Submitted:
01 May 2026
Posted:
04 May 2026
You are already at the latest version
Abstract
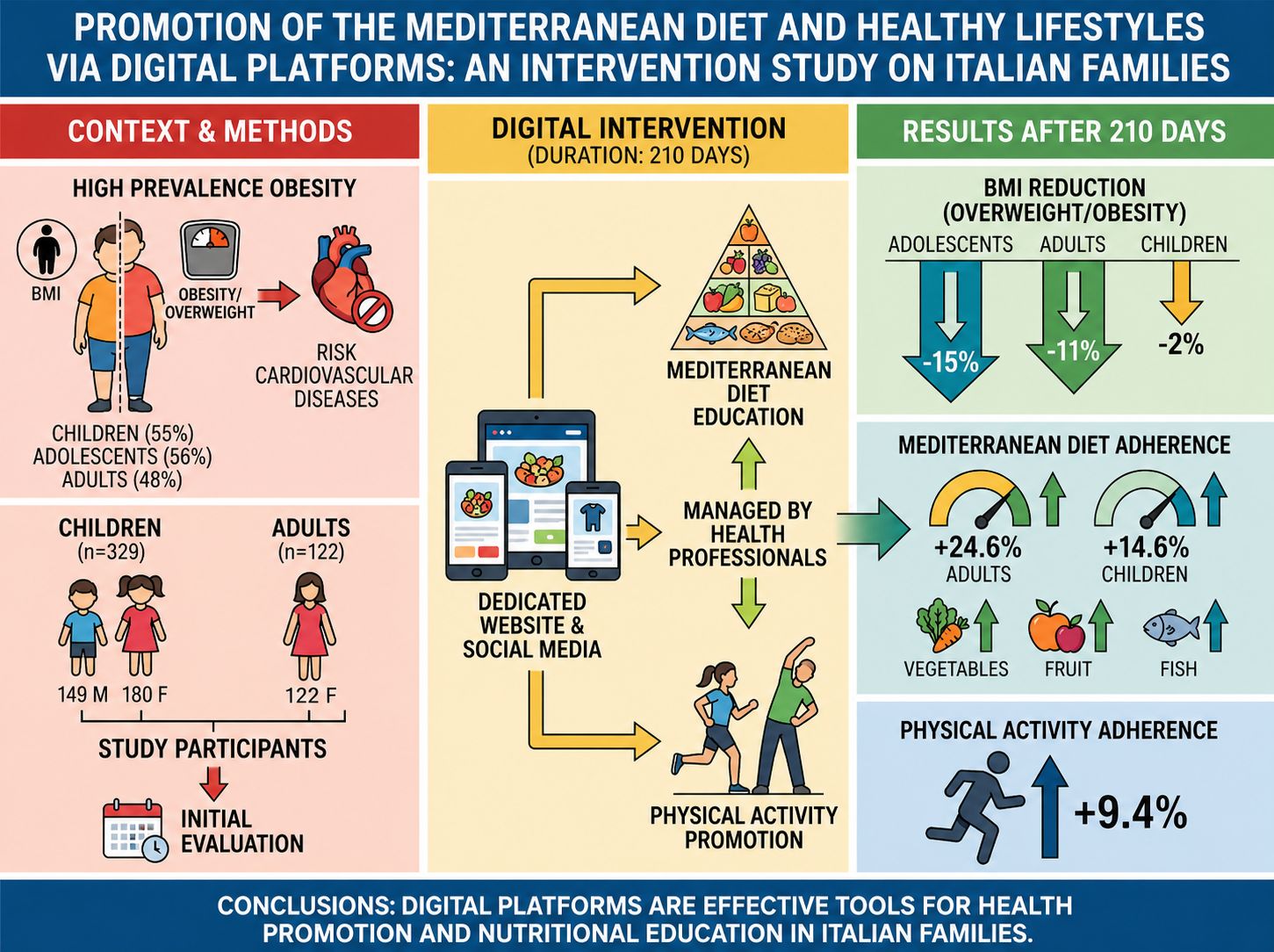
Background/Objectives: Several studies have confirmed a high prevalence of obesity among both children and adults, with significant consequences on human health. This study is aimed to develop and test effective tools (i.e., a dedicated website and social media) to promote healthy lifestyles, with the goal of re-engaging Italian families with the Mediterranean diet, an effective approach for preventing cardiovascular diseases. Methods: The study included 329 children (149 boys, 180 girls) and 122 female adults who underwent nutritional assessment and lifestyle surveys, before and after our educational intervention. Results: At baseline, Body Mass Index (BMI) analysis revealed a high incidence of overweight and obesity among children (55%), adolescents (56%), and adults (48%). Our action targeted improvements in eating habits and lifestyle in all the groups. After 210 days, adolescents showed the largest improvement in BMI, with a 15% reduction in overweight and obesity, while we observed a 2% and 11% reduction in children and adults, respectively. Furthermore, physical activity adherence increased by 9.4%. Excellent adherence to the Mediterranean diet was observed, both in children (+14.6%) and adults (+24.6%), with particular improvements in vegetable, fruit, and fish consumption. Conclusions: This study confirms the effectiveness of social media and digital platforms as tools for health promotion and nutrition education when managed by health professionals.
