Submitted:
05 May 2026
Posted:
06 May 2026
You are already at the latest version
Abstract
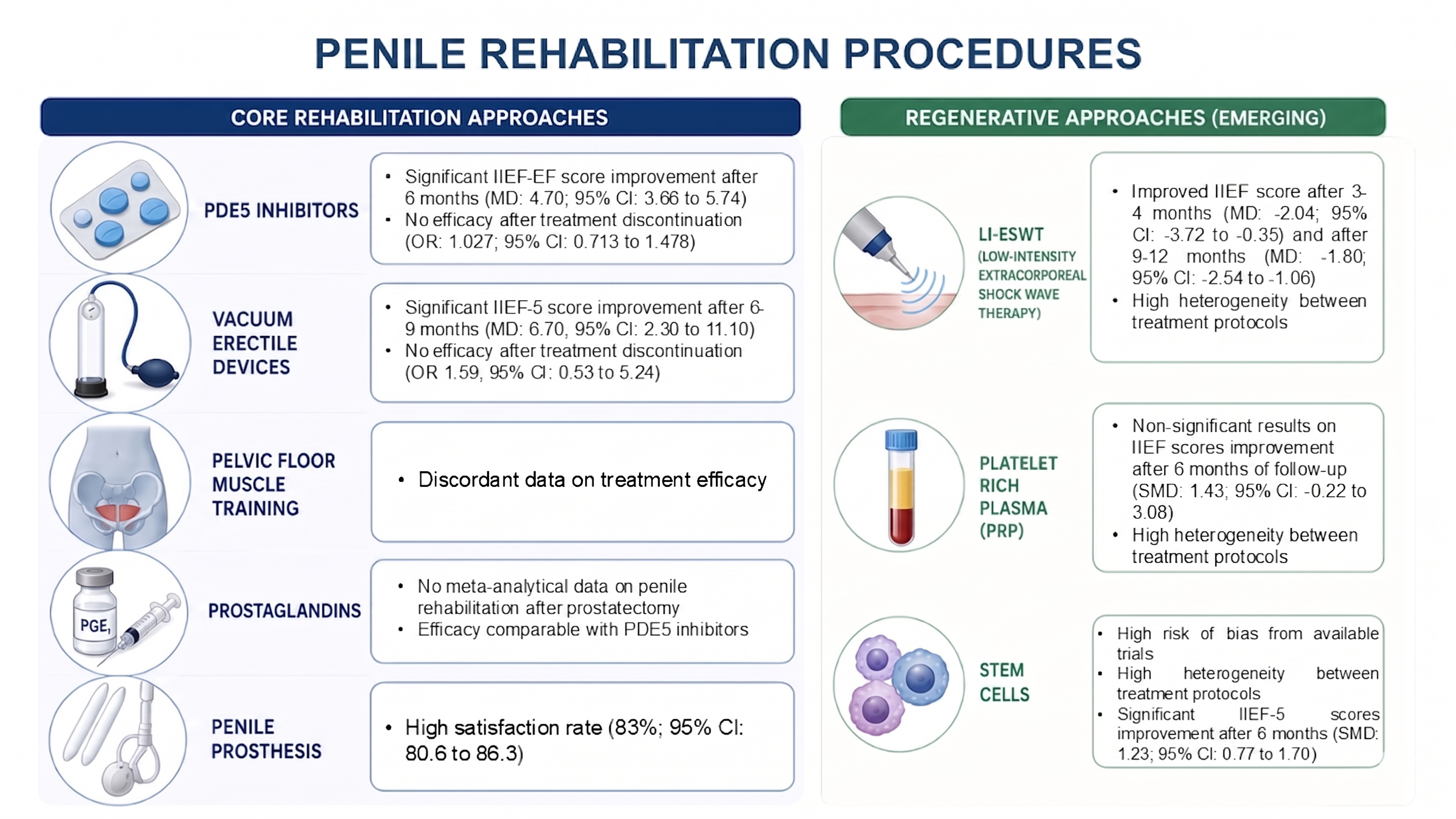
Background/Objectives: Penile rehabilitation (PR) techniques are claimed to counteract chronic degenerative processes of cavernous tissue such as penile hypoxia, neurovascular damage, and cavernous fibrosis. The objective of this umbrella review is to synthesize findings from existing meta-analyses to evaluate the efficacy of traditional and emerging PR strategies, providing an evidence-based roadmap for clinical management after surgery for prostate cancer. Methods: Conducted in accordance with PRIOR guidelines, a comprehensive literature search of PubMed, The Cochrane Library, and Scopus was performed through April 2026. The review included primarily systematic reviews and meta-analyses investigating pharmacological, physical, surgical, and regenerative interventions for post-prostatectomy erectile dysfunction (ED). Methodological quality was independently assessed using standardized tools. Results: PDE5 inhibitors (PDE5-is) significantly improve erectile function during active treatment, yet evidence supporting their role in promoting spontaneous, "unassisted" recovery remains limited. Vacuum erectile devices demonstrate high efficacy for assisted intercourse but show minimal impact on returning to baseline function compared to placebo. Penile prosthesis (PP) implantation maintains robust efficacy with exceptionally high satisfaction rates (83–85%), proving independent of prior pelvic surgery. Although early-phase trials suggest clinical potential for regenerative therapies like low-intensity extracorporeal shockwave therapy, platelet-rich plasma, and stem cell interventions, the evidence is currently undermined by substantial heterogeneity in study protocols and concerns regarding methodological quality. Conclusions: PR following radical prostatectomy remains a complex challenge characterized by poor evidence. While PDE5-Is are established first-line therapy for assisted function, PP remains the most reliable definitive treatment for refractory ED cases. Regenerative approaches show promise but remain investigational until standardized protocols and large-scale trials are established.
Keywords:
radical prostatectomy
; erectile dysfunction
; penile rehabilitation
; PDE5 inhibitors
; vacuum erectile device
; penile prosthesis
; platelet‐rich plasma
; low intensity extracorporeal shockwave therapy
; regenerative medicine
1. Introduction
Prostate cancer continues to represent a formidable global health challenge, ranking as the second most common malignancy and the fifth leading cause of cancer-related mortality among men worldwide [1]. With the continued refinement of screening programs and the aging global population, the volume of definitive treatments—specifically radical prostatectomy (RP)—has reached unprecedented levels [2]. Despite the widespread adoption of minimally invasive technologies, most notably robot-assisted radical prostatectomy (RARP), and the meticulous anatomical descriptions of the neurovascular bundles, post-surgical functional outcomes remain a critical concern [3]. While oncological control and urinary continence have seen significant improvements, the preservation and recovery of erectile function (EF) remain the most elusive goals in prostate cancer surgery [4].
The burden of iatrogenic erectile dysfunction (ED) extends far beyond the loss of penetrative capacity; it permeates the psychological, social, and relational fabric of the patient’s life [5]. For many men, the sudden loss of EF is perceived as a “de-masculinizing” event, frequently leading to profound shifts in masculine identity, decreased self-esteem, and a heightened risk of clinical depression and anxiety [5]. Furthermore, sexual dysfunction often causes significant distress for the partner and a withdrawal from intimacy, which can destabilize long-term relationships during an already stressful period of cancer survivorship [5]. This psychosocial burden is compounded by the chronic nature of the condition, as the failure to achieve early recovery can lead to “sexual abandonment,” where patients and couples cease all sexual activity, further complicating later rehabilitative efforts [5].
