Submitted:
27 April 2026
Posted:
29 April 2026
You are already at the latest version
Abstract
While joint hypermobility can result from various medical conditions, it is most commonly associated with a group of related genetic conditions that affect connective tissue known as Ehlers–Danlos syndromes (EDSs). As there is currently no specific genetic testing for the diagnosis of Ehlers–Danlos hypermobility syndrome (hEDS), diagnosis is strictly made based on clinical criteria, which include physical features such as pain and family history, in addition to a scoring system known as the Beighton Score—a 9-point scale used to measure joint hypermobility—with a score of >4 considered significant. While hEDS often causes chronic muscle and joint pain, the underlying mechanisms remains poorly understood. Dysautonomia, characterized by common symptoms such as anxiety, vertigo, and increased heart rate when standing (orthostatic intolerance), in addition to multiple gastrointestinal symptoms, is highly prevalent among hEDS patients. We hypothesize that hypermobility due to ligamentous instability of the upper cervical spine, C1 and C2, results in impingement of the carotid sheath, the carotid artery and, more significantly, the vagus nerve, thus explaining the myriad symptoms that accompany hEDS. We also propose the novel use of extracorporeal shock wave therapy (ESWT) to treat this instability.
Keywords:
Ehlers Danlos Syndrome
; dysautonomia
; extracorporeal shock wave therapy
; cervical instability
; vagus
1. Introduction
It is widely recognized that the most common cause of joint hypermobility is one of the thirteen types of Ehlers–Danlos syndrome (EDS) [1]. Ehlers–Danlos syndromes (EDSs) are a group of related genetic conditions that affect connective tissue and are typically characterized by skin hyperextensibility, joint laxity, and tissue fragility [2]. Due to the lack of specific genetic testing for the diagnosis of EDS hypermobility syndrome (hEDS), diagnosis is strictly based on clinical criteria, such as physical features, pain, and family history, in addition to a scoring system known as the Beighton Score, a test that measures joint hypermobility. A 9-point scale is used to measure joint hypermobility, with a score of >4 considered significant [3].
In earlier studies, (hEDS) has traditionally been viewed as a musculoskeletal condition [4]; however, the mechanism by which the condition exerts influence at a systemic level—often involving the cardiovascular, neurological, and other autonomic domains—remains unclear [5]. Clinical observations and the findings of smaller studies link upper cervical instability to vagus nerve compression in hEDS, with symptoms improving after neck stability is addressed [6]. This cervical instability has been most commonly linked to ligament laxity, particularly at C1-C2 or the craniocervical junction. The vagus nerve exits the skull and travels directly parallel to these vertebrae in the carotid sheath (together with the glossopharyngeal nerve). Excessive movement can pinch, irritate, or distort the nerve at the nodose ganglion, impairing its signals. This process leads to autonomic dysfunction that can significantly impair the individual’s quality of life and result in complications in the management of the disease [7]. Due to this apparent vagus nerve connection, non-invasive vagus nerve stimulation (VNS), such as auricular (ear) or acoustic methods, is being investigated in multiple clinical studies and trials to improve autonomic function to reduce GI symptoms and ease pain in hEDS [8,9]. A considerable body of research is now concentrated on the role of the vagus nerve in the etiology of the myriad of symptoms suffered by patients with the diagnosis of EDS and the effects of ligamentous instability initiating this vagus nerve involvement.
2. History of the Disease
Very early writings by Hippocrates from 400 BCE describe a condition that may have been hEDS when he noted that Scythians and nomadic populations had lax joints as well as numerous scars, which he believed may have been caused by cauterization in an attempt to tighten the joints. It was not until the late 1800s that Ehlers–Danlos syndrome (EDS) was be described in the literature by Danish dermatologist Edvard Ehlers and the French dermatologist Henri Alexandre Danlos in 1899 and 1908, respectively. In 1936, an English physician, Frederick Parkes-Weber, suggested that the disorder be named ‘Ehlers–Danlos syndrome [10].
In 1956, Victor McKusick provided the first synthesis of the clinical literature on the multisystemic and variable nature of EDS in his work on heritable connective tissue disorders. McKusick found EDS to be a generalized disorder of connective tissue, noting that the underlying biochemical defects in collagen necessarily impacted every organ system in which collagen serves as a structural scaffold rather than a mil or seemingly trivial mechanical disorder of lax joints in otherwise healthy subjects [11]. In 2017, the International Consortium on Ehlers–Danlos Syndromes established a new classification defining 13 EDS subtypes based on clinical, molecular, and genetic criteria. These criteria emphasized that EDS was not merely a joint or musculoskeletal disorder but a complex syndrome that included autonomic dysfunction [12]; however, the authors did not examine specific mechanisms in detail, such as craniocervical instability or vagus nerve compression. Research into possible mechanical effects on the vagus nerve increased from 2017 to 2021 and eventually resulted in the term cervicovagopathy (vagus nerve dysfunction secondary to ligamentous cervical instability) appearing more frequently in the clinical literature and elevating the hypothesis linking hEDS-related ligament laxity to stretch/compression of the vagus nerve in the carotid sheath [13,14,15,16].
