Submitted:
07 May 2026
Posted:
07 May 2026
You are already at the latest version
Abstract
Background: Continuous positive airway pressure (CPAP) is the primary treatment for Obstructive Sleep Apnea (OSA). Despite improvements in CPAP technology and management, adherence to therapy remains one of the main issues to be fixed. Methods: We conducted a narrative review through PubMed (1995-2025). Studies were selected by clinical relevance, methodological quality and expert consensus. Results: OSA treatment outcomes are poor when CPAP adherence is defined as four hours per night. The first step in improving adherence is active patient involvement. This involves explaining what OSA is, its consequences, what PAP therapy is, and its potential benefits. The right mask should be chosen for each patient; a nasal mask should be the first choice according to the Starling resistor model. OSA endotype and phenotype traits could be used to predict adherence, guide adjunct therapy, or suggest titration. Problems during the first night and the first month are the main predictors of future adherence. Strategies such as cognitive behavioral therapy or motivational enhancement can improve adherence, especially during the initial period. Long-term adherence can be predicted by the initial one and maintained with scheduled follow-up. Group meetings, telephone calls and telemedicine interactions are also a valid way of improving adherence. Conclusions: A Patients should initially be educated about how their symptoms are related to sleep apnoea and how CPAP treatment could resolve them. The key to improving CPAP adherence is to involve patients in personalised treatment with scheduled follow-up, particularly during the initial treatment period.
Keywords:
obstructive sleep apnea
; continuous positive airway pressure
; adherence
; obstructive sleep apnea treatment
; personalized medicine
1. Introduction
Continuous Positive airway Pressure (CPAP) therapy represents the first-line treatment for Obstructive Sleep Apnea (OSA), effectively reducing disease severity, daytime sleepiness, systemic blood pressure, and motor vehicle accidents, while significantly improving health- and sleep-related quality of life [1]. Adherence is part of the daily clinical practice of all specialists who treat patients with OSA but is also a challenge. In the last few years literature focused on the main factors able to improve the adherence and the different strategies used by clinicians [2,3,4]. Recent evidence demonstrated a statistically significant reduction in hospitalizations and emergency room visits in obese OSA patients with a good adherence to CPAP compared to poor adherent ones [5]. Although improvements in CPAP technology and their masks, only 50-60% of patients have a long-term adherence to this treatment [4]. This poor adherence to CPAP treatment among a significant proportion of the OSA population, despite technological advances, highlights the need to develop a more integrated and patient-centered approach. In this context, identifying the factors that influence treatment adherence and implementing practical strategies to address these factors is a key priority in the OSA management. The aim of this narrative review is to rethink CPAP adherence with a multifactorial approach that takes into account patient traits, their phenotype, and treatment-related factors, leading to a personalized approach to optimize long-term adherence.
2. Materials and Methods
In this narrative review, we have summarised the recent evidence regarding the factors influencing treatment adherence and strategies to improve adherence in patients with OSA.A comprehensive literature search was conducted using PubMed/MEDLINE (from January 1995 to December 2025) and Google Scholar. The search strategy included combinations of the following keywords: “obstructive sleep apnea”, “OSA”, “continuous positive airway pressure”, “CPAP adherence”, “compliance”, “telemedicine”, “cognitive behavioral therapy”, “mask interface”, “OSA phenotype” and “endotype”.Two separate authors reviewed titles, abstracts and full-text articles to select studies of high clinical and methodological quality. The review included high-quality randomized controlled trials, observational studies, meta-analyses and narrative reviews focusing on CPAP adherence, its determinants and potential solutions. This article is based exclusively on previously published studies and does not include any new studies conducted by the authors on human or animal subjects.
3. Results
3.1. The Limits of the 4-Hour Threshold in CPAP Adherence
In 2009, the Centers for Medicare & Medicaid Services adopted a requirement of minimum 4 hours of Positive Airway Pressure (PAP) use for 70% of nights, or 21 days in a consecutive 30-day period, to continue medical coverage for PAP therapy [6]. The use of an economical instead a clinical definition is the first CPAP adherence issue to be fixed. Few hours during the night could not improve symptoms, quality of life or reduce cardiovascular risk, with a subsequent reduction in patient motivation. Daytime sleepiness improves after 7 hours of sleep, with 7 hours and 30 minutes as the medium time necessary to reach a good performance status [7]. Considering that a physiological hypnogram has a prevalence of Rapid-Eye Movement (REM) sleep in the second half of the night and that REM-OSA is associated with higher cardiovascular risk, an OSA patient who removes the mask after only the first 4 hours of sleep will not treat the deeper desaturations, the more severe events and the cardiovascular risk [8,9]. Always more studies showed that CPAP efficacy have a dose-response effect [10], suggesting that the ineffectiveness of CPAP in terms of cardiovascular and metabolic health in some trials is partly due to poor adherence [11].