From a pathophysiological perspective, the rationale for intervention is rooted in the prevention of irreversible structural changes. The trauma to the cavernous nerves, whether through direct injury, traction, or thermal damage, induces a state of chronic penile hypoxia and overexpression of pro-fibrotic growth factors [6]. This oxygen deprivation triggers the pro-fibrotic cascade, characterized by the apoptosis of cavernous smooth muscle cells and the subsequent deposition of collagen within the corpora cavernosa [6]. This remodeling leads to venous leak (corporeal veno-occlusive dysfunction), often rendering the erectile tissue refractory to conventional pharmacological therapies if left untreated [7].
The concept of “penile rehabilitation” (PR) was introduced to counteract this degenerative process, shifting the clinical paradigm from a reactive, “wait-and-see” approach to a proactive, multi-modal strategy aimed at preserving tissue integrity during the window of nerve recovery [8]. Over the past two decades, the therapeutic armamentarium has expanded from the foundational use of phosphodiesterase type 5 inhibitors (PDE5i) and vacuum erectile devices (VED) to advanced intracavernosal therapies and, more recently, to the frontiers of regenerative medicine, including low-intensity extracorporeal shockwave therapy (Li-ESWT) and stem cell (SC)-based interventions [9].
However, the rapid proliferation of PR protocols has not been matched by a consensus on the most effective strategy. The existing literature is characterized by a high volume of primary studies and systematic reviews with often discordant findings, heterogeneous outcome measures, and varying levels of methodological rigor. This fragmentation of evidence poses a significant challenge for clinicians in providing evidence-based counseling. Consequently, there is an urgent need for a high-level synthesis to distill the current state of the art. This umbrella review aims to evaluate the quality and findings of existing studies—prioritizing meta-analytical findings—to provide a comprehensive, expert-level roadmap for the management of post-prostatectomy ED.
2. Materials and Methods
This umbrella review was conducted in accordance with the Preferred Reporting Items for Overviews of Reviews (PRIOR) guidelines [10]. The review protocol was registered on the PROSPERO database (registration number: CRD420261372308).
The study was designed according to the Population, Intervention, Comparison, Outcome (PICO) model [11]. The included Population considered men affected with iatrogenic ED following any type of prostatectomy, the Intervention investigated were all medical, physical and surgical therapies for ED, while the Comparison included either no intervention or a placebo or other treatments. Primary and secondary outcomes were differently chosen and ranked based on clinical relevance.
A comprehensive literature review was conducted in April 2026. The search strategy included the following keywords: ‘prostatectomy’, ‘radical prostatectomy’, ‘robotic-assisted radical prostatectomy’, ‘RARP’, ‘nerve-sparing prostatectomy’, ‘prostate cancer’, ‘PCa’, ‘iatrogenic erectile dysfunction’, ‘penile rehabilitation’, ‘erectile function recovery’, ‘sexual health recovery’, ‘PDE5 inhibitors’, ‘PDE5i’, ‘phosphodiesterase type 5 inhibitors’, ‘sildenafil’, ‘tadalafil’, ‘vardenafil’, ‘avanafil’, ‘intracavernosal injections’, ‘ICI’, ‘alprostadil’, ‘combination therapy’, ‘vacuum erectile device’, ‘VED’, ‘penile prosthesis’, ‘penile implant’, ‘inflatable penile prosthesis’, ‘IPP’, ‘low-intensity extracorporeal shockwave therapy’, ‘Li-ESWT’, ‘shockwave therapy’, ‘platelet-rich plasma’, ‘PRP’, ‘stem cell therapy’ and ‘regenerative medicine’ in PubMed, The Cochrane Library and Scopus. In addition to database searches, the reference lists of all included studies and relevant previous reviews were manually screened to identify further pertinent articles. The search was updated before the final analysis to ensure the inclusion of the most recent evidence.
Study eligibility included human subjects, English language publication, and no limitations on publication date. Systematic reviews of randomized controlled trials (RCTs) with meta-analyses individual or cumulative data were electively reported. Systematic reviews with meta-analyses of prospective non-randomized or cohort studies or without data synthesis (including only qualitative analysis) that used systematic, structured and reproducible methods to collect data from primary research were also analyzed when systematic reviews of RCTs with meta-analyses were not intercepted. The most recent and highest quality thematic review was chosen if multiple systematic reviews evaluated the same intervention. In the absence of meta-analytical data, primary research was included according to a hierarchy of evidence, prioritizing RCTs, followed by non-RCTs, and cohort studies. Furthermore, such primary studies were included even if they had not been captured by recent existing meta-analyses. If multiple systematic reviews evaluated the same intervention, the most recent and highest quality thematic review was chosen. Duplicative systematic reviews were only included if they were comparable in quality and published in the same year or presented any clear conclusion.
The literature searches, data extraction, and tabulation were carried out independently by three reviewers (G.S., L.M., and M.L.) and verified by two independent reviewers (G.A. and A.A.). The quality of the studies was assessed using the Methodological Quality of Systematic Reviews 2 (AMSTAR-2, http://www.amstar.ca) [12] for systematic reviews, Revised tool for Risk of Bias (rRoB 2, https://www.riskofbias.info/welcome/rob-2-0-tool) [13] for RCTs, Risk Of Bias in Non-randomized Studies—of Intervention (ROBINS-I) [14] for prospective non-randomized studies, and the Newcastle-Ottawa Scale (http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp) [15] for observational/cohort studies. Three reviewers (G.S., L.M. and M.L.) independently assessed the methodological quality of all included studies.
A qualitative synthesis was performed using aggregate data as reported in the original publications.
3. Results
Three relevant scientific areas were identified regarding PR treatments: 1. Conventional medical therapy; 2. Surgical therapy; 3. Regenerative therapy.
3.1. Conventional Medical Therapy
3.1.1. PDE5-is
The efficacy of PDE5-is in PR following RP has been extensively evaluated across several meta-analyses, yielding the following core findings.
The most recent meta-analysis of 39 RCTs found that PDE5-is are significantly superior to placebo in improving EF during the treatment period, as measured by the International Index of Erectile Function-Erectile Function (IIEF-EF) domain scores [16]. In particular, compared with the placebo group, patients in regular PDE5-i group (mean difference (MD): 3.07; 95% confidence interval (CI): 1.69 to 4.44; p < 0.0001; I2: 96%) and on demand group (MD: 3.92; 95% CI: 2.95 to 4.88; p < 0.00001; I2: 99%) had a significantly higher mean IIEF-EF scores within 3 months after RP [16]. These results were even more significant in patients undergoing regular PDE5-i therapy for more than 6 months after RP (MD: 4.70; 95% CI: 3.66 to 5.74; p < 0.00001; I2: 0%) [16]. As for the proportion of IIEF-EF ≥ 22, patients in regular group and on demand PDE5-i group had significantly higher proportion than those in placebo group 6 months after RP, and the odds ratios (OR)s were 1.87 (95% CI: 1.32 to 2.66; p = 0.0005; I2: 11%) and 2.17 (95% CI: 1.20 to 3.93; p = 0.01; I2: 51%), respectively [16].
The debate regarding the optimal administration protocol—regular daily or nightly versus on demand—is a central focus. No significant difference was observed between daily and on demand PDE5-i groups regardless of mean IIEF-EF score (p = 0.75) or the proportion of IIEF-EF ≥ 22 (p = 0.61) in the long term [16].