Keywords:
childhood and parental obesity
; eating habits
; mediterranean diet
; health promotion
; digital platforms
1. Introduction
In recent decades, several epidemiological studies have highlighted poor dietary habits and unhealthy lifestyles among children and adolescents [1,2,3,4,5,6,7], alongside a growing number of adults with cardiovascular risk factors and eating disorders (EDs) [8]. Factors such as increasingly hectic lifestyles, leading to meals more frequently eaten away from home, and the rise in consumption of foods rich in saturated fats and simple sugars — typical of fast food — have contributed to the increase in obesity rates. Furthermore, there is increased exposure to video games and sedentary behaviours.
World Health Organization (WHO) has estimated that in Italy 50% of adults (according to the PASSI study [9]) and 30% of children (according to the “OKkio alla Salute” study9) are overweight or obese. According to 2023 OKkio alla Salute data, Italy ranks among the European countries with the highest prevalence of weight excess in the school-age population, with 19% of children being overweight, 9.8% obese, and 2.6% severely obese⁹, with well-documented health consequences [10,11].
Despite many educational initiatives and pediatric recommendations, achieving a lasting change in dietary habits remains challenging. In this context, the Mediterranean Diet represents an effective nutritional model for preventing chronic degenerative diseases and improving quality of life [12,13,14]. However, the ZOOM8 study [15] showed that adherence to the Mediterranean Diet among Italian children is one of the lowest in Europe, underscoring the need for more impactful and effective strategies [16].
The present research aims to:
- formulate and test effective interventions and tools to sustainably promote the health of children and families;
- improve family dietary habits, rediscovering the pleasure of preparing and sharing daily meals, starting with breakfast.
The tools we designed and implemented, with the active involvement of more than 100 dietitian-nutritionists, appears to address this need. In facts, we have created a website with sections specifically designed for parents (or other adults in the family), children or teachers; we also build up social media pages (Facebook and Instagram) along with a Facebook page dedicated to teachers only, which includes didactic materials.
These platforms allowed us to provide evidence-based information to more than 91,000 users between 2019 and 2021. Since 2022, those platforms are not being updated, but they are still highly visited: the website alone (www.sanogiustocongusto.it) counts more than 305,000 visitors up to now.
Recent literature suggests that social media, if used appropriately, can be powerful tools for health education [17,18,19]. Our project fostered ongoing dialogue between families and professionals, with encouraging results, particularly for children who engaged with dieticians via social media or by participating to a recipe contest, that is, creating healthy and tasty meals together with one or both parents.
Children’s eating behaviours are strongly influenced by family environment. Parents, teachers, and grandparents play a key role in encouraging checking new foods and acquiring healthy habits. The “BATMAN Project — Children at the Table” [20], launched by Istituto Oncologico Romagnolo in 2016, and the project “Sano, Giusto e con Gusto! (Heatly, Right and Tasty)”, started in 2019, demonstrated that tasting experiences and active participation in meal preparation led to improvements in children’s taste preferences. Using simple recipes and the “kitchen-as-a-fun”, educational moment fosters food awareness and long-term adoption of healthy lifestyles.
The objective of this study is to assess whether the proposed methodology effectively brings changes in eating habits and lifestyles of adults and children/adolescents participating in the study.
2. Materials and Methods
To test our methodology, we conducted an experimental study involving children, adolescents, and adults who joined the project, with the use of an innovative multimedia approach. Such approach included the creation of an interactive, dedicated website with downloadable educational materials, as well as a cooking contest engaging both adults and children to work together.
2.1. Interventional Experimental Study on a Population Sample
- Problem: Does sample A (adults) adhere to the Mediterranean Diet? / Sample analysis
- Intervention: Use of downloadable interactive and multimedia educational materials. How many participants modified their eating habits?
- Comparison: Among adults stratified by their level of education
- Outcome: Did sample B (children and adolescents), educated by the same adults, achieve changes in eating habits and lifestyle? / Sample analysis
2.2. Sample
- Adults (teachers, parents, educators, grandparents) randomly recruited among registrants in the national project.
