Submitted:
19 May 2026
Posted:
20 May 2026
You are already at the latest version
Abstract
Objectives: Borrelia burgdorferi sensu lato, a spirochete bacterium responsible for Lyme borreliosis - the most common tick-borne infection in North America and Europe - can trigger the production of antiphospholipid antibodies. These antibodies target host lipids such as cardiolipin (CL), phosphatidic acid (PA), phosphatidylcholine (PC), and phosphatidylserine (PS), which the spirochete incorporates into its membrane from the surrounding environment. Although antiphospholipid antibodies are typically associated with antiphospholipid syndrome (APS), they may also arise during infections, including Lyme borreliosis. This study aimed to develop and optimize several enzyme-linked immunosorbent assays (ELISAs) for measuring various antiphospholipid antibodies in patients with Lyme borreliosis. Methods: Thirty patients diagnosed with Lyme borreliosis were enrolled: ten with solitary erythema migrans (EM), ten with multiple EM (MEM), and ten with late manifestations known as acrodermatitis chronica atrophicans (ACA). Forty healthy blood donors served as controls. Four distinct antiphospholipid antibody ELISAs were developed, each using a different phospholipid coating: CL, PA, PC, and PS. Serum of APS patient was used as a positive control and for standard curve generation. Results: All four ELISAs were successfully established and demonstrated good measurement precision. Significant differences in antiphospholipid antibody levels and positivity rates were observed between Lyme borreliosis patients and healthy blood donors. Notably, levels of antibodies directed against PA (aPA), PC (aPC), and PS (aPS), both IgG and IgM, were significantly higher in patients with late Lyme borreliosis, manifested as ACA, compared to healthy blood donors. In contrast, anti-CL (aCL) levels did not differ significantly between groups. Patients with ACA also showed the highest frequency of multiple antiphospholipid antibody positivity, with 7 of 10 patients testing positive for three or more antiphospholipid antibodies. Conclusions: Accurate and precise in-house ELISAs for the detection of aCL, aPA, aPC, and aPS using APS sera as standard material were developed and validated for the analysis of samples of patients with Lyme borreliosis. Our data suggest that antiphospholipid antibody levels—specifically aPA, aPC, and aPS—differ across clinical manifestations of Lyme borreliosis, with the greatest increases observed in patients with ACA.
Keywords:
Lyme borreliosis
; antiphospholipid antibodies
; anti-phosphatidylserine antibodies
; anti-phosphatidic acid antibodies
; anti-phosphatidylcholine antibodies
; Borrelia burgdorferi sensu lato
1. Introduction
Antiphospholipid antibodies are a heterogeneous group of autoantibodies directed against phospholipids or phospholipid-binding proteins, most notably β2 glycoprotein I and cardiolipin. Their persistent presence in serum is associated with an increased risk of thrombosis in various autoimmune diseases and forms the basis of the laboratory criteria for antiphospholipid syndrome (APS) [1,2]. Although antiphospholipid antibodies are now strongly linked to APS, they were originally described in the context of infectious diseases. The first observations came from patients infected with Treponema pallidum, where cardiolipin-based serological tests for syphilis revealed reactivity that was later recognized as antiphospholipid antibodies [3]. Continued use of these assays eventually showed that some patients with autoimmune diseases, particularly systemic lupus erythematosus, exhibited “false positive” results, which led to the discovery of pathogenic antiphospholipid antibodies and the later conceptualization of anticardiolipin syndrome and APS [4,5].
Beyond syphilis, transient antiphospholipid antibody production has been documented in a range of bacterial, viral, and parasitic infections. In these contexts, antiphospholipid antibodies are thought to arise due to infection-induced immune activation, molecular mimicry, and the exposure of phospholipid antigens during inflammation [6,7].
Similar to Treponema pallidum, infection with the causative agents of Lyme borreliosis (Borrelia burgdorferi sensu lato, also referred to as Lyme borreliae) has also been shown to induce the production of antiphospholipid antibodies that recognize host phospholipids. This phenomenon was first systematically demonstrated by Gwynne and co-authors, who proposed their potential utility as infection-associated biomarkers in Lyme borreliosis [8]. Lyme borreliosis is the most common tick-borne disease in the Northern haemisphere and manifests with a wide and evolving range of clinical features [9]. In the absence of antibiotic therapy, disease progression typically follows three stages, beginning with early localized skin infection presenting as erythema migrans (EM), followed by early disseminated disease such as multiple erythema migrans (MEM) or Lyme neuroborreliosis and culminating in late manifestations, of which acrodermatitis chronica atrophicans (ACA) is the most characteristic in Europe.
Diagnosing Lyme borreliosis remains challenging [10]. Clinical symptoms may be non-specific or atypical, especially in disseminated and late disease, where systemic manifestations can mimic other inflammatory or autoimmune conditions. Laboratory diagnosis relies primarily on serological tests detecting anti Borrelia antibodies. However, serology is insensitive during the first weeks of infection, when most patients present with EM. Antibody responses may be delayed, leading to false negative results early in the disease course, and antibodies can persist long after bacterial clearance, limiting their usefulness for assessing disease activity or treatment response. Thus, current serological testing cannot reliably distinguish active from past infection or evaluate antibiotic treatment efficacy, creating a diagnostic gap both in early disease and during follow up.