Moreover, a critical distinction remains between “assisted” and “unassisted” recovery. In a meta-analysis of 4 RCTs, when the data after PDE5-i washout were analyzed, the result showed that PDE5-i did not improve spontaneous EF (OR: 1.027; 95% CI: 0.713 to 1.478; p = 0.610; I2: 48.4%) [17]. The Cochrane Review (2018) emphasizes that there is no high-certainty evidence demonstrating that scheduled (nightly or daily) use leads to superior long-term recovery of unassisted (spontaneous) EF [18]. In particular, treatment discontinuation was not significantly different after at least 6 months of daily PDE5-i therapy compared with placebo [relative risk (RR): 1.12; 95% CI: 0.85 to 1.48; p = 0.41] or on demand therapy (RR: 1.09; 95% CI: 0.86 to 1.38; p = 0.98; I2: 0%) [18]. Otherwise, in a network meta-analysis of 22 RCTs involving 2711 patients which compared different interventions for PR after nerve sparing RP, only the daily dose of sildenafil 100 mg reached statistical significance for unassisted EF recovery (OR 4.00; 95% CI 1.40 to 13.4) [19].
Furthermore, early initiation of therapy post-RP is generally advocated to prevent cavernous fibrosis and structural changes. A prospective RCT demonstrated that immediate initiation of sildenafil after RARP significantly improved EF recovery at 12 months compared to delayed treatment [41.4% vs. 17.7%; hazard ratio (HR): 2.943; p = 0.034] [20]. However, the “curative” potential of early intervention remains under scrutiny due to the low to very low certainty of long-term evidence in high-quality RCTs [18].
PDE5-i are globally recognized as safe and well-tolerated in the post-prostatectomy population. The most common adverse events identified across meta-analyses include headache [Peto odds ratio (POR): 2.99; 95% CI: 2.22 to 4.04; p < 0.00001; I2: 0%], dyspepsia (POR 3.15; 95% CI: 1.86 to 5.35; p < 0.0001; I2: 0%), flushing (POR 4.71; 95% CI: 3.19 to 6.95; p < 0.00001; I2: 0%), and nasal congestion (POR 2.66; 95% CI: 1.85 to 3.84; p < 0.00001; I2: 0%) [21]. In the short term, the risk of serious adverse events (defined according to National Cancer Institute Common Terminology Criteria for Adverse Events reporting [22]; grades 3 to 5) were rare but higher in patients undergoing on demand therapy compared to placebo (RR: 0.32; 95% CI 0.11 to 0.94; p = 0.04; I2: 0%) [18]. No differences were found between the risk of serious adverse events comparing on demand and daily PDE5-i therapy in the short term (RR: 0.69; 95% CI: 0.12 to 4.04; p = 0.68) and long term (RR: 3; 95% CI: 0.13 to 71.92) [18].
A summary of the main quantitative findings on PDE5-i therapy for PR has been summarised in Table 1.
3.1.2. VEDs
The efficacy of VEDs in PR following RP has been evaluated across several systematic reviews and meta-analyses.
The most recent meta-analysis of RCTs found that International Index of Erectile Function—5 items (IIEF-5) scores were significantly higher in the VED group compared to controls at 3 months (MD: 9.70; 95% CI: 5.16 to 14.24; p < 0.0001) and 6-9 months after RP (MD: 6.70, 95% CI: 2.30 to 11.10; p = 0.003; I2: 72%) [16]. A recent meta-analysis of two RCTs reported a VED efficacy rate of 84.5% (95% CI: 73-96%) for successful intercourse or intercourse satisfaction specifically in post-RP patients [23].
Otherwhise, the network meta-analysis by Sari Motlagh et al. (2021), which analyzed 22 RCTs, did not identify VED among the interventions with significantly higher likelihood of EF recovery (i.e., the proportion of patients who experienced a return to the baseline EF at the end of washout) compared to placebo (OR 1.59, 95% CI 0.53 to 5.24) [19]. This suggests that while VED is effective for assisted sexual activity, its role as a standalone rehabilitation strategy for spontaneous EF recovery may be limited.
Notably, a systematic review of seven RCTs, five prospective and four retrospective observational studies, identified considerable heterogeneity in VED protocols across studies [24]. Among 16 included studies, 7 used daily VED protocols, while rehabilitation duration varied: less than 1 year in 4 studies, up to 12 months in 6 studies, and more than 1 year in 6 studies [24].
VEDs are generally well-tolerated with transient and non-serious adverse events. The meta-analysis by Zhang et al. reported that the most common side effect was penile bruising, with a pooled incidence of 25.3% (95% CI: 0.18 to 0.30), however no subanalysis was made in relation to VED use for PR after RP [23].
3.1.3. Prostaglandins
Evidence about prostaglandin use for PR is limited. The efficacy of intracavernosal alprostadil injection for PR was evaluated in a single RCT involving 30 patients with preoperative good erections after nerve sparing RP [25]. In particular, patients randomized to alprostadil injections three times per week (for 12 weeks), noted 67% recovery of spontaneous erection after the 6-months follow-up (in comparison with 20% in the observation group, p < 0.01) [25].
The Cochrane Review (2018) included a direct comparison of daily PDE5-is versus daily intraurethral prostaglandin E1 for PR [18]. Based on very low quality evidence derived from a single RCT [26], efficacy was comparable between the two regimens, with no significant difference in EF recovery (RR: 1.1; 95% CI: 0.79 to 1.52; p = 0.59) [18].
However, the most recent high-quality systematic reviews with meta-analysis, found no eligible trials comparing scheduled intracavernosal alprostadil injections versus on-demand use for PR, representing a significant gap in the evidence base [16,18].
No quantitative analysis was found concerning adverse effects of prostaglandins in the context of PR. A recent systematic review and meta-analysis, which included 12 studies (5 RCTs and 7 non-RCTs), compared adverse effects of intracavernosal injection therapy using isolated and combined substances [27]. Priapism showed a minimal presence in the isolated alprostadil group (OR: 1.84, 95% CI: 1.03 to 3.20, p = 0.04); however, when analyzing only RCTs, there was no significant difference between groups [27]. Fibrosis rates ranged from 0.8% to 15% across studies [27].
3.1.4. Pelvic Floor Muscle Training (PFMT)
PFMT is proposed as a physiotherapy intervention for improving EF after RP. While pooled data from three RCTs involving 126 patients indicated no significant improvement in favor of PFMT compared to control group at 3–6 months postoperatively (OR: 2.37; 95% CI: 0.79 to 7.07; p = 0.12; I2: 0%) [16], a recent network meta-analysis of 22 RCTs found a significant higher likelihood of EF recovery with PFMT (OR: 5.21; 95% CI: 1.24 to 2.98), but with low certainty of evidence due to risk of bias assessment and small sample size (n = 51) of two RCTs [19].
3.2. Surgical Therapy
Penile prosthesis (PP) is not properly considered a PR strategy, since it does not aim to rehabilitate penile function. However, when patients with post-RP ED fail to achieve adequate recovery through conventional medical interventions, surgical intervention becomes the definitive treatment strategy. Consequently, PP implantation is recommended as the third-line therapy for patients who are refractory to or have contraindications for non-invasive therapies. Our search yielded no results regarding systematic reviews with meta-analyses specifically dedicated to the use of PP in treating patients following prostate surgery. However, as this treatment is symptomatic and independent of the underlying cause of ED, efficacy outcomes from the general ED population can be generalized and considered comparable to the subcategory of iatrogenic post-prostatectomy ED.
The most recent and comprehensive meta-analysis, incorporating 83 studies (32 prospective and 51 retrospective) and 12,132 subjects with a mean follow-up of 47.6 months, demonstrated an exceptionally high overall patient satisfaction rate of 83% (95% CI: 80.6 to 86.3) following PP implantation [28]. When comparing device types, satisfaction rates were significantly higher for inflatable penile prostheses (IPP) (85.4%; 95% CI: 81.1 to 88.8) compared to malleable (72.4%; 95% CI: 63.2 to 80) or semi-rigid (84.5%; 95% CI: 81.1 to 87.3) devices, with three-piece IPPs yielding the highest levels of patient satisfaction [28]. More specifically, PP implantation significantly improved the combination of IIEF-5 and IIEF-EF score (SMD: 5.73; 95% CI: 4.51 to 6.95), after pooling data from 14 studies involving 1,263 patients [28]. Interestingly, meta-regression analyses indicated that patient satisfaction is independent to the presence of pelvic surgery (as RP) or trauma (S: 0.003; 95% CI: -0.001 to 0.009; p = 0.102) [28].