- Children and adolescents guided by the adults (teachers and/or parents/grandparents) to improve their eating and lifestyle habits.
2.3. Primary Outcomes
- To assess eating habits in adults; specifically, adherence to the Mediterranean Diet, before and after the intervention
- To assess eating habits in children and adolescents; specifically, adherence to the Mediterranean Diet and time dedicated to physical activity, before and after the intervention
- To assess BMI in all study participants: adults, children, and adolescents, before and after the intervention. BMI has been used also for children according to [27].
2.4. Secondary Outcomes
To assess differences in adherence to the Mediterranean Diet among adult groups with different level of education, before and after the intervention
2.5. Study Phases
The study was divided into three phases:
- The first phase aimed to provide a snapshot of the nutritional status, eating habits, and lifestyle of all participants.
- The second phase delivered the intervention through interactive materials distributed via dedicated social media channels.
- The third phase assessed the results after the intervention.
Data were collected, processed, and interpreted before and after the intervention to detect differences. Data collection employed validated questionnaires, data processing was conducted using Excel spreadsheets, and statistical analysis was performed using SPSS software.
2.6. Recruitment
We recruited new participants to the scientific study through a newsletter invitation. Subsequently, participating adults underwent remote training by watching eight videos presenting the scientific basis of the project, participation procedures, and use of the educational materials. The modules were released on the project’s Facebook page (Sano, Giusto e con Gusto), then shared on each professional’s social channels. The videos remain available in the events section of the website for public access.
The modules were:
- Module 1 — Scientific foundations
- Module 2 — The project: objectives, target, implementation
- Module 3 — Adolescents and food
- Module 4 — Educational pathway
- Module 5 — Food intolerances, cross-cultural plates, and environmental sustainability
- Module 6 — Physical activity
- Module 7 — Cooking together
- Module 8 — How to register for the project and the recipe contest “super-championship”.
2.7. Website Contents (Publicly Accessible Area)
- Healthy, Fair, and Tasty Recipes! (parents could take inspiration from our recipes to create new ones with their children and even participate in the recipe contest with a support from regional dietitian-nutritionists)
- Games and Quizzes! (children and adolescents could download interactive educational games such as crosswords, rebuses, and more)
- Once Upon a Time! Let Me Tell You a Story (a section dedicated to younger children, where two artists specialized in children’s communication narrate pre-approved nutrition-themed fairy tales)
- A section with educational materials for adults (teachers, educators, parents, grandparents) (Figure 1).
2.8. Phase 1—Data Collection
- Assessing adults’ eating habits using the validated PREDIMED questionnaire [28] to determine adherence to the Mediterranean Diet. The questionnaire was modified to include role (teacher, parent, or educator), level of education, age, region, weight, and height. The questionnaire was provided via Google Forms, and the link was emailed to participants, who were preliminarily required to consent to data privacy terms and commitment to complete the study. Duplicates were automatically removed based on email address.
- Assessing children’s and adolescents’ eating habits using the validated KIDMED questionnaire [29,30], also measuring Mediterranean Diet adherence. Additional questions captured weight, height, age, region, amount of physical activity, and indication of which adult guided them. The first question was modified to replace “fruit juices” with freshly squeezed juice or blended fruit, due to their lower sugar content. This questionnaire was proposed via Google Forms, too.
Parents and teachers received both their own and their children’s/adolescents’ questionnaires by email. Children’s questionnaires were identified by an invented nickname plus a number. A consent form and photo/video release were attached to the invitation.
Duration of Phase 1: 2 months — data collection at the start of the school year, followed by analysis and interpretation.
2.9. Phase 2—Intervention
- Support for adults with downloadable multimedia educational materials, created by collaborating dietitian-nutritionists: fact sheets, video clips, healthy and tasty recipes to inspire cooking with children, and other interactive resources available at [www.sanogiustocongusto.it] (http://www.sanogiustocongusto.it). The “Healthy Dish” recipe contest encouraged children to participate actively.
- Support for children and adolescents with downloadable interactive games: crosswords, riddles, etc.
- Support for young children with video fairy tales, dramatized by two Neapolitan theatre artists.
- Support for children and adolescents with physical activity programs: fact sheets and videos created by a motor activity expert using the “Cantaballo” method.
This phase enabled adults to deepen their knowledge and improve their own habits in order to effectively convey healthy messages to their children and adolescents.
Duration of Phase 2: from November to the end of March.
2.10. Phase 3—Evaluation
- Assess changes in adults’ eating habits, particularly adherence to the Mediterranean Diet, using the PREDIMED questionnaire in the same format as Phase 1.
