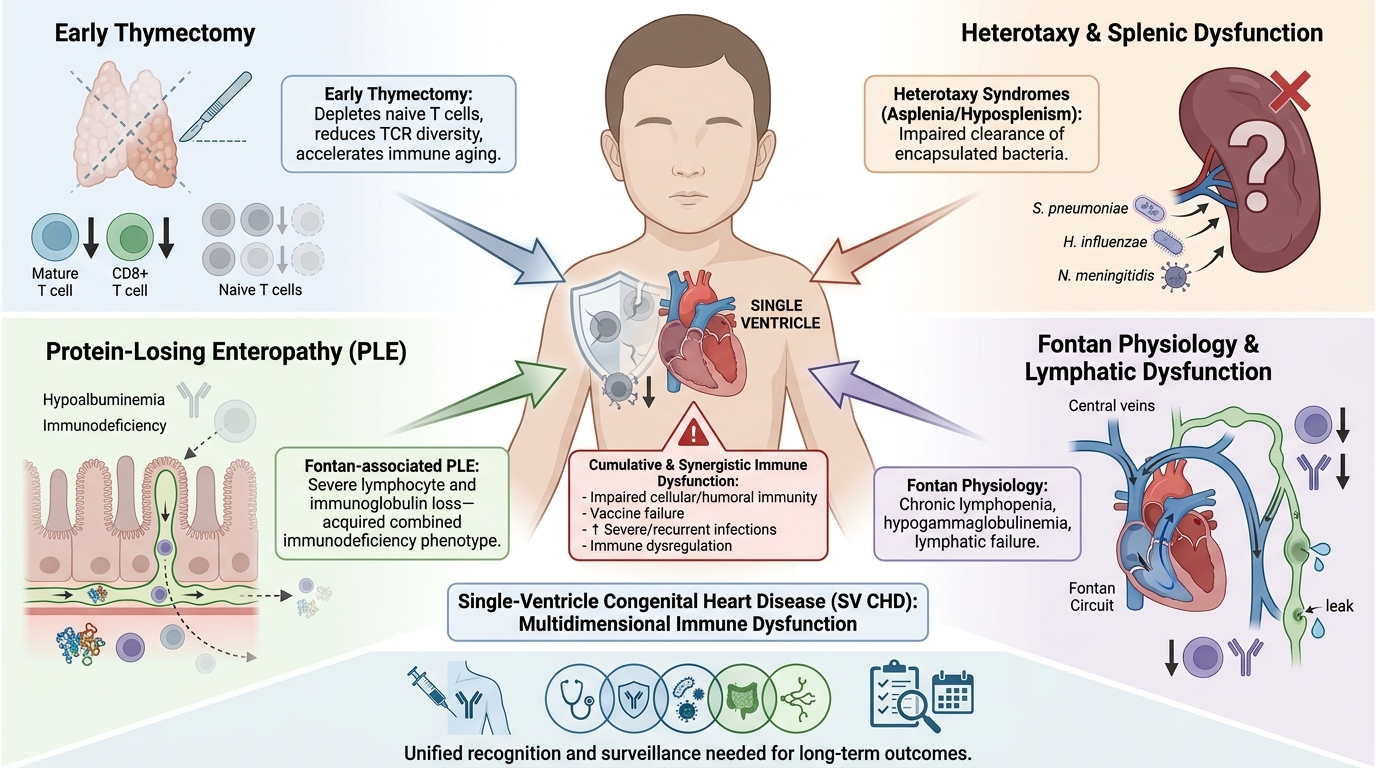
Children with single-ventricle congenital heart disease represent a uniquely vulnerable population in whom immune dysfunction remains underrecognized despite increasing evidence of clinically significant abnormalities affecting both innate and adaptive immunity. Emerging data suggest that immune injury in these patients is multifactorial and cumulative. Early thymectomy during congenital cardiac surgery may impair long-term adaptive immune maturation through depletion of naïve T cells, reduction in T-cell receptor diversity, and premature immune aging. In heterotaxy syndromes, associated asplenia or functional hyposplenism further compromises host defense against encapsulated organisms. Beyond these factors, single-ventricle and Fontan physiology are increasingly linked to lymphopenia, hypogammaglobulinemia, chronic inflammatory stress, and lymphatic dysfunction. Fontan-associated protein-losing enteropathy represents the most severe form of immune depletion, characterized by enteric loss of lymphocytes and immunoglobulins, sometimes producing a phenotype resembling acquired combined immunodeficiency. Recognition of this multidimensional immune phenotype may improve surveillance, vaccination strategies, multidisciplinary management, and long-term outcomes in single-ventricle survivors.