From a safety perspective, long-term complications associated with PP implantation are limited [28]. The mean incidence of mechanical failure is reported at approximately 4.6%, while device erosion occurs in roughly 3% of cases [28]. Post-operative infection rates remain low, ranging between 2.9% and 4.5%; however, the occurrence of infectious complications is tightly correlated with the presence of diabetes mellitus [28].
3.3. Regenerative Therapy
3.3.1. Li-ESWT
Li-ESWT has recently been considered as a treatment for ED, and more specifically for PR after prostate surgery. A meta-analysis was intercepted specifically evaluating Li-ESWT efficacy for PR [29]. Li-ESWT significantly improved International Index of Erectile Function (IIEF) score after 3-4 months in the pooled analysis of three RCTs (n = 200) (MD: -2.04; 95% CI: -3.72 to -0.35; p = 0.02) and after 9-12 months in a single RCT (n = 85) (MD: -1.80; 95% CI: -2.54 to -1.06; p < 0.00001) [29]. However, heterogeneity between studies was high (73%) due to consistently different treatment protocols [29]. In particular, higher energy flux density ranged from 0.09 to 0.15 mJ/mm2, total pulses for each treatment ranged from 1500 to 4000 and pulses for each region from 300 to 600 [29].
A recent systematic review with meta-analysis compared the benefit of Li-ESWT -PDE5-i association with monotherapy for EF [30]. In the subanalysis related to treatment of EF caused by RP (2 RCTs, n = 109), IIEF-5 score improvement was not significantly different when comparing Li-ESWT and PDE5-i association with PDE5-i or prostaglandin monotherapy [standard mean difference (SMD): 0.26; 95% CI: -1.12 to 1.65; p < 0.01; I2: 91%] [30].
No meta-analytic findings were intercepted concerning adverse events of Li-ESWT after RP. However, the most recent high-quality meta-analysis on Li-ESWT therapy for ED found no treatment-related adverse events in the short term when pooling data from 20 RCTs (n = 1400) [risk difference (RD): 0.0; 95% CI: -0.01 to 0.02; p = 0.73; I2: 0%] [31].
3.3.2. Platelet-Rich Plasma (PRP)
Our search did not identify any meta-analysis or individual RCTs regarding the use of PRP for ED following prostate surgery, reflecting the limited evidence available for this still-emerging methodology. The most recent high-quality meta-analysis on PRP monotherapy of mild-to-moderate ED of any causes intercepted six RCTs (n = 441) comparing this intervention versus placebo [32]. Interestingly, statistically non-significant results on IIEF scores improvement were found when pooling data at 1 month (SMD: 1.06; 95% CI: -0.38 to 2.50; I2: 85%), 3 months (SMD: 1.01; 95% CI: -0.40 to 2.42; I2: 84%) and 6 months of follow-up (SMD: 1.43; 95% CI: -0.22 to 3.08; I2: 89%) [32]. The high heterogeneity across studies reflected the different treatment protocols applied across studies (i.e., PRP injection volumes ranged from 5 to 10 mL in 2-4 sessions) [32]. Adverse events were infrequently reported and only one study described single cases of hematoma or plaque formation [32].
A different meta-analysis evaluated the efficacy of PRP in combination with Li-ESWT [33]. The pooled analysis of 7 RCTs comparing PRP alone or in association with Li-ESWT vs. placebo or Li-ESWT monotherapy showed a significant improvement in IIEF score in experimental group only after 24 weeks of follow-up (MD 2.46; 95% CI: 1.10 to 3.83; p = 0.0004; I2: 86%) [33]. Otherwise, peak systolic velocity (PSV) was significantly augmented after 4 weeks (1 RCT, n = 100) (MD: 14.50; 95% CI: 12.46 to 16.54; p < 0.00001), 12 weeks (1 RCT, n = 113) (MD: 8.40; 95% CI: 4.96 to 11.84; p < 0.00001) and 24 weeks (2 RCTs, n = 213) (MD: 13.75; 95% CI: 11.57 to 15.93; p < 0.00001; I2: 32%) [33]. Moreover, after pooling data from three RCTs (n = 357), the association between PRP and Li-ESWT significantly improved IIEF score at 24 weeks of follow-up compared to Li-ESWT monotherapy (MD: 2.57; 95% CI: 1.34 to 3.80; p < 0.0001; I2: 66%) [33].
3.3.3. Stem Cells (SCs)
Among the most recent therapies proposed for regenerative purposes to repair nerve damage following RP is the use of intracavernous SCs of various origins. No systematic reviews with meta-analyses focusing specifically on this patient population were found in the literature. The most recent meta-analysis on the use of SCs for ED in men aggregates several clinical trials (RCTs or uncontrolled trials) involving patients with ED from various causes, including post-RP cases [34]. The results of the pooled data indicate a significant increase of PSV after three months (SMD: 0.63; 95% CI: 0.28 to 0.98; p < 0.0001; I2: 46.31%) and sixth-months (SMD: 1.2; 95% CI: 0.23 to 2.19; p = 0.015; I2: 71.24) [34]. Two studies evaluated significant post-therapy IIEF-5 scores improvement at three months (SMD: 1.05; 95% CI: 0.61 to 1.49; p < 0.0001; I2: 50.16%) and sixth months (SMD: 1.23; 95% CI: 0.77 to 1.70; p < 0.0001; I2: 51.59%) [34]. Otherwise, the pooled analysis from two studies did not find statistically significant differences in IIEF score three months after SCs therapy (SMD: −0.11; 95% CI: –0.58 to 0.36; p = 0.647; I2 < 0.0001), while a little improvement was found at six months (SMD: 0.64; 95% CI: 0.13 to 1.15; p = 0.014; I2 < 0.0001) [34]. Finally, two studies evaluated the baseline and post-therapy sixth-month IIEF-EF scores, indicating a significant improvement in this outcome (SMD: 1.57; 95% CI: 0.98 to 2.16; p < 0.0001; I2 < 0.0001) [34]. Sources of heterogeneity included differences in SCs type (i.e., bone marrow, adipose tissue, Wharton jelly, oral mucosa, dental pulp, placental matrix, umbilical cord blood), administration protocols and patient characteristics (i.e., diabetic, post-RP) [34]. Among the clinical trials discussed in this systematic review, four clinical trials reported no adverse effects related to SCs, while four clinical trials reported minor side effects such as minor discomfort, irritation and minor pain, redness, swelling, local reaction, and itching at the injection site [34].
Two phase I-II trials focused on SCs therapy for PR [35,36]. The first one utilised intracavernous autologous adipose-derived SCs on 17 men (age: 46-69 years), reporting that 8 (47.1%) recovered their erectile function and were able to accomplish sexual intercourse [35]. Post-hoc stratification according to urinary continence status was performed. Interestingly, for the continent group 8 out of 11 men recovered EF (MD: 0.57; 95% CI: 0.38 to 0.85; p = 0.0069), while incontinent men did not regain erectile function (MD: 1; 95% CI: 0.85 to 1.18; p > 0.9999) [35]. The second study implied intracavernous autologous bone marrow mononuclear cells in 6 patients [36]. After 6 months, significant improvements versus baseline were noted in IIEF-intercourse satisfaction (p = 0.033) and IIEF-EF (p = 0.035) domains [36].