3. Significance of Upper Cervical Spine Anatomy
An emerging body of evidence suggests that structural abnormalities of the upper cervical spine, particularly craniocervical instability (CCI) and atlantoaxial instability (AAI), may contribute to or directly cause dysautonomic symptoms [17,18]. The cervical spine is comprised of seven vertebrae which, based on their anatomical characteristic are divided into two groups. The superior cervical group which is comprised of the posterior inferior aspect of the skull at CO (occiput), Cl (atlas), and C2 (axis), is essential for maintaining craniocervical stability, and is referred to as the craniocervical junction (CCJ), while the inferior cervical group is made up of C3 to C7 [19].
The CCJ comprises two distinct joints: the atlanto-occipital (AO) joint, which consists of the skull (occiput) which rests on the first cervical vertebra (atlas), and the atlantoaxial (AA) joint, where the atlas connects with the axis. This region contains several ligaments, muscles, small joints called facet joints, and occiput condyles (OC) which support the head and enable it to move in multiple directions, as well as providing stability.
Unlike vertebrae C3-C7 which are relatively uniform in shape and appearance [20], the atlas and axis possess unique anatomical features. The atlas (C1) lacks a vertebral body and spinous process and is considered atypical. To compensate for this absence of a vertebral body there are anterior and posterior arches that are joined on each side by a lateral mass. Each lateral mass comprises a kidney-shaped articular facet that enables it to articulate with the occiput above, forming the AO joint. Each facet has a transverse process that contain a foramen for the passage of nerves and blood vessels, while the anterior and posterior arches and the two lateral masses form a central ring-like anatomical space called the vertebral canal, which provides a passage for the spinal cord [21].
The stability of this segment of the vertebral column relies on the integrity of the cervical ligaments, and any decrease in ligament strength can directly impact spinal stability [22,23]. This stability primarily relies on the Posterior Ligamentous Complex (PLC), also referred to as the posterior tension band, which consists of the supraspinous ligament (SSL), interspinous ligament (ISL), ligamentum flavum (LF), and facet joint capsules (FJCs) [24,25]. It is thus postulated that the inherent laxity in hEDS leads to cervical spine ligament instability and the loss of cervical lordosis, forward translation of C1, and encroachment on the carotid sheath, thus compressing the vagus nerve and internal jugular vein [26,27].
Anatomically, a set of 12 nerves known as the cranial nerves emerge directly from the brainstem and comprises of both motor and sensory nerves which are responsible for several physiological processes, including vision, olfaction, audition, and complex facial movements. Any compromise of any of these nerves such as compression can manifest in various symptoms depending on the nerve affected and the extent of compression, particularly relevant in the case of CN X, known as the vagus nerve [28,29]. Derived from the Latin word for “wandering, straying”, the vagus nerve originates in the brainstem and terminates in the splenic flexure of the colon [30]. Along its anatomical course, the vagus nerve makes a 90° turn at the level of the C1 (atlas) vertebra; thus, any changes in cervical spine positioning, i.e., such as loss of normal lordosis due to cervical ligamentous laxity which can lead to instability, are recognized as increasing the vagus nerve’s susceptibility to kinking and compression, potentially and thus contributing to symptoms of dysautonomia [31]. The authors of other studies have recognized that the anatomical proximity of the upper cervical spine to critical neurovascular structures—including the brainstem, vagus nerve, and carotid arteries which creates potential for mechanical compression when ligamentous laxity secondary to EDS permits excessive vertebral motion [32,33]; thus, in theory, a treatment method specifically for ligament laxity in the upper cervical spine could facilitate a reduction in or complete elimination of ligamentous laxity and as a consequence the elimination of cervical instability and its effect on the vagus nerve, culminating in the reduction in or elimination of dysautonomia symptoms associated with its compression.
4. Current Treatment Options
There is a lack of published literature on the various methods used for the treatment of hEDS patients, particularly those suffering from upper cervical spine instability with current treatment modalities limited to surgical interventions that carry significant risks and conservative therapies demonstrating variable efficacy [34].
Among the treatments currently available to patients suffering from upper cervical instability is surgery. While Henderson, et al. in their study examining post-operative outcomes, concluded that patients who underwent occipitocervical fusion with intraoperative reduction exhibited significant improvements, with the most significant improvements being pain reduction (63%),reduction in cardiac palpitations (55%), improved orthostatic tolerance (52%), and a reduction in chronic fatigue (48%), they noted that the procedure carries significant risks due to the proximity of the brainstem, spinal cord, and vertebral arteries, with a complication rate of 35.7% [35]. Postsurgical complications are also likely to arise due to abnormal connective tissue healing, in addition to muscle deconditioning [36,37].
Alternatives to surgical intervention include chiropractic care [38,39,40], dietary supplements, massage therapy, acupuncture, and mindfulness/meditation [41]. More recently regenerative therapies for EDS have emerged, with the aim of stimulating the body’s own repair mechanisms to strengthen lax connective tissues, such as prolotherapy, which involves injecting an irritant solution (most commonly a dextrose solution combined with a local anesthetic) into injured or lax ligaments, tendons, or joint capsules. The mild irritation triggers a localized inflammatory response, which in turn recruits fibroblasts and growth factors to the area, promoting newly synthesized collagen and tissue strengthening. In essence, prolotherapy induces a controlled “micro-injury” to initiate the body’s repair of chronically damaged or overstretched connective tissue [42].