- Assess changes in children’s and adolescents’ eating habits, Mediterranean Diet adherence, and physical activity using the KIDMED questionnaire in the same format as Phase 1.
Children’s questionnaires were again identified by an invented nickname plus a number.
Duration of Phase 3: 2 months — data collection after the educational intervention, followed by analysis and interpretation.
2.11. Study Methods
2.12. Statistical Analysis
Data were collected in a spreadsheet and analyzed using SPSS statistical software.
2.13. Predimed Score Calculation
The PREDIMED questionnaire (Mediterranean Diet adherence score) is composed of 14 questions designed for adults. A score of +1 is assigned to each answer that expresses adherence to the Mediterranean Diet. The possible score range is from 0 to 14. Three levels of classification are defined:
- ≥10: good adherence to the Mediterranean Diet
- 6–9: medium adherence to the Mediterranean Diet
- 0–5: poor adherence to the Mediterranean Diet
2.14. Kidmed Score Calculation
The KIDMED questionnaire (Mediterranean Diet adherence score) is composed of 16 questions designed for children. A score of +1 is assigned to a “YES” response on those 12 items expressing adherence to the Mediterranean Diet, while a score of −1 is assigned to a “YES” response on those 4 items expressing counter-adherence.
We modified the original questionnaire by including two additional questions: one regarding physical activity (+1 point for the answer “2–3 times per week”), and the other one regarding use of video games and electronic devices for leisure (−1 point for the answer “more than 3 hours per day”).
The possible score range is from 0 to 13 (instead of 12 in the original questionnaire).
The original three-level classification is maintained:
- 8: good adherence to the Mediterranean Diet
- 4–7: medium adherence to the Mediterranean Diet (modifications needed)
- ≤3: poor adherence to the Mediterranean Diet
2.15. Study Duration: One School Year
Rationale for the study duration: some (end-of-cycle) classes (fifth grade of primary school and eighth grade of middle school) will change their teachers at the end of the school year, thus losing their point of reference.
3. Results
3.1. Results on 329 Children Participating in the Study
A total of 329 children participated in the study: 149 boys and 180 girls. Among these, 35.6% were guided by teachers, 26.1% by parents, and 38.3% by both. Regarding BMI calculation, the total sample was divided into two age groups: 6–10 years identified as “Sample A”, and 11–14 years identified as “Sample B”.
3.1.1. Baseline (Time 0)
Sample A (children aged 6–10): 9% (n=23) underweight, 22% (n=58) mildly underweight, 14% (n=36) normal weight, 38% (n=101) overweight, 17% (n=45) obese (Figure 2).
Sample B (children aged 11–14): 7% (n=5) underweight, 29% (n=19) mildly underweight, 8% (n=5) normal weight, 47% (n=31) overweight, 9% (n=6) obese (Figure 3).
Physical activity: In the total sample of 329 children, 55.6% engaged in physical activity 2–3 times per week, while 44.4% engaged less than twice per week.
Regarding screen time, 49.8% spent 2–3 hours daily on TV or video games, 18.8% more than 3 hours daily, and 31.4% none or at most 1 hour daily (Figure 4).
Eating habits: At baseline, the consumption of fruits, vegetables, and fish was low:
only 104 out of 329 children (31.6%) ate vegetables twice daily, 133 out of 329 (40.4%) ate fruits twice daily, and 148 out of 329 (45%) consumed fish at least 2–3 times weekly. However, breakfast habits were good: 79.6% of children ate breakfast regularly (Figure 5).
Adherence to the Mediterranean Diet: At baseline, 46.8% (n=154) had good adherence, 43.5% (n=143) medium adherence, and 9.7% (n=32) poor adherence (Figure 6).
3.1.2. Follow-Up (210 Days)
Sample A (children aged 6–10): 9% (n=23) underweight, 20% (n=54) mildly underweight, 18% (n=47) normal weight, 37% (n=97) overweight, 16% (n=42) obese (Figure 7).
Sample B (children aged 11–14): 11% (n=7) underweight, 29% (n=19) mildly underweight, 19% (n=13) normal weight, 32% (n=21) overweight, 9% (n=6) obese (Figure 8).
Physical activity: After 210 days, 65% of children engaged in physical activity 2–3 times per week, while 35% engaged less (including once a week or never). Regarding screen time, 44.8% spent 2–3 hours daily on TV or video games, 9.2% more than 3 hours daily, and 46% none or at most 1 hour daily (Figure 4).