3.4. Study Quality Assessment
The methodological quality of all the included studies in the present umbrella review has been included in Table 2.
Regarding systematic reviews, most of which included a meta-analysis, the results reveal a heterogeneous landscape: six studies demonstrated high methodological quality [18,28,30,31,32,33]. Three studies [19,23,24] were judged to be of moderate quality. However, a significant portion of the included reviews [16,17,21,24,29] was found to have critically low quality, indicating potential limitations in the robustness of the evidence reported in these papers.
4. Discussion
The management of ED following RP remains a complex clinical challenge, requiring a shift from reactive treatments to proactive, multi-modal PR strategies. This umbrella review provides a synthesis of the current evidence, evaluating traditional pharmacological and non-pharmacological approaches alongside emerging regenerative therapies to offer a comprehensive roadmap for clinicians. While the therapeutic armamentarium has expanded significantly over the last two decades, our analysis reveals a landscape characterized by varying levels of methodological rigor and a persistent lack of consensus on the most effective protocols.
PDE5-is remain the first-line treatment, showing significant efficacy in improving EF during active treatment [22]. Evidence suggests that long-term regular use (over 6 months) yields more significant IIEF-EF score improvements compared to placebo [22]. However, the strength of evidence regarding “unassisted” or spontaneous recovery is low, with several systematic reviews finding no significant difference in spontaneous EF after a washout period [17]. Furthermore, while early initiation is widely advocated to prevent cavernous fibrosis, its long-term curative potential remains supported by low to very low-certainty evidence.
VEDs demonstrate high efficacy for assisted intercourse, with satisfaction rates reaching approximately 84.5% [23]. However, their role in facilitating spontaneous recovery is questionable, as they do not significantly increase the likelihood of returning to baseline EF compared to placebo [21]. Similarly, evidence for PFMT is conflicting; while network meta-analyses suggest a benefit [21], the small sample sizes and high risk of bias in primary RCTs result in low certainty of evidence [16].
PP implantation represents the definitive third-line therapy for patients refractory to non-invasive treatments. The evidence supporting PP is robust, showing exceptionally high satisfaction rates (83-85%), particularly with three-piece inflatable devices [28]. Notably, meta-regression indicates that patient satisfaction is independent of a history of pelvic surgery like RP, suggesting it is a highly reliable option for this sub-population [28].
Emerging therapies such as Li-ESWT and SC interventions show promise in early-phase trials and meta-analyses. Li-ESWT has been shown to significantly improve IIEF scores at 3-12 months post-prostatectomy [29]. SC therapy also indicates potential for improving PSV and IIEF scores at 6 months [34]. However, these results are tempered by high heterogeneity in treatment protocols and a critical risk of bias in many primary studies [35,36].
PRP currently lacks specific meta-analytic evidence for the post-prostatectomy population, and general ED data shows no significant benefit for PRP monotherapy [32]. The relative lack of robust evidence and the significant heterogeneity observed across clinical studies are the primary factors behind why current guidelines continue to classify this methodology as investigational [37,38,39].
A primary challenge identified in this review is the high heterogeneity observed across studies, particularly regarding VED protocols, Li-ESWT energy flux densities, and the origin and administration of stem cells. Methodological quality is also a concern; while six of the included systematic reviews were of high quality, a significant portion (five reviews) was judged to have critically low quality according to AMSTAR-2. Additionally, many of the primary RCTs and clinical trials in this field exhibit a high or critical risk of bias, which mandates caution when interpreting functional outcomes.
The present review has several strengths. First of all, this review utilizes an “umbrella” approach, distilling findings from multiple meta-analyses to provide the highest level of evidence currently available. Moreover, the study adhered to PRIOR guidelines and utilized standardized tools (AMSTAR-2, RoB 2, ROBINS-I) for objective quality assessment. The literature search was conducted through April 2026, ensuring the inclusion of the most recent clinical developments and meta-analyses.
Nevertheless, we must acknowledge several limitations. Many emerging therapies (PRP, SCs) lack dedicated meta-analyses for the post-prostatectomy sub-group, forcing reliance on broader ED population data. The overall strength of our conclusions is limited by the critically low quality of several underlying systematic reviews and the high risk of bias in available RCTs. Moreover, by limiting eligibility to English-language publications, some relevant international data may have been omitted.
The results of our findings underline that clinicians should adopt a patient-centered, multi-modal approach to penile rehabilitation. PDE5-is remain the standard starting point, but patients should be counseled that these may primarily assist in “assisted” function rather than guaranteed “curative” recovery. For those seeking definitive results, early referral for PP should be considered, given the high satisfaction rates. VEDs and PFMT can be integrated as supportive therapies, though their role in long-term nerve recovery is less certain.
To move the field forward, there is an urgent need for developing consensus-based protocols for Li-ESWT, PRP and SC therapies to reduce heterogeneity. Large-scale, multicenter RCTs with long-term follow-up and standardized “unassisted” recovery measures (e.g., using a washout period) are needed. Moreover, it would be useful to investigate the synergistic effects of combining regenerative therapies (e.g., PRP plus Li-ESWT) specifically within the post-RP population. Furthermore, studies identifying predictive factors of response to individual therapies would be desirable to better guide patients toward the most effective personalized therapeutic strategy (i.e., [40,41]). Finally, research should further address the psychological and relational burden of iatrogenic ED to provide more holistic survivorship care.
5. Conclusions
At present, the clinical management of post-RP ED remains a complex challenge, characterized by an evolving therapeutic landscape that still lacks a unified consensus. While PDE5-Is remain the first-line treatment and penile prostheses may offer an effective definitive solution for refractory-ED patients, intermediate options such as VEDs and PFMT still present conflicting evidence regarding their ability to promote spontaneous functional recovery. Furthermore, although emerging therapies like Li-ESWT and SC interventions show promising potential, their clinical application is currently limited by significant heterogeneity in treatment protocols and variable methodological quality across primary studies. Therefore, it is crucial that future research focuses on harmonizing protocols and strengthening methodological rigor, in order to define proactive, evidence-based therapeutic pathways that can truly improve long-term outcomes for prostate cancer survivors.
