Submitted:
21 May 2026
Posted:
22 May 2026
You are already at the latest version
Abstract
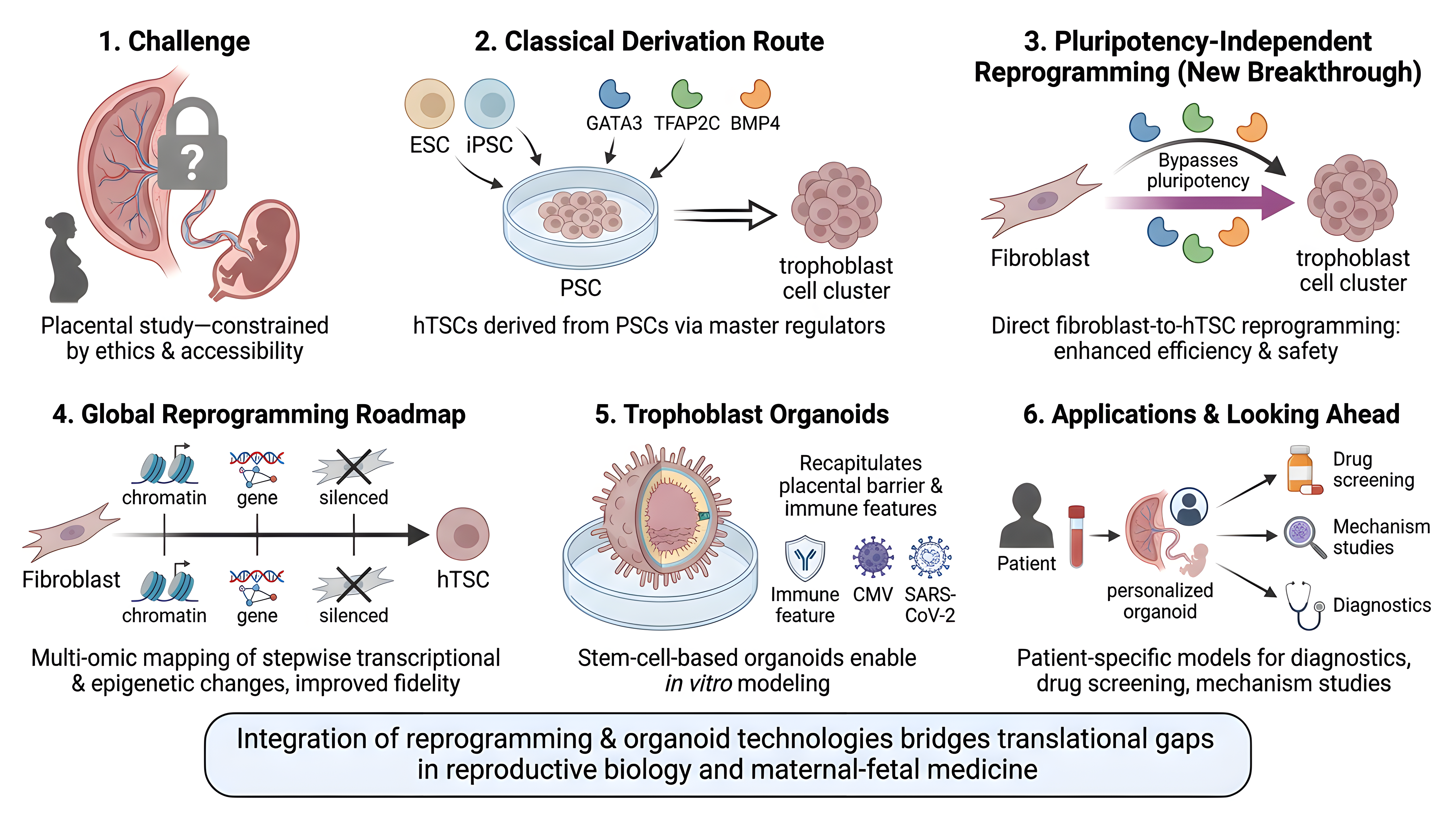
The human placenta, a transient but vital organ, governs fetal development and maternal-fetal interactions, yet its study has been stymied by ethical and accessibility constraints. Stem cell biology has now revolutionized the capacity to model human placental development, in particular with the derivation of human trophoblast stem cells (hTSCs) and organoids. Classically, hTSCs have been derived from pluripotent stem cells (PSCs) such as ESCs or iPSCs, which, under defined culture signals, can be directed into trophoblast lineages by manipulation of master regulatory pathways including GATA3, TFAP2C, and BMP4. However, a quantum leap has come with pluripotency-independent reprogramming, where somatic cells (e.g., fibroblasts) are reprogrammed directly into hTSCs. By bypassing the pluripotent stage with these specific transcription factors and trophoblast-supporting conditions, this approach enhances the efficiency, safety, and disease modeling potential of hTSC derivation. An important advance underlying these improvements is the mapping of a global reprogramming roadmap. Multi-omic and lineage-tracing experiments have mapped the stepwise transcriptional and epigenetic conversions of fibroblasts to hTSCs, including sequential chromatin reconfiguration, trophoblast gene network activation, and repression of somatic signatures. These results identify major regulatory bottlenecks and intermediate states, improving reprogramming fidelity. The derivation of stem-cell-based trophoblast organoids now enables complex modeling of placental architecture, function, and disease susceptibility in vitro. These organoids accurately recapitulate placental barrier functions and immunological features, allowing for examinations of maternal-fetal health, pregnancy disorders, and placental infection response to viruses like cytomegalovirus and SARS-CoV-2. Looking ahead, the integration of reprogramming and organoid technologies will propel patient-specific and tailor-made models for personalized diagnostics, drug screening, and mechanism studies. As we unravel the molecular ballet of trophoblast induction, such discoveries have the potential to bridge basic translational gaps in reproductive biology and maternal-fetal medicine.
Keywords:
human trophoblast stem cells (hTSCs)
; induced trophoblast stem cells (iTSCs)
; pluripotency-independent reprogramming
; human pluripotent stem cells (hPSCs)
; trophoblast lineage specification
; trophoblast organoids
; placenta-on-a-chip/organ-on-chip models
; syncytiotrophoblast and extravillous trophoblast
; BMP4–GATA3–TFAP2C signaling axis
; maternal–fetal interface and pregnancy disorders
1. Introduction
The first lineage bifurcation in mammalian preimplantation development separates trophectoderm (TE) from inner cell mass (ICM), determining whether cells contribute to extraembryonic support tissues or the embryo proper [1]. This decision has far-reaching implications for reproductive biology, placental health, and pregnancy-related complications such as miscarriage, preeclampsia, and intrauterine growth restriction [2]. Single-cell transcriptomics and epigenomics analyses indicate that trophoblast cell fate is controlled by continuous chromatin reconfiguration and a stepwise activation of the TE transcriptional regulators (GATA2, GATA3, TFAP2A, TFAP2C). In particular, this is coupled with silencing of pluripotency genes, supporting the idea that loss of pluripotency is a prerequisite to TE specification [3].
Human pluripotent stem cells (hPSCs), whether embryonic or induced, have really changed how researchers study developmental mechanisms in the lab. They sidestep a lot of the old limitations in embryology [4]. What’s fascinating is that the pluripotent state itself carries built-in cues about extraembryonic cell fate potential [5]. Differentiation methods have moved well beyond flat 2D cultures; now, scientists use 3D organoids and organ-on-chip systems. Researchers have also managed to generate self-renewing human trophoblast stem cells (hTSCs) from blastocysts, early placenta, and hPSCs. This lets them dive deep into how these cells renew themselves and later become syncytiotrophoblast or extravillous trophoblast [2,4] .
Naive hPSCs have a clear edge over primed cells when it comes to trophoblast competence. This tells us the naive state holds on to epigenetic and transcriptional traits that match extraembryonic lineage programs. It shines a light on how cell plasticity narrows as development moves from pre- to post-implantation [6]. Multi-omic studies back this up: hTSCs from naive hPSCs resemble closely trophoblast cells directly isolated from the blastocyst, even showing post-implantation TE features. Epigenetic regulation stands at the center of this process. Primate-specific microRNA clusters like C19MC are essential for strong trophoblast differentiation, underscoring how crucial epigenetic reprogramming is for lineage commitment. This insight paves the way for engineering hPSCs with specific trophoblast potential—a notable breakthrough for both developmental research and regenerative medicine [7].
2. Methodological Advances in Trophoblast Derivation from Pluripotent Stem Cells
It is now possible to derive human trophoblast stem cells (hTSCs) from human pluripotent stem cells (hPSCs) via state- and context-specific methodologies that elucidate essential characteristics of trophoblast commitment. Naive hPSCs transition directly to hTSCs by specific signaling regulation, without intermediary states [8]. In contrast, primed hPSCs necessitate BMP4 in conjunction with FGF and ACTIVIN suppression to establish trophoblast identity [9]. A two-step protocol—initial exposure to BMP4 followed by maintenance in trophoblast stem cell medium—effectively produces authentic self-renewing TSCs from both naive and primed states, with epigenetic modulation (including H3K27 methyltransferase loss) further increasing derivation efficiency from primed cells [10]. The mechanistic disparities among pluripotent states are pronounced: TGF inhibition in naive hPSCs fosters trophectoderm formation, whereas in primed cells, it skews towards neuroectoderm, highlighting unique lineage wiring [11].