Eating habits: After 210 days, fruit, vegetable, and fish consumption improved:
191 out of 329 children (58.2%) ate vegetables twice daily, 210 out of 329 (64%) ate fruits twice daily, and 189 out of 329 (58%) consumed fish at least 2–3 times weekly. Breakfast frequency also improved to 86.3% (Figure 5).
Adherence to the Mediterranean Diet: After 210 days, 61.4% (n=202) had good adherence, 36% (n=118) medium adherence, and 2.6% (n=9) poor adherence (Figure 6).
3.2. Results on 122 Adults Participating in the Study
A total of 122 female adults participated.
3.2.1. Baseline (Time 0)
52% (n=64) normal weight, 31% (n=37) overweight, 17% (n=21) obese (Figure 9).
Eating habits: At baseline, fruit, vegetable, and fish consumption was low: 44 out of 122 adults (36%) ate vegetables twice daily, 26 out of 122 (21.3%) ate fruit at least three times daily, 4 out of 122 (3.27%) consumed fish at least three times weekly, and 9 out of 122 (7.37%) consumed legumes three times weekly (Figure 10).
Adherence to the Mediterranean Diet: At baseline, 10.8% (n=13) had good adherence, 72% (n=88) medium adherence, and 17.4% (n=21) poor adherence (Figure 11).
3.2.2. Follow-Up (210 Days)
63% (n=77) normal weight, 30% (n=36) overweight, 7% (n=8) obese (Figure 12).
Eating habits: After 210 days, fruit, vegetable, and fish consumption improved:
65 out of 122 adults (53.2%) ate vegetables twice daily, 38 out of 122 (31.1%) ate fruit at least three times daily, 19 out of 122 (15.5%) consumed fish at least three times weekly, and 21 out of 122 (17.2%) consumed legumes three times weekly (Figure 10).
Adherence to the Mediterranean Diet: After 210 days, 35.4% (n=43) had good adherence, 62.2% (n=76) medium adherence, and 2.4% (n=3) poor adherence (Figure 11).
3.3. Secondary Outcomes
We observed differences in Mediterranean Diet adherence between adult groups with different level of education, before and after the intervention.
Data analysis revealed a significant correlation between body weight status and level of education at both baseline and follow-up. Specifically, normal weight and obesity were associated with a high school diploma (p < 0.0000001), whereas overweight was associated with lower educational attainment (p < 0.0000001) (Figure 13).
4. Discussion
The effectiveness of the method used was assessed by comparing eating habits and lifestyle at baseline and 210 days after the intervention. The impact of the project on both adults and minors confirmed the effectiveness of social media and digital platforms as tools for health promotion and nutrition education when managed by health professionals.
The methodological approach adopted ensured that social media and digital devices were not directly used by minors, but rather proposed and mediated by their primary caregivers—parents, teachers, and educators—who actively guided the educational process. This strategy not only provided greater safety but also strengthened the adult–child relationship through shared activities such as cooking, educational games, recipe preparation, and storytelling. Furthermore, the chosen approach represents a protective strategy against the risks associated with excessive screen use in children, as documented in recent literature [31,32].
After 210 days of our educational intervention, children in Sample A (6–10 years), who were overweight or obese, showed no significant changes, whereas underweight children reached normal weight (+2%). Sample B, consisting of adolescents (11–14 years), who are more attentive to body image, achieved more substantial results. Overweight prevalence dropped from 47% to 32% (a 15% reduction), with 11% reaching normal weight and 4% shifting to underweight.
Additionally, the proportion of children engaging in physical activity 2–3 times per week increased from 55.6% to 65% (+9.4%), with a slight reduction in sedentary behaviour: 44.8% still spent 2–3 hours daily on TV and video games. About 7% more children reported having breakfast regularly.
The proportion of children consuming vegetables twice daily rose from 31.6% to 58.2%, fruit from 40.4% to 64.8%, and fish from 45% to 58%. Good adherence to the Mediterranean Diet was observed in 61.4% of children after the intervention.
Among the 122 adults, after 210 days of our educational intervention, the proportion of overweight individuals showed little change, whereas obesity prevalence decreased from 17% to 7%, with more participants reaching normal weight.
Adults consuming vegetables twice daily increased from 36% to 53.2%, fruit at least three times daily from 21.3% to 31.1%, fish at least three times weekly from 3.27% to 15.5%, and legumes three times weekly from 7.37% to 17.2%. Good adherence to the Mediterranean Diet was observed in 35.4% of adults after the intervention.
In summary, the intervention had a positive impact on eating habits and lifestyle in both children and adults, with significant improvements in adherence to the Mediterranean Diet.