From a pathophysiological perspective, Borrelia lack complete biosynthetic pathways for several membrane lipids and therefore scavenge host-derived phospholipids and cholesterol, incorporating them into their outer membrane. Because Lyme borrelia is unable to synthesize its own fatty acids, its lipid composition mirrors that of host tissues. Lipid exchange between the bacterium and eukaryotic cell membranes occurs through direct contact or via outer membrane vesicles [11]. Several of these host-derived phospholipids—such as phosphatidylserine (PS), phosphatidylcholine (PC), and phosphatidic acid (PA)—may be recognized by antiphospholipid antibodies that emerge early in infection. Previous studies in a small American cohort demonstrated that antibody responses to host phospholipids, measured using an antiphospholipid antibodies ELISA, may outperform standard diagnostic tests in the context of Lyme borreliosis [8]. The primary objective of this study was therefore to develop an in-house ELISA for the detection of various antiphospholipid antibodies and to evaluate their diagnostic performance in a European cohort of patients with early and late Lyme borreliosis.
2. Materials and Methods
2.1. Participants
Serum samples from 30 patients with Lyme borreliosis, of which 10 were presented with early localized stage - EM, 10 with early disseminated stage – MEM, and 10 with late disseminated stage - ACA, were collected at the Department of Infectious Diseases, University Medical Centre Ljubljana, Slovenia (Table 1). Additionally, blood samples from 40 healthy blood donors (HBD) were collected. The study was performed according to the guidelines of the Declaration of Helsinki and approved by the National Medical Ethics Committee, Ljubljana, Slovenia (0120-571/2024-2711-3).
2.2. Serum Collection
Samples were collected in routine clinical settings. Blood samples were centrifuged at 1,800×g for 10 min within 2 h of collection, and serum was separated directly from the cell pellet. Samples were stored at 4 °C and analyzed the next day or aliquoted into tubes and stored at -80 °C for later analysis.
2.3. In-House ELISAs for the Measurement of Antiphospholipid Antibodies
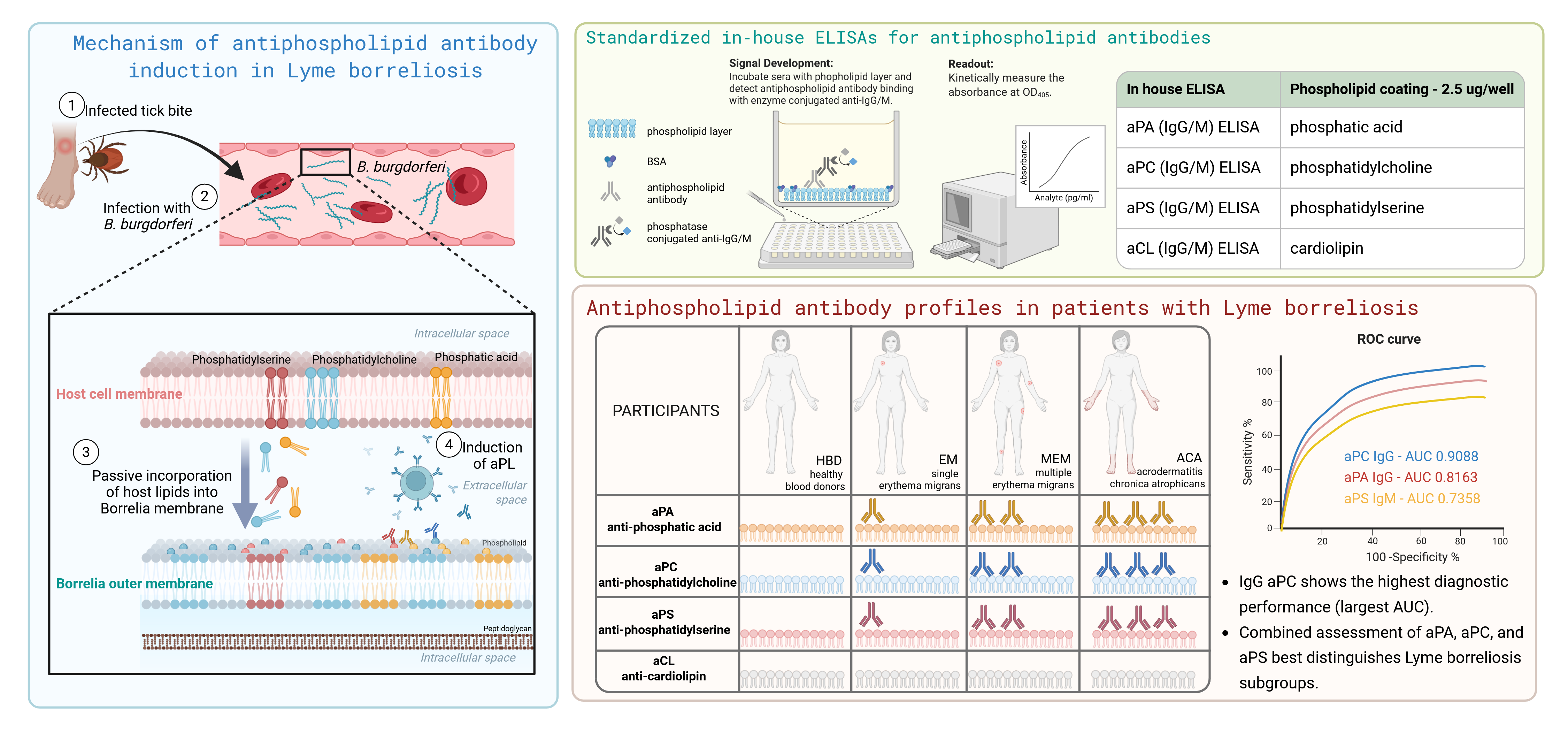
Four anti-phospholipid antibodies, including anti-cardiolipin (aCL), anti-phosphatidic acid (aPA), anti-phosphatidylcholine (aPC), and anti-phosphatidylserine (aPS) of IgG and IgM isotypes, were measured using in-house ELISAs. These assays followed the protocol first described in 1997 [12], subsequently evaluated in several studies [13,14], and adapted according to the method published by Gwynne et al. [8]. Polystyrene microliter plates (Costar medium binding EIA/RIA plates, Cambridge, MA, USA) were coated with 2.5 µg/well of cardiolipin, phosphatidylserine, phosphatidylcholine, or phosphatidic acid in absolute ethanol and dried overnight at 4°C. All subsequent steps were performed at room temperature. Wells were blocked for 2 hours with 1% bovine serum albumin (BSA) in phosphate buffer saline (PBS). After washing three times with PBS, patient sera diluted 1:100 in 1% BSA/PBS were applied in duplicate and