Primate-specific C19MC miRNAs are responsible for the increased trophoblast potential of naive hPSCs; this cluster is epigenetically silenced during the shift to primed pluripotency and can be reactivated to restore trophoblast competence [7]. Simultaneous improvements in culture microenvironments boost efficiency and fidelity even more. For example, micromesh bioscaffold systems move hiPSCs through cystic intermediates to proliferative hTSCs while keeping trophoblast programs and the ability to differentiate into syncytiotrophoblast and extravillous trophoblast [12]. 3D organoid and placenta on chip platforms, on the other hand, better mimic the structure and function of living organisms [13]. A short BMP4 treatment in TSC maintenance settings can also change primed hPSCs into trophoblast stem-like cells that look, express genes, and have long-term self-renewal that is similar to real hTSCs [14].
The TEtra network (GATA2, GATA3, TFAP2A, TFAP2C) concurrently activates trophoblast programs and represses pluripotency by binding to both placental gene and OCT4 regulatory areas [3]. Chromatin profiling reveals synchronized alterations in H3K4me3 and H3K27me3 throughout the transition from hPSC to hTSC, with the deletion of EZH1/2 significantly enhancing hTSC derivation [10]. YAP/TAZ, part of the Hippo pathway, control the balance between hTSC self-renewal and giant cell differentiation by interacting with CDX2. This connects mechano-signaling to decisions about trophoblast fate [15]. BMP4 acts as the major signal that starts trophoblast specification. Downstream pathways that depend on SMAD2/3 and are controlled by epigenetics help to solidify and keep trophoblast identity [16].
3. Comparison of Trophoblast Derivation Methods
| Derivation Method | Source Cell Type | Key Signaling Components | Culture Duration | Resulting Cell State |
| Direct differentiation | Naive hPSCs | Moderate BMP4 ± minimal inhibitors | 5-7 days | Self-renewing hTSCs with blastocyst-like features |
| BMP4-based protocol | Primed hPSCs | BMP4 + A83-01 + PD173074 (BAP) | 8 days | Mixed trophoblast population resembling first-trimester syncytiotrophoblast |
| Two-step BMP4 + TSCM | Primed hPSCs | BMP4 (step 1) + TSCM (step 2) | 3-5 days (step 1) + continuous | Bona fide self-renewing hTSCs with enhanced efficiency |
| Micromesh bioscaffold | hiPSCs | Culture-dependent signaling | 10-14 days | Proliferative hTSCs from cystic intermediates with full differentiation potential |
| 3D organoid/placenta-on-chip | hiPSC-derived trophoblasts | Perfusion + matrix interactions | 7-21 days | Polarized, invasive syncytial structures with physiological functionality |
| TSCM short-term treatment | Primed hPSCs | BMP4 in TSCM | 3-5 days | Trophoblast stem-like cells (TSLCs) equivalent to bona fide hTSCs |
| PRC2-inhibited protocol | Naive hPSCs | Inhibition of H3K27me3 deposition | Variable | Enhanced trophectoderm commitment with restricted mesoderm potential |
Figure 1.
Methodological and molecular complexities in the generation of trophoblast stem cells(hTSCs) from pluripotent stem cells.
Figure 1.
Methodological and molecular complexities in the generation of trophoblast stem cells(hTSCs) from pluripotent stem cells.

Direct Reprogramming to Induced Trophoblast Stem Cells
A transformative development has been the establishment of direct reprogramming approaches that bypass pluripotency entirely. Benchetrit and colleagues demonstrated that transient expression of three transcription factors—GATA3, EOMES, and TFAP2C—in mouse fibroblasts induces stable induced trophoblast stem-like cells (iTSCs) with transcriptional, epigenetic, and functional properties closely matching blastocyst-derived TSCs [17]. Importantly, these iTSCs exhibited extensive nuclear reprogramming comparable to induced pluripotent stem cells, including genome-wide alterations in DNA methylation and histone modifications, but without evidence of transitioning through a pluripotent intermediate.
In humans, Liu and colleagues mapped the reprogramming trajectories of fibroblasts to both naive and primed pluripotent states using single-cell transcriptomics, revealing an unexpected role for trophectoderm-associated gene expression during the reprogramming process [18]. This transient trophoblast-like subpopulation could be captured and stabilized using hTSC culture conditions, enabling direct derivation of induced trophoblast stem cells from somatic cells. The resulting iTSCs were functionally equivalent to primary hTSCs, demonstrating self-renewal capacity and multilineage differentiation potential. Subsequently, optimized protocols employing the OKSM (OCT4, KLF4, SOX2, c-MYC) reprogramming factors combined with selective culture conditions have enabled efficient generation of patient-specific iTSCs from dermal fibroblasts [19]. This approach offers significant advantages for disease modeling, as cells can be derived from readily accessible adult tissues without requiring embryonic or first-trimester placental material.
Recent work has extended direct reprogramming to term placental tissues, successfully generating iTSCs from umbilical cord cells collected non-invasively at birth. These iTSCs fulfill criteria for bona fide first-trimester trophoblasts, including long-term self-renewal, appropriate differentiation capacity, organoid formation potential, and transcriptomic similarity to primary hTSCs. Notably, this approach may better preserve patient-specific epigenetic marks compared to conventional iPSC-based methods, as cells undergo limited reprogramming without extensive epigenetic erasure associated with naive pluripotency acquisition.
Figure 2.
Direct repropgramming roadmap for Trophoblast stem cell.

4. Epigenetic and Transcriptional Regulation of Trophoblast Lineage Specification
Trophoblast lineage commitment is governed by significant epigenetic remodeling that differentiates self-renewing trophoblast stem cells (hTSCs) from pluripotent precursors. Single-cell atlases from zygote to mid-gestation delineate a fundamental self-renewal network—including MAZ, NFE2L3, TFAP2C, NR2F2, and CTNNB1—validated by siRNA knockdown as critical for hTSC maintenance [20]. The integration of chromatin accessibility, three-dimensional chromatin interactions, and transcriptomics suggests that EPAS1 functions as an upstream regulator of extravillous trophoblast transcription factors, including ASCL2 and SNAI1, hence associating this pathway with variations in birth weight and pregnancy loss [21].
The chromosome 19 microRNA cluster C19MC offers a primate-specific regulatory layer, functioning in naive human embryonic stem cells (ESCs) while being epigenetically suppressed in primed cells through DNA methylation and chromatin remodeling [7]. Reactivating C19MC with targeted genome/epigenome editing reinstates trophoblast competence in otherwise resistant primed hPSCs, illustrating that this cluster operates as a reversible molecular gate to the trophoblast lineage [7].
Histone modifications and DNA methylation reshape chromatin as cells specialize. They silence pluripotency genes and switch on regions that drive placental development. In these early stages, bivalent regions marked by both H3K27me3 and H3K4me3 start to change. Cells lose H3K27me3, and the H3K4me1 pattern shifts, kicking off trophoblast-specific gene programs and blocking other cell fates [22]. TET1 refines this whole process. In human trophoblast stem cells (hTSCs), TET1 sticks to regions that overlap with active histone marks and TFAP2C-bound enhancers. The balance between 5mC and 5hmC draws a clear line between stem and differentiated trophoblast cells, pointing out key regulators for the TSC state [23]. When chromatin accessibility, histone modifications, DNA methylation, and hydroxymethylation work together, the result is an epigenetic landscape that’s both stable and flexible. This dynamic framework maintains trophoblast cell growth and self-renewal, while permitting appropriate differentiation [7,20,21,22,23]
5. Key Epigenetic Modifications in Trophoblast Lineage Specification
H3K4me3, and H3K4me1: Numerous interconnected epigenetic processes regulate the commitment and maintenance of trophoblast lineage. Repressive H3K27me3, deposited by PRC2, silences pluripotency and developmental regulators; the loss of EZH1/2 depletes H3K27me3 and significantly enhances the derivation of hTSCs from primed hPSCs, underscoring this mark as a barrier to trophoblast specification, particularly at bivalent loci transitioning to active or stably repressed states [10]. Active marks H3K4me3 and H3K4me1 redistribute across promoters and enhancers of placental genes and TEtra factors (GATA2, GATA3, TFAP2A, TFAP2C), with H3K27me3–H3K4me1 state transitions, partly mediated by LSD1–PRC2 interactions, orchestrating trophoblast specific expression patterns [3,22].