Author Contributions
Conceptualization, G.S. and A.A.; methodology, G.S.; formal analysis, G.S., L.M. and M.L.; investigation, G.S., L.M. and M.L.; data curation, G.S.; writing—original draft preparation, G.S., L.M. and M.L.; writing—review and editing, G.A. and A.A.; supervision, A.A.; funding acquisition, A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AMSTAR-2 | Assessing the Methodological Quality of Systematic Reviews 2 |
| CI | Confidence interval |
| ED | Erectile dysfunction |
| EF | Erectile function |
| HR | Hazard ratio |
| IIEF | International Index of Erectile Function |
| IIEF-5 | International Index of Erectile Function—5 items |
| IIEF-EF | International Index of Erectile Function—Erectile Function |
| IPP | Inflatable penile prosthesis |
| Li-ESWT | Low intensity-extracorporeal shock wave therapy |
| MD | Mean difference |
| OR | Odds ratio |
| PDE5-i | Phosphodiesterase type 5-inhibitors |
| PFMT | Pelvic floor muscle training |
| PICO | Population, Intervention, Comparison, Outcome |
| POR | Peto odds ratio |
| PP | Penile prosthesis |
| PR | Penile rehabilitation |
| PRIOR | Preferred Reporting Items for Overviews of Reviews |
| PRP | Platelet-rich plasma |
| PSV | Peak systolic velocity |
| RARP | Robot-assisted radical prostatectomy |
| RCT | Randomized controlled trial |
| ROBINS-I | Risk Of Bias in Non-randomized Studies—of Intervention |
| RP | Radical prostatectomy |
| RR | Relative risk |
| rROB 2 | Revised tool for Risk of Bias |
| SC | Stem cell |
| SMD | Standard mean difference |
| VED | Vacuum erectile device |
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Monda, S.M.; Demus, T.; Jaime-Casas, S.; Meah, S.; Srivastava, A.; Sarle, R.; Labardee, C.; Ghani, K.R.; Ginsburg, K.M.; Morgan, T.M.; Borza, T. Trends in Surgical Overtreatment of Prostate Cancer. JAMA Oncol. 2025, 11, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Nahas, W.C.; Rodrigues, G.J.; Rodrigues Gonçalves, F.A.; Sawczyn, G.V.; Barros, G.G.; Cardili, L.; Guglielmetti, G.B.; Fazoli, A.J.C.; Cordeiro, M.D.; Cassão, V.D.A.; Chade, D.C.; Neves De Oliveira, L.C.; Murta, C.B.; Pontes Júnior, J.; Trindade, E.M.; Bastos, D.A.; Sarkis, A.S.; Mitre, A.I.; Trinh, Q.D.; Coelho, R.F. Perioperative, Oncological, and Functional Outcomes Between Robot-Assisted Laparoscopic Prostatectomy and Open Radical Retropubic Prostatectomy: A Randomized Clinical Trial. J. Urol. 2024, 212, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Di Nauta, M.; Falagario, U.G.; Ricapito, A.; Rubino, M.; Annese, P.; Busetto, G.M.; Cormio, L.; Carrieri, G.; Bettocchi, C. Sexual function recovery following open and robotic radical prostatectomy: results of an academic penile rehabilitation program. Asian J. Androl. 2025, 27, 680–685. [Google Scholar] [CrossRef]
- Nkoana, S.; Sodi, T.; Lentoor, A.; Maepa, M.; Thobejane, K. Psychological Impact of Treatment-Induced Erectile Dysfunction on Masculinity: A Study of a Group of Black Elderly Men Undergoing Prostate Cancer Treatment at a Tertiary Hospital in Limpopo Province, South Africa. Int. J. Environ. Res. Public Heal. 2026, 23, 110. [Google Scholar] [CrossRef] [PubMed]
- Aversa, A.; Basciani, S.; Visca, P.; Arizzi, M.; Gnessi, L.; Frajese, G.; Fabbri, A. Platelet-derived growth factor (PDGF) and PDGF receptors in rat corpus cavernosum: changes in expression after transient in vivo hypoxia. J. Endocrinol. 2001, 170, 395–402. [Google Scholar] [CrossRef]
- Song, G.; Hu, P.; Song, J.; Liu, J.; Ruan, Y. Molecular pathogenesis and treatment of cavernous nerve injury-induced erectile dysfunction: A narrative review. Front. Physiol. 2022, 13, 1029650. [Google Scholar] [CrossRef]
- Chung, E.; Brock, G. Sexual rehabilitation and cancer survivorship: a state of art review of current literature and management strategies in male sexual dysfunction among prostate cancer survivors. J. Sex. Med. 2013, 10 Suppl 1, 102–11. [Google Scholar] [CrossRef]
- Bock, M.; Burns, R.T.; Pereira, T.A.; Bernie, H.L. A contemporary review of the treatments and challenges associated with penile rehabilitation after radical prostatectomy including a proposed optimal approach. Int. J. Impot. Res. 2024, 36, 480–485. [Google Scholar] [CrossRef]
- Gates, M.; Gates, A.; Pieper, D.; Fernandes, R.M.; Tricco, A.C.; Moher, D.; Brennan, S.E.; Li, T.; Pollock, M.; Lunny, C.; Sepúlveda, D.; McKenzie, J.E.; Scott, S.D.; Robinson, K.A.; Matthias, K.; Bougioukas, K.I.; Fusar-Poli, P.; Whiting, P.; Moss, S.J.; Hartling, L. Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ. 2022, 378, e070849. [Google Scholar] [CrossRef]
- Frandsen, T.F.; Bruun Nielsen, M.F.; Lindhardt, C.L.; Eriksen, M.B. Using the full PICO model as a search tool for systematic reviews resulted in lower recall for some PICO elements. J. Clin. Epidemiol. 2020, 127, 69–75. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; Henry, D.A. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; Emberson, J.R.; Hernán, M.A.; Hopewell, S.; Hróbjartsson, A.; Junqueira, D.R.; Jüni, P.; Kirkham, J.J.; Lasserson, T.; Li, T.; McAleenan, A.; Reeves, B.C.; Shepperd, S.; Shrier, I.; Stewart, L.A.; Tilling, K.; White, I.R.; Whiting, P.F.; Higgins, J.P.T. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; Carpenter, J.R.; Chan, A.W.; Churchill, R.; Deeks, J.J.; Hróbjartsson, A.; Kirkham, J.; Jüni, P.; Loke, Y.K.; Pigott, T.D.; Ramsay, C.R.; Regidor, D.; Rothstein, H.R.; Sandhu, L.; Santaguida, P.L.; Schünemann, H.J.; Shea, B.; Shrier, I.; Tugwell, P.; Turner, L.; Valentine, J.C.; Waddington, H.; Waters, E.; Wells, G.A.; Whiting, P.F.; Higgins, J.P. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Wells, G. A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp#:~:text=It%20was%20developed%20to%20assess%20the%20quality%20of,quality%20assessments%20in%20the%20interpretation%20of%20meta-analytic%20results (accessed on 1 May 2026).
- Feng, D.; Tang, C.; Liu, S.; Yang, Y.; Han, P.; Wei, W. Current management strategy of treating patients with erectile dysfunction after radical prostatectomy: a systematic review and meta-analysis. Int. J. Impot. Res. 2022, 34, 18–36. [Google Scholar] [CrossRef]
- Liu, C.; Lopez, D.S.; Chen, M.; Wang, R. Penile Rehabilitation Therapy Following Radical Prostatectomy: A Meta-Analysis. J. Sex. Med. 2017, 14, 1496–1503. [Google Scholar] [CrossRef]
- Philippou, Y.A.; Jung, J.H.; Steggall, M.J.; O’Driscoll, S.T.; Bakker, C.J.; Bodie, J.A.; Dahm, P. Penile Rehabilitation for Postprostatectomy Erectile Dysfunction. Cochrane Database Syst. Rev. 2018, 10, CD012414. [Google Scholar] [CrossRef] [PubMed]
- Sari Motlagh, R.; Abufaraj, M.; Yang, L.; Mori, K.; Pradere, B.; Laukhtina, E.; Mostafaei, H.; Schuettfort, V.M.; Quhal, F.; Montorsi, F.; Amjadi, M.; Gratzke, C.; Shariat, S.F. Penile Rehabilitation Strategy After Nerve Sparing Radical Prostatectomy: A Systematic Review and Network Meta-Analysis of Randomized Trials. J. Urol. 2021, 205, 1018–1030. [Google Scholar] [CrossRef]
- Jo, J.K.; Jeong, S.J.; Oh, J.J.; Lee, S.W.; Lee, S.; Hong, S.K.; Byun, S.S.; Lee, S.E. Effect of Starting Penile Rehabilitation With Sildenafil Immediately After Robot-Assisted Laparoscopic Radical Prostatectomy on Erectile Function Recovery: A Prospective Randomized Trial. J. Urol. 2018, 199, 1600–1606. [Google Scholar] [CrossRef]
- Wang, X.; Wang, X.; Liu, T.; He, Q.; Wang, Y.; Zhang, X. Systematic Review and Meta-Analysis of the Use of Phosphodiesterase Type 5 Inhibitors for Treatment of Erectile Dysfunction Following Bilateral Nerve-Sparing Radical Prostatectomy. PLoS One. 2014, 9, e91327. [Google Scholar] [CrossRef]
- National Cancer Institute. Common toxicity criteria. Available online: https://dctd.cancer.gov/research/ctep-trials/for-sites/adverse-events/ctcae-v6.pdf (accessed on 1 May 2026).