incubated for 2.5 h. Plates were then washed four times with PBS containing 0.05% Tween 20, followed by the addition of alkaline phosphatase-conjugated goat anti-human IgG or IgM antibodies (ACSC, Westbury, USA) and a 60-min incubation. After another four washes, 100 mL/well of para-nitrophenyl phosphate (Sigma Chemical Company, St. Louis, MO, USA) dissolved at 1 g/L in 1 M diethanolamine buffer (pH 9.8), was applied. The OD405 was measured kinetically using a spectrometer until optimal alignment with the predicted values of the internal standards (IS) was achieved.
Figure 1.
Characteristics of aCL, aPA, aPC, and aPS ELISA. aCL, anti-cardiolipin antibodies; aPA, anti-phosphatidic acid antibodies; aPC, anti-phosphatidylcholine antibodies; aPS, anti-phosphatidylserine antibodies; BSA, bovine serum albumin; CL, cardiolipin. APS, antiphospholipid syndrome. Created with BioRender.com.
Figure 1.
Characteristics of aCL, aPA, aPC, and aPS ELISA. aCL, anti-cardiolipin antibodies; aPA, anti-phosphatidic acid antibodies; aPC, anti-phosphatidylcholine antibodies; aPS, anti-phosphatidylserine antibodies; BSA, bovine serum albumin; CL, cardiolipin. APS, antiphospholipid syndrome. Created with BioRender.com.

2.4. Verification of the ELISA Tests
Precision (repeatability and intermediate precision) of the ELISAs was evaluated in accordance with the Clinical and Laboratory Standards Institute (CLSI) EP5-A3 recommendations. A positive control sample was tested in duplicate across four separate runs to assess within-run and between-run variability. To find significant outliers among the results, the Grubbs’ test was performed.
2.5. Statistical Analysis
Group comparisons were performed using one-way ANOVA followed by Tukey’s multiple comparison test. Correlation analyses were conducted using Pearson’s correlation test. The diagnostic value of different antiphospholipid antibodies was determined by ROC curve analysis. Data processing and statistical analyses were performed using GraphPad Prism 10.3.1 software (GraphPad Software, San Diego, CA, USA). A p-value of less than 0.05 was considered statistically significant.
3. Results
3.1. Verification of the aCL, aPA, aPC and aPS ELISA Tests
To evaluate the measurement precision of aCL IgG/IgM, aPA IgG/IgM, aPC IgG/IgM, and aPS IgG/IgM ELISAs, within-run and between-run imprecision was assessed by testing a positive sample in duplicate across four independent runs (Suppl. Table S1). Within-run coefficients of variation (%CV) ranged from 2.39% to 8.80% for IgG, and from 4.45% to 7.81% for IgM. Between-run %CV ranged from 7.20% to 17.30% for IgG, and from 4.09% to 17.20% for IgM. All %CVs for both intra-assay and inter-assay precision were within acceptable limits.
3.2. Levels of Antiphospholipid Antibodies
Both IgG and IgM levels of aPA, aPC, and aPS were significantly higher in patients with late disseminated Lyme borreliosis - ACA compared to HBDs. In patients with MEM IgG aPA and aPC, as well as IgM aPS levels, were also significantly elevated compared to HBDs. In contrast, anti-cardiolipin (aCL) antibody levels did not differ significantly between the groups (Figure 2).