DNA methylation (5-methylcytosine), 5-hydroxymethylcytosine (5hmC), and C19MC (Chromosome 19 MicroRNA Cluster): DNA methylation and 5-hydroxymethylcytosine (5hmC) further refine lineage potential. The primate-specific C19MC cluster is hypomethylated and active in naive hPSCs but hypermethylated and muted in primed cells; targeted reactivation restores trophoblast competence, suggesting that C19MC functions as a reversible epigenetic gate to the trophoblast lineage [7]. The oxidation of 5mC to 5hmC at trophoblast enhancers and promoters caused by TET1 is linked to active transcription and sets self-renewing hTSCs apart from differentiated progeny. TET1-occupied, TFAP2C-enriched areas represent important regulatory elements [23].
Chromatin Accessibility and H3K9me3 : Concurrently, chromatin accessibility analysis reveals that hTSCs consolidate their trophoblast identity by gaining open chromatin at placental regulators such CDX2 and TEtra factors and closing OCT4, NANOG, and SOX2 [20]. H3K9me3-enriched heterochromatin further represses non-trophoblast programs, hence preserving lineage fidelity. These coordinated histone marks, DNA methylation/hydroxymethylation states, C19MC activity, and accessibility landscapes create a stable but adjustable epigenetic framework that allows trophoblast specification and limits other possibilities.
6. Disease Modeling and Clinical Applications of Reprogrammed Trophoblast Lineage Cells
The use of patient-derived induced pluripotent stem cells (iPSCs) presents a novel opportunity to model pregnancy problems at the trophoblast level. The pathogenesis of preeclampsia is replicated in trophoblasts that lack proper syncytialization and have a reduced ability to respond to hypoxia, suggesting that chromatin and post-transcriptional regulation play a role in this disease [24]. MA et al. (2019) [25] and Zhang et al. (2023) [26] found that adrenomedullin (ADM), a placental peptide with lower levels in at-risk pregnancies during the first trimester, is a critical regulator of trophoblast differentiation and a potential biomarker and treatment for early-onset preeclampsia.
Gestational trophoblastic disease, encompassing NLRP7-mutant moles, has been effectively modeled using patient-derived iPSC trophoblasts, demonstrating that NLRP7 dysfunction leads to premature pluripotency loss and BMP4-dependent differentiation; BMP inhibition rectified these phenotypes, suggesting potential therapeutic approaches [27]. Single-cell RNA sequencing of preeclamptic placentas reveals unique trophoblast subtypes exhibiting dysregulated adhesion, migration, and immune tolerance pathways. Additionally, NOTCH3 signaling is identified as a pivotal regulator of human trophoblast stem cell expansion and differentiation, with its dysregulation associated with placental pathology [28,29].
Derivation of disease-specific human stem cells (hTSCs) from patient induced pluripotent stem cells (iPSCs) offers genetically tractable, temporally controllable, and ethically suitable disease modeling for therapeutic screening [4]. Recent developments in monolayer cultures, 3D organoids, and placenta-on-chip technologies improve structural fidelity and the recreation of the maternal-fetal interface [30]. Reprogramming mature placental cytotrophoblasts into induced trophoblast stem-like cells reinstates developmental plasticity, facilitating the investigation of early gestational events that influence subsequent placental problems like as preeclampsia and preterm birth [31]. Integration with multi-omics and weighted correlation network analyses makes it possible to conduct complete mechanistic dissections and identify therapeutic targets that go beyond single-gene techniques.
Figure 3.
Molecular pathways regulating trophoblast stem cells(hTSCs) lineage specification.

7. Disease Models Created Using Reprogrammed Trophoblast Lineage Cells
| Disease/Condition | Source Material | Key Findings | Therapeutic Insights |
| Preeclampsia (PE) | Patient-derived iPSCs from placental tissue | Defective syncytialization, blunted hypoxic response, dysregulation of cell adhesion and migration modules (CTL9, EOPE1, EOPE2) | Identification of gene modules controlling invasion and oxygen response; potential targets for therapeutic intervention without marked DNA methylation changes; consideration of regulatory mechanisms beyond epigenetic modifications |
| Early-Onset Preeclampsia (EOPE) | iPSCs derived from umbilical cord cells of affected pregnancies | Reduced trophoblast invasive capacity under hyperoxic conditions; dysregulation of oxygen response mechanisms; aberrant weighted correlation network modules | Targeting dysregulated gene networks controlling invasiveness; modulation of oxygen-sensing pathways; potential role of adrenomedullin signaling; candidate therapeutic targets validated through in vitro disease models |
| Gestational Trophoblastic Disease (Hydatidiform Moles) | Patient-derived iPSCs harboring NLRP7 mutations | Precocious pluripotency downregulation, premature differentiation marker activation, excessive syncytiotrophoblast maturation, BMP4-dependent phenotypes | BMP4 pathway inhibition corrects phenotypes; identifies NLRP7 as essential regulator of developmental fate decisions; demonstrates pharmacological rescue potential; validates iPSC models for genetic placental disease |
| Fetal Growth Restriction (FGR) | Patient-derived iPSCs and primary trophoblasts from affected pregnancies | Aberrant trophoblast lineage-specific differentiation patterns, altered vascular remodeling, impaired nutrient transport capacity, dysregulation of invasion markers | Understanding lineage-specific differentiation defects underlying placental insufficiency; identification of candidate therapeutic targets for restoring normal trophoblast function; personalized medicine approaches |
| Placental Insufficiency (General) | Multiple patient-derived iPSC lines with various genetic backgrounds | Cellular and molecular defects in trophoblast commitment, expansion, and differentiation; tissue-specific gene dysregulation; altered chromatin accessibility at trophoblast regulatory regions | Systematic interrogation of genetic perturbations affecting placental development; compound screening for therapeutic targets; functional genomic approaches enabling discovery of novel regulators |
| NOTCH3-Associated Placental Dysfunction | iPSC-derived trophoblast stem cells from affected pregnancies | Impaired progenitor expansion, premature syncytial differentiation, reduced stemness marker expression when NOTCH3 signaling disrupted | NOTCH3 signaling pathway as therapeutic target; restoration of canonical NOTCH3 signaling to promote self-renewal and normal differentiation balance |
By integrating advanced differentiation protocols with iPSC reprogramming technology, these disease models demonstrate the ability to generate physiologically relevant in vitro systems that replicate pregnancy pathology. The development of new biomarkers for early prediction and therapeutic targets for intervention in pregnancy complications that do not yet have preventative or curative treatments beyond delivery can be aided by these systems, which allow for the systematic characterization of disease mechanisms at the cellular and molecular level.
Current Limitations and Future Directions in Trophoblast Lineage Specification
Research into in vitro-derived trophoblasts highlights a complex developmental landscape where identity and plasticity are paramount. Transcriptomic evidence confirms that BMP4-induced trophoblasts from primed hPSCs mirror authentic placental characteristics and villous cells [32], effectively resolving earlier debates regarding their similarity to amniotic tissue. However, recent findings reveal unexpected diversity: pluripotent cells can generate two distinct trophectoderm lineage stem cells. These include a CDX2-negative population similar to primary hTSCs and a CDX2-positive putative trophectoderm stem cell (hTESC), both possessing unique transcriptional profiles and differentiation requirements [33]. This variety suggest that current methodologies only capture a fraction of trophoblast states, impacting our ability to engineer specific subtypes.
While human naive epiblast cells typically lose their extraembryonic lineage potential upon transitioning to primed pluripotency [34], targeted interventions show this can be reversed. Specifically, modulating Sox2 expression allows naive hPSCs to simultaneously differentiate into embryonic germ layers and extraembryonic trophoblasts without compromising other developmental potentials [35]. This demonstrates that the pluripotent state is a dynamic landscape where epigenetic manipulation can fine-tune cell fate.
To advance the field, integrating single-cell multiomics, 3D culture, and computational modeling is essential. These technologies can identify transitional cell states and establish molecular links between signaling and epigenetics [36]. By applying machine learning to multiomic data, researchers can move from descriptive cataloging to the rational engineering of trophoblasts with specified functional properties, ultimately driving clinical translations in reproductive medicine.
8. Stem-Cell-Derived Trophoblast Organoids: Advanced Platforms for Modeling Placental Pathologies and Enabling High-Throughput Therapeutic Screening
Recent advancements in stem cell biology have facilitated the creation of three-dimensional trophoblast organoids derived from pluripotent and trophoblast stem cells, offering physiologically appropriate models for studying placental development and associated pathologies. These organoids mirror essential architectural and cellular characteristics of in vivo tissue, presenting revolutionary prospects for mechanistic exploration and therapeutic advancement [4,37,38].
8.1. Development and Characterization of Trophoblast Stem Cell-Derived Organoids
Human trophoblast stem cells are a key resource for building organoids. Lately, researchers have figured out that tweaking the culture environment and signaling molecules lets them guide these cells to form organoids that really match what happens in the body. These human trophoblast stem cells, whether they come from placental tissue, blastocysts, or reprogrammed iPSCs—can renew themselves and turn into different cell types, which is exactly what’s needed for organoid development [2,39]. Better culture conditions help these cells form organoids with syncytiotrophoblast layers that act as real, functional barriers [37]. On top of that, single-cell transcriptomics has pinpointed NOTCH3 as a major player in controlling how trophoblasts differentiate [28]. Researchers have also mapped out 15 key regulators that help these stem cells keep renewing themselves—like MAZ, NFE2L3, TFAP2C, NR2F2, and CTNNB1 [20]. All of this work sharpens our understanding of the molecular framework behind building better organoids.