Another emerging therapy for hEDS is Platelet-Rich Plasma (PRP) Therapy, which involves the utilization of the patient’s own blood plasma enriched with a high concentration of platelets. A sample of blood is drawn and processed (centrifuged) to isolate platelets and growth factors, which are then injected into the target tissue (e.g., around loose ligaments or into a damaged joint). Platelets naturally release numerous growth factors and cytokines that are delivered directly to sites of tissue weakness or injury, amplifying the regenerative signal and orchestrate tissue repair. PRP essentially provides a stronger healing stimulus than prolotherapy alone, as platelets actively secrete proteins that stimulate cell proliferation, blood vessel growth, and collagen synthesis. Similar to prolotherapy, PRP injections are usually administered under ultrasound guidance [43,44].
A more recent development in the treatment of Ehlers–Danlos patients is stem cell therapy (Mesenchymal Stem Cells.) While the safety of stem cell therapy in patients has been documented [45], and early reports and case examples illustrating the potential benefits of mesenchymal stem cells for certain EDS complications have been published [46] large-scale clinical trials in EDS remain lacking. The clinical use involves autologous MSCs. These are harvested from the patient (generally from bone marrow or adipose tissue) and delivered either to specific sites of injury or systemically. MSCs can differentiate into connective tissue cells (such as fibroblasts, cartilage, or bone cells) and also secrete anti-inflammatory and growth factors that aid tissue regeneration. While all three therapies have exhibited varied success, it should be noted that they all involve injections, which carry certain inherent risks. Injection site infection is a rare but serious risk in any treatment involving needles [47]. Additionally, immunocompromised EDS patients or those with vascular EDS require specific caution [48]. Bleeding or bruising can occur, particularly in vascular EDS, in which vessels are fragile, whereby even a minor injection could potentially cause a vascular injury or hematoma; any procedure must therefore be weighed against the potential risk [49]. Nerve damage while an uncommon complication of injection indirect damage can occur during procedures such as prolotherapy due to the use of an inflammatory agent, which can cause a flare-up of pain and swelling post-injection. This situation is generally temporary (days) and is part of the expected inflammatory reaction; in some cases, however, it can be more intense or prolonged. Rare cases of more severe reactions to prolotherapy have also been reported, such as ligament rupture or spinal headaches, in cases involving injections in anatomically sensitive areas or those not involving imaging guidance [50]. Because PRP, is autologous, it carries a very low risk of allergic reaction. Stem cell therapy risks depend on the source and method of delivery; autologous MSC injections share similar risks to PRP (in addition to the minor risk from the harvesting procedure, e.g., pain at the bone marrow puncture site); in comparison, allogeneic stem cells could, in theory, pose risks of immune reaction or disease transmission if not appropriately processed and administered [51].
In light of the above findings, we thus propose a novel use of a non-interventional therapeutic utilizing extracorporeal shock wave therapy (ESWT) to strengthen cervical ligamentous structures, thereby reducing upper cervical instability and vagus nerve compression and thus alleviating dysautonomia symptoms.
5. A Novel Therapeutic Approach to EDS: Extracorporeal Shock Wave Therapy
Extracorporeal shockwave therapy (ESWT) is a non-invasive intervention technique that has been used for over three decades. It was initially applied in urology and has evolved to treat various musculoskeletal pathologies [52,53]. In 2000, plantar fasciitis was the first orthopedic condition to receive United States Food and Drug Administration approval for shockwave management [54], followed by approval for lateral epicondylitis in 2002 [55] and diabetic foot ulcers in 2017 [56]. Subsequently, the list of conditions considered to benefit from ESWT was expanded to include additional indications; however, the vast majority of its clinical use remains off-label. Over the past decade, there has been a significant expansion of studies on central and peripheral nervous system application [57,58], in addition to degenerative diseases [59,60,61]. Extracorporeal shock wave therapy (ESWT) has emerged as a regenerative medicine modality with proven efficacy in musculoskeletal disorders, including tendinopathies, ligament injuries, and bone healing [62,63]. ESWT has been demonstrated to increase the expression of growth factors such as vascular endothelial growth factor (VEGF) and transforming growth factor-beta (TGF-β), which play crucial roles in angiogenesis and tissue healing. Enhanced blood flow and nutrient delivery to the affected area can accelerate the healing process and reduce inflammation [64]. This shift in the inflammatory milieu can contribute to pain relief and improved tissue health [65].