3.3. Correlation Between Different Antiphospholipid Antibodies
A positive linear correlation was observed among the IgG isotypes of aPA, aPC, and aPS antibodies. Specifically, the correlation coefficients were r = 0.51 for aPA vs. aPC (p < 0.0001), r = 0.40 for aPA vs. aPS (p = 0.0008), and r = 0.74 for aPC vs. aPS (p < 0.0001) (Figure 3). For the IgM isotypes, aPA IgM showed a significant positive correlation with aPS IgM, whereas no significant correlations were detected between aPA IgM and aPC IgM or between aPC IgM and aPS IgM (Figure 3).
3.4. Positivity of Antiphospholipid Antibodies in Lyme Borreliosis Patients
The threshold for individual antiphospholipid antibody positivity was determined using a non-parametric approach, based on the 99th percentile of values measured in a group of 40 HBDs, as the distribution of antiphospholipid antibody levels was not normal. Individual values, calculated thresholds, and the number of positive HBDs are presented in Table 2. Significant outliers were identified for aPA IgG/IgM and aPC IgM using Grubbs’ test, whereas no outliers were detected for aPS IgG/IgM or aPC IgG. Importantly, none of the healthy blood donors tested positive for more than one antiphospholipid antibody.
Patients with Lyme borreliosis exhibited a significantly higher overall frequency of antiphospholipid antibody positivity compared with healthy blood donors (Table 3). Among the clinical subgroups, the highest prevalence was observed in patients with ACA, where 7 out of 10 individuals tested positive for three or more antiphospholipid antibodies. In the MEM group, 6 out of 10 patients showed positivity for three or more antibodies, whereas in the EM group, this applied to 3 patients.
3.5. ROC Curve Analysis and Diagnostic Applicability of the Tested Antiphospholipid Antibodies
The diagnostic performance of the individual ELISAs for Lyme borreliosis was evaluated using ROC curve analysis (Figure 4). The areas under the curve (AUC) for the different assays ranged from 0.6988 to 0.9088. Among all tested antiphospholipid antibodies, aPC IgG demonstrated the highest diagnostic applicability for distinguishing patients with Lyme borreliosis from healthy controls, based on its AUC value.
4. Discussion
In the present study, we have expanded the currently limited knowledge on antiphospholipid antibodies in Lyme borreliosis, which has so far largely relied on a single primary study by Gwynne et al. and its subsequent commentary [8,15]. Consistent with their findings, we confirmed that infection with Borrelia burgdorferi is associated with the induction of antibodies against phosphatidic acid, phosphatidylcholine, and phosphatidylserine, whereas anti-cardiolipin antibodies do not appear to be significantly elevated. This supports the concept that lipid scavenging by Borrelia contributes to the generation of a distinct antiphospholipid antibody profile. The absence of anti-cardiolipin antibodies represents an important distinction between Lyme borreliosis and syphilis. In syphilis, infection with Treponema pallidum has been shown to induce the release of mitochondrial cardiolipin from host cells, thereby promoting the generation of aCL antibodies [16]. In contrast, Lyme borreliae does not appear to elicit a comparable cardiolipin-directed immune response, indicating differences in host–pathogen interactions and lipid-antigen exposure.
Importantly, our study extends the observations from Gwynne et al. in several key aspects. First, while previous work primarily focused on IgG responses, we systematically analyzed both IgG and IgM isotypes. We demonstrated that IgM antiphospholipid antibodies are also significantly elevated, particularly in patients with more advanced disease (ACA), suggesting that these antibodies may reflect ongoing or recent immune activation. The inclusion of IgM thus provides additional insight into the temporal dynamics of the immune response, which was not addressed in the first study.
Second, unlike the study by Gwynne et al., which included limited or heterogeneous patient cohorts, we analyzed well-defined clinical subgroups of Lyme borreliosis, encompassing early localized (EM), early disseminated (MEM), and late disease (ACA). This allowed us to demonstrate a clear gradient in antiphospholipid antibody levels and positivity rates across disease stages, with the highest levels observed in ACA. Moreover, the presence of multiple antiphospholipid antibodies was markedly more frequent in late disease, supporting the hypothesis that cumulative exposure to Borrelia-derived or host-derived phospholipids enhances the breadth of the antibody response.
Third, an important difference between our study and previous work lies in the studied population. While Gwynne et al. investigated a cohort from the United States, our study was conducted in a European population. This is particularly relevant, as differences in genetic background, environmental exposures, and circulating Borrelia species across geographical regions may influence the immune response and the profile of antiphospholipid antibodies. Therefore, our findings provide important validation and extension of previous observations in a distinct population setting.
Fourth, our study includes a larger and better-characterized cohort compared to the initial report, addressing one of the key limitations highlighted in subsequent commentary, where validation in larger patient populations was explicitly recommended. By increasing the sample size and including a control group of healthy blood donors, we were able to define robust cut-off values using a non-parametric approach and reduce the risk of false-positive interpretations. A further strength of our study lies in the standardization of the in-house ELISA assays. We employed a serum sample from a patient with antiphospholipid syndrome as a reference standard, allowing antibody levels to be expressed in arbitrary units. This approach enabled direct comparison across different ELISA runs and reduced inter-assay variability, thereby improving the reliability and reproducibility of the measurements. Such standardization represents an important methodological advantage over a previous study, where variability between assays may have limited the comparability of subsequent results.