8.2. Molecular Regulation and Signaling Pathways
Lately, single-cell studies and transcriptome analysis on trophoblast organoids have uncovered several fascinating regulatory networks behind how trophoblasts develop and function. Take NOTCH3 signaling, for example. It’s key for keeping the human placenta growing and differentiating. You’ll find NOTCH3 mostly in the proliferating cytotrophoblast progenitors. Block this pathway, and you actually get more syncytiotrophoblasts [28]. Then there’s transforming growth factor-beta signaling, which steers how extravillous trophoblasts in organoids mature. This pathway matters for proper invasion of trophoblasts and the right decidualization response [40]. Another player is the transcription factor TAZ, which really shapes extravillous trophoblast development by boosting genes linked to EVT identity, cell movement, and survival [41].
8.3. Organoid Architecture and Barrier Function
A significant breakthrough in the technology of trophoblast organoids has been the generation of physiological polarity that mirrors the natural placenta structure, which has an outer layer of syncytiotrophoblast (STB) [42]. Static culture conditions result in inverted polarity with internalized STBs; however, when grown in suspension and gently agitated, the organoids spontaneously rotate and restore physiological polarity with correct apical-basal orientation. This results in increased secretion of STB-associated hormones, such as human chorionic gonadotropin (hCG) and interferon-α2, and the formation of large syncytia with more than 50 nuclei. Following these developments, column type barrier systems have been generated from trophoblast organoids that show continuous syndecan-1-positive syncytiotrophoblast coverage and maturation similar to primary trophoblasts [37]. These systems allow the quantitative measurement of permeability coefficients and the transfer of small molecules, providing a scalable and physiologically relevant system for the study of placental transport, drug safety, and therapy during pregnancy.
Figure 4.
Trophopblast organoids and its applications.

9. Disease Modeling Applications
Trophoblast organoids are highly useful tools for research into various diseases, particularly those involving placental abnormalities. Research into infections has shown that Zika virus has a detrimental effect on the structure of the organoid and the process of syncytialization. Single-cell data have shown that there is a lack of hTSC stemness and cytotrophoblast proliferation, characteristics also seen in preeclampsia. Human cytomegalovirus infection, although not productive in trophoblasts, has shown effects on the process of differentiation and Wnt signaling, suggesting an indirect effect on placental function. Research into SARS-CoV-2 infection has shown that ORF3a has an effect on the process of maturation of the syncytiotrophoblast and invasiveness, altering autophagy, tight junctions, and vesicle secretion [43,44]. These studies show the utility of organoids in understanding viral-induced teratogenesis and maladaptation of the placenta.
9.1. Preeclampsia and Placental Insufficiency Modeling
Preeclampsia, the most common hypertensive disorder of pregnancy, is associated with defective trophoblast invasion, abnormal spiral artery remodeling, and endothelial dysfunction. Recent breakthroughs in preeclampsia modeling using a combination of stem cells and organoids, coculture, and microphysiological systems have greatly advanced our current understanding of the underlying molecular mechanisms of preeclampsia. Organoids from preeclampsia patients were found to express dysregulated genes associated with inflammation, angiogenesis, and trophoblast differentiation [45]. The use of organoids to test stem cell-derived EVs in preeclampsia modeling has also demonstrated promising therapeutic potential, with placental EVs promoting trophoblast migration through CD147 signaling [46], and umbilical cord-derived MSC exosomes carrying miR 146a 5p alleviating hypoxia-induced apoptosis through inhibition of TRAF6/NF κB signaling [47], underscoring organoids’ translational value in preeclampsia research.
9.2. High-Throughput Therapeutic Screening Applications
With trophoblast organoids and HTS, a new era is now unfolding in drug discovery for obstetrics. The response of these organoids to drugs is similar to their response in real life, unlike the response in old-fashioned 2D cell cultures [37,48,49]. Moreover, with the advent of technologies like automated 3D imaging, machine learning-based morphometrics, microfluidic gradient systems, and bio-printing, the entire procedure is now faster and more precise [50,51,52]. The data analysis pipeline is now even better, with newer technologies that can detect hits more accurately and account for variations in organoids and even patients [53,54].
9.3. Comparative Snapshot: Organoids and Other Models
Animal models have been heavily utilized in the field of reproductive toxicology but suffer from the lack of a species specific and ethically sourced model. While primary human trophoblasts have more physiological relevance, they are severely limited by their availability, short longevity, and high variability [55]. There are new placenta-on-chip devices that integrate organoid-derived cells and microfluidics that mimic physiological flow and real-time monitoring capabilities [56,57]. That said, for HTS purposes, organoid trophoblasts are more easily scalable and analytically adaptable, and their potential future use in organ-on-chip devices is a promising synergistic solution [58,59].
9.4. Technical Challenges and Future Directions
Key challenges in trophoblast organoid work are the efficiency of generation varies, an incomplete representation of the subtypes of trophoblast and limited incorporation of immune-vascular into the design [38]. The addition of maternal immune and endothelial cells may improve physiological relevance [60]. Standardized culture protocols, quality criteria and heterogeneous bio-banks are mandatory for reproducibility and clinical applicability. In combination with HTS, AI, bioprinting and microfluidics or other support technologies, these stem-cell-derived trophoblast organoids will be essential as the main tools for precision obstetrics research into 2026 and further.
10. Benchmarking Placental Organoids: A Comprehensive Validation Landscape
Placental organoids resemble first-trimester villous architecture, trophoblast lineages, methylome profiles as well as secretion of placental hormones and therefore represent physiologically relevant in vitro models [61]. They resemble in vivo trophoblast differentiation trajectories accurately when benchmarked on single cells but they contain a very extensive progenitor-like compartment compared to their in vivo tissue counterpart [62]. Spatial and single-nucleus multiomics also reconcile organoid lineages to in situ trophoblast populations, and crucially resolve multinucleated syncytiotrophoblast, focusing interrogation of how faithfully organoids recapitulate the exchange surface and niche-specific signaling environments [63,64] .
10.1. Single-Cell and Single-Nucleus Transcriptomics as the Gold Standard for Organoid Validation
Single-cell–resolution transcriptomics has become the central standard for validating trophoblast organoid fidelity. Shannon et al. systematically compared primary trophoblast-derived organoids (TBP-Org) and stem cell-derived organoids (TBS-Org) against first-trimester trophoblast, showing that both models reconstruct trophoblast differentiation trajectories, but TBP-Orgs more closely mirror in vivo global expression and cell-state heterogeneity [62]. They also found a larger progenitor-like population that is transcriptionally between villous CTB and EVT. This population is rare in vivo, which shows that the culture caused a change in the composition.
snRNA-seq has demonstrated its necessity for the precise characterization of syncytiotrophoblast (STB). Keenen et al. showed that conventional scRNA-seq recovers only 2.4–6% of STB in organoids, whereas snRNA-seq detects 38–76% of STB nuclei, closely matching stereological STB:CTB ratios (9:1 in tissue, 8:1 by snRNA-seq) [64]. Joint single-cell and single-nucleus profiling of placenta and organoids defined three conserved STB nuclear subtypes—juvenile (CTB/STB hybrid), oxygen-sensing (FLT1/hypoxia-enriched), and transport/GTPase signaling—demonstrating that organoids recapitulate syncytial nuclear heterogeneity.
Wang et al. advanced this standard by combining snRNA-seq with snATAC-seq in first-trimester and term placentas, as well as hTSC-derived organoids, delineating dynamic STB nuclear trajectories and identifying regulators such as CEBPB, TFAP2A, and TFAP2C, which were functionally validated in organoid-derived STB [58]. Karvas et al. showed that naïve hPSC-derived stem cell trophoblast organoids (SC-TOs) form five trophoblast clusters (CTB-1/2, STB-1/2, primitive EVT) in proportions and transcriptional states highly similar to primary organoids, with few differentially expressed genes, indicating that organoid culture represents a strong attractor state for trophoblast identity [65].
10.2. Epigenetic Profiling Reveals Chromatin-Level Fidelity and Culture-Dependent Modifications
Epigenetic benchmarking is now central to validating placental organoids, showing that they largely recapitulate primary placental methylation while revealing culture-specific features. Turco et al. created trophoblast organoids that clustered closely with first-trimester placentas on 850K methylation arrays. The correlations were strong, and the principal components were mostly made up of trophoblast markers like CGB3, GATA3, and PSG6, which clearly separated trophoblast samples from non-trophoblast samples [61]. Hemberger and Dean emphasized that accurate models must reflect trophoblast-specific methylation reprogramming, differentiating from embryonic lineages. They observed that stem cell-derived trophoblasts can sustain proper imprinted gene expression despite certain methylation divergence, suggesting compensatory regulation [66].