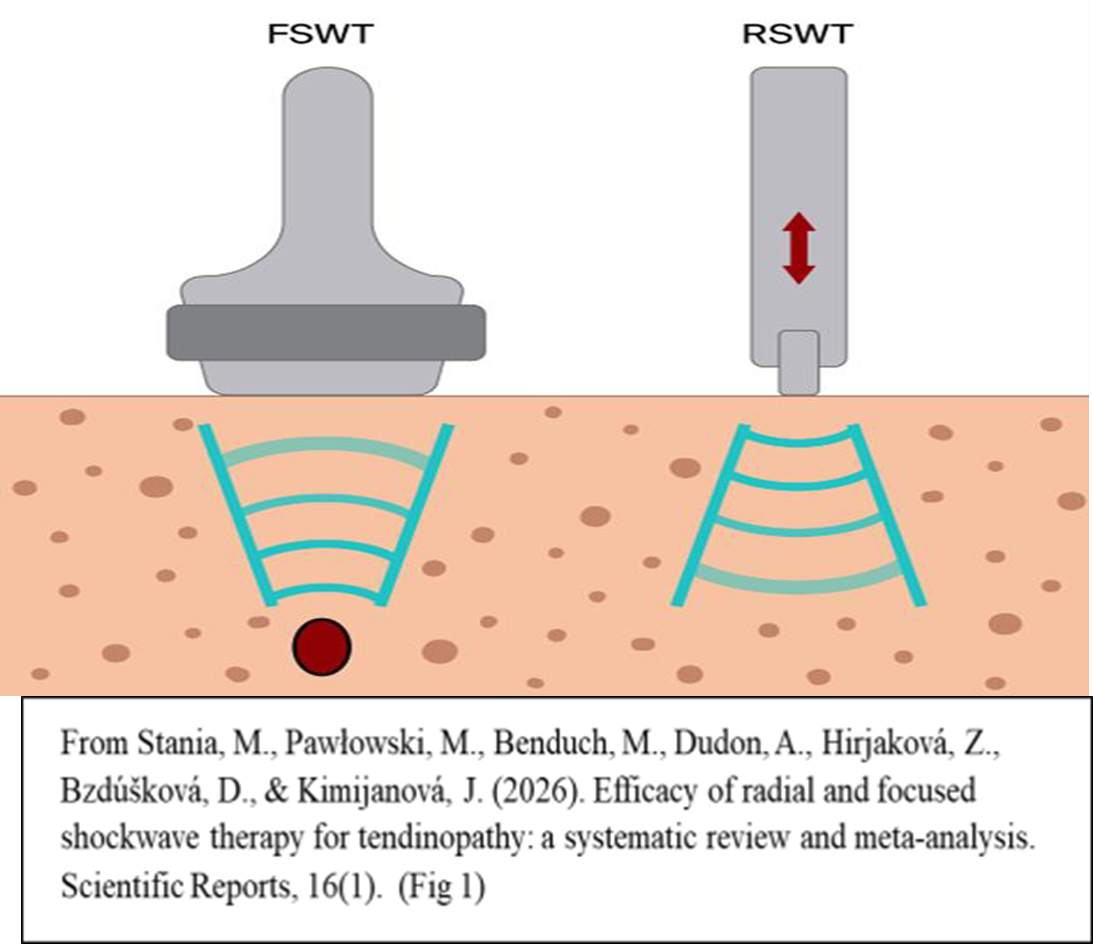
From a technical standpoint, two types of ESWT exist: focused ESWT (f-ESWT) and radial shock wave therapy (r-ESWT). While the two differ in their clinical applications, they share several clinical indications. The main differences between r-ESWT and f-ESWT lie in the pressure levels, depth of penetration, the pulse duration and the distribution field. r-ESWT enables the treatment of not only localized lesions but also more extensive tissue changes, as the wave energy disperses radially within the tissues [66]. In f-ESWT the entire energy of the shock wave is concentrated at a specific focal point and depth within the tissues, precisely targeting areas with pathological changes [67]. Both methods of shock wave application have become widely used in the treatment of various musculoskeletal disorders [68]. In one study, in which the authors compared the two types of ESWT in the treatment of coccydynia, the findings indicated both wave types (radial and focused) to be effective in terms of pain and function. However, due to the presence of pain and inflammation in the surrounding ligaments and muscles in coccydynia, it was determined that r-ESWT, rather than deep-impact focused f-ESWT, would be a more suitable choice when treating this condition [69]. The authors of other studies found that both types of ESWT effectively alleviate pain in myofascial pain syndromes, with no long-term differences between them [70]. The primary clinical decision on which equipment to use, f-ESWT or r-ESWT, is essentially the depth and location of the target pathology. (Figure 1).
An effective measure is to choose f-ESWT when the pathology is deep (typically >4–5 cm, up to ~12 cm effective penetration) and opt for r-ESWT when the pathology is superficial (effective up to ~3–4 cm) [71]. The mechanistic basis of ESWT involves mechanical stimulation, termed mechanotransduction, by which the mechanical energy from shock waves is converted into biochemical signals that stimulate tissue repair and structural reinforcement of the cellular processes, which include the proliferation of fibroblasts, collagen synthesis, growth factor release, and neovascularization [72,73].
To date, no studies in humans have directly measured biomechanical strength in cervical ligaments after ESWT; however, certain indicators, such as ultrasound evidence of decreased ossification of the nuchal ligament, indicating demineralization and potential remodeling, have been demonstrated [74]. This finding is significant as calcification stiffens ligaments, reducing tensile strength [75]. The results of a study by Li et.al. demonstrated increased range of motion and improved scores on the Neck Disability Index (NDI) following use of ESWT [76]. Together, these lines of evidence make ligamentous strengthening, with its decrease in cervical instability, particularly in patients with hEDS, via ESWT a credible hypothesis.