A major strength of our study is the evaluation of the diagnostic performance of individual antiphospholipid antibodies using ROC curve analysis. While previous studies suggested a potential biomarker role for these antibodies, they did not formally assess their diagnostic accuracy. In our cohort, several antibodies demonstrated good discriminatory capacity, with aPC IgG showing the highest AUC. These findings indicate that antiphospholipid antibodies—particularly when assessed as a panel—may have clinically relevant diagnostic value in distinguishing Lyme borreliosis patients from healthy individuals.
In addition, we performed a detailed correlation analysis between different antiphospholipid antibodies. We observed strong correlations among IgG isotypes (especially between aPC and aPS), suggesting a coordinated immune response targeting structurally or functionally related phospholipids. In contrast, IgM responses showed weaker and more selective correlations, which may reflect differences in antigen exposure, affinity maturation, or B-cell activation pathways. These findings provide novel insight into the immunological relationships between different antiphospholipid specificities.
Several limitations should be acknowledged. The sample size, although larger than in the study by Gwynne et al. [8], remains modest, and longitudinal data were not available to assess the persistence of antiphospholipid antibodies following treatment. Previous studies have suggested that these antibodies may decline after antibiotic therapy, indicating their potential role as markers of disease activity. Future studies should therefore include longitudinal sampling and comparisons with other infectious and autoimmune conditions to better define specificity and clinical relevance.
In conclusion, our study validates and significantly extends previous findings on antiphospholipid antibodies in Lyme borreliosis. By including both IgG and IgM isotypes, analyzing distinct clinical subgroups, increasing cohort size, and applying ROC and correlation analyses, we provide a more comprehensive characterization of these antibodies.
5. Conclusions
We developed and standardized in-house ELISA assays for aCL, aPA, aPC, and aPS using APS reference serum, enabling inter-assay comparability. Patients with acrodermatitis chronica atrophicans showed significantly elevated levels of IgG and IgM aPS, aPA, and aPC compared to healthy controls. Testing multiple antiphospholipid antibodies proved to be the most effective approach for distinguishing between subgroups of patients with Lyme borreliosis. ROC analysis demonstrated meaningful diagnostic potential, with IgG aPC showing the highest discriminatory performance. Overall, our findings support the use of aPC, aPA, and aPS as adjunct biomarkers in Lyme borreliosis, particularly when assessed as a panel and interpreted in the clinical context.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: The measurement precision of aCL, aPA, aPC, and aPS (IgG and IgM) ELISAs.
Author Contributions
“Conceptualization P.B. and F.S.; methodology, P.Ž., software, P.Ž.; validation, P.Ž. and K.L.; resources, K.O. and K.L.; data curation, K.O.; writing—original draft preparation, P.Ž.; writing—review and editing, K.L., P.B. and F.S.; visualization, P.Ž.; supervision, F.S.; project administration, K.O. and P.B.; funding acquisition, P.B. All authors have read and agreed to the published version of the manuscript.”
Funding
This research was funded by the Slovenian Research and Innovation Agency (grant no. P3-0296 awarded to F.S., and P3-0314 awarded to K.L.) and by the UMC Ljubljana Tertiary project (No 20250109) awarded to P.B. The funders had no role in the design of the article, collection, analyses, or interpretation of data, writing of the manuscript, or decision to publish the results.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the National Medical Ethics Committee of the Republic of Slovenia (0120-571/2024-2711-3).
Informed Consent Statement
The National Medical Ethics Committee of the Republic of Slovenia granted a waiver of informed consent for this study, which utilized previously collected patient samples.
Data Availability Statement
All relevant clinical data are reported in the article.
Conflicts of Interest
F.S. served on the scientific advisory board for Roche on Lyme disease serological diagnostics and on the scientific advisory board for Pfizer on Lyme disease vaccine, and is an unpaid member of the steering committee of the ESCMID Study Group on Lyme Borreliosis/ESGBOR. Other authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| aPA | Anti-phosphatidic acid antibodies |
| aPC | Anti-phosphatidylcholine antibodies |
| aPS | Anti-phosphatidylserine antibodies |
| HBD | Healthy blood donors |
| AUG | Arbitrary units IgG |
| AUM | Arbitrary units IgM |
| EM | Erythema migrans |
| MEM | Multiple erythema migrans |
| ACA | Acrodermatitis chronica atrophicans |
References