Data analysis revealed a significant correlation between body weight status and educational level of the participating adults, both at baseline and follow-up. Specifically, normal weight and obesity were associated with having a high school diploma (p < 0.0000001), whereas overweight was correlated with lower educational attainment (p < 0.0000001).This study has some limitations. The absence of a control group limits causal interpretation and does not allow exclusion of external influences. Participants were recruited on a voluntary basis, which may have introduced selection bias. In addition, key variables such as weight, height, and dietary habits were self-reported, and the follow-up period was relatively short to assess long-term sustainability of behavioural changes.
5. Conclusions
Several studies have shown that social media represent a powerful tool for health promotion, facilitating the creation of user networks and providing healthcare institutions and professionals with a stable, ongoing communication channel with patients and families.[8,9] These digital platforms, if properly managed, enable not only widespread dissemination of evidence-based information, but also direct, timely, and personalised interaction with the public, enhancing engagement and adherence to prevention programs.
In our study, in addition to social media pages (Facebook, Instagram, and one dedicated to the teachers only), an interactive website was developed, specifically designed to provide educational content, downloadable teaching materials, and self-monitoring tools for both adults (parents, educators, teachers, grandparents) and children/adolescents.
This multichannel approach allowed us an accessible and flexible user engagement, with content tailored to different age groups and educational levels.
Data collected after 210 days from the start of the intervention show positive results on improved eating habits and reduced sedentary behaviours, accompanied by increased time dedicated to physical activity. These behavioural changes were observed across both age subgroups (6–10 years and 11–14 years), with particularly notable effects among those jointly guided by teachers and parents.
The project, which involved the entire family, showed that 96.6% of children and adults achieved good adherence to the Mediterranean Diet and improved their dietary habits.
Regarding body weight changes, modest improvements in BMI values were observed, with an increase in the proportion of normal weight participants and a slight reduction in the percentage of obese children and adults, while the number of overweight children and adults remained nearly unchanged. Therefore, future studies should investigate parents’ perceptions of overweight in their children to better target interventions.
Moreover, although a significant correlation was found between body weight status and level of education, both at baseline and follow-up, it will be useful to assess regional differences (north, center, and south Italy) in future studies.In summary, preliminary findings suggest that an integrated, family-based digital intervention may represent a promising strategy to promote healthier lifestyles and improve adherence to the Mediterranean Diet in children, adolescents, and adults. The involvement of parents, teachers, and health professionals appears to be a key factor in supporting behavioural change. However, the absence of a control group, the use of self-reported data, and the relatively short follow-up period require cautious interpretation of the results. Future controlled studies with longer follow-up are needed to confirm these findings and assess their impact on body weight.
Author Contributions
F. Poggiante gave substantial contributions to the conception and design of the manuscript. M. Lista and L. Nemi contributed to the acquisition, analysis, and interpretation of data. I. Chinellato, V. Fanos and A. Acquaviva critically revised the manuscript. All authors read and approved the final version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study did not require ethical approval.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
Part of this study has been carried out in the framework of the “Sano, Giusto e con Gusto!” project. We are grateful to Dietitian-Nutritionists associated with Technical-Scientific Association of Food, Nutrition and Dietetics (ASAND) who helped with contents for the website and social media pages functional to this work.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Beccaria, L.; Galli, L.; Tonini, G.; Calori, G.; Gallus, G.; Chiumello, G. Studio Multicentrico sulla frequenza di obesità in età scolare in Italia. Riv. Ital. Di Pediatr. 2000, (26), 115–120. [Google Scholar]
- Poggiante, F.; Surace, A.; Antognozzi, V.; Fulgione, C.; Greco, L. Esercizio Fisico e Obesità: indagine sullo stile di vita e sul consumo di grassi in 4698 bambini della provincia di Napoli. In IV Congresso Nazionale Società Italiana di Nutrizione Pediatrica (SINUPE), III Congresso Nazionale Società Italiana per lo studio delle Malattie Metaboliche Ereditarie (SISMME), 55° Corso di Aggiornamento Sezione Lombarda Società Italiana di Pediatria, MILANOPEDIATRIA 2002; Milano, 2002; pp. pag. 227–228. [Google Scholar]
- F. Poggiante, N. D’Orazio, V. Antognozzi, G. D’Alterio, A. Surace, A. De Benedictis, L. Greco Stato Nutrizionale, Abitudini Alimentari e Stile di vita in 5000 studenti della regione Campania Atti del Congresso MILANOPEDIATRIA 2004, Milano, 11-13 Novembre 2004.