References
- Tinkle, B.; Castori, M.; Berglund, B.; Cohen, H.; Grahame, R.; Kazkaz, H.; Levy, H. Hypermobile Ehlers-Danlos syndrome (a.k.a. Ehlers-Danlos syndrome type III and Ehlers-Danlos syndrome hypermobility type): clinical description and nat-ural history. Am. J. Med. Genet C. Semin Med. Genet. 2017, 175, 48–69. [Google Scholar] [CrossRef]
- Malfait, F.; Francomano, C.; Byers, P.; et al. The 2017 international classification of the Ehlers-Danlos syndromes. Am. J. Med. Genet C. Semin Med. Genet. 2017, 175, 8–26. [Google Scholar] [CrossRef]
- Malek, S.; Reinhold, E.J.; Pearce, G.S. The Beighton Score as a measure of generalised joint hypermobility. Rheumatol. Int. 2021, 41(10), 1707–16. [Google Scholar] [CrossRef]
- Childs, Sharon G. Musculoskeletal Manifestations of Ehlers–Danlos Syndrome. Orthop. Nurs. 2010, 29(2), 133–139. [Google Scholar] [CrossRef]
- Celletti, C.; Camerota, F.; Castori, M.; Censi, F.; Gioffrè, L.; Calcagnini, G.; Strano, S. Orthostatic intolerance and postural orthostatic tachycardia syndrome in joint hypermobility syndrome/Ehlers-Danlos syndrome, hypermobility type: neu-rovegetative dysregulation or autonomic failure? Biomed. Res. Int. 2017, 2017, 9161865. [Google Scholar] [CrossRef] [PubMed]
- Hauser, R.A.; Matias, D.; Rawlings, B.R. Cervicovagopathy: ligamentous cervical instability and dysstructure as a poten-tial etiology for vagus nerve dysfunction in the cause of human symptoms and diseases. Front Neurol. 2025, 16, 1572863. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aziz, Q.; Harris, L.A.; Goodman, B.P.; Simrén, M.; Shin, A. AGA Clinical Practice Update on GI Manifestations and Auto-nomic or Immune Dysfunction in Hypermobile Ehlers-Danlos Syndrome: Expert Review. Clin. Gastroenterol. Hepatol. Epub. 2025, 23(8), 1291–1302. [Google Scholar] [CrossRef] [PubMed]
- Auricular Vagal Nerve Stimulation for Hypermobile Ehlers-Danlos Syndrome Study Details | NCT05212129 | Au-ricular Vagal Nerve Stimulation for Hypermobile Ehlers-Danlos Syndrome | ClinicalTrials.gov. Accessed. (accessed on 04/12/2025).
- Transcutaneous Auricular Vagus Nerve Stimulation in Postural Tachycardia Syndrome: a Prospective Cross-over Study Study Details | NCT07163130 | Tragus Stimulation for POTS Treatment | ClinicalTrials.gov.
- Parapia, L.A.; Jackson, C. Ehlers-Danlos syndrome--a historical review. Br. J. Haematol. 2008, 141(1), 32–5. [Google Scholar] [CrossRef] [PubMed]
- McKusick, V.A. Heritable disorders of connective tissue: IV. The Ehlers-Danlos syndrome, Journal of Chronic Diseases, 3, (1) 1956, pp 2-24, ISSN 0021-9681, https://doi.org/10.1016/0021-9681(56)90095-9. (https://www.sciencedirect.com/science/article/pii/0021968156900959). [CrossRef]
- Bloom, L.; Byers, P.; Francomano, C.; Tinkle, B.; Malfait, F. Steering Committee of The International Consortium on the Ehlers-Danlos Syndromes. The international consortium on the Ehlers-Danlos syndromes. Am. J. Med. Genet C. Semin Med. Genet 2017, 175(1), 5–7. [Google Scholar] [CrossRef] [PubMed]
- Zaborowska-Sapeta, K.; Tymińska-Wójcik, P.; Sonza, A.; Kluszczyński, M.; Skowrońska, A. The impact of modern lifestyles on spinal health in the pediatric population: a narrative review. Children 2026, 13(3), 341. [Google Scholar] [CrossRef] [PubMed]
- Hauser, R. A.; Griffiths, M.; Watterson, A.; Matias, D.; Rawlings, B. R. Characterizing Initial Cervical Spine and Neurovascular Findings in 84 Consecutive Patients with Hypermobile Ehlers–Danlos Syndrome: A Retrospective Study. J. Clin. Med. 2026, 15(6), 2212. [Google Scholar] [CrossRef]
- Weiner, G. Atrial Fibrillation and its relationship with Thoracic Outlet Syndrome. Asia-Pac Chiropr J. 2025, 6.2. Available online: www.apcj.net/papersissue-6-2/#WeinerAFib.
- Hauser, R. A.; Griffiths, M.; Watterson, A.; Matias, D.; Rawlings, B. Objective test findings in patients with chronic eye symptoms seeking care at an outpatient neck center: ligamentous cervical instability etiology? Front. Neurol. 2025, 16, 1576315. [Google Scholar] [CrossRef]
- Henderson, F. C.; et al. Neurological and spinal manifestations of the Ehlers-Danlos syndromes. Am. J. Med. Genet. Part C. Semin. Med. Genet. 2018, 175(1), 195–211. [Google Scholar] [CrossRef]
- Centenera, M.; et al. Craniocervical instability and vagus nerve compression. Centeno-Schultz Blog. 2021. Available online: https://centenoschultz.com/.