3.2. Patients-Related Factors
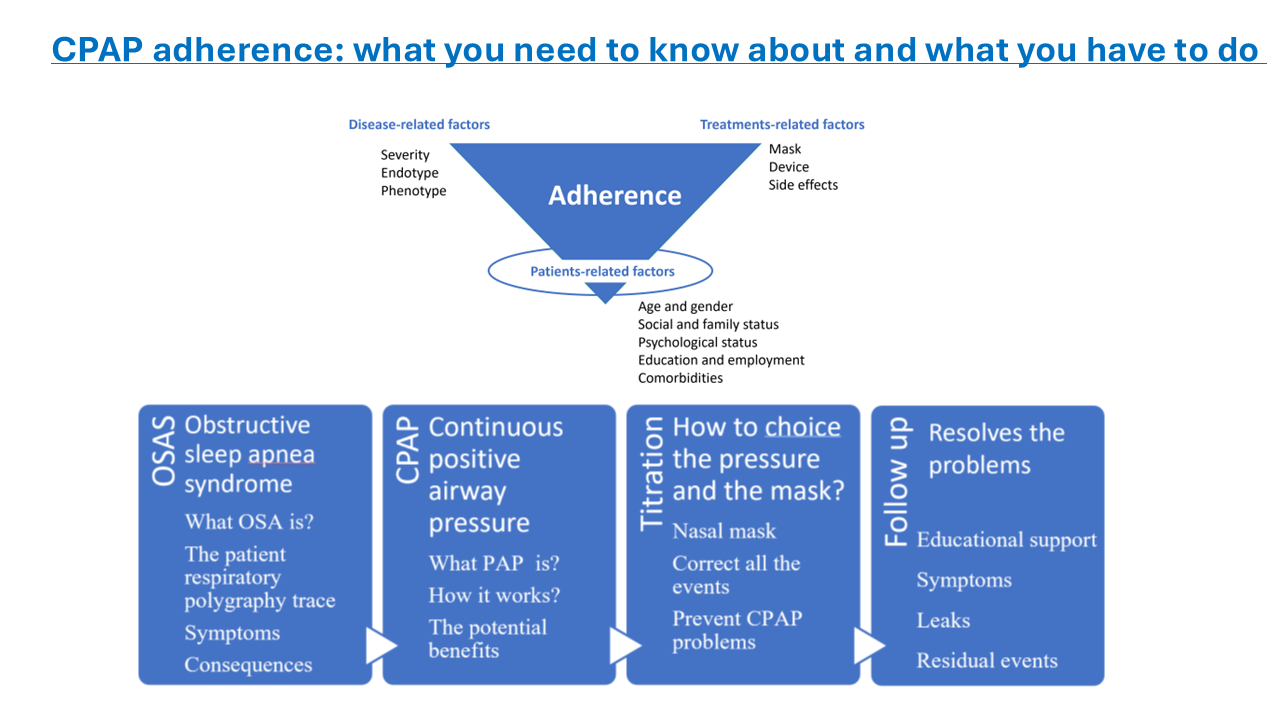
We could divide the factors that influence the adherence in patient related factors (sex, gender, age, socioeconomical status etc..), disease- related factors (endotype and phenotype), and treatment-related factors (like mask or PAP) (Fig.1). The data regarding sex is currently controversial, as some studies have shown that women adherence to CPAP is lower than men, while other studies have shown the opposite [12,13]. Recent findings suggest paying attention to the relationship with the bed partner. Concerns about the impact of CPAP on physical closeness, communication, and sexual intimacy are frequently cited by patients as barriers to regular use [14]. An adequate support is necessary to improve the CPAP adherence but in some occasions the bed partner is an obstacle to use the device [15]. Few studies suggest that a good comprehension of what is a CPAP could help to better introduce the device in the intimacy of a couple [15]. On the contrary, other patients report that the equipment used can interrupt the couple's intimacy. This has a negative effect on both the relationship and adherence to therapy, creating a vicious circle that worsens both [16]. Data on the impact of age on treatment adherence, however, consistently show a biphasic pattern: the number of hours of use per night increases gradually up to the age of 75–80, after which there is a rapid decline in night-time use [17,18]. Comorbidities also influence CPAP adherence. Comorbid Insomnia and Obstructive Sleep Apnea (COMISA), the condition in which OSA and insomnia coexist, is associated with a greater burden of symptoms and lower CPAP usage compared to those with OSA alone [19]. However, randomised clinical trials have shown that the use of Cognitive Behavioural Therapy for Insomnia (CBT-I) prior to CPAP significantly increased CPAP adherence in COMISA patients [20,21]. For this reason, it is necessary to recognise and treat insomnia first, or at the same time as starting CPAP treatment. Starting a CPAP therapy in OSA patients suffering from depression, a quite common comorbidity (around 35% according to a large systematic review), could be challenging [22]. Real-world data show that the presence of depression is associated with reduced long-term adherence to CPAP and also fewer hours of APAP use during the first week of autotitration [23,24]. Clinically significant anxiety, with a prevalence around 32% in OSA, is also associated with a reduced number of hours of night-time CPAP use, although anxiety scores improve significantly in OSA patients adhering to CPAP therapy [22,25,26]. Restless syndrome (RLS) and Periodic Limb Movements (PLMs) are others two quite common comorbidities in OSA (around 20% for RLS and and around 14% for PLMs) could interfere dramatically with the CPAP adherence [27,28,29].
Figure 1.
Main factors influencing CPAP adherence in OSA.

Fig.1 CPAP adherence is influenced by the interaction of disease-related, treatment-related, and patient-related factors. Disease-related factors include OSA severity, endotype, and phenotype, which reflect the underlying pathophysiology. Treatment-related factors encompass device characteristics, mask interface, and therapy-related side effects. Patient-related factors—such as age, gender, psychological status, social and family context, educational level, and comorbidities—represent the core component modulating treatment acceptance and long-term use. The figure highlights the central role of patient-related factors in mediating the impact of both disease and treatment variables on adherence.