Keywords:
single ventricle
; immune dysregulation
; immunodeficiency
; thymectomy
; heterotaxy
; fontan PLE
Children with single-ventricle congenital heart disease represent one of the most medically fragile populations in pediatric cardiology. Advances in staged surgical palliation and Fontan circulation have significantly improved survival, shifting attention toward the long-term systemic consequences of living with univentricular physiology. Among these consequences, immune dysfunction remains an underrecognized and insufficiently characterized problem despite growing evidence of clinically meaningful abnormalities affecting both innate and adaptive immunity1.
Historically, the immunologic vulnerability of single-ventricle patients has often been viewed through isolated clinical lenses, such as postoperative infection risk, heterotaxy-associated asplenia, or protein-losing enteropathy (PLE). However, emerging evidence suggests that immune dysfunction in this population is multifactorial, cumulative, and biologically interconnected. Several mechanisms may simultaneously contribute to immune injury, including early-life thymectomy during cardiac surgery, splenic dysfunction in heterotaxy syndromes, chronic lymphopenia associated with Fontan physiology, and immune depletion resulting from lymphatic failure and protein-losing enteropathy2.
Importantly, these mechanisms do not occur independently. Instead, they frequently coexist within the same patient, creating a compounded state of immune fragility characterized by impaired T-cell production, altered immune maturation, defective humoral immunity, chronic lymphocyte depletion, impaired vaccine protection, and increased susceptibility to severe infection. In some patients, the resulting phenotype may resemble acquired combined immunodeficiency with broader features of immune dysregulation3.
Despite these observations, immune dysfunction in single-ventricle physiology remains relatively neglected within both pediatric cardiology and immunology literature. Most surveillance frameworks continue to focus predominantly on hemodynamic, ventricular, and Fontan-related complications, while systematic immune assessment is rarely incorporated into routine follow-up.
The aim of this review is therefore to integrate the major contributors to immune dysfunction in single-ventricle congenital heart disease into a unified conceptual framework. Specifically, we review the immunologic consequences of early thymectomy, splenic dysfunction associated with heterotaxy syndromes, and lymphatic-mediated immune depletion in Fontan circulation and protein-losing enteropathy. We further propose that immune dysregulation should be recognized as a central and clinically relevant dimension of single-ventricle disease requiring multidisciplinary surveillance and long-term management.
1. Early Thymectomy and Impaired Adaptive Immune Development
One of the earliest and most important contributors to immune injury in children with single-ventricle congenital heart disease is early thymectomy performed during cardiac surgery. The thymus is essential for the generation of naïve T cells, maintenance of T-cell receptor (TCR) diversity, establishment of central immune tolerance, and preservation of long-term adaptive immune competence. During infancy and early childhood, thymic activity is particularly critical because this period represents the peak of thymopoiesis and immune repertoire development. However, partial or near total thymectomy is commonly performed during congenital cardiac surgery to facilitate operative exposure, especially in patients requiring staged palliation and repeated sternotomies4.