- Zhang, F.; Luo, Z.; Xue, Q.; Guo, X.; Zhang, W.; Xiong, Y.; Okoli, U.A.; Zhang, G.; Jiao, Y. Efficacy of vacuum erectile device in refractory erectile dysfunction: a systematic review and meta-analysis. Int. J. Impot. Res. 2026, 38, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Pirola, G.M.; Naselli, A.; Maggi, M.; Gubbiotti, M.; Rubilotta, E.; Jeremy Yuen-Chun, T.; Guarneri, A.; Gauhar, V.; Castellani, D. Vacuum erection device for erectile function rehabilitation after radical prostatectomy: which is the correct schedule? Results from a systematic, scoping review. Int. J. Impot. Res. 2024, 36, 194–200. [Google Scholar] [CrossRef]
- Montorsi, F.; Guazzoni, G.; Strambi, L.F.; Da Pozzo, L.F.; Nava, L.; Barbieri, L.; Rigatti, P.; Pizzini, G.; Miani, A. Recovery of spontaneous erectile function after nerve-sparing radical retropubic prostatectomy with and without early intracavernous injections of alprostadil: results of a prospective, randomized trial. J. Urol. 1997, 158, 1408–10. [Google Scholar] [CrossRef]
- McCullough, A.R.; Hellstrom, W.G.; Wang, R.; Lepor, H.; Wagner, K.R.; Engel, J.D. Recovery of erectile function after nerve sparing radical prostatectomy and penile rehabilitation with nightly intraurethral alprostadil versus sildenafil citrate. J. Urol. 2010, 183, 2451–6. [Google Scholar] [CrossRef]
- Lima, A.S.; Villela, B.C.; Pustilnik, H.N.; Mattos, L.F.C.; de Sá, V.P.C.; Prado, F.M.S.; Batista, L.T. Comparison of adverse effects of combined and isolated substances in Intracavernosal injection: a systematic review and meta-analysis. J. Sex. Med. 2025, 22, 1579–1591. [Google Scholar] [CrossRef]
- Corona, G.; Santi, D.; Cocci, A.; Vena, W.; Pizzocaro, A.; Vignozzi, L.; Isidori, A.M.; Pivonello, R.; Salonia, A.; Minhas, S.; Bettocchi, C.; Reisman, Y.; Maggi, M. Long-term penile prosthesis couple’s satisfaction: A systematic review and meta-analysis. Andrology 2025, 13, 610–623. [Google Scholar] [CrossRef]
- Rho, B.Y.; Kim, S.H.; Ryu, J.K.; Kang, D.H.; Kim, J.W.; Chung, D.Y. Efficacy of Low-Intensity Extracorporeal Shock Wave Treatment in Erectile Dysfunction Following Radical Prostatectomy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 2775. [Google Scholar] [CrossRef] [PubMed]
- Quistini, A.; Fallara, G.; Tozzi, M.; Depalma, M.; Damiano, R.; Palmieri, A.; Castiglione, F.; Salonia, A.; Bianchi, R.; Ferro, M.; Muneer, A.; Alnajjar, H.M.; Pang, K.H. Comparative efficacy of combination therapy including regenerative therapies versus monotherapy for erectile dysfunction: A systematic review and meta-analysis. Andrology 2026, 14, 358–367. [Google Scholar] [CrossRef]
- Ergun, O.; Kim, K.; Kim, M.H.; Hwang, E.C.; Blair, Y.; Gudeloglu, A.; Parekattil, S.; Dahm, P. Low-intensity shockwave therapy for erectile dysfunction. Cochrane Database Syst. Rev. 2025, 7, CD013166. [Google Scholar] [PubMed]
- Jacob, D.; Hay, J.; Rahemtoola, M.S.; Sim, S.; Libretto, L.; Chawareb, E.A.; Hammad, M.; Mubarak, M.; Yafi, F.; Pearce, I.; Modgil, V. Current advances in platelet-rich plasma therapy for erectile dysfunction: a meta-analysis of randomized controlled trials. J. Sex. Med. 2026, 23, qdaf325. [Google Scholar] [CrossRef]
- Zhou, Z.; Wang, Y.; Chai, Y.; Wang, T.; Yan, P.; Zhang, Y.; Yang, X. The efficacy of platelet-rich plasma (PRP) alone or in combination with low intensity shock wave therapy (Li-SWT) in treating erectile dysfunction: a systematic review and meta-analysis of seven randomized controlled trials. Aging Male 2025, 28, 2472786. [Google Scholar] [CrossRef]
- Senel, S.; Sevinc, A.H.; Gultekin, H.; Ravshanbekovich, A.J.; Besiroglu, H.; Dursun, M.; Kadioglu, A. Stem cell therapy for erectile dysfunction: promise or reality?—a systematic review and meta-analysis of clinical trials. BMC Urol. 2025, 25, 222. [Google Scholar] [CrossRef]
- Haahr, M.K.; Jensen, C.H.; Toyserkani, N.M.; Andersen, D.C.; Damkier, P.; Sørensen, J.A.; Lund, L.; Sheikh, S.P. Safety and Potential Effect of a Single Intracavernous Injection of Autologous Adipose-Derived Regenerative Cells in Patients with Erectile Dysfunction Following Radical Prostatectomy: An Open-Label Phase I Clinical Trial. EBioMedicine 2016, 5, 204–10. [Google Scholar] [CrossRef] [PubMed]
- Yiou, R.; Hamidou, L.; Birebent, B.; Bitari, D.; Le Corvoisier, P.; Contremoulins, I.; Rodriguez, A.M.; Augustin, D.; Roudot-Thoraval, F.; de la Taille, A.; Rouard, H. Intracavernous Injections of Bone Marrow Mononucleated Cells for Postradical Prostatectomy Erectile Dysfunction: Final Results of the INSTIN Clinical Trial. Eur. Urol. Focus. 2017, 3, 643–645. [Google Scholar] [CrossRef]
- Corona, G.; Cucinotta, D.; Di Lorenzo, G.; Ferlin, A.; Giagulli, V.A.; Gnessi, L.; Isidori, A.M.; Maiorino, M.I.; Miserendino, P.; Murrone, A.; Pivonello, R.; Rochira, V.; Sangiorgi, G.M.; Stagno, G.; Foresta, C.; Lenzi, A.; Maggi, M.; Jannini, E.A. The Italian Society of Andrology and Sexual Medicine (SIAMS), along with ten other Italian Scientific Societies, guidelines on the diagnosis and management of erectile dysfunction. J. Endocrinol. Invest. 2023, 46, 1241–1274. [Google Scholar] [CrossRef] [PubMed]
- Salonia, A.; Capogrosso, P.; Boeri, L.; Cocci, A.; Corona, G.; Dinkelman-Smit, M.; Falcone, M.; Jensen, C.F.; Gül, M.; Kalkanli, A.; Kadioğlu, A.; Martinez-Salamanca, J.I.; Afonso Morgado, L.; Russo, G.I.; Serefoğlu, E.C.; Verze, P.; Minhas, S. European Association of Urology Guidelines on Male Sexual and Reproductive Health: 2025 Update on Male Hypogonadism, Erectile Dysfunction, Premature Ejaculation, and Peyronie’s Disease. Eur. Urol. 2025, 88, 76–102. [Google Scholar] [CrossRef]
- Danese, M.; D’Esposito, V.; Miranda, R.; Dolo, V.; Giusti, I.; Borean, A.; Rosa, D.; Amato, B.; Rughetti, A.; Del Greco, V.; Mazzucco, L.; Aversa, A.; Cassutti, V.; Casabona, F.; Irollo, A.M.; Setacci, C.; Caradonna, E.; Ascoli Marchetti, A.; Caloprisco, G.; Farina, M.A.; Formisano, P. SIMCRI Expert Consensus Group; SIMCRI (Società Italiana di Medicina e Chirurgia Rigenerativa Polispecialistica) Expert Consensus Group members. Expert Consensus on the use of autologous platelet-rich plasma in the context of regenerative medicine: moving forward to good clinical practice. Ann. Ist. Super. Sanità. 2026, 62, 16–31. [Google Scholar]
- La Croce, G.; Schifano, N.; Pescatori, E.; Caraceni, E.; Colombo, F.; Bettocchi, C.; Carrino, M.; Vitarelli, A.; Pozza, D.; Fiordelise, S.; Varvello, F.; Paradiso, M.; Silvani, M.; Mondaini, N.; Natali, A.; Falcone, M.; Ceruti, C.; Salonia, A.; Antonini, G.; Cai, T.; Palmieri, A.; Dehò, F.; Capogrosso, P. Which patient may benefit the most from penile prosthesis implantation? Andrology 2022, 10, 1567–1574. [Google Scholar] [CrossRef] [PubMed]
- Francomano, D.; Iuliano, S.; Dehò, F.; Capogrosso, P.; Tuzzolo, P.; La Vignera, S.; Antonini, G.; Aversa, A. Regenerative treatment with platelet-rich plasma in patients with refractory erectile dysfunction: short-term outcomes and predictive value of mean platelet volume. Minerva Endocrinol. (Torino) . 2025, 50, 267–275. [Google Scholar] [CrossRef]

Table 1.