3.3. Disease-Related Factors
OSA phenotypes also influence the adherence to CPAP treatment. Patients with the sleepy phenotype are generally more likely to adhere to the treatment because their quality of life improves significantly using CPAP [30]. Snoring is another symptom that disappears immediately with CPAP, and this has a strong impact on adherence due to the beneficial effect on patient and his/her bed partner [31]. Non-sleepy, older with comorbidities and female are three phenotypes less likely to adhere to the treatment [30,32]. One common misconception is that patients with mild OSA are less likely to adhere to CPAP therapy. For example, patients with low arousal threshold usually have mild to moderate OSA but experience significant sleepiness and insomnia [33]. CPAP therapy improves their symptoms [34]. For this reason, symptomatic patients with mild OSA may be more adherent compared with severe asymptomatic ones. Clearly, we can't use OSA severity to predict our patient's adherence to CPAP treatment. Recent evidence suggests that an approach “one size fits all” is not appropriate in OSA, as the pathophysiology of upper airway collapse can differ across patients [35]. The anatomical susceptibility to upper airway collapse varies among OSA patients, leading to inter-individual differences in CPAP efficacy. In some patients, the predominant anatomical factor is associated with greater CPAP efficacy. In other patients, the anatomical factor is less prominent, while other non-anatomical traits, such as high ventilatory control instability (loop gain), low arousal threshold and low upper airway muscle responsiveness, contribute to OSA pathophysiology and may limit CPAP efficacy and tolerance [36].For example, individuals with high loop gain may predispose to an exaggerated ventilatory response to respiratory events [37]. In this case, large or rapid pressure changes during auto-adjusting APAP, may predispose patients to central apneas occurrence [37]. On the other hand, patients with low arousal threshold may report frequent arousals during pressure variations in auto-adjusting APAP [38]. However, current evidence does not support using endotypes alone to predict CPAP adherence, due to the absence of statistically significant differences for adherence between endotypes in pilot studies [39]. Although these observations support a more cautious and individualized approach to pressure titration in selected patients, dedicated prospective studies are still needed.
3.4. Device-Related Factors
The choice of an appropriate interface represents a key point for treatment adherence. An inadequate size may result in discomfort or excessive leaks. Patients generally prefer nasal masks and nasal pillow interfaces for their lower contact surface and greater comfort [40]. Current evidence supports that nasal interfaces are associated with better adherence, improved comfort, and lower leak rates compared with oronasal masks [41]. Nasal mask also reproduces natural breathing, whereas oral breathing only minimal contributes to sleep breathing pattern [42]. Indeed, oral breathing is associated with increased upper airway resistance and reduced upper airway stability [43]. For these reasons, the use of oronasal masks may be counterproductive by promoting posterior tongue collapse and increasing pharyngeal collapsibility [43]. Moreover, the usage of oronasal masks require higher PAP compared to nasal ones [44]. Between nasal masks and nasal pillows, available evidence suggests comparable efficacy in terms of residual AHI and sleep architecture, with only minimal differences in adherence [45]. Therefore, the choice between these interfaces should be guided primarily by patient comfort and preference. Another crucial point to manage is nasal obstruction. Approximately 15% of OSA patients report nasal obstructive, without any correlation between OSA severity and nasal obstruction severity [46]. Increased nasal resistance does not directly cause OSA, but can increase upper airway resistance, leading to oral breathing predominance and increased pharyngeal collapsibility [47]. As demonstrated by Sugiura T et al, an increased nasal resistance before CPAP treatment predicted CPAP non-acceptance [48]. For these reasons, we need to improve nasal patency before first CPAP trial. A complete evaluation including the investigation of nasal symptoms, history of allergic rhinitis, chronic congestion or prior nasal surgery is necessary. Saline irrigations and intranasal corticosteroids may be particularly efficacy before CPAP titration in patients with inflammatory conditions [49,50]. Another crucial point of CPAP adherence is the therapeutic PAP choice. Nowadays, home-based PAP auto-titration represent the most widely adopted and cost-effective approach [51]. Home-based PAP auto-titration starts with an initial period where PAP may be suboptimal, potentially leading to residual respiratory events, flow limitation or snoring [52]. These factors may negatively affect early adherence, highlighting the importance of appropriate patient counselling to set expectations during this phase [52]. Reducing these residual events by controlling pressure settings is associated with improved CPAP adherence and increased comfort [53]. Importanly, the first 2-4 weeks of therapy are a critical period for the future CPAP adherence [54]. During this phase, a suboptimal titration and PAP-related discomfort may significantly contribute to low long-term adherence, highlighting the importance of early PAP optimization and initial close follow-up [54]. Regarding to comparison for long-term adherence between APAP and fixed-CPAP remains debated. Current evidence did not demonstrate a clear advantage for CPAP or APAP in terms of adherence, daytime sleepiness or quality of life [55].