Functional epigenetic studies utilize organoids to elucidate chromatin regulators. Sadowski et al. utilized CUT&RUN to demonstrate that BCOR (PRC1.1) directly represses the stemness genes CDX2 and HAND1 during syncytiotrophoblast differentiation; the loss of BCOR had negligible effects in 2D but resulted in significant defects in 3D organoids, highlighting the significance of spatial context [67]. Tsolova et al. showed that the age-related increases of H3K27ac/H3K4me3 at FOXC1 seen in vivo are still present in endometrial organoids, which develop epithelial hyperplasia as the mother ages. This shows that the donor’s epigenetic memory is still there and that these organoids are good for studying age-related problems [68].
10.3. Proteomic Validation Demonstrates Functional Secretome Fidelity with Matrix-Dependent Variations
Proteomic benchmarking, while not as comprehensive as transcriptomics, has been essential for confirming the functional outputs of placental and endometrial organoids. Turco et al. used mass spectrometry on trophoblast organoid conditioned medium to find PSG1–9, GDF15, and hCGβ subunits. These were very similar to first-trimester villous secretomes, which showed that the proteins were made and released correctly [61].
Integrated miRNA-seq and secretome profiling of hormone-sensitive endometrial organoids revealed that sex steroids, through miR-3194-5p, regulate the basolateral secretion of AQP1, AQP9, and S100A9, increasing trophoblast migration and invasion by 50–80% in transwell assays [6]. Zhou et al. characterised apical intra-organoid fluid from fertile and infertile endometrial organoids, identifying 150 proteins (>1.5-fold dysregulated) whose altered secretion significantly compromised trophoblast spheroid adhesion (p<0.0001), illustrating patient-specific dysfunctional proteomes with functional ramifications [69]. Matrix context further influences proteomes: a comparative analysis of trophoblast organoids in PEG versus Matrigel demonstrated syncytiotrophoblast-dominant and EVT-dominant phenotypes, respectively, highlighting the necessity to interpret proteomic benchmarks within the framework of culture conditions [70].
10.4. Morphological and Architectural Validation Confirms Villous-like Organization with Quantifiable Fidelity
Structural benchmarking demonstrates that trophoblast organoids autonomously organise into villous-like architectures characterised by suitable layering and differentiation. First-trimester trophoblast organoids develop a proliferative villous cytotrophoblast shell, which is overlaid by syncytiotrophoblast. They remain genetically stable and preserve their structure for over a year with regular passaging, closely resembling placental villi [71]. Haider et al. demonstrated that CTB-derived organoids autonomously produce STB and can be directed towards NOTCH1⁺ HLA-G⁺ EVT, maintaining the bipotential differentiation ability of primary cytotrophoblasts [72].
Next-generation hiPSC-derived placenta-like organoids integrate endothelial and stromal cells with CTB, STB, and EVT, achieving 90–99% trophoblast purity in sorted fractions and secreting hCG-β and VEGFA, while exhibiting appropriate responses to TNF-α and VEGFR inhibition, thus enhancing physiological relevance [73]. Sun et al. elucidated that side-population trophoblast stem cells, as opposed to differentiated cytotrophoblasts, are essential for organoid formation; the resultant SpTSC organoids mimic villous architecture yet exhibit slower growth compared to Okae TSC–derived organoids [74].
10.5. Functional Validation Across Hormonal Secretion, Invasion, and Drug Transport
Endocrine, invasive, immune, and transport assays provide a comprehensive validation of placental organoids’ functionality. Trophoblast organoids produce physiologically relevant levels of hCG, progesterone, estrogens, PlGF, and placental lactogen, as measured by ELISA and mass spectrometry. Culture conditions regulate gestational phenotype, with STBout organoids inducing late-pregnancy hormones CSH1, CSHL1, GH2, and STBin inducing early-pregnancy hormones, as measured by Keenen et al. [64]. The functionality of extravillous trophoblasts is validated through differentiation of HLA-G+ EVT, which invade 3D matrices, as shown by Turco et al. [61]. scRNA-seq and trajectory analyses reveal a strong resemblance to in vivo EVT, with ligand-receptor predictions indicating appropriate interactions with dNK cells, as shown by Zhuang et al. [75]. The study of uNK-organoid co-culture shows that the cytokines made by uNK cells help control the later stages of EVT differentiation, including the processes related to blood flow and nutrient transport, as shown by Li et al. [76]. The barrier function of placenta organoids is validated through active drug transport, where trophoblast organoids show efflux activity for P-gp, BCRP, MRP1, and MRP2, with expression and localization similar to those of villous tissue, and commonly used antihypertensives and antipsychotics show transporter-specific inhibition patterns, as shown by Huang et al. [77].
10.6. Disease Modeling Demonstrates Clinical Relevance Through Preeclampsia and Infection Studies
Hypoxia-induced preeclampsia organoid cultures have also been developed, which recapitulated elevated sFLT-1/PlGF ratios, oxidative stress, and inhibition of the PI3K-AKT-mTOR pathway, while aspirin normalized sFLT-1/PlGF, restored PI3K-AKT-mTOR pathway activity, and corrected mitochondrial function [78]. In rat studies, aspirin also upregulated CYP19A1, while inhibiting CYP1A1, validating the hormonal mechanisms of aspirin in preeclampsia. In addition, high-throughput screening of flame retardant EHDPP using trophoblast organoids identified disruption of normal villous structure, inhibition of IGF1R-dependent respiration, and impairment of invasion, while exposure to EHDPP in pregnant mice caused placental abnormalities, fetal growth restriction, failure of implantation, and stillbirth, validating translational toxicity prediction [79]. In addition, infectious disease modeling using human trophoblast stem cell-derived organoids showed high permissiveness to ZIKV infection, which was mediated by AXL/TIM-1 expression, while also demonstrating limited interferon responses, while infection caused disruption of tissue structure, syncytialization, and stemness [80]. Similarly, stem cell-derived trophoblast organoids have also demonstrated biologically relevant susceptibility to SARS-CoV-2 infection, validating these systems as useful models of viral pathogenesis [65].
These organoid placental cultures are increasingly being accompanied by transparent discussions of their limitations. Single-cell benchmarking has identified an expanded population of progenitor-like cells, intermediate in transcription between cytotrophoblast (CTB) and extravillous trophoblast (EVT), which are rare in primary tissue and likely reflect compositionally biased differentiation in culture [62]. Term-derived organoids often display transcriptional profiles associated with the first trimester and co-expression of both early (hCG) and late (chorionic somatomammotropin, CSH) hormones, suggesting organoids have converged on a default gestational state [64].
11. Systematic Identification of Limitations and Divergence from In Vivo Biology
Culture-specific artifacts are consistently observed, including enrichment in ribosome biogenesis, oxidative phosphorylation, and endoplasmic reticulum stress pathways, while extracellular matrix programs are underrepresented, consistent with the lack of a whole stromal niche environment. The process is further complicated by capture biases: standard scRNA-seq protocols underrepresent large extravillous trophoblasts and multinucleated syncytiotrophoblasts, whereas snRNA-seq protocols sacrifice cytoplasmic RNA and certain proliferative cell types. Integrated single-cell and single-nucleus RNA-sequencing protocols are currently the preferred choice for organoid RNA-sequencing analysis. The ratio of syncytiotrophoblast:cytotrophoblast in organoids is still closer to 1:1 compared with the ~9:1 predominance of syncytiotrophoblast observed in term placentas, even when using STBout or STBin culture conditions to manipulate polarity and differentiation.
The gestational stage: organoid stage matching is another challenge in the field: most protocols produce organoids with an early gestation-like phenotype regardless of gestational age at the time of sample collection, and ‘term’ organoids are smaller and have distinct transcriptional profiles, indicating intrinsic barriers to fully recapitulating late-gestation placental structure and function in vitro.
12. Multi-Omic Integration and Cross-Species Validation Strengthen Conclusions
This can be achieved by using multi-omic approaches that incorporate snRNA-seq and snATAC-seq data to identify key transcription factors and then validate them using CRISPR perturbation studies on organoids, thus providing a closed loop of validation [58] Cross-species studies can provide further mechanistic insights into gene regulation and function, as BCOR targeting and loss-of-function phenotypes are shared between mouse placenta and human trophoblast stem cells64, and murine trophoblast organoids have been shown to replicate in vivo knockout phenotypes for genes such as Nubpl and Gcm1 [81]. Patient-derived induced trophoblast stem cells from term cord tissue, which have been shown to share the transcriptomic identity with first-trimester trophoblast and have the ability to form multilineage organoids, have the potential for providing personalized disease models [82].