Growing evidence suggests that thymectomy during this vulnerable developmental window may leave a durable and clinically relevant imprint on immune homeostasis. In a 2021 systematic review of 23 studies, Cavalcanti and colleagues demonstrated that thymectomy performed during infancy was consistently associated with lower total T-cell counts, reduced CD4+ and CD8+ lymphocyte subsets, depletion of naïve and CD31+ T cells, lower T-cell receptor excision circles (TRECs), and reduced TCR repertoire diversity, with many of these abnormalities persisting years after surgery5. Earlier studies support these findings. Eysteinsdottir et al. showed that children who underwent partial or total thymectomy during infancy had persistently lower lymphocyte and CD4+ T-cell counts later in life, suggesting long-lasting impairment of thymic-dependent immune maturation6. Halnon et al. similarly demonstrated impaired thymic function and reduced maintenance of peripheral T-cell populations in children with congenital heart disease following surgical thymectomy7,8. Other long-term follow-up studies described persistent depletion of naïve T cells, compensatory peripheral proliferation, oligoclonal memory expansion, narrowing of the TCR repertoire, and features of premature immune aging.
More recent evidence has further expanded understanding of the clinical implications of these immunologic abnormalities. In a 2025 case series by Kymioni et al9., children who underwent early thymectomy during congenital heart surgery demonstrated persistent long-term immune alterations with markedly reduced naïve CD4+ T-cell populations despite variable total lymphocyte counts. Importantly, the clinical manifestations extended beyond isolated laboratory abnormalities and included recurrent respiratory infections, generalized Epstein–Barr virus infection with hepatic fibrosis, lymphadenopathy, splenomegaly, immune cytopenias, hepatosplenomegaly, and evidence of broader immune dysregulation. The authors highlighted that patients shared a common immunophenotype characterized by profoundly inverted naïve-to-memory CD4 ratios, resembling patterns observed in thymic insufficiency syndromes such as 22q11.2 deletion syndrome4.
Importantly, the study also illustrated the heterogeneity of post-thymectomy outcomes. Some patients developed recurrent infections and viral complications, whereas others primarily manifested immune dysregulation and cytopenias despite relatively preserved total T-cell counts. This observation suggests that total lymphocyte numbers alone may underestimate the degree of immune dysfunction, while alterations in naïve T-cell compartments and immune maturation may provide more meaningful insight into long-term immune competence. The report further emphasized that thymectomy may affect not only T-cell quantity but also broader immune architecture, including impaired germinal center responses, reduced switched memory B cells, altered naïve-to-memory balance, and compensatory NK-cell changes10.
Another particularly important observation is the apparent influence of surgical timing. The most profound immune abnormalities were observed in the child who underwent thymectomy during the neonatal period, supporting previous studies suggesting that surgery within the first weeks of life may be associated with more severe and persistent immune consequences. Long-term follow-up studies similarly indicate that early thymectomy may accelerate immunologic aging, reduce thymic regenerative capacity, and produce persistent immune alterations extending into adolescence and adulthood. ⁷
Mechanistically, these changes are thought to result from reduced thymic emigrant production accompanied by compensatory homeostatic peripheral proliferation. Although peripheral expansion may partially preserve absolute lymphocyte counts, it may do so at the expense of repertoire diversity and immune adaptability11. Over time, this may create a state characterized by restricted immune surveillance, impaired responses to novel antigens, altered vaccine responsiveness, chronic immune activation, and potential susceptibility to autoimmunity or immune dysregulation. Indeed, several studies have reported overlap between the immunophenotype of surgically thymectomized children and that seen in genetic thymic insufficiency disorders such as DiGeorge syndrome, particularly regarding depletion of naïve T cells and inversion of naïve-to-memory ratios12.
Collectively, these findings suggest that early thymectomy should not be viewed as a benign surgical byproduct but rather as a potentially important contributor to long-term immune vulnerability in children with complex congenital heart disease. This issue may be especially relevant in single-ventricle patients, who frequently require repeated surgeries, prolonged intensive care exposure, and chronic medical follow-up. Within this population, thymectomy may therefore represent the first immunologic insult in a broader multifactorial process of immune dysfunction that later becomes amplified by Fontan physiology, lymphatic abnormalities, and protein-losing enteropathy.
2. Heterotaxy, Asplenia, and Splenic Immune Dysfunction
The second major axis of immune vulnerability in single-ventricle disease is splenic dysfunction associated with heterotaxy syndromes. Many congenital heart defects culminating in functional single-ventricle palliation arise in the setting of heterotaxy, particularly right atrial isomerism and asplenia syndrome. In these patients, splenic abnormalities are not incidental extracardiac findings, but part of a broader developmental disorder strongly associated with severe cardiac malformations and univentricular pathways10.