- Kim, D.H.; Vaccaro, A.R.; Dickman, C.A.; Cho, D.; Lee, S.; Kim, I. Surgical Anatomy and Techniques to the Spine; Elsevier: Amsterdam, Netherlands, 2013. [Google Scholar]
- Vernon, L. F.; Benn, A. Documenting Cervical Spine Injuries Following Negative MRI Findings: Clinical and Medico-Legal Overview of Dynamic Imaging. Cureus 2025, 17(7), e88121. [Google Scholar] [CrossRef] [PubMed]
- Rajani, S. Is variant anatomy of atlas clinically important? A review. Basic Sci. Med. 2014, 3, 1–7. [Google Scholar]
- Ivancic, P.C.; Ito, S.; Tominaga, Y.; et al. Whiplash causes increased laxity of cervical capsular ligament. Clin. Biomech. 2008, 23, 159–65. [Google Scholar] [CrossRef]
- Tominaga, Y.; Ndu, A.B.; Coe, M.P.; et al. Neck ligament strength is decreased following whiplash trauma. BMC Muscu-Loskelet Disord. 2006, 7, 103. [Google Scholar] [CrossRef] [PubMed]
- Holdsworth, F.W. Fractures, dislocations and fracture-dislocations of the spine. J. Bone Jt. Surg. Am. 1970, 52, 1534–51. [Google Scholar] [CrossRef]
- Magerl, F.; Aebi, M.; Gertzbein, S.D.; et al. A comprehensive classication of thoracic and lumbar injuries. Eur. Spine J. 1994, 3, 184–201. [Google Scholar] [CrossRef]
- DePace, N. L.; Soloway, S.; Yayac, M.; Colombo, J. Spine and Organ Involvement. In Ehlers-Danlos/Hyper-mobility Syndromes and Other Connective Tissue Disorders: Assessments, Diagnostics, and Therapies; Springer Nature Switzerland: Cham, 2025; pp. 163–190. [Google Scholar]
- Mehta, D.; Simmonds, L.; Hakim, A.J.; Matharu, M. Headache disorders in patients with Ehlers-Danlos syn-dromes and hypermobility spectrum disorders. Front. Neurol. 2024, 15, 1460352. [Google Scholar] [CrossRef]
- Borghei-Razavi, H.; Darvish, O.; Schick, U. Disabling vertigo and tinnitus caused by intrameatal compression of the anterior inferior cerebellar artery on the vestibulocochlear nerve: a case report, surgical considerations, and review of the literature. J. Neurol. Surg. Rep. 2014, 75, e47-51. [Google Scholar] [CrossRef]
- Verma, R.; Junewar, V.; Garg, R.K.; Malhotra, H.S. A rare case of basilar impression. BMJ Case Rep. 2012, 2012. [Google Scholar] [CrossRef]
- Baquiran, M.; Bordoni, B. Anatomy, head and neck: anterior vagus nerve. In StatPearls [Internet]; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Zimmerman, E.E.; Misulis, K.E. Chapter 3.4: brainstem and cranial nerves. In Neurologic Localization and Diagnosis; Zim-merman, E.E., Samuels, M.A., Kirshner, H.S., Eds.; Elsevier: Amsterdam, Netherlands, 2023; pp. 89–106. [Google Scholar] [CrossRef]
- Centenera, M.; et al. Craniocervical instability and vagus nerve compression. Centeno-Schultz Blog. 2021. Available online: https://centenoschultz.com/.
- Gilete, J. Craniocervical instability: Causes & treatment. 2025. Available online: https://drgilete.com/specialties/craneocervical-instability-cci/.
- Daylor, V.; Griggs, M.; Weintraub, A.; Byrd, R.; Petrucci, T.; Huff, M.; Norris, R. A. Defining the Clinical Complexity of hEDS and HSD: A Global Survey of Diagnostic Challenge, Comorbidities, and Unmet Needs. medRxiv 2025, 2025–06. Available online: https://www.medrxiv.org/content/medrxiv/early/2025/06/06/2025.06.05.25329074.full.pdf. [CrossRef]
- Henderson, F.C., Sr.; Francomano, C.A.; Koby, M.; Tuchman, K.; Adcock, J.; Patel, S. Cranio-cervical instability in patients with Ehlers–Danlos syndrome: outcomes analysis of 103 surgically treated patients. Front. Surg. 2018, 5, 116. [Google Scholar]
- Henderson, F.C.; Schubart, J.R.; Narayanan, M.V.; et al. Craniocervical instability in patients with Ehlers-Danlos syn-dromes: outcomes analysis following occipito-cervical fusion. Neurosurg. Rev. 2024, 47, 27. [Google Scholar] [CrossRef]
- Eichinger, J.K.; Byrd, R.L.; Bailey, E.P.; Reis, R.J.; Daylor, V.; Schiessl, M.; Gensemer, C.; Friedman, R.J.; Patel, S.J.; Norris, R.A. Or-thopaedic Manifestations in Hypermobile Ehlers-Danlos Syndrome. J. Bone Jt. Surg. Am. 2025, 107(16), 1848–1856. [Google Scholar] [CrossRef] [PubMed]