- Dan Nemet, Sivan Barkan, Yoram Epstein, Orit Friedland, Galit Kowen, Alon Eliakim Effetti benefici a breve e lungo termine di un intervento combinato di attività dietetica-comportamentale-fisica per il trattamento dell’obesità infantile - 2005 aprile; 115 (4): e443-9. [CrossRef] [PubMed]
- Poggiante F., Giorgini M., Ciano O., Costagliola L., Sangiovanni B., Comune C., Bolognini I., Ricciardi L., Cimaduomo L., Nardi E., Ferraiuolo S. Greco L. - Sato nutrizionale, abitudini alimentari e stile di vita in circa 1200 alunni del Comune di Napoli - Atti del Congresso MILANOPEDIATRIA 2014, Milano, 20-23 Novembre 2014.
- P Rosati 1, S Triunfo, F Zucchetti, C Gorca, R Chini, R Campana Screening di obesità, sovrappeso e magrezza in una popolazione di bambini a Roma, Italia - Minerva Pediatr. 2014, 66(3), 201–7. [PubMed]
- F. Poggiante, M. Giorgini, O. Ciano, L. Costagliola, B. Sangiovanni, C. Comune, S. Ferraiuolo, I. Bolognini, L. Ricciardi, L. Cimaduomo, E. Nardi, L. Greco - Nutritional status, dietary habits and lifestyle of 861 students residing in the municipality of Naples, a multidisciplinary approach concerning obese and overweight students - Atti del XIII Congresso Nazionale SIPREC, 12-14 marzo 2015.
- Keys, A. Mediterranean diet and public health: personal reflections. Am. J. Clin. Nutr. 1995, 61, 1321S–1323S. [Google Scholar] [CrossRef]
- Passi: Sintesi dei risultati 2022-2023, Istituto Superiore della Sanità – EpiCentro. Okkio alla salute: Sintesi dei risultati 2023, Istituto Superiore della Sanità - EpiCentro.
- Ebbeling, C.B.; Pawlak, D.B.; Ludwig, D.S. Childhood obesity: public-health crisis, common sense cure. Lancet 2002, 360, 473–482. [Google Scholar] [CrossRef]
- Wang, Y.; Lobstein, T. Worldwide trends in childhood overweight and obesity - Int J -Pediatr Obes. 2006. [Google Scholar]
- Jossa, F.; Mancini, M. La dieta mediterranea nella prevenzione dell’arteriosclerosi Recenti. Prog. Med.;Prog. Med. 1996, 87(4), 175–81. [Google Scholar] [PubMed]
- Frans J Kok 1, Daan Kromhout Aterosclerosi- studi epidemiologici sugli effetti sulla salute della dieta mediterranea - PMID: 15052492 Eur J Nutr 2004 Mar; 43 Suppl 1: I / 2-5. [CrossRef]
- AR Proietti 1, V del Balzo, S Dernini, LM Donini, C Cannella Dieta Mediterranea e prevenzione delle malattie non trasmissibili: evidenze scientifiche Ann Ig. Maggio-giugno. 2009, 21(3), 197–210. [PubMed]
- Roccaldo, R.; Censi, L.; D’Addezio, L.; et al. Adherence to the Mediterranean diet in Italian school children (The ZOOM8 Study) - - ZOOM8 Study group. Int. J. Food Sci. Nutr. 2014, 65(5), 621–8. [Google Scholar] [CrossRef]
- Gemma Enright, Margaret Allman-Farinelli, Julie Redfern Efficacia degli interventi di cambiamento del comportamento basati sulla famiglia sul cambiamento del comportamento correlato all’obesità nei bambini: una sintesi realista - - Int J Environ Res Public Health . 8 giugno 2020; 17 (11): 4099. [CrossRef] [PubMed] [PubMed Central]
- Radu, G.; Solomon, M.; Gheorghe, C.; Hostiuc, M.; Bulescu, I.; Purcarea, V. The adaptation of health care marketing to the digital era. 2017, 10, 44–46. [Google Scholar]
- Koumpouros, Y.; Toulias, T.L.; Koumpouros, N. The importance of patient engagement and the use of Social Media marketing in healthcare. Technol. Heal. Care 2015, 23, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Tyagi, M.; Sharma, D. Use of Social Media Marketing in Healthcare. J. Heal. Manag. 2013, 15, 293–302. [Google Scholar] [CrossRef]
- Acquaviva, Annamaria. Progetto Batman 2016 IOR.