3.5. The Patients’ Perception
CPAP and OSA patients’ perception represent a key point for obtaining a good long-term adherence. Effective communication should include a clear explanation of obstructive sleep apnea, its clinical consequences, and the expected benefits of CPAP therapy. Personalizing this discussion, by linking the patient’s reported symptoms to OSA and explaining how CPAP may alleviate them, can enhance treatment acceptance as demonstrated by Jurado-Gamez B et al, where a correct information about their conditions leads to 1-hour increase of CPAP daily-use [56]. Many patients are not aware that symptoms such as nocturia or morning headaches may be related to sleep apnea, and increasing this awareness may improve engagement. Another simple intervention to improve therapy adherence may be reviewing polysomnographic data (e.g., oxygen desaturation and airflow tracings), which has improved both follow-up attendance and long-term adherence in a study by Falcone VA et al [57]. Overall, these findings highlight the central role of the initial approach to CPAP therapy, underscoring the importance of patient-centered communication during both the first encounter and the titration phase.
3.6. Follow Up
Early follow up represents one of the most effective interventions for improving long-term CPAP adherence [58]. Current guidelines emphasize the crucial role of close follow up during the initial phase of CPAP therapy, in order to rapidly identify device-related issues [59]. The most commonly reported side effects within the first month include dry mouth and nasal symptoms, such as congestion or mucosal irritation [60]. Additional issues may include mask leaks, skin lesions related to the interface, airflow-related discomfort, and sleep fragmentation [61]. In these cases, a careful management of mask fitting, circuit leaks and air humidification may improve patients’ adherence [62]. Educational and behavioral interventions have been shown improvements in adherence. Continuous support with telemedicine, telephone follow-up, group-base interviews and cognitive-behavioral therapy may improve CPAP adherence by enhancing patients’ engagement [63,64]. Clinicians should always evaluate emerging conditions during initial CPAP therapy phase, including insomnia, depressive symptoms or sleep-related movement disorders because these issues can cause CPAP interruption [65,66,67].
4. Discussion
CPAP adherence in OSA is a complex issue that requires a personalised and multidimensional approach. Although CPAP has been shown to be efficacious in improving clinical outcomes, only around half of patients maintain optimal long-term adherence, leading to a critical issue which needs to be prioritized in sleep medicine [68]. In this review, we have highlighted how adherence to CPAP does not depend solely on device- or mask-related factors, but also on patient-related factors such as phenotype and endotype. This issue should be carefully considered when developing a personalised treatment plan for OSA patients. This multidynamic model emphasises that adherence should be treated as a dynamic process that evolves over time, rather than a static condition (Fig. 2). Making patients aware of their symptoms, of the condition and its consequences are the first elements to be considered during patient management. In this phase, reviewing respiratory polygraphy or polysomnographic data with the patient may significantly enhance understanding and engagement. Effective communication and patient’s active involvement can improve adherence to CPAP. In this review, we have also highlighted how psychosocial factors, including relationship dynamics, mental health disorders and socioeconomic status, can influence treatment acceptance and, consequently, adherence. Insomnia, depression and anxiety can pose significant barriers to treatment adherence if not properly recognised and managed. In this trajectory, cognitive-behavioural interventions in patients with COMISA have demonstrated a significant increase in CPAP adherence [20,21]. In the second phase, it is essential to properly introduce CPAP therapy to the patient. This involves not only explaining how it works but also highlighting the potential clinical benefits that can be achieved through CPAP. CPAP titration is a crucial step in determining future adherence to therapy, as it involves the selection of the PAP level and interface. Personalising the mask choice, optimising pressure settings and managing initial side effects are essential to ensure comfort and reduce the risk of early discontinuation of therapy. It is important to emphasise that this phase should not be viewed as purely technical. At this stage, it is vital to consider the patient’s phenotype and endotype, as our review has shown that tolerance may vary during APAP auto-titration. It is also essential to verify that all residual respiratory events are properly resolved during therapy. The final phase is follow-up. Early follow-up, particularly during the first few weeks of treatment, helps identify patients at higher risk of treatment failure, perhaps even through the use of telemonitoring, which is gaining increasingly strong scientific support.
It is important to emphasise that these phases constitute interconnected elements of a multidynamic pathway. The concept highlighted by our review is that adherence to CPAP needs a patient-centred clinical approach.
Figure 2.
The four steps to optimize CPAP adherence in OSA patients.

Fig.2 The figure illustrates a structured, stepwise approach to CPAP adherence in patients with obstructive sleep apnea (OSA). The process begins with patient education and disease awareness, including understanding symptoms, consequences, and sleep study findings. This is followed by CPAP introduction, focusing on explaining the mechanism of action and expected benefits. The next phase involves CPAP titration, including the selection of appropriate pressure settings and mask interface, with the aim of optimizing comfort and preventing early treatment-related issues. Finally, structured follow-up addresses common barriers to adherence, such as residual symptoms, mask leaks, and device-related problems, through continuous educational support and troubleshooting. This pathway emphasizes the dynamic and patient-centered nature of CPAP adherence.
5. Conclusions
This review has highlighted that CPAP prescription should follow a multidimensional, patient-centered approach that integrates clinical, physiological and educational aspects.
Early patient involvement, personalized education, optimization of therapeutic PAP, mask selection and early management of any initial adverse effects are crucial for long-term adherence. Although technological advances such as new CPAP devices and new interfaces (nasal prongs or under-the-nose masks) have improved patient comfort, these alone are not sufficient to ensure adherence. Instead, a multidimensional approach is required, including appropriate mask selection, management of nasal obstruction, personalized pressure titration and continuous follow-up. The role of telemedicine in this regard could be the key to ensuring long-term adherence on a large scale.