- Chu, E.C.P.; Lin, A.F.C. Relief of postural orthostatic tachycardia syndrome with chiropractic rehabilitation. J. Fam. Med. Prim. Care 2022, 11(7), 4006–4009. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- La Francis, M.E. A chiropractic perspective on atlantoaxial instability in Down’s syndrome. J. Manip. Physiol. Ther. 1990, 13(3), 157–60. [Google Scholar] [PubMed]
- Katz, E. A.; Katz, S. B.; Freeman, M. D. Non-Surgical Management of Upper Cervical Instability via Im-proved Cervical Lordosis: A Case Series of Adult Patients. J. Clin. Med. 2023, 12(5), 1797. [Google Scholar] [CrossRef] [PubMed]
- Doyle, T.A.; Halverson, C.M.E. Use of complementary and alternative medicine by patients with hypermobile Ehlers-Danlos Syndrome: A qualitative study. Front Med. 2022, 9, 1056438. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Baquiran, M.; Bordoni, B. Anatomy, head and neck: anterior vagus nerve. In StatPearls [Internet]; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Letson, A. K.; Dahners, L. E. The effect of combinations of growth factors on ligament healing. Clin. Orthop. Relat. Res. (1976-2007) 1994, 308, 207–212. [Google Scholar] [CrossRef]
- Fang, J.; Wang, X.; Jiang, W.; Zhu, Y.; Hu, Y.; Zhao, Y.; Wang, Y. Platelet-rich plasma therapy in the treatment of diseases associated with orthopedic injuries. Tissue Eng. Part B Rev. 2020, 26(6), 571–585. [Google Scholar] [CrossRef]
- Centeno, C.J.; Al-Sayegh, H.; Freeman, M.D.; et al. A multi-center analysis of adverse events among two thousand, three hundred and seventy two adult patients undergoing adult autologous stem cell therapy for orthopaedic condi-tions. Int. Orthop. (SICOT) 2016, 40, 1755–1765. [Google Scholar] [CrossRef] [PubMed]
- Hauser, R. A.; Orlofsky, A. Regenerative injection therapy with whole bone marrow aspirate for degenera-tive joint disease: a case series. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2013, 6, CMAMD–S10951. [Google Scholar] [CrossRef] [PubMed]
- Arita, A.; Tobita, M. Adverse events related to platelet-rich plasma therapy and future issues to be resolved. Regen. Ther. 2024, 26, 496–501. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Eymard, F.; Louati, K.; Noel, É.; Abouqal, R.; et al. Indications and contraindications to platelet-rich plasma injections in musculoskeletal diseases in case of infectious, oncological and haematological comorbidities: A 2025 formal consensus from the GRIIP (International Research Group on Platelet Injections). Knee Surg Sports Traumatol Arthrosc. 2025 Jun;33(6):2293-2306. Epub 2025 Apr 22. [CrossRef] [PubMed] [PubMed Central]
- Artoni, A.; Bassotti, A.; Abbattista, M. Hemostatic abnormalities in patients with Ehlers–Danlos syndrome. J. Thromb. Haemost. 16, 2425–2431. [CrossRef]
- Hunt, W. E.; Baird, W. C. Complications following injection of sclerosing agent to precipitate fibro-osseous proliferation. J. Neurosurg. 1961, 18(4), 461–465. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Huang, X.; Wang, H.; Liu, X.; Zhang, T.; Wang, Y.; Hu, D. The challenges and promises of allogeneic mesenchymal stem cells for use as a cell-based therapy. Stem Cell. Res. Ther. 2015, 6, 234. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schmitz, C.; Császár, N.B.; Milz, S.; Schieker, M.; Maffulli, N.; mpe, J.D.; et al. Efficacy and safety of extracorporeal shock wave therapy for orthopedic conditions: a systematic review on studies listed in the PEDro database. Br. Med. Bull. 2015, 116(1), 115–38. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chaussy, C.; Eisenberger, F.; Forssmann, B. Extracorporeal shockwave lithotripsy (ESWL): a chronology. J. Endourol. 2007, 21(11), 1249–53. [Google Scholar] [CrossRef] [PubMed]
- Konjen, N.; Napnark, T.; Janchai, S. A comparison of the effectiveness of radial extracorporeal shock wave therapy and ultrasound therapy in the treatment of chronic plantar fasciitis: a randomized controlled trial. J. Med. Assoc. Thai 2015, 98 Suppl 1, S49–56. [Google Scholar] [PubMed]
- https://provider.univerahealthcare.com/documents/d/global/uni-prv-extracorporeal-shock-wave-therapy-eswt-for-musculoskeletal-conditions-and-soft-tissue-wounds#:~:text=The%20OssaTron%20device%20(HealthTron-ics%2C%20Inc,describes%20a%20low%2Ddose%20protocol.
- https://www.medscape.com/viewarticle/890703?form=fpf.