The spleen plays a critical role in immune defense through clearance of blood-borne pathogens, maintenance of IgM memory B-cell populations, opsonization, and generation of antibody responses against encapsulated organisms. Consequently, anatomic asplenia or functional hyposplenism markedly increases susceptibility to invasive bacterial infection, particularly due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis13.
Importantly, the relationship between heterotaxy and immune dysfunction appears more complex than a simple “presence or absence of splenic tissue” model. Several studies have documented severe bacteremia and overwhelming sepsis even in patients with polysplenia or anatomically normal spleens, suggesting that splenic anatomy does not necessarily predict preserved splenic immune function. Functional hyposplenism may therefore exist despite apparently normal imaging findings3.
This distinction carries major clinical implications because children with heterotaxy-associated single-ventricle disease are already medically vulnerable due to cyanosis, repeated hospitalization, staged surgeries, and postoperative instability. Splenic dysfunction therefore acts in parallel with the hemodynamic burden of congenital heart disease, adding a separate layer of immunologic fragility and increasing susceptibility to perioperative and preventable infectious mortality14.
Accordingly, contemporary management approaches increasingly advocate routine immunologic surveillance in heterotaxy patients, including assessment of splenic function, strict vaccination strategies against encapsulated organisms, aggressive fever management, caregiver education, and consideration of antimicrobial prophylaxis when hyposplenism or asplenia is suspected.
3. Intrinsic Immune Dysfunction in Single-Ventricle and Fontan Physiology
Beyond thymic and splenic abnormalities, single-ventricle physiology itself appears intrinsically associated with immune dysregulation. Several studies have demonstrated lymphopenia, altered lymphocyte subsets, and hypogammaglobulinemia even before Fontan completion, suggesting that immune abnormalities begin early within the univentricular pathway rather than representing only late complications of Fontan failure15.
In survivors of the Fontan procedure, chronic lymphopenia is increasingly recognized as common and clinically relevant. T-cell depletion, reduced CD4+ counts, and abnormalities in humoral immunity have been reported even in patients without overt protein-losing enteropathy. These findings support the concept that chronic venous congestion, impaired lymphatic circulation, low cardiac output, and persistent inflammatory stress may independently contribute to immune dysfunction16.
Recent advances in lymphatic imaging and Fontan physiology have further highlighted the central role of lymphatic abnormalities in single-ventricle disease. Complications such as chylothorax, plastic bronchitis, and protein-losing enteropathy are now increasingly understood as manifestations of systemic lymphatic failure rather than isolated organ-specific disorders. Because lymphatic circulation is closely integrated with immune trafficking and immune homeostasis, chronic lymphatic dysfunction may itself contribute to progressive immune injury17.
4. Protein-Losing Enteropathy as an Acquired Immune Dysregulation Syndrome
Among Fontan-related complications, protein-losing enteropathy represents perhaps the most striking example of acquired immune depletion and dysregulation. Traditionally viewed primarily through the lens of hypoalbuminemia and edema, Fontan-associated PLE is increasingly recognized as a systemic lymphatic-immune disorder.18
Under normal physiologic conditions, intestinal lymphatics play an essential role in trafficking lymphocytes, antigen-presenting cells, cytokines, and immunoglobulins between tissues and secondary lymphoid organs. In the Fontan circulation, chronically elevated systemic venous pressure impairs lymphatic drainage and promotes secondary intestinal lymphangiectasia. The resulting enteric loss of protein-rich lymph leads not only to hypoalbuminemia but also to substantial depletion of immune cells and humoral immune components19.
Patients with Fontan-associated PLE frequently demonstrate profound CD4+ lymphopenia, reduced CD8+ counts, disturbance of the CD4/CD8 ratio, hypogammaglobulinemia, and loss of vaccine-derived immunity. Emerging evidence further suggests altered T-cell differentiation, depletion of naïve T-cell populations, expansion of terminally differentiated cells, and broader disruption of immune homeostasis. In some patients, the phenotype resembles acquired combined immunodeficiency20.