Summary of the main meta-analyses selected for each outcome regarding PDE5-i therapy for PR after RP.
Table 1.
Summary of the main meta-analyses selected for each outcome regarding PDE5-i therapy for PR after RP.
| Main outcome | Specific outcome | Reference | Studies included | Patients included | Results |
|---|---|---|---|---|---|
| IIEF-EF score improvement | Daily dose (≤ 3 months) | Feng et al., 2022 [16] | 5 RCTs | 668 (340 intervention group vs. 328 control group) | MD: 3.07; 95% CI: 1.69 to 4.44; p < 0.0001; I2: 96% |
| Daily dose (≥ 6 months) | Feng et al., 2022 [16] | 6 RCTs | 261 (133 intervention group vs. 128 control group) | MD: 4.70; 95% CI: 3.66 to 5.74; p < 0.00001; I2: 0% | |
| On demand dose (≤ 3 months) | Feng et al., 2022 [16] | 4 RCTs | 749 (426 intervention group vs. 323 control group) | MD: 3.92; 95% CI: 2.95 to 4.88; p < 0.00001; I2: 99% | |
| On demand dose vs. daily dose (< 6 months) | Feng et al., 2022 [16] | 2 RCTs | 159 (79 on demand dose group vs. 80 daily dose group) | MD: 0.39; 95% CI: -2.04 to 2.82; p = 0.75; I2: 0% | |
| On demand dose vs. daily dose (≥ 6 months) | Feng et al., 2022 [16] | 2 RCTs | 152 (78 on demand dose group vs. 74 daily dose group) | MD: 0.49; 95% CI: -8.80 to 9.79; p = 0.92; I2: 92% | |
| Spontaneous EF after treatment discontinuation | PDE5-i efficacy (all types) | Liu et al., 2017 [17] | 4 RCTs | 1181 (777 intervention group vs. 404 control group) | OR: 1.027; 95% CI: 0.713 to 1.478; p = 0.610; I2: 48.4% |
| PDE5-i efficacy (by drug type) | Sari Motlagh et al., 2021 [19] | 22 RCTs | 2711 (1880 treated with interventions vs. 831 controls) | Daily sildenafil 100 mg (OR: 4.0; 95% CI: 1.40 to 13.40) Daily sildenafil flexible dose (OR: 2.61: 95% CI: 0.45 to 17.3) Daily sildenafil 25 mg (OR: 2.07; 95% CI: 0.47 to 10.4) Daily sildenafil 50 mg (OR: 1.94; 95% CI: 0.82 to 5.35) Daily vardenafil 5 mg (OR: 3.27; 95% CI: 0.49 to 2.56) Daily vardenafil 10 mg (OR: 2.22; 95% CI: 0.33 to 19.5) Vardenafil on demand (OR: 1.02; 95% CI: 0.44 to 2.36) Daily vardenafil flexible dose (OR: 0.77; 95% CI: 0.33 to 1.84) Daily tadalafil 20 mg (OR: 1.38; 95% CI: 0.38 to 51.16) Daily tadalafil 5 mg (OR: 1.14; 95% CI: 0.66 to 1.91) Tadalafil 20 mg on demand (OR 0.92; 95% CI: 0.52 to 1.56) |
|
| Treatment discontinuation | Daily dose (≥ 6 months) | Philippou et al., 2018 [18] | 1 RCT | 420 (210 intervention group vs. 210 control group) | RR: 1.12; 95% CI: 0.85 to 1.48; p = 0.41 |
| Daily dose vs. on demand dose (≥ 6 months) | Philippou et al., 2018 [18] | 3 RCTs | 612 (307 daily dose group vs. 305 on demand dose group) | RR: 1.09; 95% CI: 0.86 to 1.38; p = 0.98; I2: 0% | |
| Adverse events | Headache | Wang et al., 2014 [21] | 6 RCTs | 1820 (1205 intervention group vs. 615 control group) | POR: 2.99; 95% CI: 2.22 to 4.04; p < 0.00001; I2: 0% |
| Flushing | Wang et al., 2014 [21] | 6 RCTs | 1832 (1213 intervention group vs. 619 control group) | POR 4.71; 95% CI: 3.19 to 6.95; p < 0.00001; I2: 0% | |
| Dyspepsia | Wang et al., 2014 [21] | 4 RCTs | 1470 (980 intervention group vs. 490 control group) | POR 4.71; 95% CI: 3.19 to 6.95; p < 0.00001; I2: 0% | |
| Nasal congestion | Wang et al., 2014 [21] | 5 RCTs | 1709 (1132 intervention group vs. 570 control group) | POR 2.66; 95% CI: 1.85 to 3.84; p < 0.00001; I2: 0% | |
| Serious adverse events (on demand dose) (short term) | Philippou et al., 2018 [18] | 3 RCTs | 443 (220 on demand dose group vs. 203 control group) | RR: 0.32; 95% CI: 0.11 to 0.94; p = 0.04; I2: 0% | |
| Serious adverse events (on daily dose vs. on demand dose) (short term) | Philippou et al., 2018 [18] | 1 RCT | 282 (139 daily dose group vs. 143 on demand dose group) | RR: 0.69; 95% CI: 0.12 to 4.04; p = 0.68 | |
| Serious adverse events (on daily dose vs. on demand dose) (long term) | Philippou et al., 2018 [18] | 1 RCT | 100 (50 daily dose group vs. 50 on demand dose group) | RR: 3; 95% CI: 0.13 to 71.92 |
CI: confidence interval; EF: erectile function; I2: heterogeneity; IIEF-EF: International Index of Erectile Function—Erectile Function domain; MD: mean difference; PDE5-i: phosphodiesterase type 5-inhibitors; POR: Peto odds ratio; RCT: randomized controlled trial; RP: radical prostatectomy; RR: relative risk.
Table 2.
Quality assessment of the studies included in the present review.


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