- ngela Leis Migu https://doi.org/10.1590/1984-0462/2020/38/2018242el Ángel Mayer, Javier Torres Niño, Alejandro Rodríguez- González Josep Maria Suelves , Manuel Armayones Gruppi di sostegno per un’alimentazione sana su facebook: contenuti e cratteristiche Gac Sanit. Luglio-agosto. Epub 2013, 29 gennaio. 2013, 27(4), 355–7. [CrossRef] [PubMed]
- Apatu, E.J.I.; Alperin, M.; Miner, K.R.; Wiljer, D. A Drive Through Web 2.0. Heal. Promot. Pr. 2011, 14, 88–95. [Google Scholar] [CrossRef]
- Røed, M.; Hillesund, E.R.; Vik, F.N.; Van Lippevelde, W.; Øverby, N.C. The Food4toddlers study - study protocol for a web-based intervention to promote healthy diets for toddlers: a randomized controlled trial. BMC Public Heal. 2019, 19, 563. [Google Scholar] [CrossRef]
- Juan Francisco Lisón, Gonzalo Palomar, Marinna S Mensorio, Rosa M Baños, Ausiàs Cebolla-Martí, Cristina Botella, Vicent Benavent-Caballer, Enrique Rodilla. Impact of a Web-Based Exercise and Nutritional Education Intervention in Patients Who Are Obese With Hypertension: Randomized Wait-List Controlled Trial - - J Med Internet Res. 2020 Apr 14;22(4): e14196. [CrossRef] [PubMed]
- Hammersley, M.L.; Okely, A.D.; Batterham, M.J.; A Jones, R. An Internet-Based Childhood Obesity Prevention Program (Time2bHealthy) for Parents of Preschool-Aged Children: Randomized Controlled Trial. J. Med. Internet Res. 2019, 21, e11964. [Google Scholar] [CrossRef] [PubMed]
- Karen Weber Cullen, DrPH, RD, Debbe Thompson, PhD, Tzu-An Chen, PhD. Outcome Evaluation of Family Eats: An Eight-Session Web-Based Program Promoting Healthy Home Food Environments and Dietary Behaviors for African American Families. Published May 19, 2016.
- Cole, T. A chart to link child centiles of body mass index, weight and height. Eur. J. Clin. Nutr. 2002, 56, 1194–1199. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- Lovro Štefan, Rebeka Prosoli, Dora Juranko, Marko Cule, Ivan Milinovi, Dario Novak and Goran Sporiš The Reliability of the Mediterranean Diet Quality Index (KIDMED) Questionnaire – Nutrients Received: 23 March 2017; Accepted: 21 April 2017; Published: 23 April 2017.
- Simon, M.I.S.d.S.; Forte, G.C.; Marostica, P.J.C. TRANSLATION AND CULTURAL ADAPTATION OF THE MEDITERRANEAN DIET QUALITY INDEX IN CHILDREN AND ADOLESCENTS. Rev. Paul. De Pediatr. 2020, 38, e2018242. [Google Scholar] [CrossRef]
- Mulla, W.; Ahmed, W.; Radhi, M.; Alaali, H.; Alwazeer, G.; Yusuf, F.; Alsuhim, G.; Al Suhaym, A.; Alahmari, W.; Abdulla, M.; et al. Exploring Screen Time and Its Effects on Children’s Mental Health: A Cross-Sectional Study. Cureus 2024, 16, e71215. [Google Scholar] [CrossRef]
- Muppalla, S.K.; Vuppalapati, S.; Pulliahgaru, A.R.; Sreenivasulu, H. Effects of Excessive Screen Time on Child Development: An Updated Review and Strategies for Management. Cureus 2023, 15, e40608. [Google Scholar] [CrossRef]
Figure 1.
Guide material, worksheets and video pills.

Figure 2.
Body mass Index (BMI), SAMPLE A (6-10 years) TIME 0.

Figure 3.
Body mass Index (BMI), SAMPLE B (11-14 years) TIME 0.

Figure 4.
Lifestyle (TIME 0 – TIME 210 gg.).

Figure 5.
KIDMED (eating habits from 6-14 years – (TIME 0 - TIME 210 gg).

Figure 6.
Adherence to the Mediterranean diet in children and adolescents (TIME 0 – TIME 210 gg).

Figure 7.
Body mass Index (BMI) SAMPLE A (6-10 years) (TIME 210 gg).

Figure 8.
Body mass Index (BMI) SAMPLE B (11-14 years) (TIME 210 gg.).

Figure 9.
Body mass Index (BMI) ADULTS (TIME 0).

Figure 10.
PREDIMED (adults eating habits) (TIME 0 – TIME 210 gg.).

Figure 11.
Adherence to the Mediterranean diet in adults (TIME 0 – TIME 210 gg.).

Figure 12.
Body mass Index (BMI) adults (TIME 210 gg).

Figure 13.
Correlation between cultural level and BMI.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