Importantly, the immunologic consequences of PLE likely interact synergistically with pre-existing vulnerabilities related to thymectomy and congenital immune abnormalities. Fontan-associated PLE may therefore represent a “second-hit” or even “third hit” immune injury superimposed on an already fragile immune system. The resulting phenotype may extend beyond immune deficiency alone toward broader immune dysregulation characterized by impaired immune tolerance, chronic inflammatory activation, immune exhaustion, and susceptibility to autoimmune phenomena18.
5. Conclusions and Future Directions
Emerging evidence supports a unified model in which immune dysfunction in single-ventricle congenital heart disease is cumulative, multidimensional, and clinically significant rather than incidental. Early thymectomy may impair adaptive immune maturation, heterotaxy-associated splenic dysfunction can compromise innate and humoral defense, and Fontan-related lymphatic failure may lead to chronic depletion of lymphocytes and immunoglobulins. Together, these mechanisms appear to create a persistent state of immune vulnerability characterized by impaired cellular immunity, defective humoral responses, susceptibility to recurrent or severe infections, loss of vaccine protection, and progressive immune dysregulation.
Despite these risks, systematic immunologic surveillance remains insufficiently integrated into routine cardiology follow-up. Recognition of immune dysfunction as a core component of single-ventricle disease has important implications for long-term management and preventive care. Future strategies may require multidisciplinary collaboration involving cardiology, immunology, infectious disease, gastroenterology, and lymphatic specialists, particularly in patients with heterotaxy, Fontan failure, or protein-losing enteropathy. Further research should focus on integrated immune phenotyping across stages of palliation, identification of biomarkers predicting clinically relevant immune dysfunction, and development of standardized immunologic surveillance protocols within congenital heart disease programs.
List of Abbreviations
| Abbreviation | Full Term |
| AA | Antoine AbdelMassih |
| CD | Cluster of Differentiation |
| CHD | Congenital Heart Disease |
| ICU | Intensive Care Unit |
| IgM | Immunoglobulin M |
| NK | Natural Killer |
| PLE | Protein-Losing Enteropathy |
| TCR | T-Cell Receptor |
| TRECs | T-Cell Receptor Excision Circles |
Authors’ contributions
Conceptualization, AA; Methodology, AA., E.H., M.A., M.E., N.A., N.A., R.A., R.M., S.M.M., S.A., Z.A.; software, AA., E.H., M.A., M.E., N.A., N.A., R.A., R.M., S.M.M., S.A., Z.A; investigation AA., E.H., M.A., M.E., N.A., N.A., R.A., R.M., S.M.M., S.A., Z.A; resources, AA., E.H., M.A., M.E., N.A., N.A., R.A., R.M., S.M.M., S.A., Z.A; writing—original draft preparation, AA., E.H., M.A., M.E., N.A., N.A., R.A., R.M., S.M.M., S.A., Z.A; writing—review and editing, AA., E.H., M.A., M.E., N.A., N.A., R.A., R.M., S.M.M., S.A., Z.A; supervision, AA; project administration, AA; funding acquisition, (non-applicable). All authors have read and agreed to the published version of the manuscript.”.
Funding
None.
Ethics approval and consent to participate
Not applicable.
Written Consent for publication
Not applicable.
Consent to participate
Not applicable.
Availability of data and material
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Code availability
Not applicable.
Conflicts of interest/Competing interests
The authors declare that they have no competing interests.