Future research should focus on refining personalized treatment strategies, including the potential role of phenotypic and endotypic characterization, as well as on developing targeted interventions to improve adherence in high-risk populations.
Author Contributions
Conceptualization, C.A, A.F.. and A.S.; methodology, B. R., A.N.., A.S..; software, F.O.; validation, C.A., A.F., M.B. and P.P.; formal analysis, M.C. F.O.; investigation, A.F.; resources, A.N.; data curation, F.O, F.S.; writing—original draft preparation, C.A., A.F. N. P. and A.S.; writing—review and editing, A.S., M.B. and P.P.; visualization, F.O, P.C. S. S.; supervision, P.P.; project administration, M.B.; funding acquisition, P.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
No new data were created for this review.
Acknowledgments
During the preparation of this work the authors used ChatGPT 5.0 (OpenAI) in order to improve readability, language editing and stylistic refinement of the manuscript. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Patil, S.P.; Ayappa, I.A.; Caples, S.M.; Kimoff, R.J.; Patel, S.R.; Harrod, C.G. Treatment of Adult Obstructive Sleep Apnea with Positive Airway Pressure: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2019, 15(2), 335–343. [Google Scholar] [CrossRef]
- Bakker, J.P.; Weaver, T.E.; Parthasarathy, S.; Aloia, M.S. Adherence to CPAP: What Should We Be Aiming For, and How Can We Get There? CHEST 2019, 155(6), 1272–1287. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.J.; Finnsson, E.; Ágústsson, J.S.; Sands, S.A.; Hang, L.W. Continuous positive airway pressure and adherence in patients with different endotypes of obstructive sleep apnea. J. Sleep Res. 2024, 33(1), e13999. [Google Scholar] [CrossRef]
- Wickwire, E.M.; Lettieri, C.J.; Cairns, A.A.; Collop, N.A. Maximizing positive airway pressure adherence in adults: a common-sense approach. Chest 2013, 144(2), 680–693. [Google Scholar] [CrossRef] [PubMed]
- Sert Kuniyoshi, F.H.; Cameron, A.; Pépin, J.L.; et al. Adherence to positive airway pressure therapy and healthcare resource utilization and costs among patients with obstructive sleep apnea and obesity. Int. J. Obes. (Lond) 2026, 50(4), 741–749. [Google Scholar] [CrossRef]
- Naik, S.; Al-Halawani, M.; Kreinin, I.; Kryger, M. Centers for Medicare and Medicaid Services Positive Airway Pressure Adherence Criteria May Limit Treatment to Many Medicare Beneficiaries. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2019, 15(2), 245–251. [Google Scholar] [CrossRef] [PubMed]
- Antic, N.A.; Catcheside, P.; Buchan, C.; et al. The Effect of CPAP in Normalizing Daytime Sleepiness, Quality of Life, and Neurocognitive Function in Patients with Moderate to Severe OSA. Sleep 2011, 34(1), 111–119. [Google Scholar] [CrossRef]
- Karuga, F.F.; Kaczmarski, P.; Białasiewicz, P.; et al. REM-OSA as a Tool to Understand Both the Architecture of Sleep and Pathogenesis of Sleep Apnea-Literature Review. J. Clin. Med. 2023, 12(18), 5907. [Google Scholar] [CrossRef]
- Acosta-Castro, P.; Hirotsu, C.; Marti-Soler, H.; et al. REM-associated sleep apnoea: prevalence and clinical significance in the HypnoLaus cohort. Eur. Respir. J. 2018, 52(2), 1702484. [Google Scholar] [CrossRef]
- Xu, P.H.; Hui, C.K.M.; Lui, M.M.S.; Lam, D.C.L.; Fong, D.Y.T.; Ip, M.S.M. Incident Type 2 Diabetes in OSA and Effect of CPAP Treatment: A Retrospective Clinic Cohort Study. Chest 2019, 156(4), 743–753. [Google Scholar] [CrossRef]
- Sánchez-de-la-Torre, M.; Gracia-Lavedan, E.; Benitez, I.D.; et al. Adherence to CPAP Treatment and the Risk of Recurrent Cardiovascular Events: A Meta-Analysis. JAMA 2023, 330(13), 1255–1265. [Google Scholar] [CrossRef]
- Ye, L.; Pien, G.W.; Weaver, T.E. Gender differences in the clinical manifestation of obstructive sleep apnea. Sleep Med. 2009, 10(10), 1075–1084. [Google Scholar] [CrossRef]
- Fabozzi, A.; Pasqualotto, F.; Laguardia, M.; et al. Gender differences in obstructive sleep apnea syndrome: a pilot study. Sleep Breath. 2024, 28(4), 1645–1650. [Google Scholar] [CrossRef]
- Rapelli, G.; Pietrabissa, G.; Angeli, L.; et al. Assessing the needs and perspectives of patients with obesity and obstructive sleep apnea syndrome following continuous positive airway pressure therapy to inform health care practice: A focus group study. Front Psychol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Rapelli, G.; Caloni, C.; Cattaneo, F.; et al. Three in a Bed: Can Partner Support Improve CPAP Adherence? A Systematic Review and Intervention Recommendations. J. Pers. Med. 2025, 15(5), 192. [Google Scholar] [CrossRef] [PubMed]