13. Future Directions Emphasize Vascular Integration and Immune Complexity
The next generation of placental organoids will need to overcome several obvious shortcomings. For instance, while endothelial and vascular-like cell incorporation has been achieved, most placenta organoids lack a vascular network, and achieving this will likely require organoid integration with microfluidic placenta-on-chip systems [73]. Immune modeling in placenta organoids is incomplete, with co-culture with decidual NK cells having been achieved, while comprehensive immune modeling with macrophages, Tregs, and dendritic cells, with spatial interface atlases, remains to be achieved [63,75,76]. Another area that needs to be overcome is standardization, with considerable variability in conditions used to establish, passage, and differentiate placenta organoids, even with detailed protocols available, hindering reproducibility [71]. Fidelity scoring, illustrated by single-pipeline comparisons of placenta organoid platforms, will need to be achieved, with links to multi-omic, machine learning-derived composite indices to objectively benchmark and select placenta organoids [62].
14. Research Gaps in Trophoblast Lineage Specification and Organoid Biology
There are many aspects of trophoblast reprogramming and organoid systems that are not yet fully understood. The relationship between chromatin remodeling and transcription factor binding has not been clearly established. Live cell imaging has not clarified whether epigenetic modifications such as H3K27me3, H3K4me1/3, and 5mC/5hmC occur prior to or after transcription factor binding. The miRNA cluster C19MC, which is specific to primates, is a critical gate in trophoblast reprogramming. However, it is not clear whether this represents a rate-limiting step or merely one of several redundant pathways. Current methods for generating trophoblast organoids capture a limited range of developmental stages and will almost certainly yield a skewed cell population composition. The methods will not recapitulate CDX2 positive/negative stem cell populations, EVTs, STBs, or transitional cell types. From a practical perspective, there are many challenges in establishing trophoblast organoids, including batch effects, a lack of quality control measures, culture artifacts such as expanded progenitors and inverted polarity, and difficulties in achieving reproducibility. Perhaps most importantly, placental organoids lack vasculature, maternal immune cells, and stroma. Thus, it has not been possible to model oxygen gradients, multicompartment immune tolerance, or maternal-fetal communication. Current disease modeling studies are descriptive in nature. Patient-derived organoids display abnormal networks. However, we are not yet able to use these systems for predictive purposes in patient prognosis or in informing therapeutic decisions. Progress in this area is currently limited by ethics and legislation surrounding organoid derivation and culture.
15. The Next Era: Trophoblast Organoids as Platforms for Modeling Placental Senescence: Convergence with Aging Biology, Dark Genome Reactivation, and Tauopathy
The advent of self-organizing trophoblast organoids that recapitulate villous architecture, cytotrophoblast-syncytiotrophoblast flux, and extravillous invasive competence [61,72] offers a transformative platform for studying the premature cellular senescence that drives placental dysfunction and pregnancy failure. Lessons from parallel aging-organoid disciplines provide both conceptual and methodological scaffolding: intestinal crypt organoids demonstrate that aged Lgr5⁺ stem cells exhibit impaired regenerative capacity reversible by mTOR inhibition [3]; choroid plexus and cerebral organoids derived from aged-donor iPSCs faithfully preserve neurodegenerative vulnerability [4]; and liver organoids from aged individuals accumulate somatic mutational burden mirroring clonal hepatocyte aging in vivo [5]. Crucially, iPSC reprogramming platforms have shown that epigenetic age — quantified by DNA methylation clocks — can be deliberately introduced or erased [6], enabling isogenic “aged” versus “rejuvenated” organoid pairs. Applied to trophoblast lineage reprogramming via GATA3/TFAP2C overexpression or BAP-driven naïve conversion [7], analogous strategies could generate trophoblast organoid systems differing primarily in epigenetic age, enabling precise senescence onset mapping.
A particularly compelling convergence emerges from the dark genome. De Cecco and colleagues from the Sedivy laboratory demonstrated that LINE-1 retrotransposons undergo progressive derepression during cellular aging, generating cytosolic reverse-transcribed DNA that activates cGAS-STING innate immune signaling and drives the interferon-rich senescence-associated secretory phenotype (SASP) [8] — a mechanism now being extended to organoid models of neurodegeneration and chronic inflammatory disease [9]. The placenta is one of the most LINE-1-permissive tissues in the human body, where retrotransposon dynamics contribute physiologically to ERV-driven syncytinization [10]; this very permissiveness renders trophoblasts acutely vulnerable to senescence-associated LINE-1 derepression cascades. Trophoblast organoids thus represent an ideal closed system to interrogate whether stress-induced premature senescence — triggered by hypoxia-reoxygenation, oxidative insult, or sFLT1-mediated ER stress — activates the LINE-1/cGAS-STING inflammatory axis [11], and whether retrotransposon suppression via nucleoside reverse transcriptase inhibitors or epigenetic stabilization of H3K9me3 can attenuate placental SASP and restore trophoblast functional integrity.
This dark genome framework acquires additional mechanistic depth when considered alongside an emerging and underappreciated dimension of placental pathology: tauopathy. Hyperphosphorylated tau, canonically associated with neurodegeneration, has emerged as a pathologically relevant mediator in non-neural tissues under proteotoxic and oxidative stress. Critically, Jash et al. demonstrated the presence of cis-phosphorylated tau (cis p-Tau) the toxic, non-fibrillary conformer that evades PP2A-mediated dephosphorylation — in preeclamptic placentas, establishing tauopathy as a bona fide feature of placental pathology rather than a neurological epiphenomenon [12]. This conformational tau species promotes mitochondrial dysfunction, impairs proteostatic networks including the ubiquitin-proteasome and autophagy-lysosomal axes, and accelerates SASP activation in stressed trophoblasts — a convergence point with both replicative senescence and LINE-1-driven innate immune signaling. Trophoblast organoids engineered to overexpress cis p-Tau, or exposed to preeclampsia-relevant stressors, can now model how tau misfolding disrupts angiogenic signaling, syncytialization fidelity, and invasion competence in three-dimensional tissue context. Critically, integration of cis p-Tau perturbation with LINE-1 reporter systems and spatial proteomics will allow resolution of a key unresolved mechanistic question: whether tau-driven proteotoxicity operates upstream of retrotransposon derepression — by destabilizing heterochromatin through impaired nuclear lamina integrity — or downstream of cGAS-STING activation, as a consequence of chronic innate immune-driven translational stress. The answer has profound therapeutic implications, as it would position either tau conformational correctors, retrotransposon suppressors, or STING antagonists as rational entry points for attenuating premature placental senescence. Together, the convergence of trophoblast organoid technology with aging-organoid methodology, dark genome biology, iPSC epigenetic age engineering, and placental proteinopathy research positions this platform not merely as a model system, but as a discovery engine for mechanistically dissecting — and ultimately intercepting — the senescence cascades that underlie preeclampsia and placental insufficiency.
16. Precision Maternal-Fetal Interface Engineering and AI-Driven Therapeutic Discovery
The discipline is shifting towards dynamic and multi-scale approaches that incorporate mechanisms, phenotypes, and computational predictions. This shift is supported by four fundamental pillars. First, mechanistic precision involves live single-cell chromatin imaging in conjunction with transcriptomic, proteomic, and phospho-signaling analysis, and CRISPR disruption of C19MC and other key regulators to establish causal relationships and rationally optimize reprogramming efficiency. Second, physiological integrated organoids that include perfused vasculature, decidual stroma, and spatially arranged maternal immune cells, according to spatial placental atlases, aim to recapitulate immune tolerance, oxygen sensing, and pathology. Third, standardization and scalability involve consensus protocols, artificial intelligence-based automated culture, machine learning-based quality control indices, and multi-site benchmarking to develop large and clinically annotated biobanks. Fourth, precision predictive medicine seeks to develop predictions of individual pregnancy outcomes and guide personalized prevention and therapy in obstetrics using organoid-derived multi-omic signatures and clinical data in advanced artificial intelligence models.
Author Contributions
Writing—original draft preparation, S.J.; writing—review and editing, J.S.; visualization, S.J.; supervision, S.J.; funding acquisition, J.S. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by National Institutes of Health (NIH) grants P01 AG051449, R01 AG016694, and R01 AG078925 to JS.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
During the preparation of this review manuscript/study, the author(s) used [Nano Banana 2 - Gemini AI] for the purposes of scientific image generation & photo editing. The authors have reviewed and edited the output and take full responsibility for the content of this publication. We thank the Department of Molecular Biology, Cell Biology and Biochemistry of Brown university and all the affiliated organizations for continued support.
Conflicts of Interest
The authors declare no conflicts of interest.
Disclosures: J.M.S. is a cofounder and SAB chair of Transposon Therapeutics.