- Miyakis, S. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J.Thromb.Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, K. Antiphospholipid syndrome. Nat. Rev. Dis. Prim. 2018, 4, 18005. [Google Scholar] [CrossRef] [PubMed]
- Pangborn, M.C. A New Serologically Active Phospholipid from Beef Heart. Proc. Soc. Exp. Biol. Med. 1941, 48, 484–486. [Google Scholar] [CrossRef]
- Harris, E.N. Anticardiolipin antibodies: detection by radioimmunoassay and association with thrombosis in systemic lupus erythematosus. Lancet 1983, 2, 1211–4. [Google Scholar] [CrossRef] [PubMed]
- Hughes, G.R. The anticardiolipin syndrome. Clin. Exp. Rheumatol. 1985, 3, 285–6. [Google Scholar] [PubMed]
- Martirosyan, A.; Aminov, R.; Manukyan, G. Environmental Triggers of Autoreactive Responses: Induction of Antiphospholipid Antibody Formation. Front. Immunol. 2019, 10–2019. [Google Scholar] [CrossRef] [PubMed]
- Cervera, R. Antiphospholipid syndrome associated with infections: clinical and microbiological characteristics of 100 patients. Ann. Rheum. Dis. 2004, 63, 1312–7. [Google Scholar] [CrossRef] [PubMed]
- Gwynne, P.J. Antiphospholipid autoantibodies in Lyme disease arise after scavenging of host phospholipids by Borrelia burgdorferi. J. Clin. Invest 2022, 132. [Google Scholar] [CrossRef] [PubMed]
- Steere, A.C. Lyme borreliosis. Nat. Rev. Dis. Prim. 2016, 2, 16090. [Google Scholar] [CrossRef] [PubMed]
- Guérin, M. Lyme borreliosis diagnosis: state of the art of improvements and innovations. BMC Microbiol. 2023, 23, 204. [Google Scholar] [CrossRef] [PubMed]
- Crowley, J.T. Lipid exchange between Borrelia burgdorferi and host cells. PLoS Pathog. 2013, 9, e1003109. [Google Scholar] [CrossRef] [PubMed]
- Bozic, B. Influence of degraded phosphatidylserine on binding of antiphospholipid antibodies. Int. Arch. Allergy Immunol. 1997, 112, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Avcin, T. Estimation of antiphospholipid antibodies in a prospective longitudinal study of children with migraine. Cephalalgia 2004, 24, 831–7. [Google Scholar] [CrossRef] [PubMed]
- Zigon, P. Modified phosphatidylserine-dependent antiprothrombin ELISA enables identification of patients negative for other antiphospholipid antibodies and also detects low avidity antibodies. Clin. Chem. Lab Med. 2011, 49, 1573. [Google Scholar]
- Arora, G.; Hart, T.; Fikrig, E. Use of host lipids by the Lyme disease spirochete may lead to biomarkers. J. Clin. Invest 2022, 132. [Google Scholar] [CrossRef] [PubMed]
- Luo, X. Uncovering the mechanisms of host mitochondrial cardiolipin release in syphilis: Insights from human microvascular endothelial cells. Int. J. Med. Microbiol. 2024, 316, 151627. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Levels of antiphospholipid antibodies in patients with Lyme borreliosis and healthy blood donors. aCL: anti-cardiolipin antibodies; aPA: anti-phosphatidic acid antibodies; aPC: anti-phosphatidylcholine antibodies, aPS: anti-phosphatidylserine antibodies; AUG: arbitrary units IgG; AUM: arbitrary units IgM; EM: erythema migrans; MEM; multiple erythema migrans; ACA: acrodermatitis chronica atrophicans; HBD: healthy controls.
Figure 2.
Levels of antiphospholipid antibodies in patients with Lyme borreliosis and healthy blood donors. aCL: anti-cardiolipin antibodies; aPA: anti-phosphatidic acid antibodies; aPC: anti-phosphatidylcholine antibodies, aPS: anti-phosphatidylserine antibodies; AUG: arbitrary units IgG; AUM: arbitrary units IgM; EM: erythema migrans; MEM; multiple erythema migrans; ACA: acrodermatitis chronica atrophicans; HBD: healthy controls.

Figure 3.
Correlation coefficients between aPS, aPA and aPC antibodies, shown separately for IgG and IgM isotypes. r: Pearson correlation coefficient, aPS: anti-phosphatidylserine antibodies; aPA: anti-phosphatidic acid antibodies; aPC: anti-phosphatidylcholine antibodies.
Figure 3.
Correlation coefficients between aPS, aPA and aPC antibodies, shown separately for IgG and IgM isotypes. r: Pearson correlation coefficient, aPS: anti-phosphatidylserine antibodies; aPA: anti-phosphatidic acid antibodies; aPC: anti-phosphatidylcholine antibodies.

Figure 4.
ROC analysis: comparison of area under the curve (AUC) between aPS G/M. aPA G/M and aPC G/M ELISAs.
Figure 4.
ROC analysis: comparison of area under the curve (AUC) between aPS G/M. aPA G/M and aPC G/M ELISAs.


Table 1.
Baseline demographic, serological, and clinical characteristics of study participants.
| Healthy blood donors (HBD, n=10) | Solitary erythema migrans (EM, n=10) | Multiple erythema migrans (MEM, n=10) | Acrodermatitis chronica atrophicans (ACA, n=10) | ||
| Age | Median (IQR) | 45 (12) | 56 (26) | 50 (20) | 75 (8) |
| Gender | M/F (%) | 78/22 | 60/40 | 40/60 | 10/90 |
| Skin culture for BB | n (% positive) | / | 1/7 (14.3) | 2/9 (22.2) | 0/10 (0) |
| Borrelia antibodies IgG | n (% positive) | / | 7 (70) | 9 (90) | 10 (100) |
| Borrelia antibodies IgM | n (% positive) | / | 1 (10) | 9 (90) | 7 (70) |
Table 2.