- Cao, B.; Tang, X.; Liu, C.; Xu, G.; Lei, M.; Wu, F.; Chen, W.; Ni, H.; Zhang, F. Unlocking new Frontiers: The cellular and molec-ular impact of extracorporeal shock wave therapy (ESWT) on central nervous system (CNS) disorders and peripheral nerve injuries (PNI). Exp. Neurol. 2025, 384, 115052. [Google Scholar] [CrossRef] [PubMed]
- Leuk, J.S.P.; Low, L.L.N.; Teo, W.-P. An Overview of Acoustic-Based Interventions to Improve Motor Symptoms in Parkinson’s Disease. Front. Aging Neurosci. 2020, 12, 243. [Google Scholar] [CrossRef] [PubMed]
- Simplicio, C.L.; Jácomo, A.A.E.; de Barros. GAM | Treatment with Shockwave Therapy in a Patient with Joint Hypermo-bility and Temporomandibular Dysfunction | Journal of Regenerative Science. 2024, 4(1), 09–15. [Google Scholar]
- Kou, D.; Chen, Q.; Wang, Y.; et al. The application of extracorporeal shock wave therapy on stem cells therapy to treat various diseases. Stem Cell. Res. Ther. 2024, 15, 271. [Google Scholar] [CrossRef]
- Zhai, L.; Sun, N.; Zhang, B.; Liu, S.T.; Zhao, Z.; Jin, H.C.; Ma, X.L.; Xing, G.Y. Effects of Focused Extracorporeal Shock Waves on Bone Marrow Mesenchymal Stem Cells in Patients with Avascular Necrosis of the Femoral Head. Ultrasound Med. Biol. 2016, 42(3), 753–62. [Google Scholar] [CrossRef] [PubMed]
- Wang, C. J. Extracorporeal shockwave therapy in musculoskeletal disorders. J. Orthop. Surg. Res. 2012, 7(1), 11. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC3666498/. [CrossRef]
- Moya, D.; et al. The biological effects of extracorporeal shock wave therapy on tendon injury. Interna-Tional J. Mol. Sci. 2018, 19(11), 3567. [Google Scholar]
- Venosa, M.; Vespasiani, A.; Romanini, E.; Nigri, M.; Fidanza, A.; Logroscino, G. Radial Extracorporeal Shockwave Therapy for the Treatment of Chronic Refractory Coccygodynia. J. Med. Cases 2025, 16(12), 467–474. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De la Corte-Rodriguez, H.; Roman-Belmonte, J.M.; Rodriguez-Damiani, B.A.; Vazquez-Sasot, A.; Rodriguez-Merchan, E.C. Extracor-poreal shock wave therapy for the treatment of musculoskeletal pain: a narrative review. Healthcare 2023, 11(21), 2830. [Google Scholar] [CrossRef]
- Novak, P. Physics: F-SW and R-SW. Basic information on focused and radial shock wave physics. In Multidisciplinary Medical Applications; Lohrer, H., Gerdesmeyer, L., Eds.; Level 10 Buchverlag Daniela Bamberg, 2015; pp. 28–49. [Google Scholar]
- Ogden, J. A.; Tóth-Kischkat, A.; Schultheiss, R. Principles of shock wave therapy. Clin. Orthop. Relat. Res. 2001. [Google Scholar] [CrossRef]
- Al-Abbad, H.; et al. The effects of shockwave therapy on musculoskeletal conditions based on changes in imaging: A systematic review and meta-analysis with meta-regression. BMC Musculoskelet. Disord. 2020, 21, 1–26. [Google Scholar] [CrossRef]
- Şah, V.; Elasan, S.; Kaplan, Ş. Comparative effects of radial and focused extracorporeal shock wave therapies in coccydynia. Turk. J. Phys. Med. Rehabil. 2023, 69(1), 97–104. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Şenlikci, H. B.; Yücealp, Ö.; Borman, P.; Ince Keskin, Z.; Gümüş Atalay, S.; Yaşar, E. Comparison of the efficacy of radial and focused extracorporeal shock-wave therapy (ESWT) in myofascial pain syndrome: a randomized, sham-controlled study. Lasers Med. Sci. 2025, 40(1), 404. [Google Scholar] [CrossRef] [PubMed]
- https://shockwavetherapy.org/wp-content/uploads/2024/01/ISMST-Guidelines-for-ESWT-_-engl-20240103.pdf.
- d’Agostino, M. C.; et al. Shock wave as biological therapeutic tool: From mechanical stimulation to recovery and healing. Perspect. Med. 2015, 4(1), 183–197. [Google Scholar]
- Chung, B.; Wiley, J. P. Effectiveness of extracorporeal shock wave therapy in the treatment of previ-ously untreated lateral epicondylitis. Clin. Sport Med. 2002, 12(5), 266–270. [Google Scholar]
- Lin, T.-Y.; Chen, J.-T.; Chen, Y.-Y.; Chen, T.-W.; Lee, C.-L.; Chen, C.-H.; Huang, M.-H. The efficacy of ultrasound-guided extracorporeal shockwave therapy in patients with cervical spondylosis and nuchal ligament calci-fication. Kaohsiung J. Med. Sci. 2015, 31, 337–343. [Google Scholar] [CrossRef]
- Fiani, B.; Davati, C.; Griepp, D.W.; Lee, J.; Pennington, E.; Moawad, C.M. Enhanced Spinal Therapy: Extracorporeal Shock Wave Therapy for the Spine. Cureus 2020, 12(10), e11200. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, S.; Liu, J.; Wang, Y.; Zhu, C.; Tang, Y.; Gu, M. Clinical evaluation of the efficacy of focused extracorporeal shock-wave therapy in patients with cervical spondylosis: A randomized control trial. Medicine 2024, 103(46), e40573. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