Abbreviations
The following abbreviations are used in this manuscript:
hTSCs – human trophoblast stem cells
iTSCs – induced trophoblast stem cells
hPSCs – human pluripotent stem cells
ESCs – embryonic stem cells
iPSCs – induced pluripotent stem cells
TE – trophectoderm
ICM – inner cell mass
STB – syncytiotrophoblast
EVT – extravillous trophoblast
hCG – human chorionic gonadotropin
References
- Y, T. Trophoblast lineage specification in the mammalian preimplantation embryo - PubMed. Reprod. Med. Biol. 2020, 19. [Google Scholar] [CrossRef]
- M, K.; et al. Human placenta and trophoblast development: key molecular mechanisms and model systems - PubMed. Cell. Mol. Life Sci. CMLS 2019, 76. [Google Scholar] [CrossRef]
- C, K.; et al. GATA2/3-TFAP2A/C transcription factor network couples human pluripotent stem cell differentiation to trophectoderm with repression of pluripotency - PubMed. Proceedings of the National Academy of Sciences of the United States of America 2017, 114. [Google Scholar] [CrossRef]
- M, H.; O, T.; T, B.; MM, P. Modeling human trophoblast, the placental epithelium at the maternal fetal interface - PubMed. Reproduction 2020, 160. [Google Scholar] [CrossRef]
- Io, S.; et al. Capturing human trophoblast development with naive pluripotent stem cells in vitro. Cell Stem Cell 2021, 28, 1023–1039 e1013. [Google Scholar] [CrossRef]
- Y, D.; et al. Integrated MicroRNA and Secretome Analysis of Human Endometrial Organoids Reveal the miR-3194-5p/Aquaporin/S100A9 Module in Regulating Trophoblast Functions - PubMed. Mol. Cell. Proteom. MCP 2023, 22. [Google Scholar] [CrossRef]
- N, K.; et al. The microRNA cluster C19MC confers differentiation potential into trophoblast lineages upon human pluripotent stem cells - PubMed. Nat. Commun. 2022, 13. [Google Scholar] [CrossRef]
- C, D.; et al. Derivation of trophoblast stem cells from naïve human pluripotent stem cells - PubMed. eLife 2020, 9. [Google Scholar] [CrossRef]
- RM, K.; et al. Use of a human embryonic stem cell model to discover GABRP, WFDC2, VTCN1 and ACTC1 as markers of early first trimester human trophoblast - PubMed. Mol. Hum. Reprod. 2020, 26. [Google Scholar] [CrossRef]
- Y, W.; et al. Efficient derivation of human trophoblast stem cells from primed pluripotent stem cells - PubMed. Sci. Adv. 2021, 7. [Google Scholar] [CrossRef]
- A, O.; et al. TGFβ signalling is required to maintain pluripotency of human naïve pluripotent stem cells - PubMed. eLife 2021, 10. [Google Scholar] [CrossRef]
- Z, L.; O, K.; H, I. Establishment of human trophoblast stem cells from human induced pluripotent stem cell-derived cystic cells under micromesh culture - PubMed. Stem Cell Res. Ther. 2019, 10. [Google Scholar] [CrossRef]
- A, L.; et al. Development of a human iPSC-derived placental barrier-on-chip model - PubMed. iScience 2023, 26. [Google Scholar] [CrossRef]
- YJ, J.; M, K.; BK, L.; J, K. Induction of human trophoblast stem-like cells from primed pluripotent stem cells - PubMed. Proceedings of the National Academy of Sciences of the United States of America 2022, 119. [Google Scholar] [CrossRef]
- T, B.; R, A. Molecular regulation of trophoblast stem cell self-renewal and giant cell differentiation by the Hippo components YAP and LATS1 - PubMed. Stem Cell Res. Ther. 2022, 13. [Google Scholar] [CrossRef]
- RM, R.; et al. The role of BMP4 signaling in trophoblast emergence from pluripotency - PubMed. Cell. Mol. Life Sci. CMLS 2022, 16 79. [Google Scholar] [CrossRef]
- Tan, J.P.; Liu, X.; Polo, J.M. Establishment of human induced trophoblast stem cells via reprogramming of fibroblasts. Nat. Protoc. 2022, 17, 2739–2759. [Google Scholar] [CrossRef]
- Liu, X.; Ouyang, J.F.; Rossello, F.J.; et al. Reprogramming roadmap reveals route to human induced trophoblast stem cells. Nature 2020, 586, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Benchetrit, H.; Herman, S.; van Wietmarschen, N.; et al. Extensive Nuclear Reprogramming Underlies Lineage Conversion into Functional Trophoblast Stem-like Cells. Cell Stem Cell 2015, 17, 543–556. [Google Scholar] [CrossRef] [PubMed]
- Y, C.; D, S.; C, P.; A, P.; TE, B. An integrated atlas of human placental development delineates essential regulators of trophoblast stem cells - PubMed. Development 2022, 149. [Google Scholar] [CrossRef]
- KM, V.; et al. Extravillous trophoblast cell lineage development is associated with active remodeling of the chromatin landscape - PubMed. Nat. Commun. 2023, 14. [Google Scholar] [CrossRef]
- Y, Y.; et al. H3K27me3-H3K4me1 transition at bivalent promoters instructs lineage specification in development - PubMed. Cell Biosci. 2023, 13. [Google Scholar] [CrossRef]
- CE, S.; et al. TET1 and 5-Hydroxymethylation Preserve the Stem Cell State of Mouse Trophoblast - PubMed. Stem Cell Rep. 2020, 15. [Google Scholar] [CrossRef]
- M, H.; et al. Modeling preeclampsia using human induced pluripotent stem cells - PubMed. Sci. Rep. 2021, 11. [Google Scholar] [CrossRef]
- MA, S.; et al. Early onset preeclampsia in a model for human placental trophoblast - PubMed. Proceedings of the National Academy of Sciences of the United States of America 2019, 116. [Google Scholar] [CrossRef]
- Zhang, Q.; et al. Adrenomedullin has a pivotal role in trophoblast differentiation: A promising nanotechnology-based therapeutic target for early-onset preeclampsia. Sci. Adv. 2023, 9, eadi4777. [Google Scholar] [CrossRef]
- A, A.-G.; et al. NLRP7 plays a functional role in regulating BMP4 signaling during differentiation of patient-derived trophoblasts - PubMed. Cell Death Dis. 2020, 11. [Google Scholar] [CrossRef]
- B, D.; et al. NOTCH3 signalling controls human trophoblast stem cell expansion and differentiation - PubMed. Development 2023, 150. [Google Scholar] [CrossRef]
- W, Z.; et al. Trophoblast Cell Subtypes and Dysfunction in the Placenta of Individuals with Preeclampsia Revealed by Single-Cell RNA Sequencing - PubMed. Mol. Cells 2022, 45. [Google Scholar] [CrossRef]
- X, L.; ZH, L.; YX, W.; TH, L. A comprehensive review of human trophoblast fusion models: recent developments and challenges - PubMed. Cell Death Discov. 2023, 9. [Google Scholar] [CrossRef]
- T, B.; et al. Establishment of human induced trophoblast stem-like cells from term villous cytotrophoblasts - PubMed. Stem Cell Res. 2021, 56. [Google Scholar] [CrossRef]
- AS, S.; et al. The product of BMP-directed differentiation protocols for human primed pluripotent stem cells is placental trophoblast and not amnion - PubMed. Stem Cell Rep. 2022, 17. [Google Scholar] [CrossRef]
- A, M.; et al. Two distinct trophectoderm lineage stem cells from human pluripotent stem cells - PubMed. J. Biol. Chem. 2021, 296. [Google Scholar] [CrossRef]
- G, G.; et al. Human naive epiblast cells possess unrestricted lineage potential - PubMed. Cell Stem Cell 2021, 28. [Google Scholar] [CrossRef]
- KC, T.; et al. Sox2 modulation increases naïve pluripotency plasticity - PubMed. iScience 2021, 24. [Google Scholar] [CrossRef]
- MN, S.; V, P. Early human development and stem cell-based human embryo models - PubMed. Cell Stem Cell 2024, 31. [Google Scholar] [CrossRef]
- T, H.; et al. Trophoblast stem cell-based organoid models of the human placental barrier - PubMed. Nat. Commun. 2024, 15. [Google Scholar] [CrossRef]
- BM, W.; JN, C.; VHJ, R. Trophoblast Organoids: Capturing the Complexity of Early Placental Development In Vitro - PubMed. Organoids 2024, 3. [Google Scholar] [CrossRef]
- TV, N.; IN, L. Stem Cell-Based Trophoblast Models to Unravel the Genetic Causes of Human Miscarriages - PubMed. Cells 2022, 11. [Google Scholar] [CrossRef]
- Haider, S.; et al. Transforming growth factor-β signaling governs the differentiation program of extravillous trophoblasts in the developing human placenta. Proc. Natl. Acad. Sci. 119, 2022–7–6. [CrossRef] [PubMed]
- Meinhardt, G.; et al. The multifaceted roles of the transcriptional coactivator TAZ in extravillous trophoblast development of the human placenta. Proceedings of the National Academy of Sciences of the United States of America 2025, 122. [Google Scholar] [CrossRef]