References
- Zheng, W. C.; et al. Long-term outcomes of patients with single ventricle who do not undergo Fontan palliation. Int. J. Cardiol. Congenit. Hear. Dis. 2023, 12, 100457. [Google Scholar] [CrossRef] [PubMed]
- Marrapu, S.; Kumar, R. Intestinal lymphangiectasia: Understanding the bigger picture. World J. Clin. Cases 2024, 12, 3298–3303. [Google Scholar] [CrossRef] [PubMed]
- Piano Mortari, E.; et al. Heterotaxy syndrome with and without spleen: Different infection risk and management. J. Allergy Clin. Immunol. 2017, 139, 1981–1984.e1. [Google Scholar] [CrossRef] [PubMed]
- Bremer, S. J.; et al. Thymic Atrophy and Immune Dysregulation in Infants with Complex Congenital Heart Disease. J. Clin. Immunol. 2024, 44, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, N. V.; Palmeira, P.; Jatene, M. B.; de Barros Dorna, M.; Carneiro-Sampaio, M. Early Thymectomy Is Associated With Long-Term Impairment of the Immune System: A Systematic Review. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Halnon, N. J.; et al. Thymic Function and Impaired Maintenance of Peripheral T Cell Populations in Children with Congenital Heart Disease and Surgical Thymectomy. Pediatr. Res. 2005, 57, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Eysteinsdottir, J. H.; et al. Vβ Usage and T Regulatory Cells in Children Following Partial or Total Thymectomy after Open Heart Surgery in Infancy. Scand. J. Immunol. 2009, 69, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Eysteinsdottir, J. H.; et al. The influence of partial or total thymectomy during open heart surgery in infants on the immune function later in life. Clin. Exp. Immunol. 2004, 136, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Kymioni, V. M.; Panagiotou, P.; Tzanoudaki, M.; Spoulou, V. Long-Term Immune Alterations After Thymectomy in Early Childhood: A Case Series. Cureus 2025, 17, e95517. [Google Scholar] [CrossRef] [PubMed]
- Saba, T. G.; et al. A multi-disciplinary, comprehensive approach to management of children with heterotaxy. Orphanet J. Rare Dis. 2022, 17, 351. [Google Scholar] [CrossRef] [PubMed]
- Gudmundsdottir, J.; et al. Early thymectomy leads to premature immunologic ageing: An 18-year follow-up. J. Allergy Clin. Immunol. 2016, 138, 1439–1443.e10. [Google Scholar] [CrossRef] [PubMed]
- Baliu-Piqué, M.; Tesselaar, K.; Borghans, J. A. M. Are homeostatic mechanisms aiding the reconstitution of the T-cell pool during lymphopenia in humans? Front. Immunol. 2022, 13, 1–12. [Google Scholar]
- Tatar, I. G.; Ergun, O.; Altunoglu, H.; Tatar, T. Heterotaxia associated with polysplenia. BMJ Case Rep. 2014. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.-N.; et al. Severe Bacterial Infection in Patients with Heterotaxy Syndrome. J. Pediatr. 2014, 164, 99–104.e1. [Google Scholar] [CrossRef] [PubMed]
- Mattes, M.; Connor, J.; Kelly, S. S.; Schwartz, M. C. Lymphopenia in Patients with Single-ventricle Heart Disease after the Fontan Operation. Congenit. Heart Dis. 2016, 11, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Arulselvam, V.; Agarwal, A.; Al Amer, S. R.; Kalis, N. N. Prevalence of lymphopenia in patients with Fontan circulation without protein losing enteropathy. Prog. Pediatr. Cardiol. 2022, 67, 101559. [Google Scholar] [CrossRef]
- Possner, M.; et al. Lymphopenia and immunoglobulin deficiency in adult patients with a Fontan circulation. Eur. Heart J. 2022, 43. [Google Scholar] [CrossRef]
- Magdo, H. S.; et al. Immune Abnormalities in Fontan Protein-Losing Enteropathy: A Case-Control Study. J. Pediatr. 2015, 167, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.; Hofbeck, M.; Feistel, H.; Buheitel, G.; Singer, H. Circumscribed intestinal protein loss with deficiency in CD4+ lymphocytes after the Fontan procedure. Eur. J. Pediatr. 1999, 158, 847–850. [Google Scholar] [CrossRef] [PubMed]
- Hlavackova, E.; Liska, M.; Jicinska, H.; Navratil, J.; Litzman, J. Secondary Combined Immunodeficiency in Pediatric Patients after the Fontan Operation: Three Case Reports. Int. Arch. Allergy Immunol. 2016, 170, 251–256. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