- Stannek, T.; Hürny, C.; Schoch, O.D.; Bucher, T.; Münzer, T. Factors affecting self-reported sexuality in men with obstructive sleep apnea syndrome. J. Sex. Med. 2009, 6(12), 3415–3424. [Google Scholar] [CrossRef]
- Prigent, A.; Blanloeil, C.; Serandour, A.L.; Barlet, F.; Gagnadoux, F.; Jaffuel, D. A biphasic effect of age on CPAP adherence: a cross-sectional study of 26,343 patients. Respir. Res. 2023, 24(1), 234. [Google Scholar] [CrossRef]
- Antonaglia, C.; Fabozzi, A.; Steffanina, A.; Ture, R.; Palange, P.; Confalonieri, M. Walking the fine line between OSA and aging. Sleep Breath. 2025, 29(3), 195. [Google Scholar] [CrossRef]
- Cole, K.V.; Malik, A.S.; Cistulli, P.A.; et al. Positive Airway Pressure Therapy and Health Care Resource Use in Patients With OSA and Comorbid Insomnia. Chest 2025. Published online September 25, 2025. [Google Scholar] [CrossRef] [PubMed]
- Sweetman, A.; Lack, L.; Catcheside, P.G.; et al. Cognitive and behavioral therapy for insomnia increases the use of continuous positive airway pressure therapy in obstructive sleep apnea participants with comorbid insomnia: a randomized clinical trial. Sleep 2019, 42(12), zsz178. [Google Scholar] [CrossRef]
- Ong, J.C.; Crawford, M.R.; Wallace, D.M. Sleep Apnea and Insomnia: Emerging Evidence for Effective Clinical Management. Chest 2021, 159(5), 2020–2028. [Google Scholar] [CrossRef]
- Garbarino, S.; Bardwell, W.A.; Guglielmi, O.; Chiorri, C.; Bonanni, E.; Magnavita, N. Association of Anxiety and Depression in Obstructive Sleep Apnea Patients: A Systematic Review and Meta-Analysis. Behav. Sleep Med. 2020, 18(1), 35–57. [Google Scholar] [CrossRef] [PubMed]
- Qiao, M.; Xie, Y.; Wolff, A.; Kwon, J. Long term adherence to continuous positive Airway pressure in mild obstructive sleep apnea. BMC Pulm. Med. 2023, 23(1), 320. [Google Scholar] [CrossRef]
- Law, M.; Naughton, M.; Ho, S.; Roebuck, T.; Dabscheck, E. Depression may reduce adherence during CPAP titration trial. J. Clin. Sleep Med. 2014, 10(2), 163–169, Published 2014 Feb 15. [Google Scholar] [CrossRef] [PubMed]
- Budhiraja, R.; Kushida, C.A.; Nichols, D.A.; et al. Impact of Randomization, Clinic Visits, and Medical and Psychiatric Cormorbidities on Continuous Positive Airway Pressure Adherence in Obstructive Sleep Apnea. J. Clin. Sleep Med. 2016, 12(3), 333–341. [Google Scholar] [CrossRef] [PubMed]
- Vanek, J.; Prasko, J.; Genzor, S.; et al. Cognitive Functions, Depressive and Anxiety Symptoms After One Year of CPAP Treatment in Obstructive Sleep Apnea. Psychol. Res. Behav. Manag. 2023, 16, 2253–2266. [Google Scholar] [CrossRef]
- Amirifard, H.; Jameie, M.; Akbarpour, S.; et al. Sleep microstructure and clinical characteristics of patients with restless legs syndrome. J. Clin. Sleep Med. 2022, 18(11), 2653–2661. [Google Scholar] [CrossRef]
- Lee, S.A.; Kim, S.J.; Lee, S.Y.; Kim, H.J. Periodic limb movements during sleep are associated with poor health-related quality of life in patients with obstructive sleep apnea. Sleep Breath. 2022, 26(3), 1045–1052. [Google Scholar] [CrossRef]
- Romero-Peralta, S.; Cano-Pumarega, I.; Garcia-Malo, C.; Agudelo Ramos, L.; García-Borreguero, D. Treating restless legs syndrome in the context of sleep disordered breathing comorbidity. Eur. Respir. Rev. 2019, 28(153), 190061. [Google Scholar] [CrossRef]
- Zinchuk, A.; Yaggi, H.K. Phenotypic Subtypes of OSA: A Challenge and Opportunity for Precision Medicine. Chest 2020, 157(2), 403–420. [Google Scholar] [CrossRef]
- Berry, R.B.; Block, A.J. Positive nasal airway pressure eliminates snoring as well as obstructive sleep apnea. Chest 1984, 85(1), 15–20. [Google Scholar] [CrossRef]
- Lo Bue, A.; Salvaggio, A.; Iacono Isidoro, S.; Romano, S.; Insalaco, G. OSA and CPAP therapy: effect of gender, somnolence, and treatment adherence on health-related quality of life. Sleep Breath Schlaf Atm. 2020, 24(2), 533–540. [Google Scholar] [CrossRef] [PubMed]
- Citton, G.M.; Antonaglia, C.; Fabozzi, A.; Steffanina, A.; Giannone, S.; Manna, M.; Prezioso, G.; Torregiani, C.; Confalonieri, P.; Salton, F.; Ruaro, B.; Palange, P.; Confalonieri, M. Sex differences in low arousal threshold in obstructive sleep apnea. Respir. Med. 2026, 252, 108625. [Google Scholar] [CrossRef] [PubMed]