Levels of aPS, aPA, and aPC in healthy blood donors.
| aPS | aPA | aPC | No. of positive aPL | ||||
| IgG [AUG] | IgM [AUG] | IgG [AUG] | IgM [AUG] | IgG [AUG] | IgM [AUG] | ||
| HBD 1 | 3.4 | 7.1 | 24.6 | 0.5 | 6.1 | 3.4 | 0 |
| HBD 2 | 4.5 | 3.9 | 28.1 | 4.1 | 3.3 | 3.7 | 0 |
| HBD 3 | 7.1 | 15.2 | 21.6 | 5.4 | 10.1 | 13.2 | 0 |
| HBD 4 | 5.5 | 3.8 | 17.9 | 2.9 | 8.7 | 4.4 | 0 |
| HBD 5 | 2.1 | 4.1 | 14.8 | 3.1 | 5.1 | 3.7 | 0 |
| HBD 6 | 2.0 | 8.0 | 10.8 | 4.1 | 4.4 | 3.5 | 0 |
| HBD 7 | 3.2 | 15.6 | 15.3 | 9.17** | 12.7 | 10.4 | 1 |
| HBD 8 | 1.7 | 6.1 | 8.8 | 3.0 | 5.1 | 5.7 | 0 |
| HBD 9 | 3.9 | 4.5 | 16.4 | 3.6 | 6.4 | 6.3 | 0 |
| HBD 10 | 2.3 | 9.6 | 7.4 | 4.3 | 4.3 | 3.6 | 0 |
| HBD 11 | 6.1 | 7.6 | 16.9 | 3.5 | 8.4 | 2.3 | 0 |
| HBD 12 | 1.9 | 9.4 | 11.5 | 6.36* | 8.3 | 10.6 | 1 |
| HBD 13 | 3.6 | 3.7 | 12.4 | 2.7 | 8.2 | 23.9** | 1 |
| HBD 14 | 2.8 | 4.6 | 19.9 | 1.9 | 11.1 | 2.9 | 0 |
| HBD 15 | 4.5 | 2.6 | 13.3 | 2.8 | 9.5 | 2.8 | 0 |
| HBD 16 | 1.9 | 5.7 | 17.4 | 2.4 | 5.9 | 2.6 | 0 |
| HBD 17 | 2.9 | 6.4 | 9.7 | 4.1 | 5.9 | 7.6 | 0 |
| HBD 18 | 2.0 | 14.7 | 14.2 | 3.7 | 10.7 | 5.5 | 0 |
| HBD 19 | 1.3 | 3.4 | 15.3 | 2.5 | 5.9 | 2.9 | 0 |
| HBD 20 | 4.8 | 5.4 | 21.7 | 2.7 | 5.6 | 2.3 | 0 |
| HBD 21 | 3.7 | 2.6 | 20.4 | 3.4 | 3.2 | 4.2 | 0 |
| HBD 22 | 2.4 | 3.0 | 15.5 | 2.7 | 7.6 | 2.2 | 0 |
| HBD 23 | 5.9 | 6.7 | 20.2 | 2.7 | 9.4 | 19.5* | 1 |
| HBD 24 | 4.9 | 4.0 | 23.0 | 2.6 | 8.0 | 2.7 | 0 |
| HBD 25 | 2.4 | 5.4 | 19.0 | 3.7 | 8.9 | 3.1 | 0 |
| HBD 26 | 2.5 | 12.4 | 27.3 | 4.5 | 5.2 | 2.3 | 0 |
| HBD 27 | 1.3 | 3.2 | 6.6 | 2.3 | 3.7 | 2.8 | 0 |
| HBD 28 | 2.4 | 4.9 | 8.7 | 2.6 | 4.9 | 2.9 | 0 |
| HBD 29 | 2.3 | 11.4 | 14.4 | 6.36* | 12.7 | 6.7 | 1 |
| HBD 30 | 6.5 | 7.4 | 11.7 | 4.1 | 3.8 | 6.1 | 0 |
| HBD 31 | 3.7 | 16.0* | 12.9 | 5.6 | 6.0 | 2.5 | 1 |
| HBD 32 | 1.3 | 10.3 | 7.4 | 3.5 | 4.9 | 3.8 | 0 |
| HBD 33 | 2.0 | 10.3 | 18.2 | 5.0 | 6.1 | 2.5 | 0 |
| HBD 34 | 4.3 | 11.5 | 40.1* | 5.5 | 7.8 | 4.4 | 1 |
| HBD 35 | 7.3* | 15.0 | 28.2 | 5.2 | 11.1 | 15.4 | 1 |
| HBD 36 | 2.2 | 2.2 | 9.4 | 2.1 | 7.4 | 2.5 | 0 |
| HBD 37 | 2.5 | 6.2 | 12.7 | 2.3 | 5.9 | 2.3 | 0 |
| HBD 38 | 4.5 | 2.5 | 24.4 | 2.1 | 8.3 | 2.8 | 0 |
| HBD 39 | 3.0 | 6.1 | 45.5** | 3.7 | 5.4 | 2.6 | 1 |
| HBD 40 | 2.0 | 1.5 | 8.2 | 1.5 | 3.4 | 1.8 | 0 |
| Mean | 3.3 | 6.9 | 16.6 | 3.5 | 7.0 | 4.9 | |
| 99th perc. | 6.87 | 15.48 | 35.71 | 6.36 | 12.73 | 17.95 | |
*Positive samples; **outliers, aPA: anti-phosphatidic acid antibodies; aPC: anti-phosphatidylcholine antibodies; aPS: anti-phosphatidylserine antibodies; HBD: healthy blood donors.