- L, Y.; P, L.; H, Y.; CB, C. Trophoblast organoids with physiological polarity model placental structure and function - PubMed. J. Cell Sci. 2024, 137. [Google Scholar] [CrossRef]
- D, K.; et al. SARS-CoV-2 ORF3a Protein Impairs Syncytiotrophoblast Maturation, Alters ZO-1 Localization, and Shifts Autophagic Pathways in Trophoblast Cells and 3D Organoids - PubMed. bioRxiv: the preprint server for biology. 2024. [CrossRef]
- Mysorekar, I.; et al. ORF3a is a key driver of maternal SARS-CoV-2 infection-associated placental dysfunction. Res. Sq. 2025. [Google Scholar] [CrossRef]
- J, M.-F.; LC, S. RISING STARS: Approaches to modeling placental function in preeclampsia in vitro and in vivo - PubMed. J. Endocrinol. 2023, 258. [Google Scholar] [CrossRef]
- K, B.; et al. The regulatory role of placental extracellular vesicle on trophoblast and endothelial cell functions - PubMed. Front. Cell Dev. Biol. 2025, 13. [Google Scholar] [CrossRef]
- X, L.; R, L.; J, S.; Y, Y.; L, H. Placental mesenchymal stem cell exosomes drive macrophage M2 polarization via the miR-146a-5p/TRAF6 axis to ameliorate preeclampsia - PubMed. Eur. J. Histochem. EJH 2025, 69. [Google Scholar] [CrossRef]
- D, K.; et al. Patient-Derived Organoids as Therapy Screening Platforms in Cancer Patients - PubMed. Adv. Healthc. Mater. 2024, 13. [Google Scholar] [CrossRef]
- K, Z.; et al. A Microfluidic Chip-Based Automated System for Whole-Course Monitoring the Drug Responses of Organoids - PubMed. Anal. Chem. 2024, 96. [Google Scholar] [CrossRef]
- Zhang, H.; et al. High throughput physiological micro-models for in vitro pre-clinical drug testing: a review of engineering systems approaches. Prog. Biomed. Eng. 2020, 2. [Google Scholar] [CrossRef]
- Bhusal, A.; et al. Microfluidics for High Throughput Screening of Biological Agents and Therapeutics. Biomed. Mater. Devices 2024, 2024 3, 1 3. [Google Scholar] [CrossRef]
- Y, L.; Z, C.; W, L.; H, C.; S, P. High-Throughput Screening of Anti-cancer Drugs Using a Microfluidic Spheroid Culture Device with a Concentration Gradient Generator - PubMed. Curr. Protoc. 2022, 2. [Google Scholar] [CrossRef]
- M, C. H.; et al. Comprehensive and unbiased multiparameter high-throughput screening by compaRe finds effective and subtle drug responses in AML models - PubMed. eLife 2022, 11. [Google Scholar] [CrossRef]
- Rapisarda, A.; Chan, K.; Gilardi, M.; Cairo, S.; Sridharan, B. Abstract 3993: High-throughput screening of clinically relevant patient-derived 3D cultures to inform on the efficacy of antibody drug conjugate payloads in 10 distinct cancer indications. Cancer Res. 2025, 85. [Google Scholar] [CrossRef]
- A, C.; CL, D.; C, H.; F, D. Isolation of Primary Cytotrophoblasts From Human Placenta at Term - PubMed. Bio-protocol 2021, 11. [Google Scholar] [CrossRef]
- R, M.; et al. Organ-on-chip models: Implications in drug discovery and clinical applications - PubMed. J. Cell. Physiol. 2019, 234. [Google Scholar] [CrossRef]
- L, R.; S, K.; R, M.; A, H. Organ-On-Chip Technology: The Future of Feto-Maternal Interface Research? - PubMed. Front. Physiol. 2020, 11. [Google Scholar] [CrossRef]
- M, W.; et al. Single-nucleus multi-omic profiling of human placental syncytiotrophoblasts identifies cellular trajectories during pregnancy - PubMed. Nat. Genet. 2024, 56. [Google Scholar] [CrossRef]
- H, W.; X, N.; F, Z.; H, Z.; D, L. Human organoids-on-chips for biomedical research and applications - PubMed. Theranostics 2024, 14. [Google Scholar] [CrossRef]
- IM, S.; et al. Current strategies using 3D organoids to establish in vitro maternal-embryonic interaction - PubMed. J. Vet. Sci. 2024, 25. [Google Scholar] [CrossRef]
- MY, T.; et al. Trophoblast organoids as a model for maternal-fetal interactions during human placentation - PubMed. Nature 2018, 564. [Google Scholar] [CrossRef]
- MJ, S.; et al. Single-cell assessment of primary and stem cell-derived human trophoblast organoids as placenta-modeling platforms - PubMed. Dev. Cell 2024, 59. [Google Scholar] [CrossRef]
- A, A.; et al. Spatial multiomics map of trophoblast development in early pregnancy - PubMed. Nature 2023, 616. [Google Scholar] [CrossRef]
- MM, K.; et al. Comparative analysis of the syncytiotrophoblast in placenta tissue and trophoblast organoids using snRNA sequencing - PubMed. eLife 2025, 13. [Google Scholar] [CrossRef]
- RM, K.; et al. Stem-cell-derived trophoblast organoids model human placental development and susceptibility to emerging pathogens - PubMed. Cell Stem Cell 2022, 29. [Google Scholar] [CrossRef]
- M, H.; W, D. The placenta: epigenetic insights into trophoblast developmental models of a generation-bridging organ with long-lasting impact on lifelong health - PubMed. Physiol. Rev. 2023, 103. [Google Scholar] [CrossRef]
- D, S.; et al. Polycomb Repressive Complex 1.1 Component, BCOR, Promotes Syncytiotrophoblast Differentiation in Mice and Humans - PubMed. bioRxiv: the preprint server for biology. 2024. [CrossRef]
- AO, T.; et al. Active chromatin marks and up-regulation of FOXC1 in uterine epithelial cells demarcate the onset of reproductive decline in aging females - PubMed. NAR. Mol. Med. 2025, 2. [Google Scholar] [CrossRef]
- W, Z.; et al. Infertile human endometrial organoid apical protein secretions are dysregulated and impair trophoblast progenitor cell adhesion - PubMed. Front. Endocrinol. 2022, 13. [Google Scholar] [CrossRef]
- EM, S.; N, H.; R, S.; P, P.; JD, W. Engineered 3D Hydrogel Matrices to Modulate Trophoblast Stem Cell-Derived Placental Organoid Phenotype - PubMed. bioRxiv: the preprint server for biology. 2024. [CrossRef]
- MA, S.; et al. Establishment and differentiation of long-term trophoblast organoid cultures from the human placenta - PubMed. Nat. Protoc. 2020, 15. [Google Scholar] [CrossRef]
- S, H.; et al. Self-Renewing Trophoblast Organoids Recapitulate the Developmental Program of the Early Human Placenta - PubMed. Stem Cell Rep. 2018, 11. [Google Scholar] [CrossRef]
- K, C.; et al. Engineering placenta-like organoids containing endogenous vascular cells from human-induced pluripotent stem cells - PubMed. Bioeng. Transl. Med. 2022, 8. [Google Scholar] [CrossRef]
- C, S.; LW, C.; JL, J. Organoid generation from trophoblast stem cells highlights distinct roles for cytotrophoblasts and stem cells in organoid formation and expansion - PubMed. Placenta 2025, 166. [Google Scholar] [CrossRef]
- BM, Z.; et al. Single-cell characterization of self-renewing primary trophoblast organoids as modeling of EVT differentiation and interactions with decidual natural killer cells - PubMed. BMC Genom. 2023, 24. [Google Scholar] [CrossRef]
- Q, L.; et al. Human uterine natural killer cells regulate differentiation of extravillous trophoblast early in pregnancy - PubMed. Cell Stem Cell 2024, 31. [Google Scholar] [CrossRef]
- S, H.; et al. Human trophoblast organoids for improved prediction of placental ABC transporter-mediated drug transport - PubMed. Toxicol. Appl. Pharmacol. 2024, 492. [Google Scholar] [CrossRef]
- S, H.; et al. Constructing a Preeclampsia Organoid Model to Elucidate the Mechanism of Aspirin - PubMed. Hypertension (Dallas, Tex. : 1979) 2025, 82. [Google Scholar] [CrossRef]
- C, X.; et al. Screening of Organophosphate Flame Retardants with Placentation-Disrupting Effects in Human Trophoblast Organoid Model and Characterization of Adverse Pregnancy Outcomes in Mice - PubMed. Environ. Health Perspect. 2022, 130. [Google Scholar] [CrossRef]
- H, W.; et al. Zika virus targets human trophoblast stem cells and prevents syncytialization in placental trophoblast organoids - PubMed. Nat. Commun. 2023, 14. [Google Scholar] [CrossRef]
- Q, M.; et al. Murine trophoblast organoids as a model for trophoblast development and CRISPR-Cas9 screening - PubMed. Dev. Cell 2023, 58. [Google Scholar] [CrossRef]
- AJ, v. V.; et al. Generation of Bona Fide Human Induced Trophoblast Stem Cells by Direct Reprogramming of Term Umbilical Cord Cells - PubMed. Int. J. Mol. Sci. 2024, 26. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