- Edwards, B.A.; Eckert, D.J.; McSharry, D.G.; et al. Clinical predictors of the respiratory arousal threshold in patients with obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2014, 190(11), 1293–1300. [Google Scholar] [CrossRef]
- Eckert, D.J. Phenotypic approaches to obstructive sleep apnoea - New pathways for targeted therapy. Sleep Med. Rev. 2018, 37, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Eckert, D.J.; White, D.P.; Jordan, A.S.; Malhotra, A.; Wellman, A. Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am. J. Respir. Crit. Care Med. 2013, 188(8), 996–1004. [Google Scholar] [CrossRef]
- Wellman, A.; Edwards, B.A.; Sands, S.A.; et al. A simplified method for determining phenotypic traits in patients with obstructive sleep apnea. J. Appl. Physiol. Bethesda Md. 1985 2013, 114(7), 911–922. [Google Scholar] [CrossRef]
- Hang, L.W.; Huang, C.S.; Cheng, W.J. Clinical characteristics of Asian patients with sleep apnea with low arousal threshold and sleep structure change with continuous positive airway pressure. Sleep Breath Schlaf Atm. 2021, 25(3), 1309–1317. [Google Scholar] [CrossRef]
- Cheng, W.J.; Finnsson, E.; Ágústsson, J.S.; Sands, S.A.; Hang, L.W. Continuous positive airway pressure and adherence in patients with different endotypes of obstructive sleep apnea. J. Sleep Res. 2024, 33(1), e13999. [Google Scholar] [CrossRef]
- Teo, M.; Amis, T.; Lee, S.; Falland, K.; Lambert, S.; Wheatley, J. Equivalence of nasal and oronasal masks during initial CPAP titration for obstructive sleep apnea syndrome. Sleep 2011, 34(7), 951–5. [Google Scholar] [CrossRef]
- Chen, L.Y.; Chen, Y.H.; Hu, S.W.; Lin, M.T.; Lee, P.L.; Chiang, A.A.; Tu, Y.K. In search of a better CPAP interface: A network meta-analysis comparing nasal masks, nasal pillows and oronasal masks. J. Sleep Res. 2022, 31(6), e13686. [Google Scholar] [CrossRef]
- Fitzpatrick, M.F.; Driver, H.S.; Chatha, N.; Voduc, N.; Girard, A.M. Partitioning of inhaled ventilation between the nasal and oral routes during sleep in normal subjects. J. Appl. Physiol. Bethesda Md. 1985 2003, 94(3), 883–890. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, M.F.; McLean, H.; Urton, A.M.; Tan, A.; O’Donnell, D.; Driver, H.S. Effect of nasal or oral breathing route on upper airway resistance during sleep. Eur. Respir. J. 2003, 22(5), 827–832. [Google Scholar] [CrossRef] [PubMed]
- de Andrade, R.G.S.; Piccin, V.S.; Nascimento, J.A.; Viana, F.M.L.; Genta, P.R.; Lorenzi-Filho, G. Impact of the type of mask on the effectiveness of and adherence to continuous positive airway pressure treatment for obstructive sleep apnea. J. Bras. Pneumol. Publicacao Soc. Bras. Pneumol. E Tisilogia 2014, 40(6), 658–668. [Google Scholar] [CrossRef] [PubMed]
- Deng, B.; Lai, F.; Zhang, M.; et al. Nasal pillow vs. standard nasal mask for treatment of OSA: a systematic review and meta-analysis. Sleep Breath. 2023, 27(4), 1217–1226. [Google Scholar] [CrossRef]
- Young, T.; Finn, L.; Kim, H. Nasal obstruction as a risk factor for sleep-disordered breathing. The University of Wisconsin Sleep and Respiratory Research Group. J Allergy Clin Immunol. 1997, 99(2), S757–62. [Google Scholar] [CrossRef]
- Basner, R.C.; Simon, P.M.; Schwartzstein, R.M.; Weinberger, S.E.; Weiss, J.W. Breathing route influences upper airway muscle activity in awake normal adults. J. Appl. Physiol. Bethesda Md. 1989, 66(4), 1766–1771. [Google Scholar] [CrossRef]
- Sugiura, T.; Noda, A.; Nakata, S.; et al. Influence of Nasal Resistance on Initial Acceptance of Continuous Positive Airway Pressure in Treatment for Obstructive Sleep Apnea Syndrome. Respiration 2005, 74(1), 56–60. [Google Scholar] [CrossRef]
- Charakorn, N.; Hirunwiwatkul, P.; Chirakalwasan, N.; Chaitusaney, B.; Prakassajjatham, M. The effects of topical nasal steroids on continuous positive airway pressure compliance in patients with obstructive sleep apnea: a systematic review and meta-analysis. Sleep Breath 2017, 21(1), 3–8. [Google Scholar] [CrossRef]
- Segsarnviriya, C.; Mahakit, P. 0625 The Effects of Topical Nasal Steroids on Continuous Positive Airway Pressure Compliance in Patients with Obstructive Sleep Apnea. Sleep 2020, 43 Supplement_1, A239. [Google Scholar] [CrossRef]
- Berry, R.B.; Sriram, P. Auto-adjusting positive airway pressure treatment for sleep apnea diagnosed by home sleep testing. J. Clin. Sleep Med. 2014, 10(12), 1269–75. [Google Scholar] [CrossRef]