Table 3.
Levels of aPA, aPC, and aPS in Lyme borreliosis patients.
| aPS | aPA | aPC | No. of positive aPL | ||||
| IgG [AUG] | IgM [AUG] | IgG [AUG] | IgM [AUG] | IgG [AUG] | IgM [AUG] | ||
| EM 1 | 3.2 | 5.8 | 24.1 | 2.8 | 7.3 | 2.7 | 0 |
| EM 2 | 7.3* | 10.9 | 30.4 | 9.1* | 14.3* | 9.6 | 3 |
| EM 3 | 3.2 | 14.8 | 22.5 | 7.3* | 8.6* | 27.4* | 3 |
| EM 4 | 3.4 | 5.4 | 40.2* | 3.4 | 14.5* | 2.6 | 2 |
| EM 5 | 2.8 | 24.5* | 24.8 | 12.6* | 16.2* | 13.9 | 3 |
| EM 6 | 2.8 | 8.2 | 8.1 | 4.3 | 10.7 | 2.8 | 0 |
| EM 7 | 2.1 | 1.3 | 5.7 | 2.4 | 2.8 | 0.6 | 0 |
| EM 8 | 5.9 | 10.8 | 22.3 | 4.0 | 17.7* | 8.3 | 1 |
| EM 9 | 11.0* | 15.8 | 25.3 | 5.3 | 11.0 | 6.3 | 1 |
| EM 10 | 3.4 | 4.0 | 15.5 | 3.0 | 13.2* | 6.9 | 1 |
| mean | 3.4 | 8.6 | 19.8 | 3.6 | 8.0 | 6.0 | |
| No. of positives | 2 | 1 | 1 | 3 | 5 | 1 | |
| MEM 1 | 4.4 | 2.3 | 21.5 | 1.6 | 8.7 | 2.8 | 0 |
| MEM 2 | 8.4* | 4.5 | 44.9* | 3.2 | 14.5* | 6.6 | 3 |
| MEM 3 | 5.2 | 17.4* | 33.3 | 7.6* | 7.6 | 91.7* | 3 |
| MEM 4 | 3.8 | 15.3 | 32.9 | 10.8* | 11.8 | 2.3 | 1 |
| MEM 5 | 2.3 | 17.0* | 21.3 | 5.5 | 14.2* | 2.3 | 2 |
| MEM 6 | 8.6* | 58.6* | 27.2 | 15.0* | 15.2* | 4.3 | 4 |
| MEM 7 | 4.6 | 20.8* | 24.7 | 7.0* | 19.1* | 11.0 | 3 |
| MEM 8 | 4.9 | 18.2* | 18.8 | 6.5* | 15.6* | 7.9 | 3 |
| MEM 9 | 2.8 | 7.6 | 34.9 | 5.8 | 21.1* | 13.4 | 1 |
| MEM 10 | 16.2* | 3.8 | 27.1 | 2.8 | 16.6* | 35.3* | 3 |
| mean | 4.0 | 6.7 | 26.8 | 3.8 | 9.4 | 6.3 | |
| No. of positives | 3 | 5 | 1 | 5 | 7 | 2 | |
| ACA 1 | 8.7* | 30.7* | 46.2* | 19.2* | 14.9* | 10.1 | 5 |
| ACA 2 | 4.7 | 3.3 | 48.4* | 2.2 | 14.2* | 2.4 | 2 |
| ACA 3 | 5.5 | 19.0* | 34.6 | 29.4* | 14.4* | 14.1 | 3 |
| ACA 4 | 3.4 | 47.7* | 51.5* | 15.6* | 19.9* | 12.5 | 4 |
| ACA 5 | 27.8* | 14.0 | 43.0* | 6.0 | 56.9* | 100.0* | 4 |
| ACA 6 | 3.2 | 25.5* | 44.3* | 9.1* | 12.6 | 5.5 | 3 |
| ACA 7 | 2.9 | 28.9* | 49.7* | 9.5* | 13.7* | 21.6* | 5 |
| ACA 8 | 6.5 | 13.1 | 31.6 | 6.9* | 24.7* | 37.5* | 3 |
| ACA 9 | 1.8 | 11.8 | 14.3 | 4.0 | 11.7 | 5.3 | 0 |
| ACA 10 | 5.3 | 8.5 | 28.7 | 4.0 | 12.7 | 19.6 | 0 |
| mean | 4.1 | 10.1 | 27.3 | 4.1 | 12.3 | 9.9 | |
| No. of positives | 2 | 5 | 6 | 6 | 7 | 3 | |
*Positive samples; aPA: anti-phosphatidic acid antibodies; aPC: anti-phosphatidylcholine antibodies; aPS: anti-phosphatidylserine antibodies; EM: erythema migrans; MEM: multiple erythema migrans; ACA: acrodermatitis chronica atrophicans.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