- Messineo, L.; White, D.P.; Hete, B.; Knepper, M.; Berry, R.; Noah, W.H. Auto-adjusting positive airway pressure: the fine line between engineering and medicine. Sleep Breath. 2025, 29(4), 253. [Google Scholar] [CrossRef]
- Fashanu, O.S.; Quan, S.F. Factors associated with treatment outcomes after use of auto-titrating CPAP therapy in adults with obstructive sleep apnea. Sleep Breath 2023, 27(1), 165–172. [Google Scholar] [CrossRef] [PubMed]
- Aloia, M.S.; Arnedt, J.T.; Stanchina, M.; Millman, R.P. How early in treatment is PAP adherence established? Revisiting night-to-night variability. Behav. Sleep Med. 2007, 5(3), 229–40. [Google Scholar] [CrossRef] [PubMed]
- Rotenberg, B.W.; Murariu, D.; Pang, K.P. Trends in CPAP adherence over twenty years of data collection: a flattened curve. J. Otolaryngol. Head. Neck Surg. 2016, 45(1), 43. [Google Scholar] [CrossRef]
- Sawyer, A.M.; Deatrick, J.A.; Kuna, S.T.; Weaver, T.E. Differences in perceptions of the diagnosis and treatment of obstructive sleep apnea and continuous positive airway pressure therapy among adherers and nonadherers. Qual. Health Res. 2010, 20(7), 873–92. [Google Scholar] [CrossRef] [PubMed]
- Falcone, V.A.; Damiani, M.F.; Quaranta, V.N.; Capozzolo, A.; Resta, O. Polysomnograph chart view by patients: a new educational strategy to improve CPAP adherence in sleep apnea therapy. Respir. Care 2014, 59(2), 193–8. [Google Scholar] [CrossRef]
- Duval, J.; Texereau, J.; Bailly, S.; Pépin, J.L. Impact of an early follow-up visit on adherence and adherence trajectories after initiation of continuous positive airway pressure therapy for obstructive sleep apnea. Pulmonology 2026, 32(1), 2641311. [Google Scholar] [CrossRef]
- Patil, S.P.; Ayappa, I.A.; Caples, S.M.; Kimoff, R.J.; Patel, S.R.; Harrod, C.G. Treatment of Adult Obstructive Sleep Apnea with Positive Airway Pressure: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2019, 15(2), 335–343. [Google Scholar] [CrossRef]
- Ahonen, H.; Broström, A.; Fransson, E.I.; Neher, M.; Lindmark, U. The terrible dryness woke me up, I had some trouble breathing"-Critical situations related to oral health as described by CPAP-treated persons with obstructive sleep apnea. J. Sleep Res. 2022, 31(6), e13670. [Google Scholar] [CrossRef]
- Ulander, M.; Johansson, M.S.; Ewaldh, A.E.; Svanborg, E.; Broström, A. Side effects to continuous positive airway pressure treatment for obstructive sleep apnoea: changes over time and association to adherence. Sleep Breath 2014, 18(4), 799–807. [Google Scholar] [CrossRef]
- Bachour, A.; Avellan-Hietanen, H.; Palotie, T.; Virkkula, P. Practical Aspects of Interface Application in CPAP Treatment. Can. Respir. J. 2019, 2019, 7215258. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Su, Y.; Hu, S.; Ma, J.; Zhang, Z.; Fang, F.; Guan, J. Effects of telemedicine interventions in improving continuous positive airway pressure adherence in patients with obstructive sleep apnoea: a meta-analysis of randomised controlled trials. Sleep Breath 2021, 25(4), 1761–1771. [Google Scholar] [CrossRef]
- Richards, D.; Bartlett, D.J.; Wong, K.; Malouff, J.; Grunstein, R.R. Increased adherence to CPAP with a group cognitive behavioral treatment intervention: a randomized trial. Sleep 2007, 30(5), 635–40. [Google Scholar] [CrossRef] [PubMed]
- Drakou, T.; Steiropoulos, P.; Saroglou, M.; et al. The presence of insomnia and depression contributes to the acceptance of an initial treatment trial of continuous positive airway pressure therapy in patients with obstructive sleep apnea. Sleep Breath 2021, 25(4), 1803–1812. [Google Scholar] [CrossRef]
- Morrone, E.; Braghiroli, A.; D'Artavilla Lupo, N.; et al. Anxiety and depressive symptoms on continuous positive airway pressure: long-term adherence in patients with sleep apnea syndrome. Minerva Med. 2022, 113(6), 967–973. [Google Scholar] [CrossRef] [PubMed]
- Mwenge, G.B.; Rougui, I.; Rodenstein, D. Effect of changes in periodic limb movements under cpap on adherence and long term compliance in obstructive sleep apnea. Acta Clin. Belg. 2018, 73(3), 191–198. [Google Scholar] [CrossRef]
- Jeppesen, K.; Kørvel-Hanquist, A.; Wolff, D.L.; et al. Patterns and stability of long-term adherence in continuous positive airway pressure therapy for obstructive sleep apnea: a cohort study. Sleep Breath 2025, 29(4), 243. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



